Embed Size (px)
Citation preview

10/2013 1

Objectives Identify early signs and symptoms of Acute Coronary
Syndrome
Initiate proper protocol for ACS patient
10/2013 2

Purpose of this Education Module:
September 2012 3
Chest Pain Center Accreditation involves the management of chest pain anywhere in the hospital. Intensive Care and Step down Units along with Emergency Department staff care for many patients who have or are at a high risk for heart disease.
Knowledge of ACS pathophysiology and early recognition is key to impacting patient outcomes.
Early recognition reduces the time it takes for patients experiencing symptoms of possible ACS to see a physician thus decreasing the time to treatment which is critical in the early stages when treatment is most effective.

Background Coronary Artery Disease (CAD) = #1 killer of men and
women in U.S. Affects about 12 million Americans
In the US, CAD claims more lives each year than the next 7 leading causes of death combined!
Myocardial Infarction (MI) or “Heart attack” 1.1 million people affected each year
About half present at ED triage not using EMS
460,000 deaths annually from MI
Half of these deaths occur before reaching hospital
Estimated average number of years of life lost due to a heart attack is 14.2
Average delay in presentation about 3 hours from onset on symptoms!
10/2013 4

10/2013 5
Acute Coronary Syndrome refers to a state of symptomatic ischemia or infarction resulting from a completely or partially clot-obstructed coronary artery.
ST elevated MI
(Complete occlusion)
Non ST elevation MI
(Partial occlusion)

Cardiac Risk Factors
Non-Modifiable Risk Factors Previous history Family history
1st degree relative (parents, siblings)
Men < 55; Women < 65 Age Gender Socioeconomic Factors
and Ethnicity
9 easily measured and potentially modifiable risk factors account for over 90% of the risk of an initial acute MI
Smoking Hypertension Dyslipidemia Diabetes Obesity Metabolic Syndrome Inactivity Alcohol
10/2013 6

Assessment of Pain
Linking Patient History and Risk factors
Cardiac Biomarkers
ECG Findings
10/2013 7

Assessment of “cardiac pain”
N = Normal (What is the patient’s baseline?)
O = Onset (sudden/gradual?)
P = Precipitation / provoking / palliative factors
Q = Quality or quantity (have patient describe in own words)
R = Radiation and region
S = Severity (pain scale)
T = Time (continuous/intermittent?)
10/9/2013 8

ACS Symptoms Classic
Symptoms
Stable angina
Unstable angina
MI
Symptom Variations
Women Elderly Diabetics
10/9/2013 9

Angina
Stable Occurs with physical
exertion or emotional stress
Relieved by rest or sublingual nitroglycerin
Predictable pattern
Predictable = triggered by the same amount of physical or emotional stress and should be easily relieved by rest or sublingual nitroglycerin.
Unstable Occurs with minimal
exertion OR increased dose of
nitroglycerin is required to achieve relief.
Prolonged rest angina is also considered unstable angina.
Angina that increases in severity or is very severe on first presentation
Caused by unstable or ruptured plaque that causes abrupt closure of a coronary artery which may spontaneously reperfuse.
10/2013 10

Characteristics of Angina Sensation of pressure, tightness, heaviness, burning, or squeezing.
• Rarely described as a sharp or stabbing pain.
• Should not worsen with changes in position or respiration.
Location behind the sternum and in the upper back, shoulder, arm, jaw, or epigastric area.
• Not usually located in the middle to lower abdomen and usually does not radiate to the lower extremities.
Associated symptoms (or stand alone symptoms) of dyspnea, nausea, palpitations, or diaphoresis.
Duration typically defined in minutes.
• Not typically defined in seconds or hours.
10/2013 11
CAUTION WHEN ASKING THE PATIENT ABOUT “PAIN”!
May deny pain but may state pressure, fullness or heaviness.

