Embed Size (px)
Citation preview

Page 1 of 35
Waterloo Wellington Integrated Wound Care ProgramEvidence-Based Wound Care
Pressure Injury Clinical Pathway0-7 Days Expected Outcomes Notes
Patient admitted to service/facility
Most Responsible Physician(MRP)/Nurse Practitioner (NP) identified/informed
Refer patient to ‘Care Connects’ if no responsible practioner currently involved with patient Determine if MRP/NP is part of family health team (FHT) or community health centre (CHC) and
consider additional supports availableMedical/surgical history and co-morbidity management considered within care plan
Any diagnosis that affects mobility, cognition, sensation and communication may be the cause of risk factors for Pressure Injurys
Sensory Perception Neuropathy Glycosylation (sugar attaches to cells)
of tissues Sensory impairment/altered level of
consciousness Decreased cognitive ability
Moisture Moisture on skin (e.g. bladder and bowel
incontinence, wound or fistula exudate, diaphoresis)
Edema Altered skin integrity/previous ulcerations
Activity (degree of physical activity) Immobility (bedrest, head of bed elevation
>300, chair sitting for prolonged times, hip fractures, supine or prone positioning)
Decreased level of activity Chronic or end of life pain Comorbidity that causes physical limitations
Mobility (ability to change and control body position) Obesity Prolonged anesthesia/operating room time Prematurity
Advanced age End of life Critically injured status Uncontrolled body movements Congenital abnormalities
Nutrition Nutritional deficits Alcohol/drug abuse
Friction, Pressure and Shear Unsafe transfers Medical devices (e.g. CPAP, bidirectional
positive airway pressure, oxygen tubing and masks, percutaneous endoscopic gastrostomy tubes, endotracheal tubes, nasogastric tubes, pelvic binders, pulse oximetry probes, tracheostomy faceplates and ties, sequential compression devices, external fixators and limb mobilizers)
Socioeconomic/Lifestyle Smoking Unsafe home environment Inadequate foot wear Inadequate hygiene Lack of awareness for self-care Financial insecurity Changes in routine
Current ongoing adjunctive therapies integrated into care plan
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016

Page 2 of 35
Medication reconciliation and their impact on wound healing reviewed
Prescription, non-prescription, naturopathic and illicit drug use (including e-cigarettes, inhaled substances and nicotine replacement therapy)
Medications that can affect healing include:chemotherapy, anticoagulants, antiplatelets, corticosteroids, vasoconstrictors, antihypertensives, diuretics and immunosuppressive drugs
Other medications used to treat acute episodic illnesses may affect healing (eg. antibiotics, colchicine, anti-rheumatoid arthritics)
Vitamin and mineral supplementationRecent blood work and other diagnostic test results reviewed and implictions for wound healing considered
Determine bloodwork and other diagnostic tests required (see chart in guidelines) Ensure Albumin done during this time period
Home glycemic control and monitoring if diabetic BS and A1C are within recommended range per responsible physician or NP Ensure Albumin/Urine creatinine ratio done during this time period Use of glucose log book (Diabetes Passport) Adequate insulin supplies Glucometer and required supplies Assess for barriers in monitoring glycemic control Community/health resources
Link to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Diabetic Education ProgramPatient self-referral link http://www.waterloowellingtondiabetes.ca/Public-Referrals.htmMedical professional referral link http://www.waterloowellingtondiabetes.ca/Professional-Site-Referral-Page.htm
Physical examination performed Identify pressure points, contractures and areas of reddness (note if blanchable or non-blanchable) Evidence of previous pressure injury Use of Braden Risk Scale
Link: http://www.healthcare.uiowa.edu/igec/tools/pressureulcers/bradenscale.pdfIf Pressure injury is below knee: assess potential to heal
Bilateral lower leg assessment (LLA)completed
Complete: ABPI/TPBI completed within last 3 mths and results documented If unable to obtain ABPI/TPBI, referral to medical imaging for vascular studies is recommended Repeat ABPI/TPBI assessment every 3 months if healing is not progressing Bilateral lower leg assessment that includes : Leg measurements (foot, ankle, calf, thigh) to assess edema Nail changes (thicker, dry, crumbly, presence of fungal infection) Assess interdigital spaces Presence of callous or corns Presence of varicosities (varicose veins) Ankle flare Drainage on socks History of compression
Wound and periwound assessment completed Complete: Bates-Jensen Wound Assessment Tool (BWAT) OR Pressure Ulcer Scale for Healing (PUSH)
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
ABPI 0.5 to 0.8 TPBI 0.64 to 0.7 Suggest Transcutaneous Oxygen Pressure(TcPo2), Laser Doppler Flowmetry, Doppler Arterial Waveforms or Segmental Doppler Pressure studies
ABPI <0.5 TPBI <0.64 Urgent vascular surgical consult needed
A pressure injury with adequate vascular supply, pressure distribution & receiving treatment per best practice should show signs of healing within two to four weeks. When pressure injuries are not progressing
Normal blood glucose ranges are needed for wound healing to occur

Page 3 of 35
Measure and document size of wound Stage pressure injury Assess potential to heal Assess need for debridement Assessment for infection (NERDS and STONEES) Obtain photos following best practice as per framework for individual organization policies and
procedures. Suggest following publication as guideline: http://mydigitalpublication.com/publication/?i=206722
Link to Waterloo Wellington Integrated Guidelines for Pressure Injuries: http://wwwoundcare.ca/88/Provide_Local_Wound_Care/
National Pressure Ulcer Advisory Panel (NPUAP)
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
A pressure injury with adequate vascular supply, pressure distribution & receiving treatment per best practice should show signs of healing within two to four weeks. When pressure injuries are not progressing

Page 4 of 35
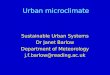
Staging System (Updated April 2016)
Stage 1Pressure Injury Intact skin with a localized area of non-blanchable erythema
May appear differently in darkly pigmented skin Presence of blanchable erythema or changes in sensation, temperature, or firmness may precede
visual changes Colour changes do not include purple or maroon discolouration; these may indicate deep tissue
pressure injury
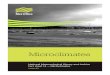
Stage 2Pressure Injury
Wound bed is viable, pink or red, moist May also present as an intact or ruptured serum-filled blister Adipose (fat) and deeper tissues are not visible• Granulation tissue, slough and eschar are not present• These injuries commonly result from adverse microclimate and shear in the skin over the pelvis and
shear in the heel.• This stage should not be used to describe moisture associated skin damage (MASD) including
incontinence associated dermatitis (IAD), intertriginous dermatitis (ITD), medical adhesive related skin injury (MARSI), or traumatic wounds (skin tears, burns, abrasions)
Stage 3Pressure Injury
Adipose (fat) is visible in the injury and granulation tissue and epibole (rolled wound edges) are often present Slough and/or eschar may be visible The depth of tissue damage varies by anatomical location; areas of significant adiposity can develop deep
wounds. Undermining and tunneling may occur Fascia, muscle, tendon, ligament, cartilage and/or bone are not exposed If slough or eschar obscures the extent of tissue loss this is an Unstageable Pressure Injury
Stage 4Pressure Injury
Full-thickness skin and tissue loss with exposed or directly palpable fascia, muscle, tendon, ligament, cartilage or bone in the injury
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
Non-blanchable erythema of intact skin

Page 5 of 35
Slough and/or eschar may be visible Epibole (rolled edges), undermining and/or tunneling often occur Depth varies by anatomical location If slough or eschar obscures the extent of tissue loss this is an Unstageable Pressure Injury
Unstageable Pressure Injury Extent of tissue damage within the injury cannot be confirmed as it is obscured by slough or eschar If slough or eschar is removed a Stage 3 or Stage 4 pressure injury will be revealed Stable eschar (i.e. dry, adherent, intact without erythema or fluctuant) on an ischemic limb or the heel(s) should
not be removed
Medical Device RelatedPressure Injury
This describes the etiology of the injury Result from the use of devices designed and applied for diagnostic or therapeutic purposes Resultant pressure injury generally conforms to the pattern or shape of the device Injury should be staged using the staging system
Mucosal MembranePressure Injury
Found on mucous membranes with a history of medical device in use at the location of the injury Due to the anatomy of the tissue these injuries cannot be staged
Moisture Associated Skin Damage (MASD) assessment completed
Assess continence of urine and stool If incontinence is a concern, a continence assessment should be completed by a qualified practioner (e.g.
an Enterstomal Therapist (ET) or Nurse Continence Advisor (NCA)
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
MASD can be defined as “inflammation and erosion of the skin caused by prolonged exposure to various sources of moisture, including urine or stool, perspiration, wound exudate, mucus, or saliva.

