Embed Size (px)
Citation preview

13th December 2011
SUBMISSION TO THE INQUIRY INTO WORKFORCE PARTICIPATION BY PEOPLE WITH MENTAL ILLNESS
Thank you for the opportunity to make this submission to the Family and Community Development Committee Inquiry into the workforce participation by people with mental illness.
Barriers to workforce participation
There are a number of barriers to the participation of people with mental ill health in preparing for work through education and training, and in employment as job seekers and once in the workforce.
Education and training
The onset of mental illness often occurs in late adolescence and early adulthood, so that it frequently interrupts secondary or tertiary education, with negative consequences for employability, workforce participation and career options. Hence, re‐engagement in education and successful attainment of qualifications is an important priority to impact longer term employment outcomes. Participation and completion rates among people with mental illness are lower than for many other students in tertiary education, with wide‐ranging barriers to entering and or re‐engaging with education, sustaining studies and successfully completing courses. These include:
• Risk factors for dropping out of higher education include the impact on studying of thinking difficulties associated with symptoms and medication effects, lowered academic self‐confidence, disclosure issues and consequent reluctance to seek assistance from academics or fellow students, and discriminatory and unhelpful responses to disclosure in academic settings.
• Barriers to re‐engagement with education include managing mental health issues or fear of relapse; financial costs including course fees and expenses associated with studying (eg, internet, computer, transport, etc); lack of knowledge, encouragement or support from mental health workers; and complexity of systems to navigate to access education and financial entitlements.
• Re‐engagement with education after a prolonged absence and ill‐health may be especially challenging without additional supports. Previous failed attempts and prior experience of inadequate support to engage in education can compound a sense of failure and further alienate adults with mental illnesses from returning to study.
• People have differing educational aspirations and, at differing points in recovery, their support needs may vary, yet pathways into the post‐secondary educational sector can be unclear and the systems to access education and support difficult to navigate. Students and aspiring students report challenges in accessing accurate information on course requirements/demands to allow them to make informed decisions about enrolment.

• Barriers to successful participation and completion of tertiary education courses include financial constraints; competing responsibilities and scheduling issues or inflexible course structures; lack of or inaccessible study supports for struggling students within educational settings; and the need to disclose mental ill health in seeking assistance. Students may not necessarily view their mental health related‐difficulties as fitting with notions of disability, yet access to additional supports and adjustments to which they are entitled within educational settings typically depends upon identifying as having ‘disability’.
• A range of supported education initiatives have been developed internationally with the aim of enabling people with mental ill health to access and successfully participate in tertiary education. These types of initiatives are less well developed in Australia, and little research has investigated what kinds of initiatives are of most assistance in Australian contexts.
Employment
Barriers to employment are also wide‐ranging and can relate to mental ill health itself, income security, job‐seeking support, employers and workplaces. They include:
• Managing employment and mental health issues, including fear of relapse and resulting loss of employment; disclosure issues and the potential for discrimination; the stressful nature of job‐seeking; and restricted employment options, particularly if one’s working life has been significantly disrupted due to ill‐health.
• Lack of supports, including practical assistance for job seekers with job searching, completion of applications and job interview preparation; financial assistance in relation to expenses associated with job‐seeking (eg, costs of communication, travel, clothing, etc); supports with the emotional demands of the job‐seeking process.
• Impact on income security of employment, particularly for those people with fluctuating ill health and capacity to participate in the workforce. Concerns about income security are compounded by the complexity of navigating unemployment and income support systems that appear to emphasize compliance and lack built‐in responsiveness to accommodate people’s fluctuating health and circumstances. Lack of accessible trusted financial information and advice further exacerbates the difficulties that people with mental ill health face in job‐seeking and weighing up their employment options.
• When job seeking is combined with experiencing slow procedures or lack of responsiveness from agencies that are expected to be providing assistance (eg Centrelink, employment agencies), these experiences are undermining, demoralising and deter job seekers.
• For employees with mental ill health, lack of understanding and support in the workplace can be a barrier to sustained employment and a reason for leaving work. Underlying this, employer and other workers may lack knowledge about how to make work adjustments or provide effective support to an employee experiencing mental ill health.
• Lack of recognition that people have a varying range of commitments at differing points in their lives (eg, raising children, caring for family or others in the community), which can impact their availability to participate in the workforce irrespective of health status. This may be a reason for discontinuing employment but also a barrier to it being sustained if return to the workforce is prematurely required.
The nature of mental ill health, its treatment and mental health services
• The symptoms of mental illnesses, effects of medications and the need for ongoing treatment and support can present significant challenges in relation to participation in study and employment. Symptoms may be fluctuating or episodic nature, so that people may experience
variation in the extent of their resulting difficulties and needs for support. Some medications for the treatment of mental ill health have effects that can make studying or undertaking employment more challenging, depending on the nature of job and tasks involved. In addition, appointments for ongoing treatment and support from mental health services are not necessarily offered at times that accommodate study or employment schedules.
• Limited attention given in clinical mental health services to education or employment issues to support students/ employees to retain enrolments/jobs when they become unwell or to encourage return to study/work and support. This is exacerbated by poor knowledge among mental health service providers, consumers and families about where people with mental ill health obtain assistance with education, training and employment and financial advice. In addition, lack of information about government subsidies and funding supports to assist people with mental ill health to participate in education, training and employment and how these may be accessed.
• The complexity of funding arrangements and programs within mental health services and disability employment services make it difficult for staff in each sector to understand the working arrangements of the other, which acts as a barrier to collaboration and ensuring people with mental ill health get appropriate assistance.
Effectiveness of programs supporting workforce participation by people with mental illness
• Individualised follow‐along support: There is international evidence that an integrated approach with individualised ongoing support during job‐seeking and once in employment can effectively assist people with mental ill health to access employment. There is also emerging evidence that this approach can be adapted to support return to learning. These approaches need to be more widely accessible in Australia. They could be further developed through partnership‐based and co‐located approaches to service delivery; and require adequate funding for workforce training and development.
Approaches that have some evidence of effectiveness but require further evaluation/ trialling/development to determine effectiveness in Australian settings include:
• Wider‐ranging support options: Peer support and mentoring, job/study support groups, employees and students as mentors are examples of ways in which the range and accessibility of supports in communities might be expanded.
• Information resources: Fund the development of multi‐media and website resources to strengthen community members’ access to information about resources, reasonable adjustments and supports that assist re‐entry and participation in education, training and employment. This should be developed with people who have direct experience of re‐entry and participating in education, training and employment, as well as consultation with other stakeholder groups for whom the information is being developed (eg, employers, teachers, families), to ensure its relevance and usefulness.
• Service integration: More seamless service provision to support access to mental health care, financial counseling, assistance and support with return to learning and employment and to reduce gaps in provision. Fund the creation of formal local partnerships between relevant agencies and service providers and co‐location of services to facilitate better access for people experiencing mental ill health and collaboration to improve the quality of information and assistance provided.
• Learning and working environments that promote mental health and wellbeing: Support and fund the development of initiatives in educational settings and workplaces to create learning
and working environments that promote mental health and wellbeing, and in so doing are naturally supportive of students and staff who may experience mental health issues.
Three top priorities for achieving improved outcomes for people with mental illness seeking to participate in the workforce:
1. Joined up approach to education and employment using individualised follow‐along support to access mainstream education and employment. This approach will support people to gain the skills and qualifications required to obtain employment they desire. It will enable people with mental illness to aspire to careers that hold meaning for them and allow their ongoing contribution as valued members of the community.
2. Better access to and support in returning to education and employment to facilitate experiences of successful education and workforce participation, thus minimising the crushing experience of repeated failure and consequent alienation from participation in education, the workforce and community.
3. A skilled‐up workforce that has: high aspirations for people with mental illness to participate in higher education, training and employment; skills to deliver individualised follow‐along support; and organisations (educational settings and workplaces/employees) that willingly accommodate such support.
For further information, we have also attached the following resources:
• Fossey E, Harvey CA (2010). Finding and sustaining mainstream employment: A qualitative meta‐synthesis of mental health consumer views. Canadian Journal of Occupational Therapy, 77(5), 303‐314.
• Two factsheets about the findings of two recent studies of workplace supports and factors that contribute to the sustainability of employment of people with mental ill health in social firms, which indicate some factors that may be helpful in promoting healthy, supportive workplaces more broadly.
• Ennals, P., Cartwright, E. & Rinaudo, B. (2010). Supported education: One pathway to social inclusion for people with interrupted educational trajectories. New Paradigm, Winter, 2010, 14‐16.
In addition, Dr Ellie Fossey’s doctoral research explored everyday life stories of opportunities and barriers to community participation with people experiencing mental health issues [PhD thesis, University of Melbourne]. This research was undertaken at The Psychosocial Research Centre, one key priority of which is to build evidence for policy and practices to promote recovery through social and economic participation. Please contact us if you would like us to elaborate on any aspect of our submission.
We look forward to following the progress of this Committee Inquiry.
Yours sincerely,
Priscilla Ennals3, Dr Ellie Fossey1, 3 and Associate Professor Carol Harvey1, 2,
Psychosocial Research Centre, a collaborative research initiative of with The University of Melbourne Department of Psychiatry1 and NorthWestern Mental Health2, also affiliated with La Trobe University Schools of Occupational Therapy3, Social Work and Social Policy.

Email addresses for correspondence: [email protected]; [email protected]; [email protected]
Supported education: One pathway to social inclusion for people with interrupted educational trajectories Priscilla Ennals Lecturer in Occupational Therapy, La Trobe University Emma Cartwright Occupational Therapist, Orygen Youth Health Ben Rinaudo Peer Support Worker, MIFellowship Introduction Education is a primary goal for many people as it is viewed as a gateway to employment and other life goals. The onset of mental illness commonly occurs in late adolescence/ early adulthood, thus interrupting many people’s educational trajectories (Waghorn, Still, Chant, & Whiteford, 2004). In Australia, research demonstrates poor completion of secondary school by students with mental health issues in comparison to the general population (Waghorn et al.). Increased participation rates of people in employment and education have been identified as indicators of improvement in social inclusion and recovery for people living with mental illness, and are a priority area of the Forth National Mental Health Plan (Commonwealth of Australia, 2009). Increasing the rates of participation in education and successful educational outcomes for people with mental illness requires greater understanding of: 1) the experiences of consumers as they attempt to re-engage with educational institutions, and 2) the interventions that best facilitate participation and success. These factors remain poorly understood in an Australian context resulting in policies and practices that miss opportunities to enhance social inclusion through education. Many people want to reengage with learning and return to study, however attempts to reengage in typical education settings are often not successful (Mowbray, Collins, & Bybee, 1999). In Australia, research investigating the participation rates in higher education for people with mental illness is limited. One study in 2003 investigated participation rates across disabilities in Australia in the Vocational Education and Training (VET) sector (NCVER, 2003). The study found that although people with mental illness were the highest participating group of all disabilities in VET, they also recorded the lowest subject and course completion rates (NCVER). This research demonstrates that although individuals with a mental illness are returning to study in typical education settings, they are often failing to succeed, with consequent impacts on their confidence and future willingness to engage. A range of barriers to education are commonly reported by individuals with a mental illness. These include internal barriers such as symptoms, personal fears, the cyclical nature of disorders and self stigma, and external barriers including stigma, inflexible course structures, costs, and lack of supports (Mowbray, et al., 2005; Padron, 2006). Supported education Supported education programs arose in North America in the late 1980s in response to many individuals with mental illness failing to succeed in typical education settings. This initiative has expanded to the UK (Isenwater, Lanham, & Thornhill, 2002), Israel (Sasson, Grinspoon, Lachman, & Ponizovsky, 2005), New Zealand (Clayton & Tse, 2003) and Australia (Best, Still, & Cameron, 2008; Waghorn, et al., 2004). Programs aim to increase access to and participation in post-secondary education and facilitate success in higher education through development of individual skills within supportive environments.

