Embed Size (px)
Citation preview
894 Intensive care medicine15 894 Intensive care medicine15in bicarbonate concentration. If hypocarbia persists, somedegree of renal compensation may occur, producing ametabolic acidosis, although in practice this is unusual. Arespiratoryalkalosisisoftenproduced,intentionallyorunin-tentionally, when patients are mechanically ventilated; itmayalsobeseenwithhypoxaemic(typeI)respiratoryfailure(see Ch. 14), spontaneous hyperventilation and in thoselivingathighaltitudes.
Metabolic acidosis (p. 675). Thismaybedue toexcessiveacidproduction,mostcommonly lactateandH+ (lacticaci-dosis)asaconsequenceofanaerobicmetabolismduringanepisode of shock or following cardiac arrest. A metabolicacidosismayalsodevelopinchronicrenalfailureor india-beticketoacidosis.Itcanalsofollowthelossofbicarbonatefromthegut,forexample,orfromthekidneyinrenaltubularacidosis.Respiratorycompensationforametabolicacidosisis usually slightly delayed because the blood–brain barrierinitially prevents the respiratory centre from sensing theincreased blood [H+]. Following this short delay, however,thepatienthyperventilatesand‘blowsoff’carbondioxidetoproduce a compensatory respiratory alkalosis. There is alimit to this respiratory compensation, since in practicevalues for Paco2 less than about 1.4kPa (11mmHg) arerarely achieved. Spontaneous respiratory compensationcannotoccurifthepatient’sventilationiscontrolledoriftherespiratory centre is depressed, for example by drugs orhead injury.
Metabolic alkalosis. Thiscanbecausedbylossofacid,forexample from the stomach with nasogastric suction, or inhigh intestinal obstruction, or excessive administration ofabsorbable alkali. Overzealous treatment with intravenoussodium bicarbonate is sometimes implicated. Respiratorycompensationforametabolicalkalosisisoftenslight,anditisraretoencounteraPaco2above6.5kPa(50mmHg),evenwithseverealkalosis.
SHOCK AND ACUTE DISTURBANCES OF HAEMODYNAMIC FUNCTION
Shockisthetermusedtodescribeacutecirculatoryfailurewith inadequateor inappropriatelydistributed tissueperfu-sionresultingingeneralizedcellularhypoxiaand/oraninabil-ityofthecellstoutilizeoxygen.
Causes of shockAbnormalitiesoftissueperfusionmayresultfrom:
■ failureofthehearttoactasaneffectivepump■ mechanicalimpedimentstoforwardflow■ lossofcirculatoryvolume■ abnormalitiesoftheperipheralcirculation.
ThecausesofshockareshowninTable15.3.Oftenshockcanresultfromacombinationofthesefactors(e.g.insepsis,distributiveshockisfrequentlycomplicatedbyhypovolaemiaandmyocardialdepression).
PATHOPHYSIOLOGY
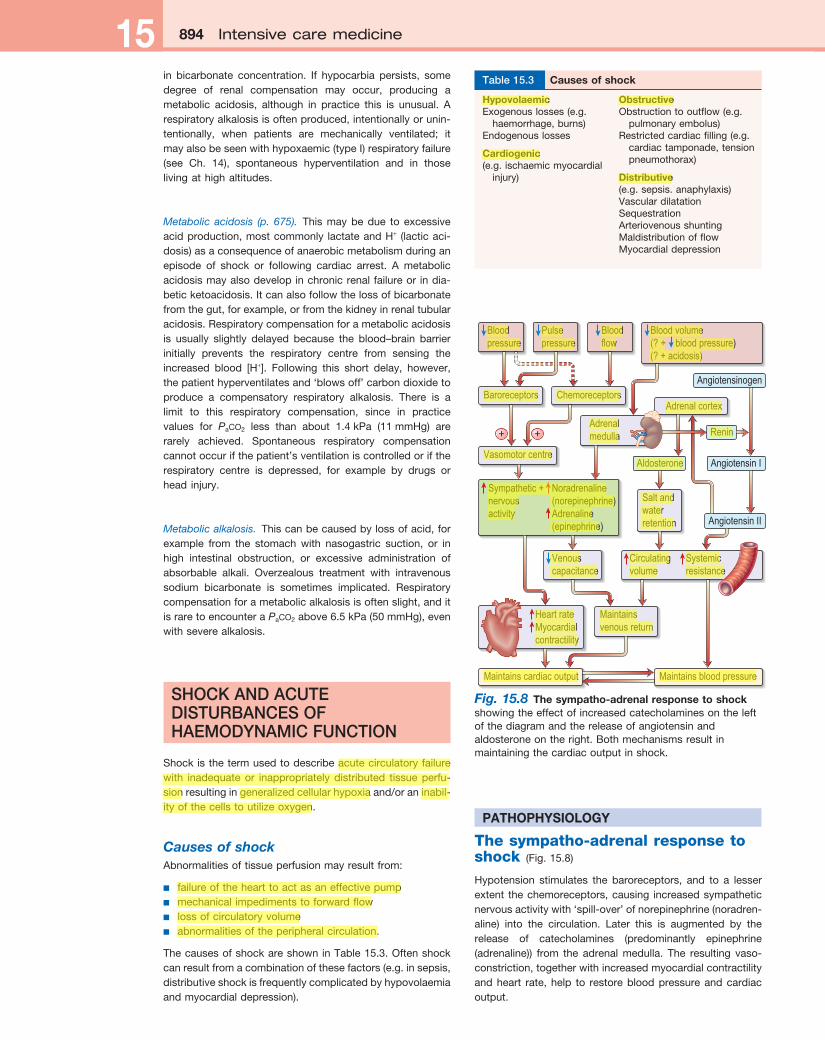
The sympatho-adrenal response to shock (Fig.15.8)
Hypotension stimulates the baroreceptors, and to a lesserextent thechemoreceptors,causing increasedsympatheticnervousactivitywith‘spill-over’ofnorepinephrine(noradren-aline) into the circulation. Later this is augmented by therelease of catecholamines (predominantly epinephrine(adrenaline)) from the adrenal medulla. The resulting vaso-constriction,togetherwithincreasedmyocardialcontractilityandheart rate,help to restorebloodpressureandcardiacoutput.
HypovolaemicExogenouslosses(e.g.
haemorrhage,burns)Endogenouslosses
Cardiogenic(e.g.ischaemicmyocardial
injury)
ObstructiveObstructiontooutflow(e.g.
pulmonaryembolus)Restrictedcardiacfilling(e.g.
cardiactamponade,tensionpneumothorax)
Distributive(e.g.sepsis.anaphylaxis)VasculardilatationSequestrationArteriovenousshuntingMaldistributionofflowMyocardialdepression
Table 15.3 Causes of shock
Fig. 15.8 The sympatho-adrenal response to shockshowingtheeffectofincreasedcatecholaminesontheleftofthediagramandthereleaseofangiotensinandaldosteroneontheright.Bothmechanismsresultinmaintainingthecardiacoutputinshock.
Adrenalmedulla
Adrenal cortex
Angiotensinogen
Angiotensin I
Renin
Angiotensin II
Aldosterone
Circulatingvolume
Systemicresistance
Heart rateMyocardialcontractility
Bloodpressure
Maintainsvenous return
Vasomotor centre
Baroreceptors Chemoreceptors
Venouscapacitance
Salt andwaterretention
Pulsepressure
Bloodflow
Blood volume(? + blood pressure)(? + acidosis)
Maintains cardiac output Maintains blood pressure
Sympathetic + Noradrenalinenervous (norepinephrine)activity Adrenaline (epinephrine)
Shock and acute disturbances of haemodynamic function 895Shock and acute disturbances of haemodynamic function 895
Reductioninperfusionoftherenalcortexstimulatesthejuxtaglomerular apparatus to release renin. This convertsangiotensinogentoangiotensinI,whichinturnisconvertedin the lungsandbythevascularendotheliumtothepotentvasoconstrictorangiotensinII.AngiotensinIIalsostimulatessecretion of aldosterone by the adrenal cortex, causingsodiumandwater retention (p.1023).Thishelpstorestorethecirculatingvolume(seep.652).
Neuroendocrine response■ Thereisrelease of pituitary hormonessuchas
adrenocorticotrophichormone(ACTH),vasopressin(antidiuretichormone,ADH)andendogenousopioidpeptides.(Insepticshocktheremaybearelativedeficiencyofvasopressin.)
■ Thereisrelease of cortisol,whichcausesfluidretentionandantagonizesinsulin.
■ Thereisrelease of glucagon,whichraisesthebloodsugarlevel.
Although absolute adrenocortical insufficiency (due, forexample, to bilateral adrenal haemorrhage or necrosis) israre,thereisevidencethatpatientswithsepticshockhaveabluntedresponsetoexogenousACTH(so-called‘relative’or‘occult’adrenocorticalinsufficiency)andthatthismaybeassociated with an impaired pressor response to norepi-nephrine (noradrenaline) andaworseprognosis. Thediag-nosis,causesandclinical significanceof thisphenomenonremainunclear.
Release of pro- and anti-inflammatory mediators(seealsoCh.3)
Severe infection (oftenwithbacteraemiaorendotoxaemia),thepresenceoflargeareasofdamagedtissue(e.g.followingtraumaorextensivesurgery)orprolonged/repeatedepisodesof hypoperfusion can trigger an exaggerated inflammatoryresponsewithsystemicactivationofleucocytesandreleaseof a variety of potentially damaging ‘mediators’. Althoughbeneficialwhen targetedagainst localareasof infectionornecrotic tissue, dissemination of this ‘innate immune’responsecanproduceshockandwidespreadtissuedamage.Characteristicallytheinitialepisodeofoverwhelminginflam-mationisfollowedbyaperiodofimmunesuppression,whichinsomecasesmaybeprofoundandduringwhichthepatientisatincreasedriskofdevelopingsecondaryinfections.Italsoseemsthatpro-andanti-inflammatoryelementsofthehostresponsemaycoexist.
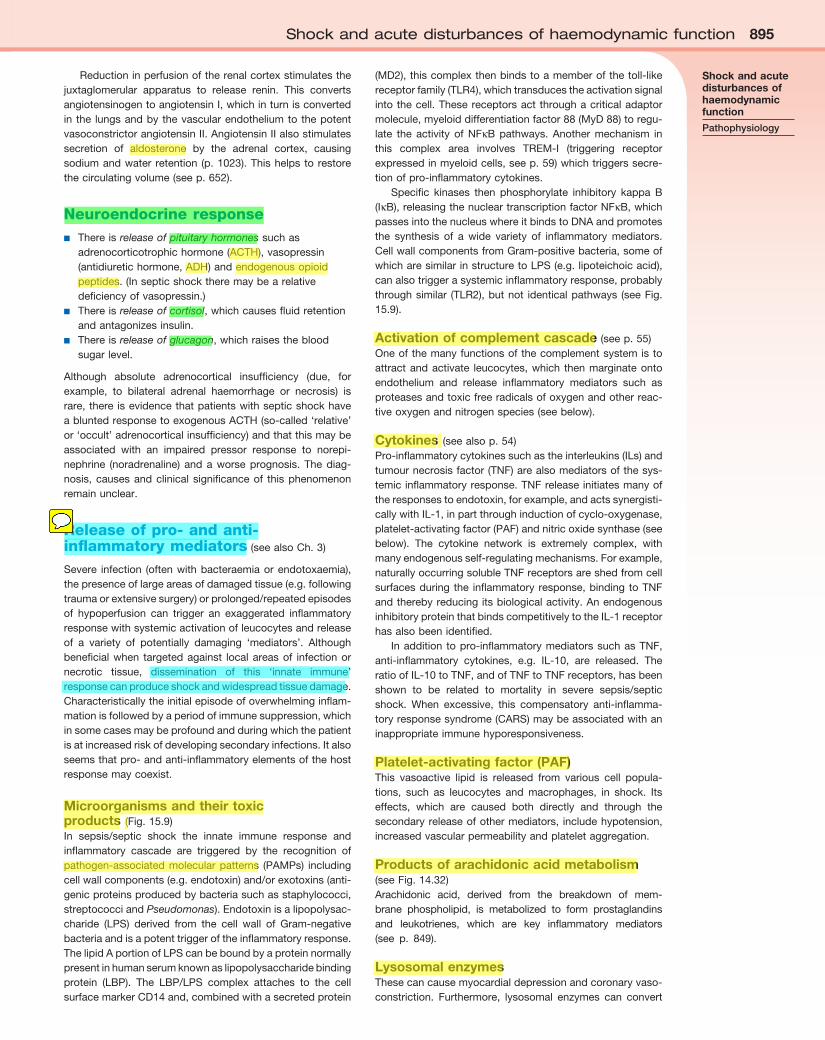
Microorganisms and their toxic products (Fig.15.9)In sepsis/septic shock the innate immune response andinflammatory cascade are triggered by the recognition ofpathogen-associatedmolecularpatterns (PAMPs) includingcellwallcomponents(e.g.endotoxin)and/orexotoxins(anti-genicproteinsproducedbybacteriasuchasstaphylococci,streptococciandPseudomonas).Endotoxinisalipopolysac-charide (LPS) derived from the cell wall of Gram-negativebacteriaandisapotenttriggeroftheinflammatoryresponse.ThelipidAportionofLPScanbeboundbyaproteinnormallypresentinhumanserumknownaslipopolysaccharidebindingprotein (LBP). The LBP/LPS complex attaches to the cellsurfacemarkerCD14and,combinedwithasecretedprotein
(MD2),thiscomplexthenbindstoamemberofthetoll-likereceptorfamily(TLR4),whichtransducestheactivationsignalintothecell.Thesereceptorsactthroughacriticaladaptormolecule,myeloiddifferentiationfactor88(MyD88)toregu-late the activity of NFκB pathways. Another mechanism inthis complex area involves TREM-I (triggering receptorexpressedinmyeloidcells,seep.59)whichtriggerssecre-tionofpro-inflammatorycytokines.
Specific kinases then phosphorylate inhibitory kappa B(IκB),releasingthenucleartranscriptionfactorNFκB,whichpassesintothenucleuswhereitbindstoDNAandpromotesthe synthesis of a wide variety of inflammatory mediators.CellwallcomponentsfromGram-positivebacteria,someofwhicharesimilarinstructuretoLPS(e.g.lipoteichoicacid),canalsotriggerasystemicinflammatoryresponse,probablythroughsimilar (TLR2),butnot identicalpathways (seeFig.15.9).
Activation of complement cascade(seep.55)Oneofthemanyfunctionsofthecomplementsystemistoattractandactivate leucocytes,which thenmarginateontoendothelium and release inflammatory mediators such asproteasesandtoxicfreeradicalsofoxygenandotherreac-tiveoxygenandnitrogenspecies(seebelow).
