Embed Size (px)
Citation preview

Health Education & Behavior 1 –13© 2014 Society for PublicHealth EducationReprints and permissions: sagepub.com/journalsPermissions.navDOI: 10.1177/1090198114558588heb.sagepub.com
Article
A high prevalence of suboptimal control of blood pressure (BP) in Malaysian patients with hypertension is attributed to a low awareness about hypertension, poor treatment compli-ance, and lack of support education (Ministry of Health Malaysia, 2006). Cognitive health education is nonexistent in primary health care clinics in Malaysia, with treatment provided only by general practitioners (GPs), without any allied health support. This situation occurs because health care is not subsidized for patients. This practice results in suboptimal management and poor outcomes among patients on antihypertensive treatment (S. C. Chan et al., 2005; Ramli & Taher, 2008). Health education support to optimize chronic disease management (CDM) and promote patient self-effi-cacy is therefore vital in Malaysia.
The Community-Based Cardiovascular Risk Factors Intervention Strategies (CORFIS) program was a 2-year multicentre pilot trial to test the chronic care model for incor-porating multidisciplinary health care into PHC clinics (Bodenheimer, Wagner, & Grumbach, 2002; Low et al.,
558588 HEBXXX10.1177/1090198114558588Health Education & BehaviorKarupaiah et al.research-article2014
1National University of Malaysia, Kuala Lumpur, Malaysia2University of Malaya, Kuala Lumpur, Malaysia3International Medical University, Kuala Lumpur, Malaysia
Corresponding Author:Tilakavati Karupaiah, Dietetics Program, School of Healthcare Sciences, Faculty of Health Sciences, National University of Malaysia, Selangor, 50300 Kuala Lumpur, Malaysia. Email: [email protected]; [email protected]
Metering Self-Reported Adherence to Clinical Outcomes in Malaysian Patients With Hypertension: Applying the Stages of Change Model to Healthful Behaviors in the CORFIS Study
Tilakavati Karupaiah, PhD, APD1, Kimberly Wong, MSc1, Karuthan Chinna, PhD2, Kanimolli Arasu, MSc1,3, and Winnie Siew Swee Chee, PhD3
AbstractThe CORFIS (Community-Based Cardiovascular Risk Factors Intervention Strategies) program was piloted in community clinics in Malaysia to address the lack of health education in chronic disease management. The stages of change model was applied in a multicenter quasi-experimental design to evaluate adherence to advocated behaviors in CORFIS patients with hypertension. Based on submitted diet and exercise records (n = 209), adherence to sodium reduction, regular exercise, and increasing fruit and vegetable intake behaviors were quantified against weight, waist circumference (WC), systolic blood pressure (SBP), and diastolic blood pressure (DBP) changes. Patients were categorized at 6 months into nonadherent/N-A (Precontemplation, Contemplation, and Preparation), newly adherent/NA (Action) and totally adherent/TA (Maintenance) groups. Self-reported adherence records did not meet recommended targets for healthful behaviors, but clinical benefits were achieved by adherent groups as indicated by effect size (Cohen’s d) comparisons. SBP reduction was associated with adherence to sodium reduction in NA (d = 0.60, p < .001) and TA (d = 0.45, p < .001) compared to N-A (d = 0.13, p > .05). Marginally increasing fruit and vegetable consumption (Δ = 0.41 servings) resulted in sizeable reductions in weight for NA (d = 0.81, p < .001) > TA (d = 0.54, p < .001) > N-A (d = 0.21, p > .05) and in WC for NA (d = 0.68, p < .00) > TA (d = 0.53, p < .001) > N-A (d = 0.52, p > .05). Exercise behavior was least successful as pedometer counting was below 10,000 steps but sizeable weight and WC reductions were largest for NA (d = 0.71 and 0.79, respectively) > TA (d = 0.60 and 0.53, respectively) > N-A (d = 0.33 and 0.35, respectively). Patients reporting a shift to positive stages of change behaviors enjoyed clinically beneficial reductions in SBP, DBP, weight, and WC.
Keywordsadherence, diet, exercise, healthful behaviors, hypertension, stages of change

2 Health Education & Behavior
2013). Nursing educators, pharmacists, and dieticians sup-ported GPs in CORFIS clinics. Lifestyle behaviors including healthy diet and physical activity are critical for moderating pathophysiological outcomes in CDM in addition to medica-tions (Appel et al., 2006; Dickinson et al., 2006; Whelton, Chin, Xin, & He, 2002). Yet uncertainty remains on how to assess effectiveness of strategies that promote patient adher-ence to these lifestyle behaviors (Weingarten et al., 2002). Atkins and Michie (2013) suggest that this is due to subopti-mal reporting compared with literature on pharmacological interventions where the formula, dosage, and mechanism of action are precisely reported. This is further compounded by a lack of or insufficient information on the content of behav-ior change interventions (Glasziou, Meats, Heneghan, & Shepperd, 2008). One noteworthy intervention used the transtheoretical model (TTM) as a structured approach facil-itating improved health and food behavior change relating to glycemic control (Jones et al., 2003). J. J. Prochaska and Prochaska (2011) suggest that most health promotion research tends to address risk factors as categorically sepa-rate entities as little is known about how to effectively pro-mote multiple health behavior change.
The realization of self-behavior is a crucial starting point for successful behavior change as theorized by the “precau-tion adoption process model” (PAPM; Weinstein, Rothman, & Sutton, 1998). However, PAPM explains only the transla-tional process taken by an individual to convert decision into action, such as cessation of risky behavior requiring deliberate conscious awareness. PAPM, therefore, would not be suitable for the gradual development of habitual pat-terns of behavior, such as exercise and diet (Weinstein, Sandman, & Blalock, 2008). Since targeted behaviors in lifestyle management are clearly specified for BP control, a theory-driven approach assessing behavior change relative to health goals is needed in evaluating program effective-ness (Atkins & Michie, 2013). Behavior change is recog-nized to be a process, not an event, with individuals at various levels of motivation or “readiness to change” (J. O. Prochaska & DiClemente, 1983). TTM or the stages of change (SOC) model was originally applied in the health psychology field related to the management of addictive behavior (Dijkstra, de Vries, & Bakker, 1996). The model is mostly applied to single behavior health promotions target-ing smoking cessation, alcohol addiction, dietary fat reduc-tion, fiber increase, increasing fruit and vegetable intake, exercise promotion, or generalized healthy eating (Kristal, Beresford, & Lazowich, 1999). Behavior change, according to the SOC construct, occurs through five distinct stages based on people’s current behavior and their intention to change (J. O. Prochaska et al., 1994). The five stages com-mon to SOC are Precontemplation (no intention to change), Contemplation (thinking about change in the future), Preparation (preparing to change), Action (implementing an action plan to modify behavior), and Maintenance (desir-able actions sustained over a period; J. O. Prochaska &
DiClemente, 1983). However, people do not necessarily progress through SOC in chronological order, and relapsing to earlier stages does occur (J. O. Prochaska & Velicer, 1997). The stage construct enables categorization of patient behaviors specific to health promotion as well as the appli-cation of motivational tools to facilitate transition from a negative to a positive stage of behavior (Horwath, 1999). Transition between stages over time permits assessment of patient adherence to target behaviors and identifies types of interventions that will be most effective at each stage of change (Kristal, Beresford, & Lazowich, 1999).
