Embed Size (px)
Citation preview
The ENRIECO Project: ENVIRONMENTAL HEALTH
RISKS IN EUROPEAN BIRTH COHORTS
Work Package 6
Report for Workshop for user groups (Deliverable 11)
- 26 July 2010 -
Department of Social Medicine, University of Crete, Heraklion, Crete, Greece
A project conducted within the European Union's 7th Framework Programme -
Theme 6, Environment FP7-226285
2
Project title: ENVIRONMENTAL HEALTH RISKS IN EUROPEAN BIRTH
COHORTS
Project acronym: ENRIECO
Grant agreement no: 226285
Grant agreement for: Coordination and support action (Coordinating)
Project Coordinator: M. J. Nieuwenhuijsen, PhD
EC Project Officer: Tuomo Karjalainen
The 2nd ENRIECO workshop meeting was held on 26-
28 May 2010 in Utrecht, The Netherlands.
The workshop was focused on the evaluations and
recommendations of the working groups within each Work
Package (WP), and the presentation and evaluation of the
outcomes of the case studies. The working groups (WG)
presented their findings and further work was planned.
3
Table of Contents
1 Relevant Meeting Programme Book Excerpts 4
1.1 Pre‐Workshop meeting on occupational exposures ‐ Programme 6
1.2 2nd ENRIECO meeting Programme (26‐28 May 2010) 7
1.3 2nd ENRIECO meeting Attendees 10
1.4 ENRIECO Working Packages 14
1.5 ENRIECO working groups 16
1.6 Countries of Participating Cohorts 17
1.7 ENRIECO Exposure and Health Summary 18
1.8 ENRIECO Exposures Assessed, by Birth Cohort 21
1.9 ENRIECO Outcomes Assessed, by Birth Cohort 22
2 Meeting Minutes 23
2.1 Pre‐Workshop meeting on occupational exposures 24
2.2 Plenary Sessions’ Minutes 26
2.2 Parallel Sessions’ Minutes 45
3 Annex 59 3.1 Plenary Session Oral Presentations 60
3.2 Deliverables and Milestone Activities until completion of ENRIECO 126 3.3 Scientific publications anticipated 128

4
Relevant Meeting “Programme Book” Excerpts
5
ENvironmental Health RIsks in European Birth COhorts
(ENRIECO)
2nd ENRIECO Meeting
Utrecht, 26-28 May 2010
A project conducted within the European Union's 7th Framework Programme -
Theme 6, Environment FP7-226285

6
Pre-Workshop meeting on occupational exposures ENRIECO Project
25 May 2010 Utrecht
Mitland Hotel, Ariënslaan 1, 3573 PT Utrecht
Agenda
13.15-13.30 Welcome
13.30-14.15 State of knowledge regarding associations between parental occupational exposures and pregnancy outcomes – Open questions for birth cohort research M Vrijheid
14.15-14.45 Objectives of the case study, S. Cordier
Inventory of occupational data in ENRIECO cohorts, S Cordier
14.45-15.15 Application and validity of JEMs in birth cohort studies: methodological challenges A Burdorf
15.15- 15.30 Existing coding systems for occupations in Europe Existing JEMS S. Cordier
15.30-16.00 Break
16.00 Discussion
- Set priority occupations (mother, father) - Set priority occupational exposures (mother, father) - Strategy for pooling occupations (coding, job titles) - Strategy for pooling occupational exposures (questionnaires, JEMS) - Agenda
18.00 End of the meeting
19.30 Dinner reservation Restaurant Rechtbank
Participants ENRIECO participants Invited Experts
S. Cordier (PELAGIE) J. Fevotte (INVS, Lyon) L. Burdorf, F. Pierik, C. Snijder (Generation R) H. Kromhout (Utrecht University) M. Eggesboe (HUMIS, MOBA) M. Van Tongeren (IOM, Edinburgh) V. Patelarou, M. Kogevinas (RHEA) N. Roeleveld (Radboud University, T.G.M. Vrijkotte (ABCD) Nijmegen Medical Center) M. Vrijheid (INMA) M. Nieuwenhuijsen (BiB)
7
2nd ENRIECO meeting
Utrecht, 26-28 May 2010
Programme
Day 1, 26 May Parallel sessions: WPs and Case studies (current work)
Aim: the various WPs and case studies spend discussing
various issues amongst themselves in preparation for the
plenary sessions
9:00-10:30 WP2, WP3 and WP4
10:30-11:00 Coffee
11:00-13:00 Case studies of Occupation, POPs and WP5 (3)
13:00-14:00 Lunch
Plenary session: Welcome and overview
Aim: to provide welcome and overview
14:00-14:30 Mark Nieuwenhuijsen, Diana Van Gent and Manolis Kogevinas
(WP6)
Plenary session: Current status of WPs
14:30-15:30 WP1 (Inventory Database)
Martine Vrijheid and Maribel Casas
Aim: to show the approach taken and basic data in the
inventory
15:30-16:00 Coffee
16:00-18:00 WP2
General overview: Ulrike Gehring / Bert Brunekreef
Current status of WGs (2-3 WG leaders)
Recommendations
19:30 ENRIECO meeting dinner, Restaurant Selamat Makan
8
Day 2, 27 May Plenary session: Current status of Case studies
Aim: to present the progress in the case studies
9:00-11:00 Case studies of Occupation, POPs and WP5 (3)
Sylvaine Cordier, Jens Peter Bonde and Thomas Keil
11:00-11:30 Coffee
Plenary sessions: Recommendations of WPs
Aim: to briefly present the working group reports, including the
main approaches and methods within the cohorts, and present
and discuss the recommendations in more detail
11:30-13:30 WP3
General overview: Remy Slama
Current status of WGs (2-3 WG leaders)
Recommendations
13:30-14:30 Lunch
14:30-16:30 WP4
General overview: Joachim Heinrich / Chih-Mei Chen
Recommendations
16:30-17:00 Meeting of the steering committee
19:30 Dinner, Restaurant de Artisjok
Day 3, 28 May Parallel sessions: WPs (future work)
Aim: to discuss within the WPs further work that needs to be
done
9:00-10:30 WP2, WP3 and WP4
10:30-11:00 Coffee
11:00-12.30 Case Studies (future work)
Aim: to discuss within the case studies further work that needs
to be done
Case studies of Occupation, POPs and WP5 (3)
9
Plenary session: Wrap-up and General Assembly
12.30-13:00 Aim: to discuss general related to the project and wrap up
Mark Nieuwenhuijsen
13:00-14:00 Lunch
14:00 End meeting
10
2nd ENRIECO meeting
Utrecht, 26-28 May 2010
Attendees
ENRIECO PARTNERS CREAL, Barcelona, Spain NIEUWENHUIJSEN, MARK (Coordinator) VAN GENT, DIANA (Project Manager) VRIJHEID, MARTINE CASAS, MARIBEL SUNYER, JORDI INSERM, Grenoble/Rennes, France SLAMA, REMY CORDIER, SYLVAINE CHEVRIER, CÉCILE Utrecht University, Utrecht, The Netherlands GEHRING, ULRIKE BRUNEKREEF, BERT DE HARTOG, JEROEN HMGU, Neuherberg, Germany CHEN, CHIH-MEI HEINRICH, JOACHIM University of Crete, Crete, Greece KOGEVINAS, MANOLIS VASSILAKI, MARIA Karolinska Institute, Stockholm, Sweden MAGNUS WICKMAN (absent) Charite, Berlin, Germany KEIL, TOMAS HOHMANN, CYNTHIA Aarhus University Hospital, Aarhus, Denmark BONDE, JENS PETER
Attendees
11
BIRTH COHORTS - participating in the meeting ABCD Study, Amsterdam VRIJKOTTE, TANJA Academic Medical Center, Department of Public Health, Amsterdam, The Netherlands ArcRisk RAUTO, ARJA Center for Arctic Medicine, Thule institute, University of Oulu ArcRisk, Finland Born in Bradford ODDIE, SAM Bradford, United Kingdom Children’s Health and Environment in the Faroes, Cohorts 1, 2, 3 & 5 WEIHE, PÁL The Faroese Hospital System, The Faroe Islands CO.N.ER LUCIANO, LORENZA Alma Mater Studiorum University of Bologna, Italy Danish National Birth Cohort (DNBC) NYBO ANDERSEN, ANNE-MARIE Institute of Public Health, University of Southern Denmark, Denmark DARC-cohort ELLER, ESBEN Odense University Hospital, Denmark Duisburg cohort KASPER-SONNENBERG, MONIKA WILHELM, MICHAEL Rurh-University Bochum, Germany EDEN mother-child cohort CHARLES, MARIE ALINE INSERM, France ELFE VANDENTORREN, STÉPHANIE Institut de veille sanitaire, France FLEHS DEN HOND, ELLY GOVARTS, EVA VITO, Belgium GENERATION R PIERIK, FRANK VAN DEN HOOVEN, EDITH TNO, ErasmusMC, The Netherlands
Attendees
12
BURDORF, ALEX SNIJDER, CLAUDIA Erasmus MC, The Netherlands GENERATION XXI SANTOS, ANNA Department of Hygiene and Epidemiology, University of Porto Medical School, Portugal GESP II, Rome FORASTIERE, FRANCESCO Department of epidemiology azienda sanitaria sanitaria locale Roma E, Italy GINIplus KRÄMER, URSULA Institut für Umweltmedizinische Forschung, University Duesseldorf, Germany HUMIS EGGESBO, MERETE Norwegian Institute of Public Health, Norway INMA Valencia BALLESTER, FERRAN CSISP, Spain INMA Sabadell BOTTON, JEREMIE CASAS, MARIBEL FORNS, JOAN GASCON, MIREIA GUXENS, MÒNICA MORALES, EVA SUNYER, JORDI Centre for Research in Environmental Epidemiology, Barcelona, Spain INMA, Menorca TORRENT, MATIES Illes Balears Salut, Menorca, Spain INUENDO BONDE, JENS PETER Aarhus University Hospital, Aarhus, Denmark KANC, Kaunas BALCIUS, GEDIMINAS GRAZULEVICIENE, REGINA Vytautas Magnus University, Lithuania KOALA Birth Cohort Study MOMMERS, MONIQUE THIJS, CAREL Maastricht University, The Netherlands LISA TISCHER, CHRISTINA HMGU München, Institute of Epidemiology, Neuherberg, Germany
Attendees
13
MAAS HANNAM, KIM University of Manchester, United Kingdom MAS KEIL, THOMAS HOHMANN, CYNTHIA Charite, Berlin, Germany PELAGIE CORDIER, SYLVAINE CHEVRIER, CÉCILE PETIT, CLAIRE INSERM, France PIAMA, Nationwide GEHRING, ULRIKE Utrecht University, Utrecht, The Netherlands SMIT, JET University Medical Centre Utrecht, The Netherlands REPRO_PL (Polish Mother and Child Cohort) HANKE, WOJCIECH POLANSKA, KINGA Nofer Institute of Occupational Medicine, Poland RHEA, Heraklion KOGEVINAS, MANOLIS VARDAVAS, CONSTANTINE VASSILAKI, MARIA University of Crete, Greece SNiP THYRIAN, JOCHEN RENÉ Institute for Community Medicine, University of Greifswald, Germany The Aarhus Birth Cohort Biobank HAMMER BECH, BODIL School of Public Health Aarhus University, Denmark Delegates collaborating in WP work RANFT, ULRICH Institut für Umweltmedizinische Forschung, University Duesseldorf, Germany
ENRIECO Work Packages
14
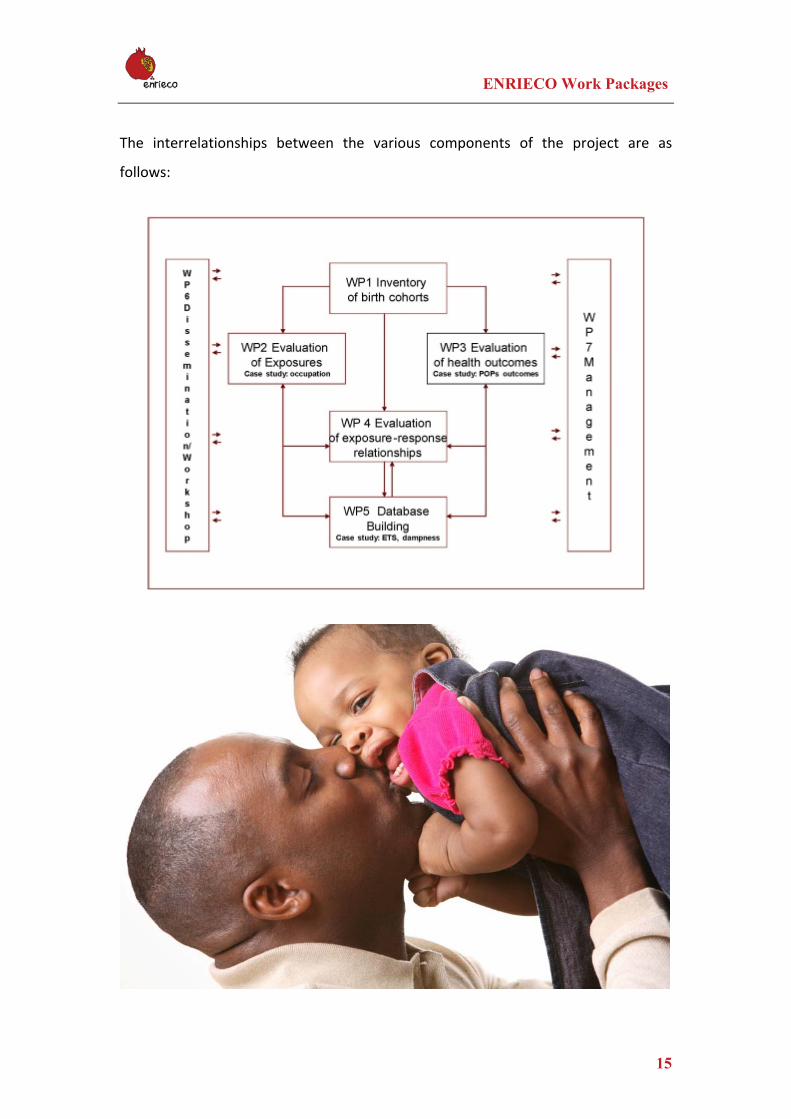
WP 1 ‐ Inventory of birth cohorts (WP leader: Martine Vrijheid, CREAL)
To make inventories of existing cohorts (health data, exposure data, biological
samples, exposure response functions, expertise), including a searchable database.
WP 2 ‐ Evaluation of exposures (WP leader: Ulrike Gehring, UU)
To evaluate existing environmental exposure information, methods and tools,
including assurance of quality and interoperability, and data access, analysis and
validation, and make recommendations.
WP 3 ‐ Evaluation of health outcomes (WP leader: Remy Slama, INSERM)
To evaluate existing health information, methods and tools, including assurance of
quality and interoperability, data access and validation, and make recommendations.
WP 4 ‐ Evaluation of exposure‐response relationships (WP leader: Joachim
Heinrich, HMGU)
Evaluation of the existing environmental exposure response data, methods and
tools, including assurance of quality and interoperability, and data access and
validation, and make recommendations.
WP 5 ‐ Database building (WP leader: Thomas Keil, Charité)
To build databases, and conduct assurance of quality and interoperability, data
access, analysis and validation.
WP 6 ‐ Dissemination (WP leader: Manolis Kogevinas, UoC)
To organise the workshops and dissemination through a project website, virtual
network, workshop(s) and easy accessible info (policy makers etc).
WP 7 ‐ Management (WP leader: Mark Nieuwenhuijsen, CREAL)
To manage the overall project.
ENRIECO Work Packages
15
The interrelationships between the various components of the project are as
follows:
Working Groups
16
In order to assess topics within Work Packages (WP) 2, 3, 4 and 5, the following working groups and Case Studies were formed per WP. WP2 ‐ Exposures
• Outdoor air pollution • Water contamination • Allergens and biological organisms • Heavy metals • Pesticides • Emerging exposures (Bisphenol A, Phthalates, Polyfluorinated Compounds and
Brominated Flame Retardants) • Radiations (non‐ionising, UV, ionizing) • Smoking and Second Hand Tobacco Smoke Exposure • Noise • Persistent organic pollutants • Occupation • Case study on Occupational Exposures during pregnancy
WP 3 ‐ Evaluation of health outcomes
• Reproductive outcomes • Allergy, asthma and respiratory health • Neurobehavioral/cognitive function • Childhood cancer • Child growth, metabolic and endocrine disorders • Case study on Persistent organic pollutants (POPs)
WP4 ‐ Evaluation of exposure‐response relationships
• Air pollution and Birth Outcomes • Air Pollution and Allergy and Asthma • Allergens/Biological Organism and Allergy and Asthma • Pesticides and Birth Outcomes • Second Hand Smoking and Birth Outcomes • Water contaminants and Birth Outcomes • Metals and Birth Outcomes • Metals and Neurobehavioural/Cognitive • POPs and Birth Outcomes • POPs and Neurobehavioural/Cognitive Function • Noise, Birth Outcomes, Asthma/Allergy, and Cardiovascular Outcomes • Occupation and Birth Outcomes
WP5 ‐ Database building
• Case Study of Working Group 1 – Dampness • Case Study of Working Group 2 – Tobacco Smoke Exposure and Asthma
• Case Study of Working Group 3 – Tobacco Smoke Exposure and Wheeze

Countries of Participating Cohorts
17
Countries of Participating Cohorts
ENRIECO Exposure and Health Summary
18
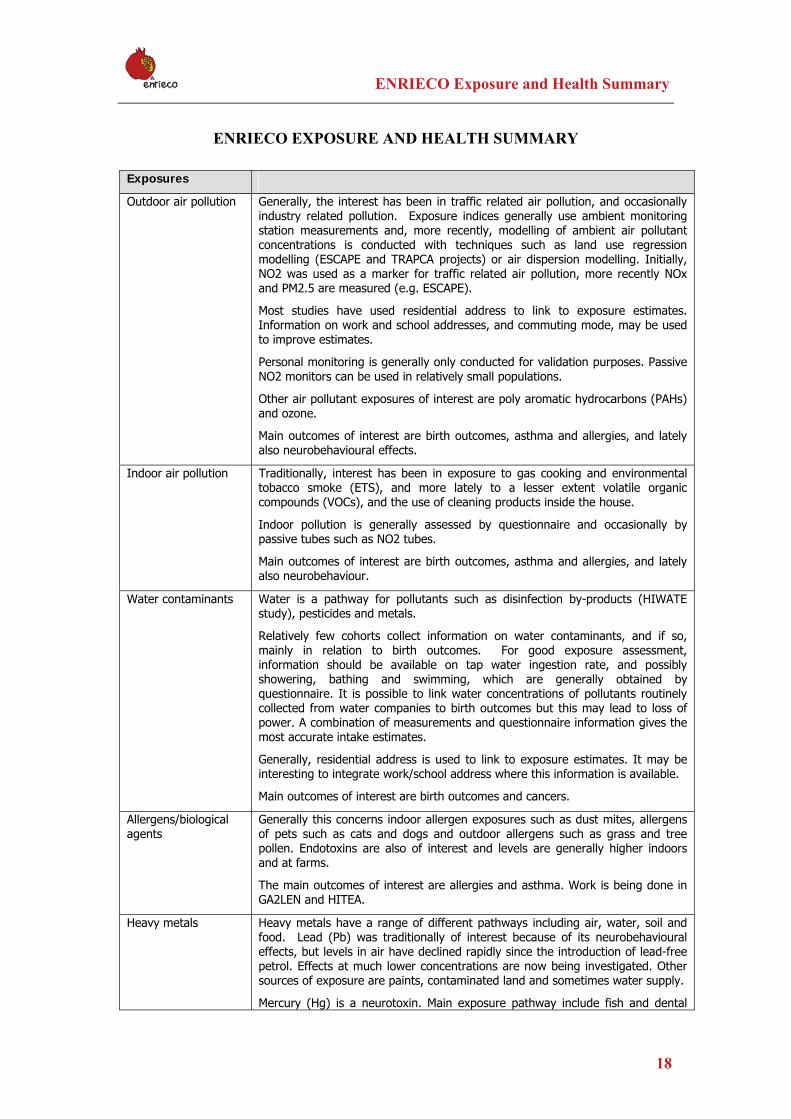
ENRIECO EXPOSURE AND HEALTH SUMMARY
Exposures
Outdoor air pollution Generally, the interest has been in traffic related air pollution, and occasionally industry related pollution. Exposure indices generally use ambient monitoring station measurements and, more recently, modelling of ambient air pollutant concentrations is conducted with techniques such as land use regression modelling (ESCAPE and TRAPCA projects) or air dispersion modelling. Initially, NO2 was used as a marker for traffic related air pollution, more recently NOx and PM2.5 are measured (e.g. ESCAPE).
Most studies have used residential address to link to exposure estimates. Information on work and school addresses, and commuting mode, may be used to improve estimates.
Personal monitoring is generally only conducted for validation purposes. Passive NO2 monitors can be used in relatively small populations.
Other air pollutant exposures of interest are poly aromatic hydrocarbons (PAHs) and ozone.
Main outcomes of interest are birth outcomes, asthma and allergies, and lately also neurobehavioural effects.
Indoor air pollution Traditionally, interest has been in exposure to gas cooking and environmental tobacco smoke (ETS), and more lately to a lesser extent volatile organic compounds (VOCs), and the use of cleaning products inside the house.
Indoor pollution is generally assessed by questionnaire and occasionally by passive tubes such as NO2 tubes.
Main outcomes of interest are birth outcomes, asthma and allergies, and lately also neurobehaviour.
Water contaminants Water is a pathway for pollutants such as disinfection by-products (HIWATE study), pesticides and metals.
Relatively few cohorts collect information on water contaminants, and if so, mainly in relation to birth outcomes. For good exposure assessment, information should be available on tap water ingestion rate, and possibly showering, bathing and swimming, which are generally obtained by questionnaire. It is possible to link water concentrations of pollutants routinely collected from water companies to birth outcomes but this may lead to loss of power. A combination of measurements and questionnaire information gives the most accurate intake estimates.
Generally, residential address is used to link to exposure estimates. It may be interesting to integrate work/school address where this information is available.
Main outcomes of interest are birth outcomes and cancers.
Allergens/biological agents
Generally this concerns indoor allergen exposures such as dust mites, allergens of pets such as cats and dogs and outdoor allergens such as grass and tree pollen. Endotoxins are also of interest and levels are generally higher indoors and at farms.
The main outcomes of interest are allergies and asthma. Work is being done in GA2LEN and HITEA.
Heavy metals Heavy metals have a range of different pathways including air, water, soil and food. Lead (Pb) was traditionally of interest because of its neurobehavioural effects, but levels in air have declined rapidly since the introduction of lead-free petrol. Effects at much lower concentrations are now being investigated. Other sources of exposure are paints, contaminated land and sometimes water supply.
Mercury (Hg) is a neurotoxin. Main exposure pathway include fish and dental
ENRIECO Exposure and Health Summary
19
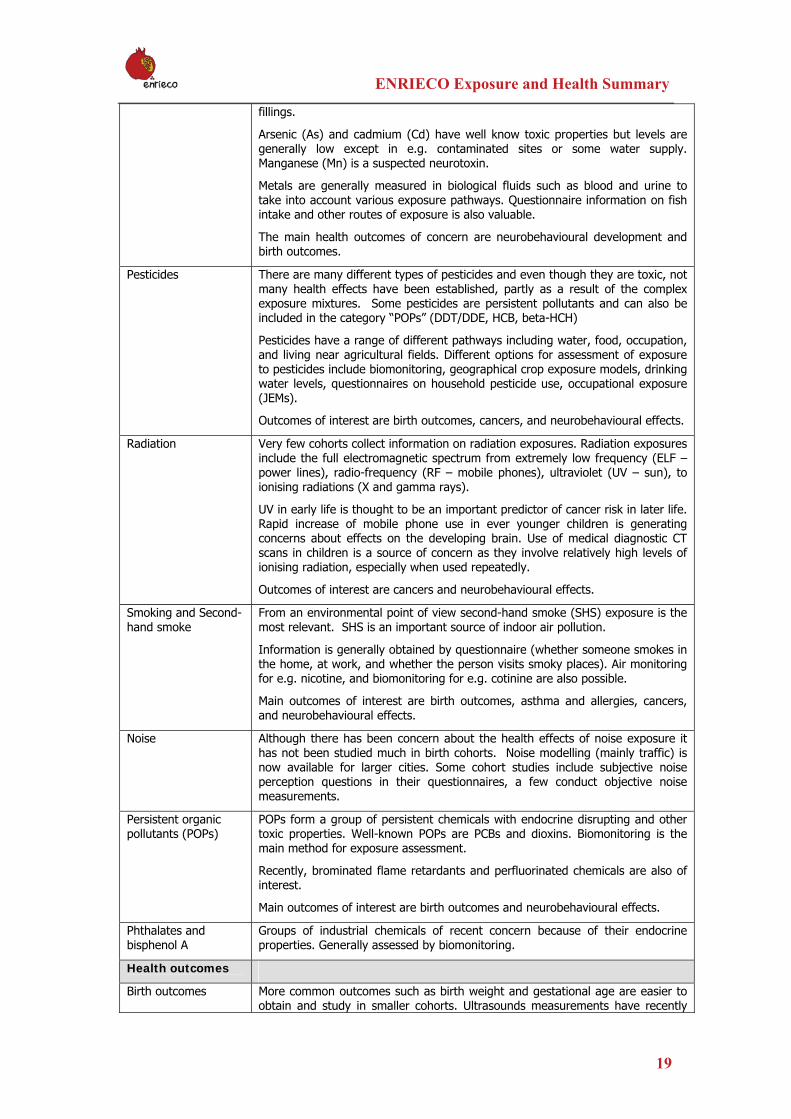
fillings.
Arsenic (As) and cadmium (Cd) have well know toxic properties but levels are generally low except in e.g. contaminated sites or some water supply. Manganese (Mn) is a suspected neurotoxin.
Metals are generally measured in biological fluids such as blood and urine to take into account various exposure pathways. Questionnaire information on fish intake and other routes of exposure is also valuable.
The main health outcomes of concern are neurobehavioural development and birth outcomes.
Pesticides There are many different types of pesticides and even though they are toxic, not many health effects have been established, partly as a result of the complex exposure mixtures. Some pesticides are persistent pollutants and can also be included in the category “POPs” (DDT/DDE, HCB, beta-HCH)
Pesticides have a range of different pathways including water, food, occupation, and living near agricultural fields. Different options for assessment of exposure to pesticides include biomonitoring, geographical crop exposure models, drinking water levels, questionnaires on household pesticide use, occupational exposure (JEMs).
Outcomes of interest are birth outcomes, cancers, and neurobehavioural effects.
Radiation Very few cohorts collect information on radiation exposures. Radiation exposures include the full electromagnetic spectrum from extremely low frequency (ELF – power lines), radio-frequency (RF – mobile phones), ultraviolet (UV – sun), to ionising radiations (X and gamma rays).
UV in early life is thought to be an important predictor of cancer risk in later life. Rapid increase of mobile phone use in ever younger children is generating concerns about effects on the developing brain. Use of medical diagnostic CT scans in children is a source of concern as they involve relatively high levels of ionising radiation, especially when used repeatedly.
Outcomes of interest are cancers and neurobehavioural effects.
Smoking and Second-hand smoke
From an environmental point of view second-hand smoke (SHS) exposure is the most relevant. SHS is an important source of indoor air pollution.
Information is generally obtained by questionnaire (whether someone smokes in the home, at work, and whether the person visits smoky places). Air monitoring for e.g. nicotine, and biomonitoring for e.g. cotinine are also possible.
Main outcomes of interest are birth outcomes, asthma and allergies, cancers, and neurobehavioural effects.
Noise Although there has been concern about the health effects of noise exposure it has not been studied much in birth cohorts. Noise modelling (mainly traffic) is now available for larger cities. Some cohort studies include subjective noise perception questions in their questionnaires, a few conduct objective noise measurements.
Persistent organic pollutants (POPs)
POPs form a group of persistent chemicals with endocrine disrupting and other toxic properties. Well-known POPs are PCBs and dioxins. Biomonitoring is the main method for exposure assessment.
Recently, brominated flame retardants and perfluorinated chemicals are also of interest.
Main outcomes of interest are birth outcomes and neurobehavioural effects.
Phthalates and bisphenol A
Groups of industrial chemicals of recent concern because of their endocrine properties. Generally assessed by biomonitoring.
Health outcomes
Birth outcomes More common outcomes such as birth weight and gestational age are easier to obtain and study in smaller cohorts. Ultrasounds measurements have recently
ENRIECO Exposure and Health Summary
20
been used as an outcome measure of fetal growth in relation to e.g. air pollution and may become more commonly available.
Rare outcomes such as congenital anomalies and still birth require very large cohorts.
Spontaneous abortion/miscarriage are generally hard to assess and needs specialised ascertainment.
Anogenital distance is of interest in relation to endocrine disrupting substances and some cohorts have started measuring this.
Asthma/allergies/ infections/atopy
Information on asthma, allergy, eczema and infection symptoms is generally obtained by questionnaire (e.g. persistent wheezing questions) or from doctor’s diagnosis. Lung function testing is generally possible from age 5 and allergen testing from age 2.
Atopy is generally assessed by skin prick testing or by specific IgE measurements and definitions may vary but generally include a positive response to either grass, cat or dust mites. Occasional assessed by questionnaire.
Projects focusing on asthma and allergies in birth cohorts are GA2LEN, TRAPCA and HITEA
Neurobehavioural effects
Assessment of neurobehavioural development can be made at many different ages, from birth into adolescence. Many different tests are available. Neurodevelopment tests in young children include the Bayley Scales of Infant Development (0-3 years), McCarthy (4-6 years). In older children a range of intelligence and performance tests is available (include, for example the Wechsler Preschool and Primary Scale of Intelligence WPPSI). Behavioural problems (incl ADHD) and autism symptoms are generally assessed by questionnaire to the parents and teachers.
Childhood cancer Very large cohorts are needed to study childhood cancer outcomes. The International Childhood Cancer Cohort Consortium (I4C) brings together birth cohort studies with the aim to conduct pooled analyses of childhood cancer.
Growth/obesity There is some recent interest in the role of environmental exposures and some studies suggest associations (smoking, POPs).
21
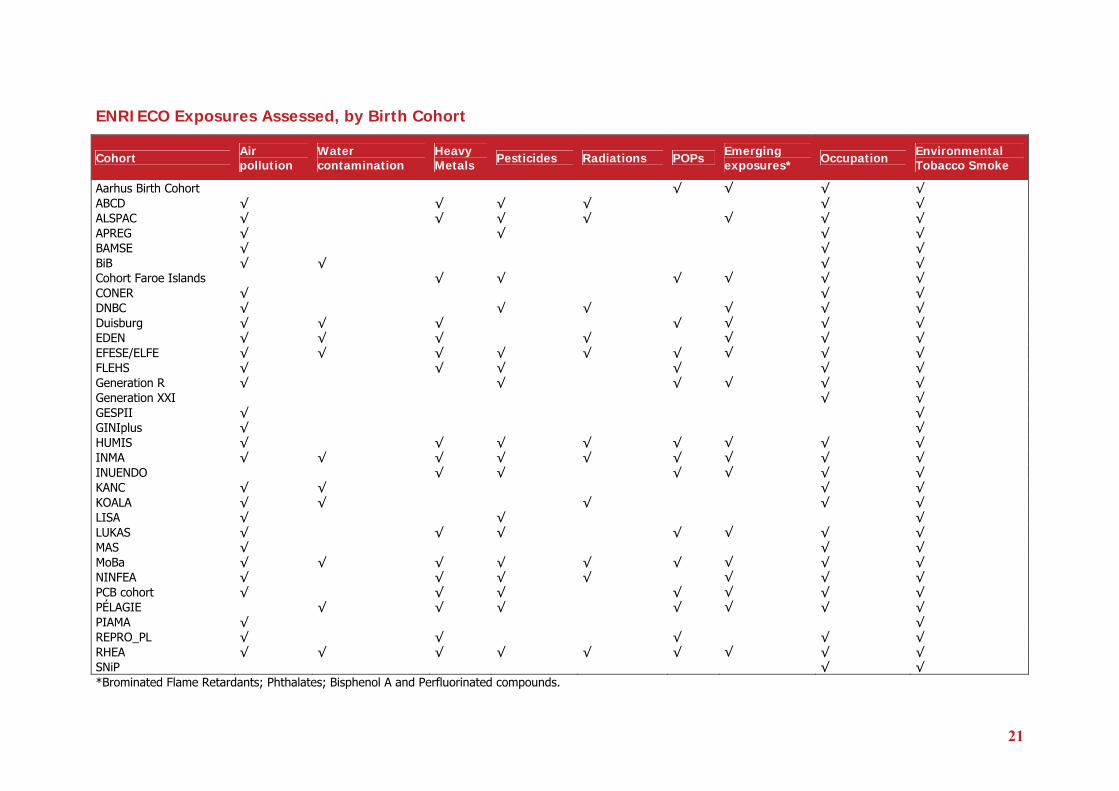
ENRIECO Exposures Assessed, by Birth Cohort
Cohort Air pollution
Water contamination
Heavy Metals Pesticides Radiations POPs Emerging
exposures* Occupation Environmental Tobacco Smoke
Aarhus Birth Cohort √ √ √ √ ABCD √ √ √ √ √ √ ALSPAC √ √ √ √ √ √ √ APREG √ √ √ √ BAMSE √ √ √ BiB √ √ √ √ Cohort Faroe Islands √ √ √ √ √ √ CONER √ √ √ DNBC √ √ √ √ √ √ Duisburg √ √ √ √ √ √ √ EDEN √ √ √ √ √ √ √ EFESE/ELFE √ √ √ √ √ √ √ √ √ FLEHS √ √ √ √ √ √ Generation R √ √ √ √ √ √ Generation XXI √ √ GESPII √ √ GINIplus √ √ HUMIS √ √ √ √ √ √ √ √ INMA √ √ √ √ √ √ √ √ √ INUENDO √ √ √ √ √ √ KANC √ √ √ √ KOALA √ √ √ √ √ LISA √ √ √ LUKAS √ √ √ √ √ √ √ MAS √ √ √ MoBa √ √ √ √ √ √ √ √ √ NINFEA √ √ √ √ √ √ √ PCB cohort √ √ √ √ √ √ √ PÉLAGIE √ √ √ √ √ √ √ PIAMA √ √ REPRO_PL √ √ √ √ √ RHEA √ √ √ √ √ √ √ √ √ SNiP √ √ *Brominated Flame Retardants; Phthalates; Bisphenol A and Perfluorinated compounds.
“ENRIECO Workshop for user groups” (D11) 22
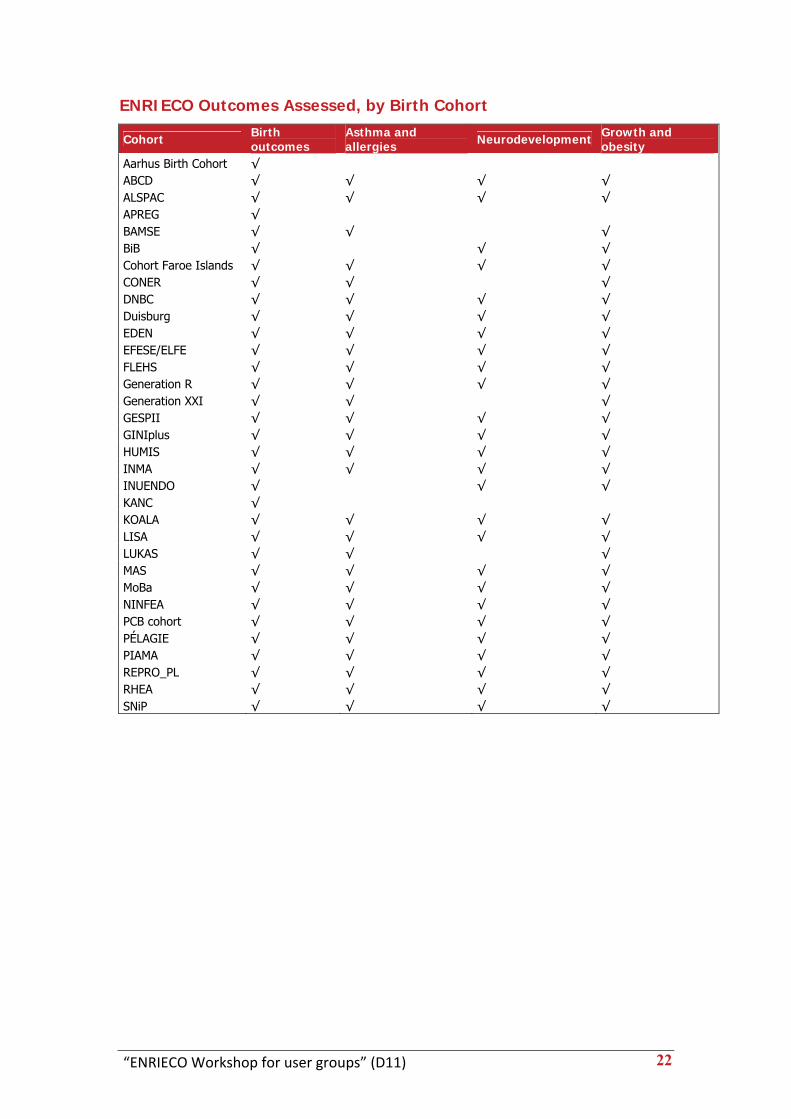
ENRIECO Outcomes Assessed, by Birth Cohort
Cohort Birth outcomes
Asthma and allergies Neurodevelopment Growth and
obesity Aarhus Birth Cohort √ ABCD √ √ √ √ ALSPAC √ √ √ √ APREG √ BAMSE √ √ √ BiB √ √ √ Cohort Faroe Islands √ √ √ √ CONER √ √ √ DNBC √ √ √ √ Duisburg √ √ √ √ EDEN √ √ √ √ EFESE/ELFE √ √ √ √ FLEHS √ √ √ √ Generation R √ √ √ √ Generation XXI √ √ √ GESPII √ √ √ √ GINIplus √ √ √ √ HUMIS √ √ √ √ INMA √ √ √ √ INUENDO √ √ √ KANC √ KOALA √ √ √ √ LISA √ √ √ √ LUKAS √ √ √ MAS √ √ √ √ MoBa √ √ √ √ NINFEA √ √ √ √ PCB cohort √ √ √ √ PÉLAGIE √ √ √ √ PIAMA √ √ √ √ REPRO_PL √ √ √ √ RHEA √ √ √ √ SNiP √ √ √ √
“ENRIECO Workshop for user groups” (D11) 23
Workshop Minutes
Abbreviations used MN: Mark Nieuwenhuijsen; MK: Manolis Kogevinas; MV: Martine Vrijheid; DvG: Diana van Gent; RS: Remy Slama; JPB; Jens Peter Bonde; ANA: Anne‐Marie Nybo Andersen; SC: Sylvaine Cordier; RG: Regina Grazuleviciene; CC: Cecile Chevrier; FP: Frank Pierik; MW: Michael Whilhelm; PW: Pál Weihe; EG: Eva Govarts; ME: Merete Eggesbo; JT: Jochen René Thyrian; MAC: Marie‐Aline Charles; FF: Francesco Forastiere; MG: Mireia Gascon; CT: Carel Thijs; MC: Maribel Casas; JF: Joan Forns; CMC: Chih‐Mei Chen; JB:Jeremie Botton; JH:Joachim Heinrich.
“ENRIECO Workshop for user groups” (D11) 24
Pre‐Workshop meeting on occupational exposures ‐ Minutes ENRIECO Project, 25 may 2010, Utrecht Participants: L Burdorf (Generation R), S Cordier (PELAGIE), M Eggesboe (HUMIS, MOBA), J Févotte, H Kromhout, M Nieuwenhuijsen (BiB), N Roeleveld, C Snijder (Generation R), M Van Tongeren, M Vrijheid (INMA), T Vrijkotte (ABCD) Apologies: V Patelarou, M Kogevinas (RHEA) Presentations
1‐ Review of knowledge concerning occupational exposures and birth outcomes (M Vrijheid)
The review conducted in WP4 points at a number of occupations “at risk ”and suspected occupational exposures and stresses the fact that birth cohorts would allow the study of long term consequences of these exposures that have not often been evaluated.
2‐ Validity of occupational exposure assessment (L Burdorf)
L Burdorf introduced the available tools (self report, interview, JEMs…) and discussed their respective properties in terms of sensitivity and specificity according to exposure prevalence. Application of JEMs relies on the quality of reporting of job title. This implies that the job has been correctly described and coded. Recommendations for data collection and coding protocol were discussed. In birth cohort studies a low prevalence of exposure is expected and, thus, a JEM with high sensitivity would be preferred. Application of a JEM is less useful to determine associations between specific agents and birth outcomes, but contributes to our understanding how important (groups of) agents are for population health through assessment of population attributable fractions.
3‐ Inventory of occupational data in ENRIECO cohorts (S Cordier)
A number of ENRIECO cohorts have recorded at least maternal occupations (see draft report). It was agreed that cohorts that can be approached for further investigation on occupational exposures should have already coded (or planned to code) maternal occupation ‐ during pregnancy‐ and/or paternal occupation ‐ before pregnancy. According to these criteria, the list of cohorts eligible is: ABCD, ALSPAC, BiB, DNBC, Generation R, Generation XXI, HUMIS, INMA, INUENDO, KANC, MoBa, PELAGIE and RHEA (NB: All cohorts have agreed to participate except for ALSPAC not contacted yet and INUENDO for which the coding status needs to be checked). Expected numbers for main “at risk” occupations (laboratory workers, health care workers, housekeepers/cleaners, hairdressers, cooks/bartenders, agricultural workers…) show reasonable power in the perspective of a pooled analysis.
“ENRIECO Workshop for user groups” (D11) 25
Discussion Invited experts felt that it would not be appropriate to apply one existing JEM to ENRIECO birth cohorts because these cohorts cover different countries and potentially different work environments. The experience of Dutch scientists in the update of the “Van Tongeren JEM” resulting in the creation of the “Brouwers JEM” shows how information varies according to time period and country. This may be especially true for certain compounds (phthalates for instance) for which occupation is not the main source of exposure. Building one “European” JEM would require a huge amount of work for a questionable result. It should be a country‐specific agent‐specific JEM. Another question was the feasibility of translating all national occupational codes into one common code. This common code should be ISCO‐88 because it has national equivalent in all European countries although it was felt that it may not be perfectly adequate for occupational exposure assessment. Since a JEM will not be applied, a translation is not required. The agreement was to conduct a meta‐analysis of the risk of adverse outcomes in the various cohorts for selected “at risk” occupations (both mothers and fathers) during the period of vulnerability (pregnancy for mother, before pregnancy for father). The list of occupations should include the ones defined above (plus drivers for male occupations). In parallel, surveys of occupational exposures present in these occupations in the different countries should be searched to interpret the risks observed. Adverse outcomes that should be studied in association with occupational exposures are: time to pregnancy, birth parameters (weight, length, head circumference), duration of gestation, perinatal mortality (including stillbirths). Other outcomes such as male genital congenital anomalies or child behavior are also relevant but the feasibility of pooling different cohorts will first have to be assessed (WP3). Recommendations for an adequate data collection on occupational exposures were also discussed. In addition to job title, one should collect description of task, industry, name of company, number of hours per week, existence of biomonitoring data. Free text should be kept in the data base for additional details. A good training of coders should be organized for standardization. Conclusion A protocol for the meta‐analysis will be elaborated and circulated to WG participants and to eligible cohorts. Note: The above minutes include also the discussions that took place in the parallel sessions for the Case study of Occupation
“ENRIECO Workshop for user groups” (D11) 26
Plenary Sessions’ Minutes
Day 1, 26 May
Plenary session: Welcome and overview Aim: to provide welcome and overview
14:00‐14:30 Mark Nieuwenhuijsen, Diana van Gent and Manolis Kogevinas (WP6)
Introduction – Mark Nieuwenhuijsen (MN)
An overview was given on the background of the ENRIECO project and its objectives.
Most important is to make recommendations for the next 5‐10 years with the outcomes of the reviews and case studies. What needs to be done is to write down the recommendations and communicate to the EU, and disseminate the work widely. Recommendations will be discussed during parallel sessions and presentations.
Introduction – Diana van Gent (DvG)
Thanked meeting organizers.
Action: Requested that minutes are taken during parallel sessions and emailed to Maria Vassilaki.
- Periodic Report I has been submitted and reviewed by Tomas Turecki, who was happy with the content. The Finance Officer is currently reviewing the financial claims from the partners. Partners will be informed of any feedback.
- Tuomo ‐ Karjalainen will take over as the EC Officer for ENRIECO.
- Deliverables are now being submitted to the EC via the EU website.
- Quarterly reports will be published to provide regular project updates. - The Coordinator needs to know of any changes in WP/WG composition.
Action: WP leads should inform Maria Vassilaki and Diana van Gent if any changes are made.
WP6 – Dissemination: Manolis Kogevinas (MK)
‐ Everyone will receive an email with instructions for using the ENRIECO intranet.
‐ Mark Nieuwenhuijsen presented ENRIECO at the Fifth Ministerial Conference on Environment and Health, Parma Italy.
“ENRIECO Workshop for user groups” (D11) 27
ENRIECO project results need to go out and have an effect on research policy and public health action. How do we do this? (Additional information in MK’s presentation on this). Very important: how to write the final report?
E.g. Should we list the 10 most important European problems, 10 most important research areas (inform media/ EC officers), most important areas for public health action, NGO, EU parliament MPs to be informed? Promote ENRIECO reports by requesting ISEE space in EHP and Epidemiology?
Discussion
A question was posed about what the EU is planning to do with our reports; do we have a specific responsibility? Our results need to be prepared such a way to be used by EU; also how can we use those? We could involve national Societies, NGOs and pediatricians.
The way we work with cohorts is not exactly the way to get e.g. 10 key recommendations (RS). We will not be confident of 10 most important exposures. Our work is based on protocol and most work is on literature and designed around study design.
