Embed Size (px)
Citation preview
Focus on CME at Dalhousie University
Apatient presenting with an acutely red eye is afamiliar challenge for family physicians. “Red
eye” can be caused by a variety of things, includinginfection, inflammation, and injury (Table 1). Itmay be an isolated ophthalmic condition, or a man-ifestation of systemic illness. Establishing thecause of a red eye often poses a diagnostic dilem-ma, especially when the patient is being examinedwithout the benefit of a slit lamp or a means tocheck intraocular pressure.
What are the essentials ofexamining a red eye?The most important part of any ophthalmologicexam is the vision evaluation, using a Snellen’schart, an inexpensive, yet essential tool for all pri-mary care physicians. Detecting decreased visionaids the triage ability of the referring physician, aswell as the physician being consulted. When deal-ing with red eye, it is helpful to use an anatomicapproach. Inspection of each of the anterior seg-ment structures in a systematic fashion greatlyhelps the diagnosis (Table 2).
Examination should start with inspection of theconjunctiva in order to classify the pattern of red-ness as sectoral, diffuse, or ciliary flush. Oculardischarge can be categorized as mucoid, mucopu-rulent, or serous.
Next, the cornea can be examined for diffuseopacification, or localized epithelial defects. Theuse of fluoroscein eye drops and cobalt blue lightwill reveal corneal abnormalities caused by abra-sion, ulcer, or dendrite. Cobalt blue light is availableon some ophthalmoscopes, or with a Wood’s lamp.
The anterior chamber depth should be assessedas normal or shallow as compared to the fellow eye.Note should be made of any layering of blood orpus in the anterior chamber. A penlight can be usedfor both of these examinations.
The Canadian Journal of CME / November 2003 113
Briar Sexton, MD
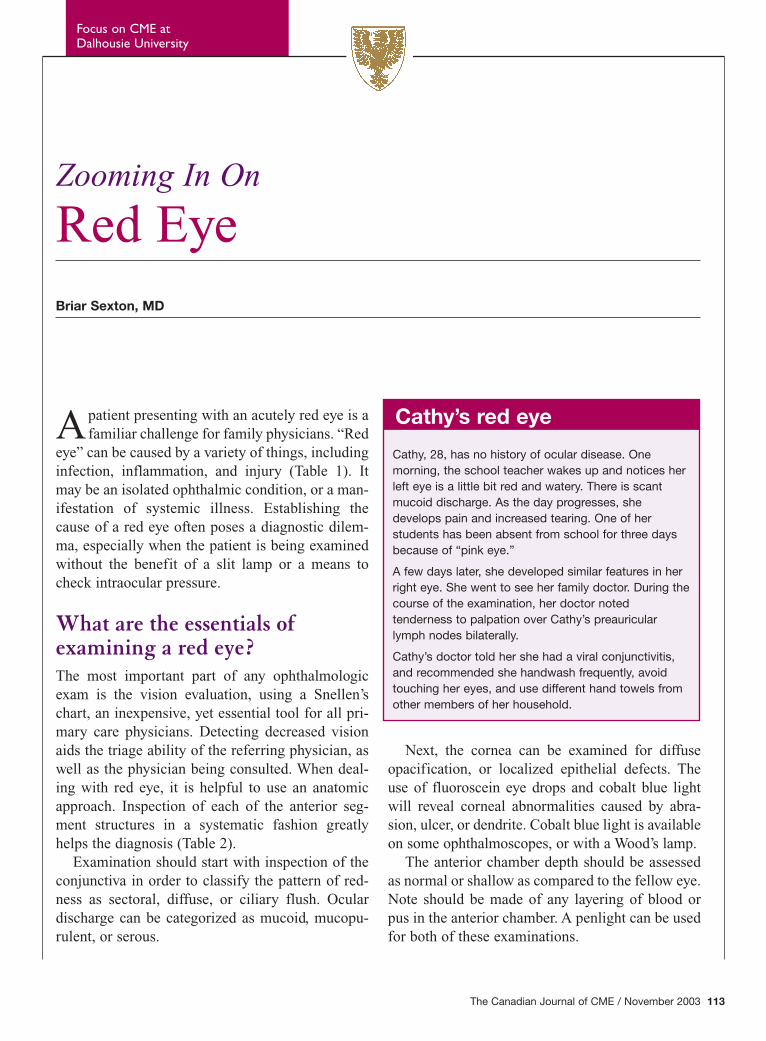
Cathy’s red eye
Cathy, 28, has no history of ocular disease. Onemorning, the school teacher wakes up and notices herleft eye is a little bit red and watery. There is scantmucoid discharge. As the day progresses, shedevelops pain and increased tearing. One of herstudents has been absent from school for three daysbecause of “pink eye.”
