Embed Size (px)
DESCRIPTION
oxygenoterapia
Citation preview

Oxygen therapy during exacerbations of chronic obstructivepulmonary disease
A.G.N. AgustõÂ, M. Carrera, F. Barbe , A. MunÄoz, B. Togores
Oxygen therapy during exacerbations of chronic obstructive pulmonary disease. A.G.N.AgustõÂ, M. Carrera, F. BarbeÂ, A. MunÄoz, B. Togores. #ERS Journals Ltd 1999.ABSTRACT: Venturi masks (VMs) and nasal prongs (NPs) are widely used to treatacute respiratory failure (ARF) in chronic obstructive pulmonary disease (COPD). Inthis study, these devices were compared in terms of their potentiality to worsenrespiratory acidosis and their capacity to maintain adequate (>90%) arterial oxy-genation (Sa,O2) through time (~24 h).
In a randomized cross-over study, 18 consecutive COPD patients who required hos-pitalization because of ARF were studied. After determining baseline arterial bloodgas levels (on room air), patients were randomized to receive oxygen therapy througha VM or NPs at the lowest possible inspiratory oxygen fraction that resulted in aninitial Sa,O2 of $90%. Arterial blood gas levels were measured again 30 min later (onO2), and Sa,O2 recorded using a computer during the subsequent ~24 h. Patients werethen crossed-over to receive O2 therapy by means of the alternative device (NPs orVM), and the same measurements obtained again in the same order.
It was observed that both the VM and NPs improved arterial oxygen tension (p<0.0001) to the same extent (p=NS), without any significant effect upon arterial carbondioxide tension or pH. However, despite this adequate initial oxygenation, Sa,O2 was<90% for 3.7�3.8 h using the VM and for 5.4�5.9 h using NPs (p<0.05). Regressionanalysis showed that the degree of arterial hypoxaemia (p<0.05) and arterial hyper-capnia (p<0.05) present before starting O2 therapy and, particularly, the initial Sa,O2
achieved after initiation of O2 therapy (p<0.0001) enabled the time (in h) that patientswould be poorly oxygenated (Sa,O2 <90%) on follow-up to be predicted.
These findings suggest that, in order to maintain an adequate (>90%) level of ar-terial oxygenation in patients with chronic obstructive pulmonary disease and moder-ate acute respiratory failure: 1) the initial arterial oxygen saturation on oxygen shouldbe maximized whenever possible by increasing the inspiratory oxygen fraction; 2) thisstrategy seems feasible because neither the VM nor NPs worsen respiratory acidosissignificantly; and 3) the Venturi mask (better than nasal prongs) should be recom-mended.Eur Respir J 1999; 14: 934±939.
Servei de Pneumologia and Unidad deApoyo a la InvestigacioÂn (FIS), HospitalUniversitari Son Dureta, Palma de Mal-lorca, Spain.
Correspondence: A.G.N. AgustõÂServei RespiratoriHospital Universitari Son DuretaAndrea Doria 5507014 Palma de MallorcaSpainFax: 349 71175228
Keywords: Acute respiratory failurechronic obstructive pulmonary diseaseemphysemanasal prongsVenturi mask
Received: September 3 1998Accepted after revision July 28 1999
Supported, in part, by ABEMAR
Patients with chronic obstructive pulmonary disease(COPD) often require hospitalization due to acute respira-tory failure (ARF) [1, 2]. The administration of oxygen isa key component of the therapeutic strategy in these cir-cumstances [3, 4]. The aim of O2 therapy in these patientsis to provide adequate arterial (and, presumably, tissue)oxygen saturation (Sa,O2), while other therapeutic mea-sures (bronchodilators, steroids, antibiotics) treat the cau-se(s) of the exacerbation [3, 4].