Page 6 of 35
Skin assessment including skin folds Link to RNAO Prompted Voiding Best Practice Guidelines
http://rnao.ca/sites/rnao-ca/files/Promoting_Continence_Using_Prompted_Voiding.pdf
Pain management considered and initiated Complete: Brief Pain Inventory Short Form (BPI-SF) Identify type of pain
1. Neuropathic Pain (described as burning, stinging, shooting, stabbing or hyperesthesia – sensitivity to touch). Suggested pharmaceutical treatment: Second generation tricyclic agents – e.g. Nortriptyline or Desipramine. If pain is not relieved try using Gabapentin or Pregabalin.
2. Nociceptive pain (described as sharp, aching or throbbing). Suggested pharmaceutical treatment: Non-Opioids – e.g. ASA or Acetaminophen Mild Opioids – e.g. CodeineStrong Opioids – e.g. Morphine or Oxycodone
Obtain physician/nurse practitioner orders for pharmaceutical treatments (opioids and non-opioids) Non-pharmacological pain control options (support surfaces, repositioning) Coordinate analgesic administration with wound care treatment times
Patient’s nutritional status optimized Calculate Body Mass Index (BMI) Determine recent weight loss/gain Complete Mini Nutritional Assessment (MNA)
http://www.mna-elderly.org/forms/mini/mna_mini_english.pdf If screening section results < 11 = complete assessment section If assessment section results< 24 = Registered Dietician referral required Recent dietary consult Identify barriers or risk factors to healthy eating Link to EatRight Ontario to talk to dietician
www.eatrightontario.ca 1-877-510-5102Wound etiology and appropriate pathway established Identify initial cause of wound. Pressure injuries are localized injury to the skin and/or underlying
tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear
Patient and caregiver concerns and goals integrated into the care plan and shared with care team
Complete: Cardiff Wound Impact Questionnaire
ORWorld Health Organization Quality of Life (WHOQOL) form
Ensure all patient/caregiver goals and concerns been addressedWound treatment plan determined in accordance to treatment goal (healable, maintenance or non-healable)
Arrange for physician/nurse practitioner orders as required to begin plan of care including agreeance to professional referral recommendations
Identify cause of pressure Provide pressure redistribution (support surfaces) for sleep, seating and use of medical devices Debridement/reduction by qualified professional Re-visit to pressure redistribution professional is recommended Ensure appropriate skin care Identify any potential barriers to wound treatment plan
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
Pain Red FlagsPossible Infection
Increase in pain level (new pain in patients with altered sensation )
Possible Arterial Involvement Pain on walking (caused by intermittent claudication) Pain with elevation of lower limbs Rest pain Nocturnal pain
Pain can be a trigger for autonomic dysreflexia that may occur in patients with spinal cord injury T6 or above
Nutrition is an essential component of wound healing. Consider dietician referral for supplementation recommmendations.
When trying a new product, allow 2 weeks to assess effectiveness unless adverse effect noted.
Initatition of compression therapy requires a lower leg assessment to be completed, ABPIs/TPBIs to be determined

Page 7 of 35
Identify appropriate footwear, offloading and repositioning options Consider required referals and further follow-up with previous professional referrals Consider compression if venous insufficiency/edema present and if APBI/TPBI is within safe range
Link to Waterloo Wellington Venous Leg Guidelines – Compression: http://wwwoundcare.ca/102/ Utilize toolkit to determine wound cleansing, debridement and dressing selection (South West
Region Wound Care Program: Wound Cleansing Table and Dressing Selection and Cleansing enablers and CAWC Product Picker chart)
Pressure Redistribution Ensure appropriate referrals for pressure redistribution have been arranged to qualified professionals
Review correct use of appropriate pressure redistribution devices Assess need for support surface (chair/bed)
Link to chart in guidelines: http://wwwoundcare.ca/81/Pressure_Reduction_and_Relief/ Review adherence to using appropriate pressure redistribution device(s) Assess barriers to appropriate pressure redistribution Initial and ongoing callous reduction is part of pressure redistribution Assess for secondary complications of offloading and refer concerns to treating practitioner
Look for redmarks, blisters, skin abrasions Ask about knee, hip or back issues (including contralateral limb) due to height difference of
offloading device Check for unsafe gait (are they stable, using appropriate aids, etc) Teach patient to assess for secondary complications
Check gait aids such as walker, cane, crutches Review goals of pressure redistribution (i.e. transition from cast to shoes, foot orthoses, etc.) Check for availability for financial compensation (e.g. private insurance, veterans medical benefits,
Assistive Devices Program (ADP), Ontario Disability Support Program –ODSP, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Patient counselled on the benefit of activity and rest for wound healing and comfort measures
Recent changes in overall activity level Daily routine including continence
concerns and/or access to bathroom Personal assistance available to perform
activities of daily living Determine where patient sleeps at night
and sits during day Safety of transfers Pressure distribution device
Consider Occupational Therapist referral for pressure redistribution device
Assess barriers to sleeping in bed Assess mobility and dexterity aids currently
being used (bedrail, superpole, trapezebar, therapeutic surfaces, raised toilet set and sitting devices)
Recommendations for exercise
Patient/caregiver educational plan initiated Rest/Activity Turning and sitting schedule for
repositioning Pillow between knees
Safety
Dietary Dietary requirements as per dietician Blood
glucose testing and recording in diary Link to EatRight Ontario to talk to dietician
www.eatrightontario.ca 1-877-510-5102
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
Initatition of compression therapy requires a lower leg assessment to be completed, ABPIs/TPBIs to be determined
‘Teach-back’ method is a way of ascertaining patients understanding about what they need to know or do regarding their health. Patients are asked to state in their own words what they understand to be important. It is a way to confirm that things have been explained in a manner that the patient understands.

Page 8 of 35
Prevention of injury – friction, shearing When to call primary caregiver (eg. signs
and symptoms of infection, deep vein thrombosis, cellulitis, impaired blood flow, difficulties with compression)
Pressure Relief/redistribution surface Offloading is required ‘for life’ Understands need of debridement Encourage appropriate footwear to be
worn at all times when weight bearing as discussed with foot care specialist
Examination of footwear, orthotics and offloading devices for foreign objects, wear pattern, pressure points and presence of wound drainage
Lifestyle Smoking and e-cigarette cessation with
goal to be nicotene-freeGuidelines can be found at:http://rnao.ca/sites/rnao-ca/files/Integrating_Smoking_Cessation_into_Daily_Nursing_Practice.pdf
Pain managementWound
Self care of wound
Diagnostic Tests Results understood by patient Diagnostic testing (nutritional blood work and
cholesterol levels) If diabetic, target ranges for A1C and blood
sugar Skin Care Wound self care Holistic self care of skin Incontinence and prevention/treatment of
Moisture Associated Skin Damage (MASD)Community Supports
Seating clinic for wheelchair Community support groups (eg. Diabetic
education and self- management sessions, walking groups, Southern Ontario Aboriginal Diabetes Initiative - SOADI)
Link to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Other ____________________________
Ability to self-manage optimized Review for independence or need for ongoing assistance with the following: Barriers to participate (poor eyesight,
physical limitations, transportation, socioeconomic, social environment, cognitive ability, other co-morbidities)
Decreased sensory perception affects ability to respond to pressure-related issues
Review importance and potential barriers to smoking cessation at every visit
Pressure relief/redistribution Adequate hygiene skin exposed to
moisture, perspiration Daily foot inspection with mirror(including
bottom of foot and between toes) Ongoing footcare arranged Home Environment – ADL’s
Compression application and removal if prescribed
Link to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Social/medical/family/employment obligationsSuggested website for reviewhttp://www.wwselfmanagement.ca/
Other ____________________________
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016

Page 9 of 35
Wound care Nutrition
Coping strategies implemented into plan of care Promoting independence to avoid practitioner/caregiver dependency Patient’s concerns and fears (including practitioner dependence) Signs of anxiety or other mental health issues (eg. delusions, hallucinations, paranoid behaviour) Depression screen using Geriatric Depression Scale assessment form –GDS15 Suicide assessment if applicable ETOH and illicit/recreational drug use Check for availability for financial compensation (e.g. private insurance, ADP, veterans medical
benefits, Ontario Disability Support Program –ODSP, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Family and caregiver support identified and incorporated into plan of care
Family/caregiver actively able to participate in treatment plan Repositioning, nutrition, continence if needed Importance of caregiver respite/relief
Social supports/community resources currently utilized is integrated into plan of care
Family support Check for availability for financial compensation (e.g. private insurance, veterans medical benefits,
Ontario Disability Support Program –ODSP/Ontario Works, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Community/health resourcesLink to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Caregiver conflicts Long or short term placement Confirm that ongoing medication coverage is arranged
Link to Trillium Drug Benefitshttp://www.health.gov.on.ca/en/public/programs/drugs/programs/odb/opdp_trillium.aspx
Professional referrals are initiated Primary Care Physician Community Nursing Advanced Wound Specialist Nurse Practitioner Occupational Therapist Urologist Infectious Disease Specialist Vascular Surgeon Orthopedic Surgeon Dermatologist Plastic Surgeon Internist/Endocrinologist Nephrologist Cardiologist Opthalmologist/Optometrist Mental Health Specialist
Physiotherapist Physiatrist Registered Kinesiologist Chiropodist Diabetic Education Program
Patient self-referral link http://www.waterloowellingtondiabetes.ca/Public-Referrals.htmMedical professional referral link http://www.waterloowellingtondiabetes.ca/Professional-Site-Referral-Page.htm
Certified Pedorothist Certified Orthotist Certified Prosthetist Podiatrist Footcare Nurse
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016

Page 10 of 35
Psychologist/Psychiatrist Social worker Registered Dietitian Pharmacist Neurologist
Lymphatic Massage Therapist Compression Stocking Fitter Other___________________________
Physician/nurse practitioner orders received as required to change plan of care including agreeance to professional referral recommendationsAppropriate documents shared
Pressure mapping Diagnostic results Identify need to reassess ABPI/TPBI in 6 months Lower leg assessment results Recent vascular study results (eg. ABPI, TPBI,
Transcutaneous Oxygen Pressure(TcPo2), Laser Doppler Flowmetry, Doppler Arterial Waveforms or Segmental Doppler Pressure studies)
Relevant consultation notes Post and current treatment and education plan List of appropriate contact information for ongoing
needs
If wound closed or eschar is stable (in arterial disease) send discharge summary outlining outstanding issues and teaching completed to:
Referral source Most responsible physician (MRP)/nurse
practitioner
Acute care Complex Continuing Care/Rehab Long-term care Community care Primary care physician/Nurse Practioner Professionals referred to Other _____________________________
8-21 Days Expected Outcomes NotesMost Responsible Physician(MRP)/Nurse Practitioner (NP) identified/informed
Communication with primary care physician and/or Nurse Practioner to update on any significant changes in patient’s condition.
Refer patient to ‘Care Connects’ if no responsible practioner currently involved with patient Determine if MRP/NP is part of family health team (FHT) or community health centre (CHC) and
consider additional supports available
If Pressure injury is below knee: assess potential to heal Complete:
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
‘Closed’ vs ‘Healed’
Closed : Skin intact, underlying tissue or structures are not visible Healed : Wound has been closed for a 2 year time period allowing
for collagen re-modelling from type 3 to type 1
These terms are often mistakenly used interchangeably.
Understand and teach the difference!

