Embed Size (px)
Citation preview

10OVARIAN CANCER
SANDRA ORSULIC
Molecular Pathology Unit, Massachusetts General Hospital Cancer Center, Charlestown, Massachusetts
Mice have been used in ovarian cancer research mainlyas hosts for cell lines derived from human ovarian tumorsand ascites. Such models provided valuable informationinto the nature of metastatic ovarian cancer and possibletreatment strategies. However, the complexity of geneticaberrations in human ovarian cancer cell lines precludedunderstanding of the initiating events responsible forovarian cancer induction. Since the majority of ovariancancer patients present at an advanced stage of thedisease, it has been difficult to identify the precursorlesions that could be used to study the early morphologicand genetic changes in ovarian cancer. It is thoughtthat the development of animal models in which ovariancancer can be induced and studied during its earlystages will enable better understanding of early ovariancancer lesions and elucidate molecular events that supportovarian cancer progression. The difficulties in generatingsuch models include the lack of an adequate ovary-specific promoter, the uncertainty about the tissue oforigin for different histologic types of ovarian cancer, andthe deficiency in understanding the genetic aberrationsresponsible for ovarian cancer induction. In spite of thesedifficulties, the first advances toward generating mousemodels for ovarian cancer have been made.
INTRODUCTION
Ovarian cancer is the fifth leading cause of cancerdeath among women in the United States and has thehighest mortality rate of all gynecologic cancers (Jemalet al., 2002). The etiology of ovarian cancer is not wellunderstood. The progress in basic ovarian cancer research
has been slow, mainly because of the lack of appropriateanimal models. Attempts to develop animal modelsthat recapitulate the development and pathophysiologicmanifestations of human ovarian cancer have primarilyresulted in the development of rare germ cell and sexcord–stromal tumors, but not epithelial tumors, whichare the prevalent ovarian cancer type in women. Thischapter provides an overview of the different types ofovarian cancer in women and the recent efforts to modelthe disease in mice in order to understand the molecularevents that are responsible for ovarian cancer initiation.
OVARY DEVELOPMENT
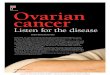
The ovaries are paired reproductive organs located oneither side of the uterus and adjacent to the lateral wallof the pelvis. The main functions of the ovary are theproduction of oocytes and the steroid hormones, estro-gen and progesterone. The ovaries consist of severaldifferent cell types that can be generally grouped intosomatic and germ cells. While the lineage of germ cells iswell established, less is known about the origin of var-ious somatic cell types in the ovary (McLaren, 2000).Precursors of primordial germ cells form in the epi-blast at the beginning of gastrulation and migrate fromthe epiblast to the extraembryonic mesoderm (Ginsburget al., 1990). They then migrate back into the embryothrough the hindgut mesentery toward the gonadal ridges(Fig. 10.1a). The gonadal ridges form by proliferation ofthe coelomic epithelium and condensation of the under-lying mesenchyme of the urogenital ridge (Fig. 10.1a).Induced by the underlying mesenchyme, the basement
Mouse Models of Human Cancer, edited by Eric C. HollandISBN 0-471-44460-X Copyright 2004 John Wiley & Sons, Inc.
171

172 OVARIAN CANCER
(a)
(b)
Figure 10.1. Lineages of somatic and germ cells in the ovary. (a) The primordial germ cellsmigrate through the gut mesentery and populate the gonadal ridges that form on the medialsurfaces of the urogenital ridges. The gonadal ridge mesenchyme is surrounded by proliferatingcoelomic epithelia. (b) As the embryo develops, derivates from the coelomic epithelia invade thegonadal ridges. These are believed to give rise to several different types of somatic cells in thedeveloped ovary, including the monolayered epithelial cells that cover the surface of the ovary.
membrane of the coelomic epithelium breaks down (Karland Capel, 1998) and epithelial derivatives enter the ridge(Fig. 10.1b). Thus the gonadal ridges are populated bygerm cells, the mesenchyme of the urogenital ridge, andthe coelomic epithelium. Various tissues in the adult ovary(Fig. 10.2) are believed to arise from these three precursorcell types.
NEOPLASMS OF THE OVARY
Ovarian cancer is a broad term used for a wide range ofneoplasms that originate in the ovary. Based on the puta-tive cell of origin, ovarian neoplasms are classified intothree broad groups: germ cell, sex cord–stromal cell, andsurface epithelial–stromal tumors. Each group containsseveral histologic ovarian tumor subtypes (Table 10.1).
Since epithelial ovarian tumors are the most common andthe most lethal tumors of the ovaries, the majority of thetext will be devoted to epithelial ovarian cancers.
Germ Cell Tumors
Ovarian germ cell tumors develop from the oocyte andaccount for less than 7% of ovarian neoplasms. Theytypically occur in teenagers and young women. Maturecystic teratomas (dermoid cysts) comprise 95% of thesetumors and often contain differentiated tissues such asskin, teeth, and hair (Fig. 10.3a). Approximately one-thirdof germ cell tumors are malignant.
Sex Cord–Stromal Cell Tumors
Sex cord–stromal cell tumors account for less than 8% ofovarian neoplasms. They originate from granulosa cells,

SCREENING AND DETECTION 173
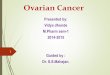
Figure 10.2. Adult mouse ovary section. The section is stained with hematoxylin and eosin(H&E), which stain nuclei and cell cytoplasm, respectively.
Table 10.1. Histologic Classification of Ovarian Tumors
SurfaceEpithelial–StromalTumors
SexCord–Stromal
TumorsGerm Cell
Tumors
Serous Fibroma-thecoma Mature teratomaMucinous Granulosa cell Immature teratomaEndometrioid Sertoli-leydig cell DysgerminomaClear cell Serotoli cell Yolk sacTransitional Mixed Embryonal
carcinomaSquamous Steroid cell ChoriocarcinomaMixed epithelial Mixed germ cellUndifferentiated
carcinomaGonadoblastoma
theca cells and their luteinized derivatives, and Sertolycells, Leydig cells, and fibroblasts of stromal origin. Mostclinically malignant sex cord–stromal tumors are of thegranulosa cell type (Fig. 10.3b).
Surface Epithelial–Stromal Tumors
More than 90% of human ovarian cancers are epithe-lial and believed to originate from the ovarian surfaceepithelium (Scully, 1977). Epithelial ovarian cancers arepredominantly a disease of perimenopausal and post-menopausal women, with 80% to 90% of ovarian cancercases occurring after the age of 40. The peak incidenceof invasive epithelial ovarian cancer occurs at age 63.Hereditary ovarian cancers occur approximately 10 yearsearlier (Boyd and Rubin, 1997). The most significant riskfactor, other than age, is family history of ovarian can-cer. The risk increases with infertility and multiparity anddecreases with multiparity. A striking discovery within
the last 20 years has been the protective effect of oralcontraceptives against ovarian cancer (Franceschi et al.,1991). After 5 years of oral contraceptive use, womenreduce their risk of ovarian cancer by 50% (Holschneiderand Berek, 2000; Purdie et al., 2003). It is believedthat hormonal changes and suppression of ovulation areresponsible for the protective effect of multiparity and oralcontraceptives. Epithelial ovarian cancers can be dividedinto four main different histologic subtypes: serous, muci-nous, endometrioid, and clear cell (Figs. 10.3c– f). Insome cases, ovarian epithelial cancers consist of more thanone distinct histologic subtype.
SCREENING AND DETECTION
The inaccessible anatomic location of the ovaries and theasymptomatic nature of the disease hinder the detection ofcancer while it is still confined to the ovary. Even in laterstages, the disease is usually associated with subtle symp-toms such as abdominal bloating, discomfort, or changesin bowel or bladder habits. These common symptomsare often misdiagnosed or simply dismissed. As a result,over 75% of ovarian cancer patients are diagnosed at anadvanced stage when peritoneal dissemination has alreadytaken place (Holschneider and Berek, 2000). Unlike manyother epithelial tumors that progress gradually and displayidentifiable preneoplastic lesions, the majority of ovarianepithelial cancers display characteristics of invasive car-cinoma without any evidence of intermediate phases ofbenign and/or borderline neoplastic lesions. Ovarian can-cers also appear to have a different pattern of invasion andmetastasis than the majority of solid epithelial tumors.The most common route of spread is by direct exten-sion to adjacent organs or by exfoliation of tumor cells

174 OVARIAN CANCER
(a)
(b)
(c)
(d)
(e)
(f )
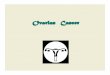
Figure 10.3. Histologic types of ovarian cancer. (a) Mature cystic teratoma, the most commonsubtype in the category of germ cell tumors. Hair is grossly seen. (b) Granulosa cell tumor(subtype of sex cord–stromal cell tumor). Four main human epithelial ovarian cancer subtypes:(c) serous, (d) mucinous, (e) endometrioid, and (f) clear-cell carcinoma. (Courtesy of E. Oliva).

