Embed Size (px)
Citation preview

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 1
Module 1.
Syllabus: Acetylcholinesterase, angiotensin converting enzyme (ACE), ACE Inhibitors, HMG Co A reductase inhibitors, pseudocholinesterase, 5'-nucleotidase (5NT), glucose-6-phosphate dehydrogenase (GPD), CKisoforms, immunoreactive trypsinogen (IRT) and chymotrypsin; amylase isoenzymes. Mechanism of coenzymes (NAD/NADP, FAD/FADH2, PLP, Coenzyme A, TPP, Biotin).
Course objective:1 To understand the mechanism of enzyme action, purification of enzymes, catalytic action of enzymes, kinetics of enzyme catalyzed reactions
Course outcome 1: Explain the various techniques involved in the extraction and utilization of enzymes in biotransformation.
1. ENZYMES AND CO- ENZYMES:
q. How angiotensin converting enzyme as a part of renin-angiotensin-aldosterone system (RAAS) is significant in
treating conditions such as high blood pressure, heart failure, diabetic nephropathy and type 2 diabetic
mellitus?
Angiotensin I-converting enzyme (ACE) is a circulating enzyme that takes part in rennin-angiotensinogen
system by mediating extra cellular volume of blood plasma, lymp and interstitial fluid, and constricting
artery, and is an exopeptide.
ACE is secreted by pulmonary and renal endothelial cells and takes part in the conversion of decapeptide
angiotensin I to octapeptide angiotensin II, which in turn is a potent vasoconstrictor.
Depending on the substrate level concentration, it narrows the diameter of the blood vessel that in turn
sends the blood pressure up.
It also degrades bradikinin that in turn prevents its activity of increasing the diameter of the blood vessel as it
is a potent vasodilator resulting in the indirect increase of blood pressure.
Because of ACE’s involvement in increasing the blood pressure, inhibiting the enzyme has significance
importance in treating conditions such as high blood pressure, heart failure, diabetic nephropathy and type
2 diabetic mellitus, since it is located at the rate limiting step hence ACE is biologically significant.
Human sACE is a type-I membrane bound protein with a 28-reside carboxy-terminal cytosolic domain, a 22-
residue hydrophobic transmembrane domain and a 1227- residue heavily glycosylated extracellular domain.
Each of the extracellular domains of ACE contains a sequence in which two Histidine residues serves as zinc-
binding ligands that along with the glutamine located 23-24 residues towards the carboxyl terminus and a
water molecule provides the metal with tetrahedral coordination geometry.
Human sACE has a single peptide that directs it to an extracellular localization, and in vertebrates it is
anchored into cell membranes through carboxy-terminal hydrophobic sequence.
Extracellular location of the ACE makes it efficient even at low concentration as single pass of blood through
the pulmonary vasculature is sufficient to convert all circulating angiotensin I to angiotensin II (Fig 2.1).
Even after with this efficiency angiotensin I is not the only one substrate for ACE, but substrates such as
bradikinin and other bioactive peptides can also be acted upon by ACE. On the other hand, gACE isoform is
expressed in only few cells such as sperm cells and mature sperm.

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 2
The cascade of processing of angiotensin peptides in both plasma and tissue by rennin and aldosterone is
known as Renin-Angiotensin-Aldosterone System (RAAS), which plays a key role in the regulation of the
blood pressure.
Blood pressure in human and some other mammal is controlled partly by a cycle involving peptide hormones
produced by the kidneys and liver, and a steroid hormone produced from adrenal cortex.
On sensing by kidney that the Na+ level in blood is very low, they release a protease known as renin into
circulation, which has a single substrate known as angiotensinogen.
Renin, and aspartyl protease cleaves the protein angiotensinogen (Aogen) to produce an inactive decapeptide
known as angiotensin I.
This is followed by the cleavage of angiotensin I (Ang-I) into active octapeptide angiotensin II (Ang-II) by
angiotensin converting enzyme (ACE) releasing dipeptide His-Leu.
Ang-II further converted by neutral endopeptidases (NEP) to produce Ang-1-7 or by angiotensin converting
enzyme- related carboxypeptidase (ACE-2) to form Ang1-9.
Ang II may also be cleaved to Ang-1-7 by ACE-2.
ACE also cleaves angiotensin (1-7) to angiotensin (1-5) and dipeptide His-Pro.
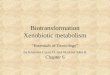
Angiotensinogen may directly gets cleaved into Angiotensin (1-12) or Angiotensin II or angiotensin (1-7) (Fig
2.2 and 2.3).
Renin
Asp Argo
Val Tyr Ile His Pro Phe
Ang-II
Asp Argo
Val Tyr Ile His Pro Phe His Leu Leu Val Tyr Ser Protein
Aogen
Leu Val Tyr Ser Protein
Ang-I
Asp Argo
Val Tyr Ile His Pro Phe His Leu
Ang-(1-7)
Asp Argo
Val Tyr Ile His Pro
Ang-(1-5)
Asp Arg Val Tyr Ile
Phe
His Leu ACE
NEP
His ACE-2
Fig 2.1 Schematic representation of cleavage of angiotensinogen

