Embed Size (px)
Citation preview
10 Topics in General Anesthesia
You NEED to KNOW
Pankaj Chhatbar, MD
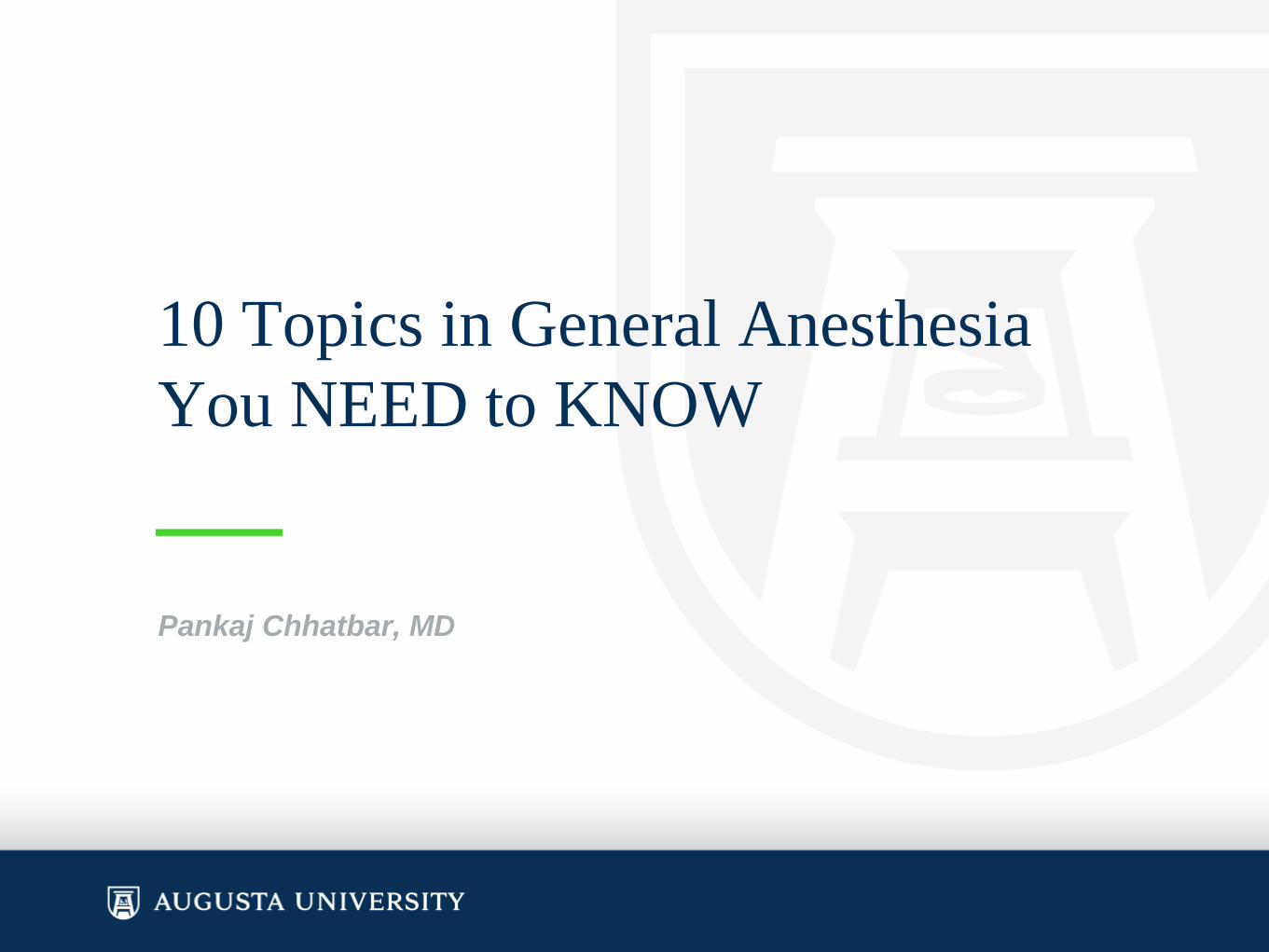
Stages of Anesthesia

