Embed Size (px)
Citation preview
Multimodal Analgesia
Rosemary C. Polomano, PhD, RN, FAAN Associate Professor of Pain Practice
University of Pennsylvania School of Nursing Associate Professor of Anesthesiology and Critical
Care (Secondary) University of Pennsylvania
Clinician Educator Hospital of the University of Pennsylvania
Objectives
• Examine pharmacological approaches to multimodal analgesia in targeting specifcic peripheral and central mechanisms and pathways for pain
• Apply Critical thinking and utilize clinical decision making to manage and treat patients with mixed pain
• Evaluate scientific information and incorporate evidence-based practice guidelines in the treatment of mixed pain with multimodal therapies.
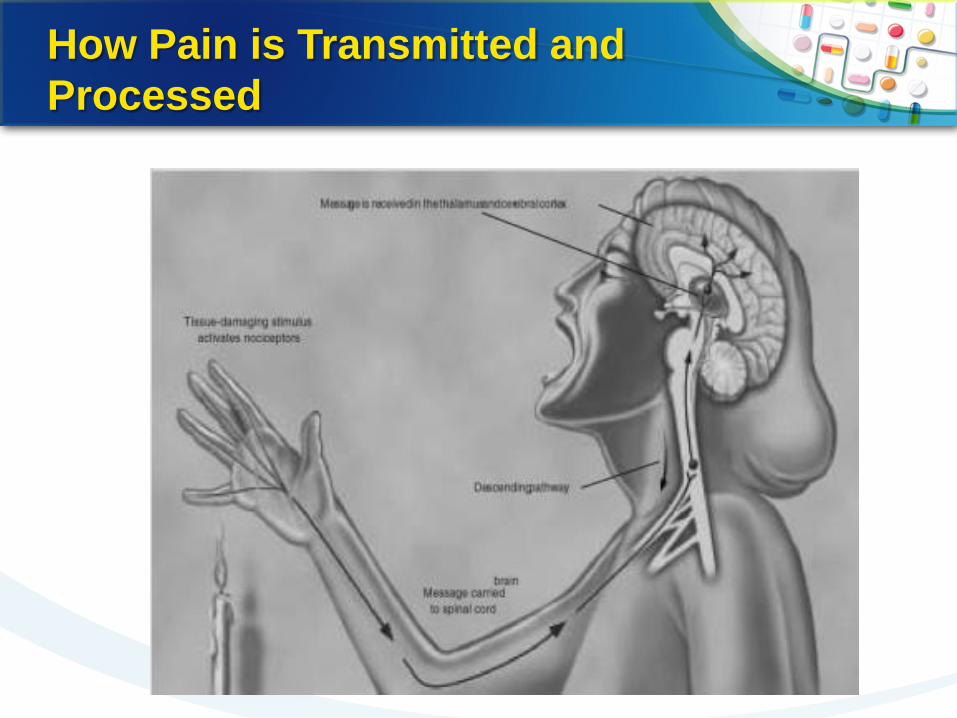
How Pain is Transmitted and Processed
Physiology of Pain: Pathways and Effects on Pain Perception
• Pain is a complex process mediated by multiple pathways and mechanisms in both the peripheral and central nervous systems (PNS and CNS [spinal cord and brain])
• Fundamental characterization of pain – Nociceptive/inflammatory
• Activation of pain-sensitive afferent neural pathways in response to injury
– Neuropathic • Abnormal pain processing due to lesions in the PNS, CNS
or both
Galer B, Gammaitoni A, Alvarez N. 6. Immunology [XIV.pain]. In: Dale DC, Federman DD, eds. WebMD Scientific American Medicine. New York, NY: WebMD Corporation; 2003. •4
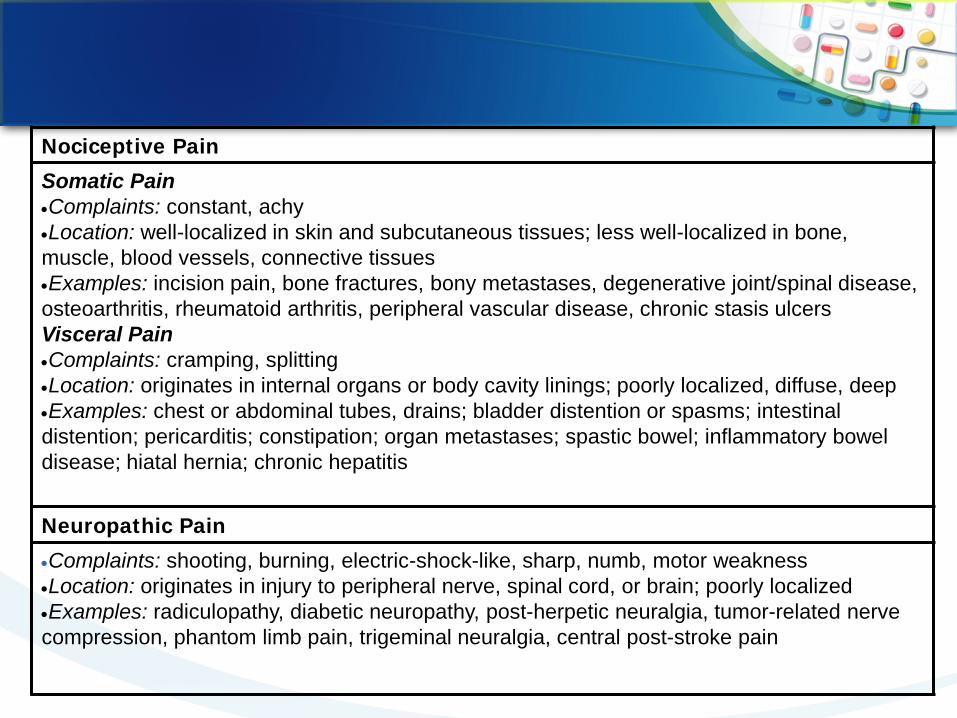
Nociceptive Pain Somatic Pain •Complaints: constant, achy •Location: well-localized in skin and subcutaneous tissues; less well-localized in bone, muscle, blood vessels, connective tissues •Examples: incision pain, bone fractures, bony metastases, degenerative joint/spinal disease, osteoarthritis, rheumatoid arthritis, peripheral vascular disease, chronic stasis ulcers Visceral Pain •Complaints: cramping, splitting •Location: originates in internal organs or body cavity linings; poorly localized, diffuse, deep •Examples: chest or abdominal tubes, drains; bladder distention or spasms; intestinal distention; pericarditis; constipation; organ metastases; spastic bowel; inflammatory bowel disease; hiatal hernia; chronic hepatitis
Neuropathic Pain •Complaints: shooting, burning, electric-shock-like, sharp, numb, motor weakness •Location: originates in injury to peripheral nerve, spinal cord, or brain; poorly localized •Examples: radiculopathy, diabetic neuropathy, post-herpetic neuralgia, tumor-related nerve compression, phantom limb pain, trigeminal neuralgia, central post-stroke pain
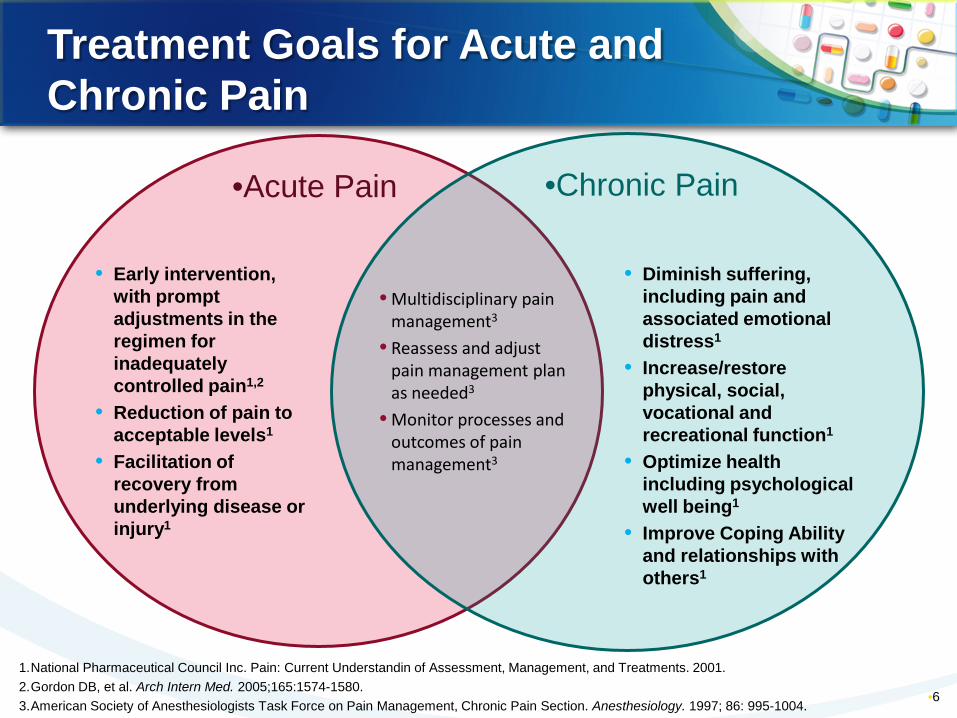
Treatment Goals for Acute and Chronic Pain
•6
• Early intervention, with prompt adjustments in the regimen for inadequately controlled pain1,2
• Reduction of pain to acceptable levels1
• Facilitation of recovery from underlying disease or injury1
• Diminish suffering, including pain and associated emotional distress1
• Increase/restore physical, social, vocational and recreational function1
• Optimize health including psychological well being1
• Improve Coping Ability and relationships with others1
• Multidisciplinary pain management3
• Reassess and adjust pain management plan as needed3
• Monitor processes and outcomes of pain management3
•Acute Pain •Chronic Pain
1.National Pharmaceutical Council Inc. Pain: Current Understandin of Assessment, Management, and Treatments. 2001. 2.Gordon DB, et al. Arch Intern Med. 2005;165:1574-1580. 3.American Society of Anesthesiologists Task Force on Pain Management, Chronic Pain Section. Anesthesiology. 1997; 86: 995-1004.
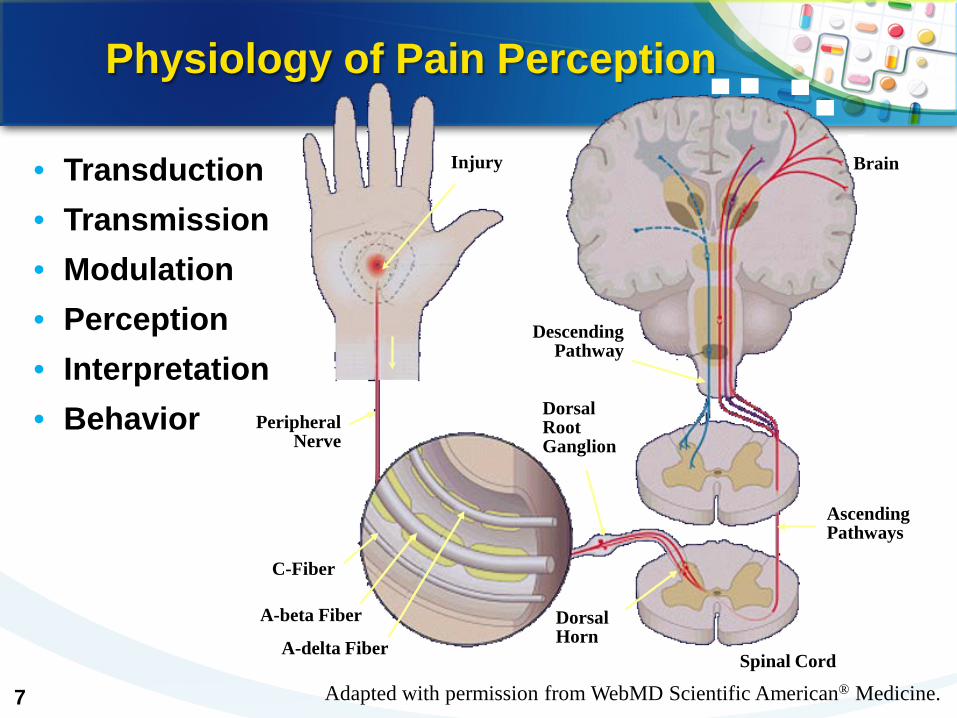
Physiology of Pain Perception
• Transduction • Transmission • Modulation • Perception • Interpretation • Behavior
Injury
Descending Pathway
Peripheral Nerve
Dorsal Root Ganglion
C-Fiber
A-beta Fiber
A-delta Fiber
Ascending Pathways
Dorsal Horn
Brain
Spinal Cord
Adapted with permission from WebMD Scientific American® Medicine.
