-
This article was downloaded by: [Gazi University]On: 18 August
2014, At: 22:45Publisher: RoutledgeInforma Ltd Registered in
England and Wales Registered Number: 1072954 Registered office:
MortimerHouse, 37-41 Mortimer Street, London W1T 3JH, UK
Neuropsychoanalysis: An Interdisciplinary Journalfor
Psychoanalysis and the NeurosciencesPublication details, including
instructions for authors and subscription
information:http://www.tandfonline.com/loi/rnpa20
A Cognitive Neuroscience Perspective onConfabulationJohn DeLuca
Ph.D.aa Neuropsychology & Neuroscience Laboratory, Kessler
Medical Rehabilitation, Research& Education Corp., 1199
Pleasant Valley Way, West Orange, NJ 07052, e-mail:Published
online: 09 Jan 2014.
To cite this article: John DeLuca Ph.D. (2000) A Cognitive
Neuroscience Perspective on Confabulation,Neuropsychoanalysis: An
Interdisciplinary Journal for Psychoanalysis and the Neurosciences,
2:2, 119-132, DOI:10.1080/15294145.2000.10773294
To link to this article:
http://dx.doi.org/10.1080/15294145.2000.10773294
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy
of all the information (the Content) containedin the publications
on our platform. However, Taylor & Francis, our agents, and our
licensors make norepresentations or warranties whatsoever as to the
accuracy, completeness, or suitability for any purpose ofthe
Content. Any opinions and views expressed in this publication are
the opinions and views of the authors,and are not the views of or
endorsed by Taylor & Francis. The accuracy of the Content
should not be reliedupon and should be independently verified with
primary sources of information. Taylor and Francis shallnot be
liable for any losses, actions, claims, proceedings, demands,
costs, expenses, damages, and otherliabilities whatsoever or
howsoever caused arising directly or indirectly in connection with,
in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private
study purposes. Any substantial or systematicreproduction,
redistribution, reselling, loan, sub-licensing, systematic supply,
or distribution in anyform to anyone is expressly forbidden. Terms
& Conditions of access and use can be found at
http://www.tandfonline.com/page/terms-and-conditions
-
119
NEURO-PSYCHOANALYTIC DIALOGUE
A Cognitive Neuroscience Perspective onConfabulation
John DeLuca
Abstract: The purpose of this paper is to provide an overviewof
the behavioral and neuroscience research on confabulation.While
most forms oforganically induced confabulatory syndromesare
reviewed, special emphasis on confabulation following ante-rior
communicating artery (ACoA) aneurysm is provided. "Psy-chiatric"
forms of confabulation will not be discussed at lengthin this
paper. For instance, while confabulation has been observedin
patients with schizophrenia, such a presentation appears to
berelated to a thought disorder (Nathaniel-lames and Frith,
1996).This paper will focus on confabulation following acquired
braindamage.
Introduction
In the late nineteenth century, Korsakoff (1889) de-scribed a
behavioral disturbance in which patientswould verbally present
seemingly erroneous recollec-tions that they believed were accurate
or correct. Infact, when Korsakoff traced a considerable number
ofthese recollections he found many of them to be actu-ally true.
This behavioral phenomenon was later la-beled confabulation by
Kraepelin (Koehler andJacoby, 1978). Today it is well known that
confabula-tion occurs across a variety of neurologic patients
in-cluding those with Korsakoff disease, anteriorcommunicating
artery (ACoA) aneurysm (e.g., De-Luca and Cicerone, 1991), stroke
and traumatic braininjury (TBI; e.g., Shapiro, Alexander, Gardner,
andMercer, 1981), and dementia (e.g., Kern, van Gorp,
Dr. DeLuca is Professor, Department of Physical Medicine and
Reha-bilitation, Department of Neurosciences, UMDNJ-New Jersey
MedicalSchool, Newark, NJ; Neuropsychology and Neuroscience
Laboratory,Kessler Medical Rehabilitation Research and Education
Corporation, WestOrange, NJ.
Cummings, Brown, and Osato, 1992). In fact, in hisoriginal
articles, Korsakoff described confabulation inpatients with lead
poisoning, carbon monoxide poison-ing, and bacterial infection
(Korsakoff, 1889). Never-theless, despite the numerous papers for
over a centurythat have documented the existence of
confabulation,the debate over what it is and what causes it
remainsto this day.
What Is Confabulation? Problems in Definition
The major conceptual problem encountered with anydiscussion of
confabulation is the lack of a generallyaccepted definition for
what it is. The problem thatthis creates should not be
underestimated. Is a patientwith anosognosia for hemiplegia with
left visual ne-glect confabulating when they deny having problemsin
utilizing their paralyzed limb (Feinberg, Roane,Kwan, Schindler,
and Haber, 1994)? Are patients withAnton's syndrome (i.e., cortical
blindness), who denytheir blindness, confabulating? Are patients
who indi-cate that they have two wives who look exactly thesame or
state that there are two identical hospitals(Capgras
syndrome/Reduplicative paramnesia) con-fabulating? While these are
all manifestions of un-awareness, it is unclear that they are all
confabulation.Can all of these diverse behavioral expressions
trulyresult from a single (or distributed) central mechanismin the
brain critical to the expression of a singularconfabulatory state?
Or are there different forms ofconfabulation, each with its own
underlying mecha-nisms? Or is confabulation a subset of a larger
prob-lem of unawareness of deficit or anosognosia? Thesequestions
remain unresolved.
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4
-
120 John DeLuca
Given the difficulties in defining confabulation,the following
definition from Mosocovitch and Mello(1997) is perhaps the most
general yet descriptive.These authors describe confabulations as
"statementsor actions that involve unintentional but obvious
dis-tortions. ..." While this definition will likely not
beuniversally accepted, it is a working definition thatwill be used
in the present paper.
It should be recognized that some form of "con-fabulation" is a
normal human phenomenon. This isbecause remembering is a
reconstructive process, of-ten resulting in memory distortion
rather than memoryloss (Mosovitch, 1995). However, when neural
circuitsinvolved in the reconstructive process are damaged,memory
distortion can become prominent and is thenrecognized as
confabulation. As a result, in clinicalpractice, there is the
tendency to recognize the more"bizarre" responses as confabulatory
because the dis-tinction between normal memory distortion and
"ab-normal" responses is more obvious. Yetconfabulation can be
subtle, nonbizarre, and elicited,for instance, only upon
provocation (i.e., provokedconfabulation, see below).
At a minimum, confabulation involves both dis-tortions of
content and temporal context. That is, con-fabulatory recollections
frequently include additions,distortions, or elaborations of events
that either actu-ally or plausibly occurred. As such, when a
confabula-tory patient is asked what they did today, they
mayincorporate events that may have actually occurred(e.g., seeing
a therapist or doctor), but with the contentdistorted or
intertwined with other seemingly unre-lated events (which also may
have occurred). How-ever, confabulations are also frequently the
intrusionof events which have actually taken place, but
becomedisplaced temporally. These two forms of distortionare
illustrated by the following ACoA patient:
DoctorPatient VR
DoctorPatient VR
What did you do today?Today I got up this morning and vis-ited
the rehabilitation insti-tute ... then I went home and I
wasexpecting some material and we re-ceived it. Then I came to the
rehabili-tation institute, no I actually went tothe Jimsburg store
and we had a smallmeeting there. Then I came to the hos-pital and
we had lunch and then metwith you....What did you do this past
weekend?There was a friend that used to workat the Jimsburg store,
that moved
away, that was a friend of mine for10 years or so, who came by
my housefor a visit with his family. We wentto New York City, and
as a matter offact, we stopped by the Jimsburg storeto say hello to
one manager that healso has become friendly with, but thisstore is
not operating anymore....
Patient VR illustrates several key aspects of con-fabulation.
First, content distortion is illustrated: De-spite having been in
the hospital for several weekspostsurgery, he states that he has
been home, had ameeting at work, yet also correctly incorporates
hisknowledge about the rehabilitation hospital and thedoctor's role
within it. These events had not actuallyoccurred on that day.
