Embed Size (px)
Citation preview

1131-Diodrast Studies in Unilateral Renal DiseaseBy JEROME B. BLOCK, M.D., GERALD J. HINE, PH.D., AND
BELTON A. BURROWS, M.D.
WTith the technical assistance of Valentine Bikerman, B.S.
U NILATERAL renal disease is an infre-quent cause of hypertension, occurring in
less than 2 per cent of unselected hyperten-sive patients.' Such a small proportion ofpatients with unilateral renal disease respondto removal of the affected kidney that hyper-tension per se is not considered an indicationfor nephrectomy. Hypertensive patients withunilateral renal arterial stenosis form an evensmaller group, but their response is good tosurgery performed before the development ofextensive vascular disease involving the con-tralateral kidney.3' 4 Ureteral catheterizationor aortography may lead to earlier diagnosisand better surgical results in this conidition,but associated technical difficulties, inconveni-ence, and complications of these procedureshave limited their use in screening hyperten-sive patients in the incipient stages of thedisease.5' 6A simple and innocuous technic has been
developed that demonstrates the excretion ofI131-Diodrast by each kidney.7 This radio-scopic method has been modified for the earlydiagnosis of unilateral renal disease by theuse of carrier Diodrast and a ratiometer.i Inthis report the findings with I131-Diodrast arecompared with the results of intravenous pyel-ography, ureteral catheterization, and surgi-eal exploration or autopsy.
From the Robert Dawson Evans Memorial, Massa-chusetts Memnorial Hospitals, the Radioisotope andMedical Services, Boston Veterans AdministrationHospital, and the Department of Medicine, BostonUniversity School of Medicine, Boston, Mass.
Supported by contract no. AT (30-1) 919 betweenthe Atomic Energy Commission and the MassachusettsMemorial Hospitals.
Presented in part at the Thirty-first ScientificSessions of the American Heart Association, SanFrancisco, Calif., October 26, 1958.
Circulation, VoTl,me XXII, November 1960
Materials and MethodsTwo hundred and twentv-six hypertensive pa-
tients were studied with both 131-Diodrast andintravenous pyelography; 49 of these were alsostudied by retrograde ureteral catheterization.When catheterization demonstrated a decrease insodium concentration (at least 15 per cent) andvolume (at least 50 per cent) of the urine fromone kidney as compared with the other kidney,the results were interpreted as a "positive How-ard test."9 All other technically satisfactory re-sults were termed negative; when insuffieient urinewas obtained from one kidney, the study wastermed unsatisfactory. Forty were surgically ex-plored: of these, 15 were subjected to unilateralnephrectomy, 3 underwent unilateral adrenalee-tomy, and the remainder submitted to lumbodorsalsympathectomy and renal biopsy. Except as notedin the text, all patients were studied with I131-Diodrast prior to surgical exploration.
Patients drank about a quart of water in thehour prior to the I131-Diodrast studies. They werethen placed in a sitting position with radiationdetectors directed horizontally at the renal areasnormal to the skin surface. Monitoring sites wereselected with the aid of available x-ray films. Anintravenous infusion of 300 mil. of 5 per centdextrose in water containing 1 Gmii. of Diodrastwas administered at a rate of 2 nil. per minutethroughout the study; 2.5 ml. of 35 per centDiodrast solution (1 Gm.) were injected directlyinto the rubber tubing of the infusion; this wasfollowed by the rapid injection of 20 mierocuriesof I13l-Diodrast (approximately 0.1 mg.).*The radioactivity that appeared in the separate
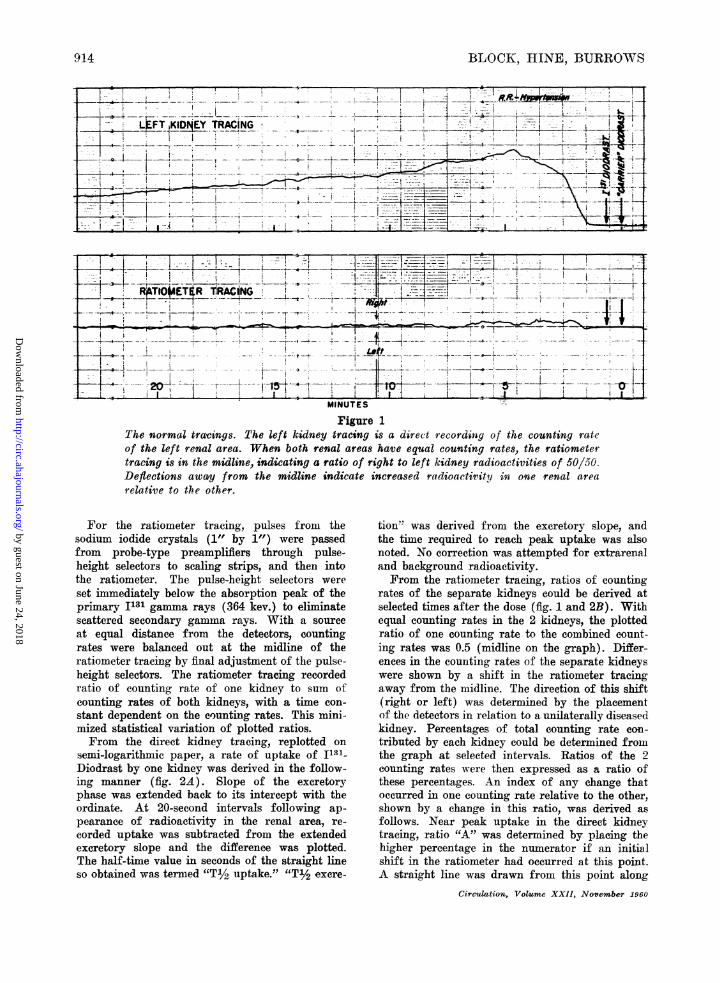
renal areas was measured with 2 collimated scin-tillation detectors, a counting rate meter, a ratiom-etert and a dual-ehannel linear recorder.t Thecounting rate in one renal area was recorded onone side of the recorder (the direct kidney trac-ing) and the ratio of the counting rate in onerenal area to the total counting rate in both renalareas on the other side of the recorder (the ratiom-eter tracing) (fig. 1).
*Abbott Laboratories, Oak Ridge, Tenn.tBaird-Atomic, Inc., Cambridge, Mass."Texas Instrument Co., Houston, Tex.
913
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
B4OCKO, HINE, BURROWS
Figure 1
The normal trarings. The left kidney tracing is a direct recording of the counting rateof the left renal area. When both renal areas have equal counting rates, the ratiometertracing is in the midline, indicating a ratio of right to left kidney radioactivities of 50/50.
Deflections away from the midline indicate increased radioactivity in one renal area
relative to the other.
