Embed Size (px)
Citation preview

1/27/2017
1
LESSONS LEARNED:Statewide Implementation
of an Evidence-BasedGuideline
Report to NAEMSP2017 Annual Meeting
Background
“...Convene a panel ofindividuals withmultidisciplinary
expertise to developevidence-based model
prehospital careprotocols for the
treatment, triage, andtransport of patients,including children.”
NHTSA EBG Project Timeline

1/27/2017
2
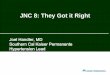
EBG Model Process Overview
11
System InputsPrehospital components of externally developed
guidelines, e.g., AHA, NAESP, BTF, NICE, NZGGProtocols from existing EMS systems, e.g., State EMS
protocols, Nova Scotia protocolsExternal evidence synthesis processes, e.g.,
Cochrane systematic reviews, EPCsIndividual researchers, EMS organizations, medical
directors, & EMS personnel
Guideline Initiation: EMS EvidenceAccumulation & Evaluation
Review proposals for guideline development,adaptation, or adoption
Identify existing systematic reviewsRecommend need for (or conduct) systematic reviewAssemble advisory panel with expertise in topic,
guideline development, library science, etc.Document conflicts of interest for all participants
National Prehospital Evidence-based GuidelineModel Process
Approved by the Federal Interagency Committee on EMS and the National EMS Advisory Council
AbbreviationsAGREE – Appraisal of Guidelines Research and Evaluation CMS – Center for Medicare and Medicaid Services NAEMSP – National Association of EMS PhysiciansAHA – American Heart Association EMSCAP – Emergency Medical Services Cost Evaluation Project NEMSIS – National EMS Information SystemBTF – Brain Trauma Foundation EMSOP – Emergency Medical Services Outcomes Project NICE – National Institute for Health and Clinical Excellence
NZGG – New Zealand Guidelines Group
Establish Priorities forGuideline Development
Evaluate quality of evidence orguideline, e.g., GRADE, AGREE
Recommend topics for furtherguideline development
Archive material not selected forfuture use
Guideline DevelopmentDocument risks & benefits of
intervention - First do no harmDevelop strength of recommendation,
e.g., GRADEDocument & disseminate rationale
for “no recommendation”EMS “contextualization”Write, adapt, or endorse guidelineProvide feedback to originating
institution or organization
EMS ProtocolDevelopment
EMS “contextualization”Clinical implications of strength of
recommendation
Dissemination of Guidelines/ProtocolsLink to EMS Education Agenda for the Future Core
Content Scope of Practice Model National EMSEducation Standards
Link to National EMS Education Program AccreditationPublications: peer-reviewed journals, trade press,
textbooks, government reportsNew products: education materials, quality
improvement materialsTarget stakeholder organizationsMultimedia approach: ems.gov, podcasts, etc.
ImplementationLink to national EMS provider certification &
recertificationLink to national EMS agency accreditationDevelop guideline implementation “tool kits,”
webinars, manuals, integration into local protocolsPartner with national orgs. To facilitate interpretation,
application & medical directionPotentially link to funding and reimbursement, e.g.,
CMS, 3rd partyDevelop health informatics & clinical decision support
softwareDevelop quality improvement measures & tools – local,
regional, state & tribal
Evaluation of Effectiveness, Outcomes,Clinical Research, Quality Improvement
EvaluationsGuideline/protocol pilot testing & feasibility studies (may
occur during development process)Monitor local quality improvement benchmarks & indicators,
quality improvement processes at all levelsApply NEMSIS data in evaluation processOutcomes research: EMSOP – local, regional, statewide,
nationalClinical research of specific questionsSystems research (See EMSOP II & IV)Cost effectiveness, cost-utility, cost-benefit analysis (See
EMSCAP papers)Implementation research – analysis of barriers & facilitators
to implementation
pre-existing protocols
new protocols
NHTSA/EMSC Funded ProjectsStatewide
Implementationof an EBG(2012-2016)
PECSupplement:EBGs in EMS(January 2014)
Model EMSClinical
Guidelines(2013-2014)
PEGASUS(2013-2015)
A National Strategy toPromote Prehospital
Evidence Based GuidelineDevelopment andImplementation
Statewide Implementationof an Evidence BasedGuidelinePeriod of Performance:
September 29, 2012 – September 30, 2016