MK: if we can get report on priorities, this would be fine.
It was suggested that we will have quite a number of reviews on knowledge in the field, which is probably something to disseminate and build on.
Post‐natal exposures are increased and not enough work done on environmental exposures (ME). For example: is it the more the better for breastfeeding? We do not really know, but are promoting it.
MK: If you know of cohorts not aware of ENRIECO, let them know about the project.
14:30‐15:30 WP1 (Inventory Database) Martine Vrijheid and Maribel Casas Aim: to show the approach taken and basic data in the Inventory
WP1 – Inventory of Birth Cohorts: Martine Vrijheid (MV)
The inventory includes 36 registered birth cohorts but is not yet fully ready. The questionnaire includes a basic protocol description which is an update of the information from www.birthcohorts.net. Overall, the inventory questionnaire is basic but enough to get an overview of the environmental health data collected by cohorts. Looking at the map, we are top‐heavy in the North but weak in the East. If anyone knows more cohorts, please let us know and provide the contact information.
For discussion: What are we going to do with the inventory? Is it useful to have it or not? Risk factors will be expanded, as part of the CHICOS project. After these
“ENRIECO Workshop for user groups” (D11) 28
projects maintenance in the future may be difficult and will require commitment from the cohorts.
MV also presented the CHICOS project, another FP7 coordination project running from 01/01/2010 until 31/12/2012 (www.chicosproject.eu). The CHICOS project focuses more on areas of policy concerns in child health and its main aim is to develop a cohort research strategy for Europe. Some WG overlap with ENRIECO but the scope is wider than environmental exposures and encompasses all child health related determinants and outcomes. CHICOS will be organising further workshops in the coming years in which all cohorts are invited to participate (next meeting 11‐12 April 2011).
Discussion
Overlap ENRIECO‐CHICOS
CHICOS WG leaders should get in touch with ENRIECO WG leaders and work closely. ENRIECO WG leaders could serve as experts in the CHICOS WGs. These aspects have not been worked out yet. MV and MC will liaise between the two projects. Repetition of the same work should be avoided.
Reports/papers will have open ends that CHICOS could continue with a broader scope (ANA).
Update birthcohorts.net
ANA: We should use the data collected for ENRIECO (basic protocol part) to update the www.birthcohorts.net (for registered cohorts). What do cohorts say?
Action: Cohort PIs will be asked by email to give permission for information collected in the ENRIECO questionnaires to update www.birthcohorts.net.CREAL and ANA will coordinate this together once the inventory is completed.
Maintenance of the ENRIECO inventory
JT: Questions the usefulness of maintaining the inventory, how much effort is required? Commitment is dependable on the funding situation. Could be useful for policy makers…
Emailing every two years to remind cohorts to check and update their data should be possible. Cohorts will be responsible for the accuracy of their own data. CREAL can send an email every 2 years and make the changes into the database.
The maintenance question can be referred to the end of the CHICOS project, resources for maintenance are secured; if useful, funding can be requested to keep this ongoing. Updating and maintaining the database is part of continued coordination for which we will need resources. This could be part of future EU project. I4C is looking at cohorts globally; Canada is also producing an inventory of cohorts... So, there is a lot of effort, much larger than this.
Publications from WP1
Are there going to be publications and how many? Are all cohorts co‐authors on these? The opinions are not uniform on this; those writing it should be the authors,
“ENRIECO Workshop for user groups” (D11) 29
possibly with cohorts as co‐authors or as part of the “consortium” or “ENRIECO Study Group”. ; data must be checked and written up together.
JT suggested it would be perfectly fine not to be included as a co‐author since cohorts have not given individual data.
Q: What kind of data information will be included in the paper? The WP1 paper will be descriptive only. It should further be noted that all WGs using information collected by WP1 should involve MV and MC in publications resulting from this big effort compiling the inventory.
Type and topic of publications have been discussed during further presentations and at the Steering Group Meeting. Publication guidelines are being finalized by MK.
16:00‐18:00 WP2 General overview: Ulrike Gehring / Bert Brunekreef Current status of WGs (2‐3 WG leaders) Recommendations
WP2 – Evaluation of Exposure: Ulrike Gehring (UG)
There will be a common format of reports by all WP2 WGs (20 pages max).
All cohorts have information on smoking; most cohorts have information in different exposures; and there are cohorts planning to measure exposures but have not done it yet. A large number of cohorts rely on questionnaires, might also have other bio‐monitoring methods, etc.
Cohorts in ESCAPE are following the same protocol for exposures.
There is limited comparability when using different methods of exposure assessment.
WG – “Heavy Metals”: Maribel Casas
Biological samples provide a better estimation of exposure.
MW: some metals included in this report are not strictly “metals” such as arsenic which is a metalloid. These terms must be checked.
MK: other EU project focused on metals, and some cohorts are not in ENRIECO (PINCHE project). They look also neurodevelopment.
RG: asked if we know the correlation between metals environmental sampling and biomonitoring.
SC questions what the best media is to use to assess metals, as e.g. a lot of new research on meconium is available. It is thought that this should probably be included. Bio‐monitoring and exposure: will there be correlation data before making recommendations? (RG) If not, these could be part of recommendations; otherwise there could be problems with quality control.
“ENRIECO Workshop for user groups” (D11) 30
WG – “ Persisten Organic Pollutants”: Jens Peter Bonde (JPB ‐ covering for Gunnar Toft).
A draft report was circulated amongst the WG members. Most part to map cohorts where these compounds are (measurements). Different media have been used.
We will be thorough about measurements in the recommendations.
The WG will be looking into bio‐assays following a suggestion from the group.
WG – “Pesticides”: Cecile Chevier.(CC)
The complexity of assessing environmental exposure to pesticides was shown (multiples sources, multiple compounds). A great variety of types of assessment in the European birth cohorts was presented.
Q: Is there data to support danger living close to crops?
CC: In literature, it was assumed that living close to crops might mean that people are exposed to food from these crops; more recently, exposure via air was considered since crops may be dedicated to animal food. In European birth cohorts, diet data are available, but unfortunately distinction between organic and nonorganic diet is not always available.
In general it is quite different when pesticides are applied, etc. This is a difficult area of research. In California, there is slightly better detail (MN). In the EU it is difficult to obtain information. Household pesticides: there is little correlation with what people use or do at home or what replied in questionnaire. People don’t regard them as pesticides. Bio‐markers maybe better.
The example of a lice epidemic resistant to shampoo was mentioned; organo phosphate (cream) in children common to use to treat lice, sold in drugstores.
When it is being used in the shower, cases of intoxication have been described (also dermal exposure ‐ prescription informs consumer not to use it in this manner). Are effects known? The cream is currently forbidden in Denmark.
WG – “Emerging Exposures”: Maribel Casas.(MC)
There are emerging concerns about health effects of exposure to certain “new” industrial chemicals (phthalates and phenols, brominated and fluorinated compounds). MC presented the background to these exposures and the ongoing work in ENRIECO cohorts. One issue is the contamination of samples, this needs to be considered carefully for each group of compounds and guidelines may be helpful.
The WG will focus of recommendations of how measurements can best be conducted, and prioritize what measurements to use. For example, for phthalates, we know that a spot sample is not recommended; the need to develop a method of storage should be underlined.
“ENRIECO Workshop for user groups” (D11) 31
A publication was proposed to describe which are the best sample, analytical methods, etc to determine exposures of emerging concern within the birth cohort study design.
WP2 ‐ Ulrike Gehring continued
It was suggested (MW) that it would be good to suggest a best method for human bio‐monitoring and also what is the small amount of sample that is needed to have good analyses?
A European working group on biomonitoring was mentioned (COPHES).
It was suggested (ME) that it would be nice to refer to what has been done well by the cohorts, what was not good enough and what cohorts should not even try?
Proper bio‐monitoring should be done for a specific agent (MN). Some things are easy to do, some not so. The type of material is of main importance (e.g. cord or maternal blood). Recommendation level will not be the same for new and old pollutants.
WH: How many cohorts have specified research questions? MW: Should we summarize different cohorts with different questions?
Design issues in recommendations would be good to be mentioned, e.g. case‐control within cohorts (FP). Another issue is problems with classification, confounders, etc which leave cohorts unable to answer all the questions in the questionnaires.
ME: What could and should new cohorts do? What do cohorts in progress need to add?
From presentations by JPB and MC it could be derived that some exposures have been looked at a lot and others not.
In recommendations: should do recommendations on need for cohorts to study specific issues. MN suggested to do this in WP4.
The assessment of mixtures still needs addressing, we are currently measuring one chemical out of many, hence we need an assay that measures toxicity of mixtures.
A WG cross‐collaboration would be appropriate here and a suggestion was made to combine WP2 and WP4, which will be discussed in the WG. Likewise for endocrine disruptors, what assessment do we need? (Low exposure).
Mixtures’ exposure approach in terms of identified sources of mixtures: for example traffic for air pollution, or renovation activities (volatile exposures). Identifying exposure scenarios to regulate the source may be more beneficial than individual studies.
MN commented on the level of recommendations. Suggested recommendations more on birth cohorts. Think about what you would do with the current cohorts; continue in the same way, use registries, etc. It would be dangerous to go beyond cohorts.
There is always the question of a Mega cohort? Which is best?
“ENRIECO Workshop for user groups” (D11) 32
New exposures may be worth looking at, like nickel and eczema ‐ looking at levels compared in adults. Low variability in cohorts may mean low priority, but how are low and high defined, e.g. does lead have any variability?
We have the opportunity to harmonize cohorts and future data collection, e.g. through mental health questionnaire.
Day 2, 27 May
Plenary session: Current status of Case studies Aim: to present the progress in the case studies
9:00‐11:00 Case studies of Occupation, POPs and WP5 (3) Sylvaine Cordier, Jens Peter Bonde and Thomas Keil
Case study – Occupational exposures: Sylvaine Cordier (SC)
Main advantages are that the long term outcomes can be studied, not only short term. Including cohorts from different countries provides more power to evaluate risk and working environment.
Confidence in collected data:
- In addition to occupation links are also made to the economic environment to combine risks (secondary exposures)
- Self reporting varies in reliability. Depends on the quality of the questionnaire, how reliable are the answers. Better for prospective studies.
- Although very time consuming, the Job Exposure Matrix (JEM) is increasingly used; detailed info extracted about type of environment, tasks etc. With JEM, occupation is linked to likely exposures
Data collection appears mainly done through cohorts for maternal and paternal occupational exposures. Detailed exposures are available mainly for women, and often once during each trimester. It would be beneficial to collect by week of pregnancy instead.
A Coding Status is essential for recording and translating into analysable data. The UK code (SOC 1990) is likely to be used by us as coding system for all cohorts.
The WP has looked at frequency of collection in cohorts, in particular of service occupations. A large amount of data collected on healthcare employees is available.
Most occupations are service workers and include few industrial or agricultural employees.
Recommendation for future data collection to include
- job title, economic activity, name of company
- number of hours per week
“ENRIECO Workshop for user groups” (D11) 33
- free text description with three most important tasks (useful to describe in text what tasks they do in much detail, from this experts (e.g., chemists) would say that this work environment gets a reasonable precise evaluation of exposure).
- Including codes?
Discussion
A list of occupations at risk was recommended.
SC: other occupations, such as clerical and industrial workers are low in numbers. So, have agricultural and Health care service worker instead. Ask cohorts to check for other jobs (electrical workers?).
Birth defects are seen as potential target but homogeneity of assessment is difficult to review. Exclude cohorts with restriction on minor malformations, but likely to diagnose differently. It would be necessary to assess all cohorts on determination of birth defects as medical terminations in particular are indicative.
A question of how many weeks of exposure in general would be looked at, as for example Polish pregnancies at 1st or 2nd trimester can be on sick leave which will decrease exposure. It was suggested that in these cases, the exposure during the first weeks would pose enough risk.
It was argued that the use of JEM needs to be assessed of benefit to type of exposure, e.g. noise, cyclical work. JEMs are good but time consuming and require adjusting to country and timescale. It would take time to be time/country specific, might not be possible for ENRIECO. A cleaner in Spain for example is not the same like a cleaner in Denmark.
Input of country experts essential. An example of endocrine disruptor study in The Netherlands was mentioned.
Those who have created questionnaires know the reasoning behind it and can add to the ‘translation’.
SC suggests to assess exposures which are definitely higher in occupational environments. A Reference group should be used rather than adhering to manual/non‐manual classification of occupations, which will provide starting point to evaluate other outcomes, during childhood (child behaviour). Some occupations are done by immigrants in particular, it may be necessary to check this issue perhaps (MK).
PW: Using education and job title we can create an exposure matrix, which is more beneficial. In parallel the description of work and job title can be done (SC).
Action: SC to contact cohorts who want to contribute – cohorts present at meeting to contact SC if interested.
“ENRIECO Workshop for user groups” (D11) 34
Case study – Persistent Organic Pollutants: Jens Peter Bonde (JPB)
Provided a summary the WG objectives and of people. The work has been coordinated through email and 2 meetings held.
Animal literature is justifying the study. The result of this study will be interesting to increase the level of evidence, either positive or negative (cohort list on slide not updated).
Harmonization POPs and health outcomes: Eva Govarts (EG)
Provided a summary of selection criteria and covariates taken into account when analyzing birth weight. The covariate alcohol intake was taken out cause it didn’t contribute to the variability of birth weight in any of the cohorts.
Distribution of POPs (PCB153 and p,p’‐DDE) and birth weight; results of regression analyses need to be interpreted, estimates going down and up for different POPs (PCB153 v DDE).
E.g. for the Flemish cohort (FLEHSI), an increase of PCB153 coincides with reduced weight, for DDE no significant correlation exists.
JPB continued.
PCB‐153 in cord blood is measured in various countries, but not yet everywhere. Variations exist in median per cohort. We should address other compounds as well. Sources of PCBs are different, so we don’t expect homogeneity in different cohorts. Will not be able to do analysis but describe profiles. The change over time in level is interesting if valid. If it means something different it is a problem. Most cohorts are new. (might be an issue for SGA)
Effects can depend on the time of study: and old Groningen study indicates high levels (but is reduced now?), while Greenland is high because the current exposure is high.
(SC) More than 50% detected, levels have been reduced (replacing 50% of missing values data is not good idea)
Discussion about the approach taken by the group:
- not to publish data that are not included
- ‘STRICT’ meta‐analysis to be a paper?
- Action: to draft a paper and approve by group by November 30th 2010
- suggestions for additional papers POPs and gestational age, sex ratio, and development of concept: ´strict´ meta‐analysis
- Dissemination to stakeholders and media (after publication), to be discussed with WP6.
“ENRIECO Workshop for user groups” (D11) 35
Questions still to be answered relate to the causes of heterogeneity; what do data show? PH implications ? Developing “strict meta‐analysis” .
Discussion
Both PCB and DDE exposures will be included, taking in account that they behave differently. Most cohorts have both. (MK) Linear regression is not good to look at thresholds. This has not been taken in account yet, and data need to be adjusted, but the WP wanted to know there was something to look at rather than focus on thresholds (JPB).
TK suggested that ‘strict’ meta‐analysis is an odd definition, and proposed the use of something like ‘individual participant meta‐analysis’
Was there adjustment for region? According to EG the model could not converge when region was in.
WP5 – Database building: Cynthia Hohmann (CH)
CH gave a summary of the WP structure (see slides) and status of the WGs.
Following indication of interested cohorts, the WP defined what study data are useful for inclusion.
Questionnaires were filled in (e.g. assessment of maternal‐paternal smoking, dampness and/or mould, asthma, allergic rhinitis, eczema). These data were used to assess whether cohorts were eligible to take part. Step4, conducting analysis has now commenced.
Number of children included in work: WG1: 38000; WG2: 36000; WG3: 50000
Data check to start soon; CH does descriptive analyses and data will be checked by the cohorts.
Action: CH to perform descriptive analyses of cohort data and send email to the cohorts to confirm the data.
Cut‐off for the work will be in November, taking in account the report which will be delivered. Papers are not a priority for WG3, 2 months delay.
MAC suggested that the EDEN study could participate. Generally, it is not feasible to complete publications by November. A draft paper may be ready but there will be reviews and revisions. Heterogeneity was brought up. Might use meta‐analysis.
JH: look at cohorts. Do test for heterogeneity, and then see.
MN agreed that third case study of this WG is not committed to deliver by Feb as this is extra. A lot of work still needs to be done (interpretations etc).
Action: CH and DG to discuss wording of changes to the DoW to fit timescale realistic to WG3.
“ENRIECO Workshop for user groups” (D11) 36
11:30‐13:30 WP3 General overview: Remy Slama Current status of WGs (2‐3 WG leaders) Recommendations
WP3 – Evaluation of Health Outcomes: Rémy Slama (RS)
RS provided a summary of the WP composition (see slides)
Following the definition of WGs, protocols were developed and WGs are following the steps as planned. WG6 – “Child growth, metabolic and endocrine disorders” ‐ was added as new group following the kick‐off meeting in Barcelona.
Preliminary conclusions:
- large sample sizes and good quality or homogeneous health data are available to study Birth Weight within European birth cohorts;
- large sample size but possible standardization issues/biases for Time to Pregnancy and General cognition;
- small sample size for Ultrasound‐based foetal growth, ADHD, airway obstruction and airway inflammation.
Are recommendations to include suggestions for follow‐up? SC suggested that factors such as diet and neurobehavioral issues could be suggested for inclusion in current (running) cohort work, rather than for future work only. Also, standardising follow‐up should be part of recommendations.
FP questioned the presence of recall bias in the retrospective study of Time to Pregnancy. RS argued that some publications (e.g., M Joffe et al) have studied the quality of recall of time to pregnancy over several years, and that, over a short period, recall bias should be limited at the group level.
Publications: (see slides)
- one planned for final report
- authorship issues: are we following general rules within ENRIECO?
Action: MK to draw up publication guideline for scientific papers.
WG6 – Child growth, metabolic and endocrine disorders: Marie‐Aline Charles (MAC)
Early neonatal weight loss is thought to be indicative of later obesity, not sure whether all cohorts have this factor included.
Response to Growth Hormone starts around 6 months; many cohorts have information on growth during the period between 6 and 24 months of age.
“ENRIECO Workshop for user groups” (D11) 37
First recommendations (see slides)
- need more cohorts, lack of data
- gaps identified in data periods, 1‐2 years; thought to have included physician measurements of paediatricians, not of parents.
Action: cohorts to let MAC know if these factors are known.
Postnatal weight and height body composition
- one evaluation of fat mass distribution
- waist circumference useful from 3 years, but before still questionable
- data on diet and physical activity: diet varies by country.
Available data: summarised in slides.
ANA asked about recommendations on fathers’ weight and use of data on development of both mothers and fathers. Are more measurements of obesity in families available? (Also taking into account children who do not live with biological parents). Information on duration of cohort is also of importance (ME).
An overview of planned questionnaires of cohorts is provided, in slides included planned exams.
MAC commented that the report will make a distinction of what is in the database and what the PI has declared as next follow‐up questions?
WG4 ‐ Childhood cancer: Manolis Kogevinas (MK)
The number of observations in the European birth cohorts is the main issue, due to the low incidence of childhood cancer.
Recommendations (also see slides)
- need for registry based studies
Shanghai launching a new 100000 children study
A problem with I4C is that it takes a long time before enough data is collected (eg US, 6 years from start).
Collaborating with ENRIECO and CHICOS for different inventories.
Biomarker based studies: valid results? The effects are not clinical outcomes. Macronuclei do not indicate much, need to wait for 8 years to know the outcome.
- Stick with the cohort design.
Discussion and comments
It was questioned how many ENRIECO studies would be able to answer the questions set; Germany for example does not have follow‐up for childhood cancer.
“ENRIECO Workshop for user groups” (D11) 38
The I4C has set a minimum limit of 1000 children for the validity of studies, yet we need more influence from Europe in I4C.
WP2 is thinking of recommending standard questions for cohorts to include in questionnaires (MV).
It was posed that too much coordinating of collection like we are aiming for may result in a lack of cohort diversity in 30 years time (ANA). Standardisation in theory works great, but should we steer clear of too much? Diversity is important because we are learning from everyone in regards to questions, focus.
WG1 ‐ Reproductive outcomes: Rémy Slama
The first results concerning specific outcomes are given as an illustration.
Time to pregnancy:
- the ideal design is an incident cohort of couples recruited at the start (or during) the pregnancy attempt, but this is a very challenging design;
- birth cohorts recruit after the end of the pregnancy attempt, once the pregnancy has started (or even ended). As a consequence, infertile couples are excluded, which is a potential source of bias. Moreover, information on exposure and confounders during the relevant period (pregnancy attempt) may not always be available in birth cohorts.
Birth weight:
- large number of observations available from the existing European birth cohorts.
Ultrasound‐based fetal growth:
- the number of pregnancies with available information is quite limited if we restrict to pregnancies with 3 ultrasound measures, and a bit higher if pregnancies with at least 1 ultrasound measure are also considered.
It will be relevant to cross the information on health outcomes with information on exposures obtained by WP2.
Discussion and comments
FF mentioned that in the case of cohorts with a recruitment at birth or later, there is some concern for "at risk" pregnancies or pregnancies with an adverse outcome (e.g., prematurity) to be under‐represented, hence possibly inducing a selection bias. RS indicated that this is indeed a possible concern, and that for this reason the WG has suggested to distinguish cohorts with a prenatal recruitment (for which a selection linked to the pregnancy outcome is less likely) from cohorts with a postnatal recruitment. Specific checks need to be done regarding the inclusion criteria of the LISA cohort.
“ENRIECO Workshop for user groups” (D11) 39
WG2 – Allergy, asthma and respiratory health: Linus Grabenhenrich and Cynthia Hohmann
Different pulmonary pathologies are considered.
Sources of bias in the assessment of pulmonary function and related outcomes include asthmatics becoming familiar to measurement techniques and false negative results if asthma is well controlled.
Assessments of pulmonary function are planned in Generation R and FLEHS, as well as in EDEN and possibly ELFE.
Recommendations for combined analysis
KOALA and LUKAS will also release data on bronchodilator response soon.
Recommendations:
- develop guidelines for pulmonary functions tests
- no lung function assessment to be recommended to cohorts with broader focus. Generally disadvantages of cost, time and dropouts.
WG3 – Neurodevelopment: Joan Forns (JF)
Background of neurodevelopment assessment
Some countries have specific questionnaires; maybe we can recommend a range of questionnaires (SC).
14:30‐16:30 WP4 General overview: Joachim Heinrich / Chih‐Mei Chen Recommendations
WP4 – Evaluation of exposure‐response relationships: Chih‐Mei Chen (CMC)
WG – Air pollution and Allergy and Asthma: Ulrike Gehring
Discussion and comments
Discussion on possible mechanism for eczema: particles can go through the skin
Most study collected data have not studied association. It would be very important if information was to come out on air pollution and eczema. More data are needed, and more analysis.
(MK) maybe also study birth weight and gestational age, other’s findings are not enough. (CMC): a review paper will come out of this project.
Review paper by CMC: slides
“ENRIECO Workshop for user groups” (D11) 40
WG – Allergens/Biological Organism and Allergy and Asthma: Chih‐Mei Chen
Question: what kind of mould are you studying? Visible mould.
WG – POPs and Neurobehavioural/Cognitive Function: Mireia Gascon (MG)
In discussion:
‐ 12 cohorts with 9 papers published within ENRIECO, plus 3 other European cohorts, with 10 other papers.
‐ The most studied compound is PCB, and in less extend DDE, DDT, HCB and others such as PFOS or PFOA. There are newer compounds which are planned to be assessed and that are increasing in levels around the world, like flame retardants (PBDE, etc). The situation is similar for studies outside Europe.
‐ For PCBs differences in results might be explained by the fact that older cohorts had higher exposures. But exposure and neurodevelopment are differently assessed within each study, which makes it difficult to compare results or to pool data for meta‐analyses, etc.
WG – Water contaminants and Birth Outcomes: Jeremie Botton (JB)
In discussion:
There was a question on why no EU cohorts are looking at this? Maybe difficult to assess contaminants, maybe not much of concern or no availability of “water” epidemiologists. Depending on the substance measured, maybe they look at ‘hot” spots only. Need to collect more data.
WG – Pesticides and Birth Outcomes: Cecile Chevrier (CC)
In discussion:
There was a suggestion that future studies be more specific in compounds or groups of compounds or use bio‐markers maybe.
Question on Best Design? (CC) Ecologic do well when we assess exposure to pesticides with residence proximity to agricultural activities in the sense that their results are consistent. However, they missed to take into account a lot of confounders whereas cohorts can. Right now, it is difficult to conclude what is the best design, except when using biomarkers, prospective cohorts are powerful.
WG – Noise and Paediatric and Birth Outcomes: presented by Chih‐Mei Chen
WG – POPs: Jens Peter Bonde (For Gunnar Toft)
Mentioned : 2004 review Gunnar Toft & 2007 Wiggle et al (see slides)
“ENRIECO Workshop for user groups” (D11) 41
Halldorsson et all 2008 recommended for POPs update general.
Recommendations
(internal)
There is a need for a new review paper which could include other outcomes.
Question: Criteria for final conclusion?
Not a very comprehensive evaluation (JPB). Have few studies available with good quality and 2 designed very well.
(external) – see slides
WG – Metals and neurobehavioural/cognitive function: Maribel Casas
MC provided a review including metals and neurotoxic effects, and a description of the work gathering data.
Conclusions (see slides)
- best predictors of mercury associated neuropsychologic deficits
- selenium is not proven to be protective against methylmercury toxicity
- more research needed as results are inconsistent
- only lead methylmercury and arsenic are proven to be neurotoxic
- more cohort involved studies are needed
More than 30 cohorts are currently included the WG is investing in future collaborations.
A suggestion was made to propose EU studies with other metals, maybe propose to do mercury exposure studies? A lot of fish eating populations in Mediterranean.
Levels in methylmercury are different between countries. Could define the lower limits.
(ME): Breastfeeding influences exposure levels. Could look at postanatal exposure in longitudinal studies. A gap of knowledge can be filled.
It would also be good to look at postnatal exposures. It may be worth looking at opportunities following recommendations from WP2 and 3?
Chih‐Mei Chen, continues on WP4 presentation
Discussion
“ENRIECO Workshop for user groups” (D11) 42
There is scope for objective evaluation into why the WHO sees particular factors as important. Are we in a position to do such an evaluation?
For one, we need to be able to justify such approach; a need exists for a WHO body, similar to IARC on carcinogenicity and reproduction. It would give power to ENRIECO reviews if they use the same standardized methodology.
CT pointed out that we need 1) sort‐out possible bias , 2) criteria for causal inference
We should exclude animal evidence. WHO criteria more relevant to epidemiology.
We need to be more modest and summarize a set of qualitative criteria.
Some guidelines should be applied. Work should be published, maybe combined with WP2. Application can be discussed during WP2&4 submeeting (CMC).
Questioned is whether evidence has been collected between all of us. We have to stick to what we have tools for, but maybe it is possible to come up with a set of basic criteria. Exposure‐response relationship work also needs to be continued.
What next (also see slides):
- Ranking evidence, harmonised evaluation strategy
- Publication of reviews
- Combine information collected in ENRIECO
“ENRIECO Workshop for user groups” (D11) 43
Day 3, 28 May Plenary session: Wrap‐up and General Assembly 12.30‐13:00 Aim: to discuss general related to the project and wrap up
Mark Nieuwenhuijsen Mark Nieuwenhuijsen chaired this session to evaluate the meeting outcomes. A general recognition that we are having a good process in place to continue while work is making progress. The workshops are considered very helpful to link with cohorts and EU partners. The need for people from different cohorts to come together is strong, more discussion face to face really provides benefits, e.g. for rare outcomes and birth defects. It allows for making more of pooled cohorts and formalises the work. Future investment in such meetings is recommended; also as this is a relatively ‘cheap’ option for the EU as it brings together cohorts which rely on national funding. The need for cohorts to meet was emphasized during the discussion. The question is whether this success counts for the environmental studies only. Besides the convention with cohorts, the meeting also greatly benefits the clear vision on WP work. It was suggested that we need another level of synthesis across the WPs, and that they should continue to meet to keep a clear overview. MN reminded all that the WPs have some funding to have a meeting later this year. Also, CREAL is hosting the 23th ISEE 13‐16th September 2011, all are invited to submit ideas for this meeting. A question was posed whether a suggestion can be made for Biobank on exposure, as this would include a lot more such as clinical cohorts. E.g. breast milk. This would pose very expensive, and policies are limiting exchange of information or materials internationally. In Czech republic programmes on biomonitoring are ongoing. A step towards biobanking would be politically unwise, as we would risk additional funding for approaching cohorts and doing follow up. It would also mean loosing direct contact and only have biological samples. On the point of the setup of ENRIECO it was commented that ongoing projects can give idea of usefulness of building on previous cohorts (ESCAPE). Suggested also was that we may have too many interests. A mega cohort as proposed by the EU would work away form cohorts and result in arguments who is going to take part, the US experience not very comforting.
“ENRIECO Workshop for user groups” (D11) 44
Small cohorts are European wide, a mega cohort reduces this. We should not be making any recommendations in the reports on this, it would be good to see more EC funding for joint efforts in using existing data, which questions to use etc. Maybe chemical analysis could be added, which is very expensive and can’t be done by existing cohorts. Exposure assessments are expensive and labs not good enough – this will be discussed in the WP3 report. Action: Final reports will be circulated amongst all participating cohorts as well as partners before submission to the EC later at the end of 2010. The deadline for submission to the Coordinator is 30th November.
“ENRIECO Workshop for user groups” (D11) 45
Parallel Sessions’ Minutes
Day 1, 26 May Parallel sessions: WPs and Case studies (current work)
Aim: the various WPs and case studies spend discussing various issues amongst themselves in preparation for the plenary sessions
9:00‐10:30 WP2, WP3 and WP4 11:00‐13:00 Case studies of Occupation, POPs and WP5 (3) Day 3, 28 May Parallel sessions: WPs (future work)
Aim: to discuss within the WPs further work that needs to be done
9:00‐10:30 WP2, WP3 and WP4 11:00‐12.30 Case Studies (future work)
Case studies of Occupation, POPs and WP5 (3)
WP2 – Evaluation of Exposures Parallel session, Wednesday 26 May, 9:00‐10:30 Ulrike Gehring gives an overview of the current status of WP. A lot of work has been delivered in preparation to the meeting. The descriptive parts of the reports are pretty advanced, need a bit more work but this can be done quickly. Guidance should be given on which topics to address in the recommendations part of the reports. Since we are working with a short timeline, we need to agree soon on what to address, to create some structure. Suggestion: give broad categories that can be filled in by the different WGs. Recommendations Things that could be addressed in the recommendations part. Ulrike Gehring presents summary of things that have been mentioned in draft recommendations by the different groups to start up the discussion:
1. Refined exposure assessment a. Repeated exposure assessment measures b. Time‐activity pattern
2. Standardization of methods and protocols 3. Validation studies 4. Inter‐laboratory comparisons/calibration 5. Limits of quantification 6. Use of routine data (pesticides, water) 7. Best method? 8. Relevant confounders (most relevant ones only)?
“ENRIECO Workshop for user groups” (D11) 46
Things that were discussed:
- Refined exposure assessment better: valid exposure assessment - Quality control to see whether the methods among the cohorts are
comparable. - Recommend ‘best’ method to be used with specific exposure assessment - Limit of quantification and how to handle the values below limit of detection - Calibration between the labs - Relevant confounders more relevant for other WP? No, if you are
interested in exposure X you need to assess exposure Y as well. For example, measure creatine in urine when interested in a specific compound in urine. Only mention few very important ones!
- Use of additional data/routine data: Water contaminants (and other e.g. pesticides) information available from water companies (map sources) could be included in the dataset. However, comparison between countries may be difficult.
• Recommendations for meta‐analysis: Minimum requirements to include a cohort when you want to perform a meta analysis.
Publications
• One overview paper with limitations recommendation s and online supplement for the groups or reference to ENRIECO website.
• Pesticides • Emerging exposures/best methods • POPs part of case study • Possibility to combine it with WP4
• Air pollution • Water contamination • Heavy metals • Noise?
• Combined paper about biomonitoring • Water group could be involved in other groups.
Parallel session, Friday 28 May, 9:00‐10:30 WP2/WP4 discussion Future work:
1. Deadlines 2. What are the next steps 3. Publications 4. Recommendations
Deadlines
“ENRIECO Workshop for user groups” (D11) 47
End of October for the separate reports since WP‐leaders need to combine them in the overall report. Deadline for the reports is November 2010. Publications • WP2: recommendation part is missing, but drafts available. One overall paper,
but not separate paper for all groups.
• WP4: minimum requirement is report on exposure‐response relationship. Since it is a systematic review which is a lot of work the group may decide that a paper is possible (Chi‐Mei).
• Deadline for publication of the papers are not strict but it is recommended that a draft is available in the start of 2011.
WP 2 (revised list from above) • One overview paper with limitations recommendation s and online
supplement for the groups or reference to ENRIECO website. • Pesticides ‐ possibly just an exposure paper but combination with WP4
possibility • Emerging exposures/best methods • POPs part of case study • Air pollution – no separate exposure paper, maybe in combination with WP 4 • Water contamination – in combination with WP 4 • Heavy metals – in combination with WP 4 • Noise – in combination with WP 4
WP 4 (Chih‐Mei Chen)
WP 2 recommendations (revised version of list from above)
1. Valid exposure assessment a. Repeated exposure measures b. Time‐activity pattern c. Best method
2. Standardization of methods and protocols; biological materials (blood, urine,…), does it matter
3. Validation studies 4. Inter‐laboratory comparisons/calibration 5. Limits of quantification/sensitivity of methods 6. Use of routine data (pesticides, water) 7. Best method? 8. Relevant confounders (most relevant ones only)? 9. What has been done good? What can we do with it in future? What would
we do different/better in future? What should we never try? 10. Address design issues; why do we need (new) cohorts to address certain
research questions?
“ENRIECO Workshop for user groups” (D11) 48
11. Lack of knowledge 12. Assessment and evaluation of mixtures of pollutants 13. Sources of mixtures: pollutant regulation/policy making 14. New exposures worth mentioning 15. Variability of different exposures within cohorts 16. Recommendations could be used for harmonized future collection of data 17. Experts/labs
WP 1 Inventory database All WG leaders: If you find any inconsistencies in the database of if there is information missing, please report this back and work closely together with Maribel Casas ([email protected]).
“ENRIECO Workshop for user groups” (D11) 49
Recommendations Idea is to have a list with broad categories (overlap with other projects (e.g. COFIS?) and have specific recommendation within the group reports. We also need to establish whether the recommendations make sense. Lessons learned should be the start of the recommendations. Questions like: Does it make sense to study component X or does it make sense if you only have one measurement should be addressed. Other data sources may be useful to include to improve the available information. Discussion on the VOC topic. There is no working group on VOC and ETS and other indoor exposures are covered in the different groups. Suggestion to use the MOOSE guidelines for reporting the evidence or develop a checklist for ourselves. The MOOSE is quite extensive but for a peer reviewed paper most of the topics listed in the MOOSE should be incorporated. For ENRIECO we could think of some key guidelines (Chi‐Mei will draft something) that should be incorporated in the reports. A way to do this is to rank to quality of the studies. The question is how to do this properly. ArcRisk has a form for data extraction that could be used as example for our own guidelines. A small working group (volunteers; Ulrike, ChiMei, Achim) on this issue may look at this problem and suggest a solution (a short list of suggestion should follow). It is not possible to set this for all working groups and there are reviews available. The strategy could be copied from other projects (WHO, IPCC) that faced similar problems. Overall recommendations; For the working groups some guidelines should be provided how to describe the recommendations and what issues to think of. From these group recommendations some overall recommendations should arise. For suggestions on recommendations we could learn from the AMAP study: ww.AMAP.no JdH will sent IPCC protocol to Chi‐Mei to integrate information coming from different science fields.
“ENRIECO Workshop for user groups” (D11) 50
WP3 Evaluation of health outcomes Parallel session, Friday 28 May, 9:00‐10:30 During this parallel session concerning WP3 (health outcomes), some general issues concerning all working groups were first discussed; a specific meeting of the birth outcomes working group was then held.
I. Issues general to all working groups
I.1) Database
In their process of identifying the cohorts in which each health outcome can be studied, WGs should create variables to be appended to ENRIECO database; similarly, variables corresponding to the groups of cohorts with homogeneous information on each health outcome defined (see protocol) by the WGs should be created. These variables will be useful to easily extract information on these cohorts (e.g., sample size, exposure information available…). This concerns all WG but cancer and case study. This information will be centralized by the work package leader, and made available to the other WP (in particular WP1).
I.2) Protocol
In the protocol, it was originally stated that the sources of bias in the assessment of each health outcomes should be listed in a table. If for some outcomes a Table does not appear as a very convenient or suitable format, then a simple list can be provided instead.
II. Birth outcomes working group
II.1) Papers
In addition to the main paper of the birth outcome working group, an additional paper (that would come after the end of the project) on the possibility to study congenital malformations and foetal loss within birth cohorts was suggested by A.M. Nyboe Andersen and S. Cordier. The issue will be anyway tackled in the report and in the main paper.
II.2) Meeting
A meeting of the birth outcomes working group will be held in the early autumn in Paris or Lyon.
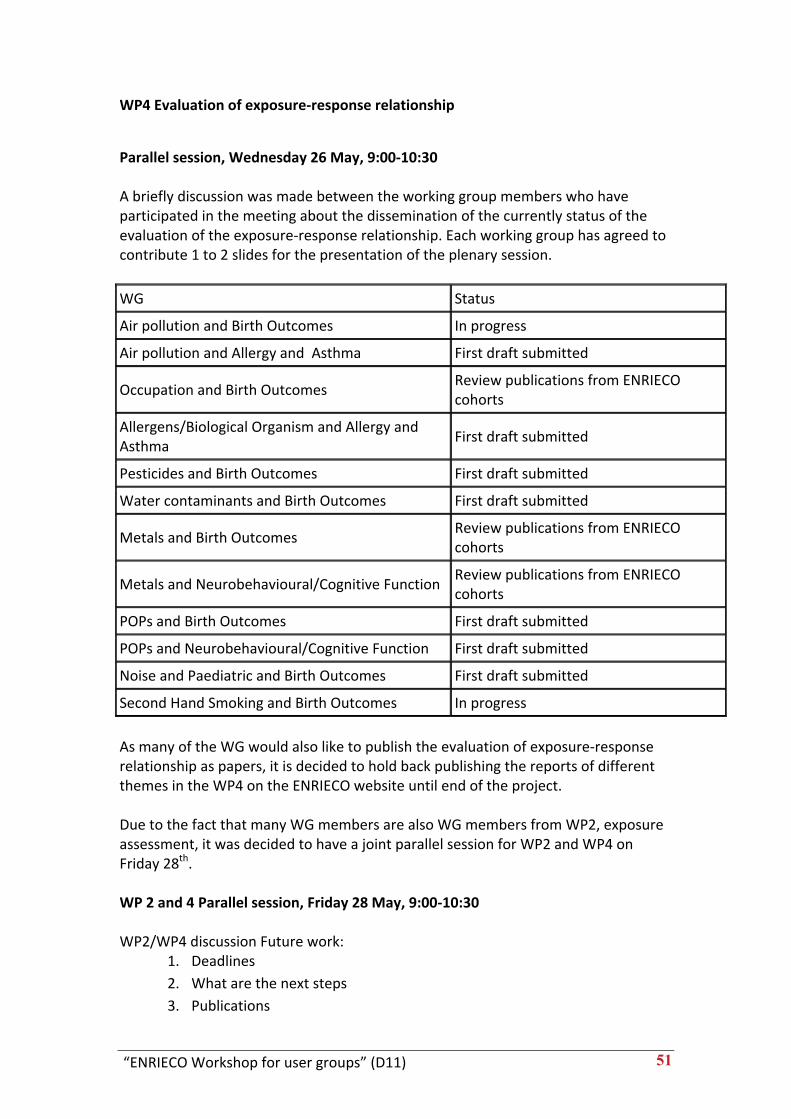
“ENRIECO Workshop for user groups” (D11) 51
WP4 Evaluation of exposure‐response relationship
Parallel session, Wednesday 26 May, 9:00‐10:30 A briefly discussion was made between the working group members who have participated in the meeting about the dissemination of the currently status of the evaluation of the exposure‐response relationship. Each working group has agreed to contribute 1 to 2 slides for the presentation of the plenary session.
WG Status
Air pollution and Birth Outcomes In progress
Air pollution and Allergy and Asthma First draft submitted
Occupation and Birth Outcomes Review publications from ENRIECO cohorts
Allergens/Biological Organism and Allergy and Asthma
First draft submitted
Pesticides and Birth Outcomes First draft submitted
Water contaminants and Birth Outcomes First draft submitted
Metals and Birth Outcomes Review publications from ENRIECO cohorts
Metals and Neurobehavioural/Cognitive Function Review publications from ENRIECO cohorts
POPs and Birth Outcomes First draft submitted
POPs and Neurobehavioural/Cognitive Function First draft submitted
Noise and Paediatric and Birth Outcomes First draft submitted
Second Hand Smoking and Birth Outcomes In progress
As many of the WG would also like to publish the evaluation of exposure‐response relationship as papers, it is decided to hold back publishing the reports of different themes in the WP4 on the ENRIECO website until end of the project. Due to the fact that many WG members are also WG members from WP2, exposure assessment, it was decided to have a joint parallel session for WP2 and WP4 on Friday 28th. WP 2 and 4 Parallel session, Friday 28 May, 9:00‐10:30 WP2/WP4 discussion Future work:
1. Deadlines 2. What are the next steps 3. Publications
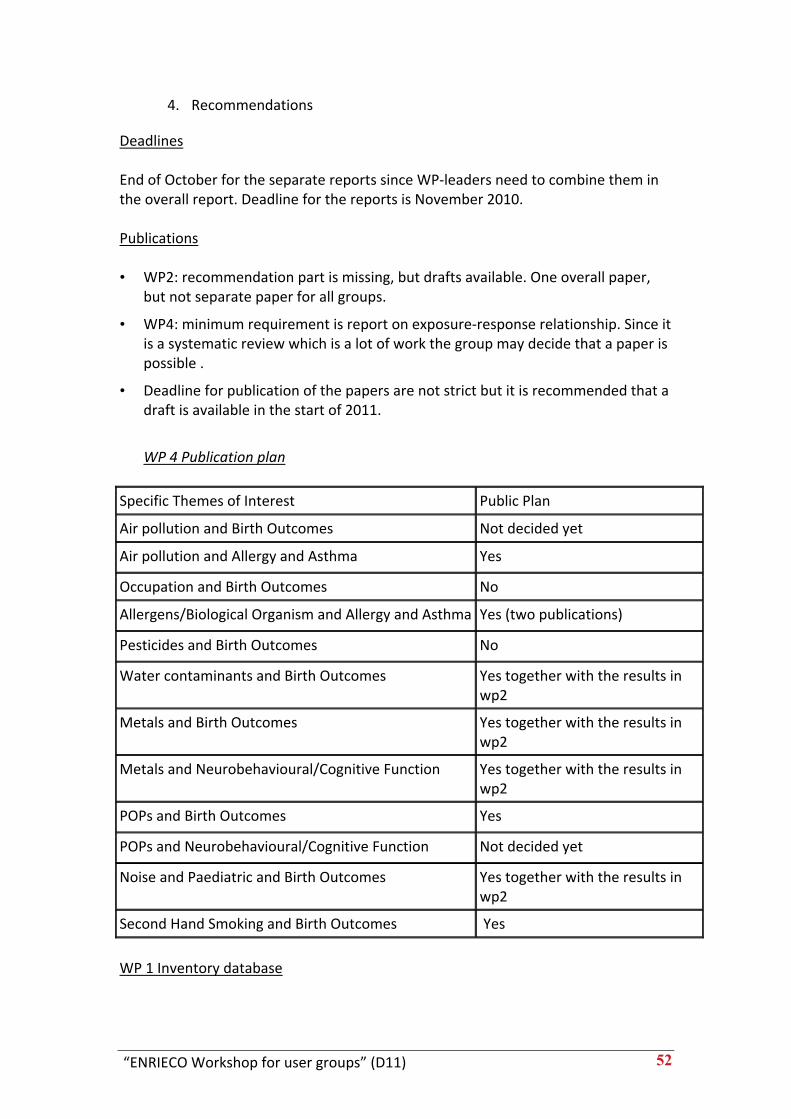
“ENRIECO Workshop for user groups” (D11) 52
4. Recommendations
Deadlines End of October for the separate reports since WP‐leaders need to combine them in the overall report. Deadline for the reports is November 2010. Publications • WP2: recommendation part is missing, but drafts available. One overall paper,
but not separate paper for all groups.
• WP4: minimum requirement is report on exposure‐response relationship. Since it is a systematic review which is a lot of work the group may decide that a paper is possible .
• Deadline for publication of the papers are not strict but it is recommended that a draft is available in the start of 2011.
