Embed Size (px)
Citation preview
6/16/14
1
13: Microbe-Human Interactions
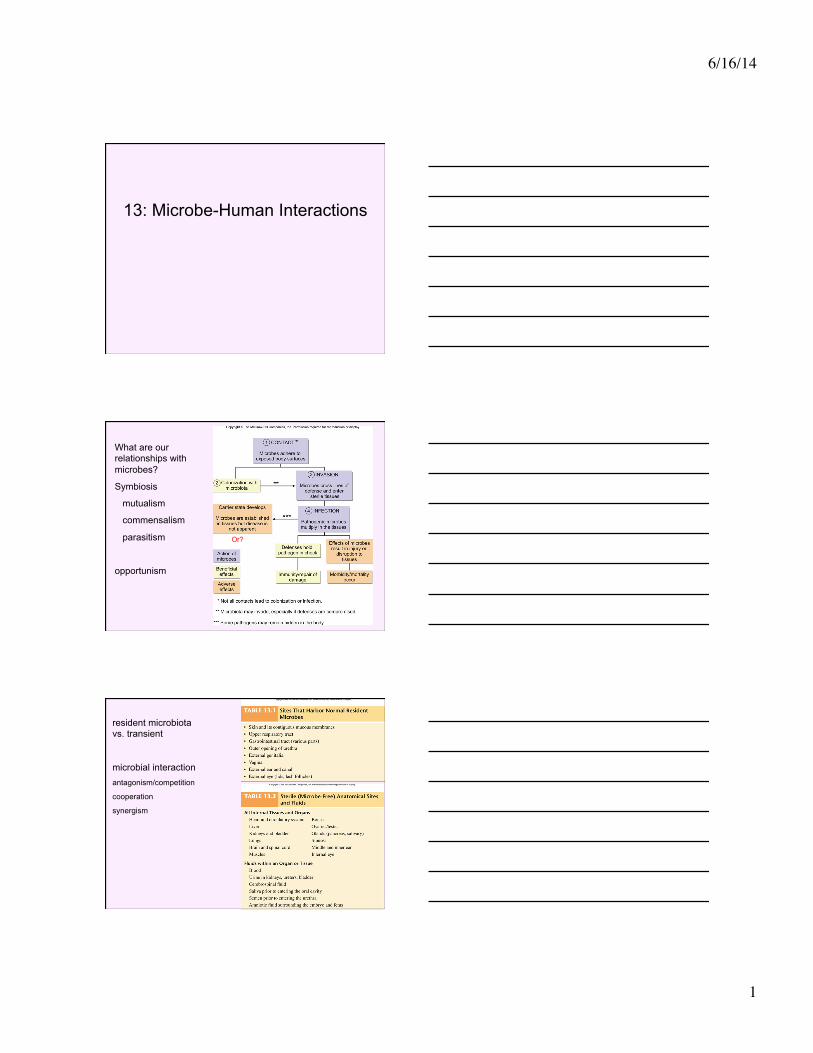
What are our relationships with microbes?
Symbiosis
mutualism
commensalism
parasitism
opportunism
Or?