The most common O2 delivery method in COPD pa-tients hospitalized because of ARF is the standard dual-prong nasal cannula (NPs) [3]. Alternatively, Venturimasks (VMs) can also be used [3]. NPs are less bulky andthere is less chance of their becoming dislodged duringsleep than VMs [5±7]. Therefore, it is conceivable thatNPs can provide a more continuous (i.e. better) Sa,O2 thanthe VM. However, because they do not maintain a con-stant inspired concentration of O2 [5, 6], NPs have thepotential to depress ventilatory drive and worsen respira-tory acidosis [1, 8±10]. In order to reach a compromisebetween these two opposite effects, an Sa,O2 of ~90% is
generally recommended in clinical practice [3, 4]. Todate, however, no studies have assessed the efficacy ofNPs or the VM in maintaining adequate Sa,O2 throughtime in patients with COPD and ARF. Further, previousstatements regarding the potential ventilatory depressanteffects of high inspired concentrations of O2 are derivedfrom studies in which subjects breathed pure O2 [1, 8±10], a situation that is highly unusual in clinical practice.To the authors' knowledge, no previous study has inves-tigated the potential worsening of respiratory acidosisassociated with the use of NPs used under conditions ofstandard clinical management of such patients (i.e. Sa,O2
~90%).This study sought to investigate the optimal mode of O2
administration (NPs versus VM) in COPD patients hospi-talized because of ARF by: 1) comparing their acute effectsupon respiratory acidosis; and 2) assessing their capacity tomaintain an Sa,O2 of >90% over a ~24-h period. The formermay provide information on the safety of use of thesedevices in this particular clinical setting; the latter maybe informative regarding their efficacy in facilitating an
Eur Respir J 1999; 14: 934±939Printed in UK ± all rights reserved
Copyright #ERS Journals Ltd 1999European Respiratory Journal
ISSN 0903-1936

adequate and continuous delivery of O2 to peripheral tis-sues. Because ARF in COPD is a frequent and potentiallylethal situation, this information is of clinical relevance.
Material and methods
Study subjects
Patients with exacerbated COPD who required hospi-talization in our institution were studied. In order to cal-culate sample size, some a priori assumptions were made.Firstly, based upon clinical experience, it was estimatedthat when using the VM patients would not be adequatelyoxygenated (Sa,O2 >90%) for 3�1 h.day-1 (dislodgment ofthe mask, visitors, use of bathroom, etc.). Secondly, it washypothesized that, when using NPs, this period of timewould be reduced to 1�1 h.day-1. Based upon these as-sumptions, and accepting an a error of 0.05, a b error of0.1 and a potential 10% of missing values, it was estimatedthat a sample size of 18 patients would be required.
Accordingly, 18 male COPD patients attending the em-ergency room of the authors' hospital because of ARF(table 1) were included in the study consecutively. Noneof them showed clinical or radiological evidence of bac-terial pneumonia, pneumothorax, pulmonary embolism,pleural effusion or left ventricular failure. Throughout thestudy (48 h), medical treatment was standardized in allpatients and included aerosolized salbutamol (5 mg every6 h) and i.v. prednisolone (40 mg every 8 h) [11]. Nopatient received antibiotics or respiratory stimulants. Allpatients gave their informed consent after being informedof the purpose, characteristics and nature of the study,which had been approved by the Ethics Committee of theinstitution.
Study design
This was a prospective randomized cross-over study. Allpatients were studied in the general ward, within 48 h ofhospital admission.
At 09:00 h, after breathing room air for 30 min, a bloodsample from the nondominant radial artery was obtainedunder local anaesthesia. Arterial oxygen tension (Pa,O2),carbon dioxide tension (Pa,CO2) and pH (baseline values)immediately measured (IL-BG3; Izasa, Barcelona, Spain).Then, patients were randomly allocated to receive O2 ther-apy via either a VM (n=8) or NP (n=10) (Proclinics, Bar-celona, Spain). According to international guidelines [3,4], all of them received the minimum inspiratory oxygenfraction (FI,O2) required to increase the transcutaneousSa,O2 (504-US pulseoxymeter; Criticare Systems, Inc.,Waukesha, WI, USA) to $90% (initial Sa,O2 on O2). FI,O2
ranged 0.24±0.28 for the VM, and gas flow 2±4 L.min-1
for NPs. In order to assess the acute effects of the selectedmode of O2 therapy (VM or NPs) on arterial blood gaslevels, 30 min later a second arterial blood sample wasobtained and analysed as above, and compared to thebaseline values obtained before starting O2 therapy. To in-vestigate the adequacy of arterial oxygenation throughtime, Sa,O2 was monitored continuously during the fol-lowing ~24 h. The analogue output of the oximeter wasdigitized on-line and stored using a computer (Atlantis,Lakeshore Technologies, Inc., Chicago, IL, USA) for lat-er off-line analysis. During this study period, the initialFI,O2 was not modified. After ~24 h, patients were swit-ched to the alternative mode of O2 therapy (VM or NPs)and the same study protocol was repeated. In brief, theminimum FI,O2 required to produce an Sa,O2 of $90%was again used, a third arterial blood sample obtained 30min later and Sa,O2 recorded continuously for a further~24 h. Because one of the main objectives of the studywas to determine the efficiency of O2 therapy in a realclinical setting, the nursing personnel were not instructedto provide supplemental care, other than that regularlygiven in these clinical circumstances.
