Embed Size (px)
Citation preview

May 2009 Healthcare for All Ages
H1N1 (Swine Flu)
American Home Health continues to strive to provide you a straight forward service. E� ective May 4th, 2009, employ-ees will be able to request PTO online. On your next PTO request, please give this new added feature a test drive. If you have any questions, please feel free to contact HR at [email protected] or call at 630.236.3501.
Intestinal Atresia and Stenosis 2Esophageal Atresia and Tra-cheosophageal Fistula
3
Making Work Pay 3
Ra� e Winners 4Laugh a little! 4
Inside this issue:
There has been a lot of talk in the press over the past few daysconcerning Swine Flu, now known as
H1N1. While the virus originallycame from pigs, it has been spreading in humans from person to person.� ere currently is no vaccine to prevent in-fection from H1N1, and it willtake about 4-6 months to manufacture one. As of 29 April, there havebeen 109 con� rmed cases in the US with 1 death in TX. While no one canpredict how many cases will occur or how far it will spread, there aremeasures we can personally take to reduce our risk of exposure:
1. Wash hands frequently with warm wa-ter or use alcohol-based hand sanitizer.
2. Cover coughs and sneezes, and don’t touch your mouth, nose, or eyes.
3. Avoid contact with people who are sick.
� e H1N1 � u has the same symptoms as seasonal � u. If you have thesesymptoms, stay home: sudden fever of 100 degrees F or more, sore throatand/or dry cough, nasal congestion, head-ache, sore joints/body aches,and general fatigue. In addition, this new virus may also cause nausea,vomiting, or diarrhea. Seek immediate medical attention for anyone whohas the � u symptoms above AND experi-ences any of these:
1. Di� cult breathing, shortness of breath2. Pain or pressure in chest or abdomen3. Sudden dizziness or confusion4. Severe or persistent vomiting
Please visit the CDC swine � u website at http://www.cdc.gov/swine� u/and monitor local government and news resources for more information. §
If you missed the com-petency fair, you will not accrue PTO until this requirement is met.
Times are changing and so are we. We are making a big e� ort to catch up with the technology age. About 70% of you opted to complete your in-services online. Since this the � rst time, is a huge response. I am truly grateful for your cooperation, and, as many of you saw, this convenience cannot be beaten. I expect those that didn’t feel comfortable to do it this way this year will give this a try in the years to come.
To those that didn’t complete the in-services online, please be informed that you can login to our site and see the results of your test. � e results are going to remain in our site indefenitly (at least until the next competency fair). I encourage all of you to login and review the results, and, if you missed any of the answers, to see the correct answer (which is also given to you in this report).
To � nalize this section, we would like to say that results encourage more action, and we have been really encouraged byyour response. We look forward to the road ahead.
Respectfully yours, Edward Lara, HR Manager
Note:

Page 2
INTESTINAL ATRESIA AND STENOSIS
What are intestinal atresia and stenosis?Intestinal atresia is a broad term used to describe a complete blockage or obstruction anywhere in the intestine. Stenosis refers to a partial obstruction that results in a narrowing of the opening (lumen) of the intestine. � ough these conditions may involve any portion of the gastrointestinal tract, the small bowel is the most commonly a� ected portion. � e frequencies, symptoms and methods of diagnosis di� er depending on the site of intestinal involvement. Nevertheless, children with all forms of intestinal atresia require surgical treatment.
Pyloric atresia involves an obstruction at the pylorus, which is the passage linking the stomach and the � rst portion of the small intestine (duodenum). � is is quite rare, and tends to run in families. Children vomit stomach contents, and due to the accumulation of intestinal contents and gas, develop a swollen (distended) upper abdomen.
Duodenal atresia: � e duodenum is the � rst portion of the small intestine that receives contents emptied from the stomach. Duodenal atresia occurs in 1 out of every 2,500 live births. Half of the infants with this condition are born prematurely and approximately two-thirds have associated abnormalities of the heart, genitourinary, or intestinal tract. Nearly 40% have Down syndrome. Infants with duodenal atresia usually vomit within hours after birth, and may develop a distended abdomen.
