Embed Size (px)
Citation preview

8/10/2016
1
Brian Forsythe, MDAssistant Professor
Division of Sports MedicineHead Orthopedic Officer: Chicago Fire Soccer Club
Team Physician: Chicago White Sox & Chicago BullsMidwest Orthopaedics at Rush, Rush University Medical Center
Case 1
Case Presentation
23 year old healthy male
• Special Education teacher
• Former D3 collegiate soccer player, assistant varsity coach
• Collided with an opposing player during a soccer tournament, falling on the lateral aspect of his leg
• Immediate onset of pain and swelling, no “pop”
Interval History
• Completed 5 wks of PT
• Describes his knee as 70% of normal
• Experiences pain with kicking and passing
• No improvement w derotational brace
• Seen by my colleague initially, then referred to me for a 3rd opinion
• Symptoms persist over 6 months
8/10/2016
2
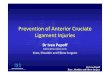
Physical Examination
• 5’10”, 187 lbs. WD/WN, somewhat anxious.
• Range of motion from 0-130 degrees
• 2A Lachman, positive pivot glide exam
• Alignment neutral
• Stable to valgus and varus stress
• No joint line tenderness
• Negative flexion McMurray
• Mild asymmetry with single leg hop
• 5/5 lower extremity strength
Radiographs
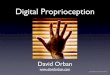
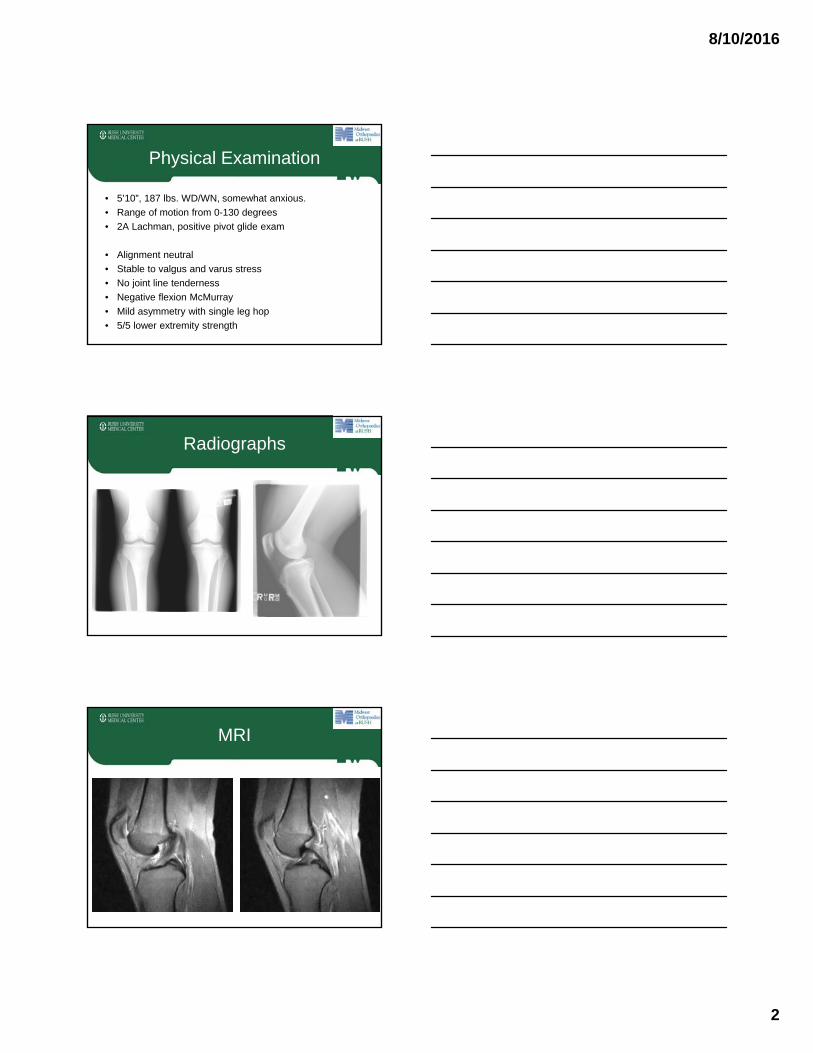
MRI
8/10/2016
3
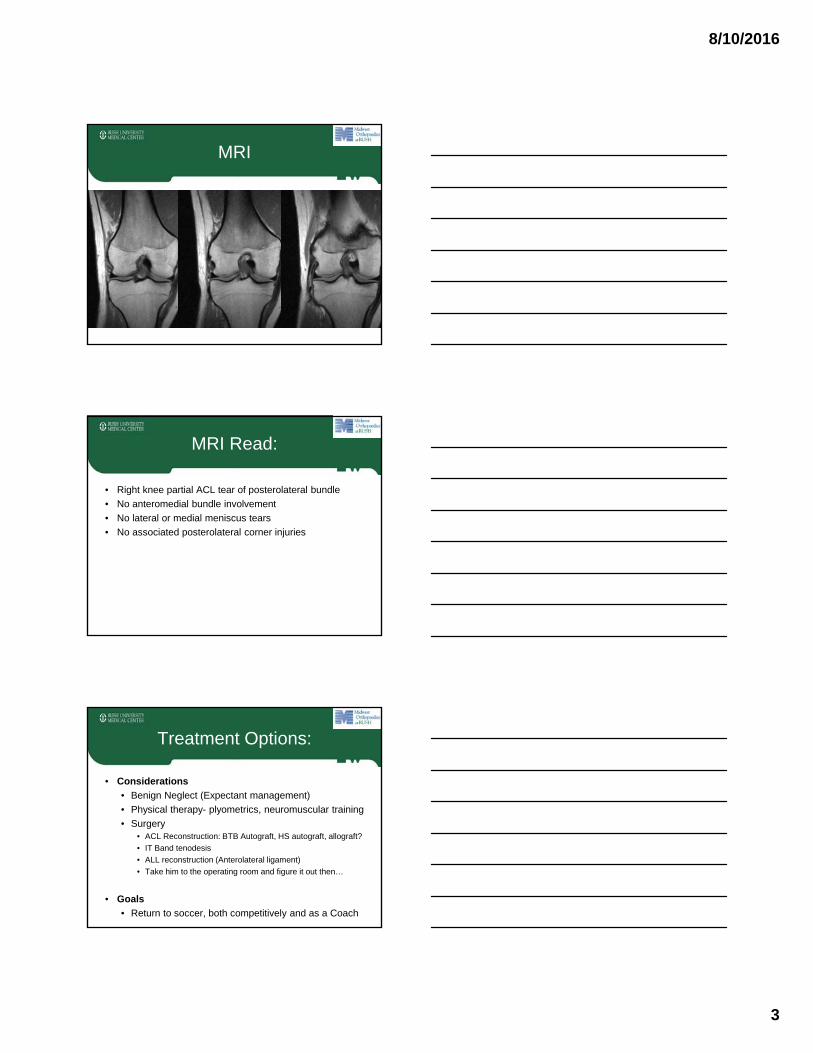
MRI
MRI Read:
• Right knee partial ACL tear of posterolateral bundle
• No anteromedial bundle involvement
• No lateral or medial meniscus tears
• No associated posterolateral corner injuries
Treatment Options:
• Considerations
• Benign Neglect (Expectant management)
• Physical therapy- plyometrics, neuromuscular training
• Surgery• ACL Reconstruction: BTB Autograft, HS autograft, allograft?
• IT Band tenodesis
• ALL reconstruction (Anterolateral ligament)
• Take him to the operating room and figure it out then…
• Goals
• Return to soccer, both competitively and as a Coach