At discharge, forced spirometry (GS plus, Collins, Bra-intree, MA, USA) was performed [13] and arterial bloodgas levels (breathing room air) measured in all patients.
Analysis
To eliminate obvious technical errors, such as cable dis-connection, the recorded Sa,O2 traces were processed man-ually (off-line) for each individual and for each Sa,O2
recording (using the VM or NPs). From this filtered Sa,O2
trace (~21 h of adequate data for each group, p=NS), thetime spent at an Sa,O2 of <90%, as an index of inadequateoxygenation, was calculated using Pegasus (Lakeshore Te-chnologies, Chicago, IL, USA). Also, to get some insightinto the severity of any abnormal oxygenation period, thetime spent within Sa,O2 intervals of 80±70%, 70±60% and60±50% was calculated. These calculations were perform-ed separately for the whole filtered recording time (~21 h)and for its daytime (09:00±21:00 h) and night-time (21:00±09:00 h) components.
Results are presented as mean�SD. One-way analysis ofvariance (followed by post hoc contrasts (Scheffe)) or atwo-tailed paired t-test were used, as appropriate, to ex-plore the statistical significance of the differences observ-ed. Correlations between variables were explored usingPearson's linear regression analysis. A p-value <0.05 wasconsidered significant.
Table 1. ± Clinical and functional characteristics of thesubjects studied
General dataAge yrs 69.1�10.5BMI kg.m-2 25.6�3.7Smoking pack-yrs 71.4�23.0
Parameters recorded on admissionCardiac frequency beats.min-1 98.1�16.4Respiratory frequency breaths.min-1 31.4�8.8Pa,O2 mmHg 47.7�8.7Pa,CO2 mmHg 50.4�10.1Arterial pH 7.38�0.04
Parameters recorded at dischargePa,O2 mmHg 61.5�9.1Pa,CO2 mmHg 48.3�7.0Arterial pH 7.42�0.03FEV1 L % pred 0.9�0.3 (33)FVC L % pred 1.9�0.5 (54)FEV1/FVC % 48�9
Data are presented as mean�SD. Spirometric reference valueswere from a mediterranean population [11]. BMI: body massindex; Pa,O2: arterial oxygen tension; Pa,CO2: arterial carbondioxide tension; FEV1: forced expiratory volume in one second;FVC: forced vital capacity.
935OXYGEN THERAPY IN COPD

Results
Clinical data
In the emergency room, all subjects had ARF as definedby the presence of severe hypoxaemia while breathingroom air (Pa,O2 6.34�1.16 kPa (47.7�8.7 mmHg)). Mostbut not all patients had hypercapnia (Pa,CO2 6.70�1.34kPa (50.4�10.1 mmHg)) (table 1). None of the variablesshown in table 1 were significantly different betweenthose patients who used the VM or those who used NPsfirst. At discharge, all patients had severe airflow obstruc-tion (forced expiratory volume in one second 33.4�10.3%of the predicted value).