Jejunoileal atresia involves an obstruction of the middle region (jejunum) or lower region (ileum) of the small intestine. � e segment of intestine just before the obstruction becomes massively enlarged (dilated) thus hindering its ability to absorb nutrients and propel its contents through the digestive tract. In 10 to 15% of infants with jejunoileal atresia, part of the intestine dies during fetal development. A signi� cant percentage of infants with this condition also have abnormalities of intestinal rotation and � xation. Cystic � brosis is also an associated disorder and may seriously complicate the management of jejunoileal atresia. Infants with jejunoileal atresia should be screened for cystic � brosis. Infants with jejunoileal atresia, regardless of the subtype, usually vomit green bile within the � rst 24 hours of life. However, those with obstructions farther down in
the intestine may not vomit until two to three days later. Infants often develop a swollen (distended) abdomen and may not have a bowel movement (as is normally expected) during the � rst day of life.
Colonic atresia: � is rare form of intestinal atresia accounts for less than 15% of all intestinal atresias. � e bowel becomes massively enlarged (dilated), and patients develop signs and symptoms similar to those associated with jejunoileal atresia. Colonic atresia may occur in conjunction with small bowel atresia, Hirschsprung’s disease or gastroschisis.
How are intestinal atresia and stenosis treated?Children with intestinal atresia and stenosis require an operation, and the exact type of operation di� ers depending on the location of the obstruction. Prior to the operation, all babies must be stabilized. � e excess intestinal contents and gas that contribute to abdominal swelling (distention) is removed through a tube that is placed into the stomach through the mouth or nose. Removing air and � uid from the intestinal tract can prevent vomiting and aspiration, and reduce the risk of bowel perforation. It also provides babies with some comfort as abdominal swelling is relieved. Intravenous � uids are given to replace vital electrolytes and � uid that has been lost through vomiting. Once the baby is stabilized, surgery is performed to repair the obstruction.
What is the long-term outlook?Children who undergo surgery for intestinal atresia require regular follow-up to ensure adequate growth and development, and to avoid nutritional de� ciencies that may occur as a result of the loss of intestine.How babies progress depends to a large extent on whether there is an associated abnormality and whether or not the baby is left with an adequate length of intestine. In general, however, most babies do well. Complications after surgery are rare, but may occur. In the immediate to early postoperative period, intestinal contents may leak at the suture line where the ends of the bowel were sewn together. � is may cause an infection within the abdominal cavity and require additional surgery. Complications that may later occur include malabsorption syndromes, functional obstruction due to an enlarged and paralyzed segment of intestine, or short gut syndrome.§

Page 3
Esophageal Atresia and Tracheoesophageal Fistula
Introduction: Esophageal atresia refers to a congenitally interrupted esophagus. One or more � stulae may be present between the malformed esophagus and the trachea. Tracheoesophageal � stula (TEF) refers to an abnormal opening between the trachea and esophagus.
Problem: � e lack of esophageal patency prevents swallowing. In addition to preventing normal feeding, this problem may cause infants to aspirate and literally drown in their own saliva, which quickly over� ows the upper pouch of the obstructed esophagus. If a TEF is present, � uid (either saliva from above or gastric secretions from below) may � ow directly into the tracheobronchial tree.Frequency: � e incidence of esophageal atresia is 1 case in 3000-4500 births. Etiol-ogy: Currently, most authorities believe that the development of esophageal atresia has a nongenetic basis. Debate about the embryopathologic process of this condition continues, and little about it is known.
Pathophysiology: � e variants of esophageal atresia have been described using many anatomic classi� cation systems. A fetus with esophageal atresia cannot e� ectively swallow amniotic � uid, especially when TEF is absent. In a fetus with esophageal atresia and a distal TEF, some amniotic � uid presumably � ows through the trachea and down the � stula to the gut. Polyhydramnios may be the result of this change in the recycling of amniotic � uid through the fetus. � e fetus also appears to derive some nutritional bene� t from the ingestion of amniotic � uid; thus, fetuses with esophageal atresia may be small for their gestational age.
