-
8/11/2019 125 Introduction to Cardiovascular Physiology
1/8
Sign up to receive ATOTW weekly email
[email protected]
INTRODUCTION TO CARDIOVASCULARPHYSIOLOGYANAESTHESIA TUTORIAL OF
THE WEEK 125
16TH
MARCH 2009
Toby Elkington, Specialist RegistrarCarl Gwinnutt,
ConsultantDepartment of Anaesthesia, Salford Royal !S
"oundationTrust, Salford, #$Correspondence to
tobyelkington%hotmail&com
This tutorial is intended as a very basic introduction to
cardiovascular physiology with particularreference to anaesthesia.
Once these basic principles have been mastered then it will be
appropriate to
move on to the more detailed tutorials that are available.
Every anaesthetic given to a patient will have an impact on
their physiology and in particular on the
cardiovascular system. Therefore understanding the physiology of
the cardiovascular system allows a !etterappreciation of the
changes that occur when an anaesthetic is given and when and how
!est to treat any adverse
events.
"efore reading this tutorial think a!out the following#$% What
events occur in the heart each time it !eats&
'% (ow much !lood does the heart pump out&)% What factors
affect the amount of !lood the heart pumps out&
*% (ow is !lood pressure related to !lood flow from the
heart&+% What are the normal cardiovascular responses to
hypovolaemia&
,% (ow do anaesthetics affect the cardiovascular system&
ANATOMY
The heart is composed of four cham!ers left atrium and ventricle
and right atrium and ventricle. The atria and
ventricles are separated !y the atrioventricular -A% valves
mitral on the left and tricuspid on the right./eo0ygenated !lood
returns from the !ody via the great veins -superior and inferior
vena cavae% to the right
atrium and then passes through the tricuspid valve into the
right ventricle. 1rom here !lood is pumped throughthe pulmonary
valve into the pulmonary artery -the only artery which carries
deo0ygenated !lood in an adult%
and on through the pulmonary capillaries in the lungs where it
is o0ygenated -and car!on dio0ide removed%."lood returns to the
left side of the heart via the pulmonary veins -the only veins to
carry o0ygenated !lood in
the adult% into the left atrium then through the mitral valve
into the left ventricle. 1rom the left ventricle !loodis pumped
through the aortic valve into the aorta and then via the systemic
vascular tree to the !ody2s organs.
The vascular tree is comprised of arteries arterioles
capillaries venules and veins conventionally descri!ed
inprogressive order leaving from the left side of the heart and
returning to the right. The arterial side of the
circulation carries o0ygenated !lood. "oth arteries and
arterioles have thick muscular walls as they carry !lood
under relatively high pressure. The average adult has a
circulating volume of appro0imately +333ml !lood. 4nthe normal
resting state only a!out $+5 -6+3ml% of the circulating volume is
within the arterial system. As
!lood traverses capillary !eds the pressure falls and the !lood
gives up o0ygen and other nutrients to the tissueswhile at the same
time collecting car!on dio0ide and other waste products of
meta!olism. The !lood now
relatively deo0ygenated starts its return 7ourney to the heart
in the venules and veins -thin8walled !ecause of thelow pressure%
finally entering the vena cavae. The venous system contains
appro0imately ,35 -)333ml% of the
!lood volume and is often referred to as a capacitance system
the volume of which can !e varied significantly!y the sympathetic
nervous system -see !elow%. The remaining '+5 -$'+3ml% of the !lood
volume is in the
pulmonary circulation and heart.
ATOTW 125. 4ntroduction to 9ardiovascular :hysiology
$,;3);'33< :age $ of =
mailto:[email protected]:[email protected]
-
8/11/2019 125 Introduction to Cardiovascular Physiology
2/8
Sign up to receive ATOTW weekly email
[email protected]
THE CARDIAC CYCLE
The cardiac cycle refers to the mechanical events that occur
during the contraction-systole% and rela0ation -diastole% of the
ventricular muscle. 4t must !e
remem!ered that this activity is initiated !y the cardiac action
potential thatoriginates in the sino8atrial -SA% node spreads
through the atrial muscle crosses
the atrio8ventricular -A% node reaches the ventricles via the
!undle of (is andsupplies the :urkin7e fi!res which innervate the
ventricles. The sum of these
action potentials is recorded as the E9>?: wave atrial
depolarisation
: interval spread of e0citation through the atria A node and
!undle of (isS comple0 spread of e0citation through the
ventricles
T wave ventricular repolarisation
There are two important points to remem!er#$. Bechanical
contraction occurs after depolarisation therefore systole starts at
the end of the S
comple0 and ends during the T wave.