Cytokines (seealsop.54)Pro-inflammatorycytokinessuchastheinterleukins(ILs)andtumournecrosisfactor(TNF)arealsomediatorsofthesys-temicinflammatoryresponse.TNFreleaseinitiatesmanyoftheresponsestoendotoxin,forexample,andactssynergisti-callywithIL-1,inpartthroughinductionofcyclo-oxygenase,platelet-activatingfactor(PAF)andnitricoxidesynthase(seebelow). The cytokine network is extremely complex, withmanyendogenousself-regulatingmechanisms.Forexample,naturallyoccurringsolubleTNFreceptorsareshedfromcellsurfacesduringthe inflammatoryresponse,bindingtoTNFandtherebyreducingitsbiologicalactivity.AnendogenousinhibitoryproteinthatbindscompetitivelytotheIL-1receptorhasalsobeenidentified.
Inaddition topro-inflammatorymediatorssuchasTNF,anti-inflammatory cytokines, e.g. IL-10, are released. TheratioofIL-10toTNF,andofTNFtoTNFreceptors,hasbeenshown to be related to mortality in severe sepsis/septicshock. When excessive, this compensatory anti-inflamma-toryresponsesyndrome(CARS)maybeassociatedwithaninappropriateimmunehyporesponsiveness.
Platelet-activating factor (PAF)This vasoactive lipid is released from various cell popula-tions, such as leucocytes and macrophages, in shock. Itseffects, which are caused both directly and through thesecondaryreleaseofothermediators, includehypotension,increasedvascularpermeabilityandplateletaggregation.
Products of arachidonic acid metabolism (seeFig.14.32)Arachidonic acid, derived from the breakdown of mem-brane phospholipid, is metabolized to form prostaglandinsand leukotrienes, which are key inflammatory mediators(see p. 849).
Lysosomal enzymesThesecancausemyocardialdepressionandcoronaryvaso-constriction. Furthermore, lysosomal enzymes can convert
Shock and acute disturbances of haemodynamic function
Pathophysiology
896 Intensive care medicine15 896 Intensive care medicine15
inactivekininogenstovasoactivekininssuchasbradykinins.Thesesubstancescausevasodilatationandincreasedcapil-larypermeability,aswellasmyocardialdepression.Theycanalsoactivateclottingmechanisms.
Adhesion molecules (seealsop.25)Adhesionofactivatedleucocytestothevesselwallandtheirsubsequentextravascularmigration isakeycomponentofthesequenceofevents leading toendothelial injury, tissuedamage and organ dysfunction. This process is mediatedbyinducibleintercellularadhesionmolecules(ICAMs)foundon thesurfaceof leucocytesandendothelialcells.Expres-sionof thesemoleculescanbe inducedbyendotoxinandpro-inflammatory cytokines such as IL-1 and TNF. Severalfamiliesofmoleculesare involved inpromoting leucocyte–endothelialinteraction.Theselectinsare‘capture’moleculesandinitiatetheprocessofleucocyterollingonvascularendo-thelium,whilstmembersoftheimmunoglobulinsuperfamily(ICAM-1andvascularcelladhesionmolecule-1)areinvolvedintheformationofamoresecurebondwhichleadstoleu-cocytemigrationintothetissues(seeFig.3.13).
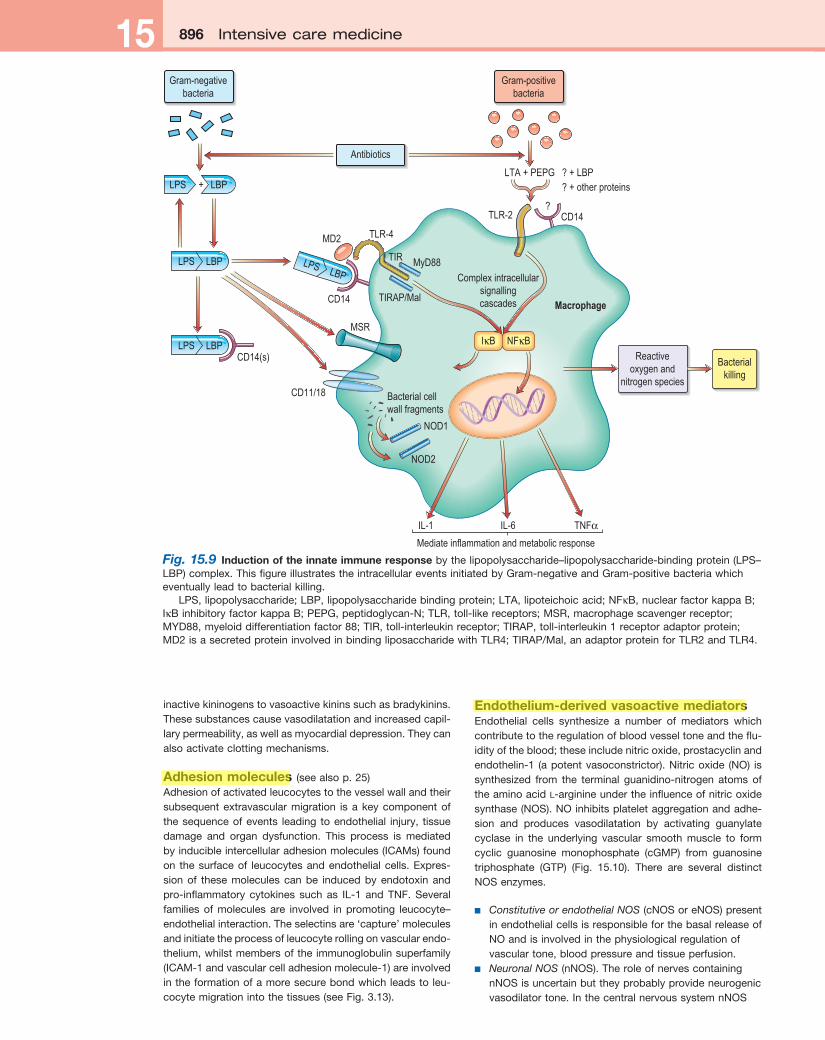
Endothelium-derived vasoactive mediatorsEndothelial cells synthesize a number of mediators whichcontributetotheregulationofbloodvesseltoneandtheflu-idityoftheblood;theseincludenitricoxide,prostacyclinandendothelin-1 (apotentvasoconstrictor).Nitricoxide (NO) issynthesized from the terminal guanidino-nitrogen atoms oftheaminoacidl-arginineundertheinfluenceofnitricoxidesynthase(NOS).NOinhibitsplateletaggregationandadhe-sion and produces vasodilatation by activating guanylatecyclase in the underlying vascular smooth muscle to formcyclic guanosine monophosphate (cGMP) from guanosinetriphosphate (GTP) (Fig. 15.10). There are several distinctNOSenzymes.
■ Constitutive or endothelial NOS(cNOSoreNOS)presentinendothelialcellsisresponsibleforthebasalreleaseofNOandisinvolvedinthephysiologicalregulationofvasculartone,bloodpressureandtissueperfusion.
■ Neuronal NOS(nNOS).TheroleofnervescontainingnNOSisuncertainbuttheyprobablyprovideneurogenicvasodilatortone.InthecentralnervoussystemnNOS
Fig. 15.9 Induction of the innate immune responsebythelipopolysaccharide–lipopolysaccharide-bindingprotein(LPS–LBP)complex.ThisfigureillustratestheintracellulareventsinitiatedbyGram-negativeandGram-positivebacteriawhicheventuallyleadtobacterialkilling.
LPS,lipopolysaccharide;LBP,lipopolysaccharidebindingprotein;LTA,lipoteichoicacid;NFκB,nuclearfactorkappaB;IκBinhibitoryfactorkappaB;PEPG,peptidoglycan-N;TLR,toll-likereceptors;MSR,macrophagescavengerreceptor;MYD88,myeloiddifferentiationfactor88;TIR,toll-interleukinreceptor;TIRAP,toll-interleukin1receptoradaptorprotein;MD2isasecretedproteininvolvedinbindingliposaccharidewithTLR4;TIRAP/Mal,anadaptorproteinforTLR2andTLR4.
?
Gram-negativebacteria
Gram-positivebacteria
LPS
IL-1 IL-6 TNFα
+ LBP
LPS LBP
LPS LBP
LPS LBP
MSR
CD14
TLR-2
TIR
TLR-4
Macrophage
MyD88
Complex intracellularsignallingcascadesTIRAP/Mal
IκB NFκB
CD14
CD14(s)
CD11/18 Bacterial cellwall fragments
NOD1
NOD2
Reactiveoxygen and
nitrogen species
Mediate inflammation and metabolic response
Antibiotics
LTA + PEPG ? + LBP? + other proteins
Bacterialkilling
MD2
Shock and acute disturbances of haemodynamic function 897Shock and acute disturbances of haemodynamic function 897
maybearegulatoroflocalcerebralbloodflowaswellasfulfillinganumberofotherphysiologicalfunctions,suchastheacutemodulationofneuronalfiringbehaviour.
■ Inducible NOS(iNOS)isinducedinvascularendothelialsmoothmusclecellsandmonocyteswithin4–18hoursofstimulationwithcertaincytokines,suchasTNF,andendotoxin.TheresultingprolongedincreaseinNOformationisbelievedtobeacauseofthesustainedvasodilatation,hypotensionandreducedreactivitytoadrenergicagonists(‘vasoplegia’)thatcharacterizessepticshock.Thismechanismmayalsobeinvolvedinsevereprolongedhaemorrhage/traumaticshock.TheNOgeneratedbymacrophagescontributestotheirroleashighlyeffectivekillersofintracellularandextracellularpathogens,inpartasaconsequenceofitsabilitytobindtocytochromeoxidaseandinhibitelectrontransport,butalsoviatheproductionofthehighlyreactiveradicalperoxynitrite.
Redox imbalanceInhealththebalancebetweenreducingandoxidizingcondi-tions (redox) iscontrolledbyantioxidantswhichmayeitherprevent radical formation (e.g. transferrin and lactoferrinwhichbindiron,acatalystforradicalformation)orremove/inactivatereactiveoxygenandnitrogenspecies(e.g.enzymessuchassuperoxidedismutases,vitaminsCandE,andsul-phydryl group donors such as glutathione). There are alsomechanismstoremoveandrepairoxidativelydamagedmol-eculesandinparticulartopreserveDNAintegrity.Inseveresystemic inflammation the uncontrolled production ofoxygen-derivedfreeradicalsandreactivenitrogenspecies,e.g. superoxide (O2•−), hydroxyl radicals (OH•), hydrogenperoxide (H2O2) and peroxynitrite (ONOO−), particularly byactivated polymorphonuclear leucocytes, can overwhelmthesedefensivemechanismsandcause:
■ lipidandproteinperoxidation■ damagetocellmembranes■ increasedcapillarypermeability■ impairedmitochondrialrespiration■ DNAstrandbreakage■ apoptosis,whichmaycontributetotheorgandamage
andimmunehypo-responsivenessassociatedwithsepsis.
Influence of genetic variationIndividualsvaryconsiderably in theirsusceptibility to infec-tion,aswellastheirabilitytorecoverfromapparentlysimilarinfections,illnessesortraumaticinsults.Evidencenowindi-cates that interindividual variations in susceptibility to, andoutcome from,sepsiscanbepartlyexplainedbypolymor-phismsofthegenesencodingproteinsinvolvedinmediatingand controlling innate immunity and the inflammatoryresponse.
Haemodynamic and microcirculatory changesThe dominant haemodynamic feature of septic shock isperipheralvascularfailurewith:
■ vasodilatation■ maldistributionofregionalbloodflow■ abnormalitiesinthemicrocirculation:
– ‘stop-flow’capillaries(flowisintermittent)– ‘no-flow’capillaries(capillariesareobstructed)– failureofcapillaryrecruitment– increasedcapillarypermeabilitywithinterstitial
oedema.
Although these vascular and microvascular abnormalitiesmaypartlyaccountforthereducedoxygenextractionoftenseeninsepticshock,thereisalsoaprimary defect of cellular oxygen utilization owing to mitochondrial dysfunction (seeabove). Initially, before hypovolaemia supervenes, or whentherapeuticreplacementofcirculatingvolumehasbeeninad-equate,cardiac output is usually high and peripheral resis-tance is low.Thesechangesmaybeassociatedwithimpairedoxygen consumption, a reduced arteriovenous oxygencontentdifference,an increased Svo2anda lacticacidosis(so-called ‘tissue dysoxia’). Vasodilatation and increasedpermeabilityalsooccurinanaphylacticshock.
In the initialstagesofother formsofshock,andsome-timeswhenhypovolaemiaandmyocardialdepressionsuper-vene in sepsis and anaphylaxis, cardiac output is low andincreased sympathetic activity causes constriction of bothprecapillaryarteriolesand,toalesserextent,thepostcapil-laryvenules.Thishelpstomaintainthesystemicbloodpres-sure. In addition, the hydrostatic pressure within thecapillariesfallsandfluidismobilizedfromtheextravascularspaceintotheintravascularcompartment.
Activation of the coagulation systemTheinflammatoryresponsetoshock,tissueinjuryandinfec-tionisfrequentlyassociatedwithsystemicactivationoftheclottingcascade,leadingtoplateletaggregation,widespreadmicrovascularthrombosisandinadequatetissueperfusion.
Initially theproductionofPGI2bythecapillaryendothe-lium is impaired.Celldamage (forexample to thevascularendothelium) leads to exposure to tissue factor (p. 431),which triggerscoagulation. In severecases thesechangesarecompoundedbyelevatedlevelsofplasminogenactiva-tioninhibitortype1whichimpairsfibrinolysis,aswellasbydeficiencies in physiological inhibitors of coagulation(including antithrombin, proteins C and S and tissuefactor-pathwayinhibitor).AntithrombinandproteinChaveanumberofanti-inflammatoryproperties,whereasthrombinispro-inflammatory.
Fig. 15.10 Synthesis and biochemical action of nitric oxide.cGMP,cyclicguanosinemonophosphate;GTP,guanosinetriphosphate.
Generator cell
Target cell
cGMPGTP
L-Arginine
Nitric oxide
Guanylatecyclase
L-Citrulline
O2
NO synthase
NO
898 Intensive care medicine15 898 Intensive care medicine15Plasminogenisconvertedtoplasmin,whichbreaksdown
thrombus, liberating fibrin/fibrinogen degradation products(FDPs). Circulating levels of FDPs are therefore increased,the thrombin time,PTTandPTareprolongedandplateletand fibrinogen levels fall. Activation of the coagulationcascade can be confirmed by demonstrating increasedplasmalevelsofD-dimers.Thedevelopmentofdisseminated intravascular coagulation (DIC) often heralds the onset ofmultipleorganfailure.BecauseclottingfactorsandplateletsareconsumedinDIC,theyareunavailableforhaemostasiselsewhereandacoagulationdefectresults–hencethealter-nativenameforDICis‘consumption coagulopathy’.Insomecasesamicroangiopathichaemolyticanaemiadevelops.DICisparticularlyassociatedwithsepticshock,especiallywhenduetomeningococcalinfection(seep.124).Managementofthe underlying cause is most urgent. Supportive treatmentmay include infusionsof fresh frozenplasma,plateletsandoccasionallyfactorVIIIconcentrates.