TREATMENT 175
from the ovary, followed by intraperitoneal dissemination,implantation, and growth of metastases on mesothelial sur-faces. The tumor cells are often transported into the upperabdomen with the continuous clockwise movement of theperitoneal fluid resulting from bowel peristalsis and res-piratory motion. In addition, ovarian cancer can spread toregional lymph nodes. Blood-borne metastases are rare.
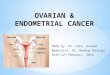
Because the five-year survival rate for patients withearly-stage ovarian cancer is significantly better thanthat for patients with advanced disease, there have beencontinued attempts to improve techniques for screeningand early detection. A screening test must have suffi-cient sensitivity and specificity to be effective. The sen-sitivity is necessary in order to detect the disease atan early stage, while the specificity is needed becausethe incidence of ovarian cancer is relatively low in theaverage population. Serum tumor marker CA125 (Bastet al., 1983) and imaging using transvaginal sonography(Fig. 10.4) are the most widely used detection methodsfor ovarian cancer. However, neither of these methodshas sufficient sensitivity and specificity to be useful forscreening of asymptomatic women in the general popu-lation (Bast et al., 2002; Gallion and Bast, 1993; Helzl-souer et al., 1993; Schwartz, 2002; Schwartz et al., 1995;Schwartz and Taylor, 1995). Improvements in early diag-nosis may be achieved by using a panel of markersthat are differentially expressed in the serum of womenwith ovarian cancer. High-throughput molecular tech-nologies, such as cDNA microarray expression profiling,comparative genomic hybridization screening, and pro-teomic pattern analysis with learning algorithms, haverecently been used to identify a discriminatory patternthat can distinguish ovarian cancer patients from healthywomen (Bayani et al., 2002; Hough et al., 2001; Ismailet al., 2000; Matei et al., 2002; Mok et al., 2001; Onoet al., 2000; Sawiris et al., 2002; Schummer et al., 1999;Schwartz et al., 2002; Shridhar et al., 2001; Tapper et al.,2001; Tonin et al., 2001; Wang et al., 1999; Welsh et al.,
Figure 10.4. Ultrasonography image of ovarian cancer. (Cour-tesy of S. Mironov and H. Hricak).
2001). Recent proteomic data demonstrated that it is pos-sible to use this nonbiased global approach to extract adiscriminatory fingerprint that recognizes stage I ovariancancer with sensitivity and specificity that exceeds that ofCA125 (Petricoin et al., 2002). This could be an importantdevelopment in ovarian cancer screening if the methodproves to be specific in a more general population.
TREATMENT
Since there are many types of tumors that can arise inthe ovaries, the treatment depends on the type of cancerand the extent of its spread. Benign tumors of the ovarycan be removed surgically without the need for furthertreatment. Management of malignant ovarian cancers gen-erally requires a multimodal approach, which commonlyincludes surgery and combination chemotherapy. The cur-rent chemotherapy regimens typically consist of combina-tions of paclitaxel or cyclophosphamide and cisplatin orcarboplatin. The two principal prognostic factors are stageat diagnosis and maximum residual disease followingcytoreductive surgery. The stage is determined at surgeryand depends upon the extent of ovarian cancer spread(Table 10.2). In most cases, the tumor has spread through-out the abdomen and cannot be completely removed bysurgery. Thus the goal of cytoreductive surgery is toremove as much cancer as possible, preferably withoutleaving nodules larger than 1 cm in size. Most patientswith advanced ovarian cancer will respond well to the
Table 10.2. Surgical Stages of Ovarian Cancer
Stage I: Limited to the ovariesIA: One ovary involvedIB: Both ovaries involvedIC: One or both ovaries involved but with
cancer on the surface of an ovary, rupture ofan ovarian cyst, malignant ascites, or positiveabdominal washings
Stage II: Spread to adjacent pelvic structuresIIA: Spread to uterus or fallopian tubesIIB: Spread to pelvic peritoneumIIC: Confined to the pelvis but with malignant
ascites or positive abdominal washings
Stage III: Spread to the upper abdomenIIIA: Microscopic spread to the upper abdomenIIIB: Cancer nodules less than 2 cm in the
abdomenIIIC: Cancer nodules more than 2 cm in the
abdomen or positive pelvic or aortic lymphnodes
Stage IV: Distant spread beyond the abdominal cavity orvisceral metastases

176 OVARIAN CANCER
initial treatment and some will have a complete remission.However, recurrent cancers are often resistant to fur-ther treatment regimens. After aggressive cytoreductivesurgery and combination chemotherapy, five-year survivalrates are as follows: stage I (93%), stage II (70%), stageIII (37%), and stage IV (25%) (Holschneider and Berek,2000). Unfortunately, less than one-third of patients arediagnosed at stage I.
ETIOLOGY
Our ability to screen for early-stage ovarian cancer is ham-pered by deficiencies in the understanding of the molec-ular and morphologic steps involved in ovarian carcino-genesis. Epidemiologic studies suggest a direct correlationbetween the number of ovulatory cycles and the risk ofovarian cancer (Bernal et al., 1995; Perez et al., 1991;Purdie et al., 2003). The first theory about the role thatovulation could play in ovarian carcinogenesis was putforward by Fathalla (1971). He speculated that the rupture
of a follicle increases the risk of ovarian cancer by causingtrauma and exposing the ovarian surface epithelium tohigh levels of steroid hormones and gonadotropins. Also,repair of the ovulatory wound in the ovarian surfacelikely results in the rapid proliferation of epithelial cells,which may increase the frequency and accumulation ofspontaneous mutations. Additionally, ovulation may leadto the entrapment of epithelial cells in the underlyingstroma with the subsequent formation of inclusion cysts.These inclusion cysts could be the precursor ovarian can-cer lesions in which the surrounding stromal environmentfacilitates neoplastic transformation (Fig. 10.5a).
Another cancer-contributing factor may result fromthe pluripotential nature of ovarian surface epithelialcells. Embryologically, the ovarian surface epitheliumis derived from the coelomic epithelium (Fig. 10.1),which overlies the presumptive gonadal ridge (Barber,1988; McLaren, 2000). The coelomic epithelium alsogives rise to the Mullerian ducts, which are the pri-mordia for the epithelia of the Fallopian tubes, uterine
(a)
(b)
Figure 10.5. Model of ovarian carcinogenesis. (a) Epithelial carcinomas are thought to arisefrom the surface epithelium or cortical inclusion cysts. Cortical inclusion cysts form as a resultof surface complexity that is associated with aging and/or as part of the surface repair processfollowing ovulation. These cysts, under the hormonal effects of the ovarian stroma, are moresusceptible to malignant change. (Reproduced with permission from • The Women’s Oncologyž Q1Review.) (b) Ovarian surface epithelium consists of a single sheet of cells that secrete a basementmembrane on their basal side. The basement membrane is thought to serve both as a barrierfrom direct contact between epithelial and stromal cells and as a medium for directing polarizedsignaling between the two cell types. In this figure, the basement membrane of the mouse ovarianepithelium was detected by immunohistochemical staining of laminin. (See color insert)

GENETIC ABERRATIONS IN SPORADIC AND HEREDITARY OVARIAN CANCERS 177
corpus, and endocervix. Developmentally, the ovarian sur-face epithelium has retained properties of uncommittedpluripotential cells and, similar to the embryonic coelomicepithelium, is competent to differentiate along several dif-ferent pathways. This pluripotential state may be neces-sary to provide the ovarian surface epithelium with thephenotypic plasticity required for its functions in ovu-latory wound repair. However, it might also contributeto the susceptibility of the ovarian surface epithelium toundergo neoplastic transformation. It is thought that anearly step in epithelial ovarian neoplasia involves aber-rant epithelial differentiation of the cells on the ovariansurface. The ability of the ovarian surface epithelial cellsto undergo Mullerian differentiation was demonstratedexperimentally by ectopic expression of the homeoboxgene HOXA7• in immortalized ovarian surface epithe-ž Q3lial cells (Naora et al., 2001). Consistent with the abilityof ovarian surface epithelial cells to differentiate alongMullerian lines, malignancies of the ovary display aremarkable range of histologic features, which generallyrecapitulate those of the Fallopian tube, endocervix, andendometrium (Fox, 1993). Based on cellular and structural
features reminiscent of normal adult tissues of Mullerianorigin, malignant epithelial neoplasms are classified intoserous, mucinous, clear-cell, and endometrioid carcinomas(Table 10.1, Figs. 10.3c– f). While substantial evidencesupports the theory that serous ovarian tumors originatefrom the ovarian surface epithelium (Auersperg et al.,1998; Berchuck and Carney, 1997; Feeley and Wells,2001; Ghahremani et al., 1999), the origin of mucinous,clear-cell and, endometrioid ovarian tumors is less clear.
GENETIC ABERRATIONS IN SPORADIC ANDHEREDITARY OVARIAN CANCERS
Cytogenetic analyses of human ovarian cancers haverevealed numerous chromosomal aberrations, but theyhave failed to identify a consistent chromosomal aber-ration that is ubiquitously present in ovarian can-cers (Gallion et al., 1990; Gray et al., 2003; Pejovic et al.,1992; Whang-Peng et al., 1984). Similarly, although manygenetic alterations have been found to be associated withovarian cancer (Table 10.3), a single individual genetic
Table 10.3. Alterations in Oncogenes and Tumor Suppressor Genes That Have Been Observed in Human OvarianCarcinomas
GeneChromosome
Location Type of Alteration Function
OncogenesPIK3CA 3q26.3 Amplification, overexpression Phosphatidylinositol 3-kinase activityc-FMS 5q33-q35 Overexpression Tyrosine kinase, cell growth, proliferationEGFR 7p12 Loss of expression Tyrosine kinase, signalingc-myc 8q24.12-q24.13 Amplification, overexpression Proliferation, transcription, cell cycle regulationK-ras 12p12.1 Mutation (codons 12,13, and 61) Signal transduction, cell cycle regulationAkt1 14q32.3 Amplification, overexpression Protein kinaseHER-2/neu 17q21.1 Amplification, overexpression Receptor signaling, cell proliferationAkt2 19q13.1-q13.2 Amplification, overexpression Protein kinaseEEF1A2 20q13.3 Amplification, overexpression Protein elongation factor
Tumorsuppressorgenes
NOEY2 (ARHII) 1p31 Loss of expression Induces p21, inhibits cyclin D1MSH2 2p21 Mutation DNA mismatch repairFHIT 3p14.2 Altered transcripts UnknownSPARC 5q31.3-q32 Loss of expression Extracellular matrix protein, cell adhesionLOT-1 6q25 Loss of expression Zinc-finger proteinp16 (NK4A) 9p21 Loss of expression Cell cycle checkpointPTEN 10q23.3 Mutations PhosphataseWT1 11p13 Mutations Transcription factorp27KIP 1 12p13 Loss of expression Cyclin-dependent kinase inhibitorBRCA2 13q12.3 Mutations DNA repair, cell cycle regulationRb1 13q14.2 Loss of expression, mutations Cell cycle regulationTP53 17p13.3 Mutations Apoptosis, cell cycle regulation, transcriptionOVCA1 and OVCA2 17p13.3 Loss of expression UnknownBRCA1 17q21 Mutations DNA repair, cell cycle regulation, transcription

