-
8/2/2019 2 Bacteria UC Probiotic
1/22
1
MEDICAL ASPECTS OF GASTROINTESTINAL BIOFILMS
Graeme A. OMay*, Jennifer A.J. Madden, Aileen Kennedy &
Sandra Macfarlane
University of Dundee, MRC Microbiology and Gut Biology Group,
Department of
Molecular and Cellular Pathology, Level 6, Ninewells Hospital
and Medical School,
Dundee, UK.
Abstract
The human gastrointestinal tract has a large surface area
available for biofilm
formation. Biofilm communities are in direct contact with the
host and are thus prime
candidates for involvement in host-microbe interaction. In this
article, we focus on
the role of these communities in patients with inflammatory
bowel disease and those
undergoing percutaneous endoscopic gastrostomy tube feeding.
Rectal mucosal
populations in both healthy and ulcerative colitis patients are
outlined. Anaerobic
bacteria outnumbered facultative anaerobes in both patient
groups. However,
healthy people had more bifidobacteria and prevotella and fewer
Gram-positive
cocci, lactobacilli and clostridia than UC patients. Biofilms
dominated by Yeasts,
Enterococcus, Staphylococcus, Bacillus andLactobacillus spp.
were detected on
percutaneous endoscopic gastronomy (PEG) tubes. PEG tube
biofilms contribute to
tube deterioration and may provide reservoirs for potential
pathogens, making them
difficult to eradicate using chemotherapeutic methods. Treatment
with probiotics
offers an alternative to chemotherapy in some instances,
although the
mechanisms by which probiotic microorganisms interact with
gastrointestinal (GI)
biofilms remain poorly understood.
-
8/2/2019 2 Bacteria UC Probiotic
2/22
2
Introduction
The human gastrointestinal (GI) tract extends from the
oesophagus to the rectum
and harbours a diversity of microhabitats which are colonised by
microorganisms to
varying degrees, depending on local environmental conditions. A
gradient of
colonisation exists from the sparsely-populated oesophagus and
stomach to the
descending colon and rectum, which may contain up to 1012
culturable bacteria per
gram contents (Hopkins et al. 2002). Evolution has dictated that
these organs
possess a large surface area to facilitate efficient nutrient
uptake. This, together with
high nutrient availability and a constant influx of
microorganisms as well as stable
autochthonous populations, makes the GI tract an ideal site for
the development of
sessile microbial communities. Those microorganisms in closest
proximity to host
tissues have the most opportunity for interaction with host
physiology and
metabolism; thus mucosal populations are an important component
of any host-
microbiota interaction, whether it be beneficial or
detrimental.
The human GI microbiota performs a number of beneficial
functions. These
include vitamin synthesis (Conly et al. 1994), absorption of
calcium, magnesium and
iron (Miyazawa et al. 1996, Younes et al. 2001), production of
colonic enterocyte
nutrients (Cummings et al. 1987) and immune
stimulation/regulation (Tannock
2001). Additionally, in colonisation resistance the normal
microbiota is known to
assist in preventing colonisation of the GI tract by
opportunistic invaders such as
Clostridiumdifficile (van der Waaij 1989).
Conversely, the GI tract microbiota has also been implicated in
disease states
such as inflammatory bowel disease (Macpherson et al. 1996),
colonic (Horie et al.
1999) and gastric (Bjorkholm et al. 2003) carcinoma and
irritable bowel syndrome
(Wyatt et al. 1988). Additionally, the microbiota has an
important role in almost any
-
8/2/2019 2 Bacteria UC Probiotic
3/22
3
medical situation involving the GI tract; for example, abdominal
surgery and enteral
nutrition. In these situations, although the GI tract microbiota
may not be the original
cause of the required intervention, it often influences the
outcome.
The research outlined in this article concentrates on the effect
of the GI
microbiota, particularly sessile populations, on patients
receiving enteral nutrition
through a percutaneous endoscopic gastrostomy (PEG) tube and in
those suffering
from inflammatory bowel disease (IBD).
Mucosal populations in ulcerative colitis
Ulcerative colitis (UC) is a chronic relapsing form of IBD of
unknown aetiology. The
inflammatory response in UC is primarily located in the colonic
mucosa and
submucosa. The distal colon is always affected and the disease
may progress
towards the proximal bowel with crypt abscesses causing severe
tissue damage.
Bacterial involvement has been proposed in both the initiation
and maintenance
stages of UC (Hill et al. 1971). Antimicrobial agents
specifically active against
obligate anaerobes have been shown to prevent ulceration in
guinea pigs
(Onderdonk & Bartlett 1979) and experiments using germ-free
animals show that
they only develop colitis when repopulated with bacteria
(Sadlack et al. 1993). A
variety of species including fusobacteria, Shigella (Onderdonk
1983) and adhesive
E. coli(Chadwick 1991) isolated from the colitic bowel have been
implicated;
however, no specific organism has been found in all patients.