Povey, Conner, Sparks, James, and Shepherd (1999) viewed the application of TTM’s SOC to dietary behaviors as problematic because the model was originally designed for addictive behavior. The likelihood of a mismatch between perceived and actual dietary behavior would increase with generalized dietary recommendations and more so if applied outside the clinical context such as in health promotion (Povey et al., 1999). We, however, felt that the 6-month CORFIS interventional design provided an appropriate clini-cal context for the application of SOC, with defined end points for the multiple specific dietary behaviors and suffi-cient exposure time for nutrition counseling to overcome these limitations. Our intention, therefore, was to apply the SOC model to assess behaviors related to regular exercise, reduction in salt intake, and increased fruit and vegetable consumption in CORFIS patients with hypertension, and we hypothesized that adherence to these behaviors would mod-erate clinical outcomes related to BP control.
Method
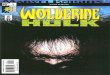
The CORFIS study was approved by the Medical Ethics Committee of the Ministry of Health Malaysia. GP clinics registered in the National Medical Health Directory for the Klang Valley were invited to participate. The 70 consenting clinics were allocated in a 2:1 ratio into intervention or con-trol arms. As the study was not blinded, more patients were less willing to join the control arm as they appreciated the provision of multidisciplinary care in the intervention arm, which was absent in the standard care model. Patient recruit-ment within each clinic was performed by the GP for a maxi-mum of 10 patients based on notification by the first 10 registrants. A total of 486 patients with hypertension pro-vided their consent to participate. From these patients, 309 met the inclusion/exclusion criteria of 18 years and older, and they were without complications associated with diabe-tes, hypertension, and cardiovascular diseases such as nephropathy, neuropathy, or ischemia. Women who were pregnant or nursing were excluded. Of the 309, a total of 302 patients agreed to participate in the dietician-provided coun-seling sessions and met study protocol requirements. The study flow of patients is presented in Figure 1. The primary outcomes considered in this study have been reported else-where (Low et al., 2013).

Karupaiah et al. 3
Study Design
A multicenter quasi-experimental design was adopted for the dietary intervention arm of CORFIS. Eligible patients received the lifestyle modification program provided by dieticians.
Demographics
The mean age of patients was 48.5 ± 9.4 years, with 194 (64.2%) men and 108 (35.8%) women (Table 1). Patients were typically sedentary, middle-aged, and living within an urban community.
Clinical History
At study initiation, 23.8% of patients had hypertension only, 16.6% had hypertension and diabetes mellitus, 27.8% had hypertension and dyslipidemia, while 31.8% had all three primary noncommunicable diseases (Table 1). Mean dura-tion of diagnosis for hypertension was 57.3 ± 60.7 months; 47.4% of patients at baseline had good systolic control (<130 mmHg) and 42.7% had good diastolic control (<85 mmHg).
Anthropometry Assessment
Mean body mass index (BMI) of patients was 29.28 ± 5.24 kg/m2. Many patients were overweight (40.4%), whereas 27.2% of patients were in Obese 1, 9.9% in Obese II, and 3.0% in Obese III categories (World Health Organisation,
2000). Patients mean waist circumference (WC) was 100.45 ± 11.70 cm for men and 90.46 ± 10.90 cm for women. As per guideline cutoffs, 80.4% of men and 82.4% women had WC > 90 cm and WC > 80 cm, respectively (Ministry of Health Malaysia, 2009).
Program Team
The core multidisciplinary health care team at each interven-tion clinic comprised its GP and the CORFIS-assigned nurse, dietician, and pharmacist. Thirty dieticians were employed on a part-time basis to provide lifestyle counseling targeting healthful behaviors.
Healthful Behaviors
Three healthy lifestyle behaviors related to BP control were identified for dietician moderation, namely, reducing salt intake, regular exercise, and increasing fruit and vegetable intakes (Appel et al., 2006; Dickinson et al., 2006; Sacks et al., 2001; Svetkey, 2004; Whelton et al., 2002). Patients were instructed to exercise regularly by targeting >10,000 steps daily (Tudor-Locke, Bassett, et al., 2008; Tudor-Locke, Hatano, Pangrazi, & Kang, 2008).
Patient Protocol
Enrolled patients received monthly dietician counseling with seven individual appointments provided over 6 months.
General practicesenrolled into CORFIS
(n=70)
Hypertensive patients recruited forusual care management (n=177)
General practices inControl Group (n=26)
General practices in intervention(n=44)
Hypertensive patients eligible forrecruitment (n=309)
Patients who attended dietary counseling sessions (n=302)
Completion of 6-month trial with self-monitoring dietary and exercise records (n=209/ 309; 67.6%)
Failed to submit dietary records andexercise diaries
(n=93)7 uninterested in joining dietician
counseling sessions
Figure 1. Study flow for patient participation.Note. The bold arrow represents the intervention arm of CORFIS (Community-Based Cardiovascular Risk Factors Intervention Strategies) with dietician counseling provided for lifestyle management.

4 Health Education & Behavior
Table 1. Descriptive Characteristics of Patient Population (n = 302).
Parameters M ± SD or n (%)
Age (years) 48.5 ± 9.4Gender Male 194 (64.2) Female 108 (35.8)Education level Primary school 16 (5.3) High school 137 (45.4) Tertiary 114 (37.7) Other 35 (11.6)Occupation Professionals 42 (20.1) Housewives/retired/unemployed 35 (16.7) Technicians, associate professionals 34 (16.3) Clerical workers 32 (15.3) Retail sales services 30 (14.4) Senior management 18 (8.6) Elementary occupations 8 (3.8) Machine operators, assemblers 5 (2.4) Craft artisans 4 (1.9) Agriculturalist 1 (0.5)Ethnicity Malay 136 (45.0) Chinese 95 (31.5) Indian 63 (20.9) Others 8 (2.6)Clinical history Hypertension only 72 (23.8) Hypertension + diabetes mellitus 50 (16.6) Hypertension + dyslipidaemia 84 (27.8) Hypertension + dyslipidaemia + diabetes mellitus 96 (31.8)Hypertension duration (months) 57.3 ± 60.7Systolic blood pressurea 135.1 ± 16.4 Controlled (<130 mmHg) 143 (47.4) Uncontrolled (>130 mmHg) 159 (52.6)Diastolic blood pressurea 84.8 ± 10.2 Controlled (<85 mmHg) 129 (42.7) Uncontrolled (>85 mmHg) 173 (57.3)Weight (kg) 78.44 ± 15.99Body mass index (kg/m2)b 29.28 ± 5.24 Overweight (25.0–29.99) 122 (40.4) Obese I (30.0–34.99) 82 (27.2) Obese II (35.0–39.99) 30 (9.9) Obese III (>40.0) 9 (3.0)Waist circumference (cm)c
Men (cm) 99.26 ± 12.40 <90 28 (23.0) ≥90 97 (77.0) Women 89.86 ± 10.66 <80 14 (16.9) ≥80 69 (83.1)
aBlood pressure control as defined in Clinical Practice Guideline Management of Hypertension, Ministry of Health Malaysia (2008). bBody mass index class distribution cutoffs as proposed by World Health Organization (2000). cWaist circumference cutoff limits as defined in Clinical Practice Guideline Management of Type 2 Diabetes Mellitus, Ministry of Health Malaysia (2009).

Karupaiah et al. 5
Standard household measuring tools such as cup, rice bowl, tablespoon, and teaspoon were issued to patients in order to facilitate accuracy of food portion recording in dietary records. A pedometer was provided to monitor daily number of footsteps, which was recorded in an exercise diary. Patients’ dietary and exercise records were reviewed during each appointment. Brochures produced by CORFIS on the hypertension diet, food exchange system, tips on eating out, reading food labels, sodium counts in foods, exercise, and weight loss were provided to patients.