8/10/2016
4
Arthroscopic Pics:
8/10/2016
5
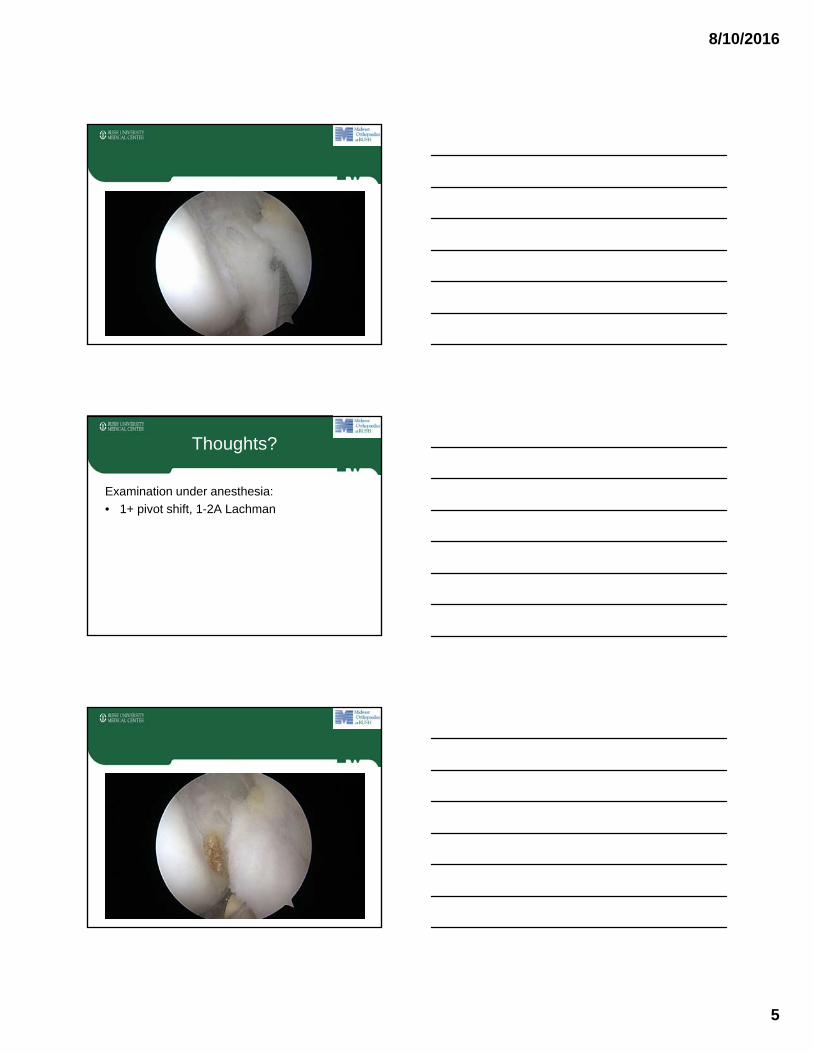
Thoughts?
Examination under anesthesia:
• 1+ pivot shift, 1-2A Lachman

