Embed Size (px)
Citation preview

100k Genomes Project
What clinicians need to know

Genomics: What is it
Video link
http://hee.nhs.uk/work-programmes/genomics/



100K Genome Project Diagnosis, personalised treatment and research
Cancer soon to affect 1 in 2 of UK population
Rare Diseases 1 in 17 of the UK population (>3 million)
Infectious diseases

Indications for genetic / genomic testing
Diagnosis (avoidance of unnecessary investigations and shorten
diagnostic odyssey)
Management (most appropriate follow up and treatment)
Genetic follow up (identification of gene carriers and
exclusion of population risk follow up)
Ensure you get the maximum clinical utility from you test
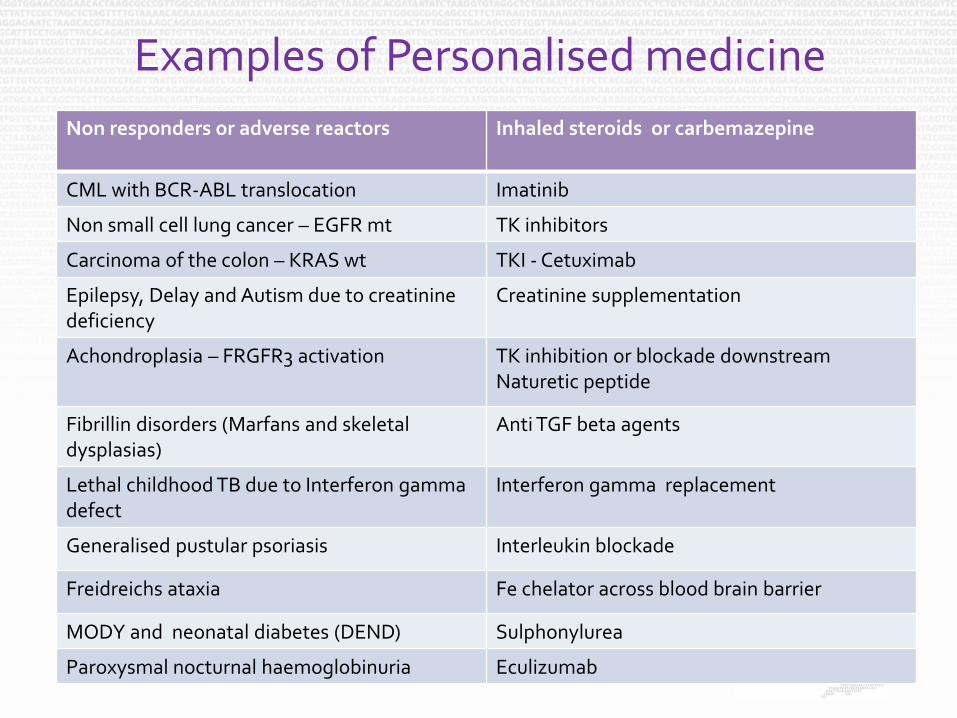
Examples of Personalised medicine
Non responders or adverse reactors Inhaled steroids or carbemazepine
CML with BCR-ABL translocation Imatinib
Non small cell lung cancer – EGFR mt TK inhibitors
Carcinoma of the colon – KRAS wt TKI - Cetuximab
Epilepsy, Delay and Autism due to creatinine deficiency
Creatinine supplementation
Achondroplasia – FRGFR3 activation TK inhibition or blockade downstream Naturetic peptide
Fibrillin disorders (Marfans and skeletal dysplasias)
Anti TGF beta agents
Lethal childhood TB due to Interferon gamma defect
Interferon gamma replacement
Generalised pustular psoriasis Interleukin blockade
Freidreichs ataxia Fe chelator across blood brain barrier
MODY and neonatal diabetes (DEND) Sulphonylurea
Paroxysmal nocturnal haemoglobinuria Eculizumab
https://www.gov.uk/government/publications/chief-medical-officer-annual-report-2016-generation-genome

Genomics: What is it
• Sequence of entire human genome
– 1st Genome 13years and £2billion
– Now £1K and 48 hours
– Approximately 20,000 genes
– Intronic/ non-coding DNA
– 3 billion letters
– Detects genetic alterations causing disease in 25-40% more cases