Page 11 of 35
Bilateral lower leg assessment (LLA)completed ABPI/TPBI completed within last 3 mths and results documented If unable to obtain ABPI/TPBI, referral to medical imaging for vascular studies is recommended Repeat ABPI/TPBI assessment every 3 months if healing is not progressing Bilateral lower leg assessment that includes : Leg measurements (foot, ankle, calf, thigh) to assess edema Nail changes (thicker, dry, crumbly, presence of fungal infection) Assess interdigital spaces Presence of callous or corns Presence of varicosities (varicose veins) Ankle flare Drainage on socks History of compression
Wound and periwound assessment completed Complete: Bates-Jensen Wound Assessment Tool (BWAT) OR Pressure Ulcer Scale for Healing (PUSH) Measure and document size of wound Stage pressure injury Assess potential to heal Assess need for debridement Assessment for infection (NERDS and STONEES) Obtain photos following best practice as per framework for individual organization policies and
procedures. Suggest following publication as guideline: http://mydigitalpublication.com/publication/?i=206722
Link to Waterloo Wellington Integrated Guidelines for Pressure Injuries: http://wwwoundcare.ca/88/Provide_Local_Wound_Care/
Wound treatment plan determined in accordance to treatment goal (healable, maintenance or non-healable)
Arrange for physician/nurse practitioner orders as required including agreeance to professional referral recommendations
Identify cause of pressure Provide pressure redistribution (support surfaces) for sleep, seating and use of medical devices Debridement/reduction by qualified professional Re-visit to pressure redistribution professional is recommended Ensure appropriate skin care Identify any potential barriers to wound treatment plan Identify appropriate footwear, offloading and repositioning options Consider required referals and further follow-up with previous professional referrals Consider compression if venous insufficiency/edema present and if APBI/TPBI is within safe range
Link to Waterloo Wellington Venous Leg Guidelines – Compression: http://wwwoundcare.ca/102/ Utilize toolkit to determine wound cleansing, debridement and dressing selection (South West
Region Wound Care Program: Wound Cleansing Table and Dressing Selection and Cleansing enablers and CAWC Product Picker chart)
Moisture Associated Skin Damage (MASD) assessment completed
Assess continence of urine and stool If incontinence is a concern, a continence assessment should be completed by a qualified practioner (e.g.
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
Initatition of compression therapy requires a lower leg assessment to be completed, ABPIs/TPBIs to be determined and results evaluated in addition to physician/NP order
A pressure injury with adequate vascular supply, pressure distribution & receiving treatment per best practice should show signs of healing within two to four weeks. When pressure injuries are not progressing towards closure (20-30%) treatment plan may include the initiation of a two-week trial of topical antimicrobials. An assessment by a wound care specialist is also recommended.
When trying a new product, allow 2 weeks to assess effectiveness unless adverse effect noted.
ABPI 0.5 to 0.8 TPBI 0.64 to 0.7 Suggest Transcutaneous Oxygen Pressure(TcPo2), Laser Doppler Flowmetry, Doppler Arterial Waveforms or Segmental Doppler Pressure studies
ABPI <0.5 TPBI <0.64 Urgent vascular surgical consult needed

Page 12 of 35
an Enterstomal Therapist (ET) or Nurse Continence Advisor (NCA) Skin assessment including skin folds Link to RNAO Prompted Voiding Best Practice Guidelines
http://rnao.ca/sites/rnao-ca/files/Promoting_Continence_Using_Prompted_Voiding.pdf
Pain management considered and initiated Complete: Brief Pain Inventory Short Form (BPI-SF) Identify type of pain
1. Neuropathic Pain (described as burning, stinging, shooting, stabbing or hyperesthesia – sensitivity to touch). Suggested pharmaceutical treatment: Second generation tricyclic agents – e.g. Nortriptyline or Desipramine. If pain is not relieved try using Gabapentin or Pregabalin.
2. Nociceptive pain (described as sharp, aching or throbbing). Suggested pharmaceutical treatment: Non-Opioids – e.g. ASA or Acetaminophen Mild Opioids – e.g. CodeineStrong Opioids – e.g. Morphine or Oxycodone
Obtain physician/nurse practitioner orders for pharmaceutical treatments (opioids and non-opioids) Non-pharmacological pain control options (support surfaces, repositioning) Coordinate analgesic administration with wound care treatment times
Pressure Redistribution Ensure appropriate referrals for pressure redistribution have been arranged to qualified professionals
Review correct use of appropriate pressure redistribution devices Assess need for support surface (chair/bed)
Link to chart in guidelines: http://wwwoundcare.ca/81/Pressure_Reduction_and_Relief/ Review adherence to using appropriate pressure redistribution device(s) Assess barriers to appropriate pressure redistribution Initial and ongoing callous reduction is part of pressure redistribution Assess for secondary complications of offloading and refer concerns to treating practitioner
Look for redmarks, blisters, skin abrasions Ask about knee, hip or back issues (including contralateral limb) due to height difference of
offloading device Check for unsafe gait (are they stable, using appropriate aids, etc) Teach patient to assess for secondary complications
Check gait aids such as walker, cane, crutches Review goals of pressure redistribution (i.e. transition from cast to shoes, foot orthoses, etc.) Check for availability for financial compensation (e.g. private insurance, veterans medical benefits,
Assistive Devices Program (ADP), Ontario Disability Support Program –ODSP, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Medical/surgical history and co-morbidity management considered within care plan
Review for changes
Medication reconciliation and their impact on wound healing reviewed
Review for changes: Prescription, non-prescription, naturopathic and illicit drug use
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
MASD can be defined as “inflammation and erosion of the skin caused by prolonged exposure to various sources of moisture, including urine or stool, perspiration, wound exudate, mucus, or saliva.
Pain Red FlagsPossible Infection
Increase in pain level (new pain in patients with altered sensation )
Possible Arterial Involvement Pain on walking (caused by intermittent claudication) Pain with elevation of lower limbs Rest pain Nocturnal pain
Pain can be a trigger for autonomic dysreflexia that may occur in patients with spinal cord injury T6 or above

Page 13 of 35
Recent blood work and other diagnostic test results reviewed and implictions for wound healing considered
Determine bloodwork and other diagnostic tests required (see chart in guidelines)
Home glycemic control and monitoring if diabetic BS and A1C are within recommended range per responsible physician or NP Use of glucose log book (Diabetes Passport) Adequate insulin supplies Glucometer and required supplies Assess for barriers in monitoring glycemic control Community/health resources
Link to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Diabetic Education ProgramPatient self-referral link http://www.waterloowellingtondiabetes.ca/Public-Referrals.htmMedical professional referral link http://www.waterloowellingtondiabetes.ca/Professional-Site-Referral-Page.htm
Patient’s nutritional status optimized Calculate Body Mass Index (BMI) Determine recent weight loss/gain Complete Mini Nutritional Assessment (MNA)
http://www.mna-elderly.org/forms/mini/mna_mini_english.pdf If screening section results < 11 = complete assessment section If assessment section results< 24 = Registered Dietician referral required Recent dietary consult Identify barriers or risk factors to healthy eating Link to EatRight Ontario to talk to dietician
www.eatrightontario.ca 1-877-510-5102Patient and caregiver concerns and goals integrated into the care plan and shared with care team
Review for changes: Cardiff Wound Impact Questionnaire
ORWorld Health Organization Quality of Life (WHOQOL) form
Ensure all patient/caregiver goals and concerns been addressedPatient counselled on the benefit of activity and rest for wound healing and comfort measures
Recent changes in overall activity level Daily routine including continence
concerns and/or access to bathroom Personal assistance available to perform
activities of daily living Determine where patient sleeps at night
and sits during day Safety of transfers Pressure distribution device
Consider Occupational Therapist referral for pressure redistribution device
Assess barriers to sleeping in bed Assess mobility and dexterity aids currently
being used (bedrail, superpole, trapezebar, therapeutic surfaces, raised toilet set and sitting devices)
Recommendations for exercise
Patient/caregiver educational plan Rest/Activity Turning and sitting schedule for
repositioning
Dietary Dietary requirements as per dietician Blood
glucose testing and recording in diary
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
Normal blood glucose ranges are needed for wound healing to occur
Nutrition is an essential component of wound healing. Consider dietician referral for supplementation recommmendations.
‘Teach-back’ method is a way of ascertaining patients understanding about what they need to know or do regarding their health. Patients are asked to state in their own words what they understand to be important. It is a way to confirm