Second, impaired temporal con-text is clearly evident in that VR
had indeed ownedthe "Jimsburg store," but he had sold this store
yearsearlier. After viewing the videotape, patient VR's
wifeindicated that the story about the friend visiting, goingto New
York City, and then seeing a mutual friendfrom the store had
actually occurred, but years earlier.The third point illustrated by
this excerpt is impairedself-monitoring. While first acknowledging
having vis-ited the Jimsburg store with his friend, in the
samesentence he acknowledges that the store is no
longeroperational. Patient VR could not realize the temporal,nor
the logical implausibility of being at the store andthe
hospital.
As such, confabulation often is a combination oftemporal
displacement of an actual event from the pastinto the present as
well as the distortion of eventsthat may be salient in the
immediate environment (i.e.,distorted content). However, it is the
lack of the pa-tient's own self-monitoring about the implausibility
ofthe temporal and content displacement that has fasci-nated
researchers and clinicians and resulted in theo-ries to understand
what drives such behavior.
Two Prominent Viewpoints on Confabulation
In general, two broad schools of thought have devel-oped in
regard to the understanding of confabulation.The first
conceptualizes confabulation as an "un-aware" process while the
second recognizes a con-scious "awareness" aspect to confabulation.
Ingeneral, the former conceptualization appears to comefrom the
neurological literature while the latter tendsto reflect work from
the psychiatric literature.
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4
-
Confabulation 121
Patient OJ was firm about the truth of his recol-lections, and
resisted attempts to convince himselfotherwise. It was clear from
his words, his affect, andhis behavior that there were no '
'gap-filling' , re-sponses.
A handful of studies were designed to experimen-tally examine
the temporal context hypothesis(Schnider, von Daniken, and Gutbrod,
1996; Moscov-ich and Melo, 1997). For instance, Schnider, von
Dan-iken, and Gutbrod (1996) found that all spontaneous
Since Korsakoff's discoveries, many researchershave recognized
that confabulation is frequently atemporal displacement of an
actual event that had oc-curred in the patient's life, although
this event canbe embellished with the intrusion of nonactual
events(Talland, 1965; Schnider, Gutbrod, Hess, and Schroth,1996;
Ptak and Schnider, 1999). In other words, whilethese confabulatory
recollections frequently includeadditions, distortions, or
elaborations, they are thoughtto be based on actual events.
Importantly, confabula-tors are unaware that they are
confabulating, nor arethey aware of the temporal displacement of
their con-fabulations. For instance, Talland (1965) reported thatin
patients with Korsakoff's syndrome, "The patienthimself is almost
certainly not aware of the gaps inhis knowledge when he
confabulates; he transposesinformation from an earlier period in
his life, con-denses or distorts material without consciousness
ofhis deficit or of the confabulatory process, and hencewithout
intent" (p. 57).
Doctor
Patient OJ
DoctorPatient OJ
Doctor
Patient OJ
You indicated that last night you wereworking on a number of
projects athome. . . . What would you say if Itold you you were
actually here in thehospital last night?I'd be surprised, because
my experi-ence, what I learn from my eyes andears tells me
differently .... I'd wantsome evidence. I'd want some indica-tion
that you knew about my privateworld before I gave any
cognizance.Would you believe me?Not out of the blue, especially
sincewe haven't even met (an illustrationof the patient's
amnesia).What if your wife was here and sheagreed with me, what
would you thinkat that point?I'd continue to resist, but it would
be-come more difficult.
confabulators, but not nonconfabulating amnesics,confused
present with previously acquired informa-tion on a continuous
recognition task. However, Mos-covitch and Melo (1997) argued that
defectivetemporal order is not the cause of confabulation, butis a
symptom of a more fundamental deficit in strategicretrieval (see
below).
Ptak and Schnider (1999) reported an amnesticACoA patient whose
confabulations could always betraced back to actual experiences,
supporting the no-tion that the key difficulty in confabulation is
the tem-poral monitoring of actual memories. The patient wasunaware
of his memory problems, and was convincedthat his beliefs were
correct, arguing with hospitalstaff. His confabulation gradually
disappeared over a4-month period.
In summary, the temporal displacement concepthas been recognized
for over 100 years, and is widelyaccepted today by many researchers
and clinicians. Amajor focus of this position is that patients are
un-aware of the temporal displacements and do not havethe
self-monitoring ability to critically examine theinconsistencies in
their discourse.
However, by the turn of the century, a secondline of thinking
began to emerge, emphasizing the fab-ricated or fictitious elements
of confabulation moreprominently. First Bonhoffer (1901; cited in
Talland,1965) and later van der Horst (1932; cited in Schnider,von
Daniken, and Gutbrod, 1996) felt that confabula-tion reflected a
desire to fill gaps in memory, whichwas termed "confabulation out
of embarrassment."That is, confabulators somehow contrive a story
toprotect themselves from embarrassment. This notionof "gap
filling" would then require some awarenessof a memory disorder on
the part of the patient. Theproblem is that there is very little
empirical support forthis position. In fact, the few studies that
empiricallyexamined gap-filling behavior did not support this
hy-pothesis (Moscovitch and Melo, 1997; Schnider, vonDaniken, and
Gutbrod, 1996). For instance, Schnider,von Daniken, and Gutbrod
(1996) classified amnesicpatients (including ACoA) into'
'spontaneous" versus"provoked" confabulators. They reported that
con-fabulators did not show an increased tendency to fillin gaps in
memory. Despite the lack of evidence, thisnotion of gap filling is
maintained even today. Forinstance, the DSM-IV (American
Psychiatric Associa-tion, 1994) defines confabulation as "the
recitation ofimaginary events to fill in gaps in memory" (p.
157).Numerous psychiatry textbooks also define confabula-tions as
conscious gap filling, with a conscious wishto deceive (Whitlock,
1981). Weinstein and Lyerly
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4
-
122
(1968) defined confabulation "as the fictitious narra-tive of
some past event or events" (p. 348). Bensonet al. (1996) define
confabulation as "compensationfor loss of memory by the fabrication
of details" (p.1239).
Joseph (1986) reported that confabulation fromgap filling can
occur following cerebral disconnectionsyndromes. For instance,
Gazzaniga and colleagues(Phelps and Gazzaniga, 1992; Gazzaniga,
1998) de-scribed a laboratory-induced confabulation in split-brain
patients resulting in a form of confabulation thatrequires
awareness of one's own behavior, but un-awareness of why one is
behaving in a particular way(gap filling without awareness).
Gazzaniga (1998) re-ported that when the speechless right
hemisphere of asplit-brain patient is given a command to "take
awalk,' , the patient begins to execute the demand.However, when
the experimenter now asks the patient(i.e., the left hemisphere)
"where are you going," theleft (language) hemisphere responds "to
get a drinkof water." Such a confabulatory response is made
be-cause the language hemisphere does not have accessto the
information in the right hemisphere that initi-ated the original
behavior. As such, according to Gaz-zaniga, the left hemisphere
contains a mechanism (the"Interpreter' ') that seeks to interpret
information bothinternally and externally to logically explain
theevents in the environment. In this example, the split-brain
patient was able to examine the immediate situa-tion and construct
a plausible, but untrue response. Isthis confabulation from
unawareness? While they areindeed filling in gaps, are such
patients aware of acognitive disorder that they need to cover up?
Theanswer is clearly no. In this example, the left hemi-sphere did
not have access to the knowledge thatprompted the original behavior
(to take a walk), andthus was not aware of the reason for the
behavior (seeSchacter, 1991, for a distinction between
unawarenessof deficit and unawareness of knowledge). While
theInterpreter is conscious of its own behavior, it is notaware of
the motivation that is driving the originalbehavior, and hence is
not consciously hiding a mem-ory or any other cognitive
disorder.
There are several other problems with the simplegap-filling
explanation of confabulation. For instance,confabulatory amnesics
typically only carry out gapfilling during the early stages of
their amnesia, despitethe fact that their amnesia is long lasting.
Why wouldsuch patients only fill in gaps early on in their
illness?Confabulation does not occur among many amnesics,including
many Korsakoff patients, and is very rareamong mesial temporal
amnesics. In addition, many
John DeLuca
amnesics readily admit to gaps in their memory with-out
confabulating (McGlynn and Schacter, 1989).