The luminal microbiota
of UC patients has been examined in many studies (van der
Wiel-Korstanje &
Winkler 1975, von Wufflen et al. 1989) and there is good
evidence for postulating
that bacteria growing on the gut wall play a major role in UC,
since they exist in close
juxtaposition to host tissues and can interact with the host
immune and
-
8/2/2019 2 Bacteria UC Probiotic
4/22
4
neuroendocrine systems. Electron microscope studies of human
colonic biopsy
tissue have suggested that mucosal bacteria are associated more
closely with the
mucus layer than the epithelial surface (Hartley et al. 1979).
Distinct populations are
known to exist on the mucosal surface and in the mucus layer in
the large gut, where
bacteroides and fusobacteria appear to predominate, but other
groups such as
eubacteria, clostridia and anaerobic Gram-positive cocci are
also present as either
heterogeneous populations or microcolonies (Croucheret al. 1983,
Edmiston et al.
1982). There have been few studies on bacteria that inhabit the
colonic mucosa
because faeces and material from the gut lumen are more readily
available for
investigation and in most studies, the patients have been
pre-treated with antibiotics
and drugs, or the bowel has been purged before colonoscopy. As a
consequence
the metabolic and health-related significance of bacteria
growing on the colonic
mucosa is largely unknown.
The objectives of the study were to enumerate and characterise
mucosal bacterial
communities in healthy people and in patients with UC. Rectal
biopsies were chosen
because the rectum is usually devoid of faecal material and
patients did not need to
be treated before the tissues were removed.
Samples (four UC, five normal) were obtained from patients
attending the
Gastroenterology Out-patients Clinic at Ninewells Hospital,
Dundee. None of the
patients were taking antibiotics or any other drugs. Tissue
samples were
immediately placed in anaerobic transport medium, brought to the
laboratory and
measured, homogenised and plated out onto a range of selective
and non-selective
agars. The bacteria were then characterised on the basis of
their Gram staining
characteristics, cellular morphology and cellular fatty acid
methyl ester (FAME)
profiles using the MIDI system. Tissue samples were also placed
in fixative for
-
8/2/2019 2 Bacteria UC Probiotic
5/22
5
analysis by fluorescent in situ hybridisation (FISH) with 16S
rRNA oligonucleotide
probes.
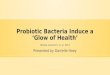
Complex bacterial communities colonised the rectal mucosa in
both healthy and
UC patients. Bacteria were found to occur as microcolonies on
the biopsies showing
that they were actively growing and that their presence was not
simply due to
passive transfer from faecal material (Fig. 1).
Figure 1 Bacterial microcolonies on the rectal mucosa visualised
by FISH usingan enterococcal probe labelled with FITC.
Total bacterial counts ranged from 104 to 106 cells per cm2
which differs from other
studies, where only low numbers of bacteria were found in
healthy patients
compared with controls (Shultsz et al. 1999, Swidinski et al.
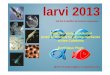
2002). Anaerobic
bacteria outnumbered facultative anaerobes in both UC and
healthy subjects (Fig.
2). Total anaerobic counts were 3-20 times higher than
facultative anaerobes. This
occurrence of a relatively high number of facultative anaerobes
on the epithelial
-
8/2/2019 2 Bacteria UC Probiotic
6/22
6
0
1
2
3
4
5
Log10bacteria(cm
2biopsymaterial)-1
U Healthy
Strict anaerobes
Facultative species
Figure 2 Comparison of strictly anaerobic (dark bars) bacterial
populations andfacultative anaerobes (light bars) on the rectal
mucosa in healthy subjects and UCpatients. Results show means
(n=3-5) SEM.
surface is in broad agreement with data obtained from colonic
tissue at autopsy
(Croucheret al. 1983), but differs from the results of Poxton
etal. (1997), where
strict anaerobes on the mucosal surface were 10- to 100-fold
higher than facultative
anaerobes. However, in this study the patients were prepared for
colonscopy and
several were taking antibiotics. Enterobacteria, bacteroides,
Gram positive cocci and
bifidobacteria had the highest prevalance in both healthy and UC
subjects with
bacteroides having the greatest species diversity (Fig. 3).
Other studies using
colonic and rectal biopsies have also indicated that bacteroides
and bifidobacteria
-
8/2/2019 2 Bacteria UC Probiotic
7/22
7
are the major anaerobes associated with the mucosal surface
(Poxton et al. 1997).
Gram-positive cocci, lactobacilli and clostridia were present in
higher numbers in the
UC patients, whereas the reverse was found with bifidobacteria
and prevotella.
Bacteroides fragilis was the main bacteroides found in both UC
and healthy subjects.
Bifidobacterium adolescentis and Bif. angulatum were predominant
in healthy people
whereas Bif. angulatum was the principal species in UC.
Peptostreptococci and
Enterococcus faecalis were not found on the rectal mucosa in
healthy people, but
did occur in UC patients.