Stages of Anesthesia
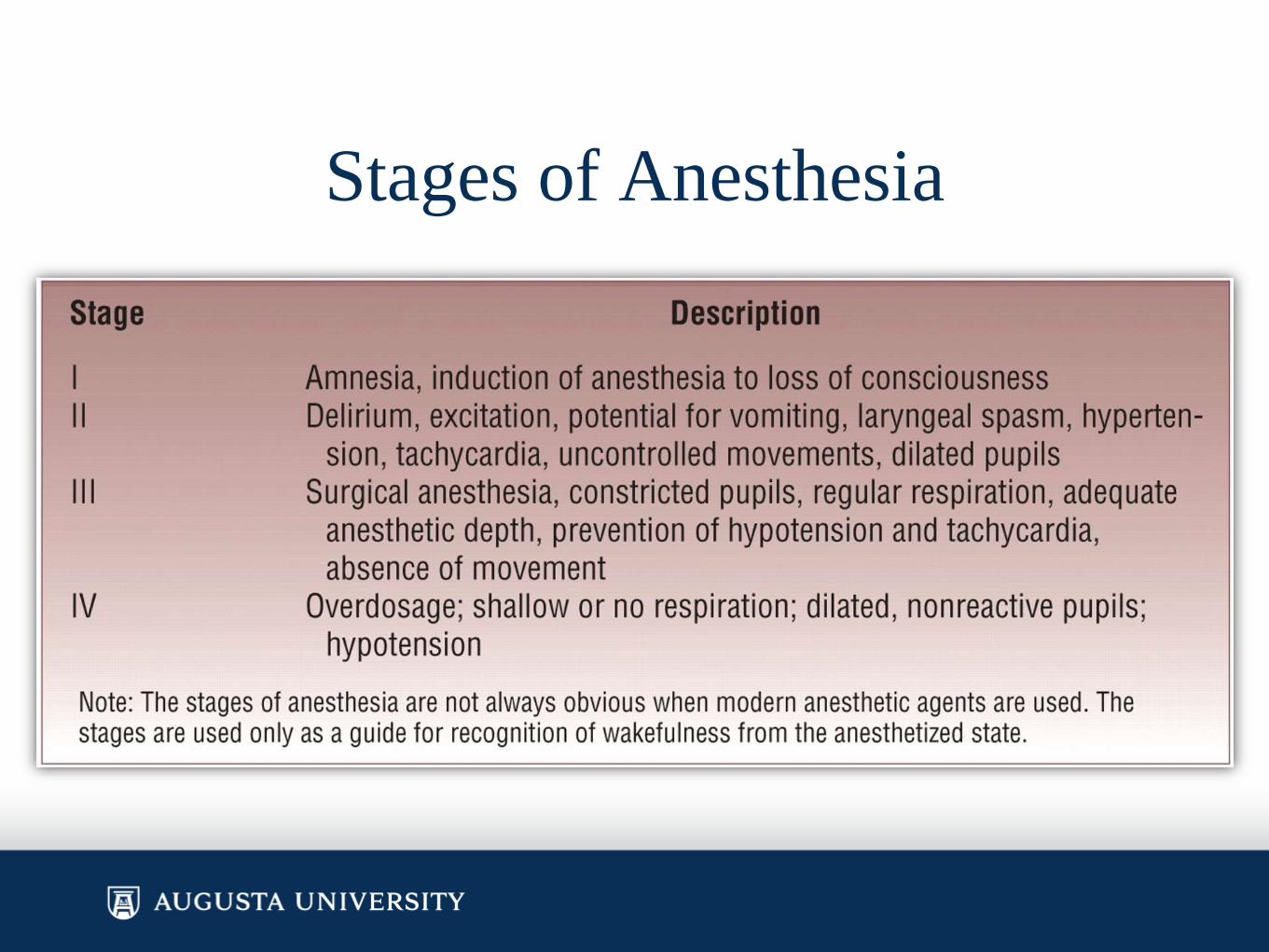
Difficult airway characteristicsAirway Examination Component
1. Length of upper incisors
2. Relation of maxillary and
mandibular incisors during
normal jaw closure
3. Relation of maxillary and
mandibular incisors during
voluntary protrusion of
4. Interincisor distance
5. Visibility of uvula
Taken from Table 1: Components of the Preoperative Airway Physical Examination from ASA practice guidelines on difficult airways
6. Shape of palate
7. Compliance of mandibular space
8. Thyromental distance
9. Length of neck
10.Thickness of neck
11.Range of motion of head and neck

