Embed Size (px)
DESCRIPTION
klklkl
Citation preview

ACUTE PULMONARY INFECTIONS
Zen AhmadZen AhmadMedical Faculty, Sriwijaya UniversityMedical Faculty, Sriwijaya University

Case presentation
A 55-year-old male with a history of type 2 diabetes, presents with dyspnea, high fever, chills, and productive cough with purulent sputum for 2 days duration. He denies hemoptysis. He has smoked 2 packs of cigarettes a day for the past 20 years and drinks six beers a day.
On physical exam he appears acutely ill. His vital signs show a temperature of 40.2°C, pulse is 130 beats/minute, RR is 48x/per minute, BP is 113/60.
Lungs are dull to percussion and bronchial breath sound heard over the left lower lobe. Chest X-ray showed infiltrates in the left lower lobe.

Key clinical questions
1. What are the most likely diagnosis in this patient? 2. What are the most likely causative organisms in
this patient?3. What further diagnostic tests are recommended
for diagnosis? 4. What are the risk factors for pneumonia 5. Can this patient be treated as an outpatient or
should he be admitted?6. What antibiotic agent would be recommended for
this patient?

What are the most likely diagnosis in this patient?

Differential diagnostic
• Pneumonia• Tuberculosis• Acute bronchitis• Acute exacerbation of chronic bronchitis• Upper respiratory infection• Sinusitis• CHF• Asthma• Lung cancer

Definition of pneumonia
An acute infection of the lung parenchyma distal to the terminal bronchiole, associated with clinical or radiologic evidence of consolidation of part or parts of one or both lungs.
Terminology
• Community Acquired Pneumonia versus Community Acquired Pneumonia versus Nosocomial pneumonia (HAP; VAP, HCAPNosocomial pneumonia (HAP; VAP, HCAP
• Typical pneumonia versus atypical pneumoniaTypical pneumonia versus atypical pneumonia• Mild pneumonia; Moderate pneumonia and Mild pneumonia; Moderate pneumonia and
Severe pneumoniaSevere pneumonia• Lobar pneumonia; Bronchopneumonia and Lobar pneumonia; Bronchopneumonia and
PleuropneumoniaPleuropneumonia

Clinical manifestationsClinical manifestations
• Sudden onset of fever, chillsSudden onset of fever, chills• CoughCough• Sputum productionSputum production• Pleuritic chest painPleuritic chest pain• Dyspnea; TachypneaDyspnea; Tachypnea• TachycardiaTachycardia• Extra pulmonary symptoms (nausea, vomiting, Extra pulmonary symptoms (nausea, vomiting,
malaise, headache, myalgia)malaise, headache, myalgia)

Physical examinationsPhysical examinations
Sign of pulmonary consolidationSign of pulmonary consolidationo Restricted movement of the afflicated hemithoraxRestricted movement of the afflicated hemithoraxo Increased fremitus Increased fremitus o DullnessDullnesso Bronchial breath soundsBronchial breath soundso RalesRales

Clinical manifestations of pneumoniaClinical manifestations of pneumonia
FeaturesFeatures TypicalTypical AtypicalAtypical
OnsetOnsetAgeAgeAppearanceAppearanceFeverFeverRigorRigorCoughCoughSputumSputumExtra pulmonal Extra pulmonal Pleuritic chest pain Pleuritic chest pain Lung consolidationLung consolidationGram stain Gram stain WBC, difrential WBC, difrential Chest x-rayChest x-ray
SuddenSuddenYoungerYoungerToxicToxicHighHighCommonCommonProductiveProductivePurulentPurulentUncommonUncommonCommonCommonCommonCommonAbundant bacteriaAbundant bacteriaElevated; left shitElevated; left shitConsolidationConsolidation
Gradual Gradual Older Older Malaise, fatiqueMalaise, fatiqueLow gradeLow gradeUncommonUncommonNonproductiveNonproductiveMucoidMucoidCommonCommonUncommonUncommonUncommonUncommonRare bacteriaRare bacteriaNormal Normal Patchy, infiltratePatchy, infiltrate

