-
8/12/2019 16 - Control Muscular de La Patela
1/14
Muscular control of the patella
Terry Malone, EdD, PT, ATCa,*,George Davies, MEd, PT, ATCb, W.
Michael Walsh, MDc
aDepartment of Physical Therapy, University of Kentucky, 900
South Limestone,
Lexington, KY 40536, USAbDepartment of Physical Therapy,
University of Wisconsin LaCrosse, LaCrosse, WI 54601,
USAcDepartment of Orthopaedics, University of Nebraska Medical
Center, Omaha, NE 68118, USA
Although a commonly discussed subject, more misinformation and
anecdotal
presentations may exist for muscular strengthening and patellar
control than in
nearly any other area of knee rehabilitation. Much of this is
the result of the
slow development of appropriate analyses of clinical efficacy in
orthopedic
rehabilitation (ie, few published significant clinical outcome
studies related to
these patients) but most importantly is related to the complex
nature of thepatellofemoral joint and its impact on function. Since
the 1950s, generations of
clinicians have been imbued with the concept that knee
rehabilitation requires
an emphasis on vastus medialis obliquus strengthening. Some of
the early
classic works included sage observations but have been
interpreted in a manner
that has led to long lasting misinformation. An interesting
example is the work
of Smillie (1962):
The extensor apparatus may be regarded as consisting of two
components, the
rectus femoris, vastus lateralis and vastus intermedius, which
extend the knee to
within 10 15 degrees of full extension, and the vastus medialis
which isselective in action and comes into force in producing the
last 1015 degrees of
extension, although it may be used throughout the whole range in
overcoming
marked resistance [1].
He also labeled the vastus medialis the key to the knee and
espoused it is
the vastus medialis which is almost entirely responsible for the
stabilization and
protection of the joint from injury [1].
Lieb and Perry addressed these major points in their
anatomic/mechanical
analysis in 1968 [2]. They determined that some of these
observations are
related to the thin fascial covering of the vastus medialis, the
orientation oflongitudinal and oblique fibers in the medialis, the
independent innervation of
0278-5919/02/$ see front matterD 2002, Elsevier Science (USA).
All rights reserved.
PII: S 0 2 7 8 - 5 9 1 9 ( 0 2 ) 0 0 0 1 4 - 5
* Corresponding author.
E-mail address:[email protected] (T. Malone).
Clin Sports Med 21 (2002) 349362
-
8/12/2019 16 - Control Muscular de La Patela
2/14
the medialis oblique fibers, and the function of the oblique
fibers to align the
patella in the last 10to 15of extension. Most importantly in
their conclusions
and summary they delineated that the early atrophy of the
medialis indicates thegeneral quadriceps rather than that of a
local medialis deficiency and that the
only selective function of the medialis is patellar alignment.
Again, the unfor-
tunate interpretation of their work was that terminal extension
(the 10 to 15
range of motion) would therefore provide a selective training
impetus for the
vastus medialisparticularly the oblique fibers responsible for
patellar align-
ment. Fig. 1 presents the generally accepted vasti muscular
orientation and
insertional pattern.
Since 1968, many clinicians have invoked the Lieb and Perry
article as
being supportive of selective recruitment and exercise. The term
VMO (vastusmedialis obliquus) strengthening or emphasis has become
synonymous with
patellofemoral exercise prescription. This article is designed
to provide the reader
a review of what the peer reviewed literature supports and
refutes related to
muscular control of the patella. Statements or concepts will be
presented and
discussed in this format.
Muscular innervationneuromuscular drive
The evolution of surface and indwelling electromyography (EMG)
has been
vital to our appreciation of muscle function. Computer analyses
have dramat-
ically enhanced our ability to interpret and examine quadriceps
femoris function.
Where previously raw electrical signals were examined, envelops
of potentials
are now rectified, integrated (area under the curve), and
manipulated to provide
better recognition and representation of muscle function. Most
investigators will
use amplitude as their measured value of muscular output in
relation to
demanded action.
It is important to recognize limitations as well as the great
value of EMG. Wecan reliably assess muscle onset and cessation of
action but must be cautious in
the use/interpretation of amplitude, as reliability is often
somewhat inconsistent,
particularly values within an individual often demonstrating
significant variation.
Thus, several areas of these analyses deserve comment.
