Embed Size (px)
DESCRIPTION
lecturer
Citation preview

Peptic Ulcer DiseasePUD

Definition
• Peptic ulcer disease = Mucosal defect in the GIT (gastric or duodenal) exposed to acid and pepsin secretion.
• Gastritis is the precursor to PUD and it is clinically difficult to differentiate the two conditions.
• Differentiation requires upper GIT endoscopy (EGD).

Disease Prevalence
• 10% of ER patients with abdominal pain are diagnosed as PUD.
• 10% of all Americans develop PUD.• The prevalence decreasing over last 30 ys • Male-to-female ratio of PUD = 2:1• Male-to-female ratio of gastritis = 1:1

Symptoms & Signs of PUD
1) Epigastric pain is most common symptom:- Nature: gnawing or burning.- Site: epigastric.- Radiation: May radiate to the back (penetration).- EXB: Starts 1-3 hrs after meals or at night. - Relieving factors: food, antacids (duodenal), or vomiting
(gastric).2)Associated symptoms: dyspepsia, belching, bloating.3)C/O: GI bleeding (Hematemesis or melena).
Differentiating Gastric From Duodenal Ulcer:
• Duodenal ulcers - age 25-75 years.• Gastric ulcer - age 55-65 years• Pain awakens the patient from sleep between
12-3 am, present in 2/3 of duodenal ulcer & 1/3 of gastric ulcer patients.
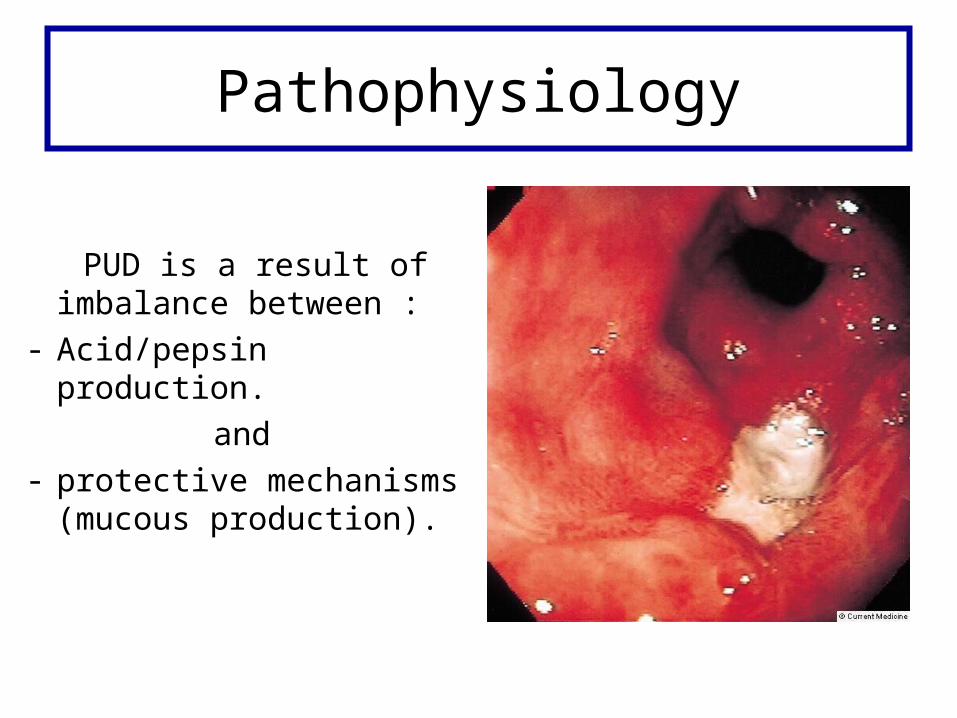
Pathophysiology
PUD is a result of imbalance between :
- Acid/pepsin production.and
- protective mechanisms (mucous production).

