-
8/12/2019 12 collyer s
1/10
-
8/12/2019 12 collyer s
2/10
(eg,7) but it also has strong advocates (eg,4). The lack of
percep-
tual study of the abdomen-ouT directive, in particular,
means
these criticismsare untested.
Swank10(p13) tested the following abdominal-inward
directive:
As you sing the next tones, feel the muscles of the
abdominal
wall contract, with gradual compression, beginning very low
and moving inward and upward gradually. Let the muscleslow in
the abdomen help you lift the airflow upward and out.
Swank10 found that this directive was less effective in
elicit-
ing vocal change on a range of acoustical measures,
including
tone duration and energy in theregion 28003300 Hz associ-
ated with the singers formant.16 Two points arise from this
observation. Firstly, the relationship between acoustical
mea-
sures and listener preferences is highly complex and not yet
fully understood.1719 Thus, the acoustical results reported
by
Swank cannot be assumed to imply a deterioration in vocal
quality. For example, an increase in tone duration can occur
when a singer increases vocal-fold medial compression, but
a voice that sounds pressed would not be considered as
animprovement in classical singing. This means that the percep-
tual implications of the acoustical changes observed by
Swank
are unclear.
Secondly, Swank10 did not measure respiratory behavior. In
an earlier study,20 we investigated the effects on female
classi-
cal singers CWK behavior of abdomen-iN and abdomen-ouT
directives. Our abdomen-iN directive was comparable with
that of Swank10 and asked that the singers steadily pull the
abdominal wall inward for each phrase whilst singing,
whereas
the abdomen-ouT directive asked that the singers steadilyexpand
the abdominal wall during singing. The abdomen-ouT
directive was of interest given the conflicting opinions of
its
appropriateness in singing pedagogy, discussed above. We
found that highly trained singers can alter aspects of their
CWK behavior under directive and can sustain these changes
throughout a song. However, the changes that occurred were
a function of the interaction of the directive and the
singers
habitual (ie, undirected) CWK behavior. Also, the amount
ofchange varied among singers, with some singers showing large
change and some very little change under each directive. Our
results showed that assessment of the influence of any
directive
on vocal quality must take into account how and to what
extent
CWK behavior has actually changed, especially given the wide
differences in singers kinematic strategies that have been
observed.
2123
It seems reasonable to assume that the singersstudied by Swank10
would have shown a similar interactive
effect of habit and directive, but without CWK data the
extent
to which this might have affected the acoustical results
cannot
be determined.
The relationship between CWK behavior under a physiolog-
ically based directive and perception of voice does not appear
to
have been investigated. Abdominal directives have been
studied
for inhalation, withmixed outcomes in terms of effect on
vocal
quality. Thomasson24 found no significant effect for profes-
sional singers on a range of voice source parameters,
including
vertical laryngeal position. Iwarsson,25 however, found a
higher
vertical laryngeal position for speakers in the abdomen-ouT
condition (after controlling for LV), which post hoc
investiga-
tion associated with changes in posture. Again, neither of
the
studies incorporated an audio perceptual component.
Studies of nonphysiologically based directives have found
perceptible changes in vocal quality with changes in
respiratory
behavior. Foulds-Elliott et al26 found that instructing
profes-
sional singers to perform with emotional connection led tohigher
LV at the start of phrases and lower at the end and con-
sequently larger expenditure of air than when merely singing
loudly. They also found that experienced listeners could
distin-
guish audio samples with and without emotional connection,
although interestingly the perceptual cues reported by the
listeners did not include any assessment of changes in
breathing
during phonation.
Another nonphysiological directive often used in pedagogy
is to support thevoice with the breath, considered essential
for the singing voice13 despite the elusiveness of an agreed
def-
inition for the term support. Thorpe et al asked singers to
imagine they were projecting their voices over a large or
small orchestra,27(p100) a directive which the authors
associ-ated with greater and lesser abdominal support,
respectively.
Kinematic patterns were similar in both conditions, but
greater
projection was associated with higher LV at the end of
phrases
and concomitantly smaller expenditure of air. Despite the
asso-
ciation of projection with abdominal activity, they found LV
changes to be mostly because of changes in ribcage
dimension.
Even so, changes in sound level and frequency spectrum char-
acteristics could not be correlated with changes in
respiratory
parameters.
Griffin et al28 (p51) found that the direction to sing with
sup-port elicited no changes in respiratory behavior, despite
noting
that the subjects in this study clearly believe that a
supported
singing voice is.
produced by managing breathing activity
differently. They did, however, find significant changes in
acoustic and laryngeal measures (including peak glottal air-
flow) that implied changes in voice quality. Although they
did
not conduct a perceptual study, strong listener agreement in
as-
sessing the presence and degree of support present in
audiosamples has beenreported by Sand and Sundberg.29
Sonninen et al30 also found laryngeal and acoustic differ-
ences in singers asked to sing with and without support, but
lis-
tener perception was more complex. Although listeners were
generally able to identify supported and unsupported singing
samples, their assessment of the degree of support (0100%)
present in a sample varied widely. Indeed, three of the
sevensingers could not differentiate between supported and
unsup-
ported singing when listening to their own recordings 2
months
after data collection. The authors noted that [t]hese
samples
also caused difficulties to other listeners.30(p231)
Respiratory
behavior was not measured, so the extent of change in the
singers breathing under directive is unknown. Interestingly,
they found no distinction between ratings for voice quality
and for support, suggesting that the terms and concepts were
interchangeable.