1/27/2017
3
Project Basics Competitive award to the National Association of State EMS
Officials (NASEMSO) through NHTSA with supplementalfunding provided by HRSA EMS for Children Program
Project Team Leads: Matthew Sholl, MD (co-PI)
Peter Taillac, MD (co-PI)
Kathleen Adelgais, MD (PEM Consultant)
Rachael Alter (NASEMSO Staff)
PURPOSE: To support the use and further refinement of theNational EBG Model Process by studying the implementationof a pain management EBG in five volunteer states with avariety of EMS organizational structures.
Project Basics State Participants: Arizona, Idaho, Kansas, Tennessee, Wyoming
Guideline: Prehospital Protocol for the Management of Acute Traumatic
Pain
EBG Manuscript: Gauche-Hill, et al., EBG for PrehospitalAnalgesia in Trauma (PEC 2014)
Why Pain Management?
Develop Strategies for Identification andManagement of Pain
“Pain is a frequent symptom among patients accessing theEMS system. The recognition and management of pain inthe EMS setting needs to be improved. Assessment toolsdesigned to accurately identify and quantify pain areneeded for all patients, including those with limitedcognitive or language abilities”
Sayre et al, Prehospital Emergency Care, 2005

1/27/2017
4
Why Pain Management? (cont’d)
Known Barriers
Evidence there aredisparities in theprehospital environment
Fear of dosing mistakes =undertreating
Need for medicaldirection approvalbefore narcotics given topatients
EBG Solution
Consistency
Easy to remember dosing& use of pain scales
Standing order to avoidcalling medical direction
State Selection Criteria Authority for Mandated
Protocols Have it, but don’t exercise it In Statute None
Mandatory vs LocalProtocols/Guidelines Mix of model guidelines and
local only 2 states were in the process of
implementing model guidelineswhen the project started
Current Pain Guideline? Yes (n=2)
All Allow Fentanyl
Licensed EMS Agencies <150 (n=2) 151-250 (n=3)
% Urban 30% - 89%
All Collecting NEMSIS 2
Agencies Submitting Data &Total Runs Submitted All above 75%

1/27/2017
5
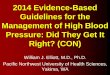
States with ALS Protocols
Courtesy of Kupas et. al, in press, PEC 2015
Project Accomplishments
Developed Implementation, Dissemination, andEvaluation Toolkit
Developed individual state implementation plans Program Plan Evaluation Roadmap
Created online training/PPTs For EMS Personnel (1 hour) Pre- & post-tests Simulation scenarios Pain assessment/self-efficacy tools
Hospital ED staff (15 minutes)
`
[This Toolkit contains resources developed for State EMS Offices participating in theNASEMSO Statewide Implementation of a Prehospital Care Guideline Project.]
TheStatewideImplementationofaPrehospitalCareGuidelineToolkitisfundedbyaCooperativeAgreementthroughtheU.S.DepartmentofTransportation,NationalHighwayTrafficSafetyAdministration,OfficeofEmergencyMedicalServices,CooperativeAgreementNumberDTNH22-12-H-00386withsupplementalfundingfromtheEmergencyMedicalServicesforChildrenProgram(HealthResourcesandServicesAdministration).
Toolkit Materials
1. Evidence-Based GuidelineInformation
a. EBQ FAQs
b. National EBG Model Process
c. GRADE Process
d. EBG & GRADE Resources
e. Guideline
f. Pain Scales
g. Guideline Key Elements
h. Guideline Data Elements
i. Example of Pain ManagementProtocol
2. References
a. Essential Articles
b. Recommended Articles
c. Supplemental Articles
3. Talking Points / FAQ
4. Implementing a StatewideGuideline – How To
5. Educational Resources
6. Evaluation Resources
a. Evaluation Components
b. Agency Adoption Assessment Tool

1/27/2017
6
Project Accomplishments
Developed Implementation, Dissemination, andEvaluation Toolkit
Developed individual state implementation plans Program Plan Evaluation Roadmap
Created online training/PPTs For EMS Personnel (1 hour) Pre- & post-tests Simulation scenarios Pain assessment/self-efficacy tools
Hospital ED staff (15 minutes)
Project Accomplishments
Developed Implementation, Dissemination, andEvaluation Toolkit
Developed individual state implementation plans Program Plan Evaluation Roadmap
Created online training/PPTs For EMS Personnel (1 hour) Pre- & post-tests Simulation scenarios Pain assessment/self-efficacy tools
Hospital ED staff (15 minutes)
State Status One state did not implement the Pain Management
Protocol
Instead, developed state-based guideline
One state did disseminate, but not implement theguideline
Three states disseminated and implemented theguideline Across the entire state
Within regions of the state
Within services

