Embed Size (px)
Citation preview

DOCUMENT RESUME
ED 294 352 EC 202 521
TITLE Focal Point. Volume 1, Fall 1986--Spring/Summer1987.
INSTITUTION Portland State Univ., Oreg. Regional Research Inst.for Human Services.
SPONS AGENCY National Inst. of Handicapped Research (ED),Washington, D.C.; National Inst. of Mental Health(DHHS), Bethesda, Md.
PUB DATE 87NOTE 37p.; Bulletin of the Research and Training Center to
Improve Services for Seriously EmotionallyHandicapped Children and Their Families.
PUB TYPE Collected Works - Serials (022) ReportsDescriptive (141)
JOURNAL CIT Focal Point; vi n1-3 Fall 1986 -Spr -Sum 1987
EDRS PRICE MF01/PCO2 Plus Postage.DESCRIPTORS Agency Cooperation; Cnild Advocacy; Conferences;
Delivery Systems; Education Work Relationship;Elementary Secondary Education; *EmotionalDisturbances; Family Role; Program Implementation;Rehabilitation; Severe Disabilities; TransitionalPrograms
ABSTRACTThe document contains three issues of the newsletter
of the Research and Training Center to Improve Services for SeriouslyEmotionally Handicapped Children and Their Families. The first issueis introduced with an article titled "Re-Thinking EmotionalDisturbances in Children," by Thomas M. Young. Topics covered includethe following: issues raised by the Child and Adolescent ServiceSystem Program initiative; the Therapeutic Case Advocacy Project; theYouth in Transition Project; the Families as Allies Project; currentactivities of states involved in the Families as Allies Conference;rehabilitative services within the Child and Adolescent ServiceSystem Program; components of the Therapeutic Case Advocacy approach;and interagency collaborative efforts. (DB)
***********************************************************************Reproductions supplied by EDRS are the best that can be made
from the original document.**********************************************.************************

o
FALL 1986
RE-THINKING EMOTIONAL DISTURBANCES IN CHILDRENby Thomas M. Young, Ph.D.
U.S. DEPARTMENT OF EDUCATION.'Office of Educational Research and Improvement
EDUCATIONAL RESOURCES INFORMATIONCENTER (ERIC)
Cl/This document has been reproduced asreceived from the person or organizationoriginating it.Minor changes have been made to improvereproduction quality
Points of view or opinions stated in t his docu-ment do not necessarily represent officialOERI position or policy
"PERMISSION TO REPRODUCE THISMATERIAL HAS BEEN GRANTED BY
'121 797C
TO THE EDUCATIONAL RESOURCESINFORMATION CENTER (ERIC)."
La Four issues raised by theChild and Adolescent Service System Program (CASSP) initiative
What is the nature of emotionaldisturbances in children?
The nature of what we customarily havereferred to as "emotional distil'. ,ance" or"mental illness" in children is not sig-nified adequately by those phrases. Itappears on the basis of accumulatedpractice experience and research(especially longitudinal research) thatwhat we refer to as "emotional dis-turbance" or "mental illness" in childrenis more accurately described as behaviorthat is disturbing to those who have tolive with it.
Case examples, when viewed in thecontext of the more recent advances inunderstanding and treating children con-sidered emotionally disturbed, have led'us here at the Portland State UniversityResearch and Training Center to changeour own terminology regarding childrenconsidered emotionally disturbed. We pre-fer the phrase "emotionally handicapped"because we believe it helps us shift ourfocus from the child-as-problem to thecontext-as-solution. It emphasizes thatemotionally handicapped children arespecial children with special needsrequiring special environments - specifi-cally, ones that can accommodate, adjustto, or compensate for their disability.
This, it turns out, is consistent withthe World Health Organization's perspec-tive on disabilities as impairments thatare defined in terms of their functional
consequences in specific settings. Sincewe are concerned witii improving servicesfor emotionally handicapped childrenand their families, we are concentratingon research and training activities de-signed to help parents, teachers, employ-ers and the helping professions find waysof modifying ilying, learning and work-ing environment; to accommodate, adjustto and compemate for children withemotional disabilities.
The CASSP i:iitiative still refers to itstarget popelation as seriously emotionallydisturbed children and adolescents. Thisis a questionable practice that should notbe encouraged to mitinue under federalauspices. Continued use of this terminol-ogy will allow the CASSP initiative to beconsidered only as a "mental health" pro-gram in a very narrow sense, namely, onethat funds and facilitates the applicationof intrapsychic treatment techniques tochildren and adolescents. All of CASSP'sefforts at systems change will founder atthe service delivery level unless newthinking emerges to guide the creation ofnew forms of intervention that focus onways of modifying environments so thatchildren are no longer handicapped bytheir emotional disabilities in those con-texts. New thinking and new forms ofintervention will not develop if we allcontinue to use the old words andphrases. And this brings us to the secondissue.
continued on page 8
The Bulletin of the Research and Training Centerto Improve Services for Seriously Emotionally Handicapped Children and Their Families
Fr -VOLUME 1 NUMBER 1
RFAIW4#01411404ifrOwifi*
.Pri40POljOe0P40,-
-theriiienik'oaselidfOOiC'v- :ProjectThomasM:Young,PhiD x
Principal Investigator; ,
Youth in Trimaition,PioieciMs tlex J: Modreii4Ph.D.,
Principal 444anttOr
:1441:0A19- 44e)4#144,104,COMdinator
i'Ocii Pointttikanis -= Editor
liliharA;j5;-4
4+;011.*:04444105.1;:Bi,
A#40.0As*,
-GRADUATE ficitOOliicii 800141 WORKBerniird-Riiss, Ph.D.; Dean,
REGIONAL' RESEARCH- INSTITUTEArthur C4Mien, Ph.D., Director
Research and Training CenterRegional Research InstitutePortland Sate UniversityP.O. Box 751-
Portland, Oregon" o7267-
(03)12940o'
Copyright©1941 by Regional Research
Institute
All Rights Reserired
We invite our audience to submitletters and comments.
FROM THE EDITOR
This is the first issue of a bulletin published bythe Portland State University Research andTraining Center to Improve Services forSeriously Emotionally Handicapped Childrenand Their Families. The center is funded bythe National Institute for Handicapped Research(NIHR) and the National Institute of MentalHealth (NIMH).
The primary activities of the center are:
1. to conduct research on ways of improvitigservices to help emotionally handicappedchildren and youth to live at home, learn inschool, and succeed at paid employment;
2. to develop training materials and programsfor professionals, parents and employers;and
3. to serve as a resource center for otherindividuals and organizations working onbehalf of emotionally handicapped childrenand their families.
The specific thrust of this initial publicationis to introduce you to the center and its primaryactivities. There are three major center projects:Families as Allies, Youth in Transition andTherapeutic Case Advocacy. Each of theseprojects is described in separate articles in thisissue of the newsletter. In addition, we have alead article by Tom Young titled "Re-ThinkingEmotional Disturbances in Children." This arti-c!,3 should be thought provoking and we hopethat it will elicit thoughtful responses to theissues raised by Dr. Young.
It is our intent to publish the bulletin on aquarterly basis. Each issue will revolve arounda specific subject area. We plan to elicit guestarticles related to the primary subject area ofthe newsletter. For example, the next bulletinwill address issues of parent-professional collab-oration in providing services to seriously emo-tionally handicapped children and youth. Moredetail is provided on page 5. We are excitedabout the progress of the Research and TrainingCenter and its activities. We invite your com-ments and criticisms regarding the issues andconcerns raised in this pc,' *.ication.
3
2 FOCAL POINT Fall 1986

CENTER PROFILESI
THERAPEUTIC CASE ADVOCACYPROJECT
The Therapeutic Case Advocacy (TCA)Project is in its second year and has beenwarmly received by a variety of agencies,organizations and institutions that servemany of Oregon's seriously emotionallyhandicapped youth and their families.The project is developing a model fordelivering services to this populationwhich combines three intlgral compo-nents:
1. case management;2. case advocacy; and3. interpersonal therapeutic skills.
The goal of the service delivery model isto provide a "system of care" for eachcase that comprehensively addresses theneeds of emotionally handicapped youthand their families.
It became apparent quite early in theproject that a model would need to beapplicable in more than one context.Hence, a model of therapeutic case advo-cacy, while utilizing the aforementionedcomponents, must have the flexibility tomake its appeal fairly widespread.
Two separate contexts were establishedfor developing such a model: one ap-proach involves structuring the model foruse within a given agency (e.g., childwelfare, juvenile justice, public school, ora mental health facility); and a secondapproach involves a model that can oper-ate among a variety of agencies whichserve a given client.
Both approaches of the model are be-ing developed in conjunction with indi-viduals and agencies who have had ex-tensive experience in serving this trou-bled population. This will help facilitatethe transition of therapeutic case advo-cacy from a conceptual or theoreticalperspective to a practical or applicableset of procedures.
The model and its development willalso benefit by receiving input from anational, as well as a local, advisorypanel--each group possessing a broadrange of expertise in serving emotionallyhandicapped youth. Included among local
advisors are an attorney, an advocate, astate hospital outreach coordinator, amental health facility executive director.an administrator from the county juve-nile court, a county mental health pro-gram specialist, and a unit manager fromthe local branch of the state Children'sServices Division. This range of repre-sentation will help in the formation andutilization of therapeutic case advocacylocally.
In any form of therapeutic case advo-cacy the idea of restructuring the youth'senvironment and related role players isof key importance. This does not implyforsaking the search for a medical orpsychological cure; however, it presentsthe system of care approach as the pri-mary focus of treating the emotionalhandicap.
The individuals and agencies withwhom we are working have graciouslywelcomed the project. Collaboration willallow the development of a viable modelof therapeutic case advocacy which uti-lizes techniques and practice skills al-ready mastered by professionals. There-fore, collaboration will permit an easytransition from the drawing board to ac-tual service delivery. Moreover, workingcollaboratively enhances the project's po-tential to identify and access resources,to identify systemic barriers to goodpractice, to expand networks and work-ing relationships, and to provide techni-cal assistance to local service providers.This has created an enthusiasm amongadministrators, managers, and line staffin youth and family serving agencies.
Currently several projects are in theworks. Our model of therapeutic case ad-vocacy is being tested in a child welfare
A comprehensive systemof care approach for treatingemotional handicaps
FOCAL POINT Fall 1986 3

agency and will be tested in two mentalhealth facilities in the near future.Drafts of the TCA Worker's Handbook, theTCA Workbook and the TCA Manual areavailable. These materials will undergo ayear of field testing and will be revisedto reflect our experiences in the field.An outline of the TCA Parent's Guide hasbeen developed and the first draft of thisguide is available as well. An annotatedbibliography of advocacy has been pub-lished and is available through ourResource Service; addendums will beavailable as the bibliography is expanded.The project staff is making plans for aTCA Training Videotape that could beused by workers across disciplines andfields of practice. This videotape mayprove valuable to parents and families ofseriously emotionally handicapped child-ren and will be available in mid-1987.
The future of the project will involveevaluation of the model of therapeuticcase advocacy and the efficacy of thetraining materials produced. This evalu-ation of the model and training materialswill not be restricted to the Oregon com-munity. indeed, to insure that the modelwill have widespread appeal, test sitesare currently being considered outsideOregon. Conceptually the approach ap-pears both viable and cost effective; how-ever, generalizing the results must occurto determine reliability, validity andoverall credibility of the model.
YOUTH IN TRANSITION PROJECT
The Youth in Transition (YIT) Project isa relatively new undertaking of theResearch and Training Center. The pro-ject was initiated during the 1985-86funding year. The original intent of theproject was to employ a psychologicalrehabilitation model developed by Dr.William Anthony and his associates atBoston University's Center for Rehabili-tation Research and Training in MentalHealth. While designed for use withadults, we wanted to explore the model'sapplicability to adolescents who areemotionally handicapped and in the pro-cess of moving from youth serving sys-tems to adult roles in the community. Asthe YIT project has evolved during thepast year and our awareness of the tran-
sition issues faced by emotionally handi-capped adolescents and their families hasincreased, our conceptualization of tran-sition programming and interventionstrategies which have an impact on theservice needs of this population hasbroadened.
The psychiatric rehabilitation modelcontinues to serve as a guide for the YITProject. However, a literature review ofalternative models of service deliveryrevealed that the psychiatric rehabilita-tion model was only one of many ap-proaches available which may be employ-ed with emotionally handicapped adoles-cents in transition.
In addition, important issues haveemerged which will influence the natureof our work and the eventual products ofthe project. These issues include:
1.
2.
3.
4.
an increased awareness of the varietyof transition programs and ap-proaches currently being used byprofessionals in special education,mental health and vocational settingswith the developmentally disabled;the need for an articulated transitionphilosophy to be used by state andprogram planners as a guide fortransition services;the need for an initial assessment ofexemplary transition programs in or-der to refine the concept of transi-tion oriented services for emotionallyhandicapped adolescents; andthe lack of literature oriented to thetransition needs of emotionally hand-icapped adolescents.
Programming andintervention strategies foremotionally handicappedadolescents moving fromyouth serving systems toadult roles
4 FOCAL POINT Fall 1986 5

