Embed Size (px)
Citation preview

CE
ON
LIN
E
Enhanced Recovery after Colorectal Surgery
An Online Continuing Education ActivitySponsored By
Educational Funds Provided By

Welcome to
Enhanced Recovery after Colorectal Surgery
(An Online Continuing Education Activity)
CONTINUING EDUCATION INSTRUCTIONSThis educational activity is being offered online and may be completed at any time. Steps for Successful Course CompletionTo earn continuing education credit, the participant must complete the following steps:
1. 1. Read the overview and objectives to ensure consistency with your own learning needs and objectives. At the end of the activity, you will be assessed on the attainment of each objective.
2. Review the content of the activity, paying particular attention to those areas that reflect the objectives.
3. Complete the Test Questions. Missed questions will offer the opportunity to re-read the question and answer choices. You may also revisit relevant content.
4. For additional information on an issue or topic, consult the references.5. To receive credit for this activity complete the evaluation and registration form. 6. A certificate of completion will be available for you to print at the conclusion.
Pfiedler Enterprises will maintain a record of your continuing education credits and provide verification, if necessary, for 7 years. Requests for certificates must be submitted in writing by the learner.
If you have any questions, please call: 720-748-6144.
CONTACT INFORMATION:
© 2015All rights reserved
Pfiedler Enterprises, 2101 S. Blackhawk Street, Suite 220, Aurora, Colorado 80014www.pfiedlerenterprises.com Phone: 720-748-6144 Fax: 720-748-6196
3
OVERVIEWThe ideal for any surgical procedure, including colorectal surgery, is for patients to experience an uneventful recovery with minimal risk, little pain and a quick discharge from the hospital. The surgical team is unable to eliminate every potential risk; however, they can employ quality pre-surgical interventions and post-surgical recovery to improve patient outcomes. The goal for optimal clinical results is to implement practices that ensure patients are as healthy as possible prior to surgery, and that they receive the best care possible during surgery and recovery. This can be achieved through routinely using Enhanced Recovery After Surgery (ERAS) protocols that include evidence-based treatment and offer standardization of health care processes that accelerate recovery and safely reduce hospital stay.
This continuing education activity will discuss how patients can be partners in achieving an uneventful recovery, decreasing the number of days a patient spends in the hospital and how to restore a patient’s optimal health when surgical care teams implement enhanced recovery pathways.
LEARNING OBJECTIVESAfter completing this continuing nursing education activity, the participant should be able to:
1. Identify practices that can reduce the delay to full recovery for the colorectal patient.2. Describe the rationale for the recommendations of enhanced recovery after surgery.3. Describe protocols for better clinical outcomes4. Evaluate traditional practices compared to an evidenced-based approach
INTENDED AUDIENCEThis continuing nursing education activity is intended for use by perioperative nurses andother healthcare professionals who are interested in learning more about enhanced recovery after colorectal surgery and how it impacts their practice.
CREDIT/CREDIT INFORMATION State Board Approval for Nurses Pfiedler Enterprises is a provider approved by the California Board of Registered Nursing, Provider Number CEP14944, for 2.0 contact hours.
Obtaining full credit for this offering depends upon attendance, regardless of circumstances, from beginning to end. Licensees must provide their license numbers for record keeping purposes.
The certificate of course completion issued at the conclusion of this course must be retained in the participant’s records for at least four (4) years as proof of attendance.
IACETPfiedler Enterprises has been accredited as an Authorized Provider by the International Association for Continuing Education and Training (IACET).
4
CEU Statements• As an IACET Authorized Provider, Pfiedler Enterprises offers CEUs for its programs
that qualify under the ANSI/IACET Standard. • Pfiedler Enterprises is authorized by IACET to offer 0.2 CEUs for this program.
RELEASE AND ExPIRATION DATE:This continuing education activity was planned and provided in accordance with accreditation criteria. This material was originally produced in May, 2015 and can no longer be used after May 2017 without being updated; therefore, this continuing education activity expires May 2017.