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 3
Ang-II activates the angiotensin II type-1(AT-1) receptor, belongs to G-protein-coupled-receptor superfamily
with various effects such as vasoconstriction and stimulation of aldosterone synthesis, and release that
ultimately leads to sodium retention, water reabsortption and elimination of potassium to elevate blood
pressure.
Stimulation of AT-1 receptor leads to a cascade of signaling pathway in several cell types that in turn leads to
vasoconstriction, inflammation and proliferation.
Hence this site is of importance in managing health conditions in various cardiovascular diseases, including
hypertension, atherosclerosis and ventricular hypertrophy.
Ang-II also inactivates bradikinin. Ang-II also activates the angiotensin II type-2(AT-2) receptor, and its effects
were believed to antagonize the effect of AT1 receptor.
Where as AT-2 receptor is mainly expressed in the foetal stage and in adult it is expressed under crucial
circumstances that are being under investigation, but appear to have opposing effects to the AT-2
receptor. AT-3 receptor was reported in cultured neuroblastoma cells, and AT-4 is more specific for Ang-IV
(Ang-3-8) than Ang-II.
Renin
Angiotensin
converting
enzyme
Aminopeptidase A
Aminopeptidase N
Angiotensin-(1-7)
Cathepsin G
Angiotensin-III
Angiotensin-IV
Angiotensinogen
Angiotensin-I
Angiotensin-II
Angiotensin converting enzyme, Chymase
Angiotensin-(1-9)
Angiotensin converting enzyme- 2 Cathepsin E
Neprilysin, membrane bound neutral endopeptidases Metalloprotease Endopeptidase
Angiotensin converting enzyme-related carboxypeptidase P
Angiotensin converting enzyme -Endopeptidase
Angiotensin-(1-5)
Fig 2.2 Angiotensin I degradative pathway.

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 4
There are various points are available in the RAAS that can be utilised to inhibit the enzymes during various
diseased conditions.
ACE along with activating Ang-I, also destroys the bradikinin, a potent vasodilator, hence any ACE inhibitor
along with preventing the formation of Ang-II also prevents the inactivation of bradikinin.
ACE inhibitors (short notes)
RAAS is central to the maintenance of blood pressure and hence serves as the target of several types of anti-
hypersensitive drugs such as ACE inhibitors, angiotensin receptor blockers (ARBs), renin inhibitor aliskiren and
aldosterone receptor antagonists.
ACE inhibitors target the ACE gene product results in the ultimate reduction of Ang-II, decrease aldosterone
secretion and reduction of blood pressure.
Angiotensin receptor blockers (ARBs), target and block the activation of AT-1receptor, and also lower levels of
aldosterone that in turn decreases the resorption of sodium and water, decreases the excretion of potassium
and decreases the pressure in blood.
AT-2 receptor is considered to act in opposition to AT-1receptor, such as vasodilation, growth inhibition and
apoptosis.
Aogen
Ang-I Ang-II
Renin
Ang-II
Ang-II Ang (1-7)
Ang (1-7)
Ang (1-12)
Ang (1-7) Ang (1-5)
ACE
ACE -2
AT-1
ACE
AT (1-7)
Aldosterone release
Classic epithelial effect: Na+ and H2O retention, K+ and Mg+ loss.
Non-epithelial effect: Increase cardiac and vascular collagen synthesis, increased PAI1 expression, increased influx of Na+ in vascular smooth muscle cells, increased pressure response to angiotensin I, endothelial dysfunction, decreased arterial compliance, and increased sensitivity to catecholamine.
Attenuate the inflammatory and fibrotic action of the Ang II-AT1 receptor pathway through inhibition of the mean arterial pressure kinase kinase (MAPKK) pathway, the potential stimulation of cellular phosphates, the inhibition of cyclooxygenase-2 (COX2), and other proinflamatory agents, stimulation of NO.
Fig. 2.3 Cascade of processing of angiotensin and their interaction with receptor.

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 5
Here, ARBs are selective for AR-1 receptor and do not bind to AT-2 receptor.
Angiotensin converting enzyme plays a major role in the biological function at different organs or the
organism.
Growth and proliferation
Nuclear factor
kappa-B
Activator
protein1
Reactive oxygen
species
Phosphotyrosine kinase
Diacylglycerol
Inflammation
Proliferation
Vasoconstriction
Inflammation
Proliferation
Coagulation
Nitric
oxide
Increased atherogenicity
NADH/ NADPH
oxidase
Oxidised low
density
lipoprotein
Phospholipase C
1, 4, 5-
inositoltriphosphate
Protein kinase C
Intracellular calcium
Vasoconstriction
Tyrosine
phosphorylation
Mitogen- activated
protein kinases
Gq uncoupling Janus kinase Signal
transducer & activator transcription
factor
Tyrosine kinase
Renin
Angiotensin converting enzyme
Angiotensinogen
Angiotensin I
Angiotensin II
Angiotensin II
AT-1 receptor
Gene
transcription
factors
(c-fos, c-myc, c-
jun)
Fig. 2.4 Schematic representation of signal transduction of the AT-1 receptor

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 6
Acetylcholinesterase
Q: How acetylcholinesterase degrades the ubiquitous neurotransmitter acetylcholine by
deesterification to produce choline and an acetate group?
Acetylcholinesterase (ACHE) is an enzyme of biological importance as it degrades the ubiquitous
neurotransmitter acetylcholine (ACH) by deesterification to produce choline and an acetate group.
Its activity serves to terminate synaptic transmission at neuromuscular junction and cholinergic
synapses in the central nervous system.
ACHE is bound to cellular membranes of excitable tissues at cholinergic synaptic junction, endoplasmic
reticulum and other membranes that are usually associated with nerve impulse condition.
ACHE is also found on the red blood cell membranes, where it constitutes the Yt blood group antigen.
It is a serine esterase with an anionic binding site that attracts the positively charged quaternary
ammonium groups of ACH.
It is highly active enzyme as it is able to degrade 25000 molecules of acetylcholine per second and choline
produced by the action of ACHE is recycled by transportation and reuptake back into nerve terminals for
the next cycle.
ACHE has one of the enzymes with fastest rate of reaction with the capacity to break each molecule in
about 80 microseconds.
Mechanism of action of ACHE is similar to chymotrypsin in which a serine attacks and cleaves the ester,
and it is an example of general base catalysis, since serine must first be deprotonated by nearby histidine.
This hydrolytic reaction proceeds by nucleophilic attack of the carbonyl carbon, acylating ACHE yielding
the enzyme and releasing choline, which is then followed by a quick hydrolysis of the acylated enzyme
yielding acetic acid that in turn restores the esteric site.
Enzyme gets quickly regenerated following ester hydrolysis.
This pathway is similar to the way through pipeline in which substrate does in one end and product
comes out through the other end through conformational changes along with the hydrophobic and
electrostatic forces.
ACHE is present in the synapse between nerve cells and muscle cells, and springs into action immediately
only after a signal is passed to cleave acetylcholine into acetic acid and choline, which in turn results in
the stoppage of signals, allowing the end products to be recycled and rebuilt into new neurotransmitter
for the next message.
ACHC has lipid attached to protein chain that helps the enzymes to get anchored into the cell
membranes, and active site of the enzyme is located deep inside the surface that is deep enough to
accommodate whole substrate, with base consisting of three triads, serine histidine and glutamate (Fig.
2.5).