In summary, studies of nonphysiologically based directives
have produced mixed results in terms of changes in
respiratory
Journal of Voice, Vol. 25, No. 1, 2011e16
-
8/12/2019 12 collyer s
3/10
behavior and consequent changes in vocal quality. The diffi-
culty with nonphysiologically based directives from a
singing
training perspective is that they lack clear and agreed
definition.
This has led singing teachers to rely on more direct,
physiolog-
ically based instruction, but the perceptible effects of such
in-
structions are unknown.
This study asked classical singing teachers and vocal
coaches
to assess the standard of singing and of breath management
ofsingers performing under three conditions: habitually (ie,
undi-
rected) and under two simple, specific, and dichotomous
abdominal kinematic directives: abdomen-iN and abdomen-
ouT. The audio samples were derived from the companion
study20 that analyzed the type and extent of change in
respira-
tory behavior elicited by the directives. That study found
that
the singers habitual abdominal behavior lay on a continuum
between the extremes elicited by the two directives,
generally
resembling one directive more than the other. Therefore, it
was hypothesized that listeners would be able to detect a
differ-
ence in standard of singing and standard of breath
management
proportionate to the degree of CWK change exhibited by the
singer. It was further hypothesized that listeners would
ratehabitual singing higher than nonhabitual singing and, in
turn,
would rate singing under the abdomen-iN directive higher
than under the abdomen-ouT directive.
METHOD
The study was approved by the Human Ethics Committee of
The University of Sydney. Fourteen singing teachers and
vocal
coaches experienced with classical singing voice assessed
audio samples of five female classical singers under three
breathing conditions. All participants received an
information
sheet and gave written informed consent.
Audio samples
Audio and respiratory recordings were made of five profes-
sional female classical singers: three sopranos (Singers A,
B,
and E), one mezzo-soprano (D), and one contralto (C),
ranging
from 31 to 44 years of age. All singers held postgraduate
qual-
ifications in singing and had between 7 and 20 years of
profes-
sional performing experience. At the time of recording,
Singer
D was in her 19th week of pregnancy but was maintaining her
full performance schedule. Recordings were made at the
audio-
recording laboratory at the Sydney Conservatorium of Music
(The University of Sydney), measuring 4.843 4.553 2.64 m
and hung with sound-absorptive curtains
(http://www.jands.com.au/). Respiratory measurements were made
using respira-
tory inductance plethysmography (Inductotrace; Ambulatory
monitoring system Inc., Ardsley, NY). Audio recordings were
made with a pair of cardioid microphones (Neumann, SKM
140, Georg Neumann GmbH, Berlin) in ORTF (Office de
Radiodiffusion Television Francaise) configuration31 placed
2.75 m from the singer. Sound intensity has been found to
influ-
ence listener assessment of voice.32 Analysis of the audio
recordings20 confirmed that the equivalent sound level
calcu-
lated from long-term average spectra of the last four
phrases
was consistent across breathing condition (F2,8 2.795,
P 0.12), that is, any listener preferences in this study
could
not be attributed to differences in sound level between
perfor-
mances.
Each singer sang two takes of Caccinis Ave Maria in g minor
(unornamented, no repeat) without instruction (Habitual) and
two takes under each of the following directives:
N Abdomen-iN: steadily pull the abdominal wall inwardduring
phonation, using an additional inward pull if re-
quired for additional support and
T Abdomen-ouT: steadily expand the abdominal wall dur-
ing phonation, using an additional outward expansion if
required for additional support.
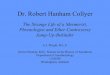
CWK plots of ribcage and abdominal dimensions during the
last four phrases of the song were made for each singer.20
Examples aregivenin Figure1. CWKplots show thecontribution
of abdominal (abscissa) and ribcage (ordinate) dimensional
change to change in LV, with the axes scaled to contribution
capacity (after22). Kinematic traces that run parallel to
the
45 isovolume lines represent a change in
ribcage:abdomenconfiguration but no change in LV. Traces that move
to the left
of an isovolume line represent a net decrease in LV even
where
the ribcage or abdominal dimension might be increasing. The
small cross represents ribcage:abdomen configuration at
end-ex-
piratory level, that is, at the end of expiration in quiet
breathing.
The plots were used to select the three takes (one per
breathing
condition) that showed the greatest variance in kinematic
behav-
ior, and the audio samples from these takes were used for the
per-
ceptual study. That is to say, the audio samples were chosen
according to respiratory behavior not according to the
sound.
Two audio CDs were constructed using the last four phrases
of
the chosen take under each breathing condition (H, N, and
T).