Other early conceptualizations of confabulationincluded: "a
disturbance in symbolism, comparableto that which occurs in
dreaming, ... wish-fulfillingfantasies, ... the means whereby
sexually traumaticmaterial could be expressed and gratified"
(Weinsteinand Lyerly, 1968, p. 348). However, there is very
littleevidence to support these very early conceptualiza-tions of
confabulation, typically relying on subjectiveobservations of
behavior. Some believe that premorbidpersonality traits are
important determinants in whowill eventually confabulate (Weinstein
and Kahn,1955; Talland, 1965). However, this notion is
basedexclusively on anecdotal data, usually involves indi-vidual
case reports, and has not been systematicallyevaluated
experimentally. Weinstein (1996) arguesthat confabulations are "in
some degree, symbolicrepresentations, dramatizations, or
explanations ofsome current personal experience, disability, or
prob-lem" (p. 336). Weinstein indicates that in such casesthe
patient has some knowledge of their disability orproblem. He does,
however, acknowledge that thistype of symbolic confabulation is
less likely to occurin patients with ACoA aneurysm.
In summary, confabulation involves both thetemporal displacement
of actual events, and distor-tions of content. Most contemporary
researchers be-lieve that confabulators believe and defend
theirconfabulations and are not engaged in an active needto fill in
gaps to avoid embarrassment or hide a mem-ory disorder.
Nonetheless, these two disparate concep-tualizations of
confabulation remain today: unawaretemporal displacement versus an
active, aware gapfilling.
Factors Associated with Confabulation
As discussed above, confabulation typically includessome element
of both content distortion and temporaldisplacement of actual
events. Severe confabulation(e.g., following ACoA aneurysm) usually
appearsacutely, and typically lasts for a period of weeks tomonths,
although it can, rarely, last for years (Talland,1965; Weinstein,
1996). Several variables important inunderstanding confabulation
are presented in Table 1.
It is very important to differentiate confabulationfrom what is
commonly observed in patients duringan acute confusional state.
While confabulation canbe observed during such confusional states,
continuedconfabulation following resolution of an acute confu-
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4
-
Confabulation
TABLE 1Important Variables in the Understanding of
Confabulation
Awareness vs. UnawarenessTemporal Displacement vs. Content
DistortionPremorbid Personality FactorsImpaired Reality
MonitoringRequires Coexistence of Amnesia vs. No Amnesic
RequirementFrontal (or Executive) Dysfunction Alone Sufficient for
Confabu-lationDifferentiated from Acute Confusional StateImpaired
Strategic RetrievalDisconnection SyndromeSubtypes of
ConfabulationIndifference or Apathy vs. Deceit or Lying
sional state is rare, and usually limited to circum-scribed
lesions. For instance, DeLuca and Cicerone(1991) studied
confabulation in ACoA patients in twonaturally occurring
conditions: while disoriented andagain with the return of
orientation to person, place,and time. Confabulatory responses to
directed ques-tions were studied in ACoA patients and a
heteroge-neous group of patients with bleeds elsewhere in thebrain.
These authors reported that confabulation wasobserved in both
groups during the disoriented stage(100% of ACoA subjects and 41 %
of the other group).However, with the return of orientation, all
ACoApatients continued to confabulate, while confabulationwas
virtually nonexistent in the other intracranial hem-orrhage group.
DeLuca and Cicerone (1991) suggestedthat the prolonged
confabulation observed in theACoA subjects was a result of specific
cerebral distur-bance that included the frontal lobes, which is
differ-ent from mechanisms involved with confabulationfrom an acute
confusional state.
A distinction between confabulation and delusionis also
important. While confabulation may at timesseem difficult to
distinguish from a delusion, confabu-lations typically involve
specific episodes or events,while most delusions concern false
beliefs (Weinstein,1996). The American Psychiatric Association
definesdelusion as "A false belief based on incorrect infer-ence
about external reality that is firmly sustained....The belief is
not one ordinarily accepted by othermembers of the person's culture
..." (p. 765).
Confabulators, particularly following ACoA an-eurysm, will
defend their confabulations as veridical,and defend their
statements readily, as illustrated bypatient OJ above.
123
Subtypes of Confabulation
Korsakoff (1889) described a continuum of confabula-tion based
on severity. However, Kraepelin (1904,1907, 1919) proposed two
subtypes: (1) Simple con-fabulation was defined as minor
distortions or recallof fact, time, or detail; (2) fantastic
confabulation con-sisted of bizarre, exaggerated, florid, or
impossibleverbalizations. Berlyne (1972) referred to "momen-tary"
(i.e., provoked by questions probing the sub-ject's memory,
consisting of temporal displacement ofactual memories) and
"fantastic" (i.e., spontaneous,grandiose) confabulation
respectively. Most recently,Kopelman (1987) argued for a
distinction between"spontaneous" and "provoked" confabulation,which
mirrors the fantastic and momentary distinc-tions respectively.
Although the terms provoked ver-sus spontaneous (Kopelman, 1987)
have gainedacceptance recently, the general distinction
remainssimilar to those first conceptualized by Kraepelin.
Theargument as to whether confabulation reflects a con-tinuum of
severity versus distinct subtypes remains acentral issue even
today.
While the dichotomous distinctions between aminor and major form
have survived, the variousterms and definitions in the literature
have contributedto the confusion regarding confabulation. A major
is-sue to address is whether provoked and spontaneousconfabulations
represent two distinct forms with dif-ferent neuropathological
mechanisms or if each is anextreme on a continuum from a single
underlyingmechanism.
Support for the contention that spontaneous andprovoked
confabulation represent extremes of a con-tinuum was presented by
DeLuca and Cicerone(1991). As described above, these authors
examinedconfabulation first when ACoA patients were disori-ented
and again when they regained orientation to per-son, place, and
time. They showed that as patientsprogressed from the disoriented
to oriented state, con-fabulation in the same subject changed from
spontane-ous to provoked in nature. Since these were the
samesubjects over the two orientation conditions, differ-ences
between types of confabulation were unlikelyto be due to
differences in lesion location. Also, bothspontaneous and provoked
forms of confabulationwere often observed in the same patient
during eitherorientation condition, suggesting that different
lesionswere not required to be present with either of the twoforms
of confabulation. Based on these data, DeLucaand Cicerone (1991)
concluded that confabulation fol-
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4
-
124
lowing ACoA aneurysm may represent differences indegree and not
kind.
Others have supported the hypothesis that formsof confabulation
represent different degrees of a com-mon disorder (Kapur and
Coughlan, 1980; Shapiroet aI., 1981; Dalla Barba, 1993; Fischer,
Alexander,D'Esposito, and Otto, 1995). Several authors havenoted
that a more substantial degree of frontal lobepathology is required
to manifest spontaneous versusprovoked confabulation. For instance,
Kapur andCoughlan (1980) reported on an ACoA case
whoseconfabulation changed from fantastic (i.e., spontane-ous) to
momentary (i.e., provoked) over severalmonths, with this change
paralleled by improvementson tests of "frontal lobe
functioning."
In contrast, several authors have suggested thatthe two forms of
confabulation reflect different under-lying pathology. Berlyne
(1972) concluded that "fan-tastic confabulation seems to be a
distinct entityhaving nothing in common with momentary
confabu-lation ..." (p. 33). Schnider, von Daniken, and Gut-brod
(1996) reported a double dissociation betweenspontaneous and
provoked confabulation. These au-thors classified patients as
either spontaneous (definedas acting-out self-generated
confabulations) or pro-voked (defined as emitting intrusions on a
verbal listlearning task). They reported that provoked but
notspontaneous confabulation was correlated with perfor-mance on
measures of verbal learning and verbal flu-ency. In contrast,
spontaneous but not provokedconfabulation was associated with
difficulties in tem-poral order processing on a continuous
recognitiontask. Based on this double dissociation, the
authorsconcluded that the two forms represent different disor-ders
rather than different degrees of the same disorder.One significant
limitation with this study is how spon-taneous and provoked
confabulation was operationallydefined. While few would argue that
acting-out con-fabulations more likely reflect spontaneous
confabula-tions, equating intrusions during list
learningperformance with confabulation is problematic. Thisis
primarily because intrusion errors on such instru-ments are not
uncommon among a broad spectrum ofneurologic populations, most of
whom do not confab-ulate.
