Embed Size (px)
Citation preview

11/21/2016
1
Malignant Melanoma: Morphology, Classification, and AJCC staging
Adriano Piris, MDAdriano Piris, MD• Co‐director, Mihm Cutaneous Pathology Consultative ServiceDepartment of Dermatology, Brigham & Women’s Hospital
• Stewart Rahr‐MRA Young InvestigatorMelanoma Research Alliance, Washington, D.C.
• Consultant Staff Department of Pathology, Dana Farber Cancer Institute
Malignant melanoma
• In situ
• Invasive
Malignant Melanoma In SituInvasive Melanoma
• Nontumorigenic:
Radial Growth Phase
• Tumorigenic:
Vertical Growth Phase
Radial Growth PhaseRadial Growth Phase
Radial Growth Phase
• In Situ: confined above basement membrane• Microinvasive: biologically indolent and commonMicroinvasive: biologically indolent and common
[none of 161 patients showed metastases at a meanFollow-up of 13.7 years]
Guerry D et al. J Invest Dermatol 100: 342S-345S, 1993

11/21/2016
2
Radial Growth PhaseCharacteristics
• Cells present individually or in small nests
• Dermal nests are no larger than epidermal nests
• Dermal mitoses are absent
• Dermal component usually confined to papillary dermis
• Papillary dermis is usually not expanded
• No single group of cells is substantially largerthan any other group
• Dermal and epidermal cells are cytologically similar
V ti l G th PhVertical Growth Phase

11/21/2016
3
Vertical Growth Phase
• Dermal cells present in one or more expansile nodules
• Dermal nests are larger than nests in epidermis
• Dermal mitoses
• Dermal component often extends into reticular dermis
• Papillary Dermis is often expanded
• Dermal and epidermal cells are cytologically different
Four Common Forms of Malignant Melanoma
Three with a Radial Growth Phase [RGP]
• Superficial Spreading Melanoma 70%
• Acral Lentiginous Melanoma 8%Acral Lentiginous Melanoma 8%
• Lentigo Maligna Melanoma 5%
One with only Vertical Growth Phase [VGP]
• Nodular Melanoma 15%

11/21/2016
4
Malignant Melanoma:Superficial Spreading Type
Malignant Melanoma:Superficial Spreading Type
Malignant Melanoma: Acral Lentiginous Type

11/21/2016
5
Malignant Melanoma: Lentigo Maligna Type
Malignant Melanoma: Nodular Type ?

11/21/2016
6
Four Common Forms of Malignant Melanoma
Three with a Radial Growth Phase [RGP]
• Superficial Spreading Melanoma BRAF/NRAS
• Acral Lentiginous Melanoma CKIT
•Lentigo Maligna Melanoma CKIT
Chronic Sun Damage (CSD)
One with only Vertical Growth Phase [VGP]
• Nodular Melanoma ?BRAF/NRAS
Superficial spreading Malignant melanoma & BRAF mutant melanomas
• Intermittent sun exposure.
• High degree of pagetoid spread
• Prominent nesting
• Large epithelioid cells• Large epithelioid cells
• Circumscription
• Minimal solar elastosis.
• Heavy melanin pigmentation
• Epidermal thickening
BRAF‐negative melanomas
• Acral lentiginous melanomas.
• Lentigo maligna melanomas (chronic s n• Lentigo maligna melanomas (chronic sun damage skin melanomas).
• Mucosal melanomas.
M ut at ion P er ce nt a ge P h e n ot yp e Ne w T her a piesB R A F 50 % Y o u ng
I nte r m it tent S u n E x p o su re M u l t ip le n e v i F ew fr ec k les T a ns w ith e a s e S u pe r fic ia l Sp r e adin g ty pe
BR A F an d M E K in h ibito rs
N R A S 15 - 20 % I nte r m it tent S u n E x p o su re ( w eak asso c ia tio n ) L o w o r a b se n t p age to id s pr e a d C ir cum scr ib ed le sio ns
? M E K , P1 3 K , a n d AK T in h ibi to rs
C ir cum scr ib ed le sio ns C K IT 10 - 20 % o f ac r a l an d
m u co sa l m e la n o m a s A c ra l and m u co sa l si te s M e lan o m a s w ith len t ig in ou s sp re ad
C K I T Oth e r tyr os in e kin a se in h ibi to rs
G N A Q /G N A 1 1 50 % o f u v e a l m e lan om as
U v e a l m e la n o m a ?
Modified from Scolyer et al, Molecular Oncology (2011)124-136
Unusual Vertical Growth Phase Components
• Balloon Cell
• Rhabdoid
M id• Myxoid
• Small cell
• Unusual Phenotypic profile: etc…
Rhabdoid melanoma

