Embed Size (px)
Citation preview

1111
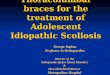
Italian perspectives: HelmetItalian perspectives: HelmetItalian perspectives: HelmetItalian perspectives: Helmet
Courtesy of Dr Massimo Antonelli (Rome)Courtesy of Dr Massimo Antonelli (Rome)
Latex-free transparent PVCLatex-free transparent PVC
Secured by 2 arm = pit Secured by 2 arm = pit
braces (A) at two hooks (B) braces (A) at two hooks (B)
of the metallic ring (C) joining of the metallic ring (C) joining
helmet with a soft collar (D) helmet with a soft collar (D)
A seal connection (E) allowsA seal connection (E) allows
the passage of NGTthe passage of NGT
Latex-free transparent PVCLatex-free transparent PVC
Secured by 2 arm = pit Secured by 2 arm = pit
braces (A) at two hooks (B) braces (A) at two hooks (B)
of the metallic ring (C) joining of the metallic ring (C) joining
helmet with a soft collar (D) helmet with a soft collar (D)
A seal connection (E) allowsA seal connection (E) allows
the passage of NGTthe passage of NGT
A
BC
D
E

2222
HelmetHelmetHelmetHelmet
InP = Inspiratory port; ExP = expiratory port; SC = sealed connector; BR= armpit braces

3333
Hypoxemic Hypercapnic
IPPVIPPV Augment ventilationAugment ventilation
CPAPCPAPRecruit lung unitsRecruit lung unitsDecrease afterloadDecrease afterload Offset PEEPiOffset PEEPi
Modes of Ventilation

4444
Recruits lung unitsRecruits lung units• improved V/Q matching > rapid correction of PaOimproved V/Q matching > rapid correction of PaO22 & PaCO & PaCO22
11
• increased functional residual capacityincreased functional residual capacity• decreased respiratory rate and WOB2 decreased respiratory rate and WOB2
Reduces airway resistanceReduces airway resistance22
Improves hemodynamics in pulmonary edemaImproves hemodynamics in pulmonary edema• decreases venous return decreases venous return • decreases afterload and increases cardiac index (in 50%)decreases afterload and increases cardiac index (in 50%)1-41-4
• decreases heart ratedecreases heart rate1-31-3
Average requirement: 10cmHAverage requirement: 10cmH22OO
Recruits lung unitsRecruits lung units• improved V/Q matching > rapid correction of PaOimproved V/Q matching > rapid correction of PaO22 & PaCO & PaCO22
11
• increased functional residual capacityincreased functional residual capacity• decreased respiratory rate and WOB2 decreased respiratory rate and WOB2
Reduces airway resistanceReduces airway resistance22
Improves hemodynamics in pulmonary edemaImproves hemodynamics in pulmonary edema• decreases venous return decreases venous return • decreases afterload and increases cardiac index (in 50%)decreases afterload and increases cardiac index (in 50%)1-41-4
• decreases heart ratedecreases heart rate1-31-3
Average requirement: 10cmHAverage requirement: 10cmH22OO
Mask CPAP in Hypoxemic FailureMask CPAP in Hypoxemic Failure
1. Bersten NEJOM 19911. Bersten NEJOM 1991 3. Rasanen AJC 19853. Rasanen AJC 1985
2. Lenique AJRCCM 19942. Lenique AJRCCM 1994 4. Bradley ARRD 19924. Bradley ARRD 1992
1. Bersten NEJOM 19911. Bersten NEJOM 1991 3. Rasanen AJC 19853. Rasanen AJC 1985
2. Lenique AJRCCM 19942. Lenique AJRCCM 1994 4. Bradley ARRD 19924. Bradley ARRD 1992