Selective action of the vastus medialis obliquus in terminal
extension
As described previously, several investigators provided clinical
observationsof what appeared to be direct evidence of the VMO being
most active in terminal
extension. The early EMG study of this phenomenon (1971) was
again by Lieb
and Perry [3] that refuted these claims. They evaluated the EMG
of the
quadriceps (including the VMO) at several positions during
maximal isometric
contractions. Using a pattern of correlation between
torque/position/EMG ampli-
tude, the quadriceps (including the VMO) was seen to exhibit a
stable, consistent
T. Malone et al / Clin Sports Med 21 (2002) 349362350
-
8/12/2019 16 - Control Muscular de La Patela
3/14
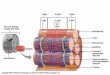
Fig. 1. Insertional patterns of the quadriceps femoris (VASTI:
VM, vastus medialis; VMO, vastus medialis o
-
8/12/2019 16 - Control Muscular de La Patela
4/14
pattern of recruitment throughout the range of motion with the
VMO having the
highest values. Again, this has often been misinterpreted by
some as supporting
terminal extension as the exercise of choice for patellofemoral
patients.Brownstein et al [4] used a similar methodology to
determine the optimal level
of EMG in relationship to torque of the quadriceps. These
researchers reported
that peak integrated EMG occurred at approximately 50 for males
and 70 for
females during maximal isometric muscle activation. VMO
activation was not
maximal in extension but rather lower in the range of motion
corresponding to
maximal torque. This is in agreement with Knight et al [5] who
showed a
decrease of vastus medialis activity occurred as one moved into
extension from a
flexed position. These data support the use of exercise lower in
the range of
motion (90
to 60
or 45
) as being more likely to maximally recruit the vastusmedialis
(longitudinal and oblique fibers) than terminal extension
activities.
It seems that terminal extension is not able to isolate the VMO
from the other
quadriceps muscular elements. The clinical observations indicate
VMO atrophy
that represents the quadriceps as a whole. Because of the
superficial location and
thin fascial covering, the VMO is much more easily palpated and
observed.
Terminal extension provides a biomechanically disadvantaged
position for the
quadriceps mechanism thus requiring high activity of the muscles
in extension
but not in an isolated fashion.
It is our recommendation to view the VMO as the mirror of the
quadriceps. Awell-defined VMO represents a strong extensor
mechanism. Palpation of a tensed
VMO also enables an estimation of function as the involved
extremity nearly
always exhibits a softness or less rigid muscle belly than the
maximally tensed
uninvolved extremity.
Isolation of the VMO by way of specific exercise
Numerous investigators have recommended a specific position or
pattern of
exercise to selectively challenge the VMO. One of the most
commonly cited is theconcept of incorporating hip adduction into
the quadriceps-strengthening program.
Hanten and Schulthies [6] examined the effect of maximal
isometric contrac-
tions of internal tibial rotation and hip adduction on EMG in
the VMO and vastus
lateralis (VL). The EMG amplitude was then normalized by way of
comparison
to the maximal voluntary contraction (MVC) values seen during
knee extension.
Hip adduction resulted in VMO values that were 61.75% of the MVC
during
extension, statistically greater than those seen in the VL
(45.63%). There were no
differences in VMO/VL during internal tibial rotation (47% and
45%). This led
these investigators to conclude that the VMO may be selectively
strengthenedthrough hip adduction. It must be noted that the
authors were speaking of hip
adduction and its resultant overflow creating activity in the
VMO (approximately
60% of what one produces with extension).
Others have attempted to incorporate hip adduction with knee
extension as a
selective means of training. Andriacchi et al used this
combination with dynamic
submaximal efforts that actually demonstrated decreased VMO and
VL EMG
T. Malone et al / Clin Sports Med 21 (2002) 349362352
-
8/12/2019 16 - Control Muscular de La Patela
5/14
than seen in corresponding static isometric positions of knee
extension [7]. Karst
and Jewett [8] asked their subjects to perform a series of
quadriceps exercises:
quadriceps setting (QS), straight leg raising (SLR), SLR with
hip lateral rotation,and SLR with hip adduction. The greatest
quadriceps EMG was seen during QS
and none of the variations provided additional emphasis to the
medial/medialis
vasti. Gryzlo et al analyzed five commonly used patellofemoral
exercises (SLR,
short arc extension, short arc extension with hamstring
cocontraction, squat, and
isometric co-contraction quadriceps/hamstrings) through EMG
activity [9]. No
selective actions were seen but increased activity in both
(simultaneously) the
medial and lateral vasti was seen in certain positions or
actions. Laprade et al
used subjects with and without patellofemoral pain comparing
their respective
EMG activity during five isometric exercises [10]. These
exercises included kneeextension, hip adduction, adduction with
knee extension, internal tibial rotation,
and knee extension with internal tibial rotation. Extension
exercises had the
greatest EMG values, no biasing (selective action or demand)
of/to the medial
vasti was seen, and no significant patterns of difference
(VMO/VL) were seen
between patients and controls. Only 13% of VMO EMG seen in this
submaximal
knee extension action was generated during hip adduction,
significantly less than
described by the maximal effort study of Hanten and
Schulthies.
Mirzabeigi et al examined nine quadriceps-strengthening
exercises to deter-
mine if an isolation or emphasis to the VMO could be created
[11]. Theseexercises included maximal isometric knee extension (hip
neutral, 30 internal
rotation, and 30external rotation); maximal isokinetic knee
extension (full range
and terminal 30range of motion); sidelying ipsilateral and
contralateral full knee
extension with a 10-pound weight; and stand and jump from a full
squat.