7
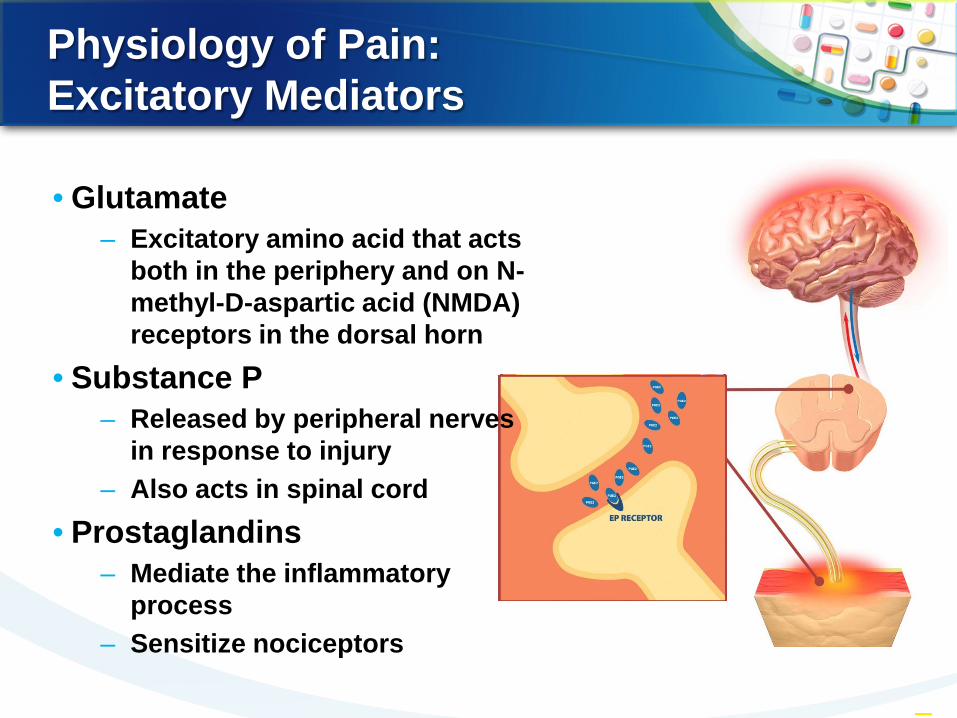
Physiology of Pain: Excitatory Mediators
–8
• Glutamate – Excitatory amino acid that acts
both in the periphery and on N-methyl-D-aspartic acid (NMDA) receptors in the dorsal horn
• Substance P – Released by peripheral nerves
in response to injury – Also acts in spinal cord
• Prostaglandins – Mediate the inflammatory
process – Sensitize nociceptors
UNIVERSITY OF PENNSYLVANIA HEALTH SYSTEM HEALTH SERVICES COMPONENT
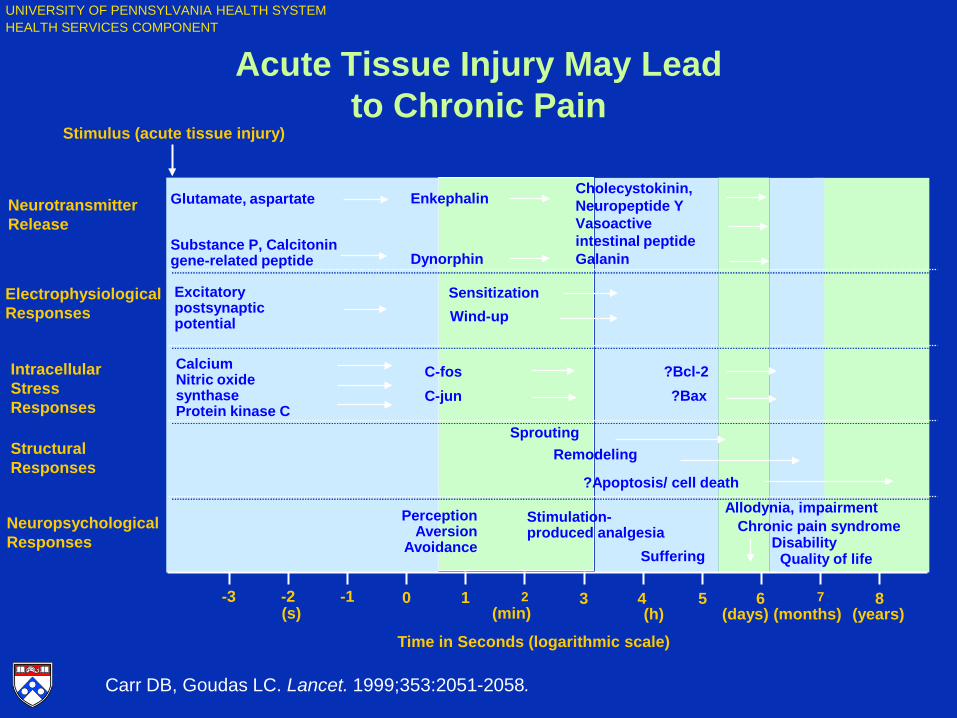
Carr DB, Goudas LC. Lancet. 1999;353:2051-2058.
-3 -2 -1 0 1 2 3 4 5 6 7 8
(s) (min) (h) (days) (months) (years)
Stimulus (acute tissue injury)
Neurotransmitter Release
Electrophysiological Responses
Intracellular Stress Responses
Structural Responses
Neuropsychological Responses
Time in Seconds (logarithmic scale)
Acute Tissue Injury May Lead to Chronic Pain
Quality of life Suffering
Glutamate, aspartate
Substance P, Calcitonin gene-related peptide
Enkephalin
Dynorphin
Cholecystokinin, Neuropeptide Y Vasoactive intestinal peptide Galanin
Excitatory postsynaptic potential
Sensitization Wind-up
Calcium Nitric oxide synthase Protein kinase C
C-fos C-jun
?Bcl-2 ?Bax
Sprouting Remodeling
?Apoptosis/ cell death
Perception
Aversion Avoidance
Stimulation-produced analgesia
Allodynia, impairment Chronic pain syndrome
Disability
UNIVERSITY OF PENNSYLVANIA HEALTH SYSTEM HEALTH SERVICES COMPONENT
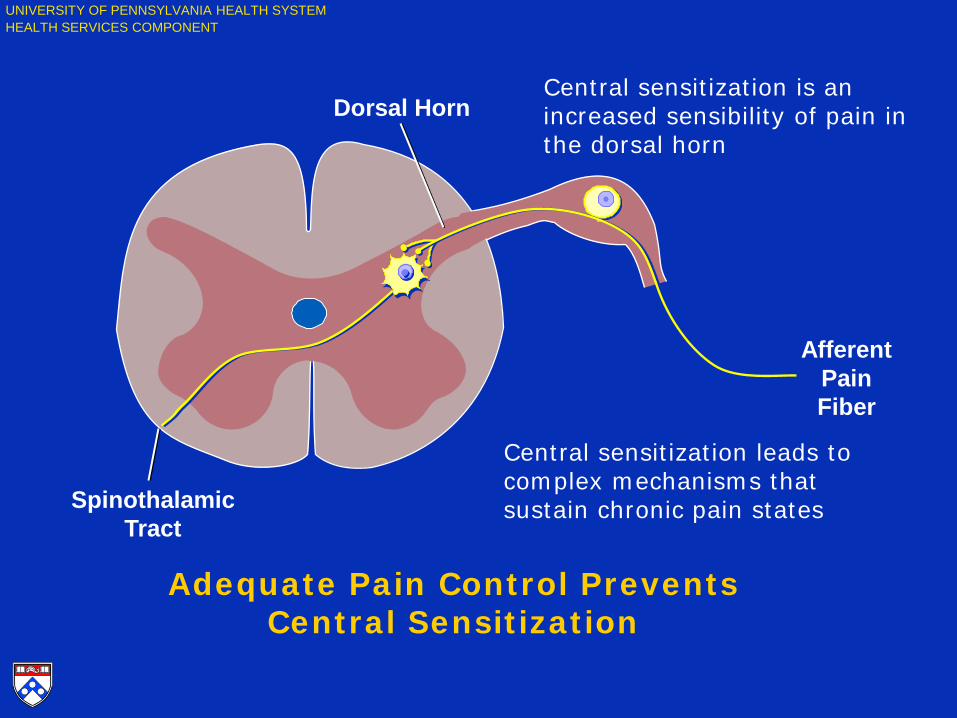
Dorsal Horn
Afferent Pain Fiber
Spinothalamic Tract
Adequate Pain Control Prevents Central Sensitization
Central sensitization is an increased sensibility of pain in the dorsal horn
Central sensitization leads to complex mechanisms that sustain chronic pain states
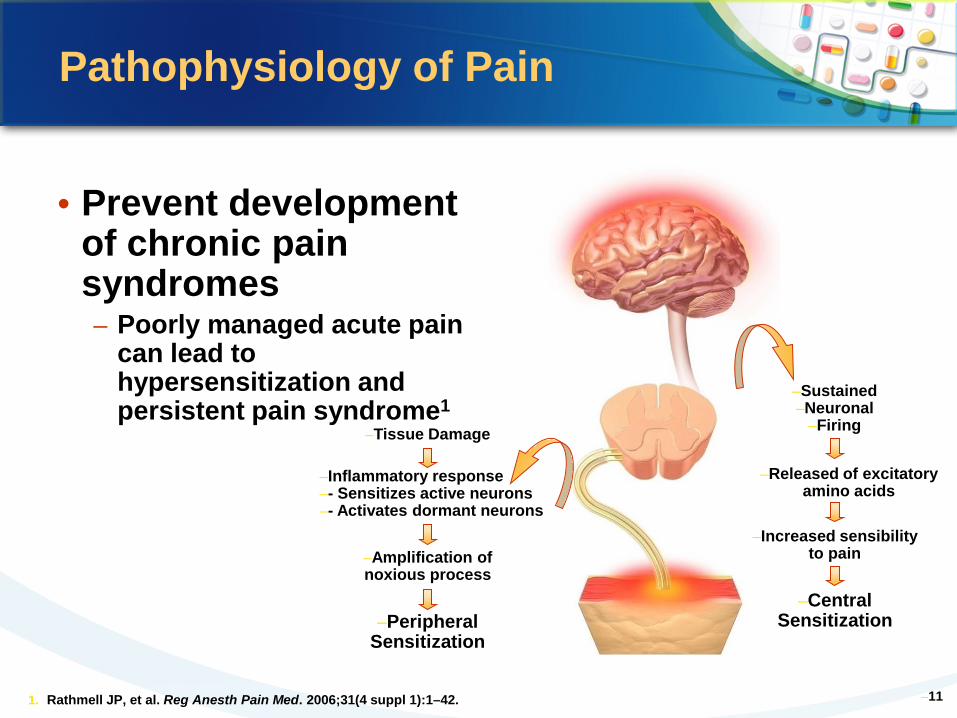
–11
–Tissue Damage
–Inflammatory response –- Sensitizes active neurons –- Activates dormant neurons
–Peripheral Sensitization
–Amplification of noxious process
–Released of excitatory amino acids
–Increased sensibility to pain
–Sustained –Neuronal
–Firing
–Central Sensitization
• Prevent development of chronic pain syndromes – Poorly managed acute pain
can lead to hypersensitization and persistent pain syndrome1
1. Rathmell JP, et al. Reg Anesth Pain Med. 2006;31(4 suppl 1):1–42.
Pathophysiology of Pain
Tailoring Analgesic Regimens: Adopting a Multimodal Strategy
• What is multimodal therapy? – Combines classes of drugs and techniques that target
more than 1 pain mechanism (eg, opioids plus NSAIDs) – Provides a way to reduce doses—and adverse effects—
of individual agents – Not a new concept, but one that is gaining increasing
attention as a therapeutic framework – Evidence-based approach incorporated into guidelines
• American Pain Society (APS)1
• American Society of Regional Anesthesia and Pain Medicine (ASRA)2
• American Society of Anesthesiologists (ASA)3
1. Gordon DB, et al. Arch Intern Med. 2005;165:1574-1580. 2. Rathmell JP, et al. Reg Anesth Pain Med. 2006;31(4 suppl 1):1-42. 3. American Society of Anesthesiologists Task Force on Acute Pain Management.
Anesthesiology. 2004;100:1573-1581.
Multimodal Therapy: Targeting Pain Throughout the Pathway
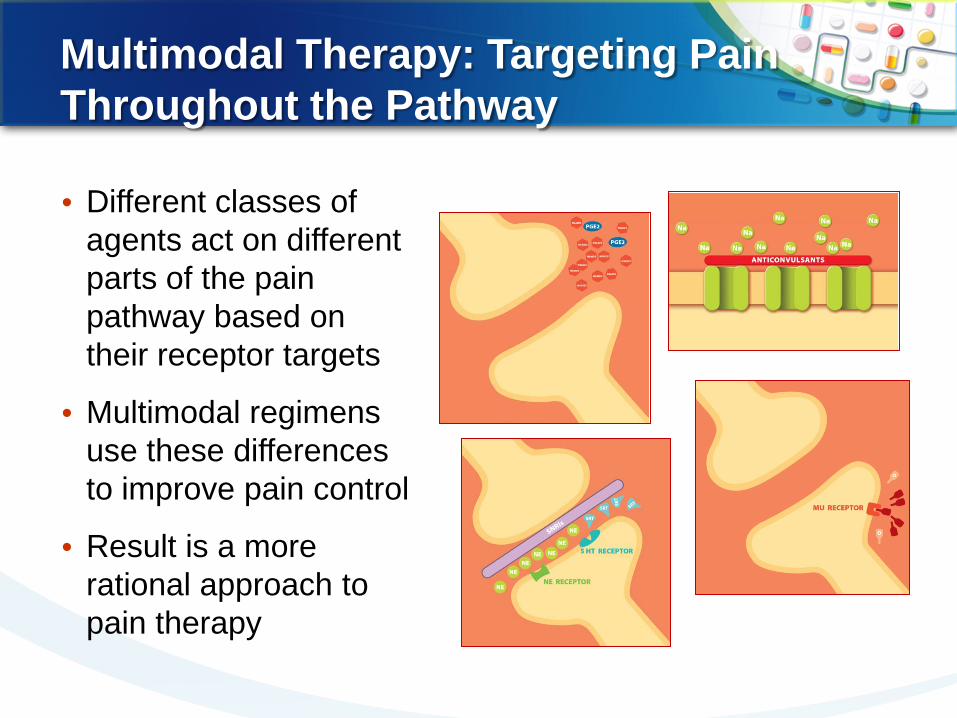
• Different classes of agents act on different parts of the pain pathway based on their receptor targets
• Multimodal regimens use these differences to improve pain control
• Result is a more rational approach to pain therapy
Multimodal Strategy: Combining Classes of Agents • Foundation of multimodal analgesia is the combination of 2
or more types of medications – Generally involves adding a second class of drug to an opioid
• NSAID blocks production of inflammatory mediators • Anticonvulsant inhibits propagation of pain impulses
• Significant clinical evidence shows that an opioid plus another class of agent better controls pain than opioids alone
– Addition of an NSAID reduced postoperative morphine use by as much as 50%, with an associated decrease in opioid-induced adverse effects and increase in patient satisfaction1-3
– Opioid plus gabapentin or pregabalin reduced opioid requirements, pain, and opioid-induced adverse effects4,5
1. Elia N, et al. Anesthesiology. 2005;103:1296-1304. 2. Stephens J, et al. Rheumatology. 2003;42(suppl
3):iii40-iii52. 3. Zemmel MH. AANA J. 2006;74:49-60.
