Embed Size (px)
Citation preview
790 ABSTRACTS
Results
Table 1
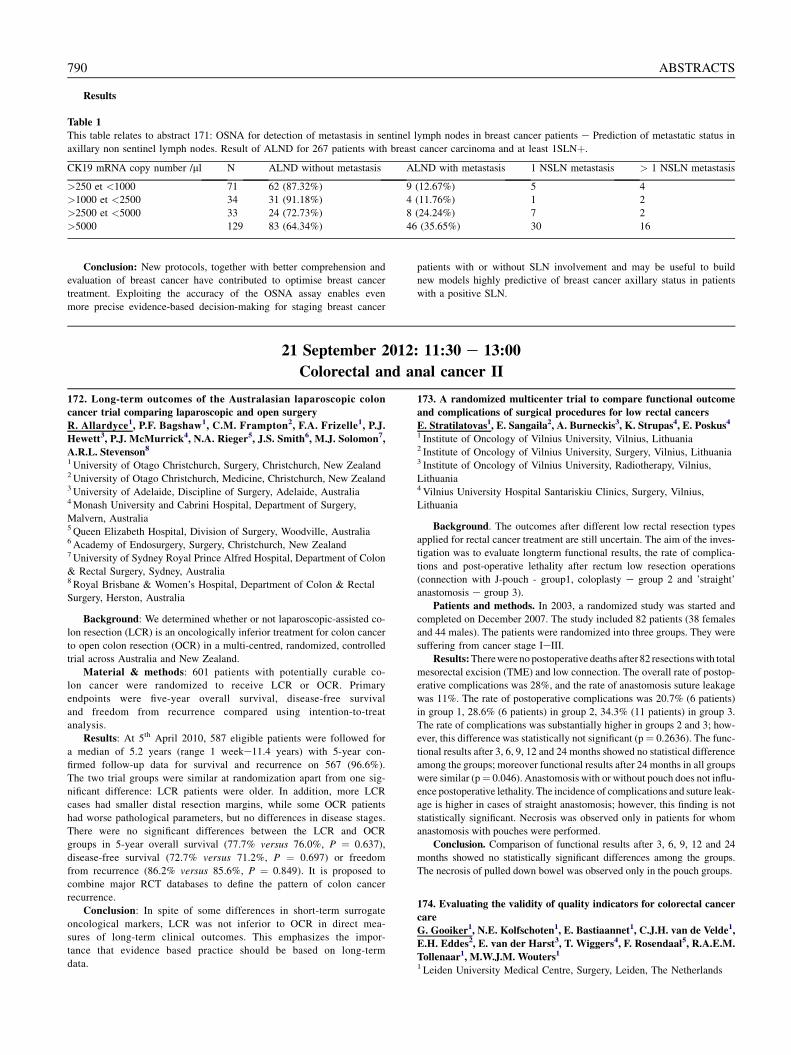
This table relates to abstract 171: OSNA for detection of metastasis in sentinel lymph nodes in breast cancer patients e Prediction of metastatic status in
axillary non sentinel lymph nodes. Result of ALND for 267 patients with breast cancer carcinoma and at least 1SLNþ.
CK19 mRNA copy number /ml N ALND without metastasis ALND with metastasis 1 NSLN metastasis > 1 NSLN metastasis
>250 et <1000 71 62 (87.32%) 9 (12.67%) 5 4
>1000 et <2500 34 31 (91.18%) 4 (11.76%) 1 2
>2500 et <5000 33 24 (72.73%) 8 (24.24%) 7 2
>5000 129 83 (64.34%) 46 (35.65%) 30 16
Conclusion: New protocols, together with better comprehension and
evaluation of breast cancer have contributed to optimise breast cancer
treatment. Exploiting the accuracy of the OSNA assay enables even
more precise evidence-based decision-making for staging breast cancer
patients with or without SLN involvement and may be useful to build
new models highly predictive of breast cancer axillary status in patients
with a positive SLN.
21 September 2012: 11:30 e 13:00
Colorectal and anal cancer II
172. Long-term outcomes of the Australasian laparoscopic colon
cancer trial comparing laparoscopic and open surgery
R. Allardyce1, P.F. Bagshaw1, C.M. Frampton2, F.A. Frizelle1, P.J.
Hewett3, P.J. McMurrick4, N.A. Rieger5, J.S. Smith6, M.J. Solomon7,
A.R.L. Stevenson8
1 University of Otago Christchurch, Surgery, Christchurch, New Zealand2University of Otago Christchurch, Medicine, Christchurch, New Zealand3University of Adelaide, Discipline of Surgery, Adelaide, Australia4Monash University and Cabrini Hospital, Department of Surgery,
Malvern, Australia5 Queen Elizabeth Hospital, Division of Surgery, Woodville, Australia6 Academy of Endosurgery, Surgery, Christchurch, New Zealand7University of Sydney Royal Prince Alfred Hospital, Department of Colon
& Rectal Surgery, Sydney, Australia8 Royal Brisbane & Women’s Hospital, Department of Colon & Rectal
Surgery, Herston, Australia
Background: We determined whether or not laparoscopic-assisted co-
lon resection (LCR) is an oncologically inferior treatment for colon cancer
to open colon resection (OCR) in a multi-centred, randomized, controlled
trial across Australia and New Zealand.
