Embed Size (px)
Citation preview

EUROPEAN JOURNAL OF INFLAMMATION
1721-727 (2007)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties115
MICROBIOLOGICAL ASPECTS AND INFLAMMATORY RESPONSE OF PULP TISSUE IN TRAUMATIC DENTAL LESIONS
D. TRIPODI, M. LATROFA and S. D’ERCOLE1
Department of Stomatology and Oral Science, University of Chieti-Pescara, 1Laboratory of Clinical Microbiology, Department of Biomedical Sciences, University of Chieti-Pescara, Chieti, Italy
Received June 4, 2007 - Accepted August 3, 2007
Mailing address: Dr. Domenico Tripodi,Dipartimento di Scienze Odontostomatologiche, Università “G. d’Annunzio” Chieti- Pescara,Via dei Vestini, 31 - Chieti, ItalyTel: ++39 0871 3554063 Fax: ++39 0871 3554063e-mail: [email protected]
REVIEW ARTICLE
Traumatic dental lesions are found at all ages, but most frequently in the paediatric population, in an age range of 2–5 years, a time period in which the muscle co-ordination and mental faculties of the child have still not been fully developed (1-2).
At the age of 5, 1/3 of children have already suffered trauma of the deciduous teeth with fractures of the corona (26%), radicular fractures (3%), intrusive luxation (26%), non-intrusive luxation (13%), evulsions (52–69%), concussions (10%), dislocation, especially of the upper incisors (84% of the deciduous against 87% of the permanent teeth), possible bud alteration in permanent teeth (48–68%), and ankylosis (5%) (3-4). On the other hand, in children between the ages of 8–12 years, due to their high physical activity during games (58.5%) and sports, there is an increase in the incidence of trauma. In fact, at 12 years of age, 25% of the pediatric population show some damage to their permanent teeth.(1-4). 18% of dental fractures, as has been observed in many studies, is represented by fractures to the corona of the permanent incisors
(the majority, 80%, are of the upper central incisors), and especially those (9.6%) which do not show complications of trauma to the hard dental tissue (5-7). Studies on germ-free animals have shown that healing of the pulp occurs independently of the grade of exposure of the same
Pulp exposure induces major morphological changes in tooth tissue, such as discolouring, acute pulp inflammation, chronic inflammation and, if the exposed pulp in not treated, necrosis. This happens even in the case of dental intrusion, since the pulp tissue, during displacement, undergoes a severe shock, which might be seen at a later stage, with clinical indications that go from colour alteration, to inflammation and subsequently to pulp necrosis (8). Following exposure, the pulp suffers from haemorrhage in the underlying tissue followed by a secondary superficial inflammation, the start of coagulation mechanisms and afterwards the alteration of the tissues in a detrimental (abscesses and necrosis) or proliferate (hyperplasia) manner (9).During histological examination of deciduous
Vol. 5, no. 3, 0-0 (2007)
Traumatic dental lesions are more frequently found in the pediatric population, with a major involve-ment, in 80% of the cases, of the superior central incisors. The exposure of the dental pulp leads to major morphological changes in dental tissue, such as discolouring, acute pulp inflammation, chronic inflam-mation and necrosis. This article reviews the various studies published on the different types of inflam-matory response of the pulp tissue following traumatic events, from the microbiological and histological point of view of various techniques.
Key words: dental trauma, pulp inflammation, bacteria

116 117Eur. J. Inflamm.
teeth having post-traumatic discolouration, with or without the presence of abscesses, both clinically and through radiographs or pain and mobility, it has been seen that these teeth show histological changes which go from total pulp necrosis to dystrophic calcification, with a partial necrosis associated to inflammation (10).
Evaluating the pulp reaction to the traumatic event through an optic microscope, it has been seen that the inflammation decreased, starting from the pulp chamber at the third apical and medial of the root canal in which the following changes were noticed: haemorrhage, damage to the odontoblast strata and the presence of inflammatory infiltration, made up mainly polymorphonucleate leukocytes (11-15).
From the histological examination of animal teeth having pulp exposure at 48 h and 72 h, it was seen that in both periods of observation there was an area of superficial inflammation, with an accumulation of polimorphonucleate leucocytes in the pulp cornua and in the third coronal, that the depth of the inflammation is greater at 48 h (4633.33 μm) than at 72 h (3933.33 μm), maybe coinciding with a major chamber opening, (x1332.14 μm a 48 h vs. x 479.52 μm a 72 h), that the strata of odontoblasts near the exposed pulp results as being completely destroyed or reduced to a small number of cells, that the amount of inflammatory infiltration reduces towards the apex, and that the periradicular area results free from inflammatory cells (16-17).
Inflammation results as being inferior in teeth where the exposure of the pulp occurred exclusively following a traumatic event in respect to those where the trauma followed an insurgence of a carious process (11).
Pulp necrosis with an inflammatory cell infiltration has also been seen in teeth having radicular fractures and vertical fractures, in the first case mostly in the coronal part of the fracture, since the more apical one is filled by collagen fibre, while in the second case only on one side of the pulp due to the presence of a plasma cell barrier between the portions of necrotic pulp and inflamed pulp (18). In agreement with previous studies, Caliskan et. al. obtained the same results in teeth with complex radicular coronal fractures where the radicular pulp tissue resulted normal, having dilated and functioning blood vessels
(19-22).Disintegration of the pulp tissue may give rise to
inflammation of the periapical tissue which could induce problems in the development of the permanent tooth’s gem, as well as determining ankylosis of the deciduous tooth, in the case of parodontal damage and, consequently, delay in the ectopic eruption of the following permanent tooth (23).
Some authors have observed, in teeth having fractured enamel and dentine and without any pulp exposure, during the first post traumatic stages (17 h), the presence of myelinic degeneration, surrounding the axis, and of oedema, while in subsequent stages (4-20 days) tissue inflammation, neuron degeneration, intramyelinic oedema, axial tumescence and an aberrant synthesis of the myelin were observed (24).
From the histological examination of the dental nerve fibres subgroup which contain the calcitonin gene related peptide (CGRP), it was possible to evaluate the progressive evolution stages of the pulp abscess and of the necrosis in relation to the proliferation of the same fibre, in the interface between the abscess and the viable pulp, in the periapical area during the lesion and around the chronic abscesses in granulomatosis parodontal tissue (25).
By classifying dental damage into 3 different stages it has been seen that for slight damage, 4 days after trauma, CGRP fibres proliferated on the odontoblast and dentine strata, returning to normality after 3 weeks. At an intermediate level of damage, there was damage on the odontobalst strata, with the formation of micro abscesses and a proliferation of CGRP around the abscess, with a consequent formation of repairing dentine and a successive healing. As regards severe damage with an exposure of the pulp there was a pulp necrosis followed by a probable development of periapical lesions (26).
CGRP-IR fibres which are immunoreactive (IR) towards the peptide relative calcitonin gene, innervate the coronal dentine in sites populated by primary odontoblasts and by associated pulp cells. In the case of dental trauma such cells are lost, in this way reducing the innervating CGRP-IR and provoking changes in dimension, form, and immunoreaction of their root endings in relation to
D. TRIPODI ET AL.

116 117Eur. J. Inflamm.
the different patterns of inflammation and healing
(27-28). Vascular changes which occur in the pulp,
following an acute pulpitis condition, consist in an increase of vascular permeability which affects first the rete vasculosum and afterwards the capillaries, while in the case of chronic pulpitis numerous morphological changes have been noticed, with a formation of tissue similar to granuloma in the rete vasculosum around the abscess (29). The nerve fibres have an important effect on the pulp blood flow and on inflammation, while cytochemical changes which are seen following dental damage occur in response to the alterations which take place in the pulp itself or are an indication of the pulp status (30).
There are two key components in an inflammatory process: microcirculation and sensory nerve activity. According to literature, the excitation of the A-delta fibre seems to have an insignificant effect on the pulp blood flow (PBF), the activation of the C fibre provokes an augmentation caused by the action of neuro-quinine. On the other hand, the increase of pulp blood flow (PBF) provokes the excitation of A-delta and C fibres and the increase of tissue pressure (31-34).
Various authors have reported that light damage gives rise to changes in the pain receptor circuit and increases the possibility of the neurotrophic system, derived from the brain, contributing to the persistent pain even after dental therapy. In fact, the kinase tyrosine receptor B (TrkB) seems to be present at a high percentage (54%) of the isolechital neurons B4+ following tooth damage, suggesting a presence in the ascending pain receptors (35).
From histological studies conducted on TrkB reactivity and the connection with the B4 isolechtin, it was seen that the TrkB receptors are present in 36.6% of the trigeminal ganglion neurons and that this percentage decreases during the first 48 h and then increases up to 41% after 7 days from the dental damage.
In the case of chronic inflammation, an irreversible destruction of the parenchymal tissue has been noticed, and the restructuring with connective and fibrous tissue of the resulting defect, as well as the activation of the cell-mediated bacterial lysase with the activation of the T and B cells and of the cytokine system (36-37)
Periapical inflammation occurs as a consequence of pulp inflammation following trauma, carious process or iatrogenic damage, and such inflammation stimulates the formation of granulomae and cysts with consequent bone inflammation. The inflammatory response consists of an initial vasodilatation, an increase of the vascular permeability, infiltration of leucocytes regulated by endogenic mediators such as neuropeptide quinine, migration of polimorphonuclear leucocytes and monocytes, cytokines.(Interleukin-1 prostaglandin-l) (38). Binomial bacterial pulp-infection inflammation has been widely demonstrated (39-40).
A coronal fracture exposes a great number of dental tubules: the main path towards the pulp of a wide variety of dangerous agents present in the oral cavity, including bacteria and bacterial products. Invasion might be followed by pulpitis, necrosis, infection of the radicular canal and periapical lesions. Of the approximately 500 different types of bacteria present in the oral cavity, only a small and select group manages to invade the dental tubules. The one mostly found is Streptococcus spp., thanks to the capability of recognising the components of the dental tubules, such as type I collagen, which stimulates bacterial adhesion and intra-tubular growth.The environment also stimulates the growth of anaerobae, such as Eubacterium spp., Propionibacterium spp., Bifidobacterium spp., Peptostreptococcus micros and Veillonella spp. Gram-negative bacillus, for example Porphyromonas spp., have been less frequently found (41).
In teeth where the viable pulp is functional, dentine has a considerable resistance towards bacterial infiltration and inflammatory changes are transient. Dental pulp defends itself by using a “passive” mechanism made up of an increase in the flow of dentinal fluid, which removes the bacteria through hydrostatic pressure, and with an active mechanism. This latter consists of the pulp’s capacity, through the blood flow, of developing an immediate inflammatory response which removes stimuli, bacterial toxins or bacteria. Alterations in these mechanisms, for example in the case of concurrent displacement which alters the pulp’s circulation, or the teeth’s age, with a consequent reduction of the healing potential, changes the prognosis of the fractured tooth (42). The dental

118 119Eur. J. Inflamm.
pulp therefore possesses a high capacity of healing in relation to any type of insult, be it trauma or a carious process, producing a pulp reaction initially localised and reversible, thanks to the capacity of the dentine-pulp group of processing the bacterial elements. The younger and more healthy the pulp, the higher its capacity for healing.
REFERENCES
1. Al-Majed I., J.J. Murray and A. Maguire. 2000. Prevalence of dental trauma in 5-6 and 12-14 year-old boys in Riyadh, Saudi Arabia. Dent. Traumatol. 17:153.
2. Bradford I. 2002. Dental Emergencies presenting to a dental teaching hospital due to complications from traumatic dental injuries. Al-Jundi Dental Trauma 18:181.
3. Andreasen J.O. and F.M. Andreasen. 1994. Classification, etiology and epidemiology of traumatic dental injuries. In Textbook and color atlas of traumatic injuries to the teeth, 3d ed. J.O. Andreasen, F.M. Andreasen, eds. Munksgaard, Copenhagen, p.151.
4. McTigue D.J. 2000. Diagnosis and management of dental injuries in children. Pediatr. Clin. North Am. 47:1067.
5. Pugliesi D.M., R.F. Cunha, A.C. Delbem and M.L. Sudenfeld. 2004. Influence of type of dental trauma on the pulp vitality and the time elapsed until treatment: a study in patients aged 0-3 years. Dent. Traumatol. 20:139.
6. Sandalli N., S. Cildir and N. Guler. 2005. Clinical investigation of traumatic injuries in Yeditepe University, Turkey during the last 3 years. Dent. Traumatol. 21:188.
7. Jank S., B.S. Maurer-Stockinger, R. Emshoff, G. Rothler, H. Strobl and E. Waldhart. 2001. Long-term outcome of dentoalveolar trauma in relation to post-traumatic instability. Mund Kiefer Gesichtschir. 5:348.
8. Diab M. and H.E. elBradway. 2000. Intrusion injuries of primary incisors. Part II: Sequelae affecting the intruded primary incisors. Quintessence Int.31:335.
9. Cvek M. 1994. Endodontic management of
traumatized teeth. In Texbook and color atlas of traumatic injuries to the teeth, 3rd edn. J.O. Andreasen, F.M. Andreasen, ed. Munksgaard-DKK, Copenhagen, p.517.
10. Soxman J.A., M.M. Nazif and J. Bouquot. 1984. Pulpal pathology in relation to discoloration of primary anterior teeth. ASDC J. Dent. Child.51:282.
11. Raslan N. and W.E. Wetzel. 2006. Exposed human pulp caused by trauma and /or caries in primary dentition: a histological evaluation. Dent. Traumatol. 22:145.
12. Caliskan M.K., F. Oztop and G. Caliskan. 2003. Histological evaluation of teeth with hyperplastic pulpitis caused by trauma or caries: case reports. Int. Endod. J. 36:64.
13. Nishimura Y., Y. Miura, M. Maeda, H. Hayashi, M. Dong, H. Katsuyama, M. Tomita, F. Hyodoh, M. Kusaka, A. Uesaka, K. Kuribayashi, K. Fukuoka, T. Nakano, T. Kishimoto and T. Otsuki. 2006. Expression of the T cell receptor Vβ repertoire in a human T cell resistant to asbestos-induced apoptosis and peripheral blood T cells from patients with silica and asbestos-related diseases. Int. J. Immunopathol. Pharmacol. 19:795.
14. Manoury B., S. Caulet-Maugendre, I. Guénon, V. Lagente and E. Boichot. 2006. TIMP-1 is a key factor of fibrogenic response to bleomycin in mouse lung. Int. J. Immunopathol. Pharmacol. 19:471.
15. Castellani M.L., V. Salini, S. Frydas, J. Donelan, M. Tagen, B. Madhappan, C. Petrarca, K. Falasca, G. Neri, S. Tete’ and J. Vecchiet. 2006. The proinflammatory interleukin-21 elicits anti-tumor response and mediates autoimmunity. Int. J. Immunopathol. Pharmacol. 19:247.
16. Croll T.P., E.A. Pascon and K. Langeland. 1987. Traumatically injured primary incisors: a clinical and histological study. ASDC J. Dent. Child. 54:401.
17. Harran-Ponce E., R. Holland, A. Barreiro-Lois, A.M. Lopez-Beceiro and J.L. Pereira Espinel. 2002. Consequences of coronal fractures with pulpal exposure: histopathological evaluation in dogs. Dent. Traumatol. 18:196.
18. Jin H., H.F. Thomas and J. Chen. 1996. Wound healing and revascularization: a histologic observation of experimental tooth root fracture. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod.
D. TRIPODI ET AL.

118 119Eur. J. Inflamm.
81:26.19. Caliskan M.K. and F. Sepetcioglu. 1993. Partial
pulpotomy in coronal-fractured permanent incisor with hyperplastic pulpitis: a case report. Endod. Dent. Traumatol. 9:171.
20. Lang S., A. Picu, T. Hofmann, M. Andratschke, B. Mack, A. Moosmann, O. Gires, S. Tiwari and R. Zeidler. 2006. Cox-inhibitors relieve the immunosuppressive effect of tumor cells and improve functions of immune effectors. Int. J. Immunopathol. Pharmacol. 19:409.
21. Trubiani O., G. Orsini, S. Caputi and A. Piattelli. 2006. Adult mesenchymal stem cells in dental research: a new approach for tissue engineering. Int J Immunopathol Pharmacol.19:451.
22. Vena G.A., N. Cassano, G. Alessandrini, D. Fai, M. Gabellone, P. Ligori, C. Malvindi, A. Mancino, S. Pellè, F. Rinaldi and M.R. Sodo. 2007. Treatment of mild to moderate plaque psoriasis with calcitriol ointment applied with or without a dosing device. Eur. J. Inflamm. 5:89.
23. Loesche W.J. 1998. Dental infections. In Infectious diseases, 2d ed. S.L. Gorbach, J.G. Bartlett, N.R. Blacklow, eds. Saunders, Philadelphia, p.499.
24. Ozcelik B., T. Kuraner, B. Kendir and F. Asan. 2000. Histopathological evaluation of the dental pulps in coronal-fractured teeth. J. Endod. 26:271.
25. Byers M.R., P.E. Taylor, B.G. Khayat and C.L. Kimberly. 1990. Effects of injury and inflammation on pulpal and periapical nerves. J. Endod. 16:78.
26. Byers M.R., H. Suzuki and T. Maeda. 2003. Dental neuroplasticity, neuro-pulpal interactions, and nerve regeneration. Microsc. Res. Tech. 60:503.
27. Byers M.R. 1992. Effects of inflammation on dental sensory nerves and vice versa. Proc. Finn. Dent. Soc. 88(S):499.
28. Woodnutt D.A., J. Wager-Miller, P.C. O’Neill, M. Bothwell and M.R. Byers. 2000 Neurotrophin receptors and nerve growth factor are differentially expressed in adjacent non-neuronal cells of normal and injured tooth pulp. Cell Tissue Res. 299:225.
29. Takahashi K. 1990. Changes in the pulpal vasculature during inflammation. J. Endo. 16:92.
30. Kim S. 1990. Neurovascular interactions in the dental pulp in health and inflammation. J. Endod. 16:48.
31. Wakisaka S. 1990. Neuropeptides in the dental pulp:
distribution, origins, and correlation. J. Endod. 16:67.32. Schiavino D., E. Nucera, C. Alonzi, A. Buonomo,
E. Pollastrini, C. Roncallo, T. De Pasquale, C. Lombardo, G. La Torre, V. Sabato, V. Pecora and G. Patriarca. 2006. A clinical trial of oral hyposensitization in systemic allergy to nickel. Int. J. Immunopathol. Pharmacol.19:593.
33. Ferrini A.M., V. Mannoni, P. Aureli, G. Salvatore, E. Piccirilli, T. Ceddia, E. Pontieri, R. Sessa and B. Oliva. 2006. Melaleuca alternifolia essential oil possesses potent anti-staphylococcal activity extended to strains resistant to antibiotics. Int. J. Immunopathol. Pharmacol. 19:539.
34. Cadoni S., M. Ruffelli, S. Fusari and O. de Pità. 2007. Oral allergic syndrome and recombinant allergens rBet v 1 and rBet v 2. Eur. J. Inflamm. 5:21.
35. Behnia A., L. Zhang, M. Charles and M.S. Gold. 2003. Changes in TrkB-like immunoreactivity in rat trigeminal ganglion after tooth injury. J. Endod. 29:135.
36. Herrera D., S. Roldan and M. Sanz. 2000. The periodontal abscess: a review. J. Clin. Periodontol. 27:377.
37. Trummel C.L. and A. Behnia. 2002. Periodontal and pulpal infections. In Oral and maxillofacial infections 4th ed. R.G. Topazian, M.H. Goldberg .J.R. Hupp, eds. Saunders, Philadelphia, p.126.
38. Stashenko P., R. Teles and R. D’Souza. 1998. Periapical inflammatory responses and their modulation. Crit. Rev. Oral Biol. Med. 9:498.
39. Robertson A., F.M. Andreasen, J.O. Andreasen and J.G. Noren. 2000. Long term prognosis of coronal-fractured permanet incisors. The effect of stage of root development and associated luxation injury. Int. J. Paediatric Dentistry 10:191.
40. K. Lakota, K. Mrak-Poljšak, B. Rozman, T. Kveder, M. Tomšič and S. Sodin-Semrl. 2007. Serum amyloid A activation of inflammatory and adhesion molecules in human coronary artery and umbilical vein endothelial cells. Eur. J. Inflamm. 5:73.
41. Love R.M. and H.F. Jenkinson. 2002. Invasion of dentinal tubules by oral bacteria. Crit. Rev. Oral Biol. Med. 13:171.
42. Olsburgh S. and I. Krejci. 2003. Pulp response to traumatic coronal fractures. Endodontic Topics 5:26.