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 7
Since acetylcholinesterase is an active enzyme with essential function, it is also a potential point in our
nervous system, as many snake poisons and plant toxins attack the enzyme causing acetylcholine to
accumulate in the nerve synapse leading to paralysis of muscle.
The active site of the acetylcholinesterase contains two structural binding sites, such as anionic binding
site and esteratic binding site located at the bottom of the narrow gorge, which is lined with hydrophobic
amino acid side chains.
Active site of the ACHE is unique compared to other serine proteases in that it contains Glutamate side
chain instead of Aspartate side chain, and choline binding site consisting of hydrophobic tryptophan
residue instead of anionic group.
During the hydrolysis of acetylcholine it form an intermediate known as Acetyl-ACHE intermediate with
the release of choline, and this intermediate ultimately gets hydrolysed into acetate and free enzyme (Fig.
2.6).
Choline binding site
Catalytic triad
Peripheral binding site
His
Glu Ser
Fig. 2.5 Schematic representation of active site of ACHE.
Anionic site
Electrostatic attraction
Acetylcholine
His Glu
Ser
Esteric site
Choline
Acetic acid
Fig. 2.6 Mechanism of action of enzyme ACHE.

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 8
This normal sequence of events takes between nerve impulse and muscle contraction takes place by
thousands of a second.
Acetylcholine is synthesised in the cytoplasm of the axon’s terminal button, from acetyl coenzyme A and
choline, and many thousands of molecules of acetylcholine are stored in each synaptic vesicle.
As soon the contents of the vesicle release into the synaptic gap, nearly half of the acetylcholine molecules are
hydrolysed by acetyl cholinesterase, but as many acetylcholine molecules accumulate due to inability of the
acetylcholinesterase, and left over acetylcholine molecule binds to nicotinic acetylcholine receptors (ACH-
receptor)on the postsynaptic side of the gap.
ACH-receptor is actually a pore in the muscle cell that gets twisted open on binding and releases ions, and
sudden rush of electrical current triggers muscle contraction.
ACHE plays a major role in terminating this event by breaking the neurotransmitter in the space between the
nerve ending and the muscle cell surface (Fig. 2.7).
Three different types of short-acting, medium-duration and irreversible inhibitors acetylcholinesterase
inhibitors differ in their interactions with the active site of acetylcholinesterase acts as inhibitors.
Medium-duration acetylcholinesterase such as neostigmine enhances cholinergic transmission in the central
nervous system, autonomic nervous system and at neuromuscular junctions. Acetylcholinesterase inhibitors
are proven therapy for Alzheimer’s disease. Short-acting inhibitors such as tacrine and donepezil are that
bind to acetylcholinesterase by hydrogen bonding and gets hydrolyzed within minutes by the body's water.
Acetate
Choline
Acetylcholine
Acetylcholinesterase
Synaptic cleft
Synaptic vesicle
Motoneuron Axon
Acetyl-SCoA
Mitochondria
Muscle fiber
Ion
Acetate
Acetylcholine
CoA
Fig. 2.7 Schematic representation of sequence of events taking place at synaptic junction.

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 9
3. 5’ – Nucleotidase
Q: Justify why 5’ – Nucleotidase is biologically significant?
Nucleotidase is a hydrolytic enzyme that catalyses the hydrolysis of a nucleotide into a nucleoside and a
phosphate, such as adenosine monophosphate to adenosine, and guanosine monophosphate to guanosine.
5'-nucleotidase removes phosphate from the 5' end of the sugar moiety and 3'-nucleotidase removes phosphate
from the 3' end of the sugar moiety.
Based on the substrate preference and subcellular location, 5'-nucleotidase are known as membrane bound or
soluble.
Membrane bound 5'-nucleotidase is specific towards adenosine monophosphate, and is mainly involved in the
salvage of preformed nucleotide and in signal transduction cascade along with purinergic receptors.
Soluble 5'-nucleotidase belongs to haloacid dehalogenases super family of enzymes such as mitochondrial 5'-3'
pyrimidine nucleotidases (mdN), cytosolic 5'-3' pyrimidine nucleotidases (cdN), cytosolic nucleotidase (cN),
pyrimidine 5'-nucleotidase (cN-III) etc.
5' –nucleotidases are biologically significant as they are involved in number of functions such as nucleic acid
repair, cell-cell communication, purine salvage pathway for the synthesis of nucleotides, membrane transport,
signal transduction etc……. so on. So ended up having more than 50 names. Let us take only one case..!
Adenosine is present both inside the cell as well as within the cells, as it is at cross roads between different
metabolic pathways.
Adenosine triphosphate (ATP) is the basic energy source for the transport system and the enzymes of
cells, which breaks down to form naturally occurring purine nucleoside, adenosine.
In most of the cases ATP gets hydrolysed to adenosine diphosphate (ADP) that can be further
dephosphorylated to adenosine monophosphate (AMO) in the cell, and most of the ADP and AMP in the
cell in the presence of oxygen are rephosphorylated enzymatically in the mitochondria.
Enzyme, by ecto-apyrase (EP) is responsible for the conversion of ATP to AMP as represented in the figure
2.10.
When the supply of oxygen is insufficient, the condition known as hypoxia, and if there are large amount
of ATP hydrolysed, portion of the AMP gets dephosphorylated to adenosine by the enzyme, 5'-
nuclotidase (5'-NT).
Adenosine level in cell and tissues fluids may vary between ten and few hundred nanomolar under normal
physiological conditions, and based on the conditions of stress and distress formation of adenosine in these
locations may vary.
Adenosine acts on four G-proteins coupled receptors, of which A1 and A3 are primarily coupled to Gi family G
proteins, and A2A and A2B are mostly coupled to Gs like G proteins.