Outcome Variables
Participants’ weight, WC, systolic blood pressure (SBP), and diastolic blood pressure (DBP) were measured at monthly intervals. Optimal control was set as BP of ≤140/90 mmHg for hypertensive patients without diabetes or chronic kidney disease and ≤130/80 mmHg for those with diabetes (Ministry of Health Malaysia, 2008).
Diet Analysis
To assess dietary intake, three 24-hour diet recalls were col-lected at monthly intervals. Records were analyzed with NutriPro software (Version 3.2.0), which includes databases for Malaysian foods (First DataBank/Hearst Corporation, 2005; Ministry of Health, Singapore, 2000; Tee, Ismail, Azudin, & Khatijah, 1997).
Physical Activity
The volume of physical activity reported by patients was cal-culated as metabolic equivalent (MET) scores as determined by the short form of the International Physical Activity Questionnaire (IPAQ; http://www.ipaq.ki.se/) at baseline and end of study (Craig et al., 2003). Average pedometer steps for the beginning and last weeks of the intervention period were also recorded as a measure of physical activity.
Assessment of SOC
An SOC form was issued to participating patients to record their SOC for each targeted behavior change. Patients com-pleted SOC assessment at baseline in the first week of inter-vention before the first counseling session and after completing their final dietician appointment.
Adherence to Medication
Medication adherence was tracked by CORFIS pharmacists. Details of adherence and standard medication protocol have been described elsewhere (Chua et al., 2012). Prescription pattern remained unchanged over 6 months, except for pos-sible increase in dosage.
Statistical Analysis
Continuous data were described as mean ± standard deviation with 95% confidence intervals, and categorical data were described in frequencies and percentages. An intention-to-treat analysis was included for all medical data. Missing data at the last follow-up were imputed by the last observation car-ried forward method. For the analysis, patients were classified into two groups: those who submitted their diet and exercise records as “completers” and those who failed to do so as “non-completers.” Within-group analysis was also performed to evaluate differences between medication treatments. Initially, changes over time within the two groups were analyzed using paired samples t test. The between-group differences were analyzed using independent samples t test. Clinical outcomes due to medication change were also verified by grouping patients into either standard prescription with fixed dose or modified prescription with increased dosage for BP optimiza-tion. Changes between baseline and 6 months for weight, WC, SBP, and DBP were tested using repeated measures analysis of covariance, controlling for age and sex. Therefore, the base-line values, 6-month values, and change scores were reported as mean ± standard error of the mean. Effect sizes were com-puted using Cohen’s d to compare magnitude of changes for each variable and were interpreted as negligible (<.2), moder-ate (~.5), and large (>.8; Cohen, 1988). Adjustments were made by taking into account the number of hypothesis tests for adjusting the critical p value by using the Benjamini–Horchberg approach. All data analyses were carried out using the IBM SPSS Statistics Version 20.0 software. Significance was interpreted at p < .05.
Results
On study completion, there were 209 (67.6%) “completers” who submitted completed records for advocated healthful behaviors and 93 “noncompleters” (n = 93) who did not sub-mit these records. In the initial analysis, comparisons between completers and noncompleters indicated improved outcomes for BP, weight, BMI, and WC, which were not sig-nificantly different (p > .05) between the two patient groups (Table 2).
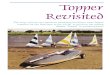
All patients were recategorized into three behavior groups based on their self-reported compliancy with advocated healthful behaviors (Figure 2). Patients remaining in Precontemplation, Contemplation, and Preparation stages or regressed at study end were classified as “nonadherent.” Patients transitioning from noncompliance to adoption of healthful behaviors by 6 months were designated as “newly adherent,” and those still in the “Maintenance” stage for behaviors were grouped as “totally adherent.” The break-down of patients according to adherence level is indicated in Table 3 in relation to targeted healthful behaviors. Trends indicated patients were less compliant with advocated exer-cise compared to the dietary behaviors.

6 Health Education & Behavior
Adequacy of Self-Reported Behaviors Categorized by SOC in Relation to Health Outcomes for Completers (n = 209)
Effect of Medication Change. (See Supplementary Table 1, available online at heb.sagepub.com/supplemental.) Among completers, 65 patients had their medication volume changed during the intervention. These patients compared to standard therapy patients had a higher mean SBP (141.6 ± 15.9 vs. 131.6 ± 14.7 mmHg) and DBP (88.7 ± 10.3 vs. 82.7 ± 9.5 mmHg) at baseline, indicating greater degree of uncontrolled hypertension. After intervention, the modified
therapy compared to standard therapy group achieved greater reduction in SBP (−12.1 ± 17.6 vs. −5.7 ± 14.9 mmHg, p = .022), but reduction in DBP (−7.7 ± 121.6 vs. −4.2 ± 11.2 mmHg, p > .05) was not significant between groups. As indicated by effect size (d) comparisons (0.69 vs. 0.38 and 0.62 vs. 0.38 for SBP and DBP, respectively), changes almost doubled with modified therapy. There were no significant differences in reductions in weight, WC, and BMI between the two groups (p > .05).
Exercise. Regular exercise, measured as daily pedometer steps, increased significantly (+898 ± 3167, p < .001,
Table 2. Intervention Outcomes for All Patients (n = 302).
Intervention outcomesAll patient recruitment
(n = 302)Completers (n = 209)
Noncompleters (n = 93) Between-group pa
Systolic blood pressure (mmHg) Before 135.1 ± 16.4 134.7 ± 15.8 135.9 ± 15. 8 .547 After 127.5 ± 14.1 126.9 ± 14.1 128.8 ± 14.3 .318 M 7.6 ± 15.9 7.7 ± 16.0 7.2 ± 15.5 .789 95% CI [5.8, 9.4] [5.5, 9.9] [4.0, 10.4] % change 5.6 5.7 5.3 pb (d) <.001 (0.48) <.001 (0.48) <.001 (0.46) Diastolic blood pressure (mmHg) Before 84.8 ± 10.2 84.6 ± 10.1 85.2 ± 10.4 .635 After 79.6 ± 9.6 79.3 ± 9.8 80.3 ± 9.3 .390 M 5.2 ± 11.1 5.3 ± 11. 8 4.9 ± 9.3 .758 95% CI [3.9, 6.5] [3.7, 6.9] [3.0, 6.8] % change 6.1 6.3 5.7 pb (d) <.001 (0.47) <.001 (0.45) <.001 (0.52) Weight (kg) Before 78.4 ± 16.0 77.1 ± 15.9 81.6 ± 15.9 .024 After 76.9 ± 15.7 75.4 ± 15.5 80.3 ± 15.7 .012 M 1.5 ± 2.9 1.7 ± 2.9 1.2 ± 2.8 .241 95% CI [1.2, 1.8] [1.3, 2.1] [0.6, 1.8] % change 2.0 2.2 1.5 pb (d) <.001 (0.53) <.001 (0.58) <.001 (0.44) Body mass index (kg/m2) Before 29.3 ± 5.3 28.9 ± 5.2 30.1 ± 5.2 .078 After 28.7 ± 5.2 28.3 ± 5.1 29.6 ± 5.1 .041 M 0.6 ± 1.1 0.6 ± 1.0 0.5 ± 1.1 .222 95% CI [0.5, 0.7] [0.5, 0.7] [0.3, 0.7] % change 1.9 2.1 1.5 pb (d) <.001 (0.54) <.001 (0.59) <.001 (0.42) Waist circumference (cm) Before 96.9 ± 12.4 95.5 ± 12.6 99.9 ± 11.4 .004 After 94.8 ± 12.2 93.5 ± 12.6 97.7 ± 10.8 .006 M 2.1 ± 4.6 2.0 ± 5.0 2.2 ± 3.5 .754 95% CI [1.6, 2.6] [1.3, 2.7] [1.5, 2.9] % change 2.1 2.1 2.2 pb (d) <.001 (0.44) <.001 (0.40) <.001 (0.62)
Note. CI = confidence interval. Completers are those who submitted health records, whereas noncompleters did not submit these records. Values reported for measured outcomes are M ± SD. Cohen’s d effect size: negligible (<.2), moderate (~.5), and large (>.8).ap value from independent t test. bp value and effect sizes from paired t test

Karupaiah et al. 7
24.8
37.4 37.7
26.5
66.2
7.3
20.9
70.5
8.6
28.2
41.6
30.1 29.3
65.6
5.3
24.9
69.9
5.3
17.2
28.0
54.8
20.4
67.7
11.8 11.8
72
16.1
0
10
20
30
40
50
60
70
80
Newl
y Adh
eren
t
Total
ly Ad
here
nt
Non-
Adhe
rent
Newl
y Adh
eren
t
Total
ly Ad
here
nt
Non-
Adhe
rent
Newl
y Adh
eren
t
Total
ly Ad
here
nt
Non-
Adhe
rent
Regular Exercise Salt Reduction Increasing Fruit and Vegetable Intake
Perce
nt Pa
tient
Distr
ibutio
n (%
)
Self-reported Behavior Change as per SOC
All (302) Completers (n=209) Non-Completers (n=93)
Figure 2. Self-reported behaviors as per SOC for targeted healthful behaviors.Note. SOC = stages of change.