EUROPEAN JOURNAL OF INFLAMMATION Vol. 5, no. 3, 0-0 (2007)
1721-727 (2007)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties121
ANTI-INFLAMMATORY CYTOKINES IN PERI-IMPLANT SOFT TISSUES: A PRELIMINARY STUDY ON HUMANS USING cDNA MICROARRAY TECHNOLOGY
F. BAMBINI, M. PELLECCHIA, L. MEMÈ, A SANTARELLI, M. EMANUELLI1, M. PROCACCINI and L. LO MUZIO2
Institute of Dental Sciences, University of Ancona; 1Istituto di Biotecnologie Biochimiche, University of Ancona, Ancona; 2Department of Surgical Sciences, University of Foggia, Foggia, Italy
Received January 2, 2007 - Accepted September 11, 2007
The mucosa around implants and the gingiva around teeth respond to plaque formation with the development of an inflammatory lesion which has similar magnitude and histological features. Different cell types in inflamed and healthy periodontal and peri-implant tissues are capable of producing a variety of important pro-inflammatory and anti-inflammatory cytokines and growth factors which mediate the host response. The aim of this study is to compare the expression levels of anti-inflammatory cytokines detectable in the peri-implant soft tissue of two single-implant crowns supported either by zirconia or titanium abutments. Two frozen samples of peri-implant soft tissue of two single-implant crowns supported either by zirconia or titanium abutments were treated to obtain mRNA. The mRNA extracted from these specimens was converted in cDNA and analyzed with “SuperArray GEArray Q Series Human Inflammatory Cytokine/Receptor Gene Array kit”, planned for studying 96 genes involved in inflammatory response. Data showed that gene expression levels of anti-inflammatory cytokines were higher in specimens sampled from the zirconia abutment compared with those from the titanium abutment. It was considered important to detect the mRNA levels of the anti-inflammatory mediators in healthy peri-implant tissues to verify the biological tolerability of zirconia compared with titanium abutments. The difference detected in cytokine expression could be due to the intrinsic biological tolerability of zirconia ceramics or to a lesser bacterial accumulation.
Mailing address:Prof. Lorenzo Lo Muzio,Via Carelli 28, 71100 Foggia, ItalyTel/Fax: ++39 0881 685809e-mail: [email protected]
Key words: zirconia, titanium, cDNA microarray, peri-implant soft tissue
Several clinical studies show a predictable high clinical success rate for implant supported oral rehabilitation (1-2). A biologic width has been demonstrated to be present around dental implants as well as around teeth and the successful barrier mechanism established at the transmucosal passage of the implant is probably critical to its long-term stability and function (3-5).
The mucosa around implants and the gingiva around teeth respond to plaque formation with the development of an inflammatory lesion which
has similar magnitude and histological features (6). Different cell types in inflamed and healthy periodontal and peri-implant tissues are capable of producing a variety of important pro-inflammatory and anti-inflammatory cytokines and growth factors which mediate the host response. Interleukin-1 β (IL-1 β) is able to activate osteoclast cells and consequently is considered one of the most important agents responsible for periodontal bone destruction at sites of periodontal inflammation (7-8). IL-6 activates B-lymphocyte differentiation, T-lymphocyte

122 123Eur. J. Inflamm.
proliferation and induces bone resorption (9). TNF-α, produced by monocytes/macrophages, stimulates fibroblasts to produce collagenase and induces bone resorption (9). IL-4 suppresses the production of proinflammatory cytokines, including IL-1 and TNF-α (9). The biological activity of IL-10 consists in the suppression of proinflammatory cytokines as IL-2, IFN-gamma, TNF, produced by Th-1 cells (10). Interleukin 13, secreted predominantly by activated T(H)2 cells, presents consistent anti-inflammatory properties in inhibiting TNF-α and IL-1β (11). Transforming Growth Factor β-1, a multipotent regulator of bone cell metabolism, has a strong immunosuppressive activity downregulating the transcription of several metalloproteinases, IL-1 and TNF-alfa (12-13).
The aim of this study is to compare the expression levels of anti-inflammatory cytokines detectable in the peri-implant soft tissue of two single-implant crowns supported either by zirconia or titanium abutments.
MATERIALS AND METHODS
Subject selectionA 39-years-old male attending the Institute of Dental
Sciences, University of Ancona, Italy, for his annual post-treatment check-up was included in this study. The patient gave informed consent to participate in the research and fulfilled the following inclusion criteria: a) medical history revealed no contraindication to implant therapy, b) no use of antibiotics in the previous six months, c) good oral hygiene standard, d) presence of implant screws inserted by the same operator at the same time e) presence of two single tooth implant supported restoration, one cemented to zirconia abutment, one to a titanium abutment, loaded at least for 12 months, f) absence of symptoms of peri-implantitis according to the success criteria proposed by Albrektsson and coworkers (17). Two implants were taken into consideration to detect the anti-inflammatory cytokines mRNA levels in peri-implant soft tissue.
SamplingAfter surgical excision of the supracrestal soft tissue
specimens around the lingual portion of the implant neck, the two samples were snap-frozen in liquid nitrogen, and stored at –80 °C until use.
RNA extraction An aliquot of the frozen tissue (20-40 mg) was
homogenized in lysis buffer, and the total RNA was then
extracted with a RNA isolation kit ( Promega, Madison, WI). RNA samples were tested by ultraviolet absorption at 260 nm in order to determine the concentration. The quality and concentration of the RNA samples were further confirmed by electrophoresis on denaturated 1% agarose gels.
Synthesis of cDNA ProbesTotal RNA was used as a template for biotinylated
probe synthesis using the Ampolabeling-LPR kit (SuperArray Bioscience Corporation, Frederick, MD). A 1-1.5 μg of total RNA was annealed with GEAprimer Mix in a final volume of 10 μl in a thermal cycler at 70°C for 3 min. It was then cooled to 37°C, and kept at that temperature for 10 min before adding 10 μl of RT Cocktail (pre-warmed to 37°C). The RT Cocktail contains a specific RT buffer, RNase Inhibitor and MMLV reverse transcriptase (Promega, Madison, WI). The reaction was incubated at 37°C for 25 min, heated at 85°C for 5 min, and kept on ice until the following LPR step. For each array, 30 μl of the LPR Cocktail (DNA polymerase, pathway specific primers, labeling buffer, and Biotin-16-dUTP) were added to each RT reaction. For LPR, the thermal cycler was programmed as follows: 85°C, 5 min; 30 cycles of (85°C, 1 min; 50°C, 1 min; 72°C, 1 min); then 72°C, 5 min. The reaction was stopped by specific solutions offered by SuperArray Bioscience Corporation. The resulting cDNA probe was ready to be used for hybridization.
Microarray hybridization and Chemiluminescent Detection
After cDNA synthesis and Biotin d-UTP labeling, the probes were hybridized with GEArray Q Series Human Inflammatory Cytokines & Receptors Gene Array HS-015 membranes, obtained from SuperArray Bioscience Corporation (Frederick, MD). The nylon arrays, containing cDNA fragments from 96 cytokine and receptor genes were designed to profile the expression of key genes associated with inflammatory response (for a complete list of genes see www.superarray.com). The genes were grouped into six categories according to their functional and structural features. Procedure followed the manufacturer’s recommendation with minor modifications.
GEArray membrane was pre-hybridized with GEAhyb Hybridization Solution (SuperArray Bioscience Corporation, Frederick, MD) containing denatured sheared salmon sperm DNA (100 μg of DNA /ml; Invitrogen, Carlsbad, CA) at 60°C for 2 h, and hybridized in the Hybridization Solution (SuperArray Bioscience Corporation, Frederick, MD) containing cDNA probe of the samples at 60°C overnight. After washing the
F. BAMBINI ET AL.

122 123Eur. J. Inflamm.
membrane twice with wash solution 1 and 2 for 15 min each at 60°C, the membrane was blocked in GEAblocking solution and incubated in the binding buffer containing alkaline phosphatase–conjugated streptavidin (1:7500) for 10 min at room temperature. After the washing and rinsing steps, the membrane was incubated with chemiluminescent substrate and exposed to X-ray film.
Microarray data analysisAnalysis of the arrays was performed by using
Scanalyze software (developed by Dr. Michael Eisen), which converts the image of tetra-spots into numerical data. All raw signal intensities were corrected for background (GEArray Analyzer software) by subtracting the signal intensity of a negative control. Intensities which were 1.3-fold as high as the background were defined as detectable signals. Normalization was performed to the housekeeping gene GAPDH, and normalized signals were used to identify gene expression profiles from both specimens, collected around zirconium and titanium abutments, respectively.
RESULTS
Cytokine expression in peri-implant soft tissue is reported in Fig. 1 A-B. Only differences in mRNA levels of at least 1-fold between the two samples were considered as significant. Data shows that gene expression levels of anti-inflammatory cytokines were higher in specimen samples from zirconia abutment compared with those from the titanium abutment. For example, experimental data showed that IL-10 expression level was three times superior, and TGFβ-1 two times higher around zirconia abutment in comparison with the titanium abutment. In gingival tissue around zirconia the expression level of CCL21 was 4-fold higher compared to those of titanium. The mRNA of IL-13R (IL-13 receptor) was evident only in the zirconia specimen.
DISCUSSION
Periodontal disease results from the interaction of the host defensive mechanism with the plaque bacteria. As for the periodontium, destruction of peri-implant tissues is due to an abnormal immune response against plaque microorganisms (14).
Cytokines, released by different host cells exposed to components of periodontal pathogenic bacteria are responsible for a wide spectrum of inflammatory,
metabolic and immunomodulatory properties (15).Pro-inflammatory cytokines are able to induce
and conserve an inflammatory and osteolytic process in the periodontium and in the peri-implant tissues (16-19).
In this study, gene expression level of anti-inflammatory cytokines in the peri-implant soft tissue was examined around zirconia and titanium abutments supporting two successful implant-supported single crowns in the same patient and inserted by the same operator at the same time.
The results showed that levels of anti-inflammatory cytokine expression was considerably higher around the zirconia abutment than around the titanium abutment examined. In particular, experimental data showed that IL-10 expression level was 3-fold higher, and TGFβ-1 2-fold higher around the zirconia abutment in comparison with the titanium abutment.
Interleukin 10 is an anti-inflammatory cytokine produced by T-helper 2 cells, macrophages and B cells which inhibits synthesis of pro-inflammatory cytokines by activated T Helper 1 clones (10-20). Transforming Growth Factor β-1, in addition to regulating bone physiology, develops a prominent immunosuppressive activity inhibiting the expression of chemokine receptors (21) and the synthesis of several metalloproteinases, IL-1 and TNF-alfa (12-22).
The cys–cys (C–C) chemokine ligand 21 (CCL21)/secondary lymphoid-tissue chemokine is expressed on the high endothelial venules and lymphatic vessels of lymph nodes and Peyer’s patches (23). In a recent study Kuroshima et al (2004) suggest that gingival lymphatic endothelium has the ability to produce CCL21, and that the CCL21 induction predominantly occurs in peripheral lymphatic endothelium in the mucosal microcirculation system under uninflamed conditions (24). Our findings show that in gingival tissue around zirconia the expression level of CCL21 was 4-fold higher compared to those of titanium. Consistent with the hypothesis that in inflamed gingival tissue the activation of inflammatory enzymes like cathepsin D, a proteolytic enzyme that has been detected in human gingival tissue with periodontitis (25), may reduce the CCL21 on lymphatic endothelium, and that TNF-α and IL-1β reduce the CCL21 expression

124 125Eur. J. Inflamm.
in vitro (26). In peri-implant tissue the expression of CCL21 could be a sign of healthiness.
Interleukin-13 is a potent anti-inflammatory cytokine that inhibits the production of several pro-inflammatory cytokines and chemokines and induces B cell proliferation and differentiation (27).
Although levels of IL-13 were not detectable either in samples from the zirconia abutment or from
titanium, the mRNA of its receptor was evident only in the zirconia specimen.
Studies have suggested that the polarization of the local immune response, basically by T helper cells, may determine the stability or progression of the periodontal disease (28-29). The polarized immune response may exhibit a Th1 pattern consisting of a predominantly pro-inflammatory cellular response, or
Fig. 1. The figure summarizes the expression profile of 96 genes associated with inflammatory response. The specimens were collected around zirconium (black bar) and titanium (gray bar) abutments. Only results for genes whose expression was detectable are shown; no bar is shown for instances when gene expression was undetectable. The gene symbol is reported on the x-axis, and its expression is shown as normalized intensity. Genes were arranged in two groups: genes with a normalized intensity ≥ 0.1 (A), and genes with a normalized intensity < 0.1 (B).
F. BAMBINI ET AL.
A
B

124 125Eur. J. Inflamm.
a Th2 pattern, with anti-inflammatory characteristics and a predominantly humoral immune response. However, the development of a predominantly Th2 response was related to chronic periodontitis, while a Th1 response was thought to be involved in aggressive periodontitis (30). Considering these recent findings, it is difficult to interpret some of our results. Indeed, our data show that in both samples it was possible to detect chemokines and receptors linked to both Th1 and Th2 immune response. Moreover, our model is linked to healthy peri-implant tissue and not to periodontal disease. However, as expression of IL-8 is found in healthy periodontal tissues and is related to a low subclinic inflammatory state (31-32), perhaps also in peri-implant soft tissue an extremely low subclinic inflammatory state linked to different molecules could be present.
It was considered important to detect the mRNA levels of the anti-inflammatory mediators in healthy peri-implant tissues to verify the biological tolerability of zirconia compared with titanium abutments. Zirconia ceramic is a new ceramic material recently used to fabricate machinable implant abutments (33). This ceramic material was originally made of partially stabilized zirconia (zirconia oxide) mixed with a small amount of alumina and silicon dioxide. In agreement with the study published by Schierano et al. in which the pro-/anti-inflammatory cytokine levels were measured around titanium abutments (34), the findings of this study indicate no inflammatory response in the soft tissues of the implant analysed one year after loading. The results of this study suggest a successful implant osseointegration (35). However, the expression of examined anti-inflammatory cytokines was higher around the zirconia abutment in comparison with the titanium abutment. This difference in cytokine expression could be due to the intrinsic biological tolerability of zirconia ceramics. Besides showing favorable mechanical properties, in particular a flexural strength higher than alumina ceramic (36), zirconia ceramic is in fact tissue compatible and chemically stable without signs of degradation during 12 months of subcutaneous implantation(37).
Another structural property that can explain the obtained results consists in the very low bacterial colonization potential of the zirconia abutment. Several studies document that partially stabilized
zirconia surfaces accumulate fewer bacteria than titanium surfaces (38-39). The reduced bacterial adhesion on zirconia abutments could prevent the appearance of an inflammatory lesion and the development of the peri-implant osteolytic process that characterizes peri-implantitis.
According to the sample size examined, the zirconia implant abutment seems to be more biologically compatible with the peri-implant soft tissues than the titanium abutment. Further research is necessary to validate the results of this study .
REFERENCES
1. Adell R., U. Lekholm, B. Rockler and P.I. Branemark. 1981. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int. J. Oral Surg. 10:387.
2. Adell R., B. Eriksson, U. Lekholm, P.I. Branemark and T. Jemt. 1990. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. Int. J. Oral Maxillofac. Implants 5:347.
3. McKinney R.V. Jr., D.E. Steflik and D.L. Koth. 1988. The epithelium dental implant interface. J. Oral Implantol. 13:622.
4. Berglundh T., J. Lindhe, I. Ericsson, C.P. Marinello, B. Liljenberg and P. Thomsen. 1991. The soft tissue barrier at implants and teeth. Clin. Oral Implants Res 2:81.
5. Apse P., G.A. Zarb, A. Schmitt and D.W. Lewis. 1991. The longitudinal effectiveness of osseointegrated dental implants. The Toronto Study: peri-implant mucosal response. Int. J. Periodontics Restorative Dent. 11:94.
6. Berglundh T., J. Lindhe, C. Marinello, I. Ericsson and B. Liljenberg. 1992. Soft tissue reaction to de novo plaque formation on implants and teeth. An experimental study in the dog. Clin. Oral Implants Res. 3:1.
7. Nguyen L., F.E. Dewhirst, P.V. Hauschka and P. Stashenko. 1991. Interleukin-1 beta stimulates bone resorption and inhibits bone formation in vivo. Lymphokine Cytokine Res. 10:15.
8. Rasmussen L., L. Hanstrom and U.H. Lerner. 2000. Characterization of bone resorbing activity

126 127Eur. J. Inflamm.
in gingival crevicular fluid from patients with periodontitis. J. Clin. Periodontol. 27:41.
9. Hirano T., S. Akira, T. Taga and T. Kishimoto. 1990. Biological and clinical aspects of interleukin 6. Immunol. Today 11:443.
10. Mosmann T.R. 1994. Properties and functions of interleukin-10. Adv. Immunol. 56:1.
11. Harris S.G., J. Padilla, L. Koumas, D. Ray and R.P. Phipps. 2002. Prostaglandins as modulators of immunity. Trends Immunol. 23:144.
12. Page R.C. 1992. Host response tests for diagnosing periodontal diseases. J. Periodontol. 63:356.
13. Musso T., I. Espinoza-Delgado, K. Pulkki, G.L. Gusella, D.L. Longo and L. Varesio. 1992. IL-2 induces IL-6 production in human monocytes. J. Immunol. 148:795.
14. Seymour G.J., E. Gemmell, L.J. Lenz, P. Henry, R. Bower and K. Yamazaki. 1989. Immunohistologic analysis of the inflammatory infiltrates associated with osseointegrated implants. Int. J. Oral Maxillofac. Implants 4:191.
15. Page R.C. 1991. The role of inflammatory mediators in the pathogenesis of periodontal disease. J. Periodontal Res. 26:230.
16. Meikle M.C., J.K. Heath and J.J. Reynolds. 1986. Advances in understanding cell interactions in tissue resorption. Relevance to the pathogenesis of periodontal diseases and a new hypothesis. J. Oral Pathol. 15:239.
17. Kao R.T., D.A. Curtis, D.W. Richards and J. Preble. 1995. Increased interleukin-1 beta in the crevicular fluid of diseased implants. Int. J. Oral Maxillofac. Implants 10:696.
18. Shimpuku H., Y. Nosaka, T. Kawamura, Y. Tachi, M. Shinohara and K. Ohura. 2003. Genetic polymorphisms of the interleukin-1 gene and early marginal bone loss around endosseous dental implants. Clin. Oral Implants Res. 14:423.
19. Santos M.C., M.I. Campos, A.P. Souza, P.C. Trevilatto and S.R. Line. 2004. Analysis of MMP-1 and MMP-9 promoter polymorphisms in early osseointegrated implant failure. Int. J. Oral Maxillofac. Implants 19:38.
20. Fiorentino D.F., M.W. Bond and T.R. Mosmann. 1989. Two types of mouse T helper cell. IV. Th2 clones secrete a factor that inhibits cytokine
production by Th1 clones. J. Exp. Med. 170:2081.21. Sallusto F., A. Lanzavecchia and C.R. Mackay.
1998. Chemokines and chemokine receptors in T-cell priming and Th1/Th2-mediated responses. Immunol. Today 19:568.
22. Musso T., I. Espinoza-Delgado, K. Pulkki, G.L. Gusella, D.L. Longo and L. Varesio. 1990. Transforming growth factor beta downregulates interleukin-1 (IL-1)-induced IL-6 production by human monocytes. Blood 76:2466.
23. Gunn M.D., K. Tangemann, C. Tam, J.G. Cyster, S.D. Rosen and L.T. Williams. 1998. A chemokine expressed in lymphoid high endothelial venules promotes the adhesion and chemotaxis of naive T lymphocytes. Proc. Natl. Acad. Sci. USA 95:258.
24. Kuroshima S., Y. Sawa, Y. Yamaoka, K. Notani, S. Yoshida and N. Inoue. 2004. Expression of cys-cys chemokine ligand 21 on human gingival lymphatic vessels. Tissue Cell 36:121.
25. Trabandt A., U. Muller-Ladner, J. Kriegsmann, R.E. Gay and S. Gay. 1995. Expression of proteolytic cathepsins B, D, and L in periodontal gingival fibroblasts and tissues. Lab. Invest. 73:205.
26. Kriehuber E., S. Breiteneder-Geleff, M. Groeger, A. Soleiman, S.F. Schoppmann, G. Stingl, D. Kerjaschki and D. Maurer. 2001. Isolation and characterization of dermal lymphatic and blood endothelial cells reveal stable and functionally specialized cell lineages. J. Exp. Med. 194:797.
27. de Vries J.E. 1998. The role of IL-13 and its receptor in allergy and inflammatory responses. J. Allergy Clin. Immunol. 102:165.
28. Seymour G.J. and E. Gemmell. 2001. Cytokines in periodontal disease: where to from here? Acta Odontol. Scand. 59:167.
29. Yamamoto M., K. Fujihashi, T. Hiroi, J.R. McGhee, T.E. Van Dyke and H. Kiyono. 1997. Molecular and cellular mechanisms for periodontal diseases: role of Th1 and Th2 type cytokines in induction of mucosal inflammation. J. Periodontal Res. 32:115.
30. Garlet G.P., W. Martins Jr., B.R. Ferreira, C.M. Milanezi and J.S. Silva. 2003. Patterns of chemokines and chemokine receptors expression in different forms of human periodontal disease. J. Periodontal Res. 38:210.
F. BAMBINI ET AL.