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 10
In coronary vascular smooth muscle adenosine binds to adenosine type-2A receptors (A2A-R) that is coupled to
the Gs-protein (Gs-P), where as in cardiac tissue it binds to type-1 receptors (A1-R) that are coupled to Gi-proteins
(Gi-P).
Activation of G-protein stimulates adenylyl cyclase (AC), increases cAMP and causes protein kinase activation
that in turn stimulates the KATP channels that hyperpolarize the smooth muscle, causing relaxation.
Increases cAMP inhibits myosin light chain kinase that lead to decreased myosin phosphorylation and decreased
contractile force.
Adenosine is also inhibits the calcium entry into the cell through L-type calcium channels, and in some type of
blood vessels it produces vasodilatation through increase in cGMP that in turn inhibits the entry of calcium into the
cell and facilitates the opening of potassium channels.
Whereas activation of Gi-proteins open potassium channels to pave the way for the calcium entry into the cell
that in turn hyperpolarizes the cell, and also decreases cAMP that results in the inhibition of L-type calcium
channels preventing calcium entry into the cell.
Adenosine in sinoatrial (SA) node acting through A1 receptor and inhibit the pacemaker current (If), which in turn
decreases spontaneous firing rate, known as negative chronotropic effect.
On the other hand, inhibition of L-type calcium channels also decreases conduction velocity at atrioventricular
(AV) nodes, known as negative dromotropic effect.
ADO
ADO
ATP
A2A-R Gs-P
ADO
↑cAMP
ATP
A1-R Gi-P
AC
↓cAMP
↓ Chronotropy ↓ Dromotropy
SA and AV node ↓ Dromotropy
Vascular smooth muscle ↓ Dromotropy
AC
Relaxation
Fig. 2.10 Schematic representation of role of adenosine on smooth muscle and pacemaker of heart.

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 11
4. Glucose -6-phosphate dehydrogenase
Q: Analyze why Glucose-6-phosphate dehydrogenase is biologically significant?
Glucose-6-phosphate dehydrogenase is biologically important enzyme that catalyses the first step of the
pentose phosphate pathway (Fig. 2.14) resulting in the production of 5-carbon sugar, ribose, required
for the nucleic acid synthesis and fatty acid synthesis.
In addition to the production of 5- carbon sugar, ribose that is an essential component of both DNA and
RNA, glucose-6-phosphate dehydrogenase is also responsible for maintaining NADPH inside the cell.
NADPH is essential cofactor in many biosynthetic pathways and also required to keep glutathione in
reduced state that in turn acts as a scavenger for dangerous oxidative metabolites in the cells by
converting harmful hydrogen peroxide to water with the help of the enzyme, glutathione peroxidase (Fig.
2.15).
Selenium dependent enzyme, glutathione peroxidase uses reduced glutathione (GSH) to detoxify
hydrogen peroxide (H2O2), and during this process oxidation power of the H2O2 is transferred to oxidised
glutathione (GSSG).
Even though H2O2 has reduced significantly, GSSG still has higher oxidising power that need to be taken
care off.
Here, glutathione reductase pays significant role in recycling GSSG using NADPH, during which NADP is
converted to NADP. Now, regenerated GSH is ready to detoxify more hydrogen peroxide.
During a normal condition, antioxidant defense system is functioning properly, and most of its
components such as H2O, GSH and NADPH are in reduced state.
However, when there is a malfunction then oxidising components such as H2O2, GSSG and NADP tend to
accumulate those in turn lead to adverse consequences.
This entire process is driven by energy production at the cellular level that involves proper thyroid hormone
levels, healthy mitochondrial function and an active pentose-phosphate metabolic pathway.
NADP+ NADPH H+
Glucose-6-phosphate
dehydrogenase
CH2
H
H
OH O
O
OH
OH H
H OH
O O
O
P
D-Glucose 6-phosphate
H
H
OH
O O
O
P
OH
CH2
H
O OH
OH
OH H
H
6-phosphoglucanolactone
Fig. 2.14 The committed oxidation/reduction reaction catalysed by glucose-6-phosophate dehydrogenase in pentose
phosphate pathway