4. Tiippana EM, et al. Anesth Analg. 2007;104:1545-1556.
5. Mathiesen O, et al. BMC Anesthesiol. 2007;7:6.
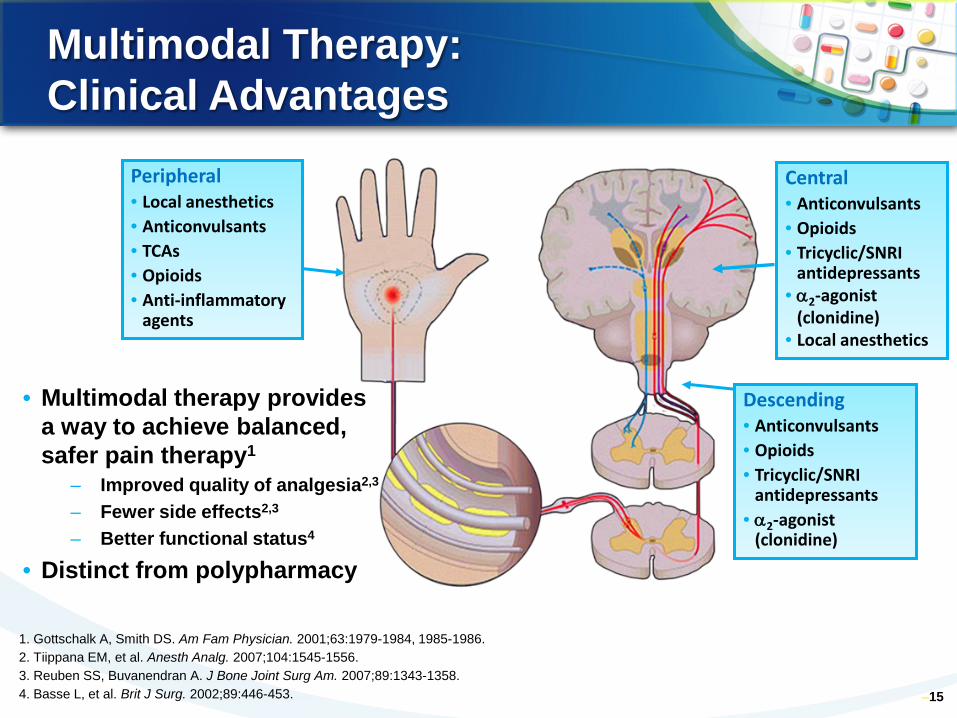
Multimodal Therapy: Clinical Advantages
• Multimodal therapy provides a way to achieve balanced, safer pain therapy1
– Improved quality of analgesia2,3
– Fewer side effects2,3
– Better functional status4
• Distinct from polypharmacy
–15
Central • Anticonvulsants • Opioids • Tricyclic/SNRI
antidepressants • α2-agonist
(clonidine) • Local anesthetics
Peripheral • Local anesthetics • Anticonvulsants • TCAs • Opioids • Anti-inflammatory
agents
Descending • Anticonvulsants • Opioids • Tricyclic/SNRI
antidepressants • α2-agonist
(clonidine)
1. Gottschalk A, Smith DS. Am Fam Physician. 2001;63:1979-1984, 1985-1986. 2. Tiippana EM, et al. Anesth Analg. 2007;104:1545-1556. 3. Reuben SS, Buvanendran A. J Bone Joint Surg Am. 2007;89:1343-1358. 4. Basse L, et al. Brit J Surg. 2002;89:446-453.
BRAIN
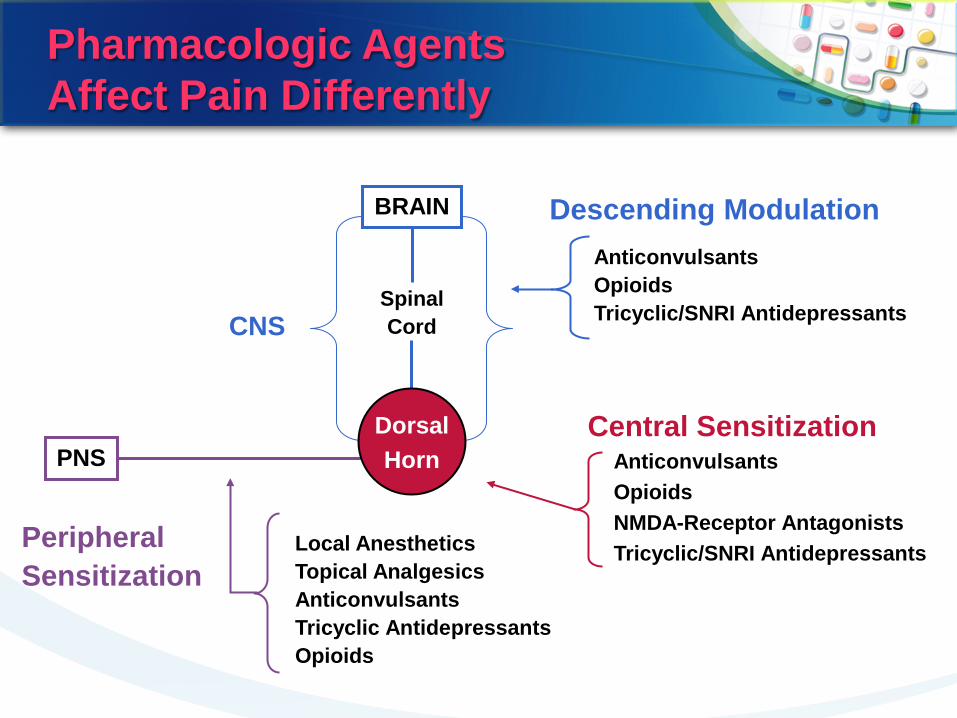
Pharmacologic Agents Affect Pain Differently
Descending Modulation
Central Sensitization PNS
Local Anesthetics Topical Analgesics Anticonvulsants Tricyclic Antidepressants Opioids
Anticonvulsants Opioids NMDA-Receptor Antagonists Tricyclic/SNRI Antidepressants
Anticonvulsants Opioids Tricyclic/SNRI Antidepressants CNS
Spinal Cord
Peripheral Sensitization
Dorsal Horn
17
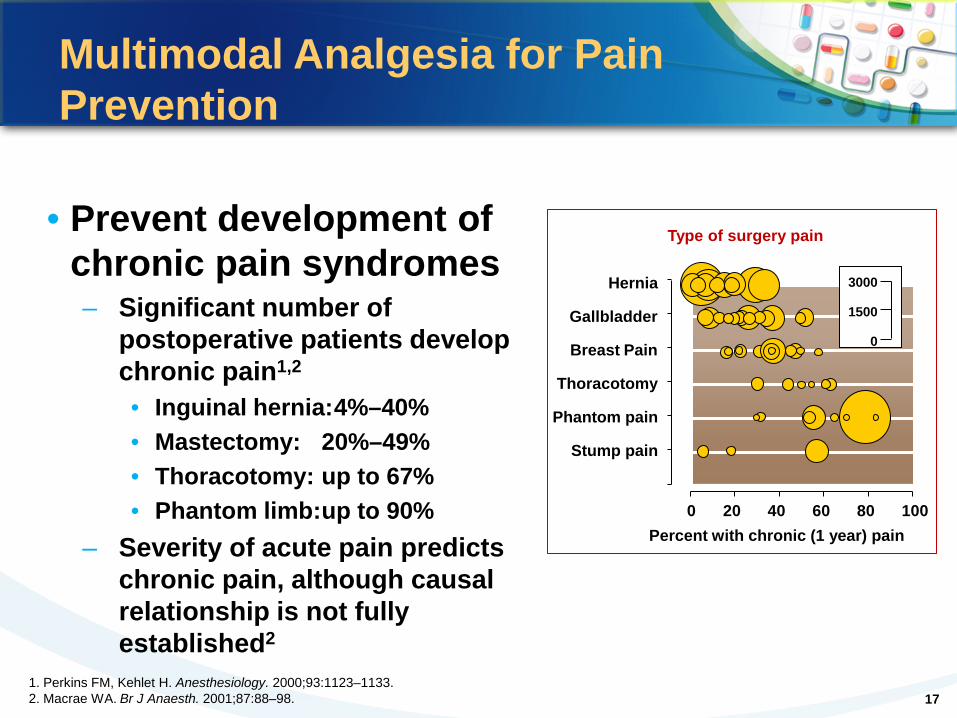
• Prevent development of chronic pain syndromes
– Significant number of postoperative patients develop chronic pain1,2
• Inguinal hernia: 4%–40% • Mastectomy: 20%–49% • Thoracotomy: up to 67% • Phantom limb: up to 90%
– Severity of acute pain predicts chronic pain, although causal relationship is not fully established2
1. Perkins FM, Kehlet H. Anesthesiology. 2000;93:1123–1133. 2. Macrae WA. Br J Anaesth. 2001;87:88–98.
Multimodal Analgesia for Pain Prevention
3000
1500
0
Hernia
Gallbladder
Breast Pain
Thoracotomy
Phantom pain
Stump pain
0 20 40 60 80 100 Percent with chronic (1 year) pain
Type of surgery pain
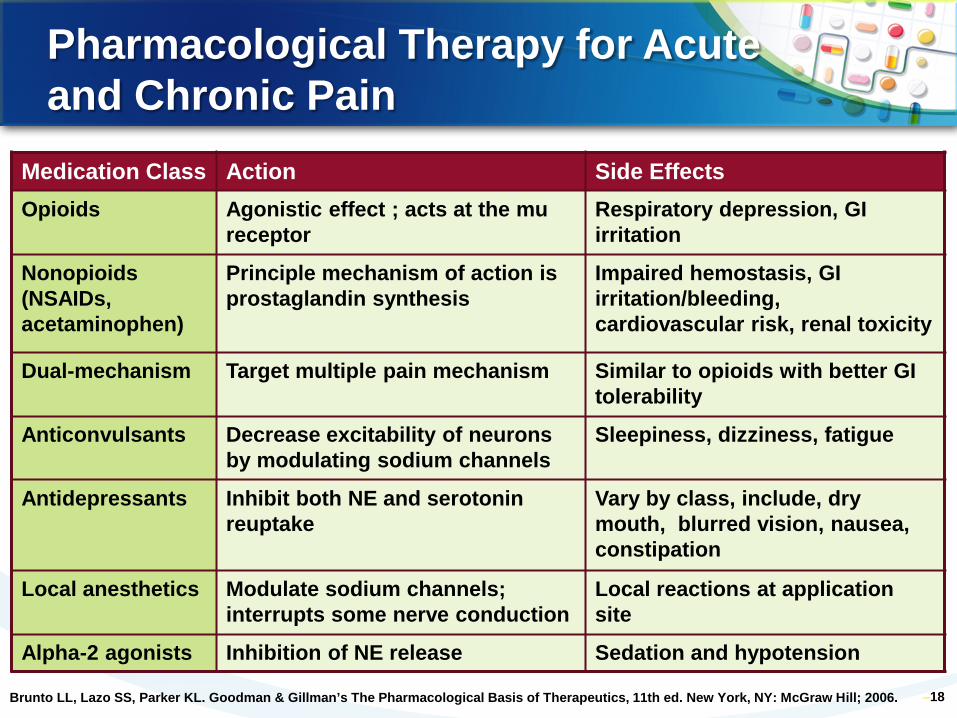
Pharmacological Therapy for Acute and Chronic Pain
–18
Medication Class Action Side Effects Opioids Agonistic effect ; acts at the mu
receptor Respiratory depression, GI irritation
Nonopioids (NSAIDs, acetaminophen)
Principle mechanism of action is prostaglandin synthesis
Impaired hemostasis, GI irritation/bleeding, cardiovascular risk, renal toxicity
Dual-mechanism Target multiple pain mechanism Similar to opioids with better GI tolerability
Anticonvulsants Decrease excitability of neurons by modulating sodium channels
Sleepiness, dizziness, fatigue
Antidepressants Inhibit both NE and serotonin reuptake
Vary by class, include, dry mouth, blurred vision, nausea, constipation
Local anesthetics Modulate sodium channels; interrupts some nerve conduction
Local reactions at application site
Alpha-2 agonists Inhibition of NE release Sedation and hypotension
Brunto LL, Lazo SS, Parker KL. Goodman & Gillman’s The Pharmacological Basis of Therapeutics, 11th ed. New York, NY: McGraw Hill; 2006.