Moore’s law vs Cost of DNA sequencing
Moore’s law: “over the history of computing hardware, the number of transistors on integrated circuits doubles ~2years”

Methodology underlying Genomic Analysis
Technology Process Advantages Disadvantages
Sanger Sequential gene analysis
Simple Few VOUS No incidental findings “Cheap” “Quick”
Multiple genes :- Slow Expensive Only analyse candidates
NGS - Panel Selected “panel of candidates”
Relatively simple Some VOUS No incidental findings Getting cheaper Getting quicker
Only analyse candidates
NGS - exomes “All” coding sequences Detects unexpected causes Getting cheaper and quicker
Needs lots of bio-informatic support Lots of VOUS Cost > panel
NGS - genomes All genetic code Highest detection rate Greatest research value
Most expensive Most Complex Most VOUS

C R C 55C a U terus C a U terus 41 + C LL
Mut -ve U terus 41 C R C 44 C R C TC C 43 C R C 47x2 C R C 43 K A x2 C R C 50 C R C 45 + 54 U terus 45 TC C x2 U terus 46 C R C 46 Mut -ve
Mut -ve Mut -ve
?
Mut -ve
Joint MTC at QEH
19 apparently sporadic MTC presenting to QEH over 2 years
A mutation was identified in 3/19 (15.8%) V804M heterozygous 43y male V804M homozygous 54y female C618S heterozygous 30y female
Subsequent cascade testing in at risk family members
• → 18 predictive genetic tests → 13 positive → 11 prophylactic thyroidectomies (5/11 MTC and 5/11 CCH)

Confirmed SDHB c423 + 1G..A
Malignant paraganglioma
Initial analysis sequential SDHB,D,VHL and Ret oncogene Analysis now NGS panel SDHB,D,VHL and Ret oncogene, plus SDHA,C, SDHAF2, MAX, TMEM127

Birmingham Joint Endocrine Genetic Clinic 2007-2009
• 26 Patients seen with Phaeochromocytoma or paragnglioma
• 15/26 – no mutation
• 9/26 mutation positive – “diagnosis and change management”
• 21 Predictive tests (10/21+ve) – cascade testing
• 10 Relatives mutation +ve - in surveillance
• 11 Relatives mutation –ve - reassured

Some other genetic causes of bone fragility (LDD list 140 disorders)
• Ehlers Danlos Syndrome (EDS)
• Osteoporosis
• Osteopetrosis
• Hypophospatasia
• Pyknodysostosis
• Pyles Disease
• Many many others – but most very rare

Definitions
Molecular studies MZ Twins Therefore could be compatible with de-novo IFITM5 mutation c.-14C>T – new splice site and insertion of Met-Ala-Leu-Glu-Pro at the 5’ end of the gene. Separate AR Develop Delay and microcephaly - 8% genome homozygous -

