Embed Size (px)
Citation preview

7/23/2019 18 Dr Ramesh Babu.pdf
http://slidepdf.com/reader/full/18-dr-ramesh-babupdf 1/7
___________________________________________________ ____________________
_______________________________________________________________________________________
Copyright ©2013
Review Article
J Res Adv Dent 2013; 2:3:91-97
Role of Dental Microscope in General Dental Practice
Kiran Kumar Nagubandi1 Vijaya Laxmi2 Ramesh babu Mutthineni3* Sabitha MR4
1Professor, Department of Periodontics, Mamta Dental College, Khammam, Andhra Pradesh, India.2Professor, Department of Periodontics, Farookiya Dental College, Mysore, Karnataka, India.
3Reader, Department of Periodontics, Mamta Dental College, Khammam, Andhra Pradesh, India.4Reader, Consultant Periodontist, Apollo White Dental Studio, Chennai.India.
ABSTRACT
Objective: The Dental microscope is an indispensible tool in dental practice. Dental therapy with high quality
and perfection is the basis for long term function and biological success, ensuring that patients remain free of
pain. State of the art equipment and thorough clinical knowledge however are vitally important to reach this
goal. The purpose of this review article is to explain the use of Dental Operating Microscopes in various branches
of dentistry providing you with new dimensions of knowledge for your every day work.
Material and Methods: A wide variety of dental microscopes which were used in the past and in the new era
were discussed.
Results: With the help of Dental Operating Microscope there is better visualization of the operating field and
hence treatment quality can be improved.
Conclusion: The dental microscope with all its advantages is now absolutely indispensable in any quality and
outcome oriented dental practice philosophy.
Keywords: Dental operating microscope (DOM), Mechanical optical rotating assembly (MORA), General dental
practice.
INTRODUCTION
DOM allows amplification of details, greater
versatility in image magnification, excellent
visualization of the working field, best lighting
possible and a better working posture.
Basically a DOM consists of a light source
and a suspension system.DOM allows the
visualization of textures and details of anatomical
structures, restorative materials and prosthetic
components that would not be visible even with
loupes.
HISTORY
In 1953, the Carl Zeiss Company of West
Germany marketed the first commercial binocular-
operating microscope. The pioneeringwork of Carl
Nylen at the University of Stockholm preceded,Zeiss
by approximately 31 yr with the development of a
monocular microscope for ear surgery in 19221,2 .
From then onwards microsurgery has spread to
literally all the surgical disciplines.
It wasn’t until 1978 that Apotheker, and
Jako, pooled their efforts to produce a DOM(Dental
Operating Microscope)3,4. Their designs were
incorporated in 1981 into the first commercially
available DOM (Dentiscope, Chayes-Virginia Inc.,
Evansville, IN).

7/23/2019 18 Dr Ramesh Babu.pdf
http://slidepdf.com/reader/full/18-dr-ramesh-babupdf 2/7
92
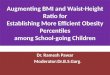
Fig 1: Showing Different parts of microscope
Fig 2: Dental Operating Microscope(DOM)
In March of 1993, 11 yr after the introduction of the
Dentiscope, the first symposium on microscopic
endodontic surgery was held at the University Of
Pennsylvania School Of Dental Medicine. By 1995,
there was an marked increase in DOM use by
endodontists.
DENTAL MICROSCOPE (Fig-2):
Parts of a microscope given in Fig-1.,
Basically a DOM consists of an optical head, a light
source and a suspension system. It has a 180°
tiltable tube with angled optics, the ergonomically
designed grips, and the focusing objective lens
adjustable for left-handed and right-handed
persons. In 1998, Friedman et al. reported that the
microscope is unusable in certain areas of the
mouth, as the 9-10 o’ clock seating positions allow
for securing the smallest distance possible between
the operator and the patients mouth, while allowing
a direct visual access in to the oral cavity when the

7/23/2019 18 Dr Ramesh Babu.pdf
http://slidepdf.com/reader/full/18-dr-ramesh-babupdf 3/7
93
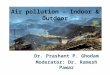
Fig 3: Showing MORA Interface
patient is reclined in to a supine position.