178 OVARIAN CANCER
aberration that is present in all ovarian carcinomas hasnot been identified. It is likely that the identified geneticaberrations represent only a fraction of the genes thatare involved in ovarian cancer initiation and progres-sion (Gray et al., 2003). It is unclear whether ovariancarcinomas of different histologic subtypes develop viadistinct molecular pathways. Aberrations in genes such asp53, c-myc, K-ras, Akt, and HER-2 have been observed inall four histologic subtypes of ovarian carcinoma. How-ever, some genetic aberrations are more prevalent incertain ovarian cancer subtypes. For example, K-ras muta-tions are more frequently found in mucinous than in seroustumors (Pieretti et al., 1995), and c-myc overexpression ismore common in serous tumors (Baker et al., 1990; Wanget al., 1999). Mutations in PTEN and ß-catenin typicallyoccur in endometrioid tumors but not in other ovarian can-cer types (Obata et al., 1998; Wu et al., 2001; Zhai et al.,2002). Recent findings that gene expression patterns inovarian carcinomas reflect both the morphologic featuresand biologic behavior of tumors (Schwartz et al., 2002;Tonin et al., 2001) indicate that the underlying geneticalterations may be the foundation of tumor heterogeneity.
The majority of ovarian cancers are sporadic, withoutany known familial history of ovarian cancer. Approx-imately 10% of ovarian cancers are hereditary (Randallet al., 1998). Most hereditary cancers can be attributed togermline mutations in the breast/ovarian cancer suscepti-bility gene Brca1 (Miki et al., 1994) or Brca2 (Woosteret al., 1995). Sporadic and hereditary cancers are sim-ilar in many respects; however, patients with heredi-tary cancers develop the disease earlier, display a longerrecurrence-free interval following chemotherapy, and havea longer overall survival rate (Zweemer et al., 1999b).This may be related to the increased sensitivity of Brca-deficient tumor cells to therapeutic DNA damaging agentsthat produce double-stranded breaks (Scully and Liv-ingston, 2000). Studies in mouse models have demon-strated that p53 is highly cooperative with Brca1 in pro-moting mammary and ovarian tumor development (Xuet al., 2001). It is thought that the absence of p53decreases apoptosis and relaxes the cell cycle control,thus preventing the Brca1-induced apoptosis and senes-cence (Cao et al., 2003). Consistently, p53 aberrationsare commonly found in ovarian and breast tumors fromwomen heterozygous for Brca1 (Zweemer et al., 1999a).Recent analysis of prophylactically removed ovaries fromBrca1-heterozygous women demonstrated that Brca1 lossof heterozygosity and inactivation of the p53 function arethe early events in the induction of hereditary ovariancancer (Werness et al., 2000).
TISSUE CULTURE MODELS
The basic biology of the ovarian surface epitheliumand the molecular mechanisms underlying the acquisition
of an invasive phenotype in this tissue are not wellunderstood. This lack of understanding is due to thedifficulties in establishing an appropriate model systemfor epithelial ovarian carcinoma. The development ofculture systems posed problems because the ovariansurface epithelium constitutes a very small fraction ofthe whole ovary and is difficult to separate from otherovarian cell types by physical or enzymatic means.However, in the 1980s, the first tissue culture systemsfor ovarian surface epithelium from different species,including human, were developed (Adams and Auersperg,1983; Auersperg et al., 1984; Dubeau et al., 1990; Nicosiaet al., 1984). Mouse and rat ovarian epithelial cellssubjected to repetitious growth in culture occasionallyundergo malignant transformation. Independent cell linesderived from such spontaneously transformed culturesdisplay a range of cytogenetic changes (Testa et al., 1994).
The main difficulty in establishing cultures of humanovarian surface epithelial cells is their limited growthpotential and early senescence. Unlike rodent cells, humanovarian surface epithelial cells do not spontaneously trans-form in culture. Even expression of the simian virus 40 Tantigen (SV40 TAg) is not sufficient to immortalize humanovarian surface epithelial cells, although it significantlyincreases their growth potential (Maines-Bandiera et al.,1992). Such ovarian surface epithelial cells are nontu-morigenic, but they acquire several other properties ofneoplastic cells, including reduced dependence on serumand genetic instability. Transformed ovarian epithelial celllines are used in many laboratories as representative ofnormal human ovarian surface epithelium. However, thesecell lines have frequently undergone genetic alterationsfollowing establishment in tissue culture and thus are nottruly representative of normal ovarian surface epithelium.Another difficulty in modeling ovarian cancer in cultureis that the ovarian stromal cells may play a crucial role inovarian cancer induction (Ghahremani et al., 1999). In anormal ovary, the monolayered ovarian surface epithe-lium lies adjacent to the basement membrane (Nicosiaet al., 1989) that separates the epithelium from the ovar-ian stroma (Fig. 10.5b). Thus, organ culture systems inwhich epithelial cells are in constant communication withthe underlying ovarian stroma may be necessary to trulymodel the normal biologic functions of this tissue and itschanges in neoplasia.
Nevertheless, the use of ovarian surface epithelialcultures, primary and immortalized, has provided theopportunity to investigate the underlying genetic changesthat induce a tumorigenic state in this tissue. The firstdemonstrations that the immortalized ovarian surfaceepithelium can be transformed by introducing definedgenetic elements were achieved by transfection of rodentovarian surface epithelial cells with K-ras (Adams andAuersperg, 1981), H-ras (Hoffman et al., 1993), and

MOUSE MODELS 179
HER-2/neu (Davies et al., 1998). Recently, the trans-formation capability of cultured human ovarian surfaceepithelium was demonstrated by the introduction of SV40TAg, the catalytic subunit of human telomerase (hTERT)and H-ras (Liu et al., 2002).
MOUSE MODELS
Over the last 20 years, the bulk of research on animalmodels for ovarian cancer has involved the xenograftingof human ovarian tumors and established ovarian cancercell lines into immunodeficient mice (Hamilton et al.,1984). The use of immunodeficient mice as surrogatehosts for human tumors has provided a valuable andreproducible system that represents the best approximationto the original human tumor. However, the majority ofovarian cancer cell lines have been established fromtumors or ascites from patients with advanced ovariancancers that have already accumulated numerous geneticchanges. The complexity of genetic events in such tumorsand cell lines has made it difficult to correlate the tumorphenotype to the primary genetic events that trigger tumorformation. Additionally, xenografting human cells intoimmunodeficient mice cannot simulate the interaction ofthe immune system in the development and progression ofovarian cancer, which may prove critical in understandingthe disease.
Unlike human ovarian tumor cells that can onlybe introduced into immunodeficient mice, transformedmouse ovarian cells can be introduced into syngeneicmice with intact immune systems, thus making mousemodels suitable for the investigation of tumor–hostinteractions and antitumor immune mechanisms (Robyet al., 2000). Additionally, new genes suspected to playa role in tumorigenesis could be introduced into thetransformed mouse cell line. The utility of this approachwas elegantly demonstrated in examining the multifacetedfunctions of vascular endothelial growth factor (VEGF)•ž Q4in modulating the tumor microenvironment and affectingthe complex interactions in angiogenesis and antitumorimmune mechanisms (Zhang et al., 2002).
The lack of common inbred laboratory animals thatdevelop epithelial ovarian cancer remains one of the majorobstacles to ovarian cancer research. It is unclear whyspontaneous epithelial ovarian cancers are rare in lab-oratory animals. One possible explanation is that theovarian surface epithelium in most laboratory animalsis structurally and functionally different and thus lacksspecific characteristics which predispose the human ovar-ian surface epithelium to neoplastic progression. It isalso possible that the life span of most laboratory ani-mals is not long enough for the development of theseneoplasms. The highest incidence of ovarian epithelial
tumors occurs in the postmenopausal period, which ischaracterized by the following changes: (1) the pool ofgerm cells (oocytes) is depleted from the ovary; (2) theloss of germ cell–dependent follicle development resultsin a reduced level of circulating estrogen; (3) the reducedestrogen production is accompanied by higher produc-tion of gonadotropins, luteinizing hormone (LH), andfollicle-stimulating hormone (FSH); and (4) the struc-tural aberrations in the ovarian surface epithelium thatresults from numerous ovulations and ruptures of the oncesmooth ovarian surface. It is possible that the accumu-lation of genetic aberrations in aged ovaries and post-menopausal conditions cooperate in the predisposition toovarian cancer.
Several attempts have been made to generate mousemodels relevant to human ovarian tumors, largely bytrying to simulate the events that occur in the ovariesof postmenopausal women. The strategies have includeddepletion of oocytes, inhibition or overproduction of estro-gen and gonadotropins, carcinogen-induced transforma-tion, X-ray irradiation, neonatal thymectomy, and aging.The most common neoplasms induced by these methodswere of stromal origin. Several mouse models of germ celltumors have also been developed. Since stromal and germcell neoplasms are very rare in women, such models didnot find a niche in human ovarian cancer research. Veryrecently, efforts have been made to design mouse modelsof epithelial ovarian cancer, which is the prevalent cancertype in women. This was achieved by direct introductionof oncogenes into the ovarian surface epithelial cells or bygenerating genetically modified mice that are predisposedto tumor development. Currently existing mouse modelsfor germ cell, sex cord–stromal, and epithelial tumors aredescribed below.
Models of Germ Cell Tumors
A transgenic mouse line predisposed to the developmentof germ cell tumors was created by insertion of animprinted transgene TG.KD• (Fafalios et al., 1996). Germ ž Q5cell tumors develop in 15% to 20% of hemizygousfemale carriers of the transgene. These tumors consist ofa mixture of immature embryonal carcinoma cells andmature embryonic cells. They are frequently metastaticand, in some instances, result in death of the mouse.Genetic analyses demonstrated that the tumors in thesemice were associated with the transgene integration siteand did not occur in other transgenic lines with thesame transgene.
Development of benign cystic germ cell tumors occursin aging transgenic mice that overexpress the apoptosissuppression protein Bcl-2 under the ovary-specific inhibingene promoter (Hsu et al., 1996). Overexpression of Bcl-2 protein in the ovary leads to decreased ovarian somatic

