Embed Size (px)
Citation preview
5/9/2016
1
Clinician Burnout and Dealing with
Difficult PatientsThe Challenging Patient: Problem Solving for the Professional Care Giver Conference
Michael R Privitera MD MSProfessor of Psychiatry
Medical Director, Medical Faculty and Clinician Wellness ProgramUniversity of Rochester Medical [email protected]
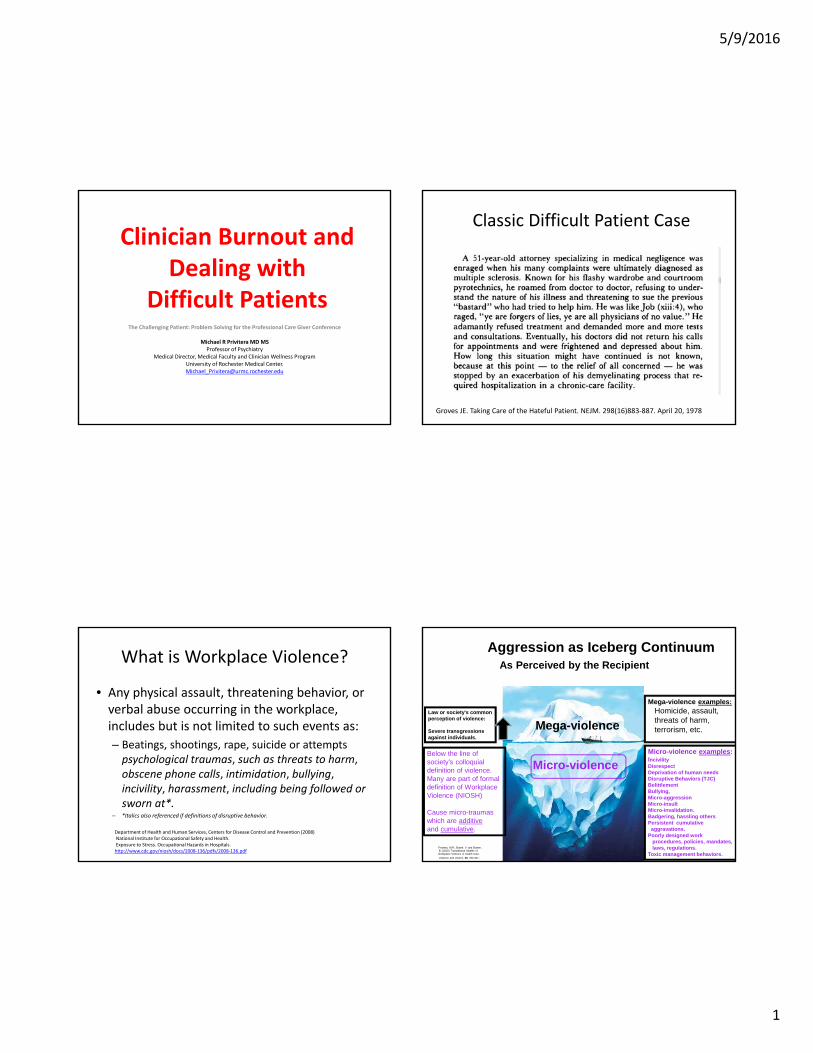
Classic Difficult Patient Case
Groves JE. Taking Care of the Hateful Patient. NEJM. 298(16)883‐887. April 20, 1978
What is Workplace Violence?
• Any physical assault, threatening behavior, or verbal abuse occurring in the workplace, includes but is not limited to such events as:
– Beatings, shootings, rape, suicide or attempts psychological traumas, such as threats to harm, obscene phone calls, intimidation, bullying, incivility, harassment, including being followed or sworn at*.
– *Italics also referenced if definitions of disruptive behavior.
Department of Health and Human Services, Centers for Disease Control and Prevention (2008)National Institute for Occupational Safety and Health.Exposure to Stress. Occupational Hazards in Hospitals.http://www.cdc.gov/niosh/docs/2008‐136/pdfs/2008‐136.pdf
Law or society's common perception of violence:
Severe transgressions against individuals.
Mega-violence examples:Homicide, assault, threats of harm, terrorism, etc.
Micro-violence examples:IncivilityDisrespect Deprivation of human needsDisruptive Behaviors (TJC)BelittlementBullying, Micro-aggressionMicro-insultMicro-invalidation.Badgering, hassling others Persistent cumulative
aggravations.Poorly designed work
procedures, policies, mandates, laws, regulations.
Toxic management behaviors.
Aggression as Iceberg ContinuumAs Perceived by the Recipient
Mega-violence
Micro-violenceBelow the line of society’s colloquialdefinition of violence.Many are part of formal definition of WorkplaceViolence (NIOSH)
Cause micro-traumas which are additiveand cumulative.
Privitera, M.R., Bowie, V. and Bowen,B. (2015) Translational Models of Workplace Violence in Health Care.
Violence and Victims, 30, 293-307.
