Embed Size (px)
Citation preview

1468 Current Drug Targets, 2010, 11, 1468-1482
1389-4501/10 $55.00+.00 © 2010 Bentham Science Publishers Ltd.
Involvement of the Toxic AGEs (TAGE)-RAGE System in the Pathogenesis of Diabetic Vascular Complications: A Novel Therapeutic Strategy
Masayoshi Takeuchi*, Jun-ichi Takino and Sho-ichi Yamagishi
1Department of Life Pharmacy, Faculty of Pharmaceutical Sciences, Hokuriku University, Ho-3 Kanagawa-machi, Kanazawa, 920-1181, Japan 2Department of Pathophysiology and Therapeutics of Diabetic Vascular Complications, Kurume University School of Medicine, 67 Asahimachi, Kurume, 830-0011, Japan
Abstract: Diabetic vascular complications are leading causes of acquired blindness, end-stage renal failure, a variety of neuropathies, and accelerated atherosclerosis, which may be involved in the disabilities and high mortality rates suffered by diabetic patients. Continuous hyperglycemia is involved in the pathogenesis of diabetic micro- and macrovascular complications via various metabolic pathways, and numerous hyperglycemia-induced metabolic and hemodynamic conditions exist, including increased generation of various types of advanced glycation end-products (AGEs). Recently, we demonstrated that glyceraldehyde-derived AGEs (Glycer-AGEs), the predominant components of toxic AGEs (TAGE), play an important role in the pathogenesis of angiopathy in diabetic patients. Moreover, a growing body of evidence suggests that the interaction of TAGE with the receptor for AGEs (RAGE) alters intracellular signaling, gene expression, and the release of pro-inflammatory molecules and elicits oxidative stress generation in numerous types of cells, all of which may contribute to the pathological changes observed in diabetic vascular complications. Therefore, the inhibition of TAGE formation, blockade of TAGE-RAGE interaction, and the suppression of RAGE expression or its downstream pathways are promising targets for therapeutic interventions against diabetic vascular complications. In this review, we discuss the pathophysiological role of the TAGE-RAGE-oxidative stress system and related therapeutic interventions for preventing the development and progression of diabetic vascular complications.
Keywords: Diabetic vascular complications, advanced glycation end-products (AGEs), toxic AGEs (TAGE), receptor for AGEs (RAGE), oxidative stress, soluble RAGE (sRAGE), renin-angiotensin system (RAS), pigment-epithelium-derived factor (PEDF).
INTRODUCTION
Diabetic vascular complications are leading causes of end-stage renal failure, acquired blindness, a variety of neuropathies, and cardiovascular disease (CVD) and may be involved in the disability and high mortality rates suffered by patients with type 1 or type 2 diabetes mellitus (DM) [1]. Although various hyperglycemia-induced metabolic and hemodynamic conditions are proposed to contribute to vascular complications in DM [2, 3], recent clinical studies have suggested that the concept of “hyperglycemic memory” plays a role in the pathogenesis of vascular injury in DM [4-6]. Indeed, the Diabetes Control and Complications Trial-Epidemiology of Diabetes Interventions and Complications (DCCT-EDIC) Study demonstrated that the reduced risk of progressive retinopathy and nephropathy brought about by intensive therapy in patients with type 1 DM persisted for at least eight years, despite increasing hyperglycemia [4, 5]. The intensive therapy administered during the DCCT resulted in decreased progression of intima media thickness (IMT) and had reduced the risk of nonfatal myocardial infarction, stroke, or death from CVD by 57% by 11 years after the end of the trial [6].
*Address correspondence to this author at the Department of Life Pharmacy, Faculty of Pharmaceutical Sciences, Hokuriku University, Ho-3 Kanagawa-machi, Kanazawa 920-1181, Japan; Tel: +81-76-229-6197; Fax: +81-76-229-2781; E-mail: [email protected]
Furthermore, a recent follow-up study, the United Kingdom Prospective Diabetes Study (UKPDS), also demonstrated that the benefits of intensive therapy in patients with type 2 DM were sustained after the cessation of the trial [7]. In this study, despite the early loss of glycemic differences between the patients administered the intensive and conventional therapies, a continued reduction in micro-vascular risk and emergent reductions in the risks of myocardial infarction and death from any cause were observed during 10 years of post-trial follow-up [7]. These observations indicate that intensive therapy aimed at controlling blood glucose levels has long-term beneficial effects on the risk of diabetic retinopathy, nephropathy, CVD, and death in patients with type 1 or type 2 DM, strongly suggesting that so-called “metabolic memory” causes chronic damage to diabetic vessels that is not easily reversed, even by subsequent, relatively good control of blood glucose. Among the various pathways activated under DM, the biochemical nature of advanced glycation end-products (AGEs) and their mode of action are the most compatible with the theory of “hyperglycemic memory” [8, 9]. There is a growing body of evidence to suggest that continuous hyperglycemia under diabetic conditions enhances the formation of AGEs, which are senescent macroprotein derivatives, through non-enzymatic glycation (which is known as the “Maillard reaction”). There is also

A Novel Therapeutic Strategy for Diabetic Complications Current Drug Targets, 2010, Vol. 11, No. 11 1469
accumulating evidence that the binding of the receptor for AGEs (RAGE) with AGEs elicits oxidative stress generation and subsequently evokes inflammatory and/or thrombogenic responses in various types of cells, thus participating in the development and progression of diabetic angiopathies [10-18]. Recently, we demonstrated that glyceraldehyde-derived AGEs (Glycer-AGEs), a predominant component of toxic AGEs (TAGE), play an important role in the pathogenesis of angiopathy in diabetic patients [10, 19, 20]. Furthermore, there is a growing body of evidence to suggest that the interaction of TAGE with the RAGE alters intracellular sig-naling, gene expression, and the release of pro-inflammatory molecules and elicits oxidative stress generation in numerous types of cells, all of which may contribute to the pathological changes associated with diabetic vascular complications. Therefore, the inhibition of TAGE formation, blockade of TAGE-RAGE interactions, and the suppression of RAGE expression or its downstream pathways are promising targets for therapeutic interventions against diabetic vascular complications. In this review, we discuss the pathophysiological role of the TAGE-RAGE-oxidative stress system and related ther-apeutic interventions against the development and progress-sion of diabetic vascular complications.
INTERACTION OF AGES-RAGE IN VIVO
AGEs are formed by the Maillard reaction, a non-enzymatic reaction between the aldehyde or ketone groups of reducing sugars (such as glucose, fructose, and trioses etc.) and the amino groups of proteins, and contribute to the aging of proteins and to the pathological complications of DM [10-13, 19-24]. In the hyperglycemia elicited by DM, this process begins with the conversion of reversible Schiff base adducts to more stable, covalently bound Amadori rearrange-ment products. Over the course of days to weeks, these Amadori products undergo further rearrangement reactions to form irreversibly bound moieties known as AGEs. AGEs were originally characterized by their yellow-brown fluorescent color and their ability to form cross-links with and between amino groups, but the term is now used for a broad range of advanced products of the glycation process, including N-(carboxymethyl)lysine (CML) and pyrraline, which do not display color or fluorescence and are not cross-linked proteins [8, 21-25]. The formation of AGEs in vivo is dependent on the turnover rate of the chemically modified target, the time available, and the sugar concentration. The structures of the various cross-linked AGEs that are gene-rated in vivo have not yet been completely determined. Due to their heterogeneity and the complexity of the chemical reactions involved, only some AGEs have been structurally characterized in vivo. The structural identity of AGEs with cytotoxic properties also remains unknown. Recent studies have suggested that AGEs arise not only from reducing sugars, but also from carbonyl compounds derived from the autoxidation of sugars and other metabolic pathways [26-28]. Indeed, we have demonstrated that glucose, α-hydroxyaldehydes (glyceraldehyde and glycol-aldehyde), and dicarbonyl compounds (methylglyoxal, MGO; glyoxal, GO; and 3-deoxyglucosone, 3-DG) are
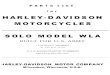
actively involved in protein glycation [21, 29-31]. Six immu-nochemically distinct classes of AGEs (glucose-derived AGEs, Glc-AGEs; glyceraldehyde-derived AGEs, Glycer-AGEs; glycolaldehyde-derived AGEs, Glycol-AGEs; MGO-derived AGEs, MGO-AGEs; GO-derived AGEs, GO-AGEs; and 3-DG-derived AGEs, 3-DG-AGEs) are present in the sera of type 2 diabetic patients on hemodialysis [21, 29-31]. Based on these findings, we proposed a pathway for the formation of distinct AGEs involving the Maillard reaction, sugar autoxidation, and sugar metabolic pathways in vivo, as shown in Fig. (1). Such receptors may play a critical role in AGEs-related biology and the pathology of diabetic vascular complications and aging disorders. Several types of AGEs binding proteins and/or receptors for AGEs such as RAGE [32-36]; oligosac-charyl transferase-48 (AGE-R1) [37]; galectin-3 (AGE-R3) [38]; CD36 [39]; macrophage scavenger receptors types 1 and 2 (MSR-1 & -2) [40]; and fasciclin EGF-like, laminin-type EGF-like, and link domain-containing scavenger receptors 1 and 2 (FEEL-1 & -2) [41] have been reported. The relative pathogenic contributions of these receptors to diabetic vascular complications are poorly defined, although RAGE is by far the best characterized, and mechanistic in vitro and in vivo studies on AGEs and their regulatory fragments such as soluble form of RAGE (sRAGE) have indicated that they play important roles in pathobiology [36, 42]. RAGE is normally expressed in a variety of cells, including endothelial cells (EC), pericytes, neurons, and microglia [32-34]. We have recently found that glycer-aldehyde rapidly reacts with the amino groups of proteins to form Glycer-AGEs both in vitro and in vivo [19, 21, 30]. Furthermore, Glycer-AGEs have the strongest binding affinity for RAGE and subsequently elicit oxidative stress generation and vascular inflammation and are therefore implicated in accelerated atherosclerosis in DM [43, 44]. Recently, we also demonstrated that Glycer-AGEs, the pre-dominant component of toxic AGEs (TAGE), play an important role in the pathogenesis of angiopathy in diabetic patients [19, 20]. Moreover, there is a growing body of evidence to suggest that the interaction of TAGE with RAGE elicits oxidative stress generation in numerous types of cells, all of which may contribute to the pathological changes associated with diabetic vascular complications [10, 19, 20]. The administration of a recombinant sRAGE consisting of its extracellular ligand-binding domain has recently been shown to not only suppress the development of atheroscle-rosis but also stabilize established atherosclerosis in diabetic apolipoprotein E-null mice [45, 46]. The blockade of the AGEs-RAGE axis by the administration of sRAGE reduces the development of acellular capillaries and pericyte ghosts in experimental diabetic retinopathy [47]. Furthermore, Kaji et al. have also shown that attenuating the RAGE axis by injecting sRAGE inhibits retinal leukostasis and blood-retinal barrier breakdown in diabetic RAGE-transgenic mice, which are accompanied by decreased expression of vascular endothelial growth factor (VEGF) and intercellular adhesion molecule 1 (ICAM-1) in the retina [48]. These observations suggest that exogenously administered sRAGE captures and eliminates circulating AGEs, thus protecting against AGEs-elicited tissue damage by acting as a decoy for AGEs.