Difficult airway characteristics Non reassuring Findings
1. Upper Incisors Relative long
2. Prominent “overbite” (maxillary incisors anterior to mandibular incisors)
3. Patient mandibular incisors anterior to (in mandible front of) maxillary incisors
4. Less than 3 cm
5. Not visible when tongue is protruded with patient in sitting position (e.g., Mallampati class greater than II)
6. Highly arched or very narrow
7. Stiff, indurated, occupied by mass, or nonresilient
8. Less than three ordinary finger breadths
9. Short
10.Thick
11.Patient cannot touch tip of chin to chest or cannot extend neck

Post op visual loss
• Associated with the following…
– Surgery > 6 hours
– EBL > 1000 ml
– Prone position
• MC = ION, Ischemic Optic Neuropathy = ischemic insult to
optic nerve
• Another type = CRAO, Central Retinal Artery Oclusion =
from direct pressure on the eye
• 10% Reverse Tburg position reverses the increased IOP
caused by prone position itself

One lung ventilation, DLTs
Laser ETT
• One of the most feared complications of laser surgery of
the larynx is fire in the airway
• “Regular" endotracheal tubes can present some issues
when performing microlaryngeal surgery with a laser
– The PVC material on regular ETTs can be damaged with laser
use, causing local damage of the mucosa at best, and a
spectacular "blow-torch" like ignition effect if the laser punctures
through the lumen of the ETT and comes into contact with
oxygen-rich fresh gas
– Lasers can also puncture an inflated cuff

An indispensable tool in the arsenal of any anesthesiologist is
the laser resistant endotracheal tube.
• ASA practice advisory for the prevention of OR fires that
recommends the use of laser resistant ETTs appropriate for
the type of laser chosen for surgery
• ASA practice advisory also recommends that the tracheal cuff
should be filled with saline rather than air and that the saline
used to fill the cuff should be dyed with methylene blue. This
allows immediate detection of laser damage to the cuff
• To prevent airway fires with laser surgery
– Use armored (laser resistant) ETT
– Minimize O2 and N2O use (both flammable)
– Bypass the area being lasered with jet ventilator

Meds you CAN give via A-line
• Heparin
• NMDBs and suxx
• Narcotics
• Isotonic Fluids
• Atropine
• Isotonic fluid administration is safe and drug administration should be limited as much as possible.
• Among the anesthetic drugs that have been injected intraarterially without adverse effects are fentanyl, midazolam, succinylcholine, pancuronium, and atropine
• Intraarterial injection of drugs not dissolved in water (such as diazepam, propofol, and etomidate) or with an alkaline pH (like thiopental, phenytoin) should be avoided at all cost.
Anesthesia & Analgesia: September 2006 - Volume 103 - Issue 3 - pp 792-794
Peripheral Neuropathies• Infiltration of an AC IV can cause median nerve damage
• Brachial plexus can be stretched if arm is Abducted > 90 degrees or shoulder is
externally rotated or if head is flexed and rotated towards opposite side
• Ulnar neuropathy is MC
– Avoid by supinating arm, padding elbow
• Radial nerve damage occurs from pressure at the grove of the humerus in
elbow
– Tourniquets and BP cuffs are MC culprits, pad this area
• Common peroneal nerve is prone to injury in lithotomy, esp if > 2 hours
– Avoid direct pressure on the head of the fibula and pad this area of the knee
– Excessive stretch of the sciatic nerve in lithotomy can also cause
neuropathy
• Femoral nerve injury can occur with extreme aBduction and external rotation of
legs in lithotomy
– Can also occur from surgical retractors in abdomen, aortic cross clamp

Anaphylaxis, Most Common Causes
• Anaphylaxis in the operating room can be caused by IgE-mediated reactions, non-IgE-mediated immunologic reactions as well as nonimmunologic reactions.
• The most common causes are neuromuscular blocking agents (#1 in Europe) and antibiotics (#1 in US), followed by latex and other induction medications.
• Cardiovascular collapse is the first detected manifestation in up to 50 percent of cases
– Tachycardia is a classic cardiovascular sign of anaphylaxis, although bradycardia occasionally develops later in the reaction if the patient becomes hypoxemic or develops heart block
– Bronchospasm may present as a sudden increase in the ventilatorypressure required to inflate the lungs, an increase in end-tidal carbon dioxide, or a decrease in arterial oxygen saturation.
– Rapidly developing laryngeal edema may present as difficulty with intubation or stridor postoperatively.
Anaphylaxis• Anaphylaxis during anesthesia may be particularly difficult to recognize for
several reasons:
– Early or mild symptoms, such as itching or shortness of breath, may go
unnoticed because the patient cannot communicate.
– Cutaneous signs, such as flushing, urticaria, and angioedema, may be
missed because the patient is draped for surgery.
• Early recognition, followed by the administration of epinephrine, benedryl,
H2 blocker, steroids, fluids, oxygen and airway control, is the key to a
successful outcome. Follow-up testing, through in-vitro and in-vivo
methods, is helpful in determining which agent caused the reaction.
• Blood collected at the time of the reaction or shortly after may reveal
elevations in tryptase or histamine, which are mediators released by mast
cells and basophils.
From UptoDate & articles online