180 OVARIAN CANCER
cell apoptosis and enhanced folliculogenesis. The bcl-2transgene in these mice is overexpressed in somatic cells,but not in oocytes, suggesting that enhanced survival ofselected somatic cells can lead to germ cell tumorigenesis.
Models of Sex Cord–Stromal Tumors
The importance of functional interaction between stromaland germ cells was demonstrated in female mice homozy-gous for the germ cell–deficient (gcd) mutation (Duncanet al., 1993; Duncan and Chada, 1993). These mice enterpremature reproductive senescence due to death of thegerm cells during embryonic development. Ovaries ofyoung gcd-null mice are atrophic and mostly consist ofconnective tissue matrix with some stromal cells. Half ofthese mice develop tubulostromal adenomas by one yearof age. Similarly, Wx/Wv mice which contain 1% of thenormal oocytes at birth rapidly lose the follicular appa-ratus and develop complex tubular adenomas from thesurface germinal epithelium (Blaakaer et al., 1995).
It is thought that the loss of germ cells in theovaries of postmenopausal women diminishes the numberof Graafian follicles and sex hormone secretion, lead-ing to compensatory over production of the pituitarygonadotropins LH and FSH. It has been suggested thatthe increase in gonadotropins contributes to the develop-ment of ovarian tumors (Capen et al., 1995). The potentialinvolvement of the pituitary gonadotropins LH and FSHin ovarian tumorigenesis has been extensively investi-gated, since the production of these hormones is elevatedin postmenopausal women. LH and FSH control ovarygrowth, differentiation, and steroidogenesis. The absenceof these hormones results in infertile individuals whomaintain a prepubescent state into adulthood with infan-tile gonads (Kendall et al., 1995). Both LH and FSH aremembers of the glycoprotein hormone family and areheterodimers that contain an α subunit common to eachhormone and a unique β subunit that dictates biologicspecificity (Pierce and Parsons, 1981). Expression of theglycoprotein α subunit and the hormone-specific β sub-unit is regulated by the gonadotropin-releasing hormone(GnRH), steroids, and the ovarian and pituitary peptides,activins, and inhibins (Matzuk et al., 1996; Pierce andParsons, 1981). The importance of gonadotropins in ovar-ian tumorigenesis was elegantly demonstrated by specificsuppression of gonadotropins in Wx/Wv mice (Blaakaeret al., 1995). Injection of Wx/Wv mice with GnRH ago-nist completely suppresses ovarian tumor development.The requirement for gonadotropins in induction of ovar-ian stromal tumors was also demonstrated in hypogo-nadotropic (hpg/hpg) mice deficient in GnRH and lackingLH and FSH. Irradiation-induced oocyte depletion orprolonged treatment with a high dose of gonadotropinsresults in mesothelial adenomas and granulosa cell tumors
in hpg/+ mice but not in hpg/hpg mice (Tennent andBeamer, 1986).
To address the role of overproduction of LH in ovar-ian tumor development, several transgenic mouse mod-els with chronic LH hypersecretion were developed (Keriet al., 2000; Nilson et al., 2000; Risma et al., 1995). Thecommon characteristics of these mice include infrequentovulation, a prolonged luteal phase, and development ofpathologic ovarian changes such as cyst formation andenlargement of ovaries with reduced numbers of pri-mordial follicles. Depending on the mouse strain, theaged female mice with chronically elevated LH developluteoma or granulosa cell tumors (Nilson et al., 2000).Overproduction of FSH has also been studied in ovar-ian tumorigenesis. For example, mice with homozygousdeletion of a member of the transforming growth fac-tor β (TGFβ) superfamily, inhibin, develop mixed orincompletely differentiated sex cord–stromal tumors asearly as four weeks with 100% penetrance (Matzuk et al.,1992). Consistent with the role of inhibin to suppresspituitary FSH synthesis and secretion, inhibin-deficientmice demonstrate an elevated concentration of FSH. Thus,besides a possible tumor suppressor role for inhibin, theaccompanying rise in FSH levels in the circulation maycontribute to tumor formation. Female mice deficient forthe FSH receptor are infertile and have high levels ofcirculating FSH (Danilovich et al., 2001; Kumar et al.,1996). They also have small ovaries resulting from ablockage in folliculogenesis at the preantral stage anddevelop stromal tumors after 12 months of age. In addi-tion to the high levels of circulating FSH, the elevatedlevels of LH in the FSH receptor mutant mice could con-tribute to ovarian tumor formation, which was shown tobe the case in LH-overexpressing mice (Keri et al., 2000;Nilson et al., 2000; Risma et al., 1995).
To delineate the biologic role of FSH in ovariangrowth and tumorigenesis, double-homozygous-mutantmice that are deficient in both inhibin and FSH were gen-erated (Kumar et al., 1999). Double-mutant mice showa significant delay in ovarian tumor development com-pared with mice deficient in inhibin alone. Mice defi-cient in inhibin and FSH have suppressed levels of FSH,but LH is still present and could contribute to ovar-ian tumorigenesis. Consistent with this hypothesis, micedeficient in inhibin and GnRH, which have suppressedlevels of both FSH and LH, develop only premalignantlesions in the ovary (Kumar et al., 1996). The role ofFSH in ovarian tumor development was further exploredby generating gain-of-function transgenic mice that over-express human FSH (Kumar et al., 1999). Female trans-genic mice expressing high levels of FSH are infertileand develop hemorrhagic and cystic ovaries but have nosigns of tumors. Together, these results suggest that pro-longed exposure to elevated FSH levels does not directly