5555
CPAP in Congestive Heart FailureCPAP in Congestive Heart FailureCPAP in Congestive Heart FailureCPAP in Congestive Heart Failure
CPAP in CHFCPAP in CHF
• Reduces systolic LVPReduces systolic LVPtmtm by changing by changing
PPeses from negative to positive from negative to positive
CPAP in CHFCPAP in CHF
• Reduces systolic LVPReduces systolic LVPtmtm by changing by changing
PPeses from negative to positive from negative to positive
Naughton et al Circulation 1995; 91:1725Naughton et al Circulation 1995; 91:1725
LVPLVPtmtm during systole during systole
• LVPLVPtmtm = ventricular systolic pressure - = ventricular systolic pressure -
extracardiac pressure (i.e., pericardial pr.) extracardiac pressure (i.e., pericardial pr.)
• Changes in PChanges in Pes es = changes in pericardial pr. = changes in pericardial pr.
• During inspiration > large negative During inspiration > large negative intrathoracic pressure swings increase intrathoracic pressure swings increase LVPLVPtmtm and afterload and afterload
LVPLVPtmtm during systole during systole
• LVPLVPtmtm = ventricular systolic pressure - = ventricular systolic pressure -
extracardiac pressure (i.e., pericardial pr.) extracardiac pressure (i.e., pericardial pr.)
• Changes in PChanges in Pes es = changes in pericardial pr. = changes in pericardial pr.
• During inspiration > large negative During inspiration > large negative intrathoracic pressure swings increase intrathoracic pressure swings increase LVPLVPtmtm and afterload and afterload
Pes
Negative
Negative
Pes
Positive
Positive
• Lung inflation Lung inflation parasympathetic tone parasympathetic tone sympathetic outflow sympathetic outflow HRHR
• Reduction in OReduction in O22 consumption consumption – MyocardialMyocardial: systolic LVP: systolic LVPtmtm x HR x HR– PulmonaryPulmonary: P: Peses x RR x RR
• Lung inflation Lung inflation parasympathetic tone parasympathetic tone sympathetic outflow sympathetic outflow HRHR
• Reduction in OReduction in O22 consumption consumption – MyocardialMyocardial: systolic LVP: systolic LVPtmtm x HR x HR– PulmonaryPulmonary: P: Peses x RR x RR

6666
Expiratory flow limitation Expiratory flow limitation
Dynamic hyperinflationDynamic hyperinflation
Respiratory muscle fatigueRespiratory muscle fatigue
Respiratory acidosis Respiratory acidosis
Expiratory flow limitation Expiratory flow limitation
Dynamic hyperinflationDynamic hyperinflation
Respiratory muscle fatigueRespiratory muscle fatigue
Respiratory acidosis Respiratory acidosis
COPD: Pathophysiology of ARFCOPD: Pathophysiology of ARF

7777
COPD: Dynamic HyperinflationCOPD: Dynamic Hyperinflation
Auto PEEP = inspiratory threshold loadAuto PEEP = inspiratory threshold load Flattened diaphragm = reduced efficiency and enduranceFlattened diaphragm = reduced efficiency and endurance
• shortening of the sarcomere length and decreased maximal forceshortening of the sarcomere length and decreased maximal force• reduced zone of apposition with the chest wall (expansion on insp.)reduced zone of apposition with the chest wall (expansion on insp.)• reduced blood supplyreduced blood supply

8888
COPD patient stableCOPD patient stable
• average PEEPi 2.4 ± 1.6 cm Haverage PEEPi 2.4 ± 1.6 cm H22OO11
COPD patient with acute exacerbationCOPD patient with acute exacerbation• average PEEPi 6.5 ± 2.5 cm H2O2,3average PEEPi 6.5 ± 2.5 cm H2O2,3• PEEPi = 43±5% total work by respiratory PEEPi = 43±5% total work by respiratory
systemsystem44
Increased OIncreased O22 cost correlates with diaphr. flattening cost correlates with diaphr. flattening
on CXRon CXR55
COPD patient stableCOPD patient stable
• average PEEPi 2.4 ± 1.6 cm Haverage PEEPi 2.4 ± 1.6 cm H22OO11
COPD patient with acute exacerbationCOPD patient with acute exacerbation• average PEEPi 6.5 ± 2.5 cm H2O2,3average PEEPi 6.5 ± 2.5 cm H2O2,3• PEEPi = 43±5% total work by respiratory PEEPi = 43±5% total work by respiratory
systemsystem44
Increased OIncreased O22 cost correlates with diaphr. flattening cost correlates with diaphr. flattening
on CXRon CXR55
COPD: Intrinsic PEEPCOPD: Intrinsic PEEP
1. Dal Vecchio et al Eur Respir J 1990; 3:741. Dal Vecchio et al Eur Respir J 1990; 3:74 3. Brocard et al NEJOM 1990; 323: 15233. Brocard et al NEJOM 1990; 323: 1523
2. Appendini et al AJRCCM 1994; 149: 10692. Appendini et al AJRCCM 1994; 149: 1069 4. Jubran et al AJRCCM 1995; 152: 129 4. Jubran et al AJRCCM 1995; 152: 129
5. Pitcher et al J Appl Physiol 1993; 74: 27505. Pitcher et al J Appl Physiol 1993; 74: 2750
1. Dal Vecchio et al Eur Respir J 1990; 3:741. Dal Vecchio et al Eur Respir J 1990; 3:74 3. Brocard et al NEJOM 1990; 323: 15233. Brocard et al NEJOM 1990; 323: 1523
2. Appendini et al AJRCCM 1994; 149: 10692. Appendini et al AJRCCM 1994; 149: 1069 4. Jubran et al AJRCCM 1995; 152: 129 4. Jubran et al AJRCCM 1995; 152: 129
5. Pitcher et al J Appl Physiol 1993; 74: 27505. Pitcher et al J Appl Physiol 1993; 74: 2750