DISCLAIMERPfiedler Enterprises does not endorse or promote any commercial product that may be discussed in this activity
SUPPORTFunds to support this activity have been provided by Ethicon
AUThORS/PLANNING COMMITTEE/REVIEWERDondra Tolerson, BS, MA Woodstock, GaMedical Writer/Author/Planning Committee Judith I. Pfister, RN, BSN, MBA Aurora, COProgram Manager/Planning CommitteePfiedler Enterprises Julia A. Kneedler, RN, MS, EdD Aurora, COProgram Manager/ReviewerPfiedler Enterprises
DISCLOSURE OF RELATIONShIPS WITh COMMERCIAL ENTITIES FOR ThOSE IN A POSITION TO CONTROL CONTENT FOR ThIS ACTIVITy Pfiedler Enterprises has a policy in place for identifying and resolving conflicts of interest for individuals who control content for an educational activity. Information below is provided to the learner, so that a determination can be made if identified external interests or influences pose potential bias in content, recommendations or conclusions. The intent is full disclosure of those in a position to control content, with a goal of objectivity, balance and scientific rigor in the activity. For additional information regarding Pfiedler Enterprises’ disclosure process, visit our website at: http://www. pfiedlerenterprises.com/disclosure
Disclosure includes relevant financial relationships with commercial interests related to the subject matter that may be presented in this continuing education activity. “Relevant financial relationships” are those in any amount, occurring within the past 12 months that

5
create a conflict of interest. A commercial interest is any entity producing, marketing, reselling, or distributing health care goods or services consumed by, or used on, patients.
Activity Authors/ Planning Committee/Reviewer Dondra Tolerson, BS, MA No conflict of interest
Judith I. Pfister, MBA, RN Co-owner of company that receives grant funds from commercial entities
Julia A. Kneedler, EdD, RN Co-owner of company that receives grant funds from commercial entities
PRIVACy AND CONFIDENTIALITy POLICyPfiedler Enterprises is committed to protecting your privacy and following industry best practices and regulations regarding continuing education. The information we collect is never shared for commercial purposes with any other organization. Our privacy and confidentiality policy is covered at our website, www.pfiedlerenterprises.com, and is effective on March 27, 2008.
To directly access more information on our Privacy and Confidentiality Policy, type the following URL address into your browser: http://www.pfiedlerenterprises.com/privacy-policy
In addition to this privacy statement, this Website is compliant with the guidelines for internet-based continuing education programs.
The privacy policy of this website is strictly enforced.
CONTACT INFORMATIONIf site users have any questions or suggestions regarding our privacy policy, please contact us at:
Phone: 720-748-6144
Email: [email protected]
Postal Address: 2101 S. Blackhawk Street, Suite 220 Aurora, Colorado 80014
Website URL: http://www.pfiedlerenterprises.com

6
INTRODUCTIONColorectal surgery is an area of medicine that deals with conditions of the rectum, anus and colon. According to the American Society of Colon and Rectal Surgeons, conditions that might require colorectal surgical intervention include, but are not limited to:
• Hemorrhoids: varicosities or swelling, and inflammation of veins in the rectum and anus
• Anal fissures: cracks or tears in the anus • Fistulas: abnormal connections or passageways between the rectum or other
anorectal area to the skin surface• Severe constipation conditions• Fecal incontinence• Rectal prolapse: protrusion of the walls of the rectum through the anus • Crohn’s disease: severe colic disorder • Colorectal cancer
Patients often remain in the hospital 1–5 days after an open colorectal surgery and an average of 1–3 days for laparoscopic procedures. Discharge criteria typically depend on evidence of bowel function (flatus or bowel movements), tolerance of diet without requiring IV fluids, and pain controlled with oral medication. Once at home, most patients require an additional 2-4 weeks before they resume a normal life schedule.
As healthcare continues to embrace patient-centric processes in all facets of care, it is important for the surgical team to understand that what occurs before and during surgery may influence recovery beyond a patient’s discharge from the hospital. In fact, the literature has determined that recovery should be measured via multiple domains driven by standard protocols, along with patient compliance to said protocols. The Enhanced Recovery After Surgery (ERAS) Society has developed such evidence-based protocols to reduce the discrepancy between the actual practices and what was already known to be the best practices, based on the literature. These protocols vary drastically from traditional practices and often require a major shift in the care team’s perspective and clinical routines.
ENhANCED RECOVERy AFTER SURGERy (ERAS) SOCIETy The ERAS Society was officially founded in 2010. Their mission, as indicated on their website, is to “develop perioperative care and to improve recovery through research, audit education and implementation of evidence-based practice.” 1 They have focused on examining traditional practices in surgery and replacing them with evidence-based practices when necessary, covering all areas of the patient’s experience through the surgical process. To that end, they’ve developed multimodal perioperative care pathways designed to achieve early recovery for patients undergoing major surgery.1 Their pathways were initially developed in the context of open procedures but have also been applied to patients undergoing laparoscopic surgery.
