-
8/3/2019 1anursing Care Study Jasin (1)
1/32
1
NURSING CARE STUDY:
DIABETES MELLITUS
NAME: NORFAZILAH BINTI AHMAD IBRAHIM
I/C NUMBER: 841029-01-6222
POST BASIC GERONTOLOGY
-
8/3/2019 1anursing Care Study Jasin (1)
2/32
2
ACKNOWLEDGEMENTS
I would like to take this opportunity to express my appreciation
and thanks to my
lecturers, Puan Rodhiah binti Mohd Yasin for the guidance and
cooperation given for me to
complete the study Diabetes Mellitus. I also would like to
thanks to Pengarah Kolej
Kejururawatan, Melaka, and the librarian for permitting me to
use the facilities in finishing the
case of my study. My appreciation and sincere thanks to all of
those individuals at 2B (Hospital
Jasin, Melaka) who were very helpful and supportive.
Besides that, I would like to give my special thanks to all my
course mates, who
always motivate and help me to do some references together and
sharing their knowledge and
ideas.
-
8/3/2019 1anursing Care Study Jasin (1)
3/32
3
LITERATURE REVIEW
Diabetes is a chronic disease, which occurs when the pancreas
does not produce enough
insulin, or when the body cannot effectively use the insulin it
produces. This leads to an
increased concentration of glucose in the blood
(hyperglycaemia).
Type 1 diabetes (previously known as insulin-dependent or
childhood-onset diabetes) is
characterized by a lack of insulin production.
Type 2 diabetes (formerly called non-insulin-dependent or
adult-onset diabetes) is caused by
the bodys ineffective use of insulin. It often results from
excess body weight and physical
inactivity.
(WHO) http://www.who.int/topics/diabetes_mellitus/en/
Diabetes is a disease in which the body doesn't produce or
properly use insulin. Insulin is a
hormone produced in the pancreas, an organ near the stomach.
Insulin is needed to turn sugar
and other food into energy. When you have diabetes, your body
either doesnt make enough
insulin or cant use its own insulin as well as it should, or
both . This causes sugars to build up
too high in your blood.
-
8/3/2019 1anursing Care Study Jasin (1)
4/32
4
Diabetes mellitus is defined as a fasting blood glucose of 126
milligrams per deciliter (mg/dL)
or more. Pre-diabetes is a condition in which blood glucose
levels are higher than normal
but not yet diabetic.
People with pre-diabetes are at increased risk for developing
type 2
diabetes, heart disease and stroke, and have one of these
conditions:
y impaired fasting glucose (100 to 125 mg/dL)y impaired glucose
tolerance (fasting glucose less than 126 mg/dL and a glucose levely
between 140 and 199 mg/dL two hours after taking an oral glucose
tolerance test)
AMERICAN HEART
ASSOCIATIONhttp://www.americanheart.org/presenter.jhtml?identifier=4546
Diabetes mellitus is a disorder in which blood sugar (glucose)
levels are abnormally high
because the body does not produce enough insulin to meet its
needs.
THE MERCK MANUALS ONLINE MEDICAL LIBRARY
(http://www.merckmanuals.com/home/sec13/ch165/ch165a.html)
Diabetes is a chronic disease that has no cure. Diabetes is a
disease in which the body does not
produce or properly use insulin, a hormone that is needed to
convert sugar, starches, and other
food into energy needed for daily life. The cause of diabetes is
a mystery, although both
genetics and environment appear to play roles.
MALAYSIAN DIABETES ASSOCIATION
(http://www.diabetes.org.my/article.php?aid=5)
-
8/3/2019 1anursing Care Study Jasin (1)
5/32
5
CONTENT
NO TOPIC
-
8/3/2019 1anursing Care Study Jasin (1)
6/32
6
1.TOPIC
1.1. WHAT IS DIABETES MELLITUS?
DIABETES MELLITUS (DM) is metabolic syndrome characterized by
hyperglycaemia that
results from an impairment of insulin action and/or
secretion.