126 127Eur. J. Inflamm.
31. Mathur A., B. Michalowicz, M. Castillo and D. Aeppli. 1996. Interleukin-1 alpha, interleukin-8 and interferon-alpha levels in gingival crevicular fluid. J. Periodontal Res. 31:489.
32. Payne J.B., R.A. Reinhardt, M.P. Masada, L.M. DuBois and A.C. Allison. 1993. Gingival crevicular fluid IL-8: correlation with local IL-1 beta levels and patient estrogen status. J. Periodontal Res. 28:451.
33. Sadoun M. and S. Perelmuter. 1997. Alumina-zirconia machinable abutments for implant-supported single-tooth anterior crowns. Pract. Periodontics Aesthet. Dent. 9:1047.
34. Schierano G., G. Bellone, E. Cassarino, M. Pagano, G. Preti and G. Emanuelli. 2003. Transforming growth factor-beta and interleukin 10 in oral implant sites in humans. J. Dent. Res. 82:428.
35. Schierano G., F. Bassi, G. Gassino, K. Mareschi, G. Bellone and G. Preti. 2000. Cytokine production and
bone remodeling in patients wearing overdentures on oral implants. J. Dent. Res. 79:1675.
36. Chong K.H., J. Chai, Y. Takahashi and W. Wozniak. 2002. Flexural strength of In-Ceram alumina and In-Ceram zirconia core materials. Int. J. Prosthodont. 15:183.
37. Ichikawa Y., Y. Akagawa, H. Nikai and H. Tsuru. 1992. Tissue compatibility and stability of a new zirconia ceramic in vivo. J. Prosthet. Dent. 68:322.
38. Rimondini L., L. Cerroni, A. Carrassi and P. Torricelli. 2002. Bacterial colonization of zirconia ceramic surfaces: an in vitro and in vivo study. Int. J. Oral Maxillofac. Implants 17:793.
39. Scarano A., M. Piattelli, S. Caputi, G.A. Favero and A. Piattelli. 2004. Bacterial adhesion on commercially pure titanium and zirconium oxide disks: an in vivo human study. J. Periodontol. 75:292.

EUROPEAN JOURNAL OF INFLAMMATION Vol. 5, no. 3, 0-0 (2007)
1721-727 (2007)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties129
THE EFFECT OF PORCINE OREXIN A ON C-PEPTIDE PLASMACONCENTRATIONS IN PIGS
P. PAPAKONSTANTINOU, N. TZIRIS, I. KESISOGLOU1, A. GOTZAMANI-PSARRAKOU2, C. TSONIDIS3, M.N. PATSIKAS and L.G. PAPAZOGLOU4
Aristotle University of Thessaloniki, AHEPA University Hospital, 13rd Surgical Clinic,2Department of Nuclear Medicine, 32nd Neurosurgical Clinic A.U.T., 4Department of Clinical Sciences, Faculty of Veterinary Medicine, Aristotle University of Thessaloniki, Macedonia,
Thessaloniki, Greece
Received June 6, 2007 - Accepted September 24, 2007
The hypothalamus and the neuropeptides that are produced and act within its neuronal circuits constitute an area of extensive laboratory research. In 1998, the neuropeptide, Orexin A, was discovered and isolated from the hypothalamus of the rat. An i.c.v. injection of Orexin A into the lateral ventricle of the rat’s brain causes an increase in the consumption of food, and, apart from appetite, it also seems to be regulating many other normal functions of the organism, whose regulatory and metabolic mechanisms remain unknown to date. The neuropeptide is produced by a small cluster located in and round the lateral hypothalamic area. It has been known for decades that this area is involved in the regulation of feeding and energy homeostasis in mammals. The intravenous, subcutaneous, or i.c.v. injection of Orexin A causes changes in insulin and glucagon concentrations. The same effect is also seen under in vitro experimental conditions. In this study, we investigated the potential effects of i.c.v. administration of porcine Orexin A on c-peptide concentrations in the peripheral blood of pigs, and tested whether these changes are associated with the potential effect of the neuropeptide on the function of the pancreas.
Mailing address:Panteleimon Papakonstantinou, MDAgias Sofias 18, 54622Tel: ++30 6944690837 Fax: ++30 2310-269709Thessaloniki, Macedonia, Greecee-mail: [email protected]
Key words: Orexin A, c-peptide, gastrointestinal (or gut) hormones, i.c.v. injection, enteroinsular axis, brain-gut axis
Apart from taking part in the phenomenon of food uptake, and, by extension, in energy homeostasis, Orexin A is directly or indirectly involved in many other normal functions, with an unknown degree of participation, e.g., in the circadian timing system, regulation of liquid homeostasis, and control of water uptake, alternation of the sleep-awakening and alertness cycle, in the possible reactions of the experimental animals under conditions of high stress, in sleeping disorders, for example, narcolepsy, and in the cardiovascular and endocrine systems (1-5).
The extremely large dispersion of the neuraxes of
the orexigenic neurons, which are located both in the central and the peripheral nervous system, is possibly the main reason for the effect of Orexin A on the aforementioned functions of the organism (3, 6-9).
The neuropeptide comes from the precursor polypeptide, i.e., prepro-Orexin, through a proteolytic process. The resulting molecular weight of Orexin A is 4562Da, and presents a structure that is similar in humans, pigs, cattle, rats, and amphibians (10).
Orexin A acts by stimulating receptors of the cell membrane of the target-cell and is denoted as OX1R (Orexin Receptor 1). This receptor is widespread

130 131Eur. J. Inflamm.
in all species, and its activation is the result of intracellular Ca++ levels (2, 11-12).
C-peptideC-peptide is formed in the process of
transformation of proinsulin into insulin, and consists of 31 amino acids with a molecular weight of 3000Da and a half-life of 13 minutes. It is stored in secretory granules, so as to be released subsequently by B cells, in equivalent amounts to those of insulin, in blood flow. It is a major factor in the formation of insulin, since it links chains A and B in such a way as to allow the proper looping in space, as well as the formation of disulphide bonds between the chains (13-15).
When c-peptide moves away from proinsulin through the proteolytic process, the carboxyl end of the part of chain B of insulin remains exposed and free for the appropriate formation of an effective interaction with the insulin receptor (13-15).
The role of c-peptide has not been clarified to date, while it has been considered to be inactive and acting only as a linking peptide in the formation of insulin (13).
There are significant interactions between c-peptide and cell membrane, while there is direct evidence of a stereospecific binding of the peptide with its receptor, which is different from the receptor of insulin and other relevant hormones. Attachment of the c-peptide to the cellular surface takes place through a pair of G-type protein receptors, thus causing the stimulation of special intracellular processes (16-20).
Published studies tried to confirm the orexigenic effect of Orexins when administered i.c.v. in rats and compared with a strong stimulant of food, neuropeptide Y (NPY) and two weaker stimulants: a) (MCH) melanin-concentrating hormone and b) galanin (21).
There are researchers who have studied the changes in insulin and glucagon levels after IV injection of Orexin A in rats. Others have studied insulin concentrations after a subcutaneous injection of the neuropeptide, as well as in vitro into the pancreas of rats. Finally, other researchers have measured the changes in insulin and glucagon concentrations both in vivo and in vitro (22).
As far as we know, no study has been published
yet on the effect of i.c.v. administration of porcine Orexin A in fasting serum c-peptide, as described in the Methods section with two different doses (5 and 10 mg), with or without simultaneous intravenous glucose injection in pigs. The duration of the experiment was 30 minutes, and all blood samples were collected 15 minutes prior to the beginning of each stage of the experiment, and immediately after the bolus, or at the beginning of continuous injection (0 minutes) and after 5, 15, and 30 minutes. The aim of this study is to investigate any possible connections between the effects of Orexin A on serum fasting concentration of c-peptide.
MATERIALS AND METHODS
Preparation of the experimental animalsThe experimental protocol was applied in seven pigs
and was carried out at two different times, with one-week interval. The injection of the neuropeptide, Orexin A (of porcine origin), was done into the lateral ventricle of the brain using a special catheter extracranially through a special valve placed at a previous time (1st time) before the injection (2nd time). In order to place the catheter and the valve properly, it was considered necessary to perform a stereotactic examination of the skull by means of a CT scan.
Experimental protocol1st time Placement of the special device (valve) in the skull of
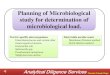
the experimental animal was done under general anesthesia. The point of cranial trepanation is determined at 1/3 of the distance (0.5 to 1 cm from midline) between the midline at the boundaries of the frontal bone (frontal part) and the occipital bone and the zygomatic process of the frontal bone (Fig. 2).
2nd Time The second time consists in the injection of the
neuropeptide, Orexin A, into the lateral ventricle of the pig’s brain. This is achieved after puncture (under local anesthesia), using a lumbar puncture needle, 21G in diameter, and with the device implanted at the 1st time as guide, under general anesthesia.
The administration of porcine Orexin A was done as follows: 1) Rapid i.c.v. injection of the neuropeptide, in two
doses of 5 and 10 mg, diluted in 0.5 ml of artificial cerebrospinal fluid (CSF), with one-hour interval.
2) The aforementioned method of administration was repeated, this time with simultaneous intravenous glucose administration.
c-peptide plasma levels were measured in samples of
P. PAPAKONSTANTINOU ET AL.

130 131Eur. J. Inflamm.
3 ml for each measure- ment.The collections of blood samples were done as
follows:1) 15 minutes prior to the injection;2) Immediately after rapid injection, and also after 5,
15, and 30 minutes. Following blood coagulation and centrifugation at
3000 rpm, the serum was collected in order to measure the levels of c-peptide. The serums were preserved at -70oC up to the date of the measurements.
For the determination of c-peptide, a radioimmunoassay method with a standardized reagent of LINCO Research (1251 Radioimmunoassay Kit) was used.
Statistical analysisThe normal distribution of the sample’s variables
was tested through the application of the Kolmogorov-Smirnov test (p>0.2). Several multivariate analyses of variance (MANOVAs) were carried out, in order to investigate the changes in c-peptide plasma levels (μU/ml) after: a) rapid i.c.v. injection and b) rapid i.c.v. injection with simultaneous intravenous glucose administration, and with injection of: a) 0.5 ml of artificial CSF, b) 5 mg of porcine Orexin A, and c) 10 mg of porcine Orexin A.
Due to the existence of more than three pairwise comparisons (post hoc comparisons), Holm’s Sequential Bonferroni Adjustment was applied to each comparison. Through this adjustment, the probability of Type-I error occurring in the study was reduced, by calculating a
different α for every comparison applied by pairs. The level of significance of the study, α, was set to 0.05.
The changes in the plasma levels of the above variables were investigated after: 1) rapid i.c.v. injection, 2) rapid i.c.v. injection with simultaneous intravenous glucose administration through injection of: a) 0.5 ml of artificial CSF, b) 5 mg of Orexin A at every time of the experiment (-15, 0, 5, 15, and 30 minutes) by applying repeated multivariate analyses of variance (repeated MANOVAs).
c-peptide plasma levels are shown in the tables and figures as means ± standard deviations. Processing of the sample’s data and drawing of figures were done through the application of SPSS 13.0 statistical software for Windows (2004, IL. USA).
The artificial cerebrospinal fluid (aCSF) was administered in a dose of 0.5 ml, and no statistically significant changes in c-peptide plasma levels were seen
before the injection (2nd time). In order to place the catheter and the valve properly, it
was considered necessary to perform a stereotactic examination of the skull by means
of a CT scan.
Fig. 1. The pig�s head at the level of lateral ventricles (transversal level): The dotted line shows the course of the catheter used in the punctures.
Experimental protocol
1st time
Placement of the special device (valve) in the skull of the experimental animal was
done under general anesthesia. The point of cranial trepanation is determined at 1/3 of
the distance (0.5 to 1 cm from midline) between the midline at the boundaries of the
frontal bone (frontal part) and the occipital bone and the zygomatic process of the
frontal bone (Fig. 2).
Fig. 1. The pig’s head at the level of lateral ventricles (transversal level): The dotted line shows the course of the catheter used in the punctures.
Fig. 2. Placement of the special device (valve) in the skull of the experimental animal was done under general anesthesia. The point of cranial trepanation is determined at 1/3 of the distance (0.5 to 1 cm from midline) between the midline at the boundaries of the frontal bone (frontal part) and the occipital bone and the zygomatic process of the frontal bone
Fig. 2. Placement of the special device (valve) in the skull of the experimental animal was done under general anesthesia. The point of cranial trepanation is determined at 1/3 of the distance (0.5 to 1 cm from midline) between the midline at the boundaries of the frontal bone (frontal part) and the occipital bone and the zygomatic process of the frontal bone

132 133Eur. J. Inflamm.
during the study (p>0.05), as shown in Fig. 4.
RESULTS
Rapid i.c.v. injection of Orexin A in two doses of 5 and 10 mg
Rapid i.c.v. injection of Orexin A in doses of 5 mg caused statistically significant changes in c-peptide plasma levels during the first 5 minutes of the experiment, resulting in an increase in c-peptide values from (1050.57±0.535 ng/ml) at time 0 to (1074.29±2.628 ng/ml) (p<0.001). C-peptide plasma levels continued to present a statistically significant increase until the end of the experiment, and reached a value of (1300.29±0.488 ng/ml) (p<0.001) (Fig. 4, Table I).
Rapid i.c.v. injection of Orexin A in doses of 10 mg caused statistically significant increases in c-peptide values from time 0 (1050.29±0.488 ng/ml) up to the time-point of 5 minutes (1130.43±0.787 ng/ml) (p<0.001). A gradual increase in c-peptide levels was observed until the end of the experiment (p<0.001) (Fig. 4, Table I).
Throughout the study, the plasma levels of c-
peptide-and those of the other hormones-affected by the i.c.v. injection of aCSF are statistically much lower than the levels induced by the i.c.v. injection of Orexin A in doses of 5 and 10 mg (Tables I & II).
Rapid i.c.v. administration of Orexin A in doses of 5 mg with simultaneous glucose administration caused statistically significant changes in c-peptide plasma levels during the first 5 minutes of the experiment, resulting in an increase in its values from (1050.29 ±0.488 ng/ml) at time 0 to (1320.43±0.787 ng/ml) (p<0.001). The plasma levels of c-peptide continued to present a statistically significant increase up to the end of the experiment reaching a value of (1890.71±0.951 ng/ml) (p<0.001) (Fig. 5, Table III).
Rapid i.c.v. injection of Orexin A in doses of 10 mg, with simultaneous glucose administration, caused statistically significant increases in c-peptide values from time 0 (1050.23±0.488 ng/ml) until 5 minutes later (1320.43±0.787 ng/ml) (p<0.001). A gradual increase in c-peptide plasma levels was seen until the end of the experiment (p<0.001) (Fig. 5, Table III).
The comparisons of c-peptide plasma levels at
Fig. 3. Schematic representation of the pig’s cerebral parenchyma at the level of lateral ventricles and cross section of the multiple-injection valve. B: Bone screw; S: Bolt (screw); L: Lumbar puncture needle; N: Needle stylet; L.V.: Lateral ventricle
P. PAPAKONSTANTINOU ET AL.

132 133Eur. J. Inflamm.
different times of the experiment (-15, 0 , 5, 15, and 30 minutes) following rapid injection of aCSF and Orexin A in doses of 5 and 10 mg, with simultaneous intravenous glucose administration, were statistically significant for 5 (p<0.001), 15 (p<0.001) and 30 minutes (p<0.001) (Table IV).
DISCUSSION
The neuropeptides of the hypothalamus, along with its neuronal circuits, are responsible for controlling feeding and energy homeostasis. Research on understanding the function of the hypothalamus
and mapping the exact number of neuropeptides led to the discovery of Orexin A in 1998 (23-28).
Orexin A comes from neurons located in and round the lateral hypothalamic area, while showing close vicinity with glucose-sensitive neurons (29-32), and neurons producing and concentrating melatonin (33).
Meanwhile, the orexigenic neurons are interconnected with the corresponding neurons of NPY (34), POMC, CART (35), a-MSH (35-36) AgRP (36-39), norepinephrine (40), dopamine, serotonin, histamine (41), glutamine (42), somatostatin, acetylcholine, vasopressin, VIP, and CRF (42-
Table I. Changes in c-peptide plasma levels (ng/ml) at different times (minutes) after rapid i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg.
*Mean ± standard deviation
Fig. 4. Mean values of c-peptide (ng/ml) after rapid i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg in seven pigs.
301550-15
Time (minutes)
1400
1300
1200
1100
1000
Mea
n c-
pept
ide
Val
ues
(ng/
ml) Orexin � 10µg
Orexin � 5µgaCSF
Time (minutes) aCSF(n=7) Orexin A, 5 mg(n=7) Orexin A, 10 mg(n=7)
-15 1050.29±0.488 1050.29±0.488 1050.29±0.488*
Injection� 0 1050.14±0.378 1050.57±0.535 1050.29±0.488
5 1051.86±0.378 1074.29±2.628 1130.43±0.787
15 1051.14±0.378 1120.71±0.787 1145.14±0.898
30 1050.29±0.78 1300.29±0.488 1389.29±0.951
Table I. Changes in c-peptide plasma levels (ng/ml) at different times (minutes) after rapid i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg.
*Mean ± standard deviation
Table I. Changes in c-peptide plasma levels (ng/ml) at different times (minutes) after rapid i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg.
*Mean ± standard deviation
Fig. 4. Mean values of c-peptide (ng/ml) after rapid i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg in seven pigs.
301550-15
Time (minutes)
1400
1300
1200
1100
1000
Mea
n c-
pept
ide
Val
ues
(ng/
ml) Orexin � 10µg
Orexin � 5µgaCSF
Time (minutes) aCSF(n=7) Orexin A, 5 mg(n=7) Orexin A, 10 mg(n=7)
-15 1050.29±0.488 1050.29±0.488 1050.29±0.488*
Injection� 0 1050.14±0.378 1050.57±0.535 1050.29±0.488
5 1051.86±0.378 1074.29±2.628 1130.43±0.787
15 1051.14±0.378 1120.71±0.787 1145.14±0.898
30 1050.29±0.78 1300.29±0.488 1389.29±0.951
Fig. 4. Mean values of c-peptide (ng/ml) after rapid i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg in seven pigs.

134 135Eur. J. Inflamm.
45). Orexin A acts by stimulating receptors of the cell membrane of the target cell. Their receptors (OX1R receptors) come under the category of those connected with G protein, which are activated based on the intracellular Ca++ levels (1-3).
Both Orexin A and its corresponding receptor are also found outside the CNS. In particular, they have been found in the following: GI tract, pancreas (41), pituitary gland, adrenal glands (42), thyroid gland, kidneys, testicles (1-2, 31), and sympathetic neurons (ganglioneuroblastomas and neuroblastomas) (46).
While Orexin A is produced by a small group of neurons located in and round the lateral hypothalamic area, their neuraxes present an impressive dispersion in different areas of the brain. The above anatomic finding also supports the involvement of Orexin A in many physiological functions, such as the effect on food or water intake, energy homeostasis, the circadian timing system, the endocrine end cardiovascular systems, the sleep-awakening and
alertness cycle as well as on the sense of pain, thermogenesis, and temperature control of the organism (2-3, 47-49).
In particular, dense shunts of the orexigenic nerve fibres are observed in many parts of the brain, e.g.: olfactory bulb, cerebral cortex, amygdaloid nuclei, septum, hippocampus, basal ganglia, Broca’s area, thalamus (anterior, medial and paraventricular nucleus), ventricular system, posterior hypothalamus, pituitary-pineal glands, dorsal nucleus of the vagus nerve, brainstem (central grey matter, nucleus of the cranial suture, locus ceruleus/LC end parabranchial nucleus), nucleus of the solitary tract, septum, midbrain, somesthetic nuclei, mammillary bodies, and spinal cord (2-3, 6, 10).
The release of Orexin A seems to be largely controlled by leptin and the overall reserves of the organism in adipose tissue (1-2, 50-51). The interactions among the three above factors, i.e., Orexin A, leptin, and adipose tissue, have not been
Pairwise comparisons revealed statistically significant variations in c-peptide
plasma levels at the time-points of 5, 15 and 30 minutes of the experiment (p< 0.001)
(Table II).
Table II. Pairwise comparisons of the c-peptide values (ng/ml) after rapid i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg in seven pigs.
SI: statistically insignificant; *statistically significant
Rapid i.c.v. administration of Orexin A in doses of 5 mg with simultaneous
glucose administration caused statistically significant changes in c-peptide plasma
levels during the first 5 minutes of the experiment, resulting in an increase in its
values from (1050.29 ±0.488 ng/ml) at time 0 to (1320.43±0.787 ng/ml) (p<0.001).
The plasma levels of c-peptide continued to present a statistically significant increase
Time (minutes) Rapid i.c.v.
injection
P value
of Comparisons
-15 (1)aCSF
(2)Orexin A 5mg
(3)Orexin A 10mg
(1)-(2): p>0.05 SI
(1)-(3): p>0.05 SI
(2)-(3): p>0.05 SI
0 (1)aCSF
(2)Orexin A 5mg
(3)Orexin A 10mg
(1)-(2): p>0.05 SI
(1)-(3): p>0.05 SI
(2)-(3): p>0.05 SI
5 (1)aCSF
(2)Orexin A 5mg
(3)Orexin A 10mg
(1)-(2): p<0.001 *
(1)-(3): p<0.001 *
(2)-(3): p<0.001 *
15 (1)aCSF
(2)Orexin A 5mg
(3)Orexin A 10mg
(1)-(2): p<0.001 *
(1)-(3): p<0.001 *
(2)-(3): p<0.001 *
30 (1)aCSF
(2)Orexin A 5mg
(3)Orexin A 10mg
(1)-(2): p<0.001 *
(1)-(3): p<0.001 *
(2)-(3): p<0.001 *
Table II. Pairwise comparisons of the c-peptide values (ng/ml) after rapid i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg in seven pigs.
SI: statistically insignificant; *statistically significant
P. PAPAKONSTANTINOU ET AL.