Heterogeneity
or
One disease more than one gene

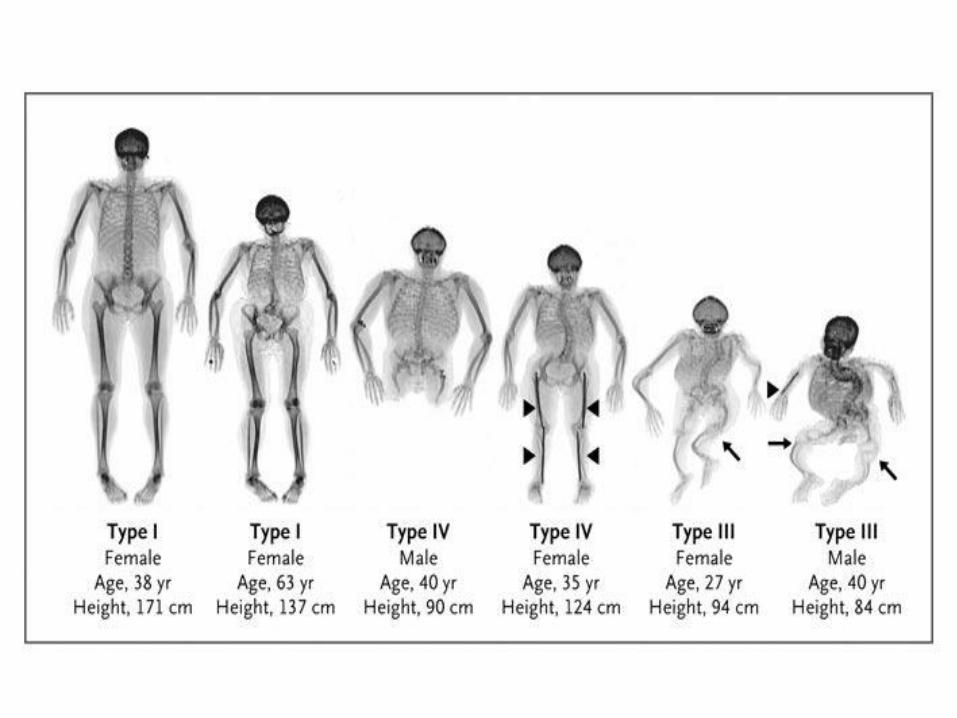
OI phenotypes and genotypes
OI Type Inheritance Phenotype Gene Defect
Classical –Silence Type
I II III IV
AD AD AD AD
Mild Lethal Progressive Moderate
Nul Col1A1 Col7A1/Col1A2 Col1A1/Col 1A2 Col1A1/Col1A2
Other V VI
AD ?AR
Distinctive histology/callus Mineralisation defect
IFITM5 SERPINF1
3 hydroxylation defects
VII VIII IX
AR AR AR
Hypomorphic (S) null (L) Severe to lethal Moderate – severe
CRTAP LEPRE1 PP1B
Chaperone Defects
X XI
AR AR
Severe to lethal BRUCK progressive
SERPINH1 FKBP10
Unclassified types
Bruck Type II AR Contractures PLOD2
Caffey Disease AD Cortical hyperostosis
Col1A1
Osteoblast maturation defect
AD Moderate SP7

Who can be recruited?
• 13.5K samples over 3 years
Cancer
Breast
Colon
Lung
Ovarian
Prostate
Sarcoma
Rare diseases (undiagnosed/unconfirmed)
Cardiovascular disorders
Dermatological disorders
Dysmorphic /Congenital abnormalities
Endocrine disorders
Growth disorders
Haematological disorders
Hearing/ear disorders
Metabolic disorders
Neurology/neurodevelopmental disorders
Opthalmological disorders
Renal and urinary tract disorders
Skeletal /rheumatological /connective tissue disorders
Cancer predisposition syndromes


Geleophysic – Acromicric Dysplasia
• Geleophysic – AR due to mutations in ADAMTLS2 gene
• Geleophysic/Acromicric – AD due to mutations in the fibrillin gene
• Prognosis differs across spectrum
• Fibrillin mutation disorders show evidence of response to anti TGF therapy
• Recurrence risk 1 in 2, 1 in 4 or very low

Pleiotropy or
Spectrum of the disorder?
One Gene – more than one phenotype


DTDST Mutations
PARTIAL FUNCTION NULL
MED Achondrogenesis type 1B
Classic
DD
Atelosteogenesis type 2
homozygous heterozygous homozygous
p.V340del p.R178X
p.R279W
p.R279W +
IVS1+2T>C or p.V340del
p.R279W +
p.R178X or p.C418X

Chondrodysplasias – Type 2 Collagen

Who can be recruited?
• Eligibility – Rare disease
• Clinical diagnosis or suspected rare genetic condition
• Routine genetic tests normal
• No molecular diagnosis
• Trio available where possible
– Cancer • Any patient with breast, lung, ovarian, prostate, colon,
sarcoma cancer
• Current diagnosis
Who Can be Recruited ?– part 2
• Not appropriate for Sanger sequencing –not just 1 known gene
• Sanger sequencing / NGS panel testing negative.
• Very heterogenous and difficult to discriminate clinically
• No known genetic cause but likely genetic
• Newly recognised genetic disorder

Why recruiting “Trios”?