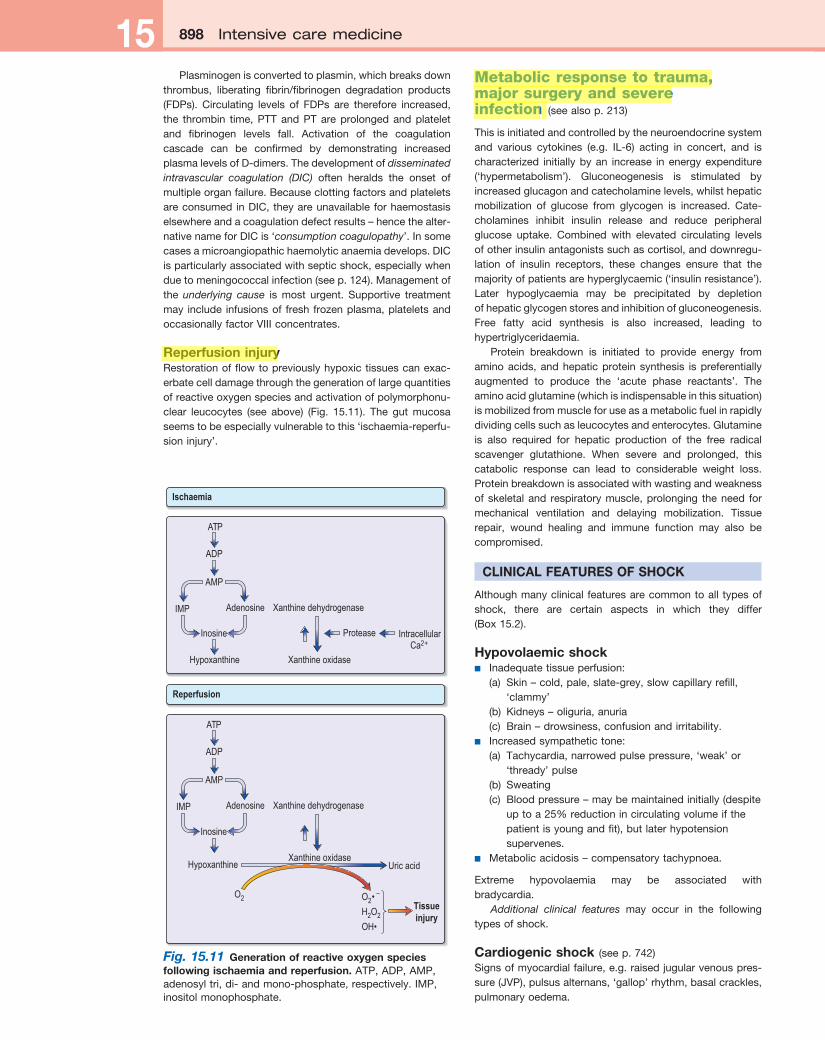
Reperfusion injuryRestorationofflowtopreviouslyhypoxictissuescanexac-erbatecelldamagethroughthegenerationoflargequantitiesofreactiveoxygenspeciesandactivationofpolymorphonu-clear leucocytes (see above) (Fig. 15.11). The gut mucosaseemstobeespeciallyvulnerabletothis‘ischaemia-reperfu-sioninjury’.
Metabolic response to trauma, major surgery and severe infection (seealsop.213)
Thisisinitiatedandcontrolledbytheneuroendocrinesystemand various cytokines (e.g. IL-6) acting in concert, and ischaracterized initiallybyan increase inenergyexpenditure(‘hypermetabolism’). Gluconeogenesis is stimulated byincreasedglucagonandcatecholaminelevels,whilsthepaticmobilization of glucose from glycogen is increased. Cate-cholamines inhibit insulin release and reduce peripheralglucose uptake. Combined with elevated circulating levelsofotherinsulinantagonistssuchascortisol,anddownregu-lation of insulin receptors, these changes ensure that themajorityofpatientsarehyperglycaemic(‘insulinresistance’).Later hypoglycaemia may be precipitated by depletionofhepaticglycogenstoresandinhibitionofgluconeogenesis.Free fatty acid synthesis is also increased, leading tohypertriglyceridaemia.
Protein breakdown is initiated to provide energy fromaminoacids,andhepaticproteinsynthesis ispreferentiallyaugmented to produce the ‘acute phase reactants’. Theaminoacidglutamine(whichisindispensableinthissituation)ismobilizedfrommuscleforuseasametabolicfuelinrapidlydividingcellssuchasleucocytesandenterocytes.Glutamineis also required for hepatic production of the free radicalscavenger glutathione. When severe and prolonged, thiscatabolic response can lead to considerable weight loss.Proteinbreakdownisassociatedwithwastingandweaknessofskeletaland respiratorymuscle,prolonging theneed formechanical ventilation and delaying mobilization. Tissuerepair, wound healing and immune function may also becompromised.
CLINICAL FEATURES OF SHOCK
Althoughmanyclinical featuresarecommontoall typesofshock, there are certain aspects in which they differ(Box15.2).
Hypovolaemic shock■ Inadequatetissueperfusion:
(a) Skin–cold,pale,slate-grey,slowcapillaryrefill,‘clammy’
(b) Kidneys–oliguria,anuria(c) Brain–drowsiness,confusionandirritability.
■ Increasedsympathetictone:(a) Tachycardia,narrowedpulsepressure,‘weak’or
‘thready’pulse(b) Sweating(c) Bloodpressure–maybemaintainedinitially(despite
uptoa25%reductionincirculatingvolumeifthepatientisyoungandfit),butlaterhypotensionsupervenes.
■ Metabolicacidosis–compensatorytachypnoea.
Extreme hypovolaemia may be associated withbradycardia.
Additional clinical features may occur in the followingtypesofshock.
Cardiogenic shock (seep.742)Signsofmyocardialfailure,e.g.raisedjugularvenouspres-sure(JVP),pulsusalternans,‘gallop’rhythm,basalcrackles,pulmonaryoedema.
Fig. 15.11 Generation of reactive oxygen species following ischaemia and reperfusion.ATP,ADP,AMP,adenosyltri,di-andmono-phosphate,respectively.IMP,inositolmonophosphate.
Ischaemia
ATP
ADP
AMP
Adenosine
Inosine
Hypoxanthine
Xanthine dehydrogenase
Xanthine oxidase
Protease IntracellularCa2+
Reperfusion
ATP
ADP
AMP
IMP
IMP
Adenosine
Inosine
Hypoxanthine
Xanthine dehydrogenase
Xanthine oxidaseUric acid
O2 O2• –
H2O2
OH•
Tissueinjury
Shock and acute disturbances of haemodynamic function 899Shock and acute disturbances of haemodynamic function 899
Obstructive shock■ ElevatedJVP.■ Pulsusparadoxusandmuffledheartsoundsincardiac
tamponade.■ Signsofpulmonaryembolism(seep.784).
Anaphylactic shock (seep.73)■ Signsofprofoundvasodilatation:
(a) Warmperipheries(b) Lowbloodpressure(c) Tachycardia.
■ Erythema,urticaria,angio-oedema,pallor,cyanosis.■ Bronchospasm,rhinitis.■ Oedemaoftheface,pharynxandlarynx.■ Pulmonaryoedema.■ Hypovolaemiaduetocapillaryleak.■ Nausea,vomiting,abdominalcramps,diarrhoea.
Sepsis, severe sepsis and septic shock■ Pyrexiaandrigors,orhypothermia(unusual).■ Nausea,vomiting.■ Vasodilatation,warmperipheries.■ Boundingpulse.■ Rapidcapillaryrefill.■ Hypotension(septicshock).■ Occasionallysignsofcutaneousvasoconstriction.■ Othersigns:
(a) Jaundice(b) Coma,stupor(c) Bleedingduetocoagulopathy(e.g.fromvascular
puncturesites,GItractandsurgicalwounds)(d) Rashandmeningism(c) Hyper-,andinmoreseverecaseshypoglycaemia.
Thediagnosisofsepsis iseasilymissed,particularly in theelderly when the classical signs may not be present. Mildconfusion, tachycardia and tachypnoea may be the onlyclues,sometimesassociatedwithunexplainedhypotension,a reduction in urine output, a rising plasma creatinine andglucoseintolerance.
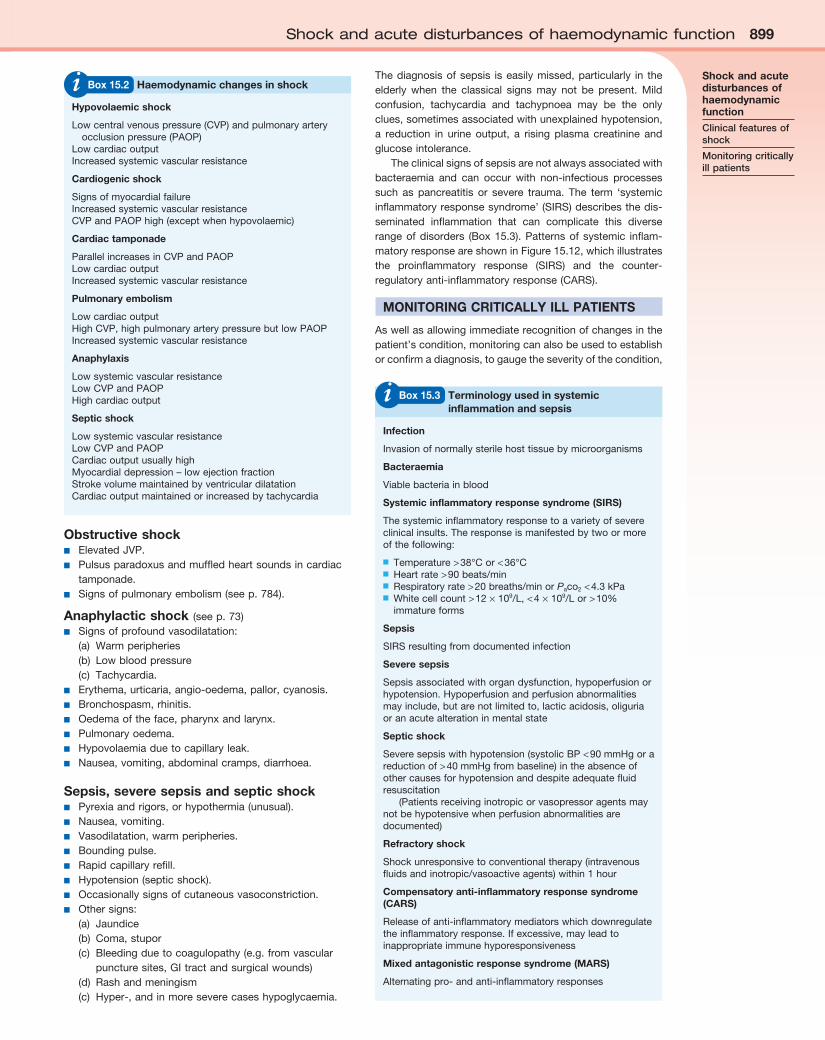
Theclinicalsignsofsepsisarenotalwaysassociatedwithbacteraemia and can occur with non-infectious processessuch as pancreatitis or severe trauma. The term ‘systemicinflammatoryresponsesyndrome’(SIRS)describesthedis-seminated inflammation that can complicate this diverserangeofdisorders (Box15.3).Patternsof systemic inflam-matoryresponseareshowninFigure15.12,whichillustratesthe proinflammatory response (SIRS) and the counter-regulatoryanti-inflammatoryresponse(CARS).
MONITORING CRITICALLY ILL PATIENTS
Aswellasallowingimmediaterecognitionofchangesinthepatient’scondition,monitoringcanalsobeusedtoestablishorconfirmadiagnosis,togaugetheseverityofthecondition,
Hypovolaemic shock
Lowcentralvenouspressure(CVP)andpulmonaryarteryocclusionpressure(PAOP)
LowcardiacoutputIncreasedsystemicvascularresistance
Cardiogenic shock
SignsofmyocardialfailureIncreasedsystemicvascularresistanceCVPandPAOPhigh(exceptwhenhypovolaemic)
Cardiac tamponade
ParallelincreasesinCVPandPAOPLowcardiacoutputIncreasedsystemicvascularresistance
Pulmonary embolism
LowcardiacoutputHighCVP,highpulmonaryarterypressurebutlowPAOPIncreasedsystemicvascularresistance
Anaphylaxis
LowsystemicvascularresistanceLowCVPandPAOPHighcardiacoutput
Septic shock
LowsystemicvascularresistanceLowCVPandPAOPCardiacoutputusuallyhighMyocardialdepression–lowejectionfractionStrokevolumemaintainedbyventriculardilatationCardiacoutputmaintainedorincreasedbytachycardia
i Box 15.2 Haemodynamic changes in shock
Infection
Invasionofnormallysterilehosttissuebymicroorganisms
Bacteraemia
Viablebacteriainblood
Systemic inflammatory response syndrome (SIRS)
Thesystemicinflammatoryresponsetoavarietyofsevereclinicalinsults.Theresponseismanifestedbytwoormoreofthefollowing:
■ Temperature>38°Cor<36°C■ Heartrate>90beats/min■ Respiratoryrate>20breaths/minorPaco2<4.3kPa■ Whitecellcount>12×109/L,<4×109/Lor>10%
immatureforms
Sepsis
SIRSresultingfromdocumentedinfection
Severe sepsis
Sepsisassociatedwithorgandysfunction,hypoperfusionorhypotension.Hypoperfusionandperfusionabnormalitiesmayinclude,butarenotlimitedto,lacticacidosis,oliguriaoranacutealterationinmentalstate
Septic shock
Severesepsiswithhypotension(systolicBP<90mmHgorareductionof>40mmHgfrombaseline)intheabsenceofothercausesforhypotensionanddespiteadequatefluidresuscitation
(Patientsreceivinginotropicorvasopressoragentsmaynotbehypotensivewhenperfusionabnormalitiesaredocumented)
Refractory shock
Shockunresponsivetoconventionaltherapy(intravenousfluidsandinotropic/vasoactiveagents)within1hour
Compensatory anti-inflammatory response syndrome (CARS)
Releaseofanti-inflammatorymediatorswhichdownregulatetheinflammatoryresponse.Ifexcessive,mayleadtoinappropriateimmunehyporesponsiveness
Mixed antagonistic response syndrome (MARS)
Alternatingpro-andanti-inflammatoryresponses
i Box 15.3 Terminology used in systemic inflammation and sepsis
Shock and acute disturbances of haemodynamic function
Clinical features of shock
Monitoring critically ill patients

900 Intensive care medicine15 900 Intensive care medicine15
to follow theevolutionof the illness, toguide interventionsandtoassesstheresponsetotreatment.Invasivemonitoringisgenerallyindicatedinthemoreseriouslyillpatientsandinthose who fail to respond to initial treatment. These tech-niques are, however, associated with a significant risk ofcomplications, as well as additional costs and patient dis-comfortandshouldthereforeonlybeusedwhenthepoten-tialbenefitsoutweighthedangers.Likewise,invasivedevicesshouldberemovedassoonaspossible.