The order of singers was different on each CD, and the order
of
breathing condition was randomized within that. Audio
samples
ofthe firsttwosingerson eachCD (SingersA and B onCD#1 and
E and D on CD#2) were repeated. Odd-numbered listeners heard
CD#1 (Singers A, B, C, A, D, E, B) and even-numbered
listeners
heard CD#2 (Singers E, D, C, B, E,A, D).Repeating two
singerssamples allowed us to assess how consistently listeners
assessed
the same sample on different hearings. Randomizing and using
two CD sets minimized the possibility that results reflected
sam-
ple order rather than inherent vocal quality. Furthermore,
the
threeindividual samples for each singer were preceded by a
com-
posite track that concatenated the threesamples (with a 4-s
pause
between) in the same order. Thus, each CD contained 28
tracks:sevensingers3 fourtracks. Studieshave found
thatlistenerstendto use the first sample heard as a context for
subsequent sam-
ples17,33 and that listeners internal standards of voice
quality
are inherently unstable.34 Playing the concatenated track
first
was designed to have all three samples set the comparative
con-
textand to providea wash-out of theinfluenceof assessment of
a previous singer on a subsequent singer.35
Listener data
The 14 listeners consisted of 11 classical singing teachers,
of
whom six maintained a national and/or international
Sally Collyer, et al Listener Perception of Abdominal Directives
in Singing e17
http://www.jands.com.au/http://www.jands.com.au/http://www.jands.com.au/http://www.jands.com.au/
-
8/12/2019 12 collyer s
4/10
performance schedule, two chorus-masters, one accompanist,
and one singing-voice researcher specializing in classical
voice.
All but one held tertiary qualifications in music, the
exception
being a singing teacher who had retired from performing
after
a career, including leading roles at Covent Garden and the
Met-
ropolitan Opera, and all were employed full-time
professionally
in their respective fields. Hearing was not tested, but all
re-
ported normal hearing and all rely on accurate hearing for
their
professions. Data collection was conducted in quiet rooms
with
only the participant and one researcher present, using a CD
player (Sony Model CFD V8; Sony CFD S300; or Sony CD
Walkman DEJ885 W, Sony Corp., Tokyo) and headphones
(Sennheiser, HD 650, Sennheiser Electronics GmbH, Wede-
mark-Wennebostel, Germany). Listeners first heard the com-
posite track containing all three samples in the same order
in
which they would be presented individually. They then heard
the first sample that they assessed using five visual analog
(VA) scales with gradations numbered 010 from left to right.
The greater resolution of continuous scales has been found
to
improve listener agreement over equal-interval scales by not
forcing a choice between ratings on samples perceived to
fall
between intervals.3537 Listeners were asked to rate the
first
sample by placing a vertical mark and the number 1 above
it on each scale, before moving to the second sample. During
explanation of the task, a dummy completed sheet was used
to illustrate how to complete the form. Sample assessments
on this dummy form included a mix of widely and closely
spaced marks, so as to encourage but not to prescribe that
lis-teners make full use of a scales range. Listeners were not
con-
strained from marking between gradations (eg, at a location
equating to 6.3) or from giving two samples the same score.
The first scale asked, Please assess the standard of singing
for each sample and the second asked, Please assess the
stan-
dard of breath management for each sample. (The three re-
maining scales addressed tone color, vibrato rate, and
vibrato
extent and are not included in this study.) Standard of
singing
was positioned first as Stanley et al38 found judges make an
overall assessment before attending to specific criteria.
Scales
also had the cues poor (underneath 0), average (under
5), and excellent (under 10). Listeners were given as much
time as they wished to assess each sample before hearing thenext
sample, but tracks were not repeated. Fresh sheets were
provided for each set of three samples, and listeners could
not
refer to previous sheets. Data collection generally took
11.5
hours.
The listener criteria standard of singing and breath man-
agement were deliberately general in nature, and no
clarifica-
tion or further explanation of the terms was provided.
Listeners
were invited, but not required, to add comments in the space
provided beneath each scale if they wished to clarify
aspects
of their assessments. Intra- and interjudge reliability in
assess-
ing singers have been found to be higher for general
(overall)
assessmentsthan for specific criteria in singing39 and in
speech
pathology.17 Listeners have also been found to differ as to
whether they assess on performance or intrinsic vocal
quality,39
and it was intended that the term standard of singing should
encompass both aspects. The implicit inclusion in listeners
assessments of factors not relevant to this study, such as
diction
and phrasing, was not considered significant because
compari-
sons were between performances by the same singer.
Listeners were made aware of the purpose of the study and of
the breathing directives that had been given to the singers.
This
ensured that listeners worked from an equal knowledge base
and encouraged them to focus on the breathing behavior of
the singers. They were informed that respiratory
measurements
had been made of the singers but not whether the directives
hadelicited changes in respiratory behavior. Because only five
singers were used, it was anticipated that experienced
listeners
would be likely to recognize a repetition. Therefore,
listeners
were explicitly told that two singers samples would be heard
twice, again to ensure that all listeners worked from an
equal
knowledge base.