Acute effects of the Venturi mask and nasal prongs uponarterial blood gas levels
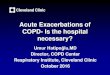
Figure 1 shows the Pa,O2, Pa,CO2 and pH values det-ermined in each individual once admitted to the authors'ward while breathing room air (baseline values), andwhen receiving O2 therapy via the VM or NPs. At base-line, most patients had moderate respiratory failure (Pa,O2
6.89�1.13 kPa (51.8�8.5 mmHg)) with mild hypercarbia(Pa,CO2 6.85�1.34 kPa (51.5�10.1 mmHg)) and normalarterial pH (7.42�0.03). Pa,O2 increased to the same ex-tent (p=NS) using the VM (9.56�1.02 kPa (71.9�7.7mmHg), p<0.0001) and NPs (9.08�1.85 kPa (68.3�13.9mmHg), p<0.0001) (fig. 1). Neither Pa,CO2 (VM, 6.90�1.45 kPa (51.9�10.9 mmHg), p=NS; NPs, 7.04�1.41 kPa(52.9�10.6 mmHg), p=NS) nor arterial pH (VM, 7.39�0.05, p=NS; NPs, 7.40�0.04, p=NS) were significantlymodified by either mode of O2 therapy; this was true evenin the subgroup of patients with higher Pa,CO2 whilebreathing room air.
Efficiency of the Venturi mask and nasal prongs in adequat-ely providing continuous arterial oxygenation
By design, the initial Sa,O2 achieved on O2 was $90% inall subjects, both using the VM (92.9�2.6%) and NPs(94.3�2.9%, p=NS). However, despite this adequate level ofinitial oxygenation, it was observed that patients subse-
quently had an Sa,O2 value <90% for 3.7�3.8 h using theVM, and 5.4�5.9 h using NPs (p<0.05). On average, thiscorresponded to ~20% of the (filtered) recording time. Inextreme cases, however, patients could be poorly oxygen-ated for as long as 15 h (~75% of (filtered) recording time)(fig. 2). Differences between daytime and night-timeintervals were not statistically significant (fig. 2).
To analyse the severity (rather than the duration) of thispoor oxygenation pattern, the times spent below otherthreshold Sa,O2 were determined. It was found that Sa,O2
was within the 80±70% interval for 80�109 min, within the70±60% interval for 38�61 min and within the 60±50%interval for 4�9 min. As shown by the SDs, however, in-tersubject variability was considerable. Within each ofthese Sa,O2 intervals, differences between devices (VM ver-sus NPs) were not statistically significant.
Factors influencing the adequacy of arterial oxygenationduring acute respiratory failure in chronic obstructive pul-monary disease
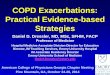
Figure 3 shows that the amount of time that any givenpatient spent at <90% Sa,O2 when using the VM washighly related to that spent by the same patient at <90%Sa,O2 when using NPs (r=0.91, p<0.0001). This suggeststhat some factor (by and large independent of the type ofdevice but dependent on the patient) strongly influencedthe time that each individual was poorly oxygenated;nonetheless, figure 3 also shows that most points lie ab-ove the line of identity, suggesting that, for a given indi-vidual, NPs tend to provide poorer control of Sa,O2 overtime than the VM. To explore what patient characteristicmight influence the adequacy of arterial oxygenation dur-ing ARF, the relationship between the time spent at <90%Sa,O2 and several variables of potential clinical interest(age, body mass index, degree of airflow obstruction, ini-tial Sa,O2 on O2 and arterial blood gas levels at baselineand during O2 therapy) were analysed. As shown in figure4, it was found that the degree of arterial hypoxaemia (fig.4a) and arterial hypercapnia (fig. 4b) present at baseline(i.e. before O2 therapy had been started) and, particularly,the initial Sa,O2 achieved at the beginning of O2 therapy(fig. 4c) were highly predictive of the duration of pooroxygenation.
80
70
60
50
40
30
Pa,C
O2
mm
Hg
b)
Roomair
VM NPs
120
100
80
60
40
20
Pa,O
2 m
mH
g
a)
Roomair
VM NPs
7.50
7.45
7.40
7.35
7.30
7.25Room
airVM NPs
Arte
rial
pH
c)
#
#
Fig. 1. ± Individual and mean (horizontal bars): a) arterial oxygen tension (Pa,O2); b) arterial carbon dioxide tension (Pa,CO2); and c) arterial pH in allpatients studied while breathing room air and while receiving oxygen through a Venturi mask (VM) and nasal prongs (NPs). Both the VM and NPs pro-duced similar increments in Pa,O2, but neither modified Pa,CO2 or arterial pH significantly. #: p<0.0001 versus room air.