134 135Eur. J. Inflamm.
clarified (1-2, 52). One of the main reasons for this is the fact that the feeding phenomenon is extremely complicated and depends, both qualitatively and quantitatively, on the composition and the quantity of each particular meal, leading finally to the sensation of saturation (52).
The orexigenic system is considered to play a role of short-term mediator in food uptake control and, generally, in energy homeostasis. In response to an acute need for energy, especially when combined with low blood glucose values, or with the lack of food in general, the orexigenic system assumes a primary functional role (24, 52).
Food uptake and energy homeostasis are affected by a large number of metabolic signals coming from
tissues, glands, organs, and systems of the organism and resulting in hypothalamus for a final evaluation and processing (52). In humans, this phenomenon has even more complicated aspects, since other factors intrude as well, e.g., emotional status, socioeconomic background, genetic predisposition, and a large number of sensual signals related to the eating habits of the individual, which vary among different ages, countries, races, or even religions (52).
The orexigenic neurons are in close vicinity to the glucose-sensitive neurons; as a result, the former are activated by a fall in glucose levels (29). Besides, this is a deterministic confirmation, since glucose is the main metabolic fuel of the brain, and any fall or rise in glucose values induces the initiation and
up to the end of the experiment reaching a value of (1890.71±0.951 ng/ml) (p<0.001)
(Fig. 5, Table III).
Rapid i.c.v. injection of Orexin A in doses of 10 mg, with simultaneous glucose
administration, caused statistically significant increases in c-peptide values from time
0 (1050.23±0.488 ng/ml) until 5 minutes later (1320.43±0.787 ng/ml) (p<0.001). A
gradual increase in c-peptide plasma levels was seen until the end of the experiment
(p<0.001) (Fig. 5, Table III).
Table III. Changes in c-peptide plasma levels (ng/ml) at different times (minutes) after rapid i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg with simultaneous intravenous glucose administration in seven pigs.
*Mean ± standard deviation
Time (minutes) aCSF(n=7) Orexin A,5mg(n=7) Orexin A,10mg(n=7)
-15 1050.29±0.488 1050.14±0.378 1050.43±0.535*
Injection� 0 1050.43±0.535 1050.29±0.488 1050.29±0.488
5 1050.86±0.69 1320.43±0.787 1418.29±0.951
15 1052.43±0.378 1590.71±0.951 1722.43±0.787
30 1050.14±0.378 1890.71±0.951 2090.29±0.488
Table III. Changes in c-peptide plasma levels (ng/ml) at different times (minutes) after rapid i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg with simultaneous intravenous glucose administration in seven pigs.
*Mean ± standard deviation
301550-15
Times (minutes)
2200
2000
1800
1600
1400
1200
1000
Mea
n c-
pept
ide
Val
ues (
ng/m
l)
Orexin � 10µgOrexin � 5µgaCSF
Fig. 5. Mean c-peptide values (ng/ml) after rapid i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg with simultaneous glucose administration in seven pigs.
The comparisons of c-peptide plasma levels at different times of the experiment
(-15, 0 , 5, 15, and 30 minutes) following rapid injection of aCSF and Orexin A in
doses of 5 and 10 mg, with simultaneous intravenous glucose administration, were
statistically significant for 5 (p<0.001), 15 (p<0.001) and 30 minutes (p<0.001) (Table
IV).
Table IV. Pairwise comparisons of the c-peptide values (ng/ml) after i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg with simultaneous intravenous glucose administration in seven pigs.
Fig. 5. Mean c-peptide values (ng/ml) after rapid i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg with simultaneous glucose administration in seven pigs.

136 137Eur. J. Inflamm.
discontinuation of feeding, respectively (24, 29). The orexigenic system is also detected in the enteric nervous system, since its neurons are located on the submucosal wall of the gastrointestinal tract and the corresponding ganglia (53). The selection of c-peptide was made based on the criterion of its direct physiological correlation with the B cells of the pancreas. The latter constitute the origin of proinsulin, which, prior to the secretion, is split into insulin and c-peptide, in equimolecular quantities (13). B cells of the pancreas in rats secreting insulin present immunoreactivity both to Orexin A and its corresponding receptor. Orexin A probably acts as a hormone and/or as a paracrine or autocrine transmitter of information from the pancreas to the hypothalamus and vice versa (3, 23). The presence of Orexin A in human plasma supports the above point of view. Very little is known, however, on the regulatory role of Orexin A in the function of the
pancreas (22). Some studies have focused on the central administration of Orexin A in rats, and found that it causes an increase in the consumption of food and an increase in their metabolism. Meanwhile, the lack of food causes mRNA over-expression of the precursor substance of the neuropeptide, i.e., prepro-Orexin, thus suggesting the potential role of Orexin A as a mediator in the central feedback mechanism regulating feeding behaviour (1-2, 21, 42).
The aim of our study is to investigate the potential effects of the neuropeptide Orexin-A on c-peptide plasma secretion and release in pigs with or without simultaneous intravenous glucose injection. By recording any changes in c-peptide plasma levels, at attempt is made to understand the principles of function and determine the degree of participation/effect of Orexin A in the function of the pancreas.
The i.c.v. injection of Orexin A caused an increase in c-peptide values in a time-and dose-dependent
SI: statistically insignificant; *statistically significant
DISCUSSION
The neuropeptides of the hypothalamus, along with its neuronal circuits, are
responsible for controlling feeding and energy homeostasis. Research on
understanding the function of the hypothalamus and mapping the exact number of
neuropeptides led to the discovery of Orexin A in 1998 (23-28).
Orexin A comes from neurons located in and round the lateral hypothalamic area,
while showing close vicinity with glucose-sensitive neurons (29-32), and neurons
producing and concentrating melatonin (33).
Meanwhile, the orexigenic neurons are interconnected with the corresponding
neurons of NPY (34), POMC, CART (35), a-MSH (35-36) AgRP (36-39),
Time (minutes) Rapid i.c.v.
Injection + Glucose
P value of
Comparisons
-15 (1)aCSF
(2)Orexin A 5mg
(3)Orexin A 10mg
(1)-(2): p>0.05 SI
(1)-(3): p>0.05 SI
(2)-(3): p>0.05 SI
0 (1)aCSF
(2)Orexin A 5mg
(3)Orexin A 10mg
(1)-(2): p>0.05 SI
(1)-(3): p>0.05 SI
(2)-(3): p>0.05 SI
5 (1)aCSF
(2)Orexin A 5mg
(3)Orexin A 10mg
(1)-(2): p<0.001 *
(1)-(3): p<0.001 *
(2)-(3): p<0.001 *
15 (1)aCSF
(2)Orexin A 5mg
(3)Orexin A 10mg
(1)-(2): p<0.001 *
(1)-(3): p<0.001 *
(2)-(3): p<0.001 *
30 (1)aCSF
(2)Orexin A 5mg
(3)Orexin A 10mg
(1)-(2): p<0.001 *
(1)-(3): p<0.001 *
(2)-(3): p<0.001 *
Table IV. Pairwise comparisons of the c-peptide values (ng/ml) after i.c.v. injection of aCSF and Orexin A in doses of 5 and 10 mg with simultaneous intravenous glucose administration in seven pigs.
SI: statistically insignificant; *statistically significant
P. PAPAKONSTANTINOU ET AL.

136 137Eur. J. Inflamm.
way. The formation of c-peptide through the process of trans- formation of proinsulin into insulin and its storage in secretory granules, in order to be released subsequently together with insulin from the B cells of the pancreas, inevi- tably classifies it together with insulin (13, 16). When injection was combined with simultaneous glucose administration, a proportionally larger stimulation was seen in mechanisms releasing c-peptide. The results of this study are probably attributed to the following physiological mechanism: the orexigenic neurons in hypothalamus are in close vicinity with the glucose-sensitive neurons, which, in turn, act on the main axis of Na+/K+ ATPase, where it is directly involved in the binding mechanism of c-peptide from its receptor, which is required for any activity (16-17). An i.c.v. injection of Orexin A probably follows the above course, while the simultaneous intravenous glucose administration provides an excessive supporting activity to the glucose-sensitive neurons of the hypothalamus (10, 24, 29).
There are no experimental studies on pigs, or other experimental animals, in the international literature correlating an i.c.v. injection of porcine Orexin A in these doses of 5 and 10 mg, in a rapid way of administration, with the simultaneous administration of glucose and the subsequent collection of blood samples at 5 successive times for the determination of c-peptide plasma levels.
In conclusion, an i.c.v. injection of porcine Orexin A into the lateral ventricle of the pig’s brain causes increases in plasma c-peptide concentrations, in a time-and dose-dependent way. When the i.c.v. injection of porcine Orexin A is accompanied by the simultaneous intravenous glucose injection, the levels of these increases in c-peptide plasma concentrations are even larger. These findings indicate the potential regulatory role of Orexin A in the function of the pancreas.
REFERENCES
1. Sacurai T., A. Amemiya, M. Ishii, I. Matsuzaki, R.M. Chemeli and H. Tanaka. 1998. Orexins and Orexin Receptors: A family of hypothalamic neuropeptides and G protein-coupled receptors that regulate feeding behavior. Cell 92:573.
2. Lecea L.D., T.S. Kilduff, C. Peyron, X.B.
Gaos, P.E. Foye and P.E. Danielson. 1998. The hypocretins: Hypothalamic-specific peptides with neuroexcitatory activity. Neurobiology 95:322.
3. Sacurai T. 1999. Orexins and orexins receptors: implication in feeding behaviour. Regulated Pept. 85:25.
4. Autorino R., M.G. Lamendola, M. De Sio, R.A. Di Trolio, F. Ferraraccio and G. Di Lorenzo. 2007. A complete response with rituximab in metastatic diffuse large B-cell lymphoma of the testis: case report. Int. J. Immunopathol. Pharmacol. 20:401.
5. Feliciani C., E. Ruocco, A. Zampetti, P. Toto, Pa. Amerio, A. Tulli, P. Amerio and V. Ruocco. 2007. Tannic acid induces in vitro acantholysis of keratinocytes via IL-1α and TNF-α. Int. J. Immunopathol. Pharmacol. 20:289.
6. Mondal M., S. Nakazatto and M. Date. 1999. Widespread distribution of orexin in rat brain and its regulation upon fasting. Biochem. Biophys. Res. Lomm. 256:495.
7. Yamamoto Y., Y. Ueta and Y. Date. 1999. Down regulators of the prepro-orexin gene expression in genetically obese mice. Mol. Brain Res. 65:14.
8. Xiong Z., E. Liu, Y. Yan, R.T. Silver, F. Yang, I.H. Chen, I. Hodge, S. Verstovsek, F.J. Segura, H. Wang, J. Prchal and X.F. Yang. 2007. A novel unconventional antigen, MPD5, elicits anti-tumor humoral immune responses in a subset of patients with polycythemia vera. Int. J. Immunopathol. Pharmacol. 20:373.
9. Zhu W., K.J. Mantione, R.M. Kream, P. Cadet and G.B. Stefano. 2007. Cholinergic regulation of morphine release from human white blood cells: evidence for a novel nicotinic receptor via pharmacological and microarray analysis. Int. J. Immunopathol. Pharmacol. 30:229.
10. Taheri S. and S. Bloom. 2001. Orexins/hypocretins: waking up the scientific world. Clin. Endocrin. 54:421.
11 Fioriti D., G. Russo, M. Mischitelli, E. Anzivino, A. Bellizzi, F. Di Monaco, F. Di Silverio, A. Giordano, F. Chiarini and V. Pietropaolo. 2007. A case of human polyomavirus BK infection in a patient affected by late stage prostate cancer: could viral infection be correlated with cancer progression? Int. J. Immunopathol. Pharmacol. 20:405.

138 139Eur. J. Inflamm.
12 Garbuglia A.R., F. Grasso, M.G. Donà, S. Mochi, P. Conti, M.A. De Lutiis, C. Giorgi and T. Iezzi. 2007. TTV infection: role of IFNs, IL-28 and IL-29 cytokines, antiviral proteins. Int. J. Immunopathol. Pharmacol. 20:249.
13. Kitabchi A. 1977. Proinsulin and c-peptide. Metabolism 26:547.
14. D’Alimonte I., R. Ciccarelli, P. Di Iorio, E. Nargi, S. Buccella, P. Giuliani, M.P. Rathbone, S. Jiang, F. Caciagli and P. Ballerini. 2007. Activation of P2X7 receptors stimulates the expression of P2Y2 receptor mRNA in astrocytes cultured from rat brain. Int. J. Immunopathol. Pharmacol. 20:301.
15. Marasini B., L. Belloli and M. Massarotti. 2007. Interstitial lung disease in systemic sclerosis. Int. J. Immunopathol. Pharmacol. 20:223.
16. Toyota T., K. Abe and A. Kudo. 1977. Inhibitory action of rat insulin and synthetic rat C-peptide on insulin secretion in the perfused rat pancreas. Acta Diabetol. Lat. 14:250.
17. Rigler R., A. Pramanik, P. Jonasson, G. Kratz, O. Jansson, P.A. Nygren, S. Stahl, K. Ekberg, B.L. Johansson, S. Uhlen, M. Uhlen, H. Jornvall and J. Wahren. 1999. Specific binding of proinsulin C-peptide to human cell membranes. Proc. Natl. Acad. Sci. USA 96:1318.
18 Karagiannis V., A. Daniilidis, N. Klearhoy, A. Mamopoulos, V. Garipidou, S. Vakalopoulou and H. Zaboulis. 2007. Acute leukemia and pregnancy. Eur. J. Inflamm. 5:47.
19. Stassi G., A. Cascio, C. Iaria, D. Gazzara, G.B. Costa, D. Iannello and A. Arena. 2007. Modulation of GRO-α and TNF-α production by peripheral blood mononuclear cells treated with killed helicobacter pylori. Eur. J. Inflamm. 5:83.
20. Rosati E., S. Mencarelli, A. Magini, R. Sabatini, C. Tassi, A. Orlacchio, S. Coaccioli, A. Frenguelli, P. Marconi and C. Emiliani. 2007. Enhancement of lysosomal glycohydrolase activity in human primary B lymphocytes during spontaneous apoptosis. Int. J. Immunopathol. Pharmacol. 20:279.
21. Edwards C.M., S. Abusnana, D. Sunter, K.G. Murphy, M.A. Ghatei and S.R. Bloom. 1999. The effect of the orexins on food intake: comparison with neuropeptides Y, melaniconcentrating hormone and galanin. J. Endocrinol. 160:7.
22. Ouedraogo R., E. Naslund and A.L. Kirchgessner. 2003. Glucose Regulates the Release of Orexin-A From the Endocrine Pancreas. Diabetes 52:111.
23. Willams G., C. Bing, X.J. Cai, J.A. Harrold, P.J. King and X.H. Liu. 2001. The hypothalamus and the control of energy homeostasis. Different circuits, different purposes. Physiol. Behav. 74:683.
24. Smart D. and J.C. Jerman. 2002. The physiology and pharmacology of the orexins. Pharmacol. Ther. 94:51.
25. Autorino R., M.G. Lamendola, M. De Sio, R.A. Di Trolio, F. Ferraraccio and G. Di Lorenzo. 2007. A complete response with rituximab in metastatic diffuse large B-cell lymphoma of the testis: case report. Int. J. Immunopathol. Pharmacol. 20:401.
26. Feliciani C., E. Ruocco, A. Zampetti, P. Toto, Pa. Amerio, A. Tulli, P. Amerio and V. Ruocco. 2007. Tannic acid induces in vitro acantholysis of keratinocytes via IL-1α and TNF-α. Int. J. Immunopathol. Pharmacol. 20:289.
27. P. Deepak, S. Kumar and A. Acharya. 2007. IL-13 neutralization modulates function of type II polarized macrophages in vivo in a murine T-cell lymphoma. Eur. J. Inflamm. 5:37.
28. Capodiferro S., C. Scully, G. Ficarra, G. de Frenza, R. Grassi, E. Maiorano, G. Favia, F. Mastrangelo and S. Tetè. 2007. Orofacial granulomatosis: report of two cases with gingival onset. Eur. J. Inflamm. 5:51.
29. Cai X.J., P.S. Widdowson, J. Harrold and S. Wilson. 1999. Hypothalamic orexin expression: modulation by blood glucose and feeding. Diabetes 48:2132.
30. P. Papoff, M. Mancuso, C.S. Barbàra and C. Moretti. 2007. The role of terlipressin in pediatric septic shock: a review of the literature and personal experience. Int. J. Immunopathol. Pharmacol. 20:213.
31. E. Bocchietto, C. Paolucci, D. Breda, E. Sabbioni and S.E. Burastero. 2007. Human monocytoid THP-1 cell line versus monocyte-derived human immature dendritic cells as in vitro models for predicting the sensitising potential of chemicals. Int. J. Immunopathol. Pharmacol. 20:259.
32. Arimoto T., H. Takano, K. Inoue, R. Yanagisawa, S. Yoshino, K Yamaki and T. Yoshikawa. 2007. Pulmonary exposure to diesel exhaust particle
P. PAPAKONSTANTINOU ET AL.

138 139Eur. J. Inflamm.
components enhances circulatory chemokines during lung inflammation. Int. J. Immunopathol. Pharmacol. 20:197.
33. Chronwall B.M., D.A. Di Maggio, V.J. Massari, V.M. Pickel, D.A. Ruggiero and T.L. O’Donohue. 1985. The anatomy of neuropeptide Y containing neurons in rat brain. Neurosience 15:1159.
34. Guan J.L., T. Saotome and Q. Wang. 2001. Orexinergic inneravation of POMC-containing neurons in the rat arcuate nucleus. Neuroreport 12:547.
35. Nambu T., T. Sakurai, K. Mizukami, Y. Hosoya, M. Yanagisawa and K. Goto. 1999. Distribution of orexin neurons in the adult rat brain. Brain Res. 827:243.
36. Stanley B.G., D.H. Schwartz, L. Hermandez, B.G. Hoebel and S.F. Leibowitz. 1989. Patterns of extracellular norepinephrine in the paraventricular hypothalamus: relationship to circadian rhythm and deprivation induced eating behavior. Life Sci. 45:275.
37. Papadopoulos P.C., P. Kotridis, B. Kokkas, V. Koutsimanis, G. Aidonidis, G. Dadoush, O. Gouli, M. Karamouzis, A. Kouyoumtzis, G. Sakantamis, D. Hatseras and C.L. Papadopoulos. 2007. Carvedilol increases atrial natriuretic peptide plasma levels in hypertensive patients. Eur. J. Inflamm. 5:97.
38. Ciprandi G., I. Cirillo, R.M. Troisi and G.L. Marseglia. 2007. Allergic subjects have more numerous respiratory infections and severe gastrointestinal infections than non-allergic subjects: preliminary results. Eur. J. Inflamm. 5:27.
39. Lakota K., K. Mrak-Poljšak, B. Rozman, T. Kveder, M. Tomšič and S. Sodin-Semrl. 2007. Serum amyloid A activation of inflammatory and adhesion molecules in human coronary artery and umbilical vein endothelial cells. Eur. J. Inflamm. 5:73.
40. Eberle-Wang K., P. Levitt and K.J. Simansky. 1993. Abnominal vagotomy dissociates anorectic mechanisms for peripheral serotonin and cholecystokinin. Am. J. Physiol. 265:602.
41. Date Y., Y. Ueta and H. Yamashita. 1999. Orexins, Orexigenic hypothalamic peptides, interact with autonomic, neurocrine and neuroregulatory systems. Proc. Natl. Acad. Sci. USA 96:748.
42. Kuru M., Y. Ueta, R. Serino, M. Nakazato and
Y. Yamamoto. 2000. Centrally administered orexin/hypocretin activates HPA axis in rats. Neuroreport 9:1977.
43. Smart D., A.C. Haynes, G. Williams and R.S. Jonathan. 2001. Orexins and the treatment of obesity. Eur. J. Pharmacol. 440:199.
44. Vena G.A., N. Cassano, G. Alessandrini, D. Fai, M. Gabellone, P. Ligori, C. Malvindi, A. Mancino, S. Pellè, F. Rinaldi and M.R. Sodo. 2007. Treatment of mild to moderate plaque psoriasis with calcitriol ointment applied with or without a dosing device. Eur. J. Inflamm. 5:89.
45. Cadoni S., M. Ruffelli, S. Fusari and O. de Pità. 2007. Oral allergic syndrome and recombinant allergens rBet v 1 and rBet v 2. Eur. J. Inflamm. 5:21.
46. Arihara Z., K. Takahashi and O. Murakami. 2000. Orexin A in the human brain and tumor tissues of ganglioneuroblastoma and neuroblastoma. Peptides 21:565.
47. de Lecea L. and J.G. Sutcliffe. 1999. The hypocretins/orexins: novel hypothalamic neuropeptides involved in different physiological systems. CMLS. Cell. Mol. Life Sci. 56:473.
48. Cardillo M.R. and F. Ippoliti. 2007. Interleukin-6, Interleukin-10 and heat shock protein-90 expression in renal epithelial neoplasias and surrounding normal-appearing renal parenchyma. Int. J. Immunopathol. Pharmacol. 20:37.
49. Lanza A., A. De Rosa, F. Femiano, P. Annese, E. Ruocco, F. Gombos, M. Lanza and N. Cirillo. 2007. Internalization of non-clustered desmoglein 1 without depletion of desmoglein 1 from adhesion complexes in an experimental model of the autoimmune disease pemphigus foliaceus. Int. J. Immunopathol. Pharmacol. 20:355.
50. Rowland N.E. 1991. Biological factors in eating and its disorders. Bull. Psychonom. Soc. 29:244.
51. Le Magnen J. 1992. Neurobiology of feeding and nutrition. Ed. Academic Press Inc. San Diego, USA, p. 1.
52. Karla S.P., M.G. Dube and S. Pu. 1999. Interacting appetite regulating pathways in the hypothalamic regulation of body Weight. Endocr. Rev. 20:68.
53. Kirchgessner A.L. and M.T. Liu. 1999. Orexin synthesis and response in the gut. Neuron 24:941.