1470 Current Drug Targets, 2010, Vol. 11, No. 11 Takeuchi et al.
PATHWAY OF GLYCER-AGES (TOXIC AGES; TAGE) FORMATION IN VIVO
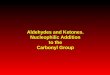
Glyceraldehyde is derived from two distinct pathways in vivo, 1) the glycolytic pathway and 2) the fructose metabo-lism pathway [19, 20, 49]. 1) The glycolytic intermediate glyceraldehyde-3-phosphate (G-3-P) is normally catabolized by the enzyme glyceraldehyde-3-phosphate dehydrogenase (GAPDH). With a decline in GAPDH activity, G-3-P accumulates intracellularly. G-3-P metabolism then shifts to another route, and the amount of glyceraldehyde is inc-reased, which leads to an increase in the formation of TAGE. This suggests a positive feedback mechanism; i.e., TAGE-induced GAPDH suppression further stimulates the gene-ration of TAGE. 2) Under hyperglycemic conditions, the increased intracellular glucose concentration stimulates the polyol pathway to generate fructose in insulin-independent tissues such as the lens and kidney, nerve tissue, brain, and red blood cells [50-52]. Furthermore, fructose, a component of table sugar and high-fructose corn syrup, is present in the daily diets of many individuals [53]. Fructose is phosphor-rylated to fructose-1-phosphate (F-1-P) and then catabolized to glyceraldehyde and dihydroxyacetone phosphate by aldolase B [52-55]. The newly synthesized glyceraldehyde is then transported or leaks passively across the plasma mem-
brane. Glyceraldehyde promotes the formation of TAGE both intracellularly and extracellularly (Fig. 2).
DIABETIC MICROVASCULAR COMPLICATIONS
The formation and accumulation of AGEs progresses at an accelerated rate in diabetes, thereby implicating it in diabetic vascular complications [10-18]. Indeed, a variety of molecular mechanisms underlying the actions of TAGE and their contribution to EC dysfunction have been proposed [10, 12, 19, 20]. TAGE-RAGE interactions have been postulated to play a role in the development and progression of microvascular disease in DM.
1) Diabetic Retinopathy
Diabetic retinopathy is one of the most important microvascular complications in DM and is a leading cause of acquired blindness among people of occupational age [56]. Hyperglycemia damages retinal microvascular cells and causes various changes in retinal tissues such as enhanced vascular permeability due to pericyte loss, followed by microvascular occlusion in the retina [57, 58]. Pericytes are elongated cells of mesodermal origin, which wrap around and along the EC of small vessels [59]. As pericytes contain
Fig. (1). Alternative routes for the formation of AGEs in vivo. Glc-AGEs, glucose-derived AGEs; Glycer-AGEs, glyceraldehyde-derived AGEs; Glycol-AGEs, glycolaldehyde-derived AGEs; MGO-AGEs, methylglyoxal (MGO)-derived AGEs; GO-AGEs, glyoxal (GO)-derived AGEs; 3-DG-AGEs, 3-deoxyglucosone (3-DG)-derived AGEs; CML, N-(carboxymethyl)lysine; P-NH2, free amino residue of protein. GOLD, GO-lysine dimmer; GA-pyridine, 3-hydroxy-4-hydroxymethyl-1-(5-carboxypentyl) pyridinium cation; DOLD, 3-DG-lysine dimmer; CEL, N-(carboxyethyl)lysine; MOLD, MGO-lysine dimmer; GLAP, glyceraldehyde derived pyridinium compound.

A Novel Therapeutic Strategy for Diabetic Complications Current Drug Targets, 2010, Vol. 11, No. 11 1471
contractile muscle filaments on their EC side, they are regarded as microvascular counterparts of smooth muscle cells and are considered to be involved in the maintenance of capillary tone [60, 61]. AGEs have been postulated to play a role in the development and progression of microvascular disease in DM. VEGF, which is also known as vascular permeability factor, is a specific mitogen to EC and is generally thought to be involved in the pathogenesis of proli-ferative diabetic retinopathy. Indeed, clinical observations have demonstrated that the VEGF level in ocular fluid is positively correlated with the amount of neovascularization in diabetic retinopathy [62, 63]. Retinal pericytes accumulate AGEs during diabetes [64], which is expected to have a detrimental effect on pericyte survival and function [65]. We have found that TAGE cause the apoptosis of retinal pericytes and induce the expression of VEGF by interacting with RAGE, indicating the invol-vement of TAGE in the pathogenesis of diabetic retinopathy, especially in the early stages [66-68]. TAGE also induce VEGF expression, DNA synthesis, and angiogenesis in EC. These changes are the hallmarks of proliferative diabetic retinopathy [69, 70]. These findings suggest that TAGE-RAGE interaction facilitates angiogenesis by two distinct
mechanisms: by relieving the restriction on EC growth caused by the apoptotic cell death of pericytes, and by autocrine and paracrine induction of VEGF proteins by vascular wall cells. Although the molecular mechanisms of the VEGF overexpression elicited by TAGE are not fully understood, our recent investigation suggested that TAGE-RAGE interaction increases VEGF gene transcription in EC by NADPH oxidase-mediated reactive oxygen species (ROS) generation and the subsequent activation of nuclear factor κB (NF-κB) via the Ras-mitogen activated protein kinase pathway [69, 70]. The abovementioned effects of TAGE strongly suggest a pathological role for these senescent macroproteins in diabe-tic vascular complications. Furthermore, Glc-AGEs and TAGE are present in human serum, and the levels of both AGEs are elevated in types 1 and 2 DM [71-74]. These AGEs, especially TAGE-epitopes, elicit angiogenesis at the concentrations present in the sera of diabetic patients. These results suggest the involvement of TAGE-epitopes in pathologic angiogenesis in vivo. Recently, we demonstrated that the vitreous levels of both TAGE and VEGF were significantly higher in diabetic patients than in control subjects and that these levels were correlated with the
Fig. (2). In vivo glyceraldehyde-derived AGEs (Glycer-AGEs) production routes. The glycolytic intermediate glyceraldehyde-3-phosphate (G-3-P) is normally catabolized by the enzyme glyceraldehyde-3-phosphate dehydrogenase (GAPDH). With a decline in GAPDH activity, G-3-P accumulates intracellularly. G-3-P metabolism then shifts to another route, and the amount of glyceraldehyde is increased, which leads to an increase in the formation of TAGE. Fructose is phosphorylated to fructose-1-phosphate (F-1-P) and then catabolized to glyceraldehyde and dihydroxyacetone phosphate by aldolase B. The newly synthesized glyceraldehyde is then transported or leaks passively across the plasma membrane. Glyceraldehyde promotes the formation of TAGE both intracellularly and extracellularly. TAGE, toxic AGEs (glyceraldehyde-derived AGEs); RAGE, receptor for AGEs; ROS, reactive oxygen species; HFCS, high-fructose corn syrup; AR, aldose reductase; SDH, sorbitol dehydrogenase; FK, fructokinase; GAPDH, glyceraldehyde-3-phosphate dehydrogenase; , TAGE.

1472 Current Drug Targets, 2010, Vol. 11, No. 11 Takeuchi et al.
severity of neovascularization in diabetic retinopathy. In addition, we also found a significant correlation between vitreous TAGE and VEGF levels [75, 76]. While many of the reported studies investigating diabetic retinopathy measured a range of ill defined AGEs moieties, others evaluated defined adducts such as CML, pentosidine, and crossline [77, 78]. However, some groups have reported that they found no correlation between AGE levels and retinopathy in diabetic patients [77, 79], although the apparent disparity between the findings of the various studies may be related to differences in the patient populations and/or the non-uniform assays used for plasma AGEs-quantification. Our studies suggest that an elevated TAGE level in DM patients is important for the initiation and prog-ression of retinopathy. Therefore, the inhibition of TAGE formation and the blockade of TAGE-RAGE interactions are potential therapeutic strategies for the prevention of diabetic retinopathy.
2) Diabetic Nephropathy
Nephropathy is one of the most common complications of DM. The disease is characterized by an increased glome-rular basement membrane thickness, a decreased glomerular filtration rate, and an expanded mesangial volume [80-82]. Diabetes-induced changes in the physical and biochemical properties of the glomerular basement membrane can result in proteinuria. However, the involvement of these changes in the development of the early phase of diabetic nephropathy has not been fully elucidated. Mesangial cells occupy a central anatomical position in the glomerulus, playing crucial roles in maintaining the structure and function of glomerular capillary tufts [83]. They also provide structural support for capillary loops and modulate glomerular filtration via smooth muscle activity [83-85]. We have found that TAGE disturb glomerular homeo-stasis by inducing apoptotic cell death in human mesangial cells. Cell growth is also strongly inhibited by TAGE. Furthermore, TAGE stimulate the secretion of VEGF and monocyte chemoattractant protein-1 (MCP-1). Hyperfiltra-tion and microalbuminuria occur subsequently, suggesting the involvement of TAGE in the pathogenesis of the early phase of diabetic nephropathy [86]. More recently, we found that the serum levels of TAGE were significantly higher in diabetic patients with nephropathy than in diabetic patients without clinically evident nephropathy (unpublished data). These results suggest that the effects of TAGE on pericytes are similar to their effects on mesangial cells, supporting the notion that attacks on vascular wall cells by TAGE are invol-ved in the early phase of diabetic vascular complications. RAGE-overexpressing diabetic mice have been found to show progressive glomerulosclerosis and renal dysfunction compared with diabetic littermates lacking the RAGE transgene [87]. Myint et al. reported that inactivation of the RAGE gene in a mouse model of diabetic nephropathy resulted in significant suppression of kidney changes, including kidney enlargement, increased glomerular cell number, mesangial expansion, advanced glomerulosclerosis, increased albuminuria, and increased serum creatinine compared with wild-type diabetic mice [88]. They also showed that low-molecular weight heparin treatment
significantly prevented albuminuria and increased glomeru-lar cell number, mesangial expansion, and glomeruloscle-rosis by antagonizing RAGE [88]. We have recently found that treatment with telmisartan or olmesartan inhibits TAGE-evoked inflammatory responses in EC via the downregu-lation of RAGE expression [89-93]. These observations suggest that the blockade of TAGE-RAGE signaling path-ways by renin-angiotensin system (RAS) inhibitors may be clinically relevant to the prevention of diabetic vascular complications.
3) Diabetic Neuropathy
DM is a major cause of peripheral neuropathy, which commonly manifests as distal symmetrical polyneuropathy [94]. In human diabetic nerves, the major pathology involves fiber loss, axonal degeneration and demyelination, and microangiopathic changes [95, 96]. The sural, peroneal, and saphenous nerves of human diabetic subjects contain AGEs in the perineurium, EC, and pericytes of endoneurial micro-vessels as well as in myelinated and unmyelinated fibers [97]. AGEs accumulation in the nerves of diabetics and the inhibition of AGEs formation by anti-glycation agents improved the neuropathic changes suffered by experimental diabetic rats [98]. However, the pathologic mechanisms behind the actions of AGEs in diabetic neuropathy are poorly understood. We investigated the effects of TAGE on the viability, replication rate, and cytokine production of cultured Schwann cells. Cell viability, replication, and the production of proinflammatory cytokines such as tumor necrosis factor-α (TNF-α) and interleukin-1β (IL-1β) were significantly affected by TAGE in Schwann cells [99]. The finding of TAGE-associated toxicity in Schwann cells is consistent with the results of previous reports investigating the effects of TAGE on other types of cells such as neuronal, vascular, and mesangial cells [66, 86, 100].
DIABETIC MACROVASCULAR COMPLICATIONS
It is well known that postchallenge and postprandial hyperglycemia are related to the development and progress-sion of diabetic macrovascular disease [101, 102]. Type 2 DM is a major risk factor for CVD morbidity and mortality, and the incidence of CVD is 2-4 times greater in diabetic patients than in the general population [103]. There is a growing body of evidence to suggest that postprandial hyper-glycemia plays an important role in the pathogenesis of CVD [104, 105]. Indeed, the Diabetes Epidemiology Collaborative Analysis of Diagnostic Criteria in Europe (DECODE) study revealed that 2-h post-load hyperglycemia was associated with an increased risk of mortality from CVD, independent of fasting plasma glucose (FPG) [101]. Furthermore, the Diabetes Intervention Study identified postprandial hyper-glycemia to be an independent risk factor for myocardial inf-arction and all-cause mortality [104]. Moreover, postprandial hyperglycemia has been shown to be associated with endo-thelial dysfunction and increased IMT as well as a higher prevalence of atherosclerotic plaques of the common carotid arteries [105]. These findings suggest that postprandial hyperglycemia would make a good a therapeutic target for preventing CVD in type 2 DM. However, there is no convenient biomarker that reflects cumulative postprandial hyperglycemia in DM.