Table 3. Patient Adherence to Targeted Healthful Behaviors (n = 209).
SOC categoriesa Baseline Final ΔChange 95% CI p (d)
Sodium intake (mg) Nonadherent (n = 11) 3,256 ± 967 3,096 ± 835 −160 ± 485 [−486, 166] .298 (0.33) Newly adherent (n = 61) 3,073 ± 771 2,796 ± 928 −276 ± 945 [−518, −34] .026 (0.29) Totally adherent (n = 137) 3,079 ± 862 2,720 ± 938 −359 ± 911 [−513, −205] <.001 (0.39)Pedometer steps (counts per day) Nonadherent (n = 63) 5,882 ± 3,696 6,428 ± 2,566 +546 ± 3,050 [−222, 1314] .074 (0.18) Newly adherent (n = 71) 7,114 ± 4,040 7,844 ± 2,982 +730 ± 2,587 [118, 1342] .006 (0.28) Totally adherent (n = 75) 6,817 ± 3,317 8,170 ± 3,320 +1,353 ± 3,704 [501, 2205] .001 (0.37)Total activity (MET, minutes/week) Nonadherent(n = 63) 846 ± 1,194 773 ± 1,035 −74 ± 1,300 [−401, 253] .667 (0.06) Newly adherent (n = 71) 1,283 ± 1,742 1,636 ± 1,926 +353 ± 1,572 [−19, 725] .067 (0.22) Totally adherent (n = 75) 1,293 ± 1,497 1,456 ± 1,278 +164 ± 1,632 [−211, 539] .129 (0.10)Fruits and vegetable intake (servings) Nonadherent (n = 11) 3.09 ± 1.03 2.50 ± 1.88 −0.59 ± 2.02 [−1.95, 0.77] .355 (0.29) Newly adherent (n = 52) 2.88 ± 1.81 3.41 ± 1.61 +0.53 ± 1.52 [0.11, 0.95] .016 (0.35) Totally adherent (n = 146) 3.63 ± 1.76 4.07 ± 1.86 +0.44 ± 1.83 [0.14, 0.74] .004 (0.24)
Note. SOC = stages of change; Δ = change difference in outcomes; CI = confidence interval; MET = metabolic equivalent. Values are M ± SD; significance = p < .05; Cohen’s d effect size: negligible (<.2), moderate (~.5), and large (>.8). Note on statistical analysis: After correcting using Benjamini–Horchberg procedure, there were significant positive changes (p < .05) in reported behaviors for fruits and vegetables intake, pedometer steps, and sodium intake in the newly adherent and totally adherent groups. There was also a change in pedometer steps for the nonadherent group but was not significant (p > .05).aNonadherent = includes patients at Precontemplation (no intention to change), Contemplation (thinking to change), and Preparation (preparing to change) stages of SOC; newly adherent = patients in Action stage (reporting change during 6 months of intervention); and totally adherent = patients in Maintenance stage for whom change became a habit before study initiation.
d = 0.28) from baseline to 6 months. Average weekly MET scores, measured by IPAQ, were 1,154 ± 1,511 minutes at
baseline and 1,311 ± 1,510 after 6 months. This increase (+157 ± 1,521 minutes, p > .05) was not significant.

8 Health Education & Behavior
Dietary Intake. With intervention, patients significantly reduced energy (−237 ± 379 kcal, p < .001), carbohydrate (−30.9 ± 65.5 g, p < .001), protein (−8.9 ± 21.4 g, p < .001), and fat (−8.9 ± 21.4 g, p = .001) intakes. Fiber intake increased marginally (0.9 ± 7.2 g, p = .072). Mean sodium intake changed from 3,087 ± 839 mg to 2,762 ± 930 mg (p < .001, d = 0.36). Fruit (before/after = 1.02 ± 1.01 vs. 1.20 ± 0.99 servings, difference = 0.18 ± 0.89, p = .005, d = 0.20) and vegetable (before/after = 2.40 ± 1.31 vs. 2.63 ± 1.34 servings, difference = 0.23 ± 1.43, p = .02, d = 0.16) intakes marginally increased. Changes in dietary intake were similar for both medication groups (p > .05).
Measuring Behaviors as Per SOC. Change in regular exercise behavior was measured by pedometer steps and IPAQ scores (Table 3). The nonadherent group marginally increased their pedometer steps (546 ± 3,050 steps, p > .05) in contrast to significant increases by newly adherent (730 ± 2,587 steps, p = .006) and totally adherent (1,353 ± 3,704 steps, p = .002) groups. No significant changes in total MET mean scores were observed between groups (p > .05). Sodium restriction behavior was least successful for nonadherent behavior (−160.5 ± 484.6 mg, p = .298, d = 0.33) compared to newly adherent (−276.3 ± 945.1 mg, p = .026, d = 0.29) and totally adherent (−359.0 ± 911.6 mg, p < .001, d = 0.39) groups. In terms of increasing fruit and vegetable intakes, nonadherent patients reported fewer servings (−0.59 ± 2.02 servings, p = .355; d = 0.29) compared with newly adherent (+0.53 ± 1.52, p = .016, d = 0.35) and totally adherent (+0.44 ± 1.83, p = .004, d = 0.24) groups.
Patient Adherence. Changes in measured outcomes were compared against level of adherence to targeted behaviors (Table 4).