The structure and setting of supported education programs vary. Curriculum is often based on developing academic and vocational skills and may be certified leading to a qualification in a specific field, for example information technology. Courses may be initiated by partnerships between community mental health services and education facilities, and can be held at clubhouses, community centres, mental health services or onsite at education campuses. Reported outcomes from both quantitative and qualitative studies include success in higher education and improved employment outcomes (Collins, Bybee, & Mowbray, 1998), improved self-esteem, social adjustment and overall quality of life (Gutman, et al., 2007; Isenwater, et al., 2002). Supported education in Victoria: The MI Fellowship Course The Mental Illness Fellowship Victoria (MI Fellowship) is a membership-based not-for-profit organisation working to improve the wellbeing of individuals with mental illness, their families and friends. MI Fellowship established a supported education course at their Melbourne base in 2004 and has recently expanded their supported education program to an outer Melbourne suburb and a regional centre. The course commences each year in January with an enrolment of approximately 15 to 20 students. Classes are held throughout the year, two days per week for four hours each day. It is a certified course (General Education for Adults (GEA) Certificate II/III) with a curriculum focused on developing literacy and numeracy skills, and the acquisition of skills instrumental for future employment and achieving life goals. Research on the course experience A partnership between La Trobe University School of Occupational Therapy and the MIFellowship has developed to investigate the course, with ongoing research evaluating course outcomes for students. An initial study, conducted by the second author, aimed to explore the experiences of students participating in the GEA-Cert III in 2007 to develop a greater understanding of one Australian Supported Education program from a consumer perspective (Cartwright, 2008). All 19 students were invited to be involved in the research, nine volunteered. The participants, five women and four men, were aged 25 to 39 years, and had mental illness diagnoses of schizophrenia, schizoaffective or borderline personality disorder. Individual semi-structured interviews were conducted with all participants. Four themes emerged from the data as depicted in Diagram 1:
1. Returning to study was a challenge. 2. Flexibility in course structure. 3. Social connections and 4. Self-discovery and growth.
Insert Diagram 1.about here
Participants found returning to study difficult, describing a variety of challenges they experienced while studying. Students reported that they overcame these challenges and achieved success through flexibility in course structure and social connections. Students described how the education course developed their confidence and self-esteem which impacted positively on their relationships with others and their participation in the community. Successful participation and increased confidence assisted students to reconstruct a positive identity, embracing the ‘student’ role. Students also reflected on how the course instilled hope for the future and were able to identify and articulate goals. This research suggests that for individuals who have a desire to return to learning, supported education is one
intervention that can have a positive impact on their recovery from mental illness (Cartwright, 2008). Ben’s story of supported education as a pathway to social inclusion One recent graduate of the course, Ben, shares his personal story of educational interruption as a result of mental illness, participation in supported education and the impact of the course for him. Mental illness is traumatic and life changing. In 2007 I experienced an acute psychotic episode. I was extremely unwell with signs and symptoms of bi-polar disorder and schizophrenia. I was taken to a hospital emergency department and was subsequently admitted to a psychiatric ward. I was studying my Honours year at university at the time and my capacity to study came to a rapid halt. Despite being offered an indefinite extension on my thesis, being unable to think straight or get organised I felt that I had no choice but to withdraw from university at the time. It appeared that my hopes of pursuing education were over. However a year after being discharged from hospital and having some time and space to recoup my case manager suggested I consider a Certificate II in General Education for Adults. This is a return to learning and self-development course aimed at helping people get back into work and study. It wasn’t an easy step for me. Embarking on the course took courage but over the year I began to feel more able and social as I picked up the pieces of my life. I was nominated as the student representative and received an award for Student of the Year, both of which added to my sense of confidence. In 2009 I went on to do the Certificate III in General Education for Adults. The courses transformed my life. They helped me to regain confidence, relearn social and communication skills and further develop my coping skills. The courses are designed in such a way that students regularly set and review short-term and long-term goals. It focused on my strengths and what I could do rather than on my limitations. This approach instilled hope in me. It put me in a better position to access the internal and external resources available to me to manage the biological and psychological aspects of my mental illness and to maintain social connection and purpose. Throughout my two years of study, I volunteered as a tutor of English to newly arrived refugees, helping them settle into Melbourne. I also became a member of the Speakers Bureau for the Mental Illness Fellowship’s Community Education Program. My uncle who is a piano tuner technician employed me in his workshop. My Disability Employment Network provided me with funds for tools and safety equipment for me to be self-employed, and I established a successful gardening small business. Equally important I developed and have sustained good friendships with fellow classmates. After completion of the courses, I was offered casual work through the new Personal Helpers and Mentors Program (PHAMS) and additionally a part time job as a Peer Support Worker with the MI Fellowship. This year as part of my workplace training I am currently studying a Certificate IV in Mental Health. I am also doing intensive Cultural Competency Training for provision of mental health services to people from culturally and linguistically diverse backgrounds. The supported education course was a significant part of my recovery. Not only is meaningful activity, including work, study, training and volunteering essential for self-esteem, finances and lifestyle; it is important to make a contribution to society, keep a routine and do purposeful and enjoyable things. It has certainly been a pathway to social inclusion for me where I discovered a new world of possibility. Now, for me, the future is looking bright.
Implications for practice and policy Personal stories of returning to education and research into supported education programs have implications for consumers, carers, mental health workers, service providers and policy makers. People with mental illness can choose the role of student and be successful in this role to gain educational qualifications. Or they may use the course as a stepping stone to enrolment in higher education, employment, or broader goal attainment such as participation in social groups or volunteering roles. People come to the student role with different motivations and at different stages in their lives and illness. For some young people it is about continuing their education while minimizing disruption to their educational and employment trajectories. For others it is about returning to study after a period of absence in an effort to reconnect with the community and find work or achieve qualifications. For others still it is a means to build skills and knowledge connected to broader goals such as staying well, being socially included and establishing a meaningful routine and role. The supported education environment is different to education environments in which students have previously failed. For people who are anxious about going back to learning this is an environment that most people find very supportive. Students experience a range of positive outcomes: successful transitions into further education and employment, increased self confidence, increased social connectedness and belonging, a student role (different to the role of patient or not having a role that is socially valued), and belief in themselves and confidence to try other things. Carers should see education as a realistic goal for the people they care for; a goal that if undertaken with support in a supportive environment, can facilitate the social inclusion, educational success and potential employment of their loved ones. Support from carers is likely to be critical throughout a course, as students experience the ups and downs that are typical of most students engaged in higher education, while they cope with the additional challenges of mental illness. Mental health workers need to challenge themselves to see educational participation and achievement as a realistic goal for many people with mental illness. While the challenges of returning to learning and the barriers within systems need to be acknowledged, workers can support students to negotiate barriers and locate supportive environments in which they are more likely to succeed. Workers need to see participation in education as a marker of recovery but not an endpoint for treatment and support. Times of transitioning into and out of education courses can be times of increased stress and risk and consumers need extra support, rather than discharge, at these times. In Australia access to supported education, as described in this paper, is extremely limited. While many educational institutions provide some services and attempt to support people with mental illness to engage, these attempts are ad hoc and frequently dependent on serendipitous knowledge and relationships, or targeted to people with high prevalence mental disorders. To facilitate social inclusion through education there needs to be marked expansion of programs and development of supported pathways through educational systems that provide real access and successful outcomes for people with serious mental illness in education. This will have the flow on impact of facilitating meaningful employment and the achievement of vocational hopes and dreams for many people living with mental illness. In acknowledgement of the gap in education services for people with mental illness, Vicserv has proposed research titled “Education: Experience, aspirations and outcomes” (VICSERV, 2008, p.40) to clarify student needs, the effectiveness and timing of supportive interventions
in education, and how these relate to employment and other social inclusion outcomes. This research is timely and necessary for creating a solid base of evidence for practice and informed policy making. As described in the Forth National Mental Health Plan, recovery “represents a personal journey toward a new and valued sense of identity, role and purpose, together with an understanding and accepting of mental illness with its attendant risks” (Commonwealth of Australia, 2009, p.26). Supported education can provide this sense of identity and purpose and promotes social inclusion and recovery, confirming the need for education to be on any agenda aiming to facilitate social inclusion for people who experience mental illness. References Best, L., Still, M., & Cameron, G. (2008). Supported education: Enabling course completion
for people experiencing mental illness. Australian Occupational Therapy Journal, 55, 65‐68.
Cartwright, E. (2008). Return to learning: A naturalistic inquiry investigating a supported education program for adults with a mental illness. La Trobe University, Melbourne.
Clayton, J., & Tse, S. (2003). An educational journey towards recovery for individuals with persistent mental illness: A New Zealand perspective. Psychiatric Rehabilitation Journal, 27, 72‐78.
Collins, M., Bybee, D., & Mowbray, C. T. (1998). Effectiveness of supported education for individuals with psychiatric disabilities: Results from an environmental study. Community Mental Health Journal, 34, 595‐613.
Commonwealth of Australia (2009). Fourth National Mental Health Plan: An agenda for collaborative government action in mental health 2009‐2014.
Gutman, S. A., Schindler, V. P., Furphy, K. A., Klein, K., Lisak, J. M., & Durham (2007). The effectiveness of a supported education program for adults with psychiatric disabilities: The Bridge Program. Occupational Therapy in Mental Health, 23(1), 21‐38.
Isenwater, W., Lanham, W., & Thornhill, H. (2002). The College Link Program: Evaluation of a supported education initiative in Great Britain. Psychiatric Rehabilitation Journal, 26, 43‐50.
Mowbray, C. T., Collins, M., Bellamy, C. D., Megivern, D., Bybee, D., & Szilvagyi, S. (2005). Supported education for adults with psychiatric disabilities: An innovation for social work and psychosocial rehabilitation practice. Social Work, 50(1), 7‐20.
Mowbray, C. T., Collins, M., & Bybee, D. (1999). Supported education for individuals with psychiatric disabilities: Long‐term outcomes from an experimental study. Social Work Research, 23, 89‐100.
NCVER (2003). Australian vocational education and training statistics: Student outcomes survey. Adelaide: National Centre for Vocational and Education Research, NCVER.
Padron, J. M. (2006). Experience with post‐secondary education for individuals with sever mental illness. Psychiatric Rehabilitation Journal, 30(2), 147‐149.
Sasson, R., Grinspoon, A., Lachman, M., & Ponizovsky, A. (2005). A program of supported education for adult Israeli students with schizophrenia. Psychiatric Rehabilitation Journal, 29, 139‐141.
VICSERV (2008). VICSERV's pathways to social inclusion proposition papers ‐ August 2008. Melbourne: Psychiatric Disability Services of Victoria (VICSERV).

Waghorn, G., Still, M., Chant, D., & Whiteford, H. (2004). Specialised supported education for Australians with psychotic disorders. Australian Journal of Social Issues, 39(4), 443‐458.
Diagram 1. Themes identified from the data: barriers, supports and outcomes of returning to learning

Canadian Journal of Occupational Therapy December 2010 77(5) 303
Ellie M. Fossey, Carol A. Harvey
Finding and sustaining employment: A qualitative meta-synthesis of mental health consumer views
Key words EmploymentMental healthQualitative studiesRehabilitation, vocational
Mots clésWord 1Word 2Word 3
Abstract Background. The viewpoints of employed people experiencing mental ill-health receive limited attention in reviews of employment-related research. Purpose. To identify implications from studies investigating the employment-related views of people with persistent mental ill-health to guide the further development of employment supports available to this group. Methods. Published qualitative studies between 1998 and 2008 were searched, resulting in 20 studies for qualitative metasynthesis. Findings. Four themes were synthesized from the findings:(a) employment has var-ied meanings, benefits, and drawbacks to weigh up; (b) strategies for maintaining employment and mental health are important and both require ongoing, active self-management; (c) diverse supports within and beyond the workplace are helpful; and (d) systemic issues add to the employment barriers. Implications. Strategies based on these themes highlight how occupational therapists could initiate improvements in employment support and mental health services to increase their success in enabling satisfying and sustainable employment.
Résumé Objective. Lorem ipsum dolor sit amet, consectetur adipiscing elit. Curabitur consec-tetur condimentum dui et posuere. In accumsan ultrices viverra. Nunc libero purus, sagittis ac tempus pharetra, sollicitudin vitae enim. Sed nec elit odio. Quisque tinci-dunt blandit nibh ut congue. Maecenas sit amet venenatis magna. Method. Nunc non neque in sem mattis tempor at tempus est. Suspendisse pulvinar, velit ut volut-pat convallis, quam urna commodo dui, vitae sodales odio massa at dui. Donec diam est, ornare quis viverra ac, scelerisque vel mi. Results. Nunc a nibh in diam adipiscing luctus a sed sapien. Etiam lacus mauris, laoreet ut rutrum ac, rhoncus ut nisl. Quisque eu leo eu tortor hendrerit volutpat a id mi. Aenean vulputate, nulla in pretium vehic-ula, tellus risus lacinia elit, et tempus justo massa quis odio. Vestibulum ante ipsum primis in faucibus orci luctus et ultrices posuere cubilia Curae; Suspendisse potenti. Conclusion. Nunc ut quam sit amet ante eleifend porta eget et nibh. Nullam tempus gravida nisl, eget placerat orci tristique sed. Lorem ipsum dolor sit amet, consectetur adipiscing elit. Curabitur consectetur condimentum dui et posuere. In accumsan ul-trices viverra. Nunc libero purus, sagittis ac tempus pharetra, sollicitudin vitae enim.
© CAOT PUBLICATIONS ACE
Ellie M. Fossey, PhD is Senior Lecturer, School of Occupational Therapy, La Trobe University, Victoria 3086, Australia. Telephone: +613-9479-5660. E-mail: [email protected].
Carol A. Harvey, MD, MRCPsych, FRANZCP is Associate Professor, Psychosocial Research Centre (Department of Psychiatry, University of Melbourne & North West Area Mental Health Service), 130 Bell St, Coburg, Victoria 3058, Australia. Telephone: +613-9355-9825. E-mail: [email protected].
Citation: Fossey, E. M., & Harvey, C. A. (2010). Finding and sustaining employ-ment: A qualitative meta-synthesis of mental health consumer views. Canadian Journal of Occupational Therapy, 77, 311-322. doi: 10.2182/cjot.2010.77.5.7
Submitted: 6 March 2010; Final acceptance: 17 June 2010.
This study was supported by a Faculty Research Enhancement Grant, Faculty of Health Sciences, La Trobe University.
Employment in paid work is socially highly valued, many aspects of life being contingent upon the income and relationships sustained by it (Grove, Secker, & Seebohm, 2005). As the International Labour Organisation (2004) describes
it, employment is a human right based on the principle that men and women should have access to decent and productive work in conditions of freedom, equity, security, and human dignity. Further, paid employment is considered beneficial to health and well-being, but jobs also bring stresses that traditionally were assumed to outweigh those of being unemployed for people with enduring mental ill-health (Warner, 2004). Yet, prolonged unemployment may actually worsen their situations owing to the constant strains imposed by poverty, isolation and loss of self-respect, identity, sense of purpose, and routine (Marrone & Golowka, 1999; Warner). Recognition of this has increased attention to employment issues in research, policy, and practice.