A Novel Therapeutic Strategy for Diabetic Complications Current Drug Targets, 2010, Vol. 11, No. 11 1473
We have recently found that glyceraldehyde rapidly reacts with the amino groups of proteins to form TAGE, which causes vascular inflammation and endothelial dys-function and is therefore implicated in accelerated atherosclerosis in DM [10, 19]. More recently, we examined whether the TAGE concentration was able act as a biomarker that reflects cumulative postprandial hyperglycemia in Goto-Kakizaki (GK) rats, a rat model of type 2 DM, that were fed twice a day [106]. At 8 weeks of age, the GK rats were divided into 2 groups: either the vehicle or 50 mg/kg of nateglinide, a rapid-acting insulin secretagogue, was admi-nistered twice daily just before each meal. After 6 weeks, nateglinide treatment was found to not only prevent post-prandial hyperglycemia, but also reduce TAGE levels in the GK rats. However, there was no significant difference in HbA1c or Glc-AGE levels between the two groups. The pre-sent study demonstrated for the first time that TAGE, but not HbA1c or Glc-AGEs, can be used as biomarkers that reflect cumulative postprandial hyperglycemia in diabetic rats. This may partly explain why decreased HbA1c levels did not lead to a significant reduction in the risk of CVD in the UKPDS, thus further strengthening the importance of identi-fying a biomarker that reflects cumulative postprandial hyperglycemia in DM [107]. Since TAGE have the strongest binding affinity for RAGE [43, 44] and exert deleterious effects on diabetic vessels through their interaction with RAGE [10, 19, 20], TAGE may partly account for the increased risk of CVD in diabetic and impaired glucose tolerant patients with postprandial hyperglycemia. Taken together, our present study also suggests that TAGE are a novel therapeutic target for preventing CVD in DM patients [106]. Furthermore, we have recently found that serum TAGE levels are positively correlated with the levels of thrombo-genic markers in humans. plasminogen activator inhibitor-1 (PAI-1) and fibrinogen levels are positively associated with serum TAGE levels [108]. These results suggest the rele-vance of TAGE-epitopes to pathologic angiogenesis and thrombogenesis in humans.
THERAPEUTIC AGENTS THAT COULD BLOCK THE TAGE-RAGE AXIS
Several therapeutic strategies such as the inhibition of TAGE formation, the blockade of TAGE-RAGE interact-tions, and the suppression of RAGE expression or its downstream pathways are promising for the treatment of vascular complications in DM.
1) Pimagedine
Double-blinded, placebo-controlled, randomized clinical trials of aminoguanidine (AG, Pimagedine) (ACTION; A Clinical Trial In Overt Nephropathy) were designed to evaluate the safety and efficacy of AG in retarding the rate of progression of renal disease in patients with overt diabetic nephropathy. Pimagedine therapy reduced 24-hour total urinary proteinuria and prevented decreases in the glomerular filtration rate in patients with type 1 diabetes [109]. In addition, compared with those receiving placebo, fewer pimagedine-treated patients experienced a three-step or greater progression of diabetic retinopathy [109].
However, the effects of pimagedine on serum creatinine doubling were not significant; serum creatinine doubled in 26% of the placebo-treated patients and in 20% of those who received pimagedine (p=0.099). This study is noteworthy as it provides the first clinical proof that inhibiting AGE formation can result in a clinically important attenuation of the serious complications of diabetes. However, as the reported side effects of AG in clinical therapy included gastrointestinal disturbance; abnormalities in liver function tests; flu-like symptoms; and the development of anti-nuclear antibody, pernicious-like anemia, and a rare form of vasculitis [109], further clinical trials of AG were terminated due to safety concerns.
2) Inhibition of TAGE Formation
Although many agents improve overall glycemic control, including postprandial plasma glucose levels, several phar-macologic therapies specifically target postprandial hyper-glycemia. More recently, we investigated the effects of nateglinide, which has been shown to improve postprandial hypergly-cemia, on HbA1c, Glc-AGE, and TAGE levels in GK rats [106]. After 6 weeks, nateglinide treatment was found to not only prevent postprandial hyperglycemia, but to also reduce TAGE levels in GK rats. However, there were no significant differences in HbA1c or Glc-AGE levels [106]. This study suggests that TAGE are formed more rapidly than HbA1c, a precursor of Glc-AGEs, under postprandial hyperglycemic conditions and show potential as novel markers of cumu-lative postprandial hyperglycemia. In this study, although we did not clarify the exact molecular mechanism by which TAGE were formed under postprandial hyperglycemic con-ditions, hyperglycemia-induced oxidative stress-mediated inhibition of GAPDH may lead to the elevation of glycer-aldehyde levels and subsequently enhance the formation of TAGE during the postprandial period [110]. The relative contribution of postprandial glucose decreased progressively from the lowest to the highest quintile of HbA1c; whereas, the relative contribution of fasting glucose increased gradually with increasing levels of HbA1c [111]. These observations suggest that a decrease in HbA1c levels does not necessarily reflect a reduction in postprandial hypergly-cemia, especially in poorly controlled diabetic patients. Acarbose, an α-glucosidase inhibitor, which delays the absorption of carbohydrates from the small intestine, reduces postprandial hyperglycemia in patients with type 2 DM [112]. Recently, acarbose treatment was reported to slow the progression of IMT of the carotid arteries and to reduce the incidence of CVD in patients with impaired glucose tolerance or type 2 DM [112], thus suggesting that acarbose treatment inhibits the development and progression of CVD by suppressing postprandial hyperglycemia. We have previously shown that glyceraldehyde reacts rapidly with the amino groups of proteins to form TAGE in vivo, which evoke vascular inflammation and oxidative stress generation, thereby implicating them in accelerated atherosclerosis in DM [10, 19, 20]. Furthermore, we recently found that the serum levels of TAGE rather than HbA1c reflect cumulative postprandial hyperglycemia in type 2 diabetic rats [106]. These observations led us to speculate

1474 Current Drug Targets, 2010, Vol. 11, No. 11 Takeuchi et al.
that acarbose treatment reduces the serum levels of TAGE, which may contribute to its cardioprotective properties in vivo. Thirteen oral hypoglycemic agent (OHA)-naive Japanese type 2 diabetic patients without microangiopathy, coronary artery disease, or any active inflammatory disease were enrolled in this study. The patients were treated with 50 mg acarbose three times a day for 12 weeks. Their TAGE levels and those of other biochemicals were measured before and after treatment with acarbose [113]. After 12 weeks, acarbose treatment was found to have significantly reduced the TAGE and free fatty acid levels of the diabetic patients. Acarbose treatment also decreased their postprandial plasma glucose (PPG) levels, but its effects on PPG were not statistically significant because of the high variability in the data and the small number of subjects enrolled in the study. Acarbose did not affect other anthropometric or metabolic variables; i.e., there were no significant differences in body mass index, blood pressure, HbA1c, FPG, or lipid parameters between before and after treatment with acarbose. This study demonstrated for the first time that acarbose treatment reduced the serum levels of TAGE in OHA-naive type 2 diabetic patients [113]. Our observations suggest that HbA1c levels do not necessarily reflect reductions in postprandial hyperglycemia by acarbose and that TAGE levels may be a biomarker that reflects cumulative postprandial hypergly-cemia in type 2 DM. Given the deleterious effects of TAGE on CVD [10, 20], the reduction of TAGE concentrations by acarbose is a novel therapeutic strategy for preventing CVD in patients with type 2 DM.
3) Blocker of the TAGE-RAGE Interaction: the Soluble Form of RAGE
Recently, endogenous sRAGE has been identified in humans [43]. Endogenous sRAGE may be generated from the cleavage of cell surface full-length RAGE or novel splice variants of RAGE (the C-truncated splice isoform of secretory RAGE, esRAGE) [43]. Endogenous total sRAGE levels are elevated in patients with types 1 and 2 DM [114-117]. Furthermore, we, along with others, have recently demonstrated that total serum sRAGE levels are positively, rather than inversely, associated with TAGE levels in both non-diabetic and diabetic subjects [117, 118]. Age-, sex-, and body mass index-adjusted TAGE levels are also significantly increased in proportion to the increased level of sRAGE in non-diabetic subjects [117, 118]. These findings suggest that the sRAGE pool is not able to efficiently capture and eliminate the circulating TAGE in vivo by acting as a decoy receptor. Since TAGE is a positive regulator of the expression of RAGE, circulating sRAGE levels may reflect RAGE expression at the tissue level and be elevated in parallel with serum TAGE levels as a counter-system against TAGE-elicited tissue damage [119-122]. The serum levels of esRAGE are also correlated with the levels of circulating AGEs such as CML and pentosidine in type 1 DM patients [123]. However, in contrast to the case for total sRAGE, circulating esRAGE levels are decreased, rather than increased, in both type 1 and 2 diabetic patients. Katakami et al. reported that the serum levels of esRAGE were significantly decreased in Japanese patients with type 1 DM compared with those in non-diabetic subjects [124] and that esRAGE levels were significantly lower in type 1
diabetic patients with retinopathy than in those without retinopathy [124, 125]. Decreased esRAGE levels were also found to be an independent risk factor for carotid atherosclerosis [126]. Indeed, Koyama et al. reported that esRAGE levels were decreased in Japanese type 2 diabetic patients compared with non-diabetic subjects and that low levels of esRAGE were associated with the components of metabolic syndrome and carotid atherosclerosis [126]. These observations were contrary to the findings of previous reports that demonstrated that total sRAGE levels were associated with conventional coronary risk factors including inflammatory markers and were independent determinants of coronary artery disease in DM [115, 119, 120]. Therefore, the kinetics and role of sRAGE and esRAGE in DM may differ [121]. Decreased levels of esRAGE may be associated with comorbidities such as diabetic retinopathy and athero-sclerosis via mechanisms other than acting as a decoy because esRAGE levels are approximately 3~4-fold lower than total sRAGE levels and may not be sufficient to efficiently eliminate circulating AGEs in humans. Further-more, sRAGE, but not esRAGE, levels were recently found to be independently correlated with albuminuria in type 2 diabetic patients [127]. On the contrary, other groups have found that total sRAGE levels were inversely correlated with ligand concentrations [128]. Basta et al. recently reported that total plasma sRAGE levels were decreased in diabetic patients. In a subgroup of 26 diabetic and 24 non-diabetic subjects of similar age, they found that total sRAGE levels were inversely associated with the level of S100A12, a non-AGEs ligand for RAGE and that low sRAGE and high S100A12 concentrations were strongly associated with an increased risk of CVD [128]. There is still some controversy over the therapeutic modulation of sRAGE. Forbes et al. reported that treatment with ramipril, an angiotensin-converting enzyme inhibitor (ACEI), restored the decreased plasma levels of total sRAGE in diabetic rats [129]. Similarly, they also found that there was a significant increase in total plasma sRAGE levels in patients who had type 1 DM and were treated with the ACEI perindopril [129]. Nakamura et al. reported that telmisartan, an angiotensin II type 1 receptor blocker (ARB), inhibited sRAGE generation by angiotensin-II-exposed EC and decreased the serum levels of total sRAGE in patients with essential hypertension [130].
4) Inhibitors of the Renin-Angiotensin System (RAS)
The interaction of the RAS and TAGE-RAGE systems has also been proposed. We have found that angiotensin II potentiates the deleterious effects of TAGE in pericytes by inducing RAGE protein expression [68]. In vivo, TAGE-injection stimulated RAGE expression in the eyes of spontaneously hypertensive rats, which was blocked by telmisartan. In vitro, angiotensin II-type 1 receptor-mediated ROS generation elicited RAGE gene expression in retinal pericytes through NF-κB activation. Furthermore, angio-tensin II augmented TAGE-induced pericyte apoptosis, the earliest hallmark of diabetic retinopathy. Telmisartan also blocks angiotensin II-induced RAGE expression in EC [130].