WP 4 Publication plan
Specific Themes of Interest Public Plan
Air pollution and Birth Outcomes Not decided yet
Air pollution and Allergy and Asthma Yes
Occupation and Birth Outcomes No
Allergens/Biological Organism and Allergy and Asthma Yes (two publications)
Pesticides and Birth Outcomes No
Water contaminants and Birth Outcomes Yes together with the results in wp2
Metals and Birth Outcomes Yes together with the results in wp2
Metals and Neurobehavioural/Cognitive Function Yes together with the results in wp2
POPs and Birth Outcomes Yes
POPs and Neurobehavioural/Cognitive Function Not decided yet
Noise and Paediatric and Birth Outcomes Yes together with the results in wp2
Second Hand Smoking and Birth Outcomes Yes
WP 1 Inventory database
“ENRIECO Workshop for user groups” (D11) 53
All WG leaders: If you find any inconsistencies in the database of if there is information missing, please report this back and work closely together with Maribel Casas ([email protected]). Recommendations Idea is to have a list with broad categories (overlap with other projects (e.g. COFIS?) and have specific recommendation within the group reports. We also need to establish whether the recommendations make sense. Lessons learned should be the start of the recommendations. Questions like: Does it make sense to study component X or does it make sense if you only have one measurement should be addressed. Other data sources may be useful to include to improve the available information. Discussion on the VOC topic. There is no working group on VOC and ETS and other indoor exposures are covered in the different groups. Suggestion to use the MOOSE guidelines for reporting the evidence or develop a checklist for ourselves. The MOOSE is quite extensive but for a peer reviewed paper most of the topics listed in the MOOSE should be incorporated. For ENRIECO we could think of some key guidelines (Chi‐Mei will draft something) that should be incorporated in the reports. A way to do this is to rank to quality of the studies. The question is how to do this properly. ArcRisk has a form for data extraction that could be used as example for our own guidelines. A small working group (volunteers; Ulrike, ChiMei, Achim) on this issue may look at this problem and suggest a solution (a short list of suggestion should follow). It is not possible to set this for all working groups and there are reviews available. The strategy could be copied from other projects (WHO, IPCC) that faced similar problems. Overall recommendations; For the working groups some guidelines should be provided how to describe the recommendations and what issues to think of. From these group recommendations some overall recommendations should arise. For suggestions on recommendations we could learn from the AMAP study: ww.AMAP.no JdH will sent IPCC protocol to Chi‐Mei to integrate information coming from different science fields.
“ENRIECO Workshop for user groups” (D11) 54
WP 5 Minutes ENRIECO WP 5 meeting during parallel session, 26th May, 2010, 11:00‐12.30 CET Participants: Chih‐Mei Chen (LISA), Joachim Heinrich (LISA), Thomas Keil (MAS), Eva Morales (INMA), Ulrike Gehring (PIAMA), Monique Mommers (KOALA), Cynthia Hohmann (MAS) 1. Introduction Overview of Work Package (WP) 5 and current status of Working Groups (WG) was reported by Cynthia Hohmann. 2. Working Group 1, mould/dampness and asthma/allergy Planned analyses were discussed.
STEP ONE: o Descriptive analyses (per cohort) STEP TWO: o Multiple logistic regression analysis (per cohort)
To determine the effect of current exposure (5‐10 years) to damp indoor environment and visible mould on current allergic diseases and symptoms
o Longitudinal analysis with random effects (per cohort) To determine the effect of exposure to damp indoor environment and visible mould during early childhood (up to age two) on the development of allergic diseases and symptoms
STEP THREE: o Meta‐Analysis (combined)
Perform meta‐analyses for the two models conducted in step one independently
3. Data transfer agreement Discussion on how long the data of cohorts should be available for the planned analyses of working groups?
• WG 1 and WG2; deadline of deliverable is set in the end of Nov 2010. The data still has to be available for further corrections, checks and alterations in the manuscript till Nov 2012.
• WG3; as this working group was not originally planned within the ENRIECO project, the deadline for the first draft of the manuscript could eventually be
“ENRIECO Workshop for user groups” (D11) 55
extended, e.g. Feb 2010. (This was discussed with Constantine Vardavas, CREAL, at Friday 28th May 2010, see protocol.)
4. Next steps
1. It was agreed that Cynthia Hohmann will provide descriptive results of harmonized data to the PIs and data managers of cohorts, asking to check information of prevalences within 2 weeks. In case of inconsistencies the data will be checked.
2. All WGs will contain updates of datasets if necessary. 3. A next meeting at the Helmholtz Institute in Munich was planned for the
beginning of July (Christina Tischer, Chih‐Mei Chen, Joachim Heinrich, Thomas Keil, Cynthia Hohmann).
After the meeting, contact to the PÉLAGIE cohort was established. Additionally, the cohorts EDEN, HUMIS, AMICS‐Barcelona and the Northern Finland Birth Cohort expressed interest in participation. Minutes ‐ ENRIECO WP 5 meeting during parallel sessions 28th May, 2010, 10:00‐11.00 CET Parallel Session Participants: Constantine Vardavas (RHEA), Maria Vassilaki (RHEA), Manolis Kogevinas (RHEA), Cynthia Hohmann (MAS) 1. Working Group 3, second hand smoke exposure and wheezing 0‐2 years Planned analyses were discussed. STEP ONE:
o Descriptive analyses (per cohort) o Exposure categories of different maternal and paternal/others
smoking will be built and checked for eligibility for analyses
STEP TWO: o Longitudinal analysis (not further specified yet, per cohort)
To determine the effect of second hand smoke exposure during pregnancy and early childhood (up to age two) on the development of early wheezing symptoms (0‐2 years).
STEP THREE:
o Meta‐Analysis Perform meta‐analyses for the model conducted in step one
3. Data transfer agreement
“ENRIECO Workshop for user groups” (D11) 56
• It was agreed that a paper ready to submission will be finalized by the end of Feb 2011. The data should be available for corrections and alterations for another year untill Feb 2012.
4. Next steps
1. It was agreed that new cohorts (HUMIS, EDEN, Northern Finland Birth Cohort, PÉLAGIE, AMICS‐Barcelona) found to be potentially eligible for combined analyses, will be contacted the week after the ENRIECO work shop in Utrecht by Cynthia Hohmann. They will be given two weeks for appropriate data provision.
2. It was agreed that Cynthia Hohmann will provide descriptive results of harmonized data to the PIs and data managers of cohorts, asking to check information of prevalences within 2 weeks. In case of inconsistencies the data will be checked.
3. All WGs will contain updates of datasets if necessary. 4. A next meeting at the Karolinska Institute in Stockholm was planned for
mid of September for discussion of the analyses of WG2 and WG3 (Magnus Wickman, Asa Neuman, Eva Hallner, Anna Bergstrom, Thomas Keil, Cynthia Hohmann and optionally further representatives of WG3, e.g. David Martinez).
“ENRIECO Workshop for user groups” (D11) 57
Minutes ENRIECO POP‐CASE study UTRECHT 26‐28.5.2010 Participants: Ulrich Ranft, Eva Govarts, Arja Ratio, Merete Eggesbo, Monica Guxens, Sylvaine Cordier, Cecile Chevrier, Stephanie Vandentorren, Mark Nieuwenhuijsen, Jens Peter Bonde A. Update of second version of analysis program:
1. Extended test of fit of the final models
2. Sensitivity analysis for lipids: adjusted values substituted by lipid as covariate in modeld
3. Fewer categories in covariates as parity and age
4. Analyses of bw in tertiles of exposures (crude and fully adjusted models)
5. Revision of axes in plots and cb153 exposure categories to fit the data ranges in all cohorts
B. Ideas for additional papers based upon the dataset that have been defined in all cohorts:
POPs and gestational age POPs and sex ratio DDE and overweight babies exposure‐response, threshold and interaction modeling (bmi/lipids) C. WORKPLAN Eva will aggregate the data and draft tables to be circulated before July 9th. Detailled workplan below. The intention is to have a draft ready for discussion at the next OBELIX meeting taking place in Belgium 22‐23.9.2010. 28.5.2010 jpb
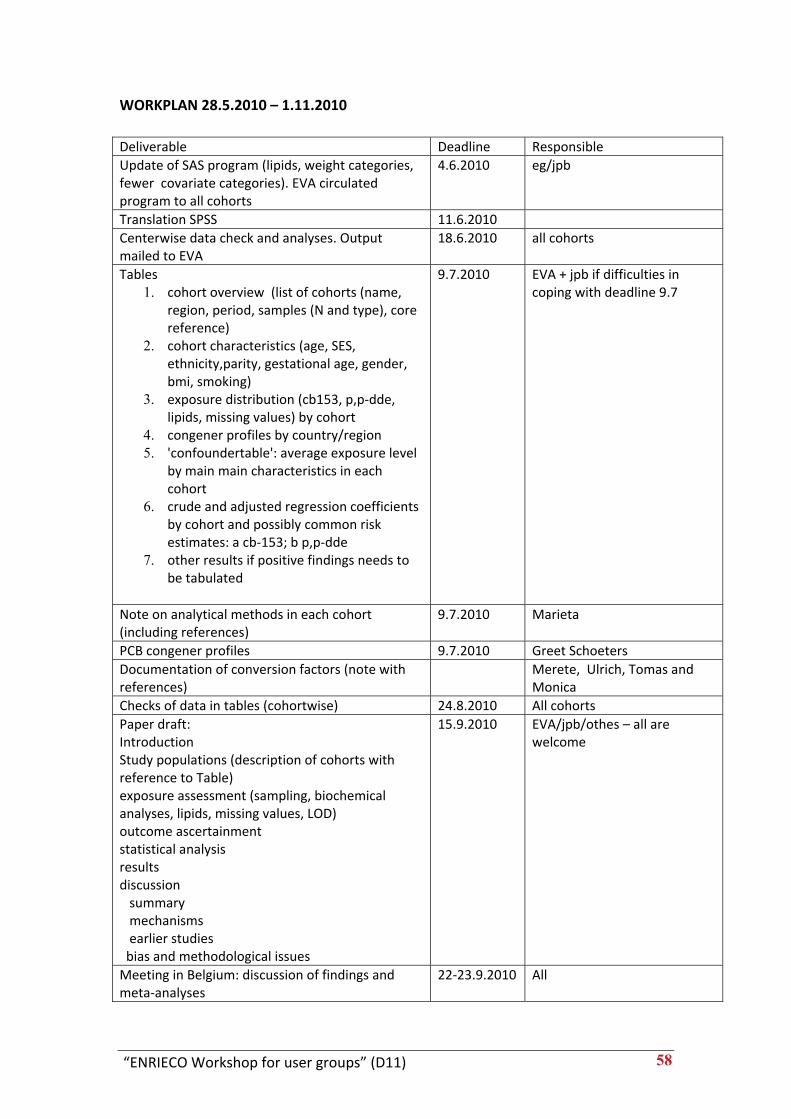
“ENRIECO Workshop for user groups” (D11) 58
WORKPLAN 28.5.2010 – 1.11.2010
Deliverable Deadline Responsible Update of SAS program (lipids, weight categories, fewer covariate categories). EVA circulated program to all cohorts
4.6.2010 eg/jpb
Translation SPSS 11.6.2010 Centerwise data check and analyses. Output mailed to EVA
18.6.2010 all cohorts
Tables 1. cohort overview (list of cohorts (name,
region, period, samples (N and type), core reference)
2. cohort characteristics (age, SES, ethnicity,parity, gestational age, gender, bmi, smoking)
3. exposure distribution (cb153, p,p‐dde, lipids, missing values) by cohort
4. congener profiles by country/region 5. 'confoundertable': average exposure level
by main main characteristics in each cohort
6. crude and adjusted regression coefficients by cohort and possibly common risk estimates: a cb‐153; b p,p‐dde
7. other results if positive findings needs to be tabulated
9.7.2010 EVA + jpb if difficulties in coping with deadline 9.7
Note on analytical methods in each cohort (including references)
9.7.2010 Marieta
PCB congener profiles 9.7.2010 Greet Schoeters Documentation of conversion factors (note with references)
Merete, Ulrich, Tomas and Monica
Checks of data in tables (cohortwise) 24.8.2010 All cohorts Paper draft: Introduction Study populations (description of cohorts with reference to Table) exposure assessment (sampling, biochemical analyses, lipids, missing values, LOD) outcome ascertainment statistical analysis results discussion summary mechanisms earlier studies bias and methodological issues
15.9.2010 EVA/jpb/othes – all are welcome
Meeting in Belgium: discussion of findings and meta‐analyses
22‐23.9.2010 All

“ENRIECO Workshop for user groups” (D11) 59
Annex
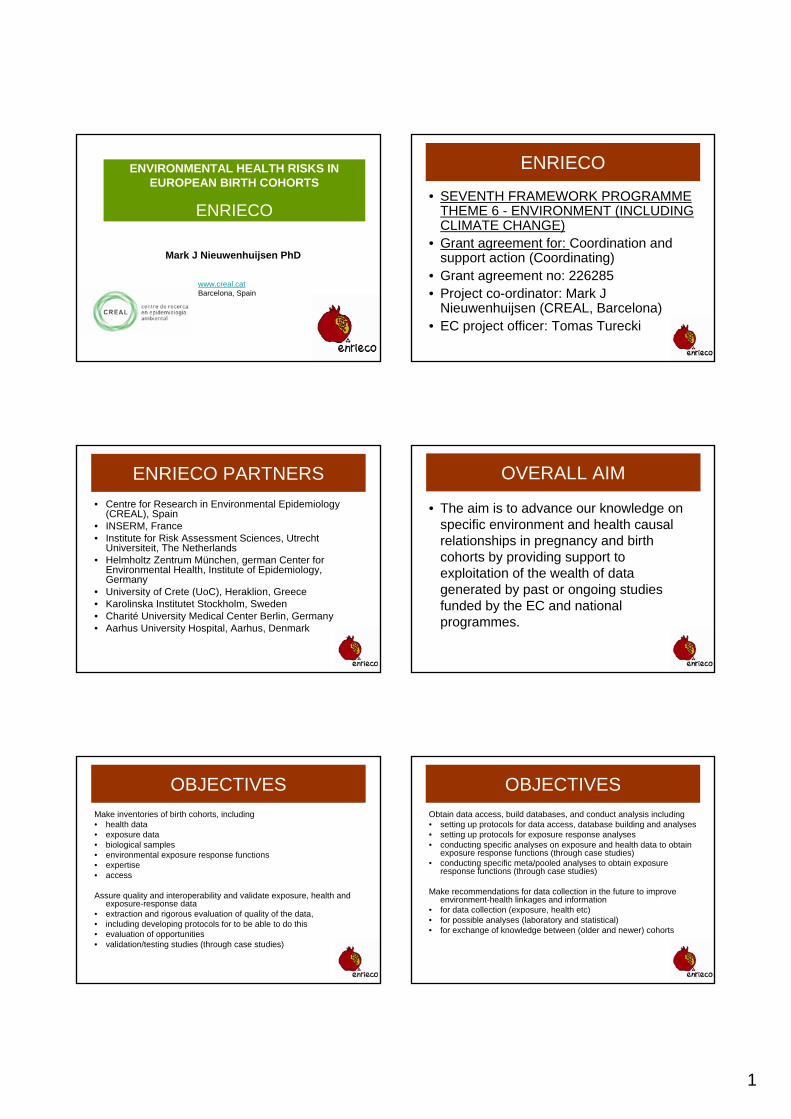
1
Mark J Nieuwenhuijsen PhD
www.creal.catBarcelona, Spain
ENVIRONMENTAL HEALTH RISKS IN EUROPEAN BIRTH COHORTS
ENRIECO
ENRIECO
• SEVENTH FRAMEWORK PROGRAMME THEME 6 - ENVIRONMENT (INCLUDING CLIMATE CHANGE)
• Grant agreement for: Coordination and support action (Coordinating)
• Grant agreement no: 226285• Project co-ordinator: Mark J
Nieuwenhuijsen (CREAL, Barcelona)• EC project officer: Tomas Turecki
ENRIECO PARTNERS• Centre for Research in Environmental Epidemiology
(CREAL), Spain• INSERM, France• Institute for Risk Assessment Sciences, Utrecht
Universiteit, The Netherlands• Helmholtz Zentrum München, german Center for
Environmental Health, Institute of Epidemiology, Germany
• University of Crete (UoC), Heraklion, Greece• Karolinska Institutet Stockholm, Sweden• Charité University Medical Center Berlin, Germany• Aarhus University Hospital, Aarhus, Denmark
OVERALL AIM
• The aim is to advance our knowledge on specific environment and health causal relationships in pregnancy and birth cohorts by providing support to exploitation of the wealth of data generated by past or ongoing studies funded by the EC and national programmes.
OBJECTIVESMake inventories of birth cohorts, including• health data• exposure data• biological samples• environmental exposure response functions• expertise• access
Assure quality and interoperability and validate exposure, health and exposure-response data
• extraction and rigorous evaluation of quality of the data, • including developing protocols for to be able to do this• evaluation of opportunities• validation/testing studies (through case studies)
OBJECTIVESObtain data access, build databases, and conduct analysis including• setting up protocols for data access, database building and analyses• setting up protocols for exposure response analyses• conducting specific analyses on exposure and health data to obtain
exposure response functions (through case studies)• conducting specific meta/pooled analyses to obtain exposure
response functions (through case studies)
Make recommendations for data collection in the future to improve environment-health linkages and information
• for data collection (exposure, health etc)• for possible analyses (laboratory and statistical)• for exchange of knowledge between (older and newer) cohorts
2
OBJECTIVESDisseminate information through• project website• virtual network• workshop(s)• easy accessible info (e.g. for policy makers etc)• database with exposure response functions
WP 1 Inventory of birth cohorts. (WP leader: Martine Vrijheid, CREAL)
• A comprehensive inventory will be made of all existing pregnancy and birth cohorts in Europe that have data which can be used to explore environment and health relationships
• The information will be stored in a searchable database on the internet
INMA – Sabadell, Valencia, Asturias, Gipuzkoa, Granada,
Menorca, Ribera d’EbreGeneration XXI –Portugal
EDEN – Poitiers and NantesPELAGIE – Bretagne
ELFE - France
ALSPAC – Avon region
BIB – Bradford
ABCD – Amsterdam
Generation R – Rotterdam
Koala – Netherlands
PIAMA – Netherlands
FLESH – Belgium
DUISBERG – DuisbergGINI-B – Munich, Wesel
LISA – MunichMAS – Berlin, Dusseldorf,Freiburg, Mainz, Munich
Co.N.ER – BolognaGESP II – RomeNINFEA – Turin
Faroes Islands I-III
DNBC – DenmarkINUENDO– Greenland,Scandinavia,Poland,
Ukraine
HUMIS – Norway
MoBa – Oslo
BAMSE – StockolmNFBC 1986/87 – Oulu
LUKAS – Kuopio
KANC – Kaunas
PCB – Slovakia
APREG – Gyor
RHEA - Heraklion
WP 2 Evaluation of exposures (WP leader Ulrike Gehring/Bert Brunekreef, UU)
• Existing environmental exposure information, methods and tools, of the cohorts will be evaluated, and recommendations for further analyses will be made
• Will develop protocols for the evaluation of such information
• The work will be divided in a number of exposure themes though working groups
• Case study on occupational exposures
WP 3 Evaluation of health outcomes (WP leader Remy Slama, INSERM)
• Existing health information, methods and tools, of the cohorts will be evaluated, and recommendations for further analyses will be made
• Will develop protocols for the evaluation of such information
• The work will be divided in a number of health outcome themes though working groups
• Case study on POPs and birth weight
WP 4 Evaluation of exposure-response relationships
(WP leader Joachim Heinrich, HMGU)
• Existing environmental exposure response information, methods and tools, of the cohorts will be evaluated, and recommendations for further analyses will be made
• Focus will be on exposure response functions that have been peer reviewed for scientific journals (in press or published).
• Will develop protocols for the evaluation of such information
• The work will be divided in a number of exposure response themes though working groups
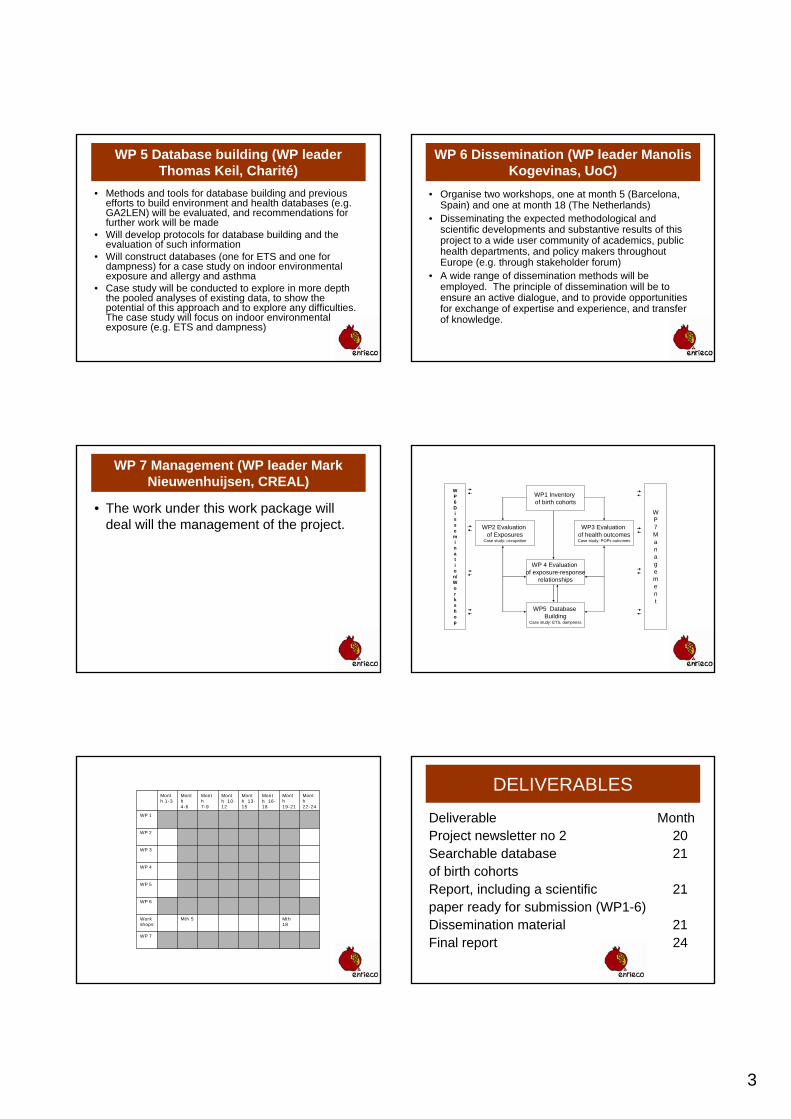
3
WP 5 Database building (WP leader Thomas Keil, Charité)
• Methods and tools for database building and previous efforts to build environment and health databases (e.g. GA2LEN) will be evaluated, and recommendations for further work will be made
• Will develop protocols for database building and the evaluation of such information
• Will construct databases (one for ETS and one for dampness) for a case study on indoor environmental exposure and allergy and asthma
• Case study will be conducted to explore in more depth the pooled analyses of existing data, to show the potential of this approach and to explore any difficulties. The case study will focus on indoor environmental exposure (e.g. ETS and dampness)
WP 6 Dissemination (WP leader Manolis Kogevinas, UoC)
• Organise two workshops, one at month 5 (Barcelona, Spain) and one at month 18 (The Netherlands)
• Disseminating the expected methodological and scientific developments and substantive results of this project to a wide user community of academics, public health departments, and policy makers throughout Europe (e.g. through stakeholder forum)
• A wide range of dissemination methods will be employed. The principle of dissemination will be to ensure an active dialogue, and to provide opportunities for exchange of expertise and experience, and transfer of knowledge.
WP 7 Management (WP leader Mark Nieuwenhuijsen, CREAL)
• The work under this work package will deal will the management of the project.
WP1 Inventoryof birth cohorts
WP2 Evaluationof Exposures
Case study: occupation
WP3 Evaluationof health outcomesCase study: POPs outcomes
WP5 DatabaseBuilding
Case study: ETS, dampness
WP 4 Evaluationof exposure-response
relationships
WP7Management
WP6Dissemination/Workshop
WP 7
Mth18
Mth 5Workshops
WP 6
WP 5
WP 4
WP 3
WP 2
WP 1
Month 22-24
Month 19-21
Month 16-18
Month 13-15
Month 10-12
Month 7-9
Month 4-6
Month 1-3
DELIVERABLES
Deliverable MonthProject newsletter no 2 20Searchable database 21of birth cohortsReport, including a scientific 21paper ready for submission (WP1-6) Dissemination material 21Final report 24
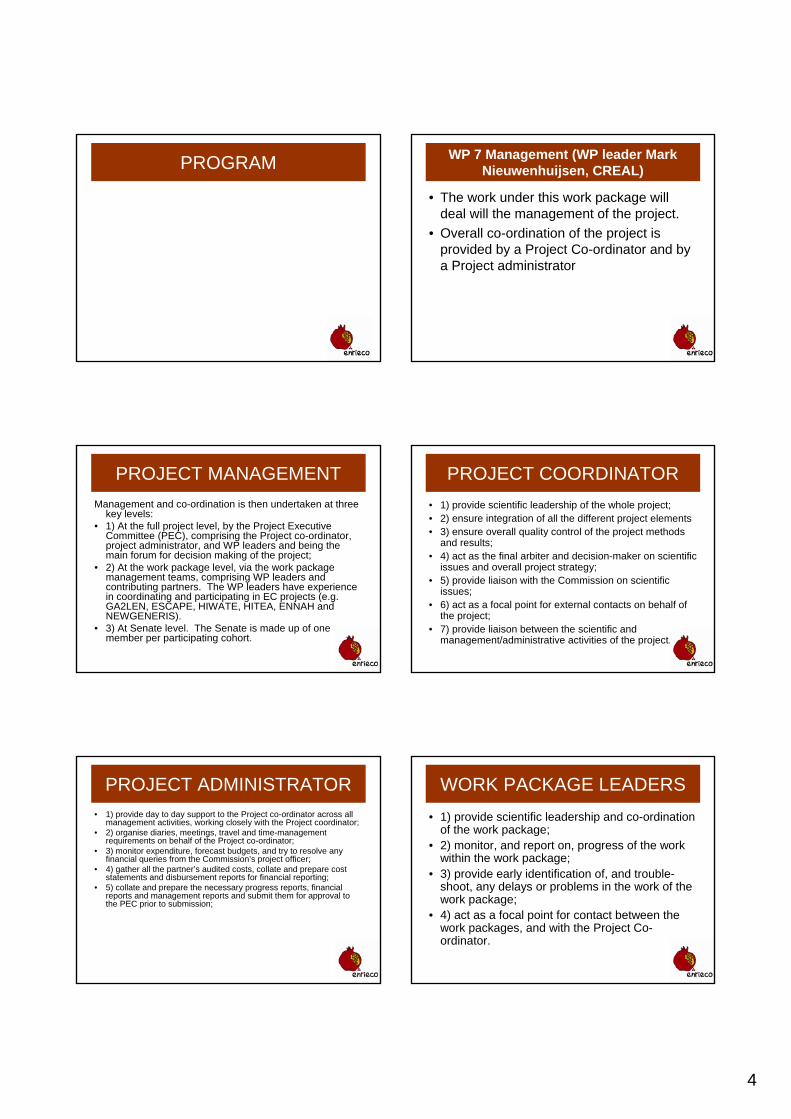
4
PROGRAM WP 7 Management (WP leader Mark Nieuwenhuijsen, CREAL)
• The work under this work package will deal will the management of the project.
• Overall co-ordination of the project is provided by a Project Co-ordinator and by a Project administrator
PROJECT MANAGEMENTManagement and co-ordination is then undertaken at three
key levels: • 1) At the full project level, by the Project Executive
Committee (PEC), comprising the Project co-ordinator, project administrator, and WP leaders and being the main forum for decision making of the project;
• 2) At the work package level, via the work package management teams, comprising WP leaders and contributing partners. The WP leaders have experience in coordinating and participating in EC projects (e.g. GA2LEN, ESCAPE, HIWATE, HITEA, ENNAH and NEWGENERIS).
• 3) At Senate level. The Senate is made up of one member per participating cohort.
PROJECT COORDINATOR• 1) provide scientific leadership of the whole project; • 2) ensure integration of all the different project elements • 3) ensure overall quality control of the project methods
and results; • 4) act as the final arbiter and decision-maker on scientific
issues and overall project strategy; • 5) provide liaison with the Commission on scientific
issues; • 6) act as a focal point for external contacts on behalf of
the project; • 7) provide liaison between the scientific and
management/administrative activities of the project.
PROJECT ADMINISTRATOR• 1) provide day to day support to the Project co-ordinator across all
management activities, working closely with the Project coordinator; • 2) organise diaries, meetings, travel and time-management
requirements on behalf of the Project co-ordinator; • 3) monitor expenditure, forecast budgets, and try to resolve any
financial queries from the Commission’s project officer; • 4) gather all the partner’s audited costs, collate and prepare cost
statements and disbursement reports for financial reporting; • 5) collate and prepare the necessary progress reports, financial
reports and management reports and submit them for approval to the PEC prior to submission;
WORK PACKAGE LEADERS• 1) provide scientific leadership and co-ordination
of the work package; • 2) monitor, and report on, progress of the work
within the work package; • 3) provide early identification of, and trouble-
shoot, any delays or problems in the work of the work package;
• 4) act as a focal point for contact between the work packages, and with the Project Co-ordinator.
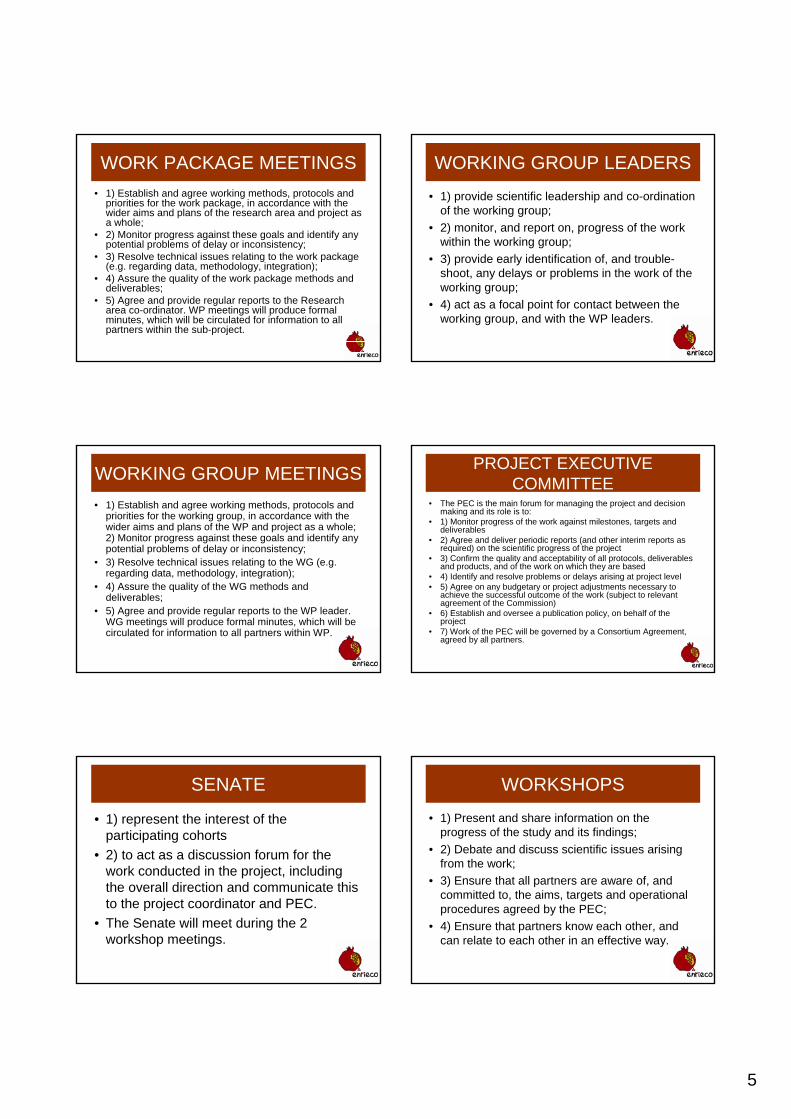
5
WORK PACKAGE MEETINGS• 1) Establish and agree working methods, protocols and
priorities for the work package, in accordance with the wider aims and plans of the research area and project as a whole;
• 2) Monitor progress against these goals and identify any potential problems of delay or inconsistency;
• 3) Resolve technical issues relating to the work package (e.g. regarding data, methodology, integration);
• 4) Assure the quality of the work package methods and deliverables;
• 5) Agree and provide regular reports to the Research area co-ordinator. WP meetings will produce formal minutes, which will be circulated for information to all partners within the sub-project.
WORKING GROUP LEADERS
• 1) provide scientific leadership and co-ordination of the working group;
• 2) monitor, and report on, progress of the work within the working group;
• 3) provide early identification of, and trouble-shoot, any delays or problems in the work of the working group;
• 4) act as a focal point for contact between the working group, and with the WP leaders.
WORKING GROUP MEETINGS• 1) Establish and agree working methods, protocols and
priorities for the working group, in accordance with the wider aims and plans of the WP and project as a whole; 2) Monitor progress against these goals and identify any potential problems of delay or inconsistency;
• 3) Resolve technical issues relating to the WG (e.g. regarding data, methodology, integration);
• 4) Assure the quality of the WG methods and deliverables;
• 5) Agree and provide regular reports to the WP leader. WG meetings will produce formal minutes, which will be circulated for information to all partners within WP.
PROJECT EXECUTIVE COMMITTEE
• The PEC is the main forum for managing the project and decision making and its role is to:
• 1) Monitor progress of the work against milestones, targets and deliverables
• 2) Agree and deliver periodic reports (and other interim reports as required) on the scientific progress of the project
• 3) Confirm the quality and acceptability of all protocols, deliverables and products, and of the work on which they are based
• 4) Identify and resolve problems or delays arising at project level • 5) Agree on any budgetary or project adjustments necessary to
achieve the successful outcome of the work (subject to relevant agreement of the Commission)
• 6) Establish and oversee a publication policy, on behalf of the project
• 7) Work of the PEC will be governed by a Consortium Agreement, agreed by all partners.
SENATE
• 1) represent the interest of the participating cohorts
• 2) to act as a discussion forum for the work conducted in the project, including the overall direction and communicate this to the project coordinator and PEC.
• The Senate will meet during the 2 workshop meetings.
WORKSHOPS
• 1) Present and share information on the progress of the study and its findings;
• 2) Debate and discuss scientific issues arising from the work;
• 3) Ensure that all partners are aware of, and committed to, the aims, targets and operational procedures agreed by the PEC;
• 4) Ensure that partners know each other, and can relate to each other in an effective way.
6
FURTHER CONTACT
• Electronic mail• Telephone conferencing• Meeting at major conferences
PROGRESS REPORTS• Internal progress reports will be required for each work
package on a regular (3 monthly) basis. • These will be delivered using a standard reporting
format, based on procedures already successfully used by the Project co-ordinator and Project administrator
• These reports are designed to provide information on targets, actions taken to achieve them, any problems that might have been encountered, and implications both for the specific partner/work package and for others.
• WP reports will be submitted to the Project Co-ordinator during the first week of each quarter. Reports will be collated and synthesised as appropriate for meetings, and will be archived to provide a record of progress on the project.
PERIODIC REPORTS• First year and second year periodic reports and final
reports, detailing both scientific progress and financial aspects, will be provided to the Commission as required.
• Draft reports will be compiled by the Project Co-ordinator and Project Administrator, based on materials provided by partners.
• Scientific materials for these reports will be channelled through the WP leader, who will be responsible for ensuring the completeness and consistency of the materials provided.
• Financial materials will be collated directly from partners by the Project Administrator.
• Reports will be considered and agreed, prior to submission, by the PEC.
WORK PLANS• Work plans will be developed and maintained at all levels of the
project, and will provide the template against which progress ismonitored.
• At the project level, the work plan will be defined by the overall Description of Work, as agreed with the Commission, and as updated or refined in the light of annual reports or interim reviews. This work plan will be agreed and reviewed at each PEC meeting.
• At WP level, more detailed plans will be compiled, and monitored. Work package plans will provide the detailed descriptions of theproposed work. They will incorporate protocols and methodological documents, as these emerge, and will be maintained to provide a clear record of the progress of the work. They will thus also provide a reference source for preparation of the final reports, and for any subsequent publications.
Project Coordinator
Project ExecutiveCommittee (PEC)
WP 1 WP 2
WP7
MANAGEMENT
WP 3 WP 4 WP 5 WP 6
WGs WGs WGs
Workshops
PEC meetings
WP meetings
WG meetings
WP = work package, WG = working group
Senate
1
Environmental Health Risks Environmental Health Risks in European Birth Cohortsin European Birth Cohorts
-- ENRIECO ENRIECO --
Welcome at the ENRIECO Project Meeting 26‐28th May 2010
Environmental Health Environmental Health Risks in European Risks in European Birth CohortsBirth Cohorts
Diana van Gent
ENRIECO Project Meeting26-28th May 2010
ENRIECOENRIECO
Meeting Logistics
- Evaluation procedure
- Meeting spaces
- Dinner arrangements
- Minutes
- WIFI
ENRIECOENRIECO
Management update
- Periodic report
- EC Officer
- Submission of Deliverables
- Quarterly reports
- WP composition changes
- Project plan year 2
ENRIECOENRIECO ENRIECOENRIECO
Nov 201021WP6D21 Dissemination material
Feb 201124WP7D22 Periodic report 2
Feb 201124WP7D23 Final report
Nov 201021WP3D18 Report for POPs related outcomes in EU birthcohorts
Nov 201021WP4D19 Report with evaluation of environmental exposureresponse information and recommendations in EU birth cohorts
Nov 201021WP5D20 Report on exposure-response relationships for thecase studies on indoor exposures and allergy andasthma
Nov 201021WP1D14 Report with inventory of EU birth cohorts onenvironment and health
Nov 201021WP3D17 Report with evaluation of health information andrecommendations in EU birth cohorts
Nov 201021WP2D16 Report of methods and approaches of evaluatingoccupational exposures in EU birth cohorts
Nov 201021WP2D15 Report with evaluation of environmentalinformation and recommendations
Nov 201021WP1D13 Searchable database of birth cohorts
Oct 201020WP6D12 Newsletter no 2
Aug 201018WP6D11 Workshop
ActualMonthResponsibleDeliverables Year 2
2
ENRIECOENRIECO
1
ENRIECO. WP6 Dissemination package
Maria Vassilaki and Manolis KogevinasUniversity of Crete
ENRIECO Newsletter No.1, December 2009 (Deliverable 9)
Presenting• Enrieco Working Groups
and Case Studies
• Participating Birth Cohorts
• Exposures Ascertained by the EnriecoParticipating Birth Cohorts
An ENRIECO dissemination message was published at
The Parliament Magazine on February 22, 2010 (Issue 302) & March 8, 2010 (Issue 303), intending to reach policy makers and
introduce them to Enrieco’s objectives, current work and goals.
NewGeneris 4th Annual Consortium Meeting, February 3‐4, 2010, University of Crete,
Heraklion, Crete, Greece
Third International Childhood Cancer Cohort Consortium (I4C) Workshop, International Agency for Research on Cancer, Lyon, France ‐November 16‐17, 2009
Website ‐Members login area1. login!
2. Go to coordination!
3. Choose a WP
Website ‐Members login area4. Choose a WG
5. Download a file to read!
2
Fifth Ministerial Conference on Environment and Health, Parma Italy
Symposium: Children's health and the environment: How does current European research respond to public
health priorities?11 March 2010, 18:00 – 19:30
Symposium co‐organised by DG Research, EuropeanCommission and the International Society for
Environmental Epidemiology–ISEE
How can we ensure thatEnrieco conclusions and
reports are disseminated and have an effect in EU research policy and in health policy?
Enrieco Dissemination: the future
• Extremely important that our reports are “readable” and with clear messages
Enrieco Dissemination: the future• Construction of lists of potentially interested persons (stakeholdres) including NGOs, EU parliament MPs, EU officials, national officials and massive emailing
• Targeted in person contact with selected stakeholders
• Information via classical routes, ie journals. Request ISEE space in EHP and Epidemiology?
• Commitment by the large Environmental Epidemiology research groups in Europe to promote Enrieco conclusions
Enrieco Dissemination: the future
• IMPORTANT: No money for all this foreseen in Enrieco budget
1
WP 1 WP 1 -- InventoryInventory
Martine Vrijheid and Maribel CasasENRIECO 2nd Workshop26-28 May 2010
WP1WP1
AIMTo make an inventory of existing pregnancy and birth
cohorts in Europe that have data that can be used to explore environment and health relationships.
For use by:1. Researchers:
- more effective exploitation of existing data - planning future collaborations
2. Policy makers and other stakeholders: - identification of cohorts with relevant information on specific environmental exposures and outcomes
ProgressProgressData collection
• Questionnaire finalised July 2009
• Data collection from cohorts July-Dec 2009
• Ongoing checks, new cohorts Jan 2010 - now
Access database with questionnaire information for WGs• Version 1 sent to WGs Dec 2009
• Version 2 sent to WGs April 2010
Web database – simplified version
• Under design March 2010 - July 2010
ScopeScope ofof inventoryinventory
A. Basic protocol details Update of birthcohorts.net
B. Environmental ExposuresWhich, when, in who, how (basic) ?
C. Health OutcomesWhich, when, in who, how (basic) ?
D. Other (diet, SES, genotyping, other important variables)
Yes (+timing) / No
⇒ Inventory questionnaire
WhichWhich cohorts?cohorts?
The main focus on cohorts that: 1. Collect data on at least one environmental
exposure topic;2. Start enrolment during pregnancy or at birth (or
during first year of life if data on birth outcomes is collected from medical records);
3. Have at least one follow-up point after birth;4. Include at least 200-300 mother-child pairs.
Cohorts that do not fit these criteria entirely can be included on request in the web database, but treated separately in the descriptive publication (to discuss, e.g. historical cohorts pre1980, no follow-up points after birth…)
Faroe Islands
Generation XXI
INMA
EDEN
EFESE/ELFE
PÉLAGIE
ALSPAC
BiB
ABCD
Generation R
KOALA
PIAMA
HUMIS
MoBaBAMSE
Inuendo LUKAS
KAUNAS
REPRO_PL
Inuendo
PCB cohort
APREG-Gyor
RHEACONER
GESPII
NINFEA
DUISBURG
GINI-B
LISA
MAS
SNiP
FLEHS
DNBC
Aarhus
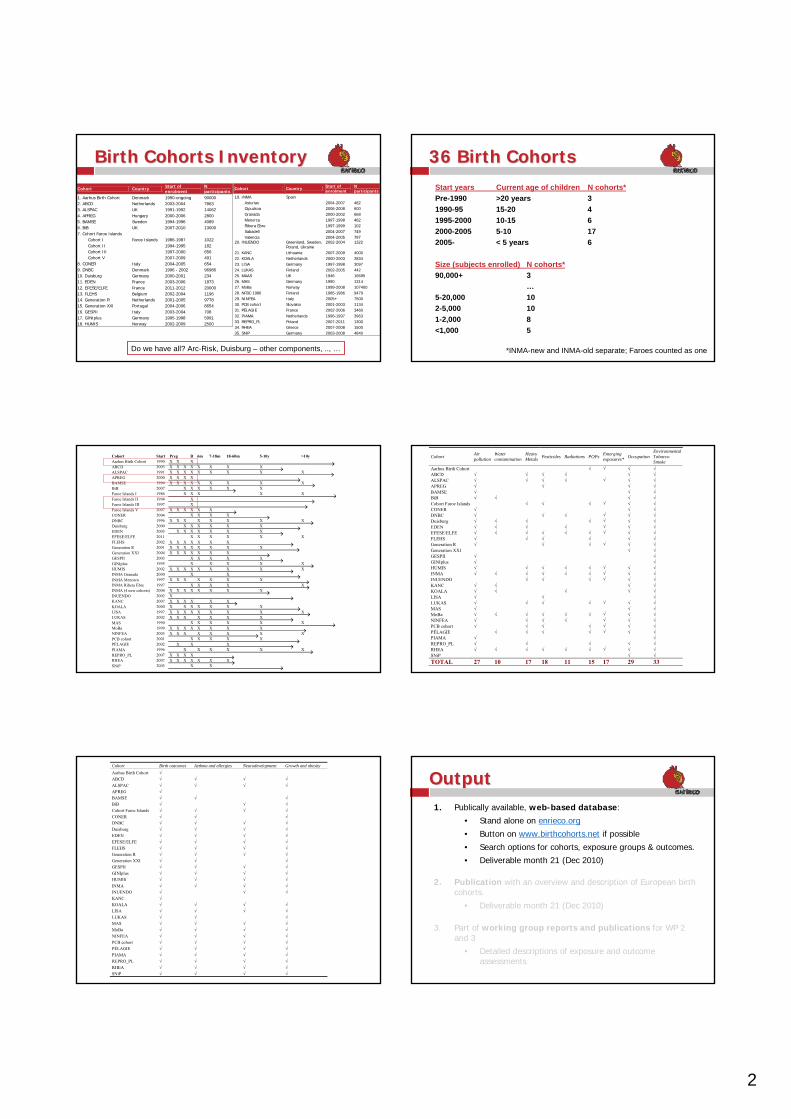
2
Cohort Country Start of enrolment
N participants
1. Aarhus Birth Cohort Denmark 1990-ongoing 90000 2. ABCD Netherlands 2003-2004 7863 3. ALSPAC UK 1991-1992 14062 4. APREG Hungary 2000-2006 2800 5. BAMSE Sweden 1994-1996 4089 6. BiB UK 2007-2010 13000 7. Cohort Faroe Islands Cohort I Faroe Islands 1986-1987 1022 Cohort II 1994-1995 182 Cohort III 1997-2000 656 Cohort V 2007-2009 491 8. CONER Italy 2004-2005 654 9. DNBC Denmark 1996 - 2002 96986 10. Duisburg Germany 2000-2001 234 11. EDEN France 2003-2006 1873 12. EFESE/ELFE France 2011-2012 20000 13. FLEHS Belgium 2002-2004 1196 14. Generation R Netherlands 2001-2005 9778 15. Generation XXI Portugal 2004-2006 8654 16. GESPII Italy 2003-2004 708 17. GINIplus Germany 1995-1998 5991 18. HUMIS Norway 2002-2009 2500
BirthBirth Cohorts Cohorts InventoryInventory
Do we have all? Arc-Risk, Duisburg – other components, .., …
Cohort Country Start of enrolment
N participants
19. INMA Spain Asturias 2004-2007 482 Gipuzkoa 2006-2008 600 Granada 2000-2002 668 Menorca 1997-1998 482 Ribera Ebre 1997-1999 102 Sabadell 2004-2007 749 Valencia 2004-2005 787 20. INUENDO Greenland, Sweden,
Poland, Ukraine 2002-2004 1322
21. KANC Lithuania 2007-2009 4000 22. KOALA Netherlands 2000-2003 2834 23. LISA Germany 1997-1998 3097 24. LUKAS Finland 2002-2005 442 25. MAAS UK 1946 16695 26. MAS Germany 1990 1314 27. MoBa Norway 1999-2008 107400 28. NFBC 1986 Finland 1985-1986 9479 29. NINFEA Italy 2005+ 7500 30. PCB cohort Slovakia 2001-2003 1134 31. PÉLAGIE France 2002-2006 3460 32. PIAMA Netherlands 1996-1997 3963 33. REPRO_PL Poland 2007-2011 1300 34. RHEA Greece 2007-2008 1500 35. SNiP Germany 2003-2008 4840
36 36 BirthBirth CohortsCohortsStart years Current age of children N cohorts*Pre-1990 >20 years 31990-95 15-20 41995-2000 10-15 62000-2005 5-10 172005- < 5 years 6
Size (subjects enrolled) N cohorts*90,000+ 3
…5-20,000 102-5,000 101-2,000 8<1,000 5
*INMA-new and INMA-old separate; Faroes counted as one
Cohort Start B 6m 7-18m 18-60m 5-10y >10yAarhus Birth Cohort 1990 X X XABCD 2003 X X X X X X X XALSPAC 1991 X X X X X X X X XAPREG 2000 X X X XBAMSE 1994 X X X X X X X X XBiB 2007 X X X X X XFaroe Islands I 1986 X X X X XFaroe Islands II 1994 XFaroe Islands III 1997 XFaroe Islands V 2007 X X X X X XCONER 2004 X X X XDNBC 1996 X X X X X X X XDuisburg 2000 X X X X X XEDEN 2003 X X X X X X XEFESE/ELFE 2011 X X X X X XFLEHS 2002 X X X X X X XGeneration R 2001 X X X X X X X XGeneration XXI 2004 X X X X X X XGESPII 2003 X X X X XGINIplus 1995 X X X X XHUMIS 2002 X X X X X X X X XINMA Granada 2000 X XINMA Menorca 1997 X X X X X X XINMA Ribera Ebre 1997 X X X X XINMA (4 new cohorts) 2004 X X X X X X X XINUENDO 2002 XKANC 2007 X X X X X XKOALA 2000 X X X X X X XLISA 1997 X X X X X X X X XLUKAS 2002 X X X X X X XMAS 1990 X X X X X XMoBa 1999 X X X X X X X XNINFEA 2005 X X X X X X X XPCB cohort 2001 X X X X XPÉLAGIE 2002 X X XPIAMA 1996 X X X X X XREPRO_PL 2007 X X X XRHEA 2007 X X X X X X XSNiP 2003 X X
Preg Cohort Air pollution
Water contamination
Heavy Metals Pesticides Radiations POPs Emerging
exposures* Occupation Environmental Tobacco Smoke
Aarhus Birth Cohort √ √ √ √ ABCD √ √ √ √ √ √ ALSPAC √ √ √ √ √ √ √ APREG √ √ √ √ BAMSE √ √ √ BiB √ √ √ √ Cohort Faroe Islands √ √ √ √ √ √ CONER √ √ √ DNBC √ √ √ √ √ √ Duisburg √ √ √ √ √ √ √ EDEN √ √ √ √ √ √ √ EFESE/ELFE √ √ √ √ √ √ √ √ √ FLEHS √ √ √ √ √ √ Generation R √ √ √ √ √ √ Generation XXI √ √ GESPII √ √ GINIplus √ √ HUMIS √ √ √ √ √ √ √ √ INMA √ √ √ √ √ √ √ √ √ INUENDO √ √ √ √ √ √ KANC √ √ √ √ KOALA √ √ √ √ √ LISA √ √ √ LUKAS √ √ √ √ √ √ √ MAS √ √ √ MoBa √ √ √ √ √ √ √ √ √ NINFEA √ √ √ √ √ √ √ PCB cohort √ √ √ √ √ √ √ PÉLAGIE √ √ √ √ √ √ √ PIAMA √ √ REPRO_PL √ √ √ √ √ RHEA √ √ √ √ √ √ √ √ √ SNiP √ √ TOTAL 27 10 17 18 11 15 17 29 33
Cohort Birth outcomes Asthma and allergies Neurodevelopment Growth and obesity Aarhus Birth Cohort √ ABCD √ √ √ √ ALSPAC √ √ √ √ APREG √ BAMSE √ √ √ BiB √ √ √ Cohort Faroe Islands √ √ √ √ CONER √ √ √ DNBC √ √ √ √ Duisburg √ √ √ √ EDEN √ √ √ √ EFESE/ELFE √ √ √ √ FLEHS √ √ √ √ Generation R √ √ √ √ Generation XXI √ √ √ GESPII √ √ √ √ GINIplus √ √ √ √ HUMIS √ √ √ √ INMA √ √ √ √ INUENDO √ √ √ KANC √ KOALA √ √ √ √ LISA √ √ √ √ LUKAS √ √ √ MAS √ √ √ √ MoBa √ √ √ √ NINFEA √ √ √ √ PCB cohort √ √ √ √ PÉLAGIE √ √ √ √ PIAMA √ √ √ √ REPRO_PL √ √ √ √ RHEA √ √ √ √ SNiP √ √ √ √
OutputOutput1. Publically available, web-based database:
• Stand alone on enrieco.org
• Button on www.birthcohorts.net if possible
• Search options for cohorts, exposure groups & outcomes.