MOUSE MODELS 181
cause ovarian tumorigenesis; however, FSH significantlyinfluences the tumor progression in inhibin-deficient mice.
Transgenic mice that express the powerful viral onco-gene SV40 TAg under regulation of the mouse inhibin-promoter develop metastatic ovarian granulosa and thecacell tumors with 100% penetrance at the age of fiveto six months (Kananen et al., 1995). The tumors aregonadotropin dependent and do not develop when thetransgenic mice are rendered gonadotropin deficient bycrossbreeding them into the hpg/hpg background. The sup-pression of gonadotropins by treating the mice with theGnRH antagonist SB-75 also results in the inhibition oftumor growth (Kananen et al., 1997).
Expression of SV40 TAg under the regulation of theMullerian-inhibiting substance (MIS) promoter in trans-genic mice induces development of granulosa cell tumors,which in advanced stages invade neighboring organsand develop metastases to the liver and lungs (Dutertreet al., 1997, 2001; Peschon et al., 1992). MIS bindsto the Mullerian inhibitory substance type II receptor(MISIIR), which is specifically localized to ovarian gran-ulosa cells (di Clemente et al., 1994; Takahashi et al.,1986) and ovarian surface epithelium (Connolly et al.,2003). Frequently, the MIS type II receptor can bedetected in human ovarian tumors derived from granu-losa cells (Gustafson et al., 1992; Imbeaud et al., 1995)and the ovarian epithelial cells (Masiakos et al., 1999).MIS treatment of MIS type II–positive tumors and celllines exhibits growth-inhibitory effects (Kim et al., 1992;Masiakos et al., 1999; Segev et al., 2000; Stephen et al.,2001).
Models of Epithelial Tumors
Epithelial tumors are the most common, and also themost deadly, ovarian tumors in women. Therefore, mousemodels of epithelial ovarian tumors are highly soughtafter. One difficulty in establishing genetically modifiedmice in which gene expression is altered specifically inthe ovarian surface epithelial cells is that these cells lackspecialized features that could be exploited as a source oftissue-specific promoters. Researchers resorted to usingpromoters of genes that are expressed in several tissues,including the ovarian surface epithelium. Hamilton andcolleagues used the upstream regulatory sequences ofthe mouse MISIIR gene to target expression of SV40TAg to the precursor cells that generate several tissuesof the female mouse reproductive tract, including theovarian surface epithelium (Connolly et al., 2003). By6–13 weeks of age, 50% of the transgenic femalemice develop bilateral ovarian masses. Histologically, theovarian tumors are poorly differentiated carcinomas withoccasional cysts and papillary structures that resemblehuman ovarian serous carcinoma (Fig. 10.6a). The tumors
are often associated with the production of bloody ascitesand extensive tumor cell dissemination and invasionto the omentum, mesentery, and parietal and visceralserosa. Consistent with the presence of MISIIR in severaltissue types, other gynecologic tumors develop, albeit lessfrequently. Unfortunately, it may be difficult to establishstable transgenic lines of MISIIR-TAg mice because therapid onset of tumor initiation renders female miceinfertile. Consistent with the expression of MISIIR inthe tubular and follicular structures of the fetal malegonads and in Sertoli and Leydig cells of adult testis,28% of the male MISIIR-TAg mice develop Sertoli celltumors but remain fertile. Thus, it may be possible totransmit the transgene and the ovarian phenotype tofemale offspring through the male transgenic mice. Thisheritable transgenic ovarian cancer model is currently themost promising model in terms of understanding howovarian cancer is initiated. The utility of the model instudying the genesis of ovarian cancer will significantlyincrease with the development of conditionally controlledexpression of SV40 TAg and with a better understandingof the individual biochemical pathways that are altered bythis potent viral oncogene.
Although the ovarian tumors in the aforementionedmouse models histologically resemble human ovarianneoplasms, they may not accurately represent geneticchanges that occur during tumor development. It isthought that most human cancers develop as a resultof the accumulation of multiple genetic events. Thus,to dissect the multigenetic etiology of cancers, it isnecessary to find technical means by which to sequentiallyintroduce multiple genetic modifications into mammaliancells. Furthermore, the majority of human cancers arisein somatic cells, initiating neoplasia in the adult, unlikemost transgenic mouse models that carry germline geneticmodifications during embryonic development. Recently,a new technique for the introduction of multiple genesinto somatic cells of adult mice was developed (Federspielet al., 1996). This system is based on avian RCAS virusdelivery to the cells that are programmed to express theavian TVA receptor.
In this system, viral infection can be restricted to a spe-cific tissue of interest by placing TVA under the controlof a tissue-specific promoter. The RCAS-TVA system hasbeen used to generate mouse models for several humancancers, including ovarian cancer (reviewed in Orsulic,2002). Due to the lack of an ovarian epithelium-specificpromoter, transgenic mice that express TVA from thekeratin 5 promoter were used. The ovary-specific genedelivery was ensured by isolating the ovaries from miceand infecting them ex vivo with RCAS vectors. Sinceovarian surface epithelial cells are the only ovarian cellsthat express the TVA receptor (Fig. 10.6b), these are theonly cells susceptible to the RCAS virus infection. RCAS

182 OVARIAN CANCER
(a)
(c)(b)
(e)(d)
(g)(f)
Figure 10.6. Mouse models of epithelial ovarian cancer. (a) The ovarian carcinoma in themouse chimeric for expression of the simian virus 40 T antigen (SV40 TAg) under controlof the Mullerian inhibitory substance type II receptor (MISIIR) promoter. Neoplastic cellsform tubular (arrowheads) and papillary (arrows) structures in the ovary and in the intrabursalspace, respectively, and invade the ovarian bursa (OB). (b–e) An RCAS-TVA mouse modelfor ovarian epithelial cancer. (b) Ovary section from a keratin 5-TVA transgenic mouse stainedwith antibody against the avian retroviral TVA receptor. Ectopic expression of the TVA receptorrenders the cells susceptible to infection with avian RCAS viruses, which are used as vehiclesfor gene transfer. Cell-specific expression of the TVA receptor restricts the infection to thecells of the ovarian surface epithelium, which is the presumptive precursor tissue for ovariancarcinoma. (c) Intraperitoneal carcinomatosis in a mouse model for epithelial ovarian cancerresembles human ovarian cancer spread. (d) Metastatic ovarian tumor spread. An • HA-labeledž Q2Akt oncogene is detected in the primary ovarian tumor and in ovarian metastases. (e) H&Estaining of an ovarian tumor induced in the RCAS-TVA mouse model. Ovarian tumors inducedin the mouse model histologically resemble human ovarian papillary serous carcinoma. (f,g)Serous adenocarcinoma induced by selective AdCre-LoxP mediated inactivation of p53 andRb1 in the ovarian surface epithelium of p53f loxP/f loxP Rbf loxP/f loxP mice. (f) H&E stainingrepresenting mitotic (arrows) carcinoma cells that form glandular structures in dense fibroustissue. (g) Immunohistochemical detection of keratin 8 in invasive neoplastic cells (arrow).(Courtesy of A. Yu. Nikitin). (See color insert)

AREAS IN WHICH MODELS ARE NEEDED 183
vectors can be designed to carry oncogenes, dominant-negative tumor suppressor genes, and various markergenes. Thus, genetically defined aberrations can be intro-duced into the ovarian epithelial cells of adult femalemice. This provides a very efficient means to evaluatethe collaboration of candidate genes in ovarian onco-genesis. For example, the minimal genetic requirementsfor induction of a tumorigenic state in primary mouseovarian epithelial cells were determined by introduc-ing combinations of c-myc, K-ras, and Akt into ovar-ian cells from p53-null mice. It was demonstrated thata loss of the p53 gene and the addition of any two ofthe c-myc, K-ras, and Akt oncogenes are sufficient toinduce transformation of mouse primary ovarian epithe-lial cells (Orsulic et al., 2002). These genetic aberrationsare commonly present in human ovarian carcinomas,although it is not known whether they act in combina-tion to induce ovarian tumors. Orthotopic implantation ofex vivo infected ovarian cells results in metastatic ovar-ian tumors in four to eight weeks, depending upon thecombination of oncogenic aberrations. The initial tumori-genic growth is confined to the implanted ovary fol-lowed by spread to adjacent tissues and finally metastaticgrowth on the surfaces of intraperitoneal organs witha special affinity for the omentum and the mesentery(Figs. 10.6c,d). The metastatic tumor development in thismodel closely resembles human ovarian tumor develop-ment and metastatic spread, including the production ofascites and tumor spread throughout the peritoneal cavity.Similar to human ovarian metastatic cancer, the tumorburden remains confined to the peritoneal cavity. Histo-logically, these tumors resemble human ovarian serouspapillary carcinomas (Fig. 10.6e). Therefore, this modelprovides direct experimental proof that the ovarian sur-face epithelium is the precursor tissue for serous ovar-ian carcinoma.
Perhaps the greatest limitation of the RCAS-TVAsystem is that the initiating genetic manipulation doesnot accurately model the sporadic molecular events thatoccur in vivo. However, the genetically defined nature ofthe model allows for the study of genotype–phenotypecorrelation and thus may lead to a clearer understandingof the contributions of individual genetic aberrationsto the process of tumor progression and metastasis.Understanding the collaboration of biochemical pathwaysin the induction of a tumorigenic state may set thestage for testing novel molecule-based therapies in thefuture. The similarities in metastatic behavior make thismodel particularly attractive for developing and testingtherapeutic approaches aimed at the advanced stages ofovarian epithelial cancer in humans.
The need for an ovary-specific promoter and/or ex vivoinfection and subsequent orthotopic implantation of
ovarian cells can be circumvented by the direct admin-istration of viruses into the intrabursal space of surgi-cally exposed mouse ovaries. The ovarian bursa envelopesthe mouse ovary to form an anatomically closed spacethat can be filled with viral supernatant and thus exposethe ovarian surface to the infectious viral particles. Thisapproach was used to introduce recombinant adenoviruswith cytomegalovirus (CMV)• driven Cre recombinase ž Q6into the ovaries of p53lox/lox /Rblox/lox mice in order toconcurrently inactivate p53 and Rb (Flesken-Nikitin et al.,2003). The mice develop tumors that contain epithelialcells (Figs 10.6f,g), which are thought to be derived fromthe adenovirus-infected ovarian surface epithelial cells.The majority of mice, with both genes inactivated, developovarian tumors at a median of 32 weeks, while mice witheither the p53 or Rb gene inactivated develop ovariantumors less frequently. These results demonstrate the col-laborative effect of concurrent inactivation of p53 and Rbin inducing tumorigenesis in ovarian cells. However, thelong tumor latency in these mice indicates that additionalgenetic aberrations are required for tumor development.
AREAS IN WHICH MODELS ARE NEEDED
None of the aforementioned mouse models for ovariancancer recapitulate the entire course of the humandisease. However, most of the models successfullyrecapitulate the later stages of the disease and themetastatic spread in the peritoneal cavity. Probably theleast understood aspect of ovarian cancer is its initiationand tissue of origin. Precursor lesions are almost neverdetected in patients and it is unclear whether ovariancarcinomas follow the gradual progression from benignto metastatic cancer or they occur de novo, withoutany identifiable premalignant stages (Bell and Scully,1994). Currently available mouse models fail to accuratelymodel the early steps in transformation of the ovariancells. Modeling ovarian cancer initiation in the mousewould significantly contribute to our understanding ofprecursor lesions and identifying recognizable histologicor molecular markers that could be used for earlyovarian cancer detection. Another aspect of ovarian cancerthat is poorly understood is the complexity of geneticaberrations and their role in ovarian cancer initiationand progression and the development of drug resistance.Mouse models in which distinct genetic aberrationscan be correlated with the tumor phenotype wouldnot only help to delineate the biochemical pathwaysresponsible for the different ovarian cancers but alsoprovide valuable systems in which to test pathway-targeted therapy. The use of mouse models for drugtesting will require concurrent development of imagingtechniques for monitoring the tumor response to the