The ERAS Society was birthed from the ERAS Study Group, comprised of leading surgical groups, and formed by Professors Ken Fearon and Olle Lungqvist in 2001 to

7
further develop ideas put forth in the 1990’s by Professor Henrik Kehlet, concerning the concept of multimodal surgical care. The ERAS Study Group discovered that there were significant variances in traditional practices within the spectrum of surgical protocols, prompting them to examine opportunities to enhance and standardize traditional practice in favor of creating best-practice care pathways.
ENhANCED RECOVERy PAThWAyS (ERP)Health care systems provide care to an increasingly complex and aging patient population who are more prone to experiencing surgical complications. Colorectal surgery in particular has a high volume of major procedures, significant morbidity, extended hospital stays, and unplanned readmissions. Enhanced recovery pathways (ERP) have been developed and utilized as a means to reduce morbidity and improve effectiveness of recovery of colorectal [and other surgical] patients.2
ERPs for colorectal surgery include standardized preoperative, in-hospital and postoperative practices steeped in evidence-based outcomes that show benefits for patients undergoing open and/or laparoscopic procedures.3 ERPs are designed to be initiated in advance of surgery in order to optimize clinical outcomes. Preoperative evaluations provide an opportunity to identify medical conditions and risk factors for postoperative morbidity and mortality, and to underscore active participation from the patient. With the exception of critically ill, unconscious or non- communicative patients, a rarity for colorectal surgery, patients should engage in their own care. With participation from all members of the care team (e.g., patient, surgeons, anesthesiologists, nurses, social worker, and therapist) the pathways have been associated with a reduced duration of hospital stay, readmissions, reoperations and decreased mortality and morbidity, improved pain control, better cost containment, and improved patient satisfaction.4,5,6,7
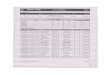
Figure 1. Achievement of Discharge Criteria Prospective Randomized Controlled Trial of Multimodal Perioperative Management Protocol in Patients Undergoing Elective Colorectal Resection for Cancer. 4

8
Figure 2. Achievement of Discharge Criteria Prospective Randomized Controlled Trial of Multimodal Perioperative Management Protocol in Patients Undergoing Elective Colorectal Resection for Cancer. 4
ERAS has included several guidelines in their ERP for colorectal surgery; they are: 2
• Preadmission information, education and counseling• Preoperative optimization• Mechanical bowel preparation• Preoperative fasting and carbohydrate treatment• Pre-anesthesia medication• Prophylaxis against thromboembolism• Antimicrobial prophylaxis and skin preparation• Standard anesthetic protocol• PONV• Laparoscopy and modifications of surgical access• Nasogastric intubation• Preventing intraoperative hypothermia• Fluid management• Drainage of the peritoneal cavity after colonic anastomosis• Urinary drainage• Prevention of postoperative ileus• Pain management• Nutritional care• Early mobilization• Measuring outcomes
OPTIMIZING CLINICAL OUTCOMESPreoperative Optimization: Alcohol and Tobacco CessationIt is in best practice for patients to be advised to stop smoking and/or drinking excessive amounts of alcohol prior to surgery. 8 Alcohol abusers are two to three times more likely to experience postoperative morbidity risks. The most frequent worries are bleeding, wound and cardiopulmonary complications. In fact, just a month of alcohol abstinence improves organ function and reduces postoperative morbidity. 9, 10 One month of tobacco cessation by active smokers is necessary to see a measurable decrease in incidence11.

9
Table 3. Clinical complications after colorectal resection, according to whether patients had abstained from alcohol in month before operation.
Effect of preoperative abstinence on poor postoperative outcome in alcohol misusers: randomized controlled trial. 10
Fasting and Carbohydrate TreatmentIt has been standard practice to require patients to fast after midnight in an effort to empty their stomach contents and, in effect, reduce the risk of pulmonary aspiration in elective surgery. However, a Cochrane review on preoperative fasting involving 22 RCTs demonstrated that fasting from midnight did not reduce gastric content, increase the pH of gastric fluid, or affect the prevalence of complications compared with patients allowed free intake of clear fluids up until two hours prior to receiving anesthesia for surgery.12 Thus, most national anesthesia societies now recommend intake of clear fluids up until two hours before the administration of anesthesia as well as a six hour fast for solid food.13 Note, although diabetic patients with neuropathy may have delayed

10
gastric emptying (thereby possibly increasing the risk of regurgitation and aspiration), patients with uncomplicated type-2 diabetes have been reported to have normal gastric emptying.14
The clinical effectiveness of preoperative carbohydrate treatment has yet to be established in diabetic subjects. By providing a clear fluid containing a relatively high concentration of complex carbohydrates two to three hours prior to anesthesia, patients can undergo surgery in a metabolically fed state. Four hundred milliliters of a 12.5 % drink of mainly maltodextrins has been shown to reduce preoperative thirst, hunger, and anxiety 12 as well as postoperative insulin resistance. Carbohydrate treatment results in less postoperative losses of nitrogen and protein as well as better-maintained lean body mass and muscle strength.