Fossey & Harvey
304 Revue canadienne d’ergothérapie décembre 2010 77(5)
However, substantial evidence has accumulated over the past decade to endorse the superior effectiveness of IPS-type pro-grams in enabling people with psychiatric disabilities to obtain competitive jobs compared to case management, prevocational training, and other psychosocial rehabilitation approaches (Bond et al., 2008; Crowther, Marshall, Bond, & Huxley, 2001; Kirsh et al.). While other types of vocational services have been less extensively or rigorously evaluated (Corbiere & Lecomte, 2007; Krupa et al., 2003; McKay et al., 2005) and the effectiveness of IPS is predominantly based on outcomes research from the U.S., recent trials suggest its transferability elsewhere (Burns et al., 2007; Killackey, Jackson, & McGorry, 2008; Latimer et al., 2006). Nevertheless, enabling people to sustain employment after getting jobs remains a challenge. Contributing factors may include the predominance of entry-level positions and limited career development opportunities, so better job matching, attention to workplace adjustments, and training are thought to be important (Kirsh et al.; Kravetz, Dellario, Granger, & Salzer, 2003).
Viewpoints of People Experiencing Mental Ill-HealthThe increased interest in and exploration of the viewpoints of employed people with mental ill-health regarding their employment-related experiences, using qualitative methods, could offer new insights into the challenges surrounding sus-taining employment. However, there has been little attempt to synthesize the findings from relevant qualitative studies. Conse-quently, their potential to contribute useful knowledge to guide practitioners and policymakers may be overlooked (Davidson, Ridgway, Kidd, Topor, & Borg, 2008; Gewurtz, Stergiou-Kita, Shaw, Kirsh, & Rappolt, 2008). Therefore, a metasynthesis of mental health consumer viewpoints of employment was car-ried out to make recommendations regarding the further development of vocational services and supports. For this purpose, we sought to address this question: what are mental health consumers’ experiences and viewpoints regarding find-ing and keeping employment in integrated workplaces?
MethodQualitative metasynthesis aims to produce findings that offer a new perspective or deeper understanding of a defined issue than is offered by individual studies (Gewurtz et al., 2008). There are different viewpoints about whether and how qualita-tive studies may be synthesized (Campbell et al., 2003; Daly et al., 2007; Gewurtz et al.). We adopted an approach similar to that outlined by Gewurtz et al.
First, to identify studies investigating the views and experiences of employed people with mental ill-health, we searched three databases (CINAHL, Medline, PsycInfo) using employment-related subject terms and keywords (work, job, employ$, vocation$, tenure, supported employment, IPS), and their respective mental illness-related subject terms. These searches were limited to qualitative studies involving adults and English-language publications between 1998 and 2008. To supplement the database searches, hand searching of key jour-nals and citations in identified articles was undertaken.
Three generations of inquiry are apparent in the rapidly growing body of research: the first and second respectively focus on predicting employability and on vocational service outcomes (Grove & Membrey, 2005; Secker, Membrey, Grove, & Seebohm, 2003), while the third explores the perspectives of people experiencing mental ill-health. The first two are exten-sively reviewed elsewhere and so briefly summarized below; the third is the main focus of this paper. While work can be paid or unpaid (Krupa, Fossey, Anthony, Brown & Pitts, 2009) and undertaken in settings with varied conditions and sup-ports (Corbiere & Lecomte, 2007), for the purpose of this paper employment refers to paid work in an integrated workplace.
EmployabilityEfforts to predict who is most likely to obtain paid employment following rehabilitation have involved investigations of various demographic and clinical characteristics among people experi-encing mental ill-health. Neither diagnosis nor symptoms are consistently related to employment outcomes (Grove & Mem-brey, 2005; Honey, 2000). In comparison, prior employment history is consistently the strongest predictor of vocational outcomes (Honey, 2003; Secker et al., 2003) and linked to the longitudinal course of illness because of the ways in which epi-sodic, fluctuating, and constant patterns of ill-health disrupt workforce participation to differing degrees (Waghorn, Chant, & Whiteford, 2002). Further, psychological factors, such as self-efficacy beliefs, may moderate the influence of employment history on vocational outcomes (Casper & Fisher, 2002; Grove & Membrey), suggesting that people with limited employment histories are not necessarily less capable of working, though they lack work experience. Thus, few strong and consistent associa-tions between person-related characteristics and employment outcomes are evident; their inter-relationships remain poorly understood; and assumptions that work exacerbates symptoms or precipitates relapse are not supported (Grove & Membrey; Honey, 2000; Kirsh, 2000a).
Vocational Service OutcomesVocational services of various types have developed (Corbiere & Lecomte, 2007; Kirsh, Cockburn, & Gewurtz, 2005). As Corbiere and Lecomte described, these include prevocational training programs; transitional employment (TE) placements in local businesses designed to support work re-entry (McKay, Johnsen, & Stein, 2005); affirmative businesses that adopt a systemic economic development approach to creating employ-ment opportunities by eliminating labour force conditions that perpetuate employment disadvantage (Krupa, Lagarde & Car-michael, 2003); and supported employment (SE) programs focusing on placement in competitive jobs with at least mini-mum wages (Corbiere & Lecomte, 2007). The latter include the Individual Placement and Support (IPS) approach, which emphasizes rapid job search, job matching to workers’ prefer-ences, and follow-along support to retain employment in inte-grated workplaces (Bond, Drake, & Becker, 2008).
Traditionally, outcomes were poor in terms of people with prolonged mental ill-health gaining this type of competi-tive employment and achieving satisfactory incomes from paid work, job satisfaction, and career goals (Kirsh et al., 2005).

Fossy & Harvey
Canadian Journal of Occupational Therapy December 2010 77(5) 305
described. We then progressively compared and contrasted the categories and themes so as to group together those conveying similar meanings and to identify overarching themes in much the same way that the constant comparative method is used in grounded theory and thematic analyses of qualitative data (Rice & Ezzy, 1999).
FindingsTable 1 presents the 20 studies grouped according to their aims and the employment-related experiences represented: (a) per-spectives of sustained employment; (b) factors contributing to gaining and sustaining employment; and (c) perspectives of job seeking and employment prospects. We summarize the main features and qualities of these studies below and then describe the themes identified from our metasynthesis.
Features and Qualities of the Included StudiesOf these twenty studies, seven were conducted in the U.S., five in Canada, four in Australia, three in England, and one in New Zealand. Participants were usually consumers recruited
Twenty-five qualitative studies were located. As Gewurtz et al. (2008) recommend, we then excluded some studies on topical grounds to ensure a focused metasynthesis. Therefore, to shed light on what enables people to sustain competitive employment, we excluded five studies that focused on employ-ment in other settings or on employment program practices (Gahnstrom-Standqvist, Luikko, & Tham, 2003; Gowdy, Carl-son, & Rapp, 2003; Gowdy, Carlson, & Rapp, 2004; Quimby, Drake, & Becker, 2001; Strong, 1998). The remaining 20 stud-ies were reviewed using previously described quality crite-ria and questions (Fossey, Harvey, McDermott, & Davidson, 2002) to consider the appropriateness, adequacy, respon-siveness, and transparency of the reported qualitative meth-ods and the interpretive rigour of the reported findings. The purpose was to identify their main methodological features, findings, and relative strengths and limitations rather than to assign comparative quality rankings to the studies, all of which addressed consumer experiences and accounts of employment but in contextually diverse settings. To then synthesize the findings manually, we began by listing the reported categories and themes across the 20 studies, as Campbell et al. (2003)
Table 1Mental Health Consumers’ Employment-related Views and Experience: Qualitative Studies from 1998–2008
Citation Purpose Design & location Participants Findings – overall themes
Perspectives of sustained employment
Auerbach & Richardson (2005)
Kennedy-Jones et al. (2005)
Secker & Membrey (2003); Secker et al. (2003) [larger study incl. Secker et al., 2002]
Boyce et al. (2008)
To explore what helps successfully employed people with psychiatric disabilities to sustain work
To explore how Clubhouse mem-bers re-estab-lished worker roles
To identify work-place factors as-sociated with job retention in open employment
To explore experiences of successfully mov-ing back into the workforce
Qualitative design; 11 semi-structured interviews; grounded theory analysis; mental health service, San Francisco, USA
Qualitative design; in-depth interviews; narrative analysis; Clubhouse, Eastern Australia
Qualitative design; 51 semi-structured interviews; thematic analysis; 5 employ-ment projects, England
Qualitative design; 20 semi-structured interviews; thematic content analysis; 6 employment support agencies, England
6 people: in com-petitive employ-ment for over 18 months of last 3 years (incl. 4 em-ployed by mental health services)
4 people: Club-house member-ship for over 6 months and in competitive jobs for over 12 months
34 people: 17 in competitive employment for 12 months; 17 work-place managers
20 people: 18 employed in competitive jobs: 2 in supported settings; duration: 9 for 6 months or less; 6 for 1–4 yrs; 5 for over 7 yrs.
Primary motivators for sustaining employment were values related to work, satisfaction, and feeling better working, despite setbacks. Active problem solving was used to address obstacles (policy, medication, entitlements, workplace and personal issues). Seek-ing diverse supports (services, work-based, inner strengths) enabled success in jobs.
Four impelling forces contributed to each person’s sense of self as a worker: (1) ongoing support from significant others; (2) personal meaning in work; (3) opportunities created by Clubhouse membership to develop support networks; and (4) self-managing struggles with illness.
Difficulties in work attributed to many issues; com-mon concerns were effects of medication, confidence, energy and stamina, unfamiliar or daunting job tasks, and the work environment. Adjusting work hours, schedules, and tasks were crucial to job retention, as were natural workplace supports in (1) training and support to learn; (2) relationships with colleagues; (3) workplace culture; and (4) staff management.
Moving back into jobs included facing perceived stigma about mental illness, fear of disclosing & disjointed work history; occupational health clear-ance was an unanticipated barrier. Job satisfaction factors included finding a balance between work demands and challenges; a sense of achieving and contributing; using and expanding work skills; more structured days; social contact; and financial reward.
Factors contributing to success in gaining and sustaining employment

Fossey & Harvey
306 Revue canadienne d’ergothérapie décembre 2010 77(5)
Citation Purpose Design & location Participants Findings – overall themes
Factors contributing to success in gaining and sustaining employment
Cunningham et al. (2000)
Henry & Lucca (2004)
Honey (2003, 2004)
Huff et al. (2008)
Killeen & O’Day (2004)
Kirsh (2000c)[larger study incl. Kirsh, 2000a, 2000b]
Krupa (2004)
To understand factors related to gaining and maintaining employment
To identify what contributes to job success from consumer & staff perspectives
To explore employment benefits and drawbacks and their influence on employment experiences
To explore reasons influencing stay-ing in or leaving jobs and uncover factors affecting job tenure
To explore experi-ences of employ-ment and service systems provid-ing income sup-port, vocational rehabilitation, & mental health care
To explore mean-ing of work and its important elements from consumers’ view-points
To advance theory about the processes in recovering work participation for individuals diagnosed with schizophrenia
Qualitative compari-son; semi-structured interviews; thematic analysis; Assertive Community Treat-ment (ACT), Michigan, USA
12 focus groups; grounded theory analysis; Clubhouse and SE services, Mas-sachusetts, USA
Grounded theory; 76 unstructured interviews & 2 focus groups; employment services, mental health services & a consumer group, New South Wales, Australia
Grounded theory; 51 interviews; constant comparative method of analysis; 9 SE pro-grams, Kansas, USA
Qualitative design; 32 semi-structured interviews; analytic approach unspecified;vocational rehabilita-tion, support groups, & consumer-run services, Southeastern USA
Grounded theory; 36 semi-structured interviews; mental health service, Ontario, Canada
Multiple case study method; in-depth interviews; grounded theory analysis; Ontario, Canada
17 people: 6 employed for over 6 months and 5 employed up to 4 months (mini-mum–moderate wage jobs); 6 not gained jobs.
74 people: 44 consumers (50% employed, most part-time); 30 em-ployment service providers.
41 people: 25 employed (15 in competitive jobs; 9 in mental health services as advo-cates or in paid rehabilitation); 15 unemployed; 5 seeking jobs; 1 unknown.
51 people: 26 stayed in jobs past 6 months; 26 left jobs within 6 months.
32 people in cur-rent or previous receipt of social security benefits due to psychiatric disability: 16 in competitive jobs for over 12 months; 16 seeking jobs
36 people: 17 in competitive jobs for at least 6 months & 19 left competitive jobs in last 6 months
3 people: 2 long-term employed (13 & 20 years); 1 unemployed (7 years); others in participants’ social networks; & rel-evant documents
Three differentiating factors were(1) ways in which people talked about their illness; (2) ways in which people talked about work; (3) strat-egies described for coping with bad days.
Person and environment factors contributed to job success: 1) strong consumer-provider relationships and individualized services considered instrumental in consumers’ achieving vocational goals; 2) Service system issues, entitlements & stigma re people with mental illness as employees were key barriers.
When making job-related decisions, issues in six domains (societal context of employment, social networks, mental health issues, job properties, dis-closure, alternatives to employment) were actively weighed up to maximize the benefits of employ-ment and minimize its drawbacks. Effects of mental illness on employment experiences related to goals, confidence, work performance, and maintaining well-being.
Individuals’ staying or leaving jobs relates to in-terests in the work, including its challenge, variety, demands, and flexibility; supervisors’ and co-workers’ support; sense of competence or confidence; physi-cal and mental well-being; and material issues with transport and money/wages.
Beliefs and expectations about work, employment bar-riers, and advancement into skilled work contribute to success. Low expectations embedded in policies and programs, and limited access to education & training, were overcome with diverse strategies to get jobs and further careers: (1) positive messages about future po-tential; (2) obtaining funds for, and pursuit of education & training; (3) collaborative relationships with service providers; (4) peer and community support.
Three themes frame relationships between work-ers, work, and workplaces: (1) Meaningfulness of work for wellness & fulfillment of needs; (2) Impact of workplace on job satisfaction, stress, & tenure; (3) Supervisory and co-worker relations affect the qual-ity of work life and job sustainability.
Work participation and persistent symptoms co-exist; ongoing efforts to integrate illness experiences and personal strengths & negotiate difficulties in work are necessary by (1) appraising work interests, goals, skills and resources through participation; (2) recognizing and managing illness experiences within the work context; (3) developing a vigilant at-titude toward symptom emergence; (4) capitalizing on strengths & resources; (5) viewing work problems as universal struggles; (6) developing a public image as a regular worker.