Unfortunately the access opening to the mouth hasa downward inclination towards the chin. This in
turn forces the operator to assume inclined neck
posture with over extension of left arm to hold
mouth mirror for use. This combination of muscle
tension leads to fatigue, pain and musculo skeletal
disorders. To overcome this difficulties MORA
interface was developed
MORA INTERFACE: :(Fig-3)
Definition of the MORA interface
The “MORA interface” is a mechanical
optical rotating assembly that connects at a right
angle the binocular tube to the body of the
operating microscope to make it capable of a limited
independent rotation around the horizontal axis of
the binocular tube.This allow the operator to be
seated in the 12 o’ clock position and allow for
adequate extension of microscope between the
objective lens and the eye pieces which prevents the
operator from bending forward to reach the
eyepieces, which causes strain on the lower back .
USES OF DENTAL MICROSCOPE IN VARIOUS
BRANCHES OF DENTISTRY
Visualization of pathological findings for patients-
communication
DOM helps in visualization of pathological
findings. In addition to visualization, these
recordings can also be used to provide convincing
evidence to insurance companies. These video
recordings also enable dentists to reexamine
complex therapies. Comfortable treatment and
ergonomics due to technological advantages and
improved treatment quality.
Since, with a dental microscope, it is
technically feasible to feed xenon light in to the
observer’s beam path view at an angle of less than 4
degrees, illumination of surgical field is perfect. In
conjunction with motorized zooming every local
detail can be recognized, especially in endodontics.
Microscopic techniques are superior to traditional
treatment concepts, as has been proven by various
studies5-8.
Conservative, adhesive restorations after systemic
caries excavation
If caries is to be excavated close to the pulp,the dental microscope is very useful because, of its
shadow free light in conjunction with rhodium
plated mirrors, it is excellent for distinguishing even
the minutely infected areas. The closer to the pulp
the operator needs to work while removing caries
the more this type of optical vision enables great
care to be exercised.As the DOM gains widespread
acceptance in endodontics, the advantages of its use
in providing precision care will carry over in to
restorative dentistry, and it will eventually become
a universal approach for all phases of dentistry.9-15
Routine dental techniques-tooth extractions with
complications
Many a times a seemingly simple extraction
of a devitalized tooth or the extraction of a partially
retained wisdom tooth may end up in a
complication. When the tooth fractures, individual
fragments can only be removed with difficulty due
to sclerosis of the individual roots with the bone,
and vision is impaired by bleeding. In these cases
the dental microscope provides steady conditionsdue to its excellent illumination and adjustable
magnification. The dentist can zoom down to depth
of the extraction alveolus and thus very precisely
mobilize a stubborn root remnant if the assistant
ensures minimal bleeding with the use of a special
micro aspirator. With microscope assisted tooth
extraction the alveolar bone can also be preserved
with a view to subsequent implantation .
Periodontal therapy in visually
inaccessible(subgingival) root sections

7/23/2019 18 Dr Ramesh Babu.pdf
http://slidepdf.com/reader/full/18-dr-ramesh-babupdf 4/7
94
In closed or open periodontitis therapy,
based on the full mouth therapy concept . One often
has the problem that the deep sub gingival pockets
or interdentally recessions and furcations already
affected by bone destruction are hardly accessible
to the naked eye. Due to the optical benefits
mentioned and the illumination of the surgical field,
we can use dental microscope in these instances
because it is possible to detect any clinging islands
of biofilm and remove them precisely.
Microsurgical techniques in periodontal plastic
surgery and implant surgery
Application of microsurgical principles from
vascular surgery to plastic dental surgery created a
desire to use very fine suture material at a high levelof magnification. Apart from the development of
microsurgical instruments it was the medical loupes
with a magnification of approximately 5x and the
dental microscope with an even higher
magnification that made it possible to see size 7.0 or
8.0 suture materials. Incised sections of papilla
must be adapted as precisely as possible, especially
in the crucial, highly aesthetic, anterior gingival
region. Here, a dental microscope allows excellent
monitoring of suture use and ligature placement.