Normalized EMG analysis was performed for the VMO, VM, vastus
intermedius,
and vastus lateralis through indwelling fine wire. Their results
showed high-
integrated EMG amplitude for the medial and lateral portions of
the vasti during
specific actions but no selective opportunities for the VMO.
The literature thus does not support that isolated VMO exercises
exist.Although adduction of the hip shows overflow to the VMO, it
is not sufficient
to provide a strong training level stimulus (greater than 70% of
MVC) to this
structure. The VMO and VL are highly active in terminal range of
extension.
Most of these exercises have been imbedded in rehabilitation
regimens that
have been successful in their overall goal of enabling
patellofemoral patients to
return to function following a six to eight week training
program. Nonsurgical
care has been effective in our clinical experience in
approximately 8085% of
patients presenting with patellofemoral symptoms. Because of
this, many of the
purported successes may not be because of the specific concept
but rather tothe general improvement of the quadriceps as a
whole.
Timing of muscle activation
Several investigators have espoused that there is an alteration
of activation
among the components of the quadriceps in patients with
patellofemoral pain.
T. Malone et al / Clin Sports Med 21 (2002) 349362 353
-
8/12/2019 16 - Control Muscular de La Patela
6/14
The implication has been that patients have an altered pattern
whereby the VMO
is not activated early enough to avoid the lateralization of the
patella.
Souza and Gross [12] compared the VMO/VL EMG ratio of controls
andpatients with patellofemoral pain during isotonic and isometric
conditions. Stair
climbing (isotonic) provided a greater ratio than isometric
actions and patients
VMO/VL ratios were lower than ratios among control subjects.
They concluded
that patients with patellofemoral pain may have abnormal VMO/VL
activation
patterns, and speculated that isotonic patterns of exercise may
be more beneficial
than isometric actions.
Voight and Wieder evaluated the reflex response time in the VL
and VMO to a
patellar tendon tap [13]. They recruited 41 control subjects and
16 patients with
anterior knee pain and evaluated the reflex latency of the VMO
and VL. Theirdata demonstrated that control subjects fired their
VMO before the VL, whereas
patients exhibited a reversal of this pattern. They concluded
that patellofemoral
pain patients might demonstrate a neurophysiologic motor control
imbalance.
Karst and Willett [14] examined the timing of reflex responses
of the
quadriceps much like the previous study. EMG signals were
recorded following
patellar tendon tap but also in active knee extension in
weightbearing and
nonweightbearing positions. There were no significant EMG
response differences
for controls versus patients in any of the conditions. These
authors explained how
their study differed from the previous study through their use
of normalizingresponses related to subject height and other
problems perceived with the
relevancy of the previous data. One additional important finding
was the lack
of difference during active exercise. The authors pointed out
that reflex patterns
might not reflect the active unit.
Powers et al [15] examined the timing and intensity of the vasti
EMG activity
during level walking, stair climbing, and walking on ramps.
Twenty-six patello-
femoral pain patients and 19 normal control subjects were
assessed by way of
fine wire EMG while knee motion was recorded through a motion
analysis
system. No differences in the onset or cessation (timing) of
muscle activity wereseen; patellofemoral pain patients often
exhibited decreased overall EMG
intensity. There were no selective VMO differences compared with
VL activity.
It seems that there are no significant differences in timing or
VMO/VL
amplitude ratio during active exercise. The early study results
supporting differ-
ences has not been duplicated by later investigators.
Although patellofemoral rehabilitation regimens incorporate a
variety of
exercises, using those that generate the best responses for each
individual
afflicted with patellofemoral pain presents a great challenge
for the clinician
and patient. We recommend a process of matching the exercise
pattern to the typeof primary problem (classification) with which
the patient presents.
What is the impact of pain in the patellofemoral patient?
The classic pattern of pain and effusion resulting in inhibition
is vividly
displayed at the patellofemoral joint in relationship to
quadriceps activation. The
T. Malone et al / Clin Sports Med 21 (2002) 349362354
-
8/12/2019 16 - Control Muscular de La Patela
7/14
work of deAndrade et al linked knee joint distension with
significant reflex
inhibition of the quadriceps [16]. It is obvious that pain is
similar in effect when
inhibition is observed as demonstrated by Miller et al who found
increased VMOEMG through decreased pain measures [17]. Spencer et
al provided data
supporting an early response to effusion in the VMO as EMG
changes were
seen with 2030 ml of effusion whereas 5060 ml were required to
have a
similar effect on the VL [18].
Boucher et al examined the vasti muscle activity in subjects
with patellofe-
moral pain [19]. These investigators included Q-angle assessment
to enable a
correlation between this and pain, strength, and EMG activity.
When they
compared the EMG of the VMO/VL ratio in the five patients with
the highest
Q-angles to control subjects, a significant difference was seen
at the terminal 15
of extension. This was only in the symptomatic group and was
demonstrated only
near extension, as the ratio was not different lower in the
range of motion. This
finding is in agreement with Sousa and Gross [12] who found a
decrease in
VMO/VL ratio as one moves into extension with patellofemoral
pain patients.