Patients reported compliance to increasing pedometer steps, reflected in greater weight and WC reductions. For weight loss, newly adherent (−1.8 ± 0.3 kg, p < .001, d = 0.71) and totally adherent (−1.9 ± 0.4 kg, p < .001, d = 0.60) groups achieved greater reductions compared to nonadherent (−1.0 kg, p = .010, d = 0.33) group. Similarly, newly adher-ent (−2.7 ± 0.4 cm, p < .001, d = 0.79) and totally adherent (−2.3 ± 0.5 cm, p < .001, d = 0.53) groups achieved greater reductions in WC compared to the nonadherent (−1.4 ± 0.5 cm, p = .007, d = 0.35) group. All groups achieved similar reductions in SBP (nonadherent, d = 0.43; newly adherent, d = 0.52; totally adherent, d = 0.45) by being compliant to increasing pedometer steps. However, a significant effect of increasing pedometer steps was observed for DBP with newly adherent (−6.1 ± 1.4 mmHg, p < .001, d = 0.52) and totally adherent (−6.5 ± 1.3 mmHg, p < .001, d = 0.59) groups compared to the nonadherent group (−2.8 ± 1.7 mmHg, p = .114, d = 0.20).
For salt reduction behavior, only adherent patients showed significant improvements in SBP, DBP, weight, and WC
outcomes. The largest impact, a 38% reduction in SBP, was achieved by the newly adherent group (−10.2 mmHg, d = 0.60) compared to overall CORFIS mean reduction (−7.6 mmHg, d = 0.47; Low et al., 2013). A similar pattern of benefit was observed in adherent patients increasing fruit and vegetable intake behavior.
Discussion
There is uncertainty on how to assess effectiveness of behav-ior change strategies related to multidisciplinary health inter-ventions (Atkins & Michie, 2013). We chose to use Prochaska’s SOC model to meter patients’ adherence to advocated behaviors, namely, regular exercise, reducing salt intake, and increasing fruit and vegetable intakes. Transition between stages was measured by comparing self-reported SOC with data from patient records. We did not find any problems with operationalization of the SOC model as sug-gested by Povey et al. (1999).
A key finding of this study was that patient-reported com-pliance to advocated healthful behaviors produced clinically beneficial reductions in SBP, DBP, weight loss, and WC. These benefits were most pronounced in newly adherent patients and least in nonadherent patients from Precontemplation, Contemplation, and Preparation stages. These findings were consistent with other studies reporting the largest dietary change occurring in Maintenance and Action stages but essentially no change in the preaction stage (Glanz et al., 1998; Kristal, Glanz, Tilley, & Li, 2000). Our finding therefore may dispute a main critique of TTM—which is that for desired behaviors such as “healthy eating” or “regular exercise,” the goal is much more nebulous, hard to define, and open to subjective interpretation on the part of those making the change (Brug et al., 2005).
Salt reduction by patients did not reach the recommended dietary goal of less than 2,300 mg (Appel et al., 2006), but newly adherent and totally adherent patients who were con-sciously making positive change in this behavior achieved significant reductions in SBP, DBP, weight, and WC as rec-ommended. The intake of 3.83 servings of fruits and vegeta-bles after 6 months was distant from the Dietary Approaches to Stop Hypertension trial’s goal of 8 to 10 servings per day (Svetkey et al., 2004). Poor dietary habits are implicated as only 40% of Malaysians are reported to be eating vegetables daily with national averages of 1.5 vegetable and 2.0 fruit servings (Hall, Moore, Harper, & Lynch, 2009; Karim et al., 2008). Similar to our study, a cognitive-based program also reported modest changes in sodium (−290 mg) and vegetable (+3.0 serves/week) intake by overweight hypertensive patients, which still enabled weight (−2.5 kg) and WC (−3.1 cm) reductions (Burke et al., 2007).
The least successful behavior measured in the study related to exercise. Achieving >10,000 steps daily is a quan-titative standard recommended for CDM (C. B. Chan, Ryan,

Karupaiah et al. 9
Table 4. Effect of Patient Adherence to Lifestyle Behaviors on Clinical Outcomes.
SOC categories n Baseline Final ΔChange 95% CI p (d)
Increasing pedometer steps SBP (mmHg) Nonadherenta 63 135.6 ± 2.2 128.1 ± 1.9 −7.5 ± 2.2 [−11.9, −3.1] .001 (0.43) Newly adherent 71 133.3 ± 1.9 125.5 ± 1.6 −7.7 ± 1.8 [−11.3, −4.1] <.001 (0.52) Totally adherent 75 135.2 ± 1.8 127.5 ± 1.8 −7.7 ± 2.0 [−11.7, −3.7] <.001 (0.45) DBP (mmHg) Nonadherenta 63 85.9 ± 1.3 82.1 ± 1.3 −2.8 ± 1.7 [−6.2, 0.6] .114 (0.20) Newly adherent 71 84.1 ± 1.2 78.1 ± 1.2 −6.1 ± 1.4 [−8.9, −3.3] <.001 (0.52) Totally adherent 75 84.6 ± 1.2 78.1 ± 1.0 −6.5 ± 1.3 [−9.1, −3.9] <.001 (0.59) Weight (kg) Nonadherenta 63 78.9 ± 2.1 77.9 ± 2.1 −1.0 ± 0.4 [−1.8, −0.2] .010 (0.33) Newly adherent 71 75.3 ± 1.5 73.5 ± 1.5 −1.8 ± 0.3 [−2.4, −1.2] <.001 (0.71) Totally adherent 75 73.4 ± 1.4 71.5 ± 1.3 −1.9 ± 0.4 [−2.7, −1.1] <.001 (0.60) Waist circumference (cm) Nonadherenta 63 98.5 ± 1.7 97.1 ± 1.6 −1.4 ± 0.5 [−2.4, −0.4] .007 (0.35) Newly adherent 71 93.3 ± 1.3 90.7 ± 1.2 −2.7 ± 0.4 [−3.5, −1.9] <.001 (0.79) Totally adherent 75 92.3 ± 1.1 89.9 ± 1.1 −2.3 ± 0.5 [−3.3, −1.3] <.001 (0.53)Reducing sodium intake SBP (mmHg) Nonadherenta 11 128.7 ± 4.6 130.5 ± 5.7 +1.8 ± 4.1 [−7.3, 10.9] .667 (0.13) Newly adherent 61 138.4 ± 2.3 128.2 ± 1.8 −10.2 ± 2.2 [−14.6, −5.8] <.001 (0.60) Totally adherent 137 133.4 ± 1.3 126.3 ± 1.2 −7.2 ± 1.4 [−10.0, −4.4] <.001 (0.45) DBP (mmHg) Nonadherenta 11 82.8 ± 2.6 78.7 ± 3.2 −4.1 ± 2.8 [−10.3, 2.1] .177 (0.44) Newly adherent 61 84.9 ± 1.3 80.2 ± 1.4 −4.6 ± 1.6 [−7.8, −1.4] .005 (0.38) Totally adherent 137 84.5 ± 0.9 78.9 ± 0.8 −5.5 ± 1.0 [−7.5, −3.5] <.001 (0.46) Weight (kg) Nonadherenta 11 92.2 ± 6.1 91.7 ± 6.3 −0.4 ± 1.5 [−3.7, 2.9] .779 (0.09) Newly adherent 61 75.5 ± 1.7 74.0 ± 1.7 −1.5 ± 0.3 [−2.1, −0.9] <.001 (0.55) Totally adherent 137 75.1 ± 1.2 73.4 ± 1.1 −1.8 ± 0.2 [−2.2, −1.4] <.001 (0.63) Waist circumference (cm) Nonadherenta 11 106.6 ± 4.7 105.8 ± 4.5 −0.8 ± 1.0 [−3.0, 1.4] .458 (0.23) Newly adherent 61 95.4 ± 1.4 93.4 ± 1.4 −2.0 ± 0.4 [−2.8, −1.2] <.001 (0.64) Totally adherent 137 93.7 ± 1.0 91.3 ± 0.9 −2.4 ± 0.4 [−3.2, −1.6] <.001 (0.57)Increasing fruit and vegetable servings SBP (mmHg) Nonadherenta 11 134.3 ± 6.0 128.7 ± 4.0 −5.5 ± 6.0 [−18.9, 7.9] .380 (0.28) Newly adherent 52 134.3 ± 2.4 127.2 ± 2.1 −7.1 ± 2.3 [−11.7, −2.5] .003 (0.43) Totally adherent 146 134.6 ± 1.3 126.6 ± 1.2 −8.0 ± 1.4 [−10.8, −5.2] <.001 (0.50) DBP (mmHg) Nonadherenta 11 87.9 ± 4.0 81.7 ± 3.7 −6.2 ± 4.3 [−15.8, 3.4] .184 (0.43) Newly adherent 52 84.9 ± 1.3 79.3 ± 1.4 −5.5 ± 1.6 [−8.7, −2.3] .001 (0.48) Totally adherent 146 84.2 ± 0.8 79.1 ± 0.8 −5.1 ± 1.0 [−7.1, −3.1] <.001 (0.42) Weight (kg) Nonadherenta 11 83.6 ± 4.8 83.3 ± 4.9 −0.3 ± 0.4 [−1.2, 0.6] .505 (0.21) Newly adherent 52 80.2 ± 2.1 78.3 ± 2.0 −1.9 ± 0.3 [−2.5, −1.3] <.001(0.81) Totally adherent 146 74.1 ± 1.1 72.5 ± 1.1 −1.7 ± 0.3 [−2.3, −1.1] <.001 (0.54) Waist circumference (cm) Nonadherenta 11 102.0 ± 4.5 100.1 ± 4.4 −2.0 ± 1.1 [−4.5, 0.5] .117 (0.52) Newly adherent 52 97.0 ± 1.8 94.6 ± 1.7 −2.4 ± 0.5 [−3.4, −1.4] <.001 (0.68) Totally adherent 146 93.6 ± 0.9 91.4 ± 0.9 −2.1 ± 0.3 [−2.7, −1.5] <.001 (0.53)
