Embed Size (px)
Citation preview

10/8/13
1
Defect Analysis & Prevention
Preventing OB Adverse Events Collaborative
October 15, 2013
CUSP: Comprehensive Unit-based Safety Program
http://www.ahrq.gov/cusptoolkit/
Definitions
Defect: Any clinical or operational event or situation that you would not want to happen again. May include events that you believe actually caused harm or put patients at risk for significant harm.
Johns Hopkins’s “Learning from Defects” tool. Appendix G of On the CUSP: Stop BSI toolkit at http://www.onthecuspstophai.org/StopManu-7618.html. Accessed June 2010
10/8/13
2
Definitions
Defect Analysis: The process of analyzing a defect to determine its root cause
Defect Prevention: The process of addressing root causes of defects to prevent their future occurrence
Lanier K. Experiences In Root Cause Analysis and Defect Prevention Methods. Presentation publically available at http://www.dtic.mil/ndia/2004cmmi/CMMIT5Tue/Root_CauseAnalysis.pdf
Accessed April 2010.
What’s in a Name?
• Defect analysis • Root cause analysis • Epidemiological investigation
1. What happened? 2. What caused it? 3. How do we prevent it from happening
again?
Normalization of Deviance (at-risk behaviors)
• Long-term phenomenon in which individuals or teams repeatedly accept a lower standard of performance until that lower standard becomes the “norm”
• I.e. what starts out as a deviation from SOP becomes routine practice and is “normalized.” It becomes acceptable and may no longer even be recognized as deviation
• Allowed because we get away with it…most of the time…

10/8/13
3
Rene Amalberti, MD, PhD
HIGH Production Performance LOW LOW
In
divi
dual
Ben
efits
HIG
H
ACCIDENT
VERY
UN
SAFE
SPA
CE
‘Illegal normal’ Real Life standards
60-90%
100% Agreement Non - acceptable
Safety Reg’s & good practices, accreditation standards
100%
Expected safe space of action as defined by professional standards
Usual Space Of Action
Systemic Migration of Boundaries: Deviation is Normal
Behavior Drift
Healthcare “Speed Limits” ??
• Inconsistent hand hygiene practices • Not performing patient ID checks all the time,
every time • Inconsistent practices for scheduling elective
deliveries • Not following Isolation Precautions • What are they on your unit? • What happens when it catches up with us?
10/8/13
4
Excuses to Deviate
• “The rule(s) is stupid” • Rule or reason for it is unknown • New technology • Complexity of work • Rule does not apply to this patient • “Rule(s) doesn’t apply to me” • “I know a better way” • Competing priorities: Cost & time; culture (politics,
hierarchy, lack of communication openness, etc.) • Perception of risks and related consequences
Errors in Complex Systems
Active Failures
• Errors that occur at the point of contact between a human and some aspect of a larger system (e.g., a human-machine interface)
• They are generally readily apparent (e.g., pushing an
incorrect button, ignoring a warning light) and almost always involve someone at the frontline or “sharp end”
Reason JT. Human Error. New York, NY: Cambridge University Press; 1990.