The concept of transition is complex and t 2.must be addressed from a variety of per-spectives. We are defining transition as aprogressive, developmental process to-wards the assumption of adult role re-sponsibilities. Inherent in this definitionare the accomplishment of adolescent de- 3.velopmental tasks and the acquisition offunctional skills for role assumption inthree primary environmental dimensions.These dimensions include:
1. the social and interpersonal environ-ment;
2. the employment and/or educationalsetting; and
3. the daily living environment(Halpern, 1979).
We view these three environmental di-mensions as interrelated and inseparablewhen designing and implementing transi-tion oriented programs. Transition pro-grams must address all three dimensionsin the services which are provided, andmust be anchored in terms of teachingand skill building towards the next pro-gressive step in the transition process. Inessence, transition programs must be out-come oriented rather than cure or symp-tom oriented. In addition, many adoles-cents who are emotionally handicappedface a second transition: from institu-tional settings to community alternatives.
The professional literature is beginn-ing to indicate that in order to minimizere-institutionalization, the most normal-ized community opcions must be used.This information directs us to the needfor a transition oriented philosophythroughout the system of care for chil-dren, adolescents and their families,which has implications for both profes-sionals providing services to this vulner-able population and planners designingservice delivery programs.
Our proposed activities for the 1986-1987 project year will address areas ofadvocacy, information dissemination, andan intervention based philosophy andconceptualization of transition orientedservice delivery. Specifically, next year'sproject goals are:
1. to advocate for the incorporation oftransition oriented services at boththe planning and program levels ofservice delivery;
to continue refinement and beginevaluation of a transition orientedphilosophy and intervention modelthat address the transition needs ofemotionally handicapped adolescentsand their families; andto provide state and treatment pro-gram consultation in order to coordi-nate a transition oriented approachbetween special education, vocationalrehabilitation, mental health, childwelfare, and juvenile justice agencieson behalf of emotionally handi-capped adolescents.
An annotated bibliography describingtreatment programs, curriculum strategiesand intervention approaches to impactthe transition needs of adolescents is nowavailable. Program planners will find thisinformation helpful in designing transi-tion programs. A transition oriented phi-losophy guided by a principal based ap-proach to service delivery will be imple-mented in a residential program in thePortland area this fall. An evaluationmechanism will be part of this project inorder to assess the initial viability of theapproach. This information will be help-ful to further articulate the conceptof transition as it applies to the emotion-ally handicapped adolescent.
Reference
1. Halpern, A.S. (1979). Adolescents andYoung Adults. Exceptional Children,45 (7), 518-523.
FAMILIES AS ALLIES PROJECT
The Families as Allies Project reflects aparticular set of beliefs about what therelationship between professionals andfamilies of seriously emotionally handi-capped children should be. The project isdesigned with the idea that the interestsof these children will be best served iftheir parents and the service providerswith whom they are involved work to-gether as partners on their behalf. Thiscollaboration should focus on developingthe very best educational and treatmentprogram for each child within the bestpossible service delivery system that canbe put together.
6FOCAL POINT Fan 1986 5

Background
Relationships between parents andservice-providing professionals hrtvetaken many forms over th.., years. Sincethe first recognition that emotional dis-turbance can and does exist amongchildren, ideas about the causes andproper treatment of emotional disordershave influenced the relationshipsbetween professionals and familymembers. .
Different theories about the etiologyof emotional handicaps cast parents in avariety of roles, both as perceived byhelping professionals and in their owneyes. For example, explanations of causethat emphasize the importance of earlychildhood experiences tend to portrayparents as (usually unwitting) villains.In other words, parents have somehow,out of ignorance or even malice, eitherfailed to create the conditions necessaryfor the optimum growth of their child, orhave allowed damaging events to be apart of the child's experience. From thispoint of view it may be difficult for pro-fessionals, who have cr isen to dedicatetheir lives to other people's children, tosee parents as other than sick or, at best,inadequate. Interventions developed fromthis perspective range from familytherapy strategies designed to changepathological family patterns to actionssuch as removing children from their(presumably pathogenic) homes. Parentsas well as their children may be seen as"patients" in need of treatment. Whateversteps are taken, a result of this perspec-tive for many families may be a sense ofguilt and shame associated with thebelief that they have somehow causedtheir child's problems. Additionally,parents may feel misunderstood,alienated and, at times, resentful ofprofessionals' attitudes and actions.
In contrast, theories featuring anorganic explanation for childhood emo-tional disorders often cast the parents,along with their children, as unfortunatevictims of poorly understood biologicalmalfunctions. In this scenario, parents arclikely to be seen as potential "clients" inneed of service and support. The linkbetween theories of causation, models oftreatment and the way parents andprofessionals relate to each other may not
II be as direct as is suggested here, and it iscertainly not as simple. The main point,however, cannnot be denied: the rela-tionship between parents of seriouslyemotionally handicapped children andrepresentatives of the helping professionshas often been uneasy. Parents havelooked to experts for answers andsolutions and have been disappointed.Professionals have often been frustratedby what appears to them to be a lack ofmotivation, resistance to treatment, orother uncooperative behavior on the partof family members.
The Families as Allies Project is aimedat achieving a more balanced and pro-ductive relationship between familymembers and service providing profes-sicaals. The project is designed to studythe parent-professional relationship andto develop and teach ways thatprofessionals and family members canjoin forces to promote positive changefor children.
With regard to the etiology of emo-tional handicaps, the Families as AlliesProject does not embrace a particularperspective or theoretical orientation. Theevidence to support any theory is farfrom overwhelming. In addition, know-ledge about causation is often irrelevantto the development of ways to promotethe growth and rehabilitation of handi-capped children and adolescents. Theproject does, however, operate from anassumption with regard to theories thatmay cause professionals to blame parentsor parents to blame themselves for achild's misfortune: even if they are true,they are not useful.
Parent-professionalcollaboration towardimproving services forseriously emotionallyhandicapped children andtheir families
76 FOCAL POINT Fall 1986

Project Activities
Survey of Parent Organizations. We havecompleted a nationwide survey of self-help, support and advocacy groups thatinclude parents of seriously emotionallyhandicapped children among their mem-bers. We conducted telephone interviewswith over 200 groups across the country.A preliminary report of these researchfindings is available through ourResource Service.
Parent Organization Directory. Using in-formation gathered from the survey, anational directory of parent organiza-tions has been published and is alsoavailable through the Resource Service.Addendums to the directory will be pub-lished regularly as we receive infor-mation on more organizations. We thinkthc. directory will be useful to parentsand professionals alike.
Annotated Bibliography. We have com-piled an extensive annotated bibliographyof the literature addressing the relation-ship between professionals and familiesof handicapped children. The biblio-graphy also contains literature pertainingto parent self-help, support and advocacygroups. We found a wide variety ofgroups described in the published litera-ture. Some of them were organized byprofessionals; others were initiated solelyby parents. Copies of this bibliographymay be obtained through the ResourceServi;,e.
Finding Kindred Programs. Through theparent organization survey and otheravenues, we have discovered a number ofinnovative and exciting programs withgoals that complement those of ourproject. Many parent organizations con-duct training designed to help profession-als understand the needs and feelings ofparents of handicapped children. Some ofthis training is conducted jointly byparent-professional teams that model thecollaboration they advocate. We plan tofeature some of these programs is futureissues of this bulletin.
Networking. Although not included as aformal goal in the original plan for theFamilies as Allies Project, linking peoplewith common interests and needs hasturned out to be an important projectfunction. In particular, our activitiesrelated to the parent organization surveyhave stimulated a number of requests forreferrals from people who want to startparent support groups.
Curriculum Development. We recentlyfunded two curriculum developmentprojects. The Parents, Let's Unite forKids (PLUK) project of the MontanaCenter for Handicapped Children, inBillings, is developing a curriculumdesigned to promote collaboration be-tween professionals and parents and topromote systems change on behalf ofseriously emotionally handicapped child-ren and youth. A second curriculum isbeing developed by the Parent AdvocacyCoalition for Educational Rights(PACER) Center, Inc., in Minneapolis.They are producing a videotape which isalso aimed at promoting collaborationbetween parents and professionals. Bothcurricula are expected to be in place inearly 1987.
Parent-Professional Conference. In April,1986, the Research and Training Centerhosted a conference in Portland, Oregon.Its purpose was to promote collaborationbetween parents and professionals. Theconference was attended by delegationsof parents and professionals from each ofthirteen western states. These delegationsengaged in a process of developingcollaborative strategies which they havebegun to share with others and use intheir home states.
The conference format was designedto serve as a prototype for similarmeetings in other parts of the country.Such conferences are being planned forthe southeast region for the winter of1986-87, the north central region for thespring of 1987, and other regions for late1987 and early 1988.
Complete proceedings of the westernconference are available through ourResource Service. A summary of the con-ference will be featured in the next issueof this publication.
8 FOCAL POINT Fall 1986 7

Rethinking Emotional Disturbancescontinued from page 1
Where are the children considered"seriously emotionally disturbed"?
This is a serious political problem. Mostof the CASSP target population is alreadyin the care of other systems (education,child welfare, juvenile justice) with theirown legal mandates that typically do notinclude the provision of mental healthservices -- meaning typically, individual,group or family counseling/therapy by anaccredited or certified mental healthprofessional. Unless the CASSP initiative(at both federal and state levels ofgovernment) redefines what constitutemental health services, we can expectthat all CASSP will produce is a moreefficient method of referring ortransferring responsibility for seriouslyemotionally handicapped children andadolescents to existing community mentalhealth centers and state hospital units forchildren.
If, on the other hand, the mentalhealth system (through CASSP) can rede-fine what constitute "mental health ser-vices" for seriously emotionally handi-capped children and adolescents, thensubstantial collaboration with other childcaring systems may be possible. But firstCASSP will need a new mental frame-work or paradigm to replace the tradi-tional conception of mental health ser-vices for this population. This brings usto the third question or issue that CASSPmust address.
What constitutes "rehabilitation" forchildren considered "seriously emotionallydisturbed"?
CASSP has not addressed this issue ex-plicitly, only indirectly through its goalof improving services for children andadolescents with serious emotional handi-caps. But even in that context, CASSP isattempting "systems change" through itsgrants to individual states, Their objec-tives are admirable, but their strategiesmay only re-shuffle existing arrange-ments.
We think services can be improved tothe extent that they hax e the goal of cre-ating and sustaining systems of care that
4 are environmentally based, functionallyspecific, advocacy oriented and familycentered. This perspective is one thatviews the nature of rehabilitation as oneof care rather than cure. It also shiftsthe locus of anticipated change from theintrapsychic arena to the child's environ-ment.
While the goal of creating and sustain-ing a system of care for the emotionallyhandicapped child is a logical extensionof more recent understandings regardingthe nature of emotional disturbances inchildren as discussed above, it haspractical consequences as well. A systemof care approach organizes servicesaround the child rather than vice-versa.It encompasses but does not require tradi-tional notions of cure. And perhaps mostimportantly, it combines the resources ofboth natural and formal supportnetworks.
The system of care approach, then, re-defines mental health services by shiftingthe focus of intervention from the child'sinternal emotional state to the variousbehavior settings--home, school, work andplay. In each setting, the "treatment is-sue" is the extent to which those in thesetting understand and adjust to thechild's disability by providing individu-alized instruction, support and reward.But as we have noted, for most seriouslyemotionally handicapped children, thesevarious behavior settings are under thecontrol of other systems of care.
What thia means in practice will vary,of course, but the central issue is that itis the interactions between the child andeach of the living, learning, play andwork settings that bring mental health.Rehabilitation is the modification ofeach behavior setting to the point wherethe child can function at some level thatis no longer perceived as disruptive. Inconcert these modified settings constitutea system of care in which the componentsmay involve caseworkers, case managers,foster parents and family therapists fromthe child welfare system; probation offi-cers, correctional counselors, recreationalor occupational therapists and youth ad-vocates from the juvenile justice system;teachers, guidance counselors and specialeducation intructors from the educationalsystem; and relatives, friends, neighborsand clergy from the child's natural sup-
8 FOCAL POINT Fall 1986 9