Cerny [20] collected IEMG from a series of patellofemoral
patients and
controls using a variety of exercise patterns examining the
VMO/VL ratio and
pain perception. Although the patients reported a significant
decrease in pain by
way of taping during exercise, no alteration was seen in the
VMO/VL EMG ratio.
Conway et al [21] documented a similar outcome in patients with
anteriorknee pain. These subjects were tested on an isokinetic
device concentrically and
eccentrically with significant decreases in pain perception seen
during exercise
when modifiers (tape or brace) were used. An increase in
strength was seen in the
taped and braced conditions but the increase was not correlated
with the level of
pain decrease.
The literature supports the concept of significant inhibition
being present with
pain and effusion. Treatments to reduce pain and swelling result
in enhanced
strength measurements but no variation of the VMO/VL ratio (no
selective
effect). There is some support for a smaller level of effusion
affecting the VMOwhile not having an equal effect on the VL.
The rehabilitation regimen must include pain modulation
facilitating pain-free
exercises, a requirement for normal recruitment of the vasti.
Without such,
normal neuromuscular patterns are not developed (or redeveloped)
and long-
term abnormal patterns may be reinforced. A variety of
techniques can be used as
outlined in an earlier article in this volume.
What are the effects of taping, foot orthotics, and bracing on
the patellofemoral
joint patient?
Jenny McConnell popularized the use of taping the patella to
enhance the
patients ability to perform pain-free exercises [22]. The
clinician evaluates the
patient related to a variety structures and typically uses tape
to place a medial pull
on the patella. Rotation and tilt of the patella are also
assessed/addressed. This
activity is then evaluated by comparing the level of pain
perceived while
T. Malone et al / Clin Sports Med 21 (2002) 349362 355
-
8/12/2019 16 - Control Muscular de La Patela
8/14
performing a step up-step down with the untaped condition.
McConnell indicates
that this process provides a true long-term solution for these
patients [22].
Gilleard et al followed these concepts and evaluated the effects
of taping onthe onset of VMO and VL muscle activity in subjects
with patellofemoral pain
[23]. Comparison of untaped and taped conditions showed there
was no
difference in onset times among untapped subjects, whereas the
VMO onset
was earlier in the taped condition during step up and step down
tasks. The
investigators indicated the earlier onset of the VMO may be
helpful in patellar
control. Further research is needed to determine if it effects
patellar position and
if this is beneficial.
Conway et al [21] evaluated a series of 30 patellofemoral pain
patients related
to the impact of patellar taping on pain perception and
quadriceps eccentric/concentric output. Taping provided a
significant increase in eccentric and
concentric outputs compared with the control condition, along
with a significant
decrease in pain perception. There was not a strong correlation
between the
strength gains and pain decrease, thus indicating other factors
were responsible
for these changes.
Gigante et al [24] examined the medialization effect of taping
on the patella
through computed tomography (CT). Sixteen females with
patellofemoral pain
related to patellar incongruence were examined by way of CT
before and after
patellar taping. The results showed no difference in the
lateralization of thepatella and thus does not support that passive
medial positioning is accomplished
through taping.
Powers evaluated a series of female patellofemoral patients and
controls for
patellar motion through kinematic magnetic resonance imaging
(KMRI) and vasti
muscle activity by way of EMG [25]. Medial/lateral displacement
and tilt of the
patella were measured during resisted knee extension (by way of
KMRI) as vasti
EMG was simultaneously collected. The investigators summary
indicated
increased VM activity most likely is in response to abnormal
patellar kinematics
rather than the cause. This investigator further proposes the
role of the femoralsulcus as being an important determinant of
patellar kinematics in the last 30of
extension [26].
Kowall et al performed a prospective study of patellar taping
compared with a
control group of patients receiving the same treatment without
the addition of
taping [27]. These patients were also assessed through vasti EMG
during stair
stepping actions; pain (VAS), and strength by way of concentric
isokinetic
contractions. Significant increases in EMG amplitude and
strength (concentric
peak torque) and reductions in pain were seen in all subjects.
No differences in
outcomes were associated with the addition of taping to the
procedures. Althoughthere was no specific benefit to the use of
tape, it should be recognized that there
were significant improvements for each group demonstrating a
successful
rehabilitation regimen.
Bracing has been espoused as assistive in the management of
patellofemoral
pain patients, particularly those with a significantly increased
lateralization of the
patella. Palumbo evaluated a dynamic patellar brace (medial
force application)
T. Malone et al / Clin Sports Med 21 (2002) 349362356
-
8/12/2019 16 - Control Muscular de La Patela
9/14
with 93% of 62 patellar pain patients responding positively to
its use [28]. Levine
likewise reported a 77% response rate in similar patients using
a patellar strap
[29]. Shellock et al [30] evaluated the ability of a dynamic
brace to createrealignment of the patella in a patient known to
have significant lateral patellar
subluxation. KMRI was able to demonstrate a reduction of
lateralization (thus
realignment) and with the brace being used during the patients
rehabilitation
regimen successfully. Worrell et al [31] documented similar
results examining
taping and bracing by way of MRI and also significant reductions
in pain during
their applications.