Data analysis
The score for each listener criterion for each sample was
mea-
sured by ruler in millimeters and input into a customized
spreadsheet (Excel 2003, Microsoft) that converted the
result
% Abdominal capacity
yticapacegacbiR
%
25 50 75
75
50
25100%LV
0%
LV
Decreasing
LV
Singer A Singer D
Singer B Singer E
Singer C
FIGURE 1. Examples of the changes in CWK behavior elicited
by
abdominal kinematic directive for the five singers. (Thick solid
line
habitual, broken line abdomen-iN, fine solid line
abdomen-ouT;
LV, lung volume.) Construction of the plots is described in
Method:
Audio samples. These plots compare the second-last phrase of
the
first or second take (whichever was used in the perceptual
study; refer
to Method: Audio samples) under the three conditions, showing
the
nature and extent of kinematic change elicited by directive and
under-lying the audio samples. Axes are scaled to percentage of
abdominal
and ribcage capacity.14
Journal of Voice, Vol. 25, No. 1, 2011e18
-
8/12/2019 12 collyer s
5/10
into a percentage. This was checked against a visually esti-
mated score. Comments were also recorded on the spreadsheet.
Statistical analysis usedlinear mixed modelingin SPSS(v14.0
for Windows) (SPSS Inc., Chicago, IL) with repeated
measures.
Model testing for best-fit of covariance structure used the
cor-
rected Akaike Information Criterion40 because of the small
sam-
ple size. A criterion ofP < 0.05 for pairwise comparisons
was
adjusted (Bonferroni) for three multiple comparisons (H vs T,N
vs T, and H vs N), giving a significance criterion ofP <
0.017.
Intralistener (test-retest) repeatability was assessed by
corre-
lation (Pearsons r) and by modeling with singer and
breathing
condition as fixed factors and hearing (first and second) as
the
repeated measure. (Only scores from the second hearing were
used in the other analyses.) The relationship between the
two
listener criteria was similarly tested by correlation and by
mod-
eling, with the score for each criterion as the repeated
measure.
Interlistener consistency for each listener criterion was
assessed
from covariance parameters obtained by a mixed effects
model,
with singer and listeneras random factors and breathing
condi-
tion as a fixed factor.41
Listener scores were analyzed using linear mixed modelingwith
fixed factors of singer and breathing condition. Data
were arranged in the order T-N-H to reflect assumptions that
the abdomen-ouT behavior is the least-favored pedagogically
and that habitual behavior would score higher than the
nonha-
bitual behaviors. For both listener criteria, the scaled
identity
covariance structure was the best fit for both random and
re-
peated effects and singer (but not breathing condition) was
a random factor. Significant interactions were assessed by
pair-
wise comparisons.
RESULTS
CWK patterns
Examples of the CWK patterns of the singers from the audio
samples used in this study are plotted in Figure 1. The
plots
show the second-last phrase drawn from the three takes (one
per breathing condition) used for the perceptualstudy.
Respira-
tory analysis reported in the companion study20 found that
the
directives led the singers to alter the abdominal and ribcage
di-mensions at the start but not at the end of phrases and that
LV
measurements were unchanged.Figure 1illustrates how habit-
ual kinematic strategy changed with directive for each of
the
singers, highlighting similarity and difference between
habitual
and directive patterns. This information allowed the
perceptual
results to take into consideration how much behavioral changewas
actually elicited.
Singer As habitual pattern lay very close to the abdomen-iNend
of the continuum; accordingly, the abdomen-ouT directive
had a major effect on her kinematic behavior, completely re-
moving ribcage paradoxing and disrupting smooth coordination
between abdomen and ribcage. Singer B showed clear differ-
ences between the three conditions: abdominal paradoxing
(ex-
pansion during phonation) under N suggested that she found
the
sharp initial decrease unsustainable but there was no such
dis-
ruption under T, although it is clear that she was resisting
her
habitual tendency for abdominal contraction. Singer C showed
the most striking differences between conditions, with
ribcage
paradoxing under N and abdominal paradoxing under T. By
contrast, Singer D showed the least change across condition,
although adjustments that were characteristic of other
singers
(increased ribcage paradoxing in N, delayed abdominal con-
traction in T) were clear in her kinematic plots. Lastly,
Singer
Es kinematic trace for N generally paralleled her habitual
trace.
In summary, habitual patterns seemed to lie toward the
abdo-men-iN end of the continuum for Singers A, D, and E,
toward
the abdomen-ouT end for Singer B, and midway for Singer C.
Intra- and interlistener consistency
For both listener criteria, test-retest correlations were
moderate
(standard of singing r 0.683,P < 0.001; breath manage-
mentr 0.674,P < 0.001), and there were significant
differ-ences between scores for the first and second hearing.
Model
testing resulted in a scaled identity covariance structure,
with
singer (but not breathing condition) as a random factor. For
standard of singing, main effects of singer (P< 0.001),
breathing condition (P 0.016), and hearing (P< 0.001)
were
all significant, as were interactions of singer3condition(P<
0.001) and singer3hearing (P 0.034). For breath man-
agement, singer was the only significant main effect
(P< 0.001), but interactions of singer3condition (P
0.003)
and singer3hearing (P 0.008) were again significant. The in-
teraction of singer3condition3hearing was not significant
for
either criterion and was removed from the final models.