Common Risk Factors for Gastric Mucosal Disruption
A) H pylori.B) NSAIDs / ASA / steroids.C) coffee/smoking/stress (Burns, CNS trauma,
surgery, Severe medical illness).D) Alcohol.
NSAIDs
• 15% of patients on long-term NSAID develop PUD.• How: NSAIDs/ASA → ↓ prostaglandin (PG) by inhibiting
the cyclooxygenase (COX) enzymes in gastric mucosa. PG protect GIT from injury.
• Three COX isoenzymes:- COX-1 → PG production in gastric mucosa.- COX-2: specific NSAIDs with ↓↓ GIT side effects.- COX-3: inhibited by acetaminophen → antipyretic.

H. pylori• It is most common cause of
PUD.• Curvelinear, G-ve rod with
flagella.• Fecal-oral transmission.• Secretes urease → converts
urea to ammonia.• Produces alkaline environment
enabling survival in stomach.
Differentiating Between H. pylori & NSAID-Induced Ulcer
Ulcers associated with H. pylori
• More often in duodenum.
• Often superficial.• Less severe GIT
bleeding.
Ulcers associated with NSAIDs
• More often in stomach.• Often deep.• More severe GIT
bleeding.
Physical Exam Findings
In uncomplicated PUD, findings are few and non-specific:
• Mild epigastric tenderness.• Normal bowel sounds.• Rectal exam: may show melena/positive
guaiac stool test (fecal occult blood).• ± Signs of possible active GI bleed.• ± Signs of peritonitis with perforation.
Signs of possible active GIT bleed?
• Signs of volume depletion: tachycardia, hypotension, loss of skin turgor,
dry tongue.
• Signs of anemia: conjunctiva or skin pallor, new heart murmur.
Lab Studies to Evaluate PUD
• CBC - evaluate acute/chronic blood loss.• Tests for H. Pylori: - Serologic antibody test for H.Pylori – does not
determine if active HP infection. - Fecal antigen test for active H.Pylori. - Urea breath test for active H.Pylori.

Imaging Studies
• CXR: free abdominal air if perforation is suspected (air under diaphragm).
• Upper gastrointestinal series.– Performed by experienced radiologist is close to
diagnostic accuracy of endoscopy.– Not as sensitive as endoscopy in diagnosis of small
ulcers (<0.5 cm).– Unable to obtain Bx to rule out malignancy.

Air Under Diaphragm

EndoscopyIndicated in following high risk patients:
• New-onset dyspepsia in >50 years old patient.• Dyspepsia with weight loss.• Evidence of GIT bleeding.• Failed appropriate trial of empiric therapy.• Using NSAIDs or other high risk drugs.• Signs of upper GIT obstruction (early satiety,
vomiting).• Ethnic background with ↑ risk upper GIT
malignancies.
Rapid Urease Test & Histopathology
Gastric mucosal biopsy obtained during endoscopy:– Rapid urease tests: bacterial urease converts urea
to ammonia → changes pH producing color change.
– Histopathology is the gold standard for Dx.

Treatment of PUD
• Over the counter remedies.• H2-blockers.• PPI: Proton pump inhibitors.• Other Pharmacotherapy agents.• H. Pylori triple therapy.
Over The Counter Remedies
• Aluminum and magnesium hydroxide salt neutralize gastric acidity.
• Aluminum side effect = constipation.• Magnesium side effect = diarrhea.• So magnesium and aluminum mixtures are
used to avoid side effects.

Over the Counter Remedies cont’d
• Calcium Carbonate calcium salt neutralizes acid.
• Bismuth subsalicylate binds to ulcer base forming a protective coat → anti-inflammatory and bacteriocidal properties.
H2-Blockers
• Selectively block H2-receptors on parietal cells →↓ acid secretion.
• Used primarily in ulcer disease not associated with H pylori.
• Treatment duration is 6-8 wk.
Side Effects of Cimetidine/Tagamet®
• Elderly patients – confusion.• Young males - impotence +/- gynecomastia• May alter levels of other drug - warfarin, TCA’s,
triamterene, phenytoin, propranolol, metronidazole, antiarrythmics.
• May alter renal function requiring lower doses.
Proton Pump Inhibitors
• Decreases gastric acid secretion by inhibiting the parietal cell H+/K+ ATP pump.
• Relieve pain and heal peptic ulcers more rapidly than H2-blockers.
• Drugs in this class are equally effective. • Four weeks to treat active PUD.• Eight weeks to treat erosive esophagitis.
Other Pharmacotherapy Agents
• Sucralfate: binds proteins in exudates and forms a viscous adhesive that protects GIT lining.
• Misoprostol: prostaglandin analog- protects lining of GI tract by replacing depleted prostaglandin E1. Prevents peptic ulcers in patients taking NSAIDs.