Fossy & Harvey
Canadian Journal of Occupational Therapy December 2010 77(5) 307
Citation Purpose Design & location Participants Findings – overall themes
Factors contributing to success in gaining and sustaining employment
Larson et al. (2007)[part of larger SE program evaluation]
Shankar (2005)[larger study incl. Shankar & Collyer, 2003]
Tse & Yeats (2002)
Woodside et al. (2006)
To explore ben-efits and costs of employment
To explore the ongoing support needs of people with psychiatric disabilities in open employ-ment
To explore fac-tors that help people succeed in employment and explain var-ied outcomes
To gain insights about vocational success following at least one epi-sode of psychosis
Qualitative compo-nent; 89 individual in-terviews using stages of change framework; thematic & content analysis; SE program, Chicago, USA
Qualitative design; semi-structured interviews; thematic analysis; vocational rehabilitation & SE services, New South Wales, Australia
Grounded theory; 67 semi-structured interviews; grounded theory analysis; Bipolar disorder regis-ter, New Zealand
Qualitative design; 8 semi-structured interviews; grounded theory analysis; an early intervention program (EIP), Ontario, Canada
89 people receiv-ing SE for one year: 30 in com-petitive employ-ment (full time or part time); 59 unemployed
36 people fol-lowed up 6 months after gain-ing employment: 25 sustained jobs; 11 had stopped working
67 people diag-nosed with bipolar disorder: 61% employed part time or full time
8 people with return to work goals: 6 in competitive employment; 2 unemployed.
Financial, emotional, cognitive, behavioural, and interpersonal benefits and costs were identified by employed and unemployed participants. Employed group identified issues in real work situations, of which unemployed persons may not be aware, which may impact employment outcomes in both groups.
Sustained employment brought positive change in familial relations, financial situations, and optimism about the future. Ongoing employment support helped in varying intensity over time. Wariness of disclosing for fear of discrimination, experiences of relapse, and stressful workplaces contributed to giv-ing up jobs and reluctance to re-enter workforce
Return to work was helped by regaining reason-able control over symptoms, while “goodness of fit” among four factors helped to explain varied vocational outcome: (1) personal attributes & health status: (2) support within workplace & outside work; (3) meaning, nature, & structure of work itself; (4) contexts: societal attitudes, government support, economy.
Identified what was helpful to vocational success: (1) self-assessing mental health to continually monitor one’s ability to work & continue working; (2) working hard to figure out how to get life back on track and to regain health; and (3) feeling connected to others, welcomed, and respected at work.
Perspectives of job seeking and prospects of employment
Alverson et al. (2006)[part of a randomised controlled trial (RCT); Mueser et al., 2004]
Bassett et al. (2001)
Krupa et al. (1998)
To identify fac-tors associated with success or failure to secure meaningful com-petitive employ-ment
To identify the issues for young people diag-nosed with psychosis and wanting jobs
To examine the nature of stress experienced dur-ing the process of negotiating employment
Ethnography; intensive participant observation & infor-mal interviews over 12 months; Clubhouse and IPS programs, Hartford, CT, USA
Qualitative design; 2 focus groups: the-matic analysis; early intervention program (EIP), Queensland, Australia
Qualitative design; 16 open-ended interviews; the-matic analysis; 2 SE programs, Ontario, Canada
25 of 204 people in RCT, incl. 13 IPS clients; 12 Club-house program clients: 9/25 in one competitive job for at least 30 days
10 young people (18–25 yrs): past or present EIP pro-gram clients with sporadic work his-tory; work status unspecified
16 people: 10 consumers (6 in competitive jobs; 4 actively seeking jobs); 6 employ-ment co-ordina-tors
Two job search styles identified: “active” job seeking (active search within & beyond vocational service) and “passive” job seeking (uncertain about work-ing, feeling unstable, relying on vocational service support). IPS program enhanced “active” job seeking; other job seekers were older, more selective about jobs, had longer illness experience & less familial contact.
Identified losses (in relationships, abilities, job pros-pects, dreams, confidence, self-esteem, body image); stigma of disclosure in job seeking and relation-ships; negative treatment experiences; difficulties in identifying vocational goals; and need for assistance to pursue these goals.
Job seeking is stressful, requires persistence, and means being disadvantaged in the job market and adopting specific strategies: (1) a helpful frame of mind; (2) behavioural strategies to present favour-ably; and (3) getting support to offset the disad-vantage and stress. Employment co-ordinators described efforts to minimize demanding aspects of job searching and inherent tensions in matching client interests, experience, and job market options.

Fossey & Harvey
308 Revue canadienne d’ergothérapie décembre 2010 77(5)
Gewurtz and Kirsh (2007) and Honey (2004), respectively, of how mental health consumers weighed their potential for work-ing and the benefits and drawbacks of employment; and Secker and colleagues’ analysis of multiple perspectives to understand how job retention and breakdown relate to natural workplace supports and differing service approaches to job seeking and support (Secker & Membrey, 2003; Secker, Membrey, Grove, & Seebohm, 2002; Secker et al., 2003). Hence, individually, few of these studies are reported rigorously in methodological and interpretive terms, but together they do illuminate the com-plexity of establishing a working life and why people persevere but also sometimes discontinue working.
Themes Identified Across the Reviewed StudiesFour main themes were synthesized from the findings across these twenty studies: (a) employment has varied meanings, benefits, and drawbacks to weigh up; (b) strategies for main-taining employment and mental health are important and both require ongoing active self-management; (c) diverse supports within and beyond the workplace are helpful; and (d) systemic issues add to the employment barriers that are faced by people experiencing mental ill-health. Each is discussed.
Employment has varied meanings, benefits, and drawbacks to weigh up.
Wide-ranging benefits of being employed were identified by people with mental ill-health in these qualitative studies: remuneration, greater autonomy, status and acceptance within society, structured use of time, a sense of purpose or focus, feeling productive and useful to others, affirmation of ability, and opportunities for social contact and personal development (Auerbach & Richardson, 2005; Boyce et al., 2008; Cunning-ham et al., 2000; Honey, 2004; Kirsh, 2000c; Marwaha & John-son, 2005; Tse & Yeats, 2002). This accords with consumer-led survey findings (McQuilken et al., 2003) and benefits noted in the general population (Marwaha & Johnson).
through mental health or vocational services, with two studies including agency staff (Henry & Lucca, 2004; Secker & Mem-brey, 2003; Secker et al., 2003). Most studies did not specify the nature of the participants’ employment, but some indicated that participants were employed in wide-ranging jobs, pre-dominantly in the administrative, domestic, and food service sectors, but also in advocacy, community service, and support roles (Boyce et al., 2008; Cunningham, Wolbert, & Brock-meier, 2000; Honey, 2003; 2004). Others provided illustrative examples in which similar jobs were represented (Huff, Rapp, & Campbell, 2008; Kennedy-Jones, Cooper, & Fossey, 2005; Killeen & O’Day, 2004; Krupa, 2004; Shankar, 2005).
In terms of study design, nine studies were informed by a grounded theory approach; one used a narrative approach (Kennedy-Jones et al., 2005); and another was an ethnographic substudy in a randomized trial of supported employment (Alverson, Carpenter, & Drake, 2006). The remaining studies were of unspecified type. Most used interviewing, whatever their methodology, and one study specified the involvement of consumer researchers in developing the interview guides and interviewing so as to enhance the understanding and repre-sentation of participants’ views (Krupa, Lagarde, Carmichael, Hougham, & Steward, 1998).
Qualitative research lends itself to in-depth studies in which the richness of the data relies on purposeful or theo-retical sampling rather than solely on sample size (Fossey et al., 2002). Yet, few reports contained detailed accounts of sampling, data collection, or analytic procedures, making their methodological quality difficult to evaluate. The find-ings in most reports were presented descriptively with illustra-tive quotations to support the themes. Fewer authors offered explanatory frameworks to account for connections between themes or participants’ views as a whole, which is considered to characterize qualitative research of higher quality (Daly et al., 2007). Examples of the latter include the thematic compari-sons of differing employment experiences and ways of talking about illness, work, and coping provided by Cunningham and colleagues (2000); the explanatory frameworks presented by
Citation Purpose Design & location Participants Findings – overall themes
Perspectives of job seeking and prospects of employment
Marwaha & Johnson (2005)
Gewurtz & Kirsh (2007)
To identify perspectives of employment of people with psy-chotic disorders
To explore how mental health team clients come to under-stand their po-tential for work
Qualitative design; 15 semi-structured interviews; thematic analysis; community mental health team(CMHT), London, UK
Grounded theory; 10 semi-structured interviews; constant comparative analysis; CMHT, Ontario, Canada
15 people: 3 employed, 4 volunteering or in sheltered work, 8 unemployed (all had worked)
10 people receiv-ing case manage-ment & employ-ment support: 6 in part-time work, including paid and volunteer roles; 2 in other produc-tive roles; 2 not in any work roles.
Working was seen as desirable, mixed with substan-tial concerns about ability to work, the “benefits trap,” managing medication at work, and relapsing at work. Fears about disclosure, discrimination by employers, and lack of help from services colored the perceived prospects of finding work.
Ideas about potential to work developed through cycles of doing and becoming, in which work characteristics and support were important: (1) doing paid and unpaid work enabled discovery of readiness, options, capabilities, and challenges; (2) experiences of doing enabled growing awareness of a possible work future and uncertainties; in the absence of doing, “stuckness” and hopelessness were felt.