resident microbiota vs. transient
microbial interaction antagonism/competition
cooperation
synergism
6/16/14
2
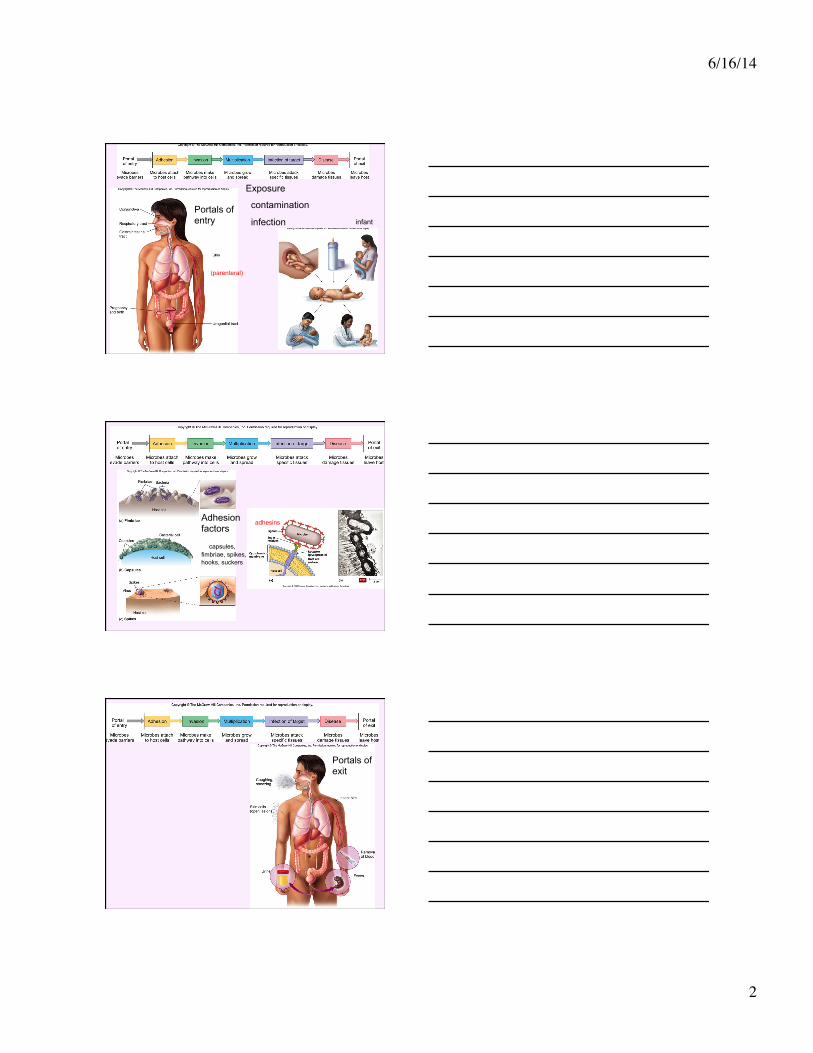
Exposure
contamination
infection
(parenteral)
Portals of entry infant
Adhesion factors
capsules, fimbriae, spikes, hooks, suckers
adhesins
Portals of exit
6/16/14
3
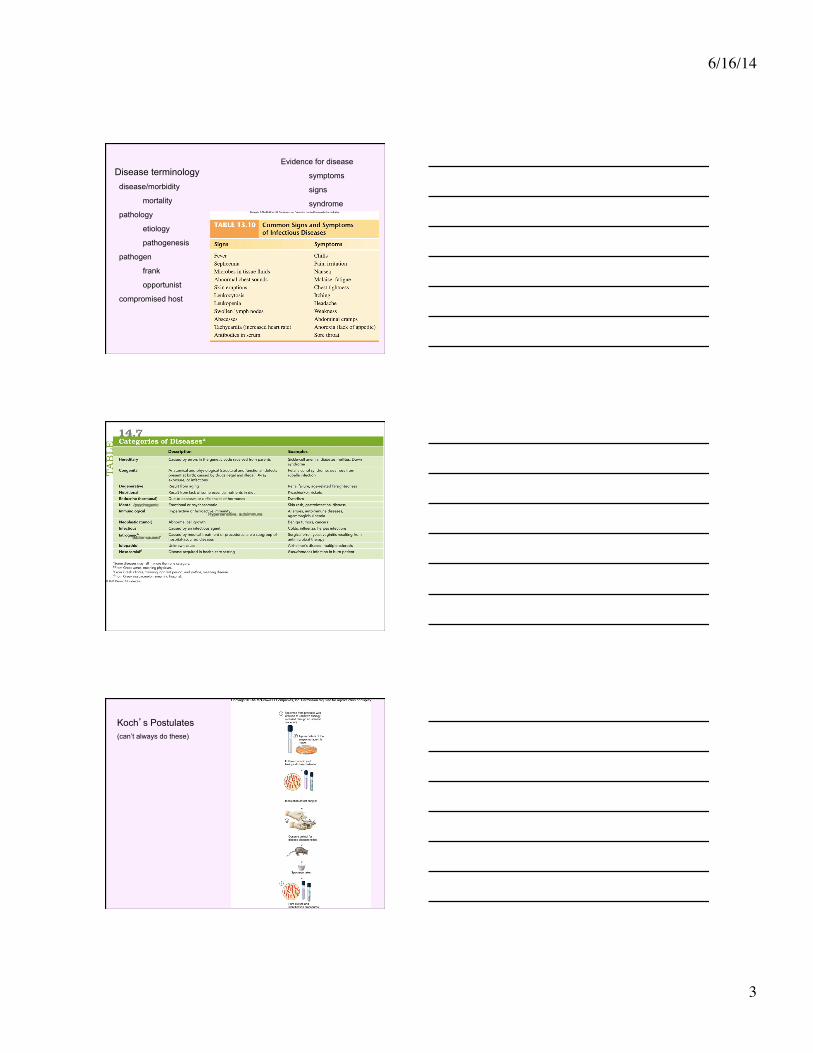
Disease terminology disease/morbidity
mortality
pathology
etiology
pathogenesis
pathogen
frank
opportunist
compromised host
Evidence for disease
symptoms
signs
syndrome
Hypersensitive, autoimmune
/psychogenic
“doctor-caused”
Koch’s Postulates (can’t always do these)
6/16/14
4
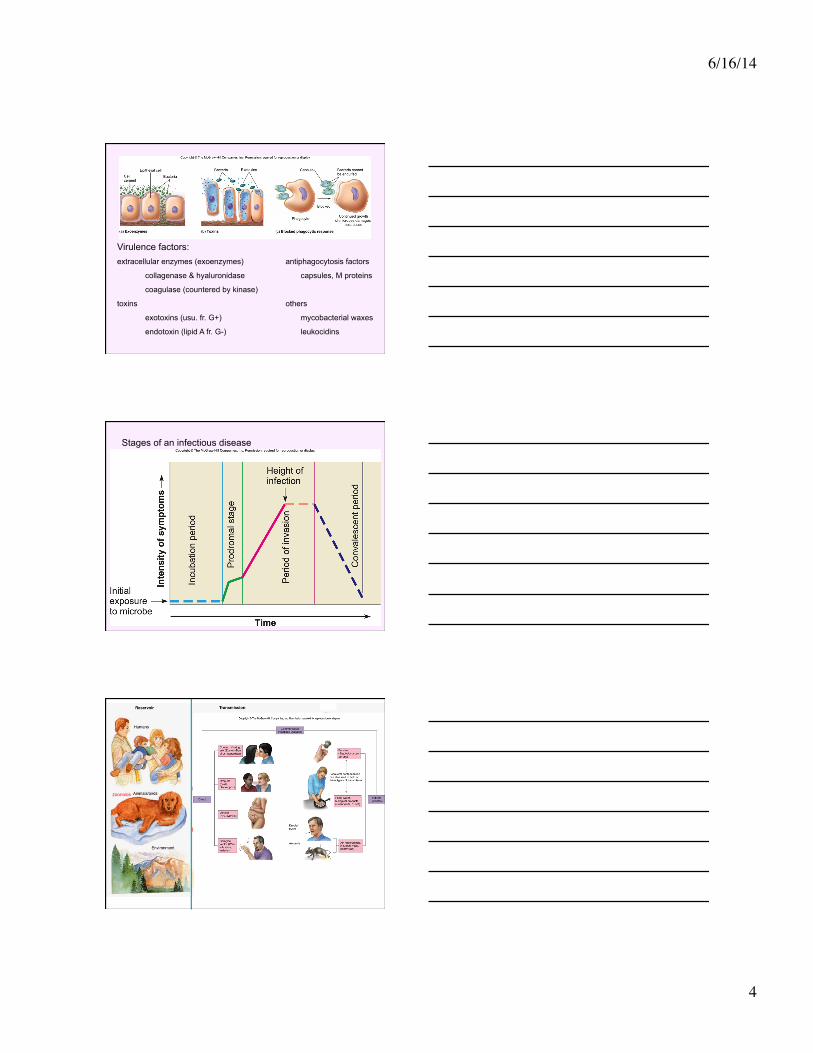
Virulence factors: extracellular enzymes (exoenzymes) antiphagocytosis factors
collagenase & hyaluronidase capsules, M proteins
coagulase (countered by kinase)
toxins others