H. Pylori Triple Therapy Treatment
• Triple therapy for 14 days is treatment of choice.
• 2 forms of triple therapy: PPI–based and bismuth-based.
• PPI based = PPI + 2 antibiotics for 2 wks, continue PPI for additional 2 wks.
• Bismuth-based = bismuth subsalicylate + 2 antibiotics, for 2 wks with addition of H2- blocker to optimize ulcer healing.
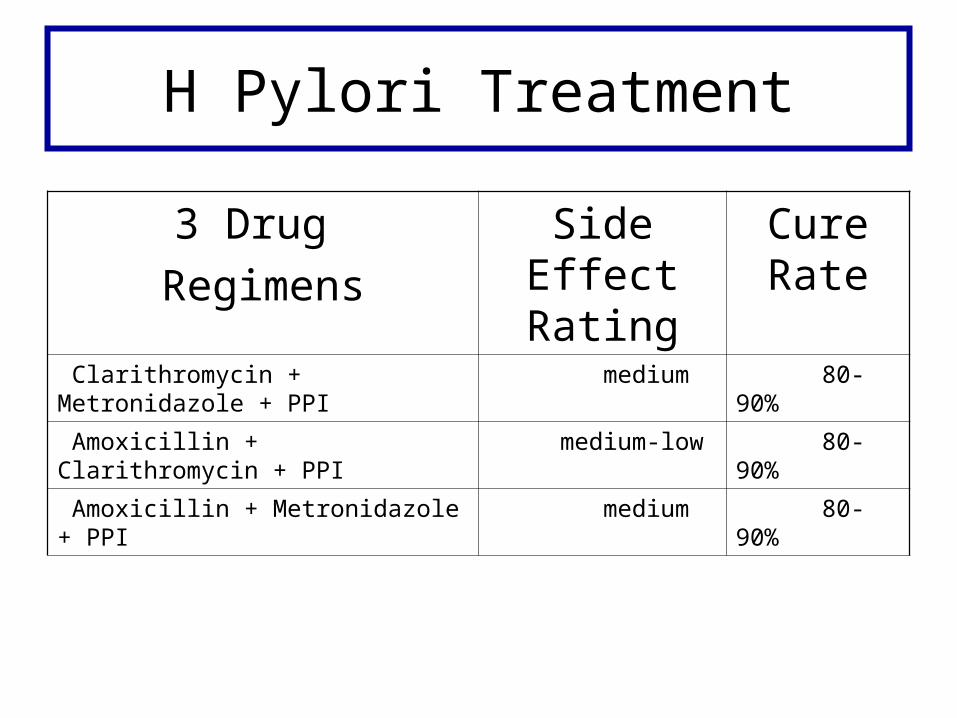
H Pylori Treatment
3 Drug Regimens
Side Effect Rating
Cure Rate
Clarithromycin + Metronidazole + PPI medium 80-90%
Amoxicillin + Clarithromycin + PPI medium-low 80-90%
Amoxicillin + Metronidazole + PPI medium 80-90%

H. Pylori Therapy cont’d
• Successful eradication of H. pylori reduces PUD recurrence rates from 90% to <10% per year.
• Patients no longer require chronic acid suppression.
• If symptoms return after ttt of PUD → re-evaluation for recurrence.
PUD Complications
• Hemorrhagic shock/peritonitis from a perforated ulcer.
• Symptoms of anemia (fatigue, dyspnea). • Symptomatic relief with PPI may mask
symptoms of gastric malignancy.