These results suggest that bacteria occur in broadly similar
numbers on the rectal
mucosa of UC and healthy patients, each having their own
distinct subpopulations.
Whether these bacteria on the rectal mucosa have a role in UC or
those on the
normal healthy mucosa are protective is currently under
investigation.
-
8/2/2019 2 Bacteria UC Probiotic
8/22
8
Figure 3 Comparison of bacterial populations on the rectal
mucosa in UC patients(closed bars, N=4) and healthy subjects (open
bars, N=5). Results represent rangesand means (vertical bars).
Values in parentheses indicate the number of species andstrains in
each bacterial group or genus, those in italics show the number
ofindividuals that harboured these microorganisms in each subject
group.
Percutaneous endoscopic gastrostomy (PEG) tube biofilms
Enteral tube feeding (ETF) through a PEG tube is sometimes
advised when a clinical
condition (most commonly cerebrovascular disease or head and
neck trauma)
results in impairment of a patients ability to ingest food
normally. PEG tubes are
placed during upper GI endoscopy and pass from the gastric lumen
to the exterior of
the abdomen. Feeding fluid is passed through the tube into the
gastrum at
predetermined intervals. ETF alters drastically the mechanisms
by which a normal
upper gastrointestinal microbiota is maintained.
In normal individuals the upper GI tract is colonised sparsely.
The gastrum is
thought to be devoid of any significant resident microbiota;
other than Helicobacter
pylori and some lactobacilli (ca . 101 - 103 CFU ml-1)
(Gustaffson 1982) any
-
8/2/2019 2 Bacteria UC Probiotic
9/22
9
microorganisms present are transients originating from food or
the oral cavity.
Lactobacilli, streptococci and Bifidobacterium spp. (102
- 104
CFU ml-1
) are present
in the duodenum (Berg 1996). This statusquo is maintained by
multiple mechanisms
including peristalsis, a low pH (ca. one to four in normal
individuals) and the
enterosalivary circulation of nitrate and thiocyanate.
A proportion of ingested nitrate is converted to nitrite by
facultatively anaerobic
bacteria on the tongue (Duncan et al. 1995, Xu et al. 2001b).
The remainder is
absorbed in the duodenum, enters the bloodstream and is
concentrated in the
salivary glands from where it is secreted back into the GI
tract. Nitrite which reaches
the gastrum is acidified to form nitric oxide along with other
nitrogenous compounds
which exert a strong antimicrobial effect in the low pH
environment (Allaker et al.
2001, Dykhuizen et al. 1996, Xu et al. 2001a). Thiocyanate is
also concentrated in
saliva and enhances the antimicrobial effect of nitrite (Xu et
al. 2001a). Recent
studies have suggested that Enterobacteriaceae can survive
exposure to extremely
low pH environments (ca.pH 2) through expression of the asrgenes
(Seputiene et
al. 2003). Perhaps, therefore, the acid environment of the
stomach may not be
sufficient to kill invading microorganisms under some
circumstances. If this were
true then the nitrite/thiocyanate system might play a central
role in the defence of the
gastrum.
Each of these three protective mechanisms is degraded in ETF
patients. Absence
of any food-related sensory stimuli (smell, taste, sound)
inhibits the production of
saliva. Lack of normal mastication results in both reduced
volumes of saliva reaching
the gastrum and lower acid secretion. Additionally, lack of
solid food inhibits
peristaltic motion. The end result of this is that the
antimicrobial defences of the
stomach are compromised and it is thus open to colonisation.
Invading
-
8/2/2019 2 Bacteria UC Probiotic
10/22
10
microorganisms may originate from one (or more) of three
sources; (i) the lower gut,
(ii) the oral cavity or (iii) from the external environment via
the PEG tube and/or the
nutrient fluid.
Bacterial overgrowth in the upper GI tract has a number of
potential sequelae.
The most common is diarrhoea although other more serious
complications occur; for
example, malabsorption and sepsis (Cabre & Gassull 1993).
Biofilm formation on
PEG tubes is likely to be an unavoidable consequence of gastral
bacterial
overgrowth and will itself have consequences. PEG tube biofilms
may act as a
reservoir of microorganisms which will be difficult to eradicate
with antimicrobial
chemotherapy. Although replacement of the PEG tube would provide
an answer to
such colonisation this would consume more valuable medical
resources. Thus a
greater understanding of PEG tube biofilm composition, formation
and physiology
would be beneficial to both patients and clinicians.
A number of studies have been conducted relating to bacterial
colonisation of
PEG tubes. Several detailed colonisation of PEG tubes by fungi,
a phenomenon
associated with deterioration of tube integrity. Several genera
of fungi were isolated,
including Candida albicans (Gottlieb et al. 1992, Gottlieb et
al. 1993). Other authors
have conducted a more comprehensive microbiological assessment
of PEG tubes.