• Deliverable month 21 (Dec 2010)
2. Publication with an overview and description of European birth cohorts.
• Deliverable month 21 (Dec 2010)
3. Part of working group reports and publications for WP 2 and 3
• Detailed descriptions of exposure and outcome assessments
3
OutputOutput1. Publically available, web-based database:
• Stand alone on enrieco.org
• Button on www.birthcohorts.net if possible
• Search options for cohorts, exposure groups & outcomes.
• Deliverable month 21 (Dec 2010)
2. Publication with an overview and description of European birth cohorts.
• Deliverable month 21 (Dec 2010)
3. Part of all working group reports and publications for WP 2 and 3
• Detailed descriptions of exposure and outcome assessments
4
PublicationPublication WP1WP1
“An Inventory/Overview of European Birth Cohort Studies with Environmental Exposure Data”
Content: descriptive- map- figure with protocol time line- table with basic details (timing, N subjects, etc)- table with biosamples collected and when
- table with exposures assessed (or with WP2 overview)- table with outcomes assessed (or with WP3 overview)
Authors: 1 representative from each cohort?
WhatWhat nextnext??By December 2010:
Further checks before data is made available publically
Final web database
Publication WP1
? Update basic protocol available on birthcohorts.net ? With permission from cohorts we could make sure that basic data on ENRIECO and birthcohorts.net databases are same…
WhatWhat nextnext??
After ENRIECO:
1. Maintenance and updates?- every 2 years: email to ask for checking and updating?
- CREAL responsible for maintenance and updates?
- commitment from cohorts needed!
2. Expansion as part of CHICOS- other risk factors
Is it useful?
“Developing a Child Cohort Strategy for Europe”
Funded by FP 7 HEALTH-2009-3.3-4
Coordination Action : 1 Jan 2010 – 31 Dec 2012
Coordinator: Martine Vrijheid – CREAL
Partners: Bristol, UK - Debbie Lawlor, Particia LucasDenmark - Anne-Marie Nybo AndersenNetherlands - Vincent Jaddoe, Hein RaatSpain - Jordi Sunyer, Mark NieuwenhuijsenNorway - Camilla Stoltenberg, Per MagnusItaly - Franco Merletti, Lorenzo RichardiGreece - Manolis Kogevinas, Leda Chatzi
www.chicosproject.eu
Background
WhyWhy should birth cohorts work together?1. Improving causal inference
• replication, comparison, pooling of data
2. Understanding inequalities• contrast needed in prevalence of disease, risk factors, and policies
3. Coordinated response to important policy questions• E.g. flu vaccine for pregnant women?
4. Greater and more efficient use of cohorts• Shared expertise
HowHow should birth cohorts work together?Towards a long-term infrastructure for birth cohort research in Europe…- Basis: existing birth cohorts- Continued coordination - Continued support for existing cohorts
5
Aims
AimTo develop an integrated strategy for mother-child cohort research in Europe.
Objectives• To update/extend the cohort inventory (birthcohorts.net and
ENRIECO)• To evaluate existing information from cohorts on child health
outcomes and determinants• To develop recommendations for research action in key
areas of policy concern• To develop recommendations for improved contribution of
mother-child cohort research to policy at European level• To disseminate project findings to stakeholders
Approach
WP 1: Inventory
WP 2: Outcomes7 Working Groups
WP 3: Determinants6 Working Groups
WP 4: Policy
WP 5: Dissemination
WP 6: Management
Tasks:Tasks:- Review existing data- Review role of cohort research- Identify gaps
- Case studies (data pooling) to highlight specific issues
RecommendationsRecommendations :- Topic specific - Strategy for coordinated infrastructure
WP2 & 3 Working Groups
Outcome ThemesPerinatal outcomes Camilla StoltenbergAsthma, allergies Johan de JongsteObesity and metabolic health Debbie LawlorNeuro-cognition and behaviour Jordi SunyerAccidents and injuries Martine VrijheidInfectious diseases Camilla StoltenbergChildhood cancers Manolis Kogevinas
Determinant ThemesSocial/cultural inequalities Hein RaatNutrition and physical activity Leda ChatziLife-style exposures Per MagnusEnvironmental exposures Mark NieuwenhuijsenBiobanks and genetics Vincent JaddoeMultiple determinants Martine Vrijheid
Role of cohorts
- Participation in expanded inventory – e.g. data on diet, breastfeeding, physical activity, …
- Participation of experts in working groups
- Participation in case studies- E.g. ENRIECO continuation on occupational exposures, on
POPs and ND, etc??
- Participation in workshops- Next workshop: April 2011 in Barcelona
Participation in writing research strategy
Institute for Risk Assessment Sciences
ENRIECO WP 2
Evaluation of existing exposure information, methods & tools
Ulrike Gehring, IRAS, Utrecht University
May 26, 2010 Institute for Risk Assessment Sciences
Outline
• General overview of WP and status
• Presentations by 4 WGs
• Recommendations
• Publications
Institute for Risk Assessment Sciences
Objective
Evaluation of existing environmental and
occupational exposure information, methods
and tools of the ENRIECO cohorts
Institute for Risk Assessment Sciences
Specific aims
1. to develop protocols for the evaluation (available at www.enrieco.org)
2. to set up database(s) with the tools and methods that have been used
3. to make recommendations for potential further use of methods and tools
• statistical analyses
• laboratory analyses
Institute for Risk Assessment Sciences
Case study
To explore in more depth how to obtain and combine environmental exposures.
• Focus on occupational exposures of expecting women during pregnancy for pregnancy outcomes and events in later life
• Evaluation of methods available to quantify occupational exposure like job coding systems and databases on occupational exposure
• Cross-validation of different methods
• Recommendations for further use
Institute for Risk Assessment Sciences
Working groups
Topic WG leader
Air pollution Ulrike Gehring
Water contamination Mark Nieuwenhuijsen
Allergens & biological organisms Chih-Mei Chen/Joachim Heinrich
Heavy metals Jordi Sunyer
Pesticides Cecile Chevrier
Radiations: EMF/UV/ionising Martine Vrijheid
Smoking and ETS Magnus Wickman
Noise Thomas Keil
Persistent organic pollutants Gunnar Toft
Occupation Sylvaine Cordier
Emerging Exposures Martine Vrijheid
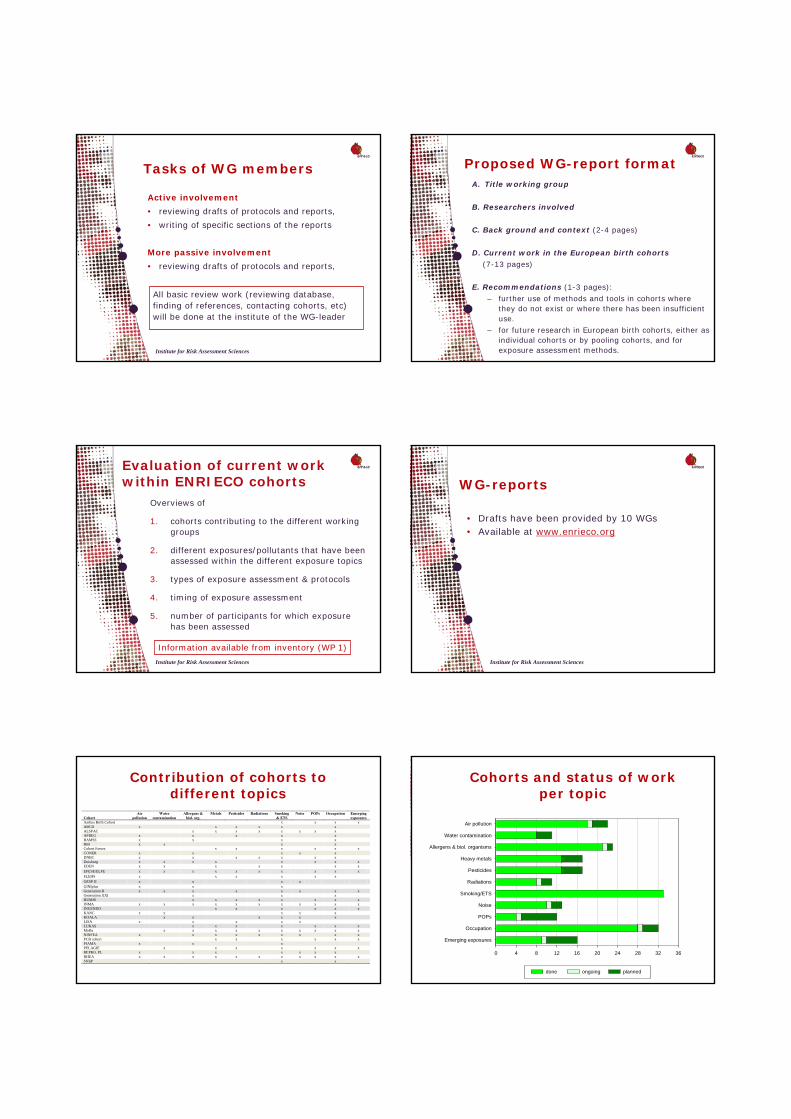
Institute for Risk Assessment Sciences
Tasks of WG members
Active involvement
• reviewing drafts of protocols and reports,
• writing of specific sections of the reports
More passive involvement
• reviewing drafts of protocols and reports,
All basic review work (reviewing database, finding of references, contacting cohorts, etc) will be done at the institute of the WG-leader
Institute for Risk Assessment Sciences
Proposed WG-report formatA. Title working group
B. Researchers involved
C. Back ground and context (2-4 pages)
D. Current work in the European birth cohorts(7-13 pages)
E. Recommendations (1-3 pages):
– further use of methods and tools in cohorts where they do not exist or where there has been insufficient use.
– for future research in European birth cohorts, either as individual cohorts or by pooling cohorts, and for exposure assessment methods.
Institute for Risk Assessment Sciences
Evaluation of current work within ENRIECO cohorts
Overviews of
1. cohorts contributing to the different working groups
2. different exposures/pollutants that have been assessed within the different exposure topics
3. types of exposure assessment & protocols
4. timing of exposure assessment
5. number of participants for which exposure has been assessed
Information available from inventory (WP 1)
Institute for Risk Assessment Sciences
WG-reports
• Drafts have been provided by 10 WGs• Available at www.enrieco.org
Institute for Risk Assessment Sciences
Contribution of cohorts to different topics
Cohort
Air pollution
Water contamination
Allergens & biol. org.
Metals Pesticides Radiations Smoking & ETS
Noise POPs Occupation Emerging exposures
Aarhus Birth Cohort x x x x ABCD x x x x x x ALSPAC x x x x x x x xAPREG x x x x x BAMSE x x x xBiB x x x xCohort Faroes x x x x x x CONER x x x x x DNBC x x x x x x x Duisburg x x x x x x x x EDEN x x x x x x x EFESE/ELFE x x x x x x x x x x FLEHS x x x x x x GESP II x x x x GINIplus x x x Generation R x x x x x x x xGeneration XXI x x x HUMIS x x x x x x x xINMA x x x x x x x x x x x INUENDO x x x x x x KANC x x x x xKOALA x x x x x xLISA x x x x x LUKAS x x x x x x xMoBa x x x x x x x x x x NINFEA x x x x x x x x xPCB cohort x x x x x x PIAMA x x x PELAGIE x x x x x x xREPRO_PL x x x x x x xRHEA x x x x x x x x x x x SNIiP x x
Institute for Risk Assessment Sciences
Cohorts and status of workper topic
0 4 8 12 16 20 24 28 32 36
Emerging exposures
Occupation
POPs
Noise
Smoking/ETS
Radiations
Pesticides
Heavy metals
Allergens & biol. organisms
Water contamination
Air pollution
done ongoing planned
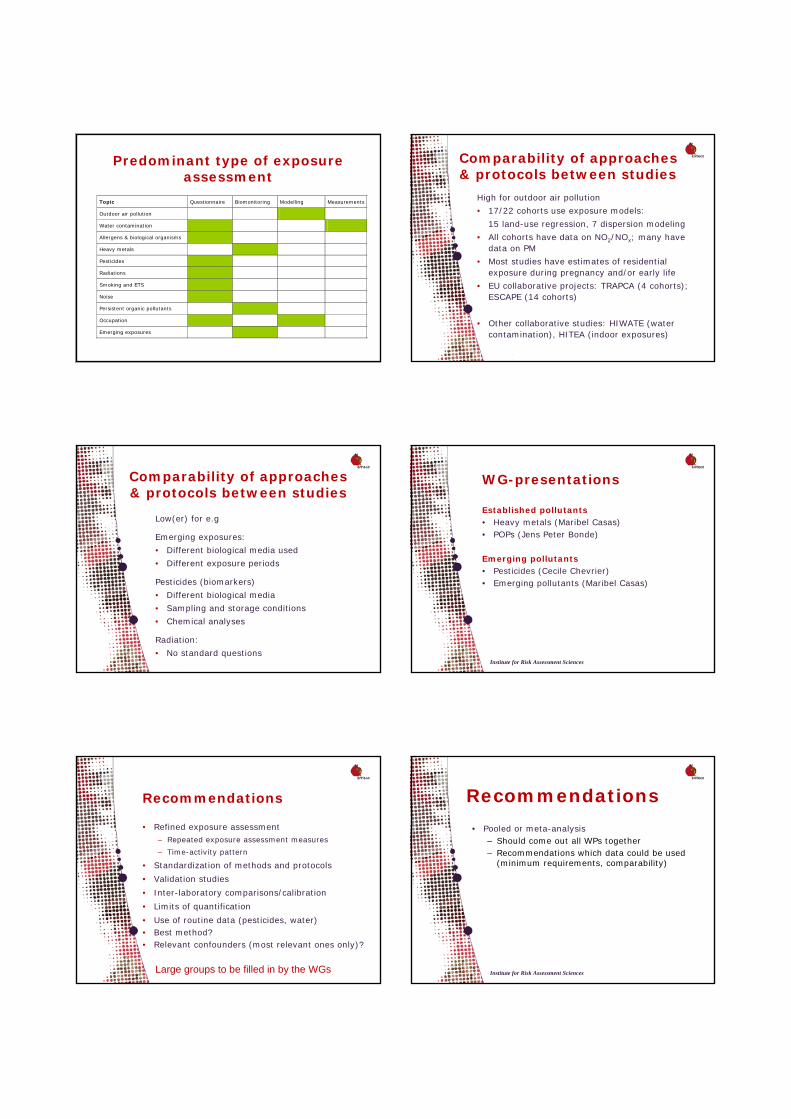
Institute for Risk Assessment Sciences
Predominant type of exposure assessment
Topic Questionnaire Biomonitoring Modelling Measurements
Outdoor air pollution
Water contamination
Allergens & biological organisms
Heavy metals
Pesticides
Radiations
Smoking and ETS
Noise
Persistent organic pollutants
Occupation
Emerging exposures
Institute for Risk Assessment Sciences
Comparability of approaches & protocols between studies
High for outdoor air pollution
• 17/22 cohorts use exposure models:
15 land-use regression, 7 dispersion modeling
• All cohorts have data on NO2/NOx; many have data on PM
• Most studies have estimates of residential exposure during pregnancy and/or early life
• EU collaborative projects: TRAPCA (4 cohorts); ESCAPE (14 cohorts)
• Other collaborative studies: HIWATE (water contamination), HITEA (indoor exposures)
Institute for Risk Assessment Sciences
Comparability of approaches & protocols between studies
Low(er) for e.g
Emerging exposures:
• Different biological media used
• Different exposure periods
Pesticides (biomarkers)
• Different biological media
• Sampling and storage conditions
• Chemical analyses
Radiation:
• No standard questionsInstitute for Risk Assessment Sciences
WG-presentations
Established pollutants• Heavy metals (Maribel Casas)• POPs (Jens Peter Bonde)
Emerging pollutants• Pesticides (Cecile Chevrier)• Emerging pollutants (Maribel Casas)
Institute for Risk Assessment Sciences
Recommendations
• Refined exposure assessment– Repeated exposure assessment measures
– Time-activity pattern
• Standardization of methods and protocols
• Validation studies
• Inter-laboratory comparisons/calibration
• Limits of quantification
• Use of routine data (pesticides, water)• Best method?• Relevant confounders (most relevant ones only)?
Large groups to be filled in by the WGs Institute for Risk Assessment Sciences
Recommendations
• Pooled or meta-analysis– Should come out all WPs together– Recommendations which data could be used
(minimum requirements, comparability)

Institute for Risk Assessment Sciences
Publications
• One overview paper with limitations recommendation s and online supplement for the groups or reference to ENRIECO website.
• Pesticides• Emerging exposures/best methods• POPs part of case study• Possibility to combine it with WP4
• Air pollution• Water contamination• Heavy metals• Noise?
• Combined paper about biomonitoring
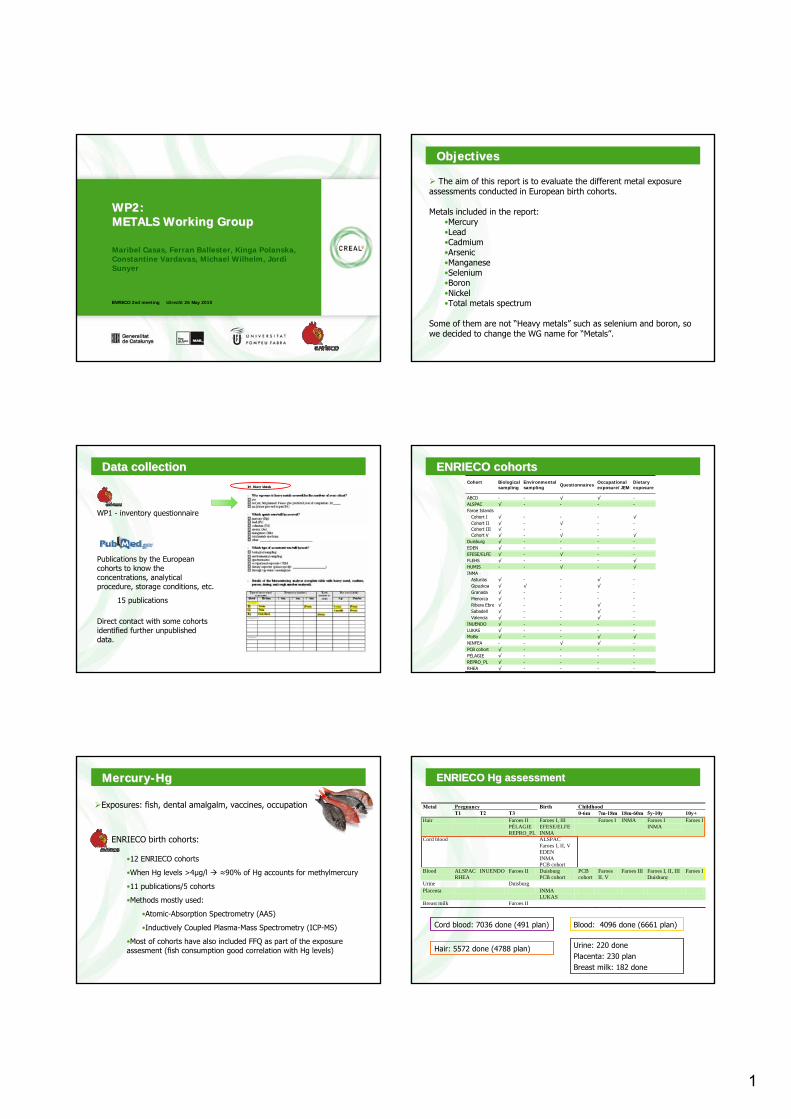
1
www.creal.cat
ENRIECO 2nd meeting Utrecht 26 May 2010
WP2:WP2:METALS Working Group METALS Working Group
Maribel Casas, Ferran Ballester, Kinga Polanska, Constantine Vardavas, Michael Wilhelm, Jordi Sunyer
www.creal.cat
ObjectivesObjectives
The aim of this report is to evaluate the different metal exposure assessments conducted in European birth cohorts.
Metals included in the report:•Mercury•Lead•Cadmium•Arsenic•Manganese•Selenium•Boron•Nickel•Total metals spectrum
Some of them are not “Heavy metals” such as selenium and boron, so we decided to change the WG name for “Metals”.
www.creal.cat
Publications by the European cohorts to know the concentrations, analytical procedure, storage conditions, etc.
15 publications
WP1 - inventory questionnaire
Data Data collectioncollection
Direct contact with some cohorts identified further unpublished data.
www.creal.cat
ENRIECO cohortsENRIECO cohortsCohort
Biological sampling
Environmental sampling Questionnaires Occupational
exposure/JEM Dietary exposure
ABCD - - √ √ - ALSPAC √ - - - - Faroe Islands Cohort I √ - - - √ Cohort II √ - √ - - Cohort III √ - - - - Cohort V √ - √ - √ Duisburg √ - - - - EDEN √ - - - - EFESE/ELFE √ - √ - - FLEHS √ - - - √
HUMIS - - √ - √
INMA Asturias √ - - √ - Gipuzkoa √ √ - √ -
Granada √ - - - - Menorca √ - - - - Ribera Ebre √ - - √ - Sabadell √ - - √ - Valencia √ - - √ - INUENDO √ - - - - LUKAS √ - - - - MoBa √ - - √ √ NINFEA - - √ √ - PCB cohort √ - - - - PÉLAGIE √ - - - - REPRO_PL √ - - - -
RHEA √ - - - -
www.creal.cat
MercuryMercury--HgHg
Exposures: fish, dental amalgalm, vaccines, occupation
ENRIECO birth cohorts:
•12 ENRIECO cohorts
•When Hg levels >4µg/l ≈90% of Hg accounts for methylmercury
•11 publications/5 cohorts
•Methods mostly used:
•Atomic-Absorption Spectrometry (AAS)
•Inductively Coupled Plasma-Mass Spectrometry (ICP-MS)
•Most of cohorts have also included FFQ as part of the exposureassesment (fish consumption good correlation with Hg levels)
www.creal.cat
ENRIECO Hg ENRIECO Hg assessmentassessment
Pregnancy Childhood Metal T1 T2 T3
Birth 0-6m 7m-18m 18m-60m 5y-10y 10y+
Hair Faroes II PÉLAGIE REPRO_PL
Faroes I, III EFESE/ELFE INMA
Faroes I INMA Faroes I INMA
Faroes I
Cord blood ALSPAC Faroes I, II, V EDEN INMA PCB cohort
Blood ALSPAC RHEA
INUENDO Faroes II Duisburg PCB cohort
PCB cohort
Faroes II, V
Faroes III Faroes I, II, III Duisburg
Faroes I
Urine Duisburg Placenta INMA
LUKAS
Breast milk Faroes II
Cord blood: 7036 done (491 plan)
Hair: 5572 done (4788 plan)
Blood: 4096 done (6661 plan)
Urine: 220 donePlacenta: 230 planBreast milk: 182 done
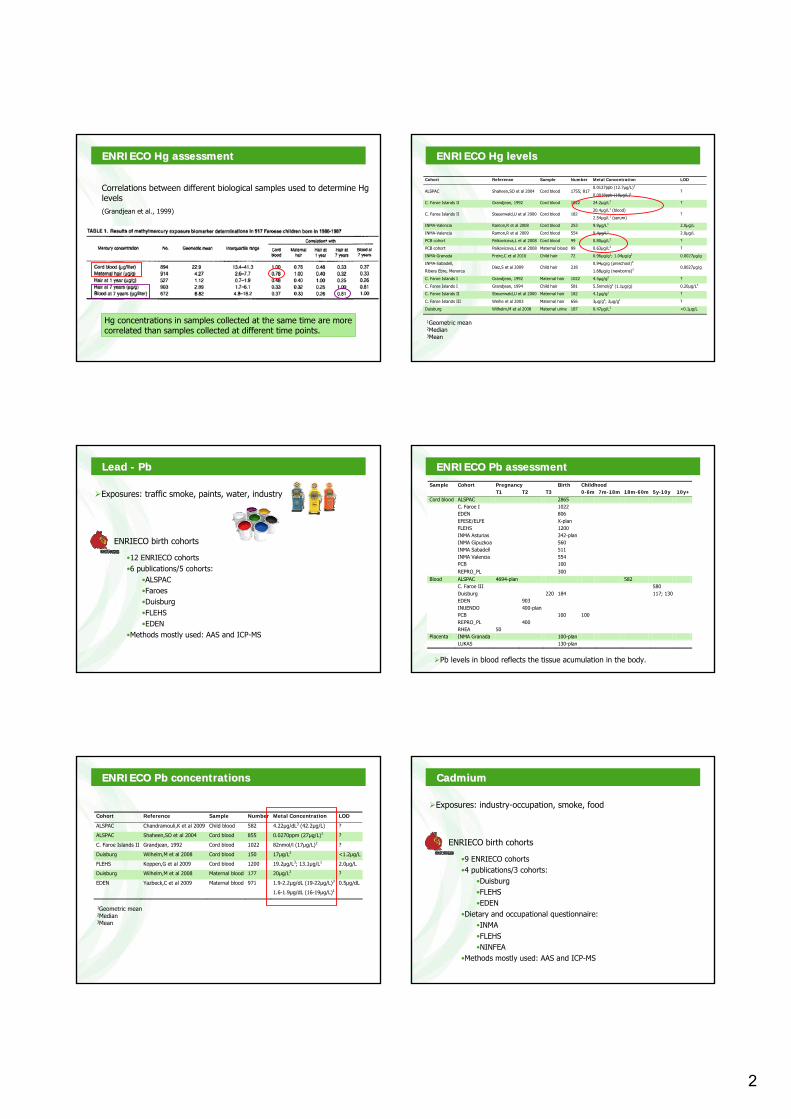
2
www.creal.cat
ENRIECO Hg ENRIECO Hg assessmentassessment
Correlations between different biological samples used to determine Hg levels(Grandjean et al., 1999)
Hg concentrations in samples collected at the same time are more correlated than samples collected at different time points.
www.creal.cat
Cohort Reference Sample Number Metal Concentration LOD
ALSPAC Shaheen,SO et al 2004 Cord blood 1755; 817 0.0127ppb (12.7μg/L)1
0.0018ppb (18μg/L)1 ?
C. Faroe Islands II Grandjean, 1992 Cord blood 1022 24.2μg/L2 ?
C. Faroe Islands II Steuerwald,U et al 2000 Cord blood 182 20.4μg/L1 (blood)
2.54μg/L1 (serum) ?
INMA-Valencia Ramon,R et al 2008 Cord blood 253 9.9µg/L1 2.0µg/L
INMA-Valencia Ramon,R et al 2009 Cord blood 554 9.4µg/L1 2.0µg/L
PCB cohort Palkovicova,L et al 2008 Cord blood 99 0.80μg/L2 ?
PCB cohort Palkovicova,L et al 2008 Maternal blood 99 0.63μg/L2 ?
INMA-Granada Freire,C et al 2010 Child hair 72 0.96µg/g1; 1.04µg/g2 0.0027µg/g
INMA-Sabadell,
Ribera Ebre, Menorca Diez,S et al 2009 Child hair 218
0.94µg/g (preschool)3
1.68µg/g (newborns)3 0.0027µg/g
C. Faroe Islands I Grandjean, 1992 Maternal hair 1022 4.5μg/g2 ?
C. Faroe Islands I Grandjean, 1994 Child hair 581 5.5nmol/g1 (1.1µg/g) 0.20µg/L4
C. Faroe Islands II Steuerwald,U et al 2000 Maternal hair 182 4.1µg/g1 ?
C. Faroe Islands III Weihe et al 2003 Maternal hair 656 3µg/g3; 2µg/g1 ?
Duisburg Wilhelm,M et al 2008 Maternal urine 187 0.47µg/L2 <0.1µg/L
ENRIECO Hg ENRIECO Hg levelslevels
1Geometric mean2Median3Mean
www.creal.cat
LeadLead -- PbPb
Exposures: traffic smoke, paints, water, industry
ENRIECO birth cohorts
•12 ENRIECO cohorts•6 publications/5 cohorts:
•ALSPAC•Faroes•Duisburg•FLEHS•EDEN
•Methods mostly used: AAS and ICP-MS
www.creal.cat
ENRIECO ENRIECO PbPb assessmentassessmentSample Cohort Pregnancy Birth Childhood T1 T2 T3 0-6m 7m-18m 18m-60m 5y-10y 10y+Cord blood ALSPAC 2865 C. Faroe I 1022 EDEN 806 EFESE/ELFE X-plan FLEHS 1200 INMA Asturias 342-plan INMA Gipuzkoa 560 INMA Sabadell 511 INMA Valencia 554 PCB 100 REPRO_PL 300 Blood ALSPAC 4694-plan 582 C. Faroe III 580 Duisburg 220 184 117; 130 EDEN 903 INUENDO 400-plan PCB 100 100 REPRO_PL 400 RHEA 50 Placenta INMA Granada 100-plan LUKAS 130-plan
Pb levels in blood reflects the tissue acumulation in the body.
www.creal.cat
ENRIECO ENRIECO PbPb concentrationsconcentrations
Cohort Reference Sample Number Metal Concentration LOD
ALSPAC Chandramouli,K et al 2009 Child blood 582 4.22µg/dL3 (42.2µg/L) ?
ALSPAC Shaheen,SO et al 2004 Cord blood 855 0.0270ppm (27µg/L)1 ?
C. Faroe Islands II Grandjean, 1992 Cord blood 1022 82nmol/l (17µg/L)2 ?
Duisburg Wilhelm,M et al 2008 Cord blood 150 17µg/L2 <1.2µg/L
FLEHS Koppen,G et al 2009 Cord blood 1200 19.2μg/L3; 13.1μg/L1 2.0μg/L
Duisburg Wilhelm,M et al 2008 Maternal blood 177 20µg/L2 ?
EDEN Yazbeck,C et al 2009 Maternal blood 971 1.9-2.2µg/dL (19-22µg/L)3
1.6-1.9µg/dL (16-19µg/L)1
0.5µg/dL
1Geometric mean2Median3Mean
www.creal.cat
CadmiumCadmium
Exposures: industry-occupation, smoke, food
ENRIECO birth cohorts
•9 ENRIECO cohorts•4 publications/3 cohorts:
•Duisburg•FLEHS•EDEN
•Dietary and occupational questionnaire: •INMA•FLEHS•NINFEA
•Methods mostly used: AAS and ICP-MS
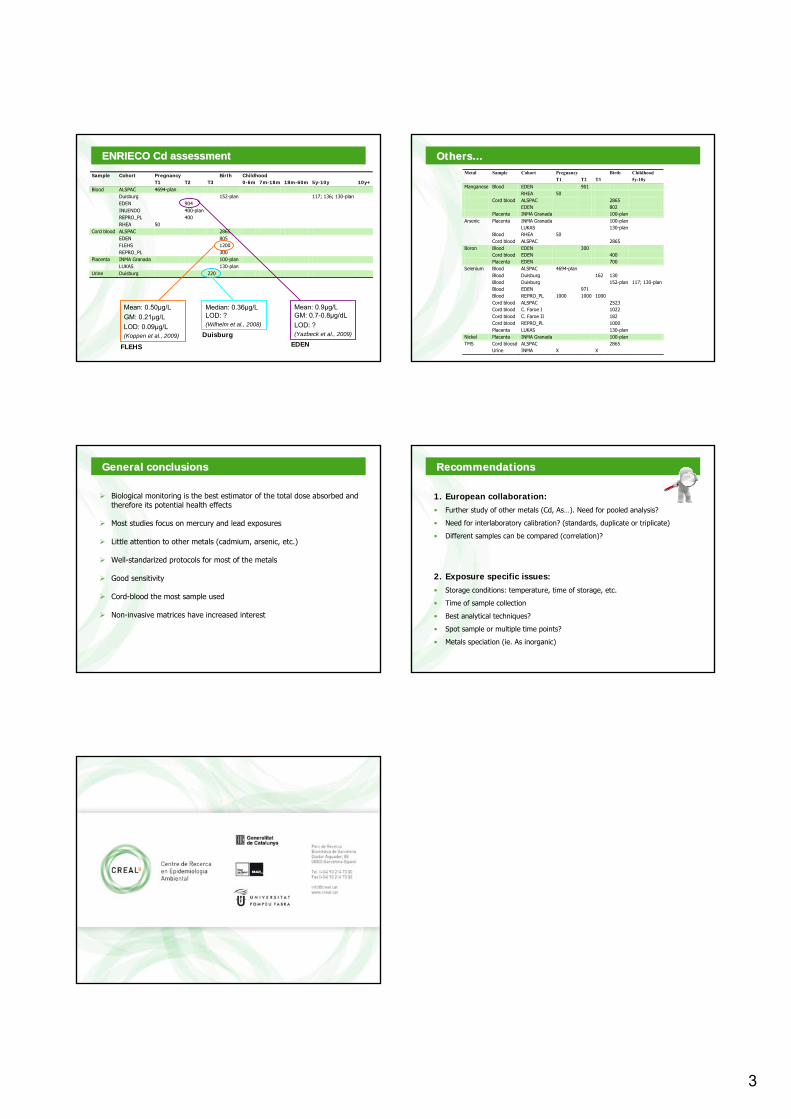
3
www.creal.cat
ENRIECO ENRIECO CdCd assessmentassessmentPregnancy Birth Childhood Sample Cohort T1 T2 T3 0-6m 7m-18m 18m-60m 5y-10y 10y+
Blood ALSPAC 4694-plan Duisburg 152-plan 117; 136; 130-plan EDEN 904 INUENDO 400-plan REPRO_PL 400 RHEA 50 Cord blood ALSPAC 2865 EDEN 805 FLEHS 1200 REPRO_PL 300 Placenta INMA Granada 100-plan LUKAS 130-plan Urine Duisburg 220
Mean: 0.50μg/LGM: 0.21μg/LLOD: 0.09μg/L(Koppen et al., 2009)
Mean: 0.9µg/L GM: 0.7-0.8µg/dLLOD: ?(Yazbeck et al., 2009)
Median: 0.36µg/LLOD: ?(Wilhelm et al., 2008)
FLEHS EDENDuisburg
www.creal.cat
OthersOthers……Pregnancy Childhood Metal Sample Cohort T1 T2 T3
Birth 5y-10y
Manganese Blood EDEN 901 RHEA 50 Cord blood ALSPAC 2865 EDEN 802 Placenta INMA Granada 100-plan Arsenic Placenta INMA Granada 100-plan LUKAS 130-plan Blood RHEA 50 Cord blood ALSPAC 2865 Boron Blood EDEN 300 Cord blood EDEN 400 Placenta EDEN 700 Selenium Blood ALSPAC 4694-plan Blood Duisburg 162 130 Blood Duisburg 152-plan 117; 130-plan Blood EDEN 971 Blood REPRO_PL 1000 1000 1000 Cord blood ALSPAC 2523 Cord blood C. Faroe I 1022 Cord blood C. Faroe II 182 Cord blood REPRO_PL 1000 Placenta LUKAS 130-plan Nickel Placenta INMA Granada 100-plan TMS Cord bloosd ALSPAC 2865 Urine INMA X X
www.creal.cat
General General conclusionsconclusions
Biological monitoring is the best estimator of the total dose absorbed andtherefore its potential health effects
Most studies focus on mercury and lead exposures
Little attention to other metals (cadmium, arsenic, etc.)
Well-standarized protocols for most of the metals
Good sensitivity
Cord-blood the most sample used
Non-invasive matrices have increased interest
www.creal.cat
RecommendationsRecommendations
1. European collaboration:• Further study of other metals (Cd, As…). Need for pooled analysis?
• Need for interlaboratory calibration? (standards, duplicate or triplicate)
• Different samples can be compared (correlation)?
2. Exposure specific issues:• Storage conditions: temperature, time of storage, etc.
• Time of sample collection
• Best analytical techniques?
• Spot sample or multiple time points?
• Metals speciation (ie. As inorganic)
www.creal.cat
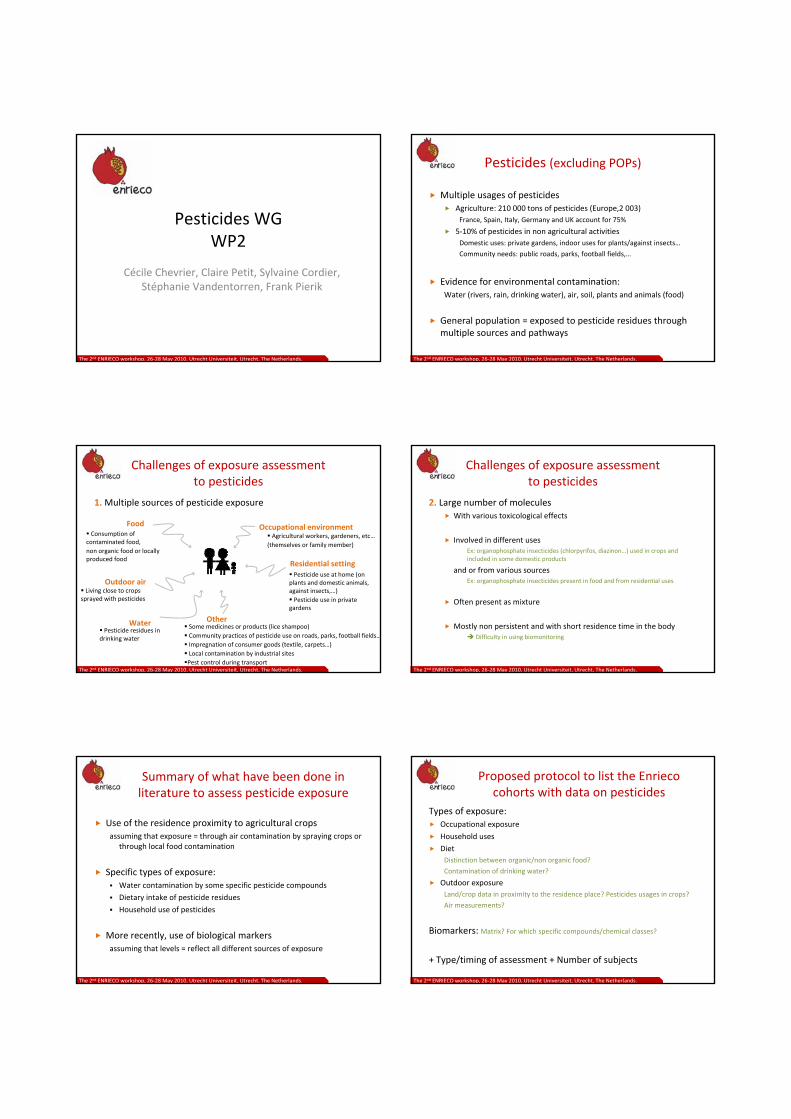
Pesticides WG WP2
Cécile Chevrier, Claire Petit, Sylvaine Cordier, Stéphanie Vandentorren, Frank Pierik
The 2nd ENRIECO workshop, 26‐28 May 2010, Utrecht Universiteit, Utrecht, The Netherlands.
Pesticides (excluding POPs)
Multiple usages of pesticidesAgriculture: 210 000 tons of pesticides (Europe,2 003)France, Spain, Italy, Germany and UK account for 75%
5‐10% of pesticides in non agricultural activitiesDomestic uses: private gardens, indoor uses for plants/against insects…
Community needs: public roads, parks, football fields,…
Evidence for environmental contamination:Water (rivers, rain, drinking water), air, soil, plants and animals (food)
General population = exposed to pesticide residues through multiple sources and pathways
The 2nd ENRIECO workshop, 26‐28 May 2010, Utrecht Universiteit, Utrecht, The Netherlands.
Challenges of exposure assessment to pesticides
1. Multiple sources of pesticide exposure
The 2nd ENRIECO workshop, 26‐28 May 2010, Utrecht Universiteit, Utrecht, The Netherlands.
Living close to crops sprayed with pesticides
Outdoor air
Food
Pesticide use at home (on plants and domestic animals, against insects,…)Pesticide use in private
gardens
Residential setting
WaterPesticide residues in
drinking water
Consumption of contaminated food, non organic food or locally produced food
Occupational environmentAgricultural workers, gardeners, etc…
(themselves or family member)
OtherSome medicines or products (lice shampoo)Community practices of pesticide use on roads, parks, football fields…Impregnation of consumer goods (textile, carpets…)Local contamination by industrial sitesPest control during transport
Challenges of exposure assessment to pesticides
2. Large number of moleculesWith various toxicological effects
Involved in different uses Ex: organophosphate insecticides (chlorpyrifos, diazinon…) used in crops and included in some domestic products
and or from various sourcesEx: organophosphate insecticides present in food and from residential uses
Often present as mixture
Mostly non persistent and with short residence time in the bodyDifficulty in using biomonitoring
The 2nd ENRIECO workshop, 26‐28 May 2010, Utrecht Universiteit, Utrecht, The Netherlands.
Summary of what have been done in literature to assess pesticide exposure
Use of the residence proximity to agricultural crops assuming that exposure = through air contamination by spraying crops or
through local food contamination
Specific types of exposure:Water contamination by some specific pesticide compounds
Dietary intake of pesticide residues
Household use of pesticides
More recently, use of biological markers assuming that levels = reflect all different sources of exposure
The 2nd ENRIECO workshop, 26‐28 May 2010, Utrecht Universiteit, Utrecht, The Netherlands.