For the ratiometer tracing, pulses from thesodium iodide crystals (1" by 1") were passedfrom probe-type preamplifiers through pulse-height selectors to scaling strips, and then intothe ratiometer. The pulse-height selectors were
set immediately below the absorption peak of theprimary I131 gamma rays (364 kev.) to eliminatescattered secondary gamma rays. With a sourceat equal distance from the detectors, countingrates were balanced out at the midline of theratiometer tracing by final adjustment of the pulse-height selectors. The ratiometer tracing recordedratio of counting rate of one kidney to sum ofcounting rates of both kidneys, with a time con-
stant dependent on the counting rates. This mini-mized statistical variation of plotted ratios.From the direct kidney tracing, replotted on
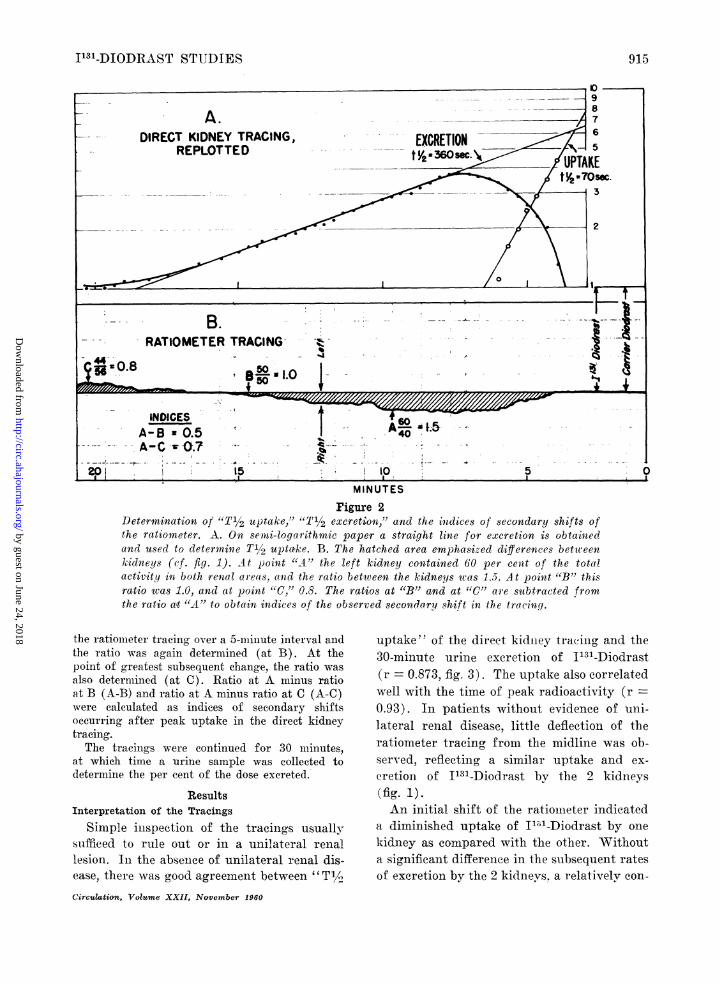
semi-logarithmic paper, a rate of uptake of I"'1-Diodrast by one kidney was derived in the follow-ing manner (fig. 2A). Slope of the excretoryphase was extended back to its intercept with theordinate. At 20-second intervals following ap-pearance of radioactivity in the renal area, re-
corded uptake was subtracted from the extendedexcretory slope and the difference was plotted.The half-time value in seconds of the straight lineso obtained was termed "'T½/2 uptake." "T1/2 exere-
tion"' was derived from the excretory slope, andthe time required to reach peak uptake was alsonoted. No correction was attempted for extrarenaland background radioactivity.From the ratiometer tracing, ratios of counting
rates of the separate kidneys could be derived atselected times after the dose (fig. 1 and 2B). Withequal counting rates in the 2 kidneys, the plottedratio of one counting rate to the combined count-ing rates was 0.5 (midline on the graph). Differ-ences in the counting rates of the separate kidneyswere shown by a shift in the ratiometer tracingaway from the midline. The direction of this shift(right or left) was determined by the placementof the detectors in relation to a unilaterally diseasedkidney. Percentages of total counting rate con-
tributed by each kidney could be determined fromthe graph at selected intervals. Ratios of the 2counting rates were then expressed as a ratio ofthese percentages. An index of any change thatoccurred in one counting rate relative to the other,shown by a change in this ratio, was derived as
follows. Near peak uptake in the direct kidneytracing, ratio "A" was determined by placing the
higher percentage in the numerator if an initialshift in the ratiometer had occurred at this point.A straight line was drawn from this point along
Circukltion, Volume XXII, November 1960
jKPtE.. .--_-tAACING- +.
a-
S
914
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
1131-DIODRAST STUDIES91
10 5I ~~~MINUTES
Figure 2Deter-mination of "T12 uptake,' "T' 2 excreti'on,"' and the indices of secondary shifts ofthe ratiometer. A. On semii-logar-ithmic paper a straight line for excretion is obtainedand used to determine Ti/2 upta,ke. B. The hatched area emphasiZed differences betweenkidneys (cf. fig. 1). At point "A"' the left kidntey contained GO per cen;t of the. totalactivity in both rienal areas, and the ratio between the kidneys was 1.5. A -t poinzt "B" thisratio was 1.0, and at point "C," 0.8. The ratios at "B" and at "C" are subtracted fromthe ratio at "A" to obtain indices of the observed secondary shift in the tracing.
the ratioiimeter tracing, aver a 05-minute interval andthe ratio was again determined (at B). At thepoint of greatest subsequent change, the ratio wasalso determiined (at C). Ratio at A minus ratioat B (A-B) and ratio at A minus ratio at C (A-C)were calculated as indices of secondary shiftsoccurring after peak uptake in the direct kidneytracing.The tracings were continued for 30 minutes,
at which time a urine sample was collected todeterm-ine the p-er cent of the dose excreted.
ResultsInterpretation of the Tracings
Simple inispection of the tracings usuallysufficed to rule out or in a unilateral reniallesion. In the absencee of unilateral renal dis-ease, there was good agreemenit betweenr "Ti2.Circulation, Volume XXII, November 1960
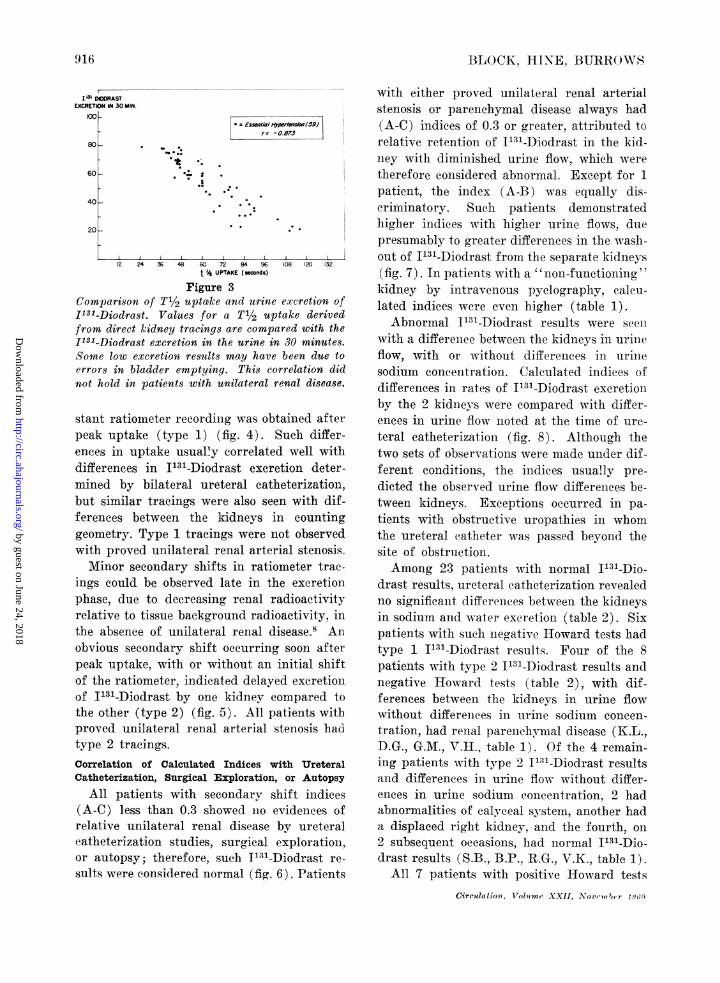
uptake" of the direct kidnley tracinig and the30-minute urinle excretioni of 1131-Diodrast(r = 0.873, fig. 3). The uptake also correlatedwell with the time of peak radioactivity (r0.93). In patients withonut evidence of uni-lateral renal disease, little deflection of theratiometer tracing, from the midline was ob-served, reflecting, a similar uptake and ex-cretioni of I'31-Diodrast by the 2 kidneys(fg.1)An initial shift of the ratioinieter indicated
a diminished uptake of I1"'-Diodrast by onlekidney as compared with the other. Withouta significant differenice in the subsequent ratesof excretion by the 2 kidneys. a relatively cona-
915
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
BLOCK, HINE, BURROWS
* £mutio,/HyperMAiOR (59)r= -0.673
12 24 36 48 60 72 84 96 108 10 132t % UPTAKE (sconds)
Figure 3Comparison of T1/2 upta'ke and urine excretion ofI'31-Diodrast. Values for a T1/2 uptake derivedfrom direct kidney tracings are compared with the1131-Diodrast excretion in the urine in 30 minutes.Some low excretion results may have been due toerrors in bladder emptying. This correlation didnot hold in patients with unilateral renal disease.