Type I or Insulin-Dependent Diabetes Mellitus
- Is the result of pancreatic islet cell destruction and a total
deficit of circulating insulin.When beta cells are destroyed,
insulin is no longer produced
- This disorder is characterized by hyperglycaemia (elevated
blood glucose levels), abreakdown of body fats and proteins, and
the development of ketosis (an accumulation of
ketone bodies produced during the oxidation of fatty acids)
Type II or Non-Insulin-Dependent Diabetes
- Is the result from insulin resistance with a defect in
compensatory insulin secretion.- Is a condition of fasting
hyperglycaemia that occurs despite the availability of
endogenous insulin (Porth, 2002).
- It can occur at any age, but it is usually seen in middle age
and older people .
-
8/3/2019 1anursing Care Study Jasin (1)
7/32
7
1.2. WHAT CAUSES OF DIABETES MELLITUS?
DM
1.3. RISK FACTORS?
1.4. SIGN AND SYMPTOMS OF DM?
- Type I - symptomatic hyperglycemia or DKA.y o plasma glucose
glucosuria osmotic diuresis (Polyuria) dehydration
(polydipsia /weight loss).
y blurred vision,fatigue,nauseay fungal and bacterial-vaginal
candidiasis
- Type II frequency routine medical examination - asymptomaticy
Glucose molecules accumulate in the circulating blood, resulting
in
hyperglycaemia.
1.5. WHAT ARE THE EFFECTS OF DM?
- Progressive complications Hyperglycaemia
Diabetic ketoasidosis Hyperglycaemic hyperosmolar nonketotic
coma
Hypoglycaemia- Late complications
y Neurologic
-
8/3/2019 1anursing Care Study Jasin (1)
8/32
8
Somatic neuropathies Paresthesias, pain, loss of cutaneous
sensation, loss of fine motor
control.
Visceral neuropathies Sweating dysfunction, pupillary
constriction, fixed heard rate,
constipation, diarrhoea, incomplete bladder emptying,
sexuality
dysfunction
y Sensory Diabetic retinopathy, cataracts, glaucoma
y Cardiovascular Orthostatic hypotension, Accelerated
atherosclerosis Coronary artery disease Cerebrovascular disease
(stroke) Peripheral vascular disease Blood viscosity and platelet
disorder
y Renal Hypertension, albuminuria, oedema, chronic renal
failure
y Musculoskeletal Joint contractures
y Integumentary Foot ulcers, gangrene of the feet, atrophic
changes.
y Immune system Impaired healing, chronic skin infections,
periodontal disease, urinary
tract infections, lung infections, vaginitis
-
8/3/2019 1anursing Care Study Jasin (1)
9/32
9
1.6. HOW IS A DIABETIC DIAGNOSE?
- Oral Glucose Tolerance Test(OGTT)- the client is given a
specified amount of glucose(either 75g or 100g) as a lemon flavour
or glucola liquid after fasting blood and urine
samples are taking.
- Fasting Blood Sugar(FBS)- this test often ordered, especially
if the client isexperiencing symptoms of hyperglycaemia and
hypoglycaemia.
- Glycosylated haemoglobin(c) HbA1C- this test determines the
average blood glucoselevel over approximately the previous
2-3months. When the glucose is elevated or
control of glucose is erratic, glucose attaches to the
haemoglobin molecule and remains
attached for the life of the haemoglobin, which is about 120
days.
- Urine glucose and ketone levels- these are not as accurate in
monitoring changes in blood glucose as blood levels. The presence
of glucose in the urine indicates
hyperglycaemia. Ketonuria (the presence of ketones in the urine)
occur with the
breakdown of fats and is an indicator of DKA; however, fat
breakdown and ketonuria
also occur in stages of less than normal nutrition.
- Serum cholesterol and triglyceride levels- these are indicator
of artherosclerosis and anincreased risk of cardiovascular
impairments.
- Serum electrolytes- levels are measured in clients who have
DKA or HHs to determineimbalances.