'. A cardiac action potential or E9> signal does not mean
that the heart is pumping !lood it onlyindicates electrical
activity -remem!er the cardiac arrest patient with pulseless
electrical activity-:EA%.
Systole is the period of ventricular contraction. As contraction
starts in !oth ventricles the A valves close toprevent !ack flow of
!lood into the atria. entricular contraction continues with a rapid
increase in pressure !ut
no change in volume? this is called isovolumetric contraction
-meaning literally Csame volumeD%. Eventuallythe pressure within
the left and right ventricles e0ceeds the pressures in the aorta
and pulmonary arteries
respectively and at this point the aortic and pulmonary valves
open and e7ection of !lood occurs. The amount of!lood e7ected in
one cycle is referred to as the stroke volume -S% and this is
around 63ml in an average adult at
rest. (owever the ventricles do not completely empty only si0ty
to eighty percent of the !lood present in the
ventricle is e7ected -the e7ection fraction%. As the ventricles
empty the pressure within them starts to fall. Whenthe pressure
drops !elow that in the aorta and pulmonary artery the aortic and
pulmonary valves respectively
close signalling the end of systole.
/iastole is the period of ventricular rela0ation. 4nitially
there is a period of isovolumetric rela0ation -again
Csame volumeD% and all the valves are closed. As the atria fill
with !lood returning to the heart the pressurerises when it e0ceeds
that in the ventricles the A valves open and as a period of passive
filling occurs the
volume of !lood in the ventricles starts to increase. This
passive filling is initially rapid !ut slows as thepressure
gradient across the A valves decreases. entricular filling is
completed !y contraction of the atria
contri!uting twenty to thirty percent of ventricular volume and
signalling the end of diastole. The volume of!lood in the ventricle
at this point is often referred to as the end8diastolic volume -E/%
and is normally around
$'3ml.
4t is interesting to consider how long each of these components
of the cycle takes as heart rate varies. ndernormal resting
conditions heart rate is appro0imately 63 !eats;min and each
cardiac cycle therefore takes
appro0imately 3.=+ sec. Systole lasts 3.) sec and diastole lasts
3.++ sec most of the time !eing taken up !yventricular filling. Fow
consider what happens when the heart rate is $=3 !eats;min? each
cycle takes up 3.)
sec with diastole and systole !oth lasting 3.$+ sec. /iastole
has !een reduced more than systole -3.*seccompared to 3.$+sec%
reducing the time for ventricular filling. Systole cannot !e
reduced any more without
affecting the stroke volume. An increase in heart rate !eyond
this rate reduces diastole further resulting ininsufficient time
for ventricular filling and a reduction in the volume of !lood
pumped out with each !eat.
Therefore for most adults the ma0imum heart rate is around
$=3!eats;min. 4n addition perfusion of the muscles
of the ventricles -via the coronary arteries% occurs
predominantly during diastole. /ue to this at very high heartrates
the duration of coronary !lood flow is reduced. This is the very
time when the heart is working ma0imally
and so has a high o0ygen demand risking myocardial ischaemia
-inadeGuate o0ygen supply to cardiac muscle%.
CARDIAC OUTPUT
So far we have defined the amount of !lood e7ected !y each heart
!eat as the stroke volume. (owever it is the
constant flow of !lood that is more important and this is
referred to as the Ccardiac outputD. 9ardiac output -9O%
ATOTW 125. 4ntroduction to 9ardiovascular :hysiology
$,;3);'33< :age ' of =
-
8/11/2019 125 Introduction to Cardiovascular Physiology
3/8
Sign up to receive ATOTW weekly email
[email protected]
is defined as the volume of !lood e7ected !y each ventricle per
minute and is theproduct of the stroke volume -S% and the heart
rate -!eats;min% it is e0pressed in
litres;min. 9learly the output of !oth ventricles has to !e the
same otherwise allthe !lood would end up in either the systemic or
pulmonary circulationH
Cardiac Output = Stroke Volume x Heart Rate
nder normal resting conditions this is appro0imately 63ml 0
63!eats;min I*
-
8/11/2019 125 Introduction to Cardiovascular Physiology
4/8
Sign up to receive ATOTW weekly email
[email protected]
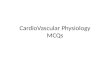
Myocardial contractilityThis refers to the intrinsic a!ility of
the cardiac muscle fi!res to contract and is independent of the
degree of
preload and afterload. This is often referred to as the degree
of inotropy and su!stances affecting this propertyare called
inotropes? those increasing rate and force of contractility have a
positive inotropic action those that
decrease contractility have a negative inotropic action. The
most important determinant of contractility is thesympathetic
nervous system. 4t acts directly or via the release of
catecholamines from the adrenal gland
stimulating adrenergic receptors -i.e. they respond to
adrenaline see !elow% which results in a positive inotropiceffect
-1ig '.%. Bany factors cause a decrease in contractility i.e. are
negatively inotropic? e0amples would !e an
acidosis hypo0ia hypocalcaemia and many drugs -particularly
anaesthetics and antiarrhythmic drugs%.