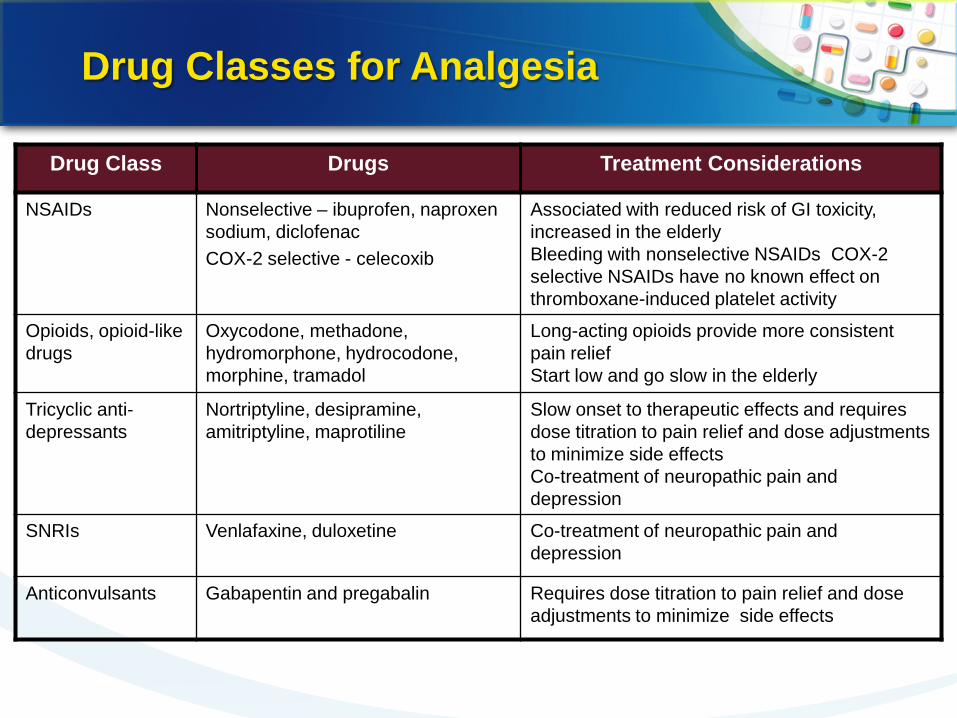
Drug Classes for Analgesia
Drug Class Drugs Treatment Considerations
NSAIDs Nonselective – ibuprofen, naproxen sodium, diclofenac COX-2 selective - celecoxib
Associated with reduced risk of GI toxicity, increased in the elderly Bleeding with nonselective NSAIDs COX-2 selective NSAIDs have no known effect on thromboxane-induced platelet activity
Opioids, opioid-like drugs
Oxycodone, methadone, hydromorphone, hydrocodone, morphine, tramadol
Long-acting opioids provide more consistent pain relief Start low and go slow in the elderly
Tricyclic anti-depressants
Nortriptyline, desipramine, amitriptyline, maprotiline
Slow onset to therapeutic effects and requires dose titration to pain relief and dose adjustments to minimize side effects Co-treatment of neuropathic pain and depression
SNRIs Venlafaxine, duloxetine Co-treatment of neuropathic pain and depression
Anticonvulsants Gabapentin and pregabalin Requires dose titration to pain relief and dose adjustments to minimize side effects
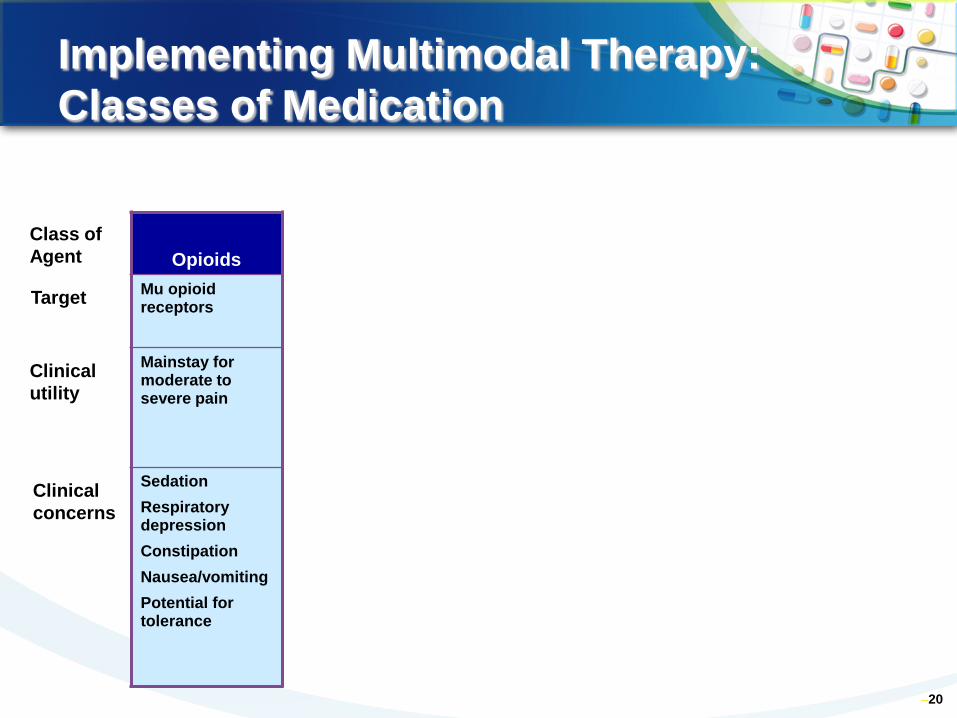
Implementing Multimodal Therapy: Classes of Medication
–20
Class of Agent
Clinical concerns
Clinical utility
Target
Opioids Mu opioid receptors
Mainstay for moderate to severe pain
Sedation Respiratory depression Constipation Nausea/vomiting Potential for tolerance
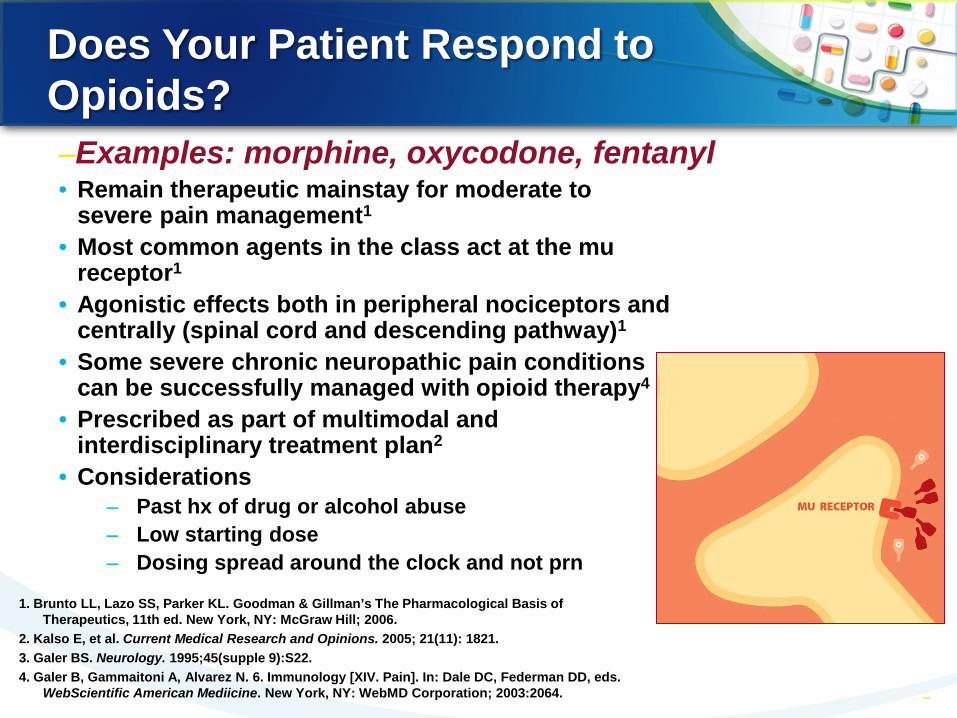
Does Your Patient Respond to Opioids?
• Remain therapeutic mainstay for moderate to severe pain management1
• Most common agents in the class act at the mu receptor1
• Agonistic effects both in peripheral nociceptors and centrally (spinal cord and descending pathway)1
• Some severe chronic neuropathic pain conditions can be successfully managed with opioid therapy4
• Prescribed as part of multimodal and interdisciplinary treatment plan2
• Considerations – Past hx of drug or alcohol abuse – Low starting dose – Dosing spread around the clock and not prn
–21 –21
–Examples: morphine, oxycodone, fentanyl
1. Brunto LL, Lazo SS, Parker KL. Goodman & Gillman’s The Pharmacological Basis of Therapeutics, 11th ed. New York, NY: McGraw Hill; 2006.
2. Kalso E, et al. Current Medical Research and Opinions. 2005; 21(11): 1821. 3. Galer BS. Neurology. 1995;45(supple 9):S22. 4. Galer B, Gammaitoni A, Alvarez N. 6. Immunology [XIV. Pain]. In: Dale DC, Federman DD, eds.
WebScientific American Mediicine. New York, NY: WebMD Corporation; 2003:2064.
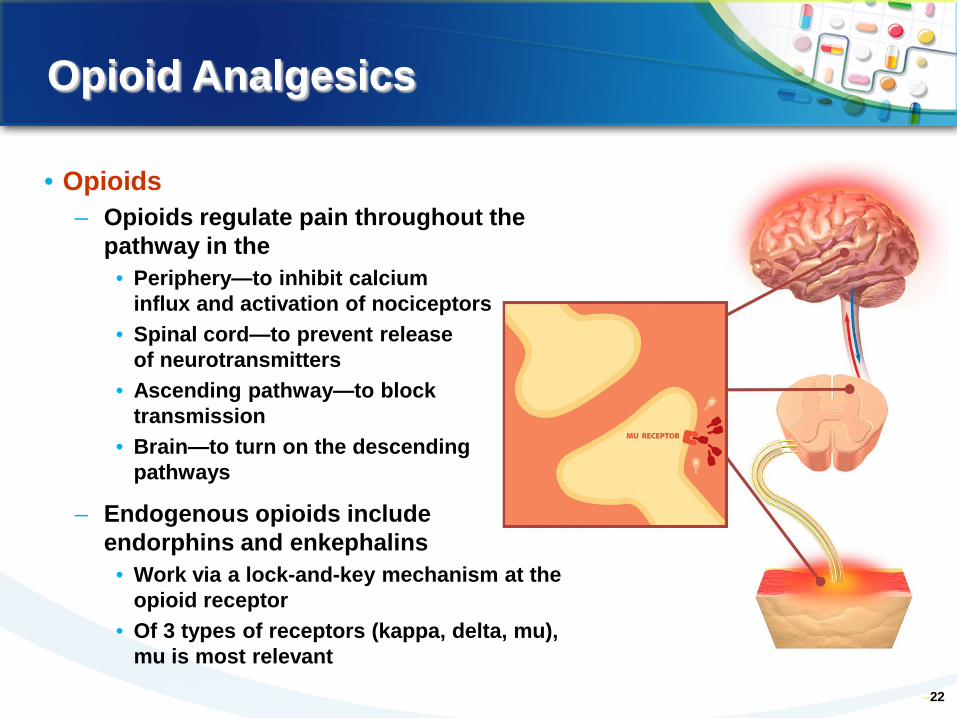
Opioid Analgesics
–22
• Opioids – Opioids regulate pain throughout the
pathway in the • Periphery—to inhibit calcium
influx and activation of nociceptors • Spinal cord—to prevent release
of neurotransmitters • Ascending pathway—to block
transmission • Brain—to turn on the descending
pathways
– Endogenous opioids include endorphins and enkephalins
• Work via a lock-and-key mechanism at the opioid receptor
• Of 3 types of receptors (kappa, delta, mu), mu is most relevant
–Characteristics of Immediate- and Controlled-Release Opioids
– Immediate-release opioids – Quick onset of action (within
minutes) – May be more appropriate for
some types of acute pain and some types of BTP
– Can be used for dose finding during initial treatment
– Inconvenient repetitive dosing – Peak and trough phenomenon
– Not ideal for chronic pain – Increased end-of-dose
breakthrough pain – Increased potential for
euphoria and adverse effects (peaks)
Controlled-release opioids – More stable blood levels – More appropriate for
persistent acute pain and chronic pain because avoids peaks and troughs
– Reduced end-of-dose breakthrough pain
– Lower potential for euphoria (due to fewer peaks) when taken as prescribed
– Decreased risk for side effects (fewer peaks)
– Improved compliance and quality of life
McCarberg BH, Barkin Rl. Amer J Ther. 2001;8:181-186.
When you Need Mechanism of Different Action: Methadone and
Ketamine
Methadone, Just Another Opioid?
• Synthetic opioid • Indicated for detoxification and treatment of opioid addiction
• Increasingly used for treatment of moderate to severe pain
• Mu-opioid receptor agonist (kappa and delta) • NMDA-receptor antagonist • Inhibits reuptake of norepinephrine and serotonin • At high doses, blocks potassium channels • Cost-effective
Pharmacokinetics • Rapidly absorbed by the GI tract • Quick onset of action 30 -60 minutes (PO),
steady state in 3-5 days; 10-20 minutes (IV), peaks in 2.5-4 hr
• Lipophilic – Analgesic efficacy 6-12 hours – Elimination half-life 24-36 hours
• Long and highly variable (range 5-130 hours) • Eliminated through feces and produces
nontoxic metabolites with minor activity – Preferred in renal insufficiency**
– Takes 4days to reach steady state
Breakthrough Pain: Definition Problems
• Definition is by consensus and has arbitrary quality
• Basis for definition is an acute, transitory pain over controlled baseline pain
• But what definitions should apply? – Timing – Severity – Population – Treatment of baseline pain
27
Breakthrough Pain: Definition Problems
• Most stringent definition – In the cancer population, breakthrough pain is a
transitory, severe, or excruciating pain, which lasts seconds to hours and is superimposed on a baseline pain controlled to a moderate or better intensity by an opioid regimen
• Very broad definition – Any severe, transient pain with intensity
exceeding baseline
–Mercadante S, et al. Cancer. 2002;94:832-839. –Svendsen KB, et al. Eur J Pain. 2005;9:195-206.
28
Breakthrough Pain: Definition Problems
• Definitional imprecision increased by use of alternative terms
– Episodic pain – Incident pain – End-of-dose failure
• Incident pain also considered a subtype of breakthrough pain associated with a voluntary action
• End-of-dose failure not considered to be breakthrough pain by some
29
–Mercadante S, et al. Cancer. 2002;94:832-839. –Svendsen KB, et al. Eur J Pain. 2005;9:195-206.
Breakthrough Pain: Characteristics
• Phenomenology usually similar to baseline pain, but large inter-individual differences
• Frequency: <1 episode/day to many per hour • Most episodes brief, but may last hours • Onset usually over minutes, but varies • 50% associated with volitional action (some nonvolitional)
• May be predictable or appear without warning • May appear or worsen at end-of-dosing interval (“end-of-dose failure”)
–Mercadante S, et al. Cancer. 2002;94:832-839; Caraceni A, et al. Palliat Med. 2004;18:177-183; Portenoy RK, Hagen NA. Pain. 1990;41:273-281
30
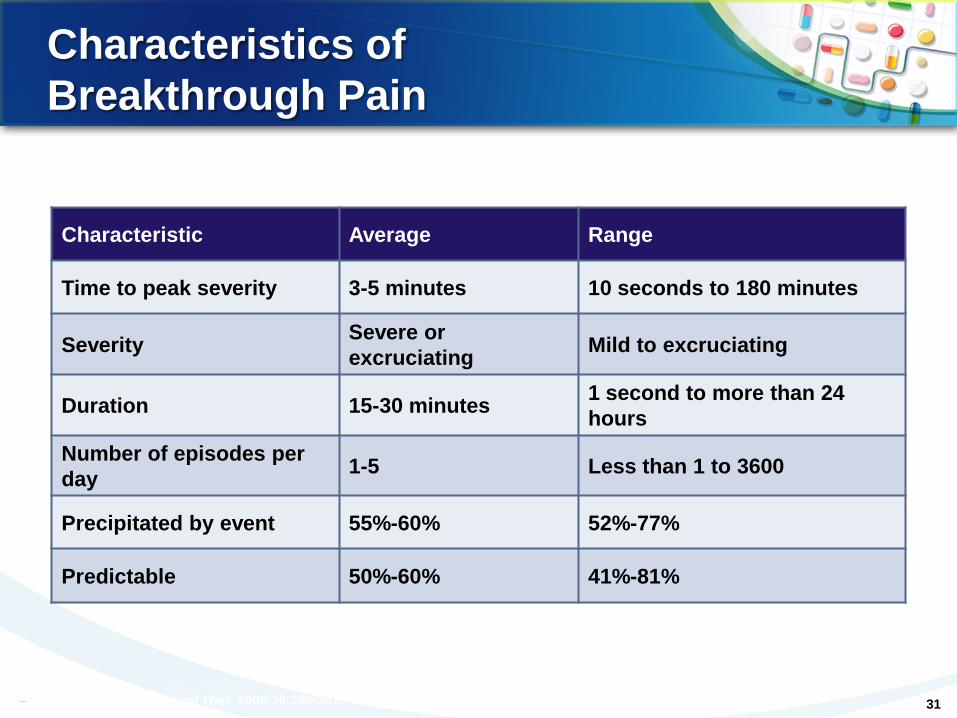
Characteristics of Breakthrough Pain
Characteristic Average Range
Time to peak severity 3-5 minutes 10 seconds to 180 minutes
Severity Severe or excruciating Mild to excruciating
Duration 15-30 minutes 1 second to more than 24 hours
Number of episodes per day 1-5 Less than 1 to 3600
Precipitated by event 55%-60% 52%-77%
Predictable 50%-60% 41%-81%
–Bennett D, et al. Pharmacol Ther. 2005;30:296-301. 31
UNIVERSITY OF PENNSYLVANIA HEALTH SYSTEM HEALTH SERVICES COMPONENT
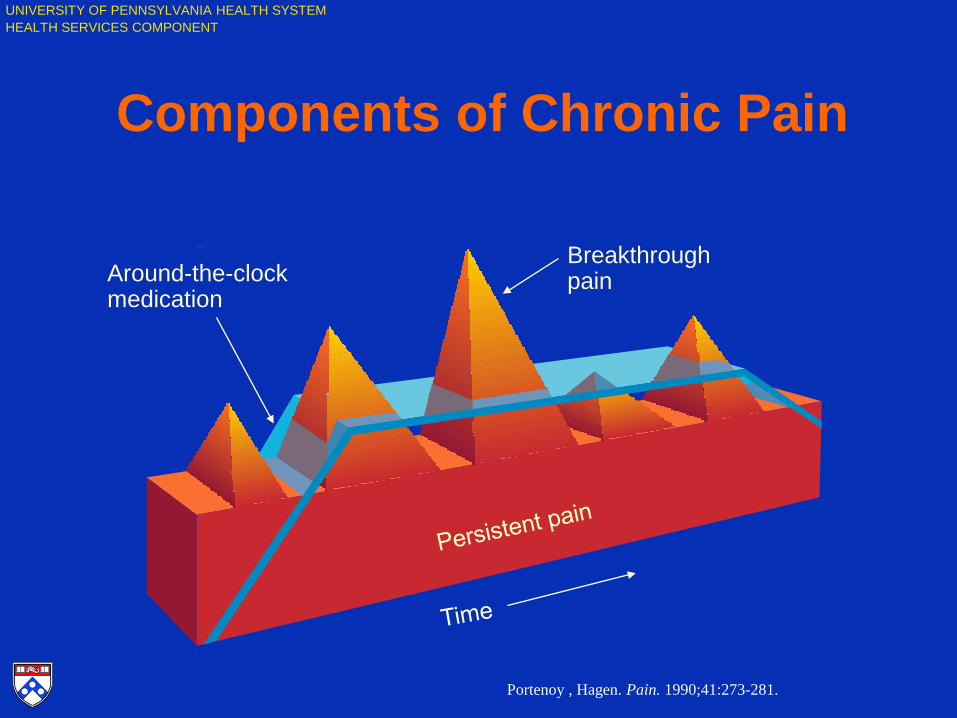
Components of Chronic Pain
Around-the-clock medication
Breakthrough pain
Portenoy , Hagen. Pain. 1990;41:273-281.