Enterococcus, Escherichia, Bacillus, Lactobacillus and
Staphylococcus spp. were
isolated from 15 paediatric patients in one study (Dautle et al.
2002). The authors
also used randomly amplified polymorphic DNA amplification
(RAPD) to type
microorganisms cultured from PEG tubes. Isolates cultured from
different parts of a
PEG tube were identical by RAPD profiling, suggesting that the
biofilm spread from
the initial attachment point. Three pairs of patients had
identical RAPD profiles forE.
coli, Staphylococcusaureus and E. faecalis. Thus PEG tube
biofilm-associated
-
8/2/2019 2 Bacteria UC Probiotic
11/22
11
microorganisms can be spread from patient to patient, raising
concerns of transfer of
detrimental attributes such as antibiotic resistance. The
culture methods in this study
involved extensive use of an antifungal (cycloheximide) at all
stages of isolation.
Given the evidence that a variety of fungi are to be found
within PEG tube biofilms
(Gottlieb et al. 1992; Gottlieb et al. 1993) the authors reasons
for deliberately
excluding such an important element of the biofilm community are
difficult to
understand.
Another study by the same group used cultural methods in
conjunction with
scanning electron microscopy (SEM) and confocal scanning laser
microscopy
(CSLM) to visualise biofilms on different areas of PEG tubes
taken from paediatric
patients (Dautle et al. 2003). The majority of isolates were of
the genera Bacillus,
Enterococcus and Staphylococcus. SEM showed that control PEG
tube surfaces
were punctuated by cracks and crevices. Microcolonies were
observed in PEG tubes
removed from patients; these were often found in association
with aberrations in the
surface, leading to the suggestion that improved manufacturing
methods might be of
use in limiting biofilm formation on PEG tubes. Biofilm
thickness was assessed
using CSLM and ranged from 28.4 mm to 128.4 mm. Depth varied
between patients
and was not related to location on the PEG tube. Additionally,
bacteria were
surrounded by a protective layer of fungi; bacterial cell mass
was lowest at the
silicone surface and highest adjacent to the fungal layer. As
before, an antifungal
was used during culture again with the result that the fungi in
these communities
remained uncharacterised.
Resistance to antibacterials was also investigated. Forty three
percent of isolates
of the genera Staphylococcus , Enterococcus and the family
Enterobacteriaceae
-
8/2/2019 2 Bacteria UC Probiotic
12/22
12
possessed multi-drug resistance, as determined by RAPD profiling
(Dautle et al.
2003).
The available literature suggests that biofilms can form on PEG
tubes in vivo.
Such communities comprise a range of microorganisms including
both fungi
(primarily Candida spp.) and prokaryotes. Bacteria isolated from
PEG tube biofilms
were primarily facultative anaerobes of the family
Enterobacteriaceae and the
genera Enterococcus, Lactobacillus and Staphylococcus together
with Bacillus and
Pseudomonas spp. Almost half of the isolates were multi-drug
resistant. However,
much work remains to be done: spatial organisation of PEG tube
biofilms is unknown
as is the sequence of colonisation. Additionally, the effect of
immune defence
mechanisms of the gastrum (acid, nitrite) on PEG tube biofilm
formation is unclear.
Knowledge of all of these factors will be vital to the
elucidation of appropriate
interventions and/or preventions.
Probiotics and gastrointestinal biofilms
Fermented milks and milk products have been in use since
antiquity, though it was
the Russian Nobel laureate Eli Metchkinoff who proposed in 1907
that the longevity
of the Balkan people could be attributed to their ingestion of
fermented milks.
Probiotics are live microbial food supplements that change
either the composition or
metabolic activities of the microbiota or modulate immune system
reactivity in a way
that benefits health (Macfarlane & Cummings 2002). They are
commercially
available in the form of yoghurts, drinks and as capsule, powder
or tablet
supplements.
The role of probiotic bacteria in intestinal biofilms is poorly
understood. The
indigenous microbiota of gastric and intestinal surfaces
certainly contributes to the
-
8/2/2019 2 Bacteria UC Probiotic
13/22
13
stability of GI ecosystem (Savage 1987). However, while the role
of potential
pathogens in the aetiology of infection has been extensively
studied, there is a lack
of information regarding mechanisms by which the indigenous
microbiota
establishes and maintains colonisation, probably due to the
innate complexity of the
intestinal ecosystem (Greene & Klaenhammer 1994).
Nonetheless, it is generally
recognised that for probiotic bacteria to exert an effect in the
intestine they must be
able to adhere, at least temporarily, to the intestinal mucosa.