Prophylaxis Against Venous Thromboembolism (VTE)Deep vein thrombosis is the formation of a blood clot in a deep vein—usually in the leg or pelvic veins. The most serious complication is that the clot could dislodge and travel to the lungs, becoming a pulmonary embolism. This condition is referred to as venous thromboembolism VTE.
It has been shown that pharmacological prophylaxis against venous thrombosis (VT) reduces the prevalence of symptomatic venous thromboembolism (VTE) without increasing side effects such as bleeding. Use of compression stockings reduces the incidence of VTE.15,16 In a recent Cochrane report, it was concluded that prolonged (four weeks postoperatively) VTE prophylaxis, as compared with in-hospital prophylaxis, was associated with a significantly reduced prevalence of VTE: 14.3% vs. 6.1%, as well as symptomatic VTE: 1.7% vs. 0.2 %, without an increase in postoperative bleeding complications or other side effects.15 Patients with an increased risk for VTE are those with extensive comorbidities, malignant disease, who take corticosteroids preoperatively, have undergone previous surgery, and those in hypercoagulable states.17
Fluid ManagementColorectal surgery patients, especially those who undergo extensive bowel resections and emergency laparotomies, may undergo acute alterations in volume status and in the composition of intracellular and extracellular fluids. Several studies have shown that the lack of oral intake after midnight, and some bowel preps may cause preoperative fluid loss in patients undergoing major colorectal surgery.
18 As a result, precise perioperative management of fluids and electrolytes plays a vital part in achieving optimal outcomes after surgery. The goal of perioperative fluid management is to achieve a balance between avoiding hypotension, impaired tissue oxygenation, and inadequate organ profusion that may be associated with too little fluid, as well as avoid interstitial edema and cardiopulmonary complications associated with fluid overload (figure 3).

11
Figure 3. Adverse consequences of a restrictive or liberal approach to perioperative fluid management in patients undergoing colorectal surgery.18
A debate exists as to whether liberal or restrictive fluid management in the postoperative period is more appropriate. More specifically, the debate surrounds the quantity of fluids that should be administered pre-, intra-, and post-surgery. Surgeons have historically relied on their clinical judgment that leaned toward excess fluid administration, going beyond measureable fluid losses, based on the notion of “third space” fluid deficit. 18
Although studies vary in their definition of restrictive vs. liberal fluid, data points in favor of a more restrictive approach. A recent review concluded that fluid excess was associated with worse outcomes.19 In a randomized prospective study in which patients were assigned to either a restricted (< 2 L) or standard (> 3 L) postoperative intravenous fluid regimen, patients receiving less IV fluids were found to have earlier gastric emptying, and a shorter time to passage of flatus and first bowel movement. Patients treated with the standard liberal formula of IV fluid repletion had longer hospital stays and more complications.
Most of the literature on fluid management in colorectal surgery does not separate the colon from the rectum. However, compared with the colon, rectal surgery leads to more fluid shift as a result of bowel preparation, bowel handling and blood loss from the pelvic area. In addition, the use of epidural local anesthetics, pneumoperitoneum, hypothermia and vasodilatation-induced by anesthetic drugs can cause changes in vascular tone.19
In open cases, goal-directed fluid therapy using the esophageal Doppler system has been shown to reduce the length of stay and the rate of postoperative complications.20,21 The rationale of using this device is that the intravenous fluids are titrated to optimize cardiac output (a better indicator of oxygen delivery and hemodynamic status than systolic blood pressure and pulse).22
12
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) is administered to patients prior to surgery to clear fecal material from the bowel. It is not recommended by ERAS as routine practice.