184 OVARIAN CANCER
drug. Development of imaging modalities in the mousemay contribute to the development of urgently neededdetection methods for the early stages of ovarian cancer.
SUMMARY
The general lack of understanding of the biology andgenetics of ovarian cancer is a stumbling block in creatingmouse models for this disease. However, several modelsthat approximate certain aspects of ovarian cancer devel-opment and metastatic spread have been generated. Exper-iments on animal cell lines and mouse models have greatlycontributed to our understanding of the biology of theovarian surface epithelium and clearly demonstrated thatthis is the precursor tissue for epithelial ovarian cancer.The mouse models have provided insight into the geneticand hormonal requirements for ovarian cancer progressionand the understanding of the biochemical pathways thatgovern the development of ovarian carcinomas. Techno-logical and informational advances and new capabilitiesof manipulating gene expression in the mouse continueto contribute to the development of more sophisticatedmouse models for ovarian cancer. The next challenge is tocorrelate the information obtained from the mouse ovariancancer models with human ovarian cancers.
ACKNOWLEDGMENTS
The author acknowledges the Varmus Lab and the Susan G.Komen Foundation for their support and Kristy Daniels forassistance in preparation of the book chapter.
REFERENCES
Adams AT, Auersperg N (1981): Transformation of cultured ratovarian surface epithelial cells by Kirsten murine sarcomavirus. Cancer Res 41:2063–2072.
Adams AT, Auersperg N (1983): Autoradiographic investigationof estrogen binding in cultured rat ovarian surface epithelialcells. J Histochem Cytochem 31:1321–1325.
Auersperg N, Edelson MI, Mok SC, Johnson SW, Hamilton TC(1998): The biology of ovarian cancer. Semin Oncol25:281–304•.ž Q7
Auersperg N, Siemens CH, Myrdal SE (1984): Human ovariansurface epithelium in primary culture. In Vitro 20:743–755.
Baker VV, Borst MP, Dixon D, Hatch KD, Shingleton HM,Miller D (1990): c-myc amplification in ovarian cancer.Gynecol Oncol 38:340–342.
Barber HR (1988): Embryology of the gonad with referenceto special tumors of the ovary and testis. J Pediatr Surg23:967–972.
Bast RC Jr, Klug TL, St John E, Jenison E, Niloff JM, LazarusH, Berkowitz RS, Leavitt T, Griffiths CT, Parker L, Zurawski
VR Jr, Knapp RC (1983): A radioimmunoassay using a mon-oclonal antibody to monitor the course of epithelial ovariancancer. N Engl J Med 309:883–887.
Bast RC Jr, Urban N, Shridhar V, Smith D, Zhang Z, SkatesS, Lu K, Liu J, Fishman D, Mills G (2002): Early detectionof ovarian cancer: Promise and reality. Cancer Treat Res107:61–97.
Bayani J, Brenton JD, Macgregor PF, Beheshti B, Albert M,Nallainathan D, Karaskova J, Rosen B, Murphy J, Lafram-boise S, Zanke B, Squire JA (2002): Parallel analysis of spo-radic primary ovarian carcinomas by spectral karyotyping,comparative genomic hybridization, and expression microar-rays. Cancer Res 62:3466–3476.
Bell DA, Scully RE (1994): Early de novo ovarian carcinoma.A study of fourteen cases. Cancer 73:1859–1864.
Berchuck A, Carney M (1997): Human ovarian cancer of thesurface epithelium. Biochem Pharmacol 54:541–544.
Bernal A, Mendez-Moran L, Fajardo-Gutierrez A, Gonzalez-Lira G, Escudero P, Ortiz H (1995): Univariate and multivari-ate analysis of risk factors for ovarian cancer: Case-controlstudy, Mexico City. Arch Med Res 26:245–249.
Blaakaer J, Baeksted M, Micic S, Albrectsen P, Rygaard J,Bock J (1995): Gonadotropin-releasing hormone agonist sup-pression of ovarian tumorigenesis in mice of the Wx/Wvgenotype. Biol Reprod 53:775–779.
Boyd J, Rubin SC (1997): Hereditary ovarian cancer: Molec-ular genetics and clinical implications. Gynecol Oncol64:196–206.
Cao L, Li W, Kim S, Brodie SG, Deng CX (2003): Senescence,aging, and malignant transformation mediated by p53 inmice lacking the Brca1 full-length isoform. Genes Dev17:201–213.
Capen CC, Beamer WG, Tennent BJ, Stitzel KA (1995): Mech-anisms of hormone-mediated carcinogenesis of the ovary inmice. Mutat Res 333:143–151.
Connolly DC, Bao R, Nikitin AY, Stephens KC, Poole TW,Hua X, Harris SS, Vanderhyden BC, Hamilton TC (2003):Female mice chimeric for expression of the simian virus 40TAg under control of the MISIIR promoter develop epithelialovarian cancer. Cancer Res 63:1389–1397.
Danilovich N, Roy I, Sairam MR (2001): Ovarian pathologyand high incidence of sex cord tumors in follitropin receptorknockout (FORKO) mice. Endocrinology 142:3673–3684.
Davies BR, Auersperg N, Worsley SD, Ponder BA (1998):Transfection of rat ovarian surface epithelium with erb-B2/neuinduces transformed phenotypes in vitro and the tumorigenicphenotype in vivo. Am J Pathol 152:297–306.
di Clemente N, Wilson C, Faure E, Boussin L, Carmillo P,Tizard R, Picard JY, Vigier B, Josso N, Cate R (1994):Cloning, expression, and alternative splicing of the receptorfor anti-Mullerian hormone. Mol Endocrinol 8:1006–1020.
Dubeau L, Velicescu M, Sherrod AE, Schreiber G, Holt G(1990): Culture of human fetal ovarian epithelium in achemically-defined, serum-free medium: A model for ovariancarcinogenesis. Anticancer Res 10:1233–1240.