1/27/2017
7
Preliminary Findings – Barriers General Barriers Need speedier release of EBGs and updates on a timely basis
(perception that EBG is ‘out of date’)
Potential push back: “Doses are too small”
“Hesitant to use opioids due to restocking”
Local feeling that current state protocol more ‘expansive’
Concern for state and federal regulatory issues surroundingscheduled medications
Dissemination Barriers Delays between project announcement and project exicution
EBG should be more inclusive of basic/intermediate levels
Preliminary Findings – Barriers Education Barriers Creation of a training at a national level may not be beneficial
to states who want a more “local touch”
Issues with state IT has caused delays in trainingimplementation
Implementation barriers Difficult in states with no “local champion”
Difficulties in states without prior process of guideline releaseor practice with a process for dissemination
Difficult to track successes of educational programs
Difficult for states to measure metrics of interest to theproject team
Preliminary Findings – Enablers General Enablers Strong local champion/advocate
Dissemination/Education Enablers Mechanisms for communication & messaging with EMS services
at the local/regional level Pre-existent Learning Management System (LMS) at the state level
Implementation Enablers Pre-existing state-based guidelines – including model guidelines
Use of implementation “tool-kit”

1/27/2017
8
Recommendation #1 – Develop state model ormandatory guidelines
States with existing model guidelines (2) appeared to haveeasier time with both dissemination and implementation
Why is this? Is it easier for local medical directors to adopt these protocols?
Are local services more aware due to history of modelguidelines?
Does the history of model guidelines within a state or regionfacilitate conversation?
Recommendation #2 – Establish protocoldissemination and implementationchampions Benefit of project champions are well described in the
literature
Essential elements include Ability to foster change – based on legislated authority or
respect within the system in question Consensus building Able to encourage evolution amongst wide variety of health
care providers
NOT ENOUGH to have champions at the state-level Need champions throughout the EMS system – regional/sub-
regional/local service
Recommendation #3 –Improve/facilitate the evidence basedguideline development process EBG release delay lead to frustration amongst
participating states and in one case lead to a statebuilding and adopting their own guideline
Concern regarding time required to develop an EBG
The EBG for Management of Pain in Trauma was one ofthe first EBG’s created
With subsequent practice developing EBG’s, process hasbeen facilitated and much shorter in duration

1/27/2017
9
Recommendation #4 – Consider learningmanagement systems as one element ofthe dissemination and implementationstrategy Prior experience suggest learning management systems can
assist with dissemination and implementation of guidelines Based on NASEMSO survey of State Medical Directors/Directors
Must be “user friendly” with easy interface for users
Allows learners to offer feedback or post questions
Must be functional in areas with poor internet connectivity
Must be functional for the state. Easy to post material Easy to track participants’ program completion/success
Recommendation #5 – Consider using atoolkit for the dissemination andimplementation process State’s uniformly thought the tool kit was helpful
Pre-Hospital Guidelines Consortium adopting the formatof the Toolkit to assist in future EBG dissemination andimplementation
Toolkit content can be found at www.NASEMSO.org -under projects
Recommendation 6 – Develop systems,coordinated with the implementationproject, that are able to track EBGimplementation One key to success is the ability to measure progress
Each state encountered difficulty measuring key projectmetrics Use of pain scales Delivery of pain medications Reassessment of pain
Without the ability to measure progress, left with onlyanecdote
Along with data – need to find means to receive feedbackfrom guideline “end-users” as a means to discover theirimpressions

1/27/2017
10
Is This Experience Only Importantto State EMS Officials?
Disseminating and Implementing pre-hospital guidelinesat the state-level may be the most difficult
Many of the lessons of this project have direct impacton regional/sub-regional/local service protocoldevelopment Champions
Learning Management systems
Toolkits
Measure and share success
Questions?www.nasemso.org/Projects/ImplementationOfEBG