Page 14 of 35
Pillow between kneesSafety
Prevention of injury – friction, shearing When to call primary caregiver (eg. signs
and symptoms of infection, deep vein thrombosis, cellulitis, impaired blood flow, difficulties with compression)
Pressure Relief/redistribution surface Offloading is required ‘for life’ Understands need of debridement Encourage appropriate footwear to be
worn at all times when weight bearing as discussed with foot care specialist
Examination of footwear, orthotics and offloading devices for foreign objects, wear pattern, pressure points and presence of wound drainage
Lifestyle Smoking and e-cigarette cessation with
goal to be nicotene-freeGuidelines can be found at:http://rnao.ca/sites/rnao-ca/files/Integrating_Smoking_Cessation_into_Daily_Nursing_Practice.pdf
Pain managementWound
Self care of wound
Link to EatRight Ontario to talk to dieticianwww.eatrightontario.ca 1-877-510-5102
Diagnostic Tests Results understood by patient Diagnostic testing (nutritional blood work and
cholesterol levels) If diabetic, target ranges for A1C and blood
sugar Skin Care Wound self care Holistic self care of skin Incontinence and prevention/treatment of
Moisture Associated Skin Damage (MASD)Community Supports
Seating clinic for wheelchair Community support groups (eg. Diabetic
education and self- management sessions, walking groups, Southern Ontario Aboriginal Diabetes Initiative - SOADI)
Link to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Other ____________________________
Ability to self-manage optimized Review for independence or need for ongoing assistance with the following: Barriers to participate (poor eyesight,
physical limitations, transportation, socioeconomic, social environment, cognitive ability, other co-morbidities)
Decreased sensory perception affects ability to respond to pressure-related issues
Review importance and potential barriers to smoking cessation at every visit
Pressure relief/redistribution Adequate hygiene skin exposed to
moisture, perspiration Daily foot inspection with mirror(including
bottom of foot and between toes)
Compression application and removal if prescribed
Link to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Social/medical/family/employment obligationsSuggested website for reviewhttp://www.wwselfmanagement.ca/
Other ____________________________
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
‘Teach-back’ method is a way of ascertaining patients understanding about what they need to know or do regarding their health. Patients are asked to state in their own words what they understand to be important. It is a way to confirm

Page 15 of 35
Ongoing footcare arranged Home Environment – ADL’s Wound care Nutrition
Coping strategies implemented into plan of care Promoting independence to avoid practitioner/caregiver dependency Patient’s concerns and fears (including practitioner dependence) Signs of anxiety or other mental health issues (eg. delusions, hallucinations, paranoid behaviour) Depression screen using Geriatric Depression Scale assessment form –GDS15 Suicide assessment if applicable ETOH and illicit/recreational drug use
Check for availability for financial compensation (e.g. private insurance, ADP, veterans medical benefits, Ontario Disability Support Program –ODSP, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Family and caregiver support identified and incorporated into plan of care
Family/caregiver actively able to participate in treatment plan Repositioning, nutrition, continence if needed Importance of caregiver respite/relief
Social supports/community resources currently utilized is integrated into plan of care
Family support Check for availability for financial compensation (e.g. private insurance, veterans medical benefits,
Ontario Disability Support Program –ODSP/Ontario Works, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Community/health resourcesLink to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Caregiver conflicts Long or short term placement Confirm that ongoing medication coverage is arranged
Link to Trillium Drug Benefitshttp://www.health.gov.on.ca/en/public/programs/drugs/programs/odb/opdp_trillium.aspx
Professional referrals are initiated Primary Care Physician Community Nursing Advanced Wound Specialist Nurse Practitioner Occupational Therapist Urologist Infectious Disease Specialist Vascular Surgeon Orthopedic Surgeon Dermatologist Plastic Surgeon Internist/Endocrinologist Nephrologist Cardiologist
Physiotherapist Physiatrist Registered Kinesiologist Chiropodist Diabetic Education Program
Patient self-referral link http://www.waterloowellingtondiabetes.ca/Public-Referrals.htmMedical professional referral link http://www.waterloowellingtondiabetes.ca/Professional-Site-Referral-Page.htm
Certified Pedorothist Certified Orthotist Certified Prosthetist
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016

Page 16 of 35
Opthalmologist/Optometrist Mental Health Specialist Psychologist/Psychiatrist Social worker Registered Dietitian Pharmacist Neurologist
Podiatrist Footcare Nurse Lymphatic Massage Therapist Compression Stocking Fitter Other___________________________
Physician/nurse practitioner orders received as required to change plan of care including agreeance to professional referral recommendationsAppropriate documents shared
Pressure mapping Diagnostic results Identify need to reassess ABPI/TPBI in 6 months Lower leg assessment results Recent vascular study results (eg. ABPI, TPBI,
Transcutaneous Oxygen Pressure(TcPo2), Laser Doppler Flowmetry, Doppler Arterial Waveforms or Segmental Doppler Pressure studies)
Relevant consultation notes Post and current treatment and education plan List of appropriate contact information for ongoing
needs
If wound closed or eschar is stable (in arterial disease) send discharge summary outlining outstanding issues and teaching completed to:
Referral source Most responsible physician (MRP)/nurse
practitioner
Acute care Complex Continuing Care/Rehab Long-term care Community care Primary care physician/Nurse Practioner Professionals referred to Other _____________________________
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
‘Closed’ vs ‘Healed’
Closed : Skin intact, underlying tissue or structures are not visible Healed : Wound has been closed for a 2 year time period allowing
for collagen re-modelling from type 3 to type 1
These terms are often mistakenly used interchangeably.
Understand and teach the difference!

Page 17 of 35
21-28 Days Expected Outcomes (Ongoing to day 76) NotesMost Responsible Physician(MRP)/Nurse Practitioner (NP) identified/informed
Communication with primary care physician and/or Nurse Practioner to update on any significant changes in patient’s condition.
Refer patient to ‘Care Connects’ if no responsible practioner currently involved with patient Determine if MRP/NP is part of family health team (FHT) or community health centre (CHC) and
consider additional supports available
If Pressure injury is below knee: assess potential to heal
Bilateral lower leg assessment (LLA)completed
Complete:1. ABPI/TPBI completed within last 3 mths and results documented2. If unable to obtain ABPI/TPBI, referral to medical imaging for vascular studies is recommended3. Repeat ABPI/TPBI assessment every 3 months if healing is not progressing4. Bilateral lower leg assessment that includes : Leg measurements (foot, ankle, calf, thigh) to assess edema Nail changes (thicker, dry, crumbly, presence of fungal infection) Assess interdigital spaces Presence of callous or corns
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
ABPI 0.5 to 0.8 TPBI 0.64 to 0.7 Suggest Transcutaneous Oxygen Pressure(TcPo2), Laser Doppler Flowmetry, Doppler Arterial Waveforms or Segmental Doppler Pressure studies

Page 18 of 35
Presence of varicosities (varicose veins) Ankle flare Drainage on socks History of compression
Wound and periwound assessment completed Complete: Bates-Jensen Wound Assessment Tool (BWAT) OR Pressure Ulcer Scale for Healing (PUSH) Measure and document size of wound Stage pressure injury Assess potential to heal Assess need for debridement Assessment for infection (NERDS and STONEES) Obtain photos following best practice as per framework for individual organization policies and
procedures. Suggest following publication as guideline: http://mydigitalpublication.com/publication/?i=206722
Link to Waterloo Wellington Integrated Guidelines for Pressure Injuries: http://wwwoundcare.ca/88/Provide_Local_Wound_Care/
Wound treatment plan determined in accordance to treatment goal (healable, maintenance or non-healable)
Arrange for physician/nurse practitioner orders as required including agreeance to professional referral recommendations
Identify cause of pressure Provide pressure redistribution (support surfaces) for sleep, seating and use of medical devices Debridement/reduction by qualified professional Re-visit to pressure redistribution professional is recommended Ensure appropriate skin care Identify any potential barriers to wound treatment plan Identify appropriate footwear, offloading and repositioning options Consider required referals and further follow-up with previous professional referrals Consider compression if venous insufficiency/edema present and if APBI/TPBI is within safe range
Link to Waterloo Wellington Venous Leg Guidelines – Compression: http://wwwoundcare.ca/102/ Utilize toolkit to determine wound cleansing, debridement and dressing selection (South West
Region Wound Care Program: Wound Cleansing Table and Dressing Selection and Cleansing enablers and CAWC Product Picker chart)
Moisture Associated Skin Damage (MASD) assessment completed
Assess continence of urine and stool If incontinence is a concern, a continence assessment should be completed by a qualified practioner (e.g.
an Enterstomal Therapist (ET) or Nurse Continence Advisor (NCA) Skin assessment including skin folds Link to RNAO Prompted Voiding Best Practice Guidelines
http://rnao.ca/sites/rnao-ca/files/Promoting_Continence_Using_Prompted_Voiding.pdf
Pain management considered and initiated Complete: Brief Pain Inventory Short Form (BPI-SF) Identify type of pain
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
Pain Red FlagsPossible Infection
Increase in pain level (new pain in patients with altered sensation )
Possible Arterial Involvement Pain on walking (caused by intermittent claudication)
MASD can be defined as “inflammation and erosion of the skin caused by prolonged exposure to various sources of moisture, including urine or stool, perspiration, wound exudate, mucus, or saliva.
Initatition of compression therapy requires a lower leg assessment to be completed, ABPIs/TPBIs to be determined and results evaluated in addition to physician/NP order
When trying a new product, allow 2 weeks to assess effectiveness unless adverse effect noted.
A pressure injury with adequate vascular supply, pressure distribution & receiving treatment per best practice should show signs of healing within two to four weeks. When pressure injuries are not progressing towards closure (20-30%) treatment plan should include the initiation of a two-week trial of topical antimicrobials. An assessment by a wound care specialist is also recommended.
ABPI <0.5 TPBI <0.64 Urgent vascular surgical consult needed