Assessment of tissue perfusion■ Pale, cold skin,delayedcapillaryrefillandtheabsenceof
visibleveinsinthehandsandfeetindicatepoorperfusion.Althoughperipheralskintemperaturemeasurementscanhelpclinicalevaluation,theearliestcompensatoryresponsetohypovolaemiaoralowcardiacoutput,andthelasttoresolveafterresuscitation,isvasoconstrictioninthesplanchnicregion.
■ Metabolic acidosis with raised lactate concentrationmaysuggestthattissueperfusionissufficientlycompromisedtocausecellularhypoxiaandanaerobicglycolysis.Persistent,severelacticacidosisisassociatedwithaverypoorprognosis.Inmanycriticallyillpatients,especiallythosewithsepsis,however,lacticacidosiscanalsobecausedbymetabolicdisordersunrelatedtotissuehypoxiaandmaybeexacerbatedbyreducedclearanceowingtohepaticorrenaldysfunction.
■ Urinary flowisasensitiveindicatorofrenalperfusionandhaemodynamicperformance.
Blood pressureAlterationsinbloodpressureareofteninterpretedasreflect-ingchangesincardiacoutput.However,ifthereisvasocon-strictionwithahighperipheralresistance,thebloodpressure
may be normal, even when the cardiac output is reduced.Conversely, the vasodilated patient may be hypotensivedespiteaveryhighcardiacoutput.
Hypotension may jeopardize perfusion of vital organs.Theadequacyofbloodpressureinanindividualpatientmustalwaysbeassessedinrelationtothepremorbidvalue.Bloodpressureistraditionallymeasuredusingasphygmomanom-eterbutifrapidalterationsareanticipated,continuousmoni-toring using an intra-arterial cannula is indicated (Practicalbox15.1,Fig.15.13).
Fig. 15.12 Pattern of systemic inflammatory response.CARS,compensatoryanti-inflammatoryresponsesyndrome;SIRS,systemicinflammatoryresponsesyndrome.FromHindsCJ,WatsonJD.Intensive Care: A Concise Textbook,3rdedn.Edinburgh:Saunders,2008,withpermissionfromElsevier.
SIRS CARS
Balanced response
Hyper-responsive
Hypo-responsive
Massiveinflammatoryresponse
Hypotension
Multipleorgan failure
Persistent orrecurrentinfection
Overwhelminginfection
Multipleorgan failure
SIRSCARS
SIRSCARS
Insult
ResolutionTechnique
1 Theprocedureisexplainedtothepatientand,ifpossible,consentobtained
2 Thearmissupported,withthewristextended,byanassistant.(Glovesshouldbeworn)
3 Theskinshouldbecleanedwithchlorhexidine4 Theradialarteryispalpatedwhereitarchesoverthehead
oftheradius5 Inconsciouspatients,localanaestheticisinjectedtoraisea
wealovertheartery,takingcarenottopuncturethevesselorobscureitspulsation
6 Asmallskinincisionismadeovertheproposedpuncturesite
7 Asmallparallel-sidedcannula(20gaugeforadults,22gaugeforchildren)isusedinordertoallowbloodflowtocontinuepastthecannula
8 Thecannulaisinsertedoverthepointofmaximalpulsationandadvancedinlinewiththedirectionofthevesselatanangleofapproximately30°
9 ‘Flashback’ofbloodintothecannulaindicatesthattheradialarteryhasbeenpunctured
10 Toensurethattheshoulderofthecannulaentersthevessel,theneedleandcannulaareloweredandadvancedafewmillimetresintothevessel
11 Thecannulaisthreadedofftheneedleintothevesselandtheneedlewithdrawn
12 Thecannulaisconnectedtoanon-compliantmanometerlinefilledwithsaline.Thisisthenconnectedviaatransducerandcontinuousflushdevicetoamonitor,whichrecordsthearterialpressure
Complications
■ Thrombosis■ Lossofarterialpulsation■ Distalischaemia,e.g.digitalnecrosis(rare)■ Infection■ Accidentalinjectionofdrugs–canproducevascular
occlusion■ Disconnection–rapidbloodloss
Practical Box 15.1 Radial artery cannulation✔
Fig. 15.13 Percutaneous cannulation of the radial artery.
Flashback ofblood whenradial arteryis punctured
Syringe
Radial artery
Cannula
Shock and acute disturbances of haemodynamic function 901Shock and acute disturbances of haemodynamic function 901
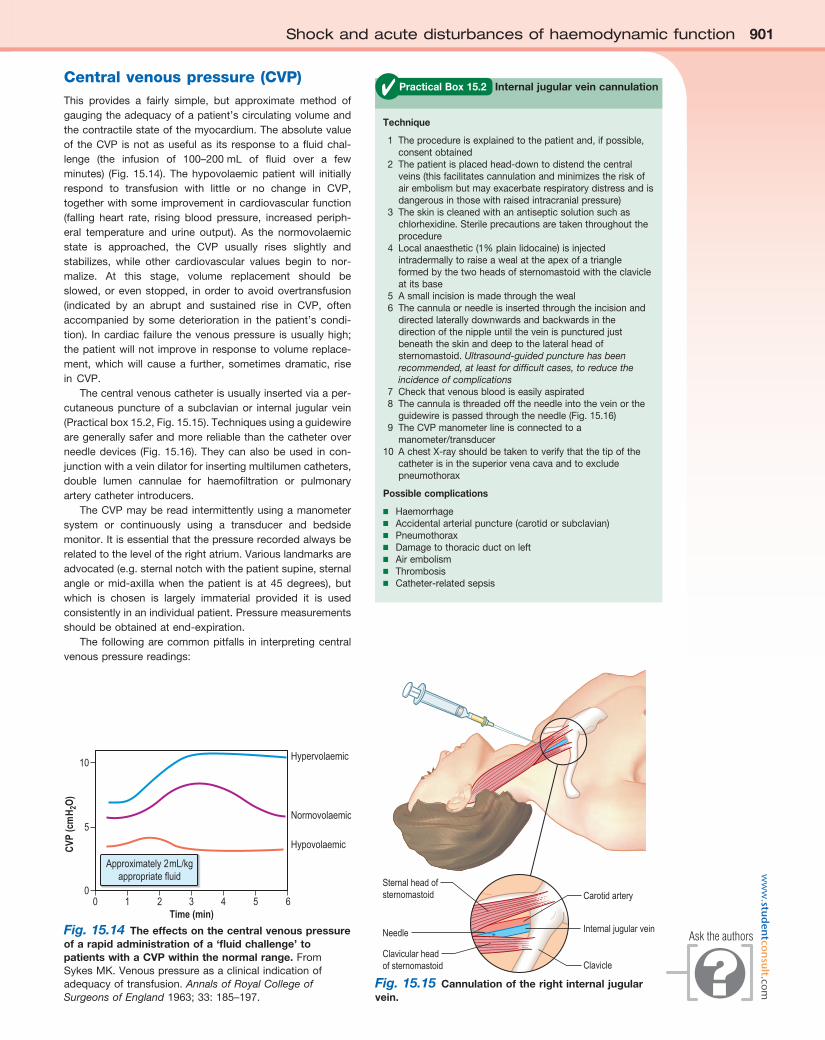
Fig. 15.14 The effects on the central venous pressure of a rapid administration of a ‘fluid challenge’ to patients with a CVP within the normal range.FromSykesMK.Venouspressureasaclinicalindicationofadequacyoftransfusion.Annals of Royal College of Surgeons of England1963;33:185–197.
5
00
Time (min)654321
Hypervolaemic
Normovolaemic
Hypovolaemic
10
CVP
(cm
H2O
)
Approximately 2mL/kgappropriate fluid
Technique
1 Theprocedureisexplainedtothepatientand,ifpossible,consentobtained
2 Thepatientisplacedhead-downtodistendthecentralveins(thisfacilitatescannulationandminimizestheriskofairembolismbutmayexacerbaterespiratorydistressandisdangerousinthosewithraisedintracranialpressure)
3 Theskiniscleanedwithanantisepticsolutionsuchaschlorhexidine.Sterileprecautionsaretakenthroughouttheprocedure
4 Localanaesthetic(1%plainlidocaine)isinjectedintradermallytoraiseawealattheapexofatriangleformedbythetwoheadsofsternomastoidwiththeclavicleatitsbase
5 Asmallincisionismadethroughtheweal6 Thecannulaorneedleisinsertedthroughtheincisionand
directedlaterallydownwardsandbackwardsinthedirectionofthenippleuntiltheveinispuncturedjustbeneaththeskinanddeeptothelateralheadofsternomastoid.Ultrasound-guided puncture has been recommended, at least for difficult cases, to reduce the incidence of complications
7 Checkthatvenousbloodiseasilyaspirated8 Thecannulaisthreadedofftheneedleintotheveinorthe
guidewireispassedthroughtheneedle(Fig.15.16)9 TheCVPmanometerlineisconnectedtoa
manometer/transducer10 AchestX-rayshouldbetakentoverifythatthetipofthe
catheterisinthesuperiorvenacavaandtoexcludepneumothorax
Possible complications
■ Haemorrhage■ Accidentalarterialpuncture(carotidorsubclavian)■ Pneumothorax■ Damagetothoracicductonleft■ Airembolism■ Thrombosis■ Catheter-relatedsepsis
Practical Box 15.2 Internal jugular vein cannulation✔Central venous pressure (CVP)This provides a fairly simple, but approximate method ofgaugingtheadequacyofapatient’scirculatingvolumeandthecontractilestateofthemyocardium.Theabsolutevalueof theCVP isnotasusefulas its response toafluidchal-lenge (the infusion of 100–200mL of fluid over a fewminutes) (Fig. 15.14). Thehypovolaemicpatientwill initiallyrespond to transfusion with little or no change in CVP,togetherwithsomeimprovementincardiovascularfunction(falling heart rate, rising blood pressure, increased periph-eral temperature and urine output). As the normovolaemicstate is approached, the CVP usually rises slightly andstabilizes, while other cardiovascular values begin to nor-malize. At this stage, volume replacement should beslowed,orevenstopped, inorder toavoidovertransfusion(indicated by an abrupt and sustained rise in CVP, oftenaccompaniedbysomedeterioration in thepatient’scondi-tion). Incardiac failure thevenouspressure isusuallyhigh;thepatientwillnot improveinresponsetovolumereplace-ment,whichwill causea further, sometimesdramatic, risein CVP.
Thecentralvenouscatheterisusuallyinsertedviaaper-cutaneouspunctureofasubclavianor internal jugularvein(Practicalbox15.2,Fig.15.15).Techniquesusingaguidewirearegenerallysaferandmorereliablethanthecatheteroverneedledevices (Fig.15.16).Theycanalsobeused incon-junctionwithaveindilatorforinsertingmultilumencatheters,double lumen cannulae for haemofiltration or pulmonaryarterycatheterintroducers.
TheCVPmayberead intermittentlyusingamanometersystem or continuously using a transducer and bedsidemonitor.Itisessentialthatthepressurerecordedalwaysberelatedtotheleveloftherightatrium.Variouslandmarksareadvocated(e.g.sternalnotchwiththepatientsupine,sternalangleormid-axillawhen thepatient is at 45degrees), butwhich is chosen is largely immaterial provided it is usedconsistentlyinanindividualpatient.Pressuremeasurementsshouldbeobtainedatend-expiration.
Thefollowingarecommonpitfalls in interpretingcentralvenouspressurereadings:
Fig. 15.15 Cannulation of the right internal jugular vein.
Sternal head ofsternomastoid
Needle
Clavicular headof sternomastoid
Carotid artery
Clavicle
Internal jugular veinAsk the authors
ww
w.stud
entco
nsult.com
902 Intensive care medicine15 902 Intensive care medicine15
Blocked catheter. This results in a sustained high reading,with a damped or absent waveform which often does notcorrelatewithclinicalassessment.
Transducer wrongly positioned. Failuretolevelthesystemisacommoncauseoferroneousreadings.
Catheter tip in right ventricle. Ifthecatheterisadvancedtoofar,anunexpectedlyhighpressurewithpronouncedoscilla-tionsisrecorded.Thisiseasilyrecognizedwhenthewave-formisdisplayed.
Arterial pressure variation as a guide to hypovolaemiaSystolic arterial pressure decreases during the inspiratoryphase of intermittent positive pressure ventilation (p. 912).Themagnitudeofthiscyclicalvariabilityhasbeenshowntocorrelatemorecloselywithhypovolaemia thanothermoni-tored variables, including CVP. Systolic pressure variationduring mechanical ventilation can therefore be used as asimpleandreliableguidetotheadequacyofthecirculatoryvolume.
Left atrial pressureIn uncomplicated cases, careful interpretation of the CVPprovidesareasonableguidetothefillingpressuresofbothsidesoftheheart.Inmanycriticallyillpatients,however,thisisnotthecaseandthere isadisparity infunctionbetweenthe two ventricles. Most commonly, left ventricular perfor-manceisworst,sothattheleftventricularfunctioncurveisdisplaceddownwardandtotheright(Fig.15.17).Highrightventricularfillingpressures,withnormalorlowleftatrialpres-sures,arelesscommonbutmayoccurwithrightventriculardysfunctionandinsituationswherethepulmonaryvascularresistance (i.e. rightventricularafterload) is raised,suchasinacuterespiratoryfailureandpulmonaryembolism.