port system. This brings us to the lastissue for re-thinking.
What is the role of parents andprofessionals in programs ofrehabilitation?
Historically, mental health pro-fessionals and other service providershave viewed parents as contributing tothe cause of emotional disturbances intheir children. That perspective viewedsuccessful treatment as requiring eitherremoval of the child from the parents'control and influence or treating themsimultaneously, or both. More recentawareness of tht iatrogenic effects ofremoving children from their parents fortreatment, combined with the changespractitioners have seen families capableof making in response to various familytherapy/training/education approaches,have led to a re-examination of ourundersta.;ding of parents' roles in theorigin and evolution of emotional disabil-ities in their children and of our assump-tions regarding their proper role in pro-grams of rehabilitation. Specifically,practitioners have noted that parents ofchildren with special needs rarely receivethe information they require to under-stand their children soon enough, butthat when they do, they are frequentlythe most effective advocates for theirchildren.
There is a growing awareness thatmost parents of emotionally handicappedchildren would be more willing to act as"case advocates" for their children, ifonly they could get the help they needbeing parents. The question is whetherthey can look to professionals for thathelp and get it.
The CASSP initiative is actively pro-moting the involvement of parents ofemotionally handicapped children instates' efforts to plan improvements inservices for emotionally handicappedchildren. But ultimately it would seemnecessary to promote professionals' in-volvement in helping the parents as par-ents. It seems doubly unfair to expectparents to struggle first with parentingtheir own handicapped child and then toadvocate for improvements in servicesfor other parents' children. It seems bothmore fair and more reasonable for pro-
fcssionals to collaborate with parents inboth roles and their respective tasks. Thesystem of care approach put forth herewould provide a natural opportunity forboth parents and professionals to workwith and learn from each other. Bothcould share the burden of parenting andcreating a system of care that combinesformal and natural support networks onthe individual "case" level. And perhapsboth could share the burden ofattempting advocacy at the "systems"level and sustain each other during theinevitable frustrations and disappoint-ments these efforts entail.
Beyond the issues of advocacy andparent/professional collaboration, thesystem of care approach views family-oriented efforts as essential to improvingservices for this population. Every childdeserves to have a viable family and thisis no less true for emotionally handi-capped children. In the system of careapproach, since children with specialneeds require special environments, thechild's natural family may not have thespecial resources to accommodate thechild's disability. A specialized or thera-peutic foster family home may be thespecial home environmen needed. Butthis does not mean that the child's natu-ral family should be excluded from thesystem of care. On the contrary, the sys-tem of care approach implies that while"home" and "family" need not be synony-mous, both are desirable for sustainingan ongoing system of care.
In summary, for the CASSP initiativeto succeed, it must de-mystify "emotionaldisturbances" in children by defining im-paired emotional functioning in terms ofspecific living, learning, working andplaying contexts; initiate collaborationwith other child caring systems in thecreation and maintenance of systems ofcare for each child; and reform profes-sionals' attitudes and behaviors regardingparents of emotionally handicappedchildren.
Tom Young is an assistant professor ofsocial work at Portand State University.He specializes in direct human services tochildren, youth and families. Dr. Youngserved as director of the Research andTraining Center during its first two yearsof operation.
10 FOCAL POINT Fall 1986 9
REVIEW
THE NEW YORK LONGITUDINALSTUDY
The following is a review of the NewYork Longitudinal Study, a study of be-havior disorders in children. The resultsof the study were authored by StellaChess, M.D., and Alexander Thomas,M.D., first in "Genesis and Evolution ofBehavioral Disorders: From Infancy toEarly Adult Life"1 , and subsequently inOrigins and Evolution of Behavior Disor-ders: From Infancy to Early Adult Life2.
The Study
The study, begun in 1956, followed 133subjects from early childhood to earlyadulthood. The focus of the study was toidentify and characterize temperamentalcharacteristics and to study their influ-ence on normal and deviant psychologicaldevelopment. Data sources includedparent and teacher interviews, school andbehavioral observations, clinical evalua-tions, and direct interviews with the sub-jects in adolescence and early adulthood.
Temperament was measured in ninecategories in terms of the child's activitylevel, regularity ill biological functions;response to new stimuli, adaptability,threshold of response, intensity of reac-tion, quality of mood, distractability andattention span.
Within these categories three "tempera-mental constellations" were defined: the"easy" child, the "difficult" child and the"slow-to-warm-up" child. The easy childwas characterized by regularity, positiveapproaches to new stimuli, high adapt-ability to change, and mild to moderatemood intensity which is generally posi-tive. The difficult child is characterizedby irregularity, negative withdrawal re-sponses to new stimuli, non- or slowadaptability to change, and intense moodexpressions which arc frequently nega-tive. The slow-to-warm-up child is char-acterized by negative responses of mildintensity to new stimuli, to which thechild would slowly adapt given repeatedcontact, less tendency toward
irregularity, and mild intensity ofreactions.
The following arc some of the resultsof the study:
1. significant correlations were foundbetween:
easy-difficult temperament atage three and temperament inearly adult lifeeasy-difficult temperament atage three and adjustment inearly adult lifeparental conflict at age threeand early adult adjustment in anegative directionadjustment at ages three andfive and adjustment in earlyadult liftclinical case status in childhood(e.g., adjustment disorder) andin early adult lifeclinical case status in childhoodand early adult adjustment ina negative direction
2. separation, divorce or death of aparent was not predictive of earlyadult status
3. there were no consistent correlationsbased on sex of the child
4. childhood factors which correlatedwith a high risk for relatively pooroverall adjustment and/or presenceof a psychiatric disorder in earlyadult life included: difficult tem-perament, parental conflict andprcscnrc of a behavior disorder.
These conclusions account for 34% ofthe subjects. ne authors explain thatthe differences in outcome for the re-maining 66% may lie in either variablesnot rated in the study or in differencesin the sequences in which individualsubjects developed psychologically.
Theoretical Implications
In cases where behavior disorders devel-oped in later childhood and adolescence,a review of early childhood data did notshow symptoms of conflict and stress thatmay have led to the disorder. In view of
Continued on page 12
10 FOCAL POINT Fall 1986 11

Research and Training CenterPUBLICATIONS
$5.00
National Directory of Organizations Serving Parents ofSeriously Emotionally Handicapped Children and YouthThe U.S. organizations included provide one or more ofthe following services: education and information; parenttraining; case and systems level advocacy; support groups;direct assistance such as respite care, transportation andchild care.
FREE (one copy per address, please)
Chad Advocacy Annotated BibliographyIncludes selected articics, books, anthology entries andconference papers written since 1970, presented in amanner useful to readers who do t'ot have access to thecited sources.
Annotated Bibliography. Parents of EmotionallyI kndicapped Children: Needs, Resources, andRelationships with ProfessionalsCovers relationships between professionals and parents,parent self-help, support and advocacy groups, parentparticipation, parents' problems and guidelines.
Annotated Bibliography. Youth in Transition: Resourcesfor Program Development and Direct Service InterventionTransition needs of adolescents: educational and vocationalissues, programs and curricutrm, research overviews,interpersonal issues, skills training.
Families as Allies Conference Proceedings:Parent-Professional Collaboration Toward ImprovingServices for Seriously Emotionally I kndicapped Childrenand Their FamiliesHeld in April 1986 and attended by delegations Promthirteen western states. Includes: agenda, presentationtranscriptions, biographical sketches, recommendations,worksheets, and evaluations.
Gathering and Sharing: An Exploratory Study of ServiceDelivery to Emotionally Handicapped Indian ChildrenFindings from Idaho, Oregon and Washington, coveringcurrent services, successes, service delivery barriers,exemplary programs and innovations.
Checks payable to: Regional Research InstituteMail order to: Research and Training Center, RegionalResearch Institute, Portland State University, P.O. Box751, Portland, Oregon, 97207, (503) 229-4040
Research and Training Center
ORDER FORM AND MAILING LIST
Please send me the publications indicated above. $ enclosed as appropriate.
Add me to your mailing list. Take me off your mailing list.
Change my address as noted below.
List my organization in the national directory. (The Research and Training Center will contact you.)
NAME
ORGANIZATION
CrrYSTATEMP
MEM IONE
CHECKS PAYABLE TO: Regional Research InstituteMAIL TO: Resource Services Coordinator, Research and Training Center, Regional Research Institute,Portland State University, P.O. Box 751, Portland, Oregon 97207, (503) 229-4040
1 2

Continued from page 10
this, the authors question Freud's theorythat neuroses are acquired only duringearly childhood.
The data do not support the theorythat anxiety plays a primary role in thedevelopment of behavior disorders.Anxiety appeared to be a consequencerather than a cause of behavior disorders.
The concepts of goodness/poorness offit and consonance and dissonance wereuseful in tracing individual developmen-tal sevences. The authors conclude that"excessive stress resulting from poornessof fit between environmental expecta-tions and demands and the capacities ofthe child at a particular level of devel-opment...leads to disturbed behavioralfunctioning" (Thomas,1984a).
Practical Implications
"Parent guidance" was used to improvethe goodness of fit for childhood clinicalcases. The emphasis of parent guidance isto effect a change in the behaviors andovertly expressed attitudes of the parents
as well as altering other unfavorableenvironmental influences. This techniquegenerally required only a few sessionsand was found to be quite effective inthe majority of cases. With few excep-tions, the recovery lasted throughoutadolescence and early adult life.
The study offers a hopeful view ofhuman development. Emotionally handi-capped children can be helped. Familypatterns and behavior can be refashionedand preventitive and theraputic interven-tions can produce change amoi.g all agegroups.
References
1.
2.
Thomas, A. and Chess, S. (1984).Genesis and evolution of behavioraldisorders: From infancy to earlyadult life. Reprint from AmericanJournal of Psychiatry, 141 (1), 1-9.Chess, S. and Thomas, A. (1984). Ori-gins and Evolution of Behavior Dis-orders: From Infancy to Adult Life,New York: Bruner/Mazel, Inc.
Research and Training CenterRegional Research InstitutePortland State UniversityP.O. Box 751Portland, OR 97207
,.0
Nonprofit Org.U.S. Postage
PAIDPortland, ORPermit #770

WINTER 1987
Families as All ConferenceThe Families as Allies Conference was held inPortland, Oregon, on April 28 and 29, 1986. Themission of the conference was to promote col-laborative working relationships between profes-sionals and parents of seriously emotionallyhandicapped children and adolescents. Designedas a working conference, parents and profes-sionals from thirteen western states were invitedto attend. Representatives from the followingstates participated: Alaska, Arizona, California,Colorado, Hawaii, Idaho, Montana, Nevada, NewMexico, Oregon, Utah, Washington andWyoming.
While the composition of each state delega-tion varied, the goal was to assemble state dele-gations composed of:
(1) policy-making, administrative and servicedelivery professionals from the major publicsystems that serve emotionally handicappedchildren and youth, i.e., mental health, childwelfare, juvenile justice, education andvocational rehabilitation;
(2) private service providers; and(3) parents of emotionally handicapped children
and adolescents.
Each delegation was encouraged to meet prior tothe conference.
The keynote address was given by SusanDeConcini. Ms. DeConcini is a practicing socialworker in the mental health field and is a childcare advocate. The keynote speaker's theme ofmutual respect helped set the tone for parent-professional collaboration and for much of thework that occurred during the rest of the con-ference. She noted, "It really is a partnership--ajoining of hands toge0 so that everybodywins." Parents of em .,.ionally handicapped chil-dren are desperate for information about emo-tional problems and are eager to learn copingskills. Open communication between parentsand professionals is essential. Subsequent
speakers, panelists, and workshop leaders pro-vided conference participants with boththought-provoking commentary and with ideasthey could adapt to their own circumstances.
Obstacles to parent-professional collabora-tion were explored during the first day of theconference. Theories of etiology of mental ill-ness of ten unwittingly cast parents as villainsand are a serious obstacle to parent-professionalcollaboration. These beliefs lead to profession-als blaming parents, holding them responsibleand viewing them as pathogenic agents. Simi-larly, parents often also believe they are toblame for their children's problems. This beliefmay lead to guilt, shame, fear and avoidance ofmental health professionals, teachers, and others.
Professionals tend to view children's needsand problems from within the context and ca-pacities of the agency in which they are em-ployed and within a relatively short time frame.
Continued on page 3
Keynote speaker Susan DeConcini. (Photo by Tom Young.)
The Bulletin of the Research and Training Centerto Improve Services for Seriously Emotionally Handicapped Children and Their Families
VOLUME 1 NUMBER 2
1 4

FROM TIM EDITOR
This issue of Focal Point features the Families asAllies Project, which is designed to promotecollaboration between families of children withemotional handicaps and the professionals whoserve them. Project objectives include conduct-ing relevant research, developing training cur-ricula and other written materials, and de-signing and presenting workshops and othertraining events.
Included in this issue is a report about anApril, 1986 conference held in Portland that in-volved equal numbers of parents and profes-sionals from thirteen western states. This meet-ing was one of the first public explorations ofour project concepts, and we were very gratifiedby the positive response of most participants.
As a part of our research program, we arecurrently conducting a survey in which we askparents about their experiences seeking and ob-taining services for their children. We are alsoinvolved in a search for innovative programsand faculty within professional schools that en-courage professionals to work collaborativelywith parents.
Curriculum development activities of theFamilies as Allies Project are also featured.Among these, we are happy to announce theavailability of training materials developed bytwo parent organizations through an agreementwith the Research and Training Center.
Because one purpose of Focal Point is toprovide a forum for various points of viewabout important issues regarding children andtheir families, we are pleased to include an es-say by Ira Lourie, M.D. and Judith Katz-Leavy,M. Ed., of the Child and Adolescent Service Sys-tem Program (CASSP) Branch at the NationalInstitute of Mental Health (NIMH). The essayconstitutes a response to an article by ThomasYoung, Ph.D., published in our last issueentitled, "Re-Thinking Emotional Disturbance."We hope that other readers will be stimulated toexpress their ideas regarding these and otherimportant issues related to the mental healthneeds of children and their families.
RESEARCH AND TiZATNLNGCENTERRegional Research Institute for
Human ServicesPortland State UniversityP.O. Box 751Portland, Oregon 97207(503) 229-4040
Copyright Co 1987 By RegionalResearch Institute for HumanServices. All rights reserved.
We invite our audience to submitletters and comments.
RESEARCH AND TRAININGCENTERBarbara J. Friesen, Ph.D., Director
Families as Allies ProjectBarbara J. Friesen, Ph.D., Principal
Investigator
Therapeutic Case Advocacy ProjectThomas M. Young, Ph.D., Principal
InvestigatorJames L. Mason, B.S., Project Manager
Youth in Transition ProjectMatthew J. Modrein, Ph.D., Principal
Investigator
Resource ServicesMarilyn C. McManus, J.D., Coordinator
Focal PointMarilyn C. McManus, J.D., Editor
Center AssocatesTerry E. Butler. B.A.Paul E. Koren, Ph.D.Loretta Norman, B.A.Douglas C Overly .k, B.A.A. Christina Rutland, B.S.E. Darey Shell, B.S.Janis K. WorthingtonKatie S. Yoakum, B.S.
GRADUATE SCHOOL OF SOCIALWORKBernard Ross, Ph.D., Dean
REGIONAL RESEARCH INSTITUTE FORHUMAN SERVICESArthur C. Emlen, Ph.D., Director
NATIONAL ADVISORY COMMITTEE
Mary Hoyt, M.S.W., Chair, Oregon StateHospital, Child and Adolescent Unit
Richard Angel, M.D., Department ofPsychiatry, Oregon Health Sciences University
William Anthony, Ph.D., Center forRehabilitation Research and Training in MentalHealth, Boston University
William Arroyo, M.D., Assistant Director,Child/Adolescent Psychiatry, Los AngelesCountyUSC Medical Center
Marva Benjamin, M.S.W., ElahanCommunity Mental Health Center,Vancouver, Washington
Betsy Burke, Ph.D., Chief, SpecialPopulations, California State Departmentof Mental Health
Lee Clark, Ph.D., EmotionallyHandicapped Programs, Bureau of Educationfor Exceptional Students, FloridaDepartment of Education
Glenda Fine, Parents Involved Network,Mental Health Association of SoutheastPennsylvania
Bud Fredericks, Ed.D., Teaching Research,Inc., Western Oregon State College
Paula Goldberg, PACER Center, Inc.,Minneapolis, Minnesota
Mareasa Isaacs, Ph.D., AssociateCommissioner for Children and Youth,New York Office of Mental Health
Phyllis Magrab, Ph.D., Director, ChildDevelopment Center, GeorgetownUniversity
Barbara Melton, B.S., Monmouth, Oregon
Larry Platt, M.D., Office of the RegionalHealth Administration, U.S. Public HealthServices, Region IX
Ann Turnbull, Ph.D., Bureau of ChildResearch, The University of Kansas
2 FOCAL POINT Winter 1987 15