1ig '.
Afterload
At the end of diastole the ventricular muscle starts to
contract. 4n order to achieve this it has to overcome thoseforces
that are preventing it namely the tension in the ventricular wall
itself and the resistance offered to the
ATOTW 125. 4ntroduction to 9ardiovascular :hysiology
$,;3);'33< :age * of =
-
8/11/2019 125 Introduction to Cardiovascular Physiology
5/8
Sign up to receive ATOTW weekly email
[email protected]
e7ection of !lood from the ventricle. 9learly this will !e very
different for !othventricles. Beasurement of true afterload is
difficult and usually appro0imated as
follows# Keft ventricular afterload is the resistance offered !y
the systemic circulation
and termed the systemic vascular resistance -S%. ight
ventricular afterload is the resistance offered !y the
pulmonary
circulation and termed the pulmonary vascular resistance
-:%.
4n health afterload is determined predominantly !y vascular tone
or the degree ofvasoconstriction -or dilatation% of the arteries
and arterioles. The greater the
degree of constriction the smaller the vascular lumen and the
greater theresistance offered to e7ection of !lood from the
ventricle. As a result for a given
preload and contractility less !lood will !e e7ected the end
systolic volume is
increased and stroke volume falls. ascular tone is controlled !y
the sympathetic nervous system and !y therelease of catecholamines
again acting on adrenergic receptors.
2. Fac!"# a$$%c&'( % %a" "a%The heart has an intrinsic
pacemaker the sinoatrial node which in the a!sence of any other
influence discharges
at around $33 !eats;min. 9hanges in heart rate are !rought a!out
!y the autonomic nervous system eitherdirectly or via effects on
the adrenal glands. >enerally speaking sympathetic stimulation
will increase the heart
rate via adrenergic receptors -a positive chronotropic effect%
and parasympathetic stimulation via the vagusnerve will decrease
the heart rate -a negative chronotropic effect%. nder normal
circumstances resting heart
rate is !elow $33 !eats;min and therefore there is dominance of
vagal -parasympathetic% activity. :rovidingstroke volume is
unchanged an increase in heart rate will cause a rise in cardiac
output and vice versa -9OIS
0 (%. This is true in normal healthy individuals as the stroke
volume is relatively unaffected !etween heartrates of +38$+3;min.
As e0plained a!ove at heart rates much greater than this stroke
volume eventually falls
along with cardiac output. At lower heart rates ventricular
filling can increase to compensate !ut the point iseventually
reached where filling -E/% is ma0imal and with a further reduction
in rate once again cardiac
output will fall. 1or e0ample if the ma0imal stroke volume is
$'3ml cardiac output will fall once the heart ratedrops !elow
*3!eats;min.
ADRENERGIC RECEPTORS AND THEIR ACTIONS
These receptors respond to stimulation !y the sympathetic
nervous system and catecholamines from the adrenal
gland. Their primary function is to prepare the !ody for the
primitive Cfight or flightD response? ventilationincreases along
with !ronchodilation cardiac output is increased through an
increase in rate and contractility
and !lood is diverted from non8vital organs -e.g. the gut% to
vital organs -e.g. heart kidneys and muscle%. Thereare two main
types of adrenergic receptors alpha -L% and !eta -M% each of which
is divided into two su!types L8
$ L8' and M8$ M8'. Their location and actions in the
cardiovascular system when stimulated is shown in ta!le
$.
Ta/+% 1.Adrenergic receptors and their effectseceptor type
Kocation Effects
Alpha8$ "lood vessels asoconstrictionAlpha8' "lood vessels
asoconstriction
"eta8$ (eart 4ncrease heart rate4ncrease force of
contraction
"eta8' "lood vesselsKungs
asodilatation"ronchodilatation
LOOD PRESSURE
So far we have concentrated on !lood flow from the heart -the
cardiac output% however in day8to8day practicewe rarely measure
flow -it is technically difficult to measure flow accurately% !ut
freGuently measure !lood
pressure. 4t is important to understand how the two are related
as pressure does not eGuate to flow? patients can
ATOTW 125. 4ntroduction to 9ardiovascular :hysiology
$,;3);'33< :age + of =
-
8/11/2019 125 Introduction to Cardiovascular Physiology
6/8
Sign up to receive ATOTW weekly email
[email protected]
have a CnormalD !lood pressure with much reduced flow and vice
versa. Whenmeasuring systemic arterial pressure a num!er of
different figures can !e
calculated.