5/9/2016
2
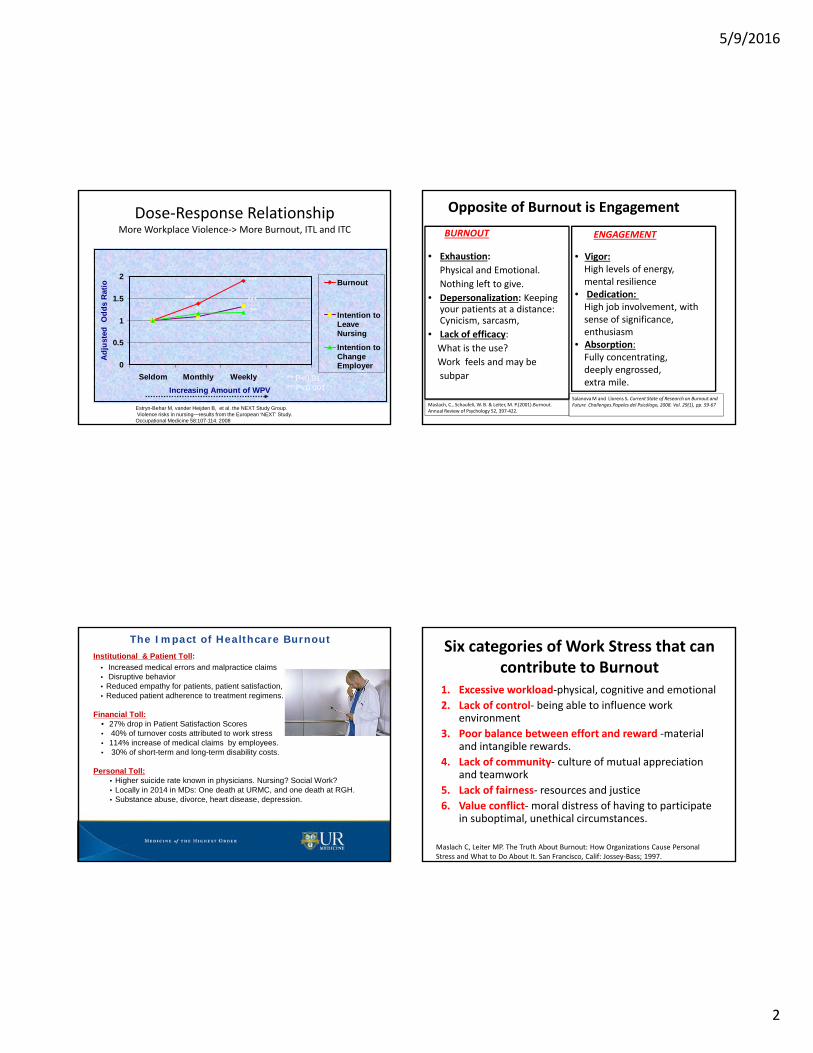
Dose‐Response RelationshipMore Workplace Violence‐> More Burnout, ITL and ITC
0
0.5
1
1.5
2
Seldom Monthly Weekly
Increasing Amount of WPV
Ad
just
ed
Od
ds
Rat
io Burnout
Intention toLeaveNursing
Intention toChangeEmployer
******
***
** **
** P<0.01***P<0.001
Estryn-Behar M, vander Heijden B, et al. the NEXT Study Group.Violence risks in nursing—results from the European ‘NEXT’ Study. Occupational Medicine 58:107-114. 2008
Opposite of Burnout is Engagement
BURNOUT
• Exhaustion:
Physical and Emotional.
Nothing left to give.
• Depersonalization: Keeping your patients at a distance: Cynicism, sarcasm,
• Lack of efficacy:
What is the use?
Work feels and may be
subpar
ENGAGEMENT
• Vigor:High levels of energy,mental resilience
• Dedication: High job involvement, with sense of significance, enthusiasm
• Absorption:Fully concentrating,deeply engrossed,extra mile.
Maslach, C., Schaufeli, W. B. & Leiter, M. P.(2001).Burnout.Annual Review of Psychology 52, 397‐422.
SalanovaM and Llorens S. Current State of Research on Burnout and Future Challenges.Papeles del Psicólogo, 2008. Vol. 29(1), pp. 59‐67
The Impact of Healthcare BurnoutInstitutional & Patient Toll:
• Increased medical errors and malpractice claims• Disruptive behavior• Reduced empathy for patients, patient satisfaction,• Reduced patient adherence to treatment regimens.
Financial Toll:• 27% drop in Patient Satisfaction Scores • 40% of turnover costs attributed to work stress• 114% increase of medical claims by employees. • 30% of short-term and long-term disability costs.
Personal Toll:• Higher suicide rate known in physicians. Nursing? Social Work? • Locally in 2014 in MDs: One death at URMC, and one death at RGH.• Substance abuse, divorce, heart disease, depression.
Six categories of Work Stress that can contribute to Burnout
1. Excessive workload‐physical, cognitive and emotional
2. Lack of control‐ being able to influence work environment
3. Poor balance between effort and reward ‐material and intangible rewards.
4. Lack of community‐ culture of mutual appreciation and teamwork
5. Lack of fairness‐ resources and justice
6. Value conflict‐moral distress of having to participate in suboptimal, unethical circumstances.
Maslach C, Leiter MP. The Truth About Burnout: How Organizations Cause PersonalStress and What to Do About It. San Francisco, Calif: Jossey‐Bass; 1997.