Several in vitro studies
have shown that Lactobacillus strains can adhere to either HT-29
or CaCo-2
epithelial cell lines (Chauviere et al. 1992) while
bifidobacteria adhere competently to
intestinal mucus (He et al. 2001, Ouwehand et al. 1999). The
adherence
mechanisms of lactobacilli and bifidobacteria are unclear and
the amount of
adhesion also differs greatly between species (Tuomola &
Salminen 1998). In earlier
animal studies it has been suggested that concanavalin A
receptors on some
Lactobacillus spp. influenced their ability to attach to
epithelial cells (Fuller 1975). In
a more recent study the authors showed that L. acidophilus LA1
exhibited a strong
calcium-independent adherence property and that adhesion of this
strain to Caco-2
cells required a strong proteinaceous adhesion-promoting
property (Bernet et al.
1994). When 13 strains ofB. longum were tested for adhesion to
both gastric and
colonic cell lines, adhesion was found to be strongly related to
autoaggregation
ability and the authors classified the adherence capabilities of
the strains according
to this ability (Del Re et al. 2000). The adherence of
bifidobacteria is thought to be
species-specific and possibly mediated by a proteinaceous
adhesion-promoting
factor, rather than a calcium-dependent one (Bernet et al.
1993).
Research on adherence of probiotic bacteria to in vitro colonic
and gastric cell
lines has provided useful data on the mechanisms of adherence,
but are probably
-
8/2/2019 2 Bacteria UC Probiotic
14/22
14
not indicative ofin vivo situations; the beneficial effects of
probiotics may result from
competitive interactions with pathogenic and non-pathogenic
organisms in the
intestine and with the immune system.
Probiotics in inflammatory bowel disease
Crohn's disease (CD) is a chronic IBD where inflammation
involves full thickness of
the intestinal wall and may affect any point along the GI tract
(Guarneret al. 2002).
Increasing research in the area of probiotics in either UC or CD
indicates that there
may be some therapeutic benefits of bacterial supplementation in
these patients.
Although most research on probiotics in IBD has been on the
maintenance and
remission of UC, Lactobacillus strain GG was shown to help
promote the barrier
function in children with CD and also improve symptoms (Gupta et
al. 2000, Malin et
al. 1996), though it had no effect in adult CD patients after
colonic resection
(Prantera et al. 2002). L. salivarius strain UCC118 was also
shown to transit the GI
tract of patients with CD (Dunne 2001) though actual adherence
to the mucosa of
these patients was not demonstrated.
Probiotics have had success in the achievement and maintenance
of remission in
UC. Pouchitis is a frequent chronic complication which occurs
after pouch surgery
for UC and manifests itself as a non-specific inflammation of
the ileal reservoir
(Gionchetti et al. 2000). When 40 patients were randomised to
receive either VSL#3
(a probiotic containing four strains of lactobacilli, three
strains of bifidobacteria and
one strain ofStreptococcus salivarius subsp. thermophilus) or a
placebo, 15% of
patients in the probiotic group experienced relapses during the
nine month follow-up
period, compared to 100% in the placebo group (P
-
8/2/2019 2 Bacteria UC Probiotic
15/22
15
baseline levels during feeding (P
-
8/2/2019 2 Bacteria UC Probiotic
16/22
16
prevalence in biofilms formed on silicone tubes in voice
prostheses in vitro
(Busscheret al. 1997, Free et al. 2001, van der Mei et al.
2000). It may be that the
use of probiotics in biofilm formation on voice prostheses
tubing could be applied to
those on ETF tubes.
Concluding remarks
Despite increasing interest in complex gastrointestinal biofilms
the health
significance of these complex communities is still largely
unknown. Microbiological
analysis of the rectal mucosa has demonstrated marked
differences in UC patients
when compared with healthy subjects indicating a possible role
for specific genera,
or groups of genera, in disease aetiology. Of several novel
treatments for the
management of UC and the complications of PEG tube feeding
probiotics appear the
most promising. The existing clinical data supports a role for
probiotics in
maintaining quiescent disease and pouchitis in remission; it is
therefore likely that
such microorganisms can indeed colonise the GI mucosa.
-
8/2/2019 2 Bacteria UC Probiotic
17/22
17
References
Allaker, R.P., Silva Mendez, L.S., Hardie, J.M. & Benjamin,
N. (2001).Antimicrobial effect of acidified nitrite on periodontal
bacteria. Oral Microbiology and
Immunology16, 253-256.
Berg, R.D. (1996). The indigenous gastrointestinal microflora.
Trends Microbiology4, 430-435.
Bernet, M., Brassart, D., Neeser, J. & Servin, A.
(1994).LactobacillusacidophilusLA 1 binds to cultured human
intestinal cell lines and inhibits cell attachment and cellinvasion
by enterovirulent bacteria. Gut35, 483-489.
Bernet, M.F., Brassart, D., Neeser, J.R. & Servin, A.L.
(1993). Adhesion of humanbifidobacterial strains to cultured human
intestinal epithelial cells and inhibition of
enteropathogen-cell interactions.Applied and Environmental
Microbiology59, 4121-4128.
Bjorkholm, B., Falk, P., Engstrand, L. & Nyren, O.
(2003).Helicobacterpylori-resurrection of the cancer link. Journal
of Internal Medicine253, 102-119.