9999
Etiology of ARFEtiology of ARF Pharmacological TreatmentPharmacological Treatment• precipitating condition • bronchodilator, anti-inflammatory
antibiotics, etc.
Physiology of ARFPhysiology of ARF Positive pressurePositive pressure
• expiratory flow limitation expiratory flow limitation • causes bronchodilation • causes bronchodilation
• • dynamic hyperinflationdynamic hyperinflation • offsets intrinsic PEEP ( • offsets intrinsic PEEP ( load) load)
• • respiratory muscle fatigue respiratory muscle fatigue • reduces diaphragmatic activity • reduces diaphragmatic activity
• • respiratory acidosis respiratory acidosis • increases VE ( • increases VE ( Vt, Vt, RR) RR)
Etiology of ARFEtiology of ARF Pharmacological TreatmentPharmacological Treatment• precipitating condition • bronchodilator, anti-inflammatory
antibiotics, etc.
Physiology of ARFPhysiology of ARF Positive pressurePositive pressure
• expiratory flow limitation expiratory flow limitation • causes bronchodilation • causes bronchodilation
• • dynamic hyperinflationdynamic hyperinflation • offsets intrinsic PEEP ( • offsets intrinsic PEEP ( load) load)
• • respiratory muscle fatigue respiratory muscle fatigue • reduces diaphragmatic activity • reduces diaphragmatic activity
• • respiratory acidosis respiratory acidosis • increases VE ( • increases VE ( Vt, Vt, RR) RR)
COPD: Management of ARFCOPD: Management of ARF

10101010

11111111
Hypoxemic Hypercapnic
IPPVIPPV Augment ventilationAugment ventilation
CPAPCPAPRecruit lung unitsRecruit lung unitsDecrease afterloadDecrease afterload Offset PEEPiOffset PEEPi
Modes of Ventilation

12121212
COPD: Inspiratory Effort and PEEPiCOPD: Inspiratory Effort and PEEPi
isometric contraction to counterbalance PEEPi (inspiratory threshold load)
isometric contraction to counterbalance PEEPi (inspiratory threshold load)
atmospheric
pressure
atmospheric
pressure
Auto PEEP
8cm H2O
external
PEEP
6 cm H2O
external
PEEP
6 cm H2O
Auto PEEP
8cm H2O
Inspiratory Pressure4 cm H2O
Inspiratory Pressure4 cm H2O
Appendini et al. AJRCCM 1994; 149: 1069Appendini et al. AJRCCM 1994; 149: 1069Appendini et al. AJRCCM 1994; 149: 1069Appendini et al. AJRCCM 1994; 149: 1069
in COPD with ARF the inspiratory effort to lower alveolar pressure below ambient pressure is divided into two components:
in COPD with ARF the inspiratory effort to lower alveolar pressure below ambient pressure is divided into two components:
Inspiratory Pressure
10 cm H2O
Inspiratory Pressure
10 cm H2O isotonic contraction to generate inspiratory flow and tidal volume
isotonic contraction to generate inspiratory flow and tidal volume
IT