10/8/13
5
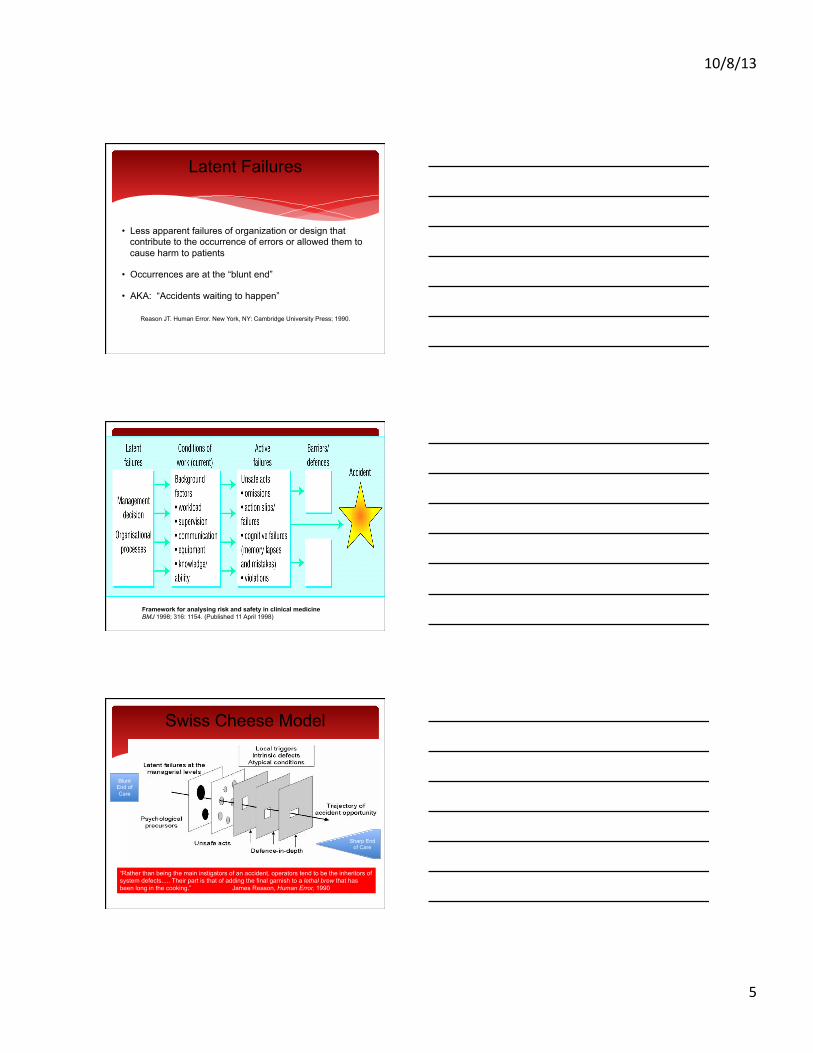
Latent Failures
• Less apparent failures of organization or design that contribute to the occurrence of errors or allowed them to cause harm to patients
• Occurrences are at the “blunt end”
• AKA: “Accidents waiting to happen”
Reason JT. Human Error. New York, NY: Cambridge University Press; 1990.
Framework for analysing risk and safety in clinical medicine BMJ 1998; 316: 1154. (Published 11 April 1998)
Swiss Cheese Model
Blunt End of Care
Sharp End of Care
“Rather than being the main instigators of an accident, operators tend to be the inheritors of system defects..... Their part is that of adding the final garnish to a lethal brew that has been long in the cooking.” James Reason, Human Error, 1990

10/8/13
6
Hindsight Bias
The phenomena in which how an accident/error occurred seems obvious after it has occurred.
“I predicted this was going to happen!”
Agans R., The hindsight bias: The role of the availability heuristic and perceived risk. Basic and Applied Social Psychology. Vol 15;4. December 1994. 439-449.
Getting to Frontline Reality
• Gemba walk: A Japanese term used in Lean methodology that means, “the real place.” In a business sense, it refers to the place where value is created. The idea behind gemba is that observation where the work is actually carried out, such as on the nursing unit, is where you learn both what the actual problems are and the best solutions for those problems. A gemba walk is an activity that takes management to the point of care to find ground truth
• Ground truth: Information that is collected on location and used to compare reality to perception.
Tips on Learning From Each Defect
• Analysis of a defect should occur as soon as possible after the defect is recognized. Do you have a process in place to learn about defects as soon as they are recognized?
• Use some type of standard investigation tool
• Utilize a multidisciplinary team
• Investigate details prior to meeting
• If you already have some type of similar process in place, build on that. (some people call it their “mini-RCA”, a “deep dive” etc.)