Patient
- Acute (2 days) - Dyspnea, High fever, Chills- Productive cough, purulent
sputum - T: 39.8°C- Pulse: 130 x/minute- RR: 48x/per minute - Percussion: dull - Auscultation: bronchial breath
sound over the left lower lobe- CXR: infiltrates in the left lower
lobe.
- Sudden onset of fever- Shortness of breathShortness of breath - Productive cough, purulent
sputum- Pleuritic chest pain- Tachypnea - Restricted movement of the
afflicated hemithorax- Increased fremitus - Dullness- Bronchial breath sounds; Rales- CXR: infiltrates (lobar, multilobar, CXR: infiltrates (lobar, multilobar,
segmental) or pleural effusionssegmental) or pleural effusions
Pneumonia

What are the most likely causative organisms in this patient?

Microbial causes of pneumoniaMicrobial causes of pneumonia
CAP NosocomialPneumonia
Atypical Pneumonia
S.pneumoniaeS.pneumoniae
H.influenzaeH.influenzae
Moraxella catarrhalisMoraxella catarrhalis
S.aureusS.aureus
Gram negative bacilliGram negative bacilli
VirusVirus
Gram negative bacilliGram negative bacilli
S.aureusS.aureus
Pseudomonas aerugi-Pseudomonas aerugi-nosanosa
M.pneumoniaeM.pneumoniae
C.pneumoniaeC.pneumoniae
Legionella pneumophilaLegionella pneumophila
Woodhead M.Medicine International 1995; 31 (9)Woodhead M.Medicine International 1995; 31 (9)
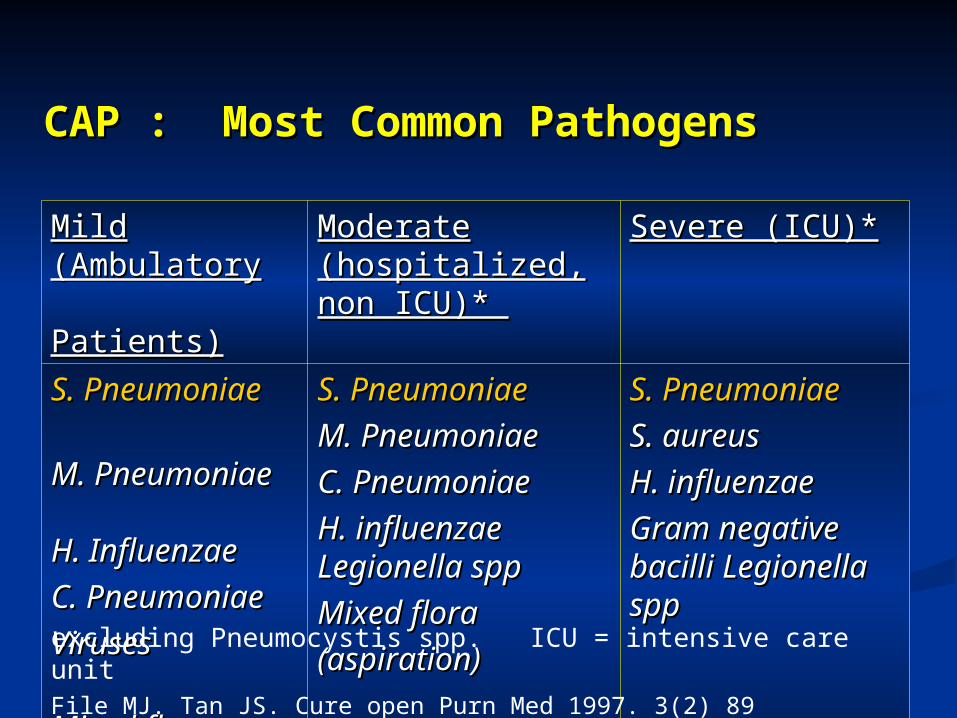
CAP : Most Common PathogensCAP : Most Common Pathogens
Mild (AmbulatoryMild (AmbulatoryPatients)Patients)
Moderate (hospitalized, Moderate (hospitalized, non ICU)* non ICU)*
Severe (ICU)*Severe (ICU)*
S. PneumoniaeS. Pneumoniae
M. PneumoniaeM. Pneumoniae H. Influenzae H. Influenzae
C. Pneumoniae C. Pneumoniae
VirusesViruses
Mixed flora Mixed flora
(aspiration)(aspiration)
S. PneumoniaeS. Pneumoniae
M. PneumoniaeM. Pneumoniae
C. PneumoniaeC. Pneumoniae
H. influenzaeH. influenzae Legionella spp Legionella spp
Mixed floraMixed flora
(aspiration)(aspiration)
S. PneumoniaeS. Pneumoniae
S. aureusS. aureus
H. influenzaeH. influenzae
Gram negative bacilli Gram negative bacilli Legionella sppLegionella spp
excluding Pneumocystis spp. ICU = intensive care unitFile MJ. Tan JS. Cure open Purn Med 1997. 3(2) 89