Microsurgery offers new possibilities to
improve periodontal care in variety of ways.Its
benefits include improved cosmetics, rapid healing
and minimal discomfort and enhanced patient
acceptance. Periodontal microsurgery appears to be
a natural evolution for the specialty of
Periodontics16.
Orthograde and retrograde endodontics-the domain
of the dental microscope
The long term success rate in orthogradeand retrograde endodontics have risen toward
100%, firstly due to the more conservative
preparation philosophies and the thermoplastic
filling technique, and secondly due to the use of
dental microscopes. The shadow free, bright xenon
light enables the straight canal sections to be
examined right down to the constriction.
Ledges, branches, fractured instruments,
perforations, foreign bodies, and even, isthmus like
branch lines can be localized and simultaneouslytreated with slender ultrasonic tips under optimal,
magnifying vision. The localization of absent canals,
pulp denticles, tooth colored restorations in the
pulp chamber, and the removal of old, insufficient
root canal fillings is much more reliable when using
magnification systems such as dental microscope or
medical loupes.
If, despite a seemingly sound orthograde
root canal filling, apical inflammation does occur in
a few cases-usually where apical ramifications are
inaccessible-a dental microscope is of great help in
apical microsurgery. Again the filigree apical
portion of the root can be removed under optical
illumination and the leakage delta responsible for
the inflammation prepared with ultrasonic tips and
ligated with a suture.A very convincing study
concerning the benefits of microsurgical procedures
was reported by Rubinstein and kim in 19996,7.
Diagnosis of a minute longitudinal fracture is often
only possible at a magnification level exceeding 12x
to 15x. Here too, the dental microscope provides
useful diagnostic reliability
Precise control of prosthetic preparations and
impressions
In order to ensure precise preparation of a hard
tooth structure, especially in the final phase ofpatient rehabilitation performed according to the
treatment plan, it is essential to provide the dental
technician with preparation margins that are as
accurate as possible-irrespective of whether the
restorations are to be made of gold or porcelain.
Finishing of the prepared crown can be done under
dental microscope. As the part of the chain of
precise quality assurance, one can quickly check the
impressions for accuracy under the dental
microscope. With an evolving level of training one
can employ the dental microscope quickly and inmany different ways, without slowing down the
working procedure significantly.
The role of the operating microscope in the
preparation stage of fixed prosthetics
The preparation stage of fixed prosthodontic
case is technically demanding. Many factors
determine the final design of the preparation,
including the required reduction of tooth
structure, detection of marginal caries,
fractures, furcations and the need for themargins of the restoration to be placed on solid

7/23/2019 18 Dr Ramesh Babu.pdf
http://slidepdf.com/reader/full/18-dr-ramesh-babupdf 5/7
95
tooth structure. Several clinicians suggested
that DOM can be used to improve tooth
preparation and final restoration in fixed
prosthodontics.17-23
In addition, the clinician must consider the
aesthetic, functional, and biologic principles
regarding placement at the margins of the
restoration and the type of margin best suited
for the tooth. While the successful provision of
inlay, onlay, and crown restorations depends
upon a solid understanding of the above,
successful treatment predicted on the ability of
the clinician.
The dental operating microscope can be used
for the entire preparation of a tooth, but somedentists use loupes for gross reduction of tooth
structure before using the microscope to finish
the preparation.
Gross reduction of tooth structure is
accomplished using medium magnification,
and margins are completed using
magnification.
After finishing the margins, the preparation is
examined at a lower magnification to ensure
that no undercuts have been created.
Clinically the use of higher magnification for
preparation of margins appears to reduce the
degree of taper of the preparations.
Close attention must be given to the lines
drawn and parallelism when preparing
multiple abutments for a fixed bridge.
An important benefit of higher magnification is
the ideal placement of the crown or veneermargin.
Cutting at high magnification polishes the
margin, resulting in a smooth and discernible
finish line.
In contrast to high magnification, at medium
magnification the entire visual field is occupied
by one tooth.