Proposed protocol to list the Enrieco cohorts with data on pesticides
Types of exposure:Occupational exposure
Household uses
DietDistinction between organic/non organic food?
Contamination of drinking water?
Outdoor exposureLand/crop data in proximity to the residence place? Pesticides usages in crops?
Air measurements?
Biomarkers: Matrix? For which specific compounds/chemical classes?
+ Type/timing of assessment + Number of subjects
The 2nd ENRIECO workshop, 26‐28 May 2010, Utrecht Universiteit, Utrecht, The Netherlands.
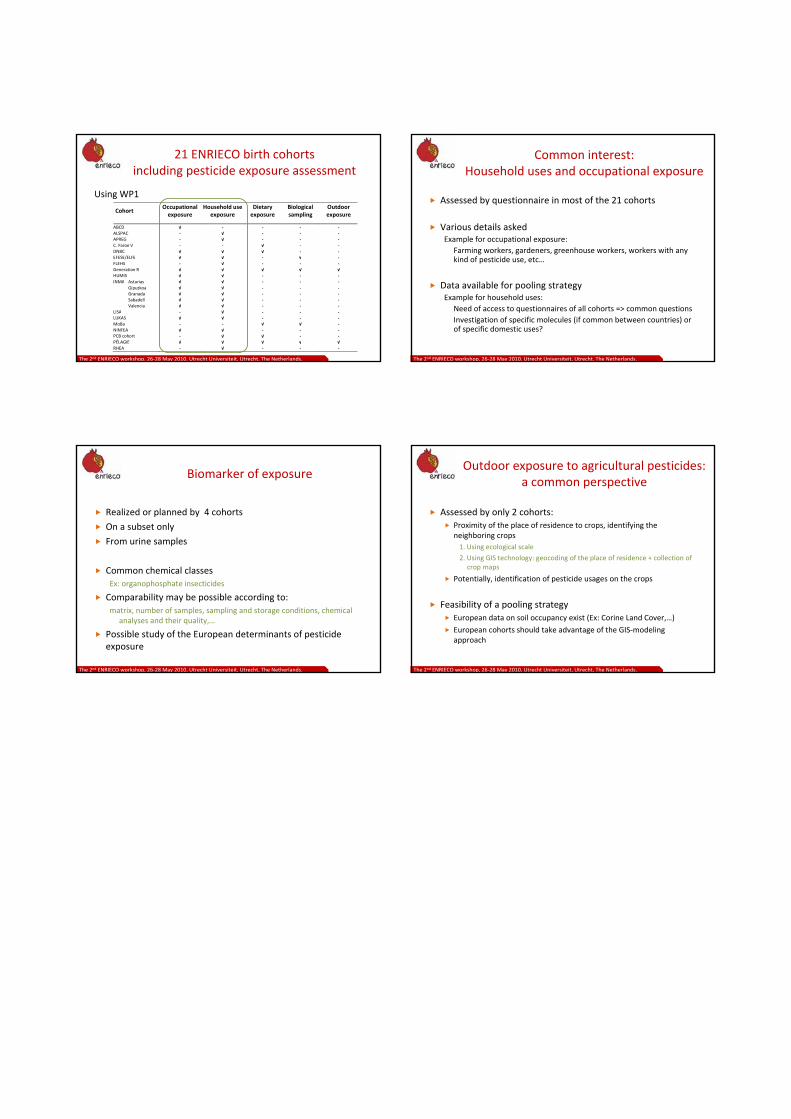
21 ENRIECO birth cohorts including pesticide exposure assessment
Using WP1
The 2nd ENRIECO workshop, 26‐28 May 2010, Utrecht Universiteit, Utrecht, The Netherlands.
Cohort Occupational exposure
Household use exposure
Dietary exposure
Biological sampling
Outdoor exposure
ABCD √ ‐ ‐ ‐ ‐ ALSPAC ‐ √ ‐ ‐ ‐ APREG ‐ √ ‐ ‐ ‐ C. Faroe V ‐ ‐ √ ‐ ‐ DNBC √ √ √ ‐ ‐ EFESE/ELFE √ √ ‐ √ ‐ FLEHS ‐ √ ‐ ‐ ‐Generation R √ √ √ √ √ HUMIS √ √ ‐ ‐ ‐ INMA Asturias √ √ ‐ ‐ ‐ Gipuzkoa √ √ ‐ ‐ ‐ Granada √ √ ‐ ‐ ‐ Sabadell √ √ ‐ ‐ ‐ Valencia √ √ ‐ ‐ ‐LISA ‐ √ ‐ ‐ ‐ LUKAS √ √ ‐ ‐ ‐ MoBa ‐ ‐ √ √ ‐ NINFEA √ √ ‐ ‐ ‐ PCB cohort ‐ √ √ ‐ ‐ PÉLAGIE √ √ √ √ √RHEA ‐ √ ‐ ‐ ‐
Common interest: Household uses and occupational exposure
Assessed by questionnaire in most of the 21 cohorts
Various details askedExample for occupational exposure:
Farming workers, gardeners, greenhouse workers, workers with anykind of pesticide use, etc…
Data available for pooling strategyExample for household uses:
Need of access to questionnaires of all cohorts => common questionsInvestigation of specific molecules (if common between countries) or of specific domestic uses?
The 2nd ENRIECO workshop, 26‐28 May 2010, Utrecht Universiteit, Utrecht, The Netherlands.
Biomarker of exposure
Realized or planned by 4 cohorts
On a subset only
From urine samples
Common chemical classesEx: organophosphate insecticides
Comparability may be possible according to:matrix, number of samples, sampling and storage conditions, chemical
analyses and their quality,…
Possible study of the European determinants of pesticide exposure
The 2nd ENRIECO workshop, 26‐28 May 2010, Utrecht Universiteit, Utrecht, The Netherlands.
Outdoor exposure to agricultural pesticides:a common perspective
Assessed by only 2 cohorts:Proximity of the place of residence to crops, identifying the neighboring crops1. Using ecological scale
2. Using GIS technology: geocoding of the place of residence + collection of crop maps
Potentially, identification of pesticide usages on the crops
Feasibility of a pooling strategyEuropean data on soil occupancy exist (Ex: Corine Land Cover,…)
European cohorts should take advantage of the GIS‐modeling approach
The 2nd ENRIECO workshop, 26‐28 May 2010, Utrecht Universiteit, Utrecht, The Netherlands.
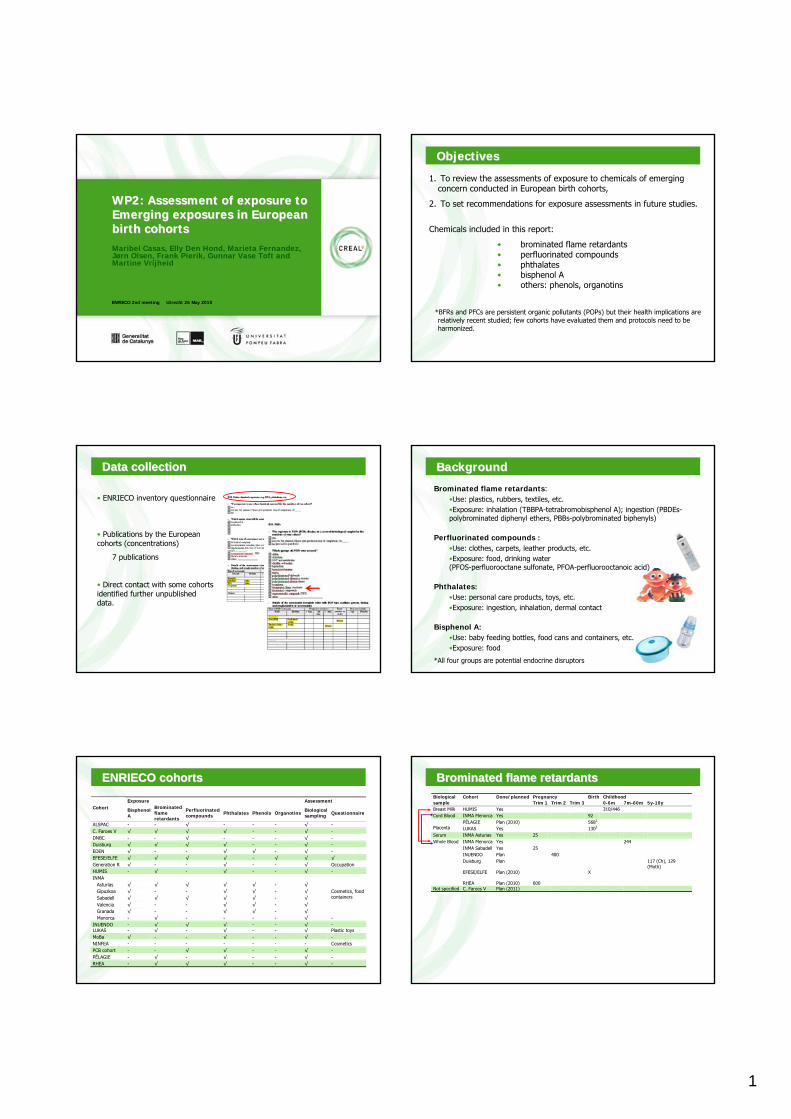
1
www.creal.cat
ENRIECO 2nd meeting Utrecht 26 May 2010
WP2:WP2: Assessment of exposure to Assessment of exposure to Emerging exposures in European Emerging exposures in European birth cohortsbirth cohortsMaribel Casas, Elly Den Hond, Marieta Fernandez, Jørn Olsen, Frank Pierik, Gunnar Vase Toft andMartine Vrijheid
www.creal.cat
ObjectivesObjectives
1. To review the assessments of exposure to chemicals of emerging concern conducted in European birth cohorts,
2. To set recommendations for exposure assessments in future studies.
Chemicals included in this report:
• brominated flame retardants • perfluorinated compounds• phthalates• bisphenol A• others: phenols, organotins
*BFRs and PFCs are persistent organic pollutants (POPs) but their health implications are relatively recent studied; few cohorts have evaluated them and protocols need to be harmonized.
www.creal.cat
Data Data collectioncollection
• ENRIECO inventory questionnaire
• Publications by the European cohorts (concentrations)
7 publications
• Direct contact with some cohorts identified further unpublished data.
www.creal.cat
Brominated flame retardants:•Use: plastics, rubbers, textiles, etc.•Exposure: inhalation (TBBPA-tetrabromobisphenol A); ingestion (PBDEs-polybrominated diphenyl ethers, PBBs-polybrominated biphenyls)
Perfluorinated compounds :•Use: clothes, carpets, leather products, etc.•Exposure: food, drinking water(PFOS-perfluorooctane sulfonate, PFOA-perfluorooctanoic acid)
Phthalates:•Use: personal care products, toys, etc.•Exposure: ingestion, inhalation, dermal contact
Bisphenol A:•Use: baby feeding bottles, food cans and containers, etc.•Exposure: food
*All four groups are potential endocrine disruptors
BackgroundBackground
www.creal.cat
ENRIECO cohortsENRIECO cohorts
Exposure Assessment Cohort Bisphenol
A
Brominated flame retardants
Perfluorinated compounds Phthalates Phenols Organotins Biological
sampling Questionnaire
ALSPAC - - √ - - - √ - C. Faroes V √ √ √ √ - - √ - DNBC - - √ - - - √ - Duisburg √ √ √ √ - - √ - EDEN √ - - √ √ - √ - EFESE/ELFE √ √ √ √ - √ √ √ Generation R √ - - √ - - √ Occupation
HUMIS - √ - √ - - √ - INMA Asturias √ √ √ √ √ - √ Gipuzkoa √ - - √ √ - √ Sabadell √ √ √ √ √ - √ Valencia √ - - √ √ - √
Cosmetics, food containers
Granada √ - - √ √ - √
Menorca - √ - - - - √ - INUENDO - √ √ √ - - √ - LUKAS - √ - √ - - √ Plastic toys
MoBa √ - - √ - - √ - NINFEA - - - - - - - Cosmetics
PCB cohort - - √ √ - - √ - PÉLAGIE - √ - √ - - √ - RHEA - √ √ √ - - √ -
www.creal.cat
BrominatedBrominated flameflame retardantsretardantsBiological Cohort Done/planned Pregnancy Birth Childhood sample Trim 1 Trim 2 Trim 3 0-6m 7m-60m 5y-10y Breast Milk HUMIS Yes 310/446 Cord Blood INMA Menorca Yes 92
PÉLAGIE Plan (2010) 5682 Placenta LUKAS Yes 1303 Serum INMA Asturias Yes 25
INMA Menorca Yes 244 INMA Sabadell Yes 25 INUENDO Plan 400
Whole Blood
Duisburg Plan 117 (Ch), 129 (Moth)
EFESE/ELFE Plan (2010) X
RHEA Plan (2010) 600 Not specified C. Faroes V Plan (2011)
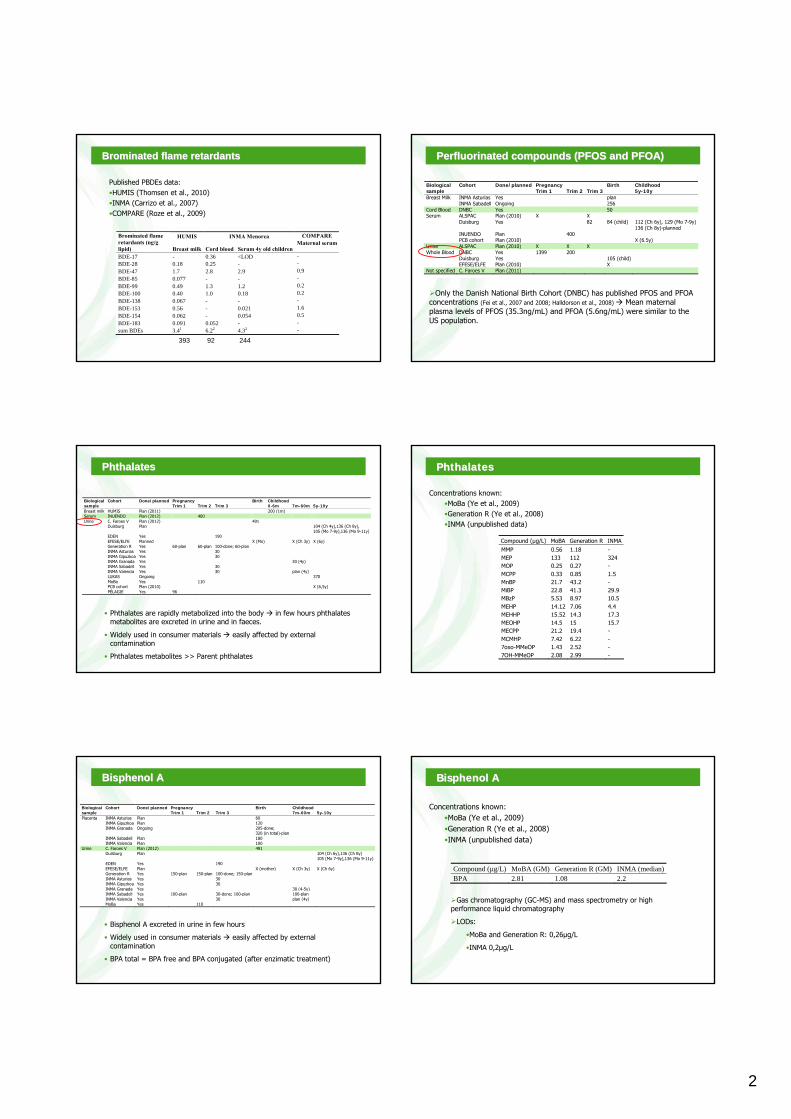
2
www.creal.cat
BrominatedBrominated flameflame retardantsretardants
Published PBDEs data:•HUMIS (Thomsen et al., 2010)•INMA (Carrizo et al., 2007)•COMPARE (Roze et al., 2009)
HUMIS INMA Menorca COMPARE Brominated flame retardants (ng/g lipid) Breast milk Cord blood Serum 4y old children
Maternal serum
BDE-17 - 0.36 <LOD - BDE-28 0.18 0.25 - - BDE-47 1.7 2.8 2.9 0.9 BDE-85 0.077 - - - BDE-99 0.49 1.3 1.2 0.2 BDE-100 0.40 1.0 0.18 0.2 BDE-138 0.067 - - - BDE-153 0.56 - 0.021 1.6 BDE-154 0.062 - 0.054 0.5 BDE-183 0.091 0.052 - - sum BDEs 3.41 6.22 4.32 -
393 92 244www.creal.cat
PerfluorinatedPerfluorinated compoundscompounds (PFOS (PFOS andand PFOA)PFOA)
Biological Cohort Done/planned Pregnancy Birth Childhood sample Trim 1 Trim 2 Trim 3 5y-10y Breast Milk INMA Asturias Yes plan INMA Sabadell Ongoing 256 Cord Blood DNBC Yes 50 Serum ALSPAC Plan (2010) X X Duisburg Yes 82 84 (child) 112 (Ch 6y), 129 (Mo 7-9y)
136 (Ch 8y)-planned INUENDO Plan 400 PCB cohort Plan (2010) X (6.5y) Urine ALSPAC Plan (2010) X X X Whole Blood DNBC Yes 1399 200 Duisburg Yes 105 (child) EFESE/ELFE Plan (2010) X Not specified C. Faroes V Plan (2011)
Only the Danish National Birth Cohort (DNBC) has published PFOS and PFOA concentrations (Fei et al., 2007 and 2008; Halldorson et al., 2008) Mean maternal plasma levels of PFOS (35.3ng/mL) and PFOA (5.6ng/mL) were similar to the US population.
www.creal.cat
PhthalatesPhthalates
Biological Cohort Done/planned Pregnancy Birth Childhood sample Trim 1 Trim 2 Trim 3 0-6m 7m-60m 5y-10y Breast milk HUMIS Plan (2011) 200 (1m) Serum INUENDO Plan (2012) 400 Urine C. Faroes V Plan (2012) 491 Duisburg Plan 104 (Ch 4y),136 (Ch 8y),
105 (Mo 7-9y),136 (Mo 9-11y) EDEN Yes 190 EFESE/ELFE Planned X (Mo) X (Ch 3y) X (6y) Generation R Yes 60-plan 60-plan 100-done; 60-plan INMA Asturias Yes 30 INMA Gipuzkoa Yes 30 INMA Granada Yes 30 (4y) INMA Sabadell Yes 30 INMA Valencia Yes 30 plan (4y) LUKAS Ongoing 370 MoBa Yes 110 PCB cohort Plan (2010) X (6,5y) PÉLAGIE Yes 96
• Phthalates are rapidly metabolized into the body in few hours phthalatesmetabolites are excreted in urine and in faeces.
• Widely used in consumer materials easily affected by external contamination
• Phthalates metabolites >> Parent phthalates www.creal.cat
PhthalatesPhthalates
Concentrations known:•MoBa (Ye et al., 2009)•Generation R (Ye et al., 2008)•INMA (unpublished data)
Compound (µg/L) MoBA Generation R INMA MMP 0.56 1.18 - MEP 133 112 324 MOP 0.25 0.27 - MCPP 0.33 0.85 1.5 MnBP 21.7 43.2 - MiBP 22.8 41.3 29.9 MBzP 5.53 8.97 10.5 MEHP 14.12 7.06 4.4 MEHHP 15.52 14.3 17.3 MEOHP 14.5 15 15.7 MECPP 21.2 19.4 - MCMHP 7.42 6.22 - 7oxo-MMeOP 1.43 2.52 - 7OH-MMeOP 2.08 2.99 -
www.creal.cat
BisphenolBisphenol AA
Biological Cohort Done/planned Pregnancy Birth Childhood sample Trim 1 Trim 2 Trim 3 7m-60m 5y-10y Placenta INMA Asturias Plan 60 INMA Gipuzkoa Plan 120 INMA Granada Ongoing 205-done;
320 (in total)-plan
INMA Sabadell Plan 180 INMA Valencia Plan 100 Urine C. Faroes V Plan (2012) 491 Duisburg Plan 104 (Ch 6y),136 (Ch 8y)
105 (Mo 7-9y),136 (Mo 9-11y) EDEN Yes 190 EFESE/ELFE Plan X (mother) X (Ch 3y) X (Ch 6y) Generation R Yes 150-plan 150-plan 100-done; 150-plan INMA Asturias Yes 30 INMA Gipuzkoa Yes 30 INMA Granada Yes 30 (4-5y) INMA Sabadell Yes 100-plan 30-done; 100-plan 100-plan INMA Valencia Yes 30 plan (4y) MoBa Yes 110
• Bisphenol A excreted in urine in few hours
• Widely used in consumer materials easily affected by external contamination
• BPA total = BPA free and BPA conjugated (after enzimatic treatment) www.creal.cat
BisphenolBisphenol AA
Gas chromatography (GC-MS) and mass spectrometry or highperformance liquid chromatography
LODs:
•MoBa and Generation R: 0,26µg/L
•INMA 0,2µg/L
Compound (µg/L) MoBA (GM) Generation R (GM) INMA (median)BPA 2.81 1.08 2.2
Concentrations known:•MoBa (Ye et al., 2009)•Generation R (Ye et al., 2008)•INMA (unpublished data)
3
www.creal.cat
OthersOthers
Biological Cohort Done/planned Pregnancy Birth Childhood sample Trim 1 Trim 2 Trim 3 0-6m 7m-60m 5y-10y Phenols and parabens Urine EDEN Yes 190 INMA Asturias Yes 30 INMA Gipuzkoa Yes 30 INMA Granada Yes 30 (4y) INMA Sabadell Yes 30 INMA Valencia Yes 30 Organotins Urine EFESE/ELFE Plan X (mother) X (Ch 3y) X (Ch 6y)
Chlorophenols: pesticides
Parabens: preservatives and antimicrobial agents (food, sahmpoo, cosmetics)
Organotins: agricultural fungicides
www.creal.cat
General General conclusionsconclusions
• few actual measurements, small samples
• little correspondence in biological media used, pregnancy/childhood period, etc
• few cohorts use multiple measurements (important for the non-persistent substances)
• little attention to multiple low-level exposures
• unknown intra and inter-laboratory variability for some compounds
• at the moment not sufficient data for pooling/comparison studies
www.creal.cat
RecommendationsRecommendations
1. European collaboration:
• Need for pooled studies? Need for replication/comparison studies? If so, prioritise compounds?
• Assessment of effects of multiple low level exposures• Mechanism for detection and prioritisation of new chemicals – in collaboration
with toxicologists• Evaluation and control of inter and intra laboratory variability
2. Exposure specific issues:
• Storage conditions: best containers; temperature; time of storage; etc.• Contamination issues• Best analytical techniques? • Preferred biological multiple media; need for duplicate/triplicate measures of
same sample; etc. • Need for measurements at multiple time points? (important for BPA,
phthalates, other non-persistent compounds...) www.creal.cat
0
WP2 Case studyOccupational exposures
WG Leader: S. Cordier
What is the specificity of occupational exposurescompared to environmental exposures in general ?
– Some agents/exposure situations are predominant in (or unique to) occupational environment ie: solvents, radiations, night work…
– Mixtures of exposures may be crucial and may explain excess risk in some occupations (i.e. hairdressers, cleaners…)
– Exposure at work to some compounds of interest is higher than environmental exposure
Why study occupational exposures in ENRIECO birth cohorts ?
(compared to occupational cohorts or birth registries)
– prospective collection of occupational data before birth(recall bias)
– evaluation of long term consequences of preconceptualor prenatal occupational exposures (maternal and paternal)
– evaluation of risks associated with exposure to mixtures present in occupations across different European countries
How to assess occupational exposures?
– From occupation and, ideally, economic activity(ex: cashier in a dry-cleaning shop)
– From self report of specific exposures– From occupation + Job-Exposure Matrix (JEM)– From expert assessment of likely exposures in a
job– From biomarkers of exposure
What is a Job-Exposure matrix ?
Table of correspondance between occupation title and likely exposurespresent in this occupation
• together with various exposure parameters: probability of exposure, level …
• period-specific, country-specific (to be discussed), sex-specific?
Advantages-pool together occupations with same exposure⇒ increase power, less confounding with co-exposures, less recall bias
Drawbacks-ecological measure, validation?
Example of “van Tongeren” JEM
• Description: van Tongeren M, Nieuwenhuijsen MJ, Gardiner K, Armstrong B, Vrijheid M, Dolk H, Botting B. A job-exposure matrix fro potential endocrine-disrupting chemicals developed for a study into the association between maternal occupational exposure and hypospadias. Annals of Occupational Hygiene46:465-477,2002.
• Job codes: OC80-UK Categories of Occupations (348 job titles)• Agents(7): pesticides, polychlorinated organic compounds,
phtalates, alkylphenolic compounds, bi-phenolic compounds, heavy metals, other substances (parabens, butylatedhydroxyanisole, phytoestrogens and synthetic steroids).
• Recent application : Ormond G, Nieuwenhuijsen M, Nelson P, Toledano MB, Iszatt N, Geneletti S, Elliott P. Endocrine disruptors in the workplace, hair spray, folates supplementation, and risk of hyspospadias: case-control study. EnvironmentalHealth Perspectives 117:303-307, 2009.
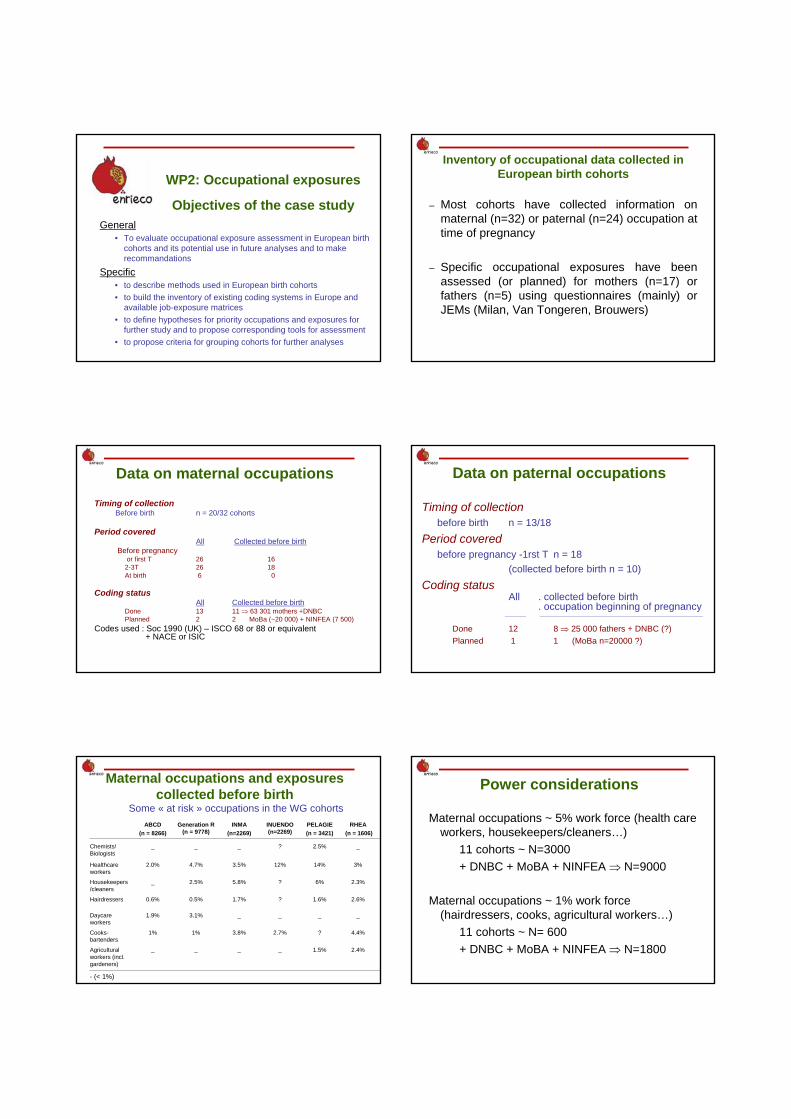
WP2: Occupational exposures
Objectives of the case studyGeneral
• To evaluate occupational exposure assessment in European birthcohorts and its potential use in future analyses and to makerecommandations
Specific• to describe methods used in European birth cohorts• to build the inventory of existing coding systems in Europe and
available job-exposure matrices• to define hypotheses for priority occupations and exposures for
further study and to propose corresponding tools for assessment• to propose criteria for grouping cohorts for further analyses
Inventory of occupational data collected in European birth cohorts
– Most cohorts have collected information on maternal (n=32) or paternal (n=24) occupation attime of pregnancy
– Specific occupational exposures have been assessed (or planned) for mothers (n=17) or fathers (n=5) using questionnaires (mainly) or JEMs (Milan, Van Tongeren, Brouwers)
Data on maternal occupations
Timing of collectionBefore birth n = 20/32 cohorts
Period coveredAll Collected before birth
Before pregnancyor first T 26 16
2-3T 26 18At birth 6 0
Coding statusAll Collected before birth
Done 13 11 ⇒ 63 301 mothers +DNBCPlanned 2 2 MoBa (~20 000) + NINFEA (7 500)
Codes used : Soc 1990 (UK) – ISCO 68 or 88 or equivalent+ NACE or ISIC
Data on paternal occupations
Timing of collectionbefore birth n = 13/18
Period coveredbefore pregnancy -1rst T n = 18
(collected before birth n = 10)Coding status
All . collected before birth. occupation beginning of pregnancy
__________ _____________________________________________________________________________
Done 12 8 ⇒ 25 000 fathers + DNBC (?)Planned 1 1 (MoBa n=20000 ?)
Maternal occupations and exposurescollected before birth
Some « at risk » occupations in the WG cohortsABCD
(n = 8266)Generation R
(n = 9778)INMA
(n=2269)INUENDO (n=2269)
PELAGIE (n = 3421)
RHEA(n = 1606)
Chemists/Biologists
_ _ _ ? 2.5% _
Healthcareworkers
2.0% 4.7% 3.5% 12% 14% 3%
Housekeepers/cleaners
_ 2.5% 5.8% ? 6% 2.3%
Hairdressers 0.6% 0.5% 1.7% ? 1.6% 2.6%
Daycareworkers
1.9% 3.1% _ _ _ _
Cooks-bartenders
1% 1% 3.8% 2.7% ? 4.4%
Agricultural workers (incl. gardeners)
_ _ _ _ 1.5% 2.4%
- (< 1%)
Power considerations
Maternal occupations ~ 5% work force (health care workers, housekeepers/cleaners…)
11 cohorts ~ N=3000+ DNBC + MoBA + NINFEA ⇒ N=9000
Maternal occupations ~ 1% work force (hairdressers, cooks, agricultural workers…)
11 cohorts ~ N= 600+ DNBC + MoBA + NINFEA ⇒ N=1800
What hypotheses do we want to test?Maternal occupations
Service workers (health workers, hairdressers…)° coding problem (check homogeneity of coding and
description of tasks)° power sufficient° heterogeneity of working conditions in Europe
Maternal Occupational exposures° shift work/night work + stress (reference pop?)
from questionnaires in selected cohorts° solvents, cosmetics, endocrine disrupters, cleaning
agents (build an agent-specific country-specificeuropean matrix??)
° MIXTURES ??
What hypotheses do we want to test?
Paternal occupationsSame as women + drivers, electricians, welders….
Occupational exposuresPAH, metals, pesticides, solvents…
Summary of discussions in the workinggroup concerning use of ENRIECO cohorts
– Most cohorts have collected only job title (mother, father)– Assessment of occupational exposures will then have to
rely on self-reports or use of a job-exposure matrix(JEM)
– Experts in occupational exposure assessment did not trust the possibility of building a general european JEM
– Pooling the different exposure questionnaires is difficultbecause of differences in wording and in exposuredefinition
Short-term action of the WG =Meta analysis
– Select a number of occupations considered as potentially « at risk »: health care workers, hairdressers/beauticians, cleaners…
– Identify mothers and fathers with occupations related to these groups in selected cohorts (ISCO 88)
– Perform a meta-analysis of risks for some pregnancyoutcomes (SGA, Premature birth) in these occupations
– Explore the possibility of studying impact of shift work– In parallel, perform the inventory of country-specific
occupational exposures for these occupations
Recommendations for future data collection of occupational data
– Collect job title plus economic activity and if possible name of the company
– Number of hours per week– Include free text description of the task in the
data base– Organize a careful training for coders
Plenary Meeting Utrecht May 26-28 2010 1
Bispebjerg Hospital (1)
WP3 POP Case Study Utrecht MeetingMAY 26-28 2010
POP case-study: 10 CohortsEva GovartsMichael WilhelmUlrich RanftGreet SchoetersMerete EggesboMonica GuxensGunnar ToftCecile ChevrierStephanie VandentorrenRemy Slama
Tomas TrnovecMarieta FernadezFerran BallesterLubiea PalkovicovaPal WeiheVicky PatelarouArja RautioJens Peter BondeMark Nieuwenhuijsen
Bispebjerg Hospital (2)
Plenary Meeting Utrecht May 26-28 2010 3
Overall objective
• To prove the Enrieco conceptTo examine the feasibility using European mother‐child cohorts to obtain additional insight into environmental effects on reproductive outcomes
To examine added value of meta or pooled analyses relative to stand‐alone analyses
Specific objectives
to model exposure-response relations between biological markers of POP-exposure and selected adverse pregnancy outcomes in order to
•Discuss causal inference•Detail dose-response relations, if any•Identify thresholds and no-effect levels, if any•Identify vulnerable subgroups, if any•Examine interactive effects of exposures and characteristics
Why POPs?
POPs were selected for a case-study because:
exposures are ubiquitousbiological markers of exposure are well documented reproductive effects at environmental exposure levels are indicated by several studies but the evidence at current levels is limitedreproductive effects have been documented in rodent studiesPOPs have been measured in several mother-child cohorts (including 10 Enrieco cohorts).
COHORT CHARACTERISTICS
Bispebjerg Hospital (6)
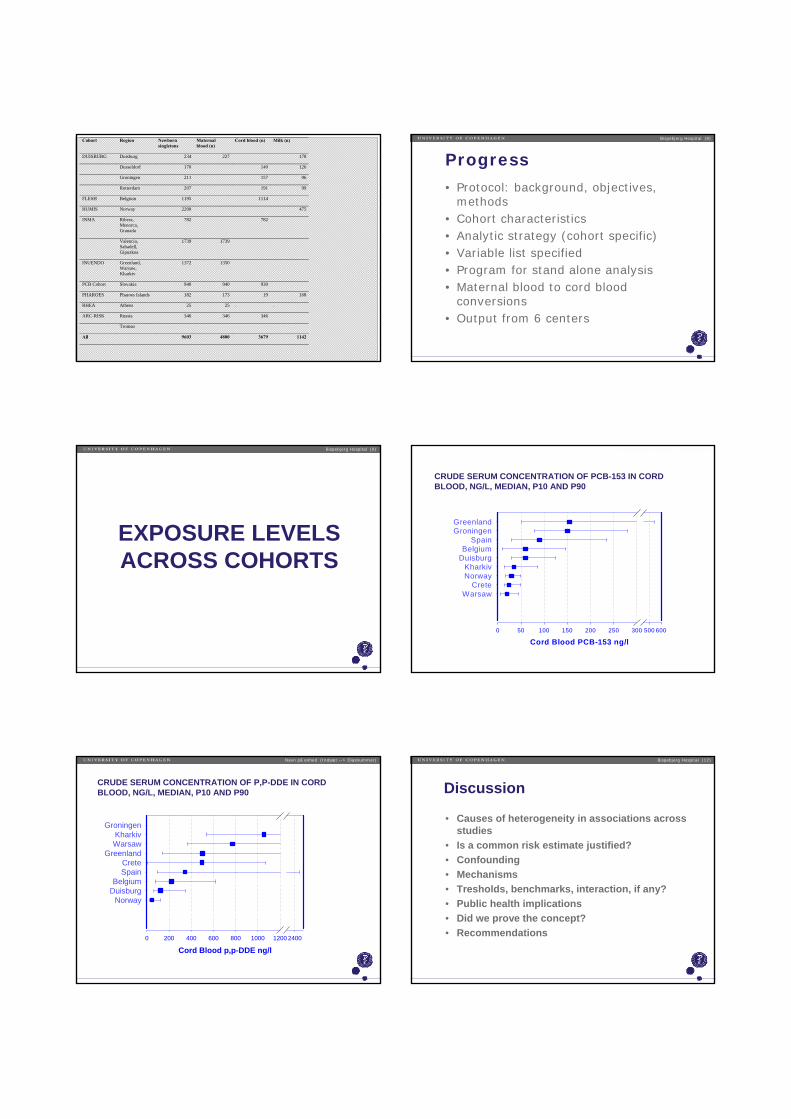
Cohort Region Newborn singletons
Maternal blood (n)
Cord blood (n) Milk (n)
DUISBURG Duisburg 234 227 178
Dusseldorf 170 140 126
Groningen 211 157 96
Rotterdam 207 191 99
FLESH Belgium 1195 1114
HUMIS Norway 2200 475
INMA Ribera, Menorca, Granada
782 782
Valencia, Sabadell, Gipuzkoa
1739 1739
INUENDO Greenland, Warsaw, Kharkiv
1372 1350
PCB Cohort Slovakia 940 940 930
PHAROES Pharoes Islands 182 173 19 168
RHEA Athens 25 25 . .
ARC-RISK Russia 346 346 346
Tromsø
All 9603 4800 3679 1142
Progress
• Protocol: background, objectives, methods
• Cohort characteristics• Analytic strategy (cohort specific)• Variable list specified• Program for stand alone analysis• Maternal blood to cord blood
conversions• Output from 6 centers
Bispebjerg Hospital (8)
EXPOSURE LEVELS ACROSS COHORTS
Bispebjerg Hospital (9)
CRUDE SERUM CONCENTRATION OF PCB-153 IN CORD BLOOD, NG/L, MEDIAN, P10 AND P90
Navn på enhed (Indsæt --> Diasnummer)
Cord Blood PCB-153 ng/l0 50 100 150 200 250 300 500 600
GreenlandGroningen
SpainBelgium
DuisburgKharkivNorway
CreteWarsaw
CRUDE SERUM CONCENTRATION OF P,P-DDE IN CORD BLOOD, NG/L, MEDIAN, P10 AND P90
Navn på enhed (Indsæt --> Diasnummer)
Cord Blood p,p-DDE ng/l0 200 400 600 800 1000 1200 2400
GroningenKharkivWarsaw
GreenlandCreteSpain
BelgiumDuisburg
Norway
Discussion
• Causes of heterogeneity in associations across studies
• Is a common risk estimate justified?• Confounding• Mechanisms• Tresholds, benchmarks, interaction, if any?• Public health implications• Did we prove the concept?• Recommendations
Bispebjerg Hospital (12)
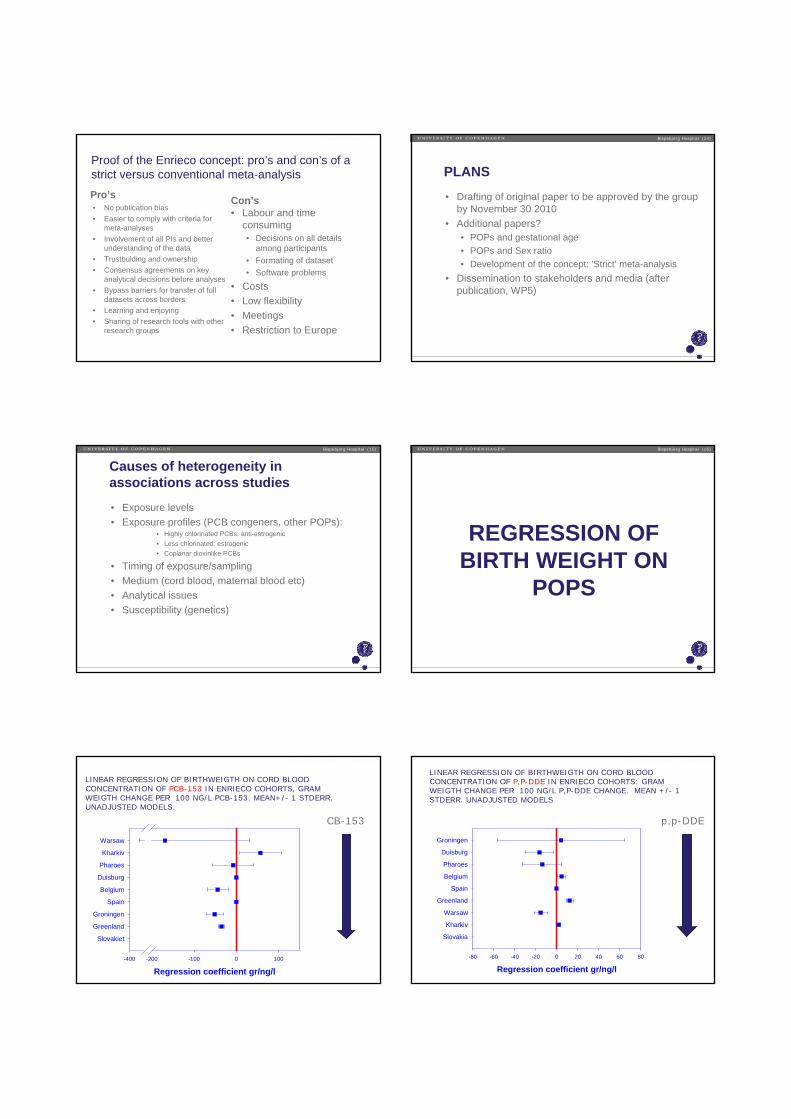
Proof of the Enrieco concept: pro’s and con’s of a strict versus conventional meta-analysisPro’s• No publication bias• Easier to comply with criteria for
meta-analyses• Involvement of all PIs and better
understanding of the data • Trustbulding and ownership• Consensus agreements on key
analytical decisions before analyses• Bypass barriers for transfer of full
datasets across borders• Learning and enjoying• Sharing of research tools with other
research groups
Con’s• Labour and time
consuming• Decisions on all details
among participants• Formating of dataset• Software problems
• Costs• Low flexibility• Meetings• Restriction to Europe
Bispebjerg Hospital (13)
PLANS
• Drafting of original paper to be approved by the group by November 30 2010
• Additional papers?• POPs and gestational age• POPs and Sex ratio• Development of the concept: ’Strict’ meta-analysis
• Dissemination to stakeholders and media (after publication, WP5)
Bispebjerg Hospital (14)
Causes of heterogeneity in associations across studies
• Exposure levels• Exposure profiles (PCB congeners, other POPs):
• Highly chlorinated PCBs: anti-estrogenic• Less chlorinated: estrogenic• Coplanar dioxinlike PCBs
• Timing of exposure/sampling• Medium (cord blood, maternal blood etc)• Analytical issues • Susceptibility (genetics)
Bispebjerg Hospital (15)
REGRESSION OF BIRTH WEIGHT ON
POPS
Bispebjerg Hospital (16)
Navn på enhed (Indsæt --> Diasnummer)
LINEAR REGRESSION OF BIRTHWEIGTH ON CORD BLOOD CONCENTRATION OF PCB-153 IN ENRIECO COHORTS, GRAM WEIGTH CHANGE PER 100 NG/L PCB-153. MEAN+/- 1 STDERR. UNADJUSTED MODELS.
Regression coefficient gr/ng/l-400 -200 -100 0 100
Slovakiet
Greenland
Groningen
Spain
Belgium
Duisburg
Pharoes
Kharkiv
Warsaw
CB-153
Navn på enhed (Indsæt --> Diasnummer)
LINEAR REGRESSION OF BIRTHWEIGTH ON CORD BLOOD CONCENTRATION OF P,P-DDE IN ENRIECO COHORTS: GRAM WEIGTH CHANGE PER 100 NG/L P,P-DDE CHANGE. MEAN +/- 1 STDERR. UNADJUSTED MODELS
Regression coefficient gr/ng/l-80 -60 -40 -20 0 20 40 60 80
Slovakia
Kharkiv
Warsaw
Greenland
Spain
Belgium
Pharoes
Duisburg
Groningen
p,p-DDE
Criteria for data quality for each cohort?
• Missing values?• …• ….
Bispebjerg Hospital (19)
Achievements since Munich
• Documentation of conversion factors
• Update of the program for stand-alone statistical analyses
• Translation of SAS to SPSS analyses
• Update of analyses each cohort• Preliminary aggregation of
findings
Bispebjerg Hospital (20)
Agenda POP case study group meeting 26.5.2010, 11.00-13.00
• Agenda and minutes (decisions)• Achievements since the Munich
meeting May 3-4• Round table: Status for stand
alone analyses• Review of preliminary findings
and plenary presentation• What can explain heterogeneity?• Criteria for data quality?