Bacterial Pathogens in CAPBacterial Pathogens in CAP
33,3%
20,8%16,7%
12,5%
12,5%
12,5%4,2%
No pathogen discover
Klebsiella
S. aureus
S. pneumoniae
Acinobacter
Pseudomonas
S.pyogenes
Persahabatan Hosp. 2000Persahabatan Hosp. 2000

What further diagnostic tests are recommended for diagnosis?

DiagnosticDiagnosticDiagnosticDiagnostic
• CXRCXR• Sputum examination Sputum examination • Blood count Blood count • Blood culturesBlood cultures• Serologic studies Serologic studies • Thoracentesis Thoracentesis • Invasive diagnostic proceduresInvasive diagnostic procedures
Transtracheal aspirationTranstracheal aspiration Bronchoscopy or BALBronchoscopy or BAL Direct needle aspirationDirect needle aspiration

CXRCXR
• CXR is the most important diagnostic toolCXR is the most important diagnostic tool
• New or progressive pulmonary infiltratesNew or progressive pulmonary infiltrates– Lobus consolidationLobus consolidation– Segmental consolidationSegmental consolidation– Patchy infiltratePatchy infiltrate
• Pulmonary cavitationsPulmonary cavitations
• LymphadenopathyLymphadenopathy
• PleuralPleural effusionseffusions

Lobar pneumonia

Location of pneumonia

Sputum examinationSputum examination
• The key factor to identification of the etiology The key factor to identification of the etiology
• Macroscopic; Gram stain and Sputum cultureMacroscopic; Gram stain and Sputum culture
• LowerLower sensitivitysensitivity
30–50% pathogen could not identified30–50% pathogen could not identified
• Frequently contaminated by MO in the URIFrequently contaminated by MO in the URI

What are the risk factors for pneumonia

Risk factors for pneumonia • Extreme of ageExtreme of age• Underlying co-morbid illnessUnderlying co-morbid illness• ImunocompromiseImunocompromise• Impaired mucociliary clearanceImpaired mucociliary clearance• AlcoholismAlcoholism; Drug abusers; Drug abusers• Smoking• Endotracheal intubationEndotracheal intubation• Upper respiratory infectionUpper respiratory infection• Impaired level of consciousnessImpaired level of consciousness• An increase in gastric pH (the use of H2 Blocker, An increase in gastric pH (the use of H2 Blocker,
Antacid)Antacid)• Neurologic dysfunctionNeurologic dysfunction

Can this patient be treated as an outpatient or should he be admitted?

Risk Factors used to determine assignment to risk classes II-V

Risk class for patients with CAP

Does the patient have a history of any of the following comorbid conditions ?
Neoplastic diseaseCongestive heart failureCerebrovascular diseaseRenal diseaseLiver disease
Patients with Community Acquired pneumonia
Is the patients over 50 years of age ?
Does the patient have any of the following on physician examination ?
Altered mental statisPulse 125/minuteRespiratory rate 30/minuteSistolic blood presure < 90 mmHgTemperature < 35C or 40 C
Assign patient to risk class I
Assign patient to risk class II-V based on prediction model scoring system
Yes
Yes
Yes
No
No
No
Algorithm pneumonia

What antibiotic agent would be recommended for this patient?