Pairwise comparisons for the singer3hearing interaction
found that listeners rated standard of singing higher on
second hearing for two of the four singers (Singer D mean
difference12.2, standard error [SE] 2.9, P< 0.001;
Singer E mean difference 6.9, P< 0.001), whereas
listeners
rated the breath management higher on second hearing for
Singer D (mean difference 10.1, SE 3.4, P
-
8/12/2019 12 collyer s
6/10
two scales being vertically aligned on the page, so that the
disparity would have been visible to the listeners.
Criterion scores
Kolmogorov-Smirnov tests were nonsignificant (standard of
singingZ
0.51; breath managementZ
0.39) and visualexamination of residual plots identified no
trends, confirming
normality of residual distribution. Tests of fixed effects
are
set out in Table 1. For both criteria, there was a
significant
main effect for singer (P< 0.001). Pairwise comparisons
found
that the scores for Singers B and E were significantly
higher
than for Singers A, C, and D, and this can be seen in Figure
2.
There was a significant main effect of breathing condition
for
standard of singing (P 0.019) but not for breath manage-
ment (P 0.102). However, the interaction of singer3breath-
ing condition was significant in both criteria (P< 0.001),
that is,
there were significant differences between condition but
only
for some singers.
These differences are broken down in the pairwise compari-
sons for the singer3breathing condition interaction in Table
2
and can also be seen in Figure 2. Pairwise comparisons were
tested at a Bonferroni-adjusted significance of P < 0.17.
For
standard of singing, Singer A scored significantly lower in
the abdomen-ouT condition than in the other conditions,
whereas
Singer D scored higher in the habitual condition than under
eitherdirective. For breath management, Singer A again scoredlower
in the abdomen-ouT condition than in the other conditions.
Singer D again scored higher in the habitual condition than
under
the abdomen-iN directive, but scores under the abdomen-ouT
di-
rective were not significantly lower, as they were for standard
of
singing. Singer B scored higher under the abdomen-ouT direc-
tive than under the abdomen-iN. Her mean score under T was
also higher than for her habitual samples but failed to reach
Bon-
ferroni-adjusted significance (P 0.17). Singer Es habitual
singing was rated more highly than her singing under T for
both criteria but again the differences were not
statistically
significant after adjusting for multiple comparisons.
TABLE 1.
Linear Mixed Modeling of the TwoCriteria Found a Significant
Interaction of Breathing Condition and Singer, That Is, There
Were Significant Differences in Ratings on Both Criteria Between
Breathing Condition but Only for Some Singers
Standard of Singing Standard of Breath Management
Fixed effects
Breathing condition F2,128.9 4.085, P 0.019 F2,128.6 2.327,P
0.102
Singer F4,68.6 22.947,P < 0.001 F4,70.4 15.645,P <
0.001
Condition3singer F8,128.9 4.969, P < 0.001 F2,128.6 3.425,P
0.001
0
20
40
60
80
100
T N H T N H T N H T N H T N H
A B C D E
Singer (by breathing condition)
)001fotuo(erocS
FIGURE 2. Estimatedmarginalmeans and standard errors of listener
scores (out of 100) for standard of singing (solidsquares) and
standard ofbreath management (crosses). Scores are grouped by
singer (AE), then by breathing condition (abdomen-ouT, abdomen-iN,
and habitual). Singers
B and E scored significantly higher than did Singers A, C, and D
on both listener criteria. Scores for the two criteria were highly
correlated, but
listeners rated breath management more critically (lower) than
standard of singing for all singers except Singer C.
Journal of Voice, Vol. 25, No. 1, 2011e20
-
8/12/2019 12 collyer s
7/10
DISCUSSIONBreath management is acknowledged as fundamental to
sing-
ing, but its training relies on the assumption that a
singers
breathing behavior has a direct and proportionate effect on
the singers vocal quality. The corollary, that changes
elicited
by physiologically based CWK directives can be monitored im-
mediately by the singing teachers assessment of vocal
quality,
is especially important because breathing instruction is
becom-
ing increasingly defined in terms of physiology. This
studytested whether the type and degree of change in CWK
pattern
elicited by two simple, specific, and dichotomous abdominal
ki-
nematic directives proportionately matched the assessment
ofstandard of singing and of breath management of female
profes-
sional classical singers, assessed from audio samples by
listeners experienced with the classical singing voice. The
singers sang under three breathing conditions: without
instruc-
tion (habitually), pulling the abdominal wall inward
duringphonation (abdomen-iN), and expanding the abdominal wall
during phonation (abdomen-ouT).
The first hypothesis was that listeners would be able to
detect
a difference in standard of singing and standard of breath
man-
agement proportionate to the degree of CWK change exhibited
by the singer. Key to this was to take into consideration
the
degree of similarity between each directive and the singers
habitual CWK strategy. The results for Singers A and B
wereconsistent with the hypothesis. Singer As habitual pattern
was very similar to her strategy under the abdomen-iN
directive
and both were markedly different from the abdomen-ouT direc-
tive. Likewise, listener ratings found no difference between
her
singing in H and N but found both differed from her singing
un-
der T. Singer Bs CWK pattern differed less between
conditions
than did Singer As, but her habitual pattern tended to be
closer
to T. Likewise, listeners rated her breath management to be
bet-ter in T than N but not different under directive than
habitually.