Conway et al [21] evaluated the Palumbo brace with use in
patellofemoral
pain patients and its effect on force output and perceived pain.
Patients
demonstrated an immediate significant increase in eccentric
quadriceps outputand decrease in pain perception. There was not a
correlation between the increase
in torque and the decrease in pain, thus demonstrating other
factors play a role in
this process.
Timm [32,33] has published information related to the use of a
dynamic
restraint brace in patellofemoral patients with some positive
functional and
financial (cost reduction) outcomes. There have not been
peer-reviewed pub-
lications duplicating these data.
Hung and Gross [34] evaluated the impact of a 10 lateral or
medial wedge
on VMO and VL EMG activity during a single leg partial squat and
maximalisometric quadriceps contraction in extension. The
normalized EMG showed
greatest activity during the single leg partial squat but there
were no differ-
ences with the use of wedges. The investigators conclude that
the alterations
seen with the use of wedges may be the result of mechanical
factors other than
EMG changes.
There is evidence that the application of patellar taping or a
brace significantly
reduces perceived pain and improves quadriceps output. There is
limited support
that taping or bracing influences patellar alignment, and if it
does occur at all, it is
likely to be only in a few specific patients.Because a decrease
in pain perception occurs, the application of tape or brace
can be an assistive measure enabling the inclusion of pain-free
exercises. It is
important to recognize the use of these modalities as a means to
an end: pain-free
exercise allowing an increase in quadriceps function.
Does the type of exercise or specific modality significantly
alter the demand on
the quadriceps?
A variety of exercises have been recommended for the
rehabilitation ofpatellofemoral patients. The literature gives many
anecdotal and technique driven
answers rather than a large volume of evidence-based practice
data. A recent
review of evidence-based practice outcomes related to
rehabilitation of the knee
gives the most common documented outcomes to the use of
therapeutic exercise
[35]. Thus the use of active exercise was seen to be effective
whereas many other
interventions have limited published support. The questions
become: (1) is there
T. Malone et al / Clin Sports Med 21 (2002) 349362 357
-
8/12/2019 16 - Control Muscular de La Patela
10/14
a specific exercise sequence that will be most effective for
patellofemoral pain
patients? and (2) are there modalities that can bias the
quadriceps response?
Gryzlo et al [9] found the highest EMG levels in the VMO and VL
to occur interminal extension, particularly with load (resistance).
They also showed the
quadriceps EMG activity increases during ascent from a squat,
emphasizing the
concentric action requiring a higher level of EMG. They also
showed no selective
action for the VMO. Laprade [10] found similar values with the
highest demand
on the VMO and VL occurring at terminal extension in isometric
contractions.
Souza and Gross [12] compared patients with patellofemoral pain
with a
group of controls for VMO/VL EMG activity in isometric or
stair-climbing
activities. They found no true isolated exercises (VMO selective
activities) but
did find that patients ratios of VMO/VL were greater during the
isotonic stairclimbing than during isometric exercises. This could
relate to the closed-chain
pattern, believed by some investigators to enable enhanced VMO
and VL
exercise. Witvrouw et al [36] attempted to compare the efficacy
of the open
kinetic chain exercise pattern versus the closed kinetic chain
pattern in patello-
femoral pain patients. They randomly assigned 60 patellofemoral
pain patients to
either an open chain or closed chain program of exercises. These
patients
participated in five weeks of rehabilitation with a variety of
objective and
subjective outcome measures. Both groups demonstrated
significant improve-
ments but there were no differences in the level of improvement
between the twoexercise groups. They found significant improvements
for both training groups
in quadriceps strength assessment (open chain) as documented
with isokinetic
evaluation. The greatest gains were at higher velocities (180,
300 per second).
These data agree with the results of Kowall, [27] who found
better results at 180
per second, rather than at 60 per second. This points toward
using higher
Table 1
Patellofemoral classifications and specific protocols
Classification Patellar compression
syndromes
Patellar instability Biomechanical dysfunction
Evaluation
features
Excessive pressure,
typically lateral
patellar facet
Abnormal patellar
ligamentous or bony
structures, active/passive
instability
Significant imbalances:
foot, limb length
discrepancies, and
flexibility deficits
Muscular
concepts
Exercise lower in
ROM, minimize
terminal
extension loads
Avoid terminal extension,
exercise lower in
ROM (4590),
Patella in the groove
Treat specifics: orthotics,
inserts (lifts), stretching
(if orthotics: watch out to
not cause limb lengthdiscrepancy by blocking
pronationmay require lift
to other leg
T. Malone et al / Clin Sports Med 21 (2002) 349362358
-
8/12/2019 16 - Control Muscular de La Patela
11/14
velocities during training when possible to better simulate
function and to reduce
pain and other inhibitory influences.