11/21/2016
7
Small cell melanoma
Melan-A PROGNOSTIC FACTORS

11/21/2016
8
Staging Melanoma
1. Characterize tumor status.
2. Stratify the risk of recurrence and metastasis.
3. Prognostication.3. Prognostication.
4. Guide clinical and surgical management/decision making.
Melanoma staging, as defined by the current AJCC staging system, reflects tumor biology and survival outcomes.
AJCC Cancer Staging Manual 8th Edition
• Gershenwald JE, et al
• Melanoma of the Skin• Melanoma of the Skin
• Pages 563‐85
• American Joint Committee on Cancer 2017
AJCC 8th:Tumor Thickness (Breslow’s thickness)
• Tumor thickness ranges maintained
• T1a subcategorized (threshold 0.8 mm)
d f• Primary determinant of T staging: T1a: non‐ulcerated and < 0.8 mm T1b: 0.8 to 1.0 mm regardless of ulceration, or < 0.8 mm if ulcerated T2: 1.1‐2.0 mm T3: 2.1‐4.0 mm T4:>4.0 mm
Measuring Breslow Thickness
• Using a calibrated ocular micrometer at a right angle to the adjacent normal skin:
• The upper point of reference is:
–The granular layer of the epidermis of the overlying skin.
–In an ulcerated lesion use the base of the ulcer.
• The lower reference point is the deepest point of tumor invasion.

11/21/2016
9
AJCC 8th: Measuring Breslow Thickness
• For tumors > 1mm: Recorded to the nearest 0.1 mm (not 0.01 mm)
• Tumors ≤ 1mm : May be measured to the nearest 0.01 mm but should be reported rounded to the nearest 0.1 mm
‐e.g. melanoma measured in the range of 0.75 to 0.84 mm are reported as 0.8 mm in thickness: T1b
FACTORS ASSOCIATED WITH AGGRESSION IN THIN MELANOMAS
• Early vertical growth phase
• Ulceration
• Level IV
• Mitosis
• Extensive regression
THESE FACTORS SHOULD LEAD TO CONSIDERATION OF SENTINEL LYMPH NODE BIOPSY.

11/21/2016
10
AJCC 8th: Primary Tumor Mitotic Rate
• No longer used as a T‐category criterion
• Remains a major determinant of prognosis
Sh ld b d d d d• Should be assessed and recorded
• May play a role in future prognostic models
• Count dermal mitoses only.
• Number of mitoses per mm2.
• 1mm2= approx. 4 to 5 HPF’s (40X).
Primary Tumor Mitotic Rate
• Count dermal mitoses only.
• Number of mitoses per mm2.
• 1mm2= approx. 4 to 5 HPF’s (40X).
Prognostic Factors: Dermal Mitoses (Hot Spot)
AJCC 8th: Primary Tumor Ulceration
• Is the second criterion for determining T category.
• Full‐thickness absence of an intact epidermis with associated host reaction above the primary melanoma (based on histopathologic examination)

11/21/2016
11
Primary Tumor Ulceration
Defined as the combination of:
– full‐thickness epidermal defect
– evidence of reactive changes (fibrin exudation and neutrophilicdebris))
– thinning, effacement, or reactive hyperplasia of the surrounding epidermis without trauma or evidence of a recent surgical procedure
Balch CM et al. Annals of Surgery. 1978
Prognostic Factors: Ulceration
CHARACTERISTICS OFULCERATED MELANOMA
5 year survival decreased from 80% to 55% in Stage I/II; 53% to 12% in Stage III
Majority of melanomas > 4.0 mm are ulceratedMedian ulcer depth is 0.8 mm (range: 0.01- 1.2 mm)Width of ulcer > 6 mm. associated with even worse
prognosis
Balch CM et al. J Surg Oncol. 2011 Florentien EM. Et al. Ann Surg. 2012
AJCC 8th: Microsatellites
•Microscopic cutaneous and/or subcutaneous metastasis adjacent or deep to a
primary melanoma on pathological examination of the primary tumor site.
AJCC 8th: Microsatellites
•The (metastatic) tumor cells must be discontinuous from the primary tumor.
•The “separating” tissue must not contain fibrosis and/or reactive inflammatory
hchanges.
•There is no minimal size threshold or distance from the primary tumor.
•Multiple levels may be necessary to confirm that the focus is indeed separate
from the tumor.