At the higher magnification, only part of the
tooth (2 or 3 surfaces) is visible at a time.
Advantage of using higher magnification is the
reduction of peripheral “visual noise”.
Therefore, properly trained auxiliary
personnel are essential.
When first using the microscope for crown and
bridge procedures, the clinician will find that it
takes longer time to prepare teeth for crowns
as compared to conventional technique. It
takes time to develop the motor skills
necessary to work at higher magnification.
The role of the operating microscope during the
insertion stage of fixed prosthesis
Once the impression reaches the lab, it is ideal
if the laboratory uses magnification during thefabrication of the prosthesis. Laboratory
technician can more precisely trim stone dies
with the aid of a microscope. During trial in
and seating appointment, the microscope is
very useful.
After the final margins have been completed,
another benefit of the operating microscope is
improved tissue management. The provisional
restoration can be trimmed under the
microscope, ensuring that the restoration is
well adapted and will allow for the healing of
the tissues during the provisional stage.
The role of operating microscope in orthodontics
After orthodontic brackets debonding,
there is a residual layer of composite left on the
enamel surface that should be removed. These
composite remnants on the enamel are potential
plaque traps. Dental microscope can be used to
examine carefully remnants of composites and
finishing of tooth surface can be done precisely.Stereomicroscope offers great possibilities of
enamel surface investigation, providing high quality
images with good sharpness23-25.
The used microscope was a binocular light
stereo microscope -Olympus SZx ZB 12 with a
WHS 30X-H ocular, a DFP LAP07 X PF lens and
3100 light system for photo micrography.
The camera was placed on the microscope and
connected to a computer and a frame grabber
of the same manufacturer.

7/23/2019 18 Dr Ramesh Babu.pdf
http://slidepdf.com/reader/full/18-dr-ramesh-babupdf 6/7
96
After cleaning the enamel surface, each surface
was examined in the following two
magnification modes:
-50x for the entire buccal tooth surface.
-For the four quadrants of the same surface.
RESULTS
Today the world’s leading dental
practioners are largely in agreement that DOM has
pushed the limits of treatment potential a long way
toward enhancing long term patient outcomes. In
particular, the digital visualization technology in
combination with the dental microscope can be
used as a powerful documentation tool for patient’s
records, legal documentation as well as the
education of the dental profession. With the help of
DOM there is better visualization of the operating
field and hence treatment quality can be improved.
DISCUSSION
The eventual dramatic change from casual
interest in microscopes to fevered involvement
heralded a new era in endodontics. Undoubtedly the
current wide-employment of DOMs in endodontics
speaks to, their obvious advantages. Microscopy inendodontics has certainly come of age, but its
gestation period was surprisingly long. With a
microscope, dental procedures can be performed
more accurately and more reliably using variable
and adjustable magnifications and shadow free light
due to a coaxial radiating light source.
In general, magnification can be set to 4x
and 24x, thereby expanding the diagnostic options
due to better lighting and sight. For example, most
fissure caries and micro fractures cannot be seenwith the naked eye. With the aid of a microscope it
is even possible to view down to the apex of a
straight root canal.
Additionally clinicians will experience an
increase in job satisfaction. Many procedures are
simplified and accelerated greatly, as much better
visibility is provided with the
microscope.Treatment results become more
predictable. For example, the outline preparation
and assessment for a crown preparation becomes
much simpler. Making a cast impression is also no
longer problematic. Moreover, working with a
dental microscope improves ergonomics.
Furthermore, the patients can be better
counseled and educated. With a video camera
attached to the dental microscope, the images can
be recorded directly. This greatly simplifies the
counseling of patients because, as we all agree,
sometimes an image talks more than a thousand
words.
Although operating microscopes can
greatly enhance dental practice there are some
disadvantages especially at the initial stages.
Sometimes specific training may be necessary. An
operator using DOM cannot see his hands or fingers,
only the tip of the instruments can be seen, and theyare used in delicate movements of small amplitude.