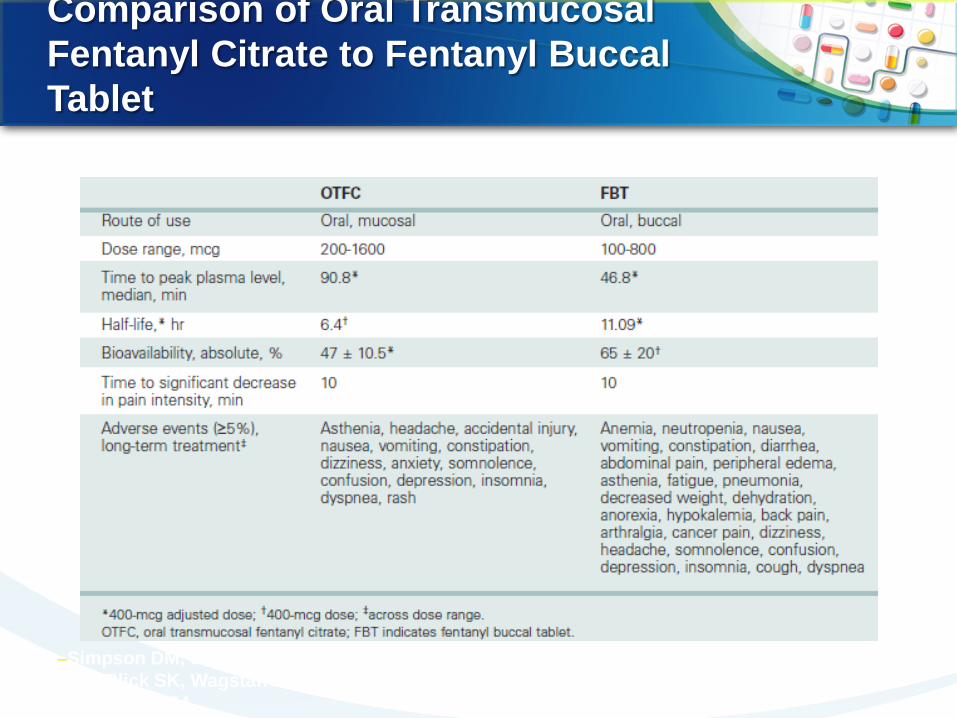
Comparison of Oral Transmucosal Fentanyl Citrate to Fentanyl Buccal Tablet
–Simpson DM, et al. Clin Ther. 2007;29:588-601.; Portenoy RK, et al. Curr Med Res Opin. 2007;23:223-233.; Blick SK, Wagstaff AJ. Drugs. 2006;66:2387-2395.; Slatkin NE, et al. J Support Oncol. 2007;5:327-334.
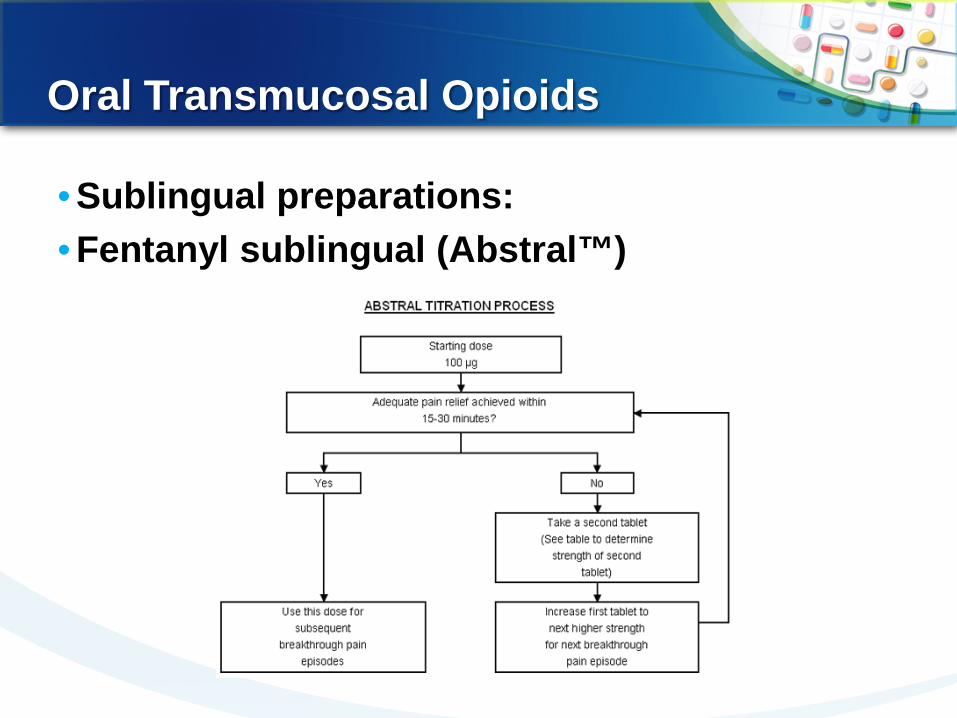
Oral Transmucosal Opioids
• Sublingual preparations: • Fentanyl sublingual (Abstral™)
Intranasal Opioids
• Intranasal fentanyl spray (Instanyl™)
• Fentanyl nasal spray (PecFent™)
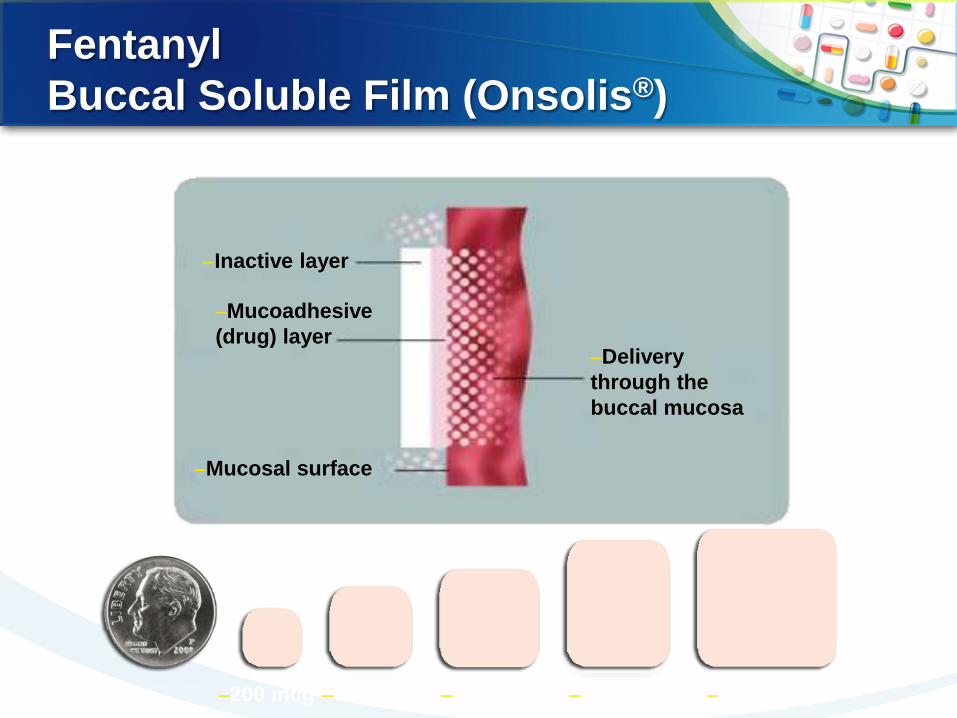
Fentanyl Buccal Soluble Film (Onsolis®)
–200 mcg –400 mcg –600 mcg –800 mcg –1200 mcg
–Inactive layer
–Mucoadhesive (drug) layer
–Mucosal surface
–Delivery through the buccal mucosa
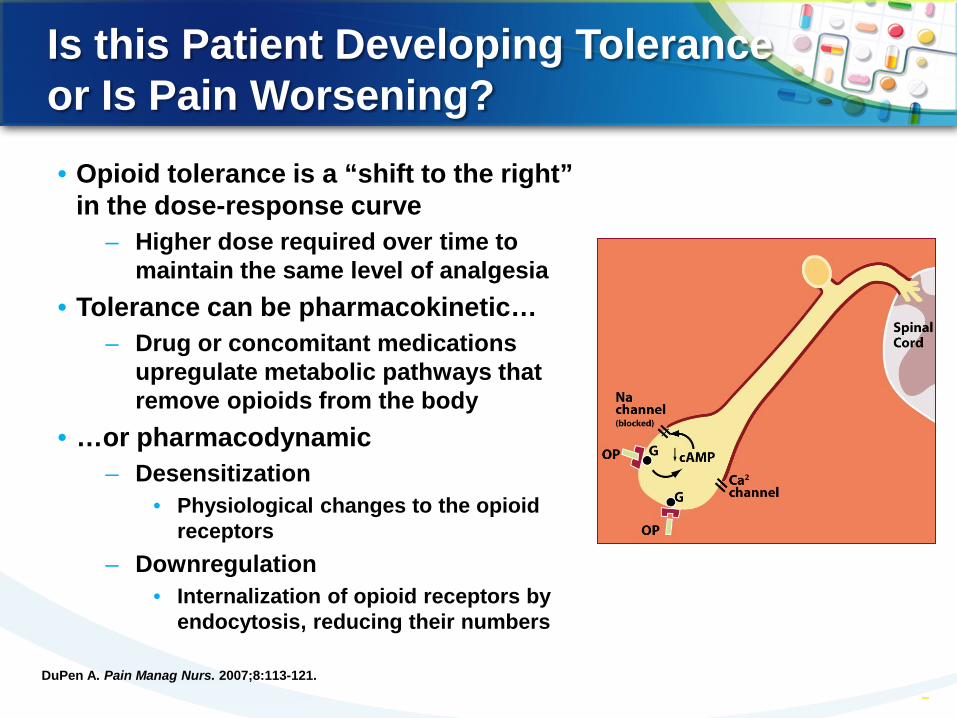
Is this Patient Developing Tolerance or Is Pain Worsening? • Opioid tolerance is a “shift to the right”
in the dose-response curve – Higher dose required over time to
maintain the same level of analgesia • Tolerance can be pharmacokinetic…
– Drug or concomitant medications upregulate metabolic pathways that remove opioids from the body
• …or pharmacodynamic – Desensitization
• Physiological changes to the opioid receptors
– Downregulation • Internalization of opioid receptors by
endocytosis, reducing their numbers
–37 –37 DuPen A. Pain Manag Nurs. 2007;8:113-121.
Could Your Patient have Opioid-induced Hyperalgesia (OIH)?