exotoxins (usu. fr. G+) mycobacterial waxes
endotoxin (lipid A fr. G-) leukocidins
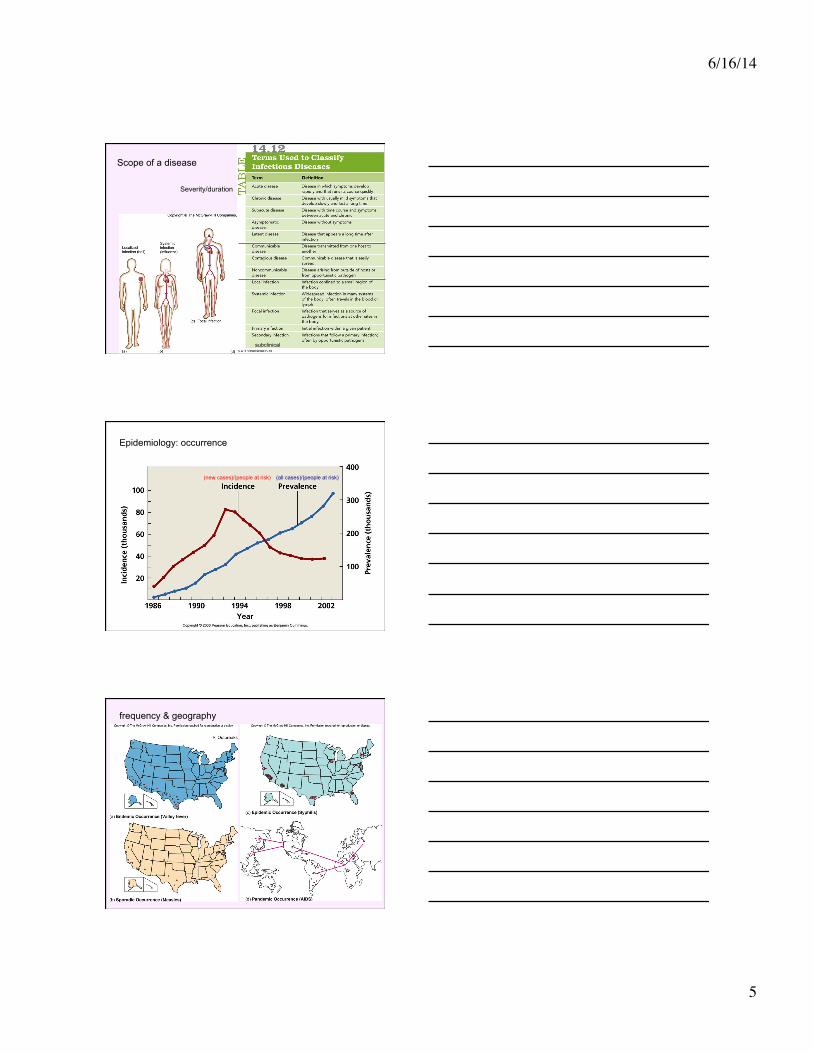
Stages of an infectious disease
zoonosis
6/16/14
5
Scope of a disease
Severity/duration
subclinical
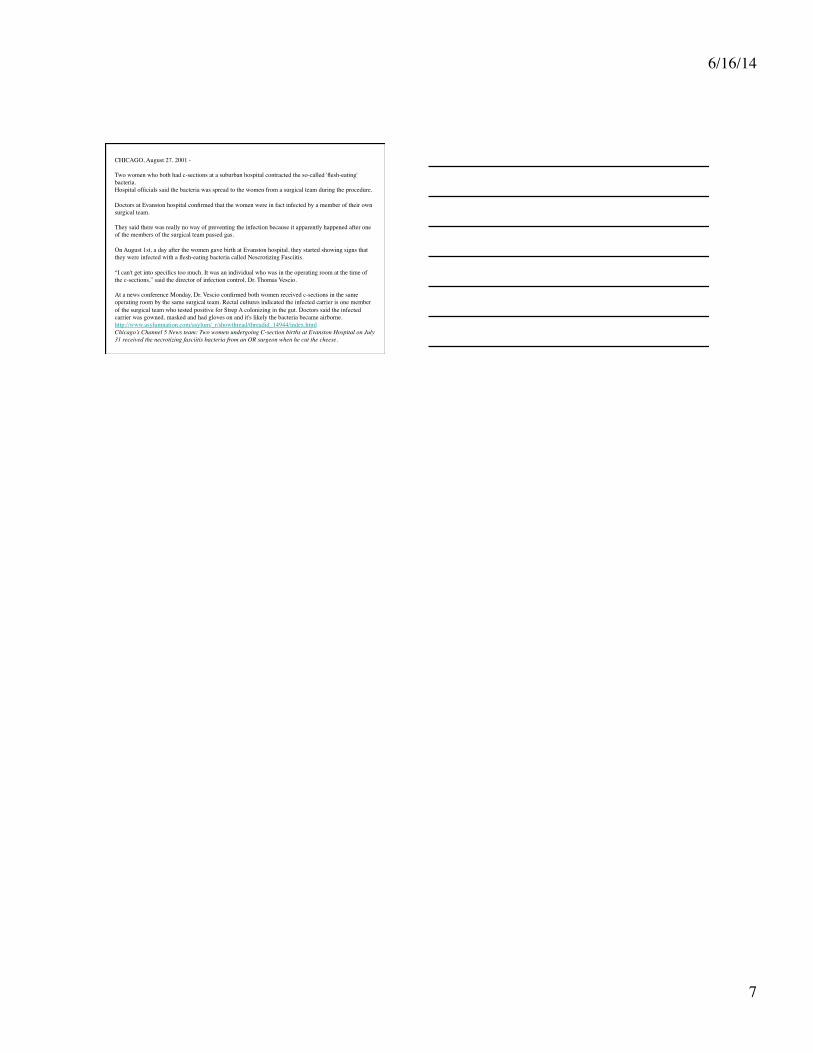
(new cases)/(people at risk) (all cases)/(people at risk)
Epidemiology: occurrence
frequency & geography
6/16/14
6
John Snow’s (1854) study of a cholera epidemic
World Health Organization (WHO)
Centers for Disease Control & Prevention (CDC), part of NIH
California Dept. of Public Health (CDPH)
Nosocomial infections At least 1 in 20 patients
iatrogenic infection
superinfection
Asepsis!!!
6/16/14
7
CHICAGO, August 27, 2001 - ������Two women who both had c-sections at a suburban hospital contracted the so-called 'flesh-eating' bacteria.