CONFERENCE continued from page 1
Parents, on the other hand, have an ability tosee the many needs of the child and the family,and thus the need for a wide range of servicesover a longer time span. Parents, however, maylack the knowledge and skills to put together along term comprehensive plan unassisted.
Professionals and parents are further con-strained by the requirement that professionalsoperate within agency policy and within thelimitations imposed by funding sources. Agencypolicies and funding requirements are often im-pediments to the delivery of appropriateservices to emotionally handicapped children.
The second day of the conference was de-voted to developing strategies to overcome bar-riers to parent-professional collaboration. Pan-elists emphasized the importance of parent em-powerment, the necessity for professionals toexamine their attitudes toward parents and toview them as equals, and the value of parents'equipping themselves dth the knowledge andskills needed to function as equal partners. Onepresenter urged that we re-examine the theoriesabout the causes of emotional disturbance thatlead us to blame parents.
Additionally, a multicultural project thattrains parents to serve as trainers and that as-sists parents to assume leadership roles, as wellas a project to develop parent support groupsand services for military families werepresented by panel members.
Following the presentations, members ofstate delegations met together to develop actionplans and strategies for implementation upon re-turn to their home states. Planned activities in-clude efforts to better coordinate the activitiesof existing statewide advocacy groups, commit-ments to establish parent support groups in spe-cific cities or regions, development of resourcedirectories, establishment of parents-training-parents capabilities, development of parenthandbooks, publishing newsletters, and engagingin legislative advocacy.
Nationally, four regional Families as Alliesconferences have been scheduled. For moreinformation, contact the following:
GREAT LAKES/APPALACHIAN REGIONALCONFERENCEIllinois, Indiana, Kentucky, Michigan, Minnesota,
Ohio, Tennessee, West Virginia, WisconsinIlp June 27 and 28, 1987
Bloomington, IndianaJim Killen (317) 232-7888 [IN]Dagmar Plenk (608) 266-2712 [WI]William Scott (502) 564-7610 [KY]Donna Simonson (217) 785-2561 [IL]
MIDWEST REGIONAL CONFERENCEArkansas, Iowa, Kansas, Missouri, Nebraska, NorthDakota, Oklahoma, South Dakota, TexasMay 13 and 14, 1987Overland Park, KansasRock Richardson (405) 521-0044 [OK](Arkansas, Oklahoma, Texas)Art Sands (913) 296-3774 [KS]Kansas, Missouri, North Dakota)Jose Soto ( '1) 471-2851 [NE](Iowa, Nebraska, South Dakota)
NORTHEAST REGIONAL CONFERENCEConnecticut, Delaware, Maine, Massachusestts, NewHampshire, New Jersey, New York, Pennsylvania,Rhode Island, Vermont, Virgin IslandsMay 20 and 21, 1987Albany, New YorkMary Armstrong (518) 474-8394 [NY]Lenore Stern (717) 783-8335 [PA]Joyce Wale (609) 987-2005 [NJ]
SOUTHEAST REGIONAL CONFERENCEAlabama, District of Columbia, Florida, Georgia,Louisiana, Maryland, Mississippi, North Carolina,South Carolina, VirginiaJune 12 and 13, 1987Mobile, AlabamaDonna Glass (205) 271-9261 [AL]Lucy Leslie (601) 359-1301 [MS]
Panelists Glenda Fine, Richard Donner and Cindy Boatman.Topic: Obstacles to Parent-Professional Collaboration. (Photoby Tont Young.)
Winter 1987 FOCAL POINT 3C

Update of StatesInvolved in the Families as Allies Conference
Alaska - Post-conference activities in Alaskahave addressed two areas:
(1) parent involvement and support at aresidential treatment facility; and
(2) governmental lobbying efforts.
A bi-weekly parent support group has beenestablished at a residential treatment facility inJuneau. Parents of children served by thisresidential treatment facility will serve on theagency's board of directors on an ongoing basis.One member of the Alaska delegation has metwith the state's CASSP project manager onseveral occasions, and has worked withlegislators on an upcoming bill to establish anAlaskan children's trust fund, and also met withmany candidates prior to the November electionto discuss issues affecting children and youth.
Arizona - Members of the Arizona delegationhave not met on a formal basis. Thecoordinator of the Arizona delegation did,however, meet with the state hospital's youthcoordinator and discussed the goals of theFamilies as Allies Conference. The governor'srepresentative on children, youth and families,as well as other gubernatorial staff members,will be included in future efforts to improveparent and professional collaboration.
California - California was unable to send aformal delegation to the Portland conferencebecause of scheduling conflicts. The relevantprofessionals in the state were meeting at thesame time as our conference to work on issuesof interagency collaboration in deliveringservices to emotionally handicapped childrenand their families. This same group plans tomeet again in the Spring of 1987, at which timethe issues of parent-professional collaborationwill be discussed. California has funded ademonstration project in Ventura County todevelop a model of service delivery to seriouslyemotionally handicapped children and theirfamilies.
Colorado - The group representing Colorado atthe conference has not met on a formal basis.However, the Department of Mental Health is
initiating the planning meetings for a forum tobe held in the Spring of 1987. The planners areseeking to identify people throughout the statewho share an interest in advocacy efforts andchildren's issues. These individuals will beinvited to attend the forum. The objectives areto:
share information on advocacy efforts;Identify children's and families' needs;identify obstacles to parent-professionalcollaboration;plan for establishment of a broad-basedconstituency; and,form task groups to work on establishingstate and local advocacy groups.
Additionally, the Department of Mental Healthis formulating plans to replicate the Families asAllies Conference for Colorado parents andprofessionals.
Hawaii - Hawaii is a CASSP state with a strong 0interagency network in place. The groupattending the conference included an equalnumber of parents and professionals. Thisgroup continues to meet monthly and planned aDecember Hawaii Families as Allies Conference.The conference was modeled on the Port.andeffort, and encouraged participants to attend asparent-professional teams. In addition, theCASSP project has hired a Parent Coordinator,Ginny Wright.
Idaho - Idaho's CASSP staff has taken numeroussteps to improve parent-professionalcollaboration within the state. These effortsinclude:
(1) the identification of parents of emotionallyhandicapped children;
(2) parent and professional participation inregional needs assessment surveys toidentify the essential components of anIdaho treatment delivery system;
(3) coalition building meetings held in each ofIdaho's seven regions with parents, mentalhealth professionals, teachers and serviceproviders;
4 FOCAL POINT Winter 1987
17
I

(4) a statewide CASSP conference involvingadministrators, parents and professionalsheld in Sun Valley in October; and
(5) publication of the first two issues of astatewide newsletter. One page of eachissue of the newsletter will be devoted to aneditorial written by a parent or to thediscussion of parent issues.
Montana - The Montana delegation to theConference formed their own organizationcalled Montana Families as Allies. SinceMontana is a large state geographically, andeach of the five parents were from differentcities, the group has not been able to meet.However, the state coordinator is incommunication with local coordinators toencourage local efforts, perhaps in conjunctionwith existing groups or organizations. The statecoordinator (a parent) is the only consumer on astate task force charged with devising a legaldefinition of emotional disturbance forpresentation to the state legislature. She hasalso written an article for the Montana MentalHealth Association Newsletter.
Nevada - The members of the Nevada delegationdisseminated a brief press release to key stateand local professionals in which they describedthe Families as Allies Conference. Thestatement identified the lack of interagencycoordination as the most pressing problemhampering the provision of services to thestate's emotionally handicapped children.Delegation members have not formally met sincethe conference.
New Mexico - The New Mexico delegation hasmaintained contact with each other. They areworking on two projects designed to help createa statewide network for parents. The first isthe production of a videotape created by aparent group. The videotape will tie used foroutreach to parents living in rural areas of thestate. The second project is the purchase ofspace in the New Mexico Alliance for theMentally Ill newsletter dedicated to children'sissues. Both projects are funded by the MentalHealth Bureau.
Oregon - Three support groups for parents ofchildren with emotional handicaps have startedsince the April conference. These groups are
located in Portland, Lake Oswego, andMonmouth. The Monmouth group has nameditself Families and Children Together (F.A.C.T.)and is seeking support from the Mental HealthAssociation of Oregon. The Oregon MentalHealth Division (OMHD) has recently namedFaye Lindemann-Tayler as the Coordinator ofPrograms for Children and Adolescents. Thisappointment should increase the emphasis givento children's mental health issues in the state.This is the first time in many years that anOMHD position has been devoted exclusively tochildren's issues.
Utah - One member of the Utah delegation metwith the state's Interagency Commission andthereafter arranged for the director of the UtahParent Center to meet with the Commission. Asa result of these meetings, agencies will nowrefer parents to the center. The center willserve as the focal information center and willdirect parents to the appropriate resource.
Washington - A follow-up meeting to thePortland conference was held in the Fall of1986. The action plan developed by the statedelegation was updated and revised. The planincludes a statewide parent-professionalconference in the second or third year ofWashington's CASSP activities. The WashingtonCASSP staff is conducting ongoing discussionswith established advocacy groups in the state toassist with their advocacy efforts and to developstrategies for working together. Three parentsserve on the state's CASSP Coordinating Council.In addition to the experience and skill he bringsto the position, the newly appointed assistantCASSP Project Director is the parent of apsychiatrically disabled child.
Wyoming - The Wyoming delegation has not metas a group. One member of the delegation, whohas since moved out of the state, made a publicpresentation in which she discussed theconference.
Winter 1987 FOCAL POINT 5

A Perspective on Rehabilitative ServicesWithin the Child and Adolescent Service System Program
byIra S. Laurie, M.D. & Judith Katz-Leavy, M.Ed.
In the lead article of the premier issue of FocalPoint, Dr. Thomas Young challenges some of thebasic concepts of the Child and Adolescent Ser-vice System Program (CASSP). Dr. Young feelsthat the terminology of "severely emotionallydisturbed" children aad adolescents will focustoo strongly on the mental health aspects of thechild's service needs and will lead to the devel-opment of a narrow system of care and a focuson behavior as perceived by parents and teach-ers. He does this in face of the reality that"severely emotionally disturbed" (SED) is an ed-ucational term that is not found in the mentalhealth literature. This term has been adoptedby CASSP as an alternntive to the concept usedin mental health to describe this population ofchronically mentally ill children and adoles-cents. The national work group brought to-gether to develop CASSP chose this definition inan attempt to demonstrate the need for a broadbased continuum of care similar to the one thatDr. Young suggests is needed.
Dr. Young implies that only by adopting arehabilitative model will CASSP be able tocreate the appropriate continuum of care. Inthe service of this conceptualization he statesthat the Portland R&T Center has changed itsown terminology from "emotionally disturbed" to"emotionally handicapped," as he states, "becausewe believe it helps us shift our focus from thechild-as-problem to the context-as-solution." Onone hand; it seems that this is just a semanticquarrel which will not prove to be particularlyuseful to the field in the long run. On the otherhand, Dr. Young urges a focus on "rehabilita-tion" which we feel may well prove detrimentalto the promotion of developmentally focusedcorrective services.
The use of the term "severely emotionallydisturbed children and adolescents" by CASSPcomes from the same concerns addressed by Dr.Young. CASSP originally selected the term"seriously emotionally disturbed" (SED) to pro-vide as much consistency as possible with thecategories of eligibility used in the Education of
the Handicapped Act, P.L. 94-142. This initialdecision was indicative of CASSP's commitmentto taking a total system-wide approach to ser-vice delivery and to our acknowledging thatmental health services take many differentforms and are provided in a variety of commu-nity-based se:tings by a broad range of agenciesand providers.
In the 1983 Concept Paper on the ChildAdolescent Service Systems Program preparedby Beth Stroul, in the CASSP grant guidelinespublished annually, and again in the July 1986monograph, A System of Care for Severely Emo-tionally Disturbed Children and Youth, by Strouland Friedman, CASSP presented a set of fivebasic parameters for defining the target popula-tion. The first parameter addressed age limita-tions, and was immediately followed by thefollowing two parameters:
"The target population should include chil-dren whose emotional problems are disabl-ing based upon social functioning criteria.Level of functioning is a critical variablefor children and adolescents, determiningthe nature and level of care that is appro-priate. Degree of disability or level offunctioning in family, school and commu-nity contexts is often more meaningful thanmental health diagnosis in planning anddelivering services."
"Children and adolescents includci in thetarget population should have a multiagencyneed. Severely emotionally disturbedyoungsters require a range of services whichnecessitates the involvement of multipleagencies including mental health, health,education, child welfare, juvenile justice,and others."
Dr. Young proposes a system-wide approachto service delivery which emanates exclusivelyfrom the rehabilitation model. We, at CASSP,feel very strongly that it should not. We con-tend that there are specific problems in apply-
6 FOCAL POINT Winter 1987
19
ing the rehabilitation model to severely emotion-ally disturbed children and adolescents whichshould not go unaddressed. Rehabilitation is aconcept that has traditionally applied to adultsand physically handicapped children. In dis-cussing the World Health Organization's perspec-tive on disabilities, Dr. Young states that thePortland R&T Center is "concentrating on re-search and training activities designed to helpparents, teachers, employers and the helpingprofessions find ways of modifying living,learning and working environments to accom-modate, adjust to and compensate for childrenwith emotional disabilities." Further, he refersto "modifying environments so that children areno longer handicapped by their emotional dis-abilities in those contexts." Dr. Young appearsto view the disabilities of these youngsters asstatic, disregarding the concepts of growth anddevelopment as well as the possibility ofcorrective change.
While rehabilitation, as used in the contextof the Portland R&T Center, should be a vitalcomponent of any service system, a total focusin that area will necessarily deny appropriateoptions to those children and adolescents whohave the capacity to decrease their disabilitiesthrough growth and psychological therapy. Ourview of intervention with severely emotionallydisturbed/handicapped children and adolescentsis based on the concept of habilitation or posi-
tive change. Orthopsychiatry describes the pro-em of corrective intervention. This has beenthe traditional rallying point for child mentalhealth professionals, special educators, juvenilejustice specialists and child welfare workers foryears, and there is no indication that we shouldgive up on it now.
While rehabilitation, as discussed by Dr.Young, serves an important role in the servicessystem defined by CASSP, the practice of cur-rent rehabilitation agencies has not been childand adolescent oriented to this time. For reha-bilitation to take its proper role, there must beadjustments ii how these principles are appliedto children. This is especially true in regard tohow the needs of adolescents are met as theyprogress from the child to the adult servicesystems.
Whether we refer to disabled children as"disturbed" or "handicapped" will not deter ourjoint efforts to provide the most appropriate in-tervention along a continuum of care that in-cludes corrective therapies as well asrehabilitative solutions.
Dr Lourie is the Assistant Chief of the CommunityService Systems Branch of the National Instituteof Mental Health. Ms. Katz-Leavy is the ProgramDirector of the Child and Adolescent Service Sys-tem Program of the National Institute of MentalHealth.
Parent Organization SurveyFrom July, 1985, to February, 1986, a nationalsurvey was conducted of organizations for par-ents of children with serious emotional handi-caps. This telephone survey was carried out byregional centers of the Technical Assistance fnrParents Program (TAPP) and by staff of the Re-search and Training Center. We gathered in-formation about the history of the parentgroups, the activities and services provided bythem, their views of the current service deliverysystem, and their plans for the future. An im-mediate practical use of the information gath-ered was to publish a national directory of par-ent organizations which is available through ourResource Center.
Some highlights of the findings include:
207 (100%) parent organizations in 47 stateswere included in the survey. Noparent groups were found in Iowa,Missouri and Wyoming.
60 (29%) of the organizations have an exclu-sive focus on emotional distur-bance and do not serve or includeother disabilities. Many of theremaining organizations developedin response to P.L. 94-142 andserve families representing a widerange of childhood disabilities.
205 (99%) provide education/information ser-vices to parents. Of these, morethan three-quarters provide spe-cific information about emotional
0Winter 1987 FOCAL POINT 7