Kopelman (1987) examined immediate and 45-minute delayed story
recall in Korsakoff and Alzhei-mer patients as well as healthy
controls, examiningprovoked confabulation (defined as intrusions on
storyrecall). Additionally, healthy subjects were also askedto
recall the stories one week after learning. The re-sults
demonstrated evidence of provoked confabula-
John DeLuca
tion in both the Korsakoff and Alzheimer groups at theimmediate
and 45-minute delay intervals. In contrast,healthy control subjects
produced provoked confabu-lations only at the one-week interval.
However, theintrusions and distortions observed by the healthygroup
at one week resembled that observed for thetwo clinical groups
during immediate and 45-minutedelays. Kopelman (1987) concluded
that there are in-deed two types of confabulation. Spontaneous
confab-ulation results from superimposing a "frontal"dysexecutive
dysfunction on an organic amnesia. Incontrast, although common in
some amnesic patients,provoked confabulation "resembles the errors
pro-duced by healthy subjects at prolonged intervals, andmay
represent a normal response to a faulty memory"(p. 1436).
Attempts at Operational Definitions of Confabulation
One common theme apparent among most of the at-tempts to
differentiate among types of confabulationis the notion of less
versus more severe confabulation.These have taken the form, for
instance, of contrastingnonconfabulators with low versus high
confabulators(Cunningham, Pliskin, Cassisi, Tsang, and Rao,
1997).Some have defined confabulation operationally as in-trusions
on verbal list learning or prose recall tests(Mercer, Wapner,
Gardner, and Benson, 1977), withsome referring to this form of
confabulation as "pro-voked," and contrasting them (spontaneous)
withthose who commit overt behavior signs of confabula-tory
behavior such as acting out one's confabulation(Schnider, von
Daniken, and Gutbrod, 1996). Suchdistinctions are based on the
hypothesis that severityof confabulation represents different forms
of confab-ulation, each with a different mechanism. The needfor
such operational definitions stems, in large part,from the lack of
a universally accepted definition ofconfabulation and its various
components. Until someconsensus on such issues is accepted,
attempts to fullyunderstand the behavioral, cognitive, and
neurologicmechanisms of confabulation will remain hindered.
In summary, the dichotomy between differencesin confabulation
that reflect differences in severityversus distinct forms, first
established at the turn ofthe nineteenth century by Korsakoff and
Kraepelin re-spectively, remain with us today. There is no
definitivesupport for either hypothesis at the turn of the
twenti-eth century. This work remains burdened by the lackof a
clear definition and conceptualization of whatconfabulation truly
is.
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4
-
Confabulation
Neurobehavioral Models of Confabulation
The underlying neurobehavioral mechanisms respon-sible for
confabulation have been of interest since con-fabulation was first
identified by Korsakoff. Ingeneral, three neurobehavioral models of
confabula-tion have been proposed. These are: the memory
im-pairment model, which stresses the importance ofimpaired memory
in confabulation; the executive im-pairment model, which identifies
frontal/executivedysfunction as the key element responsible for
confab-ulation; and the combined memory and executive dys-function
model, which states that confabulation isobserved only in the
presence of both a significantmemory disorder and frontal/executive
dysfunction.Each model is discussed in turn.
The memory impairment model stresses the needfor amnesia in
order for confabulation to be present(Talland, 1965; Talland,
Sweet, and Ballantine, 1967).The association of confabulation with
impaired mem-ory or amnesia has long been recognized. However,both
Korsakoff and Kraepelin recognized that, al-though associated with
memory impairment, defectivememory alone could not account for
confabulation.Perhaps the most compelling evidence that
impairedmemory or amnesia alone is not sufficient to
causeconfabulation is the fact that not all amnesic
patientsconfabulate. This lack of confabulation among amne-sics is
particularly true among mesial-temporal amne-sics (Parkin, 1984;
Moscovitch and Melo, 1997).Additional evidence against the impaired
memorymodel of confabulation is that confabulation clears inmost
patients (e.g., ACoA) over a period of weeksor months, yet no
change is observed in the memorydisorder (e.g., Kapur and Coughlan,
1980; Benson etaI., 1996). Further, there are several papers that
showthat lesions restricted to the basal forebrain, resultingin
impaired memory, do not produce spontaneous con-fabulation (Berti,
Arienta, and Papagno, 1990; Morris,Bowers, Chatterjee, and Heilman,
1993; Abe, Ino-kawa, Kashiwagi, and Yanagihara, 1998). For
in-stance, discrete lesions of the septal nuclei alone mayresult in
amnesia, but without confabulation (von Cra-mon, Markowitsch, and
Schuri, 1993; Berti, Arienta,and Papagno, 1999). Fischer et aI.
(1995) showed thatACoA patients with basal forebrain lesions can
showprovoked confabulation. However, it is unclearwhether such
responses were more a function of aconfusional state (DeLuca and
Cicerone, 1991).
The second model hypothesizes that confabula-tion is a
consequence solely of executive dysfunction,resulting from
disinhibition, lack of self-monitoring,
125
and decreased awareness (Kapur and Coughlan, 1980;Joseph, 1986;
Johnson, Hashtroudi, and Lindsay,1993; Benson et aI., 1996). The
notion that the frontallobes are necessary for confabulation is now
well es-tablished. Several studies have shown convincinglythat the
ventromedial region of the frontal lobes iscritical for spontaneous
confabulation (Vikki, 1985;Fischer et aI., 1995; Schnider, von
Daniken, and Gut-brod, 1996; Moscovitch and Mello, 1997; Ptak
andSchnider, 1999). Evidence for the executive model hascome from
studies showing that confabulation dimin-ishes as performance
improves on measures of execu-tive functioning (e.g., Kapur and
Coughlan, 1980;Papagno and Baddeley, 1997). In addition,
confabula-tion has been shown to be associated with
decreasedperfusion of the orbitofrontal cortex bilaterally,
withimprovements in confabulation related to increasedfrontal lobe
perfusion (Mentis, Weinstein, Murphy,McIntosh, and Pietrini, 1995;
Benson et aI., 1996).Importantly, while improvements in
frontal/executivemeasures are associated with diminished
confabula-tion, the severity of amnesia remains unchanged.
A major problem for the executive dysfunctionhypothesis of
confabulation is that not all patients withfrontal/executive
dysfunction confabulate. For in-stance, Vikki (1985) showed that
only ACoA amne-sics with frontal lesions were confabulators.
However, the executive model of confabulationalso suggests that
a memory disorder is not requiredfor confabulation to be manifested
(Johnson, 1991).The model contends that executive dysfunction
aloneis sufficient to result in confabulation. In general, thereare
few studies that support this claim, and those thatdo are
problematic. For instance, several studies havecited Kapur and
Coughlan's (1980) case report in sup-port of the notion that a
memory disorder is not re-quired for confabulation. Kapur and
Coughlan (1980)state that confabulation is not' 'dependent upon
globalamnesia." Similarly, Papagno and Baddeley (1997)state that
confabulation can occur without' 'unequivo-cal evidence of
amnesia." However, close examina-tion of both of these reports
indeed reveal significantlycompromised memory performance in these
patients,not on immediate recall, but on delayed recall.
Forinstance, on the only test provided by Papagno andBaddeley
examining delayed recall, patient MM couldnot recall anything about
the story, despite immediaterecall close to normal limits. The
exact same findingof significantly impaired delayed recall was
observedin the case by Kapur and Coughlan (1980). ManyACoA patients
show relatively intact immediate recallbut significantly
compromised delayed recall (c.f., De-
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4
-
126
Luca and Diamond, 1995). As such, a look at the fewcases in the
literature that claim that impaired memoryis not required for
confabulation provide weak evi-dence, if any, against the
dual-lesion hypothesis ofconfabulation (both impaired memory and
executivefunctions are necessary, see below).