8/10/2016
6
Arthroscopy Video
Two functional bundles:
No impingement

8/10/2016
7
Postoperative Course
• 1 week
• Range of motion from 0 to 90
• Has a 30-degree lag on straight leg raise. He has some mild interstitial edema and trace intraarticular effusion.
• 5 weeks
• Range of motion is +1 to 120 degrees
• 20 cc intraarticular effusion
• Stable 1A Lachman and a stable pivot shift.
Postoperative Course
• 10 weeks
• Pain-free at baseline and feels 100% of normal w/ ADLs
• Range of motion is +2 to 135 degrees
• Stable exam
• 15 weeks
• Range of motion of the right knee is +2 to 135 degrees
• Running without difficulty, progressing with agility training
• 5 months => Back to soccer
AM Bundle Reconstruction
• Sonnery-Cottet et al. (2012) found sig improved scores in patients undergoing AM bundle reconstruction
• Mean follow-up of 26 months
• Retrospective, multicenter study of n=168
Partial ACL reconstruction with preservation of the posterolateral bundle (2012) Orthopaedics & Traumatology: Surgery & Research
8/10/2016
8
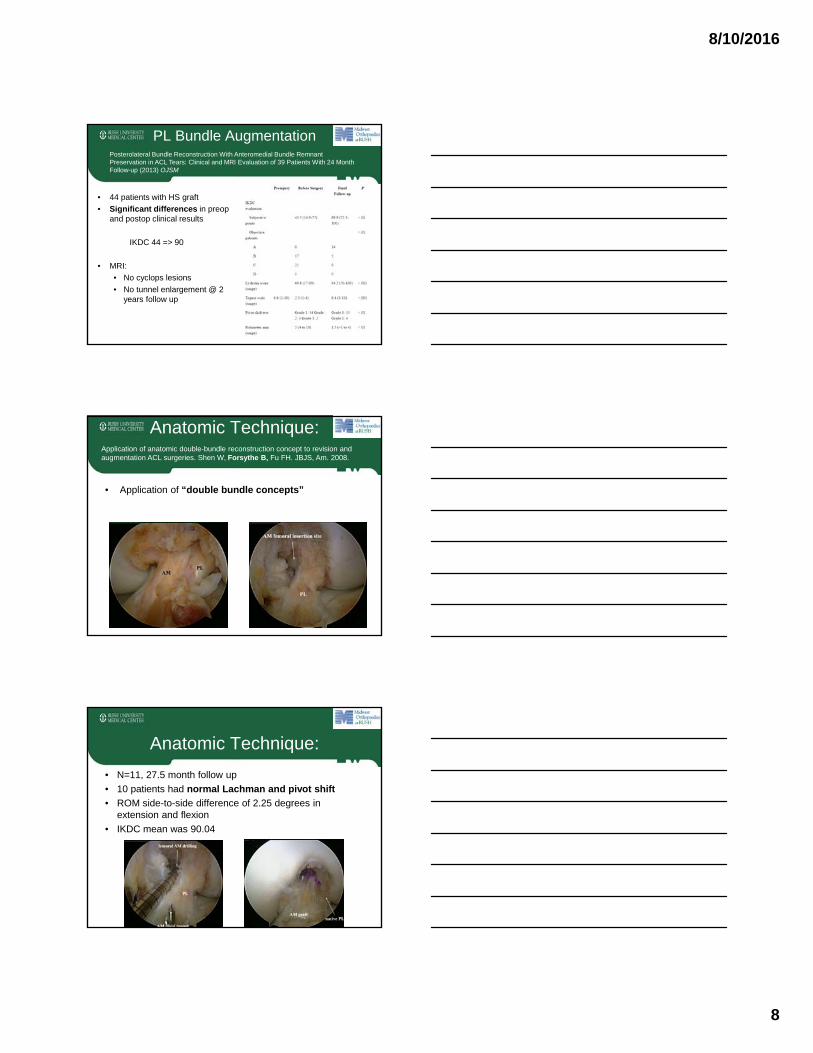
PL Bundle Augmentation
• 44 patients with HS graft
• Significant differences in preopand postop clinical results
IKDC 44 => 90
• MRI:
• No cyclops lesions
• No tunnel enlargement @ 2 years follow up
Posterolateral Bundle Reconstruction With Anteromedial Bundle Remnant Preservation in ACL Tears: Clinical and MRI Evaluation of 39 Patients With 24 Month Follow-up (2013) OJSM
Anatomic Technique:
• Application of “double bundle concepts”
Application of anatomic double-bundle reconstruction concept to revision and augmentation ACL surgeries. Shen W, Forsythe B, Fu FH. JBJS, Am. 2008.
Anatomic Technique:
• N=11, 27.5 month follow up
• 10 patients had normal Lachman and pivot shift
• ROM side-to-side difference of 2.25 degrees in extension and flexion
• IKDC mean was 90.04
8/10/2016
9
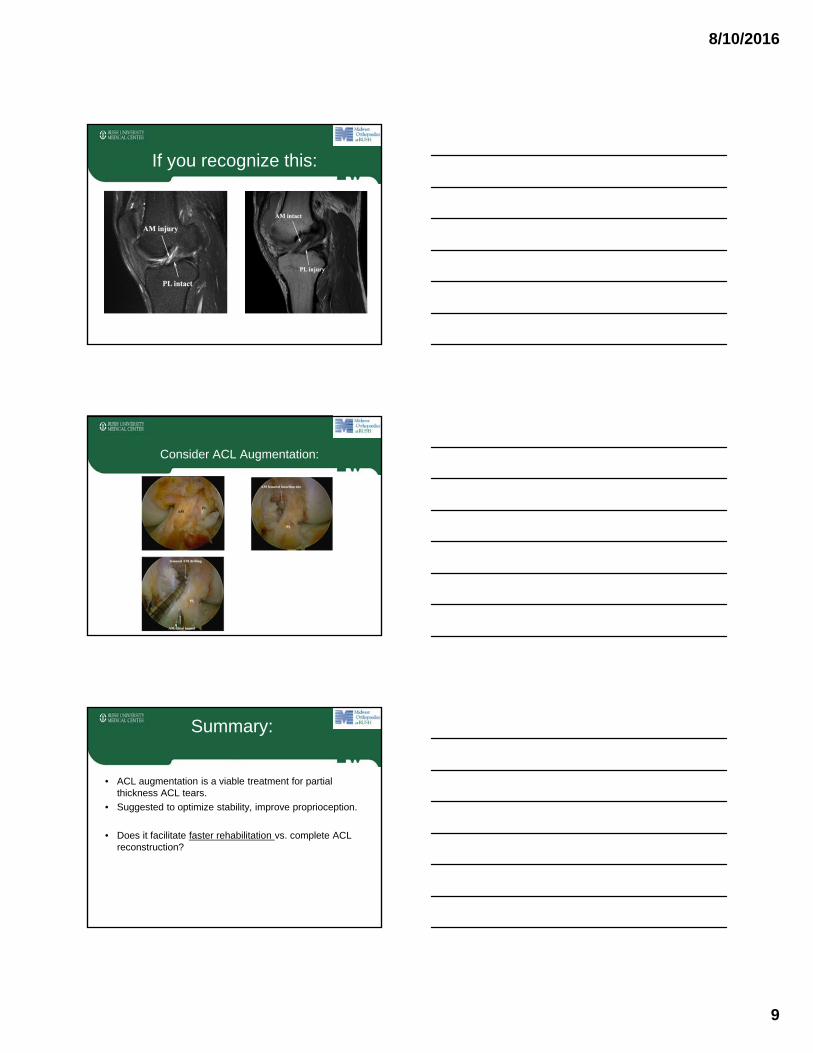
If you recognize this:
Consider ACL Augmentation:
Summary:
• ACL augmentation is a viable treatment for partial thickness ACL tears.
• Suggested to optimize stability, improve proprioception.
• Does it facilitate faster rehabilitation vs. complete ACL reconstruction?

8/10/2016
10
Brian Forsythe, MDAssistant Professor
Division of Sports MedicineHead Orthopedic Officer: Chicago Fire Soccer Club
Team Physician: Chicago White Sox & Chicago BullsMidwest Orthopaedics at Rush, Rush University Medical Center
Case 2
History:
16 year old healthy female
• Previous ACL R and LMD, 11/2013, soccer injury, as a 14 year old.
• Completed a rehabilitation exercise program pre and post-operatively
Current History:
• Right knee buckled during soccer game for U16 team
• No immediate swelling; however, swelling developed over 24 hrs.
• Attempted to practice, but knee gave way and swelling recurred.