A Novel Therapeutic Strategy for Diabetic Complications Current Drug Targets, 2010, Vol. 11, No. 11 1475
Recently, there has been increasing interest in the role of inflammatory reactions and immune phenomena in the pathogenesis of diabetic vascular complications [131-133]. Indeed, leukocyte adhesion to diabetic retinal vasculature is considered to be a critical early event in diabetic retinopathy, the development of which is mainly mediated by VEGF, ICAM-1, and MCP-1 expression [131-133]. ICAM-1 and MCP-1 are essential chemokines that mediate the recruit-ment of leukocytes to mesangial lesions [134, 135]. The selective targeting of ICAM-1 or MCP-1 was also shown to markedly decrease albuminuria and renal injury in experimental diabetic nephropathy [134, 135]. Furthermore, several experimental studies have supported the pathological role of VEGF in diabetic nephropathy: antibodies raised against VEGF have been reported to improve hyperfiltration and albuminuria in diabetic rats [136, 137]. In addition, atherosclerosis is also an inflammatory-proliferative disease [138], and the administration of VEGF is reported to enhance atherosclerotic plaque progression in animals [139]. We have recently found that treatment with telmisartan or olmesartan inhibits TAGE-evoked inflammatory responses in EC via the downregulation of RAGE expression [89-93]. These observations suggest that the blockade of the TAGE-RAGE signaling pathways by RAS inhibitors is clinically relevant to the prevention of diabetic vascular complications. As for the underlying molecular mechanisms, telmisartan may downregulate RAGE expression through its unique peroxisome proliferator-activated receptor-γ (PPAR-γ)-modulating ability on the basis of the following observations [89-91]: (1) telmisartan downregulated RAGE mRNA levels and subsequently inhibited superoxide generation as well as MCP-1 expression in mesangial cells, all of which were prevented by GW9662, an inhibitor of PPAR-γ [90]; (2) another ARB, candesartan, did not suppress TAGE-induced superoxide generation in mesangial cells; (3) the antioxidant N-acetylcysteine (NAC) inhibited MCP-1 production by TAGE-exposed mesangial cells; (4) telmisartan, but not candesartan, decreased TAGE-induced RAGE expression, ROS generation, and the subsequent C-reactive protein (CRP) expression in human Hep3B hepatoma cells [91]; (5) GW9662 also blocked the inhibitory effects of telmisartan on RAGE expression and its downstream signaling in Hep3B cells; (6) troglitazone and ciglitazone, full agonists of PPAR-γ, mimicked the effects of telmisartan on Hep3B cells; and (7) treatment with anti-oxidants or curcumin, an inhibitor of NF-κB, blocked the TAGE-induced upregulation of CRP mRNA levels in Hep3B cells. There is accumulating evi-dence to suggest that telmisartan is a promising cardiometa-bolic sartan due to its unique PPARγ-modulating ability [89, 140]. Furthermore, thiazolidinediones have been reported to reduce the endothelial expression of RAGE via NF-κB sup-pression [141]. Taken together, these observations suggest that telmisartan works as an anti-inflammatory agent against TAGE-signaling by suppressing RAGE expression in EC, mesangial cells, and the liver via PPAR-γ activation and that it plays a protective role against diabetic vascular compli-cations by limiting the susceptibility of these cells to pro-inflammatory TAGE effects. We should also describe other possible mechanisms by which RAS inhibitors such as ARB and ACEI suppress the TAGE-RAGE system. ACEI and ARB were recently found to inhibit the formation of reactive carbonyl precursors of
AGEs in vitro by chelating transition metals and inhibiting various oxidative steps, including the formation of carbon-centered and hydroxyl radicals, at both the pre- and post-Amadori steps [142]. In animal models, the ACEI ramipril also reduced the accumulation of renal and serum AGEs, probably via effects on oxidative pathways [143]. Long-term treatment with the ARB losartan seemed to exert salutary effects on AGE levels in a rat remnant kidney model, probably by improving renal function [144]. Furthermore, candesartan, another ARB, reduced AGEs accumulation and the subsequent albuminuria by downregulating the expres-sion of the NADPH oxidase component p47phox and inducible nitric oxide synthase (iNOS) and by attenuating RAGE expression in type 2 diabetic KK/Tα mouse kidneys [145]. In addition, the infusion of AGEs into rats induced tubular and glomerular hypertrophy and AGEs accumulation, which were antagonized by valsartan [146]. The administration of olmesartan medoxomil was found to inhibit increases in systolic and diastolic blood pressure and urinary N-acetyl-beta-D-glucosaminidase activity in exogenous TAGE-injec-ted rats [147], and olmesartan medoxomil treatment pre-vented glomerulosclerosis in TAGE-treated rats [147]. In humans, the administration of ramipril has recently been shown to result in a mild decline in the concentrations of fluorescent non-CML-AGEs and malondialdehyde in non-diabetic nephropathy patients [148]. In type 2 diabetic subjects, low-dose valsartan treatment was reported to decrease serum TAGE levels in a blood pressure-independent manner [149].
5) Nifedipine, a Dihydropyridine-Based Calcium Channel Blocker We have recently found that nifedipine inhibits RAGE expression in TAGE-exposed EC by suppressing ROS generation [150]. Therefore, the blockade of RAGE expres-sion by nifedipine may have therapeutic potential for the treatment of patients with CVD in DM. Furthermore, nifedipine also inhibits TAGE-induced MCP-1 expression in human cultured mesangial cells [151]. Since diphenylene iodonium, an inhibitor of NADPH oxidase, was found to mimic the effects of nifedipine, nifedipine may prevent MCP-1 expression-related AGEs-signaling in mesangial cells, probably by suppressing NADPH oxidase activity. We have previously found that nifedipine inhibited TNF-α-induced MCP-1 expression in EC by blocking NADPH oxidase-mediated ROS generation [152], further supporting the concept that NADPH oxidase is a molecular target of nifedipine in TAGE-exposed mesangial cells. The redox-sensitive transcription factor NF-κB modulates the gene expression of pro-inflammatory chemokines such as MCP-1, thus playing a central role in the pathogenesis of diabetic nephropathy [153]. Therefore, it is conceivable that nifedi-pine decreases TAGE-elicited MCP-1 overexpression in mesangial cells by inhibiting ROS generation as well as reducing the subsequent NF-κB activation by suppressing NADPH oxidase activity.
6) Pigment-Epithelium-Derived Factor (PEDF) PEDF is a glycoprotein that belongs to a superfamily of serine protease inhibitors with complex neurotrophic, neuro-protective, anti-angiogenic, anti-oxidative, and anti-inflam-matory properties, any of which could potentially be exploit-

1476 Current Drug Targets, 2010, Vol. 11, No. 11 Takeuchi et al.
ed as a therapeutic option for the treatment of vascular com-plications in DM [154, 155]. PEDF inhibits TAGE-induced ROS generation and subsequently prevents apoptotic cell death in pericytes by restoring downregulation of the gene expression of the anti-apoptotic factor bcl-2 [156]. Furthermore, PEDF also inhibits TAGE-induced ICAM-1, VEGF, and MCP-1 upregulation as well as NO suppression in EC by blocking NADPH oxidase-mediated ROS gene-ration [157-162]. In vivo, the administration of PEDF or pyridoxal phosphate, an AGEs inhibitor, decreased the retinal levels of 8-hydroxydeoxyguanosine (8-OHdG), an oxidative stress marker, and subsequently suppressed ICAM-1 gene expression and retinal leukostasis in diabetic rats [163]. Moreover, intravenous administration of TAGE to normal rats increased ICAM-1 gene expression and retinal leukostasis, which were blocked by PEDF [163]. PEDF also inhibited diabetes- or TAGE-induced RAGE gene expression by blocking superoxide-mediated NF-κB activation [164]. In addition, we have recently found that intravenous adminis-tration of TAGE to normal rats not only increased retinal vascular permeability by stimulating VEGF expression, but also decreased retinal PEDF levels [165]. Simultaneous treatment with PEDF inhibited TAGE-elicited VEGF-mediated permeability by downregulating the mRNA levels of p22phox and gp91phox, membrane components of NADPH oxidase, and subsequently decreasing the retinal levels of the oxidative stress marker 8-OHdG. PEDF also inhibited TAGE-induced vascular hyperpermeability (as measured by transendothelial electrical resistance) by suppressing VEGF expression and decreased ROS generation in TAGE-exposed EC by suppressing NADPH oxidase activity via the down-regulation of p22phox and gp91phox mRNA expression. This led to blockade of TAGE-elicited Ras activation and NF-κB-dependent VEGF gene induction in EC. These results indicate that the central mechanism of PEDF inhibition of vascular permeability-related TAGE-signaling is the sup-pression of NADPH oxidase-mediated ROS generation and subsequent VEGF expression [165]. The PEDF levels in the aqueous humor and vitreous are decreased in diabetic patients, especially in those with proliferative retinopathy, suggesting that loss of PEDF in the eye contributes to the pathogenesis of proliferative diabetic retinopathy [166, 167]. We have also found significantly higher vitreous levels of TAGE and VEGF in diabetic patients than in control subjects [75] as well as a significant correlation between vitreous TAGE and VEGF levels. Total anti-oxidant status was also decreased in the vitreous in patients with diabetes. Furthermore, both TAGE and VEGF levels (inversely) and the PEDF level (positively) were associated with the total anti-oxidant status of the vitreous [168, 169]. These observations further support the concept that PEDF is an endogenous anti-inflammatory and anti-oxidative agent that blocks the TAGE-VEGF axis, thereby protecting against the progression of diabetic retinopathy.
7) Statins and Bisphosphonates
We have found that protein prenylation is crucial for TAGE-RAGE signaling in EC [69, 70]. Cerivastatin com-pletely prevented the TAGE-induced increases in NF-κB activity and VEGF expression and the resultant increases in DNA synthesis and tube formation in microvascular EC
[70]. Since mevalonate blocked the growth-inhibitory effects of cerivastatin on TAGE-exposed EC and that FTI-276, an inhibitor of farnesyltransferase, mimicked the effects of cerivastatin, cerivastatin may block TAGE-RAGE signaling involved in vascular hyperpermeability and angiogenesis via the suppression of protein prenylation. Furthermore, we have recently found that atorvastatin dose-dependently inhibited TAGE-induced ROS generation in Hep3B cells [170]. Atorvastatin as well as the anti-oxidant NAC was found to suppress CRP expression in TAGE-exposed Hep3B cells at both the mRNA and protein levels [170]. These results dem-onstrate that atorvastatin is able to block CRP expression-associated TAGE-signaling through its anti-oxidative action. Taken together, these observations suggest that statins have vasculoprotective effects and act by inhibiting the deleterious effects of TAGE via the suppression of their downstream signaling. Bisphosphonates are potent inhibitors of bone resorption and are widely used for the treatment of osteoporosis, osteolytic bone metastasis, and tumor-associated hypercal-cemia [171-173]. These compounds have a high affinity for calcium ions and therefore target bone mineral, where they are internalized by bone-resorbing osteoclasts and inhibit osteoclast function. Recently, farnesyl pyrophosphate syn-thase has been shown to be a molecular target of nitrogen-containing bisphosphonates such as incardronate disodium and minodronate, and the inhibition of the post-translational prenylation of small molecular weight G proteins including Ras and Rac-1 is probably involved in their anti-resorptive activity in osteoclasts [171-173]. Since the protein preny-lation of GTP-binding proteins is associated with various cellular functions such as cell growth and differentiation [171-173], nitrogen-containing bisphosphonates may exert pleiotropic effects by blocking the synthesis of isoprenoid intermediates. Indeed, incardronate disodium was found to inhibit TAGE-induced increases in NF-κB activity and VEGF expression as well as the proliferation and tube formation of EC [69]. Furthermore, we have recently found that minodronate inhibits TAGE-induced NF-κB activation and subsequently suppresses VCAM-1 gene expression by reducing ROS generation in EC [171]. In addition, geranyl-geranyl pyrophosphate reversed the anti-oxidative properties of minodronate in TAGE-exposed EC [171]. Taken together, these findings suggest that nitrogen-containing bisphos-phonates are able to inhibit TAGE-elicited inflammatory-proliferative changes in EC by suppressing NADPH oxidase-derived ROS generation, probably via the inhibition of the geranylgeranylation of Rac-1, a component of endothelial NADPH oxidase [172, 173].
8) Kremezin
Recently, dietary AGEs were reported to induce oxida-tive stress and promote inflammatory signals [174]. Heat processing of foods containing sugars and proteins may generate AGEs [174]. Nutrient composition, temperature, and the method of cooking can affect the formation of AGEs in food. Recent human studies have revealed that approxi-mately 10% of dietary AGEs were absorbed, two-thirds of which remained in the body, and only one-third of which was excreted in urine within 2 days of ingestion [175]. In diabetic patients, especially those with advanced renal