A few days later, she developed similar features in herright eye. She went to see her family doctor. During thecourse of the examination, her doctor notedtenderness to palpation over Cathy’s preauricularlymph nodes bilaterally.
Cathy’s doctor told her she had a viral conjunctivitis,and recommended she handwash frequently, avoidtouching her eyes, and use different hand towels fromother members of her household.
Zooming In On
Red Eye
114 The Canadian Journal of CME / November 2003
The pupils should be examined with a penlightfor anisocoria (asymmetry), and for sluggishmovement.
If possible, the intraocular pressure should bemeasured. In the absence of a formal assessmenttool, the eyes can be digitally palpated. Inspectionfor proptosis is best performed with the patientseated, and the examiner looking down frombehind the patient.
Who should be referred?Patients exhibiting decreased vision, severe pain,photophobia, or coloured halos should be referred.Patients who, on examination, have decreasedvision, corneal opacity, pupillary abnormalities,shallow anterior chamber depth, or proptosisshould also be referred.
Patients who are not getting better despite treat-ment, who wear contact lenses, and who have ahistory of severe eye disease (i.e., herpes simplexvirus, uveitis) should also be promptly referred toan ophthalmologist.
What are the warning symptoms in red eye?There are four things to look out for:1. Blurred vision2. Severe pain3. Photophobia4. Coloured halos (Table 3).
Diagnosis and treatment pearls
Red eye presents in many different forms:
Stye/hordeolum and chalazionA hordeolum or stye is an acute inflammation ofthe eyelid caused by either an external swelling(involving the hair follicle or associated glands ofZeis or Moll), or an internal swelling (involving the
Red Eye
Dr. Sexton is a fourth year resident in ophthalmology,Dalhousie University, Halifax,Nova Scotia.
Table 2
Diagnostic steps to examining a red eye
• Check visual acuity
• Inspect conjunctiva
• Inspect for discharge
• Inspect cornea for opacification
• Inspect cornea for epithelial abnormalities
• Inspect anterior chamber depth
• Inspect pupils
• Check intraocular pressure
• Inspect for proptosis
Table 1
Most common causes of red eye byanatomic location
1. Eyelid• hordeolum/chalazion• blepharitis
2. Conjunctiva• conjunctivitis
3. Sclera• episcleritis• scleritis*
4. Cornea• corneal abrasion• infectious keratitis*• herpes simplex keratitis*
5. Anterior Chamber• iritis/uveitis*• acute angle-closure glaucoma*
* Conditions that require prompt referral
The Canadian Journal of CME / November 2003 115
meibomian glands).Patients complain of aneyelid lump with swelling,pain, and redness. Theclinician is able to identifya subcutaneous nodulewithin the eyelid.Treatment involves warmcompresses and mayinclude a topical antibiotic,such as bacitracin-polymyxin B. Patients canbe encouraged to massagethe lesion three to fourtimes a day. If the lesionfails to resolve after threeto four weeks, referral iswarranted for incision andcurettage. It is not indicat-ed to perform incision andcurettage in the acutephase of the lesion.
BlepharitisBlepharitis is an inflam-matory condition of theeyelid margins. It is often seen in patients withrosacea or with a recurrent history of styes.