disturbance and the rights of chil-dren and families under P.L. 94-142.
184 (89%) provide parent training in such ar-eas as coping with the needs ofemotionally handicapped childrenand developing effective case andsystems advocacy skills.
177 (86%) engage in advocacy activities.131 (63%) sponsor support groups that are
available to parents of emotionallyhandicapped children and adoles-cents. Only 52 organizations(25%) provided support groups ex-clusively for parents of thispopulation.
164 (79%) provide some type of direct assis-tance to parents. These servicesinclude assistance in dealing withagencies or the public schools,child care, transportation, respitecare, assistance with food, moneyor shelter, and homemaker ser-vices.
196 (95%) provide training or other servicesfor professionals. Most frequentlymentioned were information de-signed to help professionals under-stand the needs of families andservices aimed at improving theworking relationship betweenfamily members and professionals.
Asked about future plans, respondents iden-tified the following areas as those in which theywould like to expand (as one of three choices):
Education/information for parentsSkills trainingAdvocacySupport groupsServices to improve parent-
professional relationshipsDirect assistanceOther services to professionalsCounseling for parents
1091028470
63612925
Respondents were also asked about a num-ber of service delivery system issues. Three is-sues identified by a majority of respondents asextremely important were:
There are not enough services for allchildren who need them;
Low income or lack of insurance preventsfamilies from obtaining services; and
Services are not available to children andfamilies regardless of location, i.e., geo-graphical barriers and maldistribution ofservices create an uneven system of care forthis population.
A full report of the findings of the Parent Or-ganization Survey is available through theResource Cenwr.
Parent Produced Training Materials
The Families as ft Project has funded twoparent organizations )roduce training materi-als designed to promote parent-professional col-laboration. Using videotape and a workbookformat, each product takes an informative,educational approach.
The PACER (Parent Advocacy Coalition forEducational Rights) Center in Minneapolis,Minnesota has produced a professional qualityvideotape entitled Parent's Voices: A Few Speakfor Many. Intended for viewing by profession-als, the tape features a narrator and three par-ents (all of whom have children with diagnosedemotional handicaps) discussing the experiencesthey have had seeking help for their children.The parents discuss their feelings of frustration
in their efforts to communicate with helpingprofessionals and their belief that they are of-ten left out of the treatment process. They de-scribe how poor coordination between agencies,as well as the differing perspectives of schoolsand various treatment workers, added to theproblems they were already experiencing. Al-though the program is designed with a profes-sional audience in mind, it should also be usefulfor groups composed of parents or otherinterested persons.
PLUK (Parents, Let's Unite for Kids), affil-iated with the Montana Center for HandicappedChildren, has drafted Parent Information Work-book on Emotional Handicaps. Designed as aself-teaching workbook for parents, it covers a
8 FOCAL POINT Winter 1987A
21
ei1
range of topics and seeks to increase parents'awareness and decision-making capabilities onimportant issues. One section, "Being the Parentof an Emotionally Disturbed Child," discussesthoughts and feelings parents often must faceabout themselves, their children, and the peoplearound them. Many of the comments come fromparents who have children with emotional hand-icaps. Also included are information on variousdiagnoses, types of professionals and treatments,and legal aspects of the treatment and specialeducation systems.
PLUK has also produced two completeworkshop formats in the areas of parent-profes-sional collaboration and systems advocacy. Thefirst workshop, Working Together: The ParentProfessional/Partnership, includes activities de-signed to increase the understanding profession-als and parent's have for each other's feelings,needs and limitations, an examination of roles,
and strategies to promote cooperation. Makingthe System Work: An Advocacy Workshop for Par-ents, addresses topics such as the importance ofadvocacy, power and problem-solving techniquesand strategies for making effective demands.Each set of materials includes a guide for train-ers, copies of exercises, handouts and workshopevaluation forms. The materials are designed toprovide a complete set of information and mate-rials needed for a day long workshop in eacharea. Topical modules from each workshop canalso be adapted for shorter training sessions,when needed.
These four new products should help en-hance understanding and cooperation betweenparents of seriously emotionally handicappedchildren and the professionals working to helpthem. Information about the workshopmaterials cast be obtained from the ResourceService.
NOTES & COMMENTS____.____.
SEARCH FOR INNOVATIVE PROGRAMS.CAN YOU HELP?
We are in the process of identifying innovativeprograms and materials designed to help profes-sionals learn to work collaboratively with fami-lies of emotionally handicapped children. Manyprofessional training programs focus on familiesas the target for change (placing family mem-bers in the role of patient) or stress the provi-sion of services to family members (placing fam-ilies in the client role). Our focus in this searchis on programs that feature the role of parentsas partners, or allies in the process of assess-ment, planning, implementation and evaluationof services. We want to identify programs andapproaches that can be shared with facultymembers in professional schools, and with pro-fessional organizations, parent groups, and otherinterested individuals and organizations.
Some interesting programs we have un-earthed so far include a child psychiatry train-ing program that uses parents as guest lecturers;several parent-professional workshops that userole play and role reversal to increase the empa-thy of parents and professionals for each others'perspective; and a number of written materialsthat re-examine or re-interpret traditional waysof thinking about families.
While we are most interested in programsand materials pertaining specifically to parentsof children with emotional problems, we knowconsiderable development has occurred in rela-tion to groups such as adults with long termpsychiatric disabilities, or children with condi-tions such as mental retardation or developmen-tal disabilities, chronic heaith problems, autism,or learning disabilities. We welcome informa-tion from any quarter that will help us promoteprofessional training that includes a broad defi-nition of "help" for families, and encourages fu-ture professionals to work with family membersin collaborative ways.
If you know of programs, materials, or peo-ple we should know about, please let us know.Thanks for your help!
NUM NAME CHANGE
As of October 21, 1986, the National Institutefor Handicapped Research (NIHR) changed itsname to the National Institute on Disability andRehabilitation Research (NIDRR). NIDRR andthe National Institute of Mental Health (NIMH)are the two funding sources for the PortlandResearch and Training Center.
22Winter 1987 FOCAL POINT 9

PARENT-PROFESSIONAL TRAININGPROGRAM LAUNCHED
A program to prepare parent-professional teamsto provide training to help other parents andprofessionals learn to work effectively togetherwill begin Spring, 1987. Through a contractwith the Georgetown CASSP Technical Assis-tance Center, the Families as Allies Project willprepare curriculum materials and providetraining to participants from throughout thecountry.
The trainees will be parents and profession-als identified through the regional Families asAllies Conferences scheduled for May and June,1987. During an initial week of intensive train-ing in Portland, participants will increase theirtraining skills as well as learn to present spe-cific content related to parent-professional rela-tionships, parent support groups, and advocacystrategies.
When they return to their own states andcommunities, the parent-professional trainingteams will be available to conduct workshops,provide consultation, and to teach others inter-ested in becoming trainers. They will also assistin following the progress of the state delegationsas they work to implement the state action plansdeveloped during the Families as AlliesConferences.
HAWAII FAMILIES AS ALLIES CONFERENCE
On December 6, 1986 the Hawaii Families asAllies Conference was held in Honolulu. Ap-proximately 130 parents and professionalsworked productively together, and accomplisheda great deal in the short time available. Theconference was instrumental in increasing theawareness of public officials and tile public-at-large. Portions of the general session were tele-vised by the local CBS affiliate later thatevening with an estimated viewing audience ofover 42,000. An assistant to Hawaii's new gov-ernor, John Waihee, attended most of the con-ference and participated in a small group ses-sion that was very active in identifying issuesand needs. Conference participants drafted aletter to the governor requesting a meeting witha delegation of parents and professionals.
Pursuant to their request, the Governor'sAdministrative Director met with conferencerepresentatives in January. The delegation wascomposed of representatives from the CASSP of-
f ice, the Mental Health Association, the stateChildren's Mental Health Services Branch andtwo parents. The conference representativesurged the recognition of children's mentalhealth as a state priority, discussed the need fora continuum of care and offered themselves andtheir agenc'es as resources to the Governor'soffice.
The conference was sponsored by HawaiiCASSP, the Mental Health Association inHawaii, the Office of United Self Help and theChildren's Mental Health Services Branch of theMental Health Division of the Department ofHealth. Conference planners and participantsmet with great success. The conference servedto stimulate increased activity on behalf ofchildren and families in Hawaii, and showsevery sign of being politically effective as well.
NAMI CONFERENCE TO FEATURE PARENT-PROFESSIONAL COLLABORATION
Parents and Professionals: Partners for a Changeis the title of a meeting scheduled for September15-17, 1987 in conjunction with the 1987 con-vention of the National Alliance for the Men-tally Ill (NAMI). At present, there is hope thatparent scholarship funding may become avail-able through state CASSP offices. The meeting,which will focus on families of children andadolescents, will be held at the WashingtonHilton in Washington, D.C. For more informa-tion, call NAMI at (703) 524-7600, or write tothem at 1901 North Fort Meyer Drive, Suite500, Arlington, VA 22209.
PARENT SURVEY
The Families as Allies Project plans to surveyparents of children with serious emotional hand-icaps. The purpose of the survey is to identifyparental concerns about services needed and re-ceived, about interactions with service pro-viders, and about the helpfulness of varioussources of formal and informal support. The re-sults of the survey will be used to develop in-formation and training materials to promoteparent-professional collaboration. Although thequestionnaire will be completed by parents, thecooperation of state and local organizations willbe very important to reaching a cross-section ofparents. When feasil;le, the use of a group set-ting for administration of the survey instrument 410
Continued on page 12
10 FOCAL POINT Winter 1987
23

Research and Training CenterRESOURCE MATERIALS
Annotated Bibliography. Parents of EmotionallyHandicapped Children: Needs, Resources, and Relationshipswith Professionals *Covers relationships between professionals and parents,parent self-help, support and advocacy groups, parentparticipation, parents' problems and guidelines.
Annotated Bibliography. Youth in Transition: Resourcesfor Program Development and Direct Service Intervention*Transition needs of adolescents: educational and vocationalissues, programs and curriculum, research overviews,interpersonal issues, skills training.
Child Advocacy Annotated BibliographyIncludes selected articles, books, anthology entries andconference papers written since 1970, presented in a manneruseful to readers who do not have access to the citedsources. $7.00 per copy.
Families as Allies Conference Proceedings:Parent-Professional Collaboration Toward ImprovingServices for Seriously Emotionally Handicapped Childrenand Their Families*Held in April 1986 and attended by delegations fromthirteen western states. Includes: agenda, presentationtranscriptions, biographical sketches, recommendations,worksheets, and evaluations.
Gathering and Sharing: An Exploratory Study of ServiceDelivery to Emotionally Handicapped Indian Children*Findings from Idaho, Oregon, and Washington, coveringcurrent services, successes, service delivery barriers,exemplary programs and innovations.
National Directory of Organizations Serving Parents ofSeriously Emotionally Handicapped Children and YouthThe U.S. organizations included provide one or more ofthe following services: education and information; parenttraining; case and systems level advocacy; support groups;direct assistance such as respite care, transportation andchild care. $5.00 per copy.
Parent Information Workbook on Emotional HandicapsThis self-teaching workbook for parents addresses topicssuch as parents' feelings about themselves and theirchildren, labels and diagnoses, types of professionals andtreatments, and legal issues. Single copies free to parentsof children with emotional handicaps while supplies last.All others, $3.00 per copy.
Parents' Voices: A Few Speak for Many (videotape)Thrc4 p.sents of children with emotional handicaps discusstheir experiences related to seeking help for their children(45 minutes). Brochure describes videotape and providespurchase and rental information.
* One copy free per address while supplies last.
ORDER FORM AND MAILING LIST Research and Training Center
Please send me the publications indicated above. $ enclosed as appropriate.
Add me to your mailing list. Take me off your mailing list.
Change my address as noted below.
List my organization in the national directory. (The Research and Training Center will contact you.)
NAME
ORGANIZATION
STREET ADDRESS
CITY/STATE/ZIP
TELEPHONE
CHECKS PAYABLE TO: Regional Research Institute for Human ServicesMAIL TO: Resource Services Coordinator, Research and Training Center, Regional Research Institute for Human Services,Portland State University, P.O. Box 751, Portland, Oregon 97207, (503) 229-4040
ogi., ..i