11/21/2016
12
AJCC 8th: Microsatellites
•The presence of microsatellites indicates poor prognosis.
•Equivalent to patients with clinical satellites or in-transit metastasis
•Patients with microsatellites in the primary tumor site are considered Stage III
even in the absence of clinically involved lymph nodes, or grossly visible satellite
or in-transit metastases.
Prognostic Factors: Microsatellites
Microscopic Satellites
Five year survivalwith satellites 36%without satellites 89%
ReferenceHarrist TJ, Rigel DS, Day CL Jr. et al: “Microscopic satellites” are more highly associated with regional lymph node metastases than is primary melanoma thickness.Cancer. 53 (10)2183-7. 1984 May 15
Ten year survival
With satellites 37%
Without satellites 65%
Reference: Leon P, Daley JM, Synnetvedt M, et al. The prognostic Implications of microscopic satellites in patients withClinical stage One melanoma. Arch of Surgery. 126(12)1461-8.1991 Dec
AJCC 8th: Regional lymph node metastasis
• Clinically occult: Patients with microscopically documented nodal disease (lymphatic mapping and SLN biopsy) and without clinical or radiographic evidence of regional lymph node metastases (7th ed: “microscopic”)
• N1a, N2a, or N3a, based on the number of tumors involved
• N1c, N2c, or N3c, if microsatellites, satellites, or in‐transit metastases are present.
• Clinically detected: Patients with clinical or radiographic evidence of regional lymph node metastasis.
Other important considerations
• Even focal nodal disease (including isolated tumor cells) can be associated with poorer outcomes.
• Immunohistochemistry is more sensitive for yidentifying melanoma cells, (HMB‐45, Melan A, and MART 1).
Scheri RP et al. Ann Surg Oncol 2007 van Akkooi AC et al. Ann Oncol 2006Yu LL et al. Cancer 1999

11/21/2016
13
Prognosis of SLN Micrometastases• Location & extent of melanoma SN deposits predictive of
– Regional non‐SN metastases– Clinical outcome
• Parameters include– % nodal cross sectional area– Microanatomical location – Tumour penetrative
depth – Size
Regression
• Area of epidermis without recognizable tumor flanked by obvious melanoma. Deep to the tumor free epidermis, the papillary dermis is also free of tumor and usually widened because of delicate fibrous tissue with increased vascularity and scattered melanophages.
Clark WH et al. Cancer Res. 1969
Prognostic Factors: Regression
Thin melanomas with extensive regression >70 to 75% of the surface area are highly associated with metastatic behavior
Ronan S et al. Arch Dermatol. 1987.
11/21/2016
14
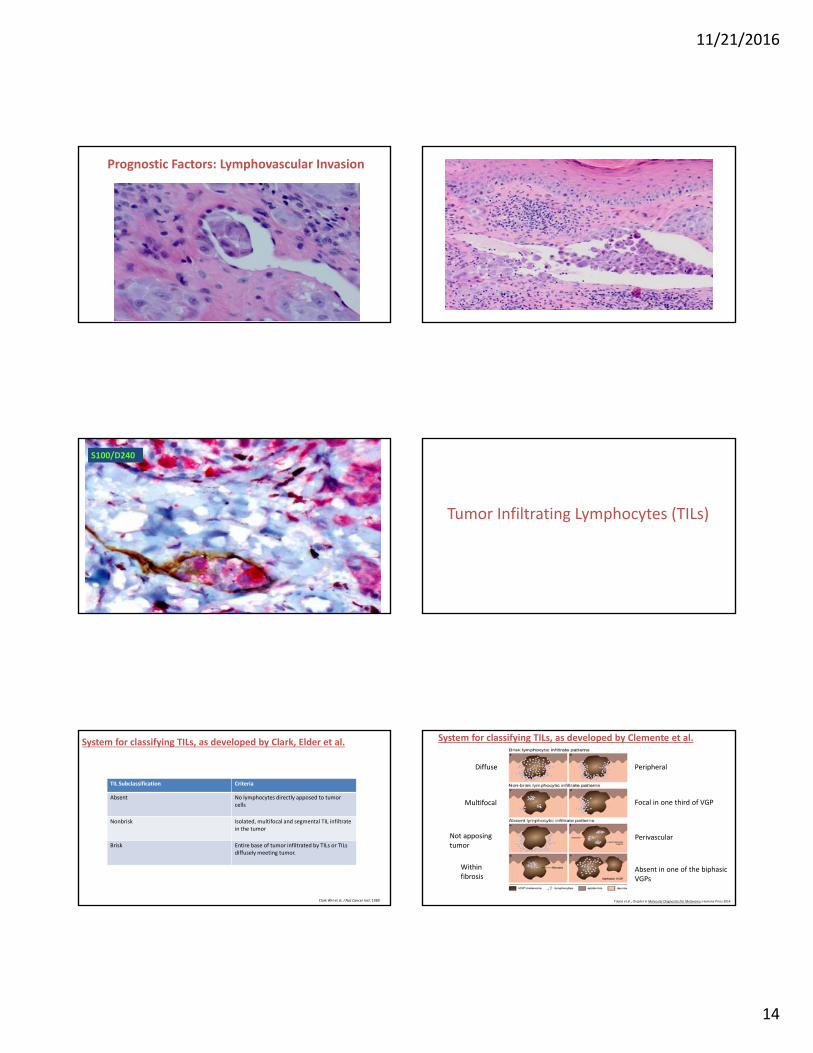
Prognostic Factors: Lymphovascular Invasion
S100/D240
Tumor Infiltrating Lymphocytes (TILs)
TIL Subclassification Criteria
Absent No lymphocytes directly apposed to tumorcells
System for classifying TILs, as developed by Clark, Elder et al.
Nonbrisk Isolated, multifocal and segmental TIL infiltrate in the tumor
Brisk Entire base of tumor infiltrated by TILs or TILs diffusely meeting tumor.
Clark WH et al. J Nat Cancer Inst. 1989
System for classifying TILs, as developed by Clemente et al.
Diffuse Peripheral
Multifocal Focal in one third of VGP
Tobias et al., Chapter in Molecular Diagnostics for Melanoma; Humana Press 2014
Not apposing tumor
Perivascular
Within fibrosis
Absent in one of the biphasic VGPs