In a 2011 update of the Cochrane review on mechanical bowel prep (MBP) in colorectal surgery, comparisons were made between patients who received MBP versus no preparation and MBP versus rectal enema only. 23 Anastomotic leakage was assessed in patients undergoing restoration of bowel continuity and showed no difference between MBP and no preparation/enema. Patients undergoing low anterior resection were also analyzed separately. In this group of patients, bowel preparation was not associated with a changed prevalence of anastigmatic leakage: 7.4% vs. 7.9 %. The review concluded that routine bowel preparation before colonic surgery was of no value, and should not be recommended. However, if an intraoperative procedure, such as a colonoscopy, is carried out due to a small lesion or for any other reason, MBP should be initiated. 23
Studies also suggest that hypertonic bowel preparations (preps that pull fluid out of cells) in healthy patients may result in dehydration, increases in plasma osmolality, urea and phosphate concentrations, and other significant changes. With accumulating evidence in several meta-analyses supporting the notion that mechanical MBPs do not improve morbidity or mortality—and in fact may increase the rates of anastomotic leakage—the use of MBPs in elective colorectal surgery is becoming less common.18
Perioperative Nutritional Care And Early MobilizationIn the well-nourished patient with preserved gastrointestinal function in the days after surgery, quality food introduced within 24 hours following surgery will fulfill most nutritional requirements, and little artificial nutritional support is required. It has been well established that any delay in the resumption of a normal oral diet after major surgery is associated with increased rates of infectious complications and delayed recovery.
Notably, early oral diet has also been shown to be safe in patients with a new non-diverted colorectal anastomosis, although considerable efforts must be made to prevent postoperative ileus and a risk of aspiration.24
A RCT in 119 patients showed that postoperative muscle training had little effect of long-term postoperative outcomes; 25 however, a study published in 2002 and a recent review published in 2011 confirmed that combining forced mobilization with nutritional support results in improved muscle strength during the early postoperative phase. 26,27
A multivariate linear regression analysis of data collected during the Laparoscopy and Fast Track (LAFA) study, supported mobilization on postsurgical days one through three, a significant factor associated with a successful outcome of ERAS. 28
Ultimately it is accepted that prolonged bed rest has several negative effects, including reduced work capacity,29 increased risk of pneumonia and muscle weakness.

13
Pain ManagementSignificant strides have been made with postoperative pain control; however, opportunity for improvement still remains. For patients undergoing surgery, controlling pain is a priority and when addressed it relieves patient anxiety and allows the patient to participate in their recovery more easily. The use of epidural analgesia is an evidence-based practice in Enhanced Recovery Pathways. It is used to promote early ambulation and mobilization post-surgery, restore normal bowel and gut function sooner, and for general pain relief. The basis for the pathway is that by minimizing the stress response following surgery, the patient will require less time to recuperate.
According to the literature, duration of pain requiring significant analgesics after laparoscopic surgery is much shorter than for open surgery. This generally leads to the patient being discharged from the hospital as soon as 23 hours post-surgery. In a review of postoperative analgesia following patients that had laparoscopic colorectal surgeries, eight studies were identified where five compared epidural vs. patient controlled analgesia ⁄ intravenous morphine. One of the outcomes revealed in the Levy et.al. study was that pain control “was superior in the epidural group”. 30
In randomized, double blind controlled trial of patients undergoing colorectal surgery; a team of anesthesiologists from the University Hospital of Clermont-Ferrand (France) compared epidural analgesia and continues wound infiltration of local anesthetics. The study involved fifty patients that were provided epidural analgesia or continuous wound infiltration over a period of 48 hours and were managed according to ERAS protocols. Findings showed epidural analgesia produced better patient outcomes, including an increase in postoperative pain relief, faster functional recovery and shorter hospital stays.31
Although some have sited added cost and increased complexity as a concern, the use of epidural analgesia is worthwhile to achieve optimum pain relief for patients.
Measurement of OutcomesAs demonstrated in the above text, measuring standards and auditing for compliance of quality of outcomes have been shown to be key motivators in assisting surgical care teams with successfully implementing the ERAS pathways. 32
Auditing ERAS can be examined under the following three purviews: 32
1. Clinical outcomes: measuring LOS, readmission rates and complications
2. Patient: determining functional recovery and patient experience
3. Process outcomes: measuring level of consistency of adherence with ERAS protocols.
There are postoperative recovery measurement tools that can be administered in-person, electronically, or via phone that can provide on-going data once the patient is discharged home. The tools provide feedback on the quality of the patient’s recovery from several
14
perspectives (e.g., physiological, nociceptive, emotive, activities of daily living, cognitive recovery and experiencial).