stant ratiometer recordinig was obtained afterpeak uptake (type 1) (fig. 4). Such differ-ences in uptake usually correlated well withdifferences in I'31-Diodrast excretion deter-mined by bilateral ureteral catheterization,but similar tracings were also seen with dif-ferences between the kidneys in countinggeometry. Type 1 tracings were not observedwith proved unilateral renal arterial stenosis.Minor secondary shifts in ratiometer trac-
ings could be observed late in the excretionphase, due to decreasing renal radioactivityrelative to tissue background radioactivity, inthe absence of unilateral renal disease.8 Anobvious secondary shift occurring soon afterpeak uptake, with or without an initial shiftof the ratiometer, indicated delayed exeretioiiof I131-Diodrast by one kidney compared tothe other (type 2) (fig. 5). All patients witbproved unilateral renal arterial stenosis hadtype 2 tracings.Correlation of Calculated Indices with UreteralCatheterization, Surgical Exploration, or Autopsy
All patients with secondary shift indices(A-C) less than 0.3 showed ilo evidenees ofrelative unilateral renal disease by ureteralcatheterization studies, surgical exploration,or autopsy; therefore, sueh T131-Diodrast re-
sults were considered normal (fig. 6). Patients
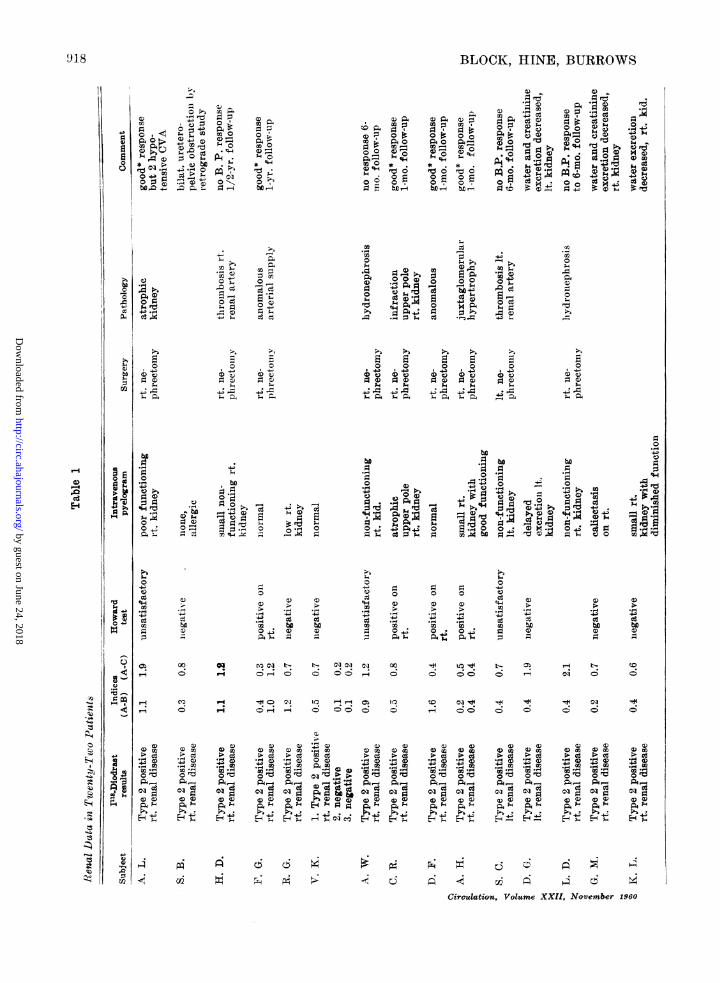
with either proved unilateral renal arterialstenosis or parenchymal disease always had(A-C) indices of 0.3 or greater, attributed torelative retention of J131-Diodrast in the kid-ney with diminished urine flow, which weretherefore considered abnormeal. Except for Ipatient, the index (A-B) was equally dis-criminatory. Such patients demonstratedhigher indices with higher urine flows, duepresumably to greater differences in the wash-out of I131-Diodrast from the separate kidneys(fig. 7). In patients with a "'non-functioning 'kidney by intravenous pyelography, caleu-lated indices were even higher (table 1).Abnormal I131-Diodrast results were seeni
with a differeiiee between the kidneys in urineflow, with or without differenees in urinesodium concentration. Calculated ilndices ofdifferences in rates of 131-Diodrast exeretionby the 2 kidneys were compared with differ-ences in urine flow noted at the time of ure-teral catheterization (fig. 8). Although thetwo sets of observations were made under dif-ferent conditions, the indices usually pre-dicted the observed urine flow differenees be-tween kidneys. Exceptions occurred in pa-tients with obstructive uropathies in whomthe ureteral catheter was passed beyond thesite of obstruction.Among 23 patients with normal 1131-Dio-
drast results, ureteral catheterization revealedno significant differences between the kidneysin sodium and water excretion (table 2). Sixpatients with such negative Howard tests hadtype 1 IT31-Diodrast results. Four of the 8patients with type 2 I131-Diodrast results andnegative Howard tests (table 2), with dif-ferences between the kidneys in urine flowwithout differences in urine sodium concen-tration, had renal paren-chyinal disease (K.L.,D.G., G.M., V.H., table 1). Of the 4 remain-ing patients with type 2 I111-Diodrast resultsand differenees in urine flow without differ-ences in urine sodium conieentration, 2 hadabnormalities of calyeeal system, another hada displaced right kidney, and the fourth, on2 subsequent occasions, had normal IT31-Dio-drast results (S.B., B.P., R.G., V.K., table 1).
All 7 patients with positive Howard tests
Circulation., Tl'olnme XXII, N?Xoccn r 1)4')
I~~~~~~~~I M DIODRAST
EXCRETION IN 30 MIN.
c0
80 .
60
40
20
I
916
ft 0 %. t .,.. .
t
*4
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from

1131-DIODRAST STUDIES
... . , . *~~- E. -."Smll"LeftKidny
LEFT KIlDNEY TRACING
t~~~~~~~~~~~~~~~~~~~~~~~__..........................
i -- - - - - A- --tI I
- I i ,, ; ii |-wMINUTES
]Figure 4The type 1 tracing, indicating an initial shift in the ratiometer. Approximately 60 percent of the radioactivity was in the right renal area.
MINUTES
Figure 5The type 2 tracing, indicating a secondary shift in the ratiometer. Both diminisheduptake and delayed excretion of I131-Diodrast by the affected kidney was observed(ef fig. 4).
Circulation, Volume XXII, November 1960
- RATtOMTER TRACING-
- ? -- - - - - - - -- -- 4- -F-- - - - - * - - - - - - -- -- -'
- T o- - *'- '- g- - ~ .i -0---|------
---~~ ii- 20 --I ----'-+ -llK' -;-|---5- - ---
917
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
BLOCK, HINE, BURROWS
4-3 000 04
I~S
"0
)Z9-
>4 0
90
t00 +ot*4MC
>4
n P. m ;z01) 0))
_ .-0
_~ Ca ..090
* 5i X-4-- ;. 9e
>-4
-0)
*,s4.04.; IS.