11/21/2016
15
Absent Host immune Response Absent Host immune Response

11/21/2016
16
• The study by Azimi et al, of the Melanoma Institute of Australia, emphasized the importance of density of lymphocytes with the best survival in densely and briskly infiltrated tumors.
Tumor Infiltrating Lymphocytes
• 10 years ago, the European Organization for the Research and Treatment of Cancer (EORTC) began a study to examine infiltrates with more detailed attention to distribution and pattern in 1080 cases with 30 year follow‐up.
Azimi F et al. J Clin Oncol. 2012Gimotty et al. EORTC. manuscript in preparation.
Advancing Edge of the Tumor
• The EORTC study emphasizes the significance of the advancing edge of the tumor (Brisk‐Peripheral).
• Four other studies support the significance of the advancing edge:1. The pERK and high Ki67 staining of the advancing edge*
2. The significance of Sox2 expression as evidence of epithelial‐mesenchymal transition (EMT) in the advancing edge of malignant melanoma**
3. Nestin depletion and its relationship to invasion***
*Edwards R et al. manuscript in preparation.**Laga et al. AJP. 2010**Laga et al. Exp Derm. 2011***Lee CW et al. Lab Invest. 2014
TILs and Metastasis: Lymph nodes
• A study in 1996 correlated melanoma survival with brisk infiltrates in draining lymph node deposits compared to non‐brisk or absent TILs*
• A recent study of metastatic melanoma in sentinel lymph nodes showed a positive correlation between recurrence and overall survival related to the number of CD3, CD4, and CD8 positive TILs**
*Mihm et al. Lab Invest. 1996**Kakavand et al. Modern Pathology. 2015
Tumor Infiltrating Lymphocytes: Metastatic Melanoma
• The importance of TILs has recently been emphasized in the work of Ribasand colleagues who demonstrated that the presence of clonalCD8+/PD1+/PD‐L1+ lymphocytes at the periphery of the tumor showed a remarkable response to Pembrolizumab in metastatic melanoma biopsies, resulting in regression.
• A predictive model based on CD8 expression at the invasive margin was proposed (Tumeh et al).
• This study emphasizes the importance of pathologists’ role in evaluating TILs in primary and metastatic disease.
Tumeh et al. Nature. 2014
• The AJCC melanoma staging system offers prognostic information and guides patient management.
• Emerging molecular data and biomarkers may eventually become incorporated in the staging and prognostication of melanoma patients.
• Molecular profiling is allowing for the development of targeted therapies, including the FDA approval of vemurafenib, dabrafenib, and trametinib in the setting of BRAF V600E mutant melanoma.
Boland GM et al. J Surg Oncol 2014Chapman PB et al. New Engl J Med 2011Flaherty et al. Nat Rev Drug Discov 2011Flaherty KT et al. New Engl J Med 2012Larkin J et al. New Engl J Med 2014
AJCC 8th Edition :International Melanoma Database
• Only patients treated since 1998
• >49,000 patients (>one third from MIA Sydney)
• Patients from Australia, USA, Italy, Greece, Spain
• Chair: Jeff Gershenwald
• Vice Chair: Richard Scolyer
• Statistician: Ken Hess
• Expert Panel: 28 other members worldwide

11/21/2016
17
Importance of HistopathologicalReporting
• Melanoma pathology report shouldp gy p– Document key diagnostic criteria Dx dased upon
– Provide the pathological parameters important for• Prognosis
• Management
Conclusions• Pathologist should produce a report with sufficient information to allow– Evidence‐based management plan be established– Reliable estimate of prognosis to be made
• Structured report format can facilitate this• More accurate prediction of prognosis in future
– Web‐based tools– Integrating other prog factors & complex data– Molecular predictive and prognostic markers
Thank you !





