The ideal antibiotic in pneumoniaThe ideal antibiotic in pneumonia
• Bactericidal +++Bactericidal +++• Low resistanceLow resistance• Coverage, almost all of respiratory pathogenCoverage, almost all of respiratory pathogen• Single drug Single drug • Once-daily doseOnce-daily dose• Safe Safe • High respiratory penetrationHigh respiratory penetration• Cost effectiveCost effective

Antibiotics in pneumoniaAntibiotics in pneumonia
• MacrolideMacrolide• TetracyclineTetracycline• CotrimoxazoleCotrimoxazole• Co-AmoxyclavCo-Amoxyclav• Sultamicillin Sultamicillin - lactam (include cephalosporin)- lactam (include cephalosporin)• FluoroquinoloneFluoroquinolone• AminoglycosideAminoglycoside• AntipseudomonasAntipseudomonas

CAP Management IssuesCAP Management Issues
• Causative pathogen frequently not foundCausative pathogen frequently not found• Typical and atypical found together Typical and atypical found together • Therapy must be started early (<8 hours)Therapy must be started early (<8 hours)• Increasing resistant to penicillin and macrolide Increasing resistant to penicillin and macrolide • Atypical: unresponsive against Atypical: unresponsive against - lactam AB- lactam AB• Cost and adverse reaction Cost and adverse reaction • Oral route more convenient Oral route more convenient • Decision to hospitalize/outpatientDecision to hospitalize/outpatient
Bartlett: Clin Infect Dis 26:811, 1998.Bartlett: Clin Infect Dis 26:811, 1998.Whitney et al.New England Journal of Medicine,December 2000Whitney et al.New England Journal of Medicine,December 2000

Outpatient treatment (Outpatient treatment (IDSA/ATS 2007)IDSA/ATS 2007)
• Previously healthy and no use of antimicrobials within the previous 3 Previously healthy and no use of antimicrobials within the previous 3 monthsmonths A macrolide A macrolide
DoxycylineDoxycyline • Have a comorbid (chronic heart, lung, liver /renal disease; DM; Have a comorbid (chronic heart, lung, liver /renal disease; DM;
alcoholism; malignancies; asplenia; immunosuppressing conditions ; alcoholism; malignancies; asplenia; immunosuppressing conditions ; use of immunosuppressing drugs; use of antimicrobials within the use of immunosuppressing drugs; use of antimicrobials within the previous 3 monthsprevious 3 months A respiratory fluoroquinolone (moxifloxacin, gemifloxacin, levofloxacin) A respiratory fluoroquinolone (moxifloxacin, gemifloxacin, levofloxacin)
A b-lactam A b-lactam plus plus a macrolide (strong recommendation; level I evidence)a macrolide (strong recommendation; level I evidence)• In regions with a high rate of infection with high-level (MIC _16 In regions with a high rate of infection with high-level (MIC _16
mg/mL) macrolide-resistant mg/mL) macrolide-resistant S. pneumoniae, S. pneumoniae, consider use of consider use of alternative agents listed above in (2) for patients without alternative agents listed above in (2) for patients without comorbiditiescomorbidities

Inpatients, non-ICU treatment
• A respiratory fluoroquinolone (strong A respiratory fluoroquinolone (strong recommendation; level I evidence)recommendation; level I evidence)
• A b-lactam A b-lactam plus plus a macrolide (strong a macrolide (strong recommendation; level I evidence)recommendation; level I evidence)