04
P4 P4 9rc0D
q44 4'go . ,'4
-')
96 0e- 0 0 (D ~
.0
02 'C
oA8g
O 0)s9 0 *9 0w
,,
04-o90)440
be
0
0)
04:
A94
3-Cd
'40
0Qx0;4
.0
90),4
.0)
0
4.)~~~~~~ct4
b*~~~~~~~0rbiO-,~) 9 $~-4 v 0IW r9
0
O)
be be
0 ;>0
944.,
;^- P4>L40 0
~~9 I-
w F) 0 0
'4-4 0) 0) 0) '4-4
-4 > - 4
4Q OQ
ce .,. -. - 4 > =0 4; 0 41 0 o' be.40-I 4
0) 0
'4 -4bo be01). .
3-
OK ciN t s N > Ct t- , t-,. ° -i 0 0 00
Cd (: P- Cs o d ce c ce ~ > d ce O. ce ce > d ce >.0-0I'-44 14 'm4 -4 -4
0)0) 0) 0) 0 0) 4.) ) a)0) 0) 0CD
)0m -O(D
_0P_
01o_ ce0_Ae c;l 03 Cs Ca*R CazA,_ C'c_pd_ A_, c_ cor_
pq $4F4 N4 ;I tOto X, 9 9 9 9 OlNN NmNNNm0)C) CD 0D 0CD Q ) 0) 0)V
P,6 '- * *P4 44; E-4P P''
A t V 4. i¢ V 6¢ Q
Circulation, Volume XXII, November 1960
91.8
'-4
0
E-4
P'.14.0)(3m.'4
90
i0
0-
4-.
1w. i
9
0)2
a¢
6 6P. P4
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
I131-DIODRAST STUDIES
a-~~~~~~~~~~~~4D
I 0~".
34 Lc r 3r
2)
.
Ce o
*~4P l X,3
M Cs cdO Hs.H .0 cd o +4e ce0 Cs
a) a) 0 4z .O e2) -4'a 2-() 0 43kD C) -k~..-q P +4Z Ce~', . . k 1-4 C eaP- 0 Cea-" 4-
0 0 0 0 0
OQ
) A 2)
V Q)
P.
-4:A . .,'aA -
Ce
0
0
6.(6
aCat
0H ,- a
04,o9 E.E ¢
Pa4 ;-4a0 0
0 0 C °
2) 2) "64 q64 2)
4. 4.4 .-6.P.
.m 5 ce Ce
o *4. o .,;, 9 9o ,.04 vA = Ao
21)P.
bIX(2)
O 0
cqi < o
(2) 2) 2L) 2)
MX a m (D m2 Qaa) OQ4)C oce oce ce Ce
.a ) - a .4 -
-. a-qct cecq cq w cqN N
A Q , ,Ap
HZ H -sEHw E E
2)W
.r.4
33.-c6a M
-4A--4ce
CqI =(L) LP 6.'
C-
(2)a.
P4-
HOWARD TEST
I/ndces (A-B) (A-C)
0.0 0000000000000 000000000
0.1 00000000 000000000000
0.2 000000 000000
0.3 @000 @000
0.4 *-xoooo 0
0.5 0oo0o *o
0.6 0 000
0.7 0 xooo
0.8 x 0
09 X o X
10-14 *xo x
_5_902.0- 2.5 x x
SURGERY or AUTOPSY
(A-B) (A-C)000 00000000000 00000000000
_ _ .-
0000 00000000
@000000 000000
_00
*00
00
@~~00
soo
* V ldec b*-&,*ey.eo_'ee
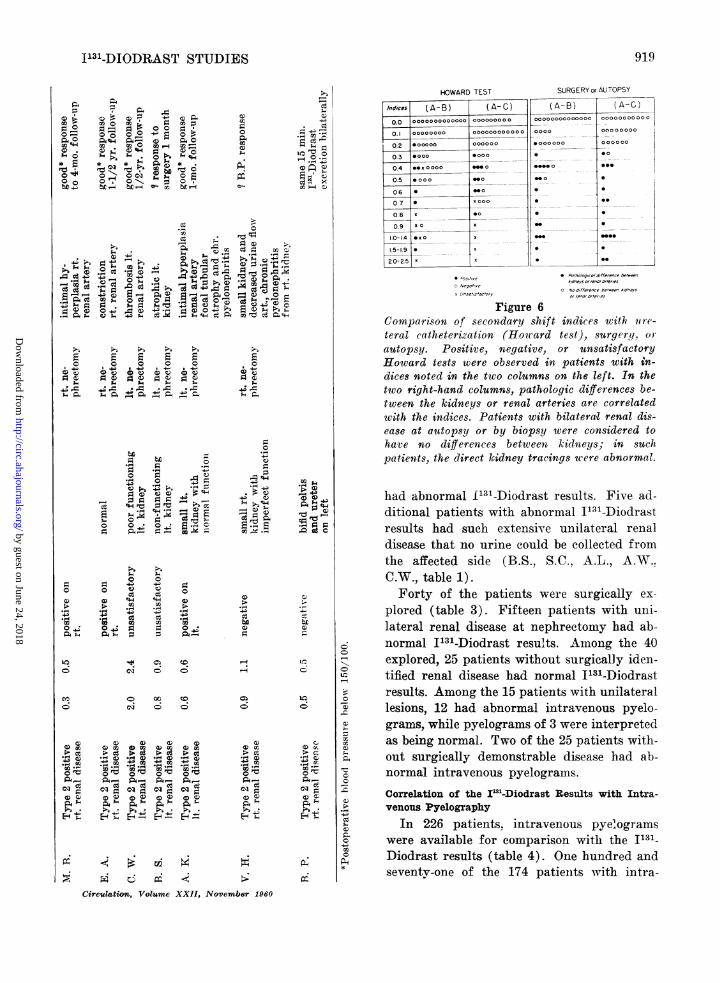
Figure 6Comparison of secondary shift indices with iun-c-teral catheterization (Howard test), surgery, or
autopsy. Positive, negative, or unsatisfactoryHoward tests were observed in patients with in-
dices noted in the two columns on the left. In thetwo right-hand columns, pathologic differences be-tween the kidneys or renal arteries are correlatedwith the indices. Patients with bilatera'l renal dis-ease at autopsy or by biopsy were considered tohave no differences between kidneys; in suchpatients, the direct kidney tracings were abnormal.
had abnormal f131-Diodrast results. Five ad-ditional patients with abnormal I131-Diodrastresults had such extensive unilateral renaldisease that no urine could be collected fromthe affected side (B.S., S.C., A.L., A.W..C.W., table 1).Forty of the patients were surgically ex-
plored (table 3). Fifteen patients with unii-lateral renal disease at nephrectomy had ab-normal I131-Diodrast results. Among the 40explored, 25 patients without surgically idell-tified renal disease had normnal I131-Diodrastresults. Among the 15 patients with unilaterallesions, 12 had abnormal intravenous pyelo-grams, while pyelograms of 3 were interpretedas being normal. Two of the 25 patients with-out surgically demonstrable disease had ab-normal intravenous pyelograms.