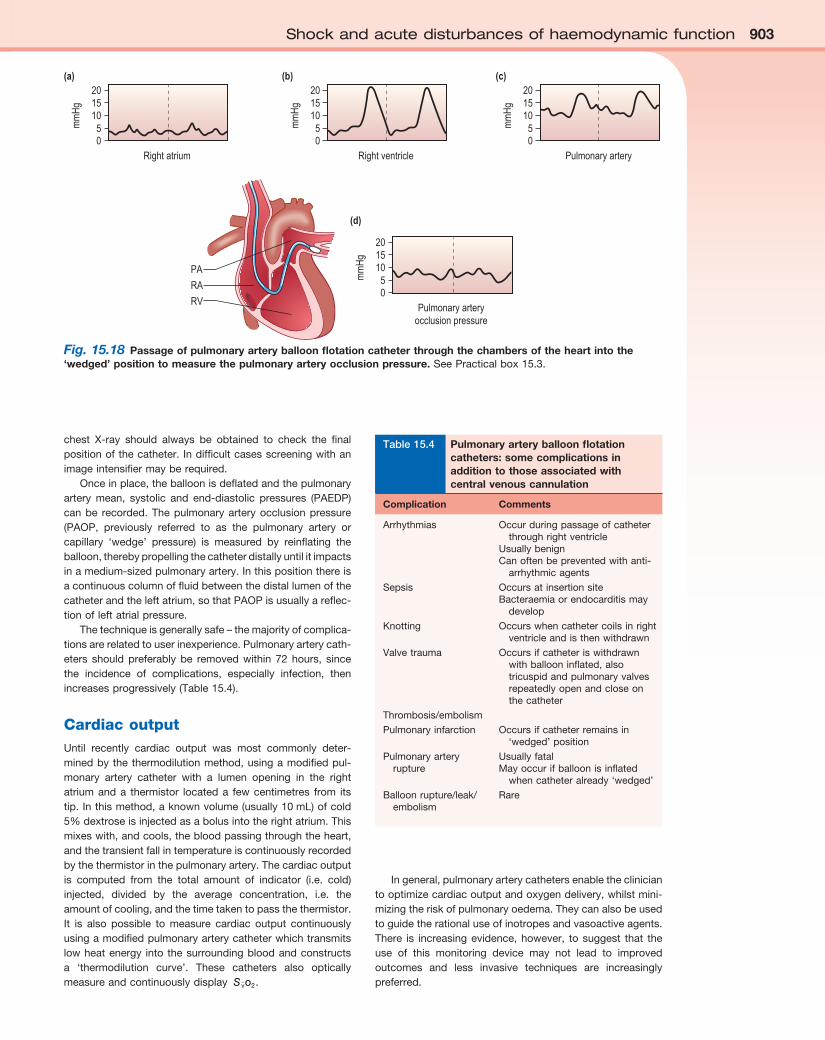
Pulmonary artery pressureA‘balloonflotationcatheter’enablesreliablecatheterizationof thepulmonaryartery.These ‘Swan–Ganz’catheterscanbeinsertedcentrally(seeFig.15.15)orthroughthefemoralvein,or viaavein in theantecubital fossa.Passageof thecatheterfromthemajorveins,throughthechambersoftheheart,intothepulmonaryarteryandintothewedgedpositionismonitoredandguidedbythepressurewaveformsrecordedfromthedistal lumen(Fig.15.18andPracticalbox15.3).A
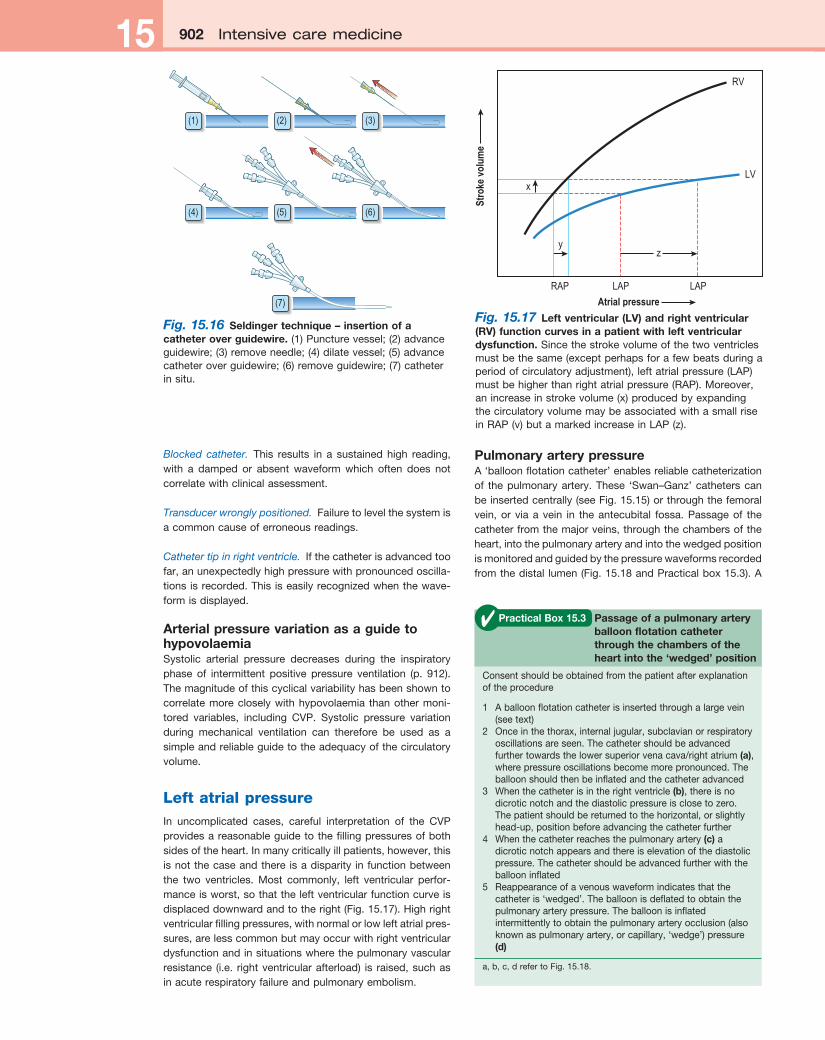
Fig. 15.16 Seldinger technique – insertion of a catheter over guidewire.(1)Puncturevessel;(2)advanceguidewire;(3)removeneedle;(4)dilatevessel;(5)advancecatheteroverguidewire;(6)removeguidewire;(7)catheterinsitu.
(1) (2) (3)
(4) (5)
(7)
(6)
Fig. 15.17 Left ventricular (LV) and right ventricular (RV) function curves in a patient with left ventricular dysfunction.Sincethestrokevolumeofthetwoventriclesmustbethesame(exceptperhapsforafewbeatsduringaperiodofcirculatoryadjustment),leftatrialpressure(LAP)mustbehigherthanrightatrialpressure(RAP).Moreover,anincreaseinstrokevolume(x)producedbyexpandingthecirculatoryvolumemaybeassociatedwithasmallriseinRAP(v)butamarkedincreaseinLAP(z).
RAP
x
yz
LAP
Atrial pressure
RV
LV
LAP
Stro
ke v
olum
e
Consentshouldbeobtainedfromthepatientafterexplanationoftheprocedure
1 Aballoonflotationcatheterisinsertedthroughalargevein(seetext)
2 Onceinthethorax,internaljugular,subclavianorrespiratoryoscillationsareseen.Thecathetershouldbeadvancedfurthertowardsthelowersuperiorvenacava/rightatrium(a),wherepressureoscillationsbecomemorepronounced.Theballoonshouldthenbeinflatedandthecatheteradvanced
3 Whenthecatheterisintherightventricle(b),thereisnodicroticnotchandthediastolicpressureisclosetozero.Thepatientshouldbereturnedtothehorizontal,orslightlyhead-up,positionbeforeadvancingthecatheterfurther
4 Whenthecatheterreachesthepulmonaryartery(c)adicroticnotchappearsandthereiselevationofthediastolicpressure.Thecathetershouldbeadvancedfurtherwiththeballooninflated
5 Reappearanceofavenouswaveformindicatesthatthecatheteris‘wedged’.Theballoonisdeflatedtoobtainthepulmonaryarterypressure.Theballoonisinflatedintermittentlytoobtainthepulmonaryarteryocclusion(alsoknownaspulmonaryartery,orcapillary,‘wedge’)pressure(d)
a,b,c,drefertoFig.15.18.
Practical Box 15.3 Passage of a pulmonary artery balloon flotation catheter through the chambers of the heart into the ‘wedged’ position
✔
Shock and acute disturbances of haemodynamic function 903Shock and acute disturbances of haemodynamic function 903
chest X-ray should always be obtained to check the finalpositionofthecatheter.Indifficultcasesscreeningwithanimageintensifiermayberequired.
Onceinplace,theballoonisdeflatedandthepulmonaryartery mean, systolic and end-diastolic pressures (PAEDP)canbe recorded.Thepulmonaryarteryocclusionpressure(PAOP, previously referred to as the pulmonary artery orcapillary ‘wedge’ pressure) is measured by reinflating theballoon,therebypropellingthecatheterdistallyuntilitimpactsinamedium-sizedpulmonaryartery.Inthispositionthereisacontinuouscolumnoffluidbetweenthedistallumenofthecatheterandtheleftatrium,sothatPAOPisusuallyareflec-tionofleftatrialpressure.
Thetechniqueisgenerallysafe–themajorityofcomplica-tionsarerelatedtouserinexperience.Pulmonaryarterycath-eters should preferably be removed within 72 hours, sincethe incidence of complications, especially infection, thenincreasesprogressively(Table15.4).
Cardiac outputUntil recently cardiac output was most commonly deter-minedbythethermodilutionmethod,usingamodifiedpul-monary artery catheter with a lumen opening in the rightatriumanda thermistor locateda fewcentimetres from itstip.Inthismethod,aknownvolume(usually10mL)ofcold5%dextroseisinjectedasabolusintotherightatrium.Thismixeswith,andcools,thebloodpassingthroughtheheart,andthetransientfallintemperatureiscontinuouslyrecordedbythethermistorinthepulmonaryartery.Thecardiacoutputis computed from the total amount of indicator (i.e. cold)injected, divided by the average concentration, i.e. theamountofcooling,andthetimetakentopassthethermistor.It is also possible to measure cardiac output continuouslyusingamodifiedpulmonaryarterycatheterwhichtransmitslowheatenergy into thesurroundingbloodandconstructsa ‘thermodilution curve’. These catheters also opticallymeasureandcontinuouslydisplay Svo2.
Ingeneral,pulmonaryarterycathetersenablethecliniciantooptimizecardiacoutputandoxygendelivery,whilstmini-mizingtheriskofpulmonaryoedema.Theycanalsobeusedtoguidetherationaluseofinotropesandvasoactiveagents.There is increasingevidence,however, tosuggest that theuse of this monitoring device may not lead to improvedoutcomes and less invasive techniques are increasinglypreferred.
Fig. 15.18 Passage of pulmonary artery balloon flotation catheter through the chambers of the heart into the ‘wedged’ position to measure the pulmonary artery occlusion pressure.SeePracticalbox15.3.
PA
RA
RV
20
Right atrium
mm
Hg 15
1050
20
Right ventricle
mm
Hg 15
1050
20
Pulmonary arteryocclusion pressure
mm
Hg 15
1050
20
Pulmonary artery
mm
Hg 15
1050
(a) (b) (c)
(d)
Complication Comments
Arrhythmias Occurduringpassageofcatheterthroughrightventricle
UsuallybenignCanoftenbepreventedwithanti-
arrhythmicagents
Sepsis OccursatinsertionsiteBacteraemiaorendocarditismay
develop
Knotting Occurswhencathetercoilsinrightventricleandisthenwithdrawn
Valvetrauma Occursifcatheteriswithdrawnwithballooninflated,alsotricuspidandpulmonaryvalvesrepeatedlyopenandcloseonthecatheter
Thrombosis/embolism
Pulmonaryinfarction Occursifcatheterremainsin‘wedged’position
Pulmonaryarteryrupture
UsuallyfatalMayoccurifballoonisinflated
whencatheteralready‘wedged’
Balloonrupture/leak/embolism
Rare
Table 15.4 Pulmonary artery balloon flotation catheters: some complications in addition to those associated with central venous cannulation
904 Intensive care medicine15 904 Intensive care medicine15Less invasive techniques for assessing cardiac function
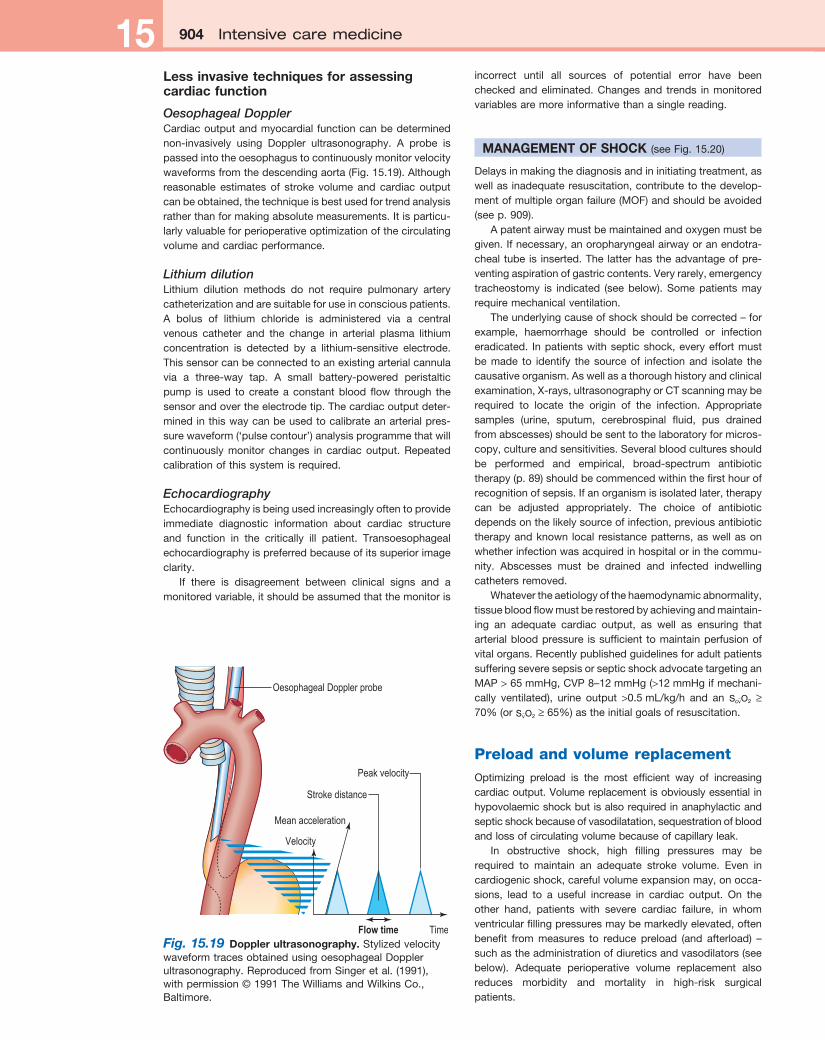
Oesophageal DopplerCardiacoutputandmyocardialfunctioncanbedeterminednon-invasively using Doppler ultrasonography. A probe ispassedintotheoesophagustocontinuouslymonitorvelocitywaveformsfromthedescendingaorta(Fig.15.19).Althoughreasonable estimates of stroke volume and cardiac outputcanbeobtained,thetechniqueisbestusedfortrendanalysisratherthanformakingabsolutemeasurements.Itisparticu-larlyvaluableforperioperativeoptimizationofthecirculatingvolumeandcardiacperformance.