Note. SOC = stages of change; SBP = systolic blood pressure; DBP = diastolic blood pressure; Δ = change difference in outcomes; CI = confidence interval. Values are mean ± standard error of the mean (corrected for age and sex); significance = p < .05; Cohen’s d effect size: negligible (<.2), moderate (~.5), and large (>.8). Note on statistical analysis: After correcting using Benjamini–Horchberg procedure, in the newly adherent and totally adherent groups, increasing daily pedometer steps, sodium reduction, and increasing fruit and vegetable servings effected significant changes (p < .05) in all four outcome variables. The nonadherent group experienced positive significant improvements (p < .05) only for SBP and weight related to pedometer steps.aNonadherent = includes patients at Precontemplation (no intention to change), Contemplation (thinking to change), and Preparation (preparing to change) stages of SOC; newly adherent = patients in Action stage (reporting change during 6 months of intervention); and totally adherent = patients in Maintenance stage for whom change already became a habit before study initiation.

10 Health Education & Behavior
& Tudor-Locke, 2004; Trinh, Wilson, Williams, Sum, & Naylor, 2012). Although an incremental trend was observed from nonadherent to totally adherent for pedometer steps, the lack of positive achievement in the nonadherent could per-haps be explained by precontemplators being likely to have more barriers to obtaining regular exercise than people in the action stage (Jaffee, Lutter, Rex, Hawkes, & Bucaccio, 1999). Also, Malaysians are largely sedentary, with 43.7% of adult Malaysians being physically inactive (Institute for Public Health, 2008). Motivating sedentary patients, unused to exercising, to take up regular exercise is a challenge, and for such patients, promoting walking as a regular form of exercise should be least burdensome (Manson et al., 2002; Stovitz, Van Wormer, Center, & Breme, 2005). In probing as to why stage-based activity promotion interventions did not work, Adams and White (2005) suggested the complexity of physical activity, lack of validated staging algorithms, and possibly real determinants not being included in TTM. Walking, as measured by pedometer steps, is not a complex form of exercise. We showed that newly adherent patients who increased their pedometer steps achieved pronounced reductions in WC and weight.
Limitations and Future Directions
Richardson, Simons-Morton, and Annegers (1993), quoting values expectancy theory, suggest that individuals ratio-nally choose noncompliance when the barriers or costs of treatment outweigh the expected benefits. Barriers to dietary and exercise plan adherence, namely, economic constraints, culture, and ethnicity, have been cited to pre-vent primary care patients with hypertension and/or diabe-tes from making effective health lifestyle changes (Orzech, Vivian, Torres, Armin, & Shaw, 2013). Economic con-straints were not an issue in our study as patients’ medica-tion and treatment costs were supported by project funding. But dietary advocacy could have been affected by budget constraints. Indeed, Karupaiah, Chee, Siew, Boon, and Chinna (2013), in a cross-sectional study on urban women living in Kuala Lumpur, found that diet quality was linked to household income, income positively correlated with fruits and food variety, and decreased vegetable intake and sodium excess were associated with poor diet quality. Successful application of the SOC model, therefore, requires addressing whether cost is an issue in achieving the right diet.
Carers’ access time to each patient was limited to 6 months based on funding availability. Obstacles to achiev-ing behaviors may require greater motivational solutions, especially with patients still hesitant about the positive adoption of multiple healthful behaviors. Dieticians are required to use empathetic, nonjudgmental, supportive, encouraging, and active listening behaviors in order to explore and resolve ambivalence and barriers to behavior
change (Spahn et al., 2010). Furthermore, as per study protocol, dieticians advocated both exercise and diet behav-iors, which added constraints to counseling time. Dieticians also expressed being “less confident” in handling exercise counseling. Predictors of weight loss and greater patient retention in a community-based weight management pro-gram were site hours of operation, nurse calls, and avail-ability of safe places to be active and feeling comfortable at the site (Abildso, Zizzi, & Fitzpatrick, 2013). These vari-ables were controlled at all CORFIS clinics as patient appointments fit into specific timed routines with the CORFIS health care team. The E-LITE (Evaluation of Lifestyle Interventions to Treat Elevated Cardiometabolic Risk in Primary Care) trial demonstrated the advantage of providing guided physical activity training (Blonstein et al., 2013). A pedometer-based strategy for diabetic patients in the Early ACTID (Activity in Diabetes) randomized con-trolled trial was found ineffective in BP lowering in con-trast to a community partnership between physicians and a physical activity stakeholder that successfully promoted pedometer use in sedentary patients (Andrews et al., 2011; Trinh et al., 2012). Bias may have resulted from false reporting of SOC in this study. However, patient-reported compliance to salt intake, pedometer steps, and fruit and vegetable servings produced clinically beneficial reduc-tions in SBP, DBP, weight loss, and WC, which were pro-nounced in newly adherent patients.