Most authors who contend that impaired memoryis not necessary
for confabulation cite the work ofWhitty and Lewin (1957, 1960) in
support of thisclaim. Whitty and Lewin reported several cases
ofconfabulation following anterior cingulectomy fortreatment of
severe obsessional neurosis. The confab-ulation identified by
Whitty and Lewin (1957, 1960)was transient, lasting 24 hours to 3
days, and tookplace while subjects were disoriented to time.
Onefeature emphasized by these authors was the vividdreamlike
experiences of these patients. However,such experiences are not
uncommon in acute confu-sional states (Lipowski, 1990). Impaired
memory anddisorientation are other features associated with anacute
confusional state (Lipowski, 1990). The case ex-amples provided by
Whitty and Lewin include exam-ples of impaired memory and
disorientation, a pointclearly acknowledged by Whitty and Lewin
(1960).As such, it is more likely that what was observed byWhitty
and Lewin (1957, 1960) was more a reflectionof an acute confusional
state, rather than confabula-tion from the primary cerebral
structures that underliea more general phenomenon. DeLuca and
Cicerone(1991) showed that while confabulation was not un-common in
patients who are disoriented, only ACoApatients continued to
confabulate with the return oforientation, suggesting a different
neuropathologicalsubstrate in the ACoA patients compared to a
hetero-geneous group of hemorrhagic stroke patients. There-fore,
citations of Whitty and Lewin's patients asevidence against the
importance of memory in confab-ulation are relatively weak.
For several reasons, it is important to be cautiousin citing
work from so long ago as definitive. First, ifthe anterior
cingulate is critical for confabulation, whyhasn't more recent work
confirmed this very earlyrelationship? Second, relative to today's
standards,neurosurgical techniques were relatively crude five
de-cades ago. As such, precise lesion characterizations inthese
patients could not be made with the precisionoffered today. Lastly,
anterior cingulate involvementis often observed in patients with
ACoA aneurysm(DeLuca and Diamond, 1995; Johnson, Hayes,
D'Es-posito, and Raye, in press). Despite decades of ACoAresearch,
few have specifically implicated the anteriorcingulate alone as
critical for confabulation. Thus,
John DeLuca
while the anterior cingulate area may play a role
inconfabulation, it is also possible that due to its proxim-ity to
regions that have been shown by ACoA patientsto be critical for
confabulation (e.g., basal forebrainand ventromedial frontal lobes,
see discussion below),the anterior cingulate may have little or no
direct rolein confabulation.
The third and most recent model is that confabu-lation
(particularly spontaneous confabulation) re-quires both amnesia and
executive dysfunction (dual-lesion hypothesis) in order to be
expressed (Stuss, Al-exander, Lieberman, and Levine, 1978;
DeLuca,1993; DeLuca and Diamond, 1995; Fischer et aI.,1995;
Schnider, von Daniken, and Gutbrod, 1996;Moscovitch and Mello,
1997; Wheatly and McGrath,1997; Cunningham, et aI., 1997; Ptak and
Schnider,1999). DeLuca (1993) compared a group of amnesicACoA
patients with a group of nonamnesic ACoApatients, all of whom
demonstrated psychometric andneuroimaging evidence of
frontal/executive dysfunc-tion. DeLuca found that only the amnesic
ACoA groupconfabulated, which supports the dual-lesion hypothe-sis
of spontaneous confabulation. Numerous other au-thors have also
supported this dual-lesion hypothesisthat requires both executive
and memory impairmentfor the expression of confabulation.
Cunningham et aI. (1997) showed that "confabu-lation results
from any general neurologic disturbancethat produces defects in
memory and executive func-tion, rather than a specific pathology or
neurologicdisorder" (p. 875). Wheatly and McCarthy (1997)showed
that while the basal forebrain may be the criti-cal site of memory
impairment in ACoA patients, whatis critical for confabulation is
impaired memory, notimpaired basal forebrain. As such, they
presented acase of confabulation in a non-ACoA patient with
ex-ecutive dysfunction and impaired memory secondaryto a
diencephalic lesion. Kopelman (1987) showedthat spontaneous
confabulation results from superim-posing a "frontal" dysexecutive
dysfunction on anorganic amnesia, while provoked confabulation was
a"normal response to a faulty memory."
Ptak and Schnider (1999) reported amnesia andconfabulation in an
ACoA patient with bilateral orbito-frontal lesions with extensive
bilateral basal forebraindamage, which included the septal region.
Ptak andSchnider (1996) suggest that the orbitofrontal cortexis the
core structure in the maintenance of temporalorder in memory by
"distinguishing between presentlyongoing and previously encountered
information."Moscovitch and Melo (1997) showed that the degreeof
memory impairment did not differ between confab-
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4
-
Confabulation
ulating and nonconfabulating amnesics, indicating thatamnesia is
not sufficient, but may be necessary forconfabulation to be
observed. Interestingly, these au-thors found that when similar
retrieval demands aremade for both episodic and semantic memory
(i.e.,typically everyday demands for semantic retrieval areeasier
to fulfill than episodic demands), confabulationwas observed among
both episodic and semanticmemories. These data do not support the
prevailingview that confabulation involves distortions primarilyof
episodic but not semantic memory (Dalla Barba,1993).
Fischer et aI. (1995) and DeLuca and Cicerone(1991) reported an
association between confabulationand executive dysfunction. Fischer
et aI. (1995) di-vided nine acute ACoA patients into two
groups,"spontaneous" confabulators and "provoked" con-fabulators.
The authors concluded that the type andseverity of confabulation
noted is largely dependentupon both impairments in memory and the
extent ofexecutive system compromise. They suggested
that"spontaneous" confabulation required disruption ofboth the
basal forebrain and frontal systems, support-ing the dual-lesion
hypothesis. More restricted lesionsto either the basal forebrain or
orbital frontal structurescan result in "provoked" or transient
confabulatoryresponses. However, Schnider, von Daniken, and
Gut-brod (1996) found that executive problems did notdifferentiate
between spontaneous and nonconfabulat-ing amnesics. Some have
suggested that confabulationwas associated more with lesions of the
right hemi-sphere (e.g., Joseph, 1986). However, an extensive
re-view by Johnson et aI. (in press) found no evidencefor this
contention.
In summary, it appears that the dual-lesion hy-pothesis, which
states that memory confabulation re-quires both a lesion resulting
in significant amnesia(i.e., to either basal forebrain,
diencephalic or mesialtemporal structures) as well as damage to the
fron-tal-executive system, provides the most convincingexplanation
for confabulation. The ventromedial por-tion of the frontal lobes
(i.e., in the distribution of theanterior cerebral artery) appears
to be the key structurewithin the frontal lobes.
Cognitive Explanations of Confabulation
Numerous authors have concluded that poor self-mon-itoring is a
primary element in the expression of con-fabulation (Johnson et
aI., 1993; Benson et aI., 1996;Schnider, von Daniken, and Gutbrod,
1996; Papagno
127
and Baddeley, 1997; Moscovitch and Melo, 1997;Ptak and Schnider,
1999; Johnson et aI., in press).However, Ptak and Schnider
cautioned that "poorself-monitoring ... may serve as a descriptive
expla-nation" and Schnider, von Daniken, and Gutbrod(1996) continue
that such an executive dysfunction"does not disclose the specific
mechanism of confabu-lations." However, recent work has shed some
lighton the cognitive mechanisms that may be responsiblefor
confabulation.
Moscovitch and Melo (1997) note that there isgeneral agreement
that confabulation is more of aproblem in retrieval rather than
encoding, consolida-tion, or storage. These authors postulate that
it is im-paired strategic retrieval (i.e., an active,
self-initiated,goal-directed, and an effortful systematic
memorysearch) that is primarily responsible for confabulationdue to
damage to ventromedial frontal structures, asopposed to associative
retrieval (passive, automaticsearch through memory). As mentioned
above, severalinvestigators suggest that spontaneous
confabulationis a result of a difficulty in recognizing the
temporalorder of events during the retrieval of stored
informa-tion. Moscovitch and Melo (1997) suggest that defec-tive
temporal order processing is not the cause ofconfabulation, but a
symptom of a more fundamentalproblem in the strategic retrieval of
the memory traceand defective self-monitoring of this trace.