Although ratings for the standard of singing showed the same
trend, the smaller differences were not statistically
significant
after Bonferroni adjustment for multiple comparisons.
Strictly speaking, Singer Es results could also be
considered
as consistent with the hypothesis. Her habitual pattern more
closely resembled that under the abdomen-iN directive, and
listener scores averaged highest for her habitual singing
and
lowest for her abdomen-ouT singing. However, the differences
between CWK patterns were small and between listeners scores
were not significantly different after Bonferroni
adjustment.
Her results, therefore, do not contradict but also do not
support
the hypothesis.
The results for Singers C and D were not consistent with
thehypothesis. Singer C showed the most change in CWK strategy
under directive, yet there was no significant difference in
listener ratings. Singer D showed the least change in CWK
pat-
tern, yet listeners found the standard of both singing and
breath
management in the nonhabitual conditions to be inferior to
habitual behavior. Thus, the results for Singers A, B, and E
appeared consistent with the hypothesis but the results for
Singers C and D were not.
It was also hypothesized that listeners would rate habitual
singing higher than nonhabitual singing and, in turn, would
rate singing under the abdomen-iN directive higher than
under
the abdomen-ouT directive, following pedagogical opinion
that
abdomen-ouT behavior is deleterious to vocal quality. Again,
the results were mixed. In terms of habitual versus
nonhabitual
breathing, only Singer D scored significantly higher for H
than
under either directive. However, the strong similarity
between
Singer As H and N CWK strategies meant that her
significantly
lower scores under Talso support this hypothesis. Lastly,
Singer
Es results showed higher listener preference for habitual
than
nonhabitual breathing but the differences were not
statistically
significant. Mean ratings for Singers B and C went against
the
hypothesis but again the differences were not statistically
significant.
TABLE 2.
Pairwise Comparisons of the Interaction of Breathing Condition
and Singer
Singer
H vs N H vs T N vs T
Mean Difference, P Mean Difference,P Mean Difference,P
Standard of singing
A 3.2,P 0.326 10.6, P 0.001* 13.8, P < 0.001*
B 5.2, P 0.106 2.5,P 0.437 7.8, P 0.017**C 4.2,P 0.194 4.2,P
0.200 0.1, P 0.988
D 11.6, P 0.001* 9.3, P 0.005* 2.3, P 0.482
E 2.9, P 0.375 7.2, P 0.027** 4.3, P 0.180
Standard of breath management
A 1.9, P 0.629 12.1, P 0.003* 10.1, P 0.011*
B 3.5, P 0.381 6.5, P 0.100 10.0, P 0.012*
C 3.6, P 0.362 3.7, P 0.349 0.1, P 0.981
D 11.6, P 0.004* 6.7, P 0.093 4.9, P 0.219
E 2.6, P 0.509 8.5, P 0.033** 5.9, P 0.138
*Significant at P < 0.17; **Significant without Bonferroni
adjustment for multiple comparisons.
Sally Collyer, et al Listener Perception of Abdominal Directives
in Singing e21
-
8/12/2019 12 collyer s
8/10
In terms of ratings under abdomen-iN being higher than un-
der abdomen-ouT, only Singer As ratings supported this and
only at face value. That is to say, the strong similarity
between
her H and N CWK strategies noted above suggests that the
lower listener rating associated with the abdomen-ouT
directive
might occur with any nonhabitual directive, as was the
case with Singer D. Singer Bs results did not support the
hypothesis, showing a significantly higher listener
preferencefor T than N. Again, habitual CWK strategy needs to be
taken
into consideration, as Singer Bs H pattern was much closer to
T
than to N. Listeners also preferred T to N for Singer D but
not
significantly so.
In summary, we found that the ability of experienced
listeners to detect changes in breathing behavior depended
on
the individual singer and on the extent to which the
directive
deviated from the singers habitual pattern. Furthermore, we
found no support for the pedagogical assertion that the
abdo-
men-ouT directive necessarily results in a perceptibly lower
standard of singing. Rather, our findings suggested that the
stan-
dard of singing was compromised by any directive that
elicited
CWK behavior antithetical to habitual behavior.Our results raise
four issues with respect to the study of
breathing training methods in singing: habitual kinematic
behavior, limitations of body-surface measurement,
participant
pool, and improving reliability in perceptual studies in
singing.
Habitual kinematic behavior
Any assessment of a breathing directive should consider CWK
strategy throughout the entire phrase, not just excursion-only
or
LV measures, and should incorporate in the assessment the
type
and extent of change in CWK strategy elicited by the
directive
in the context of the singers habitual CWK strategy. By
refer-
ring to habitual behavior, the apparently contradictory
results
for Singers A, B, and D were in fact consistent in terms of
any directive eliciting nonhabitual behavior.