Page 19 of 35
1. Neuropathic Pain (described as burning, stinging, shooting, stabbing or hyperesthesia – sensitivity to touch). Suggested pharmaceutical treatment: Second generation tricyclic agents – e.g. Nortriptyline or Desipramine. If pain is not relieved try using Gabapentin or Pregabalin.
2. Nociceptive pain (described as sharp, aching or throbbing). Suggested pharmaceutical treatment: Non-Opioids – e.g. ASA or Acetaminophen Mild Opioids – e.g. CodeineStrong Opioids – e.g. Morphine or Oxycodone
Obtain physician/nurse practitioner orders for pharmaceutical treatments (opioids and non-opioids) Non-pharmacological pain control options (support surfaces, repositioning) Coordinate analgesic administration with wound care treatment times
Pressure Redistribution Ensure appropriate referrals for pressure redistribution have been arranged to qualified professionals
Review correct use of appropriate pressure redistribution devices Assess need for support surface (chair/bed)
Link to chart in guidelines: http://wwwoundcare.ca/81/Pressure_Reduction_and_Relief/ Review adherence to using appropriate pressure redistribution device(s) Assess barriers to appropriate pressure redistribution Initial and ongoing callous reduction is part of pressure redistribution Assess for secondary complications of offloading and refer concerns to treating practitioner
Look for redmarks, blisters, skin abrasions Ask about knee, hip or back issues (including contralateral limb) due to height difference of
offloading device Check for unsafe gait (are they stable, using appropriate aids, etc) Teach patient to assess for secondary complications
Check gait aids such as walker, cane, crutches Review goals of pressure redistribution (i.e. transition from cast to shoes, foot orthoses, etc.) Check for availability for financial compensation (e.g. private insurance, veterans medical benefits,
Assistive Devices Program (ADP), Ontario Disability Support Program –ODSP, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Medical/surgical history and co-morbidity management considered within care plan
Review for changes
Medication reconciliation and their impact on wound healing reviewed
Review for changes: Prescription, non-prescription, naturopathic and illicit drug use
Recent blood work and other diagnostic test results reviewed and implictions for wound healing considered
Determine bloodwork and other diagnostic tests required (see chart in guidelines)
Home Glycemic Control and Monitoring if diabetic BS and A1C are within recommended range per responsible physician or NP Use of glucose log book (Diabetes Passport) Adequate insulin supplies Glucometer and required supplies
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
Pain Red FlagsPossible Infection
Increase in pain level (new pain in patients with altered sensation )
Possible Arterial Involvement Pain on walking (caused by intermittent claudication)
Normal blood glucose ranges are needed for wound healing to occur

Page 20 of 35
Assess for barriers in monitoring glycemic controlPatient’s nutritional status optimized Calculate Body Mass Index (BMI)
Determine recent weight loss/gain Complete Mini Nutritional Assessment (MNA)
http://www.mna-elderly.org/forms/mini/mna_mini_english.pdf If screening section results < 11 = complete assessment section If assessment section results< 24 = Registered Dietician referral required Recent dietary consult Identify barriers or risk factors to healthy eating Link to EatRight Ontario to talk to dietician
www.eatrightontario.ca 1-877-510-5102Patient and caregiver concerns and goals integrated into the care plan and shared with care team
Review for changes: Cardiff Wound Impact Questionnaire
ORWorld Health Organization Quality of Life (WHOQOL) form
Ensure all patient/caregiver goals and concerns been addressedPatient counselled on the benefit of activity and rest for comfort measures and wound healing
Recent changes in overall activity level Daily routine including continence
concerns and/or access to bathroom Personal assistance available to perform
activities of daily living Determine where patient sleeps at night
and sits during day Safety of transfers
Pressure relief device &/or redistribution Assess barriers to sleeping in bed Assess mobility and dexterity aids currently
being used (bedrail, superpole, trapezebar, airbed)
Recommendations for exercise Consider Occupational Therapist referral for
pressure relief devicePatient/caregiver educational plan continued Rest/Activity
Turning and sitting schedule for repositioning
Pillow between kneesSafety
Prevention of injury – friction, shearing When to call primary caregiver (eg. signs
and symptoms of infection, deep vein thrombosis, cellulitis, impaired blood flow, difficulties with compression)
Pressure Relief/redistribution surface Offloading is required ‘for life’ Understands need of debridement Encourage appropriate footwear to be
worn at all times when weight bearing as discussed with foot care specialist
Examination of footwear, orthotics and offloading devices for foreign objects, wear pattern, pressure points and
Dietary Dietary requirements as per dietician Blood
glucose testing and recording in diary Link to EatRight Ontario to talk to dietician
www.eatrightontario.ca 1-877-510-5102Diagnostic Tests
Results understood by patient Diagnostic testing (nutritional blood work and
cholesterol levels) If diabetic, target ranges for A1C and blood
sugar Skin Care Wound self care Holistic self care of skin Incontinence and prevention/treatment of
Moisture Associated Skin Damage (MASD)Community Supports
Seating clinic for wheelchair Community support groups (eg. Diabetic
education and self- management sessions,
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
‘Teach-back’ method is a way of ascertaining patients understanding about what they need to know or do regarding their health. Patients are asked to state in their own words what they understand to be important. It is a way to confirm that things have been explained in a manner that the patient understands.
Nutrition is an essential component of wound healing. Consider dietician referral for supplementation recommmendations.

Page 21 of 35
presence of wound drainageLifestyle
Smoking and e-cigarette cessation with goal to be nicotene-freeGuidelines can be found at:http://rnao.ca/sites/rnao-ca/files/Integrating_Smoking_Cessation_into_Daily_Nursing_Practice.pdf
Pain managementWound
Self care of wound
walking groups, Southern Ontario Aboriginal Diabetes Initiative - SOADI)
Link to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Other ____________________________
Ability to self-manage optimized Review for independence or need for ongoing assistance with the following: Barriers to participate (poor eyesight,
physical limitations, transportation, socioeconomic, social environment, cognitive ability, other co-morbidities)
Decreased sensory perception affects ability to respond to pressure-related issues
Review importance and potential barriers to smoking cessation at every visit
Pressure relief/redistribution Adequate hygiene skin exposed to
moisture, perspiration Daily foot inspection with mirror(including
bottom of foot and between toes) Ongoing footcare arranged Home Environment – ADL’s Wound care Nutrition
Compression application and removal if prescribed
Link to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Social/medical/family/employment obligationsSuggested website for reviewhttp://www.wwselfmanagement.ca/
Other ____________________________
Coping strategies implemented into plan of care Promoting independence to avoid practitioner/caregiver dependency Patient’s concerns and fears (including practitioner dependence) Signs of anxiety or other mental health issues (eg. delusions, hallucinations, paranoid behaviour) Depression screen using Geriatric Depression Scale assessment form –GDS15 Suicide assessment if applicable ETOH and illicit/recreational drug use Check for availability for financial compensation (e.g. private insurance, ADP, veterans medical
benefits, Ontario Disability Support Program –ODSP, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Family and caregiver support identified and incorporated into plan of care
Family/caregiver actively able to participate in treatment plan Repositioning, nutrition, continence if needed Importance of caregiver respite/relief
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016

Page 22 of 35
Social supports/community resources currently utilized is integrated into plan of care
Family support Check for availability for financial compensation (e.g. private insurance, veterans medical benefits,
Ontario Disability Support Program –ODSP/Ontario Works, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Community/health resourcesLink to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Caregiver conflicts Long or short term placement Confirm that ongoing medication coverage is arranged
Link to Trillium Drug Benefitshttp://www.health.gov.on.ca/en/public/programs/drugs/programs/odb/opdp_trillium.aspx
Professional referrals are initiated Primary Care Physician Community Nursing Advanced Wound Specialist Nurse Practitioner Occupational Therapist Urologist Infectious Disease Specialist Vascular Surgeon Orthopedic Surgeon Dermatologist Plastic Surgeon Internist/Endocrinologist Nephrologist Cardiologist Opthalmologist/Optometrist Mental Health Specialist Psychologist/Psychiatrist Social worker Registered Dietitian Pharmacist Neurologist
Physiotherapist Physiatrist Registered Kinesiologist Chiropodist Diabetic Education Program
Patient self-referral link http://www.waterloowellingtondiabetes.ca/Public-Referrals.htmMedical professional referral link http://www.waterloowellingtondiabetes.ca/Professional-Site-Referral-Page.htm
Certified Pedorothist Certified Orthotist Certified Prosthetist Podiatrist Footcare Nurse Lymphatic Massage Therapist Compression Stocking Fitter Other___________________________
Physician/nurse practitioner orders received as required to change plan of care including agreeance to professional referral recommendations
Appropriate documents shared Pressure mapping Diagnostic results Identify need to reassess ABPI/TPBI in 6 months Lower leg assessment results
Acute care Complex Continuing Care/Rehab Long-term care Community care
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016

