Embed Size (px)
Citation preview

INTRODUCTION • Orthopaedic surgery is that discipline of medicine that deals with the musculo-skeletal ligamentous structures of the body in health, injury, and disease. This specialty helps individuals stand erect and advance by walking against gravity. Orthopaedics also has a cross-over with other spe-cialties such as neurology, rheumatology, neurosur-gery, physiatry, and internal medicine.
Medical students learn how to conduct physi-cal examinations during their second year of post-graduate education. They start as neophytes, and the learning curve continues throughout their medi-cal careers. Over the years of practice, however, a physician becomes more proficient and develops a personal style and approach to patient evaluation. It is this unique interaction with patients that sepa-rates the medical field from any other occupation.
The components of a thorough medical evalu-ation include the following:
• The taking of a history
• Hands-on physical examination
• Review of diagnostic studies, if indicated
• An analysis of the medical records
• Clinical opinion
This chapter examines the individual parts of the orthopaedic evaluation, which encompasses the axial skeleton (spine) and the four extremities. The reader is introduced to the basics of the orthopae-dic and neurological independent medical exami-nation (IME), both from a theoretical and practi-cal approach. Written descriptions of the IME are supplemented through the use of photographs that reinforce the concepts presented in this chapter.
251
18The Independent Orthopaedic
Medical Examination
Noubar Didizian, M.D. and Samuel D. Hodge, Jr., Esq.

252 | Anatomy For Litigators
THE SCOPE OF THE INDEPENDENT MEDICAL EXAMINATION • IME stands for independent or impartial medical examination, though counsel for plaintiffs dub the examination the “defense physical.” IME patients are usually seen on only one occasion, and there is little or no doctor-patient relationship. The reader should review Chapter 17 for a discussion concerning whether the IME creates a doctor-patient relationship. An IME physician does not provide patient treatment, but can request diagnostic studies when indicated. The examining physician will also apply the same principles and components of medical evaluation whether the patient is seen for an IME or for treatment. The IME is requested by a third party such as an insurance carrier, employer, attorney, or govern-ment. It is, therefore, vital for the examining phy-sician to maintain objectivity despite the referral source. It is also important that the referring party not have unrealistic expectations as to what the evaluation can accomplish. Within this background, the IME physician has to separate and filter subjective complaints against objective findings. The latter are beyond the volitional control of the patient, such as scar forma-tion, muscle atrophy, spasticity or flaccidity, ampu-tation, and reflexes. Subjective complaints include allegations of weakness, fatigue, and decreased en-durance. The IME physician should be able to substan-tiate subjective complaints by objective means. The patient’s subjective complaints also deserve proper credence until disproved by inappropriate behav-ior exhibited by the patient during the history and examination phases. Even then, the data should be reviewed by the physician before making a clinical decision.
MEDICAL HISTORY • The patient’s medical history is the starting point for any examination. The examinee is asked questions, and the responses will be a factor in the final analysis. Sample inqui-ries include the following:“What is your age, height, and weight?”
“Are you married or single?”“Do you have children, and what are their ages? Do the children live with you?”“Are you right- or left-hand dominant?”“What is the date of injury?”“What is your occupation?” A detailed description of the pre-injury job should be obtained, with questions about when the job started, whether the employment was full- or part-time, and if it included overtime. The physician should also inquire as to the person’s current work status, physical demands of the job in terms of lift-ing (minimum and maximum), frequency of lifting, and amount of sitting, standing, walking, bending, reaching, squatting, kneeling, pushing, pulling, driv-ing, and climbing. If appropriate, responses should be obtained concerning the time devoted to work-ing on the keyboard, using the telephone, and using a calculator. It is important to learn how much time is spent writing to see if that activity will present an exacerbation of symptoms or could have been the originating cause of the problem. The history section should include a detailed description of the mechanism of injury such as whether the incident involved a motor vehicle ac-cident, work injury, or slip and fall. Other questions of interest are whether the injury was observed by a third party, if an ambulance was dispatched, wheth-er the patient went to the emergency room, and the treatment that was rendered subsequent to the inci-dent. The physician should also ask about medica-tions taken, physical therapy, whether surgery was performed, and if the patient went back to work. Diagnostic studies are very sophisticated and detect many asymptomatic abnormalities. There-fore, the patient needs to be asked if any diagnostic studies were performed and if the person has the reports. In fact, it is preferable for the physician to obtain the films for review. Abnormalities may be clinically irrelevant, arise from the result of improp-er positioning, or being read incorrectly.
Current Treatment The second part of the history deals with the patient’s current course of treatment. This includes asking for the names of the physicians that the ex-

