Embed Size (px)
Citation preview

20 years of experience in HIV cure research: redefining the challenge
Doug RichmanBarcelona
23 October 2019
RAVEN

§ What have we learned in 20+ years?
§ What do we still need to figure out?

NATURE MEDICINE, VOLUME I, NUMBER 12, 1284, DECEMBER 1995

Chun . . . Siliciano, NATURE I VOL 38718 MAY 1997
§ Provirus and latent virus found in both LN and PBMC.§ Most integrated DNA found not to be replication competent. Note the cells studied were during ongoing infection.

Perelson et al., Nature 1997
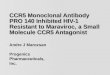
1996-7: HIV Cure Possible?
Years on ART-1 0 1 2 3 4 5 6 7
Plas
ma
HIV
-1 R
NA
(cop
ies/
mL
10-1
100
101
102103
104
105
106
107
Clinical LOD(50 copies/mL)
Initiate ART
Phase It½ = 1.5 days
Phase IIt½ = 28 days
Eradication?

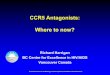
HIV Cure “Impossible”: 1997-2009
SCIENCE VOL. 278 * 14 NOVEMBER 1997
§ In contrast to the optimism for ART leading to cure, latency proves to be the obstacle.§ Archiving of both WT and drug resistant latent HIV in pre-treated subjects indicates latency established during
the course of infection (Wong et al, Finzi et al).§ No new drug resistance mutations from pre-treatment plasma virus to latent virus suggests no evolution
throughout ART (Wong et al).

§ HIV drug resistance and sequence evolution occurred after 1 or 2 in treated subjects with viral
“blips” and low levels of ongoing replication, but not in those fully suppressed on ART. Both blood
and lymph nodes tested.
§ With 10-20 years of follow-up and more sophisticated deep sequencing, we now have stronger
confirmatory evidence of no ongoing replication in highly adherent individuals.

0.00010.0010.010.1
110
1001000
10000
0 1 2 3 4 5 6 7Time on HAART (years)
Freq
uenc
y(p
er 1
06ce
lls)
Slow decay of latently infectedCD4+ T cells
-
Time to eradication> 73.4 years
0.00001
Siliciano JD, et al. Nature Med. 2003;9:727-728.Chun TW, et al. Nature Med. 1995;1:1284-1290.Chun TW, et al. Nature. 1997;387:183:188.
Finzi D, et al. Science. 1997;278:1295-1300.Wong JK, et al. Science. 1997;278:1291-1295.Chun TW, et al. PNAS. 1997;94:13193-13197 Finzi D, et al. Nature Med. 1999;5:512-517.



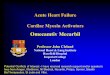
0
20
40
60
80
100
TN TTDTCM
CD45RACCR7CD27
+++
+--
-++
TTM TEM
--+
---
Cont
ribut
ion
(%) t
o th
e HI
V re
serv
oir s
ize
HIV persists in central and transitional memory CD4 T cells
Contribution of CD4 T cell subsets to HIV persistence
Chomont et al. Nat Med 2009

MJ Buzón et al
OTHER QUESTIONS:
1.Other lymphocytes to consider: Th17, Tfh , γδ T cells, Trm
2. Proportions of cells in each subset with replication competent proviruses and clonally proliferated viruses.
3. Macrophage and other reservoirs.

Ho et al, Cell 2013

Siliciano and Siliciano, Current Topics in Microbiology and Immunology (2018) 417:23–41

The Berlin Patient
Hütter G et al. N Engl J Med 2009;360:692-698.
CCR5 ∆∆32
CCR5 ∆∆32No AMLNo HIV
CCR5 WTAMLHIV
SCT x 2
Chemo and Rad
GVHD
N Engl J Med. 2009; 360:692-8
Timothy Ray Brown, The American
‘Berlin Patient’

J Cohen Science 2014;345:495-496Published by AAAS
Gupta et al (Nature 2019) now ~ 2 years