EUROPEAN JOURNAL OF INFLAMMATION Vol. 5, no. 3, 0-0 (2007)
1721-727 (2007)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties141
SALIVA LEVELS OF 15-F2t-ISOPROSTANE AS BIOMARKER OF LIPID PEROXIDATION IN AUTISTIC CHILDREN
A. KARAMOUZI, D. KOVACHEV1, I. KARAMOUZIS2, M. ANTONIADOU-HITOGLOU3,I. TSIKOULAS4 and N. AGGELOPOULOU-SAKADAMI
Laboratory of Special Education and Developmental Medicine, Department of Physical Education and Sports Medicine, University of Thessaloniki, Greece; 1Biology Laboratory , Medical University
of Varna, Bulgaria; 2Biochemistry Laboratory, Faculty of Medicine, University of Thessaloniki;3Unit of Communication Disabilities A’ ORL Clinic, University of Thessaloniki; 4First Paediatric
Clinic, Ippocratio Hospital, University of Thessaloniki, Greece
Received February 2, 2007 – Accepted October 4, 2007
Autism is a complex neurodevelopmental disorder that usually presents itself in early childhood and is thought to be influenced by genetic and environmental factors. Oxidative stress has been implicated in the etiology of neurological, neurodevelopment and neuropsychiatric disorders including Parkinson’s and Alzheimer disease, Down’s syndrome and autism. The biological fluid levels of the 15-F2t-Isoprostane (15-F2t-IsoP) are regarded as being the most significant biochemical index of oxidative stress. There are some studies that measured 15-F2t-IsoP in the plasma and urine of children with autism. However 15-F2t-IsoP has not been measured in the saliva of children with autism. This procedure is less stressful for the children with autism. The purpose of this study is to evaluate saliva levels of 15-F2t-IsoP in children diagnosed with autism. Saliva levels of 15-F2t-IsoP were determined in 18 children with autism age: 6.6±1.6 years and 21 healthy controls age: 7.5 ±1.4 years. Compared to the control group, the children with autism had significantly higher saliva levels of 15-F2t-IsoP. From the above-mentioned it is concluded that a) lipid peroxidative biomarker 15-F2t-IsoP is increased in autistic children, and b) saliva is the proper (optimal) biological fluid for the evaluation the lipid peroxidation in autistic children.
Mailing address: A. Karamouzi,Laboratory of Special Education and Developmental Medicine, Department of Physical Education and Sports Medicine, University of Thessaloniki,14 I. Zirganou str., 55134, Thessaloniki, GreeceTel: ++30 2310 999109 Fax: ++30 2310 281234e-mail: [email protected]
Key words: 15-F2t-Isoprostane, saliva, autism, autistic children
Autism is a complex neurodevelopmental disorder that usually presents itself in early childhood and that is thought to be influenced by genetic and environmental factors (1-4).
Oxidative stress has been implicated in etiology of neurological, neurodevelopmental and neuropsychiatric disorders including Parkinson’s and Alzheimer disease, Down’s syndrome and autism (5-6).
Under normal condition, a dynamic equilibrium
exists between the production of Reactive Oxygen Species (ROS), such as superoxide anion, hydroxyl radical, singlet oxygen and hydrogen peroxide, and the antioxidant capacity of the cell. Oxidative stress and injury to cells occur when redox homeostasis is altered, and ROS generation overpowers the biochemical defenses of the cell. Lipid peroxidation reflects a chain reaction between polyunsaturated fatty acids and ROS producing lipid peroxides and hydrocarbon polymers that are both highly toxic to

142 143Eur. J. Inflamm.
the cell (6-11).15-F2t-Isoprostane (15-F2t-IsoP) is an end stable
product of peroxidation of arahidonic acid (α.α.). The biological fluid levels of the 15-F2t-Isoprostane (15-F2t-IsoP) are regarded as being the most significant biochemical index of oxidative stress (12-15). Some studies have measured 15-F2t-IsoP in the plasma and urine of children with autism (1, 5, 7, 11). However, 15-F2t-IsoP has not been measured in the saliva of autistic children. This procedure is less stressful for children with autism. The purpose of this study is to evaluate saliva levels of 15-F2t-IsoP in children diagnosed with autism.
MATERIALS AND METHODS
In this study, 18 autistic children (12 male and 6 female) took part as the experimental group age: 6.6±1.6 years, from the autism unit of Varna of Boulgaria, and 21 normally developing children (14 male and 7 female) age: 7.5±1.4 years as control.
The diagnosis of autism was based on the criteria for autism disorder as defined in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) and by a diagnostic interview conducted by a developmental pediatrician (1). The research protocol was approved by the ethics committee of the faculty of Medicine, Aristotle University of Thessaloniki, Greece.
In the above subjects we determined the saliva levels of 15-F2t-IsoP with a sensitive and reliable enzymo-immunoassay method using KIT from Cayman chemical company (www.caymanchem.com). The performance characteristics of this immunoassay method were described in our previous studies (12-13).
RESULTS
Saliva levels of 15-F2t-IsoP were 129.0±±27.5 pg/ml in the autistic children and 41.5±±11.2 pg/ml in the healthy children (controls) (p<0.01). The statistical evaluation was done with the statistical program ANOVA and the couple student t-test (Fig. 1).
As shown in the histogram of Fig. 1, saliva levels of 15-F2t-IsoP in the autistic children were much higher than in the controls, with statistical significant difference between them (p<0.01).
The elevation of Saliva levels of 15-F2t-IsoP indicate increased oxidative stress in the individuals with autism compared to controls. Increased oxidative stress may lead to membrane
lipid abnormalities, mitochondrial dysfunction, exitoxicity, inflammation, and immune dysregulation in autism. These abnormalities may contribute to behavioral abnormalities, sleep disorder and gastrointestinal disturbances in autism (7, 11). Consistent with increased lipid peroxidation, children with autism were found to have increased body burdens of environmental toxins that may generate oxidative stress and lipid peroxidation (5, 16-17). A second line evidence that the lipid peroxidation and oxidative stress may play a role in autism is suggested by a reduced endogenous antioxidant capacity. Specifically, altered glutathione peroxidase (GPX). Superoxide dismutase (SOD) and catalase activities as well as total glutathione (TGSH) and GSH/GSSG and cysteine levels, were found in the autistic individuals compared to controls (6, 10, 18-19). Likewise, levels of exogenous antioxidants were also found to be reduced in autism, including vitamin C, vitamin E, and Vitamin A in plasma and zinc and selenium in erythrocytes (20). Moreover, the increased oxidative stress in autism is derived from evidence of impaired energy metabolism (reduced synthesis of ATP) (21). In addition, higher lactate and pyruvate levels in autism may suggest mitochondrial dysfunction. A major mitochondria dysfunction is the result of oxidative stress (22-27). Besides enhanced lipid peroxidation, platelet and vascular endothelium activation could also contribute to the development of autism (28). The
Fig. 1. Graphical presentation of the mean values of the Salival level of 15-F2t-IsoP in autistic children and controls.
A. KARAMOUZI ET AL.
3
(www.caymanchem.com). The performance characteristics of this immunoassay method were
described in our previous studies (12-13).
RESULTS
Saliva levels of 15-F2t-IsoP were 129.0�27.5 pg/ml in the autistic children and 41.5�11.2 pg/ml
in the healthy children (controls) (p<0.01). The statistical evaluation was done with the statistical
program ANOVA and the couple student t-test (Fig. 1).
Fig. 1. Graphical presentation of the mean values of the Salival level of 15-F2t-IsoP in autistic children and controls.
As shown in the histogram of Fig. 1, saliva levels of 15-F2t-IsoP in the autistic children were
much higher than in the controls, with statistical significant difference between them (p<0.01).
The elevation of Saliva levels of 15-F2t-IsoP indicate increased oxidative stress in the
individuals with autism compared to controls. Increased oxidative stress may lead to membrane
lipid abnormalities, mitochondrial dysfunction, exitoxicity, inflammation, and immune
dysregulation in autism. These abnormalities may contribute to behavioral abnormalities, sleep
disorder and gastrointestinal disturbances in autism (7, 11). Consistent with increased lipid
peroxidation, children with autism were found to have increased body burdens of environmental
toxins that may generate oxidative stress and lipid peroxidation (5, 16-17). A second line evidence
that the lipid peroxidation and oxidative stress may play a role in autism is suggested by a reduced
endogenous antioxidant capacity. Specifically, altered glutathione peroxidase (GPX). Superoxide
dismutase (SOD) and catalase activities as well as total glutathione (TGSH) and GSH/GSSG and
cysteine levels, were found in the autistic individuals compared to controls (6, 10, 18-19). Likewise,
levels of exogenous antioxidants were also found to be reduced in autism, including vitamin C,
vitamin E, and Vitamin A in plasma and zinc and selenium in erythrocytes (20). Moreover, the
0
2
4
6
8
10
12
14
Controls Autistic children
�p<0.01�
0
0
0
0
0
0
015-F
2t-Is
op p
g/m
l

142 143Eur. J. Inflamm.
above biological parameters assessing antioxidative stress and lipid peroxidation are examined in the blood or urine (5-7, 18-20, 28). In the current study, antioxidative stress and lipid peroxidation have been assessed in the saliva taken from children with autistic spectrum disorder. This procedure is much less stressful and, in some cases, less dangerous for children with autism, taking into account the particular difficulties in communication and social interaction of individuals within the spectrum. The measurements of saliva level 15-F2t-isoprostane in children with autism due to the particular difficulties in communication and participation, could be useful for the detection and appreciation of the oxidative stress of the children before and after the antioxidative therapy or before and after the educational intervention. Therefore, saliva is suggested as being the appropriate biological fluid to measure the aforementioned biological parameters in children with autism, compared to plasma or urine used in other studies. From the above-mentioned it is concluded that a) Saliva levels of lipid peroxidative biomarker 15-F2t-IsoP are increased in autistic children, b) saliva is the proper (optimal) biological fluid for the evaluation lipid peroxidation in autistic children.
REFERENCES
1. James S., P. Culter, St. Meenyk et al. 2004. Metabolic biomarkers of increased oxidative stress and impaired methylation capacity in children with autism. Am. J. Clin. Nutr. 80:1611.
2. Eigsti I. and T. Shapiro. 2003. Systems neuroscience approach to autism: biological, cognitive, and clinical perspectives. Ment. Retard. Dev. Disabil. Res. Rev. 9:205.
3. White J. 2003. Intestinal pathology in autism. Exp. Biol. Med. (Maywood) 228:639.
4. Lord C., E. Cook, B. Levental and D. Amaral. 2000. Autism spectrum disorders. Neuron 28:355.
5. Ming X., T. Stein, M. Brimacobe, W. Johnson, G. Lambert and G. Wagner. 2005. Increased excretion of lipid peroxidation biomarker in autism. P.L.E.F.A. 73:379.
6. Sogut S., H. Zoroglu, Y. Ozyurt et al. 2003. Changes in nitric oxide levels and antioxidant enzyme activities may have a role in the pathophysiological mechanisms involved in autism. Clin. Chim. Acta
331:111. 7. Chanham A., V. Chanham, W. Brown and I.
Cohen. 2004. Oxidative stress in autism: Increased lipid peroxidatim and reduced serum levels of ceruloplasmin and tranferrin - the antioxidant proteins. Life Science 75:2539.
8. Jain S. 1984. The accumulation of maloyldialdeyde, a product of fatty acid peroxidation, can disturb aminophospholipid organization in the membrane bilayer of human erythrocytes. J. Biol. Chem. 259:3391.
9. Horton A. and S. Fairhurst. 1987. Lipid peroxidation and mechanisms of toxicity. Crit. Rev. Toxicol. 18:27.
10. Yorbik O., A. Sayal, C. Akay, D. Akbiyik and T. Sohmen. 2002. Investigation of antioxidant enzymes in children with autistic disorder. Prostaglandins, Leukot. Essent. Fatty Acids 67:341.
11. Chauhan A. and V. Chauhan. 2006. Oxidative stress in autism. Pathophysiology 13:17.
12. Karamouzis I., A. Sioulis, M. Karamouzis et al. 2006. Effect of Physical Training on Lipid Peroxidation in Patients on Hemodialysis. In Review of Clinical Pharmacology and Pharmacokinetics, Internal Edition p. 166.
13. Karamouzis I., K. Christoulas, D. Grekas, K. Giannoulius, E. Vambakoudis and K. Mandroukas. 2004. The response of muscle interstitial F2-Isoprostane (8-iso-PGF2α) during dynamic contractions in humans. Prostaglandins, Leukot. Essent. Fatty Acids 71:87.
14. Chiabrando C., C. Rivalta, R. Bagnati et al. 2002. Identification of metabolites from type III F2-isoprostane diasterloisomers by masspectrometry. J. Lipid Res. 43:495.
15. Roberts L. and J. Morrow. 2000. Measurement of F2-isoprostanes as index of oxidative stress in vivo. Free Radical. Biol. Med. 28:505.
16. Edelson S. and D. Cantor. 1998. Autism: xenobiotic influences. Toxicol. Ind. Health 14:79.
17. Edelson S. and D. Cantor. 2000. The neurotoxic etiology of the autistic spectrum disorder: a replicative study. Toxicol. Ind. Health. 16:239.
18. Zaroglu S., F. Armutcu, S. Ozen et al. 2004. Increased oxidative stress and altered activities of erythrocyte free radical scavenging enzymes in autism. Eur. Arch. Psychiat. Clin. Neurosci. 254:

144 EUROPEAN JOURNAL OF INFLAMMATION Vol. 5, no. 3, 0-0 (2007)
1721-727 (2007)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties145
143.19. Golse B., Μ. Debray–Ritzen, P. Durosay et al.
1978. Perturbation de deux enzymes; la superoxyde-dismutase I et la glutathione-peroxydase dans la psychose infantile de developpement (autisme infantile). Rev. Neurol. (Paris) 134: 699.
20. James S., P. Culter, S. Melnyk et al. 2004. Metabolic biomarkers of increased oxidative stress and impaired methylation capacity in children with autism. Am. J. Clin. Nutr. 80:1611.
21. Minshew N., G. Goldstein and S. Dombrowski. 1993. A preliminary 31P MRS study of autism: evidence for undersynthesis and increased degradation of brain membranes. Biol. Psychiat. 33:762.
22. Coleman M. and J. Blass. 1985. Autism and lactic acidosis. J. Autism Dev. Disord. 15:1.
23. Chugani D., B.Sundram, M.Behen et al. 1999.
Evidence of altered energy metabolism in autistic children. Prog. Neuropsychopharmacol. Biol. Psychiat. 23:635.
24. Moreno H., L. Borjas, A. Arrieta et al. 1992. Clinical heterogeneity of the autistic syndrome: a study of 60 families. Invest. Clin. 33:13.
25. Graf W., J. Marin-Garcia, H. Gao et al. Autism associated with the mitochondrial DNA G8363A transfer RNA (Lys) mutation. J. Child Neurol. 15:357.
26. Filipek P., J. Juranek, M. Smith et al. 2003. Mitochondrial dysfunction in autistic patients with 15q inverted duplication. Ann. Neurol. 53:801.
27. Packer L. 1984. Oxygen radicals in biological systems. In Methods in Enzymology vol. 105, ed. Academic Press, New York. P. 105.
28. Yao Y., W. Walsh, W. McGinnis and D. Pratico. 2006. Altered vascular phenotype in autism. Arch. Neurol. 63:1161.
A. KARAMOUZI ET AL.

144 EUROPEAN JOURNAL OF INFLAMMATION Vol. 5, no. 3, 0-0 (2007)
1721-727 (2007)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties145
LYMPHOCYTE DIFFERENTIATION IN THE NASAL MUCOSA
M. GELARDI, M.L. FIORELLA, R. FIORELLA, E. CAVALLUCCI1,M. DI GIOACCHINO1 and G. CIPRANDI2
Department of Ophthalmology and Otolaryngology, Bari University, Bari; 1Allergy Related Disease Unit, CeSI, “G. d’Annunzio” University Foundation, Chieti; 2Dipartimento di Medicina Interna,
Azienda Ospedaliera Universitaria San Martino, Genova, Italy
Received April 4, 2007 - Accepted September 11, 2007
Few cytological studies have investigated the morphologic changes occurring during lymphocyte dif-ferentiation in the nose. The aim of the study is to investigate lymphocyte and plasma cell morphology in patients with allergic rhinitis. Nasal cytology was performed in 110 patients (61 men, 49 women) of ages ranging from 12 to 47 years (mean age, 27), 72 of whom were affected by pollen allergic rhinitis (32 aller-gic to olive, 21 to Parietaria, 13 to grasses, and 6 to cypress) and 38 by perennial allergic rhinitis (allergy to house dust mites). Cytological samples were obtained by scraping with Rhino-Probe™. The samples were collected from the inferior middle turbinate. After fixing and drying, the samples were stained and counted. Cells belonging to the lymphocyte-plasma cell lineage were analyzed. Within this population, 5 different cellular types were identified displaying particular morphologic features of the nucleus and the cytoplasm. These morphological variants constitute various functional stages of B lymphocytes. In aller-gic inflammation, antigen stimulation induces B lymphocytes to differentiate and become plasma cells. The findings from this strictly morphological study will need to be confirmed by immunohistochemical and immunophenotypic studies.
Mailing address: Giorgio Ciprandi, MD,Semeiotica Medica I,Padiglione 3,A.O.U. San Martino,Largo R. Benzi 10, 16132 Genoa, ItalyTel: ++ 39 10 35331820 Fax: ++ 39 10 3537573e-mail: [email protected]
Key words: lymphocytes, plasma cells, lymphocyte differentiation, nasal cytology
There is unanimous consensus that B lymphocyte is the plasma cell precursor, and the plasma cell constitutes a functional stage (1-9). Starting in the 1970s, cellular biology and immunohistochemical studies confirmed this evidence using monoclonal antibodies that permitted to differentiate different types of lymphocytes, including B and T, to identify specific subpopulations, and to correlate various stages of lymphocyte activation and maturation characterized by specific functions (10-24). Nevertheless, few cytological studies have attempted to identify and describe the morphologic changes occurring during lymphocyte differentiation
(25-27).Various disorders affecting the nasal mucosa
induce acute or chronic inflammation, that produce cellular changes (28-31). The presence of infectious agents (32), major enzyme factors, and one or more cell populations (33) on the surface of the nasal mucosa characterizes the type of disease and clinical picture. Exploiting these events, rhinocytograms of patients with allergic rhinitis were analysed to find cells belonging to the lymphocyte cellular line and to describe the cyto-morphological changes that occur during the different stages of cell differentiation.
To identify and examine the largest possible

146 147Eur. J. Inflamm.
number of lymphocytes, the study population included subjects with acute seasonal and perennial allergic rhinitis (34-35).
MATERIALS AND METHODS
Nasal cytology was performed in 110 patients (61 men, 49 women) of ages ranging from 12 to 47 years (mean age, 27), 72 of whom were affected by pollen allergic rhinitis (32 allergic to olive, 21 to Parietaria, 13 to grasses, 6 to cypress) and 38 with perennial allergic rhinitis (house dust mites). None of the patients had received pharmacological therapy up to 2 weeks before the start of the study, and all presented with the typical signs of acute allergic inflammation: nasal obstruction, rhinorrhea, sneezing and nasal itching.
Cytological samples were obtained by scraping with a Rhino-Probe™. The samples were collected from the medial aspect of the inferior middle turbinate. After fixing and drying, the samples were stained using the May-Grünwald-Giemsa method, then mounted on covered slides and examined under microscopy (Nikon E600). Cell count was performed on 20 microscopic samples at high-power magnification (x1000) in immersion.
Morphologic study evaluated particular morphologic variants of the nucleus and the cytoplasm of the lymphocyte population.
RESULTS
Cells belonging to the lymphocyte lineage were analyzed. Five different morphologic variants of the lymphocyte population were detected in the nasal mucosa, displaying particular morphologic features of the nucleus and the cytoplasm:
Cellular type I (Fig. 1)Nucleus: dense nuclear chromatin aggregates in
the center of the nucleus (heterochromatin), with a small marginal portion of finely scattered chromatin (euchromatin);
Cytoplasm: more abundant than in mature lymphocytes; basophilic. No evidence of vacuolization.
This cellular type was found in 8.9% of the cell population.
Cellular type II (Fig. 2)Nucleus: contraction of heterochromatin in the
center of the nucleus, with exposure of the nucleolus inside the euchromatin, which appears more abundant;
Cytoplasm: more abundant than in type I; numerous vacuoles of various diameter.
This cellular type was found in 45.2% of the cell population.
Cellular type III (Fig. 3)Nucleus: small chromatin clumps arranged in
a crown-like pattern, not adherent to the nuclear membrane;
Cytoplasm: basophilic, with fewer vacuoles than in type II.
This cellular type was found in 19.9% of the cell population.
Cellular type IV (Fig. 4)Nucleus: large, non-confluent chromatin clumps,
not adherent to the nuclear membrane (“tortoise shell” nucleus).
Cytoplasm: basophilic, with foamy aspect.This cellular type was found in 18.4% of the cell
population. Cellular type V (Fig. 5)Nucleus: large, confluent polygonal chromatin
clumps adhering to the nuclear membrane (wheel-shaped nucleus).
Cytoplasm: reduced, basophilic, with foamy aspect.
This cellular type was found in 7.4% of the cell population.
DISCUSSION
Nasal cytology is a very suitable diagnostic method to differentiate among numerous types of rhinitis. In this study, it has been proved to be useful in identifying particular cytological variants of lymphocyte line differentiation that have never been described up to now. The cellular types are referable to immunological features typical of some anatomic structures (36-37), including the mucosa of the respiratory tract (38-44), where the mucosal associated lymphoid tissue (MALT, NALT) is the functional site of the immune system. This area is characterized by lymphocyte aggregates of various volume and organizational complexity, inside which some cell types (immunoglobulin-secreting plasma cells) differentiate and mature (19).
The morphological variants expressed different functional stages of B lymphocyte. In the nasal mucosa, the percentage of B lymphocytes is higher
M. GELARDI ET AL.