Specifi-cally, Moscovitch and Melo (1997) state that the keydeficit
that results in confabulation is not simply theseverity of the
impaired strategic search at input (i.e.,searching for the memory
trace), but an impairmentin the monitoring at output (i.e.,
monitoring what wasretrieved). Hence, confabulation occurs when the
out-come of a disturbed strategic search is faulty and aresponse is
emitted without proper monitoring, evalua-tion, and verification of
the recovered memory trace(Rapcsak, Kaszniak, Reminger, Glisky,
Glisky, andComer, 1998).
Johnson and colleagues (Johnson, 1991; Johnson,O'Connor, and
Cantor, 1997; Johnson et aI., in press)suggest that different types
of confabulation wouldresult from different combinations of
cognitive diffi-culties. Johnson discusses confabulation within
thecontext of difficulties in reality monitoring or
sourcemonitoring. For instance, confabulation could resultfrom
difficulties in the encoding of information. Yet,confabulation may
also result from poor retrieval, orreduced motivation. Johnson et
aI. (1997) concludedthat confabulation in an ACoA case study
(patient GS)was based on a confluence of factors including:
(1)deficits in the systematic retrieval of autobiographical
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4
-
128
information; (2) source monitoring deficit; and (3) apropensity
toward detailed imaginations. Johnson etaI. (1997) conclude that
what specific combination ofcognitive deficits are observed in a
particular patientwill dictate the type and severity of
confabulation ob-served.
In summary, cognitive theories on the mechanismof confabulation
stress impaired self-monitoring andimpaired retrieval mechanisms
(i.e., strategic re-trieval) as critical elements responsible for
confabu-lation.
Confabulation and Awareness
The relationship between confabulation and disturbedawareness
has long been recognized. For instance,several studies have shown
that confabulation de-creases as awareness increases (Williams and
Rupp,1938, cited in McGlynn and Schacter, 1989; Wykeand Warrington,
1960; Mercer et aI., 1977; Stuss etaI., 1978; Shapiro et aI., 1981;
DeLuca, 1992). Bensonet aI. (1996) believe that confabulation and
defectiveself-awareness represent the same basic functional
dis-order (p. 1243). Other evidence to support this con-tention
comes from work showing that confabulationdiminishes as performance
on tests of frontal/execu-tive improves (Papagno and Baddeley,
1997; Kapurand Coughlan, 1980), and that confabulation dimin-ishes
with improvements in frontal lobe perfusion onSPECT scans of the
brain (Benson et aI., 1996). How-ever, unawareness syndromes do not
always lead toconfabulation. As described above, a major
problemwith confabulation is its broad-based definition, whichoften
confuses the picture rather than providing clar-ity. As such, many
have associated responses resultingfrom deficits of unawareness
with confabulation. Aftera brief introduction to anosognosia and
denial, a briefdescription is provided of unawareness syndromes
thathave been referred to as confabulation in the classi-cal
literature.
The syndrome of unawareness following braindamage is called
anosognosia. It was first describedby von Monakow (1885) and Anton
(1896). The indif-ference that is sometimes associated with
anosognosiahas been called anosodiphoria (Heilman, 1991).
Ano-sognosia is seen in many behavioral syndromes fol-lowing brain
damage, including Wernicke's aphasia,Anton's syndrome, and left
hemiplegia (see Heilman,1991, for a brief review), each of which is
describedbriefly below.
John DeLuca
First, however, anosognosia needs to be differen-tiated from
"denial of illness" (c.f., Prigatano andSchacter, 1991; Prigatano
and Klonoff, 1998). Psychi-atric definitions of "denial" have been
describedmore as altered self-awareness rather than un-awareness.
The American Psychiatric Association(1994) defines denial as a
defense mechanism wherethe' 'individual deals with emotional
conflict or inter-nal or external stressors by refusing to
acknowledgesome painful aspect of external reality or
subjectiveexperience that would be apparent to others" (p.
755).Prigatano and Klonoff (1998) explain that "denialafter brain
injury ... reflects the individual's attemptto use previous coping
strategies to deal with impair-ments that are only partially
recognized" (p. 57). Us-ing these definitions, "gap filling" in
confabulationcould be considered denial while displaced
temporalcontext, or the lack of information access due to
adisconnection syndrome (e.g., the Interpreter) couldreflect an
anosognosia, or unawareness of knowledge(Schacter, 1991).
Wernicke's aphasia is a well-known languagedisorder in which
patients produce fluent speechmarked by neologism and semantic and
paraphasicerrors. These errors have been viewed as confabula-tions.
While comprehension is severely compromised,such aphasics cannot
always express themselves. Im-portantly, these patients are unaware
that the personwith whom they are speaking does not understandthem.
It has been suggested that the anosognosia asso-ciated with
Wernicke's aphasia is one of defectivemonitoring. Such patients
have lost their neural repre-sentation of word sounds and are then
unable to matchtheir speech output with an intact representation
ortemplate. This lack of internal feedback results in
theanosognosia (Heilman, 1991).
Despite the inability to demonstrate sight, pa-tients with
Anton's syndrome "deny" cortical blind-ness (Heilman, 1991). They
will confabulateresponses (e.g., provide a response when asked
howmany fingers they can see during confrontation) andwill make
excuses when confronted with their errors("I'm not wearing my
glasses"). While several at-tempts have been made to explain this
phenomenon,it is likely that the explanation for Anton's syndromeis
similar to that of Wernicke's aphasia: impairedmonitoring. Some
have hypothesized that the visualassociation cortex becomes
disconnected from thespeech-language areas, leading to decreased
monitor-ing and confabulation. Others have hypothesized thatsuch
patients continue to receive input via the' 'secondvisual system";
a pathway mediated via the superior
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4
-
Confabulation 129
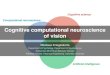
Figure 1. Broad and Narrow Sense Confabulation
aLesions resulting in memory disorder may include basal
forebrain, diencephalic, ormesial temporal structures
;.' '. j~,~;!it';.,":' NARROW SENSE
., , CONFAB~TION
RighI SilileralParielaI&FronUlI Occipital
Je$ioll lesion
"BROAD st~SEC '?t_ "CONfABULATION' ~,?~~
.~~ '
fabulation is illustrated in Figure 1. First, it is pro-posed
that two definitions of confabulation areneeded: Broad sense
confabulation, which can be de-fined in a more broad or all
encompassing sense, andNarrow sense confabulation, which is more
perceptu-ally specific. Broad sense confabulation simply refersto
the general conceptualization of distortion; that is,what is common
across various forms of confabula-tion is that information is
perceptually distorted (e.g.,one can "see" with Anton's syndrome,
one can useone's left extremities despite hemiplegia, one can
dis-place actual memories temporally). As such, under-standing
broad sense confabulation means focusing onfeatures that are
similar across the various manifesta-tions of confabulatory
behavior. It is simply descrip-tive in nature. It is unlikely that
broad senseconfabulation will have an anatomic locus, nor
should
tempts to make seemingly logical inferences (e.g., "Idon't have
my glasses"), the same as profuse, sponta-neous, and fantastic
verbal confabulation? At somelevel of argument, one can
conceptualize these broadlyas confabulations. At another level,
however, they areindeed different. This lack of a clear
understandingburdens a greater conceptual understanding of
confab-ulation. What is needed is a model of confabulationthat
outlines not only the similarities, but also the dif-ferences among
these various examples of confabu-lation.
Given the various general forms of cognitive/per-ceptual
distortions that have been referred to as con-fabulation, can any
systematic understanding ofconfabulation be made? The answer must
be "yes,"in order to move our understanding of confabulationbeyond
what was generally conceptualized at the endof the nineteenth
century. A proposed model of con-
A Proposed Model of Confabulation
Are neologisms truly confabulations? Are examplesof "denying"
cortical blindness, where the patient at-
colliculus. This may result in input to a visual monitoror
speech-language region that may be disconnectedfrom the
geniculocalcerine system (the primary visualsystem). While impaired
memory is usually associatedwith Anton's syndrome, its significance
is not clear.