Miller Syndrome – Acrofacial dysostosis - caused by DHODH gene
Nature Genetics Jan 2010 Vol 42; 30-33
Filter Fam 1 A
Fam 1
A
Fam 1
B
Fam 1
B
Fam 1
A + B
Fam 1
A + B
Fam 1 + 2
Fam 1 + 2
FAM 1 + 2 +3
Fam 1 + 2 +3
AD AR AD AR AD AR AD AR AD AR
NS/SS or InDel
4,670 2,863 4,687 2,859 3,940 2,362 3,099 1,810 2,654 1,525
Not in dbSNP 129
641 102 647 114 369 53 105 25 63 21
Not in HapMap 8
898 123 923 128 506 46 117 7 38 4
Not in either
456 31 464 33 228 9 26 1 8 1
Predicted damaging
204 6 204 12 83 1 5 0 2 0
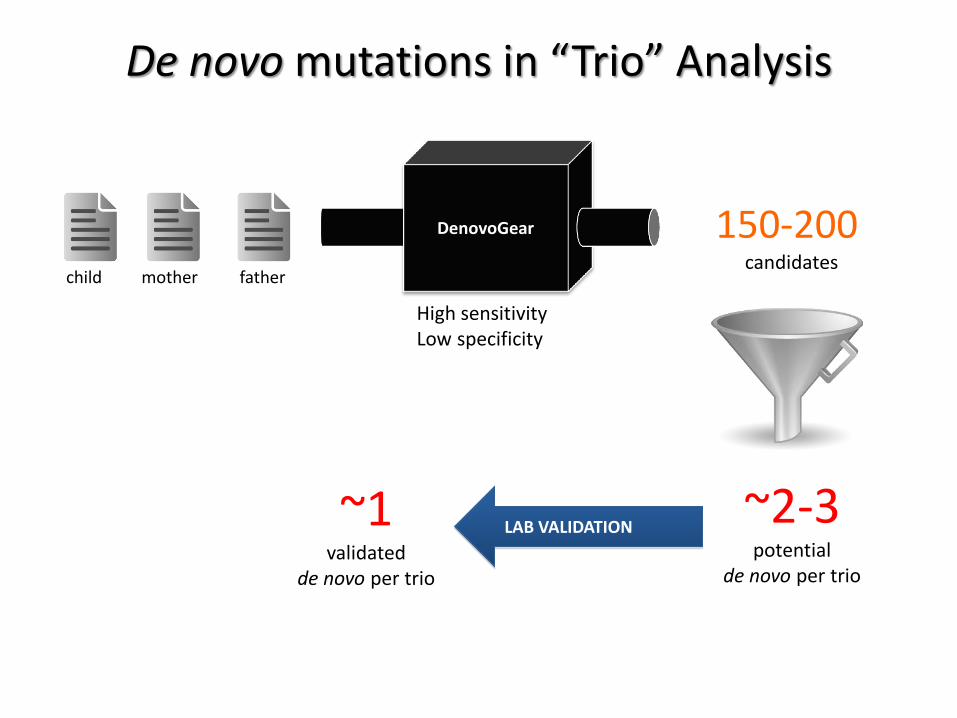
De novo mutations in “Trio” Analysis
child mother father
DenovoGear 150-200 candidates
~2-3 potential
de novo per trio
~1 validated
de novo per trio
LAB VALIDATION
High sensitivity Low specificity
Something Special About the West Midlands
• Very young population
• Very fast population growth in the <25 year olds
• High levels of consanguinity in some communities

What sort of results may there be?
• May identify
– Mutations associated with known clinical diagnosis
– Mutations of likely significance
– Mutations associated with other diagnoses
– Cancers with molecular changes suggesting particular chemotherapies

Additional looked for findings
• Cancer predisposition – BRCA1, BRCA2, (Breast, ovarian and prostate cancer) – Lynch syndrome: MLH1, MSH2, MSH6, PMS2, (Colorectal,
endometrial and ovarian cancer) – Polyposis: MYH, FAP, (Bowel polyps and colorectal cancer)
– Increase risk of cancer in adulthood
• With FAP, polyps often begin in teenage years
– Usually inherited from a parent – Identifying family members at risk can be helpful
• Screening (aids early diagnosis and improves survival) • Reducing risk (medication, risk reducing surgery, lifestyle choices)

