Embed Size (px)
Citation preview

I authorize _______________________
x_
_______(Name of person or facility which has information - example: UCSF/Mt. Zion)
to release health information to:___UCSF Medical Center: Cancer Center_____
Name of person or facility to receive healthinformation (full address)
_______________________________________Street address:
_______________________________________City, State, Zip Code
_______________________________________
Please specify the health information you authorize to be released:
Type(s) of health information: __________________________________________
Date(s) of treatment: _________________________________________________
The following information will not be released unless you specificallyauthorize it by marking the relevant box(es) below:
� Information pertaining to drug and alcohol abuse, diagnosis or treatment (42C.F.R. §§2.34 and 2.35).
� Information pertaining to mental health diagnosis or treatment (Welfare andInstitutions Code §§5328, et seq.)
� Release of HIV/AIDS test results (Health and Safety Code §120980(g)).
� Release of genetic testing information (Health and Safety Code §124980(j)).
EXPIRATION OF AUTHORIZATIONUnless otherwise revoked, this Authorization expires ____________(insertapplicable date or event). If no date is indicated, the Authorization willexpire 12 months after the date of my signing this form.
Print Name Signature (Patient, Parent, Guardian)
Date Time Relationship to Patient (Parent,Guardian, Conservator, PatientRepresentative)
Requested format: � Paper � CD
DATE:
PATIENT NAME:
BIRTHDATE:
ID VERIFICATION (TYPE):
ID VERIFIED BY:
AUTHORIZATION FOR RELEASEOF HEALTH INFORMATION
AUTHORIZATION FOR RELEASEOF HEALTH INFORMATION
756-0
20Z
(R
ev.
02/1
2)
Work
flow
One
ME
DIC
AL R
EC
OR
D C
OP
Y
The purpose of this release isfor (check one or more):
� Continuity of care ordischarge planning
� Billing and payment of bill
� At the request of the patient/patient representative
� Other (state reason)_______
_________________________
_________________________
(1)
(2)
(3)
(4)

NOTICEUCSF and many other organizations and individuals such as physicians,hospitals and health plans are required by law to keep your healthinformation confidential. If you have authorized the disclosure of yourhealth information to someone who is not legally required to keep itconfidential, it may no longer be protected by state or federalconfidentiality laws.
YOUR RIGHTSThis Authorization to release health information is voluntary. Treatment,payment, enrollment or eligibility for benefits may not be conditioned onsigning this Authorization except in the following cases: (1) to conductresearch-related treatment, (2) to obtain information in connection witheligibility or enrollment in a health plan, (3) to determine an entity’sobligation to pay a claim, or (4) to create health information to provide toa third party.
This Authorization may be revoked at any time. The revocation must be inwriting, signed by you or your patient representative, and delivered to:Health Information Management Services, UCSF Medical Center, 400Parnassus Ave., Room A68, San Francisco, CA 94143-0308. Therevocation will take effect when UCSF receives it, except to the extentUCSF or others have already relied on it.
You are entitled to receive a copy of this Authorization.

Patient Intake Form
Answers to the following questions will be helpful in managing your medical problems. Please feel free to provide additional details or discuss the answer to any of these questions with your treating physician.
Patient N arne ----------------------------------Age ________________ __
The best phone number we should use to reach you: ________________________________ _
PRIMARY CARE PHYSICIAN
Name: ________________________________________________________ __
Phone No., including area code: __________________________ __
Please list any prior medical problems:
Please list prior surgeries with approximate dates:
Please describe any prior treatment with radiation:
Please describe any prior Chemo/Hormonal Therapy treatment:
Do you have any allergies to any medications? If so, please list here.