Treatment is often chronic and patient responsemay be slow. Treatmentmainstays are lidhygiene and topicalantibiotics, such as ery-thromycin ointment.Some patients, particu-larly those with rosacea,have benefited greatlyfrom oral tetracyclines.A typical regimen wouldbe doxycycline 100 mgorally twice a day.
S u b c o n j u n c t iva lhemorrhageSubconjunctival hemor-rhage is caused by anaccumulation of bloodbetween the conjunctivaand the sclera. It is gener-ally benign and self-lim-iting. Patients may com-plain of a mild foreignbody sensation due tomass effect. No referralis necessary.
ConjunctivitisConjunctivitis can be classified as either infectious,allergic, or chemical. Infectious conjunctivitis is
Red Eye
Table 3
Warning signs in red eye
• Decreased vision
• Corneal opacification
• Pupillary abnormalities
• Shallow anterior chamber depth
• Elevated intraocular pressure
• Proptosis
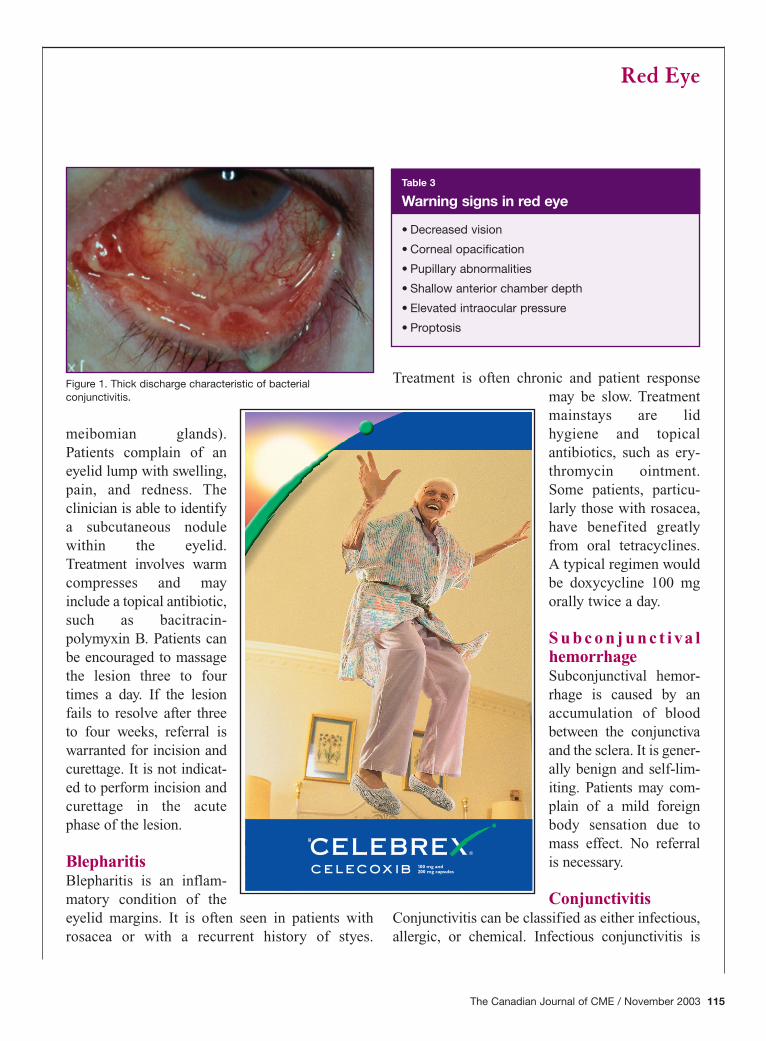
Figure 1. Thick discharge characteristic of bacterialconjunctivitis.
either bacterial or, in the vast majority of cases,viral.