-
8/3/2019 1anursing Care Study Jasin (1)
10/32
10
1.7. MANAGEMENT?
-
8/3/2019 1anursing Care Study Jasin (1)
11/32
11
ABSTRACT
This nursing care study is about a male patient Mohd Salleh
@Yahya bin Nikmat who is 69
years old he lives in Taman Damai, Bemban, Jasin, Melaka. He was
admitted to the Jasin
Hospital on 04 Mei 2011 after he was complaining of dizziness
and abdominal discomfort.
He retired as a Post Officer, and was very active and
hardworking but he was so depressed
after the death of his wife on the 7th
Mac 2011.
He was hospitalised for eleven days.
Since diabetes is a chronic disease which occurs when the
pancreas does not produce enough
insulin or when the body cannot effectively use the insulin it
produces. This leads to an
increased concentration of glucose in the blood (hyperglycemia)
and no cure to this.
The insulin theraphy was introduced to him in order to
stabilized his blood sugar level and later
when he was discharged he currently be treated as an outpatient
. A frequent routine medical
examination is recommended.
-
8/3/2019 1anursing Care Study Jasin (1)
12/32
12
ASSESSMENT
-
8/3/2019 1anursing Care Study Jasin (1)
13/32
13
2.0 ASSESSMENT
2.1. BIOGRAPHIC DATA
NAME: MOHD SALLEH @ YAHYA BIN NIKMAT
I/C NUMBER: 421121-04-5113
AGE: 69 YEARS OLD
SEX: MALE
RACE: MALAY
RELIGION: ISLAM
ADDRESS: 4957, JALAN RIA, TMN DAMAI, BEMBAN, 70000
TEL.NUMBER: 017-2054944
MARITIAL STATUS: WIDOW
2.2. INTRODUCTION: MR S
Mr S is a 3rd
son in the sibling of 6th
. His parents passed away due to old age disease.
All siblings are still alive accept the eldest brother, Mr I,
was died at the age 70 years old due
-
8/3/2019 1anursing Care Study Jasin (1)
14/32
14
to diabetes mellitus. His eldest sister Mrs H was in KL, 72
years old. His two sisters, Mrs J, 67
years old and Mrs K, 62 years old were staying in Melaka and his
brother Mr L, 60 years old
was at Johor Bahru. His sister Mrs J had a hypertension and
diabetes and now she is under
treatment.
Mr S was studying until primary six. Worked as a Post Officer
about 30 years and he
had retired at the age 55 years old. Married with Mrs B and have
seven children, four daughters
and three sons. Their eldest daughter is 49 years old, married
and as a housewife. She had three
children. Second son is 44 years old, married and had four
children. Work as a teacher and he
had diabetes. Their third son 42 years old, married and had five
children. Work as Postmen.
Fourth daughter 39 years old, married and had two children. Work
as Staff Nurse and had a
hypertension. Fifth son is 37 years old, married and had three
children. Work as a Clerk. Sixth
daughter is 28years old, married and had two children. Work as
Project Manager. Lastly, their
seventh son is 27years old and not married yet . Work as Lorry
Driver. (see Figure 1: Mr S
family tree).
According to his daughter Mrs A, Mr S is an active and
hardworking person.
After
retired he always do some chores and likes to do gardening and
farming . He always said to his
daughter that he felt he was in healthy and energetic; no need
to go to clinic for check-up.
According to his daughter, since 3 month ago, he looked very sad
and unhappy because
his wife passed away at 07.03.2011 due to DM. He always be
pensive and become quite,
sometimes he cried when he remember his wife and felt lonely and
lost. He is very secretive
with his children but sometimes he shared his sadness with his
friends.
2.3. SOCIAL AND ENVIRONMENT ASSESSMENT
-
8/3/2019 1anursing Care Study Jasin (1)
15/32
15
Currently, Mr S lives in his single storey house,four bedrooms,
and two bathroom with
a squatting and sitting toilet. There is no hand railing in his
home. His house is near the mosque
and grocery shop.
Mr S stayed with his eldest daughter who is housewife and look
after him. Besides that,
he also shared the home with his son-in-law and three
grandchildren. His economic is stable.