5/9/2016
3
Patient in need!!
Eustress Distress
Fantasy
Multiple work stresses from uncoordinated sourcesEach small alone but incrementally accumulate.1 + 2 + 3 + 4 + 5 + 6……………………….
Stress
Medical or PsychiatricBreakdown Medical Death orSuicide22
Point A
BoredomHypostress
Str
etc
h
Arousal stress, pressure, increased expectations on staff
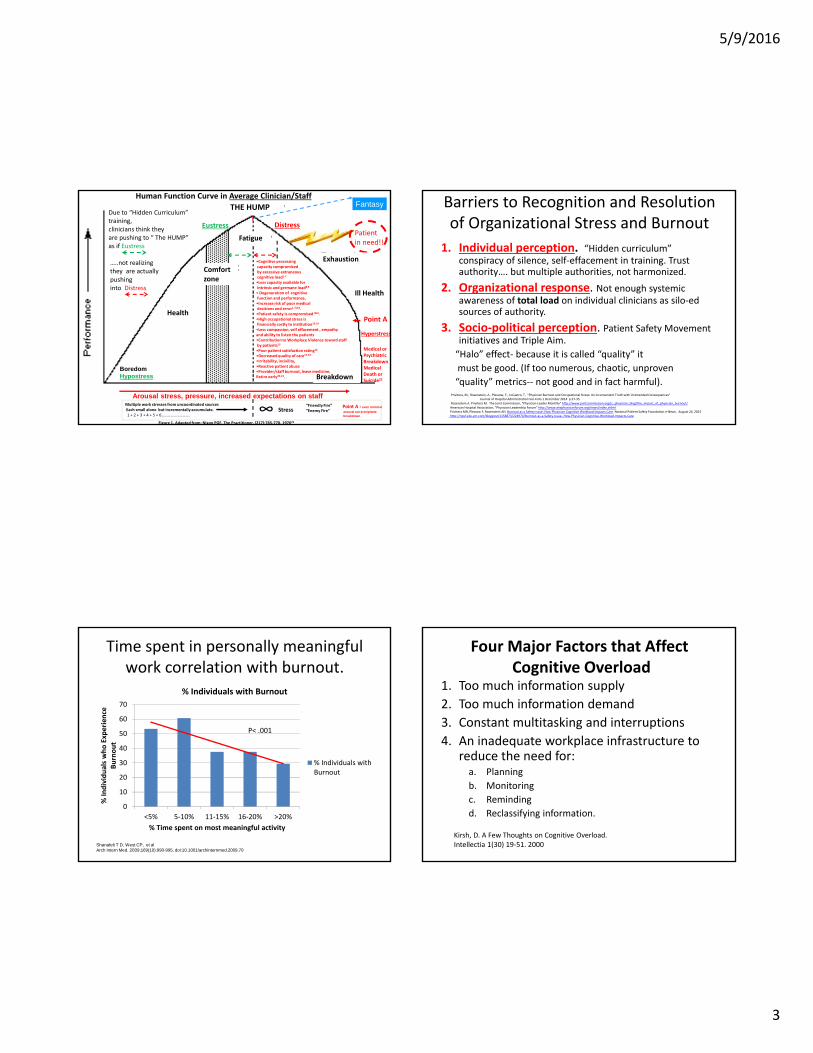
Figure 1. Adapted from: Nixon PGF. The Practitioner. (217):765‐770. 197623
Point A = even minimal
arousal can precipitatebreakdown
“Friendly Fire”“Enemy Fire”
THE HUMP
∞
Hyperstress
Due to “Hidden Curriculum”training,clinicians think theyare pushing to “ The HUMP”as if Eustress
…..not realizing they are actuallypushinginto Distress
Comfortzone
Health
Ill Health
Exhaustion
Fatigue
Breakdown
•Cognitive processingcapacity compromisedby excessive extraneous cognitive load1‐7
•Less capacity available forintrinsic and germane load8,9
• Degeneration of cognitivefunction and performance, •Increase risk of poor medicaldecisions and error1‐7,8,9.•Patient safety is compromised Ibid.•High occupational stress isfinancially costly to institution10‐14
•Less compassion, self effacement , empathy and ability to listen the patients•Contribution to Workplace Violence toward staffby patients15
•Poor patient satisfaction rating16
•Decreased quality of care17‐19
•Irritability, incivility, •Reactive patient abuse•Provider/staff burnout, leave medicine, Retire early20‐21.
Human Function Curve in Average Clinician/Staff Barriers to Recognition and Resolution of Organizational Stress and Burnout
1. Individual perception. “Hidden curriculum” conspiracy of silence, self‐effacement in training. Trust authority…. but multiple authorities, not harmonized.
2. Organizational response. Not enough systemic awareness of total load on individual clinicians as silo‐edsources of authority.