Page 23 of 35
Recent vascular study results (eg. ABPI, TPBI, Transcutaneous Oxygen Pressure(TcPo2), Laser Doppler Flowmetry, Doppler Arterial Waveforms or Segmental Doppler Pressure studies)
Relevant consultation notes Post and current treatment and education plan List of appropriate contact information for ongoing
needs
If wound closed or eschar is stable (in arterial disease) send discharge summary outlining outstanding issues and teaching completed to:
Referral source Most responsible physician (MRP)/nurse
practitioner
Primary care physician/Nurse Practioner Professionals referred to Other _____________________________
77-84 Days Expected Outcomes (Ongoing to day 90) NotesMost Responsible Physician(MRP)/Nurse Practitioner (NP) identified/informed
Communication with primary care physician and/or Nurse Practioner to update on any significant changes in patient’s condition.
Refer patient to ‘Care Connects’ if no responsible practioner currently involved with patient Determine if MRP/NP is part of family health team (FHT) or community health centre (CHC) and
consider additional supports availableIf Pressure injury is below knee: assess potential to heal
Bilateral lower leg assessment (LLA)completed
Complete: ABPI/TPBI completed within last 3 mths and results documented If unable to obtain ABPI/TPBI, referral to medical imaging for vascular studies is recommended Repeat ABPI/TPBI assessment every 3 months if healing is not progressing Bilateral lower leg assessment that includes : Leg measurements (foot, ankle, calf, thigh) to assess edema Nail changes (thicker, dry, crumbly, presence of fungal infection) Assess interdigital spaces Presence of callous or corns Presence of varicosities (varicose veins) Ankle flare Drainage on socks History of compression
Wound and periwound assessment completed Complete:
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
ABPI 0.5 to 0.8 TPBI 0.64 to 0.7 Suggest Transcutaneous Oxygen Pressure(TcPo2), Laser Doppler Flowmetry, Doppler Arterial Waveforms or Segmental Doppler Pressure studies
ABPI <0.5 TPBI <0.64 Urgent vascular surgical consult needed

Page 24 of 35
Bates-Jensen Wound Assessment Tool (BWAT) OR Pressure Ulcer Scale for Healing (PUSH) Measure and document size of wound Stage pressure injury Assess potential to heal Review etiology and consider biopsy if not healing Assess need for debridement Assessment for infection (NERDS and STONEES) Obtain photos following best practice as per framework for individual organization policies and
procedures. Suggest following publication as guideline: http://mydigitalpublication.com/publication/?i=206722
Link to Waterloo Wellington Integrated Guidelines for Pressure Injuries: http://wwwoundcare.ca/88/Provide_Local_Wound_Care/
Wound treatment plan determined in accordance to treatment goal (healable, maintenance or non-healable)
Arrange for physician/nurse practitioner orders as required including agreeance to professional referral recommendations
Identify cause of pressure Provide pressure redistribution (support surfaces) for sleep, seating and use of medical devices Debridement/reduction by qualified professional Re-visit to pressure redistribution professional is recommended Ensure appropriate skin care Identify any potential barriers to wound treatment plan Identify appropriate footwear, offloading and repositioning options Consider required referals and further follow-up with previous professional referrals Consider compression if venous insufficiency/edema present and if APBI/TPBI is within safe range
Link to Waterloo Wellington Venous Leg Guidelines – Compression: http://wwwoundcare.ca/102/ Utilize toolkit to determine wound cleansing, debridement and dressing selection (South West
Region Wound Care Program: Wound Cleansing Table and Dressing Selection and Cleansing enablers and CAWC Product Picker chart)
Moisture Associated Skin Damage (MASD) assessment completed
Assess continence of urine and stool If incontinence is a concern, a continence assessment should be completed by a qualified practioner (e.g.
an Enterstomal Therapist (ET) or Nurse Continence Advisor (NCA) Skin assessment including skin folds Link to RNAO Prompted Voiding Best Practice Guidelines
http://rnao.ca/sites/rnao-ca/files/Promoting_Continence_Using_Prompted_Voiding.pdf
Pain management considered and initiated Complete: Brief Pain Inventory Short Form (BPI-SF) Identify type of pain
1. Neuropathic Pain (described as burning, stinging, shooting, stabbing or hyperesthesia – sensitivity to touch). Suggested pharmaceutical treatment: Second generation tricyclic agents – e.g. Nortriptyline or Desipramine. If pain is not relieved try using Gabapentin or Pregabalin.
2. Nociceptive pain (described as sharp, aching or throbbing). Suggested pharmaceutical treatment: Non-Opioids – e.g. ASA or Acetaminophen Mild Opioids – e.g. CodeineStrong Opioids – e.g. Morphine or Oxycodone
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
Pain Red FlagsPossible Infection
Increase in pain level (new pain in patients with altered sensation )
Possible Arterial Involvement Pain on walking (caused by intermittent claudication) Pain with elevation of lower limbs Rest pain Nocturnal pain
Pain can be a trigger for autonomic dysreflexia that may occur in patients with spinal cord injury T6 or above
MASD can be defined as “inflammation and erosion of the skin caused by prolonged exposure to various sources of moisture, including urine or stool, perspiration, wound exudate, mucus, or saliva.
Initatition of compression therapy requires a lower leg assessment to be completed, ABPIs/TPBIs to be determined and results evaluated in addition to physician/NP order
When trying a new product, allow 2 weeks to assess effectiveness unless adverse effect noted.
A pressure injury with adequate vascular supply, pressure distribution & receiving treatment per best practice should show signs of healing within two to four weeks. When pressure injuries are not progressing towards closure (20-30%) treatment plan should include the initiation of a two-week trial of topical antimicrobials. An assessment by a wound care specialist is also recommended.

Page 25 of 35
Obtain physician/nurse practitioner orders for pharmaceutical treatments (opioids and non-opioids) Non-pharmacological pain control options (support surfaces, repositioning) Coordinate analgesic administration with wound care treatment times
Pressure Redistribution Ensure appropriate referrals for pressure redistribution have been arranged to qualified professionals
Review correct use of appropriate pressure redistribution devices Assess need for support surface (chair/bed)
Link to chart in guidelines: http://wwwoundcare.ca/81/Pressure_Reduction_and_Relief/ Review adherence to using appropriate pressure redistribution device(s) Assess barriers to appropriate pressure redistribution Initial and ongoing callous reduction is part of pressure redistribution Assess for secondary complications of offloading and refer concerns to treating practitioner
Look for redmarks, blisters, skin abrasions Ask about knee, hip or back issues (including contralateral limb) due to height difference of
offloading device Check for unsafe gait (are they stable, using appropriate aids, etc) Teach patient to assess for secondary complications
Check gait aids such as walker, cane, crutches Review goals of pressure redistribution (i.e. transition from cast to shoes, foot orthoses, etc.)
Check for availability for financial compensation (e.g. private insurance, veterans medical benefits, Assistive Devices Program (ADP), Ontario Disability Support Program –ODSP, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Medical/surgical history and co-morbidity management considered within care plan
Review for changes
Medication reconciliation and their impact on wound healing reviewed
Review for changes: Prescription, non-prescription, naturopathic and illicit drug use
Recent blood work and other diagnostic test results reviewed and implictions for wound healing considered
Determine bloodwork and other diagnostic tests required (see chart in guidelines)
Home Glycemic Control and Monitoring if diabetic BS and A1C are within recommended range per responsible physician or NP Use of glucose log book (Diabetes Passport) Adequate insulin supplies Glucometer and required supplies Assess for barriers in monitoring glycemic control
Patient’s nutritional status optimized Calculate Body Mass Index (BMI) Determine recent weight loss/gain Complete Mini Nutritional Assessment (MNA)
http://www.mna-elderly.org/forms/mini/mna_mini_english.pdf If screening section results < 11 = complete assessment section
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
Normal blood glucose ranges are needed for wound healing to occur
Nutrition is an essential component of wound healing. Consider dietician referral for supplementation recommmendations.

Page 26 of 35
If assessment section results< 24 = Registered Dietician referral required Recent dietary consult Identify barriers or risk factors to healthy eating Link to EatRight Ontario to talk to dietician
www.eatrightontario.ca 1-877-510-5102Patient and caregiver concerns and goals integrated into the care plan and shared with care team
Review for changes: Cardiff Wound Impact Questionnaire
ORWorld Health Organization Quality of Life (WHOQOL) form
Ensure all patient/caregiver goals and concerns been addressedPatient counselled on the benefit of activity and rest for comfort measures and wound healing
Recent changes in overall activity level Daily routine including continence
concerns and/or access to bathroom Personal assistance available to perform
activities of daily living Determine where patient sleeps at night
and sits during day Safety of transfers
Pressure relief device &/or redistribution Assess barriers to sleeping in bed Assess mobility and dexterity aids currently
being used (bedrail, superpole, trapezebar, airbed)
Recommendations for exercise Consider Occupational Therapist referral for
pressure relief devicePatient/caregiver educational plan continued Rest/Activity
Turning and sitting schedule for repositioning
Pillow between kneesSafety
Prevention of injury – friction, shearing When to call primary caregiver (eg. signs
and symptoms of infection, deep vein thrombosis, cellulitis, impaired blood flow, difficulties with compression)
Pressure Relief/redistribution surface Offloading is required ‘for life’ Understands need of debridement Encourage appropriate footwear to be
worn at all times when weight bearing as discussed with foot care specialist
Examination of footwear, orthotics and offloading devices for foreign objects, wear pattern, pressure points and presence of wound drainage
Lifestyle Smoking and e-cigarette cessation with
goal to be nicotene-freeGuidelines can be found at:http://rnao.ca/sites/rnao-ca/files/
Dietary Dietary requirements as per dietician Blood
glucose testing and recording in diary Link to EatRight Ontario to talk to dietician
www.eatrightontario.ca 1-877-510-5102Diagnostic Tests
Results understood by patient Diagnostic testing (nutritional blood work and
cholesterol levels) If diabetic, target ranges for A1C and blood
sugar Skin Care Wound self care Holistic self care of skin Incontinence and prevention/treatment of
Moisture Associated Skin Damage (MASD)Community Supports
Seating clinic for wheelchair Community support groups (eg. Diabetic
education and self- management sessions, walking groups, Southern Ontario Aboriginal Diabetes Initiative - SOADI)
Link to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
‘Teach-back’ method is a way of ascertaining patients understanding about what they need to know or do regarding their health. Patients are asked to state in their own words what they understand to be important. It is a way to confirm that things have been explained in a manner that the patient understands.