He got some money from his children about RM500 per month. He
also got pension money
about RM800 per month.
Mr S has a good social interaction with neighbour and friend.
Always go to the mosque
for prayig and attended religious activities.
2.4. COMMUNICATION ASSESSMENT
Mr S can only understand and communicate in Bahasa Melayu and
simple English. He
was good in communication and answer the entire question
relevant and appropriately.
However, his eyesight has developed some changes about 4-5years
ago because he
claimed having problems when reading newspapers. He wore
spectacle when he was reading.
2.5. DIETARY ASSESSMENT
Mr S likes to eat all types of food. He did not like to eat
outside food but he always eats
his wife cook. He does not have a problem with swallowing.
Breakfast roti canai/nasi lemak/fried bihun/rice/bread/coffee.
Lunch rice/chicken
curry/seafood/meat/vegetable. Tea tea/milo/coffee/nescafe/local
cakes/fried banana/biscuit.
Dinner rice/chicken curry/seafood/meat/vegetable. Supper
coffee/milk/biscuit.
-
8/3/2019 1anursing Care Study Jasin (1)
16/32
16
2.6. HABIT ASSESSMENT
2.6.1 CIGARETTE SMOKING :
Mr S used to smoke 1pack of cigarette per day. He smokes since
he was 20 years old
until now. Lately, he has stopped smoking because he was
hospitalized.
2.6.2 ALCOHOLIC BEVERAGES CONSUMPTION:
He does not drink alcoholic beverages.
2.7. SLEEP AND REST ASSESSMENT
Mr S has a good sleep and have enough rest.
He used to sleep at 11.
00pm till 6.
00am in the
morning. After that he was going to the mosque for Subuh prayer.
However, since he was
admitted in the hospital he sleeping was disturbed.
2.8. INCONTINENCE ASSESSMENT
Mr S dont have a urinary or bowel problem.
2.9. PAST ILLNESS HISTORY
In 2006, Mr S has done for haji screening. Since then he was
diagnosed DM and
Hypertension. He was under treatment for a few months only and
he missed the TCA and the
-
8/3/2019 1anursing Care Study Jasin (1)
17/32
17
treatment for almost 5 years. He always said to his daughter
that he felt he was in healthy and
energetic condition and no need to go to clinic for
check-up.
On the other hand, he has never undergone any forms of surgical
intervention and
hospital admission till now. He also does not have any known
allergies to neither drug nor
food.
2.10. HISTORY OF PRESENT ILLNESS
2.10.1 ADMISSION HISTORY:-
On 04/05/2011 at 9.00am, Mr S was complaint of dizziness, on and
off abdominal
discomfort at home and bilateral lower limb edema. He went to
Klinik Kesihatan Daerah Jasin
for check-up. B/P: 135/71mmhg, RBS: 21.4mmol/L, urine for
ketone: 1+. Doctor gave the
instruction, if possible for admission and for further
management.
At 02.52pm, Mr S went to OPD of Jasin Hospital. G/M was HI. Inj
Actrapid 12 stat
was given. Mr S was informed to be admitted to Wad 2B.
2.10.3 MR S PROGRESS IN WARD?
04/05/2011 In ward, Mr S look alert and comfortable. He still
has mild pedal oedema
bilaterally. Vital sign was taken, B/P: 121/82mmHg, Pulse:
64/min, SPO: 98%R/A,
Temperature: 37C, G/M: 18.9mmol/L. Dr Zawani planned to give S/C
Humulin R 10 TDS,
-
8/3/2019 1anursing Care Study Jasin (1)
18/32
18
S/C Humulin N 10 ON, continue anti-hypertension drug: T .
Captopril 12.5mg TDS, T.
Amlodipine 5mg OD, withhold T. Metformin, G/M QID, vital sign
monitoring every 4hourly.