The 100k Genome Project: Aims
• Rare disease: – To increase discovery of pathogenic variants for rare disease. – To add value with additional biological insights that build confidence in putative pathogenic
variants. – To enhance the clinical interpretation of whole genome sequencing in rare disease – To develop a programme of functional multi-omics pathways, specifically transcriptomics,
epigenetics, micro RNAs and biomarkers. – To return these findings to the NHS for feedback to patients. – To create a unique dataset for rare disease that may enable therapeutic innovation.
• Cancer
– To use whole genome sequencing to identify novel driver mutations for cancer and to understand the evolutionary genetic architecture of cancer through primary and secondary malignant disease (by multiple biopsy and whole genome sequencing).
– To partner stratified healthcare programmes and outcome studies with patients from the NHS in England to enable understanding of the benefit of whole genome sequencing in defining predictors of therapeutic response to cancer therapies.
– To use multi-omic approaches including transcriptomics, proteomics and epigenetics to offer additional biological insights into cancer.
– To utilise the whole genome sequencing to identify new pathways for cancer therapies.

WM GMC Vision Statement
In the next 3 years: We will implement a genomics programme, - investigating 7,000 patients, - treated at 18 hospitals across the region.
This will have a transformational effect on clinical services: - embedding genomics medicine and stratified treatment
in both cancers and rare diseases. - creating a regional platform for world leading research.
https://www.gov.uk/government/publications/chief-medical-officer-annual-report-2016-generation-genome

HEE, GEL, NHSE and PHE supported Masters Programme in Genomic Medicine
MRC EPSRC Molecular Pathology Nodes West Midlands
WMGMC Region - wide
Transformation

Finance •Business model development •Ratification of business case •Monitoring & draw down of funding:
Chris Newton
Bio-Informatics
•Bio-informatics:
Jean-Baptiste Cazier
Education and
Training •MSc: Peter Searle •Patient Recruitment & Counselling:
Laura Boyes/ Louise Banks & Trevor Cole •HEWM Rep - tba
Laboratory Services and Sample Logistics •Sample Pathways, Storage & Delivery: Jane Steele •Rare Disease & Blood Cancer Samples: Mike Griffiths •Solid Tumour (& germline blood) Samples: Phillipe Taniere • Operations: Jacqui Roper / Paula Hitch
Delivery Workstreams & Leads
Research Transformatio
n •MRC: Path Node •Scientific Discovery: Jean-Baptitse Cazier Research Portfolio:
Gideon Hirschfield
Service Innovation Adoption •WM CLAHRC - Richard Lilford •Svc Improvement: Lorraine Simmonds
Development Workstreams & Leads
Wealth Creation • WMAHSN: Tony
Davis
NHS England
Integration, Interoperability , Business Process Automation & Software Development
• Information Support Platforms: Stephen Chilton • Data Quality: Daniel Ray
• EST Sample Tracking: Daniel Ray • Clinical IT Syst Dev: Simon Ball
Project Management Team • Debbie Porter (PM)
WM GMC Management Group (MG) Co - Chairs: Dion Morton &
Trevor Cole
WM GMC Consortium Executive Group (CEG)
Chair: Tim Jones (UHB) Senior Responsible Officer
University Hospitals Birmingham Foundation Trust Board of Directors
Cancer • Adult : Mark Cook • Paed iatrics : Prof Pam
Kearns • Genetics: Kai-Ren Ong
Rare Diseases •Genetics : Trevor Cole
•Paed iatrics : Tim Barrett • Adult : Graham Lipkin •HEFT Rep : tba • SWBH Rep: tba
CEG Members UoB Dean of Medicine - David Adams BCH Chief Exec – Sarah-Jane Marsh BWH Chief Exec – Ros Keeton WM AHSN Director – Chris Parker (GMC PG Chair) WM GMC Director - Dion Morton
WM GMC Partners Group
(PG) Chair: Chris Parker
(WMAHSN)
PG Members Toby Lewis - SWBT TBC - HEFT Andy Hardy - UHCW David Loughton - RWT Mark Hackett – UHNM Jo Chambers - ROH
PPI • AHSN / BHP
Fiona Alexander
GMC MG Members WM GMC Director – Dion Morton Theme Chairs – (see below) PM - Debbie Porter Div Director Div A – Ian Sharp BHP Comms – Fiona Alexander Head of R&D Ops – Jo Plumb Regional Genetics Svc – Mike Griffiths

What is involved?