Fossy & Harvey
Canadian Journal of Occupational Therapy December 2010 77(5) 309
unable to perform their jobs. Hence, mental health issues were considered an ongoing aspect of dealing with employment (Gewurtz & Kirsh; Henry & Lucca; Kirsh, 2000c; Krupa).
Another source of stress was the workplace itself, includ-ing the physical conditions and demands of job tasks, inter-personal aspects of work situations, with symptoms sometimes amplifying the other stresses (Henry & Lucca, 2004). Thus, workers with mental ill-health spoke of actively monitoring their stress levels; managing these difficulties as a source of pride and resilience (Auerbach & Richardson, 2005; Krupa, 2004); and seeking to avoid work situations considered overly stressful (Honey, 2003; Kennedy-Jones et al., 2005; Kirsh, 2000c). Employed and unemployed mental health consumers alike expressed ongoing concerns that employment might lead to a relapse (Henry & Lucca; Honey; Krupa et al., 1998). Hence, efforts to monitor one’s mental health and to cope with work-place stresses were considered part and parcel of maintaining one’s employment (Auerbach & Richardson; Kirsh; Krupa; Tse & Yeats, 2002; Woodside et al., 2006).
Varied self-management strategies were reported for staying well and coping with bad days at work (Cunningham et al., 2000; Honey, 2003; Krupa, 2004; Tse & Yeats, 2002; Woodside et al., 2006). They included vigilance towards the occurrence of symptoms in the workplace (Krupa); adopting constructive attitudes and problem solving towards work diffi-culties (Auerbach & Richardson, 2005) or viewing work prob-lems as universal struggles (Krupa); and seeking the right kind of work to offer satisfaction and minimize potentially stress-ful aspects of employment (Auerbach & Richardson; Henry & Lucca, 2004; Huff et al., 2008; Kirsh, 2000c; Tse & Yeats). For example, specific job properties important for effective work-ing included jobs connected with personal values and interests; varied tasks; some routine to follow; flexibility in one’s work schedule; and regular breaks (Gewurtz & Kirsh, 2007; Huff et al.; Tse & Yeats), for which work adjustments were sometimes seen as helpful (Secker et al., 2003). These findings add support to Krupa’s finding that maintaining employment and mental health necessitates developing an awareness of what works for oneself through experience and ongoing use of self-manage-ment strategies to capitalize on strengths and to negotiate dif-ficulties. Likewise, actively doing paid or unpaid work enabled participants in Gewurtz and Kirsh’s study to discover their potential for working, whereas Bassett et al. (2001) noted that young people with neither employment nor related life experi-ences lacked strategies to manage work issues.
Diverse supports within and beyond the workplace are helpful.Consumer viewpoints consistently emphasize diverse sup-ports as helpful for sustaining jobs, dealing with work issues, and facilitating job seeking (Gewurtz & Kirsh, 2007; Huff et al., 2008; Kennedy-Jones et al., 2005; Killeen & O’Day, 2004; Kirsh, 2000c; Secker & Membrey, 2003; Secker et al., 2003; Shankar, 2005; Tse & Yeats, 2002). These include support within the workplace, but also beyond it from family or friends and sometimes from services.
Gaining employment held specific meanings in creating a sense of wellness: feeling better, improved relationships, more positive self-appraisals, and greater optimism being reported (Auerbach & Richardson, 2005; Kennedy-Jones et al., 2005; Kirsh, 2000c; Krupa, 2004; Shankar, 2005). These same factors were seen as helpful in sustaining employment through times of setbacks (Auerbach & Richardson), and in the process of recovering (Gewurtz & Kirsh, 2007; Kirsh; Krupa). The mean-ings and benefits attributed to working were also framed by people’s perspectives of employment and mental health issues. For example, employed clients of an ACT program in the U.S. spoke of work as a necessary activity with many of the afore-mentioned benefits and of illness as one piece of themselves, whereas unemployed clients spoke of illness as overwhelming and emphasized experiencing barriers to employment (Cun-ningham et al., 2000). As these authors suggest, experiences of success and setbacks in maintaining employment or health are also likely to contribute to these differing framings. Indeed, several studies suggest the valuing of employment is accompa-nied by facing losses, including previous job loss, altered career trajectories and a sense of disadvantage, as well as doubts and uncertainties about future work prospects and capabilities (Bassett, Lloyd, & Bassett, 2001; Gewurtz & Kirsh; Honey, 2003; Kirsh, 2000a; Krupa et al., 1998; Marwaha & Johnson, 2005).
The interplay between workers, jobs, and their employ-ment contexts also contributed to how participants viewed the meaning and benefits of employment, as several grounded theory-informed studies highlighted. For instance, according to Honey (2004), mental health consumers actively weighed up job-related, social, and societal factors when making employment-related decisions as well as their perceived alter-natives to employment and its benefits and drawbacks for their mental health. Kirsh (2000c) similarly reported that partici-pants sought a balance between perceived beneficial aspects of employment and sources of workplace stress seen as affect-ing the quality and sustainability of a working life. Further, her study highlighted the importance of congruence between per-sonal and workplace values for sustaining employment (Kirsh, 2000a, 2000b).
Strategies for maintaining employment and mental health are important. Workers with mental ill-health across several studies viewed maintaining employment and mental health as each requiring ongoing work (Cunningham et al., 2000; Gewurtz & Kirsh, 2007; Henry & Lucca, 2004; Honey, 2003; Krupa, 2004; Wood-side, Schell, & Allison-Hedges, 2006). Those with sustained employment described varied ongoing difficulties in work, rarely attributable solely to mental health issues (Henry & Lucca; Honey, 2003, 2004; Krupa; Secker & Membrey, 2003; Secker et al., 2003) but including sensitivity to stress, medi-cation effects, difficulties with thinking, confidence, energy, or relating to people, and the constant threat of getting sick (Honey, 2003). Honey reported that such difficulties made working more difficult, stressful, and sometimes less enjoyable for participants, but did not necessarily mean participants were

Fossey & Harvey
310 Revue canadienne d’ergothérapie décembre 2010 77(5)
Connections with peers and family. Family and friends’ encouragement, recognition of achieve-ments, and assistance with access to employment, education, or training was considered crucial to achieving vocational aspira-tions in several studies (Henry & Lucca, 2004; Kennedy-Jones et al., 2005; Killeen & O’Day, 2004; Tse & Yeats, 2002). People described support of peers, including friends, support groups, and other community groups, as helpful to sustain employ-ment (Killeen & O’Day). Feeling connected to peers engaged in similar struggles provided inspiration and non-threaten-ing support at times of difficulty (Henry & Lucca; Killeen & O’Day). Further, Alverson et al.’s (2006) ethnographic findings suggest familial and cultural values regarding employment, as well as the availability and closeness of kinship networks, may influence how people seek jobs: those with stronger family ties and reciprocal relationships reportedly sought job-seeking help through familial networks and services. Whether families contributed to this study is unclear from the report, but the study is unusual in considering people’s familial and cultural contexts as potential resources or barriers to employment.
Support from employment specialists and mental health services.
From the viewpoint of consumers, support from employment specialists and mental health professionals may help to sus-tain employment as well as to obtain jobs. Strong collaborative relationships with service providers, from which participants gained a sense of optimism, interest, and encouragement in their pursuit of vocational goals, were particularly emphasized (Henry & Lucca, 2004; Kennedy-Jones et al., 2005; Killeen & O’Day, 2004). Further, Shankar’s (2005) findings suggest ongoing employment support may be more helpful in varying intensity over time: participants in this study preferred to draw on support workers’ guidance but to address problems in the workplace for themselves.
Job seekers described the search for employment as particularly demanding, given the time, emotional energy, personal strength, and perseverance required (Honey, 2004; Krupa et al., 1998; Marwaha & Johnson, 2005). Disclosure issues, disrupted careers and losses of dreams, income, job prospects, and social contact were identified as contributing factors (Bassett et al., 2001; Honey, 2003; Kirsh, 2000a), and added to a sense of being disadvantaged in the labour market (Honey; Krupa et al.; Marwaha & Johnson). Krupa et al.’s study reported a range of attitudinal and behavioural strategies that participants used to persist in searching for employment and cope with the demands of job seeking. This study also high-lighted the potential importance of employment support ser-vices to offset the stresses involved in job seeking, while several others indicate that the practices of employment programs can also impede people’s obtaining and keeping jobs (Gowdy et al., 2003; 2004; Henry & Lucca, 2004; Killeen & O’Day, 2004; Secker et al., 2002). Identified issues include low expectations embedded within policies and practices regarding clients’ interest in employment and eligibility for employment support and differing perspectives among clients, employment special-ists, and mental health staff on employment. In addition, lim-
Support within workplaces.Interactions and relations at work have bearings on job sat-isfaction and retention, but also on job stress, issues around disclosure, and decisions to leave jobs. For instance, encour-agement, acknowledgment of individuals’ strengths, and prac-tical assistance from work colleagues generated a sense of being welcomed, respected, and supported at work (Killeen & O’Day, 2004; Tse & Yeats, 2002; Woodside et al., 2006). Employed par-ticipants in Kirsh’s (2000c) study appreciated respectful, fair, and supportive communication with supervisors, whereas those who had left jobs described the absence of such rela-tionships, attributing added job stress to this lack of support. Further, drawing on interviews with employees experiencing mental ill-health and their workplace managers, Secker and Membrey (2003) identified important natural workplace sup-ports, provided over and above specific work adjustments, that some employees had negotiated. These included training and support for people to learn new jobs, workplaces that encour-aged positive relationships between colleagues and an accept-ing workplace culture, and a constructive approach to staff management. Hence, these authors recommend promotion of natural supports in workplaces as potentially enabling people experiencing mental ill-health to retain their jobs without the need for disclosure.
Disclosure of mental health issues in the workplace was a repeatedly raised concern of workers and jobseekers alike. Pos-itive and negative disclosing experiences were each described (Boyce et al., 2008; Killeen & O’Day, 2004; Kirsh, 2000c; Tse & Yeats, 2002), including stories of supportive supervisors who “stuck by” people and responded with understanding when they needed time off to cope with stress or to attend appoint-ments, enabling them to continue working through difficult times. However, after disclosing information about their men-tal health to work colleagues, participants in some studies described their confidences being broken and experiencing negative social repercussions at work, including being ignored or over-protected (Auerbach & Richardson, 2005; Honey, 2004; Kirsh; Shankar, 2005). These reactions made people wary to disclose (Kirsh; Shankar; Tse & Yeats), encouraged efforts to conceal signs of ill-health at work (Kirsh; Krupa, 2004), and to weigh protection of themselves and their privacy against the possible gains in workplace support (Auerbach & Richardson; Honey; Kirsh).
Workers’ concerns about attending appointments for medication, health care, or employment support during regu-lar working hours added to the issues surrounding disclosure (Marwaha & Johnson, 2005; Shankar, 2005). So, dilemmas around disclosure were a source of substantial anxiety and ongoing stress at work; energy devoted to hiding illness, or struggles with demanding aspects of work, seemed to reduce job satisfaction and success (Kirsh, 2000c); and concerns about disclosing health information appeared to contribute to deci-sions about leaving jobs (Shankar, 2005). Facing fears of dis-crimination if they disclosed mental ill-health to prospective employers were also part of the job-seeking experience (Bas-sett et al., 2001; Boyce et al., 2008; Krupa et al., 1998; Marwaha & Johnson; Shankar).

Fossy & Harvey
Canadian Journal of Occupational Therapy December 2010 77(5) 311
about complex, easily misunderstood income support regula-tions (Henry & Lucca; Killeen & O’Day; Marwaha & Johnson) and potential loss of healthcare coverage and medication sub-sidies (Honey; Tse & Yeats), as well as poor access to trustwor-thy benefits advice seemed to exacerbate these issues for study participants.
DiscussionUndertaking a qualitative metasynthesis presents a number of challenges. These include not only whether studies adopt-ing different research perspectives and methodologies should be included, but also the contested question of how best to appraise the quality of individual qualitative studies (Daly et al., 2007; Fossey et al., 2002; Gewurtz et al., 2008). To ensure a focused research question, we excluded some studies on topi-cal grounds but none on methodological grounds for two rea-sons. First, the methodological approaches of some reviewed studies were unstated and could only be surmised, but all used recognizable qualitative methods and textual means to repre-sent participants’ perspectives of direct relevance to the topic. Second, as Campbell et al. (2003) also noted, the accounts of sampling, data collection, or analytic procedures in many stud-ies were lacking in detail. There are exceptions, such as Krupa’s (2004) description of purposeful sampling and Honey’s (2004) account of her grounded theory-building approach, but improved reporting is needed if methodological quality is to guide inclusion and exclusion decisions.
A further challenge for qualitative metasynthesis is that of interpreting findings across different studies at a distance from the perspectives and contexts represented in individual stud-
ited funding and support to access education or training were reported barriers to career development and advancement into skilled work (Killeen & O’Day).
Systemic Issues Add to the Employment Barriers FacedThreats to income support or social security benefits are widely reported employment barriers among people experiencing mental ill-health (McQuilken et al., 2003; Secker, Grove, & Seebohm, 2001) and may discourage the use of employment support programs (MacDonald-Wilson, Rogers, Ellison, & Lyass, 2003). The reviewed qualitative studies point to the complexity of the financial situation in which people receiv-ing income support benefits find themselves with respect to employment and welfare entitlements internationally (Henry & Lucca, 2004; Honey, 2004; Marwaha & Johnson, 2005; Tse & Yeats, 2002), albeit that welfare systems and entitlements differ between countries. For example, from their UK study, Mar-waha and Johnson reported participants would prefer being employed to relying on income support, but found themselves in a “benefits trap” wherein they could not obtain jobs with sufficient wages to avoid loss of income. Hence, loss of benefit entitlements acted as a deterrent to seeking part-time employ-ment on health grounds (Marwaha & Johnson). Findings of another UK study (Secker et al., 2003) concurred, whereas studies from the U.S. reported that people either felt supported to work part-time or stuck in part-time positions and unable to gradually increase their work hours due to disincentives to full-time employment built into the social security benefits system (Henry & Lucca; Killeen & O’Day, 2004). Uncertainties
Table 2Implications for Enhanced Employment Support
Theme Recommended approaches and strategies
Employment has varied meanings, benefits and draw-backs to weigh up
Strategies for main-taining employment and mental health are important and both require ongo-ing active self- management
Diverse supports within and beyond the workplace are helpful
Systemic issues add to the employment barriers faced
•In-depthandindividualizedassessmentsarerequired,todiscerntheindividualmeaningsofemploymentandtailor support accordingly.
•Processesareneededtoassistconsumers,theirfamiliesandworkers,inweighingupbenefits,drawbacksandoptions for employment.
•Stressmanagement,symptommanagementandself-monitoringtechniquesshouldbeakeyingredientofemployment support.
•Thegrowingknowledgeofhelpfulworkadjustmentsshouldbeintegratedintoresourcesforconsumersandthose supporting them.
•Closercollaborationbetweenconsumersandprogramssupportingthemisnecessarytoshareknowledgeand expertise about mental health and employment-related needs.
•Peersupportandopportunitiesforlearningfrompeersshouldbeincorporatedinemploymentprograms.
•Improvedunderstandingandpromotionofnaturalworkplacesupportsarewarranted.•Specificadviceandcounselingondisclosureofmentalhealthhistoriesintheworkplaceareindicated.•Peersupportforconsumersseekingandmaintainingemploymentshouldbeencouraged.•Moreattentiontofamilyinvolvementisrequired.•Policy,protocolsandtrainingareneededtoaddresslowexpectationsofconsumers’employmentoutcomes
among staff.
•Widelyavailableandaccessiblebenefitsadviceisneeded.•Restrictiverulesaboutearningsforconsumersinreceiptofbenefitsshouldbemodifiedtodecrease
disincentives to work.