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 12
Glucose-6-phosphate dehydrogenase is biologically important as it is situated at the rate limiting step of the
pentose-phosphate pathway for providing NADPH for red blood cells and hepatocytes.
With the reduced Glucose-6-phosphate dehydrogenase activity, supply of NADPH gets reduced, accumulation of
GSSG takes place, and control of Glucose-6-phosphate dehydrogenase activity is impaired, which in turn results in
the formation of methemoglobin, an oxidised and inactive form of hemoglobin.
And in severe cases wholesale destruction of red blood cells takes place known as hemolytic anemia.
Glucose-6-phosphate dehydrogenase activity is the only source of NADPH and GSH that is required for the
reduction of hydrogen peroxide, if not, being as strong oxidant H2O2 may degrade red blood cells leading to
hemolysis.
Even though there are many other metabolic pathway that produces NADPH in cells, red cells lack it and this has
profound effect on the stability of the red blood cells against the oxidative stress, as red blood cell contains only
glucose-6-phosphate dehydrogenase as NADPH producing enzyme.
Glucose-6-phosphate dehydrogenase is present in the cytoplasm of all the cells and it is particularly significant
in red blood cells as it lacks nuclei, mitochondria and other organelles, and this enzyme is particularly
significant.
When glucose-6-phosphate dehydrogenase present in red blood cells are not able to maintain NADPH levels that
in turn maintain glutathione levels, red blood cells rupture, leading to hemolytic anemia as it loses capacity to
with stand oxidative stress. Hence, the function of the normal Glucose-6-phosphate dehydrogenase is critical to
human survival.
A condition known as hemolytic anemia arise when the red blood cell can no longer transport oxygen effectively
throughout the body, and in addition to hemolytic anemia glucose-6-phosphate dehydrogenase deficient
individuals can expect several other manifestations of their conditions known as abdominal pain, stomach pain,
neonatal jaundice, dizziness, headache, dyspnea and palpitations.
Glucose -6-phosphate dehydrogenase
NADP
NADPH
Glutathione reductase
Oxidised glutathione (GSSG)
Reduced glutathione (GSH)
Glutathione peroxidase
H2O2
H2O
Free radicals
Oxidised state
Reduced state
Fig. 4.15 Schematic representation of role of glucose-6-phosophate dehydrogenase during oxidative stress

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 13
5. Creatine kinase
Q: Explain how creatine kinase acts as an important enzyme in tissues that lead important human performance
Creatine Kinase (CK) is a biologically important enzyme expressed by different tissues and cell types that
catalyse the reversible conversion of creatine at the expense of adenosine triphosphate to phosphocreatine.
Cells of the skeletal muscle, cells of the brain, photoreceptors cells of the retina, hair cells of the inner ear,
spermatozoa and smooth muscle rapidly consumes ATP , where phosphocreatine acts as an energy pool for
the rapid buffering and regeneration of ATP in situ, and also acts as intracellular energy transport by the
phosphocreatine shuttle.
Hence, creatine kinase acts as an important enzyme in such tissues. Creatine kinase may be cytosolic (Cy-CK)
or mitochondria (Mi-CK) (Fig.2.16).
Cytosolic creatine kinase of cells is dimer that is either brain type (B-type) or muscle type (M-type), and hence
exists in three isoenzymic forms such as CK-MM, CK-MB, and CK-BB.
Cytosolic creatine kinase regenerates ATP from ADP using phosphocreatine, and mitochondrial creatine
kinase is involved in the formation of phosphocreatine from mitochondrial ATP.
Cytosolic creatine kinase along with Ca2+ pump plays a major role in the energitics of Ca2+ homeostasis.
Mitochondrial creatine kinase is located in the mitochondrial intermembrane space, where it produces
phosphocreatine utilising ATP that is generated in the mitochondria and phosphocreatine that is imported
from the cytosol.
Mitochondrial creatine kinase along with the porin and adenine nucleotide translocase forms
microcompartment for vectorial export of phosphocreatine into cytosol.
The creatine kinase system is controlled by AMP-activated protein kinase through the ATP/AMP, and
phosphocreatine/creatine ratio.
Mitochondrial creatine kinase stabilizes and cross-links cristae or membranes that results in the formation of
parallel membrane stacks.
Here, if it gets over expressed either due to the depletion of creatine or development of cellular energy
stress, resulting in the formation of crystalline intramitochondrial inclusions as in the case of cytopathy
patients.
Mitochondrial creatine kinase is also gets damaged by the free radicals such as peroxynitrite. Mitochondrial
octomers along with the creatine kinase substrates are responsible for the stability and protection of
mitochondrial permeability transition pore (PTP) pores against opening, that is crucial patients with
neuromuscular and neurodegradative disease for creatine supplementation.
The enzyme creatine is biologically important as it is responsible for the energy homeostasis of cells with
erratic high energy requirement, energitics of calcium homeostasis and muscle contraction, adoptive
metabolic changes by acting as a energy sensor, metabolic channeling of the high energy phosphate
compounds, and mitochondrial permeability transition and early apoptosis.