936 A.G.N. AGUSTõÂ ET AL.

Discussion
The most relevant findings of the present study werethat, in COPD patients hospitalized because of ARF: 1) theadministration of O2 therapy via a VM or NPs did notworsen respiratory acidosis (fig. 1); 2) most patients were
inadequately oxygenated (Sa,O2 <90%) for a significantproportion of the day (~20% of the time analysed), al-though in extreme cases this period of time may be muchhigher (~75%) (fig. 2); 3) although these observationsappear to be more prominent when NPs are used (fig. 2),by and large they are independent of the type of deviceused (fig. 3); and 4) the severity of arterial hypoxaemiaand hypercapnia present before starting O2 therapy and,especially, the Initial Sa,O2 on O2 can predict the durationof inadequate arterial oxygenation (fig. 4).
Previous studies
The main goal of O2 therapy in patients with COPD andARF is to facilitate adequate and continuous arterial oxy-genation, whereas other measures treat the cause of theexacerbation [1, 2]. However, when high FI,O2 are used,ventilatory drive can be blunted and respiratory acidosisworsened [8±10, 14]. In order to reach a compromisebetween these two opposite phenomena, current guide-lines recommend the use of the minimum inspired FI,O2
necessary to obtain an initial Sa,O2 on O2 of ~90% [3, 4].However, no previous study has assessed the adequacy ofsuch initial Sa,O2 in maintaining an appropriate (>90%)level of arterial oxygenation through time, or whether thetwo most common devices used in the clinical setting(VM and NPs) can achieve comparable results. Further,previous investigations assessing the effects of a highFI,O2 investigated patients with stable COPD [5, 14] orundergoing mechanical ventilation [8] or have given pureO2 to breathe to the participant subjects [9, 10], but nonehas studied COPD patients with ARF.
Interpretation of results
The present results show that, under the conditions ofregular clinical use in patients with COPD hospitalizedbecause of ARF, both the VM and NPs are able to initiallyoxygenate arterial blood adequately without significantlyworsening the pre-existing degree of respiratory acidosis(fig. 1). However, neither of them is able to guarantee anSa,O2 of >90% through time in the majority of patients(fig. 2). Several potential explanations should be con-sidered for this latter observation. Technical recordingartefacts can be ruled out because the Sa,O2 trace wasmanually filtered in order to eliminate them. Dislodge-ment of the device was unlikely because the tight corr-elation observed between the time with an Sa,O2 <90%using the VM and NP (fig. 3) suggests that the mechan-ism(s) underlying this observation is, by and large, in-dependent of the device and probably dependent on thepatients themselves. As shown in figure 4, the degree ofabnormal gas exchange before starting O2 therapy and,more importantly, the initial Sa,O2 on O2 were able topredict the amount of time that the patient would be poor-ly oxygenated. From this latter observation, the authorswould suggest that, in clinical practice and in order tominimize the duration of poor oxygenation, the initialSa,O2 should be maximized by increasing the FI,O2 (par-ticularly in patients with marked gas exchange abnorm-alities). The authors consider this strategy feasible sinceO2 therapy does not appear to significantly worsen res-piratory acidosis, even in patients with marked arterialhypercapnia (fig. 1).
0 2 4 6 8 10 12 14 16 18Time with Sa,O2 <90% using the VM h
02468
1012141618
Tim
e w
ith S
a,O
2 <9
0% u
sing
NPs
h
Fig. 3. ± Relationship between the time spent with an arterial oxygensaturation (Sa,O2) of <90% in each patient while using the Venturi mask(VM) and nasal prongs (NPs). - - - : line of identity. There is a very sig-nificant linear relationship (r=0.91, p<0.0001), and most patients lieabove the line of identity, indicating that, for each individual, NPs pro-vide poorer control of Sa,O2 with time than does the VM.