A Novel Therapeutic Strategy for Diabetic Complications Current Drug Targets, 2010, Vol. 11, No. 11 1477
disease, the urinary elimination of absorbed dietary AGEs is markedly impaired, and the elevation of serum AGEs persists for longer than 48 h post-ingestion [175]. These observations suggest that dietary AGEs play a role in the pathogenesis of vascular complications in DM and that inhibiting the absorption of dietary AGEs may be a therapeutic target for treating these devastating disorders. More recently, we have demonstrated that hepatic RAGE and VEGF expression were increased in rats administered Glc-AGE-rich beverages, indicating a novel association of dietary AGEs with the hepatic expression of genes closely related to liver fibrosis [176]. Furthermore, immunohistoche-mical analysis detected Glc-AGEs- and TAGE-positive cells in the livers of the Glc-AGE-rich beverage-administered rats [176]. These results suggest that Glc-AGE-rich beverages increase hepatic RAGE and VEGF expression as well as Glc-AGEs and TAGE accumulation, bringing about TAGE-RAGE interactions. The Glc-AGEs content of foods should be taken into consideration for disease prevention, parti-cularly in individuals at a high risk of developing DM, CVD, or chronic kidney disease (CKD). Kremezin, a prominent oral adsorbent that consists of porous spherical carbonic particles, attenuates the progres-
sion of chronic renal failure (CRF) by removing uremic toxins such as precursors of indoxyl sulfate from the intestine [177]. Indeed, Kremezin shows a superior adsorp-tion ability to activated charcoal for certain organic compounds (uremic toxins) that are known to be precursors of substances that accumulate in patients with CKD and are believed to accelerate the decline in kidney function [177]. Kremezin is approved in Japan as a treatment for prolonging the time to hemodialysis therapy and improving uremic symptoms in patients with CKD. Kremezin is also reported to reduce carotid IMT and arterial stiffness, a surrogate marker of atherosclerosis, in CRF patients before dialysis [178]. Furthermore, recent multicenter and randomized trials have revealed that 12 weeks Kremezin treatment (9 g/day) was well tolerated and did not adversely affect the general status of patients with CKD [179]. Since AGEs represent an important class of uremic toxins and that, as described above, dietary AGEs may play an important role in atherogenesis, we investigated whether Kremezin treatment was able to decrease the serum levels of AGEs in non-diabetic CRF patients. The administration of Kremezin (6 g/day) for 3 months significantly decreased the serum levels of Glc-AGEs and TAGE in non-diabetic CRF patients; whereas, both AGE levels remained unchanged in age- and
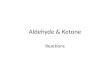
Fig. (3). The TAGE-RAGE-oxidative stress system and related therapeutic interventions against the development and progression of diabetic micro- and macrovascular complications. There is a growing body of evidence to suggest that the interaction of TAGE with RAGE alters intracellular signaling, gene expression, and the release of pro-inflammatory molecules and elicits oxidative stress generation in numerous types of cells, all of which may contribute to the pathological changes associated with diabetic vascular complications. Since TAGE have the strongest binding affinities for RAGE and exert deleterious effects on diabetic vessels through their interaction with RAGE, TAGE may partly account for the increased risk of cardiovascular disease (CVD) in diabetic and impaired glucose tolerance (IGT) patients with postprandial hyperglycemia. Glc-AGE-rich beverages increase hepatic RAGE and VEGF expression as well as the accumulation of Glc-AGEs and TAGE, bringing about TAGE-RAGE interactions. The Glc-AGEs content in foods should be taken into consideration for disease prevention, particularly in individuals at high risk of developing DM, CVD, or chronic kidney disease (CKD). Taken together, our present study also suggests that TAGE are novel therapeutic targets for preventing CVD in DM patients. Therefore, the inhibition of TAGE formation, blockade of TAGE-RAGE interactions, and the suppression of RAGE expression or its downstream pathways are promising targets for therapeutic interventions against diabetic vascular complications. TAGE, toxic AGEs; RAGE, receptor for AGEs; PEDF, pigment-epithelium-derived factor.

1478 Current Drug Targets, 2010, Vol. 11, No. 11 Takeuchi et al.
renal function-matched CRF patients who were not treated with Kremezin [180]. In addition, the patient sera obtained after Kremezin treatment showed significantly reduced mRNA levels of RAGE, MCP-1, and VCAM-1 in EC compared with the sera collected before treatment. These findings suggest that the renoprotective and anti-atheroscle-rotic properties of Kremezin can be ascribed, at least in part, to its AGEs-lowering effects mediated via the inhibition of dietary Glc-AGEs absorption and that the inhibition of dietary AGEs absorption by Kremezin is a promising therapeutic strategy for the treatment of vascular com-plications in DM.
CONCLUSION
Two recent large prospective clinical studies, DCCT and UKPDS, have shown that intensive blood glucose control effectively reduces vascular complications among patients with DM [181, 107]. However, strict control of hyper-glycemia is often very difficult to maintain and may increase the risk of severe hypoglycemia in diabetic patients. There is accumulating evidence that the TAGE-RAGE-oxidative stress system is actively involved in the pathogenesis of diabetic vascular complications. Inhibition of TAGE formation, blockade of TAGE-RAGE interactions, and the suppression of RAGE expression or its downstream pathways by the agents discussed here are promising novel therapeutic strategies for the treatment of patients with diabetic vascular complications (Fig. 3) [69, 70, 74, 106, 113, 130, 147, 150, 156, 157, 170, 171, 174, 176, 180]. Further clinical studies are needed to clarify whether the use of these agents reduces the risk of diabetic vascular complications beyond blood glucose-, blood pressure-, or cholesterol-lowering effects.
ACKNOWLEDGEMENTS
This work was supported in part by grants from the Japan Society for the Promotion of Science (Grant-in-Aid for Scientific Research (B)).
REFERENCES [1] Laakso M. Hyperglycemia and cardiovascular disease in type 2
diabetes. Diabetes 1999; 48: 937-42. [2] Nishikawa T, Edelstein D, Du XL, et al. Normalizing
mitochondrial superoxide production blocks three pathways of hyperglycemic damage. Nature 2000; 404: 787-90.
[3] Brownlee M. Biochemistry and molecular cell biology of diabetic complications. Nature 2001; 414: 813-20.
[4] The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications research group. Retinopathy and nephropathy in patients with type 1 diabetes four years after a trial of intensive therapy. N Engl J Med 2000; 342: 381-9.
[5] Writing team for the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications research group. Sustained effect of intensive treatment of type 1 diabetes mellitus on development and progression of diabetic nephropathy: the Epidemiology of Diabetes Interventions and Complications (EDIC) Study. JAMA 2003; 290: 2159-67.
[6] Nathan DM, Cleary PA, Backlund JY, et al. Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study research group, Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med 2005; 353: 2643-53.
[7] Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008; 359: 1577-89.
[8] Brownlee M, Cerami A, Vlassara H. Advanced glycosylation end products in tissue and the biochemical basis of diabetic complications. N Engl J Med 1998; 318: 1315-21.
[9] Dyer DG, Blackledge JA, Thorpe SR, Baynes JW. Formation of pentosidine during nonenzymatic browning of proteins by glucose. Identification of glucose and other carbohydrates as possible precursors of pentosidine in vivo. J Biol Chem 1991; 266: 11654-60.
[10] Yamagishi S, Imaizumi T. Diabetic vascular complications: pathophysiology, biochemical basis and potential therapeutic strategy. Curr Pharm Des 2005; 11: 2279-99.
[11] Rahbar S, Figarola JL. Novel inhibitors of advanced glycation endproducts. Arch Biochem Biophys 2003; 419: 63-79.
[12] Yamagishi S, Takeuchi M, Inagaki Y, Nakamura K, Imaizumi T. Role of advanced glycation end products (AGEs) and their receptor (RAGE) in the pathogenesis of diabetic microangiopathy. Int J Clin Pharmacol Res 2003; 23: 129-34.
[13] Vlassara H, Palace MR. Diabetes and advanced glycation endproducts. J Intern Med 2002; 251: 87-101.
[14] Bierhaus A, Hofmann MA, Ziegler R, Nawroth PP. AGEs and their interaction with AGE-receptors in vascular disease and diabetes mellitus. I. The AGE concept. Cardiovasc Res 1998; 37: 586-600.
[15] Wendt T, Bucciarelli L, Qu W, et al. Receptor for advanced glycation endproducts (RAGE) and vascular inflammation: insights into the pathogenesis of macrovascular complications in diabetes. Curr Atheroscler Rep 2002; 4: 228-37.
[16] Schmidt AM, Stern D. Atherosclerosis and diabetes: the RAGE connection. Curr Atheroscler Rep 2000; 2: 430-6.
[17] Stitt AW, Bucala R, Vlassara H. Atherogenesis and advanced glycation: promotion, progression, and prevention. Ann N Y Acad Sci 1997; 811: 115-27.
[18] Takenaka K, Yamagishi S, Matsui T, Nakamura K, Imaizumi T. Role of advanced glycation end products (AGEs) in thrombogenic abnormalities in diabetes. Curr Neurovasc Res 2006; 3: 73-7.
[19] Sato T, Iwaki M, Shimogaito N, Wu X, Yamagishi S, Takeuchi M. TAGE (toxic AGEs) theory in diabetic complications. Curr Mol Med 2006; 6: 351-8.
[20] Takeuchi M, Yamagishi S. Involvement of toxic AGEs (TAGE) in the pathogenesisi of diabetic vascular complications and Alzheimer’s Disease. J Alzheimer Dis 2009; 16: 845-58.
[21] Takeuchi M, Makita Z. Alternative routes for the formation of immunochemically distinct advanced glycation end-products in vivo. Curr Mol Med 2001; 1: 305-15.
[22] Bucala R, Cerami A. Advanced glycosylation: chemistry, biology, and implications for diabetes and aging. Adv Pharmacol 1992; 23: 1-34.
[23] Vlassara H, Bucala R, Striker L. Pathogenic effects of advanced glycosylation: biochemical, biologic, and clinical implications for diabetes and aging. Lab Invest 1994; 70: 138-51.
[24] Brownlee M. Advanced protein glycosylation in diabetes and aging. Ann Rev Med 1995; 46: 223-34.
[25] Monnier VM, Cerami A. Non-enzymatic browning in vivo: possible process for aging of long-lived proteins. Science 1981; 211: 491-3.
[26] Wells-Knecht KJ, Zyzak DV, Litchfield JE, Thorpe SR, Baynes JW. Mechanism of autoxidative glycosylation: identification of glyoxal and arabinose as intermediates in the autoxidative modification of proteins by glucose. Biochemistry 1995; 34: 3702-9.
[27] Thornalley PJ. Pharmacology of methylglyoxal: formation, modification of proteins and nucleic acids, and enzymatic detoxification--A role in pathogenesis and antiproliferative chemotherapy. Gen Pharmacol 1996; 27: 565-73.
[28] Thornalley PJ, Langborg A, Minhas HS. Formation of glyoxal, methylglyoxal and 3-deoxyglucosone in the glycation of proteins by glucose. Biochem J 1999; 344: 109-16.
[29] Takeuchi M, Makita Z, Yanagisawa K, Kameda Y, Koike T. Detection of non-carboxymethyllysine and carboxymethyllysine advanced glycation end products (AGE) in serum of diabetic patients. Mol Med 1999; 5: 393-405.