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 14
One of the most crucial functions of the creatine kinase system in muscle is related to the energitics of Ca2+
homeostasis and muscle contraction.
MM-CK isoenzyme is specifically associated with the SR membrane to fuel the energetically highly demanding
Ca2+-ATPase required for Ca2+ regulation by SR.
Hence, in intact skeletal muscle under the condition of fatigue, Ca2+ regulation by SR gets impaired due to the
depletion of phosphocreatine.
MM-CK isoenzyme is also associated with myofibril and responsible for muscle contraction.
Creatine kinase is also linked to the AMP-activated protein kinase (AMPK) in radiometric sensing of
phosphocreatine and creatine.
AMP-activated protein kinase is able to inhibit creatine kinase to certain extent by binding tightly to muscle
type MM-CK and phosphorylates creatine kinase.
And on the other hand AMP-activated protein kinase itself is regulated not only by ATP/AMP ratio but also by
creatine/phosphocreatine ratio.
Hence, AMP-activated protein kinase is the energy sensor system and is involved in the regulation of the
adoptive metabolic changes, conditions such as post depletion of creatine level in skeletal and cardiac muscle.
Decreased creatine phosphocreatine ratio and increased AMP levels is responsible for the activation of
activation of AMP-activated protein kinase, hence high work load during muscle activation results in the
stronger inactivation of cytosolic muscle type MM-CK. Hence this system is involved in the adoptational effects
in the cardiac and skeletal muscle.
Mitochondrial creatine kinase located in the mitochondrial intermembrane space and the inner membrane is
responsible for metabolic channeling of high-energy phosphate compound.
Mitochondrial creatine kinase is responsible for the direct transphosphorylation of ATP produced within the
mitochondria into phosphocreatine, which subsequently is exported to the cytosol. Hence, mitochondrial
creatine kinase is functionally coupled to oxidative phosphorylation and facilitates the antiport of ATP versus
ADP through the inner membrane via the adenine nucleotide translocator (ANT).
Mitochondrial creatine kinase is also physically linked to outer mitochondrial membrane porin (VDAC) and
responsible for the exchange of energy metabolites between mitochondria and the cytosol.
Mitochondrial creatine kinase is physically interacted and functionally coupled to porin and adenine nucleotide
translocator (ANT), and involved in the regulation of mega channel, mitochondrial permeability transition pore
(MTP).
Mitochondrial creatine kinase is also involved in mitochondrial permeability transition (MPT), and this Ca2+-
dependent enhancement of inner membrane permeability to ions and solutes is also dependent on other
factors such as transmembrane potential difference, matrix pH, SH-group reactants and various effectors, and
hence the target of mitochondrial permeability transition is the target of components such as cyclosporine-A
that inhibits it.

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 15
Mitochondrial creatine kinase is also shown to functionally couple to adenine nucleotide translocator (ANT) and
form complexes with porin, and affects ANT-mediated permeability transition. Hence mitochondrial creatine
kinase as an energy channeling unit is not only involved in the high energy phosphate conversion and transport,
but also act as a protective regulatory component of the permeability transition complex.
Octomeric mitochondrial creatine kinase, depending on the cellular energy state and intracellular Ca2+, may
prevent mitochondrial permeability transition (MPT), which is an early onset of apoptosis in high energy
demanding cell with, and thus preventing or delaying the death of the cells.
adenine nucleotide translocator (ANT) to switch to its mitochondrial permeability transition pore (MTP)-like
state, which in turn results in apostasies.
ATP ADP Cr
Inter membrane space
Matrix
CK CK Mi- CK
CK CK Mi- CK
Oxidative phosphorylation Oxidative phosphorylation
PCr Cr PCr
ATP ADP
ADP ATP
ADP
ADP
IM ANT VNT VNT
Cytosol
VDAC OM VDAC VDAC
Cy CK Cy CK
PCr Cr PCr
ATP ADP ADP ATP
ATPase
Cy CK
PCr Cr
ATP ADP
Fig. 4.16 Schematic representation of biological role of creatine kinase

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 16
6. Trypsin
Trypsin is a serine protease found in the gastrointestinal tract of many vertebrates and is produced in the
pancreas in inactive form know as trypsinogen.
Trypsin hydrolyses the peptide chain generally at the carboxyl side of the amino acids such as lysine or
arginine, only if neither of these two is followed by proline.
Trypsin plays a major role in the duodenum as it hydrolyse the peptides into their smaller building blocks that
in turn facilitates the uptake of the protein in the food, as peptides are too big to be absorbed along the lining
of the ileum.
Enzymatic mechanism of the trypsin is similar to that of other serine proteases, as these enzymes contains a
catalytic triad of histidine-57, aspartate-102 and serine-195, by forming a charge relay that serve to make the
active site serine nucleophilic.
When the pancreas is stimulated by the cholecytokinine, trypsinogen is produced in the pancreas and then
secreted into small intestine, where it gets activated by small quantity of enteropeptidase or by Cathepsin B
into trypsin by proteolytic cleavage, followed by self activation of trypsinogen by resulting trypsin.
Once the trypsinogen is activated, it catalyse the activation of the other hydrolytic enzymes such as
chymotrypsinogen, proelastase, kallikreinogen, pro-carboxypeptidase, prophospholipase and procolipase into
chymotrypsin, elastase, kallikrein, carboxypeptidase, phospholipase and colipase.
This is very important mechanism as it prevents the auto-digestion of the pancreas by trypsin. One of the
consequences of the autosomal recessive disease known as cystic fibrosis that causes the body to secrete thick
and stick mucus blocking the organs such as lung and pancreas. In a normal person, epithelial cells produce
thin watery mucus that protects the body tissue by its lubricating characteristics.
Person with cystic fibrosis, this thick sticky mucus can block the pancreatic duct and prevents the pancreatic
enzyme reaching the duodenum that may lead to improper digestion, malabsorption, malnutrition etc.
Persons suffering from cystic fibrosis are categorised according to the functional status of the exocrine
pancreas, such as pancreatic insufficiency that requires exogeneous pancreatic replacement therapy with
meals observed in about 85-90% of the patients and pancreatic sufficiency that does not requires exogeneous
pancreatic replacement therapy with meals observed in about 10-15% of the patients with the evidence of the
pancreatic diseases.
Since mucus plug can obstruct the pancreatic duct and prevent the trypsinogen from reaching the intestine,
trypsinogen can reach the blood vessel due to the increased pancreatic pressure and back flow.
This immunoreactive trypsinogen level gets elevated in new born with cystic fibrosis. Since there is a transition
from pancreatic sufficiency to pancreatic insufficiency in new born, monitoring of the progress of the
pancreatic disease is very much important.
Since most of the clinical diagnostic methods for exocrine pancreatic function are too invasive or too
insensitive, a non-invasive tests such as the measurement of blood immunoreactive trypsinogen is helpful in