SURVEY continued from page 10
will facilitate completion of the questionnaire aswell as provide help to parents in interpretingthe questions. In addition to using the surveyresults for training curriculum development, theresults may augment needs assessment informa-tion rclatcd to services for seriously emotionallyhandicapped children in individual states. Par-ents willing to participate in this survey shouldcontact us directly by writing the Families asAllies Project. Your help will be appreciated.
OFFICE BURGLARY
Our offices were burglarized over the holidays.Five computers were stolen. One computer con-tained the Focal Point mailing list on its harddisk. Fortunately, the bulk of the list wasbacked up; however, some later changes to thelist were lost. We have reconstructed the list tothe best of our ability, but some information(such as changes in address) may have been lost.Please bear with us and send any address or per-sonnel changes to us again. We apologize for theinconvenience.
FOCUS: THERAPEUTIC CASEADVOCACY
The Therapeutic Casc Advocacy Project isdeveloping a model to deliver services to se-riously emotionally handicapped youth andtheir families. The model coordinates theefforts of youth serving systems, organiza-tions and agencies as well as the informalsupports in the client's environment. Clientcentered systems of care arc establishedthrough case advocacy, interpersonal inter-ventions and care management. Collabora-tion at the case, organizational and inf:er-agency levels is an integral aspect of theconcept.
The next issue of Focal Point will fea-ture the Therapeutic Case Advocacy Pro-ject. We arc interested in hearing aboutsimilar models of interagency collaborationat the local level and would like to high-light them in our next issue. If you knowof programs or models with similar ap-proaches, please notify: James L. Mason,Therapeutic Case Advocacy ProjectManager.
PORTLAND STATE UNIVERSITYResearch and Training CenterRegional Research Institute for Human ServicesP.O. Box 751Portland, Oregon 97207
25
Nonprofit Org.U.S. Postage
PAIDPortland, ORPermit #770

4* INK
RECEIVED OCT U 6 IS67
Spring/Summer 1987
Therapeutic Case Advocacy: A SummaryTherapeutic Case Advocacy (TCA) is oneapproach to helping emotionally handicappedchildren and their families. It is described hcrcas a multi-level model to improve serviccs forthis population for two reasons. First, the ap-proach typically requires planned, coordinatedactivity on three levels: the child and family,the lead organization providing services, and in-teragency collaboration. Second, the word"model" conveys the idea of what the real thingmight look like.
The model is a preliminary pattern, a planfor guiding the actual process of helping emo-tionally handicapped children and their fami-lies. It is not a recipe. Any actual process ofhelping guided by this model may vary fromthat describer', here according to individualchild and family need, organizational capacity,and community context. Nevertheless, there arcthree core components of this model for helpingthat, if adopted, would improve scrviccs foremotionally handicapped children and theirfamilies.
The first is the use of case advocacy to crc-atc an individualized system of care for eachemotionally handicapped child and his or herfamily. The second is the use of a set of intcr-personal interventions in order to engage thechild and family in the process of designing,constructing and maintaining a system of care;persuade others in their organizations to ap-prove and finance certain components of thesystem of care; and facilitate the interagencycollaboration necessary to coordinate the activi-ties of staff from two or more agencies andintegrate them with the efforts of naturalhelpers in the family's personal community.The third is the application of care managementskills to sustain the child and family and, selec-tively, both the formal and natural helperscontributing to the system of care.
The use of each component is guided bycertain principles and requires certain skillslisted below.
Component No. 1: Case Advocacy
Principles
1. The primary, over-amhing goal is tocreate a system of care that surroundsand supports the child and family on adaily
2. The "targets" of case advocacy efforts of-ten arc people too. Nothing is to begained by declaring them enemies; advo-cacy can be partisan without beingadversarial.
3. Child and family involvement in all as-pects of the advocacy process is essentialso that one end result of the advocacy isan enhanced capacity of children andtheir families to speak for themselves.
Skills: To Be Able To...
1. Identify "target areas" within an idealsystem of care.
2. Define the resource development task foreach behavior setting encompassed by thesystem of care.
3. For each behavior setting, locate whocould provide alternative instruction,support, and reward for the child and/orfamily.
4. Acquire the history, if any, of previousinteractions bctwccn child/family andpotential providers.
5. Use the process of assessing the discrep-ancy between what child/family needsand what is currently provided to forge apersonal relationship with the prov'Aer.
The Bulletin of the Research and Training Centerto Improve Services for Seriously Emotionally Handicapped Children and Their Families
VOLUME 1 NUMBER 3
26

6. Analyze the "price structure," in personalterms, for mobilizing the modified set ofinstruction, support, and reward desiredin each behavior setting.
7. Specify the basis for having leverage inthe situation.
8. Consider the effect of timing on the suc-cess of a request to provide (or allowprovision of) alternative instruction,support and reward.
9. Formulate and prepare contingency plansin the event that the alternatives pro-vided provoke a crisis between child/family and provider.
10. Propose, persuade, or entice potentialprovider to try alternative instruction,support, and reward.
Therapeutic Case Advocacy Project staff: (from left) Principal Investigator Tom Young, Project Manager James Mason, CenterAssociate Katie Yoakum. (Photos by Marilyn McManus.)
RESEARCH AND TRAININGCENTER
Regional Research Institute forHuman Services
Portland State UniversityP.O. Box 751Portland, Oregon 97207-0751(503) 464 .4040
Copyright © 1987 By RegionalResearch Institute for HumanServices. All rights reserved.
We invite our audience to submitletters and comments.
RESEARCH AND TRAININGCENTERBarb2ra J. Friesen, Ph.D., Director
Families as Allies ProjectBarbara J. Frier,, Ph.D., Principal
InvextigatorRichard Vosler-Hunter, M.S.W., Training
Coordinator
Therapeutic Case Advocacy ProjectThomas M. Young, Ph.D., Principal
InvestigatorJames L Mason, B.S., Project Manager
Youth In Transition ProjectMatthew J. Modrein, Ph.D., Principal
Investigator
Resource c vicesMarilyn McManus, J.D., M.S.W.,Coordinator
Focal PointMarilyn C. McManus, J.D., M.S.W., Editor
Center AssociatesPatty BundrenTerry E. Butler, B.A.Steven Cooper, B.S.Kaye Exo, M.S.Paul E. Koren, Ph.D.Loretta Norman, B.A.A. Christina Rutland, M.S.W.E. Darcy Shell, B.S.Katie S. Yoakum, B.S.
GRADUATE SCHOOL OF SOCIAL WORKBernard Ross, Ph.D., Dean
REGIONAL RESEARCH INSTITUTE FORHUMAN SERVICESArthur C. Emlen, Ph.D., Director
NATIONAL ADVISORY COMMITTEE
Mary Hoyt, M.S.W., Chair, Oregon StateHospital, Child and Adolescent Unit
Richard Angell, M.D., Department of Psychiatry,Oregon Health Sciences University
William Anthony, Ph.D., Center forRehabilitation Research and Training in MentalHealth, Boston University
William Arroyo, M.D., Assistant Director,Child/Adolescent Psychiatry, Los Angeles
CountyUSC Medical Center
Marva Benjamin, M.S.W., ElahanCommunity Mental Health Center,Vancouver, Washington
Betsy Burke. Ph.D., Chief, SpecialPopulations, California State Department ofMental Health
Lee Clark, Ph.D., Emotionally HandicappedPrograms, Bureau of Education forExceptional Students, Florida Departmentof Education
Glenda Fine, Parents Involved Network,Mental Health Association of SoutheastPennsylvania
Bud Fredericks, Ed.D., Teaching Research,Inc., Western Oregon State College
Paula Goldberg, PACER Center, Inc.,Minneapolis, Minnesota
Mareasa Isaacs, Ph.D., AssociateCommissioner for Children and Youth,New York Office of Mental Health
Phyllis Magrab, Ph.D., Director, ChildDevelopment Center, GeorgetownUniversity
Barbara Melton, B.S., Monmouth, Oregon
Larry Platt, M.D., Office of the RegionalHealth Administration, U.S. Public HealthServices, Region IX
Ann Turnbull, Ph.D., Bureau of ChildResearch, The University of Kansas
2 FOCAL POINT Spring/Summer 198727
Component No. 2: Interpersonal Interventions
Principles
1. The primary, over-arching goal is toengage and sustain the child and familyin the process of working out a newaccommodation between them and theirenvironment.
2. Interpersonal interventions are carriedout in the service of case advocacy andmanagement efforts to establish andmaintain a system of care, not vice-versa.
3. The use of interpersonal interventions isnot synonomous with providing psycho-therapy. These skills are relevant towork with both the official client andwith others in the client's environment.
Skills: The Ability To...
1. "Listen with a third ear" for things otherswould like to talk about but feel theycannot.
2. Absorb verbal abuse and aggression inresponse to the offer of help.
3. Understand and describe one's ownfeelings directly.
4. Acquire an empathic comprehension ofanother person's difficulties and conveythat in both words and gestures.
5. Translate another person's psychologicalneeds into plans for enhancing, restruc-turing, or otherwise modifying his/herenvironment's provision of instruction,support and reward.
6. Clarify one's own role and the purpose ofthe relationship, namely, to design andestablish a system of care.
7. Break a larger problem or difficultydown into manageable but meaningfultasks to be pursued sequentially.
8. Encourage repeated feedback on bothhelpfulness of the relationship and theprocess of accomplishing tasks.
9. Anticipate the demands that new accom-modations among children, parents, andtheir environments will make upon eachother and devise opportunities for respiteand reward as part of the process ofconstructing the system of care.
10. Set enforceable limits on the behavioralexpression of anxiety, impatience, f rus-tration, or anger and negotiate theconsequences for when those limits areexceeded.
Component No. 3: Care Management
Principles
1. The primary over-arching goal is to coor-dinate, integrate and maintain a networkof services that together with naturalhelping sources establish and support afunctioning balance beween child, familyand their environment.
2. The guiding idea behind care manage-ment is the routinization of an individ-ualized system of care that remains flex-ible and adaptive over time as needs andcircumstances change. Accountability,therefore, is ultimately to the child andfamily.
3. The process of care management is moreimportant than its product. By definition,the process is individualized, interactive,and pluralistic.
Skills: The Ability To...
1. Assemble the people involved in each ofthe child/family's behavior settings todesign the individualized system of careand each person's contribution (the TCAservice team).
2. Involve the child and in the pro-cess and verify mutual understandingsand expectations.
3. Define goals for each component withinthe system of care against which accom-plishments can be assessed at a futurepoint in time.
4. Select a care manager from among themembers of the TCA service team.
5. Review plans for modifying the provisionof instruction, support, and reward ineach behavior setting and establish atime/task chart that records who hasplanned to do what and by when.
6. Schedule meeting times and places forsubsequent reviews and modifications ofthe planned provision of alternativeinstructions, supports, and rewards.
7. Establish measures of satisfaction withthe system of care to be completed by thechild, the parents, and each of theconstituent members of the system ofcare.
8. Devise a system of 24-hour response ca-pability for crisis intervention, prefer-ably one that rotates responsibility amongteam members.
28Spring/Summer 1987 FOCAL POINT 3
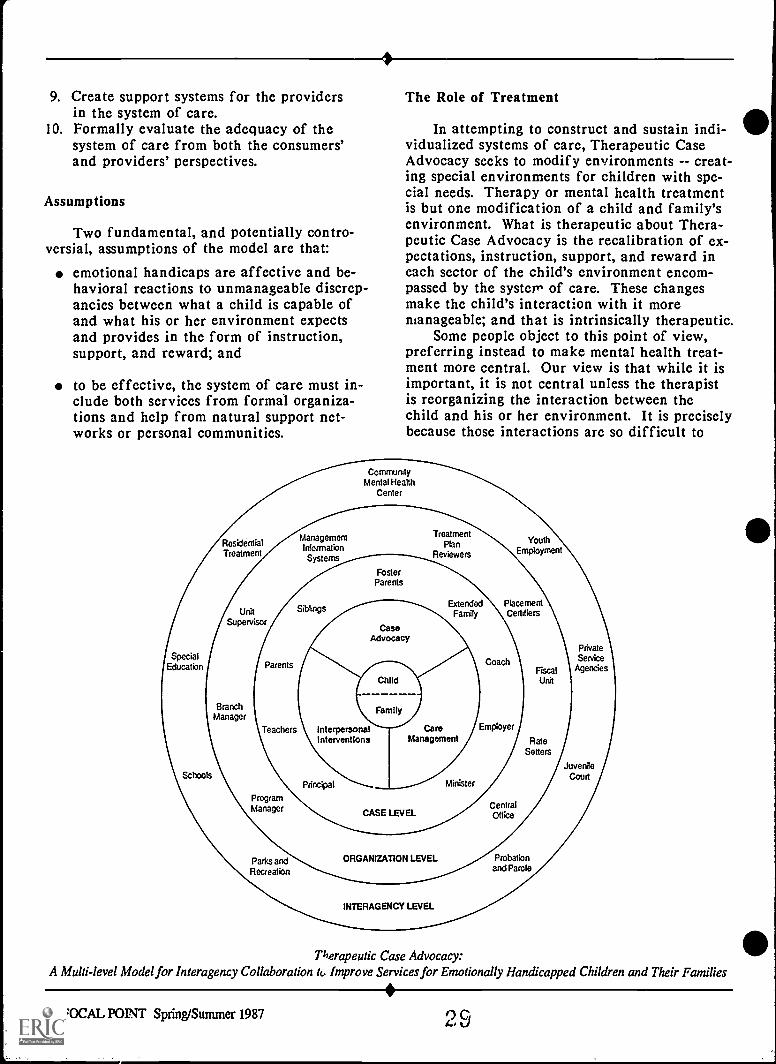
9. Create support systems for the providersin the system of care.
10. Formally evaluate the adequacy of thesystem of care from both the consumers'and providers' perspectives.
Assumptions
Two fundamental, and potentially contro-versial, assumptions of the model are that:
emotional handicaps are affective and be-havioral reactions to unmanageable discrep-ancies between what a child is capable ofand what his or her environment expectsand provides in the form of instruction,support, and reward; and
to be effective, the system of care must in-clude both services from formal organiza-tions and help from natural support net-works or personal communities.
The Role of Treatment
In attempting to construct and sustain indi-vidualized systems of care, Therapeutic CaseAdvocacy seeks to modify environments -- creat-ing special environments for children with spe-cial needs. Therapy or mental health treatmentis but one modification of a child and family'senvironment. What is therapeutic about Thera-peutic Case Advocacy is the recalibration of ex-pectations, instruction, support, and reward ineach sector of the child's environment encom-passed by the system of care. These changesmake the child's interaction with it moremanageable; and that is intrinsically therapeutic.
Some people object to this point of view,preferring instead to make mental health treat-ment more central. Our view is that while it isimportant, it is not central unless the therapistis reorganizing the interaction between thechild and his or her environment. It is preciselybecause those interactions are so difficult to
CommunityMental Health
Center
ResidentialTreatment
ManagementInformationSystems
TreatmentPlan
Reviewers
YouthEmployment
FosterParents
SiblingsExtended Placement
Family Certifiers
SpecialEducation Parents
PrivateService
Agencies
Child
BranchManager
Family
InterpersonalInterventions
CareManagement Rate
Setters
SchoolsPrincipal Minister
JuvenileCourt
ProgramManager CASE LEVEL
CentralOffice
Parks andRecreation
ORGANIZATION LEVEL
INTERAGENCY LEVEL
Probationand Parole
Therapeutic Case Advocacy:A Multi-level Model for Interagency Collaboration tc, Improve Services for Emotionally Handicapped Children and Their Families
4 FOCAL POINT Spring/Summer 1987 4,J