8/10/2016
11
Physical Examination
• Active range of motion from +5 to 140 degrees
• 2B Lachman, 3+ pivot shift
• Alignment: approx 3 degrees of valgus
• Stable to varus, valgus stress 0 and 30 degrees
• Negative McMurray's exam
• Trace effusion
• No joint line tenderness
• Neurovascular exam intact
• 5-/5 quad strength
Radiographs
MRI
8/10/2016
12
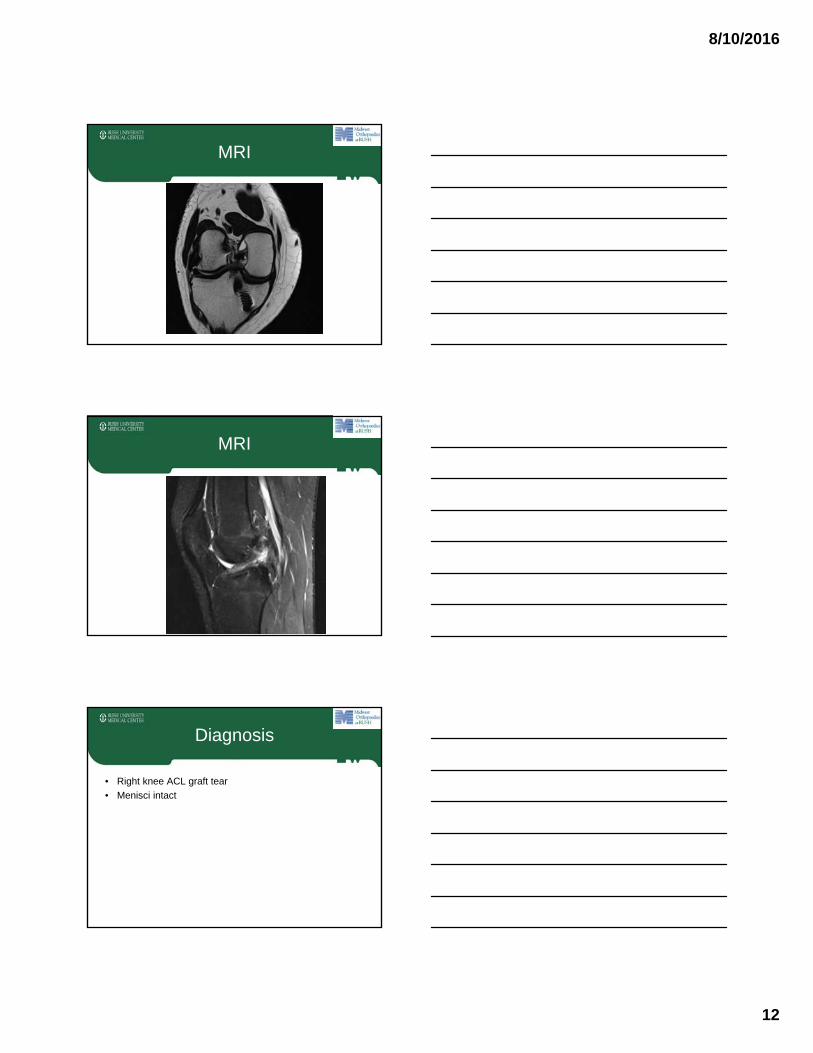
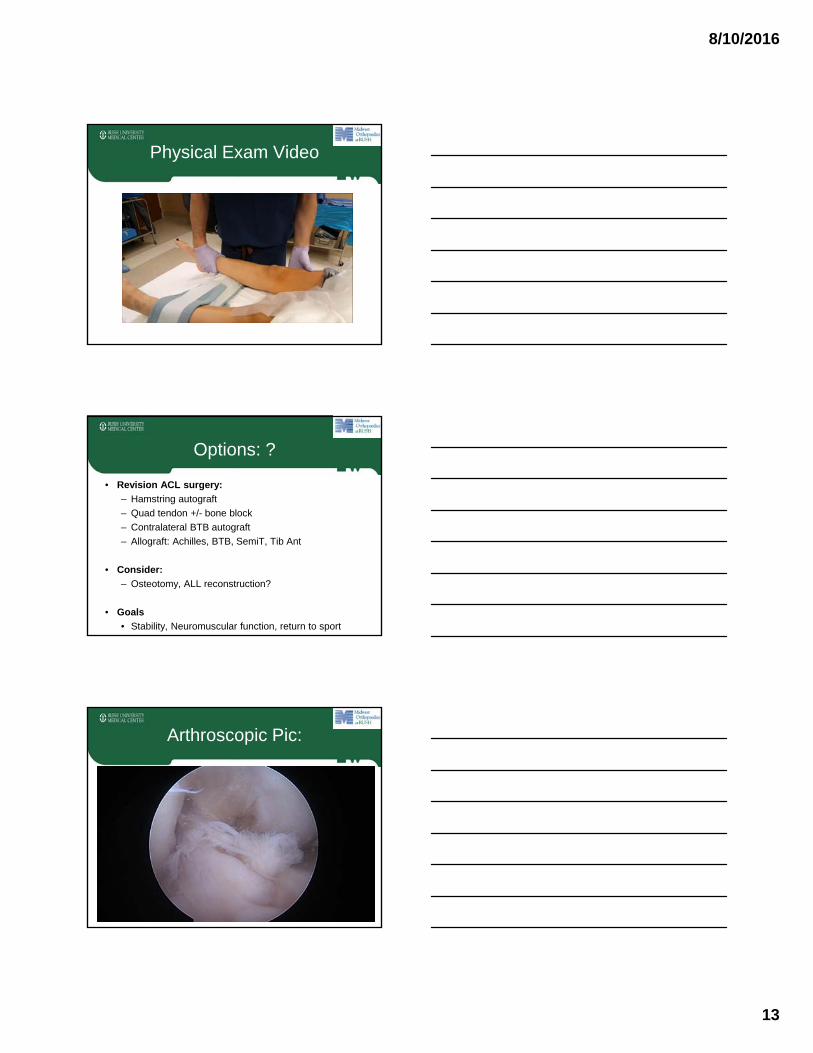
MRI
MRI
Diagnosis
• Right knee ACL graft tear
• Menisci intact
8/10/2016
13
Physical Exam Video
Options: ?
• Revision ACL surgery:
– Hamstring autograft
– Quad tendon +/- bone block
– Contralateral BTB autograft
– Allograft: Achilles, BTB, SemiT, Tib Ant
• Consider:
– Osteotomy, ALL reconstruction?
• Goals
• Stability, Neuromuscular function, return to sport
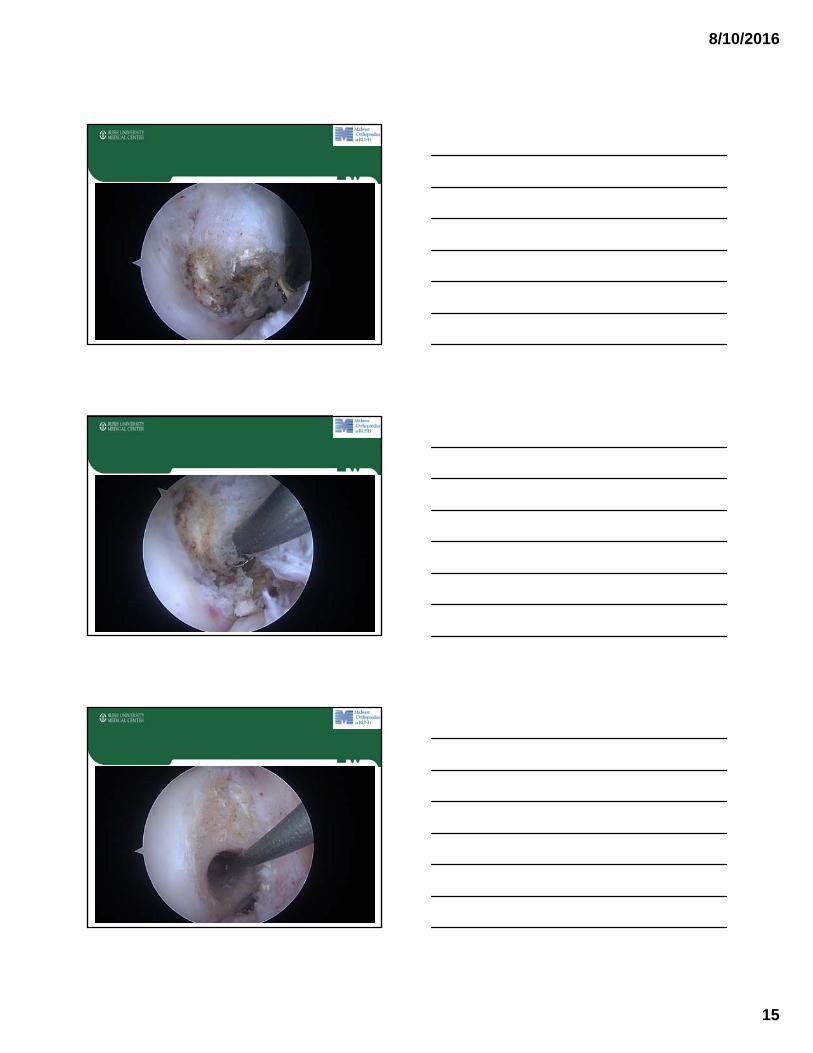
Arthroscopic Pic:

8/10/2016
14
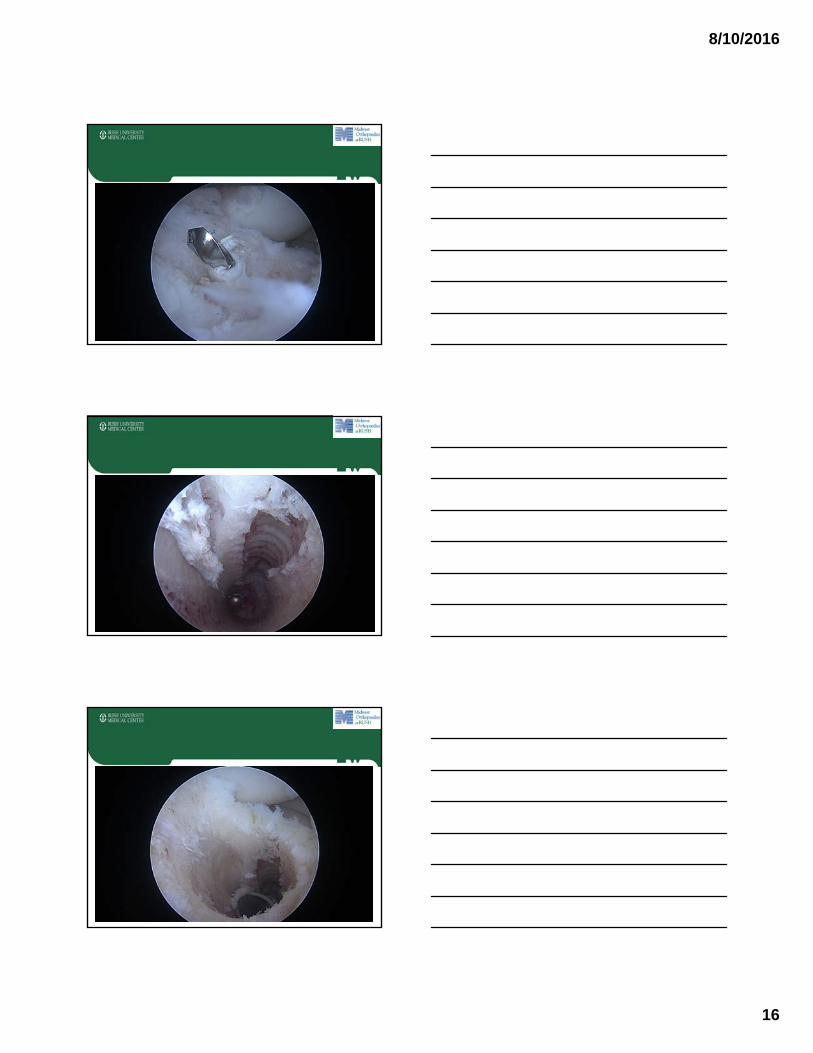
Procedure:
• Revision ACL reconstruction BTB Allograft
• Extra-articular ligament reconstruction:
– IT Band rerouting and tenodesis
• Removal femoral and tibial metal interference screws.
Arthroscopy Pic:
8/10/2016
15
8/10/2016
16

8/10/2016
17
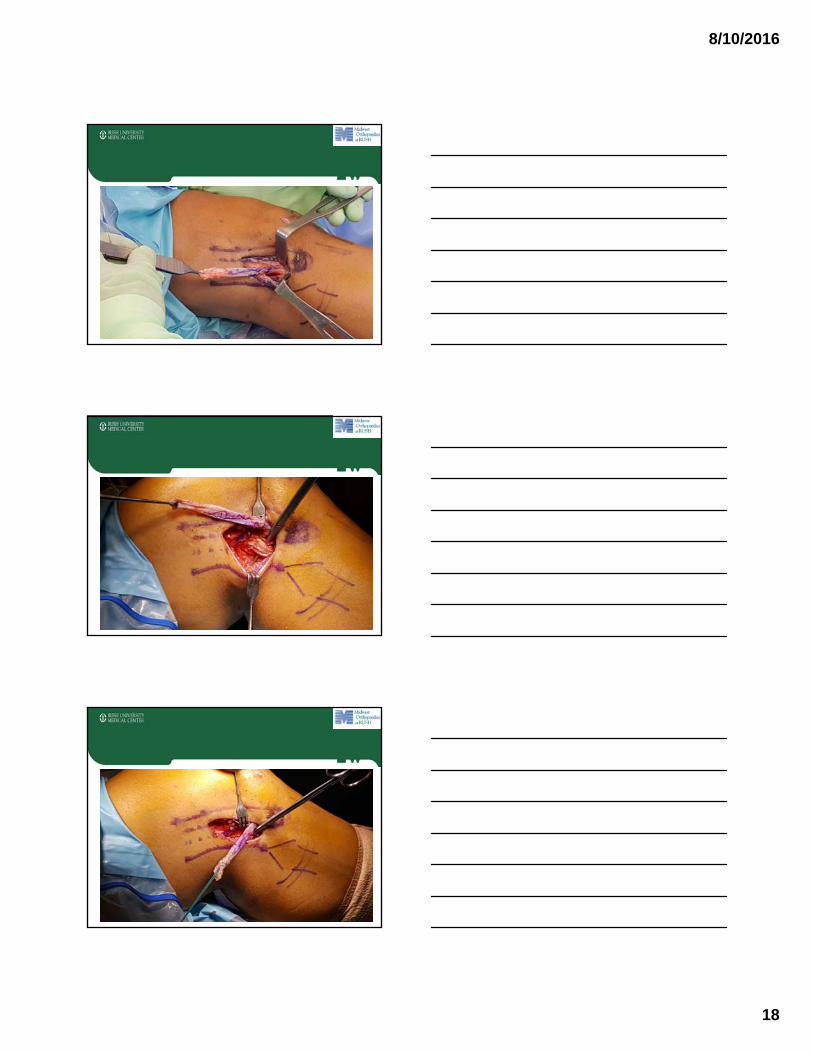
Revision ACL R, BTB Allograft
IT Band Rerouting/Tenodesis:
8/10/2016
18