• Don’t be afraid to really challenge practice and traditional ways of thinking!
• Environment of psychological safety is critical to learn from defect.
10/8/13
7
Defect Analysis and Prevention
Most critical step is to include the right folks: • Obstetrical services • OB(s) & their office staffs • Schedulers • Administration • Nursing • Quality, Safety, Risk representatives as appropriate • Patient/Family as appropriate • Who else? Think through who would make sense…
Basic Steps in the “L-from-D” Process
1. What happened?
2. Why did it happen?
3. How will you reduce the likelihood of it happening again?
4. How will you know the risk is reduced?
5. With whom should you share the learning?
Step 1: What Happened?
• Use a standard event investigation format • Tool should be easy to use and tailored for your organization
• Must establish a chronological order of events and data related to the event
• Requires some research and gemba walks
• One person should not do all the research or gemba walks (Science of Safety principle: Teams make wise decisions when there is diverse and independent input.)
10/8/13
8
Don’t Forget Critical Info!
Assess for latent failures: go “upstream” from the defect to identify issues in the blunt realm of care delivery.
• Staffing at time of event • Emotional/psychological aspects of the team and the patient when
the delivery was scheduled/ when the hard stop was ignored • Environmental conditions at time of event (consider environment in
room/unit, facility)
Build in key questions onto event tool Resource: http://www.onthecuspstophai.org/stop-bsi/manuals-and-toolkits/
Step 2: Why Did It Happen?
• Patient factors • Task factors • Caregiver factors • Team factors • Training and education factors • IT factors • Local environment • Institutional environment
Step 3: How Can We Prevent It From Happening Again?
• Interventions to reduce the risk of it happening again
• Interventions need to address the key contributing factors
10/8/13
9
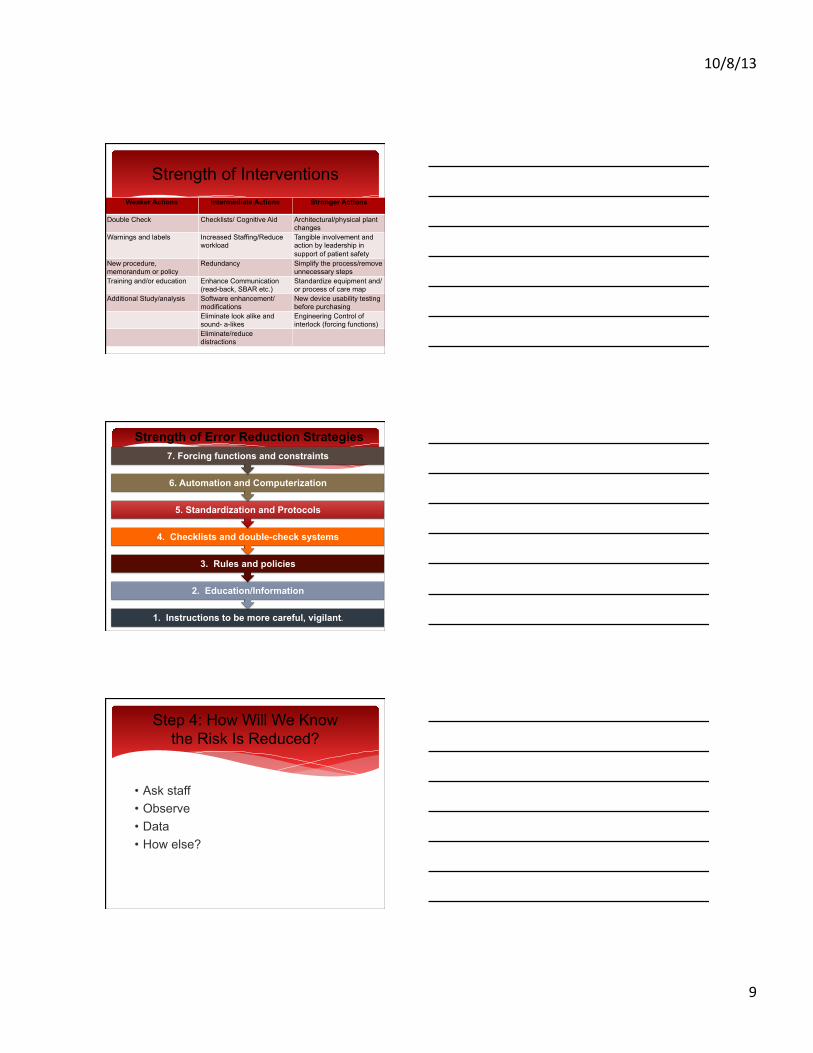
Strength of Interventions Weaker Actions Intermediate Actions Stronger Actions
Double Check Checklists/ Cognitive Aid Architectural/physical plant changes
Warnings and labels Increased Staffing/Reduce workload
Tangible involvement and action by leadership in support of patient safety
New procedure, memorandum or policy
Redundancy Simplify the process/remove unnecessary steps
Training and/or education Enhance Communication (read-back, SBAR etc.)