Limitations of body-surface measurement
It must be remembered that body-surface measurement has lim-
itations in describing underlying change in respiratory
behav-
ior. This was clearly a factor in the results for Singer D,
whose CWK strategies showed small differences between
breathing conditions, yet were quite audible to experienced
lis-
teners. It is possible that her pregnancy reduced the range of
her
abdominal movement that could be detected by
body-surfacemeasurement, although we are not aware of any studies
into
the effect of pregnancy on CWK behavior in singers, and the
singer was maintaining a full performance schedule. Techno-
logical limitations mean that the relationship between CWK
strategy, muscular activity, and respiratory proprioception
is
poorly understood. Likewise, from the teachers perspective,
the relationship between CWK strategy defined in terms of
con-
tribution to LV change (as used in respiratory research) and
in
terms of dimensional change (as observed in the teaching
studio) needs much clarification before results of CWK
studies
can be applied in the studio.
Participant pool
It could be argued that the highly trained singers in our
study
have already optimized their habitual abdominal behavior. If
so, mean scores for breath management for Singers A, C,
and D (
-
8/12/2019 12 collyer s
9/10
management is in effect a subset of the scale for standard
of
singing. A subscale would suggest a wider range of scores
for
breath management. It would also suggest that a given in-
crease in rating for breath management should lead to
a smaller increase in standard of singing because it repre-
sents only a portion of potential improvement. Although our
re-
sults (Figure 2) did not show these trends, our study was
not
designed to investigate these issues. Another possibility isthat
listeners made an overall assessment that they then justi-
fied, consciously or unconsciously. The greater consistency
of
general criteria as used in our study comes at the cost of
iden-
tifying and ranking the vocal characteristics that are
important
to listeners. Our results suggest that teasing out the
components
of vocal assessment might be complicated by an initial
general
assessment (solicited or unsolicited) providing a contextual
influence similar to the effect on comparing audio samples
discussed above.
CONCLUSION
In summary, our results question pedagogical assumptions
about direct relationships between breathing behavior,
breath-
ing training directives, and perceptible changes in vocal
quality.
There is little examination in research or pedagogy of the
cir-
cumstances under which training approaches fail or are less
successful, despite the value of such information to
understand-
ing and refining methods and practices in any domain.
Although
the enormous variability in habitual CWK behavior in singers
has been well documented in research studies, it is yet to
be
integrated into pedagogical thinking. Our study begins the
im-
portant work of identifying why certain directives work for
some singers and not for others, so that training can be
tailored
and streamlined.
Acknowledgments
The authors are grateful to the participants and to Dr Helen
Mitchell for her advice on data collection. This study was
sup-
ported by an Australian Research Council Discovery Grant
(DP066559) to Professor Dianna T. Kenny and Dr C. William
Thorpe.
REFERENCES1. Blades-Zeller EL. A Spectrum of Voices: Prominent
American Voice
Teachers Discuss the Teaching of Singing. Lanham, MD: Scarecrow;
2003.
2. Chapman JL.Singing and Teaching Singing: A Holistic Approach
to Clas-
sical Voice. San Diego, CA: Plural Publishing; 2006.
3. Duey PA. Bel Canto in Its Golden Age: A Study of Its Teaching
Precepts .New York, NY: Da Capo; 1980.
4. Greene A.The New Voice: How to Sing and Speak Properly .
Milwaukee,
WI: Hal Leonard; 1985.
5. Hemsley T. Singing and Imagination: A Human Approach to a
Great
Musical Tradition. Oxford, UK: Oxford University Press;
1998.
6. Hines J. Great Singers on Great Singing. New York, NY:
Limelight
Editions; 1982.
7. Miller R. The Structure of Singing:Systemand Art in
VocalTechnique. New
York, NY: Schirmer; 1996.
8. Monahan BJ.The Art of Singing: A Compendium of Thoughts on
Singing
Published Between 1777 and 1927. Metuchen, NJ: Scarecrow;
1978.
9. Spillane KW. Breath support directives used by singing
teachers: a Delphi
study.NATS J. 1989;45:921. 57.
10. Swank H. Some verbal directives regarding support concepts
and their
effects upon resultant sung tone. NATS J. 1984;40:1218.
11. Miller R.Solutions for Singers: Tools for Performers and
Teachers. Breath
management. New York, NY: Oxford University Press; 2004. 14.
12. Hixon TJ, Hoffman C. Chest wall shape in singing. In:
Lawrence V, ed.
Transcripts of the Seventh Symposium Care of the Professional
Voice,
1978 June. New York, NY: The Voice Foundation; 1979:910. Part
1.
13. Hixon TJ. Respiratory Function in Singing: A Primer for
Singers and
Singing Teachers. Tucson, AZ: Redington Brown; 2006.
14. Leanderson R, Sundberg J, Von Euler C. Role of diaphragmatic
activity
during singing: a study of transdiaphragmatic pressures. J Appl
Physiol.
1987;62:259270.
15. Sundberg J, Leanderson R, Von Euler C. Voice source effects
of diaphrag-
matic activity in singing.J Appl Physiol. 1986;14:351357.
16. Sundberg J.The Science of the Singing Voice. DeKalb, IL:
Northern Illinois
University Press; 1987.
17. Kreiman J, Gerratt BR, Precoda K, Berke GS. Individual
differences in
voice quality perception.J Speech Hear Res. 1992;35:512520.