3. Socio‐political perception. Patient Safety Movement initiatives and Triple Aim.
“Halo” effect‐ because it is called “quality” it
must be good. (If too numerous, chaotic, unproven
“quality” metrics‐‐ not good and in fact harmful).Privitera, M., Rosenstein, A., Plessow, F., LoCastro, T. "Physician Burnout and Occupational Stress: An Inconvenient Truth with Unintended Consequences"
Journal of Hospital Administration Vol.4 No.1 December 2014 p.27‐35Rosenstein A. Privitera M. The Joint Commission, “Physician Leader Monthly” http://www.jointcommission.org/jc_physician_blog/the_impact_of_physician_burnout/American Hospital Association, “Physician Leadership Forum” http://www.ahaphysicianforum.org/news/index.shtmlPrivitera MR, Plessow F, Rosenstein AH. Burnout as a Safety Issue: How Physician Cognitive Workload Impacts Care. National Patient Safety Foundation e‐News. August 24, 2015http://npsf.site‐ym.com/blogpost/1158873/224974/Burnout‐as‐a‐Safety‐Issue‐‐How‐Physician‐Cognitive‐Workload‐Impacts‐Care
Time spent in personally meaningful work correlation with burnout.
0
10
20
30
40
50
60
70
<5% 5‐10% 11‐15% 16‐20% >20%
% Individuals who Experience
Burnout
% Time spent on most meaningful activity
% Individuals with Burnout
% Individuals withBurnout
Shanafelt T D, West CP, et alArch Intern Med. 2009;169(10):990-995. doi:10.1001/archinternmed.2009.70
P< .001
Four Major Factors that AffectCognitive Overload
1. Too much information supply
2. Too much information demand
3. Constant multitasking and interruptions
4. An inadequate workplace infrastructure to reduce the need for:a. Planning
b. Monitoring
c. Reminding
d. Reclassifying information.
Kirsh, D. A Few Thoughts on Cognitive Overload. Intellectia 1(30) 19‐51. 2000

5/9/2016
4
Extraneous Load- burden in cognitive processing information that
can be improved by better design.
Germane Load, manage the care, emotional work of patient care, work with families, operate EHR
Intrinsic Load: inherent level of difficulty. E.g. Diagnosis and treatment of
CHF, HTN, CVA, Depression etc etcthought to be immutable load)
MDM Normal
Cognitive Load Theory
Goal is to reduce extraneous load and promote germane load.Sweller, J. (1988). "Cognitive load during problem solving:Effects on learning". Cognitive Science 12 (2): 257–285..
Mental Reserve RemainingHave access to Cognitive Flexible memory
Tota
l M
en
tal
Ca
pa
cit
yT
he
re a
re in
her
en
t lim
its
of
wo
rkin
g m
em
ory
an
d
info
rma
tio
n p
roc
es
sin
g c
ap
ab
ility
Extraneous Load-
Excessive
Germane Load
Intrinsic Load
MDM Impaired !!**
Mental overload/ poor decision outcomeGoal shielding-- looses larger context issuesRevert to Habit Memory Executive Functions of the Brain
1. Focus, Attention
2. Self Control of Behavior and Speech
3. Plan and Organize
4. Perspective Taking
5. Cognitive Flexibility
6. Medical and other Decision Making
7. Ability to Defer Gratification
8. Estimating Time
9. Working Memory
Executive Function (EF) of Brain
• Controlled by Prefrontal Cortex ( PFC) – with connections throughout the brain.
• Sensitive to stress exposure. – Even mild acute uncontrollable stress can cause a rapid and dramatic loss of prefrontal
cognitive abilities.
• Prolonged stress exposure Anatomical change (architectural changes in prefrontal nerve cells (cortex thins) and amygdala enlarges .
• Executive Function affected by:• Personality
• Culture*
• Genetics
• Sleep deprivation*
• Substances*
• Excessive task switching*
• Interruptions*
• Cognitive load*
• Poor design of workflow*
• Burnout*
• Symptomatic* Major Mood Disorders
(Unipolar and Bipolar disorder).
* We can do something to help these factors.
Structures affected by Chronic Occupational StressCognitive Flexible Memory:
1. Examine and weigh multiple factors
• Synthesize a more accurate diagnosis from many things
learned in medical training (good differential diagnosis).
• More comprehensive and effective care plan.
2. Make the mental connection for planning next steps.
• The anticipated need to have emotional availability to the patient and family……...
Habit Memory:• Spares cognitive resources• Automates response to a preceding stimuli,
without link to outcome that follows.
Involves the striatum and the basal ganglia. These structures are not the ones used byother memory systems.
