Embed Size (px)
DESCRIPTION
Materi the 2nd MAMCN
Citation preview

NUTRITION IN GERIATRIC WITH COPD
HARUN ALRASYID DAMANIK
FAC.OF MEDICINE UNIVERSITY OF SUMATERA UTARA
/GENERAL HOSPITAL H.ADAM MALIK MEDAN

OBJECTIVES
TO RAISE THE AWARENESS OF MEDICAL NUTRITION WITH RESPIRATORY HEALTHCARE AND GERIATRIC PATIENTS
TO PROVIDE A SIMPLE TOOL TO AID FIRST LINE
MEDICAL NUTRITIONAL THERAPY
TO IMPROVE THE NUTRITIONAL STATUS OF THE GERIATRIC PATIENTS (NUTR.CARE PLAN & MONITOR)
TO UNDERSTAND POSSIBLE, FUTURE, NUTRITION STRATEGY

Epid. & Pathophysiology
Pathophysiology: chronic lung inflammation in response to noxious particles,gases; the 4th cause of death in the world
Taking less O2, retaining CO2
Emphysema,chronic bronchitis,ashmatic bronchitis (irreversible)
“Pink Puffers:significant weight loss,”Blue Bloaters”: normal-overweight
Protein energy malnutrition as a consequence of disease progression
Not apparent until damage is done (underdiagnosed/treatment)

COPD theories & discoveries
1968: rare geneticmarker, defic. α-one-antitrypsin
2006: autoimmune disease
2008:systemic inflammation ↑ plasma leptinRise global mortality (3rd leading cause worldwide,2020)
National Health Education Program
Tayde P,kumar S .COPD in the elderly.Asian J Gerontol Geriatrn2013: 8:90-7

Body Weight in COPD patients
25-40% (FEV1< 50%): significant weight loss
(> 5 % in past 3 months,or >10% in the past 6 month)
Frequently underweight (30-50% by different studies)
Normal BMI with ↓FFM : MR with low BMI and depletion of FFM
17-21 % with Very low BMI (<20 kg/m2),38-45 % with lean body mass depletion
Vestbo et al.Copenhagen City Heart Study.Am J. Resp Crit Care Med 2006,173

Effect of COPD on nutrition
A catabolic wasting disease (19%-74% malnutrition)
Dyspnea & coughing dietary intake <
Fatigue: buying and preparing food ?
Chronic mouth breathingtaste of food ?
Headaches,mental status changes cause by hypercapnia
Pharmacologic agents
Benson et al,Nutr.Clin Prac 5,1990 Antonione R.Basic in Clinical Nutrition 4th ed.ESPEN 2011

COPD....
Low grade inflammatory condition ↑proinflammatory cytokines liver need muscular amino acid to maintain acute phase mediator.
Cytokine direct action on muscle tissue ↓FFM
↑Energy demand during ventilation & systemic inflammationREE >
Systemic inflammatory condition insulin resistance & hyperglycaemia metabolic ?

COPD.............
Mortality by malnutrition (BMI in BODE index)
Respiratory muscle strength <<
Aerobic metabolism <<
Surfactant synthesis & elastic fibre in lung parenchyme <<
↑dyspnea & ventilatory drive
Prolonged ventilators weaning QOL & MR
Impaired immune function (undernutrition) systemic & pulmonal defenceinfection & mortality >

Nutritional Screening
A. S G A
History
Weight Change
Dietary Intake Change Relative to Normal
GI Symptoms (Persisting more than 2 weeks)
Functional Capacity
Disease and its relationship to nutritional requirements

Physical Examination
Loss of subcutaneous fat (triceps, chest)
Muscle wasting (quadriceps, deltoids)
Ankle edema, Sacral Edema
For Each Specify: 0= normal, 1+= Mild, 2+ = Moderate, 3+ = Severe

SGA Rating
Well nourished
Moderately (or suspected of being) malnourished
Severely malnourished

B. Regularly screening (elderly with COPD) using a tool like MNA:
a.Food decline d.Psychological/acute disease
b.Weight loss e.Neuropsychologic problem
c.Mobility f.BMI
>12 point not at risk/no need complement assessment
<11 point possible malnutrition continue assessment
(subtotal screening score 14)

MNA vs SGA in geriatic COPD
patients
Identified more patient as malnutritioned than SGA
Early diagnosis & early administration of MNT
SGA correlated with frequent hospital admissionsbad prognostic markers in COPD
Yuceege MB et al.The Evaluation Of Nutrition in Male COPD using SGA and MNA.International Journal of Internal Medicine 2013,2(1):1-5

Assessment
FFM relates closely to muscle mass gold standard for nutritional evaluation for respiratory failure
Estimated by:
- Anthropometric (skinfold determination)
- Bioimpendance analysis (BIA)
- Dual energy x-ray absorptiometry (DEXA)
FFM depleted FFM index (kg FFM –m2) < 16(♂) and < 15 (♀)

Simple Steps:
1.Review weight history (BW < ?)
2.Calculate BMI
3.Current Nutritional Status
4.Identify for new guideline
5.Appropiate action
6.Review and monitor: quick check about poor quality diet,BW and nutrition every appointment
Nici et al.ATS/ERS Statement on Pulmonary Rehab.Am J Respir Crit Care Med 2006,173:1390-1413

Open question
1.How is your appetite?
2.Are you managing to eat?
3.Any changes in your weight?
4.Any changes to your body shape(muscle strength)?
5.Do you have any concerns about your food intake and diet?