05/05/[email protected]: Mr S was seen by Dr Amudra. She planned an
asked pharmacist
to collect back all metformin which he consumed from other
sources, advised family
members to buy G/M, S/C Humulin R 12 TDS, if G/M >10 to add 2
and if G/M >14 to add
4, S/C Humulin N 14 ON. At 12.00pm: Seen by Diabetic Nurse (M/A
M. Hafiz bin
Sulaiman). Diabetic counselling was given to Mr S. Then he was
referred to Counsellor about
complication of diabetic, blood glucose control, insulin
injection, and self-monitoring blood
glucose. At 4.00pm: Mr S was conscious but have mild lethargic .
RIB. He complained of
giddiness, cold and clammy. He took one glass of sweet drink and
two pieces of bread. Vital
sign was taken, B/P: 93/51mmHg, Pulse: 42/min, SPO: 95%R/A, G/M:
3.1mmol/L. Dr
Zawani was noted and ordered to give I/V Dextrose 5%/24hrs. At
4.45pm: B/P 119/65mmHg,
Pulse: 51/min, SPO:98%R/A, G/M: 13.2mmol/L. At 05.45pm: Seen by
Pharmacist, Miss Fan
Siew Kim. She was consulted Mr Ss daughter about hypoglycaemia
attack. Mr Ss daughter
claimed that shell buy glucometer herself. All the medications
was taken by pharmacist and
plans for switch the dosage of insulin to BD once Mr S
discharge.
06/05/[email protected]: Seen by Dietician. Mr S claimed giddiness and
not feeling well. Planned
to review Mr S Tuesday or as outpatient if discharge and ward
staff to indent low soft diabetic
diet for Mr S.
07/05/[email protected]: Mr S still had lethargic and giddiness. His
condition was very labile
during the first three days. His temperature fluctuates ranging
39.1C 37.5C. T.PCM 1gm
was given and IVD 3 Normal Saline in progress. Besides that, his
blood sugar level was not
controlled, ranging from 14.0 23.8mmol/L. G/M QID and insulin
therapy was introduced in
order to stabilize Mr Ss blood sugar level. (Refer appendix:
Blood Sugar Chart). However,
-
8/3/2019 1anursing Care Study Jasin (1)
19/32
19
there were two incidents, where Mr S had hypoglycaemia episode.
This related to loss of
appetite.
09/05/2011: Mr S still complained of headache on and off and
redness at right hand, cough,
nausea and vomiting for four times. Dr Zawani was diagnosed as
thrombophlebitis at dorsum
right hand. She was ordered I/V Cloxacillin 1mg QID, T. PCM 1gm
QID, T. Maxalon 10mg
BD and off IVD.
11/05/[email protected]: Mr S still having cough. He claimed that he
had chest pain and SOB.
During the examination by Dr Amudha, he had crepts at lower site
of lung and the implication:
Carers for hospitalization due to pneumonia TRO pulmonary
embolism.
She planned to give
I/V Tazosin 4.5gm stat & TDS, repeat FBC/BUSE/ESR, chest
X-ray, D-dimer and off OHA.
At 01.25pm: D-dimer result was positive 1.8. Dr Amudha planned
for urgent CTPA at Malacca
General Hospital: if positive finding to admit Malacca General
Hospital but if normal finding
to send back to Jasin. Dr Amudha was spoken to Dr Roza
(Radiologist specialist) and planned
to refer Mr S to Malacca General Hospital. 03.30pm: Mr S gone to
Malacca General Hospital
accompanied by SN Norazean and PPK Walid.
2.11. PHYSICAL EXAMINATION
1. GENERAL CONDITION: Mr S was alert and conscious but mild
lethargic. Can dohis activities daily by himself.