• Increased sensitivity to pain resulting from opiate administration
• Opioids, in addition to providing analgesia, set in motion anti-analgesic or hyperalgesic processes
• Pain-free animals made tolerant to morphine have significantly decreased tolerance to pain1
• Opioid “tolerance” may not be a downregulation of analgesic systems, but an upregulation of hyperalgesic systems2
–38
1. Compton MA. Pain Symptom Manage. 1994; 9:462-473. 2. Laulin JP, et al. Neuroscience. 1999;89:631-636.
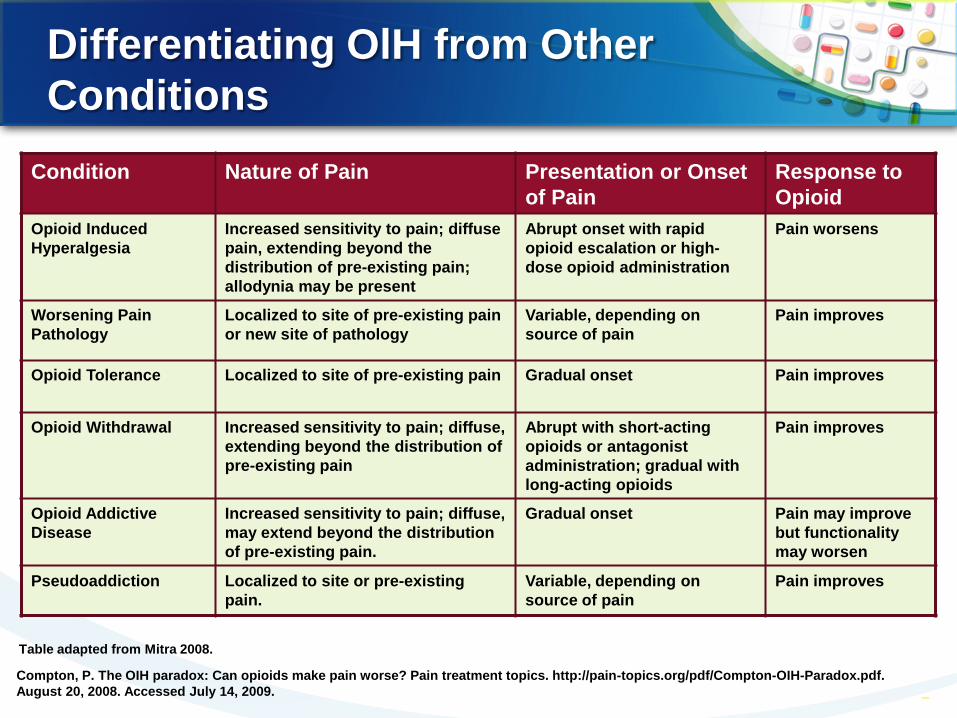
Differentiating OlH from Other Conditions
–39
Condition Nature of Pain Presentation or Onset of Pain
Response to Opioid
Opioid Induced Hyperalgesia
Increased sensitivity to pain; diffuse pain, extending beyond the distribution of pre-existing pain; allodynia may be present
Abrupt onset with rapid opioid escalation or high-dose opioid administration
Pain worsens
Worsening Pain Pathology
Localized to site of pre-existing pain or new site of pathology
Variable, depending on source of pain
Pain improves
Opioid Tolerance Localized to site of pre-existing pain Gradual onset Pain improves
Opioid Withdrawal Increased sensitivity to pain; diffuse, extending beyond the distribution of pre-existing pain
Abrupt with short-acting opioids or antagonist administration; gradual with long-acting opioids
Pain improves
Opioid Addictive Disease
Increased sensitivity to pain; diffuse, may extend beyond the distribution of pre-existing pain.
Gradual onset Pain may improve but functionality may worsen
Pseudoaddiction Localized to site or pre-existing pain.
Variable, depending on source of pain
Pain improves
Table adapted from Mitra 2008.
Compton, P. The OIH paradox: Can opioids make pain worse? Pain treatment topics. http://pain-topics.org/pdf/Compton-OIH-Paradox.pdf. August 20, 2008. Accessed July 14, 2009.
Moving to a Multimodal Strategy: Dual-mechanism Analgesics
• A single medication with dual mechanisms of action
– First in class: tramadol • Newest dual-mechanism agent is tapentadol
– Acts on mu opioid receptors and inhibits reuptake of NE1 – Clinical trial experience
• Comparable to oxycodone in acute pain (bunionectomy)2 and in more chronic pain (up to 90 days in joint or back pain)3
• Comparable or better pain relief than morphine in dental surgery4
• Main side effects similar to conventional opioids (GI, CNS), but significantly better GI profile, including lower rate of constipation3,5
– May be associated with less tolerance1 – May be useful in patients with opioid sensitivity
–40
1. Tzschentke TM et al. Drugs Future. 2006;31:1053-1061. 2. Oh C, et al. Presented at: American Pain Society’s 27th Annual Scientific
Meeting. 2008.Abstract 229. 3. Oh C, et al. Presented at: American Pain Society’s 27th Annual Scientific
Meeting. 2008. Abstract 226.
4. Kleinert R, et al. J Pain. 2006;7(4 suppl 2):S44 Abstract 773. 5. Hartrick C, et al. Presented at: American Pain Society’s 27th Annual
Scientific Meeting. 2008. Abstract 222.
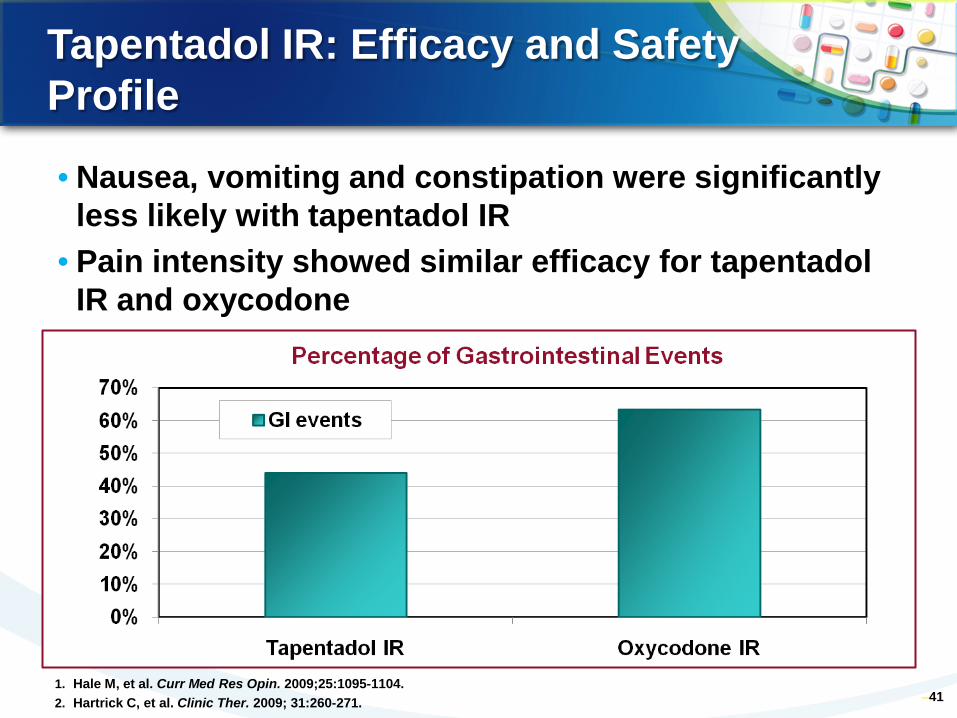
Tapentadol IR: Efficacy and Safety Profile
• Nausea, vomiting and constipation were significantly less likely with tapentadol IR
• Pain intensity showed similar efficacy for tapentadol IR and oxycodone
–41 1. Hale M, et al. Curr Med Res Opin. 2009;25:1095-1104. 2. Hartrick C, et al. Clinic Ther. 2009; 31:260-271.
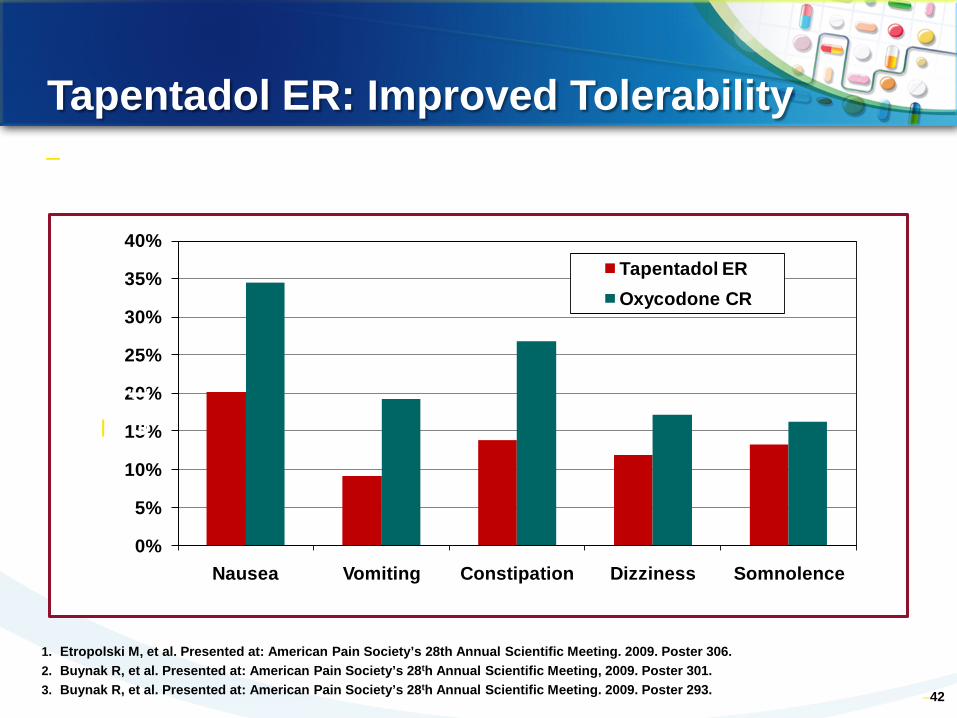
Tapentadol ER: Improved Tolerability
–42
0%
5%
10%
15%
20%
25%
30%
35%
40%
Nausea Vomiting Constipation Dizziness Somnolence
Tapentadol EROxycodone CR
–Incidences of Treatment Emergent Events for Tapentadol ER and Oxycodone CR
1. Etropolski M, et al. Presented at: American Pain Society’s 28th Annual Scientific Meeting. 2009. Poster 306. 2. Buynak R, et al. Presented at: American Pain Society’s 28th Annual Scientific Meeting, 2009. Poster 301. 3. Buynak R, et al. Presented at: American Pain Society’s 28th Annual Scientific Meeting. 2009. Poster 293.
–Pat
ien
ts
–43
Class of Agent
Clinical concerns
Clinical utility
Target
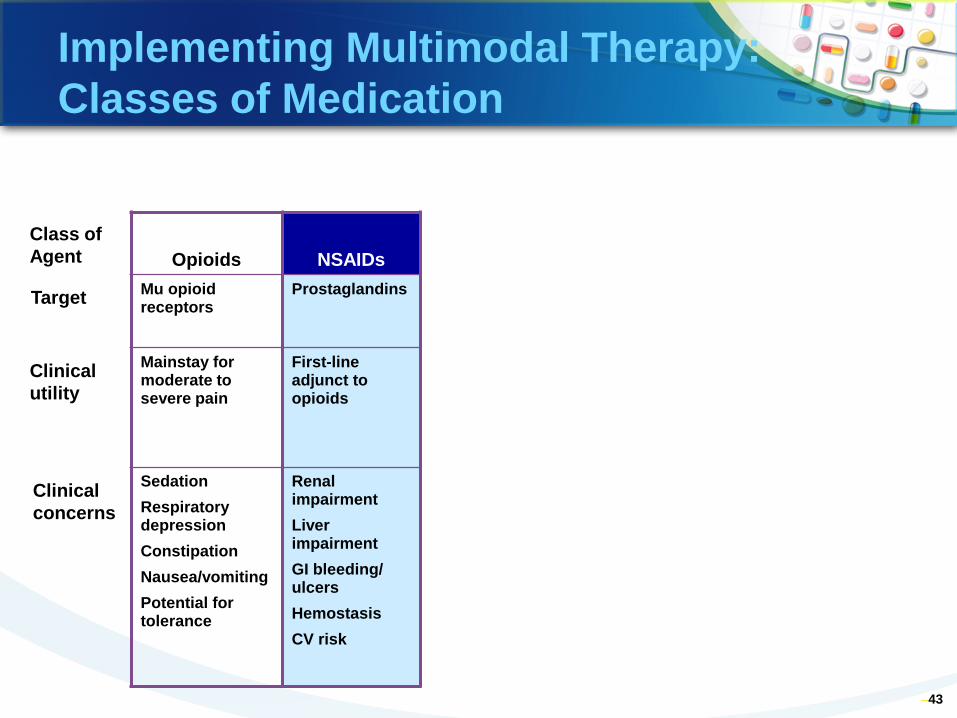
Implementing Multimodal Therapy: Classes of Medication
Opioids NSAIDs Mu opioid receptors
Prostaglandins
Mainstay for moderate to severe pain
First-line adjunct to opioids
Sedation Respiratory depression Constipation Nausea/vomiting Potential for tolerance
Renal impairment Liver impairment GI bleeding/ ulcers Hemostasis CV risk
Classes of Pain Medications: Nonopioids
• Nonsteroidal anti-inflammatory drugs (NSAIDS) – Examples: celecoxib, ketorolac – Anti-inflammatory and analgesic effects – Principal mechanism of action: inhibition of
prostaglandin synthesis – Activity at peripheral nociceptors and in spinal
cord – Side effects due in part to selectivity for
cyclooxygenase-2 • Impaired hemostasis (nonselective) • GI irritation/bleeding (nonselective) • Cardiovascular risk • Renal toxicity
• Acetaminophen – Analgesic but not anti-inflammatory – Less potent than NSAIDs – Lacks adverse effects of NSAIDs – Hepatotoxic in overdose
–44
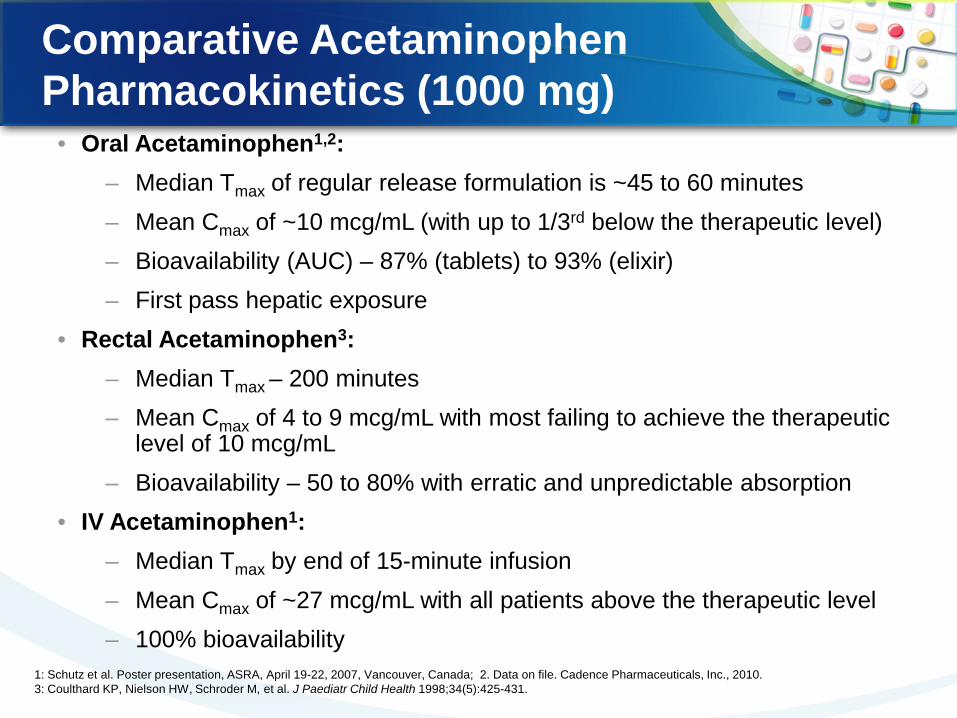
• Oral Acetaminophen1,2: – Median Tmax of regular release formulation is ~45 to 60 minutes – Mean Cmax of ~10 mcg/mL (with up to 1/3rd below the therapeutic level) – Bioavailability (AUC) – 87% (tablets) to 93% (elixir) – First pass hepatic exposure
• Rectal Acetaminophen3: – Median Tmax – 200 minutes – Mean Cmax of 4 to 9 mcg/mL with most failing to achieve the therapeutic
level of 10 mcg/mL – Bioavailability – 50 to 80% with erratic and unpredictable absorption
• IV Acetaminophen1: – Median Tmax by end of 15-minute infusion – Mean Cmax of ~27 mcg/mL with all patients above the therapeutic level – 100% bioavailability
Comparative Acetaminophen Pharmacokinetics (1000 mg)
1: Schutz et al. Poster presentation, ASRA, April 19-22, 2007, Vancouver, Canada; 2. Data on file. Cadence Pharmaceuticals, Inc., 2010. 3: Coulthard KP, Nielson HW, Schroder M, et al. J Paediatr Child Health 1998;34(5):425-431.
