-
7/30/2019 15 Th Oct Course
1/40
-
7/30/2019 15 Th Oct Course
2/40
-
7/30/2019 15 Th Oct Course
3/40
Two third of deaths from pulmonaryembolism occur within 30
minutes
of the first symptoms
-
7/30/2019 15 Th Oct Course
4/40
Explain the importance of venousthromboembolism in
gynaecologicalsurgeryIdentify the level of risk in preoperative
patientsExplain the pros and cons of various
prophylactic methodsBased on best evidence, use theappropriate
method/s of VTE prophylaxis inclinical practice
-
7/30/2019 15 Th Oct Course
5/40
Most common cause of preventable deathin hospitalized
patientsRisk of fatal perioperative PE ~0.8%International
Multicentre Trial. Lancet . 1975
150,000 to 200,000 deaths per year; ~1/3 inperioperative
patients
Horlander et al. Arch Intern Med . 2003;163:1711-1717.AHRQ: VTE
prevention is number one priorityto improve safety in hospitals
-
7/30/2019 15 Th Oct Course
6/40
2003 Nationwide Inpatient SampleAdult surgical patients, LOS 2
days
7.8 million surgical discharges44% low risk 15% moderate risk
24% high risk 17% very high risk
4.4 million at risk for VTE
Anderson et al. Am J Hematol . 2007;82:777-782.
-
7/30/2019 15 Th Oct Course
7/40
Population-based, prospective cohort study947,454 middle-aged
women in U.K.
enrolled between 1996-2001Mean follow-up 6.2 years239,614
underwent surgery
5,419 readmitted for VTE within 12 weeks ofinpatient surgery
270 deaths from fatal PE
Sweetland et al. BMJ. 2009;339:b4583.
-
7/30/2019 15 Th Oct Course
8/40
-
7/30/2019 15 Th Oct Course
9/40
Degree of risk for individual patientOutcomes Research: What are
our bestoptions?Intensity of
prophylaxisManagementRecommendations/ConsensusStatementsFuture
directions
-
7/30/2019 15 Th Oct Course
10/40
Venous stasisHypercoagulability
Endothelial damage
-
7/30/2019 15 Th Oct Course
11/40
Past history of DVTCancer Age>40 >60Prior radiation
therapyAnkle edema
Varicose veinsRadical vulvectomy or exenterationProlonged OT
time (> 4 hrs)
Clarke-Pearson, Obstet Gynecol, 69:146, 1987
-
7/30/2019 15 Th Oct Course
12/40
-
7/30/2019 15 Th Oct Course
13/40
Low-dose heparinLow molecular weight heparin
Anti -embolism stockings Pneumatic leg compression
WarfarinIVC interruption
-
7/30/2019 15 Th Oct Course
14/40
Controls (2076)
Fatal PE 16
Death assoc with PE 6
Heparin (2045)
2 p
-
7/30/2019 15 Th Oct Course
15/40
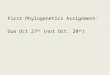
Outcome LDUHN=2045
No ProphylaxisN=2076
RR
Death any cause 80 100 0.81 (0.61 to 1.1)
Fatal PE 2 16 0.13 (0.02 to 0.55)
Death with PE 3 6 0.51 (0.13 to 2.0)
Suspected DVT 39 81 0.49 (0.33 to 0.71)Confirmed DVT 11 32 0.35
(0.18 to 0.69)
DVT by FUT 48/625 164/667 0.31 (0.23 to 0.42)
Proximal DVT 5/625 49/667 0.11 (0.04 to 0.27)
-
7/30/2019 15 Th Oct Course
16/40
In benign gynaecologic surgeryLDUH 5000 u every 12H
Control heparin
Ballard 1973 29% 3.6%
Adolf 1978 29% 7%
Taberner 1978 23% 6%
-
7/30/2019 15 Th Oct Course
17/40
Does Low Dose Heparin Work for Every Patient?
How about gynecologic cancer
patients?
-
7/30/2019 15 Th Oct Course
18/40
LOW-DOSE HEPARIN In GynecologicOncology Surgery5000 U every 12
hours for 7 day
Clarke-Pearson. Am J Obstet Gynecol 145:606, 1983
DVT(FUT) (%)
Contros n=97 12 (12.4)
LDUH n=88 13 (14.8)
-
7/30/2019 15 Th Oct Course
19/40
What about a more intense
Low Dose Heparin Regimen for Cancer Patients?