A Novel Therapeutic Strategy for Diabetic Complications Current Drug Targets, 2010, Vol. 11, No. 11 1479
[30] Takeuchi M, Makita Z, Bucala R, Suzuki T, Koike T, Kameda Y. Immunological evidence that non-carboxymethyllysine advanced glycation end-products are produced from short chain sugars and dicarbonyl compounds in vivo. Mol Med 2000; 6: 114-25.
[31] Takeuchi M, Yanase Y, Matsuura N, et al. Immunological detection of a novel advanced glycation end-product. Mol Med 2001; 7: 783-91.
[32] Yan SD, Chen X, Fu J, et al. RAGE and amyloid-β peptide neurotoxicity in Alzheimer's disease. Nature 1996; 382: 685-91.
[33] Schmidt AM, Yan SD, Yan SF, Stern DM. The biology of the receptor for advanced glycation end products and its ligands. Biochim Biophys Acta 2000; 1498: 99-111.
[34] Bucciarelli LG, Wendt T, Rong L, et al. RAGE is a multiligand receptor of the immunoglobulin superfamily: implications for homeostasis and chronic disease. Cell Mol Life Sci 2002; 59: 1117-28.
[35] Hudson BI, Bucciarelli LG, Wendt T, et al. Blockade of receptor for advanced glycation endproducts: a new target for therapeutic intervention in diabetic complications and inflammatory disorders. Arch Biochem Biophys 2003; 419: 80-8.
[36] Ramasamy R, Vannucci SJ, Yan SS, Herold K, Yan SF, Schmidt AM. Advanced glycation end products and RAGE: a common thread in aging, diabetes, neurodegeneration, and inflammation. Glycobiology 2005; 15: 16R-28R.
[37] Li YM, Mitsuhashi T, Wojciechowicz D, et al. Molecular identity and cellular distribution of advanced glycation endproduct receptors: relationship of p60 to OST-48 and p90 to 80K-H membrane proteins. Proc Nat Acad Sci USA 1996; 93: 11047-52.
[38] Vlassara H, Li YM, Imani F, et al. Identification of galectin-3 as a high-affinity binding protein for advanced glycation end products (AGE): a new member of the AGE-receptor complex. Mol Med 1995; 1: 634-46.
[39] Ohgami N, Nagai R, Ikemoto M, et al. CD36, serves as a receptor for advanced glycation endproducts (AGE). J Diabetes Complications 2002; 16: 56-9.
[40] el Khoury J, Thomas CA, Loike JD, Hickman SE, Cao L, Silverstein SC. Macrophages adhere to glucose-modified basement membrane collagen IV via their scavenger receptors. J Biol Chem 1994; 269: 10197-200.
[41] Tamura Y, Adachi H, Osuga J, et al. FEEL-1 and FEEL-2 are endocytic receptors for advanced glycation end products. J Biol Chem 2003; 278: 12613-7.
[42] Hudson BI, Harja E, Moser B, Schmidt AM. Soluble levels of receptor for advanced glycation endproducts (sRAGE) and coronary artery disease. The next C-reactive protein?. Arterioscler Thromb Vasc Biol 2005; 25: 879-82.
[43] Yonekura H, Yamamoto Y, Sakurai S, et al. Novel splice variants of the receptor for advanced glycation end-products expressed in human vascular endothelial cells and pericytes, and their putative roles in diabetes-induced vascular injury. Biochem J 2003; 370: 1097-109.
[44] Yamamoto Y, Yonekura H, Watanabe T, et al. Short-chain aldehyde-derived ligands for RAGE and their actions on endothelial cells. Diabetes Res Clin Prac 2007; 77: S30-S40.
[45] Park L, Raman KG, Lee KJ, et al. Suppression of accelerated diabetic atherosclerosis by the soluble receptor for advanced glycation end products. Nat Med 1998; 4: 1025-31.
[46] Bucciarelli LG, Wendt T, Qu W, et al. RAGE blockade stabilizes established atherosclerosis in diabetic apolipoprotein E-null mice. Circulation 2002; 106: 2827-35.
[47] Barile GR, Pachydaki SI, Tari SR, et al. The RAGE axis in early diabetic retinopathy. Invest Ophthalmol Vis Sci 2005; 46: 2916-24.
[48] Kaji Y, Usui T, Ishida S, et al. Inhibition of diabetic leukostasis and blood-retinal barrier breakdown with a soluble form of a receptor for advanced glycation end products. Invest Ophthalmol Vis Sci 2007; 48: 858-65.
[49] Takeuchi M, Yamagishi S. Alternative routes for the formation of glyceraldehyde-derived AGEs (TAGE) in vivo. Med Hypotheses 2004; 63: 453-5.
[50] Oates PJ. Polyol pathway and diabetic peripheral neuropathy. Int Rev Neurobiol 2002; 50: 325-92.
[51] Maekawa K, Tanimoto T, Okada S. Gene expression of enzymes comprising the polyol pathway in various rat tissues determined by
the competitive RT-PCR method. Jpn J Pharmacol 2002; 88: 123-6.
[52] Schalkwijk CG, Stehouwer CD, van Hinsbergh VW. Fructose-mediated non-enzymatic glycation: sweet coupling or bad modification. Diabetes Metab Res Rev 2004; 20: 369-82.
[53] Gaby AR. Adverse effects of dietary fructose. Altern Med Rev 2005; 10: 294-306.
[54] Hallfrisch J. Metabolic effects of dietary fructose. FASEB J 1990; 4: 2652-60.
[55] Mayes PA. Intermediary metabolism of fructose. Am J Clin Nutr 1993; 58: 754S-65S.
[56] L'Esperance FA, James WA, Judson PH. Ellenberg and Rifkin's Diabetes Mellitus, Theory and Practice. Elsevier New York 1990: 661-83.
[57] Mandarino LJ. Current hypotheses for the biochemical basis of diabetic retinopathy. Diabetes Care 1992; 15: 1892-901.
[58] Frank RN. On the pathogenesis of diabetic retinopathy. A 1990 update. Ophthalmology 1991; 98: 586-93.
[59] Sims DE. Recent advances in pericyte biology--implications for health and disease. Can J Cardiol 1991; 7: 431-43.
[60] Herman IM, D'Amore PA. Microvascular pericytes contain muscle and nonmuscle actins. J Cell Biol 1985; 101: 43-52.
[61] Joyce NC, Haire MF, Palade GE. Contractile proteins in pericytes. II. Immunocytochemical evidence for the presence of two isomyosins in graded concentrations. J Cell Biol 1985; 100: 1387-95.
[62] Adamis AP, Miller JW, Bernal MT, et al. Increased vascular endothelial growth factor levels in the vitreous of eyes with proliferative diabetic retinopathy. Am J Ophthalmol 1994; 118: 445-50.
[63] Aiello LP, Avery RL, Arrigg PG, et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N Engl J Med 1994; 331: 1480-7.
[64] Stitt AW, Li YM, Gardiner TA, Bucala R, Archer DB, Vlassara H. Advanced glycation end products (AGEs) co-localize with AGE receptors in the retinal vasculature of diabetic and of AGE-infused rats. Am J Pathol 1997; 150: 523-31.
[65] Sharma NK, Gardiner TA, Archer DB. A morphologic and autoradiographic study of cell death and regeneration in the retinal microvasculature of normal and diabetic rats. Am J Ophthalmol 1985; 100: 51-60.
[66] Yamagishi S, Amano S, Inagaki Y, et al. Advanced glycation end products-induced apoptosis and overexpression of vascular endothelial growth factor in bovine retinal pericytes. Biochem Biophys Res Commun 2002; 290: 973-8.
[67] Yamagishi S, Amano S, Inagaki Y, Okamoto T, Takeuchi M, Makita Z. Beraprost sodium, a prostaglandin I2 analogue, protects against advanced glycation end products-induced injury in cultured retinal pericytes. Mol Med 2002; 8: 546-50.
[68] Yamagishi S, Takeuchi M, Matsui T, Nakamura K, Imaizumi T, Inoue H. Angiotensin II augments advanced glycation end product-induced pericyte apoptosis through RAGE overexpression. FEBS Lett 2005; 579: 4265-70.
[69] Okamoto T, Yamagishi S, Inagaki Y, et al. Incadronate disodium inhibits advanced glycation end products-induced angiogenesis in vitro. Biochem Biophys Res Commun 2002; 297: 419-24.
[70] Okamoto T, Yamagishi S, Inagaki Y, et al. Angiogenesis induced by advanced glycation end products and its prevention by cerivastatin. FASEB J 2002; 16: 1928-30.
[71] Koga K, Yamagishi S, Okamoto T, et al. Serum levels of glucose-derived advanced glycation end products are associated with the severity of diabetic retinopathy in type 2 diabetic patients without renal dysfunction. Int J Clin Pharmacol Res 2002; 22: 13-7.
[72] Miura J, Yamagishi S, Uchigata Y, et al. Serum levels of non-carboxymethyllysine advanced glycation endproducts are correlated to severity of microvascular complications in patients with Type 1 diabetes. J Diabetes Complications 2003; 17: 16-21.
[73] Miura J, Uchigata Y, Yamamoto Y, et al. AGE down-regulation of monocyte RAGE expression and its association with diabetic complications in type 1 diabetes. J Diabetes Complications 2004; 18: 53-9.
[74] Jinnouchi Y, Yamagishi S, Takeuchi M, et al. Atrovastatin decreases serum levels of advanced glycation end products (AGEs) in patients with type 2 diabetes. Clin Exp Med 2006; 6: 191-3.