–46
Class of Agent
Clinical concerns
Clinical utility
Target
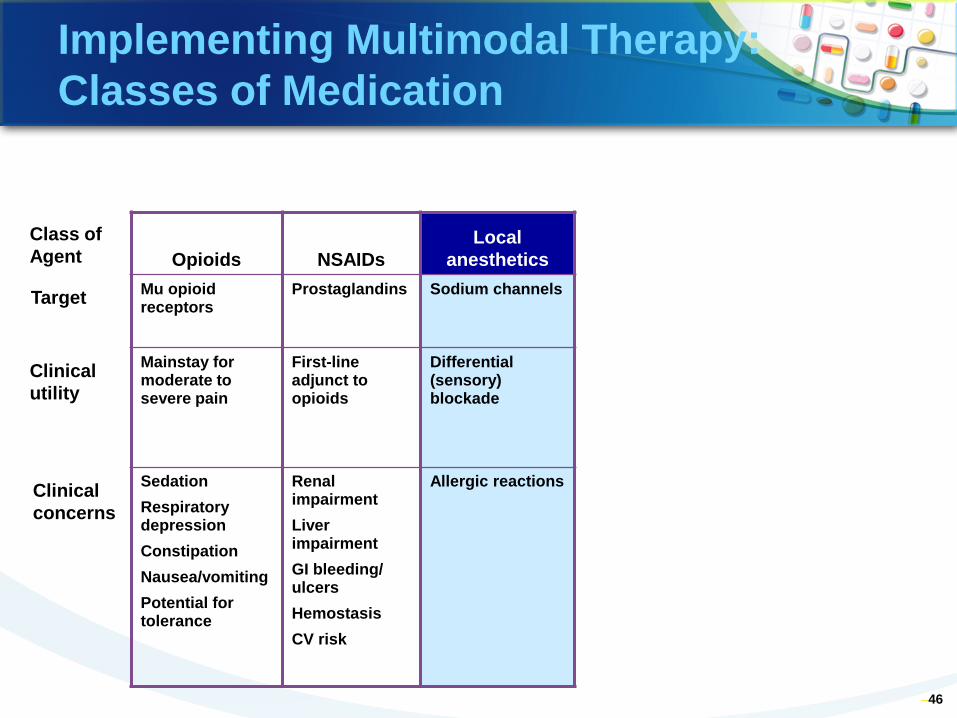
Implementing Multimodal Therapy: Classes of Medication
Opioids NSAIDs Local
anesthetics Mu opioid receptors
Prostaglandins Sodium channels
Mainstay for moderate to severe pain
First-line adjunct to opioids
Differential (sensory) blockade
Sedation Respiratory depression Constipation Nausea/vomiting Potential for tolerance
Renal impairment Liver impairment GI bleeding/ ulcers Hemostasis CV risk
Allergic reactions
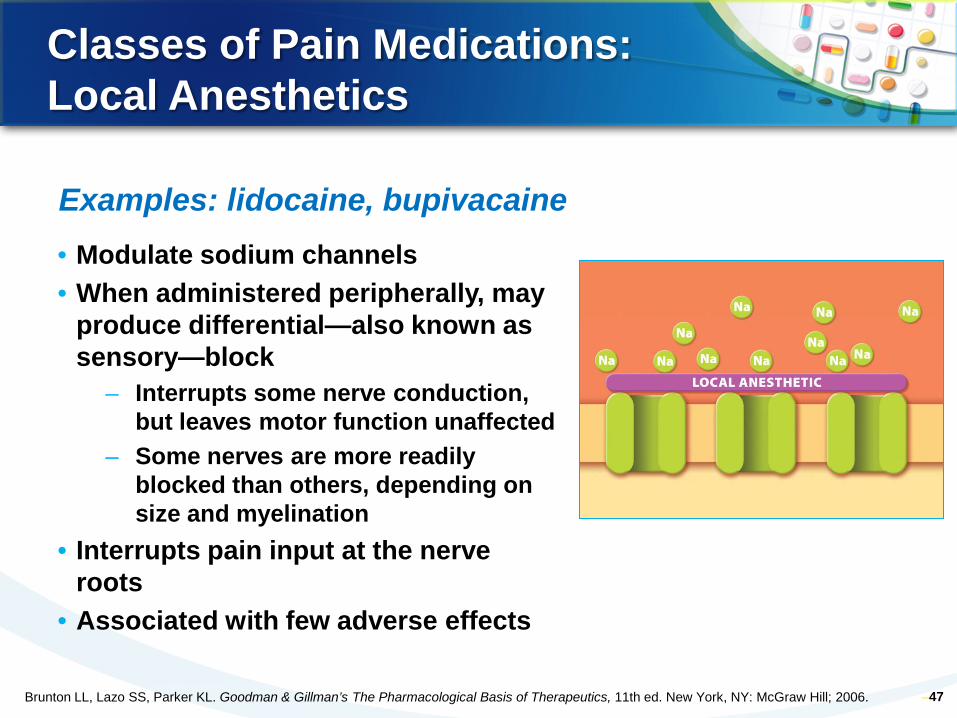
Classes of Pain Medications: Local Anesthetics
• Modulate sodium channels • When administered peripherally, may
produce differential—also known as sensory—block
– Interrupts some nerve conduction, but leaves motor function unaffected
– Some nerves are more readily blocked than others, depending on size and myelination
• Interrupts pain input at the nerve roots
• Associated with few adverse effects
–47
Examples: lidocaine, bupivacaine
Brunton LL, Lazo SS, Parker KL. Goodman & Gillman’s The Pharmacological Basis of Therapeutics, 11th ed. New York, NY: McGraw Hill; 2006.
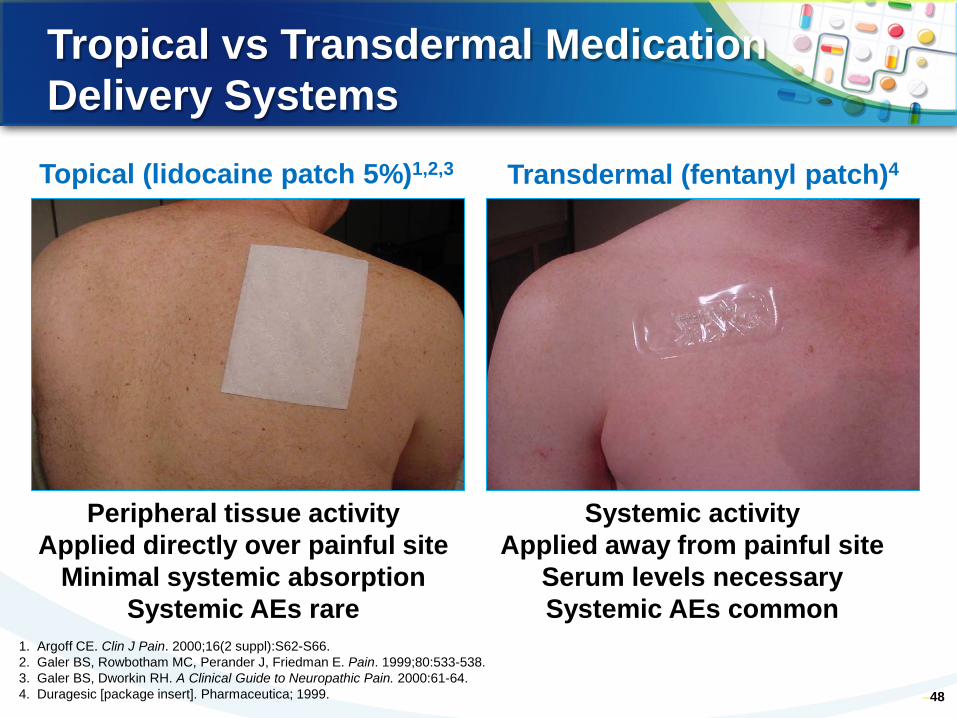
Tropical vs Transdermal Medication Delivery Systems
–48
Systemic activity Applied away from painful site
Serum levels necessary Systemic AEs common
Peripheral tissue activity Applied directly over painful site
Minimal systemic absorption Systemic AEs rare
Topical (lidocaine patch 5%)1,2,3 Transdermal (fentanyl patch)4
1. Argoff CE. Clin J Pain. 2000;16(2 suppl):S62-S66. 2. Galer BS, Rowbotham MC, Perander J, Friedman E. Pain. 1999;80:533-538. 3. Galer BS, Dworkin RH. A Clinical Guide to Neuropathic Pain. 2000:61-64. 4. Duragesic [package insert]. Pharmaceutica; 1999.
Lidocaine Patch 5%
• Lidocaine 5% in pliable patch1
• Up to 3 patches applied once daily directly over painful site2,3
– 12 h on, 12 h off (FDA-approved label) – Recently published data indicate 4 patches (18–24 h) safe
• Efficacy demonstrated in 3 randomized controlled trials on PHN3-5
• Drug interactions and systemic side effects unlikely6-8
– Most common side effect: application-site sensitivity • Clinically insignificant serum lidocaine levels7
• Mechanical barrier decreases allodynia4
–49
1. Lidoderm (lidocaine patch 5%) [package insert]. 2. Alvarez NA, et al. Programs and Abstracts of the IASP 10th World Congress on Pain. 2002. Abstract 175-P171. 3. Rowbotham MC, et al. In: Programs and Abstracts of the 8th World Congress on Pain. 1996. Abstract 274. 4. Rowbotham MC, et al. Pain. 1996;65:39-44. 5. Galer BS, et al. Pain. 1999;80:533-538. 6. Argoff CE. Clin J Pain. 2000;16(2 suppl):S62-S66. 7. Galer BS, et al. A Clinical Guide to Neuropathic Pain. 2000:61-64; 8. Gammaitoni AR, et al. Ann Pharmacother. 2002;36:236-240.
–50
Class of Agent
Clinical concerns
Clinical utility
Target
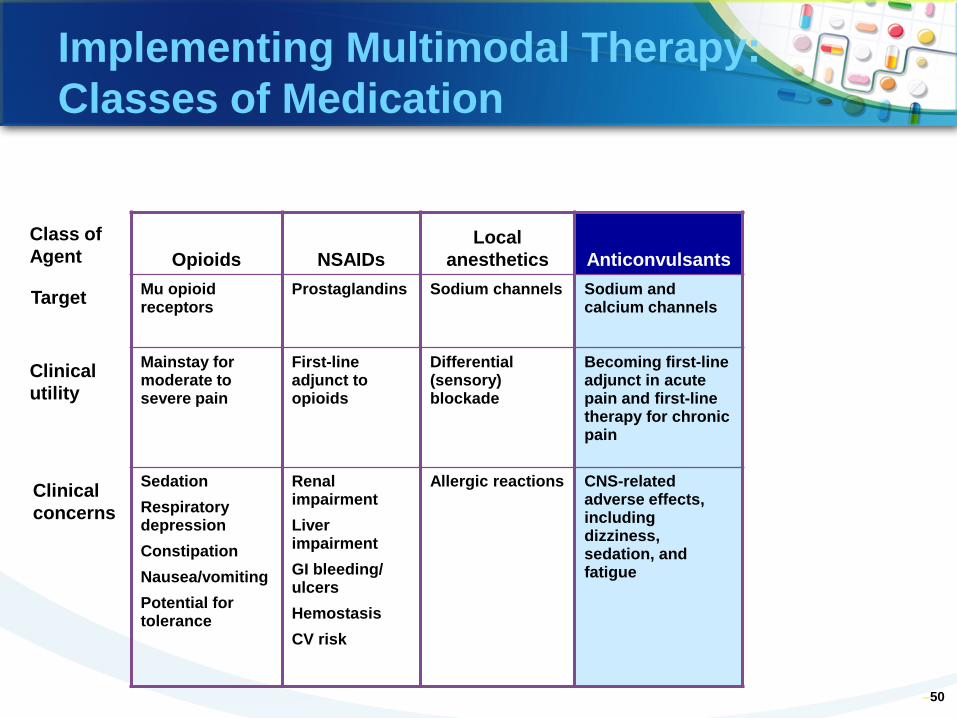
Implementing Multimodal Therapy: Classes of Medication
Opioids NSAIDs Local
anesthetics Anticonvulsants Mu opioid receptors
Prostaglandins Sodium channels Sodium and calcium channels
Mainstay for moderate to severe pain
First-line adjunct to opioids
Differential (sensory) blockade
Becoming first-line adjunct in acute pain and first-line therapy for chronic pain
Sedation Respiratory depression Constipation Nausea/vomiting Potential for tolerance
Renal impairment Liver impairment GI bleeding/ ulcers Hemostasis CV risk
Allergic reactions CNS-related adverse effects, including dizziness, sedation, and fatigue
Classes of Pain Medications: Anticonvulsants
• Decrease excitability of neurons by modulating sodium channels; do not act on GABA
• Emerging as top-line adjunct in acute pain and first-line therapy in chronic pain
• Adverse effects/limitations – Most common adverse effects
are CNS related, including sleepiness, dizziness, and fatigue
–51
–Examples: gabapentin, pregabalin, lamotrigine
Brunto LL, Lazo SS, Parker KL. Goodman & Gillman’s The Pharmacological Basis of Therapeutics, 11th ed. New York, NY: McGraw Hill; 2006.