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 17
neonatal cystic fibrosis, or measurement of Reg protein in the blood is useful in cystic fibrosis patients as it is
found in higher levels in both in patients with pancreatic sufficiency and pancreatic insufficiency.
One more severe consequence can arise through inheritable alpha 1-antitrypsin deficiency, where the body
can create alpha 1-antitrypsin antibodies against trypsin leading to the series of cascading organ complications
in liver, lung and skin.
A deficiency of alpha 1-antitrypsin allows proteases to damage tissues in the body. Alpha 1-antitrypsin
antibodies deficiency effects both male and female of all ethnic background.
However many individual with this condition may not develop any disease associated with it, and in order to
develop alpha -1 antitrypsin deficiency an individual must inherit two abnormal Alpha 1-antitrypsin antibodies
(AAT) genes.
Individuals with the disorder are at increased risk of developing lung disease due to damage of the lung tissues
leading to a condition known as emphysema, a lung disease that results in shortness of breath.
These individuals are at increased risk of liver disease due to damage of the liver tissues leading to a condition
known as cirrhosis, a scarring of the liver.
Alpha 1-antitrypsin antibodies (AAT) genes deficient individuals are also at increased risk of having
panniculitis, a group of skin conditions that involve inflammation of the fat under the skin.
Symptoms of the disease may develop during infancy or in some individuals may have their symptoms get
worse over the time or not.
Trypsinogen can also initiate the auto digestive cascade charactering acute pancreatitis.
Activation of the trypsinogen into trypsin by brush borders enzyme enteropeptidase results in the release of
the 7-10 amino acid peptide N-terminal region of the trypsinogen that are immunologically completely distinct
from the same sequence within trypsinogen, known as trypsinogen activation peptide (TAP).
In case of acute pancreatitis, inappropriate and premature activation of the trypsinogen within the pancreas
results in the release of TAP into the peritoneum, plasma and urine.
Trypsinogen could be activated into trypsin either by brush border enzyme enteropeptidase in the small
intestine or by acinar cell lysosomal enzyme Cathepsin B, and also in human by auto activation.
Once it gets activated it can lead to the activation of number of other hydrolytic enzymes, leading to the auto
digestion of the gland.
There are two controversial major theories that have been postulated to explain the site and mechanism of
trypsin activation, such as the co-localisation theory that is more appropriate in rodents and the Trypsinogen
auto-activation theory that is relevant to human trypsinogen.
According to the co-localisation theory (Fig. 2.17) intra acinar cell activation of digestive enzymes is initiated
by lysosomal hydrolases either due to fusion mechanism where fusion of the zymogen granule and the
lysosomes, or due to missorting mechanism where non-segregation of the lysosomal enzymes from secretary
pathway with complete fidelity.

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 18
Hence, initiation of the acute pancreatitis occurs in a compartment containing both lysosomal hydrolases and
Cathepsin B. Actually, proteolytic and lipolytic pancreatic enzymes are stored as zymogens, pro-enzymes, and
get activated in the duodenum by duodenal enzymes.
However in the acinar cells, lysosomal hydrolases can activate trypsinogen and other zymogens. Hence, first
phase of the defense mechanism against this is the physical separation of granules of these zymogens and
activating hydrolases into two.
According to the co-localisation theory, in acute pancreatitis, this physical separation is lost, and that zymogen
and hydrolases co-localisation results in intra-acinar enzyme activation.
According second theory, known as trypsinogen auto-activation theory, activation of trypsinogen occurs in the
normal way at low pH and becomes pathological due to secretary blockade.
Under normal conditions, portion of human trypsinogen auto-activates to trypsin, and further catalyse a
cascade of trypsinogen that in turn activates other hydrolytic enzymes leading to auto-digestion of the glands.
However, this process is regulated by two defense mechanisms, first by serine protease inhibitor Kazal type 1
(SPINK1) and second by trypsin itself.
When the activity of the trypsin is at lower level SPINK1 inhibits the trypsin to prevent the further activation of
the trypsinogen and when the trypsinogen and other pro-enzymes, and if during excessive activation of
trypsinogen high activity of trypsin overwhelm the inhibitory capacity of SPINK1 resulting in increased
trypsinogen activation.
The second type of the defense is due to the trypsin by itself by feedback inhibition by trypsin and trypsin-like
enzymes, which hydrolyse the chain connecting the two globular domains of the trypsin at R122H resulting in
permanent damage of the trypsin.
Nucleus REC Golgi
Duct
Normal Pancreatitis
Lysosomal granules
Zymogen granules
Zymogen granules accumulate at the apex of the cells
Direct diffusion of zymogen with liposomal granules
Derangement of the intracellular sorting event of zymogen and lysosomal proteins
Activation of trypsinogen by Cathepsin B due to colocalisation
Fig. 4.17 Schematic representation of co-localization theory