Lithium dilutionLithium dilution methods do not require pulmonary arterycatheterizationandaresuitableforuseinconsciouspatients.A bolus of lithium chloride is administered via a centralvenous catheter and the change in arterial plasma lithiumconcentration is detected by a lithium-sensitive electrode.Thissensorcanbeconnectedtoanexistingarterialcannulavia a three-way tap. A small battery-powered peristalticpump isused tocreateaconstantbloodflow through thesensorandovertheelectrodetip.Thecardiacoutputdeter-minedinthiswaycanbeusedtocalibrateanarterialpres-surewaveform(‘pulsecontour’)analysisprogrammethatwillcontinuously monitor changes in cardiac output. Repeatedcalibrationofthissystemisrequired.
EchocardiographyEchocardiographyisbeingusedincreasinglyoftentoprovideimmediate diagnostic information about cardiac structureand function in the critically ill patient. Transoesophagealechocardiographyispreferredbecauseofitssuperiorimageclarity.
If there is disagreement between clinical signs and amonitoredvariable,itshouldbeassumedthatthemonitoris
incorrect until all sources of potential error have beencheckedandeliminated.Changesand trends inmonitoredvariablesaremoreinformativethanasinglereading.
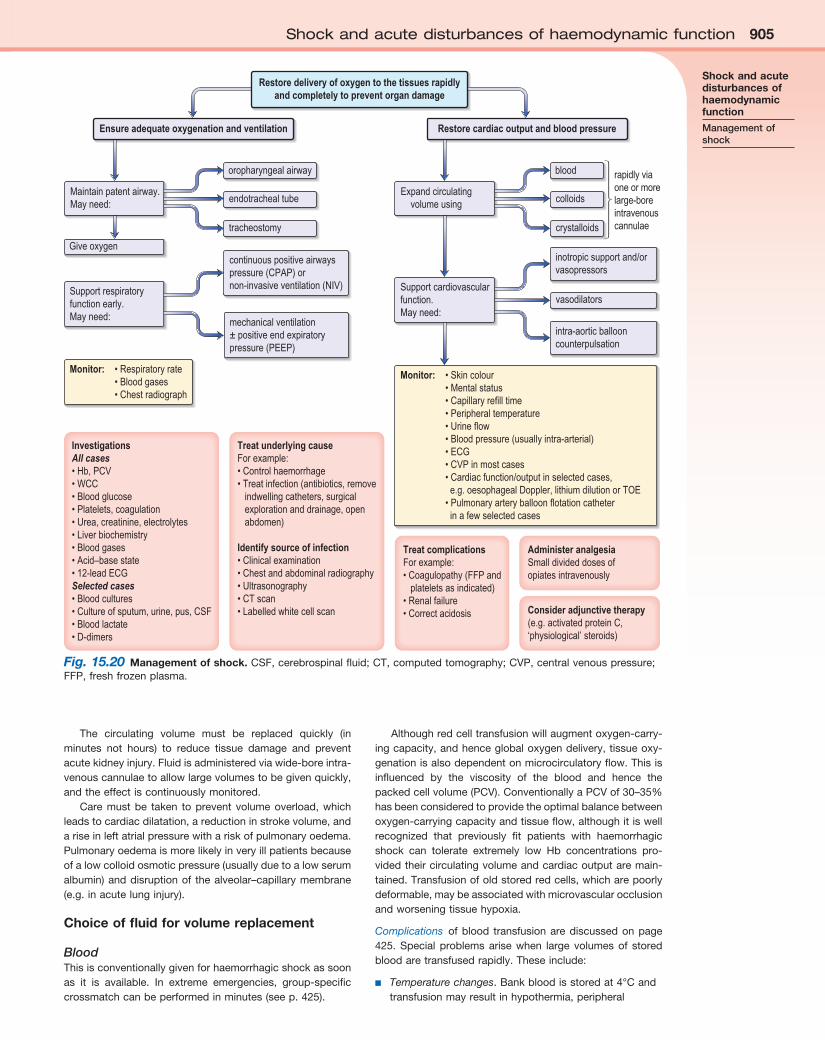
MANAGEMENT OF SHOCK (seeFig.15.20)
Delaysinmakingthediagnosisandininitiatingtreatment,aswellasinadequateresuscitation,contributetothedevelop-mentofmultipleorganfailure(MOF)andshouldbeavoided(seep.909).
Apatentairwaymustbemaintainedandoxygenmustbegiven.Ifnecessary,anoropharyngealairwayoranendotra-chealtubeis inserted.Thelatterhastheadvantageofpre-ventingaspirationofgastriccontents.Veryrarely,emergencytracheostomy is indicated (seebelow).Somepatientsmayrequiremechanicalventilation.
Theunderlyingcauseofshockshouldbecorrected–forexample, haemorrhage should be controlled or infectioneradicated. Inpatientswithsepticshock,everyeffortmustbemade to identify thesourceof infectionand isolate thecausativeorganism.Aswellasathoroughhistoryandclinicalexamination,X-rays,ultrasonographyorCTscanningmayberequired to locate the origin of the infection. Appropriatesamples (urine, sputum, cerebrospinal fluid, pus drainedfromabscesses)shouldbesenttothelaboratoryformicros-copy,cultureandsensitivities.Severalbloodculturesshouldbe performed and empirical, broad-spectrum antibiotictherapy(p.89)shouldbecommencedwithinthefirsthourofrecognitionofsepsis.Ifanorganismisisolatedlater,therapycan be adjusted appropriately. The choice of antibioticdependsonthelikelysourceofinfection,previousantibiotictherapyandknown local resistancepatterns,aswellasonwhetherinfectionwasacquiredinhospitalorinthecommu-nity. Abscesses must be drained and infected indwellingcathetersremoved.
Whatevertheaetiologyofthehaemodynamicabnormality,tissuebloodflowmustberestoredbyachievingandmaintain-ing an adequate cardiac output, as well as ensuring thatarterialbloodpressure issufficient tomaintainperfusionofvitalorgans.RecentlypublishedguidelinesforadultpatientssufferingseveresepsisorsepticshockadvocatetargetinganMAP>65mmHg,CVP8–12mmHg(>12mmHgifmechani-cally ventilated), urine output >0.5mL/kg/h and an S Ocv 2 ≥70%(orS Ov 2≥65%)astheinitialgoalsofresuscitation.
Preload and volume replacementOptimizing preload is the most efficient way of increasingcardiacoutput.Volumereplacementisobviouslyessentialinhypovolaemicshockbutisalsorequiredinanaphylacticandsepticshockbecauseofvasodilatation,sequestrationofbloodandlossofcirculatingvolumebecauseofcapillaryleak.
In obstructive shock, high filling pressures may berequired to maintain an adequate stroke volume. Even incardiogenicshock,carefulvolumeexpansionmay,onocca-sions, lead to a useful increase in cardiac output. On theother hand, patients with severe cardiac failure, in whomventricularfillingpressuresmaybemarkedlyelevated,oftenbenefit from measures to reduce preload (and afterload) –suchastheadministrationofdiureticsandvasodilators(seebelow). Adequate perioperative volume replacement alsoreduces morbidity and mortality in high-risk surgicalpatients.
Fig. 15.19 Doppler ultrasonography.StylizedvelocitywaveformtracesobtainedusingoesophagealDopplerultrasonography.ReproducedfromSingeretal.(1991),withpermission©1991TheWilliamsandWilkinsCo.,Baltimore.
Peak velocity
Time
Stroke distance
Mean acceleration
Velocity
Flow time
Oesophageal Doppler probe
Shock and acute disturbances of haemodynamic function 905Shock and acute disturbances of haemodynamic function 905
The circulating volume must be replaced quickly (inminutes not hours) to reduce tissue damage and preventacutekidneyinjury.Fluidisadministeredviawide-boreintra-venouscannulaetoallowlargevolumestobegivenquickly,andtheeffectiscontinuouslymonitored.
Caremustbe taken toprevent volumeoverload,whichleadstocardiacdilatation,areductioninstrokevolume,andariseinleftatrialpressurewithariskofpulmonaryoedema.Pulmonaryoedemaismorelikelyinveryillpatientsbecauseofalowcolloidosmoticpressure(usuallyduetoalowserumalbumin)anddisruptionof thealveolar–capillarymembrane(e.g.inacutelunginjury).
Choice of fluid for volume replacement
BloodThisisconventionallygivenforhaemorrhagicshockassoonas it is available. In extreme emergencies, group-specificcrossmatchcanbeperformedinminutes(seep.425).
Althoughredcelltransfusionwillaugmentoxygen-carry-ingcapacity,andhenceglobaloxygendelivery,tissueoxy-genationisalsodependentonmicrocirculatoryflow.Thisisinfluenced by the viscosity of the blood and hence thepackedcellvolume(PCV).ConventionallyaPCVof30–35%hasbeenconsideredtoprovidetheoptimalbalancebetweenoxygen-carryingcapacityandtissueflow,althoughitiswellrecognized that previously fit patients with haemorrhagicshock can tolerate extremely low Hb concentrations pro-videdtheircirculatingvolumeandcardiacoutputaremain-tained.Transfusionofoldstoredredcells,whicharepoorlydeformable,maybeassociatedwithmicrovascularocclusionandworseningtissuehypoxia.
Complications ofblood transfusionarediscussedonpage425. Special problems arise when large volumes of storedbloodaretransfusedrapidly.Theseinclude:
■ Temperature changes.Bankbloodisstoredat4°Candtransfusionmayresultinhypothermia,peripheral
Fig. 15.20 Management of shock.CSF,cerebrospinalfluid;CT,computedtomography;CVP,centralvenouspressure;FFP,freshfrozenplasma.
Restore delivery of oxygen to the tissues rapidlyand completely to prevent organ damage
Ensure adequate oxygenation and ventilation Restore cardiac output and blood pressure
Expand circulatingvolume using
Maintain patent airway.May need:
inotropic support and/orvasopressors
intra-aortic ballooncounterpulsation
Support cardiovascularfunction.May need:
continuous positive airwayspressure (CPAP) ornon-invasive ventilation (NIV)Support respiratory
function early.May need:
Monitor: • Respiratory rate • Blood gases • Chest radiograph
Monitor: • Skin colour • Mental status • Capillary refill time • Peripheral temperature • Urine flow • Blood pressure (usually intra-arterial) • ECG • CVP in most cases • Cardiac function/output in selected cases, e.g. oesophageal Doppler, lithium dilution or TOE • Pulmonary artery balloon flotation catheter in a few selected cases
Treat complicationsFor example:• Coagulopathy (FFP and platelets as indicated)• Renal failure• Correct acidosis
Administer analgesiaSmall divided doses ofopiates intravenously
Consider adjunctive therapy(e.g. activated protein C,‘physiological’ steroids)
InvestigationsAll cases• Hb, PCV• WCC• Blood glucose• Platelets, coagulation• Urea, creatinine, electrolytes• Liver biochemistry• Blood gases• Acid–base state• 12-lead ECGSelected cases• Blood cultures• Culture of sputum, urine, pus, CSF• Blood lactate• D-dimers
Treat underlying causeFor example:• Control haemorrhage• Treat infection (antibiotics, remove indwelling catheters, surgical exploration and drainage, open abdomen)
Identify source of infection• Clinical examination• Chest and abdominal radiography• Ultrasonography• CT scan• Labelled white cell scan
mechanical ventilation± positive end expiratorypressure (PEEP)
colloids
crystalloids
vasodilators
blood
endotracheal tube
tracheostomy
Give oxygen
oropharyngeal airway rapidly viaone or morelarge-boreintravenouscannulae
Shock and acute disturbances of haemodynamic function
Management of shock

906 Intensive care medicine15 906 Intensive care medicine15venoconstriction(whichslowstherateoftheinfusion)andarrhythmias.Ifpossible,bloodshouldthereforebewarmedduringmassivetransfusionandinthoseatriskofhypothermia(e.g.duringprolongedmajorsurgerywithopenbodycavity).
■ Coagulopathy.Storedbloodhasvirtuallynoeffectiveplateletsandisdeficientinclottingfactors.Largetransfusionscanthereforeproduceacoagulationdefect.Thismayneedtobetreatedbyreplacingclottingfactorswithfreshfrozenplasmaandadministeringplateletconcentrates.Occasionallycryoprecipitatemayberequired.
■ Metabolic acidosis/alkalosis.Storedbloodispreservedincitrate/phosphate/dextrose(CPD)solution,andmetabolicacidosisattributablesolelytobloodtransfusionisrareandinanycaseseldomrequirescorrection.Ametabolicalkalosisoftendevelops24–48hoursafteralargebloodtransfusion,probablymainlyowingtometabolismofthecitrate.Thiswillbeexacerbatedifanyprecedingacidosishasbeencorrectedwithintravenoussodiumbicarbonate.
■ Hypocalcaemia.Citrateinstoredbloodbindscalciumions.Duringrapidtransfusion,citratemayreducetotalbodyionizedcalciumlevels,causingmyocardialdepression.Thisisuncommoninpractice,butcanbecorrectedbyadministering10mLof10%calciumchlorideintravenously.Routinetreatmentwithcalciumisnotrecommended.
■ Increased oxygen affinity.Instoredblood,theredcell2,3-disphosphoglycerate(2,3-DPG)contentisreduced,sothattheoxyhaemoglobindissociationcurveisshiftedtotheleft.Theoxygenaffinityofhaemoglobinisthereforeincreasedandoxygenunloadingisimpaired.ThiseffectislessmarkedwithCPDblood.Redcelllevelsof2,3-DPGaresubstantiallyrestoredwithin12hoursoftransfusion.
■ Hyperkalaemia.Plasmapotassiumlevelsriseprogressivelyasbloodisstored.However,hyperkalaemiaisrarelyaproblemasrewarmingofthebloodincreasesredcellmetabolism–thesodiumpumpbecomesactiveandpotassiumlevelsfall.
■ Microembolism.Microaggregatesinstoredbloodmaybefilteredoutbythepulmonarycapillaries.Thisprocessisthoughtbysometocontributetoacutelunginjury(ALI)(seep.917).
Red cell concentratesStandard red cell concentrates are being replaced bysupplemental red cell concentrates, in which most of theplasma is removed and the red cells are suspended in100mL of nutrient additive solution. The most commonlyused additive is SAG (saline, adenine, glucose) to whichmannitol (M) is added to reducespontaneous lysis (SAGMblood).
Concern about the supply, cost and safety of blood,includingtheriskofdiseasetransmissionandimmunesup-pression,hasencouragedamoreconservativeapproachtotransfusion.Thereissomeevidencetosuggestthatinnor-movolaemiccriticallyillpatientsarestrictivestrategyofredcell transfusion (Hb maintained at >7.0g/dL) is at least aseffective,andmaybesaferthanaliberaltransfusionstrategy(Hb maintained at 10–12g/dL). However, in some groupsofpatients(e.g.theelderlyandthosewithsignificantcardiacorrespiratorydiseaseandpatientswhoareactivelybleeding)
it may be preferable to maintain Hb closer to the higherlevel.