5/9/2016
5
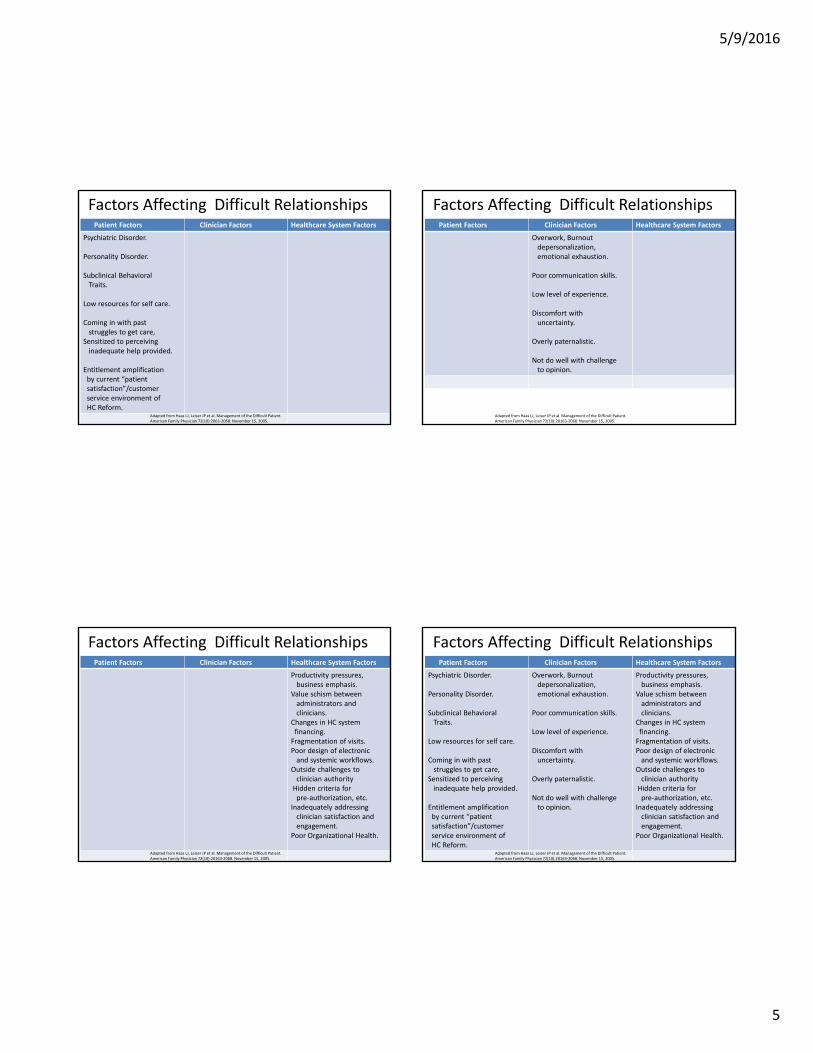
Factors Affecting Difficult RelationshipsPatient Factors Clinician Factors Healthcare System Factors
Psychiatric Disorder.
Personality Disorder.
Subclinical BehavioralTraits.
Low resources for self care.
Coming in with past struggles to get care,
Sensitized to perceiving inadequate help provided.
Entitlement amplification by current “patient satisfaction”/customer service environment of HC Reform.
Adapted from Haas LJ, Leiser JP et al. Management of the Difficult Patient. American Family Physician 72(10):2063‐2068. November 15, 2005.
Factors Affecting Difficult RelationshipsPatient Factors Clinician Factors Healthcare System Factors
Overwork, Burnout depersonalization, emotional exhaustion.
Poor communication skills.
Low level of experience.
Discomfort with uncertainty.
Overly paternalistic.
Not do well with challenge to opinion.
Adapted from Haas LJ, Leiser JP et al. Management of the Difficult Patient. American Family Physician 72(10):20163‐2068. November 15, 2005.
Factors Affecting Difficult RelationshipsPatient Factors Clinician Factors Healthcare System Factors
Productivity pressures, business emphasis.
Value schism between administrators and clinicians.
Changes in HC system financing.Fragmentation of visits.Poor design of electronic and systemic workflows.
Outside challenges to clinician authorityHidden criteria for pre‐authorization, etc.
Inadequately addressing clinician satisfaction and engagement.
Poor Organizational Health.
Adapted from Haas LJ, Leiser JP et al. Management of the Difficult Patient. American Family Physician 72(10):20163‐2068. November 15, 2005.
Factors Affecting Difficult RelationshipsPatient Factors Clinician Factors Healthcare System Factors
Psychiatric Disorder.
Personality Disorder.
Subclinical BehavioralTraits.
Low resources for self care.
Coming in with past struggles to get care,
Sensitized to perceiving inadequate help provided.
Entitlement amplification by current “patient satisfaction”/customer service environment of HC Reform.
Overwork, Burnout depersonalization, emotional exhaustion.
Poor communication skills.
Low level of experience.
Discomfort with uncertainty.
Overly paternalistic.
Not do well with challenge to opinion.
Productivity pressures, business emphasis.
Value schism between administrators and clinicians.
Changes in HC system financing.Fragmentation of visits.Poor design of electronic and systemic workflows.
Outside challenges to clinician authorityHidden criteria for pre‐authorization, etc.
Inadequately addressing clinician satisfaction and engagement.
Poor Organizational Health.
Adapted from Haas LJ, Leiser JP et al. Management of the Difficult Patient. American Family Physician 72(10):20163‐2068. November 15, 2005.