Sheehy et al [37] examined the vasti EMG activity in the
commonly usedstair-climbing activity in patellofemoral pain
patients and control subjects. There
were no differences in the ratio between patients and control
subjects in any
assessment. They found the peak VMO/VL ratio occurred during
ascent
(concentric) with lower values seen in descent (eccentric).
Attempting to predict the effect of exercise on long-term
outcome is
difficult. Natri et al [38] performed a prospective seven-year
follow-up study
of chronic patellofemoral patients. Their results support the
concept that
restoring the quadriceps functional capacity is important in the
long-term
success of these patients.Several clinicians and researchers
have used biofeedback and electrical
stimulation in treatment programs and research studies to alter
quadriceps demand
or response. Draper demonstrated the positive effect of
biofeedback as an adjunct
in facilitating the return of quadriceps function following
anterior cruciate
ligament (ACL) reconstruction [39]. Her data support the use of
biofeedback to
enhance voluntary recruitment of motor units (often referred to
as re-education).
Ingersoll and Knight [40] showed patellar medialization
(decreased congruence
angle) through the use of VMO biofeedback during quadriceps
strengthening
compared with the exercises used alone. Wise et al [41]
developed a three-phasesequential protocol culminating in an
attempt to use biofeedback to facilitate
VMO activity during functional movements. LeVeau [42]
recommended a two-
phase process of attempting to decrease VL activity during
quadriceps setting
followed by attempting to enhance VMO. Electrical stimulation
has been shown to
assist in muscle activation and medialization of the patella in
vivo. Koh et al [43]
Direct patellar
trauma
Soft tissue
lesions
Overuse syndromes Osteochondritis
diseases
Neural disorders
Direct impact
to patella
dashboard
Palpation or
tension pain
about the knee/
patella (plica,
fat pad, bursa)
Tendon (itis/osis)
palpation
of the apophyses
(patella or tibia)
Deep pain,
dissecans of
patella or femur
Pain out
of proportion
Avoid pain
and crepitation,
exercise in
pain-freeROM, partial
ROM isotonics
and isometrics
(above/below
painful area
of contact)
Avoid pain,
decrease
inflammation,
Avoid exercisethat causes
irritation/pain,
isometrics and
selected/partial
ROM isotonics
Avoid acute
painful actions,
quadriceps
program-eccentricemphasis: 10 12
weeks required,
pain modulation,
protect tibia
insertion from
direct impacts
(donut pad)
Gentle quadriceps
strengthening,
pain-free program
Often medial
saphenous nerve,
do it early, early
pain managementis the best
initial option
T. Malone et al / Clin Sports Med 21 (2002) 349362 359
-
8/12/2019 16 - Control Muscular de La Patela
12/14
showed that through passive electrical stimulation of the VMO a
patellar
medialization occurred whereas lateralization occurred during
unstimulated active
knee extension. Bohannon [44] found a similar effect, with VMO
electricalstimulation providing maintenance of a medial patellar
position in a patient
experiencing lateral patellar dislocation.
Although no quadriceps exercise is able to isolate specific
portions of the
mechanism, it seems isolation is not required for long-term
success. The appro-
priate selection of exercise should be based on signs and
symptoms as discerned
during the evaluation. The integration of open and closed chain
exercises may be
required for optimal rehabilitation in many patients. The use of
biofeedback and
electrical stimulation may provide adjuncts to overall
treatment.
Unfortunately, too many clinicians attempt to treat all
patellofemoral patientsby way of a single sequence of exercises.
This does not work well as the needs of
the patellar subluxating patient are different from those of the
patient with an
articular cartilage defect. Most patellofemoral patients have
signs and symptoms
that allow them to be grouped or classified, enabling a specific
protocol to match
their needs to be applied. We recommend using a classification
scheme to provide
an evaluation-based regimen and also better defining outcomes
with these
challenging patients [45]. Our system provides the following
eight classes with
recommendations for specific rehabilitation: patellar
compression syndromes,
patellar instability, biomechanical dysfunction, direct patellar
trauma, soft tissuelesions, overuse syndromes, osteochondritis
diseases, and neurologic disorders
[45]. This process of evaluation, classification, and specific
protocol and applica-
tion is presented in Table 1. It is important that clinicians
recognize their level of
success should be 80%+ overall, but not with each of these
classes will this be true.