Blood substitutesAttempts todevelopaneffectiveandsafeoxygen-carryingbloodsubstitutehavesofarbeenunsuccessful.
Crystalloids and colloidsThe choice of intravenous fluid for resuscitation and therelativemeritsofcrystalloidsorcolloidshaslongbeencon-troversial. Crystalloid solutions such as saline are cheap,convenienttouseandfreeofside-effects,althoughtheyarerapidlylostfromthecirculationintotheextravascularspaces.It has been generally accepted that volumes of crystalloidseveraltimesthatofcolloidarerequiredtoachieveanequiv-alent haemodynamic response and that colloidal solutionsproduceagreaterandmoresustainedincreaseincirculatingvolume, with associated improvements in cardiovascularfunctionandoxygentransport.
Nevertheless, a large, prospective, randomized, con-trolledtrialhasdemonstratedthatinaheterogeneousgroupofcritically illpatients theuseofeitherphysiologicalsalineor 4% albumin for fluid resuscitation resulted in similaroutcomes.
Polygelatin solutions (Haemaccel, Gelofusin) have anaverage molecular weight of 35000, which is iso-osmoticwithplasma.Theyarecheapanddonotinterferewithcross-matching.Largevolumescanbeadministered,asclinicallysignificantcoagulationdefectsareunusualandrenalfunctionis not impaired. However, because they readily cross theglomerularbasementmembrane,theirhalf-lifeinthecircula-tionisonlyapproximately4hoursandtheycanpromoteanosmotic diuresis. These solutions are particularly usefulduring the acute phase of resuscitation, especially whenvolumelossesarecontinuing.Allergicreactionscan,however,occur.
Hydroxyethyl starches (HES).Numerouspreparationsarenow available, characterized by their concentrations (3%,6%,10%)and low,mediumorhighmolecularweight.Thehalf-life of high and medium molecular weight solutions isbetween12and24hours,whilst thatof the lowmolecularweight solutions is 4–6 hours. Elimination of HES occursprimarily via the kidneys following hydrolysis by amylase.HESarestoredinthereticuloendothelialsystem,apparentlywithout causing functional impairment, but skin depositshave been associated with persistent pruritus. HES, espe-ciallythehighermolecularweightfractions,haveanticoagu-lantpropertiesandmany therefore recommend limiting thevolumeadministered.Recentevidencehas implicatedHESinthedevelopmentofacutekidneyinjury.
Dextransarepolymolecularpolysaccharidesthathaveapowerful osmotic effect. They interferewith crossmatchingand have a small rate of allergic reactions (0.1–1%) whichmaybelife-threatening.Normallyadoseof1.5gdextranperkilogram of bodyweight (as Dextran 70) should not beexceededbecauseoftheriskofrenaldamage.Inpractice,dextransarerarelyusedintheUKbecauseoftheavailabilityofotheragents.
Human albumin solution(HAS)isanaturalcolloidwhichhasbeenusedforvolumereplacementinshockandburns,andforthetreatmentofhypoproteinaemia.HASisnotgener-allyrecommendedforroutinevolumereplacement,becausesuppliesarelimitedandothercheapersolutionsareequallyeffective.

Shock and acute disturbances of haemodynamic function 907Shock and acute disturbances of haemodynamic function 907
Myocardial contractility and inotropic agentsMyocardial contractility can be impaired by many factorssuchashypoxaemiaandhypocalcaemia,aswellasbysomedrugs (e.g. beta-blockers, antiarrhythmics, angiotensin-convertingenzymeinhibitorsandsedatives).
Severe lactic acidosis conventionally is said to depressmyocardialcontractilityandlimittheresponsetovasopres-sor agents. Attempted correction of acidosis with intrave-nous sodium bicarbonate, however, generates additionalcarbondioxidewhichdiffusesacrosscellmembranes,pro-ducing or exacerbating intracellular acidosis. Other disad-vantages of bicarbonate therapy include sodium overloadand a left shift of the oxyhaemoglobin dissociation curve.Ionizedcalciumlevelsmaybereducedand,combinedwiththefallinintracellularpH,thismayimpairmyocardialperfor-mance. Treatment of lactic acidosis should therefore con-centrate on correcting the cause. Bicarbonate should onlybeadministeredtocorrectextreme persistent metabolic aci-dosis(seep.675).
If the signs of shock persist despite adequate volumereplacement, and perfusion of vital organs is jeopardized,pressor agents shouldbeadministered to improvecardiacoutput and blood pressure. Vasopressor therapy may alsoberequiredtomaintainperfusioninthosewithlife-threaten-inghypotension,evenwhenvolumereplacement is incom-plete.Allinotropesincreasemyocardialoxygenconsumption,particularlyifatachycardiadevelops,andthiscanleadtoanimbalancebetweenmyocardialoxygensupplyanddemand,withthedevelopmentorextensionofischaemicareas.Ino-tropesshouldthereforebeusedwithcaution,particularlyincardiogenic shock following myocardial infarction and inthoseknowntohaveischaemicheartdisease.
Manyof themostseriously illpatientsbecome increas-inglyresistanttotheeffectsofpressoragents,anobserva-tion attributed to ‘downregulation’ of adrenergic receptorsandNO-induced‘vasoplegia’(p.895).
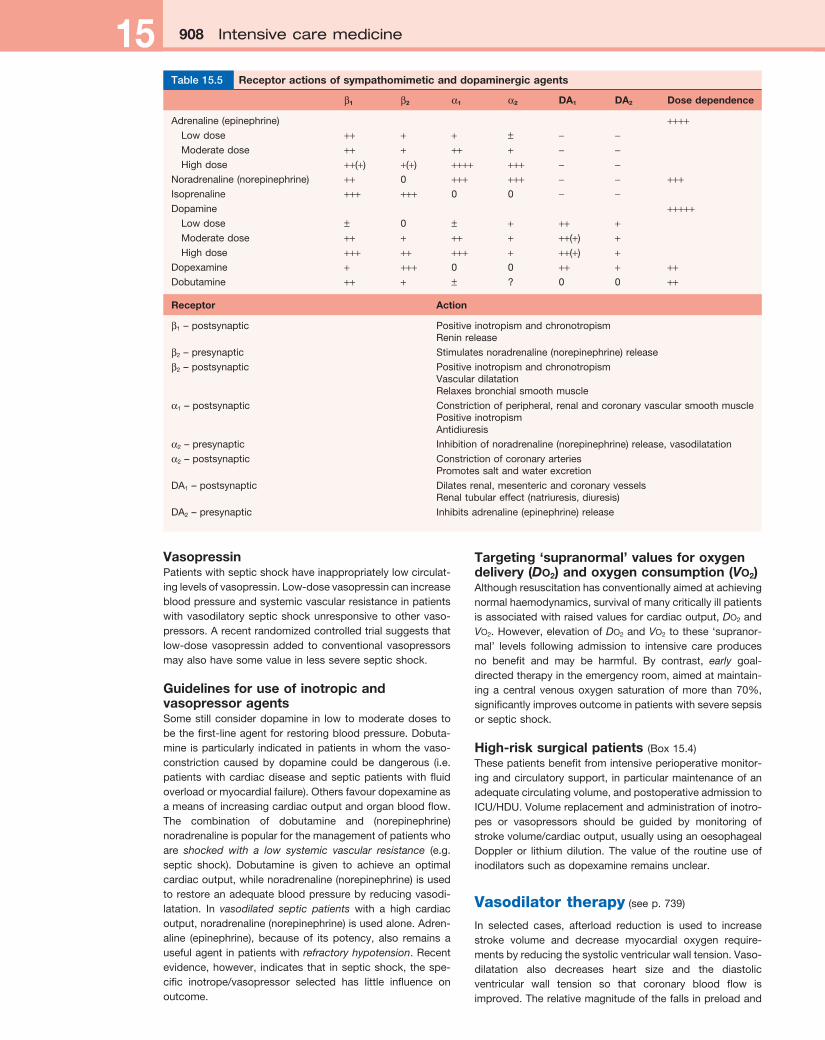
All inotropic agents should be administered via a largecentralvein,andtheireffectsmonitored(seealsop.908andTable15.5).
Adrenaline (epinephrine)Epinephrinestimulatesbothα-andβ-adrenergicreceptors,but at low doses β effects seem to predominate. Thisincreases heart rate and cardiac index whilst reducingperipheralresistance.Ifthisisassociatedwithanincreaseinperfusionpressure,urineoutputmay improve.Epinephrineathigherdosescancauseexcessive(α-mediated)vasocon-striction, with reductions in splanchnic flow, and cardiacoutput may fall. Prolonged high-dose administration cancauseperipheralgangreneandlacticacidosis.Theminimumeffectivedoseofadrenalineshouldthereforebeusedforasshortatimeaspossible.
Noradrenaline (norepinephrine)Thisispredominantlyanα-adrenergicagonist.Itisparticu-larlyusefulinthosewithhypotensionassociatedwithalowsystemic vascular resistance, for example in septic shock.Thereisariskofproducingexcessivevasoconstrictionwithimpairedorganperfusionandincreasedafterload.Noradren-alineadministrationshouldnormallythereforebeguidedbycomprehensive haemodynamic monitoring, including inva-
siveornon-invasivedeterminationofcardiacoutput(seep.903)andcalculationofsystemicvascularresistance.
DopamineDopamineisanaturalprecursorofadrenaline(epinephrine)whichactsonβreceptorsandαreceptors,aswellasdopa-minergicDA1andDA2receptors.
Inlow doses(e.g.1–3µg/kg/min),dopaminergicvasodila-toryreceptorsintherenal,mesenteric,cerebralandcoronarycirculationsareactivated.DA1receptorsarelocatedonpost-synapticmembranesandmediatevasodilatation,whilstDA2receptorsarepresynapticandpotentiatethesevasodilatoryeffectsbypreventingthereleaseofadrenaline(epinephrine).Renalandhepaticflowincreaseandurineoutputisimproved.Thesignificanceoftherenalvasodilatoreffectofdopaminehas,however,beenquestionedand ithasbeensuggestedthatthe increasedurineoutput is largelyattributabletotheriseincardiacoutputandbloodpressure,combinedwithadecrease in aldosterone and inhibition of tubular sodiumreabsorptionmediatedviaDA1stimulation.
In moderate doses (e.g. 3–10µg/kg/min), dopamineincreases heart rate, myocardial contractility and cardiacoutput.Insomepatientsthedoseofdopamineislimitedbyβ-receptoreffectssuchastachycardiaandarrhythmias.
In higher doses (e.g. >10µg/kg/min) the increased nor-adrenaline (norepinephrine) produced is associated withvasoconstriction. This increases afterload and raises ven-tricularfillingpressures.
DopexamineDopexamineisananalogueofdopaminewhichactivatesβ2receptorsaswellasDA1andDA2receptors.Dopexamineisaweakpositiveinotrope,butisapowerfulsplanchnicvaso-dilator,reducingafterloadandimprovingbloodflowtovitalorgans,includingthekidneys.Insepticshock,dopexaminecanincreasecardiacindexandheartrate,butcausesfurtherreductionsinperipheralresistance.Itismostusefulinthosewithlowcardiacoutputandperipheralvasoconstrictionandhasbeenusedasanadjunct to theperioperativemanage-mentofhigh-riskpatients(seebelow).
DobutamineDobutamineiscloselyrelatedtodopamineandhaspredomi-nantlyβ1activity.Dobutaminehasnospecificeffectontherenalvasculaturebuturineoutputoftenincreasesascardiacoutput and blood pressure improve. It reduces systemicvascular resistance, as well as improving cardiac perfor-mance, thereby decreasing afterload and ventricular fillingpressures. Dobutamine is therefore useful in patients withcardiogenicshockandcardiacfailure.Insepticshock,dobu-taminecanbeusedtoincreasecardiacoutputandoxygendelivery.
Phosphodiesterase inhibitors (e.g. milrinone, enoximone)Theseagentshavebothinotropicandvasodilatorproperties.BecausethephosphodiesterasetypeIIIinhibitorsbypasstheβ-adrenergicreceptortheydonotcausetachycardiaandarelessarrhythmogenicthanβagonists.Theymaybeusefulinpatients with receptor ‘downregulation’, those receivingbeta-blockers, for weaning patients from cardiopulmonarybypassand forpatientswithcardiac failure. Invasodilatedseptic patients, however, they may precipitate or worsenhypotension.
908 Intensive care medicine15 908 Intensive care medicine15
VasopressinPatientswithsepticshockhaveinappropriatelylowcirculat-inglevelsofvasopressin.Low-dosevasopressincanincreasebloodpressureandsystemicvascularresistanceinpatientswithvasodilatorysepticshockunresponsive toothervaso-pressors.Arecentrandomizedcontrolledtrialsuggeststhatlow-dose vasopressin added to conventional vasopressorsmayalsohavesomevalueinlessseveresepticshock.
Guidelines for use of inotropic and vasopressor agentsSomestillconsiderdopamine in lowtomoderatedoses tobethefirst-lineagentforrestoringbloodpressure.Dobuta-mineisparticularly indicatedinpatients inwhomthevaso-constriction caused by dopamine could be dangerous (i.e.patientswithcardiacdiseaseandsepticpatientswithfluidoverloadormyocardialfailure).Othersfavourdopexamineasameansofincreasingcardiacoutputandorganbloodflow.The combination of dobutamine and (norepinephrine)noradrenalineispopularforthemanagementofpatientswhoare shocked with a low systemic vascular resistance (e.g.septic shock). Dobutamine is given to achieve an optimalcardiacoutput,whilenoradrenaline(norepinephrine)isusedtorestoreanadequatebloodpressurebyreducingvasodi-latation. In vasodilated septic patients with a high cardiacoutput,noradrenaline(norepinephrine)isusedalone.Adren-aline (epinephrine), because of its potency, also remains ausefulagentinpatientswithrefractory hypotension.Recentevidence,however, indicatesthat insepticshock, thespe-cific inotrope/vasopressor selected has little influence onoutcome.
Targeting ‘supranormal’ values for oxygen delivery (Do2) and oxygen consumption (Vo2)Althoughresuscitationhasconventionallyaimedatachievingnormalhaemodynamics,survivalofmanycriticallyillpatientsisassociatedwithraisedvaluesforcardiacoutput,Do2andVo2.However,elevationofDo2andVo2tothese‘supranor-mal’ levels following admission to intensive care producesno benefit and may be harmful. By contrast, early goal-directedtherapyintheemergencyroom,aimedatmaintain-ingacentral venousoxygensaturationofmore than70%,significantlyimprovesoutcomeinpatientswithseveresepsisorsepticshock.
High-risk surgical patients (Box15.4)Thesepatientsbenefitfromintensiveperioperativemonitor-ingandcirculatorysupport, inparticularmaintenanceofanadequatecirculatingvolume,andpostoperativeadmissiontoICU/HDU.Volumereplacementandadministrationofinotro-pes or vasopressors should be guided by monitoring ofstrokevolume/cardiacoutput,usuallyusinganoesophagealDoppler or lithium dilution. The value of the routine use ofinodilatorssuchasdopexamineremainsunclear.