2. VITAL PARAMETERS3. HAIR: Grey, clean and tidy
4. EYES :USED A GLASSES, hypermetropia5. EARS : no discharge and
no hearing problem6. MOUTH AND THROAT: clean, used a dentures, no
cough and sputum7. NECK: no lymph nodes enlargement/tender8. SKIN
:redness at right hand9. NAILS:clean and short10.CHEST&HEART:
C/O chest pain& SOB
-
8/3/2019 1anursing Care Study Jasin (1)
20/32
20
11.LUNGS : Crept+12.ABDOMEN: soft and tender13.GENITALIA :no
enlarged prostate/hernias14.PERIPHERAL VASCULAR15.NEUROLOGICAL
2.12
.FUNCTIONAL ASSESSMENT
1.SELF-CARE ASSESSMENTThis nursing care study adopted from
Barthel Index in assessing how well Mr S was able
to care for himself. (Refer appendix: Barthel Index). After a
session of interview with Mr S,
Barthel Index revealed that Mr Ss ADL was mid dependent.
2.PSYCHOLOGICAL ASSESSMENTa) COGNITIVE FUNCTIONING
Cognitive assessment such as the ECAQ and the Mini-mental State
Examination
shows that(Refer appendix: ECAQ & MMSE)
b) AFFECTIVE FUNCTIONINGMr S has demonstrated sign and symptoms
of depression such as loss of interest
to do. Depression scale show that (Refer appendix: Depression
scale)
3.SOCIAL ASSESSMENTIn this context, Mr S is taken care by his
daughter. It is essential to assess his daughter for carer
assessment (Refer appendix: The Caregiver Strain Index)
-
8/3/2019 1anursing Care Study Jasin (1)
21/32
21
NURSING CARE
PLAN
-
8/3/2019 1anursing Care Study Jasin (1)
22/32
22
3.NURSING CARE PLAN: NURSING PROCESS
APPROACH
1) NURSING DIAGNOSA#1: Risk for impaired skin integrity related
to diabetic process
GOAL: Patient will experience intact skin status, and skin will
be free of irritation or trauma
especially at feet and lower extremities
INTERVENTION:
1) Conduct baselines and on-going assessment on the feet
including:- Musculoskeletal assessment that includes foot and ankle
joint range of motion,
bone abnormalities (bunions, hammertoes, overlapping digits),
gait patterns, and
abnormal wear patterns on shoes.
- Neurologic assessment that includes sensations of touch and
position, pain andtemperature
.
- Vascular examination that includes assessment of lower
extremity pulses, capillary
refill, colour and temperature of skin, lesions and oedema .
- Hydration status, including dryness or excessive
perspiration.- Lesions, fissures between toes, corns, calluses,
cracks in the skin, plantar warts,
ingrown or overgrown toenails, redness, blisters, cellulitis or
gangrene.
: Identifies potential circulatory insufficiency that may lead
to skin breakdown as
perfusion of oxygen and nutrients are reduced
-
8/3/2019 1anursing Care Study Jasin (1)
23/32
23
2) Teach foot hygiene. Wash the foot daily with lukewarm water
and mild hand soap; patdry, and dry well between the toes. Apply a
very thin coat of lubricating cream if
dryness is present (but not between the toes)
: proper hygiene decreases the chance of infection. Temperature
receptors may be
impaired, so the water should always be tested before use.
3) Conduct foot care teaching sessions as often as necessary.-
Use proper shoes
y Shoe that allow to inch of toe room are best; there should be
room for toesto spread out and wiggle. The lining and inside
stitching should be smooth and
the insole soft.
y Do not wear open-toed shoes, sandals, high heels, or thongs;
they increase therisk of trauma.
y Buy shoes late in the afternoon, when feet are at their
largest; always buy shoesthat feel comfortable and do not need to
be broken in
.
y Check the shoes before each wearing for foreign objects,
wrinkled insoles and
cracks that might cause lesions.
---- Care of toenails
y Cut the toenails after washing, when they are softer and
easier to trim.y Cut the nails straight across with a clipper and
smooth edges and corners with
and emery board.
yDo not use razor blades to trim the toenails
.
- Check the feet daily for red areas, cuts, blisters, corns,
calluses, or cracks in the
skin. Check between the toes for cracks or reddened area.