Page 27 of 35
Integrating_Smoking_Cessation_into_Daily_Nursing_Practice.pdf
Pain managementWound
Self care of wound
%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Other ____________________________
Ability to self-manage optimized Review for independence or need for ongoing assistance with the following: Barriers to participate (poor eyesight,
physical limitations, transportation, socioeconomic, social environment, cognitive ability, other co-morbidities)
Decreased sensory perception affects ability to respond to pressure-related issues
Review importance and potential barriers to smoking cessation at every visit
Pressure relief/redistribution Adequate hygiene skin exposed to
moisture, perspiration Daily foot inspection with mirror(including
bottom of foot and between toes) Ongoing footcare arranged Home Environment – ADL’s Wound care Nutrition
Compression application and removal if prescribed
Link to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Social/medical/family/employment obligationsSuggested website for reviewhttp://www.wwselfmanagement.ca/
Other ____________________________
Coping strategies implemented into plan of care Promoting independence to avoid practitioner/caregiver dependency Patient’s concerns and fears (including practitioner dependence) Signs of anxiety or other mental health issues (eg. delusions, hallucinations, paranoid behaviour) Depression screen using Geriatric Depression Scale assessment form –GDS15 Suicide assessment if applicable ETOH and illicit/recreational drug use
Check for availability for financial compensation (e.g. private insurance, ADP, veterans medical benefits, Ontario Disability Support Program –ODSP, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Family and caregiver support identified and incorporated into plan of care
Family/caregiver actively able to participate in treatment plan Repositioning, nutrition, continence if needed Importance of caregiver respite/relief
Social supports/community resources currently utilized is integrated into plan of care
Family support Check for availability for financial compensation (e.g. private insurance, veterans medical benefits,
Ontario Disability Support Program –ODSP/Ontario Works, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Community/health resourcesLink to Waterloo Wellington Diabetes Directory can be found at
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016

Page 28 of 35
http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Caregiver conflicts Long or short term placement Confirm that ongoing medication coverage is arranged
Link to Trillium Drug Benefitshttp://www.health.gov.on.ca/en/public/programs/drugs/programs/odb/opdp_trillium.aspx
Professional referrals are initiated Primary Care Physician Community Nursing Advanced Wound Specialist Nurse Practitioner Occupational Therapist Urologist Infectious Disease Specialist Vascular Surgeon Orthopedic Surgeon Dermatologist Plastic Surgeon Internist/Endocrinologist Nephrologist Cardiologist Opthalmologist/Optometrist Mental Health Specialist Psychologist/Psychiatrist Social worker Registered Dietitian Pharmacist Neurologist
Physiotherapist Physiatrist Registered Kinesiologist Chiropodist Diabetic Education Program
Patient self-referral link http://www.waterloowellingtondiabetes.ca/Public-Referrals.htmMedical professional referral link http://www.waterloowellingtondiabetes.ca/Professional-Site-Referral-Page.htm
Certified Pedorothist Certified Orthotist Certified Prosthetist Podiatrist Footcare Nurse Lymphatic Massage Therapist Compression Stocking Fitter Other___________________________
Physician/nurse practitioner orders received as required to change plan of care including agreeance to professional referral recommendationsAppropriate documents shared
Pressure mapping Diagnostic results Identify need to reassess ABPI/TPBI in 6 months Lower leg assessment results Recent vascular study results (eg. ABPI, TPBI,
Transcutaneous Oxygen Pressure(TcPo2), Laser Doppler Flowmetry, Doppler Arterial Waveforms or Segmental Doppler Pressure studies)
Relevant consultation notes Post and current treatment and education plan
Acute care Complex Continuing Care/Rehab Long-term care Community care Primary care physician/Nurse Practioner Professionals referred to Other _____________________________
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016

Page 29 of 35
List of appropriate contact information for ongoing needs
If wound closed or eschar is stable (in arterial disease) send discharge summary outlining outstanding issues and teaching completed to:
Referral source Most responsible physician (MRP)/nurse
practitioner
91-98 Days Expected Outcomes NotesMost Responsible Physician(MRP)/Nurse Practitioner (NP) identified/informed
Communication with primary care physician and/or Nurse Practioner to update on any significant changes in patient’s condition.
Refer patient to ‘Care Connects’ if no responsible practioner currently involved with patient Determine if MRP/NP is part of family health team (FHT) or community health centre (CHC) and
consider additional supports availableIf Pressure injury is below knee: assess potential to heal
Bilateral lower leg assessment (LLA)completed
Complete: ABPI/TPBI completed within last 3 mths and results documented If unable to obtain ABPI/TPBI, referral to medical imaging for vascular studies (arterial segmented
pressures) is recommended Repeat ABPI/TPBI assessment every 3 months if healing is not progressing Bilateral lower leg assessment that includes : Leg measurements (foot, ankle, calf, thigh) to assess edema Nail changes (thicker, dry, crumbly, presence of fungal infection) Assess interdigital spaces Presence of callous or corns Presence of varicosities (varicose veins) Ankle flare Drainage on socks History of compression
Wound and periwound assessment completed Complete: Bates-Jensen Wound Assessment Tool (BWAT) OR Pressure Ulcer Scale for Healing (PUSH) Measure and document size of wound Stage pressure injury Assess potential to heal Assess potential to heal Review etiology and consider biopsy if not healing Assess need for debridement
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
A pressure injury with adequate vascular supply, pressure distribution & receiving treatment per best practice should show signs of healing within two to four weeks. When pressure injuries are not progressing towards closure (20-30%) treatment plan may include the initiation of a two-week trial of topical antimicrobials. An assessment by a wound care specialist is also recommended.
ABPI 0.5 to 0.8 TPBI 0.64 to 0.7 Suggest Transcutaneous Oxygen Pressure(TcPo2), Laser Doppler Flowmetry, Doppler Arterial Waveforms or Segmental Doppler Pressure studies
ABPI <0.5 TPBI <0.64 Urgent vascular surgical consult needed

Page 30 of 35
Assessment for infection (NERDS and STONEES) Obtain photos following best practice as per framework for individual organization policies and
procedures. Suggest following publication as guideline: http://mydigitalpublication.com/publication/?i=206722
Link to Waterloo Wellington Integrated Guidelines for Pressure Injuries: http://wwwoundcare.ca/88/Provide_Local_Wound_Care/
Wound treatment plan determined in accordance to treatment goal (healable, maintenance or non-healable)
Arrange for physician/nurse practitioner orders as required including agreeance to professional referral recommendations
Identify cause of pressure Provide pressure redistribution (support surfaces) for sleep, seating and use of medical devices Debridement/reduction by qualified professional Re-visit to pressure redistribution professional is recommended Ensure appropriate skin care Identify any potential barriers to wound treatment plan Identify appropriate footwear, offloading and repositioning options Consider required referals and further follow-up with previous professional referrals Consider compression if venous insufficiency/edema present and if APBI/TPBI is within safe range
Link to Waterloo Wellington Venous Leg Guidelines – Compression: http://wwwoundcare.ca/102/ Utilize toolkit to determine wound cleansing, debridement and dressing selection (South West
Region Wound Care Program: Wound Cleansing Table and Dressing Selection and Cleansing enablers and CAWC Product Picker chart)
Moisture Associated Skin Damage (MASD) assessment completed
Assess continence of urine and stool If incontinence is a concern, a continence assessment should be completed by a qualified practioner (e.g.
an Enterstomal Therapist (ET) or Nurse Continence Advisor (NCA) Skin assessment including skin folds Link to RNAO Prompted Voiding Best Practice Guidelines
http://rnao.ca/sites/rnao-ca/files/Promoting_Continence_Using_Prompted_Voiding.pdf
Pain management considered and initiated Complete: Brief Pain Inventory Short Form (BPI-SF) Identify type of pain
1. Neuropathic Pain (described as burning, stinging, shooting, stabbing or hyperesthesia – sensitivity to touch). Suggested pharmaceutical treatment: Second generation tricyclic agents – e.g. Nortriptyline or Desipramine. If pain is not relieved try using Gabapentin or Pregabalin.
2. Nociceptive pain (described as sharp, aching or throbbing). Suggested pharmaceutical treatment: Non-Opioids – e.g. ASA or Acetaminophen Mild Opioids – e.g. CodeineStrong Opioids – e.g. Morphine or Oxycodone
Obtain physician/nurse practitioner orders for pharmaceutical treatments (opioids and non-opioids) Non-pharmacological pain control options (support surfaces, repositioning) Coordinate analgesic administration with wound care treatment times
Pressure Redistribution Ensure appropriate referrals for pressure redistribution have been arranged to qualified professionals
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
Pain Red FlagsPossible Infection
Increase in pain level (new pain in patients with altered sensation )
Possible Arterial Involvement Pain on walking (caused by intermittent claudication) Pain with elevation of lower limbs Rest pain Nocturnal pain
Pain can be a trigger for autonomic dysreflexia that may occur in patients with spinal cord injury T6 or above
MASD can be defined as “inflammation and erosion of the skin caused by prolonged exposure to various sources of moisture, including urine or stool, perspiration, wound exudate, mucus, or saliva.
Initatition of compression therapy requires a lower leg assessment to be completed, ABPIs/TPBIs to be determined and results evaluated in addition to physician/NP order
When trying a new product, allow 2 weeks to assess effectiveness unless adverse effect noted.