Post obstructive Pulmonary Edema• Noncardiogenic cause of pulmonary edema with an incidence of 0.05-0.1%.
• Risk factors include male gender, head and neck surgeries, OSA, acromegaly, difficult intubation, and young age (probably associated to the ability to generate a significant pressure change).
• POPE is categorized as type I (inhalation against an obstruction) or type II (exhalation against an obstruction).
• Type I has a multifactorial etiology, which include negative pressure pulmonary edema, hypoxia, and hyperadrenergic states.
• During inhalation against an obstruction pressures up to -140 cmH2O (normal -4 cmH2O) are generated. This leads to an increase in right ventricular preload and afterload. These increases generate higher pulmonary venous pressures, which in turn increases capillary hydrostatic pressures. This, along with the negative intrapleural pressures being transmitted to alveoli, drives flow into the interstitium causing edema. Hypoxia adds to this effect by increase pulmonary vascular resistance due to hypoxic pulmonary vascular constriction again increasing hydrostatic pressure while also disrupting capillary wall integrity. Hyperadrenergic states are thought to redistribute blood to pulmonary system, again increasing pulmonary vascular resistance and driving up hydrostatic pressure.
Post obstructive Pulmonary Edema
• Type II is thought to be similar to a valsalva maneuver during exhalation against an obstruction. During exhalation, positive intrapleural and alveolar pressures are generated. This leads to a decrease in venous return, decrease in RV preload and subsequent decrease in pulmonary blood flow. Upon relief of obstruction the mechanism is similar to type I. There is a significant decrease in airway pressure, increase in venous return, increase preload and pulmonary blood volume.
• This leads to increase in hydrostatic pressure leading to edema.
Monitoring: ASA Standards
• Standard I: qualified anesthesia personnel
• Standard II ("VOTC"): oxygenation, ventilation,
circulation, temperature
– Ventilation: ETCO2, inspired anesthetic gases
– Oxygenation: SpO2 and inspired O2 (with an alarm)
– Temperature
– Circulation: HR, BP q5m, EKG
10 Topics in
Pharmacology You
NEED to KNOW

Inhalation agents• Inhaled anesthetics have presynaptic and postsynaptic effects
in the brain and spinal cord at specific neuronal membrane proteins that permit the translocation of ions during membrane excitation.
• Factors affecting no changes in MAC:
– Duration of anesthesia
– Gender
– Hyperthyroidism
– Hyperkalemia or hypokalemia
– paCO2 15-95
– BP above 40mmHg
• Uptake from the lungs is the product of three factors: blood solubility, cardiac output and the partial pressure driving anesthetic from one phase (e.g., lung) into a second phase (e.g., venous blood)

Inhalation agents
• Concentration effect: the greater the inspired
concentration, the more rapid is the rise in the FA/FI ration.
• All inhaled anesthetics depress the ventilator responses to
hypercarbia and hypoxia by altering central and peripheral
chemoreceptor function in a dose-dependent fashion.
• Inhaled anesthetics (with the exception of xenon) reduce
tidal volume and minute ventilation and cause tachypnea in
a dose-related fashion.
• Xenon is essentially devoid of cardiovascular effects
Intravenous Nonopioid Anesthetics
• Propofol provides rapid onset and offset with context-sensitive decrement times of approximately 10 minutes when infused for less than 3 hours and under 40 minutes when infused for up to 8 hours. Its mechanism of action is thought to be potentiation of GABA-induced chloride currents.
• Ketamine primarily acts by NMDA antagonism but also acts at opioid, nicotinic, muscarinic receptors and with voltage-sensitive calcium channels. Physostigmine may reverse some actions of ketamine.
• Ketamine is metabolized almost exclusively in the liver by cytochrome P-450 to norketamine, which is one fifth to one third as potent as ketamine.