Bispebjerg Hospital (21)
11/06/2010
WP3: Case Study of POPsAnalytical strategy
e.g. FLemish Environment & Health Study(2002-2004)
Eva Govarts
11/06/2010 2© 2010, VITO NV
Specific Objectives
to model exposure-response associations between biological markers of POP-exposure to selected adverse pregnancy outcomes in order to
» Discuss causal inference» Detail dose-response relations, if any» Identify thresholds and no-effect levels, if any» Identify vulnerable subgroups, if any» Examine interactive effects of exposures and
characteristics
11/06/2010 3© 2010, VITO NV
Selected POPs and health outcomes
» Selected POPso PCB153o p,p’-DDE
» Selected Health Outcomeso Birth weighto Small for Gestational Age (SGA)
11/06/2010 4© 2010, VITO NV
Harmonization POPs and health outcomes» POPs
o Selected matrix: cord blood• Conversion of maternal blood to cord blood
PCB153 * 0.2 and DDE * 0.23• Conversion of breast milk to cord blood
PCB153 *4.5 * 0.2 and DDE * 4.8 * 0.23
o Lipid unadjustedo Unit: ng/Lo Values below LOD replaced by
• LOD/ √2 if < 50% below LOD• LOD/2 if > 50% below LOD
» Health outcomeso Small for Gestational Age (SGA)
Defined as birth weight less than the 10th percentile of birth weight for each week of pregnancy defined by external data
11/06/2010 5© 2010, VITO NV
Selection and harmonization covariates
» Gestational age» Region» Socio-economic status» Maternal age» Parity» Gender of the baby» BMI mother» Smoking during pregnancy» Ethnicity» Maternal height» Time of sampling
11/06/2010 6© 2010, VITO NV
Descriptive statistics: POPs
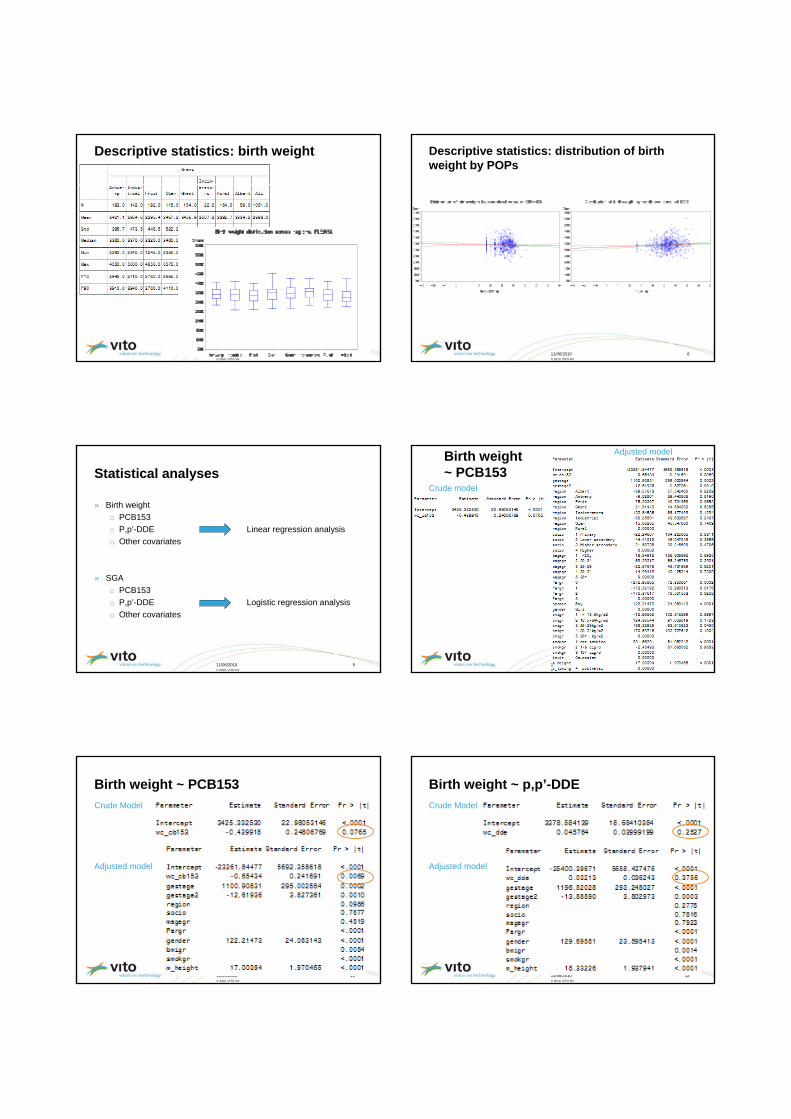
11/06/2010 7© 2010, VITO NV
Descriptive statistics: birth weight
11/06/2010 8© 2010, VITO NV
Descriptive statistics: distribution of birth weight by POPs
11/06/2010 9© 2010, VITO NV
Statistical analyses
» Birth weighto PCB153o P,p’-DDE Linear regression analysiso Other covariates
» SGAo PCB153o P,p’-DDE Logistic regression analysiso Other covariates
11/06/2010 10© 2010, VITO NV
Birth weight ~ PCB153
Adjusted model
Crude model
11/06/2010 11© 2010, VITO NV
Birth weight ~ PCB153Crude Model
Adjusted model
11/06/2010 12© 2010, VITO NV
Birth weight ~ p,p’-DDECrude Model
Adjusted model
11/06/2010 13© 2010, VITO NV
Effect modification
» POP interaction with gendero PCB153: interaction with gender not significant (p = 0.48)o p,p’-DDE: interaction with gender not significant (p = 0.31)
» POP interaction with maternal ever smokingo PCB153: interaction with smoking not significant (p = 0.47)o p,p’-DDE: interaction with smoking not significant (p = 0.45)
» POPs interaction: not significant (p=0.76)
11/06/2010 14© 2010, VITO NV
Sensitivity analysis
» Lipid adjustment o f_PCB153: stays negatively significanto f_DDE: stays not significant
» Loglinear modelo lnPCB153: becomes borderline not significant (p=0.07)o lnDDE: stays not significant
11/06/2010 15© 2010, VITO NV
Meta-analyses
1
U N I V E R S I T Ä T S M E D I Z I N B E R L I N
ENRIECO, Second Workshop, Utrecht May 2010
WP 5: Process and current status
Cynthia Hohmann, Thomas Keil
WP5 - Aims
To examine associations between:
Indoor environmental exposures (a. dampness/mould; b. second hand tobacco smoke)
Asthma & allergic diseases in children
Using the original raw data from European birth cohorts focused on asthma and allergies.
ENRIECO second workshop, May 2010
WP5- Aims, Why now?
• Allergic diseases most common chronic diseases occurring from infancy to adulthood
• Most evidence on indoor environment exposure and asthma/allergies comes from cross-sectional studies
=> We need data from long-term birth cohort studies
ENRIECO second workshop, May 2010
WP5 - Process
1. Preparation of protocols2. Database building (data collection and
harmonization of data).3. Combined analyses to obtain exposure-response
functions (through 3 case studies).
ENRIECO second workshop, May 2010
WP5 – Preparation of protocols
1. Deliverable Number 6• Protocol for database building
2. Deliverable Number 7• Protocol for indoor exposures (ETS and dampness) and
allergy and asthma case study
3. Annual activity report
4. Deliverable 2 manuscripts (Nov 2010)
ENRIECO second workshop, May 2010
√
√
√
WP5 - Process
1. Preparation of protocols2. Database building (data collection and
harmonization of data).3. Combined analyses to obtain exposure-response
functions (through 3 case studies).
ENRIECO second workshop, May 2010
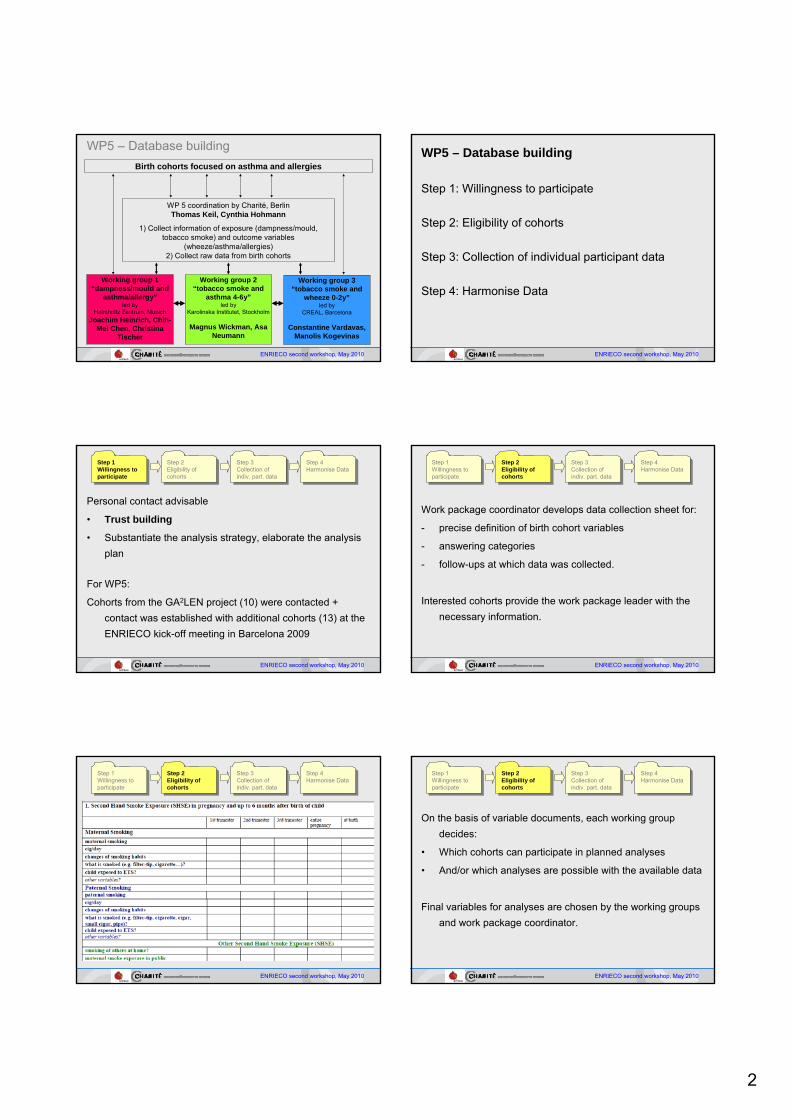
2
WP5 – Database building
WP 5 coordination by Charité, Berlin Thomas Keil, Cynthia Hohmann
1) Collect information of exposure (dampness/mould, tobacco smoke) and outcome variables
(wheeze/asthma/allergies) 2) Collect raw data from birth cohorts
Birth cohorts focused on asthma and allergies
ENRIECO second workshop, May 2010
Working group 3“tobacco smoke and
wheeze 0-2y”led by
CREAL, Barcelona
Constantine Vardavas, Manolis Kogevinas
Working group 2“tobacco smoke and
asthma 4-6y”led by
Karolinska Institutet, Stockholm
Magnus Wickman, AsaNeumann
Working group 1 “dampness/mould and
asthma/allergy”led by
Helmholtz Zentrum, MunichJoachim Heinrich, Chih-
Mei Chen, Christina Tischer
WP5 – Database building
Step 1: Willingness to participate
Step 2: Eligibility of cohorts
Step 3: Collection of individual participant data
Step 4: Harmonise Data
ENRIECO second workshop, May 2010
Personal contact advisable
• Trust building
• Substantiate the analysis strategy, elaborate the analysis plan
For WP5:
Cohorts from the GA2LEN project (10) were contacted + contact was established with additional cohorts (13) at the ENRIECO kick-off meeting in Barcelona 2009
ENRIECO second workshop, May 2010
Step 1Willingness to participate
Step 1Willingness to participate
Step 2Eligibility of cohorts
Step 2Eligibility of cohorts
Step 3 Collection of indiv. part. data
Step 3 Collection of indiv. part. data
Step 4 Harmonise Data
Step 4 Harmonise Data
Work package coordinator develops data collection sheet for:
- precise definition of birth cohort variables
- answering categories
- follow-ups at which data was collected.
Interested cohorts provide the work package leader with the necessary information.
ENRIECO second workshop, May 2010
Step 1Willingness to participate
Step 1Willingness to participate
Step 2Eligibility of cohorts
Step 2Eligibility of cohorts
Step 3 Collection of indiv. part. data
Step 3 Collection of indiv. part. data
Step 4 Harmonise Data
Step 4 Harmonise Data
ENRIECO second workshop, May 2010
Step 1Willingness to participate
Step 1Willingness to participate
Step 2Eligibility of cohorts
Step 2Eligibility of cohorts
Step 3 Collection of indiv. part. data
Step 3 Collection of indiv. part. data
Step 4 Harmonise Data
Step 4 Harmonise Data
On the basis of variable documents, each working group decides:
• Which cohorts can participate in planned analyses
• And/or which analyses are possible with the available data
Final variables for analyses are chosen by the working groups and work package coordinator.
ENRIECO second workshop, May 2010
Step 1Willingness to participate
Step 1Willingness to participate
Step 2Eligibility of cohorts
Step 2Eligibility of cohorts
Step 3 Collection of indiv. part. data
Step 3 Collection of indiv. part. data
Step 4 Harmonise Data
Step 4 Harmonise Data
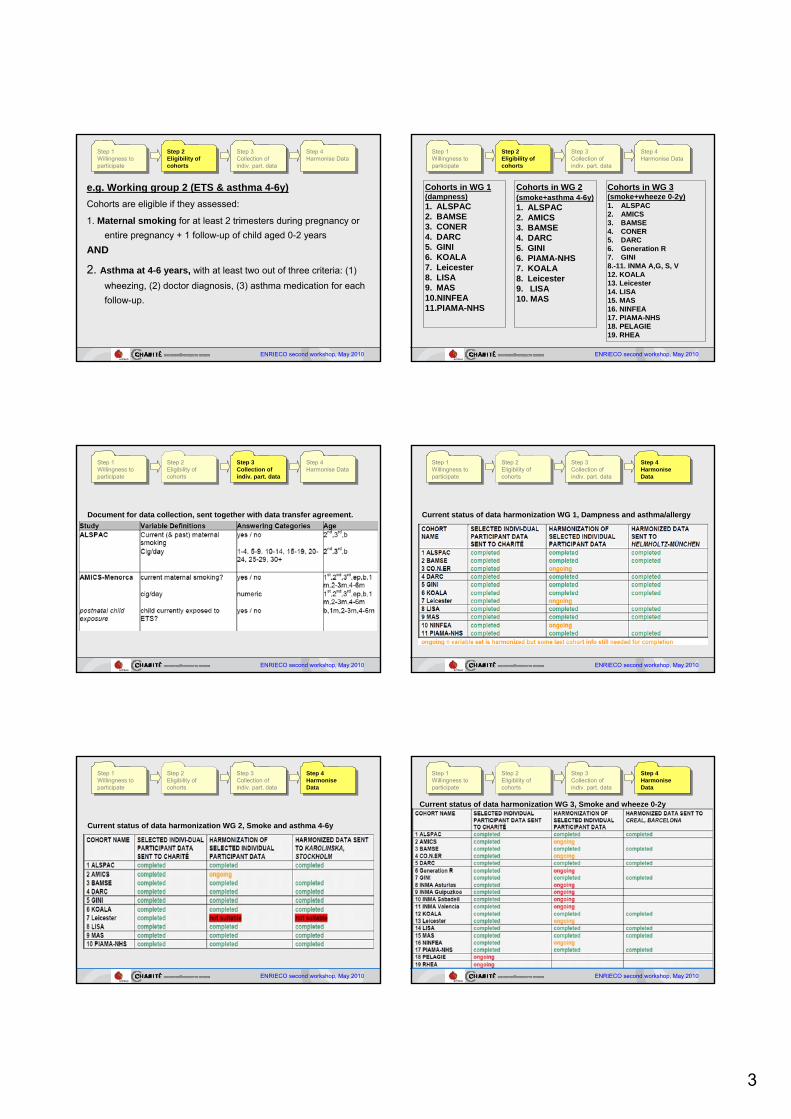
3
e.g. Working group 2 (ETS & asthma 4-6y)Cohorts are eligible if they assessed:
1. Maternal smoking for at least 2 trimesters during pregnancy or entire pregnancy + 1 follow-up of child aged 0-2 years
AND
2. Asthma at 4-6 years, with at least two out of three criteria: (1) wheezing, (2) doctor diagnosis, (3) asthma medication for each follow-up.
ENRIECO second workshop, May 2010
Step 1Willingness to participate
Step 1Willingness to participate
Step 2Eligibility of cohorts
Step 2Eligibility of cohorts
Step 3 Collection of indiv. part. data
Step 3 Collection of indiv. part. data
Step 4 Harmonise Data
Step 4 Harmonise Data
ENRIECO second workshop, May 2010
Step 1Willingness to participate
Step 1Willingness to participate
Step 2Eligibility of cohorts
Step 2Eligibility of cohorts
Step 3 Collection of indiv. part. data
Step 3 Collection of indiv. part. data
Step 4 Harmonise Data
Step 4 Harmonise Data
Cohorts in WG 1 (dampness)1. ALSPAC2. BAMSE3. CONER4. DARC5. GINI6. KOALA7. Leicester8. LISA9. MAS10.NINFEA11.PIAMA-NHS
Cohorts in WG 2 (smoke+asthma 4-6y)1. ALSPAC2. AMICS3. BAMSE4. DARC5. GINI6. PIAMA-NHS7. KOALA8. Leicester9. LISA10. MAS
Cohorts in WG 3(smoke+wheeze 0-2y)1. ALSPAC2. AMICS3. BAMSE4. CONER5. DARC6. Generation R7. GINI8.-11. INMA A,G, S, V 12. KOALA13. Leicester14. LISA15. MAS16. NINFEA17. PIAMA-NHS18. PELAGIE19. RHEA
ENRIECO second workshop, May 2010
Step 1Willingness to participate
Step 1Willingness to participate
Step 2Eligibility of cohorts
Step 2Eligibility of cohorts
Step 3 Collection of indiv. part. data
Step 3 Collection of indiv. part. data
Step 4 Harmonise Data
Step 4 Harmonise Data
Document for data collection, sent together with data transfer agreement.
ENRIECO second workshop, May 2010
Step 1Willingness to participate
Step 1Willingness to participate
Step 2Eligibility of cohorts
Step 2Eligibility of cohorts
Step 3 Collection of indiv. part. data
Step 3 Collection of indiv. part. data
Step 4 HarmoniseData
Step 4 HarmoniseData
Current status of data harmonization WG 1, Dampness and asthma/allergy
ENRIECO second workshop, May 2010
Step 1Willingness to participate
Step 1Willingness to participate
Step 2Eligibility of cohorts
Step 2Eligibility of cohorts
Current status of data harmonization WG 2, Smoke and asthma 4-6y
Step 4 HarmoniseData
Step 4 HarmoniseData
Step 3 Collection of indiv. part. data
Step 3 Collection of indiv. part. data
ENRIECO second workshop, May 2010
Step 1Willingness to participate
Step 1Willingness to participate
Step 2Eligibility of cohorts
Step 2Eligibility of cohorts
Current status of data harmonization WG 3, Smoke and wheeze 0-2y
Step 3 Collection of indiv. part. data
Step 3 Collection of indiv. part. data
Step 4 HarmoniseData
Step 4 HarmoniseData
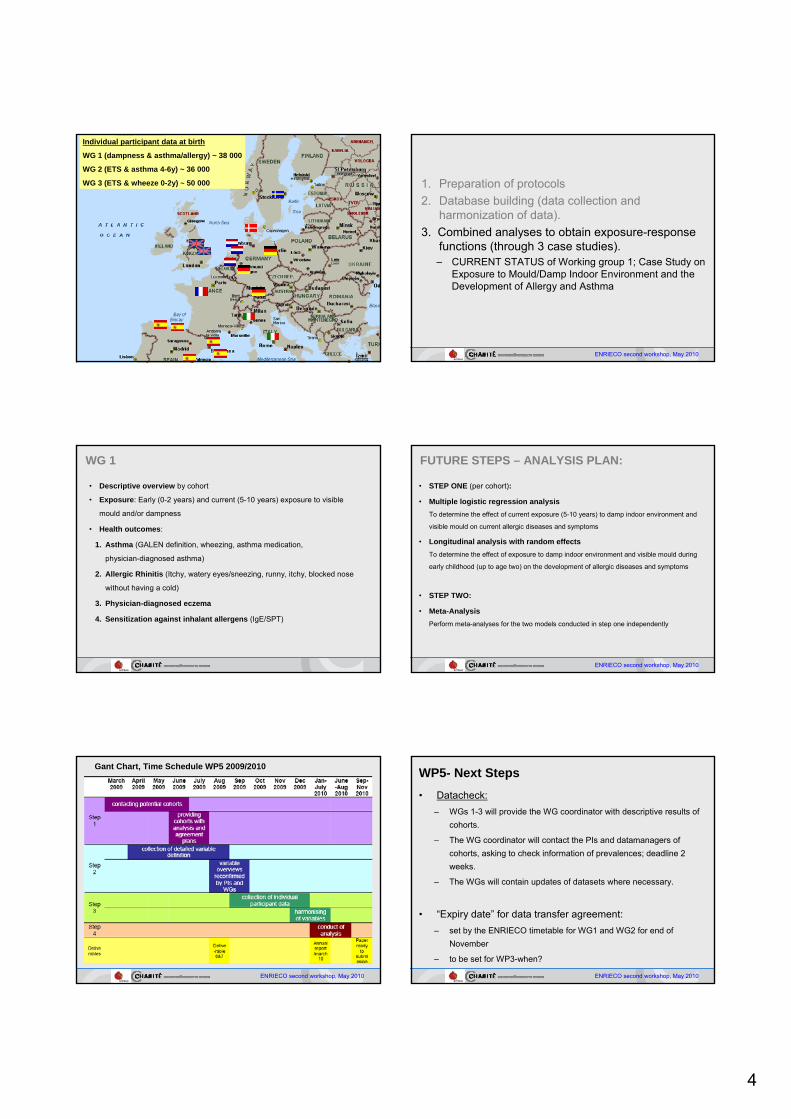
4
Individual participant data at birth
WG 1 (dampness & asthma/allergy) ~ 38 000
WG 2 (ETS & asthma 4-6y) ~ 36 000
WG 3 (ETS & wheeze 0-2y) ~ 50 000
ENRIECO second workshop, May 2010
1. Preparation of protocols2. Database building (data collection and
harmonization of data).3. Combined analyses to obtain exposure-response
functions (through 3 case studies).– CURRENT STATUS of Working group 1; Case Study on
Exposure to Mould/Damp Indoor Environment and the Development of Allergy and Asthma
• Descriptive overview by cohort
• Exposure: Early (0-2 years) and current (5-10 years) exposure to visible
mould and/or dampness
• Health outcomes:
1. Asthma (GALEN definition, wheezing, asthma medication,
physician-diagnosed asthma)
2. Allergic Rhinitis (Itchy, watery eyes/sneezing, runny, itchy, blocked nose
without having a cold)
3. Physician-diagnosed eczema
4. Sensitization against inhalant allergens (IgE/SPT)
WG 1 FUTURE STEPS – ANALYSIS PLAN:
• STEP ONE (per cohort):
• Multiple logistic regression analysisTo determine the effect of current exposure (5-10 years) to damp indoor environment and
visible mould on current allergic diseases and symptoms
• Longitudinal analysis with random effectsTo determine the effect of exposure to damp indoor environment and visible mould during
early childhood (up to age two) on the development of allergic diseases and symptoms
• STEP TWO:
• Meta-AnalysisPerform meta-analyses for the two models conducted in step one independently
ENRIECO second workshop, May 2010
ENRIECO second workshop, May 2010
Gant Chart, Time Schedule WP5 2009/2010 WP5- Next Steps• Datacheck:
– WGs 1-3 will provide the WG coordinator with descriptive results of cohorts.
– The WG coordinator will contact the PIs and datamanagers of cohorts, asking to check information of prevalences; deadline 2 weeks.
– The WGs will contain updates of datasets where necessary.
• “Expiry date” for data transfer agreement: – set by the ENRIECO timetable for WG1 and WG2 for end of
November
– to be set for WP3-when?
ENRIECO second workshop, May 2010
WP3: Health outcomes
Jens‐Peter Bonde, Marie‐Aline Charles, Thomas Keil, Manolis Kogevinas, Jordi Sunyer, Rémy SlamaInserm (National Institute of Health and Medical Research)
Joint research Center Inserm – Univ. J Fourier Grenoble (Institut Albert Bonniot)Team “Environmental Epidemiology applied to Fecundity and Reproduction”,
Grenoble
enrieco 2nd workshopUtrecht, May 2010 WP3: Health outcomes
Outline of this presentation
• Aims, coverage, and structure of the work package
• Outline of the general protocol
• Deliverables
• Preliminary results of the working groups
WP3: Health outcomes
Background• Many European birth cohorts did collect information on
health outcomes and environmental exposures
• For some rather rare birth outcomes, environmental exposures or rather small birth cohorts, projects gathering several cohorts might allow provide more relevant results than individual analyses of cohorts
• Need for further identification of relevant studies on health effects of environmental factors that could be performed on the existing cohorts
• Probable need for recommendations in terms of standardisation of methods to assess health outcomes in future cohorts and in the future follow‐up of existing cohorts
WP3: Health outcomes
Overall aim of the work package
To evaluate existing health information of the birth cohorts included in ENRIECO
and to make recommendations for further analyses.
WP3: Health outcomes
Specific aims1) to develop protocols for the evaluation of existing information on
health outcomes in terms of availability, quality and potential use
2) to set up a database with the tools and methods that have been used to assess health outcomes.
3) to discuss the feasibility to study environmental influences on specific health outcomes little or not considered so far in studies based on single cohorts, such as childhood cancer and congenitalmalformations.
4) to make recommendations for potential further use of methods and tools in cohorts where they do not exist or where there has been insufficient use.
5) where possible, to harmonize health outcome information for future environment and health analyses in the cohorts
create a minimum set: select the priorities, standardize methods, provide tools, create methods
6) To conduct a case‐study on Persistent Organic Pollutants (POPs) and reproductive outcomes or children’s health. (not covered here)
WP3: Health outcomes
What we expect from Enrieco workshop
Have some feedback on our protocol and philosophy of ourapproach
Have your comments on our preliminary results
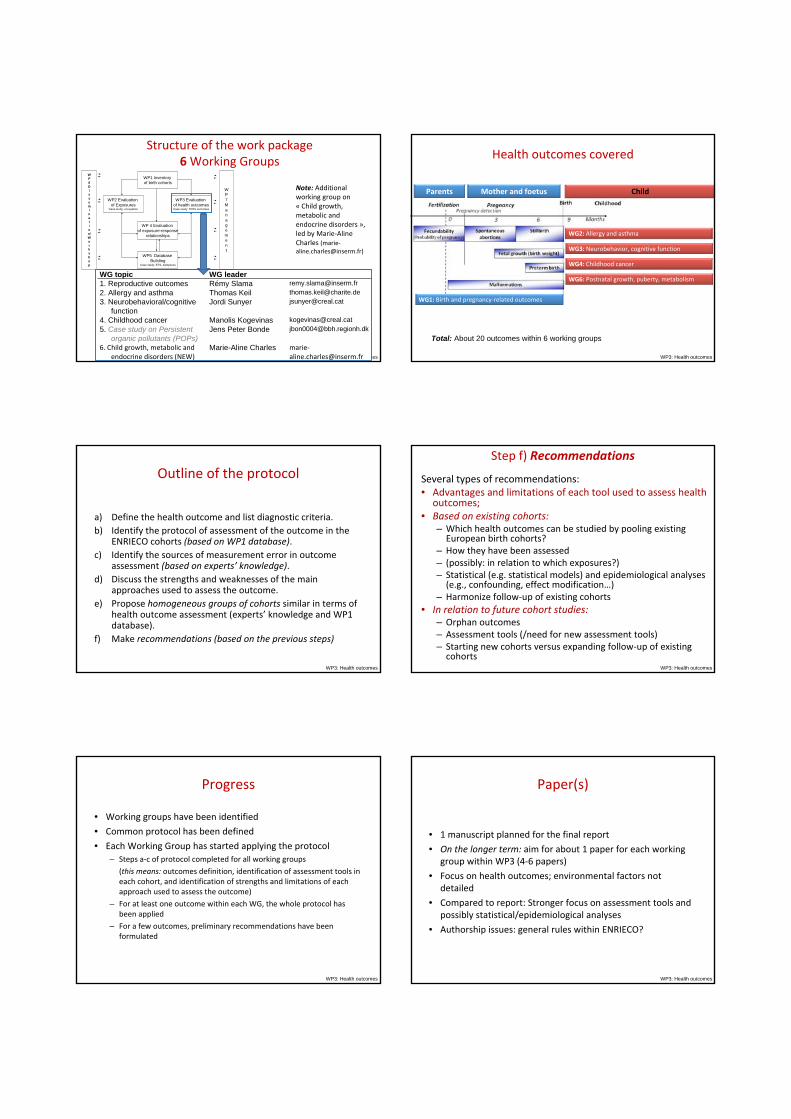
WP3: Health outcomes
WG topic WG leader1. Reproductive outcomes Rémy Slama [email protected]. Allergy and asthma Thomas Keil [email protected]. Neurobehavioral/cognitive
functionJordi Sunyer [email protected]
4. Childhood cancer Manolis Kogevinas [email protected]. Case study on Persistent
organic pollutants (POPs)Jens Peter Bonde [email protected]
6. Child growth, metabolic and endocrine disorders (NEW)
Marie-Aline Charles marie‐[email protected]
WP1 Inventoryof birth cohorts
WP2 Evaluationof Exposures
Case study: occupation
WP3 Evaluationof health outcomesCase study: POPs outcomes
WP5 DatabaseBuilding
Case study: ETS, dampness
WP 4 Evaluationof exposure-response
relationships
WP7Management
WP6Dissemination/Workshop
Structure of the work package6Working Groups
Note: Additional working group on « Child growth, metabolic and endocrine disorders », led by Marie‐Aline Charles (marie‐[email protected])
WP3: Health outcomes
Health outcomes covered
Parents Mother and foetus Child
Total: About 20 outcomes within 6 working groups
WG4: Childhood cancer
WG6: Postnatal growth, puberty, metabolism
WG3: Neurobehavior, cognitive function
WG2: Allergy and asthma
WG1: Birth and pregnancy‐related outcomes
WP3: Health outcomes
Outline of the protocol
a) Define the health outcome and list diagnostic criteria.b) Identify the protocol of assessment of the outcome in the
ENRIECO cohorts (based on WP1 database).c) Identify the sources of measurement error in outcome
assessment (based on experts’ knowledge).d) Discuss the strengths and weaknesses of the main
approaches used to assess the outcome.e) Propose homogeneous groups of cohorts similar in terms of
health outcome assessment (experts’ knowledge and WP1 database).
f) Make recommendations (based on the previous steps)
WP3: Health outcomes
Step f) Recommendations
Several types of recommendations:• Advantages and limitations of each tool used to assess health
outcomes;• Based on existing cohorts:
– Which health outcomes can be studied by pooling existing European birth cohorts?
– How they have been assessed– (possibly: in relation to which exposures?)– Statistical (e.g. statistical models) and epidemiological analyses (e.g., confounding, effect modification…)
– Harmonize follow‐up of existing cohorts• In relation to future cohort studies:
– Orphan outcomes– Assessment tools (/need for new assessment tools)– Starting new cohorts versus expanding follow‐up of existing cohorts
WP3: Health outcomes
Progress
• Working groups have been identified
• Common protocol has been defined
• Each Working Group has started applying the protocol– Steps a‐c of protocol completed for all working groups
(this means: outcomes definition, identification of assessment tools in each cohort, and identification of strengths and limitations of each approach used to assess the outcome)
– For at least one outcome within each WG, the whole protocol has been applied
– For a few outcomes, preliminary recommendations have been formulated
WP3: Health outcomes
Paper(s)
• 1 manuscript planned for the final report
• On the longer term: aim for about 1 paper for each working group within WP3 (4‐6 papers)
• Focus on health outcomes; environmental factors not detailed
• Compared to report: Stronger focus on assessment tools and possibly statistical/epidemiological analyses
• Authorship issues: general rules within ENRIECO?
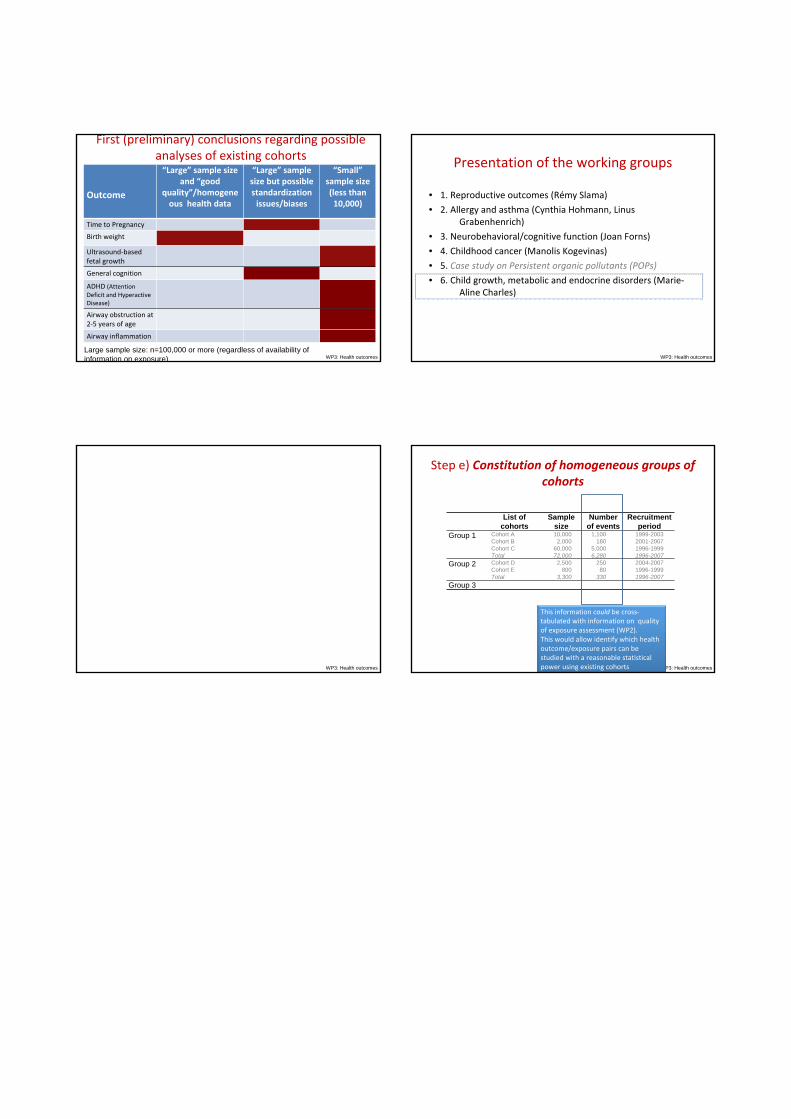
WP3: Health outcomes
First (preliminary) conclusions regarding possible analyses of existing cohorts
Outcome
“Large” sample size and “good
quality”/homogeneous health data
“Large” sample size but possible standardization issues/biases
“Small”sample size (less than 10,000)
Time to Pregnancy
Birth weight
Ultrasound‐based fetal growth
General cognition
ADHD (Attention Deficit and Hyperactive Disease)
Airway obstruction at 2‐5 years of age
Airway inflammation
Large sample size: n=100,000 or more (regardless of availability of information on exposure) WP3: Health outcomes
Presentation of the working groups
• 1. Reproductive outcomes (Rémy Slama)
• 2. Allergy and asthma (Cynthia Hohmann, LinusGrabenhenrich)
• 3. Neurobehavioral/cognitive function (Joan Forns)
• 4. Childhood cancer (Manolis Kogevinas)
• 5. Case study on Persistent organic pollutants (POPs)
• 6. Child growth, metabolic and endocrine disorders (Marie‐Aline Charles)
WP3: Health outcomes WP3: Health outcomes
Step e) Constitution of homogeneous groups of cohorts
List of cohorts
Sample size
Number of events
Recruitment period
Group 1 Cohort ACohort BCohort CTotal
10,0002,000
60,00072,000
1,100180
5,0006,280
1999-20032001-20071996-19991996-2007
Group 2 Cohort DCohort ETotal
2,500800
3,300
25080
330
2004-20071996-19991996-2007
Group 3
This information could be cross‐tabulated with information on quality of exposure assessment (WP2). This would allow identify which health outcome/exposure pairs can be studied with a reasonable statistical power using existing cohorts
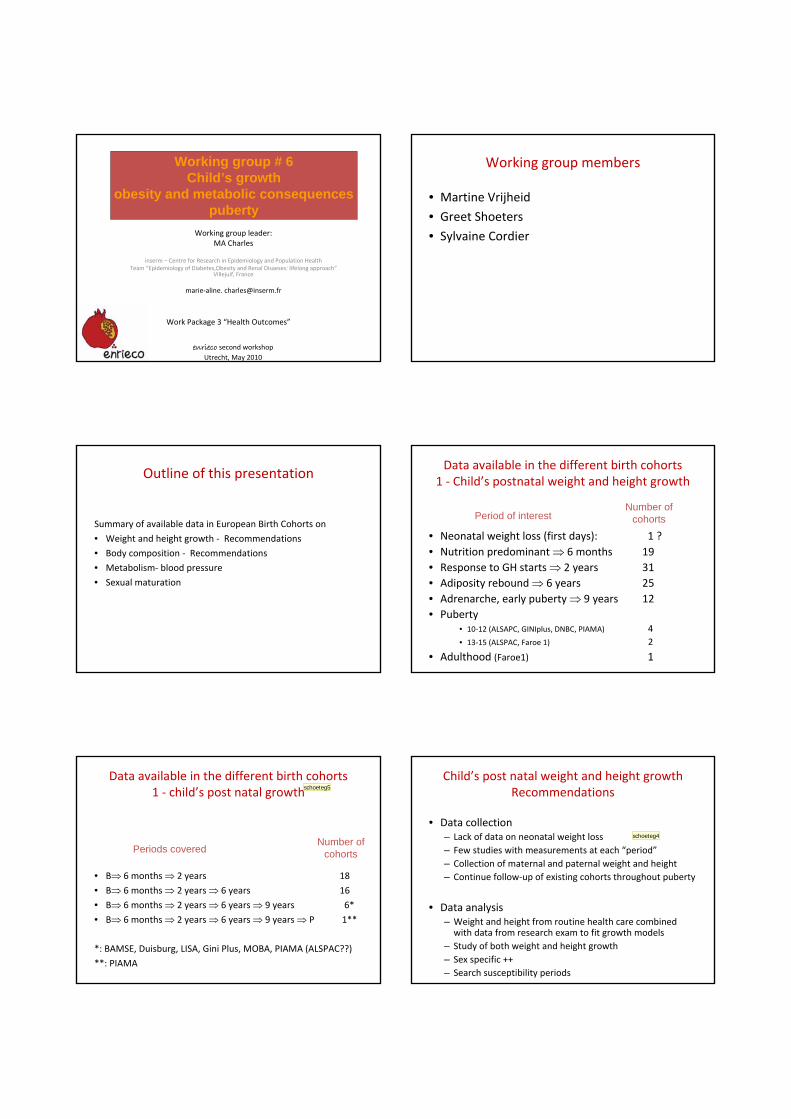
Work Package 3 “Health Outcomes”
enrieco second workshopUtrecht, May 2010
Working group leader: MA Charles
inserm – Centre for Research in Epidemiology and Population HealthTeam “Epidemiology of Diabetes,Obesity and Renal Disaeses: lifelong approach”
Villejuif, France
marie‐aline. [email protected]
Working group # 6Child’s growth
obesity and metabolic consequencespuberty
Working group members
• Martine Vrijheid
• Greet Shoeters
• Sylvaine Cordier
Outline of this presentation
Summary of available data in European Birth Cohorts on
• Weight and height growth ‐ Recommendations
• Body composition ‐ Recommendations
• Metabolism‐ blood pressure
• Sexual maturation
Data available in the different birth cohorts1 ‐ Child’s postnatal weight and height growth
• Neonatal weight loss (first days): 1 ?• Nutrition predominant ⇒ 6 months 19• Response to GH starts ⇒ 2 years 31• Adiposity rebound ⇒ 6 years 25• Adrenarche, early puberty ⇒ 9 years 12• Puberty
• 10‐12 (ALSAPC, GINIplus, DNBC, PIAMA) 4• 13‐15 (ALSPAC, Faroe 1) 2
• Adulthood (Faroe1) 1
Period of interestNumber of
cohorts
Data available in the different birth cohorts1 ‐ child’s post natal growth
• B⇒ 6 months ⇒ 2 years 18
• B⇒ 6 months ⇒ 2 years ⇒ 6 years 16
• B⇒ 6 months ⇒ 2 years ⇒ 6 years ⇒ 9 years 6*
• B⇒ 6 months ⇒ 2 years ⇒ 6 years ⇒ 9 years ⇒ P 1**
*: BAMSE, Duisburg, LISA, Gini Plus, MOBA, PIAMA (ALSPAC??)
**: PIAMA
Periods coveredNumber of
cohorts
schoeteg5
Child’s post natal weight and height growthRecommendations
• Data collection– Lack of data on neonatal weight loss– Few studies with measurements at each “period”– Collection of maternal and paternal weight and height– Continue follow‐up of existing cohorts throughout puberty
• Data analysis– Weight and height from routine health care combined with data from research exam to fit growth models
– Study of both weight and height growth– Sex specific ++– Search susceptibility periods
schoeteg4

Διαφάνεια 5
schoeteg5 you mean lenghth, weight, BMI?schoeteg; 24/05/2010
Διαφάνεια 6
schoeteg4 comparison with existing national ref curves of weight, height, BMI would be valuable report deviations from ref curvesschoeteg; 24/05/2010
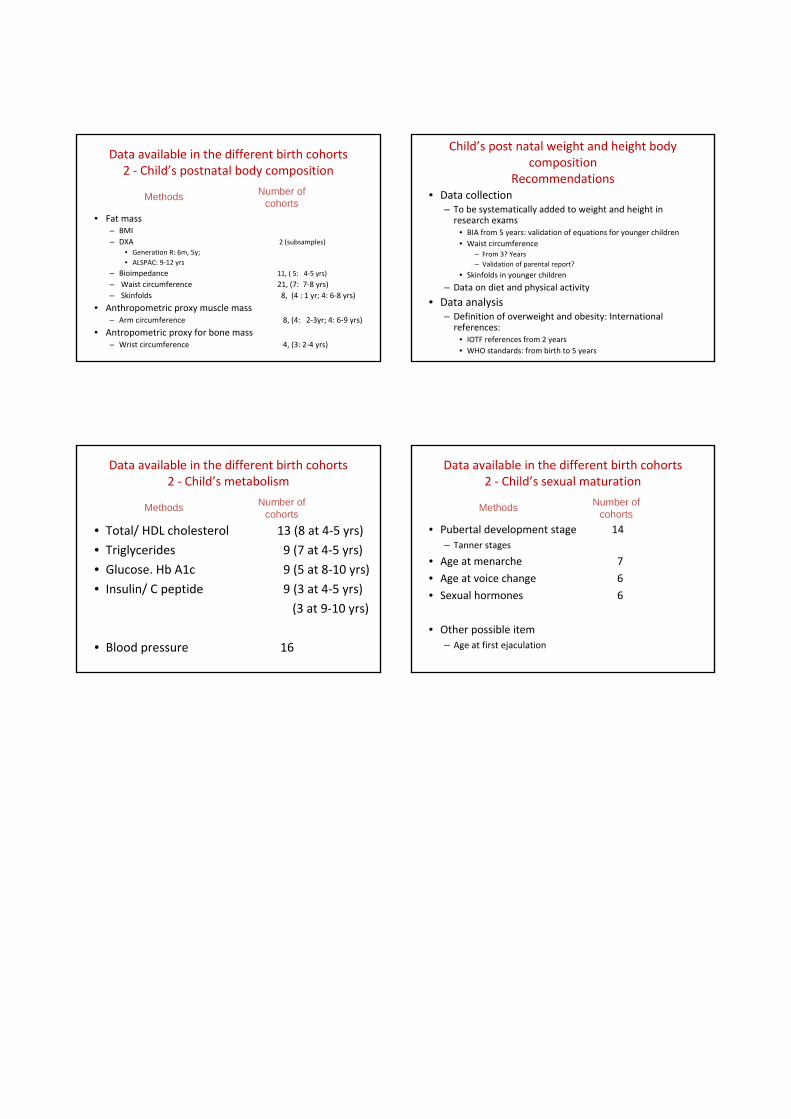
Data available in the different birth cohorts2 ‐ Child’s postnatal body composition
• Fat mass– BMI– DXA 2 (subsamples)
• Generation R: 6m, 5y; • ALSPAC: 9‐12 yrs
– Bioimpedance 11, ( 5: 4‐5 yrs)
– Waist circumference 21, (7: 7‐8 yrs)– Skinfolds 8, (4 : 1 yr; 4: 6‐8 yrs)
• Anthropometric proxy muscle mass– Arm circumference 8, (4: 2‐3yr; 4: 6‐9 yrs)
• Antropometric proxy for bone mass– Wrist circumference 4, (3: 2‐4 yrs)
Methods Number ofcohorts
Child’s post natal weight and height body composition
Recommendations• Data collection
– To be systematically added to weight and height in research exams
• BIA from 5 years: validation of equations for younger children• Waist circumference
– From 3? Years– Validation of parental report?