change that this model is a multi-level model.In many situations, only concurrent interven-tions at all three levels can mobilize theresources necessary to effect such changes.
Comprehending the model is made difficultby its complexity. In part, this is because inpractical terms it is three models in one. It is apractice model for working directly with emo-tionally handicapped children and their fami-lies. It is also an organizational change model formanaging the conflict within organizations thatis generated by the practice model. And it is aninteragency collaboration model for implementing(creating and sustaining) the systems of care forindividual children and their families. Thediagram is an attempt to describe the model'sthree levels in one picture.
What this diagram still does not depict ade-quately is how actions taken at one level haveimportant effects on the other two levels. Forexample, when a worker using this model uniteshis agency and several others with the child'sparents, extended family, and church to designand implement a system of care, the worker isengaged simultaneously at all three levels. Theinitiative of his agency is an incentive for otheragencies to collaborate, as is the participation ofrepresentatives from the child's personal com-munity. Simultaneously, the resources madeavailable through the interagency level provideboth incentive and enhanced capacity for those
at the case level to attempt modifications in theinstructions, supports, and rewards they bring tothe child's interaction with their environment.
Conclusion
This model is still in the process of devel-opment. We do not claim to be its sole inven-tors. Many others in the field have provided uswith ideas, clarifying suggestions, and encour-agement to proceed further in its development,demonstration, and evaluation. At the presenttime, therefore, our efforts are directed at thepreparation of a training guide and an evalua-tion procedure. These will allow us to pilot testthe model's introduction into a community anddocument its effects.
We continue to learn of others' efforts thatare similar or at least compatible with ours. Weare most eager to pursue the possibility of ar-ranging a national conference at which thoseworking in these ways on behalf of emotionallyhandicapped children and their families couldmeet and share their experiences. If you wishto participate in such a conference or to obtainadditional information about Therapeutic CaseAdvocacy, please address your inquiries to usc/o Marilyn C. McManus, Resource ServicesCoordinator.Thomas M. Young, Ph.D., Principal Investigator, TherapeuticCase Advocacy.
Case Management or Care Management?Some of our colleagues have asked whetherTherapeutic Case Advocacy is not just a form ofintensive case management. Others have ques-tioned our use of the phrase care managementinstead of the more familiar case management.We would like to take thiQ ^,,nortunity to clarifyour own point of view or 'ssues raised bythese questions.
Both questions require a generally accepteddefinition of case management from which toproceed. That, of course, is part of the problem.As Weil, Karls, and Associates have said in CaseManagement for Human Service Practice, "casemanagement is a developing method of servicecoordination and accountability in the humanservices." (Weil, et. al. 1985:1) Recognizing thediversity of conceptions inherent in a devel-oping concept, they supply their own definition.
"Case management is a set of logical steps and aprocess of interaction within a service networkwhich assure that a client receives neededservices in a supportive, effective, efficient, andcost effective manner." (Weil, et. al. 1985:2)
They note that "throughout its history, casemanagement has had dual sets of goals -- one setrelated to service quality, effectiveness, andservice coordination and the other related togoals of accountability and cost effective use ofresources." (Weil et. al. 1985:2)
Care management is very much "a set oflogical steps and a process of interaction withina service network" with goals of maintaining theprovision of effective, coordinated services. Butit is not concerned with efficiency or cost effec-tiveness. It is concerned only with the qualita-tive response of the system of care created
i, - 30Spring/Summer 1987 FOCAL POINT 5
....______.-r

through use of the Therapeutic Case Advocacyapproach. Nor is it conce .ed with accountabil-ity, except to the child auu his or her parents.Finally, unlike case management, care manage-ment includes persons in the informal orpersonal community of the child and family.
We think these are very important differ-ences. Too many applications of the case man-agement concept have been "geared to the needsof the service network" rather than to the indi-vidual needs of clients and the development ofresources to meet those needs. The planned in-clusion of the child and family's personal com-munity is part of Therapeutic Case Advocacy'sview that the system of care will be managedbest by the people who care the most. Together,we think these two differences shift the focusin a fundamental way from the management ofa case to the continuation of personal care. Asthe late Nicholas Hobbs put it: "No one wants tobe a 'case', and no one wants to be managed."(Hobbs, 1979:30)
Modrcin, Rapp, and Chamberlain, in theirwork to develop a model of case managementfor use with (adult) psychiatric disabled popula-tions, outlined the many roles case managerswere expected to fill and noted that they variedaccording to which model for case managementwas being used. They observed that the inten-sity of the case management process increases asthe case manager assumes a greater number ofroles. (Modrcin, et. al. 1985:35-40) In this sense,Therapeutic Case Advocacy certainly is inten-sive, requiring a worker to fill the roles ofcounselor, advocate, broker, manager, coordina-tor, spokesperson, and (at times) therapist. But,obviously, there is much more to TherapeuticCase Advocacy than managing cases. The or-ganizational level of the model, particularly,adds a new dimension to most other models ofcase management.
Modrcin, et. al. also reviewed case manage-ment research. They found "substantial dis-agreement over the best way to operationalizecase management"; "no conclusive evidence thatcase management significantly improves care"for the chronically mentally disabled (adult)population; and "experimental studies comparingmodels of case management .... non-existent."(1985:55-57)
More importantly, perhaps, for thisdiscussion are the findings they culled fromdescriptive studies of can managers in mentalhealth settings. These findings suggest that thecase managers preferred not to be identified as
such, spent most of their direct client timeengaged in counseling or psychotherapy, andunderutilized community resources on behalf oftheir clients. (1985:45-46)
We think the research suggests that, at leastin mental health settings, the therapist-casemanager dilemma first articulated by Lamb(1980) remains unresolved. And further, boththe substantive content of case management andits efficacy remain undetermined. For theseand other reasons, we have attempted to developa model of helping, Therapeutic Case Advocacywith a distinct role for care management withiit.
Therapeutic Case Advocacy views the coodination of formal services and natural helpiresources as central rather than auxiliary. Itfoundation is the use of case advocacy at eaof the three levels described in the lead artiand its goal is to modify those interactionstween the child and his or her environmentare handicapping. Instead of wrapping auiary services around mental health treatmTherapeutic Case Advocacy sees the systecare that such services make possible as ically therapeutic. In these ways, TherapCase Advocacy is of a different order tmodel of intensive case management.Thomas M. Young, Ph.D., Principal Investigator, ThCase Advocacy
References
shle
be-that
xil-nt,
m ofntrinsi-eutican any
n
r-g
rapeutic
Hobbs, N. November 1979. Helping DisturbedChildren: Psychological and EcologicalStrategies, II: Project Re-ED, Twenty YearsLater. Center for the Study of Families andChildren, Vanderbilt Institute for PublicPolicy Studies, Vanderbilt University.
Lamb, R.H. 1986. "Therapist -Case Managers:More Than Brokers of Service." Hospital andCommunity Psychiatry, 31, 11, 762-764.
Modrcin, M., Rapp, C. A., and Chamberlain, R.1985. Case Management with PsychiatricallyDisabled Individuals: Curriculum andTraining Program. Lawrence, Kansas: TheUniversity of Kansas, School of SocialWelfare.
Weil, M., Karls, J. M., and Associates. 1985.Case Management in Human Service Practice.San Francisco: Josscy-Bass.
6 FOCAL POINT Spring/Summer 1987 31

Interagency Collaborative EffortsIn the last issue of Focal Point we asked forinformation regarding programs using inter-agency collaboration to establish comprehensivesystems of care for seriously emotionally handi-capped children and their families. The follow-ing is a summary of the responses we received.
LANE COUNTY DIRECTION SERVICEEugene, OregonMarshall Peter, Executive Director
The agency addresses clients' needs by arrangingcoordinated interdisciplinary/inter-agency ser-vice planning on both a long range and shortterm basis, mediating between parents and pro-fessionals and providing materials for trainingworkshops.
LANE COUNTY JUVENILE DEPARTMENTEugene, OregonKevin Collins, Program Manager
Many juvenile offenders are considered behav-iorally disordered or emotionally disturbed. Ju-venile department staff make daily contact withclients' family, school, work, recreational andother settings to monitor client performance andenvironmental support. Their interagency teamshave included judges, police officers, probationand parole officers, training school personnel,special educators, mental health providers, childwelfare workers, recreation workers, and alcoholand drug treatment staff.
WEST VIRGINIA DEPARTMENT OF MENTAL HEALTH/OFFICE OF BEHAVIORAL HEALTH SERVICES/ CHILD ANDADOLESCENT SERVICE SYSTEM PROGRAMCharleston, West VirginiaSusan Mann, Program Coordinator
This new organization is planning a statewideconference designed to generate a sense of in-teragency ownership of the problems associatedwith serving children with serious emotionalhandicaps. They may develop a task force com-prised of conference participants who willoutline interagency protocol recommendations.
MAINE DEPARTMENT OF MENTAL HEALTH AND MENTALRETARDATION/ BUREAU OF CHILDREN WITH SPECIALNEEDS/ CHILD AND ADOLESCENT SERVICE SYSTEMPROJECTAugusta, MaineJames B. Harrod, Ph.D., Technical Assistance Coordinator
The project has three sites (Bangor, Portland,and Saco) and is the central referral point forparents, mental health professionals, educators,and others who serve children with serious emo-tional handicaps. The group works closely withseveral service systems, including education,mental health, child welfare, and juvenile jus-tice. Services are tailored to the strengths andneeds of the child. Transition services are coor-dinated and parents are assisted with education,self-help, and other support activities.
CONTINUUM OF CARE FOR EMOTIONALLY DISTURBEDCHILDRENColumbia, South CarolinaJeanne Rivard, Coordinator of Program and Staff Development
This small state agency's mission is to ensurecontinuing delivery of appropriate services toseriously emotionally disturbed children whoseneeds are not met by existing services and pro-grams. Each child is assigned a service coordi-nator who provides case advocacy andmanagement services.
THERAPEUTIC IN-HOME EMERGENCY SERVICES: APROGRAM OF THE CRISIS INTERVENTION CENTER OFSTARK COUNTY AND CASSPCanton, OhioCarole Pastore, Program Coordinator
The center offers intensive in-home crisis inter-vention and family therapy to prevent out-of-home placements. Ongoing services are providedfollowing the period of crisis intervention.Therapists are available 24 hours a day.
CHILD AND ADOLESCENT SERVICE CENTER DAYTREATMENT PROGRAMCanton, OhioSandra Dragomire, MA., Associate Director
The program relies upon a multidisciplinaryteam and an active case management system.Case managers follow-up on recommendations,which may range from community/home visitsto contracts with social service systems.
2 Spring/Summer 1987 FOCAL POINT 7