Systolic pressure the ma0imum pressure generated normally
around$'3mm(g
/iastolic pressure the minimum pressure generated normally
around=3mm(g
:ulse pressure the difference !etween systolic and diastolic
normally*3mm(g
Bean pressure the average over each complete cardiac cycle. This
can !eappro0imated to diastolic pressure plus one third of the
pulse pressure and is
normally around
-
8/11/2019 125 Introduction to Cardiovascular Physiology
7/8
Sign up to receive ATOTW weekly email
[email protected]
maintains adeGuate organ perfusion. 4nitially S will increase to
a greatere0tent than 9O hence we may have a CnormalD !lood pressure
!ut reduced
9O.+. The sympathetic activity will also constrict vessels of
non8essential organs
e.g. the skin and gut to divert !lood to vital organs e.g. !rain
and heart.,. A/( is released from the pituitary which increases
rea!sorption of water and
sodium in the kidneys to help maintain the circulating volume
and inducesfurther vasoconstriction.
6. As a result of decreased renal !lood flow and the sympathetic
activity therenin8angiotensin8aldosterone system is activated
further increasing retention
of water and electrolytes with angiotensin 44 acting as a
vasoconstrictor.=. 4f there is overshoot most of the a!ove systems
have a negative feed!ack loop
and stretching of the atria will stimulate release of AF1
causing salt and
water loss via the kidneys.
HOW DOES THIS MANIFEST CLINICALLY
Our hypovolaemic trauma patient will have a num!er of signs and
symptoms as a result of the a!ove. The first
signs will !e as a result of the increase in sympathetic
activity? the patient will have a tachycardia !evasoconstricted
-cool pale peripheries increased capillary refill time slightly
increased perspiration% and the
diastolic !lood pressure may !e elevated -increased S%. They may
have an increased respiratory rate-tachypnoea%. Eventually if
untreated the tachycardia and tachypnoea will increase and as
venous return falls
and the S cannot compensate cardiac output falls the systolic
!lood pressure will decrease. The diastolic
!lood pressure may not !e measura!le. rine output will decrease
due to activation of the renin8angiotensin8aldosterone system
stimulated !y a reduced !lood pressure across the renal capillary
!ed. 1inally consciousness
is impaired as !lood flow to the !rain falls. Fot surprisingly
the key principle in managing these patients isresuscitation of the
circulation to maintain an adeGuate !lood pressure -not necessarily
normal% for organ
perfusion along with haemorrhage control.
HOW IS ALL THIS RELEVANT TO ANAESTHESIA
G%'%"a+ a'a%#%#&aAlmost all anaesthetic drugs have important
actions on the cardiovascular system#
asodilators decreasing !oth preload and afterloadFegatively
inotropic reducing cardiac contractility
Fot surprisingly induction and maintenance of anaesthesia is
usually accompanied !y a fall in the patient2s
!lood pressure? cardiac output falls due to decreased preload
and myocardial contractility and the reducedafterload decreases
systemic vascular resistance. The situation may !e worsened !y the
fact that some drugs
also depress the !aroreceptor refle0 to a varying degree and so
there may not !e a compensatory tachycardia.1inally the
anaesthetics also depress the medulla reducing the sympathetic
response to the fall in !lood
pressure. 1ortunately most healthy adults will tolerate a fall
in !lood pressure of appro0imately '35 and oncesurgery starts this
increases sympathetic activity and !lood pressure is restored. 4f
the !lood pressure remains
low then treatment may !e reGuired. 1rom the information a!ove
we can now formulate a logical method torestore the !lood pressure
and ensure an adeGuate !lood flow to the various organs.
Increase preload.4n an emergency the patient2s legs can !e
elevated to augment venous return and preload.(owever it is more
usual to give a !olus of fluid intravenously $3ml;kg initially and
monitor the response.
4ncreasing preload increases cardiac output and in turn systemic
!lood pressure. emem!er continuing to give
fluid will eventually cause over8stretching of the myocardial
muscles fi!res and reduce the force of contraction
-1ig $.% leading to cardiac failure -although in practice this
is hard to achieve in young fit adults%.