- Check the skin of the feet for dry or damp areas.- Use a
mirror to check each sole and the back of each heel.- If you unable
to inspect the feet daily, be sure that someone else does so.- Do
not sit with the legs crossed at the knees or ankles.-
4) Instruct patient/family to avoid use of over-the-counter
products for calluses and corns .: Some commercial products contain
harsh chemicals that may injure already-
compromised skin.
5) Discuss the importance of maintaining blood glucose levels
through prescribed diet,medication and exercise.
: Hyperglycaemia promotes the growth of microorganisms.
EVALUATIONS
-
8/3/2019 1anursing Care Study Jasin (1)
24/32
24
1) Patient will have intact skin that is free from redness,
irritation, bruises and rashes.
1) NURSING DIAGNOSA#2: Deficient knowledge related to
self-administration of insulin
GOAL: patient will obtain appropriate knowledge and able to
maintain safety of self-
administration of insulin.
INTERVENTION:
1) Instruct patient the importance to take insulin2) Instruct
patient in administration of insulin; name, action, peak, levels,
dosage, how to
store, preparation and filling syringe, rotation sites, and
procedure to inject insulin.
EVALUATIONS:
1) NURSING DIAGNOSA#3: Risk for injury related to decreased
temperature sensation,
decreased tactile sensation and lack of awareness of
environmental dangers.
GOAL: i) Patient will experience no injury, trauma or fall.
ii) Patient will avoid injury to extremities from environmental
hazards
INTERVENTION:
1) Assess patients mobility and stability status, muscular
weakness, cognitive limitations,balance, or gait difficulties, and
factors related to disease process.
: Provides information for baseline data to establish plan care.
Falls are common in
elderly patient and may result from muscle weakness and skeletal
support dysfunction,
as well as decreased tactile and sensory status . Claudication
may result at difference
times dependent on the weather, incline of walking, or rapidity
with which the patient
ambulates.
2) Assess patients sensory deficits of visual, tactile,
perceptual, and kinaesthetic changes.: May contribute to falls and
other trauma because of insensitivity to pain,
temperature extremities or visual acuity.
3) Asses patients mentation, changes, in mental status, vertigo,
syncope, and penchant forwandering
.
: Provide information regarding potential for falls and
trauma.
4) Assess environment for safety hazards. Ensure lighting,
pathways are cleared, beds arein lowest position and locked,
hazardous object out of reach, and ability to summon
help, within reach.
: Safety hazard predispose patient to falls or serious injury.
By ensuring that
hazardous objects are removed, patients environment is made
safer.
-
8/3/2019 1anursing Care Study Jasin (1)
25/32
25
5) Provide night light as needed and ensure that pathways are
clear, and floor is dry andnot slippery.
: Prevents bumping into objects or stumbling and falling.
6) Assist with ambulation as needed.: Promotes safety and
prevents falls if patient is too weak or impaired to ambulate
alone.
7) Stay with patient if complaints of faintness or
dizziness.
: Reduces anxiety and potential injury from fall if patient dose
faint
8) Apply alarm system to bed or chair to alert caregivers that
patient has wandered outsideof safe limitations.
: provide patient the opportunity to ambulate and wander about a
safe distance rather
than use restrains or other confinement method, yet maintaining
a safe environment
9) Instruct patient regarding need for extreme caution when
caring for wounds or burnscause by disease process
complications.
: Diabetic patient have poor wound healing that may take much
longer than normal .
Elderly patient usually have fragile skin that can easily be
traumatized
10)Instruct patient/family regarding medication effects and side
effects of medicationscurrently being taken, and regarding
potential for causing injury.
: Promotes understanding of effect that medication have on
well-being or that
medications can predispose patient to injury or trauma.
EVALUATIONS:
1) Patient will have safe environment maintained with absence of
safety hazards.2) Patient will have no incident of falls or injury
from dangerous objects .3) Patient will be able to ambulate and
wander about in a safe environment.4) Patient/family will be able
to maintain safety with medication administration and home
environmental safety
5) Patient/family will be able to accurately verbalize
understanding of disease process asto how it affects safety within
the environment.