13131313
Offsets PEEPiOffsets PEEPi11
acute COPD exacerbation: average PEEPi 6.5 acute COPD exacerbation: average PEEPi 6.5 ++ 2.5 cmH 2.5 cmH22OO11
apply PEEP at 80-90% of PEEPi to avoid overdistentionapply PEEP at 80-90% of PEEPi to avoid overdistention11
Reduces transdiaphragmatic pressureReduces transdiaphragmatic pressure22
May improve Vt, VE, or PaCOMay improve Vt, VE, or PaCO2244
no response within 30 min in 4 studies no response within 30 min in 4 studies 1,2,5,6 1,2,5,6
delayed response (> 4 h) in clinical studiesdelayed response (> 4 h) in clinical studies44
Average CPAP requirement: Average CPAP requirement: 5 cmH5 cmH2200
Offsets PEEPiOffsets PEEPi11
acute COPD exacerbation: average PEEPi 6.5 acute COPD exacerbation: average PEEPi 6.5 ++ 2.5 cmH 2.5 cmH22OO11
apply PEEP at 80-90% of PEEPi to avoid overdistentionapply PEEP at 80-90% of PEEPi to avoid overdistention11
Reduces transdiaphragmatic pressureReduces transdiaphragmatic pressure22
May improve Vt, VE, or PaCOMay improve Vt, VE, or PaCO2244
no response within 30 min in 4 studies no response within 30 min in 4 studies 1,2,5,6 1,2,5,6
delayed response (> 4 h) in clinical studiesdelayed response (> 4 h) in clinical studies44
Average CPAP requirement: Average CPAP requirement: 5 cmH5 cmH2200
COPD: Mask CPAP in ARFCOPD: Mask CPAP in ARF
1. Appendeni AJRCCM 19941. Appendeni AJRCCM 1994 3. Martin ARRD 19823. Martin ARRD 1982 5. Shivaram Resp 19875. Shivaram Resp 1987
2. Gottfried Chest 19872. Gottfried Chest 1987 4. De Lucas Chest 19934. De Lucas Chest 1993 6. Elliot BMJ 19946. Elliot BMJ 1994
1. Appendeni AJRCCM 19941. Appendeni AJRCCM 1994 3. Martin ARRD 19823. Martin ARRD 1982 5. Shivaram Resp 19875. Shivaram Resp 1987
2. Gottfried Chest 19872. Gottfried Chest 1987 4. De Lucas Chest 19934. De Lucas Chest 1993 6. Elliot BMJ 19946. Elliot BMJ 1994

14141414 BMJ 2003; 326:185.

15151515
Resetting responses to PaCOResetting responses to PaCO22Resetting responses to PaCOResetting responses to PaCO22
In COPD, the ventilatory response to raised PaCOIn COPD, the ventilatory response to raised PaCO22 is is
decreased especially during sleep. decreased especially during sleep.
NPPV lowers nocturnal PaCONPPV lowers nocturnal PaCO22 and resets the respiratory and resets the respiratory
control centre to become more responsive to increased control centre to become more responsive to increased
PaCOPaCO22 by increasing the neural output to the diaphragm and by increasing the neural output to the diaphragm and
other respiratory muscles. other respiratory muscles. These patients are then able to maintain a more normal These patients are then able to maintain a more normal
PaCOPaCO22 throughout the daylight hours without the need for throughout the daylight hours without the need for
mechanical ventilation.mechanical ventilation.
In COPD, the ventilatory response to raised PaCOIn COPD, the ventilatory response to raised PaCO22 is is
decreased especially during sleep. decreased especially during sleep.
NPPV lowers nocturnal PaCONPPV lowers nocturnal PaCO22 and resets the respiratory and resets the respiratory
control centre to become more responsive to increased control centre to become more responsive to increased
PaCOPaCO22 by increasing the neural output to the diaphragm and by increasing the neural output to the diaphragm and
other respiratory muscles. other respiratory muscles. These patients are then able to maintain a more normal These patients are then able to maintain a more normal
PaCOPaCO22 throughout the daylight hours without the need for throughout the daylight hours without the need for
mechanical ventilation.mechanical ventilation.

16161616
Hypoxemic Hypercapnic
IPPVIPPV Augment ventilationAugment ventilation
CPAPCPAPRecruit lung unitsRecruit lung unitsDecrease afterloadDecrease afterload Offset PEEPiOffset PEEPi
Modes of Ventilation