8/10/2016
19
IT Band Rerouting/Tenodesis:
8/10/2016
20
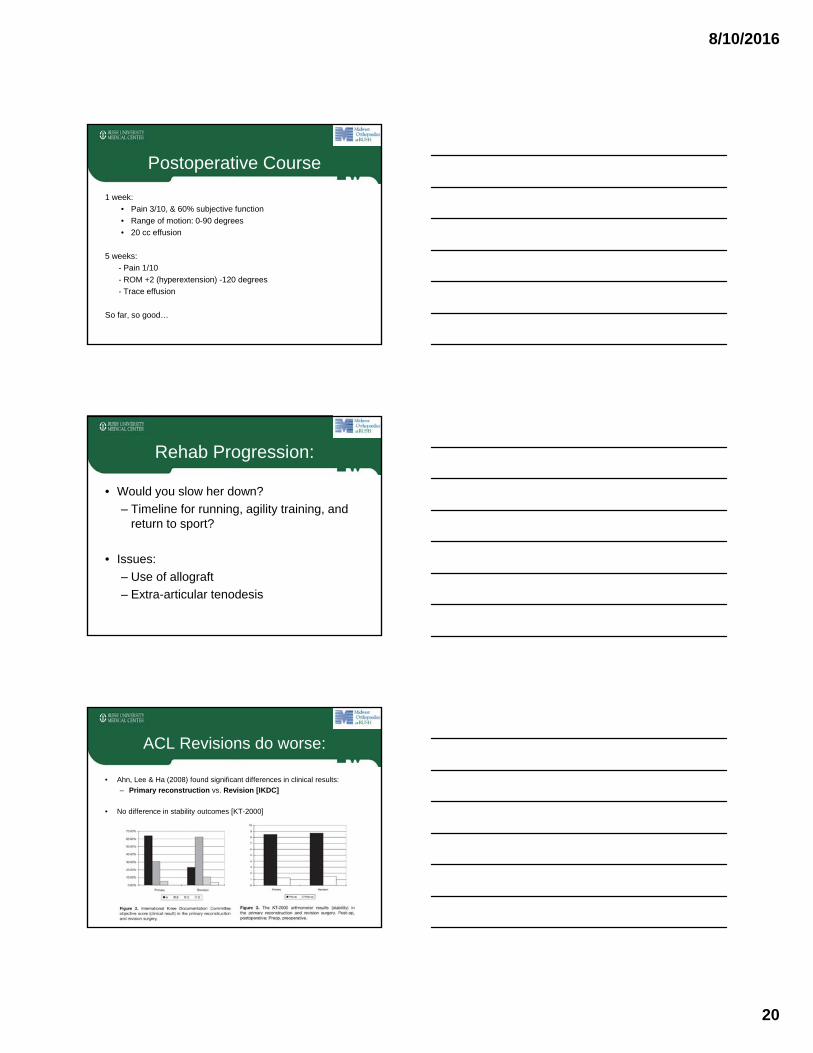
Postoperative Course
1 week:
• Pain 3/10, & 60% subjective function
• Range of motion: 0-90 degrees
• 20 cc effusion
5 weeks:
- Pain 1/10
- ROM +2 (hyperextension) -120 degrees
- Trace effusion
So far, so good…
Rehab Progression:
• Would you slow her down?
– Timeline for running, agility training, and return to sport?
• Issues:
– Use of allograft
– Extra-articular tenodesis
ACL Revisions do worse:
• Ahn, Lee & Ha (2008) found significant differences in clinical results:
– Primary reconstruction vs. Revision [IKDC]
• No difference in stability outcomes [KT-2000]

8/10/2016
21
Influence of a Lateral Tenodesis
• Tojani et al (2011) found lateral tenodesis w revision ACLR increased knee stability
• 80% negative pivot shift vs. 63% without tenodesis
Knee Surg Sports Traumatol Arthrosc. 2012 Aug;20(8):1565-70. Revision ACL reconstruction: influence of a lateral tenodesis.
Trojani C1, Beaufils P, Burdin G, Bussière C, Chassaing V, Djian P, Dubrana F, Ehkirch FP, Franceschi JP, Hulet C, Jouve F, Potel JF, Sbihi A, Neyret P,Colombet P.
Effect of Lateral Tenodesis on Internal Rotation
• Monaco et al (2007) found that single bundle ACL reconstruction with lateral tenodesis significantly reduced internal rotation
Knee Surg Sports Traumatol Arthrosc. 2007 Oct;15(10):1168-74. Double bundle or single bundle plus extraarticular tenodesis in ACL reconstruction?
A CAOS study.Monaco E1, Labianca L, Conteduca F, De Carli A, Ferretti A.
Summary:
• Revision ACL surgeries often suffer from functional stability issues
• IT band tenodesis can add rotational stability and potentially improve clinical outcomes

8/10/2016
22
Moderator: Brian Forsythe, MD
A 34 Year-Old Male with Right Knee Hyperextension Injury
Case PresentationCase Presentation
• 34 year-old healthy male• Hyperextension injury to right
knee while playing slow pitch softball
• Felt a pop
• Immediate pain and swelling
• Unable to walk after injury
• No prior knee pain or injury
• Described it as a “Mariano Rivera” injury mechanism
Physical ExaminationPhysical Examination
• Palpable defect in patellar tendon
• Range of motion 0-70
• Unable to perform straight leg raise
• 2-3+ soft tissue swelling
• Ligamentous exam limited secondary to pain and swelling
• Neurovascularly intact with palpable pulses
8/10/2016
23
RadiographsRadiographs
MRI – Coronal VideoMRI – Coronal Video
MRI – Sagittal VideoMRI – Sagittal Video

8/10/2016
24
DiagnosesDiagnoses
• Patellar tendon rupture
• ACL tear
• Grade 2 posterolateral corner injury
• Lateral meniscus tear (bucket handle displaced into notch)
• Medial meniscus tear (complex posterior horn)
Treatment PlanningTreatment Planning
• Goals:• Stable knee
• Intact extensor mechanism
• Full range of motion
• Minimize complications
• Considerations:• Timing of surgery?
• Single versus staged procedure?
Exam Under Anesthesia VideoExam Under Anesthesia Video

8/10/2016
25
Arthroscopy VideoArthroscopy Video
Thoughts?
• Meniscus: repair or debride?
• Should we fix: – ACL?
– Patellar Tendon?
– Posterolateral Corner?
Patellar Tendon RupturePatellar Tendon Rupture