D f il h . oes anyone In your am 1y ave cancer· or ano th "fi d" I er s1gn1 Icant me Ica pro bl ? em. Age Medical Problem Cause of death if deceased
Father: Mother: Siblings:
Grandparents
Other:
Social History: Do you/did you use tobacco? If you quit, then when? __ _
Cigarettes: packs per day ____ _ How many years did you smoke? ___ _ Other tobacco: describe type/use
Do you/did you drink alcohol? If you quit, then when? ___ _ Average number of drinks per week ____ _
Do you/did you use recreational drugs? -----Describe type and use
Birthplace _________ _ Occupation ______ _
Relationship/marital status _____ _ Name of spouse/significant other ______ _
Any other concerns or anything you want your doctor to know about you?
Do you currently have or have you had any of the following illnesses/complaints? Yes No Details
General Weight change Fatigue Weakness Fevers/chills/night sweats Hot Flashes Pain Enlarged lymph nodes Skin Sores/ulcers Respiratory Shortness of breath/trouble breathing Asthma/bronchitis/ emphysema Coughing up blood Cardiac/vascular Hypertension/high blood pressure

Heart murmur Chest pain/ angina Heart attack Swelling/edema in feet/ankles/hands Gastrointestinal Nausea/vomiting Black/bloody stool Abdominal pain Hepatitis/liver disorder Diarrhea Constipation Incontinence of stool Renal/Genitourinary Kidney disease
Yes No Details Blood in urine Bladder infection Sexually transmitted disease Incontinence of urine Hematologic Anemia/transfusions Blood clots Musculoskeletal Weakness Arthritis Neurologic Headache Seizures Visual changes Hearing problems/changes
· Memory changes Dizziness/vertigo Numbness/tingling Stroke Psychiatric Depression Other
;
Cancer Immune disorder Lupus/other autoimmune disorder Other (please describe) Other (please describe)
For women only: How many times have you been pregnant? __ How many children do you have? __ _
Age at first child birth? ___ _
Age at first menstrual period? ____ _ Age at menopause? ____ _

Are you using/ did you use hormone replacement therapy? __ _
Are you sexually active? -------
Are you using birth control? -----Which type? ___ _
Could you be pregnant?------------

........................................................................... ---------------------------, : I.,...._ H 1 D"ll r::: •1 : Patient Name : ~ een 1 er.---am1 y 1 ----------
~ Comprehensive 1 Date of Birth : Cancer Center : : L--------------------------~Prescription Medications, Over-the-Counter Medications, and Supplements . . ~Please ensure that everything you list here is also accounted for in the medical history section.
ll :I :I !I :I ll :I
Name of Medication or Supplement
I I I I I I I
Form Dosage Strength per (tablet, chewable Tablet or Liquid tablet, elixir, etc) Concentration
I I I I I I I
Amount of Medication per Dose
II II II II II II II
Frequency
\I II II II !I I I II
,. :========~
...._______.!! ~Your Pharmacy :Pharmacy Name
:Pharmacy Address
:city State ZIP
~ Pharmacy Phone
:ucSF Cancer Center Patient Health Questionnaire, revised 08/04/13

UCSF and Mount Zion Comprehensive Cancer Center
Department of Radiation Oncology
"Next Provider of Care" Information
Please answer the following questions so that we may provide a list of your current medications to your next provider of care:
1. When is your next appointment with a physician other than your Radiation
Oncologist? Date:-----------------------
2. Please provide the following information for the physician with whom you have your next appointment: Name: --------------------------Address: -------------------------City, State, ZIP: -------------------Telephone Number: ------------------Fax Number: ----------------------Medical Specialty:------------------
3. Please provide the following information for your Primary Care Physician: Name: --------------------------Address: ------------------------City,State,ZIP: __________________ __
Telephone Number:------------------Fax Number: ----------------------Medical Specialty:------------------
4. Please provide the following information for the physician who referred you to the Department of Radiation Oncology at UCSF: Name: -------------------------Address: ______________________ ___
City, State, ZIP:------------------Telephone Number:-----------------Fax Number: -----------------------Medical Specialty:------------------
Do you give the Department of Radiation Oncology at UCSF permission to provide a copy of your Medication Reconciliation List to the physicians listed above? Yes No ----
Signature:-------------------- Date: ________ _