REFERENCES 185
Duncan M, Cummings L, Chada K (1993): Germ cell deficient(gcd) mouse as a model of premature ovarian failure. BiolReprod 49:221–227.
Duncan MK, Chada KK (1993): Incidence of tubulostromaladenoma of the ovary in aged germ cell-deficient mice. JComp Pathol 109:13–19.
Dutertre M, Gouedard L, Xavier F, Long WQ, di Clemente N,Picard JY, Rey R (2001): Ovarian granulosa cell tumorsexpress a functional membrane receptor for anti-Mullerianhormone in transgenic mice. Endocrinology 142:4040–4046.
Dutertre M, Rey R, Porteu A, Josso N, Picard JY (1997): Amouse Sertoli cell line expressing anti-Mullerian hormone andits type II receptor. Mol Cell Endocrinol 136:57–65.
Fafalios MK, Olander EA, Melhem MF, Chaillet JR (1996):Ovarian teratomas associated with the insertion of animprinted transgene. Mamm Genome 7:188–193.
Fathalla MF (1971): Incessant ovulation—a factor in ovarianneoplasia? Lancet 2:163.
Federspiel MJ, Swing DA, Eagleson B, Reid SW, Hughes SH(1996): Expression of transduced genes in mice generated byinfecting blastocysts with avian leukosis virus-based retroviralvectors. Proc Natl Acad Sci USA 93:4931–4936.
Feeley KM, Wells M (2001): Precursor lesions of ovarianepithelial malignancy. Histopathology 38:87–95.
Flesken-Nikitin A, Choi KC, Eng JP, Shmidt EN, Nikitin AY(2003): Induction of carcinogenesis by concurrent inactivationof p53 and Rb1 in the mouse ovarian surface epithelium.Cancer Res 63:3459–3463.
Fox H (1993): Pathology of early malignant change in the ovary.Int J Gynecol Pathol 12:153–155.
Franceschi S, Parazzini F, Negri E, Booth M, La Vecchia C,Beral V, Tzonou A, Trichopoulos D (1991): Pooled analysisof 3 European case-control studies of epithelial ovariancancer: III. Oral contraceptive use. Int J Cancer 49:61–65.
Gallion HH, Bast RC Jr (1993): National Cancer Institute Con-ference on Investigational Strategies for Detection and Inter-vention in Early Ovarian Cancer. Cancer Res 53:3839–3842.
Gallion HH, Powell DE, Smith LW, Morrow JK, Martin AW,van Nagell JR, Donaldson ES (1990): Chromosome abnor-malities in human epithelial ovarian malignancies. GynecolOncol 38:473–477.
Ghahremani M, Foghi A, Dorrington JH (1999): Etiology ofovarian cancer: A proposed mechanism. Med Hypotheses52:23–26.
Ginsburg M, Snow MH, McLaren A (1990): Primordial germcells in the mouse embryo during gastrulation. Development110:521–528.
Gray JW, Suzuki S, Kuo WL, Polikoff D, Deavers M, Smith-McCune K, Berchuck A, Pinkel D, Albertson D, Mills GB(2003): Specific keynote: Genome copy number abnormalitiesin ovarian cancer. Gynecol Oncol 88:S16–21; discussionS22–14.
Gustafson ML, Lee MM, Scully RE, Moncure AC, Hirakawa T,Goodman A, Muntz HG, Donahoe PK, MacLaughlin DT,Fuller AF Jr (1992): Mullerian inhibiting substance as
a marker for ovarian sex-cord tumor. N Engl J Med326:466–471.
Hamilton TC, Young RC, Ozols RF (1984): Experimental modelsystems of ovarian cancer: Applications to the designand evaluation of new treatment approaches. Semin Oncol11:285–298.
Helzlsouer KJ, Bush TL, Alberg AJ, Bass KM, Zacur H, Com-stock GW (1993): Prospective study of serum CA-125 levelsas markers of ovarian cancer. JAMA 269:1123–1126.
Hoffman AG, Burghardt RC, Tilley R, Auersperg N (1993): Anin vitro model of ovarian epithelial carcinogenesis: Changesin cell-cell communication and adhesion occurring duringneoplastic progression. Int J Cancer 54:828–838.
Holschneider CH, Berek JS (2000): Ovarian cancer: Epidemi-ology, biology, and prognostic factors. Semin Surg Oncol19:3–10.
Hough CD, Cho KR, Zonderman AB, Schwartz DR, Morin PJ(2001): Coordinately up-regulated genes in ovarian cancer.Cancer Res 61:3869–3876.
Hsu SY, Lai RJ, Finegold M, Hsueh AJ (1996): Targeted over-expression of Bcl-2 in ovaries of transgenic mice leadsto decreased follicle apoptosis, enhanced folliculogene-sis, and increased germ cell tumorigenesis. Endocrinology137:4837–4843.
Imbeaud S, Faure E, Lamarre I, Mattei MG, di Clemente N,Tizard R, Carre-Eusebe D, Belville C•, Tragethon L, Ton- ž Q8kin C, et al. (1995): Insensitivity to anti-mullerian hormonedue to a mutation in the human anti-mullerian hormonereceptor. Nat Genet 11:382–388.
Ismail RS, Baldwin RL, Fang J, Browning D, Karlan BY, Gas-son JC, Chang DD (2000): Differential gene expressionbetween normal and tumor-derived ovarian epithelial cells.Cancer Res 60:6744–6749.
Jemal A, Thomas A, Murray T, Thun M (2002): Cancer statis-tics, 2002. CA Cancer J Clin 52:23–47.
Kananen K, Markkula M, Rainio E, Su JG, Hsueh AJ, Huh-taniemi IT (1995): Gonadal tumorigenesis in transgenic micebearing the mouse inhibin alpha-subunit promoter/simianvirus T-antigen fusion gene: Characterization of ovariantumors and establishment of gonadotropin-responsive gran-ulosa cell lines. Mol Endocrinol 9:616–627.
Kananen K, Rilianawati•, Paukku T, Markkula M, Rainio EM, ž Q9Huhtanemi I (1997): Suppression of gonadotropins inhibitsgonadal tumorigenesis in mice transgenic for the mouseinhibin alpha-subunit promoter/simian virus 40 T-antigenfusion gene. Endocrinology 138:3521–3531.
Karl J, Capel B (1998): Sertoli cells of the mouse testis originatefrom the coelomic epithelium. Dev Biol 203:323–333.
Kendall SK, Samuelson LC, Saunders TL, Wood RI, CamperSA (1995): Targeted disruption of the pituitary glycoproteinhormone alpha-subunit produces hypogonadal and hypothy-roid mice. Genes Dev 9:2007–2019.
Keri RA, Lozada KL, Abdul-Karim FW, Nadeau JH, Nilson JH(2000): Luteinizing hormone induction of ovarian tumors:Oligogenic differences between mouse strains dictates tumordisposition. Proc Natl Acad Sci USA 97:383–387.

186 OVARIAN CANCER
Kim JH, Seibel MM, MacLaughlin DT, Donahoe PK, Ran-sil BJ, Hametz PA, Richards CJ (1992): The inhibitory effectsof mullerian-inhibiting substance on epidermal growth factorinduced proliferation and progesterone production of humangranulosa-luteal cells. J Clin Endocrinol Metab 75:911–917.
Kumar TR, Palapattu G, Wang P, Woodruff TK, Boime I, ByrneMC, Matzuk MM (1999): Transgenic models to studygonadotropin function: The role of follicle-stimulating hor-mone in gonadal growth and tumorigenesis. Mol Endocrinol13:851–865.
Kumar TR, Wang Y, Matzuk MM (1996): Gonadotropins areessential modifier factors for gonadal tumor development ininhibin-deficient mice. Endocrinology 137:4210–4216.
Liu J, Yang Z, Thomson JA, Auersperg N, Mills GB, Hahn WC,Bast Jr RC (2002): Malignant transformation of humanovarian surface epithelial cells through genetic modifications.Proc Am Assn Cancer Res 43:72•.ž Q10
Maines-Bandiera SL, Kruk PA, Auersperg N (1992): Simianvirus 40-transformed human ovarian surface epithelial cellsescape normal growth controls but retain morphogeneticresponses to extracellular matrix. Am J Obstet Gynecol167:729–735.
Masiakos PT, MacLaughlin DT, Maheswaran S, Teixeira J, Ful-ler AF Jr, Shah PC, Kehas DJ, Kenneally MK, DombkowskiDM, Ha TU, Preffer FI, Donahoe PK (1999): Human ovariancancer, cell lines, and primary ascites cells express the humanMullerian inhibiting substance (MIS) type II receptor, bind,and are responsive to MIS. Clin Cancer Res 5:3488–3499.
Matei D, Graeber TG, Baldwin RL, Karlan BY, Rao J, ChangDD (2002): Gene expression in epithelial ovarian carcinoma.Oncogene 21:6289–6298.
Matzuk MM, Finegold MJ, Su JG, Hsueh AJ, Bradley A (1992):Alpha-inhibin is a tumour-suppressor gene with gonadalspecificity in mice. Nature 360:313–319.
Matzuk MM, Kumar TR, Shou W, Coerver KA, Lau AL, Beh-ringer RR, Finegold MJ (1996): Transgenic models to studythe roles of inhibins and activins in reproduction, oncogenesis,and development. Recent Prog Horm Res 51:123–154;discussion 155–127.
McLaren A (2000): Germ and somatic cell lineages in thedeveloping gonad. Mol Cell Endocrinol 163:3–9.
Miki Y, Swensen J, Shattuck-Eidens D, Futreal PA, Harsh-man K, Tavtigian S, Liu Q, Cochran C, Bennett LM•, Dingž Q11W, et al. (1994): A strong candidate for the breast and ovariancancer susceptibility gene BRCA1. Science 266:66–71.
Mok SC, Chao J, Skates S, Wong K, Yiu GK, Muto MG,Berkowitz RS, Cramer DW (2001): Prostasin, a potentialserum marker for ovarian cancer: Identification throughmicroarray technology. J Natl Cancer Inst 93:1458–1464.
Naora H, Montz FJ, Chai CY, Roden RB (2001): Aberrantexpression of homeobox gene HOXA7 is associated withmullerian-like differentiation of epithelial ovarian tumors andthe generation of a specific autologous antibody response.Proc Natl Acad Sci USA 98:15209–15214.
Nicosia SV, Johnson JH, Streibel EJ (1984): Isolation and ultra-structure of rabbit ovarian mesothelium (surface epithelium).Int J Gynecol Pathol 3:348–360.
Nicosia SV, Narconis RJ, Saunders BO (1989): Regulation andtemporal sequence of surface epithelium morphogenesis in thepostovulatory rabbit ovary. Prog Clin Biol Res 296:111–119.
Nilson JH, Abbud RA, Keri RA, Quirk CC (2000): Chronichypersecretion of luteinizing hormone in transgenic micedisrupts both ovarian and pituitary function, with some effectsmodified by the genetic background. Recent Prog Horm Res55:69–89; discussion 89–91.
Obata K, Morland SJ, Watson RH, Hitchcock A, Chenevix-Trench G, Thomas EJ, Campbell IG (1998): Frequent PTEN/MMAC mutations in endometrioid but not serous or mucinousepithelial ovarian tumors. Cancer Res 58:2095–2097.
Ono K, Tanaka T, Tsunoda T, Kitahara O, Kihara C, Oka-moto A, Ochiai K, Takagi T, Nakamura Y (2000): Identifi-cation by cDNA microarray of genes involved in ovariancarcinogenesis. Cancer Res 60:5007–5011.
Orsulic S (2002): An RCAS-TVA-based approach to designermouse models. Mamm Genome 13:543–547.
Orsulic S, Li Y, Soslow RA, Vitale-Cross LA, Gutkind JS,Varmus HE (2002): Induction of ovarian cancer by definedmultiple genetic changes in a mouse model system. CancerCell 1:53–62.
Pejovic T, Heim S, Mandahl N, Baldetorp B, Elmfors B, Flo-derus UM, Furgyik S, Helm G, Himmelmann A, Willen H,et al. (1992): Chromosome aberrations in 35 primary ovariancarcinomas. Genes Chromosom Cancer 4:58–68•. ž Q12
Perez RP, Godwin AK, Hamilton TC, Ozols RF (1991): Ovar-ian cancer biology. Semin Oncol 18:186–204.
Peschon JJ, Behringer RR, Cate RL, Harwood KA, Idzerda RL,Brinster RL, Palmiter RD (1992): Directed expression of anoncogene to Sertoli cells in transgenic mice using mullerianinhibiting substance regulatory sequences. Mol Endocrinol6:1403–1411.
Petricoin EF, Ardekani AM, Hitt BA, Levine PJ, Fusaro VA,Steinberg SM, Mills GB, Simone C, Fishman DA, Kohn EC,Liotta LA (2002): Use of proteomic patterns in serum toidentify ovarian cancer. Lancet 359:572–577.
Pierce JG, Parsons TF (1981): Glycoprotein hormones: Struc-ture and function. Annu Rev Biochem 50:465–495.
Pieretti M, Cavalieri C, Conway PS, Gallion HH, Powell DE,Turker MS (1995): Genetic alterations distinguish differenttypes of ovarian tumors. Int J Cancer 64:434–440.
Purdie DM, Bain CJ, Siskind V, Webb PM, Green AC (2003):Ovulation and risk of epithelial ovarian cancer. Int J Cancer104:228–232.
Randall TC, Bell KA, Rebane BA, Rubin SC, Boyd J (1998):Germline mutations of the BRCA1 and BRCA2 genes in abreast and ovarian cancer patient. Gynecol Oncol 70:432–434.
Risma KA, Clay CM, Nett TM, Wagner T, Yun J, Nilson JH(1995): Targeted overexpression of luteinizing hormonein transgenic mice leads to infertility, polycystic ovaries,and ovarian tumors. Proc Natl Acad Sci USA 92: 1322–1326.
Roby KF, Taylor CC, Sweetwood JP, Cheng Y, Pace JL, Taw-fik O, Persons DL, Smith PG, Terranova PF (2000): Devel-opment of a syngeneic mouse model for events related toovarian cancer. Carcinogenesis 21:585–591.