Vasodilator therapy(seep.739)
In selected cases, afterload reduction is used to increasestroke volume and decrease myocardial oxygen require-mentsbyreducingthesystolicventricularwalltension.Vaso-dilatation also decreases heart size and the diastolicventricular wall tension so that coronary blood flow isimproved.Therelativemagnitudeofthefallsinpreloadand
β1 β2 α1 α2 DA1 DA2 Dose dependence
Adrenaline(epinephrine) ++++ Lowdose ++ + + ± − − Moderatedose ++ + ++ + − − Highdose ++(+) +(+) ++++ +++ − −Noradrenaline(norepinephrine) ++ 0 +++ +++ − − +++Isoprenaline +++ +++ 0 0 − −Dopamine +++++ Lowdose ± 0 ± + ++ + Moderatedose ++ + ++ + ++(+) + Highdose +++ ++ +++ + ++(+) +Dopexamine + +++ 0 0 ++ + ++Dobutamine ++ + ± ? 0 0 ++
Receptor Action
β1–postsynaptic PositiveinotropismandchronotropismReninrelease
β2–presynaptic Stimulatesnoradrenaline(norepinephrine)release
β2–postsynaptic PositiveinotropismandchronotropismVasculardilatationRelaxesbronchialsmoothmuscle
α1–postsynaptic Constrictionofperipheral,renalandcoronaryvascularsmoothmusclePositiveinotropismAntidiuresis
α2–presynaptic Inhibitionofnoradrenaline(norepinephrine)release,vasodilatation
α2–postsynaptic ConstrictionofcoronaryarteriesPromotessaltandwaterexcretion
DA1–postsynaptic Dilatesrenal,mesentericandcoronaryvesselsRenaltubulareffect(natriuresis,diuresis)
DA2–presynaptic Inhibitsadrenaline(epinephrine)release
Table 15.5 Receptor actions of sympathomimetic and dopaminergic agents

Shock and acute disturbances of haemodynamic function 909Shock and acute disturbances of haemodynamic function 909
afterloaddependsonthepre-existinghaemodynamicdistur-bance, concurrent volume replacement and the agentselected(seebelow).Specificvasodilatorsmayalsoimprovemicrocirculatoryflow.
Vasodilatortherapycanbeparticularlyhelpfulinpatientswithcardiacfailureinwhomtheventricularfunctioncurveisflat(seeFig.15.3)sothatfallsinpreloadhaveonlyalimitedeffectonstrokevolume.Thisformoftreatment,combinedinselectedcaseswithinotropicsupport, isthereforeuseful incardiogenicshockand in themanagementofpatientswithcardiogenic pulmonary oedema, mitral regurgitation or anacuteventricularseptaldefect.
Nitrate vasodilatorsareusuallyused.Nitrates,becauseoftheirabilitytoimprovethemyocardialoxygensupply/demandratio, alsohelp tocontrol anginaand limit ischaemicmyo-cardial injury.Theagentsusedmostcommonly toachievevasodilatationinthecriticallyillarethosewhichactdirectlyonthevesselwall.
Sodium nitroprusside(SNP)dilatesarteriolesandvenouscapacitance vessels, aswell as thepulmonary vasculaturebydonatingnitricoxide.SNPthereforereducestheafterloadand preload of both ventricles and can improve cardiacoutput and the myocardial oxygen supply/demand ratio.SNP,however,canexacerbatemyocardialischaemiabypro-ducinga‘steal’phenomenoninthecoronarycirculation.TheeffectsofSNParerapidinonsetandspontaneouslyrevers-iblewithinafewminutesofdiscontinuingtheinfusion.AlargeoverdoseofSNPcancausecyanidepoisoning,withintracel-lularhypoxiacausedbyinhibitionofcytochromeoxidase,theterminalenzymeoftherespiratorychain.Thisismanifestedasametabolicacidosisandafallinthearteriovenousoxygencontentdifference.
Nitroglycerine (NTG) and isosorbide dinitrate (ISDN). Atlow doses, these agents are both predominantly venodila-tors,butas thedose is increased, theyalsocausearterialdilatation, thereby decreasing both preload and afterload.Nitrates are particularly useful in the treatment of cardiacfailurewithpulmonaryoedemaandareusuallyusedincom-binationwith intravenous furosemide.BothNTGand ISDNreduce pulmonary vascular resistance, an effect that canoccasionally be exploited in patients with a low cardiacoutputsecondarytopulmonaryhypertension.
Hydralazine predominantly affects arterial resistancevessels. It therefore reducesafterloadandbloodpressure,whilecardiacoutputandheartrateincrease.Hydralazineisusually given as an intravenous bolus to control acuteincreasesinbloodpressure.
Mechanical support of the myocardiumIntra-aortic balloon counterpulsation (IABCP) is the tech-niqueusedmostwidelyformechanicalsupportofthefailingmyocardium.Itisdiscussedonpage714.
Sepsis and multiple organ failure (MOF) (alsoknownasmultipleorgandysfunction
syndrome–MODS)
Sepsis isbeingdiagnosedwithincreasingfrequencyandisnow thecommonest causeofdeath innon-coronaryadultintensive care units. The estimated incidence of severesepsishasvaried from77 to300casesper100000of thepopulation.Mortalityratesarehigh(between20%and60%)and are closely related to the severity of illness and thenumberoforganswhichfail.Thosewhodieareoverwhelmedby persistent or recurrent sepsis, with fever, intractablehypotensionandfailureofseveralorgans.
Sequentialfailureofvitalorgansoccursprogressivelyoverweeks,althoughthepatternoforgandysfunctionisvariable.Inmostcasesthelungsarethefirsttobeaffected(acutelunginjury–ALI;acuterespiratorydistresssyndrome–ARDS;seep.917)inassociationwithcardiovascularinstabilityanddete-rioratingrenalfunction.Damagetothemucosalliningofthegastrointestinaltract,asaresultofreducedsplanchnicflowfollowedbyreperfusion,allowsbacteriawithinthegutlumen,ortheircellwallcomponents,togainaccesstothecircula-tion. The liver defences, which are often compromised bypoor perfusion, are overwhelmed and the lungs and otherorgans are exposed to bacterial toxins and inflammatorymediatorsreleasedbylivermacrophages.Somehavethere-forecalledthegutthe‘motorofmultipleorganfailure’.Sec-ondary pulmonary infection, complicating ALI/ARDS, alsofrequently acts as a further stimulus to the inflammatoryresponse.Later, renal failureand liverdysfunctiondevelop(seep.910).Gastrointestinalfailure,withaninabilitytotoler-ateenteralfeedingandparalyticileus,iscommon.Ischaemiccolitis,acalculouscholecystitis,pancreatitisandgastrointes-tinalhaemorrhagemayalsooccur.Featuresofcentralnervoussystemdysfunctionincludeimpairedconsciousnessanddis-orientation, progressing to coma. Characteristically, thesepatientsinitiallyhaveahyperdynamiccirculationwithvasodi-latation and a high cardiac output, associated with anincreasedmetabolicrate.Eventually,however,cardiovascu-larcollapsesupervenesandistheusualterminalevent.
Adjunctive treatmentInitialattemptstocombatthehighmortalityassociatedwithsepsisconcentratedoncardiovascularandrespiratorysupportin the hope that survival could be prolonged until surgery,antibioticsandthepatient’sowndefenceshaderadicatedtheinfection and injured tissues were repaired. Despite somesuccess, mortality rates remained unacceptably high. Sofar,attemptstoimproveoutcomebymodulatingtheinflam-matoryresponse(includinghigh-dosesteroids)orneutralizingendotoxin(Table15.6)orinhibitingnitricoxidesynthesis(e.g.with N-monomethyl-l-arginine) have proved disappointingandinsomecasesmayevenhavebeenharmful.
AdministrationofrecombinanthumanactivatedproteinC(rhAPC), an endogenous anticoagulant with anti-inflamma-toryproperties,mayimproveoutcomeinsomeadultpatientswith severe sepsis andmultipleorgandysfunction.Also, it
■ Patientswithjeopardizedcardiorespiratoryfunction■ Patientswithtraumatotwobodycavitiesrequiring
multiplebloodtransfusions■ Patientsundergoingsurgeryinvolvingextensivetissue
dissection,e.g.oesophagectomy,pancreatectomy,aorticaneurysmsurgery
■ Patientsundergoingemergencysurgeryforintra-abdominalorintrathoraciccatastrophicstates,e.g.faecalperitonitis,oesophagealperforation
ModifiedfromShoemakerWCetal.Chest1988;94:1176–1178.
i Box 15.4 Patients at risk of developing perioperative multiorgan failure

910 Intensive care medicine15 910 Intensive care medicine15
seemsthattheadministrationofrelativelylow,‘stress’dosesof hydrocortisone to patients with refractory vasopressordependentsepticshockmayassistshockreversal.Carefulcontrolof thebloodsugar level tobelow8.3mmol/L (‘tightglycaemiccontrol’)isalsorecommended.
Theaimofcurrentsepsisguidelinesistocombinethese,andotherevidence-basedinterventions,withearlyeffectiveresuscitation(aimedespeciallyatachievinganadequatecir-culatingvolume,combinedwiththerationaluseofinotropesand/orvasoactiveagentstomaintainbloodpressure,cardiacoutputandoxygentransport) inordertocreate‘bundlesofcare’ delivered within specific time limits (see http://www.survivingsepsis.org).
volume and restoring blood pressure. Restoration of theurineoutputisagoodindicatorofsuccessfulresuscitation.Evidence now suggests that dopamine is not an effectivemeansofpreventingorreversingrenal impairmentandthisagentshouldnotbeused for renalprotection insepsis (p.907).Ifthesemeasuresfailtoreverseoliguria,administrationofdiureticssuchasfurosemidebybolusorinfusion,orlessoftenmannitol(forexampleinrhabdomyolysis)maybeindi-cated (see Ch. 11). If oliguria persists, it is necessary toreducefluidintakeandreviewdrugdoses.
Intermittent haemodialysis has a number of disadvan-tagesinthecritically ill. Inparticular it isfrequentlycompli-cated by hypotension and it may be difficult to removesufficientvolumesoffluid.Peritonealdialysis isalsounsat-isfactory in these patients and is contraindicated in thosewho have undergone intra-abdominal surgery. The use ofcontinuousveno-venoushaemofiltration,usuallywithdialy-sis(CVVHD), isthereforepreferred(seeCh.11)andis indi-catedforfluidoverload,electrolytedisturbances(especiallyhyperkalaemia), severe acidosis and, to a lesser extent,uraemia.
Iftheunderlyingproblemsresolve,renalfunctionalmostinvariablyrecoversafewdaystoseveralweekslater.
High-dosesteroids
Endotoxinantibodies
Bactericidalpermeability-increasingprotein
TNFantibodies
SolubleTNFreceptors
Interleukin-1receptorantagonists
Platelet-activatingfactorantagonists
N-acetylcysteine
Nitricoxidesynthaseinhibition
Antithrombin
ActivatedproteinC
Table 15.6 Some of the therapeutic strategies tested in randomized, controlled phase II or III trials in human sepsis
FURTHER READING
BrunkhorstFM,EngelC,BloosFetal.Intensiveinsulintherapyandpentastarchresuscitationinseveresepsis.New England Journal of Medicine 2008;358: 125–139.
DellingerRP,LevyMM,CarletJMetal.fortheInternationalSurvivingSepsisCampaignGuidelinesCommittee.SurvivingSepsisCampaign:InternationalGuidelinesforManagementofSevereSepsisandSepticShock.Critical Care Medicine 2008;36: 296–327.
FinferS,BellornoR,BoyceNetal.Acomparisonofalbuminandsalineforfluidresuscitationintheintensivecareunit.New England Journal of Medicine 2004;350: 2247–2256.
SprungCL,AnnaneD,KehDetalfortheCORTICUSStudyGroup.Hydrocortisonetherapyforpatientswithsepticshock.New England Journal of Medicine 2008;358: 111–124.
RENAL FAILURE (ACUTE KIDNEY INjURY)
Acutekidney injury isacommonandseriouscomplicationofcriticalillnesswhichadverselyaffectstheprognosis.Theimportanceofpreventingrenalfailurebyrapidandeffectiveresuscitation,aswellastheavoidanceofnephrotoxicdrugs(especiallyNSAIDs),andcontrolofinfectioncannotbeover-emphasized.Shockandsepsisarethemostcommoncausesofacuterenalfailureinthecriticallyill,butdiagnosisofthecauseofrenaldysfunctionisnecessarytoexcludereversiblepathology,especiallyobstruction(seeCh.11).
Oliguriaisusuallythefirstindicationofrenalimpairmentandimmediateattemptsshouldbemadetooptimizecardio-vascular function, particularly by expanding the circulating
FURTHER READING
FriedrichJO,AdhikariN,HerridgeMSetal.Meta-analysis:lowdosedopamineincreasesurineoutputbutdoesnotpreventrenaldysfunctionordeath.Annals of Internal Medicine 2005;142: 510–524.
HoKH,SheridanOJ.Meta-analysisoffurosemide(topreventortreatacuterenalfailure).British Medical Journal 2006;333: 420–426.
RESPIRATORY FAILURE (seeCh.14)
Types and causesTherespiratorysystemconsistsofagas-exchangingorgan(the lungs) and a ventilatory pump (respiratory muscles/thorax),eitherorbothofwhichcanfailandprecipitaterespi-ratoryfailure.Respiratoryfailureoccurswhenpulmonarygasexchangeissufficientlyimpairedtocausehypoxaemiawithorwithouthypercarbia.Inpracticalterms,respiratoryfailureispresentwhenthePao2is<8kPa(60mmHg)orthePaco2is>7kPa(55mmHg).Itcanbedividedinto:
■ typeIrespiratoryfailure,inwhichthePao2islowandthePaco2isnormalorlow
■ typeIIrespiratoryfailure,inwhichthePao2islowandthePaco2ishigh.
Type I or ‘acute hypoxaemic’ respiratory failure occurswithdiseasesthatdamage lungtissue.Hypoxaemia isdueto right-to-left shunts or V Q mismatch. Common causesinclude pulmonary oedema, pneumonia, acute lung injuryand,inthechronicsituation,lungfibrosis.
Type II or ‘ventilatory failure’occurswhenalveolarventila-tion is insufficient toexcrete thevolumeofcarbondioxidebeing produced by tissue metabolism. Inadequate alveolarventilation is due to reduced ventilatory effort, inability toovercome an increased resistance to ventilation, failure tocompensate for an increase in deadspace and/or carbondioxideproduction,or acombinationof these factors.Themost common cause is chronic obstructive pulmonary





