Correlation of the I'2-Diodrast Results with Intra-venous Pyelography
In 226 patients, intravenous pyelograms
were available for comparison with the I131-Diodrast results (table 4). One hundred andseventy-one of the 174 patients with intra-
OC0
2)
0
~C
6;rir
I-
0
r_O
Q)P
ct-
--;,P.,
Cirultion1tz, Volume XXII, November 1960
919
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
BLOCK, HINE, BURROWS
MINUTES
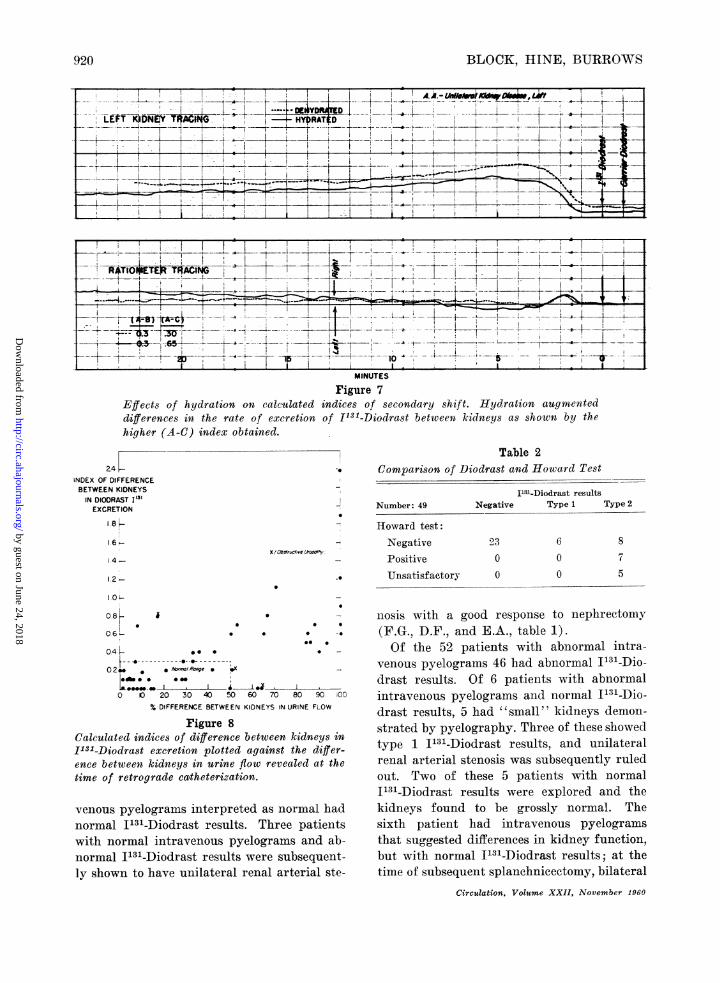
Figure 7Effects of hydration on calculated indices of secondary shift. Hydration augmenteddifferences in the rate of excretion of 1131-Diodrast between kidneys as shown by thehigher (A-C) index obtained.
Table 2-. Comparison of Diodrast and Howard Test24-
INDEX OF DIFFERENCEBETWEEN KIDNEYS
IN DIODRAST I'3'EXCRETION
1.8
X (OstWruct've k.ro5hy4.-
1 2-
OL
- Number: 49 Negative
Howard test:- Negative 23
Positive 0
* Unsatisfactory 0
I113-Diodrast resultsType 1
6
00
0.8 * - nosis with a good response to nephrectomy06 . * . (F.G., D.F., and E.A., table 1).04-e v Of the 52 patients with abnormal intra-
O2* t*M-;R-Ronge venous pyelograms 46 had abnormal
1- -0 *" 00 drast results. Of 6 patients with abnormal0 20 30 40 50 60 70 80 K iOO intravenous pyelograms and normal I131-Dio-
% DIFFERENCE BETWEEN KIDNEYS INURINE FLOW drast results, 5 had "'small'" kidneys demon-Figure 8 strated by pyelography. Three of these showed
Calculated indices of difference between kidneys inI31-Diodrast excretion plotted against the differ- type 1 1131-Diodrast results, and unilateral
ence between kidneys in urine flow revealed at the renal arterial stenosis was subsequently ruledtime of retrograde catheterization. out. Two of these 5 patients with normal
I131-Diodrast results were explored and thevenous pyelograms interpreted as normal had kidneys found to be grossly normal. Thenormal I131-Diodrast results. Three patients sixth patient had intravenous pyelogramswith normal intravenous pyelograms and ab- that suggested differences in kidney function,normal I131-Diodrast results were subsequent- but with normal I131-Diodrast results; at thely shown to have unilateral renal arterial ste- time of subsequent splanchnicectomy, bilateral
Circulation, Volume XXII, November 1960
Type 2
8
7
5
i
920
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
I'31-DIODRAST STUDIES
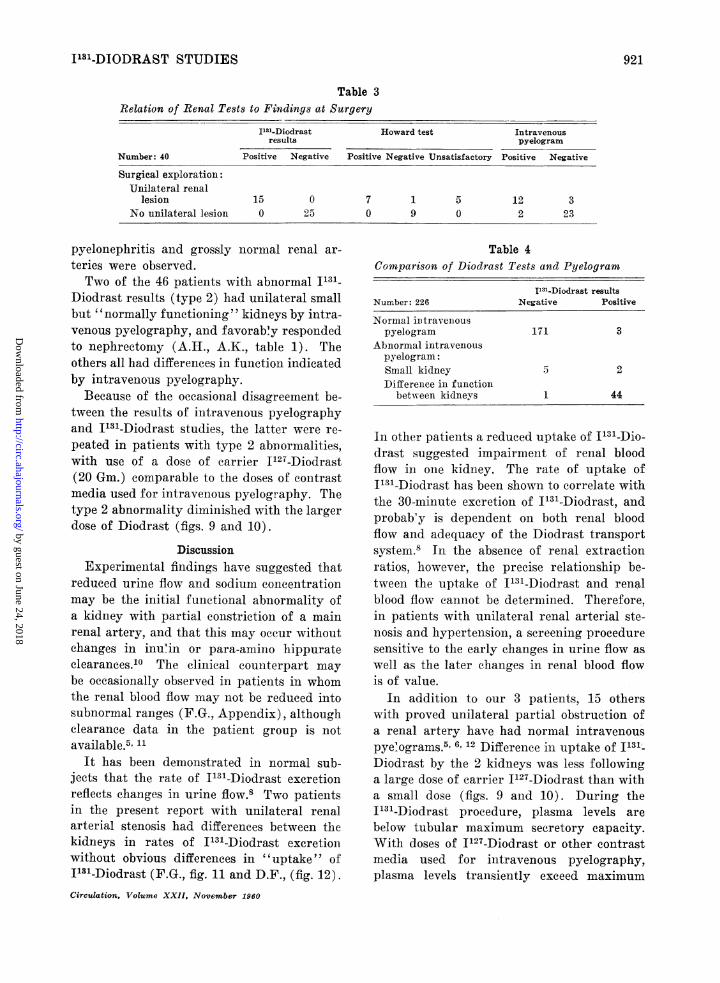
Table 3Relation of Renal Tests to Findings at Surgery
I"1-Diodrast Howard test Intravenousresults pyelogram
Number: 40 Positive Negative Positive Negative Unsatisfactory Positive Negative
Surgical exploration:Unilateral renal
lesion 15 0 7 1 5 12 3No unilateral lesion 0 25 0 9 0 2 23
pyelonephritis and grossly normal renal ar-teries were observed.Two of the 46 patients with abnormal I13_-
Diodrast results (type 2) had unilateral smallbut "normally functioning" kidneys by intra-venous pyelography, and favorably respondedto nephrectomy (A.H., A.K., table 1). Theothers all had differences in function indicatedby intravenous pyelography.