Independent Medical Examination | 253
aminee is seeing on an active basis, the frequency of those visits, and the medications being used. If medication was taken on the day of the examina-tion, it is important to learn when it was taken, the response to the drug in terms of pain relief, and whether it causes drowsiness. Sleepiness is a danger-ous side effect, especially if the person has to drive or perform a job that requires dexterity or concen-tration. Physical therapy is part of the patient’s history of treatment; therefore, the orthopaedic specialist should learn the nature, duration, and response to therapy. Additional probing is needed to ascertain if the examinee was provided with equipment for home use such as a transelectrical nerve stimulation (TENS) unit, Theraband, or electrical stimulation and whether the patient is using an immobilizer such as a cast, brace, collar, or splint.
Past Medical History Causation is a component of the IME, so it is relevant to ascertain the person’s past medical his-tory in the form of allergies, operations, fractures, diabetes, and thyroid disease. For instance, a patient who complains of radiating pain from an alleged back injury may really be suffering from the effects of a diabetic neuropathy. Prior injuries are also part of the patient’s past medical history, and they are important to learn for obvious reasons. A person who hides previous incidents of trauma or illness certainly creates an unfavorable impression and raises credibility questions. Finally, the patient should be asked about heart and lung disease as well as blood pressure and vas-cular problems. A physician should never overlook asking about new injuries to the anatomical area in question. Not all people will volunteer this informa-tion, so it should be a standard question during the examination. Patients should even be asked about injuries during their childhood to see if a growth plate injury is involved in the current problem.
Social History This section focuses on the family unit, as well as learning if the person smokes or has a drink-ing habit. It is common knowledge that smoking
has a number of adverse consequences, including causing a delay in the healing process such as from back surgery. It also indicates that the person takes health risks.
Physical Activities The patient should be questioned about whether the physical symptoms interfere with sleep-ing and other activities of daily living. This includes inquiring about the comfortable range of walking, sitting, standing, and driving.
Symptoms And Signs By definition, symptoms are what the patient reports as complaints and include assertions of pain, stiffness, numbness, and radiating pain. On the other hand, signs are what the physician observes, hears, or feels during the examination. Examples include a rapid pulse, sweating, and tenderness to palpation. Questions concerning symptoms can be gen-eral or specific. General inquiries involve asking about the location, degree, and frequency of the pain, as well as relieving and aggravating factors. Specific questions focus on different anatomi-cal areas. For example, inquiries dealing with the cervical spine involve the following:• The presence or absence of radiculopathy, stiffness, limited motion, crepitation, referred pain, increase of pain with the Valsalva maneuver (coughing), and the presence or absence of long tract signs• The presence or absence of numbness or tingling, urinary or gastrointestinal incontinence, gait abnor-malities in the form of a drop foot or limping, and any particular weakness in the extremities For the joints of the body, such the shoulders, elbows, wrists, fingers, hips, knees, and ankles, ques-tions include the following:• Limitations in range of motion, swelling, trigger points, crepitation, or instability • Presence or absence of deformities or movements that produce symptoms As for the knee and ankle joints, additional questions about whether there is buckling or lock-ing are warranted.

254 | Anatomy For Litigators
Nervous System
The nervous system is divided into the central and peripheral nerves. The central nervous system is composed of the brain and spinal cord (see Fig. 18-1). The peripheral nervous system includes the cervical, thoracic, and lumbar nerve roots and their extension to the four extremities (see Fig. 18-2).
Figure 18-1
peripheralnervoussystem
Figure 18-2
In the cervical and thoracic spine, the nerve roots emerge as an extension of the spinal cord. In the lumbar spine, however, the cord ends at L1-2. Below that level, the spinal cord turns into the cau-da equina, a collection of individual fibers that re-semble a horse’s tail. These fibers travel down from the L1-2 level and exit at the appropriate neural fo-ramen in the form of the L2, L3, L4, L5, S1, and S2 nerve roots. The primary unit of the nervous system is the neuron, and the brain contains billions of these units (see Fig. 18-3). The neuron is made of an axon and a dendrite, as well as the communicating sys-tems between those units.
Figure 18-3
The vertebral system is made of seven cervi-cal, 12 thoracic, and five lumbar vertebrae, as well as five fused sacral and five fused coccygeal verte-brae (see Fig. 18-4).
Figure 18-4
The first cervical nerve emerges between the occiput and the C1 vertebra, also known as the atlas. The C2 vertebra is called the axis. Half of cervical rotation takes place between the atlas and the axis, and half of extension-flexion takes place between the occiput and C1 (see Fig. 18-5). The rest of the vertebrae contribute to those two movements as well. Tilting of the neck is a com-bination of rotation, extension, and flexion units us-ing different sets of muscles (see Fig. 18-6). All nerve roots carry motor and sensory fi-bers (see Fig. 18-7). Certain roots also carry reflex fibers. The sensory fibers include afferent fibers that transmit stimuli from the extremity into the spinal cord and then to the cerebral cortex. When someone touches a hot object, the afferent fibers carry that sensation to the spinal cord and the mo-

Independent Medical Examination | 255
tor, or efferent, fibers immediately pull the fingers away from the heat. This sequence takes a frac-tion of a second and is mediated at the spinal cord level, which is also known as the reflex arc. Most non-emergency movements are coordinated by the cerebral cortex, which includes the sensory cortex and motor cortex.
Figure 18-5
Figure 18-6
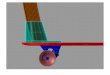
SPINAL NERVEDorsal Root
Spinal NerveVentral Root
White Matter
Dorsal RootGanglionGray Matter
Figure 18-7
Sensory fibers detect such stimuli as pain, tem-perature, position, stereognosis (identification of objects when palpated in the hand), graphesthesia (identification of writing in the palm of the hand), and two-point discrimination (see Fig. 18-8). Chang-es in light touch and pain sensation associated with sensory nerve involvement include the following: • Decreased sensation (hypesthesia) • Total loss of sensation (anesthesia) • Perversion of sensation (paresthesia)
Figure 18-8
While the examiner is conducting testing for sensory changes with a pinwheel, the patient will respond subjectively to the three categories listed above (see Fig. 18-9).
Figure 18-9
The physician will mark the areas of alterations in sensation and try to match them to a dermatome. Every sensory nerve has a dermatomal pattern as far as cutaneous innervation is concerned. These dermatomal patterns are well defined in anatomy books, but the patient’s responses to the sensory examination are subjective. Counsel will be