• Skinfolds in younger children
– Data on diet and physical activity
• Data analysis– Definition of overweight and obesity: International references:
• IOTF references from 2 years• WHO standards: from birth to 5 years
Data available in the different birth cohorts2 ‐ Child’s metabolism
• Total/ HDL cholesterol 13 (8 at 4‐5 yrs)
• Triglycerides 9 (7 at 4‐5 yrs)
• Glucose. Hb A1c 9 (5 at 8‐10 yrs)
• Insulin/ C peptide 9 (3 at 4‐5 yrs)
(3 at 9‐10 yrs)
• Blood pressure 16
Methods Number ofcohorts
Data available in the different birth cohorts2 ‐ Child’s sexual maturation
• Pubertal development stage 14– Tanner stages
• Age at menarche 7
• Age at voice change 6
• Sexual hormones 6
• Other possible item– Age at first ejaculation
Methods Number ofcohorts
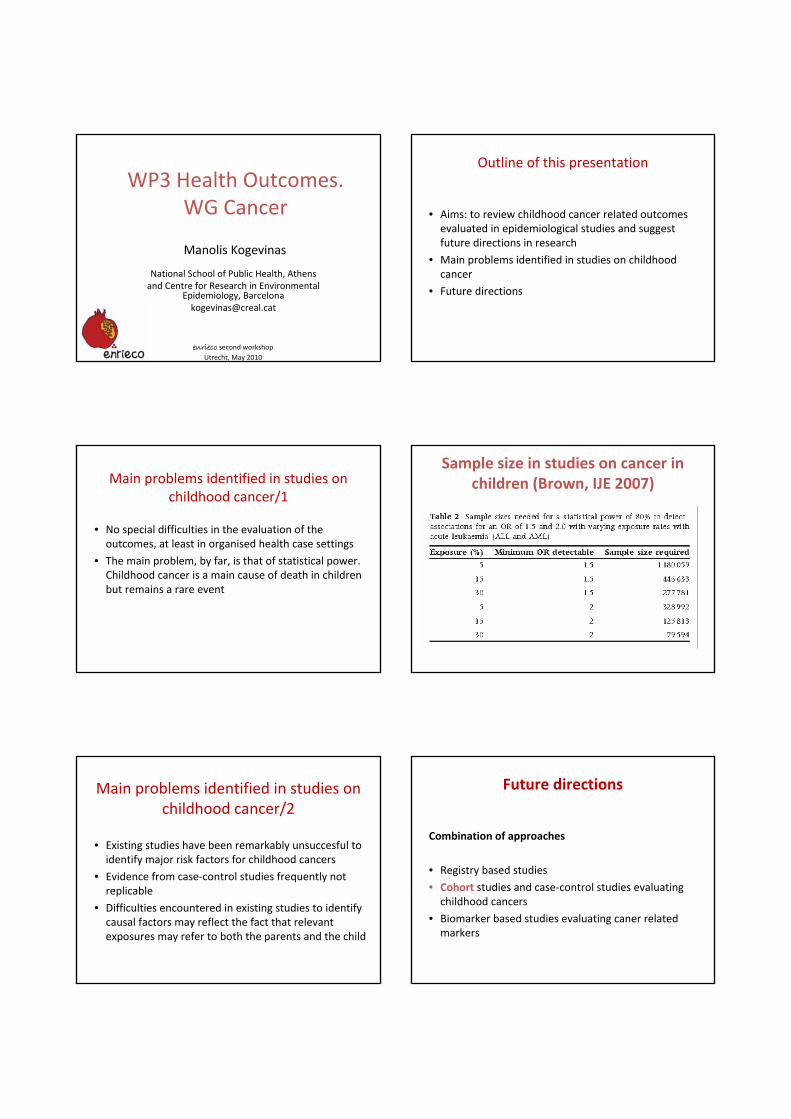
enrieco second workshopUtrecht, May 2010
Manolis Kogevinas
National School of Public Health, Athens and Centre for Research in Environmental
Epidemiology, [email protected]
WP3 Health Outcomes. WG Cancer
Outline of this presentation
• Aims: to review childhood cancer related outcomes evaluated in epidemiological studies and suggest future directions in research
• Main problems identified in studies on childhood cancer
• Future directions
Main problems identified in studies on childhood cancer/1
• No special difficulties in the evaluation of the outcomes, at least in organised health case settings
• The main problem, by far, is that of statistical power. Childhood cancer is a main cause of death in children but remains a rare event
Sample size in studies on cancer in children (Brown, IJE 2007)
Main problems identified in studies on childhood cancer/2
• Existing studies have been remarkably unsuccesful to identify major risk factors for childhood cancers
• Evidence from case‐control studies frequently not replicable
• Difficulties encountered in existing studies to identify causal factors may reflect the fact that relevant exposures may refer to both the parents and the child
Future directions
Combination of approaches
• Registry based studies
• Cohort studies and case‐control studies evaluating childhood cancers
• Biomarker based studies evaluating caner related markers
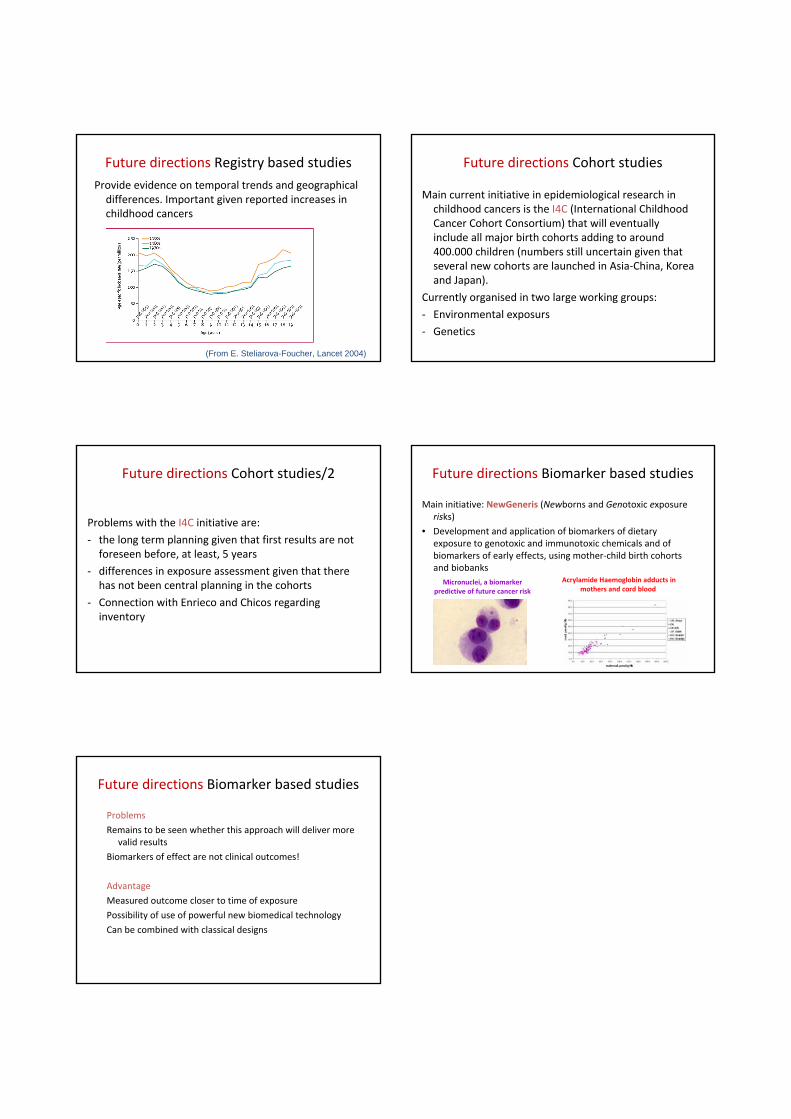
Future directions Registry based studies Provide evidence on temporal trends and geographical differences. Important given reported increases in childhood cancers
(From E. Steliarova-Foucher, Lancet 2004)
Future directions Cohort studies
Main current initiative in epidemiological research in childhood cancers is the I4C (International Childhood Cancer Cohort Consortium) that will eventually include all major birth cohorts adding to around 400.000 children (numbers still uncertain given that several new cohorts are launched in Asia‐China, Korea and Japan).
Currently organised in two large working groups:
‐ Environmental exposurs
‐ Genetics
Future directions Cohort studies/2
Problems with the I4C initiative are:
‐ the long term planning given that first results are not foreseen before, at least, 5 years
‐ differences in exposure assessment given that there has not been central planning in the cohorts
‐ Connection with Enrieco and Chicos regarding inventory
Future directions Biomarker based studies
Main initiative: NewGeneris (Newborns and Genotoxic exposure risks)
• Development and application of biomarkers of dietary exposure to genotoxic and immunotoxic chemicals and of biomarkers of early effects, using mother‐child birth cohorts and biobanks
Acrylamide Haemoglobin adducts in mothers and cord blood
Micronuclei, a biomarker predictive of future cancer risk
Future directions Biomarker based studies
Problems
Remains to be seen whether this approach will deliver more valid results
Biomarkers of effect are not clinical outcomes!
Advantage
Measured outcome closer to time of exposure
Possibility of use of powerful new biomedical technology
Can be combined with classical designs
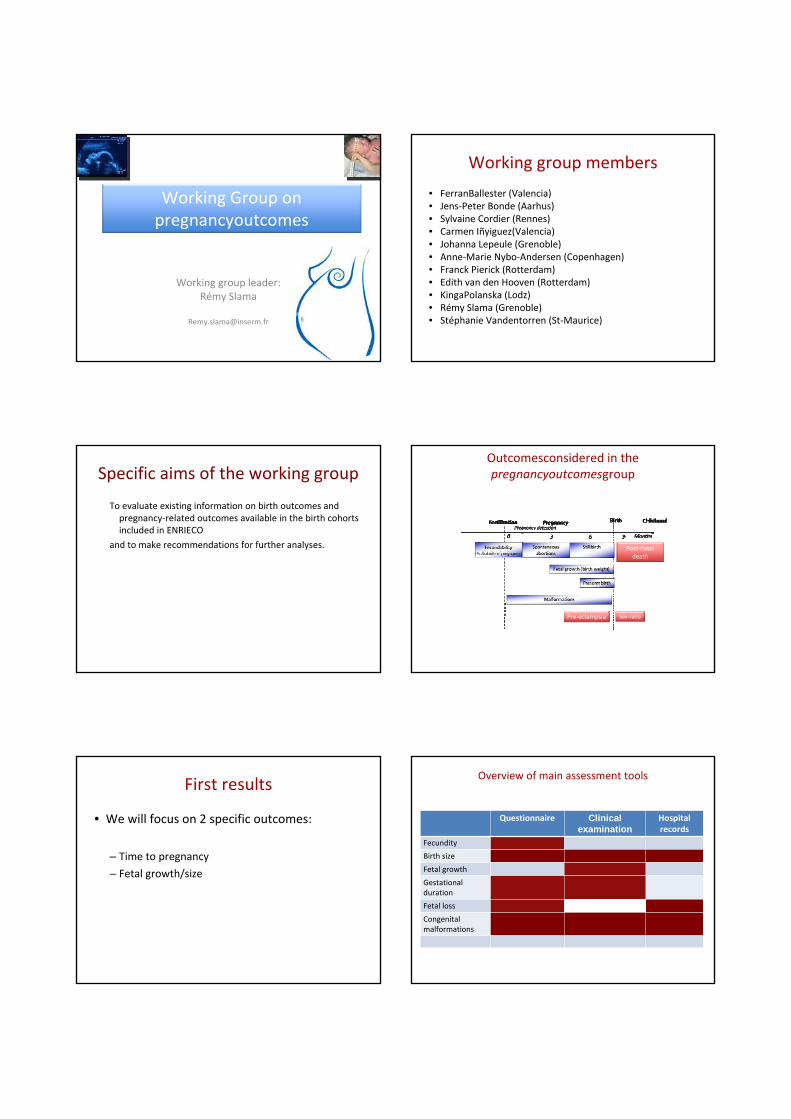
Working Group on pregnancyoutcomes
Working group leader:Rémy Slama
Working group members
• FerranBallester (Valencia)• Jens‐Peter Bonde (Aarhus)• Sylvaine Cordier (Rennes)• Carmen Iñyiguez(Valencia)• Johanna Lepeule (Grenoble)• Anne‐Marie Nybo‐Andersen (Copenhagen)• Franck Pierick (Rotterdam)• Edith van den Hooven (Rotterdam)• KingaPolanska (Lodz)• Rémy Slama (Grenoble)• Stéphanie Vandentorren (St‐Maurice)
Specific aims of the working group
To evaluate existing information on birth outcomes and pregnancy‐related outcomes available in the birth cohorts included in ENRIECO
and to make recommendations for further analyses.
Outcomesconsidered in thepregnancyoutcomesgroup
Post‐natal death
Pre‐eclampsia Sex‐ratio
First results
• We will focus on 2 specific outcomes:
– Time to pregnancy
– Fetal growth/size
Overview of main assessment tools
Questionnaire Clinical examination
Hospital records
Fecundity
Birth size
Fetal growth
Gestational duration
Fetal loss
Congenital malformations
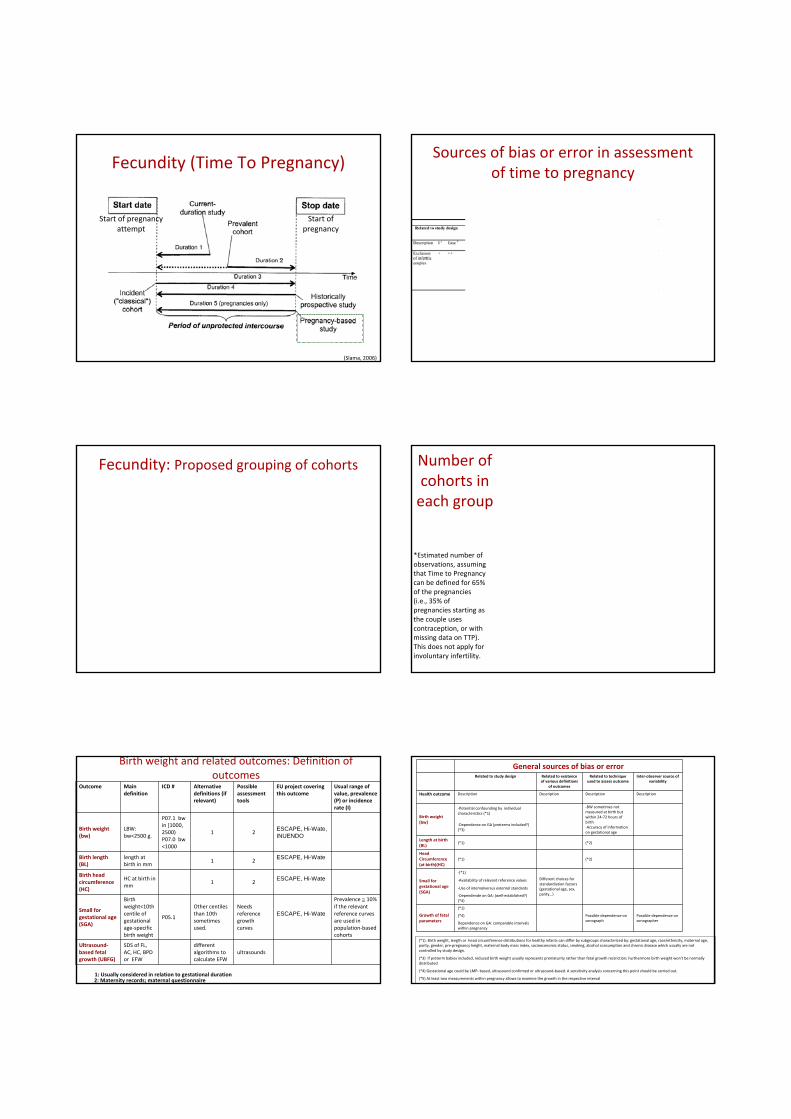
Fecundity (Time To Pregnancy)
Start of pregnancy attempt
Start of pregnancy
(Slama, 2006)
Sources of bias or error in assessment of time to pregnancy
Fecundity: Proposed grouping of cohorts
* Group 3 also includes all cohorts belonging to groups 1 and 2
Number of cohorts in each group
*Estimated number of observations, assuming that Time to Pregnancy can be defined for 65% of the pregnancies (i.e., 35% of pregnancies starting as the couple uses contraception, or with missing data on TTP). This does not apply for involuntary infertility.
Outcome Main definition
ICD # Alternative definitions (if relevant)
Possible assessment tools
EU project covering this outcome
Usual range of value, prevalence (P) or incidence rate (I)
Birth weight (bw)
LBW: bw<2500 g.
P07.1 bw in [1000, 2500) P07.0 bw <1000
1 2 ESCAPE, Hi-Wate, INUENDO
Birth length (BL)
length at birth in mm
1 2 ESCAPE, Hi-Wate
Birth head circumference (HC)
HC at birth in mm
1 2ESCAPE, Hi-Wate
Small for gestational age (SGA)
Birth weight<10th centile of gestational age‐specific birth weight
P05.1
Other centiles than 10th sometimes used.
Needs reference growth curves
ESCAPE, Hi-Wate
Prevalence ≅ 10% if the relevant reference curves are used in population‐based cohorts
Ultrasound‐based fetal growth (UBFG)
SDS of FL, AC, HC, BPD or EFW
different algorithms to calculate EFW
ultrasounds
1: Usually considered in relation to gestational duration2: Maternity records; maternal questionnaire
Birth weight and related outcomes: Definition of outcomes
General sources of bias or errorRelated to study design Related to existence
of various definitions of outcomes
Related to technique used to assess outcome
Inter‐observer source of variability
Health outcome Description Description Description Description
Birth weight (bw)
‐Potential confounding by individual characteristics (*1)
‐BW sometimes not measured at birth but within 24‐72 hours of birth‐Accuracy of information on gestational age
‐Dependence on GA (preterms included?) (*3)
Length at birth (BL)
(*1) (*2)
Head Circumference (at birth)(HC)
(*1) (*2)
Small for gestational age (SGA)
‐(*1)
Different choices for standardiation factors (gestational age, sex, parity…)
‐Availability of relevant reference values
‐Use of internalversus external standards
‐Dependende on GA: (well‐established?) (*4)
Growth of fetal parameters
(*1)
Possible dependence on sonograph
Possible dependence on sonographer
(*4)
Dependence on GA: comparable intervals within pregnancy
(*1). Birth weight, length or head circumference distributions for healthy infants can differ by subgroups characterized by: gestational age, race/ethnicity, maternal age, parity, gender, pre‐pregnancy height, maternal body mass index, socioeconomic status, smoking, alcohol consumption and chronic disease which usually are not controlled by study design.
(*3) If preterm babies included, reduced birth weight usually represents prematurity rather than fetal growth restriction; Furthermore birth weight won't be normally distributed
(*4) Gestational age could be LMP‐ based, ultrasound confirmed or ultrasound‐based. A sensitivity analysis concerning this point should be carried out.
(*5) At least two measurements within pregnancy allows to examine the growth in the respective interval
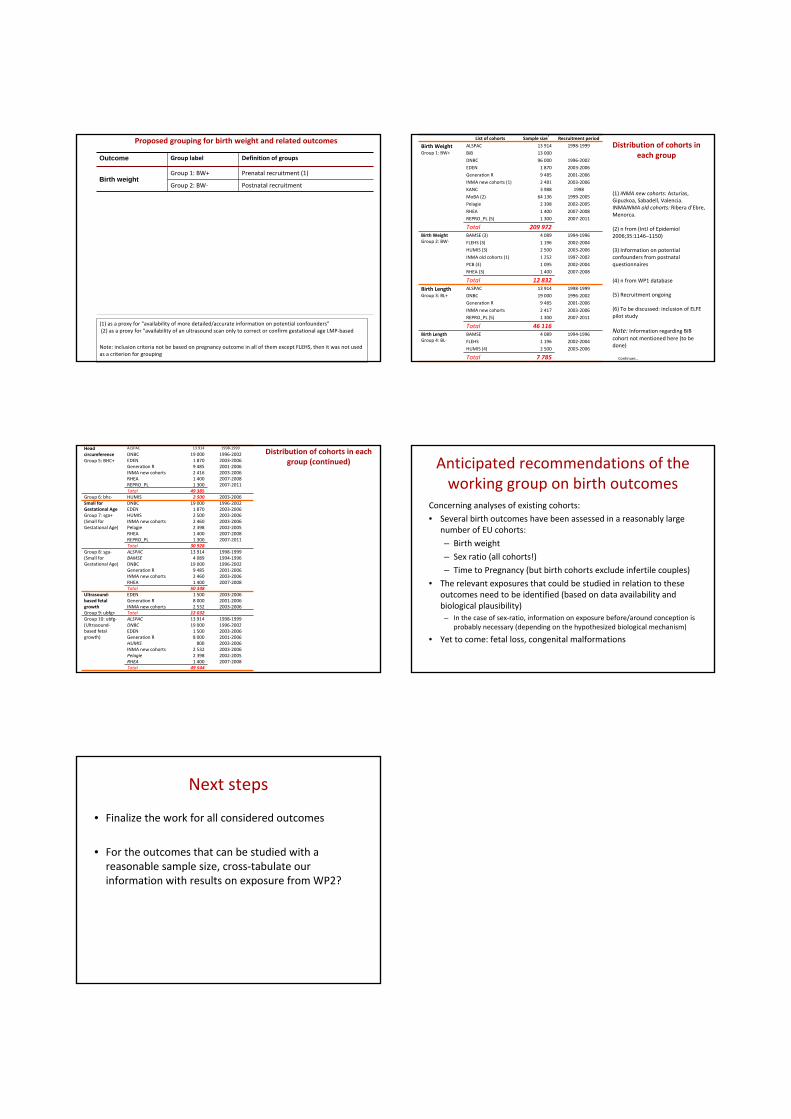
(1) as a proxy for "availability of more detailed/accurate information on potential confounders"(2) as a proxy for "availability of an ultrasound scan only to correct or confirm gestational age LMP‐based
Note: inclusion criteria not be based on pregnancy outcome in all of them except FLEHS, then it was not used as a criterion for grouping
Outcome Group label Definition of groups
Birth weightGroup 1: BW+ Prenatal recruitment (1)
Group 2: BW‐ Postnatal recruitment
Birth length (BL)Group 3: BL+ Birth length available, prenatal recruitment (1)
Group 4: BL‐ Birth length available, postnatal recruitment
Head Circumference at birth (HC)
Group 5: BHC+Birth head circumference available, prenatal recruitment (1)
Group 6: BHC‐Birth head circumference available, postnatal recruitment
Small for Gestational Age births (SGA)
Group 7: SGA+ External standard
Group 8: SGA‐ Internal standard
Ultrasound-based fetal growth (UBFG)
Group 9: UBFG+At least 2 ultrasound measurements in each trimester for 80% of the cohort
Group 10: UBFG‐ At least 1 ultrasound measurement (2)
Proposed grouping for birth weight and related outcomes List of cohorts Sample sizea
Recruitment period
Birth WeightGroup 1: BW+
ALSPAC 13 914 1998‐1999BiB 13 000
DNBC 96 000 1996‐2002EDEN 1 870 2003‐2006
Generation R 9 485 2001‐2006INMA new cohorts (1) 2 481 2003‐2006KANC 3 988 1998
MoBA (2) 64 136 1999‐2005Pelagie 2 398 2002‐2005
RHEA 1 400 2007‐2008REPRO_PL (5) 1 300 2007‐2011
Total 209 972Birth WeightGroup 2: BW‐
BAMSE (3) 4 089 1994‐1996
FLEHS (3) 1 196 2002‐2004HUMIS (3) 2 500 2003‐2006
INMA old cohorts (1) 1 252 1997‐2002PCB (3) 1 095 2002‐2004RHEA (3) 1 400 2007‐2008
Total 12 832Birth LengthGroup 3: BL+
ALSPAC 13 914 1998‐1999DNBC 19 000 1996‐2002Generation R 9 485 2001‐2006
INMA new cohorts 2 417 2003‐2006REPRO_PL (5) 1 300 2007‐2011
Total 46 116Birth LengthGroup 4: BL‐
BAMSE 4 089 1994‐1996FLEHS 1 196 2002‐2004
HUMIS (4) 2 500 2003‐2006
Total 7 785
(1) INMA new cohorts: Asturias, Gipuzkoa, Sabadell, Valencia. INMAINMA old cohorts: Ribera d’Ebre, Menorca.
(2) n from (IntJ of Epidemiol2006;35:1146–1150)
(3) Information on potential confounders from postnatal questionnaires
(4) n from WP1 database
(5) Recruitment ongoing
(6) To be discussed: inclusion of ELFE pilot study
Note: Information regarding BiBcohort not mentioned here (to be done)
Continues…
Distribution of cohorts in each group
Head circumferenceGroup 5: BHC+
ALSPAC 13 914 1998‐1999
DNBC 19 000 1996‐2002EDEN 1 870 2003‐2006Generation R 9 485 2001‐2006INMA new cohorts 2 416 2003‐2006RHEA 1 400 2007‐2008REPRO_PL 1 300 2007‐2011Total 49 385
Group 6: bhc‐ HUMIS 2 500 2003‐2006Small for Gestational AgeGroup 7: sga+(Small for Gestational Age)
DNBC 19 000 1996‐2002EDEN 1 870 2003‐2006HUMIS 2 500 2003‐2006INMA new cohorts 2 460 2003‐2006Pelagie 2 398 2002‐2005RHEA 1 400 2007‐2008REPRO_PL 1 300 2007‐2011Total 30 928
Group 8: sga‐(Small for Gestational Age)
ALSPAC 13 914 1998‐1999BAMSE 4 089 1994‐1996DNBC 19 000 1996‐2002Generation R 9 485 2001‐2006INMA new cohorts 2 460 2003‐2006RHEA 1 400 2007‐2008Total 50 348
Ultrasound‐based fetal growthGroup 9: ubfg+
EDEN 1 500 2003‐2006Generation R 8 000 2001‐2006INMA new cohorts 2 532 2003‐2006Total 12 032
Group 10: ubfg‐(Ultrasound‐based fetal growth)
ALSPAC 13 914 1998‐1999DNBC 19 000 1996‐2002EDEN 1 500 2003‐2006Generation R 8 000 2001‐2006HUMIS 800 2003‐2006INMA new cohorts 2 532 2003‐2006Pelagie 2 398 2002‐2005RHEA 1 400 2007‐2008Total 49 544
Distribution of cohorts in each group (continued) Anticipated recommendations of the
working group on birth outcomesConcerning analyses of existing cohorts:• Several birth outcomes have been assessed in a reasonably large
number of EU cohorts:
– Birth weight
– Sex ratio (all cohorts!)
– Time to Pregnancy (but birth cohorts exclude infertile couples)• The relevant exposures that could be studied in relation to these
outcomes need to be identified (based on data availability and biological plausibility)– In the case of sex‐ratio, information on exposure before/around conception is
probably necessary (depending on the hypothesized biological mechanism)
• Yet to come: fetal loss, congenital malformations
Next steps
• Finalize the work for all considered outcomes
• For the outcomes that can be studied with a reasonable sample size, cross‐tabulate our information with results on exposure from WP2?
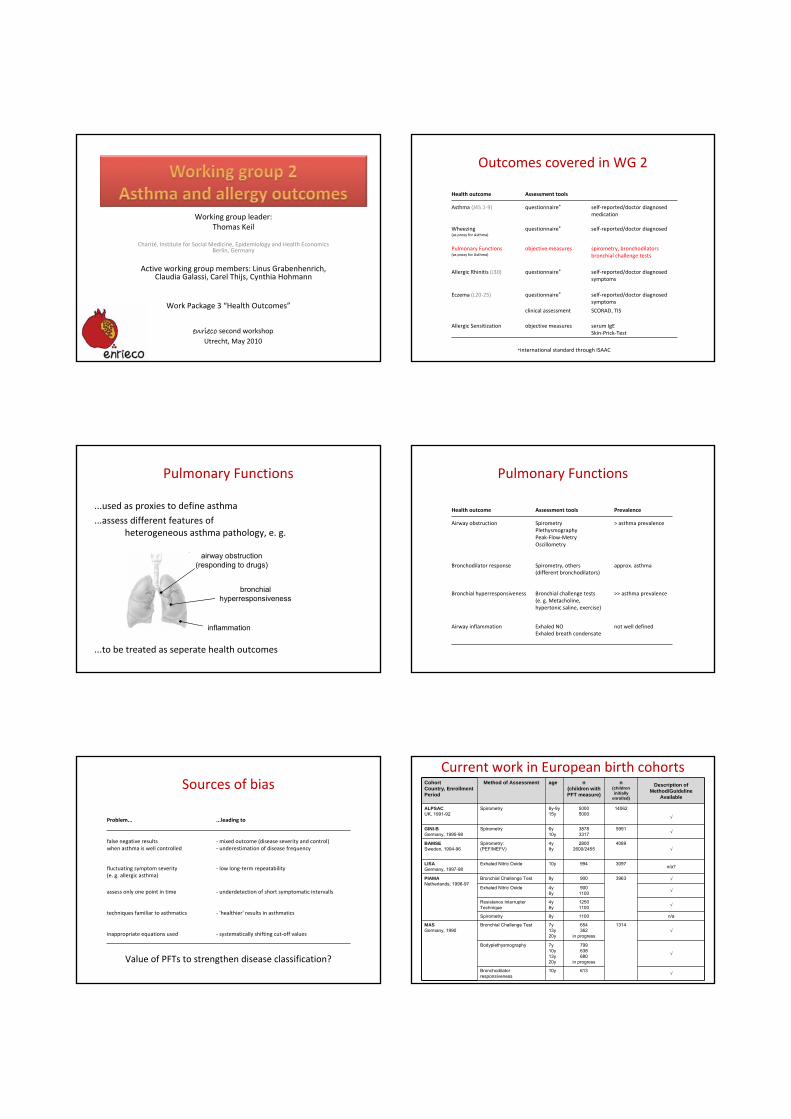
Work Package 3 “Health Outcomes”
enrieco second workshopUtrecht, May 2010
Working group leader:Thomas Keil
Charité, Institute for Social Medicine, Epidemiology and Health EconomicsBerlin, Germany
Active working group members: Linus Grabenhenrich, Claudia Galassi, Carel Thijs, Cynthia Hohmann
Outcomes covered in WG 2
Health outcome Assessment tools
Asthma (J45.1‐9) questionnaire* self‐reported/doctor diagnosedmedication
Wheezing(as proxy for Asthma)
questionnaire* self‐reported/doctor diagnosed
Pulmonary Functions(as proxy for Asthma)
objective measures spirometry, bronchodilatorsbronchial challenge tests
Allergic Rhinitis (J30) questionnaire* self‐reported/doctor diagnosedsymptoms
Eczema (L20‐25) questionnaire* self‐reported/doctor diagnosedsymptoms
clinical assessment SCORAD, TIS
Allergic Sensitization objective measures serum IgESkin‐Prick‐Test
*international standard through ISAAC
...used as proxies to define asthma
...assess different features ofheterogeneous asthma pathology, e. g.
...to be treated as seperate health outcomes
Pulmonary Functions
airway obstruction(responding to drugs)
bronchialhyperresponsiveness
inflammation
Pulmonary Functions
Health outcome Assessment tools Prevalence
Airway obstruction SpirometryPlethysmographyPeak‐Flow‐MetryOscillometry
> asthma prevalence
Bronchodilator response Spirometry, others(different bronchodilators)
approx. asthma
Bronchial hyperresponsiveness Bronchial challenge tests(e. g. Metacholine,hypertonic saline, exercise)
>> asthma prevalence
Airway inflammation Exhaled NOExhaled breath condensate
not well defined
Sources of bias
Problem... ...leading to
false negative resultswhen asthma is well controlled
‐mixed outcome (disease severity and control)‐ underestimation of disease frequency
fluctuating symptom severity(e. g. allergic asthma)
‐ low long‐term repeatability
assess only one point in time ‐ underdetection of short symptomatic intervalls
techniques familiar to asthmatics ‐ 'healthier' results in asthmatics
inappropriate equations used ‐ systematically shifting cut‐off values
Value of PFTs to strengthen disease classification?
Current work in European birth cohortsCohortCountry, EnrollmentPeriod
Method of Assessment age n (children with PFT measure)
n(children initially
enrolled)
Description of Method/Guideline
Available
ALPSACUK, 1991-92
Spirometry 8y-9y15y
50005000
14062
√
GINI-BGermany, 1995-98
Spirometry 6y10y
38783317
5991 √
BAMSESweden, 1994-96
Spirometry:(PEF/MEFV)
4y8y
28002600/2455
4089√
LISAGermany, 1997-98
Exhaled Nitric Oxide 10y 994 3097 n/a?
PIAMANetherlands, 1996-97
Bronchial Challenge Test 8y 900 3963 √
Exhaled Nitric Oxide 4y8y
9001100 √
Resistance Interrupter Technique
4y8y
12501100 √
Spirometry 8y 1100 n/a
MASGermany, 1990
Bronchial Challenge Test 7y13y20y
654362
in progress
1314√
Bodyplethysmography 7y10y13y20y
799638680
in progress
√
Bronchodilator responsiveness
10y 613 √
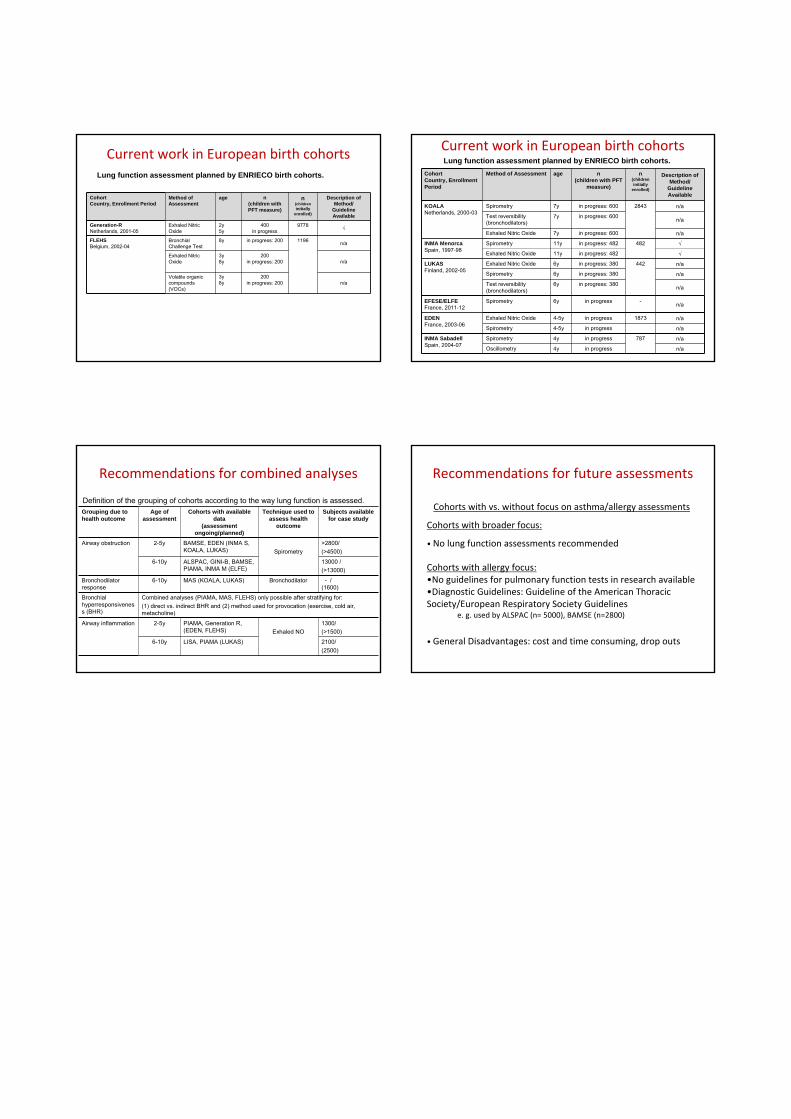
Current work in European birth cohortsLung function assessment planned by ENRIECO birth cohorts.
CohortCountry, Enrollment Period
Method of Assessment
age n (children with PFT measure)
n(children initially
enrolled)
Description of Method/
GuidelineAvailable
Generation-RNetherlands, 2001-05
Exhaled Nitric Oxide
2y5y
400in progress
9778 √
FLEHSBelgium, 2002-04
Bronchial Challenge Test
8y in progress: 200 1196 n/a
Exhaled Nitric Oxide
3y 8y
200in progress: 200 n/a
Volatile organic compounds (VOCs)
3y 8y
200in progress: 200 n/a
Current work in European birth cohortsLung function assessment planned by ENRIECO birth cohorts.
CohortCountry, EnrollmentPeriod
Method of Assessment age n (children with PFT
measure)
n(children initially
enrolled)
Description of Method/
GuidelineAvailable
KOALANetherlands, 2000-03
Spirometry 7y in progress: 600 2843 n/a
Test reversibility (bronchodilators)
7y in progress: 600 n/a
Exhaled Nitric Oxide 7y in progress: 600 n/a
INMA MenorcaSpain, 1997-98
Spirometry 11y in progress: 482 482 √
Exhaled Nitric Oxide 11y in progress: 482 √
LUKASFinland, 2002-05
Exhaled Nitric Oxide 6y in progress: 380 442 n/a
Spirometry 6y in progress: 380 n/a
Test reversibility (bronchodilators)
6y in progress: 380 n/a
EFESE/ELFEFrance, 2011-12
Spirometry 6y in progress - n/a
EDENFrance, 2003-06
Exhaled Nitric Oxide 4-5y in progress 1873 n/a
Spirometry 4-5y in progress n/a
INMA SabadellSpain, 2004-07
Spirometry 4y in progress 787 n/a
Oscillometry 4y in progress n/a
Recommendations for combined analyses
Grouping due to health outcome
Age of assessment
Cohorts with available data
(assessment ongoing/planned)
Technique used to assess health
outcome
Subjects available for case study
Airway obstruction 2-5y BAMSE, EDEN (INMA S, KOALA, LUKAS) Spirometry
>2800/(>4500)
6-10y ALSPAC, GINI-B, BAMSE, PIAMA, INMA M (ELFE)
13000 /(>13000)
Bronchodilator response
6-10y MAS (KOALA, LUKAS) Bronchodilator - /(1600)
Bronchial hyperresponsiveness (BHR)
Combined analyses (PIAMA, MAS, FLEHS) only possible after stratifying for:(1) direct vs. indirect BHR and (2) method used for provocation (exercise, cold air, metacholine)
Airway inflammation 2-5y PIAMA, Generation R, (EDEN, FLEHS) Exhaled NO
1300/(>1500)
6-10y LISA, PIAMA (LUKAS) 2100/(2500)
Definition of the grouping of cohorts according to the way lung function is assessed.
Recommendations for future assessments
Cohorts with vs. without focus on asthma/allergy assessments
Cohorts with broader focus:
• No lung function assessments recommended
Cohorts with allergy focus: •No guidelines for pulmonary function tests in research available•Diagnostic Guidelines: Guideline of the American Thoracic Society/European Respiratory Society Guidelines
e. g. used by ALSPAC (n= 5000), BAMSE (n=2800)
• General Disadvantages: cost and time consuming, drop outs
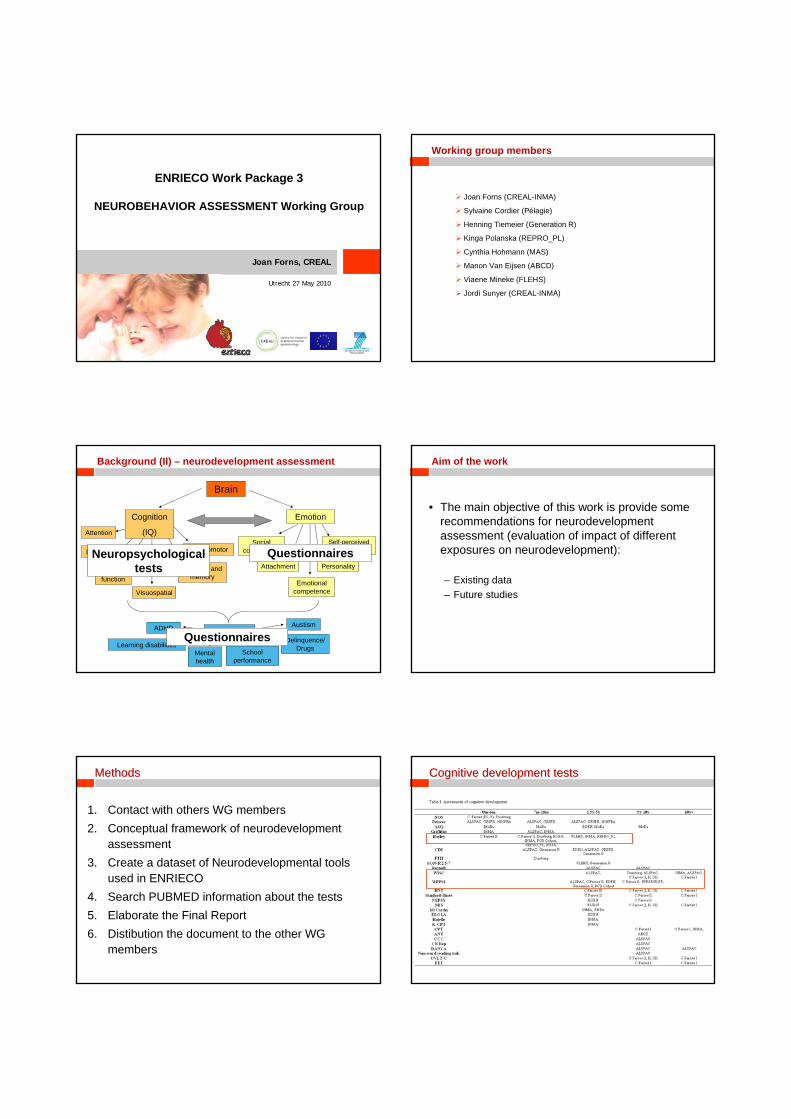
ENRIECO Work Package 3
NEUROBEHAVIOR ASSESSMENT Working Group
Joan Forns, CREAL
Utrecht 27 May 2010
Joan Forns (CREAL-INMA)
Sylvaine Cordier (Pélagie)
Henning Tiemeier (Generation R)
Kinga Polanska (REPRO_PL)
Cynthia Hohmann (MAS)
Manon Van Eijsen (ABCD)
Viaene Mineke (FLEHS)
Jordi Sunyer (CREAL-INMA)
Working group members
Brain
Cognition
(IQ)
Emotion
Executivefunction
Visuospatial
Learning andmemory
PsychomotorSocial
competence
Attachment
Emotionalcompetence
Personality
Self-perceivedcompetence
BehaviorADHD
Learning disabilitiesMental health
Schoolperformance
Austism
Delinquence/Drugs
Attention
Language
Background (II) – neurodevelopment assessment
Neuropsychologicaltests
Questionnaires
Questionnaires
• The main objective of this work is provide some recommendations for neurodevelopment assessment (evaluation of impact of different exposures on neurodevelopment):
– Existing data– Future studies
Aim of the work
MethodsMethods
1. Contact with others WG members2. Conceptual framework of neurodevelopment
assessment3. Create a dataset of Neurodevelopmental tools
used in ENRIECO4. Search PUBMED information about the tests5. Elaborate the Final Report6. Distibution the document to the other WG
members
Cognitive Cognitive developmentdevelopment teststests
BehavioralBehavioral developmentdevelopment teststests PotentialPotential biasesbiases in in neurodevelopmentneurodevelopment outcomesoutcomes
• One assessment of all the areas of neurodevelopment– Cognitive– Social-emotional– Behavioural
• Several measures in cognitive development – First two years, preschool years, preadolescence…– To establish developmental trajectories
• Only psychologists can assess global IQ tests (neuropsychological tests)– For different interviewers better use computerized tests and/or self-reported
questionnaires – To have at least one measure assessed by psychologist
• Validated and published tests– If not, we must apply a validation study
RecommendationsRecommendations
• High quality of data collection:– To elaborate a strict protocol of assessment– To apply a previous training of the interviewers– To have as few interviewers as possible– To apply several quality controls during fieldwork
• In analysing the relationships between different exposures and child neurodevelopment it is crucial several confounding factors
• To create a protocol of neurodevelopmental tests for future studies– This will be included in Final Report and scientific paper
RecommendationsRecommendations
• Many cohorts have collected information on cognitive and behavior
• Many different tests have been used to assess these outcomes
• Even though different, the harmonization can be achieved
SummarySummary
“The basic aim of every neuropsychological assessment - be it with adults, adolescents,
or children - is to produce a reliable and valid “picture” of the relationships between
the brain and behaviour.”
Byron Rourke et al. 1983
1
ENRIECO WP4 –Evaluation of Exposure – Response Relationship
ENRIECO General Assembly 27.May 10 Utrecht
ENRIECO WP4 –Evaluation of Exposure – Response Relationship
Aim – to evaluate existing environmental exposure response information, methods and tools of cohort studies and make recommendations for further analyses
Method-1. Develop protocols for the evaluation of exposure-
response information on specific themes2. In each theme, perform systematic review of peer reviewed scientific publications from European birth cohort studies (and other evidence)
ENRIECO WP4 –Environmental Exposure - Response Working Groups
Ulrike GehringAir pollution and Allergy and Asthma
Thomas Keil/ Cynthia HochmannNoise and Paediatric and Birth Outcomes
Second Hand Smoking and Birth Outcomes
POPs and Neurobehavioural/Cognitive Function
POPs and Birth Outcomes
Metals and Neurobehavioural/Cognitive Function
Metals and Birth Outcomes
Water contaminants and Birth Outcomes
Pesticides and Birth Outcomes
Allergens/Biological Organism and Allergy and Asthma
Occupation and Birth Outcomes
Air pollution and Birth Outcomes
Specific Themes of Interest
Constantine Vardavas/ Vicky Patelarou
Jordi Sunyer /Mireia Gascon
Jens Peter Bonde/ Gunnar Toft
Jordi Sunyer / Maribel Casas
Jordi Sunyer / Maribel Casas
Mark Nieuwenhuijsen/ Jeremy Botton
Sylvaine Cordier/ Cecile Chevrier
Chih-Mei Chen/ Christina Tischer
Martine Vrijheid/ Maribel Casas
Manolis Kogevinas
Reviewer
ENRIECO WP4 – achievements by the end of year one
Protocols for the evaluation of exposure- response information on specific themes are completed and submitted
Progress of the systematic review of peer reviewed scientific publications from European birth cohort studies (and other evidence) in each themes:
ENRIECO WP4 –Current status of the systematic review
First draft submittedAir pollution and Allergy and Asthma
First draft submittedNoise and Paediatric and Birth Outcomes
Second Hand Smoking and Birth Outcomes
POPs and Neurobehavioural/Cognitive Function
POPs and Birth Outcomes
Metals and Neurobehavioural/Cognitive Function
Metals and Birth Outcomes
Water contaminants and Birth Outcomes
Pesticides and Birth Outcomes
Allergens/Biological Organism and Allergy and Asthma
Occupation and Birth Outcomes
Air pollution and Birth Outcomes
Specific Themes of Interest
In progress
First draft submitted
First draft submitted
Review publications from ENRIECO cohorts
Review publications from ENRIECO cohorts
First draft submitted
First draft submitted
First draft submitted
Review publications from ENRIECO cohorts
In progress
Status
Current evidence of exposure and response relationship -based on the first draft submitted
More frequently studied theme 1:
Air pollution and Allergy and AsthmaRecent review (Braback and Fosberg, Environ Health 2009) on long-term exposure to traffic-related air pollution and asthma and allergy development in children – evidence from cohort studies
• January 1, 2002 to October 2008
• Conclusion : traffic-related air pollution contributes to the development of respiratory illness and allergic sensitization.