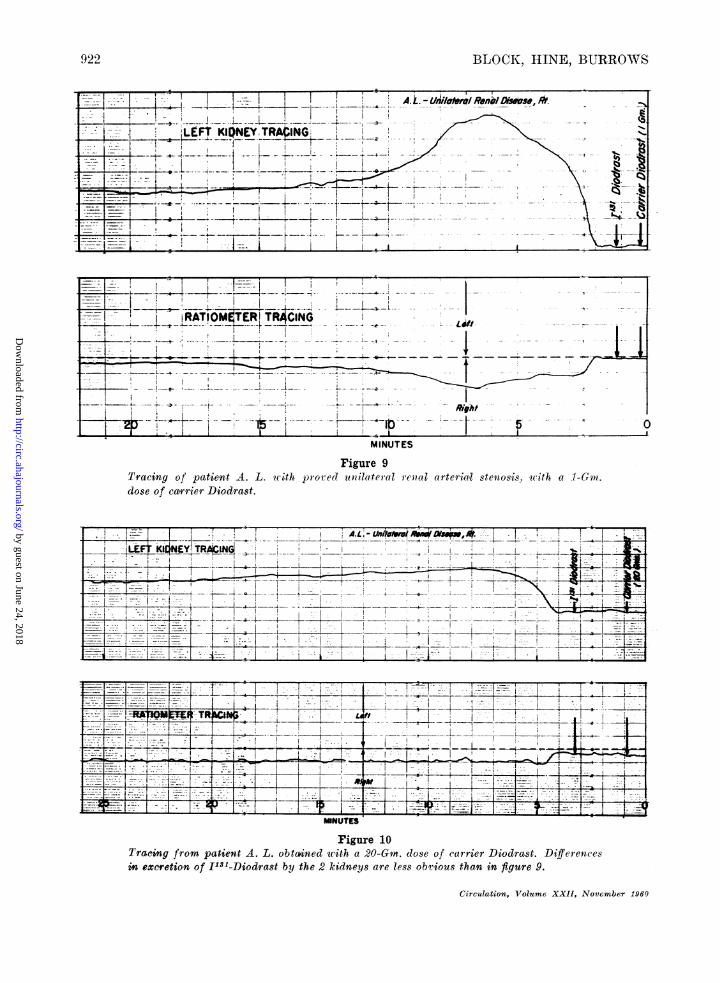
Because of the occasional disagreement be-tween the results of intravenous pyelographyand I131-Diodrast studies, the latter were re-peated in patients with type 2 abnormalities,with use of a dose of carrier J127-Diodrast(20 Gm.) comparable to the doses of contrastmedia used for intravenous pyelography. Thetype 2 abnormality diminished with the largerdose of Diodrast (figs. 9 and 10).
DiscussionExperimental findings have suggested that
reduced urine flow and sodium concentrationmay be the initial functional abnormality ofa kidney with partial constriction of a mainrenal artery, and that this may occur withoutchanges in inun in or para-amino hippurateclearances.10 The clinical counterpart maybe occasionally observed in patients in whomthe renal blood flow may not be reduced intosubnormal raiiges (F.G., Appendix), althoughclearance data in the patient group is notavailable.5' 11
It has been demonstrated in normal sub-jects that the rate of I131-Diodrast excretionreflects changes in urine flow.8 Two patientsin the present report with unilateral renalarterial stenosis had differences between thekidneys in rates of I131-Diodrast exeretioniwithout obvious differences in "uptake" ofI131-Diodrast (F.G., fig. 11 and D.F., (fig. 12).Circulation, Volume XXII, November 1960
Table 4Comparison of Diodrast Tests and Pyelogram
1I31-Diodrast resultsNumber: 226 Negative Positive
Normal intravenouspyelogram 171 3
Abnormal intravenouspyelogram:Small kidney 5 2Difference in function
between kidneys 1 44
In other patients a reduced uptake of I131-Dio-drast suggested impairment of renal bloodflow in one kidney. The rate of uptake ofI'31-Diodrast has been shown to correlate withthe 30-minute excretion of I131-Diodrast, andprobably is dependent on both renal bloodflow and adequacy of the Diodrast transportsystem.8 In the absence of renal extractionratios, however, the precise relationship be-tween the uptake of I131-Diodrast and renalblood flow cannot be determined. Therefore,in patients with unilateral renal arterial ste-nosis and hypertension, a screening proceduresensitive to the early changes in urine flow aswell as the later changes in renal blood flowis of value.
In addition to our 3 patients, 15 otherswith proved unilateral partial obstruction ofa renal artery have had normal intravenouspye&ograms.5 6, 12 Difference in uptake of I's'-Diodrast by the 2 kidneys was less followinga large dose of carrier I127-Diodrast than witha small dose (figs. 9 and 10). During theI'31-Diodrast procedure, plasma levels arebelow tubular maximum secretory capacity.With doses of I'27-Diodrast or other contrastmedia used for intravenous pyelography,plasma levels transiently exceed maximum
921
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
BLOCK HINE, BURROWS
]~~~~~~~~~~ - I- - - F- L --ll
_~~ Right§X
---1- iRATIOiM0TR TRCING
___
MINUTES
Figure 9Tracing of patient A. L. wuith pro red dilateral renaldose of caTrier Diodrast.
arteriaill stenosis, wwith at -1-Gm.
... ___ .__. ______.__ ._ _ ,,_ _.~~~~~~~~~~~~~~~~___
I ~ ~ Fiue10*
Tracing from patient A. L. obta4ned -ith a 20-Gm. dose of ca._rier Diodrast Differencesin excretion of 11'81-Diodrast by the 2 kidneys are less obv-ious than in figure 9.
Circulation, Volume XXII, November 1960
9 2'2
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
1131-DIODRAST STUDIES
MINUTES
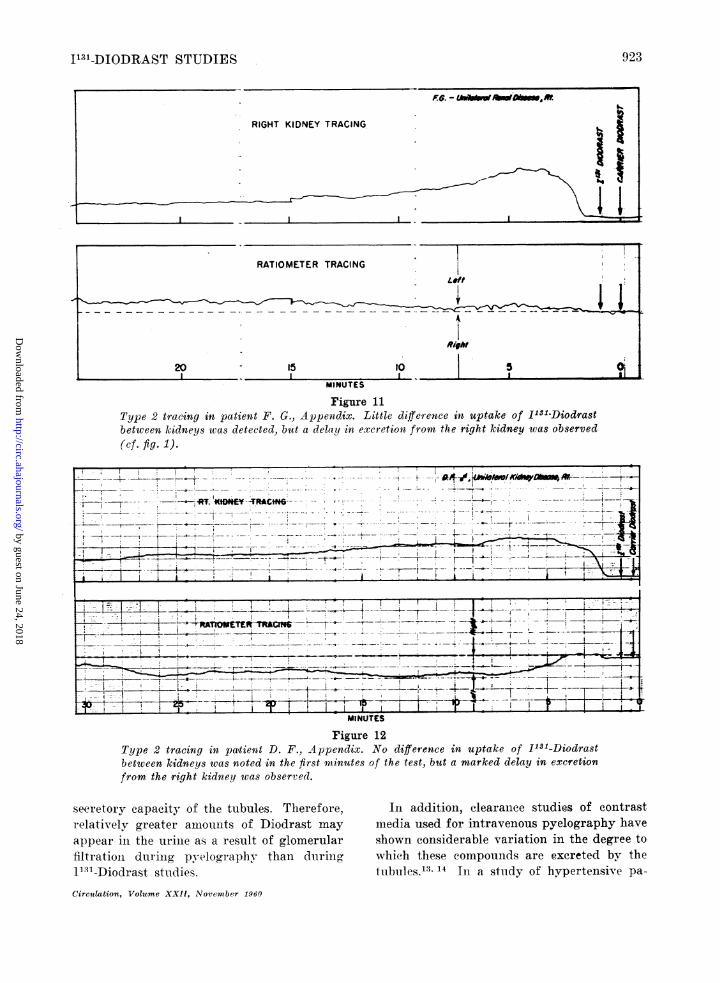
Figure 11Type 2 tracing in patient F. G., Appendix. Little diffeience in uptake of I151-Diodrastbetween kidneys was detected, but a delay in excretion from the right kidney was observed
(cf. fig. 1).