High initial cost of the equipment and instruments,
the need for retraining of the auxiliary staffand an
adjustment for the new treatment paradigms and
operator postures are other disadvantages.
The dental microscope has many benefits,
and when integrated with documentation devices it
offers an unparalleled opportunity to document
patient care in an efficient manner and unique
perspective .Future clinical advancements will makethe microscope an essential part of daily patient
care.
CONCLUSION
The dental microscope, in conjunction with
further technological developments and an increase
in experience, is bound to lead to specialization that
will continue to enjoy a high degree of protection
against emulation in the competitive world of
dentistry.
One advantage of the dental microscope
that should not be under estimated, especially in the
physically and psychologically highly strenuous
dental profession, is a healthy, namely upright,
working posture. Due to its superior technological
features the convenience to use microscope can
provide the dentist with considerable quality of life
and good health. To put it crudely, the microscope
can “hump up” for us as we sit in a highly
ergonomic, upright position keeping the spine
relaxed.

7/23/2019 18 Dr Ramesh Babu.pdf
http://slidepdf.com/reader/full/18-dr-ramesh-babupdf 7/7
97
The popularity of the dental operating
microscope will likely increase in the future for
prosthodontic procedures also.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this
article was reported.
REFERENCES
1. Hoerenz P. The design of the surgical microscope:
part I. OphthalmicSurg 1973; 4:40–45.
2. Dohlman CF. Carl Olof Nylen. The birth of the
otomicroscope and Microsurgery. Arch
Otolaryngology 1969; 90:813–817.
3. Apotheker H, Jako GJ. A microscope for use in
Dentistry. J Microsurg1981;3:7–10.
4. Apotheker H. The applications of the dental
microscope: preliminary Report. J Microsurg
1981;3:103–106.
5. Baldassari-curz.a., lillyJ.p, Rivera
e.m.(1998):effectiveness of mesiolingual canal
location with and without use of microscope.
J.Endod 1998;24:287-290.
6.Rubinstein R.A.,Kims S:Short term observation of
the results of Endodontic surgery with the use of a
surgical operating microscope and super-EBA as
root end filling material.J. Endod 2002;28:378-383.
7.Rubinstein R.A., Kim S.:Long term follow up of
cases considered healed one year after apical
microsurgery.J. Endod 2002;28:378-383.
8. Stropko J.J.Clinical observations of canal
configurations.J.Endo 1999;25:446-450.
.
9. Carr GB.Magnification and Illumination in
Endodontics.in: hardin FJ, editor.Clark’s clinical
dentistry,vol 4 st.louis,MO:Mosby:1998.p 1-14.
10. Sheets CG, Paquette JM. The magic of
magnification.J. Dent today 1998:17(12):60-63.
11. Carr GB.Endodontics at the crossroads.J Calif
Dent Assoc 1996:24(12):20-26.
12. Carr GB.Ultrasonic root end preparation. Dent
Clin North Am 1997:41(3); 541-54.
13. Castellucci A. Magnification in endodontics; the
use of the operating microscope. J.Aesthet Dent
2003; 15(5):377-384.
14. Murgel CAF, Gondim E Jr, Souza Filho FJ.Surgical
microscope; the search for excellence on clinical
dentistry. Rev da assoc Paul cir dent 1997:51:31-35
15. sheets CG, paquetteJM. Enhancing precision
through magnification.J Dent today.1998; 17:44-49
16. Sheets CG, Paquette JM. The magic of
magnification. J.Dent today.1998; 17:60-67.
17.Friedman MJ, Landesman HM.Microscope
assisted precision (MAP) dentistry: advancing
excellence in restorative dentistry. J.Contemp
Esthet.1997; 1:45-50.
18.Cruci p. An operating microscopeingeneral
dental practice. J.Dent pract.1999; 37:1-5.
19. Friedman M, Mora AF, Schmidt R.Microscope
assisted precision dentistry.J.compend contin educ
dent.1999; 20:723-736.
20. Piontkowski PK. The renaissance of dentistry;
an introduction to the surgical microscope.J.dent
today.1998; 17:82-87.