146 147Eur. J. Inflamm.
Fig. 1. Cellular type I showing aggregates of heterochromatin in the nuclei with small portion of euchromatin and basophilic cytoplasm without vacuolation.
Fig. 2. Cellular type II showing nucleolus inside euchromatin and numerous vacuoles in the cytoplasm.
Fig. 3. Cellular type III showing crown-like pattern of chromatin in nuclei and few vacuoles in the cytoplasm.
Fig. 4. Cellular type IV with “tortoise shell” nucleus and foamy aspect of cytoplasm.
Fig. 5. Cellular type V showing wheel-shapend nucleus and foamy aspect of cytoplasm.

148 149Eur. J. Inflamm.
than T lymphocytes, which are more abundant in the blood stream. In response to antigen stimulation, which is particularly intense in allergic inflammation, B lymphocytes differentiate to form plasma cells. These constitute the final phase in the differentiation of B lymphocytes, after they have passed through the “intermediate” cyto-morphological variants. The immune cells remain long enough on the mucosal surface to be activated by numerous immune stimuli, thus promoting cell differentiation. Similar to a cell culture medium, the nasal mucosa becomes a favourable substrate for this process.
We have listed a chronological series of various cellular types, well aware that the list represents a hypothesis that should be supported by immunohistochemical studies.
Cellular type I represented a phase of lymphocyte activation by the nucleus. It was morphologically demonstrated by the transformation of heterochromatin into euchromatin, functionally active, which stained pink and had a finely granular aspect. The basophilic cytoplasm had a more intense colour than the non-activated lymphocyte, as sign of intense metabolism. The nucleus-to-cytoplasm ratio tipped toward the former. Cellular type II represented the most characteristic element of lymphocyte differentiation and the most often observed cyto-
morphological element in our samples (40%). Compared to the Cellular type I the euchromatin component of the nucleus increased. This transformation brought out the nucleolus, which is usually “hidden” in the lymphocyte. Cytoplasm was more abundant, and the proportion of nucleus to cytoplasm was the inverse of that of Cellular type I. Numerous vacuoles of various size were present. This represented the phase of the cell’s maximum functional activity. While losing lymphocyte morphology, it gained the functional characteristics of the plasma cell, where the intracytoplasmic vacuoles constituted the morpho-functional expression of immunoglobulin production, typical activity of plasma cells.
Immunoglobulin production persisted up to Cellular type III, where numerous vacuoles were immersed in a wide cytoplasm, even though the initial alterations in the nucleus, such as increased heterochromatin which conferred a crown-shaped appearance to the nucleus, that seemed to indicate this cellular type was in initial quiescence. This condition precedes the phase of functional rest in the plasma cells. In our samples represented by Cellular type IV cells that were characterized by a sharp reduction in euchromatin and a rise in heterochromatin, the heterochromatin first formed
Fig. 6. Difference in the frequency of various Cellular types in sample from nasal mucosa (type II > types I > III > IV > V).
M. GELARDI ET AL.

148 149Eur. J. Inflamm.
small clumps that did not adhere to the nuclear membrane (tortoise shell nucleus), and then large, roughly triangular chromocenters whose base adhered to the nuclear membrane (Pappenheim wheel nucleus). This Cellular type (type V), which is the one usually described in literature, constitutes the functionally inactive plasma cell.
The different percentages of cellular types calculated from the rhinocytograms indicate that some cells were functionally active longer than others (type II versus types I, III, IV and V) (Fig. 6).
In conclusion, nasal cytology was found to be advantageous for demonstrating several cellular types whose morphologic characteristics express the consecutive phases through which activated B lymphocytes differentiate into plasma cell. Our microscopic findings will need to be confirmed by cellular biology and immunohistochemical studies to gain a better understanding of the functional role these cells play in inflammatory events.
REFERENCES
1. Serjeva S., C. Malmhall. J. Lotvall and T Pullerits. 2005. Increased number of CD34+ cells in nasal mucosa of allergic rhinitis patients: inhibition by a local corticosteroid. Clin. Exp. Allergy. 35:34.
2. Moller G. 1986. Population dynamics of lymphocytes. Immunol. Rev. 91:233.
3. Cooper M.D. 1987. Current concepts. B lymphocytes, normal development and function. N. Engl. J. Med. 317:1452.
4. Nossal G.J.V. 1987. The basic components of the immune system. N. Engl. J. Med. 316:1320.
5. Zola H. 1987. The surface antigens of human B lymphocytes. Immunol. Today 8:122.
6. Sacchetti C. and L. Morra. 1988. Morfologia e citogenesi dei linfociti e delle plasmacellule. In Trattato Italiano di Medicina Interna. Vol. 5. P. Introzzi. ed. USES, Firenze, p. 414.
7. Corrigan C.J. 1998. Biology of lymphocytes. In Allergy. Principles and Practice. Vol 1. E. Middleton, C.E. Reed, E.F. Ellis, N.F. Adkinson, J.W. Yunginger, W.W. Busse eds. Mosby, St. Louis, p.228.
8. Delves P.J. and I.M. Roitt. 2000. The immune system. N. Engl. J. Med. 343:108.
9. Mayer L. 2003. Mucosal immunity. Pediatrics 111:
1595.10. Bianco D., R. Patrick and V. Nussenzweig. 1970.
A population of lymphocytes bearing a membrane receptor for antigen antibody-complement complexes. J. Exp. Med. 132:702.
11. Pernis B., M. Ferrarini, L. Forni and L. Amante. 1971. Immunoglobulins in lymphocyte membrane. In Progress in Immunology. Academic Press, New York, p.95.
12. Wilson J.D. and G.J.V. Nossal. 1971. Identification of human T and B lymphocytes in normal peripheral blood and in chronic lymphocytic leukemia. Lancet 2:788.
13. Jondall M., G. Holm and H. Wigzell. 1972. Surface markers on human T and B lymphocytes. I: A large population of lymphocytes forming non-immune rosettes with sheep red blood cells. J. Exp. Med. 136:207.
14. Dickler H.B., N.F. Adkinson and W.D. Terry. 1974. Evidence for individual human peripheral blood lymphocytes bearing both B and T cell markers. Nature 247:213.
15. Davis S. 1975. Hypothesis: differentiation of the human lymphoid system based on cell surface markers. Blood 45:871.
16. Moretta L., M.C. Zingari and A. Moretta. 1979. Human T cell subpopulations in normal and pathologic conditions. Immunol. Rev. 45:163.
17. Reinherz E.L. and S.F. Schlossman. 1980. The differentiation and function of human T lymphocytes. A review. Cell 19:821.
18. Haynes B. 1981. Human T lymphocyte antigens as defined by monoclonal antibodies. Immunol. Rev. 57:127.
19. Paul W.E., J. Mizuguchi, M. Brown et al. 1986. Regulation of B lymphocyte activation, proliferation and immunoglobulin secretion. Cell. Immunol. 99:7.
20. Adkins B., C. Mueller and C.Y. Okada. 1987. Early events in T cell maturation. Ann. Rev. Immunol. 5:325.
21. Springer T.A., M.L. Dustin, T.K. Kishimoto and S.D. Marlin. 1987. The lymphocyte function-associated LFA-1, CD2, and LFA-3 molecules: cell adhesion receptors of the immune system. Ann. Rev. Immunol. 5:223.

150 EUROPEAN JOURNAL OF INFLAMMATION Vol. 5, no. 3, 0-0 (2007)
1721-727 (2007)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties151
22. Cambier J.C. and J.T. Ransom. 1987. Molecular mechanisms of transmembrane signaling in B lymphocytes. Ann. Rev. Immunol. 5:175.
23. Kishimoto T. and T. Hirano. 1988. Molecular regulation of B lymphocyte response. Ann. Rev. Immunol. 6:485.
24. Royer H.D. and E.L. Reinherz. 1987. T lymphocytes: ontogeny, function, and relevance to clinical disorders. N. Engl. J. Med. 317:1136.
25. Bessis M. 1980. Reinterpretation des frottis sanguins. Springer Verlag, Berlin-Heidelberg.
26. Gelardi M., P. Cassano, M. Cassano and M.L. Fiorella. 2003. Nasal cytology: description of hyperchromatic supranuclear stria as a possible marker for the anatomical and functional integrity of the ciliated cell. Am. J. Rhinol. 5:263.
27. Gelardi M. 2004. Atlas of Nasal Cytology. Centro Scientifico Editore, Torino, p. 1.
28. Bickmore J.T. 1978. Nasal cytology in allergy and infection. Otorhinolaryngol. Allergy 40:39.
29. Ventura M.T., M. Musti, G. Giuliano, A. Arsieni, E. Di Leo, R. Buquicchio, G. Accettura, A. Spanevello, M.P. Foschino-Barbaro and O. Resta. 2006. Latex allergy and sensitization in cities: a survey in a population at risk. Int. J. Immunopathol. Pharmacol. 19:821.
30. Santino I., F. Scazzocchio, L. Ciceroni, S. Ciarrocchi, R. Sessa and M. Del Piano. 2006. In vitro susceptibility of isolates of Borrelia burgdorferi s.l. to antimicrobial agents. Int. J. Immunopathol. Pharmacol. 19:545.
31. Trubiani O., G. Orsini, S. Caputi and A. Piattelli. 2006. Adult mesenchymal stem cells in dental research: a new approach for tissue engineering. Int. J. Immunopathol. Pharmacol. 19:451.
32. Chapelin C., A. Coste, L. Gilain, F. Poron, F. Verra and E. Escuidier. 1996. Modified epithelial cell distribution in chronic airways inflammation. Eur. Respir. J. 2:2474.
33. Meltzer E.O., H.A. Orgel and A. Jalowayscki.
1999. Nasal Cytology. In Rhinitis. R. Naclerio et al. eds. Marcel Dekker, New York, p.175.
34. Pelikan Z. and M. Pelikan-Filipek. 1988. Cytologic changes in the nasal secretions during the immediate nasal response. J. Allergy Clin. Immunol. 82:1103.
35. Pelikan Z. and M. Pelikan-Filipek. 1989. Cytologic changes in the nasal secretions during the late nasal response. J. Allergy Clin. Immunol. 83:1068.
36. Hein W.R. 1999. Organization of mucosal lymphoid tissue. Curr. Top. Microbiol. Immunol. 236:1.
37. Mowat A.M. and J.L. Viney. 1997. The anatomical basis of intestinal immunity. Immunol. Rev. 156:145.
38. Wolf J.L. and W.A. Bye. 1984. The membranous epithelial (M) cell and the mucosal immune system. Ann. Rev. Med. 35:95.
39. Neutra M.R., A. Frey and J.P. Kraehenbuhl. 1996. Epithelial M cells: gateways for mucosal infection and immunization. Cell 86:345.
40. MacDonald T.T. 1999. Effector and regulatory lymphoid cells and cytokines in mucosal sites. Curr. Top. Microbiol. Immunol. 236:113.
41. Bienenstock J. 1994. Bronchus-associated lymphoid tissue. In Immunology of the Lung and Upper Respiratory Tract, J. Bienenstock ed. McGraw-Hill, New York, p. 96.
42. Kaltreider H.B. 1994. Local immunity. In Immunology of the Lung and Upper Respiratory Tract, J. Bienenstock ed. McGraw-Hill, New York, p.191.
43. Di Iorio A., M. Abate, D. Di Renzo, A. Russolillo, C. Battaglini, P. Ripari, R. Saggini, R. Paganelli and G. Abate. 2006. Sarcopenia: age-related skeletal muscle changes from determinants to physical disability. Int. J. Immunopathol. Pharmacol. 19:703.
44. Manoury B., S. Caulet-Maugendre, I. Guénon, V. Lagente and E. Boichot. 2006. TIMP-1 is a key factor of fibrogenic response to bleomycin in mouse lung. Int. J. Immunopathol. Pharmacol 19:471.
M. GELARDI ET AL.

150 EUROPEAN JOURNAL OF INFLAMMATION Vol. 5, no. 3, 0-0 (2007)
1721-727 (2007)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties151
THE EFFICACY OF FOUR WAYS OF ADMINISTRATING DEXAMETHASONE DURING SURGICAL EXTRACTION OF PARTIALLY IMPACTED LOWER THIRD MOLARS
S. PAPPALARDO, S. PUZZO, V. CAPPELLO, F. MASTRANGELO1, G. ADAMO,
A CARAFFA2 and S. TETÈ1
Dentistry Sector II, Department 2 of Medicine-Surgery, University of Catania; 1Department of Oral Sciences, University of Chieti,2Orthopedic and Traumatology Division, University of Perugia, Italy.
Received July 18, 2007 - Accepted October 4, 2007
Glucocorticoids are drugs noted for their potent anti-inflammatory effect and long lasting half-life. Various studies have been carried out to identify which of these molecules is best for reducing the post-operative sequelae after surgical extraction of the impacted lower third molar. This study examines four different ways of administering dexamethasone after surgical extraction of impacted lower third molars: endoalveolar application, submucous injection, intravenous administration and intramuscular injection, with the aim of identifying which method gives the least discomfort to the patient in regard to reduction of pain, edema and post-operative lock-jaw. Results show that a greater reduction of the post-operative sequelae was obtained in the group of patients treated with dexamethasone intravenously. Satisfying results were also obtained in the group treated with a topical administration of dexamethasone in powder form and in the group which was given dexamethasone through an intramuscular injection. These last two groups had similar results. Instead, the results obtained in the group that received dexamethasone through local submucous injection were not satisfactory.
Mailing address: Prof. Stefano Tetè, Department of Oral Sciences,University of Chieti ,Via dei Vestini 31 66013 Chieti, ItalyTel: ++39 0871 3554095 Fax: ++39 0871 3554095e-mail: [email protected]
Excision of the third lower molar under local anesthetic is one of the most frequently performed interventions in oral surgery. This intervention is usually associated with post-operative pain, edema and trismus, as direct consequences immediately after surgery, influencing the quality of life of the patient. Various studies have therefore been carried out on the control of this post-operative reaction and various perioperative strategies have been proposed aimed at preventing the onset of inflammation which is the cause of pain. The introduction of NSAIDs (non-steroidal anti-inflammatory drugs) has greatly modified the way in which post-operative pain is dealt with in dentistry and medicine in general in
the last thirty years. Thanks to the notable analgesic effect of NSAIDs on acute post-operative pain caused by inflammation, nowadays they have almost totally replaced the use of opiate analgesic combinations such as acetaminophene and codeine (Tylenol with codeine), or acetaminophene and oxicodone (Percocet) (1-13).
However, the prescription of NSAIDs, in particular aspirin, is often cause for concern as these drugs cause the inhibition of the platelet aggregation with a possible increase of intra- and post-operative bleeding and the formation of post-operative hematomas and ecchymosis. Therefore, a valid preventive strategy, as an alternative to the use of NSAIDs for limiting edema, pain and

152 153Eur. J. Inflamm.
trismus following the excision of the lower third molar, is offered by corticosteroids, as has been shown by various clinical tests that have demonstrated the efficacy of betamethasone, dexamethasone and mehylprednisolone; among which dexamethasone has shown to have a good efficacy and half-life (2, 7, 14-30).
Because this post-operative reaction may in part be due to the conversion of phospholipids into arachidonic acid by phospholipase A2 and the consequent production of leucotrienes, prostacyclin, prostaglandin and tromboxane A2, active as mediators in the inflammatory response, the use of corticosteroids may inhibit the initial phase of this process. The glucocorticoids can successfully control the acute inflammation by interfering with a complex cascade of signals in response to the inflammation. Their biologic action is still not fully understood, but the primary mechanism induces the suppression of the accumulation of leukocytes and macrophages at the inflammation focus point and prevents the formation of prostaglandin through the interruption of the cascade of arachidonic acid. The most important point against the use of corticosteroids is the suppression of the normal function of the hypothalamus-hypophysial adrenergic system (HPS). Fortunately, high doses of corticosteroids used for short periods do not significantly alter the HPS (2, 8, 30-40).
Various studies have been carried out to evaluate the efficacy of corticosteroids in reducing the post-operative sequelae after excision of partially or totally impacted lower third molars.
The aim of this study is to evaluate the efficacy of four different ways of administering dexamethasone:- endoalveolar application of dexamethasone in
powder form; - local submucous injection;- intravenous injection;- intramuscular injection.
The study proposes to evaluate the efficacy of these four ways of administering the drug on edema, reduction of the greatest opening (trismus) and pain after excision of partially impacted lower third molars, with the aim of identifying the modality that produces the least discomfort for the patients.
MATERIALS AND METHODS
Patient selection100 patients were included in this study, 52 male and
48 female, with an average age of 26.45±4.2 years. In the study only excisions of partially impacted lower third molars were included, of similar difficulty, including osteotomy and odontotomy when necessary, with the extraction time for each operation not differing by more or less than five minutes in every case. The position of the third molar had to be in class IB according to the Pell and Gregory classification.
Criteria for exclusion were: systemic diseases; contraindications for surgery; contraindications for being administered corticosteroids; patients who had acute periodontitis at the time of the operation; patients who had recently taken anti-inflammatory drugs.
All the patients were informed of the nature of the study and gave their consent before the operation.
Diagnostic investigationTo evaluate the area to be treated and for the
identification of the position of the lower third molar, an ortopantomography (OPT) was used.
Surgical procedureAll the operations were carried out under local
anesthetic, by the same operator, in the same operating room and under similar conditions.
The analgesia of the interested area was carried out by blocking the lower alveolar nerve and injecting for infiltration on the vestibular, distal and lingual sides of the tooth. An incision was then made from the distal-vestibular edge of the lower second molar to the mucogingival junction, and a distal discharge incision with an inclination of about 45° in respect to the first. After the elevation of the mucoperiostal flap, an ostectomy was performed to obtain sufficient bone space to allow for the insertion of the levers and the excision of the lower third molar.
The post-extraction alveolar was then treated and washed by a sterile saline solution. The edges were sutured with single separate stitches, using vicryl 4.0.
The duration of each operation was recorded.
Test groupsTreatment of the patients was randomized and they
were divided into five groups: - group A was treated with 10 mg of endoalveolar
dexamethasone powder wedged into the post-extraction alveolar before the sides were sutured;
- group B was treated with 10 mg dexamethasone by submucous injection, in correspondence to the previously treated area;
- the patients of group C were treated with an intraoperative administration of 4 mg of dexamethasone i.v.;
S. PAPPALARDO ET AL.