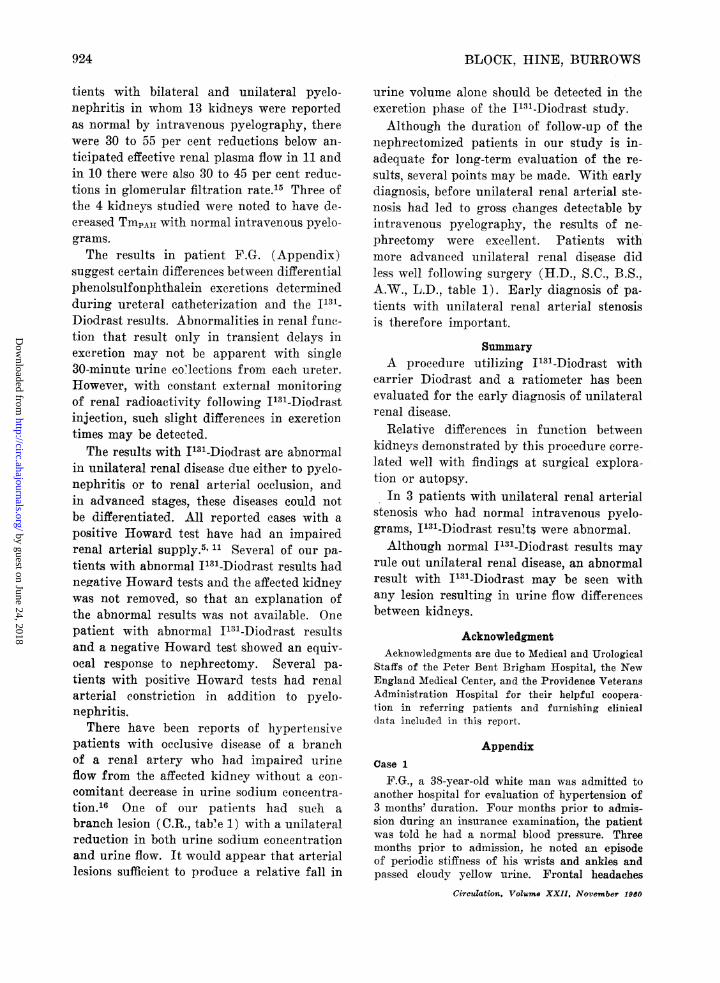
Figure 12Type 2 tracing in patient D. F., Appendix. No difference in uptake of 1131-Diodrastbetween kidneys was noted in the first minutes of the test, but a marked delay in excretion
from the right kidney was observed.
seeretory capacity of the tubules. Therefore,relatively greater amiounlts of Diodrast may
appear in the urinie as a result of glomerularfiltrationl dur ing pyelography than duringI1 31-Diodrast studies.
In addition, clearaniee studies of contrastmedia used for intravenous pyelography have
shown considerable variation in the degree towhich these compounds are excreted by thetubules.13' 14 In a study of hypertensive pa-
Circulation, Volume XXII, November 1960
RATIOMETER TRACING
Ridh
20 15 to 5 0jI I I~1
923
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
BLOCK, HINE, BURROWS
tients with bilateral and unilateral pyelo-nephritis in whom 13 kidneys were reportedas normal by intravenous pyelography, therewere 30 to 55 per cent reductions below an-ticipated effective renal plasma flow in 11 andin 10 there were also 30 to 45 per cent reduc-tions in glomerular filtration rate.15 Three ofthe 4 kidneys studied were noted to have de-creased TmPAI with normal intravenous pyelo-grams.The results in patient F.G. (Appendix)
suggest certain differences between differentialphenolsulfonphthalein excretions determinedduring ureteral catheterization and the I131_Diodrast results. Abnormalities in renal fune-tion that result only in transient delays inexeretion may not be apparent with single30-minute urine co7lections from each ureter.However, with constant external monitoringof renal radioactivity following I131-Diodrastinjection, such slight differences in excretiontimes may be detected.The results with I131-Diodrast are abnormal
in unilateral renal disease due either to pyelo-nephritis or to renal arterial occlusion, andin advanced stages, these diseases could notbe differentiated. All reported cases with apositive Howard test have had an impairedrenal arterial supply.5' 11 Several of our pa-tients with abnormal I131-Diodrast results hadnegative Howard tests and the affected kidneywas not removed, so that an explanation ofthe abnormal results was not available. Onepatient with abnormal I131-Diodrast resultsand a negative Howard test showed an equiv-ocal response to nephrectomy. Several pa-tients with positive Howard tests had renalarterial constriction in addition to pyelo-nephritis.
There have been reports of hypertensivepatients with occlusive disease of a branchof a renal artery who had impaired urineflow from the affected kidney without a con-comitant decrease in urine sodium concentra-tion.16 One of our patients had such abranch lesion (C.R., table 1) with a unilateralreduction in both urine sodium concentrationand urine flow. It would appear that arteriallesions sufficient to produce a relative fall in
urine volume alone should be detected in theexcretion phase of the I131-Diodrast study.Although the duration of follow-up of the
nephrectomized patients in our study is in-adequate for long-term evaluation of the re-sults, several points may be made. With earlydiagnosis, before unilateral renal arterial ste-nosis had led to gross changes detectable byintravenous pyelography, the results of ne-phreetomy were excellent. Patients withmore advanced unilateral renal disease didless well following surgery (H.D., S.C., B.S..A.W., L.D., table 1). Early diagnosis of pa-tients with unilateral renal arterial stenosisis therefore important.
SummaryA procedure utilizing I'31-Diodrast with
carrier Diodrast and a ratiometer has beenevaluated for the early diagnosis of unilateralrenal disease.
Relative differences in function betweenkidneys demonstrated by this procedure corre-lated well with findings at surgical explora-tion or autopsy.
In 3 patients with unilateral renal arterialstenosis who had normal intravenous pyelo-grams, I'31-Diodrast resul-ts were abnormal.Although normal I'31-Diodrast results may
rule out unilateral renal disease, an abnormalresult with I131-Diodrast may be seen withany lesion resulting in urine flow differencesbetween kidneys.
AcknowledgmentAcknowledgments are due to Medical and Urological
Staffs of the Peter Bent Brigham Hospital, the NewEngland Medical Center, and the Providence VeteransAdministration Hospital for their helpful coopera-tion in referring patients and furnishing clinicaldata included in this report.
AppendixCase 1
F.G., a 38-year-old white man was admitted toanother hospital for evaluation of hypertension of3 months' duration. Four months prior to admis-sion during an insurance examination, the patientwas told he had a normal blood pressure. Threemonths prior to admission, he noted an episodeof periodic stiffness of his wrists and ankles andpassed cloudy yellow urine. Frontal headaches
Circulation. Volume XXII, November 1960
924
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
I131-DIODRAST STUDIES
became prominent but there were no other symp-tomns. Thereafter he remained in good healthuntil he consulted his physician concerning anupper respiratory infection, 2 weeks before ad-mission. Because of a blood pressure of 210/120,hospitalization was advised.
There was no history of known cardiovascularor renal disease. The patient's mother was ob-served to have hypertension following a heart at-tack at the age of 71.On physical examination the blood pressure was
180/120 in both arms without postural hypoten-sion. Grade-2 hypertension retinopathy was de-scribed. The heart and lungs were normal. Theabdomen was unremarkable and there was nocostovertebral angle tenderness. Laboratory exam-ination showed a normal hemogram; repeateduniralyses showed occasional 1 plus albuminuriaand a normal urinary sediment. The serum elec-trolytes were normal. The electrocardiogram, chestx-ray, and intravenous pyelogram were interpretedas normal.
Prior to nephrectoiiy the patient remainiedhypertensive. Both Regitine and Etamon testswere negative. The Howard test, performed twicewithin a week's interval, disclosed markedly de-creased sodium concentration and urine flow fromthe right kidney. There was no difference inphenolsulfonphthalein excretion from the 2 kid-neys. I131-Diodrast results demonstrated no differ-ence in uptake, but significant delay in excretionby the right kidney with an (A-B) index of 0.4and (A-C) of 0.5 (fig. 11).The right kidney was explored and removed.