-
7/30/2019 15 Th Oct Course
20/40
-
7/30/2019 15 Th Oct Course
21/40
Enoxaparin, dalteparin, tinzaparin,fondaparinuxEffectiveness in
thromboprophylaxis
- equivalent to LDUH- similar frequency of complications
Convenience of once a day dosing with
dose variation between different LMWH(greater bioavailability,
rapid onset, predictable dose- response effect and low rate HIT,
more anti Xa, lessantithrombin thus less bleeding &
haematoma)
Cost vs. Convenience
-
7/30/2019 15 Th Oct Course
22/40
16 RCTs11,847 patients with cancers.Efficacy and
safetyConclusion: no difference betweenperioperative
thromboprophylaxis withLMWH vs. LDUH on mortality and
embolicoutcomes
-
7/30/2019 15 Th Oct Course
23/40
Graded compression
stockings, anti embolismstockings (TED Hose).Intermittent
pneumaticcompression
-
7/30/2019 15 Th Oct Course
24/40
Systematic reviews should be integralpart of VTE prophylaxis in
both moderateor high risk patients either asmonotherapy or in
combination.More efficacious when combined with
pharmacological methods
-
7/30/2019 15 Th Oct Course
25/40
Obstet Gynecol. 1984 Jan;63(1):92-8.Prevention of postoperative
venous thromboembolism by external pneumatic
calf compression in patients with gynecologic
malignancy.Clarke-Pearson DL , Synan IS , Hinshaw WM , Coleman RE ,
Creasman WT .
Most effective in first 5 daysIncidence mostly among patient
high risk group
http://www.ncbi.nlm.nih.gov/pubmed/6691021http://www.ncbi.nlm.nih.gov/pubmed?term=Clarke-Pearson%20DL[Author]&cauthor=true&cauthor_uid=6691021http://www.ncbi.nlm.nih.gov/pubmed?term=Synan%20IS[Author]&cauthor=true&cauthor_uid=6691021http://www.ncbi.nlm.nih.gov/pubmed?term=Hinshaw%20WM[Author]&cauthor=true&cauthor_uid=6691021http://www.ncbi.nlm.nih.gov/pubmed?term=Coleman%20RE[Author]&cauthor=true&cauthor_uid=6691021http://www.ncbi.nlm.nih.gov/pubmed?term=Creasman%20WT[Author]&cauthor=true&cauthor_uid=6691021http://www.ncbi.nlm.nih.gov/pubmed?term=Creasman%20WT[Author]&cauthor=true&cauthor_uid=6691021http://www.ncbi.nlm.nih.gov/pubmed?term=Coleman%20RE[Author]&cauthor=true&cauthor_uid=6691021http://www.ncbi.nlm.nih.gov/pubmed?term=Hinshaw%20WM[Author]&cauthor=true&cauthor_uid=6691021http://www.ncbi.nlm.nih.gov/pubmed?term=Synan%20IS[Author]&cauthor=true&cauthor_uid=6691021http://www.ncbi.nlm.nih.gov/pubmed?term=Clarke-Pearson%20DL[Author]&cauthor=true&cauthor_uid=6691021http://www.ncbi.nlm.nih.gov/pubmed?term=Clarke-Pearson%20DL[Author]&cauthor=true&cauthor_uid=6691021http://www.ncbi.nlm.nih.gov/pubmed?term=Clarke-Pearson%20DL[Author]&cauthor=true&cauthor_uid=6691021http://www.ncbi.nlm.nih.gov/pubmed/6691021http://www.ncbi.nlm.nih.gov/pubmed/6691021
-
7/30/2019 15 Th Oct Course
26/40
Low dose heparin Intermittent pneumaticcompression
N= 107 N=101
DVT7 (6.5%) 4 (4%)
Pulmonary emboli0
p=0.54
Increased transfusion Increasedretroperitoneal drainage 23%
prolonged PTT
0
-
7/30/2019 15 Th Oct Course
27/40
No difference in bloodloss and transfusionpost op
DVT PE
IPC 1/106 0
-
7/30/2019 15 Th Oct Course
28/40
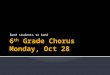
Regimens #trials #patients #DVT Incidence(%)
RRR
controls 54 4710 1074 25
LDUH 50 7716 648 8 68
LMWH 13 4320 226 5 80
IPC 14 780 61 8 67
GCS 9 472 51 11 56
-
7/30/2019 15 Th Oct Course
29/40
-
7/30/2019 15 Th Oct Course
30/40
-
7/30/2019 15 Th Oct Course
31/40
-
7/30/2019 15 Th Oct Course
32/40
-
7/30/2019 15 Th Oct Course
33/40
-
7/30/2019 15 Th Oct Course
34/40
-
7/30/2019 15 Th Oct Course
35/40
-
7/30/2019 15 Th Oct Course
36/40
What should we do toprevent VTE following
gynaecological surgery?
-
7/30/2019 15 Th Oct Course
37/40
-
7/30/2019 15 Th Oct Course
38/40
-
7/30/2019 15 Th Oct Course
39/40
Major gyn surgery with additional risk factors, major surgery
for malignancy-LDUH 5000u tds, LMWH high dose, IPC (1A)
Alternatively combination LDUH/LMWH + GCS/IPC,prophylaxis should
continue until discharge
Continued prophylaxis up to 4 weeks after discharge for cancer
cases & >60 years
-
7/30/2019 15 Th Oct Course
40/40
Explain the importance of venousthromboembolism in
gynaecologicalsurgery
Identify the level of risk in preoperativepatientsExplain the
pros and cons of various
prophylactic methodsBased on best evidence, use theappropriate
method/s of VTE prophylaxis inclinical practice