5/9/2016
6
Three‐way interaction:Patient, Clinician and Healthcare Environment
Patient PatientClinician Clinician
Work Environment Healthy Work Environment Toxic
High Risk High RiskHigh RiskHigh Risk
Low RiskLow Risk
Low Risk Low Risk
Difficult Relationship
Difficult Relationship
High ThresholdBefore enterinto problems
Low Threshold before enter Into problems
Overlapping Organizational Factors Contributing to Burnout and WPV
Privitera, M.R. (2016) Organizational Contributions to Healthcare Worker (HCW) Burnout andWorkplace Violence (WPV) Overlap: Is This an Opportunity to Sustain Prevention of Both? Health, 8, 531‐537.http://dx.doi.org/10.4236/health.2016.86056
Vicious Cycle of Burnout and WPV
Privitera, M.R. (2016) Organizational Contributions to Healthcare Worker (HCW) Burnout andWorkplace Violence (WPV) Overlap: Is This an Opportunity to Sustain Prevention of Both? Health, 8, 531‐537.http://dx.doi.org/10.4236/health.2016.86056
Heartsink Patients
• There are patients in every practice who give the doctor and staff a feeling of 'heartsink' every time they consult. O'Dowd (1988)
O’Dowd TC. Five years of heartsink patients in general practice. BMJ 1988; 297(6647):528–530.

5/9/2016
7
Signs and Symptoms of Potentially Difficult Interactions
• Thick chart
• Labeled non‐compliant “Psych patient”
• Suicidal
• Unexplained somatic symptoms
• Alcoholic
• “Drug‐seeking”
• Personality disorder
• Demanding
• Threatening
• Agitated
• Tearful
• Untreatable illness
• Social problems
Counterproductive Strategies
• Ignore the problem
• Export the problem patient to another MD
• Accuse and blame the patient as the PROBLEM
• Solve the problem with drugs/RX.
More counterproductive strategies
• Tell the patient there is nothing wrong
• Tell the patient it is all in their head and see a shrink.
• Tell the patient there is nothing you can do for them.
(Haas LJ. Am Fam Physician. 2005;72:206308.)
Reactions to Difficult Patients Interactions
• Anger that you have to see the patient when there are really sick people to treat.
• Guilt that you as a healthcare professional hate the patient.
• Fear that you will not be able to handle his/ her problems and how they will react.
• A sense of failure that you will not be able to help this patient no matter how hard you try

5/9/2016
8
“Drug‐Seeking” Patients
• Humanitarian perspective‐may still need to treat with opioid in some patients if it is obvious that it is the most effective treatment‐but try to mitigate risks.
• Try not to call them “drug‐seeking”—stigmatizes and creates immediate prejudice of other staff.
• Don’t fixate on whether you believe them
• Help solve the problem, not stand in judgment
• Come in, sit down (not stand over them), face to face conversation.
• Focus on the treatment plan• Can be honest about your
concern about them, risks , and your duty to give them the best care
• Important to frame as giving good care, not trying to withhold something from them.
Problem in certainty:1. Can never be sure how much pain they are in. 2. Being in pain and misusing opioids are not mutually exclusive
Can be 50%/50%, 10%/90% , 90%/10%, etc.3. Prescription drug monitoring system may help
Exceptions: drugs through VA, Military system, mail order prescriptions,or can go across state lines to fill other prescriptions
Approaches:
Butterfield S. Dealing with drug‐seeking behavior. How to handle opioids and some of the patients who take them From the February ACP Hospitalist, copyright © 2014 by the American College of Physicians http://www.acphospitalist.org/archives/2014/02/coverstory.htm?print=true#sb1
Difficult Patient Personality StereotypesPersonality Characteris
ticsMeaning of Illness
EvokeCountertransference
Intervention
Dependent NeedyDemandingClingyUnable to reassure self, seeks reassurance from others.
Threat of abandonmentMay affect fear of becoming well and loosing Doc.
Initially positive, feel powerful and neededThen: Aversion, overwhelmed,annoyed, may try to avoid the patient.
Reassure within limitsSchedule visits (even “appointment” for approximate rounding time in hospital)Limits on expectations Reward independence that is constructiveAvoid tendency to withdraw from patient.
Obsessional Meticulous,likes to feel in control
Loss of control over body, emotions,impulses
May admire; when extreme: anger—”battle of wills”.
Try to set routine. Give patient choices to increase sense of controlGive detailed information and “homework”, foster collaborative approach.
Narcissistic Arrogant,devaluing , vain, demanding
Threat to self concept of perfection and invulnerabilityShame evoking.
A wish to counter‐attack, angerFeelings of inferiority, or feeling of status of working with an important patient.
Resist the desire to challenge patient’s entitlement.Channel it into partnership that acknowledges entitlement to good clinical care but not to unrealistic demands.Humble stance, provide opportunities for the patient to show off. Offer consultations if appropriate.
Groves JE. Taking Care of the Hateful Patient. NEJM. 298(16)883‐887. April 20, 1978Groves MS, Muskin PR Psychological Responses to Illness In Levenson JL.Textbook of Psychosomatic Medicine . American Psychiatric Press 67‐88. 2005
Groves JE. Taking Care of the Hateful Patient. NEJM. 298(16)883‐887. April 20, 1978Groves MS, Muskin PR Psychological Responses to Illness In Levenson JL.Textbook of Psychosomatic Medicine . American Psychiatric Press 67‐88. 2005
Personality Characteristics
Meaning of illness
Evoke Countertransference
Intervention
Histrionic EntertainingMelodramaticFlirtatious, seductive
Loss of love, or attractiveness
Anxiety, impatience, erotic, may find patient attractive
Strike a balance between warmth and formalityClear boundaries, do not confront head on. Encourage patient to discuss fears.