Bacterial conjunctivitisBacterial conjunctivitis presents with tearing,purulent discharge, and lid stickines (Figure 1).Most adult bacterial conjunctivitis is caused byStaphylococcus species. Treatment must involve abroad spectrum antimicrobial with both gram pos-itive and gram negative activity. Available agentsinclude bacitracin-polymyxin B, fusidic acid, gen-tamicin sulfate, and sodium sufacetamide. Use oftopical aminoglycosides has been associated withcorneal toxicity. Sulfonamides have a high rate ofocular allergy. Bacitracin-polymyxin B or fusidicacid are good first-line choices. An alternate diag-nosis should be considered in any patient whoworsens or fails to improve after two to seven daysof topical antibiotics. Rarely, neisseria species willbe the cause of a hyperacute bacterial conjunctivi-tis. These pathogens can cause corneal ulcerationand perforation, and require urgent referral.Chlamydial conjunctivitis is suspected in chronic,unilateral, follicular conjunctivitis. It requires sys-temic treatment. If any of the “warning” signs andsymptoms discussed previously are present,prompt referral is warranted.
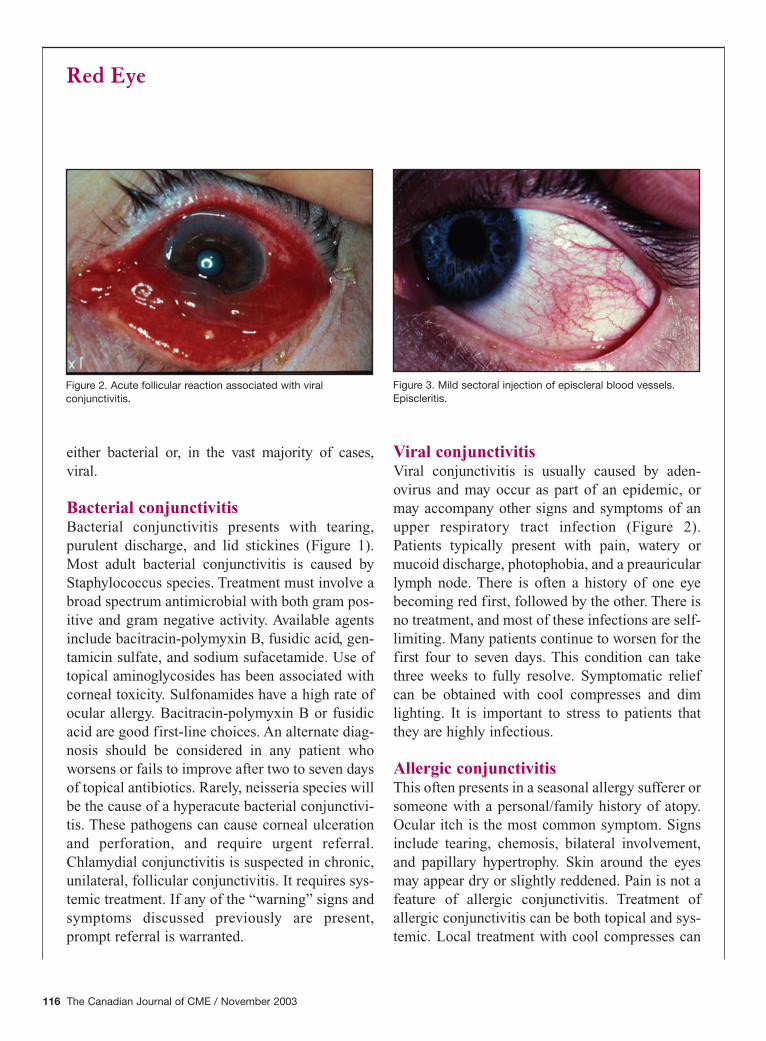
Viral conjunctivitisViral conjunctivitis is usually caused by aden-ovirus and may occur as part of an epidemic, ormay accompany other signs and symptoms of anupper respiratory tract infection (Figure 2).Patients typically present with pain, watery ormucoid discharge, photophobia, and a preauricularlymph node. There is often a history of one eyebecoming red first, followed by the other. There isno treatment, and most of these infections are self-limiting. Many patients continue to worsen for thefirst four to seven days. This condition can takethree weeks to fully resolve. Symptomatic reliefcan be obtained with cool compresses and dimlighting. It is important to stress to patients thatthey are highly infectious.