COMMON CONCERNS ABOUT IMPLEMENTING ERPSThe implementation of ERP brings up several concerns. These concerns include early readmission, delayed diagnosis of complications and increased nursing utilization. However, consistent data shows that discharging patients from the third day after open or laparoscopic segmental colectomy was associated with approximately a 10% readmission rate, similar to the 10–15% readmission observed after colorectal resections with traditional care. In fact, ERP patients discharged earlier had fewer readmissions than those with a longer primary stay.33,34,35,36,37,38
The idea that initiating ERPs increases nursing utilization has proven unfounded. The concern is that the care team’s workload increases due to promoting ambulation, oral intake and incentive spirometer use. Available data suggest the opposite, with early restoration of organ function and recovery actually decreasing nursing care. A prospective, controlled study of 160 patients who underwent open colorectal procedures showed that ERP patients regained functional capabilities earlier, with less fatigue and need for sleep than patients receiving traditional care. Early discharge was not associated with an increased burden to the care team.39
SUMMARyClinicians around the world are functioning in an era of healthcare management reform, reduced cost initiatives concomitant with increased patient safety for improved outcomes, and pay-for-performance programs. Optimization of health care practice is therefore urgent, especially in colorectal surgery where complications occur at a disproportionately high rate compared with all other operative procedures.40 As with any intervention or care pathway, variability in outcomes exists between healthcare systems. Some outcomes (i.e., length of stay, readmission due to complications, etc) may be important as a marker for improved care. For example, a patient is not actually ‘‘healthier’’ because he/she leaves the hospital fourteen hours sooner than another, but he may be recovering with lesser difficulty and therefore can meet discharge criteria sooner.41 Yet several studies have demonstrated that the ERAS pathways are associated with earlier recovery and discharge after colorectal surgery as compared with traditional perioperative care.
Through the development of recovery pathways, ERAS encompasses a systematic and evidence-based approach that has proven to be efficacious in improving the quality and efficiency of surgical care.
15
REFERENCES
1. History of the ERAS Society. (n.d.). Retrieved February 7, 2015, from http://www.erassociety.org/index.php/about-us/history
2. Adamina, M., Kehlet, H., Tomlinson, G., Senagore, A., & Delaney, C. Enhanced recovery pathways optimize health outcomes and resource utilization: A meta-analysis of randomized controlled trials in colorectal surgery. 2011 Jun;149(6):830-40. doi: 10.1016/j.surg.2010.11.003. Epub, 2011 Jan 14.
3. Nygren, J., Thacker, J., Carli, F., Fearon, K., Norderval, S., Lobo, D., Ramirez, J. (2013). Guidelines for perioperative care in elective rectal/pelvic surgery: Enhanced Recovery After Surgery (ERAS) Society recommendations. Clinical Nutrition, 37, 285-305. doi: 10.1007/s00268-012-1787-6.
4. Khoo, C., Vickery, C., Forsyth, N., Vinall, N., & Eyre-Brook, I. A Prospective Randomized Controlled Trial of Multimodal Perioperative Management Protocol in Patients Undergoing Elective Colorectal Resection for Cancer. Annals of Surgery, 245, 867-872. 2007.
5. Kehlet, H., & Dahl, J. Anesthesia, Surgery and Challenges in Postoperative Recovery.The Lancet, 362, 921-8. 2003.
6. Wind, J., Polle, S., Jin, P., Dejong, C., & Bemelman, W. (n.d.). Enhanced recovery after surgery programs in colonic surgery: A systematic review. European Journal of Gastroenterology & Hepatology, 93,800-9.
7. Gouvas, N., Tan, E., Windsor, A., Xynos, E., & Tekkis, P. (2009). Fast-track vs. standard care in colorectal surgery: A meta-analysis update. International Journal of Colorectal Disease, 24, 1119-31 doi: 10.1007/s00384-009-0703-5.
8. Tonnesen, H., Nielsen, P., Lauritzen, J., & Moller, A. (2009). Smoking and alcohol intervention before surgery: Evidence for best practice. British Journal of Anaesthesia, 102, 297-306.
9. Preoperative alcoholism and postoperative morbidity. Tonnesen, H., Kehlet, H., Br J Surg. 1999 Jul;86(7):869-74.
10. Tonnesen H, Rosenberg J, Nielsen HJ, Rasmussen V, Hauge C, Pedersen IK et .al. Effect of preoperative abstinence on poor postoperative outcome in alcohol misusers: randomized controlled trial. 1999. BMJ 318(7194):1311–1316
11. Lindstrom D, Sadr Azodi O, Wladis A, Tonnesen H, Linder S, Nasell H et. al., Effects of a perioperative smoking cessation intervention on postoperative complications: a randomized trial. 2008. Ann Surg 248(5):739–745

16
12. Brady, M., Kinn, S., & Stuart, P. Preoperative fasting for adults to prevent perioperative complications. January 2009. Retrieved February 7, 2015, from http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD004423
13. Soreide, E., & Ljungqvist, O. Modern Preoperative Fasting Guidelines: A Summary Of The Present Recommendations And Remaining Questions. Best Practice & Research Clinical Anaesthesiology, 20, 483-491. 2006.