Masochistic “Perpetual victim”Self‐sacrificing martyr
Conscious or unconsciouspunishment
Anger, hate frustration, helplessness
Avoid excessive encouragementShare patient’s pessimismSuggest patient consider treatment as another burden to endure, and it’s positive effect on loved ones.
Paranoid Guarded mistrustful, sensitive to slights
Proof that world is against patient. Care is invasive and exploitative
Anger, feeling attached or accused, may become defensive.
Avoid defensive stance, acknowledge patient’s feelings without disputing themAvoid excessive warmth, do not confront irrational fears.
Schizoid Aloof, socially awkward
Fear of intrusion
Little connection to patient, difficult to engage
Respect patient’s privacy, gentle quiet interest in the patient. Encourage routine and regularity.
Difficult Patient Personality Stereotypes continued
Groves JE. Taking Care of the Hateful Patient. NEJM. 298(16)883‐887. April 20, 1978Groves MS, Muskin PR Psychological Responses to Illness In Levenson JL.Textbook of Psychosomatic Medicine . American Psychiatric Press 67‐88. 2005
Perpetrator Characteristics
ClinicallyConfused
Anti-Social/Angry Socially
IsolatedIntoxicated Frustrated Distressed
/Frightened

5/9/2016
9
CYCLE OF AGGRESSION
• Patient Stress / Loss
• Unmet Needs / Expectations
• Relief
• Anxiety Decreased
• Feelings of Power /Control
• Assaultive Behavior
• Anxiety Converts to Anger
• Frustration
• Anxiety Aroused
• Feelings of
Powerlessness and
Hopelessness
• Anxiety Increases
12
3
6
9
From Lt. Cynthia Coates, URMC Security Services
Warning Signs‐Phase I
• Red face• Pacing• Scowling or sneering• Crossing arms and legs• Tenseness of muscles/clenched jaw• Sweating• Trembling or shaking• Rigid posture• Exaggerated gestures• Glaring eye contact• Exaggerated gestures• Clenching of fists and teeth• Statements of fear of losing control
From Lt. Cynthia Coates, URMC Security Services
DO• Show respect
• Personalize interaction
• Validate feelings
• Offer apologies
• Project positive outcome
• Ask questions
• Hear them out
• Provide choices
• Problem solve/solutions
• Establish behavior plan for identified risks
• Follow through on what you say you will do for them
DON’T• Pass judgment
• Avoid involvement
• Dismiss or minimize
• Cite rules
• Out talk them
• Back them into a corner
• Leave them hanging
From Lt. Cynthia Coates, URMC Security Services
Defuse Phase I Warning Signs‐Phase II
• Verbally abusive• Speaks and/or complains loudly• Uses profanity/sexual comments• Boasting of prior violence• States he/she will lose control• Challenges authority• Appears to be under the influence of drugs and/or alcohol• Makes a mess, scatters clothes or objects• Blames others for his/her problems, error or mistakes• Communicates unrealistic and unnecessary demands for
service
From Lt. Cynthia Coates, URMC Security Services

5/9/2016
10
Defuse Phase II
DO• Speak calmly and clearly• Respect personal space• Project confidence• Be aware and alert• Set limits/redirect• Contain the person• Remove potential weapons• Remove others• Get assistance• Remove yourself if you’re
the target• Mobilize resources
DON’T• Enter into argument
• Touch or get too close
• Turn your back
• Tell them to “Calm down”
• Think you can handle it yourself
• Allow your ego to rule
• Talk to large groups of people
From Lt. Cynthia Coates, URMC Security Services
Warning Signs‐Phase IIISignificant change in baseline activity
Hyperactivity:
• Threatening gestures
• Throws objects down, banging, kicking walls or furniture
• Vicious cursing
• States there is “nothing to lose”
• Develops plan or makes clear, concise threat
From Lt. Cynthia Coates, URMC Security Services
De‐Escalation Concepts
• “Calming the patient” has dominant‐submissive connotation
• Contemporary goal: “helping the patient calm himself”—a form of treatment, help patient find internal locus of control
• 4 main objectives:1. Ensure safety of patient, staff and others in the area2. Help patient manage his emotions, distress, and maintain or regain
control of his behavior3. Avoid use of restraint when at all possible4. Avoid coercive interventions that escalate agitation
• If unable to engage in conversation ‐may be on edge of new or repeated violence (e.g. Phase III) Different management, safety issues of imminent risk, but remember compassion and respect.