Standardize equipment and/ or process of care map
Additional Study/analysis Software enhancement/modifications
New device usability testing before purchasing
Eliminate look alike and sound- a-likes
Engineering Control of interlock (forcing functions)
Eliminate/reduce distractions
Strength of Error Reduction Strategies
1. Instructions to be more careful, vigilant.
2. Education/Information
3. Rules and policies
4. Checklists and double-check systems
5. Standardization and Protocols
6. Automation and Computerization
7. Forcing functions and constraints
Step 4: How Will We Know the Risk Is Reduced?
• Ask staff • Observe • Data • How else?
10/8/13
10
Step 5: With Whom Should We Share This Learning?
• Leadership • Providers • Staff • Boards • Other hospitals • Patients
Case Study
• Zoe is a primigravida and her pregnancy has been uncomplicated. She has nl aches/pains of pregnancy
• Large family • Brother is being deployed • Family history of EED • Doctor wants to please patients so induces early • Knows of guidelines but doesn’t follow them, no bad
outcome • Although discussed no hard stop is in place • Nursing staff notes Zoe is 37 weeks • Baby has complications
Step 1: What Happened?
• Zoe requests early delivery at 36 week prenatal check • Zoe and her family are unaware of the risks of EED • Dr. Partee wants to please his patients • Dr. Partee is aware of the ACOG guideline but doesn’t follow
them • Dr. Partee has not had a bad outcome with an EED • Dr. Partee is not aware of complications from EED • Dr. Partee schedules Zoe’s induction at 37 weeks
10/8/13
11
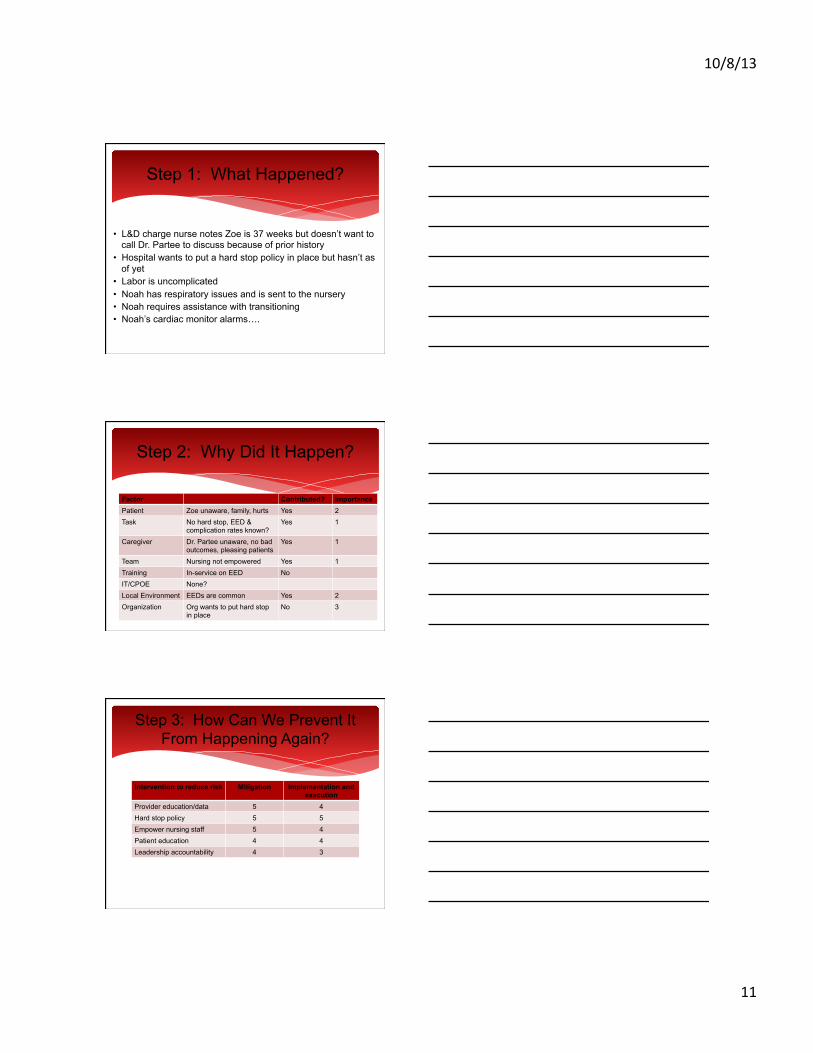