Page 31 of 35
Review correct use of appropriate pressure redistribution devices Assess need for support surface (chair/bed)
Link to chart in guidelines: http://wwwoundcare.ca/81/Pressure_Reduction_and_Relief/ Review adherence to using appropriate pressure redistribution device(s) Assess barriers to appropriate pressure redistribution Initial and ongoing callous reduction is part of pressure redistribution Assess for secondary complications of offloading and refer concerns to treating practitioner
Look for redmarks, blisters, skin abrasions Ask about knee, hip or back issues (including contralateral limb) due to height difference of
offloading device Check for unsafe gait (are they stable, using appropriate aids, etc) Teach patient to assess for secondary complications
Check gait aids such as walker, cane, crutches Review goals of pressure redistribution (i.e. transition from cast to shoes, foot orthoses, etc.) Check for availability for financial compensation (e.g. private insurance, veterans medical benefits,
Assistive Devices Program (ADP), Ontario Disability Support Program –ODSP, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Medical/surgical history and co-morbidity management considered within care plan
Review for changes
Medication reconciliation and their impact on wound healing reviewed
Review for changes: Prescription, non-prescription, naturopathic and illicit drug use
Recent blood work and other diagnostic test results reviewed and implictions for wound healing considered
Determine bloodwork and other diagnostic tests required (see chart in guidelines)
Home Glycemic Control and Monitoring if diabetic BS and A1C are within recommended range per responsible physician or NP Use of glucose log book (Diabetes Passport) Adequate insulin supplies Glucometer and required supplies Assess for barriers in monitoring glycemic control
Patient’s nutritional status optimized Calculate Body Mass Index (BMI) Determine recent weight loss/gain Complete Mini Nutritional Assessment (MNA)
http://www.mna-elderly.org/forms/mini/mna_mini_english.pdf If screening section results < 11 = complete assessment section If assessment section results< 24 = Registered Dietician referral required Recent dietary consult Identify barriers or risk factors to healthy eating Link to EatRight Ontario to talk to dietician
www.eatrightontario.ca 1-877-510-5102
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
Normal blood glucose ranges are needed for wound healing to occur
Nutrition is an essential component of wound healing. Consider dietician referral for supplementation recommmendations.

Page 32 of 35
Patient and caregiver concerns and goals integrated into the care plan and shared with care team
Review for changes: Cardiff Wound Impact Questionnaire
ORWorld Health Organization Quality of Life (WHOQOL) form
Ensure all patient/caregiver goals and concerns been addressedPatient counselled on the benefit of activity and rest for comfort measures and wound healing
Recent changes in overall activity level Daily routine including continence
concerns and/or access to bathroom Personal assistance available to perform
activities of daily living Determine where patient sleeps at night
and sits during day Safety of transfers
Pressure relief device &/or redistribution Assess barriers to sleeping in bed Assess mobility and dexterity aids currently
being used (bedrail, superpole, trapezebar, airbed)
Recommendations for exercise Consider Occupational Therapist referral for
pressure relief devicePatient/caregiver educational plan continued Rest/Activity
Turning and sitting schedule for repositioning
Pillow between kneesSafety
Prevention of injury – friction, shearing When to call primary caregiver (eg. signs
and symptoms of infection, deep vein thrombosis, cellulitis, impaired blood flow, difficulties with compression)
Pressure Relief/redistribution surface Offloading is required ‘for life’ Understands need of debridement Encourage appropriate footwear to be
worn at all times when weight bearing as discussed with foot care specialist
Examination of footwear, orthotics and offloading devices for foreign objects, wear pattern, pressure points and presence of wound drainage
Lifestyle Smoking and e-cigarette cessation with
goal to be nicotene-freeGuidelines can be found at:http://rnao.ca/sites/rnao-ca/files/Integrating_Smoking_Cessation_into_Daily_Nursing_Practice.pdf
Pain managementWound
Self care of wound
Dietary Dietary requirements as per dietician Blood
glucose testing and recording in diary Link to EatRight Ontario to talk to dietician
www.eatrightontario.ca 1-877-510-5102Diagnostic Tests
Results understood by patient Diagnostic testing (nutritional blood work and
cholesterol levels) If diabetic, target ranges for A1C and blood
sugar Skin Care Wound self care Holistic self care of skin Incontinence and prevention/treatment of
Moisture Associated Skin Damage (MASD)Community Supports
Seating clinic for wheelchair Community support groups (eg. Diabetic
education and self- management sessions, walking groups, Southern Ontario Aboriginal Diabetes Initiative - SOADI)
Link to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Other ____________________________
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016
‘Teach-back’ method is a way of ascertaining patients understanding about what they need to know or do regarding their health. Patients are asked to state in their own words what they understand to be important. It is a way to confirm that things have been explained in a manner that the patient understands.

Page 33 of 35
Ability to self-manage optimized Review for independence or need for ongoing assistance with the following: Barriers to participate (poor eyesight,
physical limitations, transportation, socioeconomic, social environment, cognitive ability, other co-morbidities)
Decreased sensory perception affects ability to respond to pressure-related issues
Review importance and potential barriers to smoking cessation at every visit
Pressure relief/redistribution Adequate hygiene skin exposed to
moisture, perspiration Daily foot inspection with mirror(including
bottom of foot and between toes) Ongoing footcare arranged Home Environment – ADL’s Wound care Nutrition
Compression application and removal if prescribed
Link to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Social/medical/family/employment obligationsSuggested website for reviewhttp://www.wwselfmanagement.ca/
Other ____________________________
Coping strategies implemented into plan of care Promoting independence to avoid practitioner/caregiver dependency Patient’s concerns and fears (including practitioner dependence) Signs of anxiety or other mental health issues (eg. delusions, hallucinations, paranoid behaviour) Depression screen using Geriatric Depression Scale assessment form –GDS15 Suicide assessment if applicable ETOH and illicit/recreational drug use Check for availability for financial compensation (e.g. private insurance, ADP, veterans medical
benefits, Ontario Disability Support Program –ODSP, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Family and caregiver support identified and incorporated into plan of care
Family/caregiver actively able to participate in treatment plan Repositioning, nutrition, continence if needed Importance of caregiver respite/relief
Social supports/community resources currently utilized is integrated into plan of care
Family support Check for availability for financial compensation (e.g. private insurance, veterans medical benefits,
Ontario Disability Support Program –ODSP/Ontario Works, Non-Insured Health Benefits -NIHB and Southern Ontario Aboriginal Diabetes Initiative – SOADI for First Nations people and Inuit)
Community/health resourcesLink to Waterloo Wellington Diabetes Directory can be found at http://www.waterloowellingtondiabetes.ca/userContent/documents/Public-Resource%20Library/Waterloo%20Wellington%20Diabetes%20Directory%202015%20-%20proof%204.pdf
Caregiver conflicts Long or short term placement Confirm that ongoing medication coverage is arranged
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016

Page 34 of 35
Link to Trillium Drug Benefitshttp://www.health.gov.on.ca/en/public/programs/drugs/programs/odb/opdp_trillium.aspx
Professional referrals are initiated Primary Care Physician Community Nursing Advanced Wound Specialist Nurse Practitioner Occupational Therapist Urologist Infectious Disease Specialist Vascular Surgeon Orthopedic Surgeon Dermatologist Plastic Surgeon Internist/Endocrinologist Nephrologist Cardiologist Opthalmologist/Optometrist Mental Health Specialist Psychologist/Psychiatrist Social worker Registered Dietitian Pharmacist Neurologist
Physiotherapist Physiatrist Registered Kinesiologist Chiropodist Diabetic Education Program
Patient self-referral link http://www.waterloowellingtondiabetes.ca/Public-Referrals.htmMedical professional referral link http://www.waterloowellingtondiabetes.ca/Professional-Site-Referral-Page.htm
Certified Pedorothist Certified Orthotist Certified Prosthetist Podiatrist Footcare Nurse Lymphatic Massage Therapist Compression Stocking Fitter Other___________________________
Physician/nurse practitioner orders received as required to change plan of care including agreeance to professional referral recommendations
Appropriate documents shared Pressure mapping Diagnostic results Identify need to reassess ABPI/TPBI in 6 months Lower leg assessment results Recent vascular study results (eg. ABPI, TPBI,
Transcutaneous Oxygen Pressure(TcPo2), Laser Doppler Flowmetry, Doppler Arterial Waveforms or Segmental Doppler Pressure studies)
Relevant consultation notes Post and current treatment and education plan List of appropriate contact information for ongoing
needs
If wound closed or eschar is stable (in arterial disease) send discharge summary outlining outstanding issues and
Acute care Complex Continuing Care/Rehab Long-term care Community care Primary care physician/Nurse Practioner Professionals referred to Other _____________________________
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016

Page 35 of 35
teaching completed to: Referral source Most responsible physician (MRP)/nurse
practitioner
Waterloo Wellington Integrated Wound Care Program wwwoundcare.ca May 2016