17171717
Synchrony between patient effort and delivered assistanceSynchrony between patient effort and delivered assistance NPPV with PSV is superior to (ABG and RMR)NPPV with PSV is superior to (ABG and RMR)
• spontaneous breathingspontaneous breathing1-51-5
• CPAPCPAP Comparison to volume-cycled ventilation (COPD)Comparison to volume-cycled ventilation (COPD)66
• equally effective in improving gas exchangeequally effective in improving gas exchange
• better tolerated and lower incidence of complicationsbetter tolerated and lower incidence of complications
• lower mask air leakage (lower peak mask pressure)lower mask air leakage (lower peak mask pressure)
Synchrony between patient effort and delivered assistanceSynchrony between patient effort and delivered assistance NPPV with PSV is superior to (ABG and RMR)NPPV with PSV is superior to (ABG and RMR)
• spontaneous breathingspontaneous breathing1-51-5
• CPAPCPAP Comparison to volume-cycled ventilation (COPD)Comparison to volume-cycled ventilation (COPD)66
• equally effective in improving gas exchangeequally effective in improving gas exchange
• better tolerated and lower incidence of complicationsbetter tolerated and lower incidence of complications
• lower mask air leakage (lower peak mask pressure)lower mask air leakage (lower peak mask pressure)
Mask Inspiratory Pressure SupportMask Inspiratory Pressure Support
1. Appendeni AJRCCM 19941. Appendeni AJRCCM 1994 3. Broachard NEJOM 19903. Broachard NEJOM 1990 5. Ambrosino Chest 19925. Ambrosino Chest 1992
2. Belman Chest 19902. Belman Chest 1990 4. Carrey Chest 19904. Carrey Chest 1990 6. Vitacca ICM 19936. Vitacca ICM 1993
1. Appendeni AJRCCM 19941. Appendeni AJRCCM 1994 3. Broachard NEJOM 19903. Broachard NEJOM 1990 5. Ambrosino Chest 19925. Ambrosino Chest 1992
2. Belman Chest 19902. Belman Chest 1990 4. Carrey Chest 19904. Carrey Chest 1990 6. Vitacca ICM 19936. Vitacca ICM 1993

18181818
Effect of Mask Pressure Effect of Mask Pressure
COPD patient with acute exacerbationCOPD patient with acute exacerbationCOPD patient with acute exacerbationCOPD patient with acute exacerbation
PSV 15 cmHPSV 15 cmH22OO
Positive Pes swings
Additional reduction
PSV 12 cmHPSV 12 cmH22OO
synchrony
Reduction Pes swings
spontaneousspontaneousbreathingbreathing
AsynchronyPAM
Carrey et al. Chest 1990; 97:150Carrey et al. Chest 1990; 97:150

19191919
Timing to Suppression of EMG Activity Timing to Suppression of EMG Activity
Carrey et al. Chest 1990; 97: 150.Carrey et al. Chest 1990; 97: 150.Carrey et al. Chest 1990; 97: 150.Carrey et al. Chest 1990; 97: 150.
Initiation of NPPV
Within5 breathes

20202020
Mask CPAP and PSV in COPDCritical Pdi max
Mask CPAP and PSV in COPDCritical Pdi max
Seven COPD patients with acute exacerbation Seven COPD patients with acute exacerbation Nasal mask - 15 min. recordingsNasal mask - 15 min. recordingsSeven COPD patients with acute exacerbation Seven COPD patients with acute exacerbation Nasal mask - 15 min. recordingsNasal mask - 15 min. recordings
5 cmH5 cmH22OO 10 cmH10 cmH22OO
Appendini AJRCCM 1994; 149: 1069Appendini AJRCCM 1994; 149: 1069Appendini AJRCCM 1994; 149: 1069Appendini AJRCCM 1994; 149: 1069

21212121
Hypercapnic Hypoxemic
Gas
Exchange Transdiaphragmatic
Pressure Gas
Exchange Transdiaphragmatic
Pressure
CPAP —
PSV
CPAP + PSV
Hypercapnic Hypoxemic
Gas
Exchange Transdiaphragmatic
Pressure Gas
Exchange Transdiaphragmatic
Pressure
CPAP —
PSV
CPAP + PSV
Data obtained from:Data obtained from: Ambrosino Ambrosino ChestChest 1992; 1992; Apprendini Apprendini AJRCCMAJRCCM 1994; 1994; Brochard Brochard NEJOMNEJOM 1990; 1990; Carrey Carrey ChestChest 1990; 1990; De Lucas De Lucas ChestChest 1993; 1993; Elliot Elliot Anaesthesia Anaesthesia 19941994
Data obtained from:Data obtained from: Ambrosino Ambrosino ChestChest 1992; 1992; Apprendini Apprendini AJRCCMAJRCCM 1994; 1994; Brochard Brochard NEJOMNEJOM 1990; 1990; Carrey Carrey ChestChest 1990; 1990; De Lucas De Lucas ChestChest 1993; 1993; Elliot Elliot Anaesthesia Anaesthesia 19941994
Effects of CPAP and IPPVEffects of CPAP and IPPVHypercapnic vs Hypoxemic ARFHypercapnic vs Hypoxemic ARF
Effects of CPAP and IPPVEffects of CPAP and IPPVHypercapnic vs Hypoxemic ARFHypercapnic vs Hypoxemic ARF








![Antonelli, Nature & Purpose of Numbers [21 pgs]](https://img.pdfslide.us/doc/110x75/577cdfe91a28ab9e78b243ff/antonelli-nature-purpose-of-numbers-21-pgs.jpg)