14. Gustafsson, U., Nygren, J., Thorell, A., Soop, M., Hellstrom, P., Ljunggvist, O., & Hagstrom-Toft, E. Pre-operative carbohydrate loading may be used in type 2 diabetes patients.Acta Anaesthesiologica Scandinavica, 52, 946-951.
doi: 10.1111/j.1399-6576.2008.01599. 2008.
15. Rasmussen, M., Jorgensen, L., & Wiille-Jorgensen, P. Prolonged thromboprophylaxis with Low Molecular Weight heparin for abdominal or pelvic surgery. January 2009. Retrieved February 7, 2015, from http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD004318.pub2/abstract
16. Amaragiri, S., & Lees, T. Graduated compression stockings for prevention of deep vein thrombosis. January 2000. Retrieved February 7, 2015, from http://onlinelibrary.wiley.com/o/cochrane/clsysrev/articles/CD001484/frame.html
17. Fleming, F., Kim, M., Salloum, R., Young, K., & Monson, J. How Much Do We Need to Worry About Venous Thromboembolism After Hospital Discharge? A Study of Colorectal Surgery Patients Using the National Surgical Quality Improvement Program Database.Diseases of the Colon & Rectum, 53, 1355-1360. 2010.
18. Bamboat, Z., & Bordeianou, L. Perioperative fluid management. Clinics in Colon and Rectal Surgery, 22, 28-33. 2009.doi: 10.1055/s-0029-1202883 PMCID: PMC2780230.
19. Bundgaard-Nielsen, M., Secher, N., & Kehlet, H. ‘Liberal’ vs. ‘restrictive’ perioperative fluid therapy - a critical assessment of the evidence. Acta Anaesthesiologica Scandinavica,53, 843-851. 2009.
20. Baca, B., Gönenç, M., Hamzaodlu, I., & Karahasanodlu, T. Randomized clinical trial comparing epidural anaesthesia and patient-controlled analgesia after laparoscopic segmental colectomy(Br J Surg 2003; 90: 1195-1199). British Journal of Surgery, 90, 1195-1199.
21. Virlos, I., Clements, D., Beynon, J., Ratnalikar, V., & Khot, U. Short-term outcomes with inthrthecal versus epidural analgesia in laparoscopic colorectal surgery. 2010. The British Journal of Surgery, 97, 1401-1406 doi: 10.1002/bjs.7127.

17
22. Noblett, S., Snowden, C., & Horgan, A. (2006). Authors’ reply: Randomized clinical trial assessing the effect of Doppler-optimized fluid management on outcome after elective colorectal resection (Br J Surg 2006; 93: 1069–1076). British Journal of Surgery, 93, 1069-1076.
23. Guenaga, K., Matos, D., & Wille-Jorgensen, P. Mechanical bowel preparation for elective colorectal surgery. January 2011. Retrieved February 7, 2015, from http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD001544.pub4/abstract
24. Anderson, H., Lewis, S., & Thomas, S. (2006, January 1). Early enteral nutrition within 24 h of colorectal surgery versus later commencement of feeding for postoperative complications. Retrieved February 7, 2015, from http://onlinelibrary.wiley.com/CD004080/abstract.
25. Houborg KB1, Jensen MB, Hessov I, Laurberg S. Little effect of physical training on body composition and nutritional intake following colorectal surgery--a randomised placebo-controlled trial.
26. Henriksen MG, Jensen MB, Hansen HV, Jespersen TW, Hessov I. Enforced mobilization, early oral feeding, and balanced analgesia improve convalescence after colorectal surgery. 2002. Nutrition 18(2):147–152]. Eur J Clin Nutr. 2005 Aug;59(8):969-77.
27. Jensen MB, Houborg KB, Norager CB, Henriksen MG, Laurberg S. Postoperative changes in fatigue, physical function and body composition: an analysis of the amalgamated data from five randomized trials on patients undergoing colorectal surgery. 2001. Colorectal Dis 13(5):588–593.
28. Vlug MS, Wind J, Hollmann MW, Ubbink DT, Cense HA, Engel AF et a. Laparoscopy in combination with fast track multimodal management is the best perioperative strategy in patients undergoing colonic surgery: a randomized clinical trial (LAFA-study). 2011. Ann Surg 254(6):868–875.
29. Convertino VA. Cardiovascular consequences of bed rest: effect on maximal oxygen uptake. 1997. Med Sci Sports Exerc 29(2):191–196.
30. B. F. Levy, H. S. Tilney, H. M. P. Dowson and T. A. Rockall. A systematic review of postoperative analgesia following laparoscopic colorectal surgery. doi:10.1111/ j.1463-1318.2009.01799.