Allergic conjunctivitisThis often presents in a seasonal allergy sufferer orsomeone with a personal/family history of atopy.Ocular itch is the most common symptom. Signsinclude tearing, chemosis, bilateral involvement,and papillary hypertrophy. Skin around the eyesmay appear dry or slightly reddened. Pain is not afeature of allergic conjunctivitis. Treatment ofallergic conjunctivitis can be both topical and sys-temic. Local treatment with cool compresses can
Red Eye
116 The Canadian Journal of CME / November 2003
Figure 3. Mild sectoral injection of episcleral blood vessels.Episcleritis.
Figure 2. Acute follicular reaction associated with viralconjunctivitis.
be soothing. If the allergy isvery mild, topical lubrica-tion with artificial tearsmay suffice. More severeallergy provokes the use ofa topical antihistamine/mastcell stabilizer (i.e., patanol)four times daily. Oral anti-histamines are anotheradjunct of therapy, particu-larly if systemic features ofallergy are present. If thisfails to control the condi-tion, referral is indicated forthe addition of topical corti-costeroids or possiblycyclosporine.
EpiscleritisEpiscleritis is an inflamma-tory condition affecting theepisclera (between the con-junctiva and the sclera). It isusually unilateral. It pre-sents with mild pain andredness, which may be sec-toral (Figure 3). It is not associated with dischargeor photophobia. Attacks are usually self-limited
but may last fromweeks to months.Recurrent episcleritisshould be referred, asit may be associatedwith an underlyinginflammatory condi-tion, although it ismost often idiopathic.
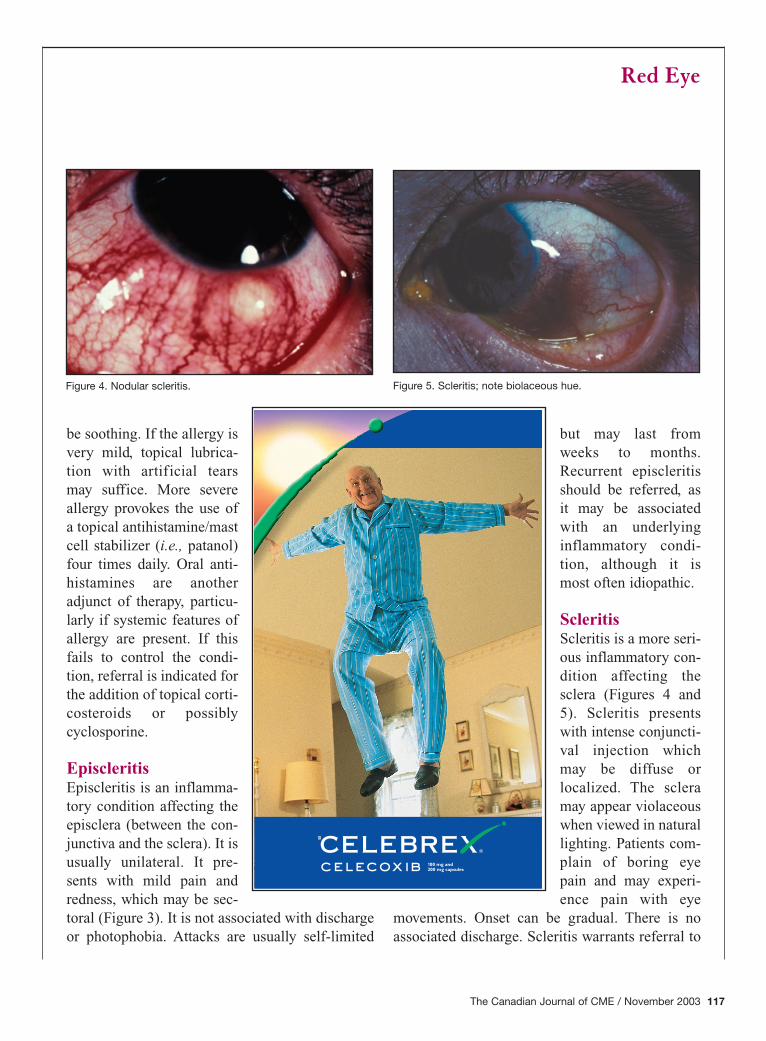
ScleritisScleritis is a more seri-ous inflammatory con-dition affecting thesclera (Figures 4 and5). Scleritis presentswith intense conjuncti-val injection whichmay be diffuse orlocalized. The scleramay appear violaceouswhen viewed in naturallighting. Patients com-plain of boring eyepain and may experi-ence pain with eye
movements. Onset can be gradual. There is noassociated discharge. Scleritis warrants referral to
Red Eye
The Canadian Journal of CME / November 2003 117
Figure 5. Scleritis; note biolaceous hue.Figure 4. Nodular scleritis.