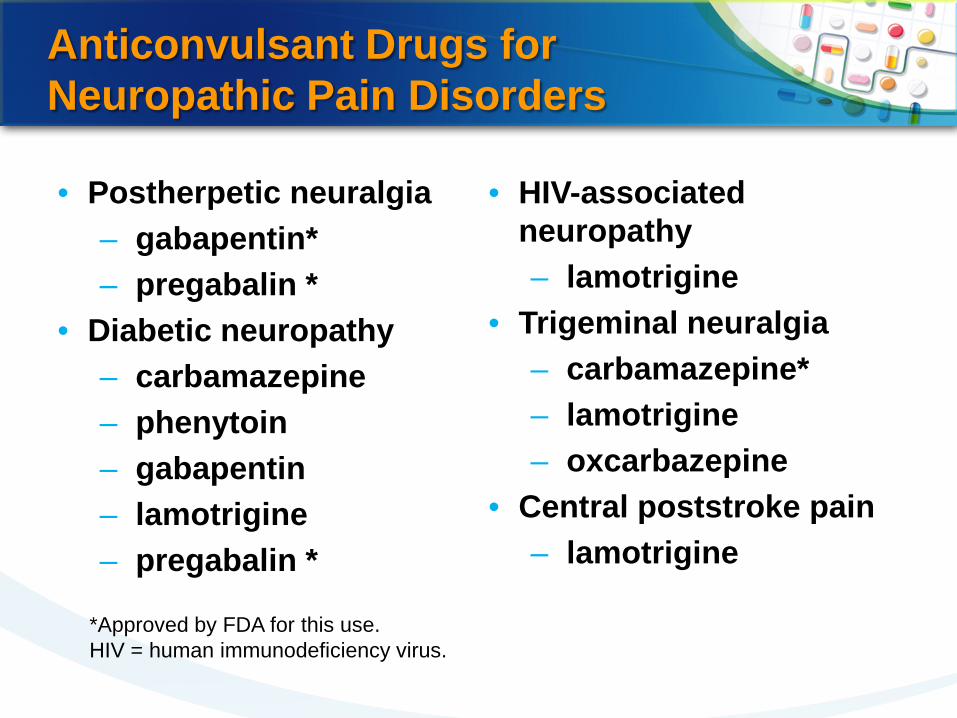
Anticonvulsant Drugs for Neuropathic Pain Disorders
• Postherpetic neuralgia – gabapentin* – pregabalin *
• Diabetic neuropathy – carbamazepine – phenytoin – gabapentin – lamotrigine – pregabalin *
• HIV-associated neuropathy – lamotrigine
• Trigeminal neuralgia – carbamazepine* – lamotrigine – oxcarbazepine
• Central poststroke pain – lamotrigine
*Approved by FDA for this use. HIV = human immunodeficiency virus.
–53
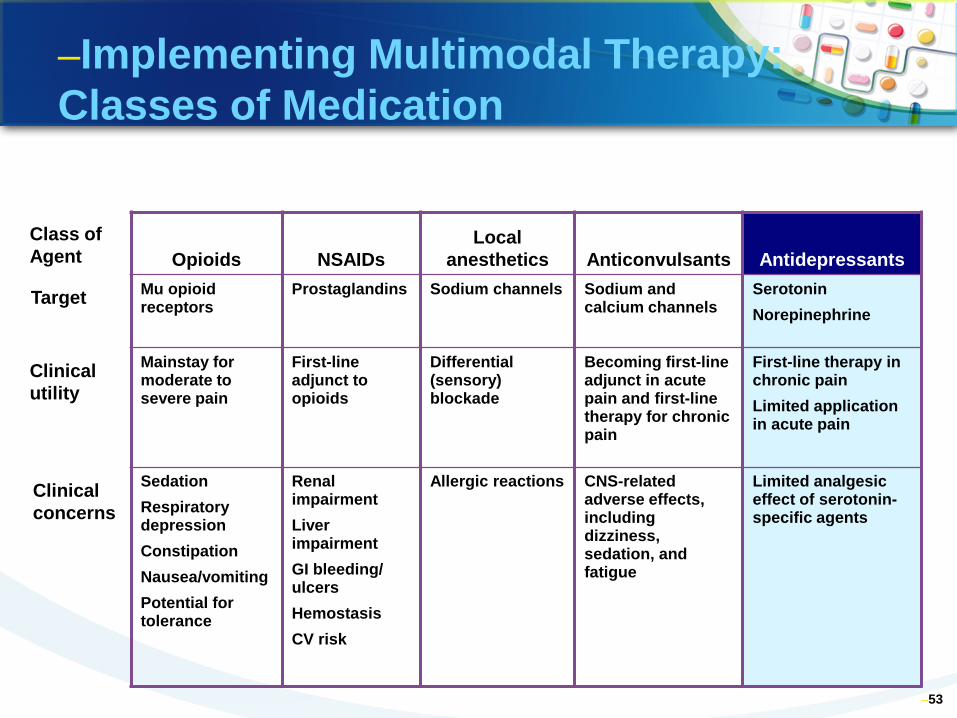
–Implementing Multimodal Therapy: Classes of Medication
Opioids NSAIDs Local
anesthetics Anticonvulsants Antidepressants Mu opioid receptors
Prostaglandins Sodium channels Sodium and calcium channels
Serotonin Norepinephrine
Mainstay for moderate to severe pain
First-line adjunct to opioids
Differential (sensory) blockade
Becoming first-line adjunct in acute pain and first-line therapy for chronic pain
First-line therapy in chronic pain Limited application in acute pain
Sedation Respiratory depression Constipation Nausea/vomiting Potential for tolerance
Renal impairment Liver impairment GI bleeding/ ulcers Hemostasis CV risk
Allergic reactions CNS-related adverse effects, including dizziness, sedation, and fatigue
Limited analgesic effect of serotonin-specific agents
Class of Agent
Clinical concerns
Clinical utility
Target
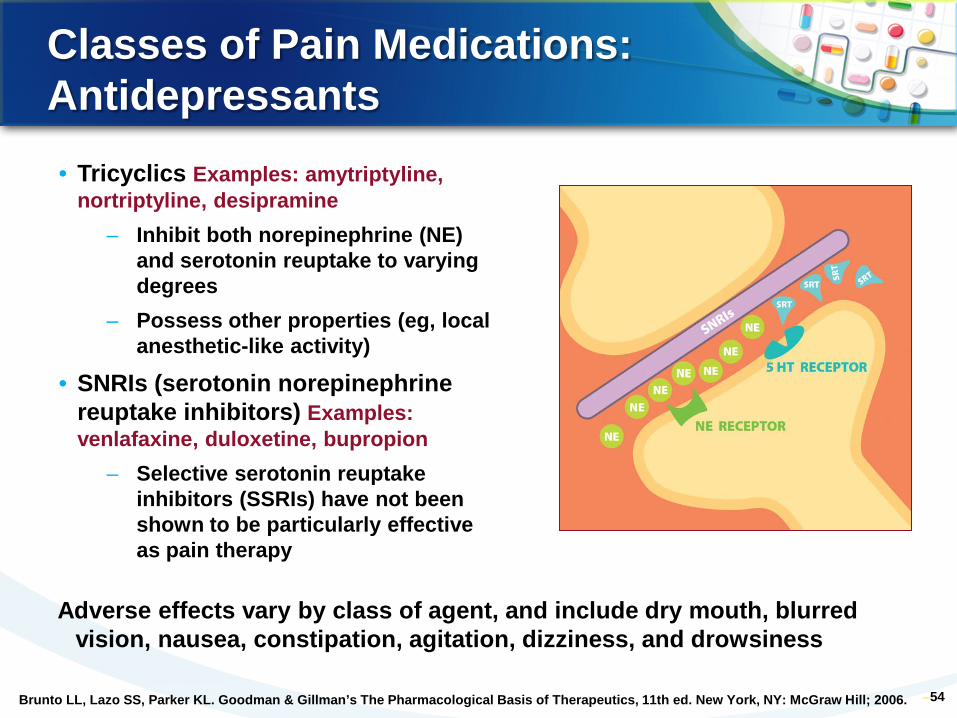
Classes of Pain Medications: Antidepressants
–54
• Tricyclics Examples: amytriptyline, nortriptyline, desipramine
– Inhibit both norepinephrine (NE) and serotonin reuptake to varying degrees
– Possess other properties (eg, local anesthetic-like activity)
• SNRIs (serotonin norepinephrine reuptake inhibitors) Examples: venlafaxine, duloxetine, bupropion
– Selective serotonin reuptake inhibitors (SSRIs) have not been shown to be particularly effective as pain therapy
Adverse effects vary by class of agent, and include dry mouth, blurred vision, nausea, constipation, agitation, dizziness, and drowsiness
Brunto LL, Lazo SS, Parker KL. Goodman & Gillman’s The Pharmacological Basis of Therapeutics, 11th ed. New York, NY: McGraw Hill; 2006.
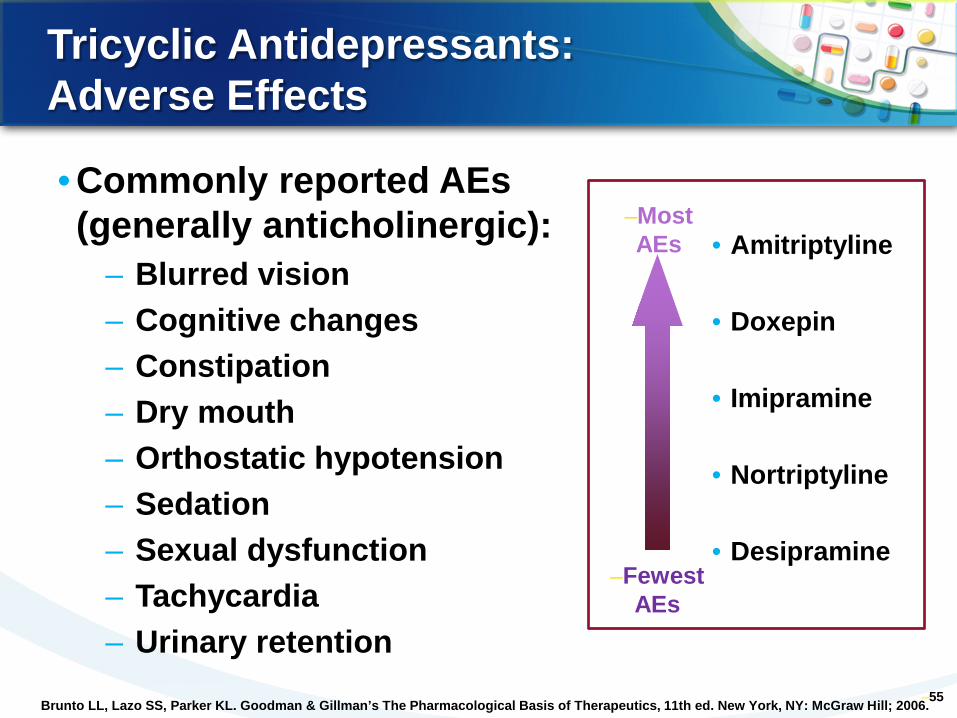
Tricyclic Antidepressants: Adverse Effects
• Commonly reported AEs (generally anticholinergic):
– Blurred vision – Cognitive changes – Constipation – Dry mouth – Orthostatic hypotension – Sedation – Sexual dysfunction – Tachycardia – Urinary retention
–55
• Amitriptyline • Doxepin
• Imipramine
• Nortriptyline • Desipramine
–Fewest AEs
–Most AEs
Brunto LL, Lazo SS, Parker KL. Goodman & Gillman’s The Pharmacological Basis of Therapeutics, 11th ed. New York, NY: McGraw Hill; 2006.
Multimodal Strategy: Implications for Nursing Practice
• Effective and safe practices with multimodal strategies require that nurses:
– Understand the rationale for combining analgesics1,2,4 – Be knowledgeable about classes of analgesics1,2,4
• Mechanisms of action and pharmacodynamics • Synergistic and AEs
– Ensure timely administration of all analgesics, avoiding gaps in analgesia2-4
– Institute proper assessment and monitoring practices2,3 – Aggressively manage AEs of analgesics1,2,4 – Remain informed about novel dual-mechanism analgesics
and drug delivery systems1,2,4
–56 1. Krenzischek DA, et al. Pain Manag Nurs. 2008;9:S22-32. 2. Dunwoody CJ, et al. Pain Manag Nurs. 2008;9:S11-21.
3. Polomano RC, et al. Pain Manag Nurs. 2008;9:S3-10. 4. Polomano RC, et al. Pain Manag Nurs. 2008;9:S33-41.
Drug Therapy of Chronic Pain: Implications for Future Practice
• Multimodal therapy will continue to evolve through use of novel agents and technologies
– Dual-mechanism agents
• Increased knowledge of the physiology of pain and pharmacotherapy helps nurses safely and effectively understand and administer multimodal analgesia
– Focused assessments and reassessments – More consistent and reliable dosing to reduce
analgesic gaps – More options to advocate for individual patient’s
treatment needs
–57 Polomano RC, et al. Pain Manag Nurs. 2008;9:S33-41.
• Pain protocols – Consider what constitutes best
clinical care • Protocols are useful tools to
direct care, but nurses must also apply their clinical judgment
– Treat the patient, not the number • Evidence shows that the
incidence of opioid-induced adverse effects increases significantly after implementing a policy to titrate opioids to a specific numeric rating scale (NRS) number1,2
58
Treat the PATIENT,
not the number
1. White PF, Kehlet H. Anesth Analg. 2007;105:10-12. 2. Vila H Jr, et al. Anesth Analg. 2005;101:474-480.
Individualizing Pain Therapy: Practice Factors
Multimodal Analgesia For Acute Pain
• Acute postoperative pain remains significantly undertreated and is associated with substantial short- and long-term consequences
• Despite multiple guidance documents, barriers to the successful management of acute and chronic pain still remain
• Multimodal analgesia and the avoidance of “analgesic gaps” are central to effective management of postoperative pain
• Emerging treatment options may assist in removing barriers to optimal postoperative pain management
Multimodal Analgesia For Chronic Pain
• Chronic neuropathic pain is a disease, not a symptom
• “Rational” polypharmacy is often necessary • combining peripheral and central nervous
system agents enhances pain relief • Treatment goals include:
• balancing efficacy, safety, and tolerability • reducing baseline pain and pain
exacerbations • improving function and QOL
• New agents and new uses for existing agents offer additional treatment options