Intravenous Opioid Anesthetics
• Mu1: Supraspinal analgesia, bradycardia, sedation, pruritus
• Mu2: Respiratory depression, euphoria, physical dependence, pruritus
• K: Spinal analgesia, respiratory depression, sedation, miosis
• Sigma: hypertension, tachycardia, dysphoria, delirium, mydriasis
• Delta: spinal analgesia, respiratory depression
Intravenous Opioid Anesthetics
• All opioids cause bradycardia without significant myocardial depression at clinically relevant doses except meperidine which may cause tachycardia because of its structural similarities to atropine.
• N2O, alfentanil and older patients are more often associated with muscle rigidity.
• Context sensitive half-time is the time necessary to achieve a 50% decrease in drug concentration after termination of a variable-length continuous infusion at a steady-state drug level.
• Fentanyl >alfentanil>sufentanil>remifentanil
• Meperidine exerts its antishivering effects via Kappa receptors.

Muscle Relaxants and their
Antagonists• Atracurium and cisatracurium undergo chemical breakdown in
the plasma (Hofmann elimination) as well as ester hydrolysis.
• Vecuronium and rocuronium undergo primarily hepatic metabolism and biliary excretion with limited renal excretion (10-25%).
• Only the long-duration NM blockers d-TC, pancuronium, doxacurium and pipecuronium are primarily excreted in the urine (>70%).
• Neostigmine, pyridostigmine and edrophonium are quarternaryammonium compounds and do not pass BBB
• Physostigmine is a tertiary amine and does cross the BBB –useful in the treatment for central anticholinergic syndrome.

Muscle Relaxants and their
Antagonists
• Echothiophate (used for refractory open angle glaucoma) is an organophosphate that irreversibly inhibits acetylcholinesterase–an enzyme that breaks down ACh, sux and mivacurium.
• Drugs potentiating neuromuscular blockers are volatile anesthetics, aminoglycosides, magnesium, IV local anesthetics, furosemide, dantrolene, calcium channel blockers and lithium.
• Edrophonium -Atropine
• NeostigmingGlycopyrrolate
• Phase I block after succinylcholine can be enhanced by anticholinesterase drugs.
• Onset of NDMR is inversely related to potency.
Local Anesthetics• Tachyphylaxis is a well-known phenomenon associated with
repetitive or continuous administration of local anesthetics.
• Prilocaine is metabolized by the liver to o-toludine, which is responsible for the oxidation of hemoglobin to methemoglobin. Rx methylene blue
• Ester local anesthetics are hydrolyzed by plasma cholinesterase.
• Potency of local anesthetics is directly related to its lipid solubility. Speed of onset is related to the pKa. The degree of protein binding is important for toxicity and metabolism.
• Neurolytic blockade with phenol (6% to 10% in glycerine) is painless beause phenol has a dual action as both a local anesthetic and a neurolytic agent. Alcohol (100% ethanol) is painful on injection and should be preceded by local anesthetic injection.

Cardiac Pharmacology• Milrinone is a selective phosphodieseterase III inhibitor and produces
both positive inotropic and vasodilatory effects (lusiotropic) by
increasing cAMP levels by decreasing cAMP breakdown.
• Glucagon increases myocardial contractility and HR primarily by
increasing cAMP formation.
• Norepinephrine has alpha and beta agonist activity but alpha effects
are significantly stronger than beta.
• Epinephrine actions are complex and mimic the stress response.
– most significant effect on metabolism.
• Insoproteronol is a nonselective beta agonist
• Dobutamine works selectively on beta1 receptors.
• Dopamine: at low doses, it increases contractility, HR and SVR, at
moderate doses it acts like epinephrine and high doses takes on the
characteristics of norepineprine.

Anti-neoplastic Pharmacology
• Vincristine: neuropathy
• Doxorubicin: cardiomyopathy
• Bleomycin: Pulmonary fibrosis
Neuromonitoring and Anesthesia
• Inhalation agents prolongs latency and reduce
amplitude in dose dependent manner except N2O
which only reduces amplitude.
• Etomidate and ketamine can increase amplitude

Pharmacokinetics
• When a drug is eliminated by first-order elimination, its
concentration is generally reduced by 97% after five half-
times of elimination.
• Hepatic extraction ratio is the fraction of the drug removed
from the blood passing through the liver. The extraction
ratios for lidocaine, meperidine, propofol and metoprolol
are very high; the ER for rocuronium is much lower.
• Pharmacogenetics is gradually explaining some of the
variability in response to drugs, e.g., hepatic cytochromes
CYP2D6 for codeine.

Thank you