There is emerging evidence related to usage of TTM and social cognitive theory as a framework for nutrition counsel-ing (Spahn et al., 2010). Further research should therefore explore why movement between stages varies for the type of advocated behavior. As Povey et al. (1999) suggest, dynamic change would be dependent on the levels of motivation and self-efficacy, which are facilitated by the use of cognitive and behavioral processes. Experiences and degree of success in making the change by patients should be understood, and accounting for the cyclical nature of behavior change and accommodating for relapse should be addressed as part of an intervention. Given the short period of the study, these con-structs of patient behavior could not be included in the study design. Progression to capacity building in patients as advo-cated in the COM-B (capability, opportunity, and motivation behavioural) model and provided for in the United Kingdom’s National Institute of Clinical Excellence guidelines should follow for further enhancement of care in CDM (Atkins & Michie, 2013).
Implications for Research and Practice
This is the first time patient categorization for healthful behaviors according to the SOC model has been applied to hypertension management. Importantly, it demonstrated that patient adherence to behaviors could moderate clinical out-comes related to BP control.

Karupaiah et al. 11
The application of the SOC construct in the clinical con-text of CDM is important in community health for optimal patient care. The implication of this study is that SOC appli-cation could be metered to behavior change therapy that is linked to defined clinical endpoints and specific for multiple behaviors. Furthermore, sufficient exposure time for nutri-tion counseling to truly take effect may be necessary to over-come limitations. Therefore, research should address identifying barriers to adherence for realistically longer peri-ods of time.
Acknowledgment
We wish to acknowledge the Director General of Health Malaysia for encouraging this work and for granting permission to publish this article. We appreciate the Clinical Research Center, Ministry of Health Malaysia, for project management services inclusive of human resources, website design and maintenance, and database management. We wish to particularly thank our 30 service dieti-cians who provided the locum support for patient intervention and our CORFIS Dietician group members who helped develop the medical nutrition therapy protocol for hypertension. Above all, we wish to thank our patients and the health care team led by the general practitioner at each one of the participating CORFIS clinics who together contributed to the meaningful outcomes of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a research grant (MRG-CRC 2007-00) from the National Institute of Health, Ministry of Health Malaysia.
Supplemental Material
Additional supporting information is available at heb.sagepub.com/supplemental.
References
Abildso, C. G., Zizzi, S., & Fitzpatrick, S. J. (2013). Predictors of clinically significant weight loss and participant retention in an insurance-sponsored community-based weight management program. Health Promotion Practice, 14, 580-588.
Adams, J., & White, M. (2005). Why don’t stage-based activity promotion interventions work? Health Education Research, 20, 237-243.
Andrews, R. C., Cooper, A. R., Montgomery, A. A., Norcross, A. J., Peters, T. J., Sharp, D. J., . . . Dayan, C. M. (2011). Diet or diet plus physical activity versus usual care in patients with newly diagnosed type 2 diabetes: The early ACTID randomised con-trolled trial. The Lancet, 378, 129-139.
Appel, L. J., Brands, M. W., Daniels, S. R., Karanja, N., Elmer, P. J., & Sacks, F. M. (2006). Dietary approaches to prevent and treat hypertension: A scientific statement from the American Heart Association. Hypertension, 47, 296-308.
Atkins, L., & Michie, S. (2013). Changing eating behaviour: What can we learn from behavioural science? Nutrition Bulletin, 38, 30-35.
Blonstein, A. C., Yank, V., Stafford, R. S., Wilson, S. R., Rosas, L. G., & Ma, J. (2013). Translating an evidence-based lifestyle intervention program into primary care: Lessons learned. Health Promotion Practice, 14, 491-497.
Bodenheimer, T., Wagner, E. H., & Grumbach, K. (2002). Improving primary care for patients with chronic illness: The chronic care model: Part 2. Journal of American Medical Association, 16, 1909-1914.
Brug, J., Conner, M., Harre, N., Kremers, S., McKellar, S., & Whitelaw, S. (2005). The transtheoretical odel and stages of change: A critique. Observations by five Commentators on the paper by Adams, J. and White, M. (2004) Why don’t stage-based activity promotion interventions work? Health Education Research, 20, 244-258.
Burke, V., Beilin, L. J., Cutt, H. E., Mansour, J., Williams, A., & Mori, T. A. (2007). A lifestyle program for treated hyperten-sives improved health-related behaviors and cardiovascular risk factors, a randomized controlled trial. Journal of Clinical Epidemiology, 60, 133-141.
Chan, C. B., Ryan, D. A. J., & Tudor-Locke, C. (2004). Health benefits of a pedometer-based physical activity intervention in sedentary workers. Preventive Medicine, 39, 1215-1222.
Chan, S. C., Chandramani, T., Chen, T. Y., Chong, K. N., Harbaksh, S., Lee, T. W., . . . Teoh, L. C. (2005). Audit of hyperten-sion in general practice. Medical Journal of Malaysia, 60, 475-482.
Chua, S., Kok, L. C., Yusof, F. A. M., Tang, G. T., Lee, S. W. H., Efendie, B., & Thomas, P. (2012). Pharmaceutical care issues identified by pharmacists in patients with diabetes, hyperten-sion or hyperlipidaemia in primary care settings. BMC Health Services Research, 12, 388.
Cohen, J. (1988). Statistical power analyses for the behavioural sci-ences. Hillsdale, NJ: Lawrence Earlbaum.
Craig, C. L., Marshall, A. L., Sjöström, M., Bauman, A. E., Booth, M. L., Ainsworth, B. E., . . . Oja, P. (2003). International Physical Activity Questionnaire: 12-country reliability and validity. Medical Science & Sports Exercise, 35, 1381-1395.
Dickinson, H. O., Mason, J. M., Nicolson, D. J., Campbell, F., Beyer, F. R., Cook, J. V., . . . Ford, G. A. (2006). Lifestyle interven-tions to reduce raised blood pressure: A systematic review of randomized controlled trials. Journal of Hypertension, 24, 215-233.
Dijkstra, A., de Vries, H., & Bakker, M. (1996). Pros and cons of quitting, self-efficacy, and the stages of change in smoking cessation. Journal of Consulting & Clinical Psychology, 64, 758-763.
First DataBank/Hearst Corporation. (2005). Nutritionist Pro™ [Computer software]. Stafford, Texas: Author.
Glanz, K., Patterson, R. E., Kristal, A. R., Feng, Z., Linnan, L., & Hebert, J. (1998). Impact of worksite health promotion on stages of dietary change: The Working Well Trial. Health Education Behavior, 25, 448-463.

12 Health Education & Behavior
Glasziou, P., Meats, E., Heneghan, C., & Shepperd, S. (2008). What is missing from descriptions of treatment in trials and reviews? British Medical Journal, 336, 1472-1474.
Hall, J. N., Moore, S., Harper, S. B., & Lynch, J. W. (2009). Global variability in fruit and vegetable consumption. American Journal of Preventive Medicine, 36, 402-409.
Horwath, C. C. (1999). Applying the transtheoretical model to eat-ing behaviour change: Challenges and opportunities. Nutrition Research Reviews, 12, 281-317.
Institute for Public Health. (2008). The Third National Health and Morbidity Survey (NHMS III) 2006: General findings. Kuala Lumpur, Malaysia: Ministry of Health Malaysia.
Jaffee, L., Lutter, J. M., Rex, J., Hawkes, C., & Bucaccio, P. (1999). Incentives and barriers to physical activity for working women. American Journal of Health Promotion, 13, 215-218.