>a_ 0 0 w 0 i= 0 <( a: a_
I
~ g .....J w >-
>a_ 0 0 0 a: 0 0 w a: .....J
UNIT NUMBER
lJCsF Medical Center PT. NAME
BIRTH DATE
OUTPATIENT PAIN SCREENING RECORD LOCATION DATE
Have you experienced any pain within the past week? No 0 Yes 0
( If "No," stop here and give this to your provider. If "Yes," please answer the rest of the questions)
Where is your pain?
Circle a number from 0-10 that best describes how much pain you are having now.
0 1 2 3 4 5 6 7 8 9 10 No Pain Worst Pain Possible
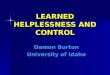
For a child or non-English speaking adult, use Wong-Baker FACES Pain Rating Scale© or FLACC Pain Scale.
Ask the patient to circle the score that best describes how he/she feels:
Categories
FACE
LEGS
ACTIVITY
CRY
CONSOLABILITY
0 1-2 3-4 5-6 7-8 No Hurt Hurts Little Bit Hurts Little More Hurts Even More Hurts Whole Lot
FLACC PAIN SCALE
0
No particular expression or smile.
Normal position or relaxed.
Lying quietly, normal position, moves easily .
No cry (awake or asleep).
Content, relaxed.
Scoring
1
Occasional grimace or frown, withdrawn, disinterested.
Uneasy, restless, tense.
Squirming, shifting back and forth, tense.
Moans or whimpers; occasional complaint.
Reassured by occasional touching, hugging, or being talked to - distractible.
9-10 Hurts Worst
2
Frequent to constant quivering chin; clenched jaw.
Kicking, or legs drawn up.
Arched, rigid or jerking.
Crying steadily, screams or sobs - frequent complaints.
Difficulty to console or comfort.
<3 What does your pain feel like? Circle response: sharp dull burning aching throbbing tender numb 0 w ~ stabbing gnawing shooting exhausting penetrating miserable unbearable continuous occasional <( z <3 a: 0 Ql What makes the pain better? _______________________________ _ 0 ~ What makes the pain worse? ______________________________ _ 0 ~ Are you currently taking medication(s) or using some type of treatment for pain relief? m NoD Yes D ~ o If yes, list medication and/or treatment: ___________________________ ~ ~ [£ U") !'-
~ PatientorCareg~erSignature ______________________ ~Date t'-
t'- ~------------------------------------------------------------------------------------~ "'wong, DL: Whaley and Wong·s Nursing Care of Infants and Children, 6th ed.
St. Louis, MO Mosby 1999. used with permission OUTPATIENT PAIN SCREENING RECORD

The NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) are a statement of evidence and consensus of the authors regarding their views of currently accepted approaches to treatment. Any clinician seeking to apply or consult the NCCN Guidelines® is expected to use independent medical judgment in the context of individual clinical circumstances to determine any patient’s care or treatment. The National Comprehensive Cancer Network® (NCCN®) makes no representations or warranties of any kind regarding their content, use, or application, and disclaims any responsibility for their application or use in any way. The NCCN Guidelines are copyrighted by National Comprehensive Cancer Network®. All rights reserved. The NCCN Guidelines and the illustrations herein may not be reproduced in any form without the express written permission of NCCN. ©2013.
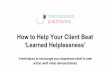
Instructions: First please circle the number (0-10) that bestdescribes how much distress you have been experiencing inthe past week including today.
YES NO YES NOPractical Problems
Family Problems
Emotional Problems
Spiritual/religiousconcerns
Physical ProblemsChild careHousingInsurance/financialTransportationWork/schoolTreatment decisions
Dealing with childrenDealing with partnerAbility to have childrenFamily health issues
DepressionFearsNervousnessSadnessWorryLoss of interest inusual activities
AppearanceBathing/dressingBreathingChanges in urinationConstipationDiarrheaEatingFatigueFeeling SwollenFeversGetting aroundIndigestionMemory/concentrationMouth soresNauseaNose dry/congestedPain
s/feet
SexualSkin dry/itchySleepSubstance abuseTingling in hand
Second, please indicate if any of the following has been aproblem for you in the past week including today. Be sure tocheck YES or NO for each.
Other Problems: _________________________________________
________________________________________________________
SCREENING TOOLS FOR MEASURING DISTRESS
Extreme distress
No distress
10
9
8
7
6
5
4
3
2
1
0
10
9
8
7
6
5
4
3
2
1
0
NCCN Distress Thermometer for Patients
Help for distress
Distress is an unpleasant emotional state that may affect how you feel, think, and act. It can include feelings of unease, sadness, worry, anger, helplessness, guilt, and so forth. Everyone with cancer has some distress at some point of time. It is normal to feel sad, fearful, and helpless.
Feeling distressed may be a minor problem or it may be more serious. You may be so distressed that you can’t do the things you used to do. Serious or not, it is important that your treatment team knows how you feel.
The Distress Thermometer is a tool that you can use to talk to your doctors about your distress. It has a scale on which you circle your level of distress. It also asks about the parts of life in which you are having problems. The Distress Thermometer has been tested in many studies and found to work well. Please complete the Distress Thermometer and share it with your treatment team at your next visit.
The Distress Thermometer helps your treatment team know if you need supportive services. You may be referred to supportive services at your cancer center or in your community. Supportive services can include help from support groups, chaplains, social workers, counselors, and many other experts. Supportive services can also be found through the support services at right.
Support Services
National Cancer Institute’s Cancer Information ServiceTelephone 1-800-4-CANCERWebsite www.cancer.gov/aboutnci/cis/page1
Cancer Support CommunityTelephone 1- 888-793-9355Website www.cancersupportcommunity.org/MainMenu/Cancer-Support
U.S. Health Resources and Services AdministrationWebsite www.findahealthcenter.hrsa.gov/Search_HCC.aspx
U.S. Substance Abuse and Mental Health Services AdministrationWebsite www.findtreatment.samhsa.gov

The NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) are a statement of evidence and consensus of the authors regarding their views of currently accepted approaches to treatment. Any clinician seeking to apply or consult the NCCN Guidelines® is expected to use independent medical judgment in the context of individual clinical circumstances to determine any patient’s care or treatment. The National Comprehensive Cancer Network® (NCCN®) makes no representations or warranties of any kind regarding their content, use, or application, and disclaims any responsibility for their application or use in any way. The NCCN Guidelines are copyrighted by National Comprehensive Cancer Network®. All rights reserved. The NCCN Guidelines and the illustrations herein may not be reproduced in any form without the express written permission of NCCN. ©2013.
Instructions: First please circle the number (0-10) that bestdescribes how much distress you have been experiencing inthe past week including today.
YES NO YES NOPractical Problems
Family Problems
Emotional Problems
Spiritual/religiousconcerns
Physical ProblemsChild careHousingInsurance/financialTransportationWork/schoolTreatment decisions
Dealing with childrenDealing with partnerAbility to have childrenFamily health issues
DepressionFearsNervousnessSadnessWorryLoss of interest inusual activities
AppearanceBathing/dressingBreathingChanges in urinationConstipationDiarrheaEatingFatigueFeeling SwollenFeversGetting aroundIndigestionMemory/concentrationMouth soresNauseaNose dry/congestedPain
s/feet
SexualSkin dry/itchySleepSubstance abuseTingling in hand
Second, please indicate if any of the following has been aproblem for you in the past week including today. Be sure tocheck YES or NO for each.
Other Problems: _________________________________________
________________________________________________________
SCREENING TOOLS FOR MEASURING DISTRESS
Extreme distress
No distress
10
9
8
7
6
5
4
3
2
1
0
10
9
8
7
6
5
4
3
2
1
0
NCCN Distress Thermometer for Patients
The NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) are a statement of evidence and consensus of the authors regarding their views of currently accepted approaches to treatment. Any clinician seeking to apply or consult the NCCN Guidelines® is expected to use independent medical judgment in the context of individual clinical circumstances to determine any patient’s care or treatment. The National Comprehensive Cancer Network® (NCCN®) makes no representations or warranties of any kind regarding their content, use, or application, and disclaims any responsibility for their application or use in any way. The NCCN Guidelines are copyrighted by National Comprehensive Cancer Network®. All rights reserved. The NCCN Guidelines and the illustrations herein may not be reproduced in any form without the express written permission of NCCN. ©2013.
Instructions: First please circle the number (0-10) that bestdescribes how much distress you have been experiencing inthe past week including today.
YES NO YES NOPractical Problems
Family Problems
Emotional Problems
Spiritual/religiousconcerns
Physical ProblemsChild careHousingInsurance/financialTransportationWork/schoolTreatment decisions
Dealing with childrenDealing with partnerAbility to have childrenFamily health issues
DepressionFearsNervousnessSadnessWorryLoss of interest inusual activities
AppearanceBathing/dressingBreathingChanges in urinationConstipationDiarrheaEatingFatigueFeeling SwollenFeversGetting aroundIndigestionMemory/concentrationMouth soresNauseaNose dry/congestedPain
s/feet
SexualSkin dry/itchySleepSubstance abuseTingling in hand
Second, please indicate if any of the following has been aproblem for you in the past week including today. Be sure tocheck YES or NO for each.
Other Problems: _________________________________________
________________________________________________________
SCREENING TOOLS FOR MEASURING DISTRESS
Extreme distress
No distress
10
9
8
7
6
5
4
3
2
1
0
10
9
8
7
6
5
4
3
2
1
0
NCCN Distress Thermometer for Patients