1480 Current Drug Targets, 2010, Vol. 11, No. 11 Takeuchi et al.
[75] Yokoi M, Yamagishi S, Takeuchi M, et al. Elevations of AGE and vascular endothelial growth factor with decreased total antioxidant status in the vitreous fluid of diabetic patients with retinopathy. Br J Ophthalmol 2005; 89: 673-5.
[76] Yokoi M, Yamagishi S, Takeuchi M, et al. Positive correlation between vitreous levels of advanced glycation end products and vascular endothelial growth factor in patients with diabetic retinopathy sufficiently treated with photocoagulation. Br J Ophthalmol 2007; 91: 397-8.
[77] Sugiyama S, Miyata T, Ueda Y, et al. Plasma levels of pentosidine in diabetic patients: an advanced glycation end product. J Am Soc Nephrol 1998; 9: 1681-8.
[78] Yamaguchi M, Nakamura N, Nakano K, et al. Immunochemical quantification of crossline as a fluorescent advanced glycation endproduct in erythrocyte membrane proteins from diabetic patients with or without retinopathy. Diabet Med 1998; 15: 458-62.
[79] Wagner Z, Wittmann I, Mazak I, et al. N(epsilon)-(carboxymethyl)lysine levels in patients with type 2 diabetes: role of renal function. Am J Kidney Dis 2001; 38: 785-91.
[80] Friedman EA. Ellenberg and Rifkin’s Diabetes Mellitus, Theory and Practice. Elsevier New York 1990: 684-709.
[81] Krolewski AS, Warram JH, Valsania P, Martin BC, Laffel LM, Christlieb AR. Evolving natural history of coronary artery disease in diabetes mellitus. Am J Med 1991; 90: 56S-61S.
[82] Sharma K, Ziyadeh FN. Hyperglycemia and diabetic kidney disease. The case for transforming growth factor-beta as a key mediator. Diabetes 1995; 44: 1139-46.
[83] Dworkin LD, Ichikawa I, Brenner BM. Hormonal modulation of glomerular function. Am J Physiol 1983; 244: F95-104.
[84] Kreisberg JI, Venkatachalam M, Troyer D. Contractile properties of cultured glomerular mesangial cells. Am J Physiol 1985; 249: F457-63.
[85] Schlondorff D. The glomerular mesangial cell: an expanding role for a specialized pericyte. FASEB J 1987; 1: 272-81.
[86] Yamagishi S, Inagaki Y, Okamoto T, et al. Advanced glycation end product-induced apoptosis and overexpression of vascular endothelial growth factor and monocyte chemoattractant protein-1 in human-cultured mesangial cells. J Biol Chem 2002; 277: 20309-15.
[87] Yamamoto Y, Kato I, Doi T, et al. Development and prevention of advanced diabetic nephropathy in RAGE-overexpressing mice. J Clin Invest 2001; 108: 261-8.
[88] Myint KM, Yamamoto Y, Doi T, et al. RAGE control of diabetic nephropathy in a mouse model: effects of RAGE gene disruption and administration of low-molecular weight heparin. Diabetes 2006; 55: 2510-22.
[89] Yamagishi S, Nakamura K, Matsui T. Potential utility of telmisartan, an angiotensin II type 1 receptor blocker with peroxisome proliferator-activated receptor-γ (PPAR-γ)-modulating activity for the treatment of cardiometabolic disorders. Curr Mol Med 2007; 7: 463-9.
[90] Matsui T, Yamagishi S, Ueda S, et al. Telmisartan, an angiotensin II type 1 receptor antagonist, inhibits advanced glycation end-product (AGE)-induced monocyte chemoattractant protein-1 expression in mesangial cells through downregulation of receptor for AGEs via peroxisome proliferator-activated receptor-γ activation. J Int Med Res 2007; 35: 482-9.
[91] Yoshida T, Yamagishi S, Nakamura K, et al. Telmisartan inhibits AGE-induced C-reactive protein production through downregulation of the receptor for AGE via peroxisome proliferator-activated receptor-gamma activation. Diabetologia 2006; 49: 3094-9.
[92] Yamagishi S, Matsui T, Nakamura K, et al. Olmesartan blocks advanced glycation end products (AGEs)-induced angiogenesis in vitro by suppressing receptor for AGEs (RAGE) expression. Microvasc Res 2008; 75: 130-4.
[93] Yamagishi S, Matsui T, Nakamura K, et al. Olmesartan blocks inflammatory reactions in endothelial cells evoked by advanced glycation end products by suppressing generation of reactive oxygen. Ophthalmic Res 2008; 40: 10-5.
[94] Vinik AI, Park TS, Stansberry KB, Pittenger GL. Diabetic neuropathies. Diabetologia 2000; 43: 957-73.
[95] Yagihashi S. Pathology and pathogenetic mechanisms of diabetic neuropathy. Diabetes Metab Rev 1995; 11: 193-225.
[96] Dyck PJ, Giannini C. Pathologic alterations in the diabetic neuropathies of humans: a review. J Neuropathol Exp Neurol 1996; 55: 1181-93.
[97] Thornalley PJ. Glycation in diabetic neuropathy: characteristics, consequences, causes, and therapeutic options. Int Rev Neurobiol 2002; 50: 37-57.
[98] Wada R, Nishizawa Y, Yagihashi N, et al. Effect of OPB-9195, anti-glycation agent, on experimental diabetic neuropathy. Eur J Clin Invest 2001; 31: 513-20.
[99] Sekido H, Suzuki T, Jomori T, Takeuchi M, Yabe-Nishimura C, Yagihashi S. Reduced cell replication and induction of apoptosis by advanced glycation end products in rat Schwann cells. Biochem Biophys Res Commun 2004; 320: 241-8.
[100] Takeuchi M, Bucala R, Suzuki T, et al. Neurotoxicity of advanced glycation end-products for cultured cortical neurons. J Neuropathol Exp Neurol 2000; 59: 1094-105.
[101] DECODE Study Group. Glucose tolerance and cardiovascular mortality: comparison of fasting and 2-hour diagnostic criteria. Arch Intern Med 2001; 161: 397-405.
[102] Levitan EB, Song Y, Ford ES, Liu S. Is nondiabetic hyperglycemia a risk factor for cardiovascular disease? A meta-analysis of prospective studies. Arch Intern Med 2004; 164: 2147-55.
[103] Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 1998; 339: 229-34.
[104] Hanefeld M, Fischer S, Julius U, et al. Risk factors for myocardial infarction and death in newly detected NIDDM: the Diabetes Intervention Study, 11-year follow-up. Diabetologia 1996; 39: 1577-83.
[105] Yamagishi S, Nakamura K, Matsui T, Ueda S, Imaizumi T. Role of postprandial hyperglycaemia in cardiovascular disease in diabetes. Int J Clin Pract 2007; 61: 83-7.
[106] Kitahara Y, Takeuchi M, Miura K, Mine T, Matsui T, Yamagishi S. Glyceraldehyde-derived advanced glycation end products (AGEs). A novel biomarker of postprandial hyperglycemia in diabetic rats. Clin Exp Med 2008; 8: 175-7.
[107] UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulfonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998; 352: 837-53.
[108] Enomoto M, Adachi H, Yamagishi S, et al. Positive association of serum levels of advanced glycation end products with thrombogenic markers in humans. Metabolism 2006; 55: 912-7.
[109] Bolton WK, Cattran DC, Williams ME, et al. Randomized trial of an inhibitor of formation of advanced glycation end products in diabetic nephropathy. Am J Nephrol 2004; 24: 32-40.
[110] Du X, Matsumura T, Edelstein D, et al. Inhibition of GAPDH activity by poly(ADP-ribose) polymerase activates three major pathways of hyperglycemic damage in endothelial cells. J Clin Invest 2003; 112: 1049-57.
[111] Monnier L, Lapinski H, Colette C. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic patients: variations with increasing levels of HbA(1c). Diabetes Care 2003; 26: 881-5.
[112] Yamagishi S, Matsui T, Ueda S, Fukami K, Okuda S. Clinical utility of acarbose, an alpha-glucosidase inhibitor in cardiometabolic disorders. Curr Drug Metab 2009; 10: 159-63.
[113] Tsunosue M, Mashiko N, Ohta Y, et al. An alpha-glucosidase inhibitor, acarbose treatment decreases serum levels of glyceraldehyde-derived advanced glycation end products (AGEs) in patients with type 2 diabetes. Clin Exp Med 2010; 10: 139-41.
[114] Challier M, Jacqueminet S, Benabdesselam O, Grimaldi A, Beaudeux JL. Increased serum concentrations of soluble receptor for advanced glycation endproducts in patients with type 1 diabetes. Clin Chem 2005; 51: 1749-50.
[115] Nakamura K, Yamagishi S, Adachi H, et al. Elevation of soluble form of receptor for advanced glycation end products (sRAGE) in diabetic subjects with coronary artery disease. Diabetes Metab Res Rev 2007; 23: 368-71.
[116] Tan KC, Shiu SW, Chow WS, Leng L, Bucala R, Betteridge DJ. Association between serum levels of soluble receptor for advanced glycation end products and circulating advanced glycation end products in type 2 diabetes. Diabetologia 2006; 49: 2756-62.