Summary
Patellofemoral patients are among the most common yet most
challengingindividuals presenting for orthopedic care. The key word
in the previous sentence
is individual. A single protocol of care is not sufficient for
these special
individuals. Many concepts have been evaluated through review of
the peer-
reviewed literature with the following highlights: (1) the
concept of VMO
isolation through specific exercise should no longer be part of
our lexicon; (2)
patellofemoral patients improve when they are able to enhance
quadriceps
functional patterns by way of pain-free exercise; (3)
patellofemoral patients do
not fit into a single box but rather require an evaluation-based
classification
and specific interventional pattern.Many of the special
techniques used by clinicians in treating these patients
have not been well defined through research and also are lacking
in evidence of
clinical efficacy. We also must recognize, however, that good
clinical observa-
tions can be the first step in defining what questions should be
asked and how
they can be answered. It is vital that we answer the questions
without allowing
bad science through dogma and anecdote to prevail. Likewise, we
need to be
T. Malone et al / Clin Sports Med 21 (2002) 349362360
-
8/12/2019 16 - Control Muscular de La Patela
13/14
diligent in determining our successes and failures through well
designed and
implemented clinical and research studies.
References
[1] Smillie IS. Injuries of the knee joint. 3rd edition.
Baltimore, MD: Williams and Wilkins Publish-
ers; 1962.
[2] Lieb FJ, Perry J. Quadriceps function: an anatomic and
mechanical study using amputated limbs.
J Bone and Joint Surg 1968;50:153548.
[3] Lieb FJ, Perry J. Quadriceps function : an electromyographic
study under isometric conditions.
J Bone and Joint Surg 1971;53:74958.
[4] Brownstein BA, Lamb RL, Mangine RE. Quadriceps torque and
integrated electromyography.
J Orthop Sports Phys Ther 1985;6(6):30914.
[5] Knight KL, Martin JA, Londerdee BR. EMG comparison of
quadriceps femoris activity during
knee extensions and straight leg raises. Am J Phys Med
1979;58:5769.
[6] Hanten WP, Schulthies SS. Exercise effect on EMG activity of
the vastus medialis oblique and
vastus lateralis muscles. Phys Ther 1990;70(9):5615.
[7] Andriacchi TP, Andersson GBJ, Ortengren R, Mikosz RP. A
study of factors influencing muscle
activity about the knee joint. J Orthop Res 1984;1:26675.
[8] Karst GM, Jewett PD. EMG analysis of exercises proposed for
differential activation of the
medial and lateral quadriceps femoris muscle components. Phys
Ther 1993;73(5):286 95.
[9] Gryzlo SM, Patek RM, Pink M, Perry J. EMG analysis of knee
rehabilitation exercises. J Orthop
Sports Phys Ther 1994;20(1):3643.[10] Laprade J, Culham E,
Brouwer B. Comparison of five isometric exercises in the
recruitment of
the VMO in persons with and without patellofemoral pain
syndrome. J Orthop Sports Phys Ther
1998;27(3):197204.
[11] Mirzabeigi E, Jordan C, Gronley JK, Rockowitz NL, Perry J.
Isolation of the VMO muscle
during exercise. Am J Sports Med 1999;27(1):503.
[12] Souza DR, Gross MT. Comparison of VMO:VL muscle integrated
EMG ratios between healthy
subjects and patients with patellofemoral pain. Phys Ther
1991;71(4):310 20.
[13] Voight ML, Wieder DL. Comparative reflex response times of
VMO and VL in normal subjects
and subjects with extensor mechanism dysfunction. An EMG study.
Am J Sports Med 1991;
19(2):1317.
[14] Karst GM, Willett GM. Onset timing of EMG activity in the
VMO and VL muscles in subjectswith and without patellofemoral pain
syndrome. Phys Ther 1995;75(9):81323.
[15] Powers CM, Landel R, Perry J. Timing and intensity of
vastus muscle activity during func-
tional activities in subjects with and without patellofemoral
pain. Phys Ther 1996;76(9):
94655.
[16] deAndrade JR, Grant C, Dixon A. Joint distension and reflex
muscle inhibition in the knee.
J Bone and Joint Surg 1965;47:31322.
[17] Miller JP, Sedory D, Croce RV. Vastus medialis obliquus and
vastus lateralis activity in patients
with and without patellofemoral pain syndrome. J Sport Rehab.
1997;6:110.
[18] Spencer JD, Hayes KC, Alexander IJ. Knee joint effusion and
quadriceps reflex inhibition in
man. Arch Phys Med Rehab 1984;65:1717.
[19] Boucher JP, King MA, Lefebvre R, Pepin A. Quadriceps
femoris muscle activity in patellofe-moral pain syndrome. Am J
Sports Med 1992;20(5):52732.
[20] Cerny K. Vastus medialis oblique/vastus lateralis muscle
activity ratios for selected exercises in
persons with and without patellofemoral pain syndrome. Phys Ther
1995;75(8):672 83.
[21] Conway A, Malone TR, Conway P. Patellar alignment/tracking
alteration: effect on force output
and perceived pain. Isokinetics Exercise Science 1992;2(1):9
17.
[22] McConnell J. The management of chondromalacia patella: a
long-term solution. Aust J Physio
1986;32:21523.