Jones, H., Edwards, L., Vallis, T. M., Ruggiero, L., Rossi, S. R., Rossi, J. S., . . . Zinman, B. (2003). Changes in diabetes self-care behaviors make a difference in glycemic control. Diabetes Care, 26, 732-737.
Karim, N. A., Safiah, M., Jamal, K., Zuhaida, S. H., Rohida, S., Norazlin, S., . . . Azmi, M. Y. (2008). Food consump-tion patterns: Findings from the Malaysian Adult Nutrition Survey (MANS). Malaysian Journal of Nutrition, 14, 25-39.
Karupaiah, T., Chee, W. S. S., Siew, Y. L., Boon, K. N., & Chinna, K. (2013). Dietary health behaviors of women living in high rise dwellings: A case study of an urban community in Malaysia. Journal of Community Health, 38, 163-171.
Kristal, A. R., Beresford, S. A., & Lazowich, D. (1999). Assessing change in diet-intervention research. American Journal of Clinical Nutrition, 59(Suppl.), 185S-189S.
Kristal, A. R., Glanz, K., Tilley, B. C., & Li, S. (2000). Mediating factors in dietary change: Understanding the impact of a work-site nutrition intervention. Health Education Behavior, 27, 112-125.
Low, W. H. H., Seet, W., Ramli, A. S., Ng, K. K., Jamaiyah, H., Dan, S. P., . . . Lim, T. O. (2013). Community-based cardiovas-cular Risk Factors Intervention Strategies (CORFIS) in man-aging hypertension: A pragmatic non-randomised controlled trial. Medical Journal of Malaysia, 68, 129-135.
Manson, J. E., Greenland, P., La Croix, A. Z., Stefanick, M. L., Mouton, C. P., Oberman, A., . . . Siscovick, D. S. (2002). Walking compared with vigorous exercise for the prevention of cardiovascular events in women. New England Journal of Medicine, 347, 716-725.
Ministry of Health Malaysia. (2006). National Health Morbidity Survey III. Kuala Lumpur, Malaysia: Author.
Ministry of Health Malaysia. (2008). Clinical practice guideline management of hypertension (3rd ed). Putrajaya, Malaysia: Author.
Ministry of Health Malaysia. (2009). Clinical practice guideline management of type 2 diabetes mellitus (4th ed.). Putrajaya, Malaysia: Author.
Ministry of Health, Singapore. (2000). The composition of foods commonly eaten in Singapore. Singapore: Author.
Orzech, K. M., Vivian, J., Torres, C. H., Armin, J., & Shaw, S. J. (2013). Diet and exercise adherence and practices among medi-cally underserved patients with chronic disease variation across four ethnic groups. Health Education Behavior, 40, 56-66.
Povey, R., Conner, M., Sparks, P., James, R., & Shepherd, R. (1999). A critical examination of the application of the Transtheoretical Model’s stages of change to dietary behav-iours. Health Education Research, 14, 641-651.
Prochaska, J. J., & Prochaska, J. O. (2011). Review of multiple health behavior change interventions for primary preven-tion. American Journal of Lifestyle Medicine, 5, 208-221. doi:10.1177/1559827610391883
Prochaska, J. O., & DiClemente, C. C. (1983). Stages and processes of self-change of smoking: Toward an integrative model of change. Journal of Consulting & Clinical Psychology, 51, 390-395.
Prochaska, J. O., & Velicer, W. F. (1997). The transtheoretical model of health behavior change. American Journal of Health Promotion, 12, 38-48.
Prochaska, J. O., Velicer, W. F., Rossi, J. S., Goldstein, M. G., Marcus, B. H., Rakowski, W., . . . Rossi, S. R. (1994). Stages of change and decisional balance for 12 problem behaviors. Health Psychology, 13, 39-46.
Ramli, A. S., & Taher, S. W. (2008). Managing chronic diseases in the Malaysian primary health care: A need for change. Malaysian Family Physician, 3, 7-13.
Richardson, M. A., Simons-Morton, B., & Annegers, J. F. (1993). Effect of perceived barriers on compliance with antihyperten-sive medication. Health Education Behavior, 20, 489-503.
Sacks, F. M., Svetkey, L. P., Vollmer, W. M., Appel, L. J., Bray, G. A., Harsha, D., . . . Cutler, J. A. (2001). Effects on blood pressure of reduced dietary sodium and the dietary approaches to stop hypertension (DASH) diet. New England Journal of Medicine, 344, 3-10.
Spahn, J. M., Reeves, R. S., Keim, K. S., Laquatra, I., Kellogg, M., Jortberg, B., & Clark, N. A. (2010). State of the evidence regarding behavior change theories and strategies in nutrition counseling to facilitate health and food behaviour change. Journal of American Dietetic Association, 110, 879-891.
Stovitz, S. D., Van Wormer, J. J., Center, B. A., & Breme, K. L. (2005). Pedometers as a means to increase ambulatory activ-ity for patients seen at a family medicine clinic. Journal of American Board of Family Practice, 18, 335-343.
Svetkey, L. P., Simons-Morton, D. G., Proschan, M. A., Sacks, F. M., Conlin, P. R., Harsha, D., . . . DASH-Sodium Collaborative Research Group. (2004). Effect of the dietary approaches to stop hypertension diet and reduced sodium intake on blood pressure control. Journal of Clinical Hypertension, 6, 373-381.
Tee, E. S., Ismail, M. N., Azudin, M., & Khatijah, I. (1997). Nutrient composition of Malaysian foods. Kuala Lumpur, Malaysia: Institute for Medical Research.
Trinh, L., Wilson, R., Williams, H. M., Sum, A. J., & Naylor, P-J. (2012). Physicians promoting physical activity using pedom-eters and community partnerships: A real world trial. British Journal of Sports Medicine, 46, 284-290.
Tudor-Locke, C., Bassett, J. D. R., Rutherford, W. J., Ainsworth, B. E., Chan, C. B., Croteau, K., . . . Wojcik, J. R. (2008). BMI-referenced cut points for pedometer determined steps per day in adults. Journal of Physical Activity & Health, 5(Suppl.), S126-S139.
Tudor-Locke, C., Hatano, Y., Pangrazi, R. P., & Kang, M. (2008). Revisiting “how many steps are enough?” Medicine & Science in Sports & Exercise, 40(7 Suppl.), S537-S543.

Karupaiah et al. 13
Weingarten, S. R., Henning, J. M., Badamgarav, E., Knight, K., Hasselblad, V., Gano, A. Jr., & Ofman, L. L. (2002). Interventions used in disease management programmes for patients with chronic illness—which one works? Meta-analysis of published reports. British Medical Journal, 325, 925.
Weinstein, N. D., Rothman, A. J., & Sutton, S. R. (1998). Stage theories of health behavior: Conceptual and methodological issues. Health Psychology, 17, 290-299.
Weinstein, N. D., Sandman, P. M., & Blalock, S. J. (2008). The precaution adoption process model. In K. Glanz, B. K. Rimer,
& K. Viswanath (Eds.), Health behavior and health education (4th ed., pp. 123-147). San Francisco, CA: Jossey-Bass.
Whelton, S. P., Chin, A., Xin, X., & He, J. (2002). Effect of aerobic exercise on blood pressure: A meta-analysis of ran-domized, controlled trials. Annals of Internal Medicine, 136, 493-503.
World Health Organization. (2000). Obesity: Preventing and man-aging the global epidemic. Report of a WHO Consultation (WHO Technical Report Series 894). Geneva, Switzerland: Author.