A Novel Therapeutic Strategy for Diabetic Complications Current Drug Targets, 2010, Vol. 11, No. 11 1481
[117] Nakamura K, Yamagishi S, Matsui T, Adachi H, Takeuchi M, Imaizumi T. Serum levels of soluble form of receptor for advanced glycation end products (sRAGE) are correlated with AGEs in both diabetic and non-diabetic subjects. Clin Exp Med 2007; 7: 188-90.
[118] Yamagishi S, Adachi H, Nakamura K, et al. Positive association between serum levels of advanced glycation end products and the soluble form of receptor for advanced glycation end products in non-diabetic subjects. Metabolism 2006; 55: 1227-31.
[119] Nakamura K, Yamagishi S, Adachi H, et al. Serum levels of sRAGE, the soluble form of receptor for advanced glycation end products, are associated with inflammatory markers in patients with type 2 diabetes. Mol Med 2007; 13: 185-9.
[120] Nakamura K, Yamagishi S, Adachi H, et al. Circulating advanced glycation end products (AGEs) and soluble form of receptor for AGEs (sRAGE) are independent determinants of serum monocyte chemoattractant protein-1 (MCP-1) levels in patients with type 2 diabetes. Diabetes Metab Res Rev 2008; 24: 109-14.
[121] Yamagishi S, Imaizumi T. Serum levels of soluble form of receptor for advanced glycation end products (sRAGE) may reflect tissue RAGE expression in diabetes. Arterioscler Thromb Vasc Biol 2007; 27: e32, author reply e33-34.
[122] Yamagishi S, Matsui T, Nakamura K. Kinetics, role and therapeutic implications of endogenous soluble form of receptor for advanced glycation end products (sRAGE) in diabetes. Curr Drug Targets 2007; 8: 1138-43.
[123] Miura J, Yamamoto Y, Osawa M, et al. Endogenous secretory receptor for advanced glycation endproducts levels are correlated with serum pentosidine and CML in patients with type 1 diabetes. Arterioscler Thromb Vasc Biol 2007; 27: 253-4.
[124] Katakami N, Matsuhisa M, Kaneto H, et al. Decreased endogenous secretory advanced glycation end product receptor in type 1 diabetic patients: its possible association with diabetic vascular complications. Diabetes Care 2005; 28: 2716-21.
[125] Sakurai S, Yamamoto Y, Tamei H, et al. Development of an ELISA for esRAGE and its application to type 1 diabetic patients. Diabetes Res Clin Pract 2006; 73: 158-65.
[126] Koyama H, Shoji T, Yokoyama H, et al. Plasma level of endogenous secretory RAGE is associated with components of the metabolic syndrome and atherosclerosis. Arterioscler Thromb Vasc Biol 2005; 25: 2587-93.
[127] Humpert PM, Djuric Z, Kopf S, et al. Soluble RAGE but not endogenous secretory RAGE is associated with albuminuria in patients with type 2 diabetes. Cardiovasc Diabetol 2007; 6: 9.
[128] Basta G, Sironi AM, Lazzerini G, et al. Circulating soluble receptor for advanced glycation end products is inversely associated with glycemic control and S100A12 protein. J Clin Endocrinol Metab 2006; 91: 4628-34.
[129] Forbes JM, Thorpe SR, Thallas-Bonke V, et al. Modulation of soluble receptor for advanced glycation end products by angiotensin-converting enzyme-1 inhibition in diabetic nephropathy. J Am Soc Nephrol 2005; 16: 2363-72.
[130] Nakamura K, Yamagishi S, Nakamura Y, et al. Telmisartan inhibits expression of a receptor for advanced glycation end products (RAGE) in angiotensin-II-exposed endothelial cells and decreases serum levels of soluble RAGE in patients with essential hypertension. Microvasc Res 2005; 70: 137-41.
[131] Mamputu JC, Renier G. Advanced glycation end-products increase monocyte adhesion to retinal endothelial cells through vascular endothelial growth factor-induced ICAM-1 expression: inhibitory effect of antioxidants. J Leukoc Biol 2004; 75: 1062-9.
[132] Miyamoto K, Khosrof S, Bursell SE, et al. Prevention of leukostasis and vascular leakage in streptozotocin-induced diabetic retinopathy via intercellular adhesion molecule-1 inhibition. Proc Natl Acad Sci USA 1999; 96: 10836-41.
[133] Matsumoto Y, Takahashi M, Ogata M. Relationship between glycoxidation and cytokines in the vitreous of eyes with diabetic retinopathy. Jpn J Ophthalmol 2002; 46: 406-12.
[134] Okada S, Shikata K, Matsuda M, et al. Intercellular adhesion molecule-1-deficient mice are resistant against renal injury after induction of diabetes. Diabetes 2003; 52: 2586-93.
[135] Chow FY, Nikolic-Paterson DJ, Ozols E, Atkins RC, Rollin BJ, Tesch GH. Monocyte chemoattractant protein-1 promotes the development of diabetic renal injury in streptozotocin-treated mice. Kidney Int 2006; 69: 73-80.
[136] De Vriese AS, Tilton RG, Elger M, et al. Antibodies against vascular endothelial growth factor improve early renal dysfunction in experimental diabetes. J Am Soc Nephrol 2001; 12: 993-1000.
[137] Flyvbjerg A, Dagnaes-Hansen F, De Vriese AS, Schrijvers BF, Tilton RG, Rasch R. Amelioration of long-term renal changes in obese type 2 diabetic mice by a neutralizing vascular endothelial growth factor antibody. Diabetes 2002; 51: 3090-4.
[138] Yamagishi S, Nakamura K, Takenaka K, Matsui T, Inoue H. Pleiotropic effects of nifedipine on atherosclerosis. Curr Pharm Des 2006; 12: 1543-7.
[139] Celletti FL, Waugh JM, Amabile PG, Brendolan A, Hilfiker PR, Dake MD. Vascular endothelial growth factor enhances atherosclerotic plaque progression. Nat Med 2001; 7: 425-9.
[140] Yamagishi S, Takeuchi M. Telmisartan is a promising cardiometabolic sartan due to its unique PPAR-gamma-inducing property. Med Hypotheses 2005; 64: 476-8.
[141] Marx N, Walcher D, Ivanova N, et al. Thiazolidinediones reduce endothelial expression of receptors for advanced glycation end products. Diabetes 2004; 53: 2662-8.
[142] Miyata T, van Ypersele de Strihou C, Ueda Y, et al. Angiotensin II receptor antagonists and angiotensin-converting enzyme inhibitors lower in vitro the formation of advanced glycation end products: biochemical mechanisms. J Am Soc Nephrol 2002; 13: 2478-87.
[143] Forbes JM, Cooper ME, Thallas V, et al. Reduction of the accumulation of advanced glycation end products by ACE inhibition in experimental diabetic nephropathy. Diabetes 2002; 51: 3274-82.
[144] Sebekova K, Schinzel R, Munch G, Krivosikova Z, Dzurik R, Heidland A. Advanced glycation end-product levels in subtotally nephrectomized rats: beneficial effects of angiotensin II receptor 1 antagonist losartan. Miner Electrolyte Metab 1999; 25: 380-3.
[145] Fan Q, Liao J, Kobayashi M, et al. Candesartan reduced advanced glycation end-products accumulation and diminished nitro-oxidative stress in type 2 diabetic KK/Tα mice. Nephrol Dial Transplant 2004; 19: 3012-20.
[146] Thomas MC, Tikellis C, Burns WM, et al. Interactions between renin angiotensin system and advanced glycation in the kidney. J Am Soc Nephrol 2005; 16: 2976-84.
[147] Yamagishi S, Takeuchi M, Inoue H. Olmesartan medoxomil, a newly developed angiotensin II type 1 receptor antagonist, protects against renal damage in advanced glycation end product (age)-injected rats. Drugs Exp Clin Res 2005; 31: 45-51.
[148] Sebekova K, Gazdikova K, Syrova D, et al. Effects of ramipril in nondiabetic nephropathy: improved parameters of oxidatives stress and potential modulation of advanced glycation end products. J Hum Hypertens 2003; 17: 265-70.
[149] Saisho Y, Komiya N, Hirose H. Effect of valsartan, an angiotensin II receptor blocker, on markers of oxidation and glycation in Japanese type 2 diabetic subjects: blood pressure-independent effect of valsartan. Diabetes Res Clin Prac 2006; 74: 201-3.
[150] Yamagishi S, Takeuchi M. Nifedipine inhibits gene expression of receptor for advanced glycation end products (RAGE) in endothelial cells by suppressing reactive oxygen species generation. Drugs Exp Clin Res 2004; 30: 169-75.
[151] Matsui T, Yamagishi S, Nakamura K, Inoue H, Takeuchi M. Nifedipine, a calcium-channel blocker, inhibits advanced glycation end-product-induced expression of monocyte chemoattractant protein-1 in human cultured mesangial cells. J Int Med Res 2007; 35: 107-12.
[152] Yamagishi S, Inagaki Y, Kikuchi S. Nifedipine inhibits tumor necrosis factor-alpha-induced monocyte chemoattractant protein-1 overexpression by blocking NADPH oxidase-mediated reactive oxygen species generation. Drugs Exp Clin Res 2003; 29: 147-52.
[153] Mezzano S, Aros C, Droguett A, et al. NF-kappaB activation and overexpression of regulated genes in human diabetic nephropathy. Nephrol Dial Transplant 2004; 19: 2505-12.
[154] Tombran-Tink J, Barnstable CJ. PEDF: a multifaceted neurotro-phic factor. Nat Rev Neurosci 2003; 4: 628-36.
[155] Abe R, Fujita Y, Yamagishi S. Angiogenesis and metastasis inhibitors for the treatment of malignant melanoma. Mini Rev Med Chem 2007; 7: 649-61.
[156] Yamagishi S, Inagaki Y, Amano S, Okamoto T, Takeuchi M, Makita Z. Pigment epithelium-derived factor protects cultured retinal pericytes from advanced glycation end product-induced

1482 Current Drug Targets, 2010, Vol. 11, No. 11 Takeuchi et al.
injury through its antioxidative properties. Biochem Biophys Res Commun 2002; 296: 877-82.
[157] Inagaki Y, Yamagishi S, Okamoto T, Takeuchi M, Amano S. Pigment epithelium-derived factor prevents advanced glycation end products-induced monocyte chemoattractant protein-1 production in microvascular endothelial cells by suppressing intracellular reactive oxygen species generation. Diabetologia 2003; 46: 284-7.
[158] Yamagishi S, Amano S, Inagaki Y, Okamoto T, Takeuchi M, Inoue H. Pigment epithelium-derived factor inhibits leptin-induced angiogenesis by suppressing vascular endothelial growth factor gene expression through anti-oxidative properties. Microvasc Res 2003; 65: 186-90.
[159] Yamagishi S, Inagaki Y, Nakamura K, et al. Pigment epithelium-derived factor inhibits TNF-alpha-induced interleukin-6 expression in endothelial cells by suppressing NADPH oxidase-mediated reactive oxygen species generation. J Mol Cell Cardiol 2004; 37: 497-506.
[160] Yamagishi S, Nakamura K, Ueda S, Kato S, Imaizumi T. Pigment epithelium-derived factor (PEDF) blocks angiotensin II signaling in endothelial cells via suppression of NADPH oxidase: a novel anti-oxidative mechanism of PEDF. Cell Tissue Res 2005; 320: 437-45.
[161] Yamagishi S, Matsui T, Nakamura K, et al. Pigment-epithelium-derived factor (PEDF) inhibits angiotensin-II-induced vascular endothelial growth factor (VEGF) expression in MOLT-3 T cells through anti-oxidative properties. Microvasc Res 2006; 71: 222-6.
[162] Yamagishi S, Ueda S, Matsui T, et al. Pigment epithelium-derived factor (PEDF) prevents advanced glycation end products (AGEs)-elicited endothelial nitric oxide synthase (eNOS) reduction through its anti-oxidative properties. Protein Pept Lett 2007; 14: 832-5.
[163] Yamagishi S, Matsui T, Nakamura K, Takeuchi M, Imaizumi T. Pigment epithelium-derived factor (PEDF) prevents diabetes- or advanced glycation end products (AGE)-elicited retinal leukostasis. Microvasc Res 2006; 72: 86-90.
[164] Yamagishi S, Matsui T, Nakamura K, et al. Pigment-epithelium-derived factor suppresses expression of receptor for advanced glycation end products in the eye of diabetic rats. Ophthalmic Res 2007; 39: 92-7.
[165] Yamagishi S, Nakamura K, Matsui T, et al. Pigment epithelium-derived factor inhibits advanced glycation end product-induced retinal vascular hyperpermeability by blocking reactive oxygen species-mediated vascular endothelial growth factor expression. J Biol Chem 2006; 281: 20213-20.
[166] Spranger J, Osterhoff M, Reimann M, et al. Loss of the antiangiogenic pigment epithelium-derived factor in patients with angiogenic eye disease. Diabetes 2002; 50: 2641-5.
[167] Boehm BO, Lang G, Volpert O, et al. Low content of the natural ocular anti-angiogenic agent pigment epithelium-derived factor (PEDF) in aqueous humor predicts progression of diabetic retinopathy. Diabetologia 2003; 46: 394-400.
[168] Yokoi M, Yamagishi S, Saito A, et al. Positive association of pigment epithelium-derived factor with total antioxidant capacity
in the vitreous fluid of patients with proliferative diabetic retinopathy. Br J Ophthalmol 2007; 91: 885-7.
[169] Yoshida Y, Yamagishi S, Matsui T, et al. Positive correlation of pigment epithelium-derived factor and total antioxidant capacity in aqueous humour of patients with uveitis and proliferative diabetic retinopathy. Br J Ophthalmol 2007; 91: 1133-4.
[170] Yoshida T, Yamagishi S, Nakamura K, et al. Atorvastatin inhibits advanced glycation end products (AGE)-induced C-reactive protein expression in hepatoma cells by suppressing reactive oxygen species generation. Vasc Dis Prevent 2007; 4: 213-6.
[171] Yamagishi S, Matsui T, Nakamura K, Takeuchi M. Minodronate, a nitrogen-containing bisphosphonate, inhibits advanced glycation end product-induced vascular cell adhesion molecule-1 expression in endothelial cells by suppressing reactive oxygen species generation. Int J Tissue React 2005; 27: 189-95.
[172] Yamagishi S, Nakamura K, Matsui T, Takeuchi M. Minodronate, a nitrogen-containing bisphosphonate, is a promising remedy for treating patients with diabetic retinopathy. Med Hypotheses 2006; 66: 273-5.
[173] Yamagishi S, Abe R, Inagaki Y, et al. Minodronate, a newly developed nitrogen-containing bisphosphonate, suppresses melanoma growth and improves survival in nude mice by blocking vascular endothelial growth factor signaling. Am J Pathol 2004; 165: 1865-74.
[174] Yamagishi S, Ueda S, Okuda S. Food-derived advanced glycation end products (AGEs): a novel therapeutic target for various disorders. Curr Pharm Des 2007; 13: 2832-6.
[175] Koschinsky T, He CJ, Mitsuhashi T, et al. Orally absorbed reactive glycation products (glycotoxins): an environmental risk factor in diabetic nephropathy. Proc Natl Acad Sci USA 1997; 94: 6474-9.
[176] Sato T, Wu X, Shimogaito N, Takino J, Yamagishi S, Takeuchi M. Effects of high-AGE beverage on RAGE and VEGF expressions in the liver and kidneys. Eur J Nutr 2009; 48: 6-11.
[177] Niwa T, Nomura T, Sugiyama S, Miyazaki T, Tsukushi S, Tsutsui S. The protein metabolite hypothesis, a model for the progression of renal failure: an oral adsorbent lowers indoxyl sulfate levels in undialyzed uremic patients. Kidney Int Suppl 1997; 62: S23-S8.
[178] Nakamura T, Kawagoe Y, Matsuda T, et al. Oral ADSORBENT AST-120 decreases carotid intima-media thickness and arterial stiffness in patients with chronic renal failure. Kidney Blood Press Res 2004; 27: 121-6.
[179] Schulman G, Agarwal R, Acharya M, Berl T, Blumenthal S, Kopyt N. A multicenter, randomized, double-blind, placebo-controlled, dose-ranging study of AST-120 (Kremezin) in patients with moderate to severe CKD. Am J Kidney Dis 2006; 47: 565-77.
[180] Ueda S, Yamagishi S, Takeuchi M, et al. Oral adsorbent AST-120 decreases serum levels of AGEs in patients with chronic renal failure. Mol Med 2006; 12: 180-4.
[181] The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993; 329: 977-86.
Received: March 03, 2010 Revised: May 26, 2010 Accepted: June 10, 2010