T. Malone et al / Clin Sports Med 21 (2002) 349362 361
-
8/12/2019 16 - Control Muscular de La Patela
14/14
[23] Gilleard W, McConnell J, Parsons D. The effect of patellar
taping on the onset of VMO and VL
muscle activity in persons with patellofemoral pain. Phys Ther
1998;78(1):2532.
[24] Gigante A, Pasquinelli FM, Paladini P, Ulisse S, Greco F.
The effects of patellar taping on
patellofemoral incongruence: a computed tomography study. Am J
Sports Med 2001;29(1):
8892.
[25] Powers CM. Patellar kinematics, part I: the influence of
vastus muscle activity in subjects with
and without patellofemoral pain. Phys Ther 2000;80(10):956
64.
[26] Powers CM. Patellar kinematics, part II: the influence of
the depth of the trochlear groove in
subjects with and without patellofemoral pain. Phys Ther
2000;80(10):965 73.
[27] Kowall MG, Kolk G, Nuber GW, Cassisi JE, Stern SH. Patellar
taping in the treatment of
patellofemoral pain: a prospective randomized study. Am J Sports
Med 1996;24(1):61 6.
[28] Palumbo PM. Dynamic patellar brace: a new orthosis in the
management of patellofemoral
disorders. A preliminary report. Am J Sports Med
1981;9(1):459.
[29] Levine J, Splain SH. Use of the infrapatella strap in the
treatment of patellofemoral pain. Clin
Orthop 1979;139:17981.
[30] Shellock FG, Mink JH, Deutsch AL, Molnar T. Effect of a
newly designed patellar realignment
brace on patellofemoral relationships. Med Sci Sports Exerc
1995;27(4):469 72.
[31] Worrell T, Ingersoll CD, Bockrath-Pgliese K. Effect of
patellar taping and bracing on patellar
position as determined by MRI in patients with patellofemoral
pain. J Athl Train 1998;33(1):
1620.
[32] Timm KE. Randomized controlled trial of Protonics on
patellar pain, position, and function. Med
Sci Sports Exerc 1998;30(5):66570.
[33] Timm KE. The clinical and cost effectiveness of two
different programs for rehabilitation
following ACL reconstruction. J Orthop Sports Phys Ther
1997;25(1):43 8.
[34] Hung YJ, Gross MT. Effect of foot position on EMG activity
of the VMO and VL during lowerextremity weight-bearing activities.
J Orthop Sports Phys Ther 1999;29(2):93 102.
[35] Philadelphia panel evidence-based clinical practice
guidelines on selected rehabilitation inter-
ventions for knee pain. Phys Ther 2001;81(10):1675700.
[36] Witvrouw E, Lysens R, Bellemans J, Peers K, Vanderstraeten
G. Open versus closed kinetic
chain exercises for patellofemoral pain: a prospective,
randomized study. Am J Sports Med 2000;
28(5):68794.
[37] Sheehy P, Burdett RG, Irrgang JJ, VanSwearingen J. An EMG
study of the VMO and VL activity
while ascending and descending steps. J Orthop Sports Phys Ther
1998;27(60):4239.
[38] Natri A, Kannus P, Jarvinen M. Which factors predict the
long-term outcome in chronic patel-
lofemoral pain syndrome? A seven-year prospective follow-up
study. Med Sci Sports Exerc
1998;30(11):15727.[39] Draper V. Electromyographic biofeedback
and recovery of quadriceps femoris muscle function
following ACL reconstruction. Phys Ther 1990;70(11):11 7.
[40] Ingersoll CD, Knight KL. Patellar location changes
following EMG biofeedback or progressive
resistance exercises. Med Sci Sports Exerc 1991;23:11227.
[41] Wise HH, Fiebert IM, Kates JL. EMG biofeedback as treatment
for patellofemoral pain syn-
drome. J Orthop Sports Phys Ther 1984;6:95103.
[42] LeVeau BF, Rogers C. Selective training of the vastus
medialis muscle using EMG biofeedback.
Phys Ther 1980;60:14105.
[43] Koh TJ, Grabiner MD, DeSwart RJ. In vivo tracking of the
human patella. J Biomech 1992;25:
63743.
[44] Bohannon RW. Effect of electrical stimulation to the vastus
medialis muscle in a patient withchronically dislocating patellae.
Phys Ther 1983;63:14457.
[45] Wilk KE, Davies GJ, Mangine RE, Malone TR. Patellofemoral
disorders: a classification system
and clinical guidelines for nonoperative rehabilitation. J
Orthop Sports Phys Ther 1998;28(5):
30722.
T. Malone et al / Clin Sports Med 21 (2002) 349362362













![UNIT 6 – Muscular system · Web view[UNIT 6 – Muscular system] Notes Outline 1 Functions of Skeletal Muscle Movement - Tone and Posture - Protection - Control Openings - Maintain](https://img.pdfslide.us/doc/110x75/5f3016e30e95ce5ccf63b0a2/unit-6-a-muscular-system-web-view-unit-6-a-muscular-system-notes-outline-1.jpg)