Step 1: What Happened?
• L&D charge nurse notes Zoe is 37 weeks but doesn’t want to call Dr. Partee to discuss because of prior history
• Hospital wants to put a hard stop policy in place but hasn’t as of yet
• Labor is uncomplicated • Noah has respiratory issues and is sent to the nursery • Noah requires assistance with transitioning • Noah’s cardiac monitor alarms….
Step 2: Why Did It Happen?
Factor Contributed? Importance Patient Zoe unaware, family, hurts Yes 2 Task No hard stop, EED &
complication rates known? Yes 1
Caregiver Dr. Partee unaware, no bad outcomes, pleasing patients
Yes 1
Team Nursing not empowered Yes 1 Training In-service on EED No IT/CPOE None? Local Environment EEDs are common Yes 2 Organization Org wants to put hard stop
in place No 3
Step 3: How Can We Prevent It From Happening Again?
Intervention to reduce risk Mitigation Implementation and execution
Provider education/data 5 4 Hard stop policy 5 5 Empower nursing staff 5 4 Patient education 4 4 Leadership accountability 4 3
10/8/13
12
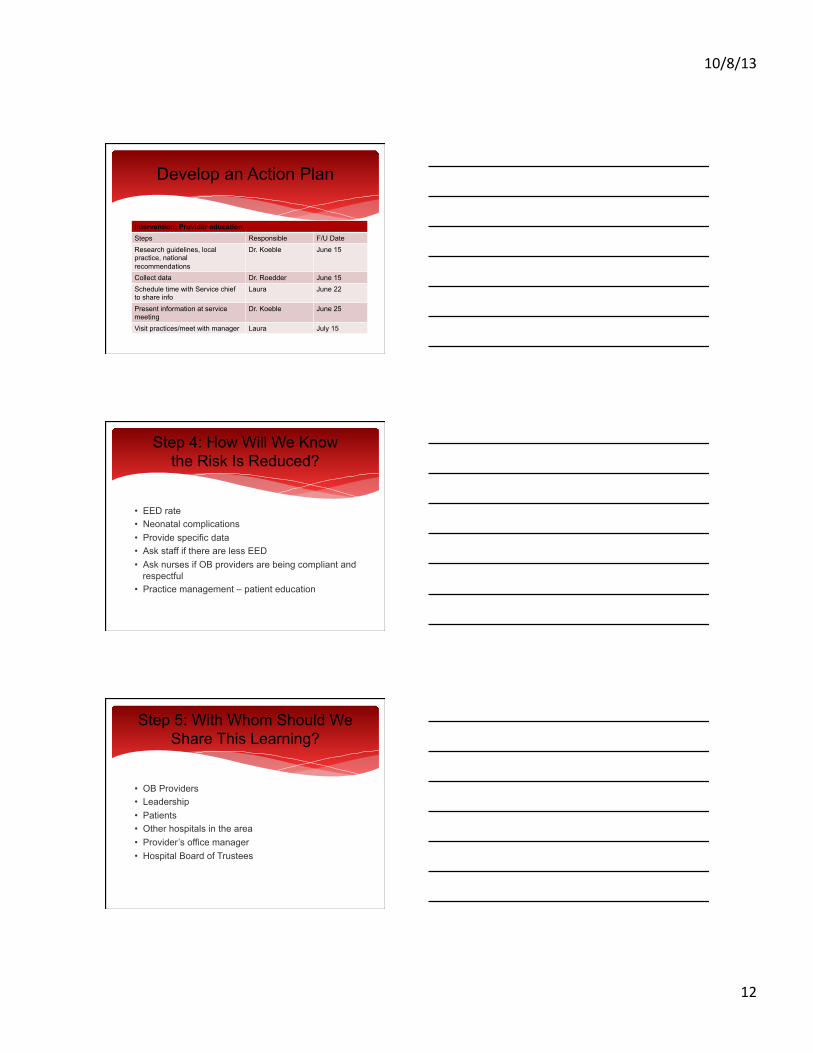
Develop an Action Plan
Intervention: Provider education Steps Responsible F/U Date Research guidelines, local practice, national recommendations
Dr. Koeble June 15
Collect data Dr. Roedder June 15 Schedule time with Service chief to share info
Laura June 22
Present information at service meeting
Dr. Koeble June 25
Visit practices/meet with manager Laura July 15
Step 4: How Will We Know the Risk Is Reduced?
• EED rate • Neonatal complications • Provide specific data • Ask staff if there are less EED • Ask nurses if OB providers are being compliant and