Night-timeDaytime
Tim
e w
ith S
a,O
2 <9
0% h
a)Ti
me
with
Sa,
O2
<90%
h
b)
10
8
6
4
2
0
10
8
6
4
2
0
Fig. 2. ± Time that each patient spent with an arterial oxygen saturation(Sa,O2) of <90%, during the daytime and night-time periods, while usinga) the Venturi mask; and b) nasal prongs. Horizontal bars represent meanvalues. For further explanation, see text.
937OXYGEN THERAPY IN COPD

The Venturi mask versus nasal prongs
Despite the frequent occurrence of ARF in patients withCOPD, and the relevance of O2 therapy in these cir-cumstances [1, 2, 15, 16], there have been no detailedstudies comparing the potential benefits and risks of thetwo most common methods of O2 administration (the VMand NPs) in these patients. In the present study, twoobservations suggest that NPs provide worse control ofarterial oxygenation through time than the VM. Firstly, thetime spent with an Sa,O2 <90% was longer using NPs (5.4�5.9 h) than using the VM (3.7�3.8 h, p<0.05). Secondly,when this variable was directly compared in each patientusing both devices (fig. 3), most points lay above the id-entity line. These results, therefore, support the use of theVM rather than of NPs, in patients with COPD hos-pitalized because of ARF. This observation is interpretedas reflecting, on the one hand, the variation in FI,O2 thatoccurs when NPs are used [17] and, on the other, thecapacity of the VM to provide adequate O2 therapy evenin patients who are mouth breathers.
Potential limitations
Several potential limitations of the present study deservecomment. Firstly, at baseline (fig. 1), the patients were notacidotic and the degree of hypercarbia was modest inapproximately half of them. Therefore, the observationsshould not be directly extrapolated to patients with moresevere degrees of respiratory acidosis. However, it isinteresting to note that, even in those patients with veryhigh Pa,CO2 (fig. 1), no obvious deleterious effects of NPsor the VM could be detected. Secondly, the study was notdesigned to assess the potential clinical consequences ofthe inadequate arterial oxygenation seen in most of thepatients. Therefore, further studies are needed to inves-tigate whether or not the maintenance of a higher Sa,O2
during hospitalization would result in a better clinicaloutcome by enhancing recovery (improved oxygenationof respiratory muscles and other tissues?) and/or mini-mizing potential complications (less cardiac arrhythmi-as?). Thirdly, in clinical practice, FI,O2 is normally variedaccording to Sa,O2 changes. It is well known that the latter
can change for a wide variety of reasons (use of bron-chodilators, altered cardiac output, disease state, etc.).However, it is important to realize that, for the purposesof this study, the FI,O2 was set at the start of the study andleft unchanged throughout, and that both groups receivedthe same standardized medical therapy. Finally, it wasdeliberately decided not to provide extra nursing attentionto the patients during the course of the study in order toavoid any interference with their spontaneous use of theVM or NPs in a real clinical setting. Of course, the resultsmay have been altered had the study been carried outdifferently.
Conclusions
The present study shows that many patients with chronicobstructive pulmonary disease hospitalized because ofmoderate acute respiratory failure are poorly oxygenatedfor significant periods of time. In order to avoid this, it wassuggested that: 1) arterial oxygen saturation is maximizedat the beginning of treatment by increasing the inspiratoryoxygen fraction; this appears to be feasible since neitherthe VM nor NPs worsen respiratory acidosis in these pa-tients; and 2) the Venturi mask is used whenever possible.Overall, these results provide evidence on the basis ofwhich oxygen therapy can be prescribed in patients withchronic obstructive pulmonary disease hospitalized be-cause of acute respiratory failure.
Acknowledgements. The authors thank the te-chnical staff of the Gabinet de Funcio Pulmonarof the Servei de Pneumologia (Hospital Univer-sitari Son Dureta, Palma de Mallorca, Spain) fortheir help during the studies.
References
1. Derenne JPh, Fleury B, Pariente R. Acute respiratory fail-ure of chronic obstructive pulmonary disease. Am RevRespir Dis 1988; 138: 1006±1033.