Patient clinics:
Rare Diseases
Patient clinics:
Haemato-oncology
Patient clinics: Solid
Cancers
Sample and Validation Pathways in Birmingham GMC sample hub - OUT
Results
WMRGL & MPDS (& LDPs) NHS laboratory with retained DNA receives results via HBRC .
NHS laboratory with retained DNA is responsible for validation, via: Own existing tests
Existing tests elsewhere in Bham GMC Existing tests elsewhere in GMC network, UKGTN network, or elsewhere.
Bespoke assays.
HBRC Single report receipt point within GMC Distributes results to NHS laboratories
Links results to patient records .
WMRGL West
Midlands Regional Genetics
Laboratory
MPDS Molecular Pathology Diagnostic
Service
HBRC Human
Biomaterials Resource
Centre
GEL Biorepository
GEL Sequencing
Samples & DNA
all bloods
results
DNA DNA
DNA
all bloods, marrow
results results
results
results
results
supp bloods
tumour, all bloods supp bloods
DNA
Sample Hub
V1.1

Patient clinics
Expert Triumvirate
Site Specific
MDT
Clinician/ Notes
‘Normal’ Results
Report/ Liaison
Membership consists of • (Pathologist) • Consultant from The Expert
Advisory Group • Clinical Geneticist
WMRGL MPDS
Validation of GEL Results
Sample Hub
Results
Feedback and Validation Pathways for Results V1.2

Rare Diseases A rare disease with residual unmet diagnostic need identified by a proband
within the NHS in England – Clinical diagnosis or suspected rare genetic condition – Routine genetic tests normal – No molecular diagnosis – Trio available where possible
Up to 9000 samples over 3 years – Cardiovascular disorders – Dermatological disorders – Dysmorphic /Congenital abnormalities – Endocrine disorders – Growth disorders – Haematological disorders – Hearing/ear disorders – Metabolic disorders – Neurology/neurodevelopmental disorders – Opthalmological disorders – Renal and urinary tract disorders – Skeletal /rheumatological /connective tissue disorders – Cancer predisposition syndromes