Fossey & Harvey
312 Revue canadienne d’ergothérapie décembre 2010 77(5)
tion initiatives (Secker & Membrey, 2003). Occupational therapy researchers undertook 11 of the 20
reviewed studies, whereas the effectiveness of vocational pro-grams for people with persisting mental illness has predomi-nantly been investigated by other disciplines. The reviewed qualitative studies hint that people’s repertoires of employ-ment-related and other occupations, family responsibilities and support beyond work, and understanding of how to balance participation and well-being in the face of persistent health conditions may each affect maintaining employment. These represent several areas in which an occupational perspective and qualitative research can usefully contribute new knowl-edge. Further, the recent emphasis on promoting recovery increases the usefulness of qualitative studies to inform policy and service development (Davidson et al., 2008). Therefore, it behooves occupational therapists to actively use the knowl-edge gained from these studies to initiate strategies aimed at enabling people experiencing persistent mental ill-health to access satisfying and sustainable employment. This also adds to the ways in which occupational therapists can ensure that consumer viewpoints inform service delivery.
ConclusionThis metasynthesis sought to integrate the findings from stud-ies of mental health consumers’ viewpoints regarding finding and keeping employment in integrated workplaces. Notwith-standing the previously described limitations, these consumer viewpoints add to existing understandings and reinforce the importance of attending to the meaning and value of employ-ment in research and practice. Work adjustments, natural workplace supports, self-management strategies, and peer support are among the helpful strategies that occupational therapists and others should pursue to improve employment outcomes for mental health consumers.
Key messages• Consumerviewpointsrepresentedinthismetasynthe-
sis reinforce central ideas about attending to the mean-ing and value of occupations in occupational therapy.
• Improved knowledge of helpfulwork adjustments andnatural workplace supports should be promoted in occu-pational therapy education and used to inform policies and practices aiming to enable sustainable employment.
• Consumer expertise related to self-management andpeer support could be a helpful additional element of employment support and mental health services.
AcknowledgementsAn earlier version of this metasynthesis formed part of the liter-ature review presented in Ellie Fossey’s PhD thesis, supervised by Associate Professor Fiona McDermott (BA Dip Soc Studs., M. Urban Planning, PhD), now at Monash University, whose support and guidance is acknowledged with appreciation.
ies (Gewurtz et al., 2008), particularly if qualitative research reports include relatively little contextual “data.” This is espe-cially challenging since varying terminology and program content make it difficult to appraise the comparability of the mental health and vocational programs (Corbiere & Lecomte, 2007) through which participants were typically recruited. Without access to the original data and detailed knowledge of the diverse study contexts, this is difficult to overcome. Nev-ertheless, there were recognizable views and ideas in common to suggest that the findings could be meaningfully brought together. Recruitment from these services may also account for the importance attached to the support from employment specialists and mental health services reported in some find-ings. Studies conducted through affirmative businesses and other kinds of employer organizations might yield differing findings.
Implications for PracticeA complex range of personal, workplace-related, systemic, and material factors were identified as contributing to finding and sustaining employment from consumer viewpoints. These fac-tors were identified across studies from five English-speaking countries, although specific details of systemic barriers varied by country. Table 2 summarizes approaches and strategies that can be drawn from the identified themes.
In many of the reviewed studies, little mention is made of the types of employment that participants found, yet assistance to weigh up the available options is critical to successful job seeking. This suggests that the process of job matching, which is identified as important but not well addressed within the IPS approach (Kirsh et al., 2005), could be helpfully expanded by enabling such opportunities. Further, people’s trajectories of employment and participation within and beyond paid employment need to be better considered (Becker, Whitley, Bailey, & Drake, 2007; Kravetz et al., 2003). Thus, in-depth exploration to discern the meaning of employment with each individual becomes crucial. This supports central principles in occupational therapy theory and practices about attending to the meaning and value of people’s occupations to enable their participation (Ennals & Fossey, 2009; Krupa et al., 2009). It also suggests that enabling opportunities for consumers to learn from peers who have discovered ways to overcome or mitigate the challenges faced in seeking and re-entering employment may improve employment outcomes.
While ongoing support to sustain employment is recog-nized as a key ingredient of effective vocational services (Kirsh et al., 2005), the reviewed studies highlight some helpful ele-ments of this support that may not have been focused upon. These include support to develop personalized stress manage-ment and self-monitoring strategies for managing both one’s job and mental well-being; attending to disclosing as an ongo-ing process in the workplace; and building natural networks of support in and outside the workplace. In these areas, lessons might be drawn from self-management approaches for people with long-term health conditions (Barlow, Wright, Sheasby, Turner, & Hainsworth, 2002; Jerant, von Friederishcs-Fitzwa-ter, & Moore, 2005), family psycho-educational approaches (McFarlane et al., 2000), and workplace-based health promo-
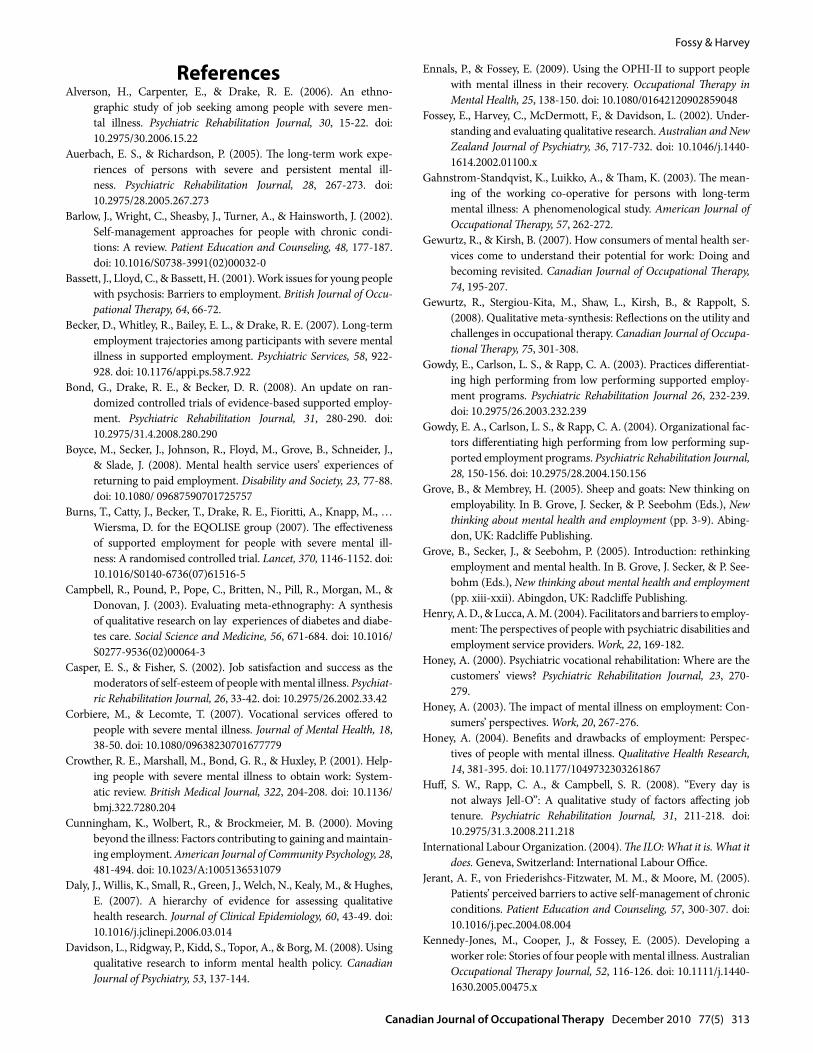
Fossy & Harvey
Canadian Journal of Occupational Therapy December 2010 77(5) 313
Ennals, P., & Fossey, E. (2009). Using the OPHI-II to support people with mental illness in their recovery. Occupational Therapy in Mental Health, 25, 138-150. doi: 10.1080/01642120902859048
Fossey, E., Harvey, C., McDermott, F., & Davidson, L. (2002). Under-standing and evaluating qualitative research. Australian and New Zealand Journal of Psychiatry, 36, 717-732. doi: 10.1046/j.1440-1614.2002.01100.x
Gahnstrom-Standqvist, K., Luikko, A., & Tham, K. (2003). The mean-ing of the working co-operative for persons with long-term mental illness: A phenomenological study. American Journal of Occupational Therapy, 57, 262-272.
Gewurtz, R., & Kirsh, B. (2007). How consumers of mental health ser-vices come to understand their potential for work: Doing and becoming revisited. Canadian Journal of Occupational Therapy, 74, 195-207.
Gewurtz, R., Stergiou-Kita, M., Shaw, L., Kirsh, B., & Rappolt, S. (2008). Qualitative meta-synthesis: Reflections on the utility and challenges in occupational therapy. Canadian Journal of Occupa-tional Therapy, 75, 301-308.
Gowdy, E., Carlson, L. S., & Rapp, C. A. (2003). Practices differentiat-ing high performing from low performing supported employ-ment programs. Psychiatric Rehabilitation Journal 26, 232-239. doi: 10.2975/26.2003.232.239
Gowdy, E. A., Carlson, L. S., & Rapp, C. A. (2004). Organizational fac-tors differentiating high performing from low performing sup-ported employment programs. Psychiatric Rehabilitation Journal, 28, 150-156. doi: 10.2975/28.2004.150.156
Grove, B., & Membrey, H. (2005). Sheep and goats: New thinking on employability. In B. Grove, J. Secker, & P. Seebohm (Eds.), New thinking about mental health and employment (pp. 3-9). Abing-don, UK: Radcliffe Publishing.
Grove, B., Secker, J., & Seebohm, P. (2005). Introduction: rethinking employment and mental health. In B. Grove, J. Secker, & P. See-bohm (Eds.), New thinking about mental health and employment (pp. xiii-xxii). Abingdon, UK: Radcliffe Publishing.
Henry, A. D., & Lucca, A. M. (2004). Facilitators and barriers to employ-ment: The perspectives of people with psychiatric disabilities and employment service providers. Work, 22, 169-182.
Honey, A. (2000). Psychiatric vocational rehabilitation: Where are the customers’ views? Psychiatric Rehabilitation Journal, 23, 270-279.
Honey, A. (2003). The impact of mental illness on employment: Con-sumers’ perspectives. Work, 20, 267-276.
Honey, A. (2004). Benefits and drawbacks of employment: Perspec-tives of people with mental illness. Qualitative Health Research, 14, 381-395. doi: 10.1177/1049732303261867
Huff, S. W., Rapp, C. A., & Campbell, S. R. (2008). “Every day is not always Jell-O”: A qualitative study of factors affecting job tenure. Psychiatric Rehabilitation Journal, 31, 211-218. doi: 10.2975/31.3.2008.211.218
International Labour Organization. (2004). The ILO: What it is. What it does. Geneva, Switzerland: International Labour Office.
Jerant, A. F., von Friederishcs-Fitzwater, M. M., & Moore, M. (2005). Patients’ perceived barriers to active self-management of chronic conditions. Patient Education and Counseling, 57, 300-307. doi: 10.1016/j.pec.2004.08.004
Kennedy-Jones, M., Cooper, J., & Fossey, E. (2005). Developing a worker role: Stories of four people with mental illness. Australian Occupational Therapy Journal, 52, 116-126. doi: 10.1111/j.1440-1630.2005.00475.x
ReferencesAlverson, H., Carpenter, E., & Drake, R. E. (2006). An ethno-
graphic study of job seeking among people with severe men-tal illness. Psychiatric Rehabilitation Journal, 30, 15-22. doi: 10.2975/30.2006.15.22
Auerbach, E. S., & Richardson, P. (2005). The long-term work expe-riences of persons with severe and persistent mental ill-ness. Psychiatric Rehabilitation Journal, 28, 267-273. doi: 10.2975/28.2005.267.273
Barlow, J., Wright, C., Sheasby, J., Turner, A., & Hainsworth, J. (2002). Self-management approaches for people with chronic condi-tions: A review. Patient Education and Counseling, 48, 177-187. doi: 10.1016/S0738-3991(02)00032-0
Bassett, J., Lloyd, C., & Bassett, H. (2001). Work issues for young people with psychosis: Barriers to employment. British Journal of Occu-pational Therapy, 64, 66-72.
Becker, D., Whitley, R., Bailey, E. L., & Drake, R. E. (2007). Long-term employment trajectories among participants with severe mental illness in supported employment. Psychiatric Services, 58, 922-928. doi: 10.1176/appi.ps.58.7.922
Bond, G., Drake, R. E., & Becker, D. R. (2008). An update on ran-domized controlled trials of evidence-based supported employ-ment. Psychiatric Rehabilitation Journal, 31, 280-290. doi: 10.2975/31.4.2008.280.290
Boyce, M., Secker, J., Johnson, R., Floyd, M., Grove, B., Schneider, J., & Slade, J. (2008). Mental health service users’ experiences of returning to paid employment. Disability and Society, 23, 77-88. doi: 10.1080/ 09687590701725757
Burns, T., Catty, J., Becker, T., Drake, R. E., Fioritti, A., Knapp, M., … Wiersma, D. for the EQOLISE group (2007). The effectiveness of supported employment for people with severe mental ill-ness: A randomised controlled trial. Lancet, 370, 1146-1152. doi: 10.1016/S0140-6736(07)61516-5
Campbell, R., Pound, P., Pope, C., Britten, N., Pill, R., Morgan, M., & Donovan, J. (2003). Evaluating meta-ethnography: A synthesis of qualitative research on lay experiences of diabetes and diabe-tes care. Social Science and Medicine, 56, 671-684. doi: 10.1016/S0277-9536(02)00064-3
Casper, E. S., & Fisher, S. (2002). Job satisfaction and success as the moderators of self-esteem of people with mental illness. Psychiat-ric Rehabilitation Journal, 26, 33-42. doi: 10.2975/26.2002.33.42
Corbiere, M., & Lecomte, T. (2007). Vocational services offered to people with severe mental illness. Journal of Mental Health, 18, 38-50. doi: 10.1080/09638230701677779
Crowther, R. E., Marshall, M., Bond, G. R., & Huxley, P. (2001). Help-ing people with severe mental illness to obtain work: System-atic review. British Medical Journal, 322, 204-208. doi: 10.1136/bmj.322.7280.204
Cunningham, K., Wolbert, R., & Brockmeier, M. B. (2000). Moving beyond the illness: Factors contributing to gaining and maintain-ing employment. American Journal of Community Psychology, 28, 481-494. doi: 10.1023/A:1005136531079
Daly, J., Willis, K., Small, R., Green, J., Welch, N., Kealy, M., & Hughes, E. (2007). A hierarchy of evidence for assessing qualitative health research. Journal of Clinical Epidemiology, 60, 43-49. doi: 10.1016/j.jclinepi.2006.03.014
Davidson, L., Ridgway, P., Kidd, S., Topor, A., & Borg, M. (2008). Using qualitative research to inform mental health policy. Canadian Journal of Psychiatry, 53, 137-144.