The Personal CommunityWe all belong to at least one community andmany of us belong to several. From our com-munity affiliations we develop relationshipswith individuals we trust and seek out to helpus interpret our experiences in the world. Manyfamilies and particularly those with seriouslyemotionally handicapped children need the sup-port of this kind of community structure tohandle the pressures they face. Workers, too,need a source of support and encouragement inserving emotionally handicapped children andtheir families.
Systems of care can be structured in waysthat support both clients and professionals byproviding a collaborative environment con-ducive to addressing the needs and solving theproblems encountered by seriously emotionallyhandicapped children and their families. Suchcare systems impart a sense of 'community' totheir members; that is, a common notion of pur-pose, belonging, value to the group, 'and mutualsupport. In particular, such a system of carewill validate the client's (child and family) rolein the treatment process, while reliving profes-sionals from the burden of providing service inisolation from other professionals and the fam-ily's natural support network. A system of carethat supports clients, professionals, and otherconcerned individuals is what we call a"personal community."
In addition to including individuals impor-tant to serving the seriously emotionally handi-capped child and family comprehensively, asystem of care is a personal community when itencourages the development of supportive rela-tionships among its members and is flexible, dy-namic and, at times, even fun. The individualsinvolved come to recognize their interdepen-dence and how they can function in complemen-tary fashion. As a result, all of its members areempowered and supported in working on behalfof a particular child and family. The personalcommunity is personal in the sense that it pur-sues client-specific needs and goals through so-cial service systems that are essentiallyimpersonal.
Each system of care, then, can be structuredto serve as a personal community. It can con-tain the peers, mentors, friends, and otherpeople we need to generate and maintain focus,values, and goals. For seriously emotionallyhandicapped children, their families, and theirworkers this type of system of care envelopsthem in a climate that supports and empowersthem in what tends to be very demanding andoften frustrating work.
James L. Mason, Project Manager, Therapeutic Case Advocacy
Process Evaluation of Interagency Collaboration EffortThe Therapeutic Case Advocacy Project (TCA)conducted a process evaluation of an in-teragency collaboration effort called CAPS,funded by Multnomah County, for the Portlandmetropolitan area. This undertaking encouragedcommunity mental health centers to work withother child serving agencies in the community toprovide comprehensive, integrated services forchildren and youth with emotional handicaps.TCA staff were involved in the planning andimplementation of the CAPS project, as evalua-tors and consultants. A the end of the project'sfirst year, TCA staff submitted a process evalu-ation to the County which helped persuade theMultnomah County Board of Commissioners tofund the effort for another year.
The CAPS project model is similar to that
8 FOCAL POINT Spring/Summer 1987
-4
being developed by the Therapeutic Case Advo-cacy Project, especially in the area of teamplanning on the case level to develop a systemof care for each child. Due to the interest ex-pressed in this local effort to implement inter-agency collaboration at the practice level, TCAproject staff edited the process evaluation fordistrioution to those in other communities con-cerned with line level implementation of collab-orative efforts. The evaluation report docu-ments the planning process -- its problems,compromises, successes, and pitfalls. The reportalso includes a description of the team processand recommendations based on both partici-pants' and administrators' observations. Toorder a copy of this report, see page 11.
33

Families as Allies Regional ConferencesStrategies to improve and promote collaborativeworking relationships between professionals andparents of children with serious emotional hand-icaps were the focus of four Families as Alliesconferences held throughout the country duringMay and June. Equal numbers of parents andprofessionals met in regional conferences held inKansas, New York, Alabama and Indiana.
All four regional conferences addressedproblems of current service delivery systems forchildren with emotional handicaps and theirfamilies, barriers to collaboration between par-ents and professionals, and strategies to enhanceparent and professional partnerships. Partici-pants in each of the regional conferences at-tended as members of state delegations com-posed of parents, policy makers, programadministrators, and direct service providers.
Panels of parents and professionals inOverland Park, Kansas, described barriers to ef-fective services, and the successes and frustra-tions in establishing a partnership between par-ents and professionals. The panel members dis-cussed common problems such as misdiagnosis,the lack of respite care for parents, lack ofcommunication between agencies in planning,problems of transportation, and lack of compre-hensive insurance to cover the costs of care andtreatment. Panel members emphasized the im-portance of parent and professional collabora-tion to enhance parents' roles as sources of in-formation about their children, and fully in-volve parents as team members in the planning,provision and evaluation of services. Parentswere urged to recognize the limitations and con-straints experienced by providers, and to becomeinvolved in local parent support and advocacygroups to assist in the improvement of servicesfor children with emotional handicaps.
The Albany, New York conference openedwith a "Challenge to Partnership" by a profes-sional and a parent. Obstacles to parent-profes-sional collaboration were addressed through apsychodrama experience that demonstrated thatboth parents and professionals experience manyof the same frustrations in trying to reach acommon goal -- a better, more responsive systemof care. The participants then eas«ged in smallgroup, structured experiences which identifiedways parents and professionals can collaboratein effecting change. A panel presentation dis-
cussed the organization of parent support andself-help groups in a variety of settings.
Participants in the Mobile, Alabama Fami-lies as Allies conference attended a variety ofworkshops dealing with support groups for par-ents, special education laws, working with cul-tural and ethnic minorities, and dealing withmultiple systems of care. Plenary session panelsspoke to the need for parent-professional collab-oration and specific techniques and strategiesfor creating and nurturing such collaboration.A film festival on the second evening of theconference provided participants an opportunityto view selected films on a variety of issuesconcerning services to youth and their families,including program examples and topical issuessuch as AIDS education.
The Families as Allies Conference inBloomington, Indiana, spoke to a wide array ofproblems and issues faced by those seeking toimprove the system of care. Workshop topics in-cluded respite care, educational rights, legisla-tive and case advocacy, case management sys-tems, parent support groups, and community ad-vocacy strategies. Keynote speakers discussedthe nature of the current crisis in service provi-sion to children with emotional handicaps, theimportance of the parent-professionalpartnership, and some recommended futuredirections.
State delegations at each of the regionalconferences met to identify barrie s to col-laboration and strategies to promote collabora-tion within their individual states. Members ofeach state delegation left the conferences with aplan of action for their state, many of whichincluded proposals to improve coordination ofadvocacy groups, develop parent support groups,develop parent information packets, and offerstate level Families as Allies conferences.
il 40 Spring/Summer 1987 FOCAL POINT 9
,

NOTES & COMMENTS
IN MEMORIUM
We were saddened to learn of the death of ArtSands, the administrator of the Kansas Childand Adolescent Mental Health Services Office.We extend our sympathies to his family andfriends. In addition to the personal loss to thoseclosest to him, his death is a loss nationally tothe Child and Adolescent Service SystemProgram, as well as to the people of Kansas. Wewill remember him for his boundless energy anddevotion to children's mental health services.
RESEARCH AND TRAINING CENTERS'CONFERENCE AND CONGRESSIONALRECEPTION
The National Association of RehabilitationResearch and Training Centers (NARRTC) heldits ninth annual training conference in Washing-ton, D.C. in May. The thirty-six rehabilitationresearch and training centers funded by theNational Institute on Disability and Rehabilita-tion Research (NIDRR) are all NARRTC mem-bers. Highlights of the conference includedspeeches by David Gray, Ph.D., NIDRR directorand the presentation of the association's Distin-guished Service Award to Connecticut SenatorLowell Weicker, Jr.
The theme of the conference was facili-tating personal independence through research.Participants shared their research with one an-other and explored methods of enhancing per-sonal independence through minimizing physicalimpairments, improving the community envi-ronment, improving vocational opportunities,minimizing barriers found within particular cul-tures, and improving family opportunity andcommunity linkages.
NIDRR Director David Gray explored theconcept of interdependence. He emphasized thecoequal relationship between professionals anddisabled patients or clients. For example, theresponses of doctors and patients are not inde-pendent; they are interdependent. Successrequires mutual effort and respect.
NARRTC's Distinguished Service Awardwas presented to Senator Lowell Weicker, Jr. atthe association's first Congressional reception.The reception, which was held in the RayburnHouse Office Building, provided the association
with an opportunity to honor a member ofCongress who has contributed greatly to rehabil-itation research. Invited guests included mem-bers of Congress, their assistants, guests fromNIDRR and other government agencies involvedwith rehabilitation research. Each of the re-search and training centers had the opportunityto exhibit its products and display its signifi-cant accomplishments.
CASSP PROJECT DIRECTORS MEETING
The Child and Adolescent Service System Pro-gram (CASSP) project directors held their Springmeeting in Portland. Ira Lourie, Assistant Chiefof the Community Service Systems Branch ofthe National Institute of Mental Health, an-nounced that CASSP would achieve branch sta-tus. CASSP will have the distinction ofbecoming the first children's branch withinNIMH.
Featured presentations included anoverview of the Medicaid program, a summaryof the use of media by mental health agencies, areview of paraprofessional partnerships withtroubled youth in Idaho, and reviews of theKansas Family Input Project and Washingtonstate's Strategic Planning Training Project. Thestaff of the Portland Research and TrainingCenter presented overviews of the TherapeuticCase Advocacy model and the Youth in Transi-tion Project, as well as a review of videotapedand written resources designed to promoteparent involvement.
The highlight of the meeting was a one day"Focus on Families" session. The seventy partic-ipants explored ways to facilitate collaborativeefforts between families and professionals. Par-ticipants explored the similarities and differ-ences in the agendas of CASSP personnel andfamilies, strategies for involving families, thelack of available respite services, and CASSP di-rectors' need for knowledge about how to assistin the development of parent support groups.The Georgetown University CASSP TechnicalAssistance Center is currently preparing asummary of proposed solution strategies.
The Fall CASSP Project Directors meetingwill be held September 14-15, 1987 inWashington, D.C.
continued on last page
10 FOCAL POINT Spring/Summer 1987

Research and Training Center Resource Materials
Annotated Bibliography. Parents of EmotionallyHandicapped Children: Needs, Resources, andRelationships with Professionals *Covers relationships between professionals and parents,parent self-help, support and advocacy groups, parent par-ticipation, parents' problems and guidelines.
Annotated Bibliography. Youth in Transition: Resourcesfor Program Development and Direct Service Intervention*Transition needs of adolescents: educational and vocationalissues, programs and curriculum, research overviews,interpersonal issues, skills training.
Child Advocacy Annotated BibliographyIncludes selected articles, books, anthology entries andconference papers written since 1970, presented in amanner useful to readers who do not have access to the cit-ed sources. $7.00 per copy.
Families as Allies Conference Proceedings: Parent-Professional Collaboration Toward Improving Services forSeriously Emotionally Handicapped Children and TheirFamilies*Held in April 1986 and attended by delegations fromthirteen western states. Includes: agenda, presentationtranscriptions, biographical sketches, recommendations,worksheets, and evaluations.
Gathering and Sharing: An Exploratory Study of ServiceDelivery to Emotionally Handicapped Indian ChildrenFindings from Idaho, Oregon, and Washington, coveringcurrent services, successes, service delivery barriers,exemplary programs and innovations. $2.00 per copy.
0
0
0
The Multnomah County CAPS Project: An Effort toCoordinate Service Delivery for Children and YouthConsidered Seriously Emotionally DisturbedA process evaluation of an interagency collaborative effortis reported. The planning process is documented andrecommendations are offered. $3.00 per copy.
National Directory of Organizations Serving Parents ofSeriously Emotionally Handicapped Children and YouthThe U.S. organizations included provide one or more of thefollowing services: education and information, parenttraining, case and systems level advocacy, support groups,direct assistance such as respite care, transportation andchild care. $5.00 per copy.
Parent Information Workbook on Emotional HandicapsThis self-teaching workbook for parents addresses topicssuch as parents' feelings about themselves and theirchildren, labels and diagnoses, types of professionals andtreatments, and 11-1.01 issues. Single copies free to parents ofchildren with emotional handicaps while supplies last. Allothers, $3.00 per copy.
Parents' 1, oices: A Few Speak for Many (videotape)Three parents of children with emotional handicaps discusstheir experiences related to seeking help for their children(45 minutes). A trainers' guide is available to assist inpresenting the videotape. Brochure describes the videotapeand trainers' guide and provides purchase or rentalinformation.
* One copy free per address while supplies last.
ORDER FORM AND MAILING LIST Research and Training Center
Please send me the publications indicated above. $ enclosed as appropriate.
Add me to your mailing list. Take me off your mailing list.
Change my address as noted below.
O List my organization in the national directory. (The Research and Training Center will contact you.)
NAME
ORGANIZATION
STREET ADDRESS
CITY/STATE/ZIP
TELEPHONE
CHECKS PAYABLE TO: Regional Research Institute for Human ServicesMAIL TO: Resource Services Coordinator, Research and Training Center, Regional Research Institute for Human Services,Portland State University, P.O. Box 751, Portland, Oregon 97207-0751, (503) 464-4040
`),(10
NOTES & COMMENTS continued from page 10
WASHINGTON STATE FAMILY INITIATIVE
Washington State CASSP project staff are devel-oping a comprehensive family support modelthat includes crisis resolution, education, skillsdevelopment, support and advocacy. They areseeking curricula that have been developed orcan be easily adapted for use with families withchildren who have emotional/behavioral diffi-culties. Topical areas include effective ver-bal/non-verbal communication, problem solving,stress management/coping skills, behavior man-agement, social support network development,service systems and case advocacy. If you knowof such materials, please contact: Dennis Olson,Washington State CASSP Project, MS: OB-42F,Dept. of -Sucial and Health Services, MentalHealth Division, Olympia, WA 98504.
NATIONAL SCHOOL STUDY
Jane Knitzer, author of Unclaimed Children, andher colleagues at Bank Street College arcconducting a national study of how well schoolsrespond to children with emotional and behav-ioral difficulties. She would welcome any in-formation about individual programs and/orschool districts that are particularly responsiveto the needs of troubled children, and theirfamilies. If you know of such programs orschool districts, or wish to share other perspec-tives on the issue, she would welcome hearingfrom you. Contact her at: Bank Street Collegeof Education, 610 West 112th Street, New YorkCity, New York 10025, (212) 663-7200.
PORTLAND STATE UNIVERSITYResearch and Training CenterRegional Research Institute for Human ServicesP.O. Box 751Portland, Oregon 97207-0751
TELEPHONE NUMBER CHANGE
The prefix for all Portland State Universitytelephone numbers has changed. The Researchand Training Center's new telephone number is(503) 464-4040.
FOCUS: YOUTH IN TRANSITION
The Youth in Transition Project is de-veloping an approach for addressing transi-tion issues faced by emotionally handicappedadolescents as they leave youth-serving sys-tems and move toward the assumption ofadult roles. The next issue of Focal Pointwill feature the Youth in Transition Project.We would like to identify innovative transi-tion programs which set-ire emotionallyhandicapped adolescents. Programs shouldbe oriented to facilitating the adjustment ofemotionally handicapped youth to adultroles. Social skills training, vocational op-portunities, and independent living ex-periences are all critical components of atransition approach. If you know of pro-grams or models for youth with emotionalhandicaps that have a transition focus,please notify: Matthew J. Modrcin, Youth inTransition Project Director.
Janet DrillDepartmeW: of Information
ServicesThe Council for ExceptionalChildren1920 Association
DriveReston, VA 22091
0
Nonprofit Org.U.S. Postage
PAIDPortland, ORPermit #770





