Increase afterload.Once preload has !een addressed then
vasopressor drugs can !e used. These increase thesystemic vascular
resistance !y acting as agonists -stimulating% the alpha adrenergic
receptors -ta!le '%. /rugsthat act in this way include
phenylephrine metaraminol and noradrenaline -norepinephrine%. 9are
must !e taken
as the !aroreceptor refle0 is preserved and profound !radycardia
may occur. Ephedrine has weak alpha and
!eta8$ agonist effects. Adrenaline -epinephrine% is usually only
used if other drugs have !een ineffective or areunavaila!le. 4t is
an agonist at !oth alpha and !eta adrenergic receptors and the
effects are dose8dependant? atlow doses it is predominantly a !eta
-$ N '% agonist and so whilst the increased heart rate and force
of
ATOTW 125. 4ntroduction to 9ardiovascular :hysiology
$,;3);'33< :age 6 of =
-
8/11/2019 125 Introduction to Cardiovascular Physiology
8/8
Sign up to receive ATOTW weekly email
[email protected]
contraction -!eta8$ effect% may improve cardiac output S may
fall due to the!eta8' effects. With increasing doses the alpha
agonist effect dominates
peripherally and S is increased.
Remember# increasin$ SVR alone may increase blood pressure# but
at the expense
of a reduction in stroke "olume and cardiac output%
Increase contractility. 4f myocardial depression with reduced
contractility iscontri!uting to hypotension then it would !e
sensi!le to use a drug with an
inotropic action. /o!utamine has !eta8$ agonist actions
increasing contractilityand heart rate. /opamine the !iological
precursor of noradrenaline has alpha and
!eta8$ agonist actions with the latter predominating at low
doses and !oth effectsat higher doses.
Ta/+% 2.Drugs and their actions at adrenergic receptors/rug
eceptor
Alpha8$ Alpha8' "eta8$ "eta8'
Adrenaline -low dose%
Adrenaline -high dose% Foradrenaline
:henylephrine
Betaraminol Ephedrine
/opamine -low dose% /opamine -high dose%
/o!utamine -%
R%(&!'a+ a'a%#%#&a #3&'a+ !" %3&4,"a+These
techniGues result in vasodilatation -reduced S% proportional to the
height of the !lock. As the local
anaesthetic drug spreads cranially there is an increasing !lock
of the sympathetic nerves leaving the spinal cord-the sympathetic
chain% that supply the vascular !eds. 4f cardiac output is
maintained there will !e a slight fall in
!lood pressure -remem!er ":I9O 0 S%. 4f however the cardiac
output also falls due to reduced preload-failure to maintain an
adeGuate venous return% then !lood pressure will fall
significantly. This may !e
compounded further if the !lock e0tends to reach a!ove the level
of T+ -anaesthesia a!ove the nipple% as thesympathetic supply to
the heart will !e reduced and result in a !radycardia -due to
unopposed parasympathetic
activity% and profound hypotension.
Mild hypotension. >ive intravenous fluid !olus $38'3ml;kg to
maintain preload and cardiac output.Alternatively an alpha agonist
could !e used to counteract the vasodilatation eg phenylephrine or
metaraminol.9are must !e taken if these drugs are used as the
!aroreceptor refle0 is preserved and the increase in !lood
pressure may !e accompanied !y a !radycardia. (owever ephedrine
is often used as the first line drug despite
the fact that its main effects are due to its !eta8$ agonist
action increasing heart rate.
Although theoretically a head8down position will increase venous
return -preload% it may also encourage the
spread of the !lock and cause further vasodilatation. 9are must
!e taken if this techniGue is employed.
Moderate to severe hypotension. This is usually a result of a
high !lock accompanied !y a !radycardia. 4naddition to adeGuate
fluid volume to maintain preload atropine will !e reGuired -3.+mg
iv%. Althoughmetaraminol or phenylephrine will cause
vasoconstriction the pro!lem of a refle0 !radycardia remains.
(ypotension and !radycardia that does not respond to the a!ove
measures should !e treated with small !olusdoses -$3micrograms% of
adrenaline.
CONCLUSION
The key to treating the changes that occur in a patient2s
cardiovascular status as a result of giving them an
anaesthetic is understanding the underlying physiology and how
this has !een distur!ed. This will then allowdistur!ances to !e
treated in the safest and most effective manner with little
potential for harm to the patient.
ATOTW 125. 4ntroduction to 9ardiovascular :hysiology
$,;3);'33< :age = of =