1) NURSING DIAGNOSA#1:
a)
b)
OBJ:
INTERVENTION:
EVALUATIONS:
-
8/3/2019 1anursing Care Study Jasin (1)
26/32
26
CONCLUSION
-
8/3/2019 1anursing Care Study Jasin (1)
27/32
27
REFERENCING
-
8/3/2019 1anursing Care Study Jasin (1)
28/32
28
APPENDIX
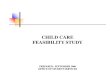
1) FAMILY TREE
-
8/3/2019 1anursing Care Study Jasin (1)
29/32
29
Mr Ss father Mr Ss mother
Mr I Mrs H Mrs J Mrs K Mr L
Died at the age 72yrs 67yrs 62yrs 60yrs
of70yrs HPT & DM
DM
Mr. S Mrs. N
69yrs 62yrsPatient Died on 07.03.2011
Uncontrolled DM DM-amputation both leg since 5years ago
&
all Right finger since Feb 2011.
Mrs. A Mr. B Mr. C Mrs. D Mr. E Mrs. F Mr. G49yrs 44yrs 42yrs
39yrs 37yrs 28yrs 27yrs
Housewife Teacher Postman Staff nurse Clerk Project manager
Driver
Married Married Married Married Married Married Married
3 child 4 child 5child 2child 3child 2child
DM HPT
2) INVESTIGATIONS & FINDINGS(X-RAY)
- Diperihilar Haziness
-
8/3/2019 1anursing Care Study Jasin (1)
30/32
30
ECG
3) LABORATORY INVESTIGATION FINDINGSDATE 04/05/11
FBC:
- HB- TW- PLATELET
15.2mmol/L
7.61mmol/L
201mmol/L
BUSE:- UREA- SODIUM- POTASSIUM- CHLORIDE- CREATININE
8.3mmol/L
132.8mmol/L4.770mmol/L
92.8mmol/L
117mmol/L
FBS 9.0mmol/L
URINALYSIS:
- GLUCOSE- KETONES- SG- PH
56mmol/LNegative
1.015mmol/L5
LIPID PROFILE- CHOL- LDL- HDL- TRIGLYCERIDES
4.75mmol/L
3.21mmol/L
1.
11mmol/L
URINE ACETONE Negative
ABG:- PH- PCO- PO
7.332mmhg
46.1mmhg
34.6mmhg
D-DIMER Positive1.8ug/ml
CE:- AST- LDH- CK
26.08ul/L
555ul/L
178ul/LESR 64mm fall 1
st
hour
-
8/3/2019 1anursing Care Study Jasin (1)
31/32
31
4) BLOOD SUGAR PROFILEDATE/TIME BLOOD
SUGAR
PRE-BF
BLOODSUGAR
PRE-LUNCH
BLOODSUGAR
POSTLUNCH
BLOODSUGAR
PREDINNER
BLOODSUGAR
PRE BED
REMARKS/SIGNATURE
5) I/O CHART6) INTRAVENOUS FLUID THERAPY REGIMENT
DATE/TIME TYPE OF I/V SOLUTION AMOUNT
7) FEEDING REGIMENTENTERAL FEEDING CHART
DATE/TIME TYPES OF FEEDING AMOUNT
ORAL FEEDING CHART
DATE/TIME TYPES OF FEEDING AMOUNT
8) ELDERLY COGNITIVE ASSESSMENT QUESTIONNAIRE-ECAQ9) MMSE10)
BARTHEL INDEX
11)THE CAREGIVE STRAIN INDEX www.hartfordign.org12)NORTON
SCALE13)ROM EXERCISE14)TECHNIQUES OF TRANSFERRING &
LIFTING15)DRUG REFFERENCES
NAME OF
DRUG
ACTIONS OF
DRUG
INDICATIONS SIDE
EFFECT/
NURSING
INTERVENTION
-
8/3/2019 1anursing Care Study Jasin (1)
32/32
ADVERSE
REACTION
16)DRUG CHART NAME OF MEDICINE INSTRUCTION &
INDICATION OF
MEDICINE
SIDE EFFECTS