Symptoms in Special Populations ACS in Women Delay presenting with symptoms Attribute symptoms to other
non-cardiac causes Presentation
epigastric discomfort less specific complaints:
dyspnea or fatigue symptoms of discomfort
from nose to navel should be evaluated for presence of heart disease
Older women have higher incidence of complications
ACS in the Elderly Generalized symptoms
Dyspnea, diaphoresis, N&V, and syncope
Confusion Symptoms often attributed to the aging
process such as “activity intolerance” ACS in the Diabetic Patient
Autonomic dysfunction can affect symptoms experienced with angina
Less likely to experience pain.
25% of all patients presenting with ACS are diabetic
Have severe multi-vessel disease
Have higher rates of complications
Have a greater proportion of ulcerated plaques resulting in intracoronary thrombi
10/2013 12

Cardiac Biomarkers
Released into the blood when necrosis occurs as a result of membrane rupture of the myocytes
Used in the evaluation of ACS Myoglobin
Rises the earliest Within 2 hours after damage Very sensitive, not specific
CK (creatine kinase) Enzyme present in the heart, brain, and skeletal muscle Elevations are not specific to myocardial damage.
CK-MB More specific to the heart Helpful in identifying more than minor amounts of myocardial damage Rapidly rises in the presence of myocardial damage.
10/2013 13
Cardiac Biomarkers
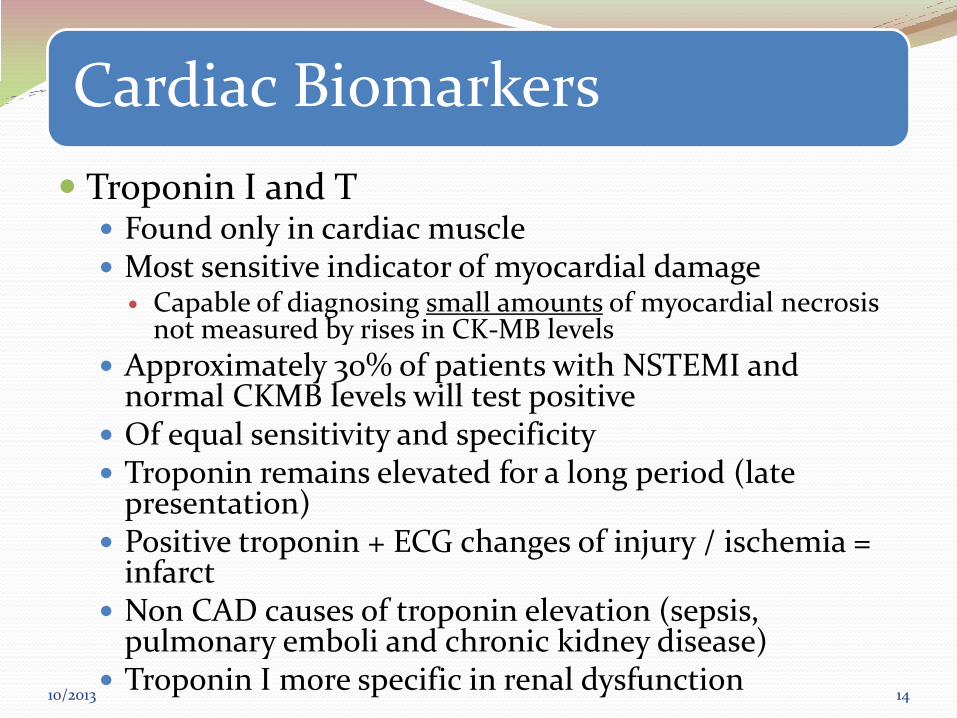
Troponin I and T Found only in cardiac muscle Most sensitive indicator of myocardial damage
Capable of diagnosing small amounts of myocardial necrosis not measured by rises in CK-MB levels
Approximately 30% of patients with NSTEMI and normal CKMB levels will test positive
Of equal sensitivity and specificity Troponin remains elevated for a long period (late
presentation) Positive troponin + ECG changes of injury / ischemia =
infarct Non CAD causes of troponin elevation (sepsis,
pulmonary emboli and chronic kidney disease) Troponin I more specific in renal dysfunction
10/2013 14