an ophthalmogist, as a higher percentage of thesepatients have an associated systemic illness.Scleritis also has the potential for serious compli-cations, including ocular perforation. Treatment ofscleritis is via immune suppression and is sys-temic. Non-steroidals and corticosteroids are con-sidered first-line treatment, followed by immuno-suppressants. Non-steroidal anti-inflammatorydrug therapy can be initiated by the primary carephysician for pain control.
Corneal abrasionCorneal abrasions present with a red, tearing,painful, photophobic eye in the setting of trauma.The cornea has an area of staining with fluroscein.Alternately, the history of trauma may be remote(usually a fingernail or organic matter), and thepain may onset first thing in the morning. This is arecurrent erosion syndrome. Corneal abrasions arebest managed by frequent applications of anantibiotic ointment, such as bacitracin-polymyxinB, until the defect is sealed. At that time, patientsmay wish to use a bland ointment, such as a teargel, at bedtime to prevent an erosion syndrome.
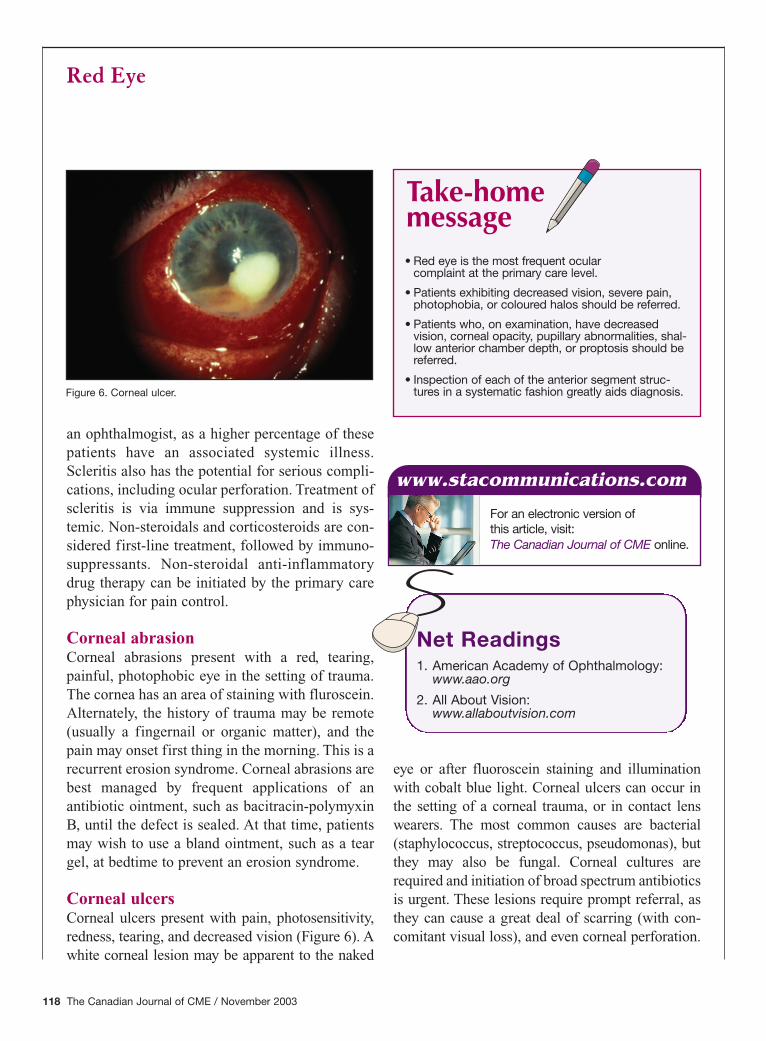
Corneal ulcersCorneal ulcers present with pain, photosensitivity,redness, tearing, and decreased vision (Figure 6). Awhite corneal lesion may be apparent to the naked
eye or after fluoroscein staining and illuminationwith cobalt blue light. Corneal ulcers can occur inthe setting of a corneal trauma, or in contact lenswearers. The most common causes are bacterial(staphylococcus, streptococcus, pseudomonas), butthey may also be fungal. Corneal cultures arerequired and initiation of broad spectrum antibioticsis urgent. These lesions require prompt referral, asthey can cause a great deal of scarring (with con-comitant visual loss), and even corneal perforation.