152 153Eur. J. Inflamm.
- the patients of group D were treated with an intraoperative administration of 8 mg of dexamethasone i.m.;
- group E (control group) were administered a sterile saline solution.
Postoperative Management All the patients were prescribed an antibiotic therapy
based on amoxicillin+acid clavulanate, 1g/day every 12 hours for 3 days or, in patients who were allergic to penicillin, based on azithromycin, 500mg/day for 3 days. A cold, semi-liquid diet was also suggested. Normal oral hygiene was recommenced by the patients three days after the operation.
MeasuringThe patient’s measurements were taken in the pre-
and post-operative phases (at 2 and 7 days) from each operation. To evaluate the efficacy of treatments, the edema (obtained from the sum of the distance between tragus-pogonion, labial tragus-commissure and palpebral gonion-commissure), the trismus (obtained from the difference in distance between the interincision and the greatest opening, measured in the pre-and post-operative phases) and the pain, were taken into consideration.
To evaluate the pain, the patients were asked to assign each day, for the 7 days following the operation, a value of from 1 to 10 inclusive of their perception of neuralgia on an appropriately planned visual analogical scale (VAS), where 0 corresponds to an absence of pain and 10 to the worst possible sensation of pain imaginable.
Statistical analysis An ANOVA test was done to calculate the average age
of the patients. To calculate the average percentage variation of the
edema and the greatest opening, and the pain at 1 and 7 days from the operation a Kruskal-Wallis test (non-parametric ANOVA) was performed. To evaluate the pain within the individual groups during the 7 post-operative days, a Friedman test (non-parametric repeated ANOVA) was performed.
RESULTS
The values obtained from the measures taken at 1 and 7 days after the operation were analyzed.
From the evaluation of the facial edema at one day after the operation it was deduced that the patients who developed a minor facial edema were those treated with dexamethasone intravenously (group C), followed by the patients of groups A and D. The patients in group B, however, showed a higher value
in respect to the other groups.. The P value was <0.001 in the comparison of the
results from groups A, C and D with group E, and in the comparison of the results of group C with group E. The P value resulted <0.01 in the comparison of the results of group A with those of group B, and in the comparison of the results of group D with those of group B. No significant differences were found between groups A, C and D.
The evaluation of the facial edema at 7 days from the operation showed highly significant results (P<0.01) in the comparison of the results of group C with groups B and E. No significant differences were found between the results of groups A, C, and D (Table I and Fig. 1).
From the evaluation of the reduction of the greatest opening (trismus) at 1 and 7 days from the operation, it is found that the way of administering the drug that offers the best results is the intravenous one, followed by the intramuscular and endoalveolar ones. Also in this evaluation, the submucous way of administering the drug did not result very satisfactory (Table II and Fig. 2).
Highly significant differences were observed in the variation of the average percentage of the greatest opening, at one day from the operation, between groups A, C and D in respect to groups B and E. Also in this case no significant differences were found between groups A, C and D.
The evaluation of the variation of the average percentage of the greatest opening at 7 days from the operation showed a value of P<0.001 (highly significant) when compared to groups A, C and D in respect to group E. The P value results of group C were <0.01 compared with those of group B.
Regarding the analysis of the pain, previous results were confirmed also in this case. The pain reduced more rapidly in the seven days post-operative in the patients of groups A, C and D (Fig. 3).
Comparison of the pain at one and seven days from the operation, as recorded by the 5 groups, showed respectively P<0.001 and P<0.01 in groups A, C and D in respect to groups B and E (see Fig. 4).
Summarizing, the most notable differences regarding the post-operative facial edema were recorded between groups A, C, D and groups B and E (control); the best results were, however, recorded in group C, followed by group A and that did not,

154 155Eur. J. Inflamm.
however, present significant differences with the results obtained by group C. With regard to the facial trismus, the analysis showed satisfying results only in groups A, C and D at one as well as at 7 days from the operation, while for group B, a value very near to that of the control group E was recorded for the facial trismus. Lastly, it can be seen that the perception of neuralgia of the patients examined after each procedure, was less in groups A, C and D. It can therefore be presumed that a reduction of inflammation means a reduction of pain. The results obtained in group B, treated with a local injection of dexamethasone in the mucosa, did not give significantly different results from the control group.
The surgical sequels of impacted lower third molar extractions influence the daily life of the patients causing considerable discomfort. Many researchers,
to limit this post-operative inconvenience, have supported the use of corticosteroids. Among the corticosteroids, dexamethasone is that which has the longest lasting action, a long half-life, and is also considered very strong.
There are many studies that support the association of dexamethasone with other drugs, such as the combined administration of dexamethasone with diclofenac potassium or with rofecoxib (35). These combined drugs have proved effective in the prevention of edema, pain and facial trims following oral surgery.
The aim of this study is concentrated on the effects on the edema, trims and pain of the administration of dexamethasone alone (effect obtained thanks to the suppressive action of dexamethasone on the formation of the transudate) and the variation of this effect when different methods of administering the drug
1414� 1
FIGURES
.
Fig. 1. Evaluation of the variations of the average percentage of the edema at 1 and 7 days from
the operation.
Fig. 2. Evaluation of the variations of the average percentage of the reduction of the greatest opening at 1 and 7 days from the operation.
day 1 day 7 Group A 2.48±0.90 0,21±0.27 Group B 4.35±0.30 0.4±0.31 Group C 1.94±0,16 0.07±0.14 Group D 2.43±0,27 0.19±0.23 Group E 5.16±0.27 0.35±0.28
day 1 day 7 Group A -27±3.4 -1.53±2.3 Group B -53.64±5.2 -3.95±2.7 Group C -19.19±3.6 -1.2±3.4 Group D -23.5±4,1 -1.5±2.1 Group E -53.47±3.5 -4±2.9
0
1
2
3
4
5
6
Group A Group B Group C Group D Group E
-60
-50
-40
-30
-20
-10
0
Group A Group B Group C Group D Group E
day1day 7
Fig. 1. Evaluation of the variations of the average percentage of the edema at 1 and 7 days from the operation.
1414� 1
FIGURES
.
Fig. 1. Evaluation of the variations of the average percentage of the edema at 1 and 7 days from
the operation.
Fig. 2. Evaluation of the variations of the average percentage of the reduction of the greatest opening at 1 and 7 days from the operation.
day 1 day 7 Group A 2.48±0.90 0,21±0.27 Group B 4.35±0.30 0.4±0.31 Group C 1.94±0,16 0.07±0.14 Group D 2.43±0,27 0.19±0.23 Group E 5.16±0.27 0.35±0.28
day 1 day 7 Group A -27±3.4 -1.53±2.3 Group B -53.64±5.2 -3.95±2.7 Group C -19.19±3.6 -1.2±3.4 Group D -23.5±4,1 -1.5±2.1 Group E -53.47±3.5 -4±2.9
0
1
2
3
4
5
6
Group A Group B Group C Group D Group E
-60
-50
-40
-30
-20
-10
0
Group A Group B Group C Group D Group E
day1day 7
1414� 1
FIGURES
.
Fig. 1. Evaluation of the variations of the average percentage of the edema at 1 and 7 days from
the operation.
Fig. 2. Evaluation of the variations of the average percentage of the reduction of the greatest opening at 1 and 7 days from the operation.
day 1 day 7 Group A 2.48±0.90 0,21±0.27 Group B 4.35±0.30 0.4±0.31 Group C 1.94±0,16 0.07±0.14 Group D 2.43±0,27 0.19±0.23 Group E 5.16±0.27 0.35±0.28
day 1 day 7 Group A -27±3.4 -1.53±2.3 Group B -53.64±5.2 -3.95±2.7 Group C -19.19±3.6 -1.2±3.4 Group D -23.5±4,1 -1.5±2.1 Group E -53.47±3.5 -4±2.9
0
1
2
3
4
5
6
Group A Group B Group C Group D Group E
-60
-50
-40
-30
-20
-10
0
Group A Group B Group C Group D Group E
day1day 7
Fig. 2. Evaluation of the variations of the average percentage of the reduction of the greatest opening at 1 and 7 days from the operation.
S. PAPPALARDO ET AL.

154 155Eur. J. Inflamm.
are used. Considering the effect of dexamethasone on the reduction of the facial edema, which is highly significant at the second post-operative day, a time in which the facial edema is imposing. A marked improvement was seen of the post-operative sequelae when the dexamethasone was applied directly onto the tissue, with a consequent higher anti-edematous effect. In fact, the genesis of the facial edema is connected to the trauma of the soft tissue during the avulsion, therefore the direct application of the drug on the traumatized tissue, can significantly reduce the events connected with the inflammation; this is substantially in agreement with the relative literature. This study maintains that the use of dexamethasone in powder form reduces the post-operative trims immediately, as well as a week after the operation. An unexpected conclusion emerged from the results obtained: the topical injection of dexamethasone was no more beneficial for the trims when comparing the control group to the other groups. This appears to confirm the reports from other studies that maintain that, because corticosteroids do not have a direct effect on muscle contraction, the reduction of the facial trims may be due to the lessening of the local inflammation (1).
The post-operative pain after avulsion of an impacted lower third molar is mainly a consequence of the inflammation caused by the attack on the tissue. As shown by another study, dexamethasone, in association with dipirone, prevents the hypersensitivity of the lower alveolar nerve and the
buccal nerve that follows surgery on an impacted lower third molar, while the role of dexamethasone is questionable in the prevention of post-operative pain and does not always have a clinically significant analgesic effect (2, 21). In this study, in particular, this aspect may be due to the method used for measuring pain (VAS), even though this is confirmed by the consistent reduction of pain perceived on the day after as well as a week after the operation on the patients in groups A and D, i.e. in the same groups that had reduced post-operative trims. It can be assumed, therefore, that the higher neuralgic perception of groups B and D in respect to the previous mentioned groups, was due to the facial trims that in the patients of these groups were not reduced. Yuasa and Sugiura maintain that the edema, the trims and the facial pain, after the avulsion of an impacted lower third molar are influenced by the surgery therapy and the patient age and sex ( 12).
Many studies have been carried out on the relationship between some pre- and post-operative variables and the post-operative sequelae following excision of impacted lower third molars. An increase in age seems to be significantly correlated to the degree of the post-operative trims but not to the facial edema. A similar predictive effect has been demonstrated by the radiologic position of the impacted tooth with Pell & Gregory classification. The intraoperative variables also influence the edema, trims and facial pain; in fact the duration of the operation is significantly connected to the degree of post-operative facial trims and edema, while the duration of the osteotomy is significantly connected only with the post-operative facial trims. In conclusion, from this study it was found that a
1515� 1
0
5
10
15
20
25
30
day 1 day 2 day 3 day 4 day 5 day 6 day 7
Gruppo E
Gruppo D
Gruppo C
Gruppo B
Gruppo A
Fig. 3. Evaluation of the decrease of pain in the 7 post-operative days in patients of all patientgroups.
Fig. 4. Evaluation of pain at days 1 and 7 after the operation in all 5 groups.
0
1
23
45
67
Group A Group B Group C Group D Group E
day 1day 7
Fig. 3. Evaluation of the decrease of pain in the 7 post-operative days in patients of all patient groups.
1515� 1
0
5
10
15
20
25
30
day 1 day 2 day 3 day 4 day 5 day 6 day 7
Gruppo E
Gruppo D
Gruppo C
Gruppo B
Gruppo A
Fig. 3. Evaluation of the decrease of pain in the 7 post-operative days in patients of all patientgroups.
Fig. 4. Evaluation of pain at days 1 and 7 after the operation in all 5 groups.
0
1
23
45
67
Group A Group B Group C Group D Group E
day 1day 7
Fig. 4. Evaluation of pain at days 1 and 7 after the operation in all 5 groups.

156 157Eur. J. Inflamm.
greater reduction of the post-operative sequelae was obtained in the group of patents who were treated with dexamethasone intravenously. Satisfying results were also obtained in the group treated with a topical application of dexamethasone in powder form and in the group which received dexamethasone by intramuscular injenction. Good results, however, were not obtained in the group treated with a local sub-mucosa injection of dexamethasone. This phenomena may probably be explained by the precocious removal of the drug from the treated area in that it is hyperaemic. Post-operative edema, trismus, and facial pain in the patients of groups A and D had similar values, slightly lower than those in the group treated with i.m. dexamethasone; no significant differences were, in fact, observed between these three groups. It is possible, therefore, to adopt the endoalveolar administration of dexamethasone as an alternative systemic administration for satisfying results. The immediate post-operative administration of dexamethasone has a favorable effect in impeding the inflammatory consequences after avulsion of an impacted lower third molar. In particular, the topical application of dexamethasone created a lesser edema and facial trismus and reduced the number of patients who felt pain at 1 and 7 days after the avulsion of the impacted lower third molar. Because dexamethasone is usually administrated intravenously or intramuscularly, the results of this study may have a clinically significant effect because the intraoperative topical application of dexamethasone is easier, does not increase the morbidity and does not cause secondary side-effects.
REFERENCES
1. Graziani F., F. D’Aiuto, P.G. Arduino, M. Tonelli and M. Gabriele. 2006. Perioperative dexamethasone reduces post-surgical sequelae of wisdom tooth removal. A split-mouth randomized double-masked clinical trial Int. J. Oral Maxillofac. Surg. 35:241.
2. Alexander R.E. and R.R. Throndson. 2000. A review of perioperative corticosteroid use in dentoalveolar surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 90:406.
3. Barron R.P., R. Benoliel, R. Zeltser, E. Eliav, O. Nahlieli and R.H. Gracely. 2004. Effect of dexamethasone and dipyrone on lingual and inferior alveolar nerve hypersensitivity following third molar
extractions: preliminary report. J. Orofac. Pain 18:62.4. Ventura M.T., M. Musti, G. Giuliano, A. Arsieni,
E. Di Leo, R. Buquicchio, G. Accettura, A. Spanevello, M.P. Foschino-Barbaro and O. Resta. 2006. Latex allergy and sensitization in cities: a survey in a population at risk. Int. J. Immunopathol. Pharmacol. 19:821.
5. Jiang F., W.P. Li, J. Kwiecien and J. Turnbull. 2006. A study of the purine derivative AIT-082 in G93A SOD1 transgenic mice. Int. J. Immunopathol. Pharmacol. 19:489.
6. Avanzini M.A., A. Ricci, C. Scaramuzza, L. Semino, F. Pagella, A.M. Castellazzi, M. Marconi, C. Klersy, A. Pistorio, A.L. Boner and G.L. Marseglia. 2006. Deficiency of INFγ producing cells in adenoids of children exposed to passive smoke. Int. J. Immunopathol. Pharmacol. 19:609.
7. Bui C.H., E.B. Seldin and T.B. Dodson. 2003. Types, frequencies, and risk factors for complications after third molar extraction. J. Oral Maxillofac. Surg. 61:1379.
8. Dhariwal D.K., R. Goodey and J.R. Shepherd. 2002. Trends in oral surgery in England and Wales. Br. Dent. J. 192:639.
9. Dionne R.A., S.M. Gordon, J. Rowan, A. Kent and J.S. Brahim. 2003. Dexamethasone suppresses peripheral prostanoid levels without analgesia in a clinical model of acute inflammation. J. Oral Maxillofac. Surg. 61:997.
10. Sirolli V., L. Amoroso, M. Pietropaolo, G. Grandaliano, G. Pertosa and M. Bonomini. 2006. Platelet-leukocyte interactions in hemodialysis patients: culprit or bystander? Int. J. Immunopathol. Pharmacol. 19:461.
11. Ogilvie A.L.J., M. Lüftl, C. Antoni, G. Schuler, J.R. Kalden and H.M. Lorenz. 2006. Leukocyte infiltration and mRNA expression of IL-20, IL-8 and TNF-R p60 in psoriatic skin is driven by TNF-α. Int. J. Immunopathol. Pharmacol. 19:271.
12. Yuasa H. and M. Sugiura. 2004. Clinical postoperative findings after removal of impacted mandibular third molars: prediction of postoperative facial swelling and pain based on preoperative variables. Br. J. Oral Maxillofac. Surg. 42:209.
13. Kawamura M., K. Hatanaka, M. Saito, M. Ogino, T. Ono, K. Ogino, S. Matsuo and Y. Harada. 2000.
S. PAPPALARDO ET AL.

156 157Eur. J. Inflamm.
Are the anti-inflammatory effects of dexamethasone responsible for inhibition of the induction of enzymes involved in prostanoid formation in rat carrageenin-induced pleurisy? Eur. J. Pharmacol. 400:127.
14. Hidemichi Y. and S. Masayuki. 2004. Clinical postoperative findings after removal of impacted mandibular third molars: prediction of postoperative facial swelling and pain based on preoperative variables. Br. J. Oral Maxillofac. Surg. 42:209.
15. De Berardis D., D. Campanella, F. Gambi, R. La Rovere, A. Carano, C.M. Conti, C. Silvestrini, N. Serroni, D. Piersanti, B. Di Giuseppe, F.S. Moschetta, C. Cotellessa, M. Fulcheri, R.M. Salerno and F.M. Ferro. 2006. The role of C-reactive protein in mood disorders. Int. J. Immunopathol. Pharmacol.19:703.
16. Di Iorio A., M. Abate, D. Di Renzo, A. Russolillo, C. Battaglini, P. Ripari, R. Saggini, R. Paganelli and G. Abate. 2006. Sarcopenia: age-related skeletal muscle changes from determinants to physical disability. Int. J. Immunopathol. Pharmacol. 19:703.
17. Passacantando A., I. Parzanese, M. Rascente, C. Petrucci, G. Minisola and G Tonietti. 2006. Synovial fluid OX40T lymphocytes of patients with rheumatoid arthritis display a Th2/Th0 polarization. Int. J. Immunopathol. Pharmacol. 19:499.
18. Gargallo-Albol J., R. Buenechea-Imaz and C. Gay-Escoda. 2000. Lingual nerve protection during surgical removal of lower third molars. A prospective randomised study. Int. J. Oral Maxillofac. Surg. 29:268.
19. Renton T. and M. McGurk. 2001. Evaluation of factors predictive of lingual nerve injury in third molar surgery. Br. J. Oral Maxillofac. Surg. 39:423.
20. Hargreaves K.M. 1995. Use of ibuprofen and methylprednisolone for the prevention of pain and swelling after removal of impacted third molars. J. Oral Maxillofac. Surg. 53:7.
21. Moore P.A., B. Pardeep and E.R. Smiga. 2005. Pre-emptive rofecoxib and dexamethasone for prevention of pain and trismus following third molar surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 99:1.
22. Schiavino D., E. Nucera, C. Alonzi, A. Buonomo, E. Pollastrini, C. Roncallo, T. De Pasquale, C. Lombardo, G. La Torre, V. Sabato, V. Pecora
and G. Patriarca. 2006. A clinical trial of oral hyposensitization in systemic allergy to nickel. Int. J. Immunopathol. Pharmacol. 19:593.
23. Ferrini A.M., V. Mannoni, P. Aureli, G. Salvatore, E. Piccirilli, T. Ceddia, E. Pontieri, R. Sessa and B. Oliva. 2006. Melaleuca alternifolia essential oil possesses potent anti-staphylococcal activity extended to strains resistant to antibiotics. Int. J. Immunopathol. Pharmacol. 19:539.
24. Nishimura Y., Y. Miura, M. Maeda, H. Hayashi, M. Dong, H. Katsuyama, M. Tomita, F. Hyodoh, M. Kusaka, A. Uesaka, K. Kuribayashi, K. Fukuoka, T. Nakano, T. Kishimoto and T. Otsuki. 2006. Expression of the T cell receptor Vβ repertoire in a human T cell resistant to asbestos-induced apoptosis and peripheral blood T cells from patients with silica and asbestos-related diseases. Int. J. Immunopathol. Pharmacol. 19:795.
25. Manoury B., S. Caulet-Maugendre, I. Guénon, V. Lagente and E. Boichot. 2006. TIMP-1 is a key factor of fibrogenic response to bleomycin in mouse lung. Int. J. Immunopathol. Pharmacol. 19:471.
26. Desjardins P.J., V.S. Shu, D.P. Recker, K.M. Verburg and C.J. Woolf. 2002. A single preoperative oral dose of valdecoxib, a new cyclooxygenase- 2 specific inhibitor, relieves post-oral surgery or bunionectomy pain. Anesthesiology 97:565.
27. Reuben S.S. and N.R. Connelly. 2000. Postoperative analgesic effects of celecoxib or rofecoxib after spinal fusion surgery. Anesth. Analg. 91:1221.
28. Mahmstrom K., S. Daniels, P. Kotey, B.C. Seidenberg and P.J. Desjardin. 1999. Comparison of rofecoxib and celecoxib, two cyclooxygenase-2 inhibitors, in postoperative dental pain: a randomized, placebo and active-comparator-controlled clinical trial. Clin. Ther. 21:1653.
29. Simonetti O., G. Lucarini, G. Goteri, A. Zizzi, G. Biagini, L. Lo Muzio and A. Offidani. 2006. VEGF is likely a key factor in the link between inflammation and angiogenesis in psoriasis: results of an immunohistochemical study. Int. J. Immunopathol. Pharmacol. 19:751.
30. Williamson L.W., E.L. Lorson and D.B. Osborn. 1980. Hypothalamicpituitary-adrenal suppression after short-term dexamethasone therapy for oral surgical procedures. J. Oral Surg. 38:20.