Patients with right hemisphere lesions (usuallyinvolving the
parietal and frontal regions) often dis-play left-sided hemiplegia,
but also may' 'deny" thatanything is wrong with their left side
(e.g., denyingthat their own hand is theirs, confabulating a
responsewhen confronted). Many theories have been positedto explain
the unawareness, indifference, and confabu-lation associated with
this behavioral syndrome, rang-ing from premorbid personality
features (Weinsteinand Kahn, 1955, 1996) to disconnection
syndromesand impaired monitoring of somatosensory input(Heilman,
1991).
One important feature that is different betweenthese three
neurobehavioral syndromes that lead toconfabulation, versus those
often evident from ACoAaneurysm or Korsakoff's syndrome, is the
depth ofthe confabulation itself. While ACoA confabulationcan be
very elaborate and lengthy, confabulation asso-ciated with
Wernicke's aphasia, Anton's syndrome,and anosognosia for hemiplegia
is usually targeted(i.e., on the left-hemiplegia or blindness) and
limitedin content.
An aspect that appears common to all of theseclinical entities
is an unawareness syndrome (anosog-nosia). This unawareness may
result from differentcerebral mechanisms, but the behavioral effect
is thesame. For instance, with the Interpreter describedabove, the
information within the right hemisphere isnot available to the left
hemisphere in split-brain pa-tients (i.e., disconnection syndrome)
resulting in con-fabulation from an intelligent verbal
hemispheretrying to make logical sense of cues in the environ-ment.
However, this mechanism is different from, forinstance, the
compromised neural representation ofword sounds that prevents
Wernicke's aphasics frombeing aware of their own jargon speech.
Lastly, mem-ory confabulators (e.g., ACoA patients) can producea
long verbal discourse about seemingly inaccurateevents, not being
able to self-monitor the temporal andoften illogical relationships
within their own state-ments. While the specific behavioral feature
of theseexamples differ, the anosognosia associated with
thebehavior is the common denominator.
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4
-
130
one be forced upon it. Broad sense confabulation canthus be
defined as follows: statements or actions thatinvolve apparently
unintentional but obvious distor-tions.
Narrow sense confabulation involves the
specificcognitive-perceptual system that is being confabu-lated.
Narrow sense confabulation can be viewed asconfabulation that is a
manifestation of damage to aspecific cognitive-perceptual mechanism
that is im-paired, each with its own identifiable lesion (see
Fig-ure 1).
Because confabulation is not a unitary behavioralconstruCt, the
need for narrow sense confabulation be-comes critical once one
begins to discuss mechanismor neuropathology. For instance, the
hypothesis of im-paired strategic retrieval for memory
confabulationmay not apply to explanations of confabulation
associ-ated with left hemiplegia. Narrow sense confabulationallows
for a discussion of specific mechanisms respon-sible for a
particular form of confabulation, withouthaving to provide a more
global explanation for allforms of confabulation.
While the dichotomy between broad and narrowsense confabulation
may seem simplistic and "obvi-ous" to researchers and students of
confabulation, theinappropriate use of the term in the literature
and med-ical textbooks cited throughout this paper speaks vol-umes
for the need for a more refined terminologywhen confabulation is
discussed.
Conclusions
In many ways, much has been learned about confabu-lation during
the past century. However, in other verysignificant ways we have
progressed little from whatwas known 100 years ago. Korsakoff
believed thatmemory confabulation consisted of actual events
dis-placed temporally of which patients were unaware.In contrast,
Bonhoffer (1901) felt that confabulationswere an active attempt to
cover up a disorder of whichthe patient was consciously aware.
Despite the lack ofempirical support for the active gap filling
hypothesis,these two opposing viewpoints remain prominent intoday's
literature and thinking. Little progress hasbeen made in 100 years
of research in identifyingwhether memory confabulation represents a
single en-tity, differing only in degree, as hypothesized by
Kor-sakoff, versus having two (or more) distinct forms
ofconfabulation, each with its own neuropathologicmechanism, as
initially outlined by Kraepelin. It isbelieved that much of the
difficulty in understanding
John DeLuca
factors such as these stems from the lack of a univer-sally
accepted definition or model of confabulation. Itis hoped that the
model proposed in the present papercan serve as a starting point,
eventually resolving intoan accepted conceptual framework from
which tostudy confabulation.
References
Abe, K., Inokawa, M., Kashiwagi, A., Yanagihara, T.(1998),
Amnesia after a discrete basal forebrain lesion.J. Neurol.
Neurosurg. & Psychiatry, 65: 126-30.
American Psychiatric Association (1994), Diagnostic
andStatistical Manual of Mental Disorders, 4th ed. (DSM-IV).
Washington, DC: American Psychiatric Press.
Anton, G. (1896), Blindheit nach beiderseitiger
Gehirner-krankung mit Verlust der Orienterung in Raume.
Mitteil.Vereines Arzte Steirmark, 33:41-46.
Benson, D. F., Djenderedjian, A., Miller, B. L., Pachana,N. A.,
Chang, L., Itti, L., & Mena, I. (1996), Neural basisof
confabulation. Neurology, 46:1239-1243.
Berlyne, N. (1972), Confabulation. Brit. J.
Psychiatry,120:31-39.
Berti, A., Arienta, C., & Papagno, C. (1990), A case
ofamnesia after excision of the septum pellucidum. J. Neu-rol.,
Neurosurg. & Psychiatry, 53:922-924.
Bonhoeffer, K. (1901), Der Korsakowsche Symptomen-komplex in
seinen Beziehungen zu den 'verschiedenenKrankheitsformen. Algemeine
Zeitschr. fur Psychiatrie,61:744-752.
Cunningham, J. M., Pliskin, N. H., Cassisi, J. E., Tsang,B.,
& Rao, S. M. (1997), Relationship between confabu-lation and
measures of memory and executive function.J. Clin. & Exper.
Neuropsychology, 19:867-877.
Dalla Barba, G. (1993), Confabulation: Knowledge and
rec-ollective experience. Cog. Neuropsychol., 10:1-20.
DeLuca, J. (1992), Rehabilitation of confabulation: The is-sue
of unawareness of the deficit. NeuroRehab., 2:23-30.
--- (1993), Predicting neurobehavioral patterns follow-ing
anterior communicating artery aneurysm. Cortex,29:639-647.
--- Cicerone, K. D. (1991), Confabulation followinganeurysm of
the anterior communicating artery. Cor-tex, 27:417-423.
---Diamond, B. J. (1995), Aneurysm of the anteriorcommunicating
artery: A review of neuroanatomical andneuropsychological sequelae.
J. Clin. Experiment. Neu-ropsychol., 17: 100-121.
Feinberg, T. E., Roane, D. M., Kwan, P. C., Schindler, R.J.,
& Haber, M. (1994), Anosognosia and visuoverbalconfabulation.
Arch. Neurol., 51 :468-473.
Fischer, R. S., Alexander, M. P., D'Esposito, M., & Otto,R.
(1995), Neuropsychological and neuroanatomical cor-relates of
confabulation. J. Clin. Exp. Neuropsychol.,17:20-28.
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4
-
Confabulation
Gazzaniga, M. S. (1998), The Mind's Past. Berkeley: Uni-versity
of California Press.
Heilman, K. M. (1991), Anosognosia: Possible neuropsy-chological
mechanisms. In: Awareness of Deficit afterBrain Injury: Clinical
and Theoretical Issues, ed. F. P.Prigatano & D. L. Schacter.
New York: Oxford Univer-sity Press.
Johnson, M. K. (1991), Reality monitoring: Evidence
fromconfabulation in organic brain disease patients. In:Awareness
of Deficit after Brain Injury: Clinical andTheoretical Issues, ed.
G. P. Prigatano & D. L. Schacter.New York: Oxford University
Press, pp. 176-197.
---Hashtroudi, S., & Lindsay, D. S. (1993),
Sourcemonitoring. Psycholog. Bull., 114:3-28.
---Hayes, S. M., D'Esposito, M., & Raye, C. L. (inpress),
Confabulation. In: Handbook of Neuropsychol-ogy, Vol. 4, 2nd ed.,
ed. F. Boller & J. Grafman. Amster-dam: Elsevier Science.
---O'Connor, M., & Cantor, J. (1997), Confabulation,memory
deficits, and frontal dysfunction. Brain & Cog-nit., 34:
189-206.