Bleichner, G., Blehaut, H., Mentec, H. & Moyse, D.
(1997).Saccharomycesboulardiiprevents diarrhea in critically ill
tube-fed patients. Intensive Care Medicine23, 517-523.
Bliss, D.Z., Johnson, S., Savik, K., Clabots, C.R., Willard, K.
& Gerding, D.N.(1998). Acquisition ofClostridium difficile and
Clostridium difficile-associateddiarrhoea in hospitalized patients
receiving tube feeding.Annals of Internal Medicine129,
1012-1019.
Busscher, H.J., van Hoogmoed, C.G., Geertsema-Doornbusch, G.I.,
van derKuijl-Booij, M. & van der Mei, H.C. (1997).Streptococcus
thermophilus and itsbiosurfactants inhibit adhesion by Candida spp.
on silicone rubber.Applied andEnvironmental Microbiology63,
3810-3817.
Cabre, E. & Gassull, M.A. (1993). Complications of enteral
feeding. Nutrition9, 1-9.
Chadwick, V. (1991). Etiology of chronic ulcerative colitis and
Crohn's disease. InThe large intestine: physiology, pathophysiology
and disease. Edited by S. Philips, J.Pemberton & R. Shorter.
New York: Raven Press.
Chauviere, G., Coconnier, M.H., Kerneis, S., Fourniat, J. &
Servin, A.L. (1992).Adhesion of human Lactobacillus acidophilus
strain LB to human enterocyte-likeCaco-2 cells. Journal of General
Microbiology138, 1689-1696.
Conly, J., Stein, K., Worobetz, L. & Rutledge-Harding, S.
(1994). The contributionof vitamin K2 (metaquinones) produced by
the intestinal microflora to human
nutritional requirements for vitamin K.American Journal of
Gastroenterology89,915-923.
-
8/2/2019 2 Bacteria UC Probiotic
18/22
18
Cremonini, F., Di Caro, S., Nista, E.C., Bartolozzi, F.,
Capellii, G., Gasbarrini, G.& Gasbarrini, A. (2002).
Meta-analysis: the effect of probiotic administration
onantibiotic-associated diarrhoea.Alimentary Pharmacology and
Therapeutics16,1461-1467.
Croucher, S., Houston, A. & Bayliss, C. (1983). Bacterial
populations associatedwith different regions of the human colon
wall.Applied and EnvironmentalMicrobiology45, 1025-1033.
Cummings, J., Pomare, E., Branch, W., Naylor, C. &
Macfarlane, G. (1987). Shortchain fatty acids in human large
intestine, portal, hepatic and venous blood. Gut28,1221-1227.
D'Souza, A.L., Rajkumar, C., Cooke, J. & Bulpitt, C.J.
(2002). Probiotics inprevention of antibiotic-associated diarrhoea:
meta-analysis. British Medical Journal
324, 1361-1367.
Dautle, M., Ulrich, R. & Hughes, T. (2002). Typing and
subtyping of 83 clinicalisolates purified from surgically implanted
silicone feeding tubes by random amplifiedpolymorphic DNA
amplification. Journal of Clinical Microbiology40, 414-421.
Dautle, M.P., Wilkinson, T. R. & Gauderer, M.W. (2003).
Isolation and identificationof biofilm microorganisms from silicone
gastrostomy devices. Journal of PediatricSurgery38, 216-220.
Del Re, B., Sgorbati, B., Miglioli, M. & Palenzona, D.
(2000). Adhesion,autoaggregation and hydrophobicity of 13 strains
ofBifidobacterium longum. Lettersin Applied Microbiology31,
438-442.
Duncan, C., Dougall, H., Johnston, P., Green, S., Brogan, R.,
Leifert, C., Smith,L., Golden, M. & Benjamin, N. (1995).
Chemical generation of nitric oxide in themouth from the
enterosalivary circulation of nitrate. Nature Medicine1,
546-551.
Dunne, C. (2001). Adaptation of bacteria to the intestinal
niche:probiotics and gutdisorder. Inflammatory Bowel Diseases7,
136-145.
Dykhuizen, R.S., Frazer, R., Duncan, C., Smith, C.C., Golden,
M., Benjamin, N.& Leifert, C. (1996). Antimicrobial effect of
acidified nitrite on gut pathogens:importance of dietary nitrate in
host defense.Antimicrobial Agents andChemotherapy40, 1422-1425.
Edmiston, C.J., Avant, G. & Wilson, F. (1982). Anaerobic
bacterial populations onnormal and diseased human biopsy tissue
obtained at colonoscopy.Applied andEnvironmental Microbiology43,
1173-1181.
Free, R.H., Busscher, H.J., Elving, G.J., van der Mei, H.C., van
Weissenbruch,R. & Albers, F.W. (2001). Biofilm formation on
voice prostheses: in vitro influence
on probiotics.Annals of Otology, Rhinology and Laryngology110,
946-951.