No fall in blood pressure occurred upon clampingthe renal artery. Four small arteries supplied thekidney, which was otherwise normal pathologically.After the first postoperative day, the patient'sblood pressure fell to normotensive levels and hasremained in this range during a 7-month follow-upperiod.Case 2
D.F., a 49-year-old white male engraver wasadmitted for evaluation of hypertension of 6months' duration. The patient was in good healthuntil 6 months prior to admission, when nervous-ness and headaches appeared. A physician wasconsulted, and the patient's blood pressure wasnoted to be 240/145. He did not respond tomedical therapy. There was no family history ofhypertension or renal disease. Urinary symptomswere absent. Episodes of dizziness and sweatingwere noted after taking a highball.On physical examination the blood pressure was
250/210 lying and 274/140 standing, but posturalhypotension was noted on several occasions.Funduscopic examination showed grade 2 hyper-tensive and grade 1 arteriosclerotic retinopathy.Circulation, Volume XXII, November 1960
The lungs and heart were normal. No abdominalmasses were felt. There was no costovertebralangle tenderness. There was atrophy of all musclegflroups and shortening of the left arm due tochildhood poliomyelitis.
The hemogram was normiial. Urinalyses showedrepeated 1 plus to 2 plus albuminuria, with a rarehyaline and finely granular cast. The excretion ofphenolsulfonphthalein was normal. The blood ureanitrogen was 28 mg. per cent and the serumereatinine was 0.2 mg. per cent. Serum electrolyteswere normal. The electrocardiogram showed leftventricular hypertrophy. An intravenous pyelo-gram was read as normal.
There was good blood pressure response tosedation. A Regitine test was negative. I131-Diodrast results were abnormal, showing a markeddecrease in the rate of excretion by the rightkidney, with an (A-C) index of 1.9 (fig. 12). AHoward test was positive for right renal disease.At surgical exploration, 2 tiny right renal arterieswere noted, which did not pulsate. The left renalartery was normal. Clamping the right renalpediele was without effect on the blood pressure.The right kidney was removed. Pathologic exam-ination showed slight arteriolar nephrosclerosis,focal calcification of the medulla, and tubularvacuolization similar to that seen with hypoka-lemia. In the first postoperative week, the bloodpressure fell to levels of 190 to 160/110 to 80. Theblood urea nitrogen was 27 mg. per cent. Thepatient felt well throughout the period of nitrogenretention and at the time of discharge, 18 daysafter nephrectomy, the blood pressure was 160 to140/100 to 90.
Summario in InterlinguaEs evalutate un metho:lo utilisante Diodrast a I"'
con Diodrast como portator e uIn ratiometro in leprecoce diagnose de morbo renal unilateral.Le relative differentias funetional inter le duo
renes, demonstrate per medio de iste methodo, mon-strava un alte correlation con le constatationes a]exploration chirurgic o al necropsia.In 3 patientes eon stenosis reno-arterial uinilateral,
le pyelogramma intravenose esseva normal, sed leresultatos del studio con Diodrast a 1"n essevaa normal.Ben que nornmal resultatos obtenite con Diodrast a
I"n exclude le presentia de morbo renal unilateral,anormal resultatos pote obtener se con Diodrast aI"n in casos de non importa qual lesion que causa undifferentia del fluxos urinari ab le duo renes.
References1. PUPPEL, A. D., AND ALYEA, E. P.: Hypertension
and the surgical kidney. J. Urol. 67: 433, 1952.2. SMITH, H. W.: Unilateral nephrectomy in hyper-
tensive disease. J. VUrol. 76: 683, 1956.
925
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
BLOCK, HINE, BURROWS
3. THOMPSON, J. E., AND SMITHwVICK, R. H.: Humanhypertension due to unilateral renal disease,with special refereiiee to r-enal arterial lesions.Angiology 3: 493, 1952.
4. CLOIGH, P. W.: Editorial. Uniilateral renal ische-mia as a cause of hypertension. Ann. Int.Med. 50: 232, 1959.
5. HOWARD, J. E., BERTHRONG, M., GOULD, D. MI.,AND YENDT, E. R.: Hypertension resulting froniunilateral renal vascular disease and its reliefby nephrectoniy. Bull. Johns Hopkins Hosp.94: 51, 1954.
6. POUTASSE, E. F.: Occlusioii of renal artery caus-iIng hyperteasioa. Circulation 13: 37, 1956.
7. TAPLIN, G. V., -MEREDITH, 0. M., KADE, H., ANDWINTER, C. C.: The radioactive diodrastrenograin. J. Lab. & Clin. MIed. 48: 886, 1956.
8. BLOCK, J. B., HINE, G. J. AND BURROWs, B. A.:The effects of carrier diodrast on the excretionof J131-diodrast. J. Lab. & Cliii. -Med. 56: 110,1960.
9. HOWARD, J. E.: Hypertensioin due to vascularlesions its significance to problem of hyper-tension in general. Am. J. Obst. & Gynec. 68:1212, 1954.
10. MUELLER, C. B., SURTSHIN, A., CARLIN, M. R.,
AND WHITE, H. L.: Glomerular and tubularinfluences on sodium and water excretion. Am.J. Physiol. 165: 411, 1951.
11. CONNOR, T. B., BERTHRONG, M., THOM ,S W. C.,AND HOWARD, J. E.: Hypertension due to uni-lateral renial disease-with a report on fune-tional test helpful in diagnosis. Bull. JohnsHopkins Hosp. 100: 241, 1957.
12. POUTASSE, E. F., AND -DUSTAN, H. P.: Arterio-sclerosis and renal hypertension. J.A.M.A. 165:1521, 1957.
13. SMITHI, W. WX., AND RANGES, H. A.: Renalclearances of iopax, neoiopax, and skiodan inman. Am. J. Physiol. 123: 720, 1938.
14. LANDIS, E. M., ELSOM, K. A., BOTT, P. A., ANDSHEILS, E. H.: Simultaneous plasma clearancesof creatiiiine and certain organic compoundsof iodine in relation to human kidniey functioin.J. Cliii. Invest. 15: 1397, 1936.
15. GRABER, F. G., AND SHACKMAN, R.: Dividedrenial funietion studies in hypertension. Brit.M. J. 1: 1391, 1956.
16. PAGE, I. H., DUSTANN, H. P., AND POUTASSE, E. F.:Mechanism, diagnosis and treatment of hyper-tension of renal vascuilar origin. Ann. Int.Med. 51: 196, 1959.
The critical sense and skeptical attitude of the Hippocratic school laid the foundation-of modern medicine on broad lines, and we owe to it: first, the emancipation of mediciwefrom the shackles of priesteraft and of caste; secondly, the conception of medicine as anart based on accurate observation, and, as a science, an integral part of the science ofman and of nature; thirdly, the high moral ideals expressed in that most memorableof human documents, the Hippocratic oath; and fourthly, the conception and realizationof medicine as a profession of a cultivated gentleman.-SIR WILLIAM OSLER. Aphorismsfrom His Bedside Tea4chings and Writings. Edited by Williamii Bennett Bean, M.D.New York, Henrv Sehuman, Inc., 1950, p. 114-.
Circulation, Volune XXII, Novemtber 1960
926
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from

BikermanJEROME B. BLOCK, GERALD J. HINE, BELTON A. BURROWS and Valentine
-Diodrast Studies in Unilateral Renal Disease131I
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1960 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.22.5.913
1960;22:913-926Circulation.
http://circ.ahajournals.org/content/22/5/913located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on June 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
![Acute Unilateral Renal Infarction in the Setting of an …downloads.hindawi.com/journals/crihem/2017/3159363.pdf2007[12] 2011[13] 2012[14] 2014[15] 2016[16] 2016[17] Renal(unilateral](https://img.pdfslide.us/doc/110x75/5f05b7387e708231d41457d4/acute-unilateral-renal-infarction-in-the-setting-of-an-200712-201113-201214.jpg)




