Eligibility- rare disease Inclusion criteria Exclusion Criteria
A rare disease with residual unmet diagnostic need
Prior identification of a known causative gene variant an affected family member.
Particular conditions that have undergone a defined gene panel test or other tests to exclude known genetic mutations.
The absence of valid consent.
Access to appropriate family structures (ideally parent-offspring trio,) with suspected Mendelian dominant, recessive or X-Linked conditions
Probands not under the care of the NHS in England.
Families with suspected Mendelian conditions with one or more affected individuals in a single generation (likely to be due de novo mutations)
Inadequate phenotyping or failure to provide data and samples to the Genomics England central biorepository within 14 days.
Individuals with extreme forms of common disorders (e.g. particularly early onset or unusually severe forms) will also be considered
DNA of insufficient quality for whole genome sequencing (we may request further samples).
Multiple unrelated families with evidence of linkage to the same chromosomal region/s
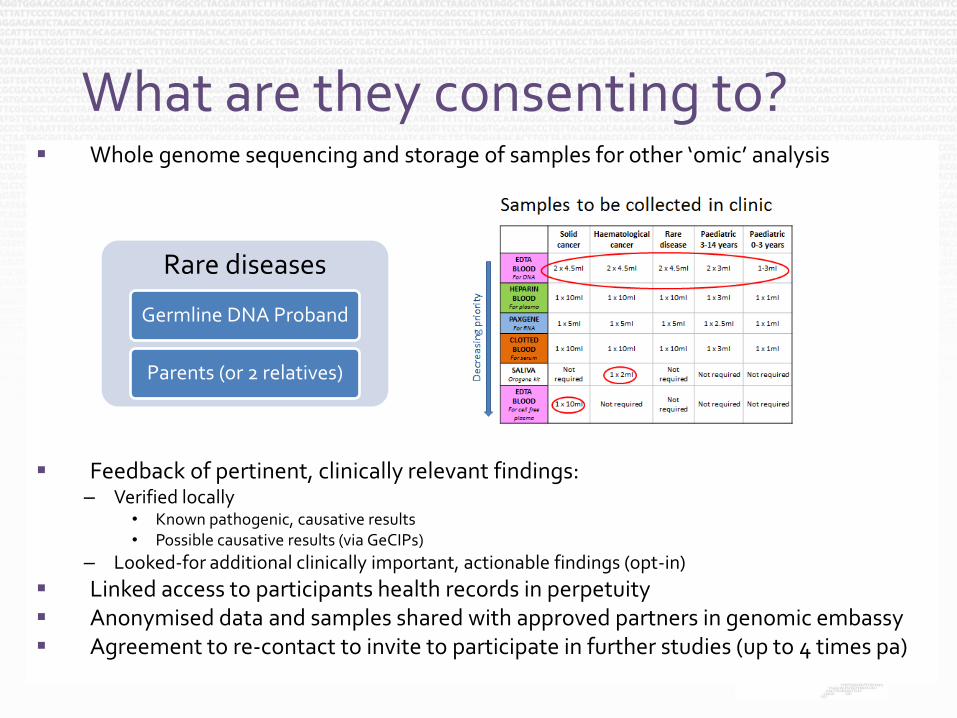
What are they consenting to? Whole genome sequencing and storage of samples for other ‘omic’ analysis
Feedback of pertinent, clinically relevant findings: – Verified locally
• Known pathogenic, causative results • Possible causative results (via GeCIPs)
– Looked-for additional clinically important, actionable findings (opt-in)
Linked access to participants health records in perpetuity Anonymised data and samples shared with approved partners in genomic embassy Agreement to re-contact to invite to participate in further studies (up to 4 times pa)
Rare diseases
Germline DNA Proband
Parents (or 2 relatives)

Additional looked-for findings
Additional looked for findings – Adult Onset
• BRCA1, BRCA2, • MLH1, MSH2, MSH6, PMS2, • MYH, APC, • Familial Hypercholesterolaemia
– Childhood Onset • MEN1, MEN2, RB, VHL, FMTC
– Carrier Testing • Sickle Cell Anaemia, Alpha Thalassemia, Bet Thalassemia • CF, CAH, SMA • DMD, Adrenoleukodystrophy, Haemophilia A