31. Jouve, P., Bazin, JE., Petit, A., Minville, V., Gerard, A., Buc, E., Dupre, A., Kwiatkowski, F., Constantin, JM., Futier, E. Epidural versus continuous preperitoneal analgesia during fast-track open colorectal surgery: a randomized controlled trial. 2013 Mar;118(3):622-30.

18
32. Gustafsson UO, Hausel J, Thorell A, Ljungqvist O, Soop M, Nygren J. Adherence to the Enhanced Recovery After Surgery protocol and outcomes after colorectal cancer surgery. 2011. Arch Surg 146(5):571–577.
33. Goodney, P., Stukel, T., Lucas, F., Finlayson, E., & Birkmeyer, J. Hospital Volume, Length of Stay, and Readmission Rates in High-Risk Surgery. 2003. Annals of Surgery, 238, 161-167.
34. Senagore, A., & Delaney, C. A critical analysis of laparoscopic colectomy at a single institution: Lessons learned after 1000 cases. 2006.The American Journal of Surgery, 191, 377-380.
35. Kariv, Y., Delaney, C., Senagore, A., Manilich, E., Hammel, J., Church, J., ... Fazio, V. Clinical Outcomes and Cost Analysis of a “Fast Track” Postoperative Care Pathway for Ileal Pouch-Anal Anastomosis. A Case Control Study. Diseases of the Colon & Rectum, 50, 137-146. 2007.
36. Kariv, Y., Wang, W., Senagore, A., Hammel, J., Fazio, V., & Delaney, C. (2006). Multivariable analysis of factors associated with hospital readmission after intestinal surgery. The American Journal of Surgery, 191, 364-371.
37. Azimuddin, K., Rosen, L., Reed, J., Stasik, J., Riether, R., & Khubchandani, I. (2001). Readmissions after colorectal surgery cannot be predicted. Diseases of the Colon & Rectum, 44, 942-946.
38. Delaney, C. Outcome of Discharge Within 24 to 72 Hours After Laparoscopic Colorectal Surgery. Diseases of the Colon & Rectum, 51, 181-185. 2008.
39. Jakobsen, D., Sonne, E., Andreasen, J., & Kehlet, H. (2006). Convalescence after colonic surgery with fast-track vs conventional care. Colorectal Disease, 8, 683-687.
40. Schilling, P., Dimick, J., & Birkmeyer, J. (2008). Prioritizing Quality Improvement in General Surgery. Journal of the American College of Surgeons, 207, 698-704.
41. Gustafsson, U., Hausel, J., Thorell, A., Ljungqvist, O., Soop, M., & Nygren, J. (2011). Adherence to the Enhanced Recovery After Surgery Protocol and Outcomes After Colorectal Cancer Surgery. Archives of Surgery, 146, 571-577.
19
GLOSSARyAnastomotic leakage Leaking of fluids through an anastomosis, or the
new connection created in the intestines during surgery.
Cochrane Reviews/Reports Full-text systematic reviews which provide an overview of the effects of interventions in health care. The reviews are highly structured.
Evidence from clinical trials is included on the basis of explicit quality criteria, thus minimizing bias.
Enhanced Recovery After Surgery An organization dedicated to developing (ERAS) Society perioperative care and improving recovery through research, audit education and implementation of evidence-based practice.Enhanced Recovery Pathway (ERP) A clinical tool, or care map, used to manage
the quality in healthcare concerning the standardization of care processes.
Hypercoaguable State An abnormality of blood coagulation that increases the risk of blood clots in blood vessels.
LAFA Study A study that combines laparoscopy and fast track multimodal management.
Mechanical Bowel Preparation The use of an oral preparation given prior to (MBP) surgery to clear fecal material from the bowel lumen often prescribed preoperatively for patients undergoing elective colorectal surgery.Multivariate Linear Regression Where multiple correlated dependent variables Analysis are predicted, rather than a single scalar variableEsophageal Doppler system A probe is inserted into the patient’s esophagus,
and measures velocity of blood flow in the descending aorta.
Pneumoperitoneum The presence of air or gas in the abdominal (peritoneal) cavity.
Randomized Controlled Trials A scientific (often medical) experiment, where (RCT) the patient group being studied are randomly allocated one or other of the different treatments under study. The RCT is the gold standard for a clinical trial.Third Space Fluid Retention Functional loss of fluid that cannot be accounted
for by measurable fluid losses during bowel surgery.

20
Please click here for thePost-Test and Evaluation