10 Domains of De‐Escalation
1. Respect Personal Space of patient and yourself. (2 arm’s lengths)
2. Do Not be Provocative (avoid Iatrogenic Escalation)– Humiliation of patient needs to be strongly avoided.Body Language: – Stand at angle to patient (to not appear confrontational),– No clenched fists– Hands visible.– Avoid excessive eye contact– Avoid arm folding or turning away.– Body language should be congruent with words (otherwise seems
insincere)3. Establish Verbal Contact and 1 person verbally interacts
4. Be Concise, and keep it simple, repetition may be needed.
5. Identify Wants and feelings –Use “Free information” (trivial things patient says, his body language or even past encounters with patient) to identify wants and feelings.
Richmond JS et al. Verbal De-escalation of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA De Escalation Workgroup. Western Journal of Emergency Medicine.Vol XIII, No 1. 17-25. Feb 2012.

5/9/2016
11
10 Domains of De‐Escalation (cont’d)
6. Listen Closely to what patient is saying: – Active Listening. – Use “Miller’s Law”‐ assume patient’s point is truth and try to
imagine what it could be true of.7. Agree or Agree to Disagree:
– “Fogging” is empathic behavior in which one finds something of patient’s position upon which to agree.
8. Lay down Law and Set Clear Limits:– Establish basic working conditions. – Must be reasonable and done in respectful manner. – Coach patient how to stay in control
9. Offer Choices and Optimism.– Broach subject of medications. – Be optimistic and provide hope.
10. Debrief the patient and staff.
Conclusions:Step One in Managing Difficult Patients
Interactions: Understand Yourself
• Be aware of your negative feelings toward certain types of patients.
• Understand what it is that upsets you about these patients.
• Realize you are not a “bad” clinician because you feel antipathy toward the patient.
• Recognize your not alone if having trouble dealing with difficult pts.
Step Two: Understand the patient
• Difficult behavior is a form of communication.
• There are legitimate fears, and needs behind the demands and complaints.
• Behind the labels: There is terrible pain.
Take Home Messages
• Negative reactions constitute important clinical data.
• Awareness and responsible use of these negative reactions can facilitate better understanding, care and improve management.
Grove J. N Eng J Med. 1978: 298; 883.

5/9/2016
12
Need both:PersonalAndOrganizational interventions to beeffective
Change in Paradigm
• We currently are acting under the belief (illusion?) that it is actually possible to do all we’re expected to do.
Paradigm shift:1. Accept that everything expected from all sources is individually
impossible to do2. How can we achieve all “boxes checked” to satisfy evaluators?3. “Satisficing” (Herbert Simon, Nobel Prize winner) [combination
of satisfy + suffice]– For lesser priority decisions: Not getting the very best option but one
that is good enough. Cost‐benefit analysis between effort and benefit
4. High priority decisions are different—>can continue to invest pursuit of excellence there.
Personal Reduction of Stress (Quadrant I)
1. Mindfulness Based Stress Relief (MBSR), Mindful Practice2. Squeegee Breath3. Gratefulness Journaling4. Narrative Medicine to vent past traumas in training and practice5. Celebrate all wins ( “treat yourself like a dog”)6. Acquire leadership, delegation and patient flow skills7. Vision‐Career alignment: What is your ideal patient encounter, procedures, 8. ideal practice? Blue‐sky vision.
What do you need to do to get close to achieving it?9. Ways of dealing with Upset Patients10. Ways to master EMR11. Three Good Things that happen each day (Duke, USF & Georgia Tech)12. Personal Time management13. E‐mail grouping in batches during the day ( e.g.11:30 and 4:30 PM)14. Re‐think how much you need to document.15. Stress reduction classes16. Yoga17. Employee Assistance Program (EAP) 475‐043218. Behavioral Health Partners (BHP) 276‐6900
Seven Essentials of Mindfulness
1. Non‐Judging: Impartial witness to your experience. Observe w/o judging, editing or intellectualizing it.
2. Non‐Striving: No goal other than to be yourself.3. Acceptance: Willingness to see things the way they are.4. Letting Go: Of thoughts, ideas, things, pleasant and
unpleasant.5. Beginner’s Mind: Free of expectations from past
experience. Breath as anchor to present moment.6. Patience: Things must unfold in their own time.7. Trust: In yourself and your feelings. Confidence that things
can unfold in framework that embodies order and integrity.
Kabat‐Zinn, 2004

5/9/2016
13
Squeegee Breath
• 4 part super‐breath (highly concentrated mini‐meditation)
1. Set intention‐ that going to release anything that doesn’t need to be here. Become calm, relaxed, completely present.
2. Breathe in. Hold in….two….three
3. Breathe out and release. Hold out…two…three
4. Smile
Stand up practice
To clean the window of your awareness
Drummond D. 2014.
Transform native behavior into intentional
Personal Recharge (Quadrant II)
1. Honoring Self2. Boundary ritual between work and home
Car ride home relaxing music, mindful breathingMr. Rogers routine ( yeah, the sweater, the slippers !)
3. Schedule the things you are going to do outside of work. Get them on your calendar that you can see at work.
4. Recreation and Exercise Start small and sustainable ‐simple, frequent and fun
5. Care for your body and its physical needs6. Bucket List activities
Write them down and start doing the list.
7. Regular Vacation: Don’t run yourself ragged before you decide to take off.
8. Spirituality: Put work within the larger context.