-
8/2/2019 2 Bacteria UC Probiotic
19/22
19
Fuller, R. (1975). Nature of the determinant responsible for the
adhesion oflactobacilli to chicken crop epithelial cells. Journal
of General Microbiology87, 245-250.
Gionchetti, P., Rizzello, F., Venturi, A., Brigidi, P.,
Matteuzzi, D., Bazzocchi, G.,
Poggioli, G., Migliolli, M. & Campieri, M. (2000). Oral
bacteriotherapy asmaintenance treatment in patients with chronic
pouchitis: a double-blind, placebo-controlled trial.
Gastroenterology119, 305-309.
Gottlieb, K., deMeo, M., Borton, P. & Mobarhan, S. (1992).
Gastrostomy tubedeterioration and fungal colonisation.American
Journal of Gastroenterology87,1683.
Gottlieb, K., Leya, P., Kruss, M., Mobarhan, S. & Iber, F.
(1993). Intraluminalfungal colonisation of gastrostomy tubes.
Gastrointestinal Endoscopy39, 413-415.
Greene, J. D. & Klaenhammer, T. R. (1994). Factors involved
in adherence oflactobacilli to Human Caco-2 Cells.Applied and
Environmental Microbiology60,4487-4494.
Guarner F., Casellas F., Borruel N., Antolin M., Videla S.,
Vilaseca J. &Malagelada, J-R (2002). Role of microecology in
chronic inflammatory boweldiseases. Eur J Clin Nutr56(Suppl 4),
S34-S38
Gupta, P., Andrew, H., Kirschner, B. S. & Guandalini, S.
(2000). Is LactobacillusGG helpful in children with Crohn's
disease? Results of a preliminary, open-labelstudy. Journal of
Paediatric Gastroenterology and Nutrition31, 453-457.
Guslandi, M., Mezzi, G., Sorghi, M. & Testoni, P. A.
(2000).Saccharomycesboulardiiin maintenance and treatment of
Crohn's disease. Digestive Disease andSciences45, 1462-1464.
Gustaffson, B. (1982). The physiological importance of the
colonic microflora.Scandinavian Journal of Gastroenterology77
(Suppl.), 117-131.
Hartley, C., Neumann, C. & Richmond, M. (1979). Adhesion of
commensalbacteria to the large intestine wall in humans. Infection
and Immunity23, 128-132.
He, F., Ouwehand, A. C., Hashimoto, H., Isolauri, E., Benno, Y.
& Salminen, S.(2001). Adhesion ofBifidobacterium spp. to human
intestinal mucus. MicrobialImmunology45, 259-262.
Hill, M., Drasar, B. & Aries, V. (1971). Bacteria and
aetiology of cancer of the largebowel. Lancet, 95-100.
Hopkins, M. J., Sharp, R. & Macfarlane, G. T. (2002).
Variation in human intestinalmicrobiota with age. Digestive and
Liver Diseases34 Suppl 2, S12-18.
-
8/2/2019 2 Bacteria UC Probiotic
20/22
20
Horie, H., Kanazawa, K., Okada, M., Narushima, S., Itoh, K.
& Terada, A. (1999).Effects of intestinal bacteria on the
development of colonic neoplasm: anexperimental study. European
Journal of Cancer Prevention8, 237-245.
Kruis, W., Schutz, E., Fric, P., Fixa, B., Judmaier, G. &
Stolte, M. (1997). Double-
blind comparison of an oral Escherichia colipreparation and
mesalazine inmaintaining remission of ulcerative colitis.Alimentary
Pharmacology andTherapeutics11, 853-858.
Macfarlane, G. T. & Cummings, J. H. (2002). Probiotics,
infection and immunity.Current Opinion in Infectious Diseases15,
1-6.
Macpherson, A., Khoo, U., Forgacs, I., Philpott-Howard, J. &
Bjarnason, I.(1996). Mucosal antibodies in inflammatory bowel
disease are directed againstintestinal bacteria. Gut48,
365-375.
Malin, M., Suomalainen, H., Saxelin, M. & Isolauri, E.
(1996). Promotion of IgAimmune response in patients with Crohn's
disease by oral bacteriotherapy withLactobacillus GG.Annals of
Nutrition and Metabolism40, 137-145.
Metchnikoff, E. (1907).The Prolongation of Life, Heinemann.
Miyazawa, E., Iwabuchi, A. & Yoshida, T. (1996). Phytate
breakdown andapparent absorption of phosphorus, calcium and
magnesium in germfree andconventionalised rats. Nutrition
Research16, 603-613.
Onderdonk, A. (1983). Role of the intestinal microflora in
ulcerative colitis. InHuman Intestinal Microflora in Health and
Disease. Edited by D. Hentges. London:Academic Press.
Onderdonk, A. & Bartlett, M. (1979). Bacteriological studies
of experimentalulcerative colitis.American Journal of Clinical
Nutrition32.