Inpatients, ICU treatment
A b-lactam (cefotaxime, ceftriaxone, or ampicillin-sulbactam) plus
either azithromycin (level II evidence) or a respiratory fluoroquinolone (level I evidence) (strong recommendation)
(for penicillin-allergic patients, a respiratory fluoroquinolone and aztreonam are recommended)
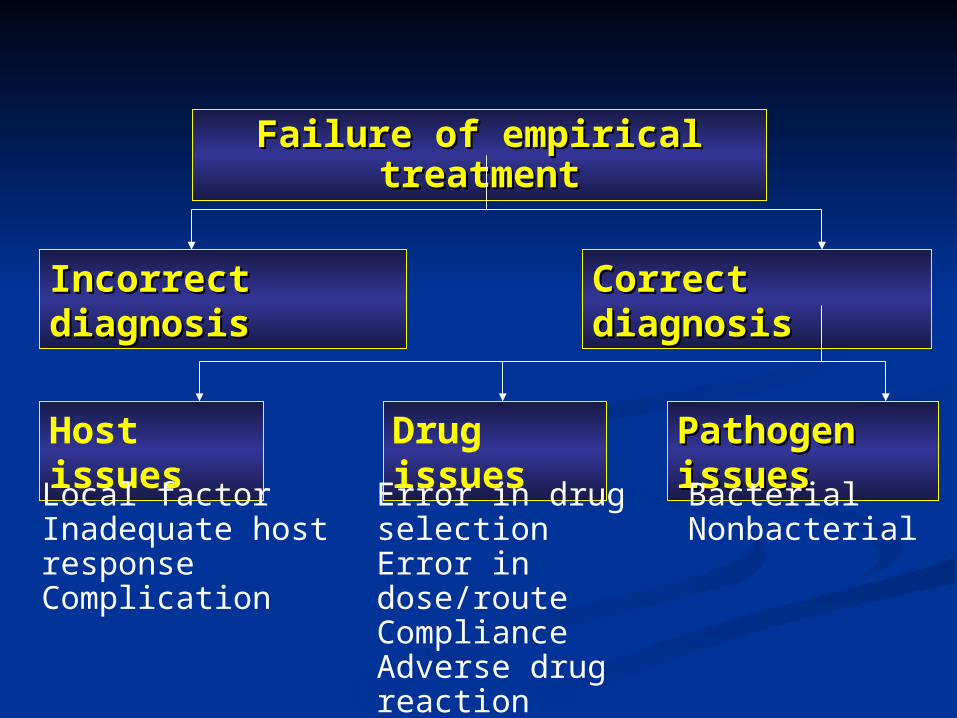
Incorrect diagnosisIncorrect diagnosis
Host issues Pathogen issuesPathogen issues
Failure of empirical treatmentFailure of empirical treatment
Correct diagnosisCorrect diagnosis
Drug issues
BacterialNonbacterial
Error in drug selectionError in dose/routeComplianceAdverse drug reaction
Local factorInadequate host responseComplication

Prognostic factorsPrognostic factors
• Extremes of ageExtremes of age
• Inappropriate antibiotic therapyInappropriate antibiotic therapy
• ShockShock
• Involvement of Involvement of 1 lobe 1 lobe
• Peripheral WBC count Peripheral WBC count 5000/ 5000/ll• Presence of associated disorders (eg: Presence of associated disorders (eg:
cirhosis; heart/renal failure)cirhosis; heart/renal failure)• Development of extrapulmonaryDevelopment of extrapulmonary
complications (eg: meningitis, endocarditis)complications (eg: meningitis, endocarditis)

Mortality in patients with CAPMortality in patients with CAP
Study FocusStudy Focus Patients Mortality (%)Patients Mortality (%)
Hospitalized and ambulatoryHospitalized and ambulatoryHospitalized onlyHospitalized onlyElderlyElderlyBacteriemicBacteriemicNursing homeNursing homeIntensive Care UnitIntensive Care Unit
5.15.113.613.617.617.619.619.630.830.836.536.5
Fine et al. JAMA 1995;274: 134-141

Complications
• Acute respiratory distress syndromeAcute respiratory distress syndrome• Lung abscessLung abscess• Renal failure Renal failure • Septic shockSeptic shock• Pleural effusions/EmpyemaPleural effusions/Empyema• Bacteriemia (Septic arthritis; Endocarditis; Bacteriemia (Septic arthritis; Endocarditis;
Meningitis; Peritonitis; Endopthalmitis.Meningitis; Peritonitis; Endopthalmitis.