Joseph, R. (1986), Confabulation and delusional denial:Frontal
lobe and lateralized influences. J. Clin. Psy-chol.,
42:507-520.
Kapur, N., & Coughlan, A. K. (1980), Confabulation
andfrontal lobe dysfunction. J. Neurol. Neurosurg. &
Psy-chiatry, 43:461-463.
Kern, R. S., van Gorp, W. G., Cummings, J. L., Brown, W.S.,
& Osato, S. S. (1992), Confabulation in Alzheimer'sdisease.
Brain & Cognit., 19: 172-182.
Koehler, K., & Jacoby, C. (1978), Acute confabulatory
psy-chosis: A rare form of unipolar mania? Acta Psychiatr.Scand.,
57:415-425.
Kopelman, M. D. (1987), Two types of confabulation. J.Neurol.,
Neurosurg. & Psychiatry, 50:1482-1487.
Korsakoff, S. S. (1889), Psychic disorder in conjunctionwith
peripheral neuritis, tr. M. Victor & P. I. Yakovlev.Neurology,
5:394-406, 1955.
Kraepelin, E. (1904), Lectures on Clinical Psychiatry, tr.
T.Johnstone. London: Bailliere, Tindall, & Cox.
--- (1907), Clinical Psychiatry: A Textbook for Stu-dents and
Physicians, tr. A. R. Diefendorf. New York:Macmillan.
--- (1919), Dementia Praecox and Paraphrenia, tr. R.M. Barclay.
Edinburgh: E. & S. Livingstone.
Lipowski, Z. J. (1990), Delirium: Acute Confusional States.New
York: Oxford University Press.
McGlynn, S. M., & Schacter, D. L. (1989), Unawarenessof
deficits in neuropsychological syndromes. J. Clin. Ex-periment.
Neuropsychol., 11: 143-205.
Mentis, M., Weinstein, E. A., Murphy, D. G. M., McIntosh,A. R.,
& Pietrini, P. (1995), Abnormal brain glucosemetabolism in the
delusional misidentification syn-dromes. Biolog. Psychiatry,
38:438-439.
Mercer, B., Wapner, W., Gardner, H., & Benson, F. (1977),A
study of confabulation. Arch. Neurol., 34:429-433.
131
Morris, M. D., Bowers, D., Chatterjee, A., & Heilman, K.M.
(1993), Amnesia following a discrete basal forebrainlesion. Brain,
115:1827-1847.
Moscovitch, M. (1995), Confabulation. In: Memory Distor-tion:
How Minds, Brains, and Societies Reconstruct thePast, ed. D. L.
Schacter. Cambridge, MA: Harvard Uni-versity Press, pp.
226-251.
---Melo, B. (1997), Strategic retrieval and the frontallobes:
Evidence from confabulation and amnesia. Neu-ropsychologia, 35:
1017-1034.
Nathaniel-James, D. A., & Frith, C. D. (1996),
Confabula-tion in schizophrenia: Evidence of a new form?
Psy-cholog. Med., 26:391-399.
Papagno, C., & Baddeley, A. (1997), Confabulation in
adysexecutive patient: Implication for models or retrievel.Cortex,
33:743-752.
Parkin, A. J. (1984), Amnesic syndrome: A
lesion-specificdisorder. Cortex, 20:479-503.
Phelps, E. A., & Gazzaniga, M. S. (1992),
Hemisphericdifferences in mnemonic processing: The effects of
lefthemisphere interpretation. Neuropsychologia, 30:293-297.
Prigatano, G. P., & Klonoff, P. S. (1998), A
clinician'srating scale for evaluating impaired self-awareness
anddenial of disability after brain injury. Clin.
Neuropsy-chologist, 12:56-67.
--- Schacter, D. L., Eds. (1991), Awareness of Deficitafter
Brain Injury: Clinical and Theoretical Issues. NewYork: Oxford
University Press.
Ptak, R., & Schnider, A. (1999), Spontaneous
confabulationafter orbitofrontal damage: The role of temporal
contextconfusion and self-monitoring. Neurocase, 5:243-250.
Rapcsak, S. Z., Kaszniak, A. W., Reminger, S. L., Glisky,M. L.,
Glisky, E. L., & Comer, J. F. (1998), Disssociationbetween
verbal and autonomic measures of memory fol-lowing frontal lobe
damage. Neurology, 50:1259-1265.
Schacter, D. L. (1991), Unawareness of deficit and un-awareness
of knowledge in patients with memory disor-ders. In: Awareness
ofDeficit after Brain Injury: Clinicaland Theoretical Issues, ed.
G. P. Prigatano & D. L.Schacter. New York: Oxford University
Press, pp.127-151.
Schnider, A., Gutbrod, K., Hess, C. W., & Schroth, G.(1996),
Memory without context: Amnesia with confabu-lations after infarct
of the right capsular genu. J. Neurol.,Neurosurg. & Psychiatry,
61:186-193.
--- von Daniken, C., & Gutbrod, K. (1996), The mech-anisms
of spontaneous and provoked confabulations.Brain,
119:1365-1375.
Shapiro, B. E., Alexander, M. P., Gardner, H., & Mercer,B.
(1981), Mechanisms of confabulation. Neurology,31: 1070-1076.
Stuss, D. T., Alexander, M. F., Lieberman, A., & Levine,H.
(1978), An extraordinary form of confabulation. Neu-rology, 28:
1166-1172.
Talland, G. A. (1965), Deranged Memory. New York: Aca-demic
Press.
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4
-
132
-- Sweet, W. H., & Ballantine, H. T. (1967), Amnes-tic
syndrome in anterior communicating artery aneu-rysms. J. Nerv.
& Ment. Dis., 145:179-192.
van der Horst, L. (1932), Die Psychologie des Korsakow-syndroms.
Monatschr. Psychiatr. Neurol., 83:65-84.
Vikki, J. (1985), Amnesic syndromes after surgery of ante-rior
communicating artery aneurysm. Cortex,21:431-444.
von Cramon, D. Y., Markowitsch, H. J., & Schuri, U.(1993),
The possible contribution of the septal region tomemory.
Neuropsychologie, 31: 1159-1180.
von Monakow, A. (1885), Experimentelle und
patholog-ischanatomisch Untersuchungen uber die Beziehungender
sogennanten Sehs pare zu den infracorticalen Optic-uscentren und
zum Nervus opticus. Arch. Psychiatr. ,16: 151-199.
Weinstein, E. A., (1996), Symbolic aspects of
confabulationfollowing brain injury: Influence of premorbid
personal-ity. Bull. Menninger Clin., 60:331-350.
--Kahn, R. L. (1955), Denial of Illness. Springfield,IL: Charles
C Thomas.
--- Lyerly, O. G. (1968), Confabulation followingbrain injury:
Its analogues and sequelae. Arch. Gen. Psy-chiatry, 18:348-454.
John DeLuca
Wheatly, J., & McGrath, J. (1997), Co-occurence of
execu-tive impairment and amnestic syndrome following sub-archnoid
haemorrhage: A case study. Cortex,33:711-721.
Whitlock, F. A. (1981), Some observations on the meaningof
confabulation. Brit. J. Med. Psychol., 54:213-218.
Whitty, C. W. M., & Lewin, W. (1957), Vivid day-dream-ing:
An unusual form of confusion following anteriorcingulectomy in man.
Internat. J. Neurol., 5:403-409.
------ (1960), A Korsakoff syndrome in the post-cingulectomy
confusional state. Brain, 83:648-653.
Williams, H. W., & Rupp, C. (1938), Observation on
con-fabulation. Amer. J. Psychiatry, 95:95-105.
Wyke, M., & Warrington, E. K. (1960), An
experimentalanalysis of confabulation in a case of Korsakoff s
syn-drome using a tachistoscopic method. J. Neurol. Neuro-surg.,
& Psychiatry, 23:327-333.
John DeLuca, Ph.D.Neuropsychology & Neuroscience
LaboratoryKessler Medical RehabilitationResearch & Education
Corp.1199 Pleasant Valley WayWest Orange, NJ 07052e-mail: delucaj.
@umdnj.edu
Dow
nloa
ded
by [G
azi U
nivers
ity] a
t 22:4
5 18 A
ugus
t 201
4