0
5
10
15
20
30 40 50 60 70
Tim
e w
ith S
a,O
2 <9
0% h
a)
30 40 50 60 70 80 90 92 94 96 98 100
b) c)
Pa,O2 mmHg Pa,CO2 mmHg Sa,O2 %
Fig. 4. ± Relationship between the duration of poor oxygenation (arterial oxygen saturation (Sa,O2) <90%) and: a) oxygen tension (Pa,O2) (r= -0.51,p<0.05); and b) carbon dioxide tension (Pa,CO2) (r=0.51, p<0.05) measured at baseline while breathing room air (before beginning the study); and c)the initial Sa,O2 on O2 (r=0.66, p<0.0001) using the Venturi mask (s) and nasal prongs (*). For further explanations, see text.
938 A.G.N. AGUSTõÂ ET AL.

2. Schmidt GA, Hall JB. Acute on chronic respiratory fail-ure: assessment and management of patients with COPDin the emergent setting. JAMA 1989; 261: 3444±3453.
3. Celli B, Snider GL, Heffner J, et al. Standards for thediagnosis and care of patients with chronic obstructivepulmonary disease. Official statement of the AmericanThoracic Society. Am J Respir Crit Care Med 1995; 152:S77±S120.
4. Siafakas NM, Vermeire P, Pride NB, et al. Optimal ass-essment and management of chronic obstructive pulmon-ary disease (COPID). European Respiratory Society con-sensus statement. Eur Respir J 1995; 8: 1398±1420.
5. Costello RW, Liston R, McNicholas WT. Compliance atnight with low flow oxygen therapy: a comparison ofnasal cannulae and Venturi face masks. Thorax 1995; 50:405±406.
6. Ooi R, Joshi P, Soni N. An evaluation of oxygen deliveryusing nasal prongs. Anaesthesia 1992; 47: 591±593.
7. Nolan KM, Winyard JA, Goldhill DR. Comparison of nas-al cannulae with face mask for oxygen administration topostoperative patients. Br J Anaesth 1993; 70: 440±442.
8. Dunn WF, Nelson SB, Hubmayr RD. Oxygen-inducedhypercarbia in obstructive pulmonary disease. Am RevRespir Dis 1991; 144: 526±530.
9. Aubier M, Murciano D, Milic-Emili J, et al. Effects of theadministration of O2 on ventilation and blood gases inpatients with chronic obstructive pulmonary disease dur-ing acute respiratory failure. Am Rev Respir Dis 1980;122: 747±754.
10. Aubier M, Murciano D, Fournier M, Milic-Emili J,Pariente R, Derenne JPh. Central respiratory drive inacute respiratory failure of patients with chronic ob-structive pulmonary disease. Am Rev Respir Dis 1980;122: 191±200.
11. Roca J, Sanchis J, AgustõÂ -Vidal A, et al. Spirometricreference values for a mediterranean population. Bull EurPhysiopathol Respir 1986; 22: 217±224.
12. Barbe F, Togores B, Rubõ M, Pons S, Maimo A, AgustõÂAGN. Noninvasive ventilatory support does not facilitaterecovery from acute respiratory failure in chronic obstruc-tive pulmonary disease. Eur Respir J 1996; 9: 1240±1245.
13. American Thoracic Society Official Statement. Standard-ization of Spirometry. 1994 Update. Am J Respir CritCare Med 1995; 152: 1107±1136.
14. Sassoon CSH, Hassell KT, Mahutte CK. Hyperoxic-in-duced hypercarbia in stable chronic obstructive pulmon-ary disease. Am Rev Respir Dis 1987; 135: 907±911.
15. Campbell EJM. The J. Burns Amberson lecture. Themanagement of acute respiratory failure in chronic bron-chitis and emphysema. Am Rev Respir Dis 1967; 196:626±639.
16. Mithoefer JC, Karetzky MS, Mead GD. Oxygen ther-apy in respiratory failure. N Engl J Med 1967; 277: 947±949.
17. Bazuaye EA, Stone TN, Corris PA, Gibson GI. Variabilityof inspired oxygen concentration with nasal cannulas.Thorax 1992; 47: 609±611.
939OXYGEN THERAPY IN COPD