18. Ekholm E, Papagiannis GC, Chagnon FP. Relating objective
measurements
to expert evaluation of voice quality in western classical
singing: critical
perceptual parameters.J Voice. 1998;12:182196.
19. Mitchell HF, Kenny DT. The effects of open throat technique
on long term
average spectra (LTAS) of female classical voices. Logoped
Phoniatr
Vocol. 2004;29:99118.
20. Collyer S, Kenny DT, Archer M. The effect of abdominal
kinematic direc-tives on respiratory behavior in female classical
singing.Logoped Phoniatr
Vocol. 2009;34:100110.
21. Collyer S, ThorpeCW,Callaghan J, Davis PJ.The influence
offundamental
frequency and sound pressure level range on breathing patterns
in female
classical singing. J Speech Lang Hear Res. 2008;51:612628.
22. Watson PJ, Hixon TJ. Respiratory kinematics in classical
(opera) singers.
J Speech Hear Res. 1985;28:104122.
23. Watson PJ, Hixon TJ, Stathopoulos ET, Sullivan DR.
Respiratory kinemat-
ics in female classical singers. J Voice. 1990;4:120128.
24. Thomasson M. Belly-in or belly-out? Effects of inhalatory
behavior and
lung volume on voice function in male opera singers. Speech
Transm Lab
Q Status Prog Rep. 2003;45:6174 [Internet]. Available at:
http://www.
speech.kth.se/prod/publications/files/qpsr/2003/2003_45_1_061-074.pdf,
2003.Accessed May 4, 2009.
25. Iwarsson J. Effects of inhalatory abdominal wall movement on
vertical la-ryngeal position during phonation.J Voice.
2001;15:384394.
26. Foulds-Elliott SD, Thorpe CW, Cala SJ, Davis PJ. Respiratory
function in
operatic singing: effects of emotional connection.Logoped
Phoniatr Vocol.
2000;25:151168.
27. Thorpe CW, Cala SJ, Chapman J, Davis PJ. Patterns of breath
support in
projection of the singing voice. J Voice. 2001;15:86104.
28. Griffin B, Woo P, Colton R, Casper J, Brewer D.
Physiological characteris-
tics of the supported singing voice: a preliminary study.J
Voice. 1995;9:45
56.
29. Sand S, Sundberg J. Reliability of the term support in
singing. Logoped
Phoniatr Vocol. 2005;30:5154.
30. Sonninen A, Laukkanen A-M, Karma K, Hurme P. Evaluation of
support in
singing. J Voice. 2005;19:223237.
31. Farina A, Lamberto T. Measurements and reproduction of
spatial sound
characteristics of auditoria. Acoust Sci Tech.
2005;26:193199.
32. Kempster GB, Kistler DJ, Hillenbrand J.
Multidimensionalscaling analysis
of dysphonia in two speaker groups.J Speech Hear Res.
1991;34:534543.
33. Repp B, Crowder RG. Stimulus order effects in vowel
discrimination.
J Acoust Soc Am. 1990;88:20802090.
34. Gerratt BR, Kreiman J, Antonanzas-Barroso N, Berke GS.
Comparing in-
ternal and external standards in voice quality judgments. J
Speech Hear
Res. 1993;36:1420.
35. Shrivastav R, Sapienza CM, Nandur V. Application of
psychometric theory
to the measurement of voice quality using rating scales. J
Speech Lang
Hear Res. 2005;48:323335.
36. Kreiman J, Gerratt BR, Kempster GB, Erman A, Berke GS.
Perceptual
evaluation of voice quality: review, tutorial, and a framework
for future
research.J Speech Hear Res. 1993;36:2140.
Sally Collyer, et al Listener Perception of Abdominal Directives
in Singing e23
http://www.speech.kth.se/prod/publications/files/qpsr/2003/2003_45_1_061-074.pdfhttp://www.speech.kth.se/prod/publications/files/qpsr/2003/2003_45_1_061-074.pdfhttp://www.speech.kth.se/prod/publications/files/qpsr/2003/2003_45_1_061-074.pdfhttp://www.speech.kth.se/prod/publications/files/qpsr/2003/2003_45_1_061-074.pdf
-
8/12/2019 12 collyer s
10/10
37. Kreiman J, Gerratt BR, Ito M. When and why listeners
disagree in voice
quality assessment tasks. J Acoust Soc Am.
2007;122:23542364.
38. Stanley M, Brooker R, Gilbert R. Examiner perceptions of
using criteria in
music performance assessment. Res Stud Music Educ.
2002;18:4656.
39. Wapnick J, Ekholm E. Expert consensus in solo voice
performance evalu-
ation.J Voice. 1997;11:429436.
40. Clifford MH, Tsai CL. Regression and time series model
selection in small
samples. Biometrika. 1989;76:297307.
41. Hakkesteegt MM, Wieringa MH, Brocaar MP, Mulder PGH,
Feenstra L.
The interobserver and test-retest variability of the Dysphonia
Severity In-
dex. Folia Phoniatr Logop. 2008;60:8690.
Journal of Voice, Vol. 25, No. 1, 2011e24