Specific Nutrition Concerns
Shortness of breath/swallowing air
Bloating or gas
Thick mucus
Dental problem
Fatigue
Reliance on oxygen
Constipation
Chronic Disease Network and Access Program 2009

• Intercurrent Illness• Hypercytokinemia
in response to disease
• Increased effort in breathing
Weight Loss
Muscle Waisting
Abnormal diaphragmatic function
Abdominal Distension
and GI Congestion
Difficulty in Eating
Hypoxemia Acidosis
Increased Metabolic
Rate
Metabolic and
Hormonal Aterations
Insulin Resistance, reduced IGF-1,
Reduced Testosterone
Reduced Respiratory
function
Increased Morbidity and
Mortality, Decreased
Quality of Life Modified from R. Antonione in Basics in Clinical Nutrition, Fourth Ed. 2011

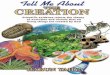
Patophysiology &
Consequences of malnutritionUndernutrition ↓glycoytic & oxidative enzyme impaired skeletal muscle aerobic metabolism phosphocreatine & glycogen enzyme <<
↑ respiratory muscle burden by ↑ lactic acidosis (ventilatory demand)
Chronic hypoxia calcium dependent proteolysis muscle metabolism> , ↑reactive oxygen & cytokine conc.

Protein synthesis & protein breakdown imbalance
Excess in EE,energy intake << muscle wasting
Skeletal muscle impairement & dysfunction + atrophy & structural modification+ global weight loss ↓phsyical activity (FFM <<)
Wasted COPD (↓ plasma glutamine/glutamate/
BCAA) amino acids modification
Glucocorticoid protein & muscle degradation
Beta agonist & hormonal modification unclear

Nutrition Support
A. Energy
Calorie (involuntary weight loss, mechanical efficiency <<), small meal frequent; 35-45 kcal/kg
MNT ( BMI < underweight, 10 % involuntary weight loss in 6 mth, 5% in past, FFM depletion)
Malnourished high energy & protein diet
CH (40%) CO2 production during metabolism, complex CH
High fat diet early satiety, diaphragma movement & thoracic dynamics
Increased meal OxyHB desaturation resp.?

B.Protein
(0,8 g)1-1,5 g/kg/day (1,2-2,0) protein synthesis
Amino- acid supplementation (Glutamine) before exercise benefit for resp.muscle &reduced infective complication; Leucine (60-120 g) also
CKD avoid excess protein
C. Fat: 35% - 55% (20% MCT)

C. Fluid
6 – 8 cup/non carbonated
Water, milk, 100 % juice, tea,soup etc.
Caution : COPD with CHF
D. Sodium (salt)
Recommended 2300 mg sodium or less (1 cth)
Salt subsitutes may not be for everyone

E.Micronutrients: vit.K, Ca, vit.D, P, Mg ?
(osteoporosis: 1200 mg Ca, 700-1000 IU vit.D); analog Vit.D (alphacalcidol/
calcitriol muscle strenght

ESPEN guidelines
Enteral nutrition with excercise and anabolic pharmacotheraphy
Frequent small oral nutr.suppl.
Anker SD et al.ESPEN Guidelines on Enteral Nutrition.Clin Nutr 2006,25:311-8

GHRELIN
Novel GH-releasing peptide
-↓ fat utility & stimulating feeding - positive energy balance Decrease in COPD
repeated administration improves body composition and functional capacity, reduced muscle wasting,
↑ symphatetic in cachectic COPD patient
Nagaya N, et al.Treatment of cachexia with ghrelin in patients with COPD.Chest 2005, 128: 1187-93

Medical Foods
To prevent hypercapniaApproaches to prevent hypercapnia
1.Reduce feeding rate 2.Change to a formula with higher proportion
of fat vs carbohydrateStable COPD : oral nutrition with standard high- protein/high energy
Voss AC,E.Mayer K.Role of Liquid Dietary Supplement in Nutrition in the Prevention & Treatment of Disease,2001,235-6
Zadak Z.et al. Commercially prepared diet for enteral nutrition. Basics in Clinical Nutrition 4rd ed.ESPEN 2011

FOOD Access
Enteral Diet/Formula:
Calorie –dense Diet,limited CH high lipid
Calorie-dense,complet oral supplement,high
Vitamin & mineral; very cold/small sip
(avoid stomach ache/diarrhea)

Conclusion for succesful eating Prepare meals early
Rest & medicated before eating
Oral care before meal
Appetite stimulans
Liquify foods to reduced chewing
Eat small and frequent
Adequate water intake

THANK YOU