Material & methods: 601 patients with potentially curable co-
lon cancer were randomized to receive LCR or OCR. Primary
endpoints were five-year overall survival, disease-free survival
and freedom from recurrence compared using intention-to-treat
analysis.
Results: At 5th April 2010, 587 eligible patients were followed for
a median of 5.2 years (range 1 weeke11.4 years) with 5-year con-
firmed follow-up data for survival and recurrence on 567 (96.6%).
The two trial groups were similar at randomization apart from one sig-
nificant difference: LCR patients were older. In addition, more LCR
cases had smaller distal resection margins, while some OCR patients
had worse pathological parameters, but no differences in disease stages.
There were no significant differences between the LCR and OCR
groups in 5-year overall survival (77.7% versus 76.0%, P ¼ 0.637),
disease-free survival (72.7% versus 71.2%, P ¼ 0.697) or freedom
from recurrence (86.2% versus 85.6%, P ¼ 0.849). It is proposed to
combine major RCT databases to define the pattern of colon cancer
recurrence.
Conclusion: In spite of some differences in short-term surrogate
oncological markers, LCR was not inferior to OCR in direct mea-
sures of long-term clinical outcomes. This emphasizes the impor-
tance that evidence based practice should be based on long-term
data.
173. A randomized multicenter trial to compare functional outcome
and complications of surgical procedures for low rectal cancers
E. Stratilatovas1, E. Sangaila2, A. Burneckis3, K. Strupas4, E. Poskus4
1 Institute of Oncology of Vilnius University, Vilnius, Lithuania2 Institute of Oncology of Vilnius University, Surgery, Vilnius, Lithuania3 Institute of Oncology of Vilnius University, Radiotherapy, Vilnius,
Lithuania4 Vilnius University Hospital Santariskiu Clinics, Surgery, Vilnius,
Lithuania
Background. The outcomes after different low rectal resection types
applied for rectal cancer treatment are still uncertain. The aim of the inves-
tigation was to evaluate longterm functional results, the rate of complica-
tions and post-operative lethality after rectum low resection operations
(connection with J-pouch - group1, coloplasty e group 2 and ’straight’
anastomosis e group 3).
Patients and methods. In 2003, a randomized study was started and
completed on December 2007. The study included 82 patients (38 females
and 44 males). The patients were randomized into three groups. They were
suffering from cancer stage IeIII.
Results:Therewere no postoperative deaths after 82 resectionswith total
mesorectal excision (TME) and low connection. The overall rate of postop-
erative complications was 28%, and the rate of anastomosis suture leakage
was 11%. The rate of postoperative complications was 20.7% (6 patients)
in group 1, 28.6% (6 patients) in group 2, 34.3% (11 patients) in group 3.
The rate of complications was substantially higher in groups 2 and 3; how-
ever, this difference was statistically not significant (p¼ 0.2636). The func-
tional results after 3, 6, 9, 12 and 24 months showed no statistical difference
among the groups; moreover functional results after 24 months in all groups
were similar (p¼ 0.046). Anastomosis with or without pouch does not influ-
ence postoperative lethality. The incidence of complications and suture leak-
age is higher in cases of straight anastomosis; however, this finding is not
statistically significant. Necrosis was observed only in patients for whom
anastomosis with pouches were performed.
Conclusion. Comparison of functional results after 3, 6, 9, 12 and 24
months showed no statistically significant differences among the groups.
The necrosis of pulled down bowel was observed only in the pouch groups.
174. Evaluating the validity of quality indicators for colorectal cancer
care
G. Gooiker1, N.E. Kolfschoten1, E. Bastiaannet1, C.J.H. van de Velde1,
E.H. Eddes2, E. van der Harst3, T. Wiggers4, F. Rosendaal5, R.A.E.M.
Tollenaar1, M.W.J.M. Wouters1
1 Leiden University Medical Centre, Surgery, Leiden, The Netherlands






















![Retrospective Study Critical appraisal of laparoscopic vs ... · with colon and rectal cancer[1214]. This is suboptimal as the prognosis and recurrence pattern of colon and rectal](https://img.pdfslide.us/doc/110x75/5edc7da5ad6a402d66672bbb/retrospective-study-critical-appraisal-of-laparoscopic-vs-with-colon-and-rectal.jpg)