respectful • Practice management – patient education
Step 5: With Whom Should We Share This Learning?
• OB Providers • Leadership • Patients • Other hospitals in the area • Provider’s office manager • Hospital Board of Trustees
10/8/13
13
From: Duke Patient Safety Center, dukepatientsafetycenter.com
Learning from Defects Analysis:
• Preventing error and harm • Consistent discipline • “Diverse and Independent Input” • Drives constructive open communication
Comments and Discussion
10/8/13
14
Shoulder Dystocia Case Study
• Patient Anna is obese and the baby is large • Dr. Jones is new to the hospital, young, eager to be liked,
learning the ropes • Smaller hospital, very few cases of shoulder dystocia are
documented, but nurses suspect more occur than are documented.
• Anna proceeds well with labor, unremarkable, but during delivery Dr. Jones is unable to move the baby
• Nursing staff suspect shoulder dystocia and begin the protocol for that (timing, calling out time, obtain the stepstool, etc) although Dr. Jones does not ever say “shoulder dystocia”
Shoulder Dystocia Case Study
• Dr. Jones attempts the appropriate maneuvers, but is initially unsuccessful
• Nurses call out the time elapsed. Nurse Josie asks Dr. Jones if she should call for assistance. He says “no”
• Staff are stressed and anxious, Dr. Jones is agitated and upset, chaos ensues
• Baby is delivered successfully, without harm
Learning from Defects
1. What happened? 2. Why did it happen? 3. How will we reduce the likelihood of it happening
again? 4. Action plan for each intervention 5. How will you know risk is reduced?