10/2013 15
Cardiac Biomarker Summary
Cardiac
Biomarker
Specificity /
Sensitivity
Rise Peak Duration
Myoglobin Sensitive but
not specific
Within 2 hours 4 to 10 hours < 24 hours
CK-MB
(more specific to
the heart than CK
levels)
Highly specific 4 to 6 hours 18 to 24 hours 2 to 3 days
Troponin I or T Highly specific
and sensitive
4 to 6 hours 18 to 24 hours 10 or more days

ECG Findings A discussion of injury/ischemia ECG findings is
beyond the scope of this module.
Key tips
Mark chart copy as “pain free” or “with pain” on top of ECG
ECG Critical Values at Aultman include the following and require physician notification
• Acute MI
• Bradycardia <45 beats
• Ventricular Tachycardia
10/2013 16

STAT ECG Indications
Chest pain or severe epigastric pain, non traumatic in origin, with components typical of myocardial ischemia or MI: Central/substernal compression or crushing chest pain
Pressure, tightness, heaviness, cramping, burning, aching sensation
Unexplained indigestion, belching, epigastric pain
Radiating pain in neck, jaw, shoulders, back, or 1 or both arms
Associated dyspnea
Associated nausea/vomiting
Associated diaphoresis
10/2013 17
If non diagnostic:
Repeat every 15 to 30 minutes
Use ST segment monitoring
Consider right-sided/posterior ECG

SCREEN for ACS if … > 30 years old with any of the following: Chest discomfort of any kind
“Heartburn”, indigestion, or epigastric pain
Complaints of “heart racing” (HR >150 or irregular and >120)
Complaints of “heart too slow” (HR < 50 and symptomatic)
Syncopal episode or severe weakness in patients > 45 years old
Difficulty breathing (no obvious non cardiac cause)
</= 30 with any of the above PLUS: Prior Cardiac disease
Family history of early heart disease
Diabetes mellitus
Severe Obesity
Recent cocaine use
Remember: Women and diabetic patients are more likely to present with atypical symptoms
Elderly patients may have symptoms such as generalized weakness, altered mental status, shortness of breath, or syncope, as their only sign of acute heart attack.
10/2013 18
When in doubt, do the ECG!

< 25% of ACS patients Complete occlusion of a vessel by a thrombus
Fibrin stable clot (red clot)
Classified more specifically by the portion of the left ventricle suffering injury.
Mortality is greatest within the first 24 to 48 hours of symptom onset
TREATMENT FOCUS = REPERFUSION
10/2013 19

Acute MI Symptoms
Symptoms occur spontaneously and are not relieved by rest or nitroglycerin
Chest pressure or discomfort may be accompanied by nausea, vomiting, or diaphoresis
Patient may have hemodynamic instability or cardiac arrest from ventricular fibrillation
Acute MI patients have positive biomarkers and are classified as STEMI or NSTEMI based on ECG presentation
10/2013 20

STEMI Management
Reperfusion is number one treatment strategy
Primary Coronary Intervention (PCI) preferred treatment strategy if within 90 minutes
Goal: 90 minutes from 1st medical contact
Fibrinolytics within 30 minutes of hospital
presentation (or 30 minutes from EMS to fibrinolytics)
10/2013 21
Facilitated PCI with full dose fibrinolytics is not recommended.
Rescue PCI may be done after failed fibrinolytics

10/2013 22
Reperfusion Therapy
Primary PCI Fibrinolytic Therapy
Primary PCI has clear outcome advantage in those > 65 years: Mortality Stroke Intracranial Hemorrhage
Reperfusion has proven benefit up to age 85.
The Winner!