Fossey & Harvey
314 Revue canadienne d’ergothérapie décembre 2010 77(5)
McFarlane, W. R., Dushay, R. A., Deakins, S. M., Stastny, P., Lukens, E. P., Toran, J., & Link, B. (2000). Employment outcomes in fam-ily-aided assertive community treatment. American Journal of Orthopsychiatry, 70, 203-214. doi: 10.1037/0002-9432.70.2.203
McKay, C., Johnsen, M., & Stein, R. (2005). Employment outcomes in Massachusetts Clubhouses. Psychiatric Rehabilitation Journal, 29, 25-33. doi: 10.2975/ 29.2005.25.33
McQuilken, M., Zahniser, J. H., Novak, J., Starts, R. D., Olmos, A., & Bond, G. R. (2003). The work project survey: Consumer perspec-tives on work. Journal of Vocational Rehabilitation, 18, 59-68.
Mueser, K. T., Clark, R. E., Haines, M., Drake, R. E., McHugo, G., Bond, G. R., … Swain, K. (2004). The Hartford study of supported employment for severe mental illness: Employment and non-vocational outcomes. Journal of Consulting and Clinical Psychol-ogy, 72, 479-490. doi: 10.1037/0022-006X.72.3.479
Quimby, E., Drake, R. E., & Becker, D. R. (2001). Ethnographic findings from the Washington, D.C., vocational services study. Psychiatric Rehabilitation Journal, 24, 368-374.
Rice, P. L., & Ezzy, D. (1999). Qualitative research methods: A health focus. Melbourne, Australia: Oxford University Press.
Secker, J., Grove, B., & Seebohm, P. (2001). Challenging barriers to employment, training and education for mental health service users: The services user’s perspective. Journal of Mental Health, 10, 395-404. doi: 10.1080/ 09638230123559
Secker, J., & Membrey, H. (2003). Promoting mental health through employment and developing healthy workplaces: The potential of natural supports at work. Health Education Research, 18, 207-215.
Secker, J., Membrey, H., Grove, B., & Seebohm, P. (2002). Recover-ing from illness or recovering your life? Implications of clinical versus social models of recovery from mental health problems for employment support services. Disability and Society, 17, 403-418. doi: 10.1080/09687590220140340
Secker, J., Membrey, H., Grove, B., & Seebohm, P. (2003). The how and why of workplace adjustments: Contextualizing the evidence. Psy-chiatric Rehabilitation Journal, 27, 3-9. doi: 10.2975/27.2003.3.9
Shankar, J. (2005). Improving job tenure for people with psychiatric dis-abilities through ongoing employment. 37-47. Retrieved from www.ausienet.com/journal/vol4iss1/ shankar.pdf
Shankar, J., & Collyer, F.(2003). Vocational rehabilitation of people with mental illness: The need for a broader approach. Austra-lian e-Journal for the Advancement of Mental Health, 2,77-89. Retrieved from www.ausienet.com/ journal/vol2iss2/shankar.pdf
Strong, S. (1998). Meaningful work in supportive environments: Expe-riences with the recovery process. American Journal of Occupa-tional Therapy, 52, 31-38.
Tse, S., & Yeats, M. (2002). What helps people with bipolar affective disorder succeed in employment: A grounded theory approach. Work, 19, 47-62.
Waghorn, G., Chant, D., & Whiteford, H. (2002). Clinical and non-clinical predictors of vocational recovery for Australians with psychotic disorders. Journal of Rehabilitation, 68(4), 40-51.
Warner, R. (2004). Recovery from schizophrenia: Psychiatry and polit-ical economy (3rd ed.). London: Routledge.
Woodside, H., Schell, L., & Allison-Hedges, J. (2006). Listening for recovery: The vocational success of people living with mental ill-ness. Canadian Journal of Occupational Therapy, 73, 36-43.
Killackey, E., Jackson, H. J., & McGorry, P. D. (2008). Vocational inter-vention in first-episode psychosis: individual placement and support v. treatment as usual. British Journal of Psychiatry, 193, 114-120. doi: 10.1192/ bjp.bp.107.043109
Killeen, M. B., & O’Day, B. L. (2004). Challenging expectations: How individuals with psychiatric disabilities find and keep work. Psychiatric Rehabilitation Journal, 28, 157-163. doi: 10.2975/28.2004.157.163
Kirsh, B. (2000a). Factors associated with employment for mental health consumers. Psychiatric Rehabilitation Journal, 24, 13-21.
Kirsh, B. (2000b). Organizational culture, climate and person-environ-ment fit: Relationships with employment outcomes for mental health consumers. Work, 14, 109-122.
Kirsh, B. (2000c). Work, workers, and workplaces: A qualitative analy-sis of narratives of mental health consumers. Journal of Rehabili-tation, 66(4), 24-30.
Kirsh, B., Cockburn, L., & Gewurtz, R. (2005). Best practice in occupa-tional therapy: Program characteristics that influence vocational outcomes for people with serious mental illnesses. Canadian Journal of Occupational Therapy, 77, 265-279.
Kravetz, S., Dellario, D., Granger, B., & Salzer, M. (2003). A two-fac-eted work participation approach to employment and career development as applied to persons with a psychiatric dis-ability. Psychiatric Rehabilitation Journal, 26, 278-289. doi: 10.2975/26.2003.278.289
Krupa, T. (2004). Employment, recovery, and schizophrenia: Integrat-ing health and disorder at work. Psychiatric Rehabilitation Jour-nal, 28, 8-15. doi: 10.2975/28.2004.8.15
Krupa, T., Fossey, E., Anthony, W. A., Brown, C., & Pitts, D. (2009). Doing daily life: How occupational therapy can inform psychiat-ric rehabilitation practice. Psychiatric Rehabilitation Journal, 32, 155-161. doi: 10.2975/ 32.3.2009.155.161
Krupa, T., Lagarde, M., & Carmichael, K. (2003). Transforming workshops into affirmative businesses: An outcome evalu-ation. Psychiatric Rehabilitation Journal, 26, 359-367. doi: 10.2975/26.2003.359.367
Krupa, T., Lagarde, M., Carmichael, K., Hougham, B., & Stewart, H. (1998). Stress, coping and the job search process: The experience of people with psychiatric disabilities in supported employment. Work, 11, 155-162. doi: 10.1016/S1051-9815(98)00032-1
Larson, J. E., Barr, L. K., Corrigan, P. W., Kuwabara, S. A., Boyle, M. G., & Glenn, T. L. (2007). Perspectives on benefits and costs of work from individuals with psychiatric disabilities. Journal of Vocational Rehabilitation, 26, 71-77.
Latimer, E. A., Lecomte, T., Becker, D. R., Drake, R. E., Duclos, I., Piat, M., … Xie, H. (2006). Generalisability of the individual place-ment and support model of supported employment: Results of a Canadian randomised controlled trial. British Journal of Psychia-try, 189, 65-73.
MacDonald-Wilson, K. L., Rogers, S., Ellison, M. L., & Lyass, A. (2003). A study of the social security work incentives and their relations to perceived barriers to work among persons with psychiatric disability. Rehabilition Psychology, 48, 301-309.
Marrone, J., & Golowka, E. (1999). If work makes people with mental illness sick, what do unemployment, poverty, and social isolation cause?. Psychiatric Rehabilitation Journal, 23, 187-193.
Marwaha, S., & Johnson, S. (2005). Views and experiences of employ-ment among people with psychosis: A qualitative descriptive study. International Journal of Social Psychiatry, 51, 302-316. doi: 10.1177/0020764005057386

What types of supports are available to employees in social firms?
1
Impetus for study A major barrier to employment for people with mental illness is limited access to supportive and non-discriminatory workplaces. Social firms are an innovative approach to vocational opportunity, which differ in philosophy and practice from traditional vocational rehabilitation approaches. Social firms have existed for over thirty years, and appear to support job tenure for people with mental illness. However, little health and social research has been conducted in order to understand the workings of this model. This study investigated the experiences of eight people employed at a social firm, and the workplace’s characteristics and culture.
What is a social firm?
Mainstream business employing 25-50% staff with a mental illness
Reinvests profits to support the business’ social mission, thus relying on commercial success rather than external funding
Claims to offer a disclosure-friendly and supportive workplace
Where was this study conducted? Acacia was a small high-volume specialist nursery located in outer Melbourne. The business operated as a wholesale and production enterprise supplying chain stores and independent retailers, with some retail output. How was the study conducted? Ethnography aims to explore social processes and culture. The ethnographic research tools included:
Participant-observation: The researcher worked alongside Acacia’s team for two days a week over three months to gain a sense of the workplace, and recorded observations as field-notes.
Interviews: Conducted at the end of the three month fieldwork, these interviews explored the experience of working in the social firm. Interviews were recorded, transcribed and analysed.
Document analysis: To understand how the business defined and promoted itself, the researcher reviewed documents produced by the social firm, as part of her data analysis.
Staff profile
Nine social firm employees (men and women aged 20-52 years) working at Acacia for 4 months to 13 years, including some who had been employed in the business prior to it becoming a social firm.
Most staff reported exposure to mental illness either indirectly through previous work or family members, or directly through personal experience.
Most staff with an identified mental illness found jobs at Acacia through the affiliated employment service and during their first six months of employment were considered supported workers.
What did we find? This study highlights the complexity of working in a social firm, the business and the social processes that occur within this environment (Diagram 1).
Acacia was a responsive and nurturing environment that enabled worker identity, skill development and social membership.
Even in a supportive and disclosure-friendly workplace, ‘knowing’ about mental illness is a complex social process bound up with challenging pervasive societal attitudes about the capability of workers with mental illness, and fostering support, respect and an appreciation of diversity.
Diagram 1: Social and business processes interconnecting to create a unique workplace environment
2
Social processes
Knowing-not knowing
Knowing-responding
Knowing-supporting
Knowing-seeing-understanding
Knowing-normalising
Business processes
Managing the pressures
Investing in social
& business outcomes
Our business or someone else’s?
Cultivating
opportunity
Social processes
Knowing-not knowing
Knowing-responding
Knowing-supporting
Knowing-seeing-understanding
Knowing-normalising
Social processes
Knowing-not knowing
Knowing-responding
Knowing-supporting
Knowing-seeing-understanding
Knowing-normalising
Business processes
Managing the pressures
Investing in social
& business outcomes
Our business or someone else’s?
Business processes
Managing the pressures
Investing in social
& business outcomes
Our business or someone else’s?
Cultivating
opportunity
Cultivating
opportunity
Business processes at Acacia The business faced internal, external and existential pressures associated with its operation.
Acacia faced the types of pressures that all businesses face – competition, industry pressures, drought; and internal pressures related to resources, staff, time and money.
Its social mission added another layer of complexity that did not necessarily offer particular market leverage or advantage, yet for workers ‘added value’ to being part of the business (see Figure 1).
The workplace was highly adaptable and was organized in a way that buffered the potential for constraints on productivity and related work pressures.
The impacts of mental illness, and the challenges of managing it, were nonetheless experienced differently across the organization.
Social processes at Acacia ‘Knowing’ about mental illness was a prism for issues of identity, status, stigma, and discrimination in workplaces.
Challenging and interesting Greater confidence Greater understanding of mental illness
Develop skills
Changed attitudes Friendly, patient and secure workplace
Sense of responsibility and investment
Change over time
Rewarding to see change All employees related to ‘normally’ and naturally
Positive and inspiring interactions
Social network
Enhanced purpose and value of work
Being given a chance
Opportunity to experience diversity
Being accepted
Figure 1. Acacia: An added value business
The way that mental illness was understood and navigated at Acacia involved a complex set of social processes. Workers frequently spoke about the idea of ‘knowing’ about co-worker’s mental illnesses and the responsibilities, concerns and feelings that this evoked.