•
Objectives ENRIECO review: completion of previous work :
• November 2008 to present
• Eczema and hayfever as additional health endpoints
• 4 papers on 4 European birth cohorts (GINIplus and LISAplus, PIAMA, Oslo birth cohort, cohort from Krakau)
• 6 papers from 3 non-European birth cohorts (Canada birth cohort, CCAAPS, OMCHS
• 2 papers from non-birth cohorts (FACES-LiTE, CHS )
2
Current evidence of exposure and response relationship -based on the first draft submitted
Summary:
• Confirmation of earlier findings that traffic-related air pollution contributes to the development of respiratory illness and allergic sensitization.
• Positive associations have been found between levels of traffic-related air pollution at the birth address and the incidence.
• Growing evidence for an association between traffic-related air pollution exposure and eczema.
Recommendations:• Cross-sectional vs longitudinal analysis • Incidence vs prevalence• Relevance of timing of exposure • Exposure other than residential exposure • Long-term validity of land-use regression models • Long-term validity of personal measurements
Air-pollution and reproductive outcomes, main findings
Recent reviews available
Several studies evaluating birth weight (and outcomes related to growth) and gestational age
Heterogeneous study designs and evaluation of exposure
Fairly consistent findings for LBW and Preterm deliveries
Few studies and inconsistent findings on other outcomes e.g. spontaneous abortions, congenital malformations
Current evidence of exposure and response relationship -based on the evidence collected
Heterogeneity in exposures and timing evaluated
(adapted fromSlama EHP 2008)
Air-pollution and reproductive outcomes future research
Main ongoing study, ESCAPE measuring NOx and PM
Need for further research on timing of exposure, evaluation of differentcontaminants, biological mechanisms, biomarker based studies and studiesevaluating other outcomes
Current evidence of exposure and response relationship -based on the evidence collected
Current evidence of exposure and response relationship -based on the first draft submitted
More frequently studied theme 2:Allergens/Biological Organism and Allergy and Asthma
Recent review (Chen et al.): exposure to cats and dogs and asthma and allergy development in childrenJanuary 1, 2000 to January 2009
Review on exposure to mould / mould components and endotoxin (ENRIECO):January 1980 to March 2010Mould Endotoxin4 European birth cohorts 5 European birth cohorts7 non-European birth cohorts 8 non-European birth cohorts7 cohorts 2 cohorts
Evidence: Visible mould: adverse effect on children’s respiratory health.Mould components: inversely associated with respiratory health and atopic
sensitization in young children Endotoxin: increased risk of developing wheezing symptoms at younger age;
protective effects on respiratory health at older ages.
More frequently studied theme 3: POPs and Neuro-development
3 Previous reviews:Korrick 2008: modest association between prenatal exposure to PCBs and ND outcomes. -Wigle 2007-2008: PCBs
Eskenazi 2009 (review between 2003 -08): studies suggest that DDT, and less so DDE, may be associated with neurodevelopmental deficits.
ENRIECO’s review:
- 9 articles within ENRIECO + 2 abstracts
- 10 articles within EU, not ENRIECO
- 27 articles + 2 abstracts (5 in 2008-09)
Evidence?: only European studies were deeply read…
- PCBs results are not consistent (pre-natal and post-natal exposure)
- DDT, DDE negative effects on cognitive function, specially for DDT
- HCB negative effects on social competence & ADHD, but only one study
- New compounds (Mirex, PFOA, PFOS and PBDEs) few data provided
Current evidence of exposure and response relationship -based on the first draft submitted
3
More frequently studied theme 3: POPs and Neuro-developmentRecommendations: - Identify the most problematic congeners and metabolites (contradictive results could
be due to this)- Follow up the cohorts to older ages (only children up to 8 y were assessed)- Further research on new POPs (Mirex, PFOA, PFOS, PBDEs)- Give guidelines on the topics below so then it will become easier to compare results
and draw - Study multi-pollutant effectsconclusions:
1. Methods to measure levels and unique expression units2. Neurotests used (now there are computer based tests)3. Data analysis methods (tests, confounders, etc)
Current evidence of exposure and response relationship -based on the first draft submitted
Current evidence of exposure and response relationship -based on the first draft submitted
Few existing publications theme 1:
Water contaminants and Birth OutcomesNo paper found in European Birth Cohort studies
→ review of other designs/countries (n=42, but on DBPs only)
HiWATE: ongoing study (5 cohorts also in ENRIECO) on DBPs and birth outcomes
Evidence: Some evidence: DBPs (THMs) on fetal growth deficit
Evidence at best limited: nitrates, pesticides, metals, PFOS/PFOA, fluorides
Recommendations: ENRIECO: 11 cohort studies with data on water consumption:A complete questionnaire on water exposure (by ingestion, inhalation, dermal) in each of the cohort
Routine measures from water companies
Current evidence of exposure and response relationship -based on the first draft submitted
Few existing publications theme 1:
Pesticides and Birth Outcome
Multiple usages of pesticides
Evidence for environmental contamination:Water (rivers, rain, drinking water), air, soil, plants and animals (food)
General population = exposed to pesticide residues through multiple sources and pathways
Agricultural activities:210 000 tons of pesticides
used in Europe in 2003(France, Spain, Italy, Germany
and UK account for 75%)
Nonagricultural activities:5-10% of the pesticidesCommunity needs: public roads,parks,…Domestic uses: private gardens, indoor
uses for plants/against insects…
Current evidence of exposure and response relationship -based on the first draft submitted
Few existing publications theme 1:
Pesticides and Birth Outcome
Inclusion year1990‐2010
PubMed search: 2582 articles
Hand search of citations of previous review and personal files: 0
2554 articles failed to meet the inclusion criteria28 articles included in the review5 European Studies
Summary: Results in literature (USA + Europe) still inconsistent: partly because of the great variety and complexity of pesticide exposure assessment
Lack of studies in Europe
21 ENRIECO cohorts have planned to assess pesticide exposure => pooling strategy to be considered?
Current evidence of exposure and response relationship -based on the first draft submitted
Few existing publications theme 1:
Noise and peadiatric (P)/birth outcomes (B)
Inclusion year, no restriction
PubMed search: (P) 149/ (B) 157
Hand search of citations of previous review and personal files: (P) 1/ (B) 1
(P) 133/ (B) 145 articles failed to meet the inclusion criteria(P) 14/ (B) 13 articles included in the review(P) 1 / (B) 2 European birth cohorts
Summary: At first glance, there is a lack of study in Europe and there is a big diversity among the methods (exposure assessments) and the confounders used
ENRIECO WP4: Next Step
Ranking of the evidence, harmonised evaluation strategy for each theme:
MOOSE guidelines for meta-analyses of observational studies (Stroup et al., 2000)
WHO evaluation criteria for causal interference
Publication of the reviewsFor those with less evidence or systematic review already exist – combined publication?
Combine information collected in ENRIECO (WP1, WP2, WP3, and WP4) for recommendations
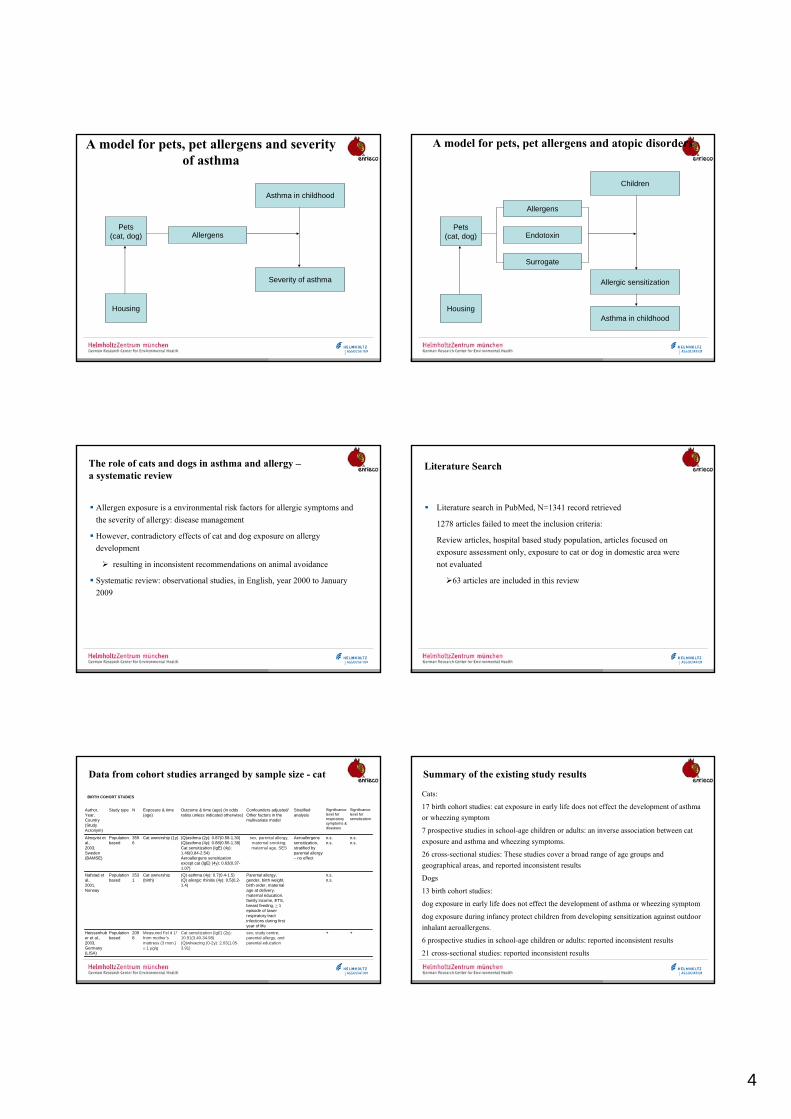
4
A model for pets, pet allergens and severityof asthma
Pets(cat, dog) Allergens
Asthma in childhood
Severity of asthma
Housing
A model for pets, pet allergens and atopic disorders
Pets(cat, dog)
Allergens
Endotoxin
Surrogate
Children
Allergic sensitization
Asthma in childhoodHousing
The role of cats and dogs in asthma and allergy –a systematic review
Allergen exposure is a environmental risk factors for allergic symptoms and the severity of allergy: disease management
However, contradictory effects of cat and dog exposure on allergy development
resulting in inconsistent recommendations on animal avoidance
Systematic review: observational studies, in English, year 2000 to January 2009
Literature Search
Literature search in PubMed, N=1341 record retrieved
1278 articles failed to meet the inclusion criteria:
Review articles, hospital based study population, articles focused on exposure assessment only, exposure to cat or dog in domestic area were not evaluated
63 articles are included in this review
Data from cohort studies arranged by sample size - cat
++sex, study centre, parental allergy, and parental education
Cat sensitization (IgE) (2y): 10.91(3.40-34.98)(Q)wheezing (0-2y): 2.03(1.05-3.91)
Measured Fel d 1§
from mother’s mattress (3 mon.) ≥ 1 µg/g
2098
Population based
Heissenhuber et al., 2003, Germany(LISA)
n.s.n.s.
Parental allergy, gender, birth weight, birth order, maternal age at delivery, maternal education, family income, ETS, breast feeding, ≥ 1 episode of lower respiratory tract infections during first year of life
(Q) asthma (4y): 0.7(0.4-1.5)(Q) allergic rhinitis (4y): 0.5(0.2-1.4)
Cat ownership (birth)
2531
Population based
Nafstad et al., 2001, Norway
n.s.n.s.
n.s.n.s.
Aeroallergens sensitization, stratified by parental allergy – no effect
sex, parental allergy, maternal smoking, maternal age, SES
(Q)asthma (2y): 0.87(0.58-1.30)(Q)asthma (4y): 0.88(0.56-1.38)Cat sensitization (IgE) (4y): 1.46(0.84-2.54)Aeroallergens sensitization except cat (IgE) (4y): 0.63(0.37-1.07)
Cat ownership (1y)3596
Population based
Almqvist et al., 2003,Sweden(BAMSE)
Significance level for sensitization
Significance level for respiratory symptoms & diseases
Stratified analysis
Confounders adjusted/Other factors in the multivariate model
Outcome & time (age) (in odds ratios unless indicated otherwise)
Exposure & time (age)
NStudy typeAuthor,Year, Country (Study Acronym)
BIRTH COHORT STUDIES
Summary of the existing study results
Cats:
17 birth cohort studies: cat exposure in early life does not effect the development of asthma or wheezing symptom
7 prospective studies in school-age children or adults: an inverse association between cat exposure and asthma and wheezing symptoms.
26 cross-sectional studies: These studies cover a broad range of age groups and geographical areas, and reported inconsistent results
Dogs
13 birth cohort studies:
dog exposure in early life does not effect the development of asthma or wheezing symptom
dog exposure during infancy protect children from developing sensitization against outdoor inhalant aeroallergens.
6 prospective studies in school-age children or adults: reported inconsistent results
21 cross-sectional studies: reported inconsistent results
5
What do we learn from this review-recommendations
Study Design
Exposure Assessment
Community effect
Avoidance effect
Gene-environmental interaction
Conclusion
The evidence of the effects of pet keeping on subsequent development of asthma or allergic diseases presented are not overwhelmingly strong
Decision of whether to keep a cat or a dog in the family should be based on arguments other than the concern of developing asthma and allergy
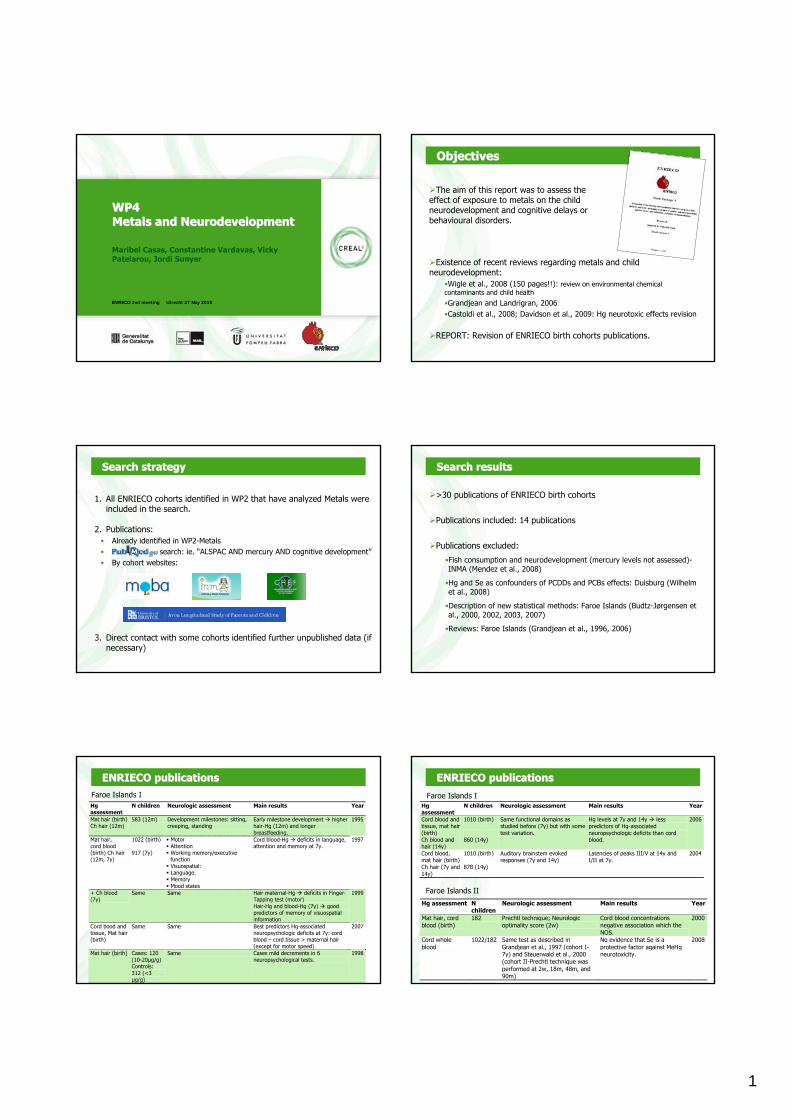
1
www.creal.cat
ENRIECO 2nd meeting Utrecht 27 May 2010
WP4WP4MetalsMetals and and NeurodevelopmentNeurodevelopment
Maribel Casas, Constantine Vardavas, VickyPatelarou, Jordi Sunyer
www.creal.cat
ObjectivesObjectives
The aim of this report was to assess the effect of exposure to metals on the child neurodevelopment and cognitive delays or behavioural disorders.
Existence of recent reviews regarding metals and child neurodevelopment:
•Wigle et al., 2008 (150 pages!!): review on environmental chemical contaminants and child health
•Grandjean and Landrigran, 2006 •Castoldi et al., 2008; Davidson et al., 2009: Hg neurotoxic effects revision
REPORT: Revision of ENRIECO birth cohorts publications.
www.creal.cat
SearchSearch strategystrategy
1. All ENRIECO cohorts identified in WP2 that have analyzed Metals were included in the search.
2. Publications:• Already identified in WP2-Metals• search: ie. “ALSPAC AND mercury AND cognitive development”• By cohort websites:
3. Direct contact with some cohorts identified further unpublished data (if necessary)
www.creal.cat
SearchSearch resultsresults
>30 publications of ENRIECO birth cohorts
Publications included: 14 publications
Publications excluded:
•Fish consumption and neurodevelopment (mercury levels not assessed)-INMA (Mendez et al., 2008)
•Hg and Se as confounders of PCDDs and PCBs effects: Duisburg (Wilhelm et al., 2008)
•Description of new statistical methods: Faroe Islands (Budtz-Jørgensen et al., 2000, 2002, 2003, 2007)
•Reviews: Faroe Islands (Grandjean et al., 1996, 2006)
www.creal.cat
ENRIECO ENRIECO publicationspublicationsFaroe Islands IHg assessment
N children Neurologic assessment Main results Year
Mat hair (birth) Ch hair (12m)
583 (12m) Development milestones: sitting, creeping, standing
Early milestone development higher hair-Hg (12m) and longer breastfeeding.
1995
Mat hair, cord blood (birth) Ch hair (12m, 7y)
1022 (birth) 917 (7y)
Motor Attention Working memory/executive function
Visuospatial: Language. Memory Mood states
Cord blood-Hg deficits in language, attention and memory at 7y.
1997
+ Ch blood (7y)
Same Same Hair maternal-Hg deficits in Finger-Tapping test (motor) Hair-Hg and blood-Hg (7y) good predictors of memory of visuospatial information
1999
Cord bood and tissue, Mat hair (birth)
Same Same Best predictors Hg-associated neuropsychologic deficits at 7y: cord blood – cord tissue > maternal hair (except for motor speed)
2007
Mat hair (birth) Cases: 120 (10-20µg/g) Controls: 312 (<3 µg/g)
Same Cases mild decrements in 6 neuropsychological tests.
1998
www.creal.cat
Hg assessment
N children Neurologic assessment Main results Year
Cord blood and tissue, mat hair (birth) Ch blood and hair (14y)
1010 (birth) 860 (14y)
Same functional domains as studied before (7y) but with some test variation.
Hg levels at 7y and 14y less predictors of Hg-associated neuropsychologic deficits than cord blood.
2006
Cord blood, mat hair (birth)Ch hair (7y and 14y)
1010 (birth) 878 (14y)
Auditory brainstem evoked responses (7y and 14y)
Latencies of peaks III/V at 14y and I/II at 7y.
2004
Hg assessment N children
Neurologic assessment Main results Year
Mat hair, cord blood (birth)
182 Prechtl technique; Neurologic optimality score (2w)
Cord blood concentrations negative association which the NOS.
2000
Cord whole blood
1022/182 Same test as described in Grandjean et al., 1997 (cohort I-7y) and Steuerwald et al., 2000 (cohort II-Prechtl technique was performed at 2w, 18m, 48m, and 90m)
No evidence that Se is a protective factor against MeHg neurotoxicity.
2008
ENRIECO ENRIECO publicationspublications
Faroe Islands II
Faroe Islands I
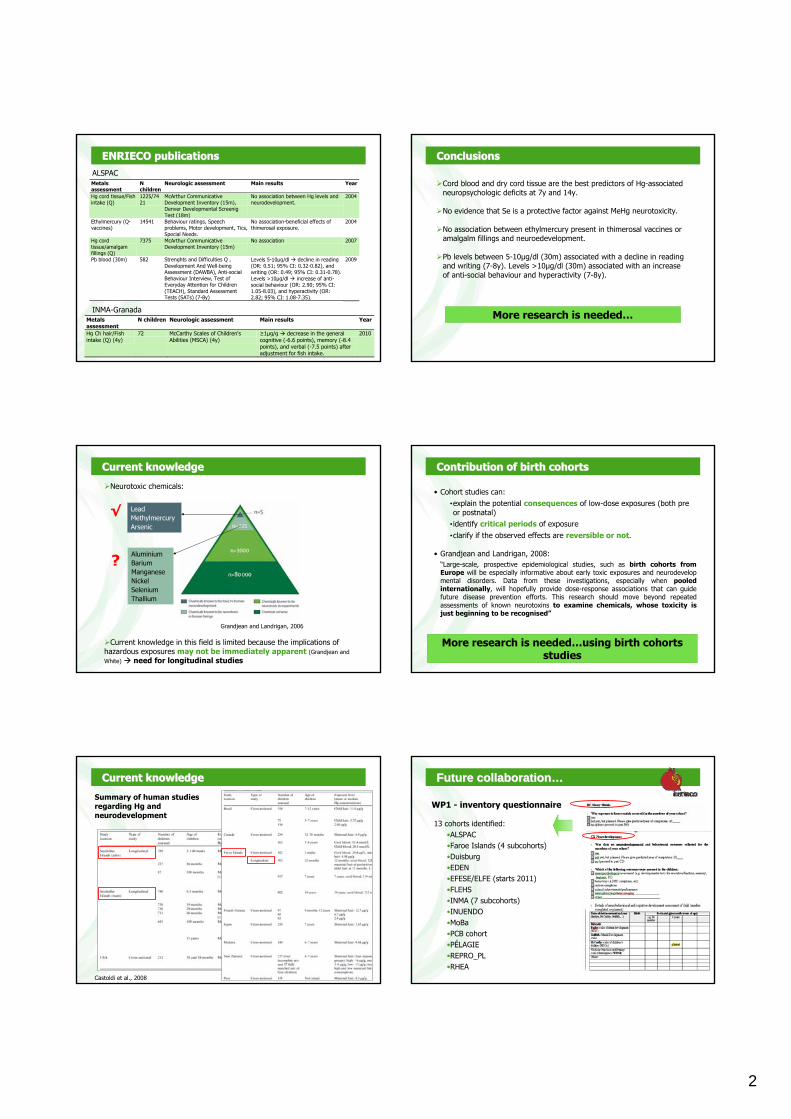
2
www.creal.cat
Metals assessment
N children
Neurologic assessment Main results Year
Hg cord tissue/Fish intake (Q)
1225/7421
McArthur Communicative Development Inventory (15m), Denver Developmental Screenig Test (18m)
No association between Hg levels and neurodevelopment.
2004
Ethylmercury (Q- vaccines)
14541 Behaviour ratings, Speech problems, Motor development, Tics, Special Needs.
No association-beneficial effects of thimerosal exposure.
2004
Hg cord tissue/amalgam fillings (Q)
7375 McArthur Communicative Development Inventory (15m)
No association 2007
Pb blood (30m) 582 Strenghts and Difficulties Q , Development And Well-being Assessment (DAWBA), Anti-social Behaviour Interview, Test of Everyday Attention for Children (TEACH), Standard Assessment Tests (SATs) (7-8y)
Levels 5-10µg/dl decline in reading (OR: 0.51; 95% CI: 0.32-0.82), and writing (OR: 0.49; 95% CI: 0.31-0.78). Levels >10µg/dl increase of anti-social behaviour (OR: 2.90; 95% CI: 1.05-8.03), and hyperactivity (OR: 2.82; 95% CI: 1.08-7.35).
2009
ENRIECO ENRIECO publicationspublications
INMA-Granada
ALSPAC
Metals assessment
N children Neurologic assessment Main results Year
Hg Ch hair/Fish intake (Q) (4y)
72 McCarthy Scales of Children's Abilities (MSCA) (4y)
≥1µg/g decrease in the general cognitive (-6.6 points), memory (-8.4 points), and verbal (-7.5 points) after adjustment for fish intake.
2010
www.creal.cat
ConclusionsConclusions
Cord blood and dry cord tissue are the best predictors of Hg-associated neuropsychologic deficits at 7y and 14y.
No evidence that Se is a protective factor against MeHg neurotoxicity.
No association between ethylmercury present in thimerosal vaccines or amalgalm fillings and neuroedevelopment.
Pb levels between 5-10µg/dl (30m) associated with a decline in reading and writing (7-8y). Levels >10µg/dl (30m) associated with an increase of anti-social behaviour and hyperactivity (7-8y).
More research is needed…
www.creal.cat
CurrentCurrent knowledgeknowledge
AluminiumBariumManganeseNickelSeleniumThallium
LeadMethylmercuryArsenic
Grandjean and Landrigan, 2006
Current knowledge in this field is limited because the implications ofhazardous exposures may not be immediately apparent (Grandjean andWhite) need for longitudinal studies
Neurotoxic chemicals:
√
?
www.creal.cat
ContributionContribution ofof birthbirth cohortscohorts
• Cohort studies can:•explain the potential consequences of low-dose exposures (both preor postnatal)
• identify critical periods of exposure•clarify if the observed effects are reversible or not.
• Grandjean and Landrigan, 2008:“Large-scale, prospective epidemiological studies, such as birth cohorts fromEurope will be especially informative about early toxic exposures and neurodevelopmental disorders. Data from these investigations, especially when pooledinternationally, will hopefully provide dose-response associations that can guidefuture disease prevention efforts. This research should move beyond repeatedassessments of known neurotoxins to examine chemicals, whose toxicity isjust beginning to be recognised”
More research is needed…using birth cohortsstudies
www.creal.cat
CurrentCurrent knowledgeknowledge
Castoldi et al., 2008
Summary of human studiesregarding Hg andneurodevelopment
www.creal.cat
WP1 - inventory questionnaire
13 cohorts identified:•ALSPAC•Faroe Islands (4 subcohorts)•Duisburg•EDEN•EFESE/ELFE (starts 2011)•FLEHS•INMA (7 subcohorts)•INUENDO •MoBa•PCB cohort•PÉLAGIE•REPRO_PL•RHEA
FutureFuture collaborationcollaboration……
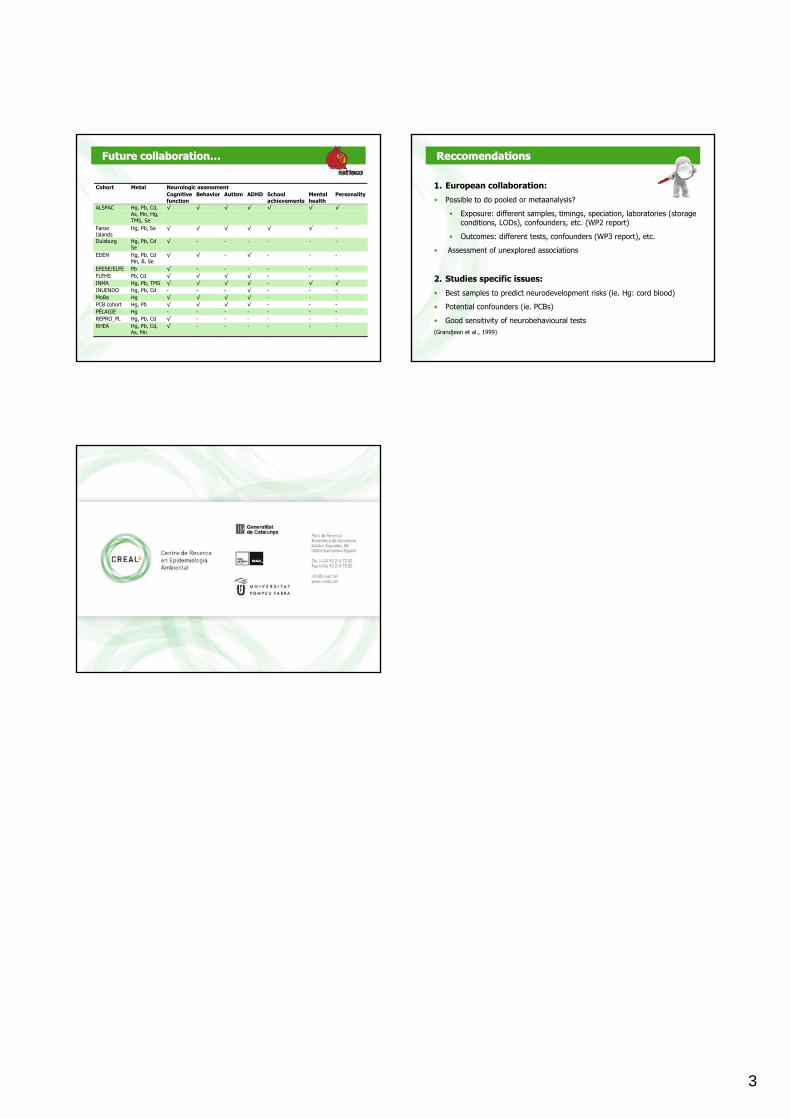
3
www.creal.cat
FutureFuture collaborationcollaboration……
Neurologic assessment Cohort Metal Cognitive function
Behavior Autism ADHD School achievements
Mental health
Personality
ALSPAC Hg, Pb, Cd, As, Mn, Hg, TMS, Se
√ √ √ √ √ √ √
Faroe Islands
Hg, Pb, Se √ √ √ √ √ √ -
Duisburg Hg, Pb, Cd Se
√ - - - - - -
EDEN Hg, Pb, Cd Mn, B, Se
√ √ - √ - - -
EFESE/ELFE Pb √ - - - - - - FLEHS Pb, Cd √ √ √ √ - - - INMA Hg, Pb, TMS √ √ √ √ - √ √ INUENDO Hg, Pb, Cd - - - √ - - - MoBa Hg √ √ √ √ - - - PCB cohort Hg, Pb √ √ √ √ - - - PÉLAGIE Hg - - - - - - - REPRO_PL Hg, Pb, Cd √ - - - - - - RHEA Hg, Pb, Cd,
As, Mn √ - - - - - -
www.creal.cat
ReccomendationsReccomendations
1. European collaboration:
• Possible to do pooled or metaanalysis?
• Exposure: different samples, timings, speciation, laboratories (storageconditions, LODs), confounders, etc. (WP2 report)
• Outcomes: different tests, confounders (WP3 report), etc.
• Assessment of unexplored associations
2. Studies specific issues:
• Best samples to predict neurodevelopment risks (ie. Hg: cord blood)
• Potential confounders (ie. PCBs)
• Good sensitivity of neurobehavioural tests (Grandjean et al., 1999)
www.creal.cat
Plenary Meeting Utrecht May 26-28 2010 1
Bispebjerg Hospital (1)
WP4 exposure-response review:
POPs and birth outcomes
Gunnar Toft et al
ObjectiveReview the epidemiologic evidence on effects of prenatal POP exposure during pregnancy on adverse outcomes in the offspring
Bispebjerg Hospital (2)
A 2004 review by Toft et al (Reprod Toxicol) concluded:
• Some evidence that HIGH concentrations of POPs above current European exposure levels may cause delayed pregnancy, spontaneous abortions, reduced birth weight, skewed sex ratio and changed puberty
• It is uncertain if low level POP exposure may affect birth outcomes
Bispebjerg Hospital (3)
A 2007 review by Wigle et al (Journal of Toxicology and Environmental Health, Part B, 10:3–39, 2007)
Major sources of uncertainty include the limited number of studies conducted on specific expo-sure–outcome relationships and methodologic limitations:
(1) crude exposure indices(2) limited range of exposure levels(3) small sample sizes(4) limited knowledge and control of
potential confounders
Bispebjerg Hospital (4)
Systematic PUBMED literature search 1.1.2007-31.4.2010
Bispebjerg Hospital (5)
Exposures: selection of POPs• chlordane• DDT and metabolites• dieldrin and endrin• Heptachlor• Hexachlorobenzene• Mirex• Polychlorinated biphenyls • Polychlorinated dibenzo-p-dioxins• Polychlorinated dibenzo furans• Toxaphene• Brominated flame retardants• Flourinated compounds• Organometallic compunds (TBT)
Bispebjerg Hospital (6)
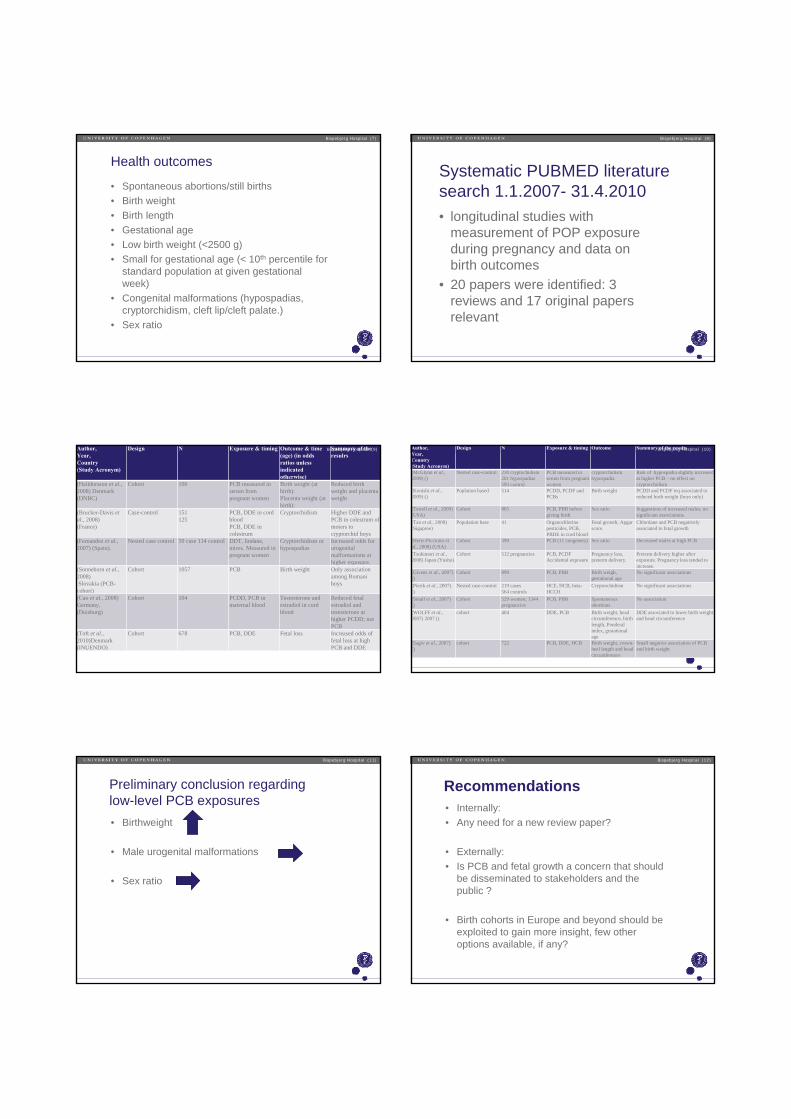
Health outcomes
• Spontaneous abortions/still births• Birth weight• Birth length• Gestational age• Low birth weight (<2500 g)• Small for gestational age (< 10th percentile for
standard population at given gestational week)
• Congenital malformations (hypospadias, cryptorchidism, cleft lip/cleft palate.)
• Sex ratio
Bispebjerg Hospital (7)
Systematic PUBMED literature search 1.1.2007- 31.4.2010• longitudinal studies with
measurement of POP exposure during pregnancy and data on birth outcomes
• 20 papers were identified: 3 reviews and 17 original papers relevant
Bispebjerg Hospital (8)
Author,Year, Country (Study Acronym)
Design N Exposure & timing Outcome & time (age) (in odds ratios unless indicated otherwise)
Summary of the resulrs
(Halldorsson et al., 2008) Denmark (DNBC)
Cohort 100 PCB measured in serum from pregnant women
Birth weight (at birth): Placenta weight (at birth):
Reduced birth weight and placenta weight
(Brucker-Davis et al., 2008)(France)
Case-control 151 125
PCB, DDE in cord bloodPCB, DDE in colestrum
Cryptorchidism Higher DDE and PCB in colestrum of moters to cryptorchid boys
(Fernandez et al., 2007) (Spain).
Nested case control 50 case 114 control DDT, lindane, mirex. Measured in pregnant women
Cryptorchidism or hypospadias
Increased odds for urogenital malformations at higher exposure.
(Sonneborn et al., 2008)Slovakia (PCB-
cohort)
Cohort 1057 PCB Birth weight Only association among Romani boys
(Cao et al., 2008)Germany,(Duisburg)
Cohort 104 PCDD, PCB in maternal blood
Testosterone and estradiol in cord blood
Reduced fetal estradiol and testosterone at higher PCDD; not PCB
(Toft et al., 2010)Denmark (INUENDO)
Cohort 678 PCB, DDE Fetal loss Increased odds of fetal loss at high PCB and DDE
Bispebjerg Hospital (9) Author,Year, Country (Study Acronym)
Design N Exposure & timing Outcome Summary of the results
(McGlynn et al., 2009) ()
Nested case-control 230 cryptochidism201 hypospadias593 control
PCB measured in serum from pregnant women
cryptorchidism hypospadia
Risk of hypospadia slightly increased at higher PCB – no effect on cryptorchidism
(Konishi et al., 2009) ()
Poplation based 514 PCDD, PCDF and PCBs
Birth weight PCDD and PCDF teq associated to reduced birth weight (boys only)
(Terrell et al., 2009) (USA)
Cohort 865 PCB, PBB before giving birth
Sex ratio Suggestions of increased males; no significant associations.
(Tan et al., 2009) (Sigaproe)
Population base 41 Organochlorine pesticides, PCB, PBDE in cord blood
Fetal growth; Apgar score.
Chlordane and PCB negatively associated to fetal growth
(Hertz-Picciotto et al., 2008) (USA)
Cohort 399 PCB (11 congeners) Sex ratio Decreased males at high PCB
(Tsukimori et al., 2008) Japan (Yusho)
Cohort 512 pregnancies PCB, PCDFAccidental exposure
Pregnancy loss, preterm delivery.
Preterm delivery higher after exposure. Pregnancy loss tended to increase.
(Givens et al., 2007) ()
Cohort 899 PCB, PBB Birth weigh, gestational age
No significant associations
(Pierik et al., 2007) ()
Nested case-control 219 cases564 controls
HCE, HCB, beta-HCCH
Cryptorchidism No significant associations
(Small et al., 2007) ()
Cohort 529 women; 1344 pregnancies
PCB, PBB Spontaneous abortions
No association
(WOLFF et al., 2007) 2007 ()
cohort 404 DDE, PCB Birth weight, head circumference, birth length, Ponderal index, gestational age
DDE associated to lower birth weight and head circumference
(Sagiv et al., 2007) ()
cohort 722 PCB, DDE, HCB Birth weight, crown-heel length and head circumference
Small negative association of PCB and birth weight
Bispebjerg Hospital (10)
Preliminary conclusion regarding low-level PCB exposures• Birthweight
• Male urogenital malformations
• Sex ratio
Bispebjerg Hospital (11)
Recommendations• Internally:• Any need for a new review paper?
• Externally:• Is PCB and fetal growth a concern that should
be disseminated to stakeholders and the public ?
• Birth cohorts in Europe and beyond should be exploited to gain more insight, few other options available, if any?
Bispebjerg Hospital (12)
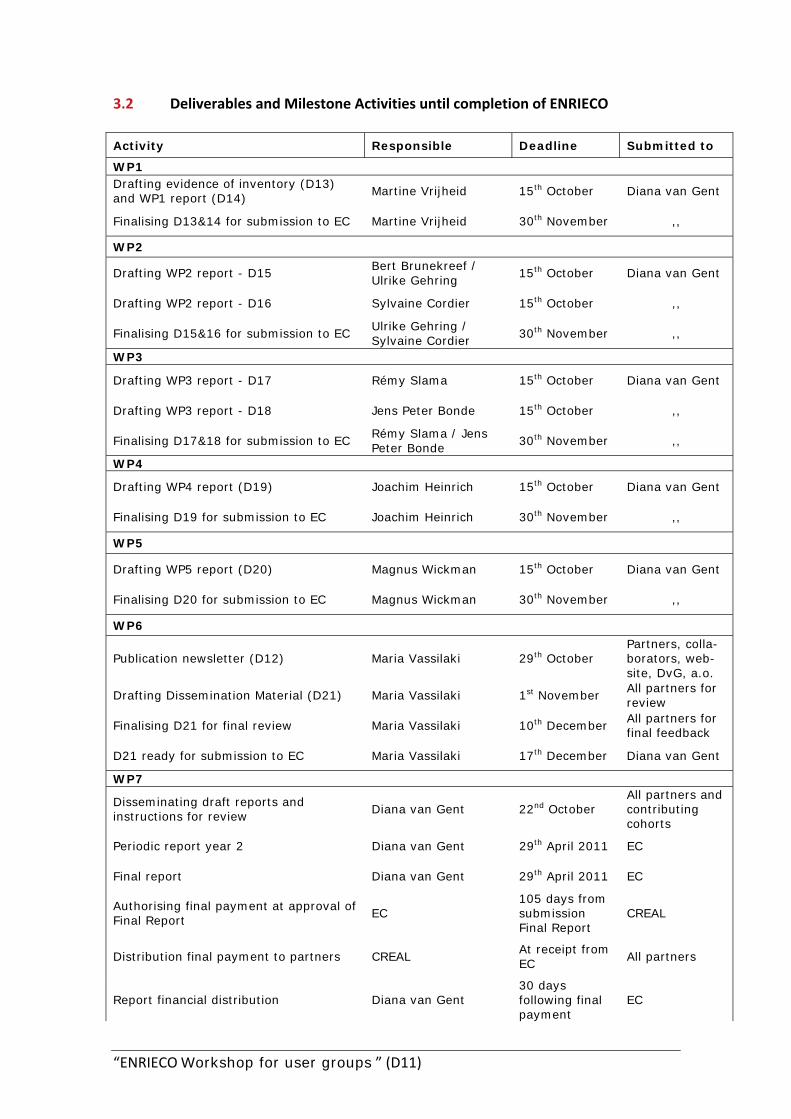
“ENRIECO Workshop for user groups ” (D11)
3.2 Deliverables and Milestone Activities until completion of ENRIECO Activity Responsible Deadline Submitted to
WP1 Drafting evidence of inventory (D13) and WP1 report (D14)
Martine Vrijheid 15th October Diana van Gent
Finalising D13&14 for submission to EC Martine Vrijheid 30th November ,,
WP2
Drafting WP2 report - D15 Bert Brunekreef / Ulrike Gehring
15th October Diana van Gent
Drafting WP2 report - D16 Sylvaine Cordier 15th October ,,
Finalising D15&16 for submission to EC Ulrike Gehring / Sylvaine Cordier
30th November ,,
WP3
Drafting WP3 report - D17 Rémy Slama 15th October Diana van Gent
Drafting WP3 report - D18 Jens Peter Bonde 15th October ,,
Finalising D17&18 for submission to EC Rémy Slama / Jens Peter Bonde
30th November ,,
WP4
Drafting WP4 report (D19) Joachim Heinrich 15th October Diana van Gent
Finalising D19 for submission to EC Joachim Heinrich 30th November ,,
WP5
Drafting WP5 report (D20) Magnus Wickman 15th October Diana van Gent
Finalising D20 for submission to EC Magnus Wickman 30th November ,,
WP6
Publication newsletter (D12) Maria Vassilaki 29th October Partners, colla-borators, web-site, DvG, a.o.
Drafting Dissemination Material (D21) Maria Vassilaki 1st November All partners for review
Finalising D21 for final review Maria Vassilaki 10th December All partners for final feedback
D21 ready for submission to EC Maria Vassilaki 17th December Diana van Gent
WP7
Disseminating draft reports and instructions for review
Diana van Gent 22nd October All partners and contributing cohorts
Periodic report year 2 Diana van Gent 29th April 2011 EC
Final report Diana van Gent 29th April 2011 EC
Authorising final payment at approval of Final Report
EC 105 days from submission Final Report
CREAL
Distribution final payment to partners CREAL At receipt from EC
All partners
Report financial distribution Diana van Gent 30 days following final payment
EC
“ENRIECO Workshop for user groups ” (D11)
3.2 continued…
Activity Responsible Deadline Submitted to
General
PEC Teleconference Partner representatives
13th September
-
Providing feedback on draft WP reports All partners and contributing cohorts
1st November WP leads
Providing feedback dissemination materials All partners 30th November Maria Vassilaki
PEC Meeting Partner representatives
January 2011 - tbc -
Submission WP information for Periodic Report year 2
WP leads and partner representatives
February 2011 - tbc
Diana van Gent
“ENRIECO Workshop for user groups ” (D11)
3.3 Scientific publications anticipated to be published following the completion of ENRIECO: Large overview papers:
Overall ENRIECO paper discussing findings and recommendations WP1: Inventory of Birth Cohorts WP2: Evaluation of Exposures, including overall recommendations WP5: Database Building: one paper discussing all the case studies performed
Specific papers:
WP2: Evaluation of Exposures: Pesticides
Evaluation of Exposures: Emerging exposures/best methods Evaluation of Exposures: Persistent Organic Pollutants (POPs)
WP3: Evaluation of Health Outcomes: Water (non‐DPPs)
Evaluation of Health Outcomes: Allergy and asthma WP2 and 4: Evaluations of Exposure (and Response): Air pollution
Evaluations of Exposure‐Response (and Response): Water contamination Evaluations of Exposure‐Response (and Response): Heavy metals Evaluations of Exposure‐Response (and Response): Noise




![Agreement number: […] Model grant agreement (mono … · 2017. 12. 14. · Agreement number: […] Model grant agreement (mono beneficiary): October 2016 6 ARTICLE I.8 – SPECIAL](https://img.pdfslide.us/doc/110x75/5fbd350816f85d4961670c83/agreement-number-model-grant-agreement-mono-2017-12-14-agreement-number.jpg)
