���Hospital officials said the bacteria was spread to the women from a surgical team during the procedure.������Doctors at Evanston hospital confirmed that the women were in fact infected by a member of their own surgical team.������They said there was really no way of preventing the infection because it apparently happened after one of the members of the surgical team passed gas.������On August 1st, a day after the women gave birth at Evanston hospital, they started showing signs that they were infected with a flesh-eating bacteria called Nescrotizing Fasciitis.������“I can't get into specifics too much. It was an individual who was in the operating room at the time of the c-sections,” said the director of infection control, Dr. Thomas Vescio.������At a news conference Monday, Dr. Vescio confirmed both women received c-sections in the same operating room by the same surgical team. Rectal cultures indicated the infected carrier is one member of the surgical team who tested positive for Strep A colonizing in the gut. Doctors said the infected carrier was gowned, masked and had gloves on and it's likely the bacteria became airborne. http://www.asylumnation.com/asylum/_r/showthread/threadid_14944/index.html Chicago’s Channel 5 News team: Two women undergoing C-section births at Evanston Hospital on July 31 received the necrotizing fasciitis bacteria from an OR surgeon when he cut the cheese.


![Review Article Gammarus-MicrobialInteractions:AReviewhyphomycetes was negligible [ 17]. Aquatic hyphomycetes produce secondary metabolites that function in microbe-microbe interactions](https://img.pdfslide.us/doc/110x75/60c9d3a89f80e602464161fa/review-article-gammarus-microbialinteractionsareview-hyphomycetes-was-negligible.jpg)