REFERENCES 187
Sawiris GP, Sherman-Baust CA, Becker KG, Cheadle C, Teich-berg D, Morin PJ (2002): Development of a highlyspecialized cDNA array for the study and diagnosis of epithe-lial ovarian cancer. Cancer Res 62:2923–2928.
Schummer M, Ng WV, Bumgarner RE, Nelson PS, Schum-mer B, Bednarski DW, Hassell L, Baldwin RL, Karlan BY,Hood L (1999): Comparative hybridization of an array of21,500 ovarian cDNAs for the discovery of genes overex-pressed in ovarian carcinomas. Gene 238:375–385.
Schwartz DR, Kardia SL, Shedden KA, Kuick R, Michaili-dis G, Taylor JM, Misek DE, Wu R, Zhai Y, Darrah DM,Reed H, Ellenson LH, Giordano TJ, Fearon ER, Hanash SM,Cho KR (2002): Gene expression in ovarian cancer reflectsboth morphology and biological behavior, distinguishing clearcell from other poor-prognosis ovarian carcinomas. CancerRes 62:4722–4729.
Schwartz PE (2002): Current diagnosis and treatment modalitiesfor ovarian cancer. Cancer Treat Res 107:99–118.
Schwartz PE, Chambers JT, Taylor KJ (1995): Early detectionand screening for ovarian cancer. J Cell Biochem Suppl23:233–237.
Schwartz PE, Taylor KJ (1995): Is early detection of ovariancancer possible? Ann Med 27:519–528.
Scully R, Livingston DM (2000): In search of the tumour-suppressor functions of BRCA1 and BRCA2. Nature 408:429–432.
Scully RE (1977): Ovarian tumors. A review. Am J Pathol87:686–720.
Segev DL, Ha TU, Tran TT, Kenneally M, Harkin P, Jung M,MacLaughlin DT, Donahoe PK, Maheswaran S (2000): Mul-lerian inhibiting substance inhibits breast cancer cell growththrough an NFkappa B-mediated pathway. J Biol Chem275:28371–28379.
Shridhar V, Lee J, Pandita A, Iturria S, Avula R, Staub J, Mor-rissey M, Calhoun E, Sen A, Kalli K, Keeney G, Roche P,Cliby W, Lu K, Schmandt R, Mills GB, Bast RC, Jr., JamesCD, Couch FJ, Hartmann LC, Lillie J, Smith DI (2001):Genetic analysis of early-versus late-stage ovarian tumors.Cancer Res 61:5895–5904.
Stephen AE, Masiakos PT, Segev DL, Vacanti JP, Donahoe PK,MacLaughlin DT (2001): Tissue-engineered cells producingcomplex recombinant proteins inhibit ovarian cancer in vivo.Proc Natl Acad Sci USA 98:3214–3219.
Takahashi M, Hayashi M, Manganaro TF, Donahoe PK (1986):The ontogeny of mullerian inhibiting substance in granulosacells of the bovine ovarian follicle. Biol Reprod 35:447–453.
Tapper J, Kettunen E, El-Rifai W, Seppala M, Andersson LC,Knuutila S (2001): Changes in gene expression duringprogression of ovarian carcinoma. Cancer Genet Cytogenet128:1–6.
Tennent BJ, Beamer WG (1986): Ovarian tumors not inducedby irradiation and gonadotropins in hypogonadal (hpg) mice.Biol Reprod 34:751–760.
Testa JR, Getts LA, Salazar H, Liu Z, Handel LM, Godwin AK,Hamilton TC (1994): Spontaneous transformation of rat
ovarian surface epithelial cells results in well to poorlydifferentiated tumors with a parallel range of cytogeneticcomplexity. Cancer Res 54:2778–2784.
Tonin PN, Hudson TJ, Rodier F, Bossolasco M, Lee PD, Nov-ak J, Manderson EN, Provencher D, Mes-Masson AM (2001):Microarray analysis of gene expression mirrors the biology ofan ovarian cancer model. Oncogene 20:6617–6626.
Wang K, Gan L, Jeffery E, Gayle M, Gown AM, Skelly M,Nelson PS, Ng WV, Schummer M, Hood L, Mulligan J(1999): Monitoring gene expression profile changes in ovariancarcinomas using cDNA microarray. Gene 229:101–108.
Welsh JB, Zarrinkar PP, Sapinoso LM, Kern SG, Behling CA,Monk BJ, Lockhart DJ, Burger RA, Hampton GM (2001):Analysis of gene expression profiles in normal and neoplasticovarian tissue samples identifies candidate molecular markersof epithelial ovarian cancer. Proc Natl Acad Sci USA98:1176–1181.
Werness BA, Parvatiyar P, Ramus SJ, Whittemore AS, Garling-house-Jones K, Oakley-Girvan I, DiCioccio RA, Wiest J,Tsukada Y, Ponder BA, Piver MS (2000): Ovarian carci-noma in situ with germline BRCA1 mutation and loss ofheterozygosity at BRCA1 and TP53. J Natl Cancer Inst92:1088–1091.
Whang-Peng J, Knutsen T, Douglass EC, Chu E, Ozols RF,Hogan WM, Young RC (1984): Cytogenetic studies in ovar-ian cancer. Cancer Genet Cytogenet 11:91–106.
Wooster R, Bignell G, Lancaster J, Swift S, Seal S, Mangion J,Collins N, Gregory S, Gumbs C, Micklem G (1995): Identifi-cation of the breast cancer susceptibility gene BRCA2. Nature378:789–792.
Wu R, Zhai Y, Fearon ER, Cho KR (2001): Diverse mecha-nisms of beta-catenin deregulation in ovarian endometrioidadenocarcinomas. Cancer Res 61:8247–8255.
Xu X, Qiao W, Linke SP, Cao L, Li WM, Furth PA, Harris CC,Deng CX (2001): Genetic interactions between tumor sup-pressors Brca1 and p53 in apoptosis, cell cycle and tumori-genesis. Nat Genet 28:266–271.
Zhai Y, Wu R, Schwartz DR, Darrah D, Reed H, Kolligs FT,Nieman MT, Fearon ER, Cho KR (2002): Role of beta-catenin/T-cell factor-regulated genes in ovarian endometrioidadenocarcinomas. Am J Pathol 160:1229–1238.
Zhang L, Yang N, Garcia JR, Mohamed A, Benencia F, RubinSC, Allman D, Coukos G (2002): Generation of a syngeneicmouse model to study the effects of vascular endothe-lial growth factor in ovarian carcinoma. Am J Pathol161:2295–2309.
Zweemer RP, Shaw PA, Verheijen RM, Ryan A, Berchuck A,Ponder BA, Risch H, McLaughlin JR, Narod SA, Menko FH,Kenemans P, Jacobs IJ (1999a): Accumulation of p53 proteinis frequent in ovarian cancers associated with BRCA1 andBRCA2 germline mutations. J Clin Pathol 52:372–375.
Zweemer RP, Verheijen RH, Menko FH, Gille JJ, van Diest PJ,Coebergh JW, Shaw PA, Jacobs IJ, Kenemans P (1999b):Differences between hereditary and sporadic ovarian cancer.Eur J Obstet Gynecol Reprod Biol 82:151–153.