HEE, GEL, NHSE and PHE supported Masters Programme in Genomic Medicine
MRC EPSRC Molecular Pathology Nodes West Midlands
WMGMC Region - wide
Transformation
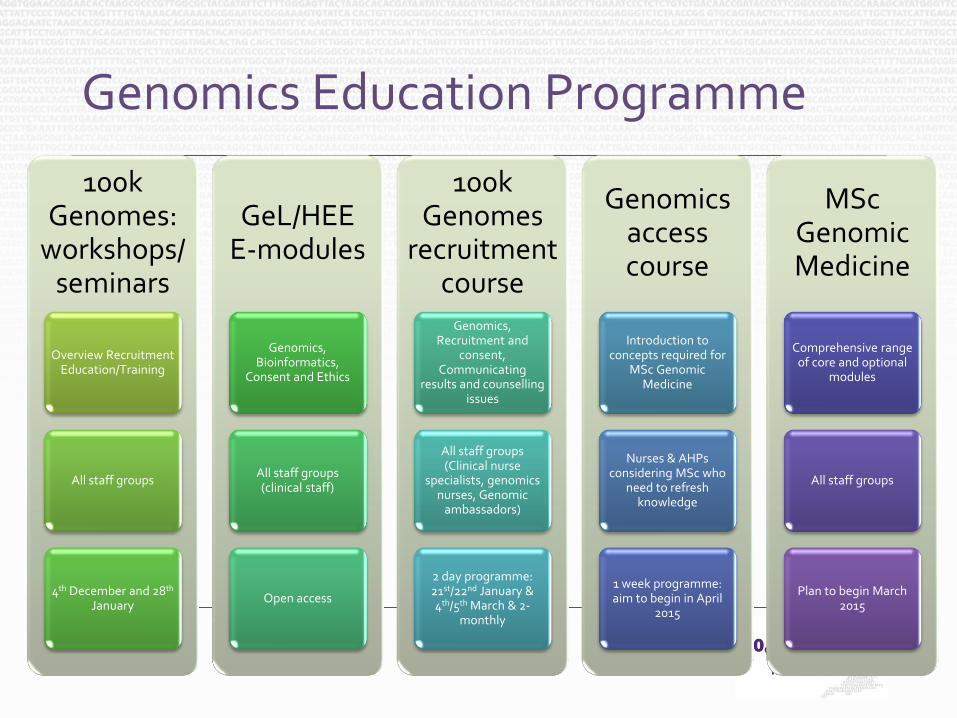
Genomics Education Programme
100k Genomes:
workshops/ seminars
Overview Recruitment Education/Training
All staff groups
4th December and 28th January
GeL/HEE E-modules
Genomics, Bioinformatics,
Consent and Ethics
All staff groups (clinical staff)
Open access
100k Genomes
recruitment course
Genomics, Recruitment and
consent, Communicating
results and counselling issues
All staff groups (Clinical nurse
specialists, genomics nurses, Genomic
ambassadors)
2 day programme: 21st/22nd January & 4th/5th March & 2-
monthly
Genomics access course
Introduction to concepts required for
MSc Genomic Medicine
Nurses & AHPs considering MSc who
need to refresh knowledge
1 week programme: aim to begin in April
2015
MSc Genomic Medicine
Comprehensive range of core and optional
modules
All staff groups
Plan to begin March 2015
http://www.birmingham.ac.uk/postgraduate/courses/taught/med/genomic-medicine.aspx
MSc in Genomic Medicine
Health Education England (HEE) will support 550 NHS staff to study this MSc between 2015 & summer 2018 – www.birmingham.ac.uk/genomicmedicine
Can be taken Full-time (1 year) or Part-time (2 years) – Modules also available for PGDip, PGCert or CPPD
Start— from 19th March 2015!
Apply through the University; HEE will pay tuition fees – UoB accepting EOIs
• Email [email protected]

MSc Genomic Medicine
Programme Stucture & Delivery Model
Blended learning. – At UoB, most modules involve 5 days of campus-based teaching; combined
with distance-learning – ~45 days on campus.
Core modules covering: – 1) Introduction; 2) Omics Technologies; 3) Inherited Diseases; 4) Cancer; 5)
Pharmacogenomics & Stratified Healthcare; 6) Infectious Diseases; 7) Bioinformatics
Projects: — At University, place of work or online (bioinformatics)
Optional modules: – i) Ethical, Legal & Social Issues; ii) Counselling Skills; iii) Economic Models;
iv) Workplace-Based Learning; v) Professional & Research Skills; vi) Advanced Bioinformatics
For more information:
– www.genomicseducation.hee.nhs.uk – www.birmingham.ac.uk/genomicmedicine

Questions and discussion https://www.genomicsengland.co.uk/information-for-gmc-staff/

Contacts Staffordshire and Shropshire
Christopher Clowes
Genomics Ambassador – West Midlands North (including UHNM, SaTH, RJAH and BurtonFT)
Tel: 01782 671939
Email: [email protected] & [email protected]
Address: Research and Development Department, Courtyard Annexe – C Block, Royal Stoke University Hospital, University Hospitals of North Midlands NHS Trust, Newcastle Road, Stoke-on-Trent, Staffordshire, ST4 6QG.
Black Country and Worcestershire
Charlotte Hitchcock
Genomics Ambassador – West Midlands Black Country and Worcestershire
Tel 01902 447146
E mail [email protected]