Ouwehand, A.C., Isolauri, E., Pirkka, V., Kirjavainen, P.V.
& Salminen, S. (1999).Adhesion of fourBifidobacterium strains
to human intestinal mucus from subjects indifferent age groups.
FEMS Microbiology Letters172, 61-64.
Poxton, I., Brown, R., Sawyerr, A. & Ferguson, A. (1997).
Mucosa-associatedbacterial flora of the human colon. Journal of
Medical Microbiology46, 85-91.
Prantera, C., Scribano, M.L., Falasco, G., Andreoli, A. &
Luzi, C. (2002).Ineffectiveness of probiotics in preventing
recurrence after curative resection forCrohn's disease; a
randomised controlled trial with Lactobacillus GG. Gut51,
405-409.
Sadlack, B., Merz, H. & H.S. (1993). Ulcerative colitis-like
disease in mice with adisrupted interleukin-2 gene. Cell75,
253-261.
Savage, D.C. (1987). Microorganisms associated with epithelial
surfaces andstability of the indigenous gastrointestinal
microflora. Nahrung31, 383-395.
-
8/2/2019 2 Bacteria UC Probiotic
21/22
21
Seputiene, V., Motiejunas, D., Suziedelis, K., Tomenius, H.,
Normark, S.,Melefors, O. & Suziedeliene, E. (2003). Molecular
characterisation of the acid-inducible asrgene ofEscherichia
coliand its role in acid stress response. Journal
ofBacteriology185, 2475-2484.
Shultsz, C., van der Berg, F. & Ten Kate, F. (1999). The
intestinal mucous layerfrom patients with inflammatory bowel
disease harbours high numbers of bacteria.Gastroenterology117,
1089-1097.
Swidinski, A., Ladhoff, A. & Pernthaler, A. (2002). Mucosal
flora in inflammatorybowel disease. Gastroenterology122, 44-54.
Tannock, G. (2001). Molecular assessment of intestinal
microflora.AmericanJournal of Clinical Nutrition73 Suppl,
S410-414.
Tuomola, E. M. & Salminen, S. J. (1998). Adhesion of some
probiotic and dairyLactobacillus strains to Caco-2 cell cultures.
International Journal of FoodMicrobiology41, 45-51.
van der Mei, H.C., Free, R. H., Elving, G.J., van Weissenbruch,
R., Albers, F.W.& Busscher, H.J. (2000). Effect of probiotic
bacteria on prevalence of yeasts inoropharyngeal biofilms on
silicone rubber voice prostheses in vitro. Journal ofMedical
Microbiology49, 713-718.
van der Waaij, D. (1989). The ecology of the human intestine and
its consequencesfor overgrowth by pathogens such as
Clostridiumdifficile.Annual Review ofMicrobiology43, 69-87.
van der Wiel-Korstanje, J. & Winkler, K. (1975). The faecal
flora in ulcerativecolitis. Journal of Medical Microbiology8,
491-501.
Venturi, A., Gionchetti, P., Rizzello, F., Johansson, R.,
Zucconi, E., Brigidi, P.,Matteuzzi, D. & Campieri, M. (1999).
Impact on the composition of the faecal floraby a new probiotic
preparation: preliminary data on maintenance treatment ofpatients
with ulcerative colitis.Alimentary Pharmacology and Therapeutics13,
1103-1108.
von Wufflen, H., Russman, H. & Karch, H. (1989).
Verotoxin-producingEscherichiacoliO2:H5 isolated from patients with
ulcerative colitis. Lancet, 1449-1450.
Whelan, K., Gibson, G.R., Judd, P. A. & Taylor, M.A. (2001).
The role of probioticsand prebiotics in the management of diarrhoea
associated with enteral tube feeding.Journal of Human Nutrition and
Dietetics14, 423-433.
Wyatt, G.M., Bayliss, C.E., Lakey, A.F., Bradley, H.K., Hunter,
J.O. & Alun-Jones, V. (1988). The faecal flora of two patients
with food-related irritable bowel
syndrome during challenge with symptom-provoking foods. Journal
of MedicalMicrobiology26, 295-299.
-
8/2/2019 2 Bacteria UC Probiotic
22/22
22
Xu, J., Xu, X. & Verstraete, W. (2001a). The bactericidal
effect and chemicalreactions of acidified nitrite under conditions
simulating the stomach. Journal ofApplied Microbiology90,
523-529.
Xu, J., Xu, X. & Verstraete, W. (2001b). Quantitative
measurement of the nitratereductase activity in the human oral
cavity. Food and Chemical Toxicology39, 77-84.
Younes, H., Coudray, C., Bellanger, J., Demigne, C.,
Rayssiguier, R. & Remesy,C. (2001). Effects of two fermentable
carbohydrates (inulin and resistant starch) andtheir combination on
calcium and magnesium balance in rats. British Journal
ofNutrition86, 479-485.