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 19
7. Amylase
Amylase is found in both plants and animals, is a very important enzyme physiologically, commercially and
historically.
Amylase hydrolyses starch, glycogen and dextrin to glucose, maltose and the limit-dextrin.
Salivary amylase in humans is known as ptyalin begins the digestion of starch in the mouth and the
process is subsequently completed by pancreatic amylase known as amylopsin in small intestine.
Amylase is biologically significance as it is needed to digest carbohydrate, which is one of the three major
food groups needed for proper nutrition.
Carbohydrates in food are an important and immediate source of energy for the body. Carbohydrates
may be stored in the body as glycogen for future purpose and if it is eaten in excessive amount, our body
changes into fats and stores them in that form.
And, if the carbohydrates are not properly broken down before they are absorbed in the intestine,
subsequent health consequences can occur.
All amylases are glycoside hydrolases and acts on α-1, 4- glycosidic bond, and in human both salivary and
pancreatic amylases are α –amylase. α -amylase or α-1,4- D-glucan glucanohydrolase are calcium
metalloenzymes and completely unable to function in the absence of calcium, and it breaks down long-
chain carbohydrates by acting at random locations along the starch chain, yielding maltotriose and
maltose from amylose, glucose and limit dextrin from amylopectine. α –amylase is faster than β-amylase
as it is able to break the bond anywhere on the substrate.
Saliva is primarily produced in acini and secondarily in salivary duct, is a mixture of watery solutions of
electrolytes such as bicarbonate and K+, glycoprotein known as mucin and enzymes.
Water content and mucin of, lubricates foods, dissolve particles, salivary epidermal growth factor
promotes the healing of wound, electrolytes buffers the pH optimum of to 6.8 during first period in the
stomach to suit amylase, salivary lysozyme lyses bacterial cell wall, salivary amylase cleaves a-1-4
glycoside bindings in starch, and also other components such as immuno-defensive secretary globulin A
(IgA), amino acids, urea, and blood-type antigens in secreting persons.
As a whole, saliva dilutes injurious agents, cleans the mouth and pharynx to prevent caries and ease
swallowing. Secretion of the saliva is controlled by the autonomic nervous system and minimally
influenced by hormones.
The prevalent infection of the salivary glands is acute parotitis caused by the mumps virus. Similarly,
exocrine pancreas is an ‘abdominal-salivary-gland’, where secretions from the zymogen containing acinar
cells gets collected from the acinar duct and travel through a network of converging ducts to the main
pancreatic duct and then through common duct to duodenum.
Acinar cells produce primary secretions with an ionic composition similar to that of plasma and duct cells
forms the secondary secretion by modification of secondary secretion. These organic components present

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 20
in the saliva contain digestive enzymes such as α-amylase to digest starch, lipase to digest fats, and
protease to digest proteins, anti bacterial agents such as lysozymes, peroxidases, lactoferrin, histatins and
cystatins.
Human α-amylase is produced in the pancreas, salivary gland, to lesser extent in the fallopian tubes and
very little is present in other organs. Pancreatic amylase is secreted via the pancreatic duct and then
through common bile duct into duodenum, where it plays an important role in digestion of complex
carbohydrate.
Normally, in circulation 40% of the amylolytic activity is of pancreatic amylase and rest from the salivary
gland. Blood serum levels of amylase are of medical diagnostic importance, as a normal activity is in the
range of 21-101 U/L. Any deviation from this range is the reflection of one of several medical conditions
such as acute inflammation of the pancreas, perforated ulcer, ovarian cyst torsion, strangulation ileus,
macroamylasemia and mumps.
Amylase activity is also measured in other body fluids such as urine and peritoneal fluids. Measurement of
alpha amylase activity in serum is very much important in the evaluation of parotitis and pancreatic
disease. Amylase gets released into the blood circulation by damage to tissues containing high levels of
the enzyme or by escape from the gastrointestinal tract.
High levels of serum amylase is found in acute pancreatitis, chronic pancreatitis, mumps, parotitis, other
salivary gland disorders, perforated gastric ulcer, abdominal aortic aneurism, intestinal obstruction,
peritonitis, tubo-ovarian abscess, pancreatic pseudocyst, blunt abdominal trauma, macroamylasaemia,
renal diseases, drug abuse, chronic alcoholism and diabetic keto-acidosis.
Amylase is normally measures in plasma as test for pancreatitis. Serum amylase activity also gets elevated
in the implications of fallopian tube and salivary gland. However, elevated serum lipase activity is specific
for pancreatic disease.
The diagnosis of the acute pancreatitis is sometimes difficult to make, as it must be differentiated from
other acute intra-abdominal disorders, and on the other hand increase in serum amylase activity may not
necessarily due to pancreatitis.
Organ source of the enzyme is done by determining whether the major isoenzymes present are P-type or
S-type. Separation of amylase into pancreatic amylase (P1, P2, P3) and salivary amylase (S1, S2, S3)
isoenzymes is clinically significant to investigate pancreatic disorders. P2S1S2 is the common pattern in
normal individual, followed by P1P2S2, P2S2S3, and P2. In normal individual other less common forms such as
P1P2, P1 P2S2S3, and P1P2 also exists. Chronic pancreatitis, acute pancreatitis and renal transplantations P3 is
most common pattern.
Macroamylase are sometimes present in the blood sample, and these forms the believed to be due to the
complexes formed between ordinary amylase such as S-type and immunoglobulin such as IgA, IgG, or

dR
18BT53: Enzyme Technology and Biotransformation MODULE 2
D r . K r i s h n a P r a s a d N o o r a l a b e t t u
Page 21
other high molecular proteins. Since the molecular weight of such macroamylases are more than 2,
00,000, cannot be filtered through the glomeruli of the kidney and hence retained in the plasma.
This result in the increase of the serum amylase activity by 6-8 folds compared to normal individual is
known as macroamylasemia.
Even though, it has no clinical significance, this has been associated with celiac diseases, ulcerative colitis,
rheumatoid arthritis, lymphoma and HIV infection.
Hence, persistent elevated amylase with normal plasma lipase and no other features of pancreatic,
salivary or abdominal disease is suggestive of macroamylasemia.
Serum amylase activity is also increased in some non-pancreatic disorders, such as renal insufficiency,
renal impairment, tumors of the lung, serous tumor, ovarian tumor, salivary gland lesion, mumps and
maxillofacial surgery.