What do we still need to figure out? (Research Opportunities)
1. How is latency established and maintained?
2. What cellular targets are candidates for drug discovery to activate latent
virus safely (”shock and kill”)?
3. Is “block and lock” logical?
4. Do our current regimens completely suppress replication?
5. What is the composition of the latent reservoir (size, cell types)?
6. Are the anatomic sanctuaries (CNS, genital tract, other) pharmacologic
sanctuaries?
7. Can drugs that induce HIV transcription result in cytolytic death or will an
additional factor be required?
8. Will gene therapy or immunologic interventions obviate the “shock and
kill” approach?
9. How do you measure the latent reservoir and the impact of candidate
eradication strategies?
10. Do translationally competent, but replication incompetent proviruses,
contribute to pathogenesis and merit measurement and targeting?

Is there a latent HIV reservoir in cells other than CD4+ lymphocytes?
§ Myeloid cells (tissue macrophages, microglia, but not monocytes are susceptible to HIV infection)§ Requires tissue, not blood§ Infectible in vitro and infected in vivo (and at high levels in late stage infection)§ In vitro, infected macrophages survive and produce infectious virus for many months.§ Terminally differentiated in vitro
§ In vivo, how long do infected myeloid cells survive and do they maintain a latent state and on ART?§ What is the T1/2 of infected myeloid cells in vivo?
§ Can infected myeloid cell self renew (proliferate) (Siekewe and Allen, Science, 2013), or are they all terminally differentiated?
§ Can they maintain a latent state in vivo and how long do they survive during ART?

Types of Cures

Strategies for cure: Unmet discovery opportunities
§ Eliminate residual virus replication and then eliminate latently infected cells (shock and kill)§ Cytolysis mediated by virus replication§ T cell killing of cells expressing viral antigens
§ Enhance HIV-specific immunity§ “therapeutic” vaccine§ anti-PD1/anti-PDL1§ bNAbs§ DARTs (Dual-Affinity Re-Targeting agents)
§ Cure or make cells “resistant” to HIV § Target HIV provirus (Zinc finger, CRISPR)§ Target CCR5 (Zinc finger, CRISPR)§ CAR T cells

“SHOCK” Candidates (LRAs)• PKC agonists
§ most potent activators but toxicity of concern• Brd4 inhibitors
§ JQ1 and analogs• TLR agonists
§ TLR-4, 7• Cytkokines
§ IL-15• SMAC mimetics (non-canonical NFkB)
§ AZD5582• HDACi
§ vorinostat, panobinostat, romidepsin
23

Find the Latently Infected Cell

QVOA, QVOA using digital ELISA or RNA PCR, and induced HIV RNA assays on the same CD4 cells in the RAVEN study (Mars et al, JID, in press)

Caveats to all assays
§ The measurable analytes represent only the “tip of the iceberg” of the reservoir that must be eradicated.§ There are perhaps 106-107 latently infected cells.§ As with cancer, the ultimate test for no residual reservoir is treatment
interruption. Absence of detection is not detection of absence.§ The extra-circulatory reservoir is not homogeneous and is difficult
to access. § Most published reports have inadequate validation of performance
characteristics.§ Which assays are best for measuring a reduction of the reservoir
requires an intervention that can reduce the reservoir.

The future of HIV Cure/RemissionHIV chemotherapy has been a major medical accomplishment over the past 2 decades and has dramatically reduced the morbidity and mortality of those with access to care. There are 2 major challenges for HIV research. § For HIV uninfected people, develop an HIV vaccine.§ For HIV infected people, develop approaches to cure the latent reservoir.
AZT was step 1 in the development of ART. We do not yet have an intervention (other than HCST) that reduces the latent reservoir by a measureable amount. The needs/research opportunities are boundless.
![Journal of Falkenhagen et al, J Antivir Antiretrovir 213 ... · CCR5 gene via Zinc finger nucleases [4], cleavage of CCR5 mRNA by multimeric ribozymes [5], inhibition of CCR5 mRNA](https://img.pdfslide.us/doc/110x75/5fd3f8f670db7b30b42beea9/journal-of-falkenhagen-et-al-j-antivir-antiretrovir-213-ccr5-gene-via-zinc.jpg)