Red Eye
118 The Canadian Journal of CME / November 2003
• Red eye is the most frequent ocular complaint at the primary care level.
• Patients exhibiting decreased vision, severe pain,photophobia, or coloured halos should be referred.
• Patients who, on examination, have decreasedvision, corneal opacity, pupillary abnormalities, shal-low anterior chamber depth, or proptosis should bereferred.
• Inspection of each of the anterior segment struc-tures in a systematic fashion greatly aids diagnosis.
Take-homemessage
Net Readings1. American Academy of Ophthalmology:
www.aao.org
2. All About Vision:www.allaboutvision.com
www.stacommunications.com
For an electronic version of this article, visit:The Canadian Journal of CME online.
Figure 6. Corneal ulcer.

Herpes simplex keratitisViral keratitis is more likely to occur without a his-tory of trauma. Patients often have a history ofcold sores. The condition presents with red eye,foreign body sensation, and tearing (Figure 6). Onexamination, the patient may have a dendrite visiblewith fluoroscein staining. In some cases, cornealulceration may be seen. Patients often havedecreased corneal sensation, and there may beinvolvement of other ocular structures. A diagnosisor suspicion of herpes simplex keratitis requiresophthalmologic referral.
Iritis/iridocyclitisUveitis is an inflamma-tion of the iris or the irisand ciliary body. It pre-sents with pain, red eye,photophobia, decreasedvision, and tearing. Onexamination the con-junctival injection pat-tern is one of ciliaryflush. The pupil may besmaller on the affectedside. Uveitis is anothercondition which shouldbe referred to ophthal-mology, as it requiressteroid drops and dila-tors as part of the initialmanagement. Iritis canbe associated with manyconditions, including thes e r o n e g a t i v earthropathies, and sorepeated episodes war-rant systemic investiga-tion.
Angle-closure glaucomaAngle-closure glaucoma is a relatively rare causeof increased intraocular pressure. It occurs when
the drainage system of the eye becomes occluded.Patients present with extreme pain, and may havenausea and vomiting. The eye is red, rigid to digi-tal palpation and the cornea is usually opaque,obscuring iris detail. The pupil is mid-dilated andmay have minimal response to light. Patientsrequire urgent referral to prevent damage to theoptic nerve.
References1. Berson FG: Basic Ophthalmology for Medical Students and
Primary Care Residents. Sixth Edition. American Academyof Ophthalmology, San Francisco, 1993 pp. 69.
2. Teoh DL, Reynolds S:Diagnosis and managementof pediatric conjunctivitis.Pediatr Emerg Care 2003;19(1):48-55.
The author would like to
thank Dr. Chris Seamone for
providing the accompanying
photos.
Red Eye
The Canadian Journal of CME / November 2003 119
CME
Anti-inflammatory analgesic agent. Product Monograph available upon request.General warnings for NSAIDs should be borne in mind.CELEBREX® is a registered trademark of G.D. Searle & Co., used under permission by Pharmacia Canada Inc.