158 EUROPEAN JOURNAL OF INFLAMMATION Vol. 5, no. 3, 0-0 (2007)
1721-727 (2007)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties159
31. Jackson D.L., P.A. Moore and M.T. Roszkowski. 2000. Management of Acute Postoperative Pain. In Oral and Maxillofacial Surgery. Ed. R.J. Fonseca, London, Saunders p. 114.
32. García-Pérez M.A., R. del Val, I. Noguera, C. Hermenegildo, B. Pineda, A. Martínez-Romero and A. Cano. 2006. Estrogen receptor agonists and immune system in ovariectomized mice. Int. J. Immunopathol. Pharmacol. 19:807.
33. Flati V., L.I. Pastore, A.W. Griffioen, S. Satijn, E. Toniato, I. D’Alimonte, E. Laglia, P. Marchetti, A. Gulino and S. Martinotti. 2006. Endothelial cell anergy is mediated by βFGF through the sustained activation of p38-MAPK and NF-κB inhibition. Int. J. Immunopathol. Pharmacol. 19:761.
34. Norholt S.V., E. Aagaard, S. Svensson and S. Sindet-Pedersen. 1998. Evaluation of trismus, bite force, and pressure algometry after third molar surgery: a placebo-controlled study of ibuprofen. J. Oral Maxillofac. Surg. 56:420.
35. Burastero S.E., C. Paolucci, D. Breda, J. Ponti, B. Munaro and E. Sabbioni. 2006. Chromium (VI)-induced immunotoxicity and intracellular accumulation in human primary dendritic cells. Int. J. Immunopathol. Pharmacol. 19:581.
36. Castellani M.L., V. Salini, S. Frydas, J. Donelan, M. Tagen, B. Madhappan, C. Petrarca, K. Falasca, G. Neri, S. Tete’ and J. Vecchiet. 2006. The proinflammatory interleukin-21 elicits anti-tumor response and mediates autoimmunity. Int. J. Immunopathol. Pharmacol. 19(2):247.
37. Lang S., A. Picu, T. Hofmann, M. Andratschke, B. Mack, A. Moosmann, O. Gires, S. Tiwari and R. Zeidler. 2006. Cox-inhibitors relieve the immunosuppressive effect of tumor cells and improve functions of immune effectors. Int. J. Immunopathol. Pharmacol. 19:409.
38. Trubiani O., G. Orsini, S. Caputi and A. Piattelli. 2006. Adult mesenchymal stem cells in dental research: a new approach for tissue engineering. Int. J. Immunopathol. Pharmacol. 19:451.
39. White R.P. Jr, D.A. Shugars, D.M. Shafer, D.M. Laskin, M.J. Buckley and C. Phillips. 2003. Recovery after third molar surgery: clinical and health-related quality of life outcomes. J. Oral Maxillofac. Surg. 61:535.
40. Phillips C., R.P. White Jr, D.A. Shugars and X. Zhou. 2003. Risk factors associated with prolonged recovery and delayed healing after third molar surgery. J. Oral Maxillofac. Surg. 61:1436.
S. PAPPALARDO ET AL.

158 EUROPEAN JOURNAL OF INFLAMMATION Vol. 5, no. 3, 0-0 (2007)
1721-727 (2007)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties159
HYPERTONIC SALINE SOLUTION IN CHILDREN WITH ADENOIDAL HYPERYTROPHY: PRELIMINARY EVIDENCE
G. CIPRANDI, A. VARRICCHIO1, M. CAPASSO2, A.M. VARRICCHIO3, A. DE LUCIA1,E. ASCIONE1, F. AVVISATI1, M. DI GIOACCHINO4 and U. BARILLARI5
Department of Internal Medicine, Azienda Ospedaliera Universitaria San Martino, Genoa; 1U.O.C.
di O.R.L. - Ospedale San Gennaro, ASL Na1, Naples; 2U.O. Pediatria con Nido, Ospedale Civile di Piedimonte Matese (CE); 3U.O.C. di O.R.L. - Azienda Ospedaliera Pediatrica Santobono
Pausilipon, Naples; 4Allergy Related Disease Unit, G. d’Annunzio Universtity Foundation, Chieti; 5Servizio di Foniatria ed Audiologia, Second University of Naples, Italy
Received May 31 2007 – Accepted October 9, 2007
Adenoidal hypertrophy (AH) is a frequent problem in children. A preliminary study evidenced that intranasal hypertonic solutions may exert an anti-inflammatory activity. The aim of the study is to evaluate the effect of intranasal hypertonic or isotonic solutions in children affected with AH. For this purpose, 78 children with AH were evaluated in a randomised and controlled study. Inclusion criteria for the study required that each patient had to have a III or IV degree of AH on the initial endoscopic examination. Children were treated with intranasal hypertonic or isotonic saline solution for 8 weeks. After treatment, endoscopy was performed to evaluate AH degree. Hypertonic treatment was associated with significant (p<0.05) reduction of AH degree. There was a consistent reduction of children with III degree of AH. No adverse events were reported. This preliminary study demonstrates that an 8-week treatment with intranasal hypertonic solution is associated with significant reduction of AH. Therefore, this study evidences that hypertonic solution may exert an anti-inflammatory activity and is safe.
Mailing address: Giorgio Ciprandi, M.D.Semeiotica Medica I - Padiglione 3,A.O.U. San Martino,Largo R. Benzi 10,16132 Genoa, ItalyTel: ++ 39 10 35338120 Fax: ++39 10 3537573e-mail: [email protected]
Key words: adenoidal hypertrophy, children, intranasal hypertonic solution
Adenoidal hypertrophy (AH) represents one of the most frequent indications for surgery in children (1). Moreover, AH is associated with significant morbidity ranging from nasal airway obstruction, recurrent otitis media and cronic rhinosinusitis to obstructive sleep apnea and cardiorespiratory syndrome (2-7).
It was recently reported that treatment with corticosteroids can decrease the size of AH, both using beclomethasone (8) and fluticasone (9-13). It has also been demonstrated that nasal beclomethasone is capable of decreasing the
frequency of adenotonsillectomy (14-17). On the other hand, these preliminary trials are not conclusive as there is no indication of the real effectiveness and overall duration of adenoidal size reduction. Moreover, corticosteroids may also induce side effects.
Recently, preliminary evidence suggested that hypertonic saline nasal sprays alone are effective in treating nasal symptoms in children with seasonal allergic rhinitis (18). Therefore, the present study aimed at evaluating the effect of intranasal hypertonic solution among children affected by AH.

160 161Eur. J. Inflamm.
MATERIALS AND METHODS
Study PopulationSeventy-eight children, 44 males and 34 females, aged
3 to 6 years (mean age 4.5) and complaining of chronic nasal obstruction, were recruited from two Hospitals in Naples.. Inclusion criteria for the study required a III or IV degree of AH in each patient at the initial endoscopic examination (19-22).
Subjects were excluded if they had used intranasal, topical, or systemic corticosteroids within the last year; had used any intranasal medication within 2 weeks before entering the study; had an active upper respiratory infection within 2 weeks before entering the study; or had a history of chronic epistaxis or immunodeficiency.
Study DesignThe study was single blind, randomised, and
controlled in design. All children enrolled were individually randomised to receive 8 weeks of either intranasal hypertonic nasal spray or isotonic saline solution. Both intranasal solutions were administered by a Rinowash aerosolizer, as modern therapeutic strategies suggest the use of a device able to administer a correct aerosol therapy, and Rinowash is a device specifically designed to administer a correct endonasal therapy, and proves particularly effective in the treatment of the upper respiratory ways (URW). Rinowash is able to selectively treat the osteomeatal complex and the rhino-pharynge thanks to the dimension of the nebulized particles. The mass median aerodynamic diameter (MMAD) of the particles is greater than 10 micron, in accordance with the European Resiratory Society Guidelines.
Informed consent for participation in the study was obtained from the children’s parents. The study was approved by the Review Committee. Physicians performing visits were blinded from knowing whether children assumed the hypertonic solution or not.
During the 8-week study, the patients administered the saline solutions twice daily.
Evaluation and Patient ManagementInitial assessment of each patient upon entering the
study included the following: case history, physical examination and fiberoptic endoscopy to evaluate adenoid tissue as well as to assess nasal and sinus disease. Following assessment was made at 8 weeks, including case history and fiberoptic endoscopy.
Adenoid size was assessed during rhinolaryngoscopic examination with an Olympus flexible P-2 Rhinolaryngoscope.
AH degree has been extensively described previously (19). Briefly, during the first and at second evaluation,
color 35-mm transparencies were taken with the child in quiet nasal respiration. Photographs were taken of both left and right posterior choanae and adenoid using an Olympus OM-2 camera adapted to the rhinoscope.
Any adverse event was recorded.
Statistical AnalysisStatistical analysis was performed using the
appropriate non-parametric test for nominal or ordinal data: the Wilcoxon signed-rank.
RESULTS
All 78 children enrolled in the study completed the 8-week trial (39 and 39 in two sections). The use of intranasal hypertonic solution was associated with a significant (p<0.05) reduction of AH in 43.5% of them. On the contrary, isotonic saline solution was not associated with significant improvement of AH as reported in 30.7% of children.
Intergroup comparison showed that hypertonic solution-treated children achieved a significantly (p<0.05) greater reduction of AH in comparison with isotonic solution-treated patients (Fig. 1).
The analysis of AH degrees showed that 18 children had a reduction of adenoidal size after treatment with hypertonic solution (Table I).
No adverse events were reported in either group.
DISCUSSION
Adenoidal hypertrophy which obstructs the nasal airway in children is associated with numerous symptoms, including: snoring, nasal obstruction, oral breathing, rhinolalia, restsleep, hypersomnolence, and enuresis (2-3, 23-28).
The most common cause of obstructive sleep apnea and the cardiorespiratory syndrome is adenoidal or adenotonsillar hyperplasia (3, 29-31). Moreover, AH plays a major role in the pediatric syndromes of chronic rhinosinusitis and chronic otitis media.
Adenoidectomy has been the definitive treatment for relief of upper airway obstruction and diseases complicated by or attributable to AH (2, 24). The most common complication of adenoidectomy is post-operative bleeding (2). Sometimes, re-growth of the adenoid after surgical removal may occur (32).
G. CIPRANDI ET AL.

160 161Eur. J. Inflamm.Table I. Number and percentage of children belonging to different AH degrees before and treatment with flunisolide or saline solution.
Hypertonic Solution At baseline After treatment
IV degree 4 (10.2%) 3 (7.7%)
III degree 35 (89.7%) 19 (48.7%)
II degree 12 (30.7%)
I degree 5 (12.8%)
Isotonic Solution At baseline After treatment
IV degree 6 (15.4%) 5 (12.8%)
III degree 33 (84.6) 24 (61.5%)
II degree 10 (25.6%)
I degree
Table I. Number and percentage of children belonging to different AH degrees before and treatment with flunisolide or saline solution.
-1-0.9-0.8-0.7-0.6-0.5-0.4-0.3-0.2-0.10
Fig. 1. Mean values (SD) of AH reduction in the two treated groups. Hypertonic solution-treated children achieved a significantly greater reduction of AH in comparison with isotonic solution-treated patients: p<0.05 (Wilcoxon signed-rank).
Hypertonic Solution Isotonic Solution
P< 0.05
-0.28
-0.58
Fig. 1. Mean values (SD) of AH reduction in the two treated groups. Hypertonic solution-treated children achieved a significantly greater reduction of AH in comparison with isotonic solution-treated patients: p<0.05 (Wilcoxon signed-rank).
In non-life-threatening AH, medical alternatives to adenoidectomy are usually directed toward treatment of symptoms and concurrent infections.
Systemic corticosteroids may produce a prompt, but temporary, decrease in adenoid size. However, significant side effects preclude their prolonged
employment to suppress AH. Recent trials demonstrated that intranasal corticosteroids, such as beclomethasone and fluticasone, were capable of reducing AH (8-9). Moreover, a very recent study provided evidence that treatment with nasal corticosteroids could represent, for some children,

162 163Eur. J. Inflamm.
an effective means for avoiding adenoidectomy (14).
However, no definitive indication for their use exists. On the other hand, hypertonic solution may exert symptomatic activity in children with seasonal allergic rhinitis (18).
Thus, this study is aimed at evaluating the possible effect of intranasal hypertonic solution in the treatment of children with III or IV degree of AH. The results provide preliminary evidence that hypertonic solution alone may reduce adenoidal size. An anti-inflammatory activity, due to osmolar effect, may explain the effectiveness of hypertonic solution. Even though this treatment is not resolutive, it is completely devoid of side effects. Therefore, hypertonic solution may be used for long periods as an adjunctive treatment to active drugs, such as topical corticosteroids, and might be used for long periods as an alternative to a short course of corticosteroids.
In conclusion, this study demonstrates that an 8-week treatment with intranasal hypertonic solution is associated with significant reduction of AH and is safe.
REFERENCES
1. Ratkow I.M. 1986. Ear, nose, and throat operations in the United States. Arch. Otolaryngol. Head Neck Surg. 112:873.
2. Gates G.A., H.R. Muntz and B. Gaylis. 1992. Adenoidectomy and otitis media. Am. Otol. Rhinol. Laryngol. 101:24.
3. Potsic W.P. and R.F. Wetmore. 1990. Sleep disorders and airway obstruction in children. Otolaryngol. Clin. North Am. 23:651.
4. Grundfast K.M. and D.J. Wittich. 1982. Adenotonsillar hypetrophy and upper airway obstruction in evolutionary perspective. Laryngoscope 92:650.
5. Choucair N., V. Laporte, R. Levy, C. Tranchant, J-P. Gies, P. Poindron and Y. Lombard. 2006. The role of calcium and magnesium ions in uptake of β-amyloid peptides by microglial cells. Int. J. Immunopathol. Pharmacol. 19:683.
6. Castellani M.L., V. Salini, S. Frydas, J. Donelan, M. Tagen, B. Madhappan, C. Petrarca, K.
Falasca, G. Neri, S. Tetè and J. Vecchiet. 2006. The proinflammatory interleukin-21 elicits anti-tumor response and mediates autoimmunity. Int. J. Immunopathol. Pharmacol. 19:247.
7. Mayilyan K.R., J.S. Presanis, J.N. Arnold and R.B. Sim. 2006. Discrete MBL-MASP complexes show wide inter-individual variability in concentration: data from UK vs. Armenian populations. Int. J. Immunopathol. Pharmacol. 19:567.
8. Demain J.G. and D.W. Goetz. 1995. Pediatric adenoidal hypertrophy and nasal airway obstruction reduction with aqueous nasal beclomethasone. Pediatrics 95:355.
9. Brouilette R.T., J.J. Manoukian and F.M. Ducharme. 2001. Efficacy of fluticasone nasal spray for pediatric obstructive sleep apnea. J. Pediatr. 138:838.
10. Serra A., G.C. Schito, G. Nicoletti and G. Fadda. 2007. A therapeutic approach in the treatment of infections of the upper airways: thiamphenicol glycinate acetylcysteinate in sequential treatment (systemic-inhalatory route). Int. J. Immunopathol. Pharmacol. 20:607.
11. Papoff P., M. Mancuso, C.S. Barbàra and C. Moretti. 2007. The role of terlipressin in pediatric septic shock: a review of the literature and personal experience. Int. J. Immunopathol. Pharmacol. 20:213.
12. Deepak P., S. Kumar and A. Acharya. 2007. IL-13 neutralization modulates function of type II polarized macrophages in vivo in a murine T-cell lymphoma. Eur. J. Inflamm. 5:37.
13. Karagiannis V., A. Daniilidis, N. Klearhoy, A. Mamopoulos, V. Garipidou, S. Vakalopoulou and H. Zaboulis. 2007. Acute leukemia and pregnancy. Eur. J. Inflamm. 5:47.
14. Criscuoli G., S. D’Amora, G. Ripa, G. Cinquegrana, N. Mansi, N. Impagliazzo and A. Pisacane. 2003. Frequency of surgery among children who have adenotonsillar hypertrophy and improbe after treatment with nasal beclomethasone. Pediatrics 111:236.
15. Burastero S.E., C. Paolucci, D. Breda, J. Ponti, B. Munaro and E. Sabbioni. 2006. Chromium (VI)-induced immunotoxicity and intracellular accumulation in human primary dendritic cells. Int.
G. CIPRANDI ET AL.

162 163Eur. J. Inflamm.
J. Immunopathol. Pharmacol. 19:581.16. Di Trolio R., G. Di Lorenzo, M. Delfino and S.
De Placido. 2006. Role of pegylated lyposomal doxorubicin (PLD) in systemic Kaposi’s sarcoma: a systematic review. Int. J. Immunopathol. Pharmacol. 19:253.
17. Scuderi N., M. Mazzocchi and C. Rubino. 2007. Effects of zafirlukast on capsular contracture: controlled study measuring the mammary compliance. Int. J. Immunopathol. Pharmacol. 20:577
18. Garavello W., M. Romagnoli, L. Sordo, G. Sambataro and R.M. Gaini. 2003. Hypersaline nasal irrigation in children with symptomatic seasonal allergic rhinitis: a randomized study. Ped. Allergy Immunol. 14:140.
19. Cassano P., M. Gelardi, M. Cassano, M.L. Fiorella and R. Fiorella. 2003. Adenoid tissue rhinopharyngeal obstruction grading based on fiberendoscopic findings: a novel approach to therapeutic management. Int. J. Pediatr. Otorhinolaryngol. 67:1303.
20. Lakota K., K. Mrak-Poljšak, B. Rozman, T. Kveder, M. Tomšič21. and S. Sodin-Semrl. 2007. Serum amyloid A activation of inflammatory and adhesion molecules in human coronary artery and umbilical vein endothelial cells. Eur. J. Inflamm. 5:73.
21. Stassi G., A. Cascio, C. Iaria, D. Gazzara, G.B. Costa, D. Iannello and A. Arena. 2007. Modulation of GRO-α and TNF-α production by peripheral blood mononuclear cells treated with killed helicobacter pylori. Eur. J. Inflamm. 5:83.
22. Stassi G., A. Cascio, C. Iaria, D. Gazzara, G.B. Costa, D. Iannello and A. Arena. 2007. Modulation of GRO-α and TNF-α production by peripheral blood mononuclear cells treated with killed helicobacter pylori. Eur. J. Inflamm. 5:83.
23. Lo Muzio L., A. Santarelli, M. Emanuelli, F. Pierella, D. Sartini, S. Staibano, C. Rubini and G. De Rosa. 2006. Genetic analysis of oral squamous cell carcinoma by cDNA microarrays focused apoptotic pathway. Int. J. Immunopathol. Pharmacol.
19:675.24. Brodsky L. 1989. Modern assessment of tonsils and
adenoids. Pediatr. Clin. North Am. 36:1551.25. Tankel J.W. and A.D. Chessman. 1986. Symptom
relief by adenoidectomy and relationship to adenoid and post-nasal airway size. J. Laryngol. Otol. 100:637.
26. Muthusamy A.S.R., A. Vaidya and P.J. Friend. 2006. Clopidogrel associated acute migratory arthritis following kidney-pancreas transplantation. Int. J. Immunopathol. Pharmacol. 19:443.
27. Ammendolia M.G., F. Superti, L. Bertuccini, F. Chiarini, M.P. Conte, D. Cipriani, L. Seganti and C. Longhi. 2007. Invasive pathway of Listeria Ivanovii in human amnion-derived WISH cells. Int. J. Immunopathol. Pharmacol. 20:509.
28. D’Onofrio F., L. Miele, M. Diaco, L. Santoro, G. De Socio, M. Montalto, A. Grieco, G. Gasbarrini and R. Manna. 2006. Sjogren’s syndrome in a celiac patient: searching for environmental triggers. Int. J. Immunopathol. Pharmacol. 19:445.
29. Vena G.A., N. Cassano, G. Alessandrini, D. Fai, M. Gabellone, P. Ligori, C. Malvindi, A. Mancino, S. Pellè, F. Rinaldi and M.R. Sodo. 2007. Treatment of mild to moderate plaque psoriasis with calcitriol ointment applied with or without a dosing device. Eur. J. Inflamm. 5:89.
30. Yonkers J.W. and R.C. Spaurc. 1987. Upper airway obstruction and the pharyngeal lymphoid tissue. Otolaryngol. Clin. North Am. 20:235.
31. Falasca K., C. Ucciferri, M. Manzoli, P. Mancino, E. Pizzigallo, P. Conti and J. Vecchiet. 2007. Metabolic syndrome and cardiovascular risk in HIV-infected patients with lipodystrophy. Int. J. Immunopathol. Pharmacol. 20:519.
32. Marasini B., L. Belloli and M. Massarotti. 2007. Interstitial lung disease in systemic sclerosis. Int. J. Immunopathol. Pharmacol. 20:223.
33. Rasmussen N. 1987. Complications of tonsillectomy and adenoidectomy. Otolaryngol. Clin. North Am. 20:383.