Presentation and Associated AnomaliesCharacteristically, the neonate born with esophageal atresia drools and has substantial mucus, with excessive oral secretions. If suckling at the breast or bottle is allowed, the baby appears to choke and may have di� culty maintaining an airway. Signi� cant respiratory distress may result. If an oral tube is placed to suction the stomach, as it is in some delivery rooms, it characteristically becomes blocked 10-11 cm from the lips. � e overall incidence of associated anomalies is approximately 50%. Cardiovascular anomalies occur in 35% of cases, genitourinary anomalies occur in 20% of cases, and associated gastrointestinal anomalies occur in approximately 20% of cases.
• Vertebral defects, anorectal malformations, cardiovascular defects, tracheoesopha-geal defects, renal anomalies, and limb deformities (VACTERL) are associated anomalies. If any of these anomalies are present, the presence of the others must be assessed. � e VACTERL syndrome occurs when 3 or more of the associated anomalies are present. � is syndrome occurs in approximately 25% of all patients with esophageal atresia.
• Other associated conditions include coloboma, heart defects, atresia choanae, devel-opmental retardation, genital hypoplasia, and ear deformities (CHARGE).
� e following anomalies also occur with increased frequency in esophageal atresia
• Neurologic defects, GI defects, Respiratory defects, Genitalia defects.• Also, trisomies 13, 21, or 18 may be present. §
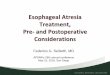
Common anatomical types of esopha-geal atresia
a. Esophageal atresia with distal tra-cheoesophageal � stula (86%).
b. Isolated esophageal atresia without tracheoesophageal � stula (7%).
c. H-type tracheoesophageal � stula (4%).
Esophageal atresiaClassi� cation and external resources
Did you notice that your paycheck was slightly larger in April? � e increase is due to a provision of the
American Reinvestment and Recovery Act signed by President Obama on February 17, 2009. � e provision is called the Making Work Pay tax credit.
For 2009 and 2010, the “Making Work Pay” tax credit provides a refundable tax credit of 6.2 percent of earned income up to $400 for working individuals or $800 for married taxpayers.Families should see at least a $65 dollar per month increase in their take home pay.
MAKING WORK PAY� e credit will phase out for taxpayers with adjusted gross income in excess of $150,000 for married couples � ling jointly and $75,000 for other workers, and thus is fully phased out for taxpayers with modi� ed adjusted gross income in excess of $190,000 for married workers and $95,000 for other workers.
� e IRS issued a new set of withholding tables structured to get a tax credit to America’s workers in cash over the course of the year. By reducing required withholding amounts, workers’ take home pay was increased immedi-ately.

Page 4
Winner Prize Item Gi� Provided ByAna M. Calculator with Writing Pad HumanaAndrea T. Calculator with Writing Pad HumanaCarol W. Digital Photo Frame American Home HealthCarolyn W. American Home Health Tee-Shirt American Home HealthCathy H-B. American Home Health Tee-Shirt American Home HealthCharlene D. Calculator with Writing Pad HumanaClaudia M. Calculator with Writing Pad HumanaDeb R. American Home Health Tee-Shirt American Home HealthDelicia H. Garmin GPS American Home HealthDiane B. Digital Photo Frame - credit card size American Home HealthFlorence L. Calculator with Writing Pad HumanaJanet H. Calculator with Writing Pad HumanaJean J. Kodak Camera American Home HealthJune W-S. American Home Health Tee-Shirt American Home HealthKaren F. American Home Health Tee-Shirt American Home HealthLouva L. American Home Health Tee-Shirt American Home HealthMarion M. $50 McNalley’s Gi� Card Assurance AgencyMartha R. American Home Health Tee-Shirt American Home HealthMelinda K. $50 McNalley’s Gi� Card Assurance AgencyMichelle G. Cubs Tickets with Parking Pass Insurance Plans AgencySherel H. American Home Health Tee-Shirt American Home HealthSr. Brigitta N. Calculator with Writing Pad HumanaTeresa H. American Home Health Tee-Shirt American Home HealthTinesia N. American Home Health Tee-Shirt American Home Health
Congratulations!
Laugh a little!
For General Newsletter Submissions, please contact Edward Lara or Karen Centowski at 630.236.3501 or [email protected] Home Health Corp.
You are a winner of a door or ra� e ticket prize from the 6th Annual Competency Fair