8/10/2016
26
Patellar Tendon RepairPatellar Tendon Repair
Patellar Tendon RepairPatellar Tendon Repair
Patellar Tendon RepairPatellar Tendon Repair
8/10/2016
27
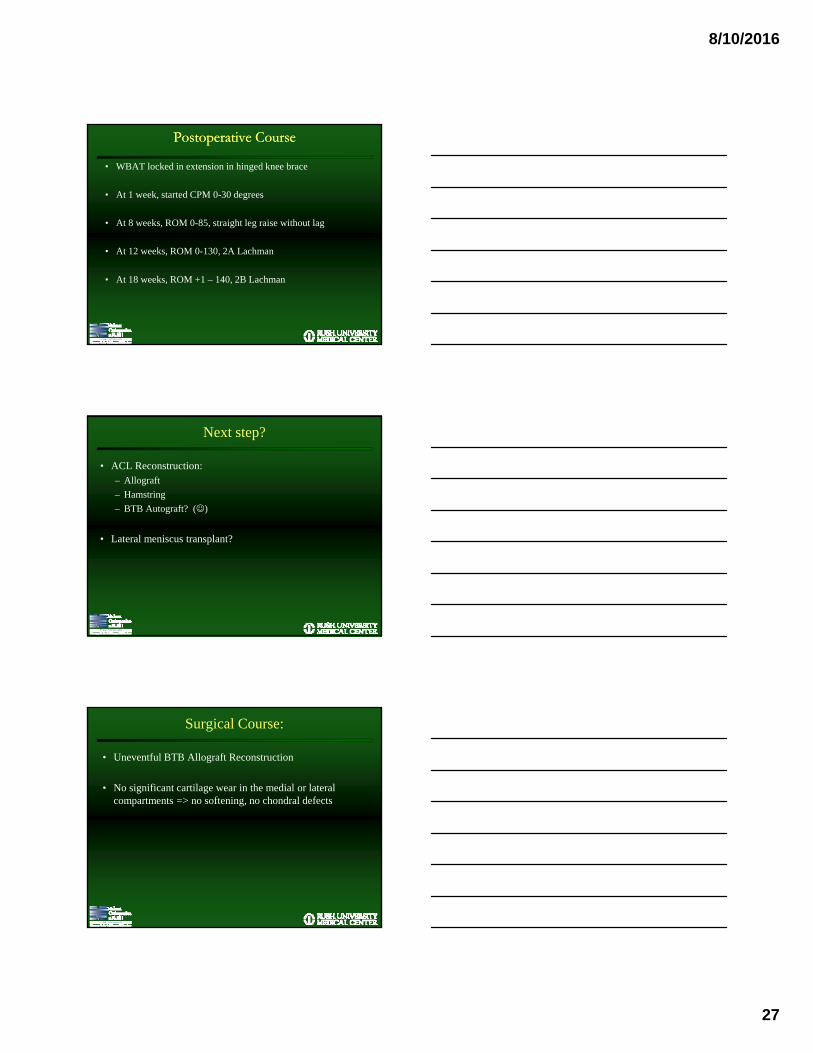
Postoperative CoursePostoperative Course
• WBAT locked in extension in hinged knee brace
• At 1 week, started CPM 0-30 degrees
• At 8 weeks, ROM 0-85, straight leg raise without lag
• At 12 weeks, ROM 0-130, 2A Lachman
• At 18 weeks, ROM +1 – 140, 2B Lachman
Next step?
• ACL Reconstruction: – Allograft
– Hamstring
– BTB Autograft? ()
• Lateral meniscus transplant?
Surgical Course:
• Uneventful BTB Allograft Reconstruction
• No significant cartilage wear in the medial or lateral compartments => no softening, no chondral defects

8/10/2016
28
Post-op Radiographs
ACL reconstruction with BTB allograft
• At 2 weeks, trace effusion, ROM 0-115– Weight bearing, brace locked in extension. Kept
locked for 2-3 more weeks
• At 14 weeks, ROM +1-135, Lachman 1A, stable valgus, varus
• At 6 months, +1-135, Lachman 1A, quad weakness, steroid injection => Return to sports 7-8 months
Combined Patellar Tendon and ACL Injury
Combined Patellar Tendon and ACL Injury
• Rare injury
• Lack of evidence to guide treatment (case reports)
• Patellar tendon rupture has 30% rate of associated knee injuries (McKinney et al KSSTA 2008)
8/10/2016
29
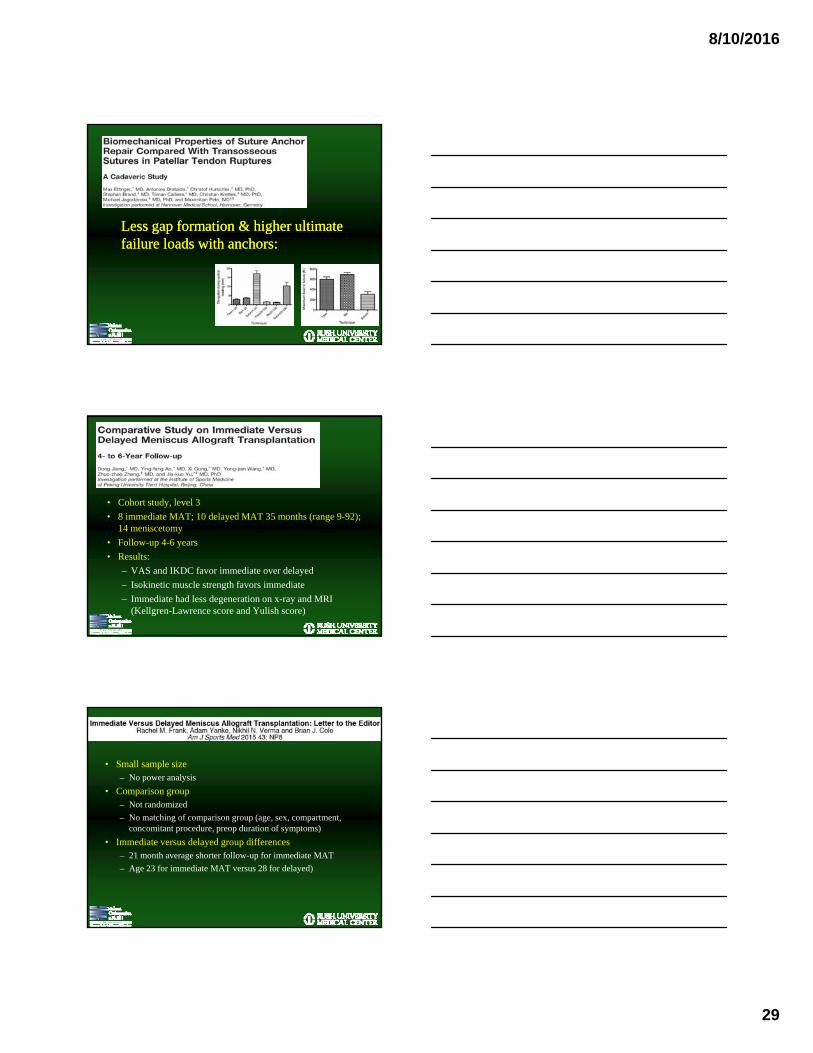
Less gap formation & higher ultimate failure loads with anchors:Less gap formation & higher ultimate failure loads with anchors:
• Cohort study, level 3
• 8 immediate MAT; 10 delayed MAT 35 months (range 9-92); 14 meniscetomy
• Follow-up 4-6 years
• Results:
– VAS and IKDC favor immediate over delayed
– Isokinetic muscle strength favors immediate
– Immediate had less degeneration on x-ray and MRI (Kellgren-Lawrence score and Yulish score)
• Small sample size– No power analysis
• Comparison group– Not randomized
– No matching of comparison group (age, sex, compartment, concomitant procedure, preop duration of symptoms)
• Immediate versus delayed group differences– 21 month average shorter follow-up for immediate MAT
– Age 23 for immediate MAT versus 28 for delayed)

8/10/2016
30
THANK YOU!
Brian Forsythe, MDAssistant Professor
Division of Sports MedicineTeam Physician Chicago White Sox, Chicago Bulls, & Chicago Fire
Midwest Orthopaedics at RushRush University Medical Center
Anterior Cruciate Ligament Reconstruction: A Review of Rehabilitation Outcome Measurements and Factors
Governing Return to Play
IntroductionIntroduction
• High yield of anterior cruciate ligament (ACL) tears• 125,000 reconstructions performed annually (Kim et al, 2011)
• Regain of function usually 6-9 months after
• Variability in Return to Play (RTP) protocols• Inconsistency in RTP guidelines between different practices
• Lack of uniformity in evaluation of readiness for RTP
• Optimization of RTP allows strategic, efficient, and appropriate decision making