Medical Management of STEMI
ASA Clopidogrel (with or without reperfusion)
Oxygen NTG MS D/C NSAIDS Beta-blockers (within 24 hours)
ACE Inhibitors (within 24 hours with impaired EF, HTN, diabetes or chronic kidney disease)
Anticoagulants (related to reperfusion strategy)
Intravenous insulin may be indicated in first 24 to 48 hours after STEMI to tightly control blood sugars.
10/2013 23
Reperfusion is primary management strategy.
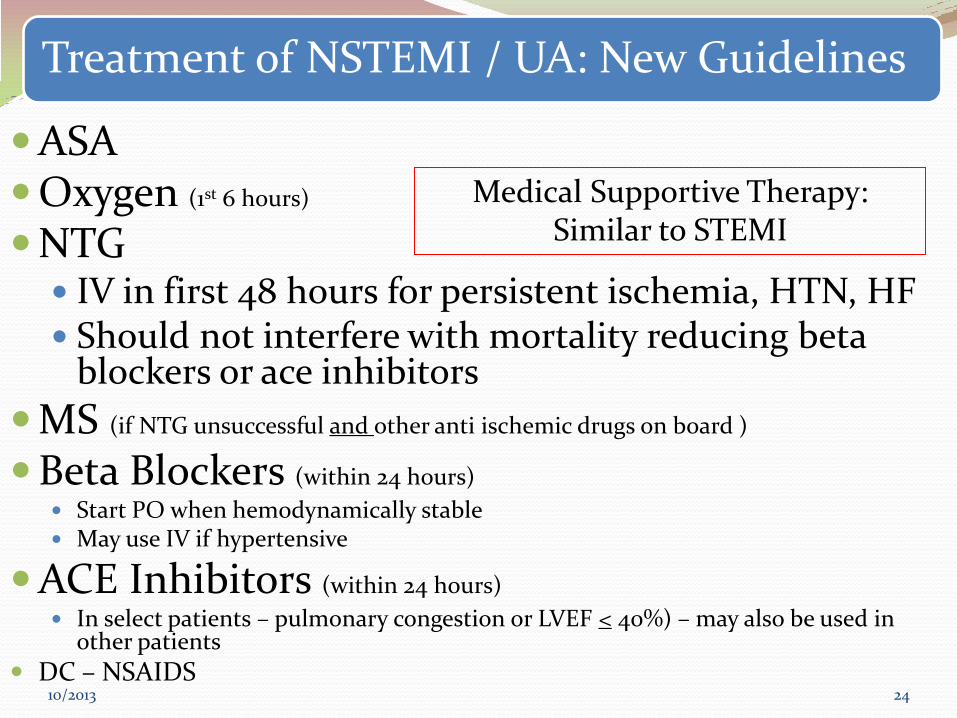
Treatment of NSTEMI / UA: New Guidelines
ASA Oxygen (1st 6 hours) NTG
IV in first 48 hours for persistent ischemia, HTN, HF Should not interfere with mortality reducing beta
blockers or ace inhibitors
MS (if NTG unsuccessful and other anti ischemic drugs on board )
Beta Blockers (within 24 hours)
Start PO when hemodynamically stable May use IV if hypertensive
ACE Inhibitors (within 24 hours)
In select patients – pulmonary congestion or LVEF < 40%) – may also be used in other patients
DC – NSAIDS
10/2013 24
Medical Supportive Therapy: Similar to STEMI

Complications of MI
Hemodynamic Alterations Ventricular Arrhythmias Atrial Arrhythmias Pericarditis Ventricular Aneurysms Mechanical Complications
Myocardial Rupture (free wall or VSD) Papillary Muscle Rupture
Long Term: Ventricular Remodeling
10/2013 25

New addition to all admission power plans
In order to improve our patient care for an In house STEMI patient a communication order will be added to each admission power plan. This order is pre-checked and states
“Stat ECG will be obtained in the setting of a Rapid Response for suspected heart attack signs or symptoms”
This will allow the rapid response team to immediately obtain an ECG allowing quicker diagnosis and “STEMI alert” will be called if ECG is diagnostic for STEMI.
10/2013 26

Information that needs charted with In House STEMI patient
Onset of symptoms EKG time Notification of physician Time STEMI called Departed from floor ( to either Heart Cath lab or CCU) It is important to accurately chart the times the above occurs. Use
IP phone or computer for atomic time. Atomic time is a synchronized time and is very important when
tracking quality data. This patient may be in three different locations during this quality data collection and each area using this atomic time will allow accurate data collection.
This data will be tracked and used as quality data to improve our care for the In house STEMI patient.
10/2013 27

Summary
10/2013 28
Remember, time is muscle!
Save hearts and lives by knowing the signs/symptoms of ACS
Activate the rapid response team and notify the physician
Obtain an EKG