Diagram 2: Social processes of ‘knowing’ about mental illness in the workplace
3
KNOWING
Not k
nowin
g
Supportin
g
Responding
Seein
g
& u
nderstandin
g
Normalising
KNOWING
Not k
nowin
g
Not k
nowin
g
Supportin
g
Supportin
g
Responding
Responding
Seein
g
& u
nderstandin
g
Seein
g
& u
nderstandin
g
NormalisingNormalising
Knowing-not knowing: There was no consensus on what should be ‘known’ or ‘not known’ at Acacia. ‘Knowing’ could lead to judgments about work performance. On the other hand, ‘knowing’ could be quite useful. Knowing-responding: Knowing could enable “basic workplace safety” and the ability to respond sensitively and mindfully to employee needs. Knowing-supporting: Knowing could help workers make sense of mental illness and be supportive. Workers drew on past experience with mental illness, or resources of common sense and treating people as equals. They acknowledged that much of their actual knowledge was acquired ‘on the fly’, despite basic training in mental illness awareness. Knowing-normalising: Knowing about mental illness in the workplace carried a responsibility that all workers recognised – maintaining normalcy and balancing the delicate tension of knowing-not knowing.
Knowing-understanding-seeing: Because mental illness was acknowledged in the workplace, workers felt understood. Understanding, in turn, enabled ‘seeing’ individuals for who they were and for their worker contribution. Safe and small size Good communication
Nature of people Clear and basic expectations
Equal regard and treatment Diversity supported
Flexibility as needed Trust and familiarity
Positive interactions Mindfulness
Understanding Supported learning -demonstration and patience
Willingness to accommodate
Figure 2: Types of supports identified at Acacia
Navigating the social-business tension created an avenue for cultivating opportunity.
Cultivating support Acacia was characterized by adaptability, mindfulness, and responsiveness in how work tasks were organised and assigned; in its willingness to be flexible; its understanding of the employees whom it suited most; and the naturally occurring
“I don’t want to ‘know’ so that I can discriminate and ‘I
don’t want to know’ so that I cannot
discriminate”
I think the principles of treating people as adult
equals has served us well, so that you start
out as you mean to…exactly as you would relate to anybody else.
“Fitting in here was really that the people in the nursery were
just good, empathetic people…”
"They felt comfortable coming into the
organisation because their situation was known. It wasn’t
something that anyone was trying to hide…or
worry about being exposed as someone with a mental health
condition."
“Just a general sense of open mindedness towards… what might appear in another workplace as apparent
eccentricity (smile) … That for me has made the workplace… a very secure, friendly place to be”.

4
supports provided the workplace (Figure 2).
Cultivating identity At Acacia, difference was accommodated for and diversity valued. Employees were able to focus on developing their personal and worker identity because they knew that they did not have to fear discrimination on the basis of mental illness. Workers were not made to feel that they were one-way recipients of support, rather they had something to offer the workplace.
Cultivating understanding Knowing about mental illness required a balance – knowing enough to be able to support co-workers, but being aware how ‘knowing’ could also play into existing preconceptions about the ability of people with mental illness to work. This workplace highlighted the important role of sharing normalising experiences as a way to break down stigma. However, the need for debriefing – or ‘supporting the supporters’ became apparent since workers wanted to feel secure, competent and listened to with regard to supporting their colleagues. Cultivating participation Being part of the social firm fostered a sense of investment and healthy critique amongst staff. However this sometimes translated to frustration about the way that the social agenda was conducted. As with many organisations, workers perceived a dissonance between how the workplace was understood by external stakeholders and their own view on the ground. This suggests the importance of participatory mechanisms to support workers’ sense of investment in the business.
What does this mean for social firms? This study highlights:
The value of natural supports when accommodating employees with mental illness;
The importance of workplace adaptability and responsiveness;
The challenges of understanding and working with mental illness;
The need for enhanced workplace knowledge about mental illness, better-defined support structures in the workplace and improved participatory workplace practices.
This study raised valuable questions about the purpose of social firms and the possibilities they hold for advancing economic and social opportunity for people with mental illness. Social firms have the potential to move beyond limitations associated with traditional vocational rehabilitation approaches, by virtue of their systemic approach to creating supportive work environments, and being situated in the business, rather than rehabilitation world. To extend the evidence base for social firms, future research should focus on the environmental and systemic factors influencing the work experiences of people with a mental illness.
The lessons learnt can extend further By creating socially-invested businesses, social firms demonstrate how business can be done differently. In light of the increasing prevalence of mental health disorders and related occupational health risks, as well as growing job insecurity and changing work patterns internationally, this is an important global message. We are grateful to the staff at Acacia for sharing of themselves so generously and supporting this research project. We also thank Social Firms Australia and the affiliated community health network for their support.
This study was undertaken by Tamar Paluch as part of her Master of Occupational Therapy degree with supervision by Dr Ellie Fossey (La Trobe University) & A/Prof Carol Harvey (The University of Melbourne). To contact us, email: [email protected]

Sustaining Employment in a Social Firm: Views of Employees with a Psychiatric Disability
IN BRIEF: Participants’ views about
why they stayed working in a
social firm
You’re used to it and you know what to do.
Regular and flexible work schedules, locations and
tasks made working easy.
Participants saw themselves as experienced as a
result of opportunities for training, making
decisions and being responsible.
It’s a good team to work in.
Practical and personal support, especially from the
manager, made this job different to other jobs.
Feedback from the manager, supervisors and
customers let participants know they were doing a
good job.
People at work, including everyone in the team,
were cooperative and friendly, making this a good
team to work in.
It’s doing positive things in my life
Having something to do and somewhere to go were
highly important to participants as a means of
staying well.
Participants valued supplementing their pension and
having job security: a permanent position and
additional unpaid leave if they became unwell.
Working here was right for now: having this job
contrasted positively with illness and employment
problems in the past and with perceived problems
in finding and sustaining a different job in the
future.
This study was undertaken by Anne Williams and Dr Ellie
Fossey (La Trobe University, School of Occupational
Therapy) and A/Prof. Carol Harvey (The University of
Melbourne) through the Psychosocial Research Centre
(PRC). The study was part of Anne’s Master of
Occupational Therapy degree in 2008/2009.
Contact us on: (03) 9479 5717 or email
Why was this study done?
Social firms offering supportive employment where people
with psychiatric disabilities work alongside other employees
and receive the same pay and conditions are relatively new to
Australia. Little is known about what it is like to work in a
social firm. This study aimed to find out the views of
employees with psychiatric disabilities about their social firm
workplace and factors that helped them to sustain their jobs.
What was done?
1) SHINE, a commercial cleaning company, was selected for
this study as this social firm had been operating long
enough for its employees to have experienced working
for six months or more.
2) Seven SHINE employees, five men and two women, who
had been in their jobs for at least six months and
identified as having a psychiatric disability, volunteered
to participate. The participants worked from 6 to 13.5
hours per week, usually on alternate days for three shifts
per week and cleaned in up to three sites per shift.
3) Each participant was interviewed about their view of the
work environment and the reasons they stayed in their
jobs. Questions were based on the Work Environment
Impact Scale, an occupational therapy interview
developed to understand how qualities and
characteristics of the work environment affect
individuals.
4) After the interview, the researcher rated how 17 features
of the workplace affected each participant. Ratings were
from 1 (feature strongly interferes with the participant’s
work performance, satisfaction and well-being) to 4
(feature strongly supports worker).
5) Participants also completed four questionnaires; one
each about their job satisfaction; quality of life; social
connection; and making decisions - empowerment.
6) Interviews were audio taped, transcribed and analysed to
describe individual stories and identify common themes
in participants’ views. Questionnaires were reviewed to
add further depth to participants’ views.
7) De-identified findings were shared with participants,
other employees from the social firm, the social firm
sector and occupational therapists.
Ethics approval was obtained for this study from La Trobe
University Faculty of Health Sciences’ Human Ethics
Committee and the employment agency that established the
social firm. Pseudonyms have been used in all reporting to
protect confidentiality.
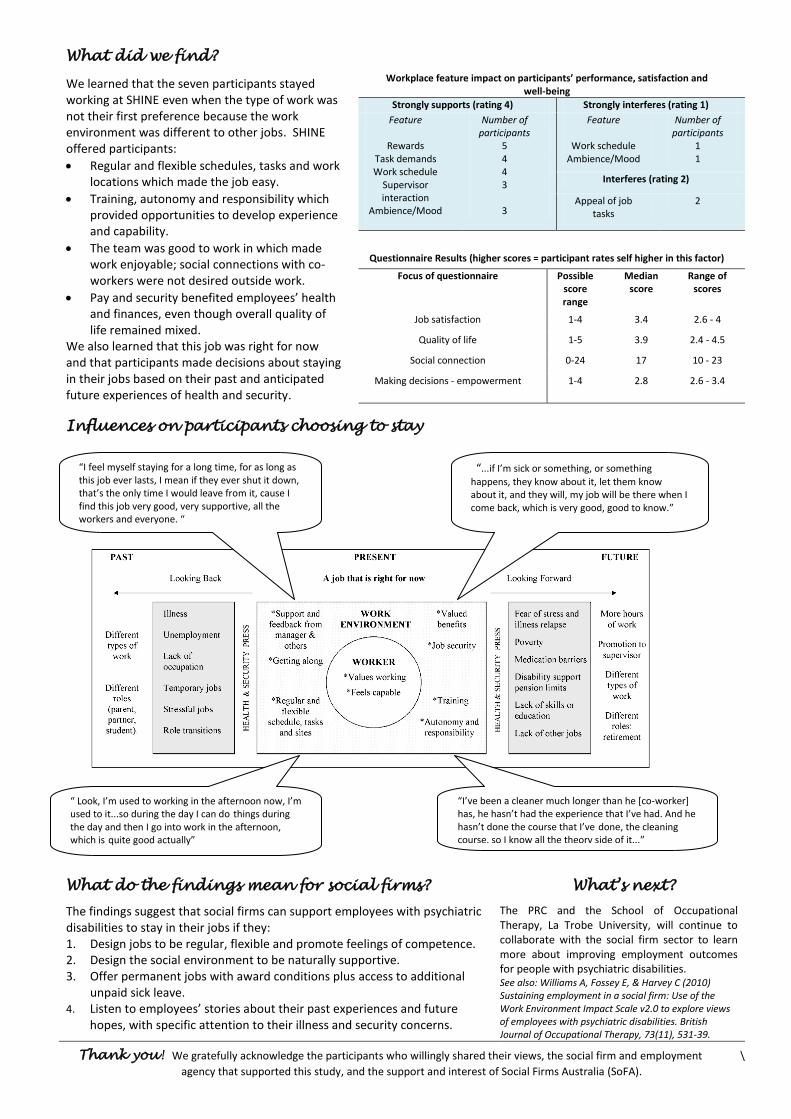
What did we find?
Workplace feature impact on participants’ performance, satisfaction and well-being
We learned that the seven participants stayed working at SHINE even when the type of work was not their first preference because the work environment was different to other jobs. SHINE offered participants:
Regular and flexible schedules, tasks and work locations which made the job easy.
Training, autonomy and responsibility which provided opportunities to develop experience and capability.
The team was good to work in which made work enjoyable; social connections with co-workers were not desired outside work.
Pay and security benefited employees’ health and finances, even though overall quality of life remained mixed.
We also learned that this job was right for now and that participants made decisions about staying in their jobs based on their past and anticipated future experiences of health and security.
Strongly supports (rating 4) Strongly interferes (rating 1)
Feature
Rewards Task demands Work schedule
Supervisor interaction
Ambience/Mood
Number of participants
5 4 4 3
3
Feature
Work schedule Ambience/Mood
Number of participants
1 1
Interferes (rating 2)
Appeal of job tasks
2
Questionnaire Results (higher scores = participant rates self higher in this factor)
Focus of questionnaire Possible score range
Median score
Range of scores
Job satisfaction 1-4 3.4 2.6 - 4
Quality of life 1-5 3.9 2.4 - 4.5
Social connection 0-24 17 10 - 23
Making decisions - empowerment 1-4 2.8 2.6 - 3.4
Influences on participants choosing to stay
What do the findings mean for social firms?
The findings suggest that social firms can support employees with psychiatric disabilities to stay in their jobs if they: 1. Design jobs to be regular, flexible and promote feelings of competence. 2. Design the social environment to be naturally supportive. 3. Offer permanent jobs with award conditions plus access to additional
unpaid sick leave. 4. Listen to employees’ stories about their past experiences and future
hopes, with specific attention to their illness and security concerns.
What’s next?
The PRC and the School of Occupational Therapy, La Trobe University, will continue to collaborate with the social firm sector to learn more about improving employment outcomes for people with psychiatric disabilities. See also: Williams A, Fossey E, & Harvey C (2010) Sustaining employment in a social firm: Use of the Work Environment Impact Scale v2.0 to explore views of employees with psychiatric disabilities. British Journal of Occupational Therapy, 73(11), 531-39.
Thank you! We gratefully acknowledge the participants who willingly shared their views, the social firm and employment \
agency that supported this study, and the support and interest of Social Firms Australia (SoFA).
“I feel myself staying for a long time, for as long as this job ever lasts, I mean if they ever shut it down, that’s the only time I would leave from it, cause I find this job very good, very supportive, all the workers and everyone. “
“...if I’m sick or something, or something
happens, they know about it, let them know about it, and they will, my job will be there when I come back, which is very good, good to know.”
“ Look, I’m used to working in the afternoon now, I’m used to it...so during the day I can do things during the day and then I go into work in the afternoon, which is quite good actually”
“I’ve been a cleaner much longer than he [co-worker] has, he hasn’t had the experience that I’ve had. And he hasn’t done the course that I’ve done, the cleaning course, so I know all the theory side of it...”





