8/10/2016
31
• Limited ”validated reliable consensus guidelines with objective criteria to facilitate the return to play process”
The ProblemThe Problem
AAOS 2015AAOS 2015
• What specific criteria and tests are we currently using?
• What tests should we be using?
• Can we come to consensus regarding RTP guidelines?
Substantial questions remain…Substantial questions remain…
8/10/2016
32
PurposePurpose
• To assess orthopedic surgeon and other providers’ (PT, research, ATC) views on RTP protocols following ACL reconstruction
• To compare what different practices view as optimal criteria for engaging in RTP
MethodsMethods
• Electronic survey distributed to 89 potential participants• Asked to evaluate importance of variables to initiate RTP (time of
surgery, pain, effusion…)
• Asked to rank outcome surveys in RTP decision making
• Asked for RTP management preferences and opinions
• Data analyzed to compare responses between surgeons and other respondents
• Reached out to different practices for RTP protocols
Created by Taskforce Founders
• Vetted by small panel of experts– Mayo Clinic
• Tim Hewett– University of Pittsburgh
• Jim Irrgang– Santa Monica Sport Medicine Foundation
• Holly Silver– Rush University
• Brian Cole and team– University of Missouri
• Patrick Smith
8/10/2016
33
• Initiated in 2015
– Seth L. Sherman, MD (University of Missouri)
– Jo Hannafin , MD PhD (HSS)
– Tim Hosea, MD (Rutgers)
• Deceased
– Brian Forsythe, MD (Rush University)
8/10/2016 97
U.S. Multicenter ACL RTP TaskforceU.S. Multicenter ACL RTP Taskforce
Participants:
17 academic medical centers 40 surgeons 18 non-surgeons (i.e. PhD, ATC, PT, PA)
• Goals of Taskforce:– Phase 1: Understand variation in current RTP guidelines
• A) Review and analyze existing protocols from each center
• B) Create and implement survey on ACL RTP
• C) Compare/contrast findings with existing RTP literature
– Phase 2: Validate and test uniform RTP protocol following ACL reconstruction
U.S. Multicenter ACL RTP TaskforceU.S. Multicenter ACL RTP Taskforce
8/10/2016
34
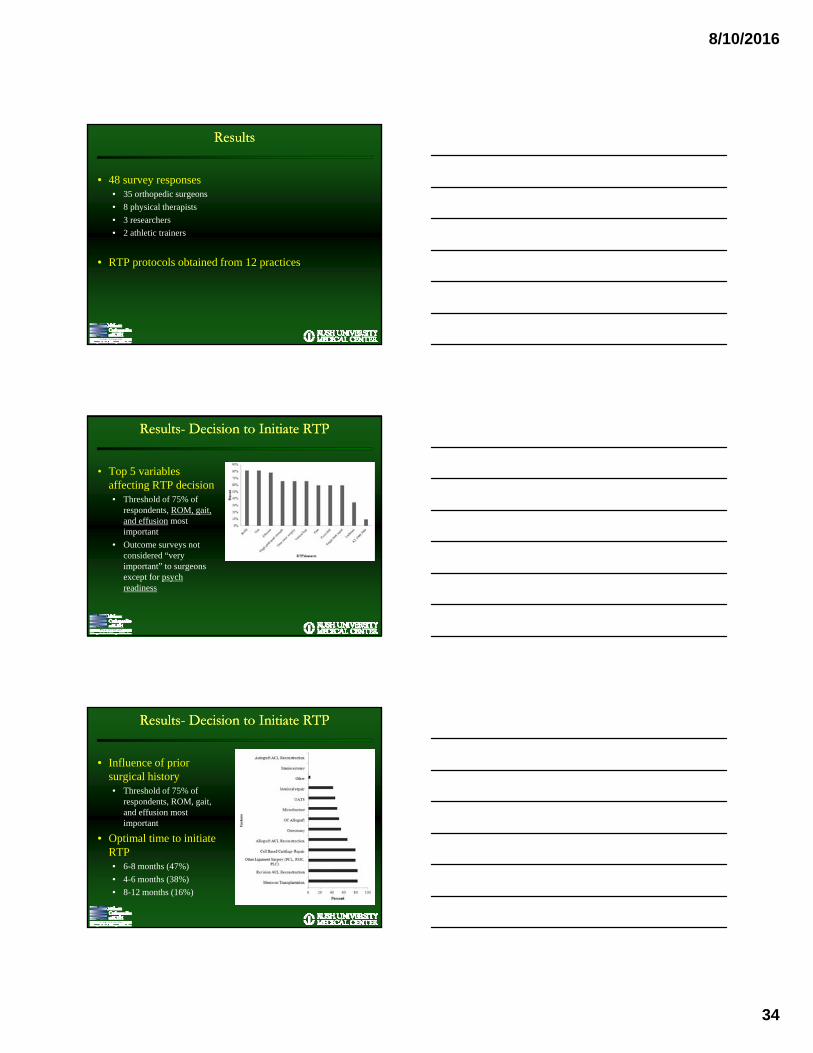
ResultsResults
• 48 survey responses• 35 orthopedic surgeons
• 8 physical therapists
• 3 researchers
• 2 athletic trainers
• RTP protocols obtained from 12 practices
Results- Decision to Initiate RTPResults- Decision to Initiate RTP
• Top 5 variables affecting RTP decision• Threshold of 75% of
respondents, ROM, gait, and effusion most important
• Outcome surveys not considered “very important” to surgeons except for psych readiness
Results- Decision to Initiate RTPResults- Decision to Initiate RTP
• Influence of prior surgical history• Threshold of 75% of
respondents, ROM, gait, and effusion most important
• Optimal time to initiate RTP• 6-8 months (47%)
• 4-6 months (38%)
• 8-12 months (16%)

8/10/2016
35
Results- Functional TestingResults- Functional Testing
• Surgeon vs. non-surgeon opinion of functional tests• Non-surgeons considered crossover hop test, drop vertical jump
test, and 6m timed hop test as “very important”
Results- Functional Testing and RTPResults- Functional Testing and RTP
• Assessment of performance ability, symmetry, pain and movement quality in functional tests
Results- RTP ProtocolsResults- RTP Protocols
• Functional tests deemed as “very important” in surveys inconsistently appear on RTP protocols• Of 12 protocols, separate RTP testing only in 58%

8/10/2016
36
DiscussionDiscussion
• ROM, gait, and presence of an effusion were very important factors for over 75% of respondents• RTP protocols do not fully reflect what providers view as
important
• No agreement on time interval to begin RTP testing
• Inconsistencies in the evaluation of individual functional tests and the RTP protocols remain
• There is need for objective guidelines that can be feasibly incorporated into any orthopedic practice
THANK YOU!