w >
~ z w (j)
lJCsF Medical Center
UCSF Benioff Children's Hospital
NOTICE OF PRIVACY PRACTICE ACKNOWLEDGEMENT OF RECEIPT
UNIT NUMBER
PT. NAME
BIRTHDATE
LOCATION DATE
The UCSF Notice of Privacy Practice provides information about how we may use and disclose protected health information about you.
In addition to the copy we have provided you, copies of the current notice are available by accessing our website at http://www.ucsfhealth.org and may be obtained throughout UCSF Health System.
I acknowledge that I have received the Notice of Privacy Practice.
__ ! ! __ Signature of Patient or Patient's Representative Date
Print Name Relationship to Patient
~ Name of Interpreter (if applicable) w 0: (j)
Fz w
~ If written acknowledgement is not obtained, please check reason: 0: 0 1-z ~ D Notice of Privacy Practice Given - Patient Unable to Sign c... I
~ D Notice of Privacy Practice Given - Patient Declined to Sign _J
w >-
0 0: 0 (..)
DOther ________________________________________ __
~ ........••............•..•.............••..............•................................................••.••.............•••...... _J <( (..)
15 w ~ I
w I-
~ Signature of UCSF Representative
> Q)
~ 0
~ cb ,.....
Print Name
__ ! ! __ Date
Department
00 ~----------------------------------------------------------------------·--~ NOTICE OF PRIVACY PRACTICE ACKNOWLEDGEMENT OF RECEIPT

'-··
>"-0 ()
f-z UJ
l.JCSF Medical Center
TERMS AND CONDITIONS OF SERVICE: ADMISSION, MEDICAL SERVICES AND FINANCIAL AGREEMENT
UNIT NUMBER
PT. NAME
BIRTHDATE
LOCATION DATE
1. UCSF Medical Center is part of the University of California and is comprised of its hospital(s), medical center(s), its hospital-based clinics, and the UCSF School of Medicine.
2. MEDICAL CONSENT: I consent to medical treatments or procedures X-ray examinations, drawing blood for tests, medications, injections, taking of medical photographs, videotaping, laboratory procedures, and hospital services rendered to me under the general and special instructions of the physicians or other health care professionals assisting in my care. I also consent to my admission to the UCSF Medical Center if this is necessary for my care.
3. TEACHING, RESEARCH AND HEALTHCARE INSTITUTION: The University of California including UCSF Medical Center, is a teaching, research and healthcare institution. I understand that residents, interns, medical students, students of ancillary health care professions (e.g., nursing, x-ray, rehabilitation therapy), post-graduate fellows, and other trainees may observe, examine, treat, and participate at the request and under the supervision of the attending physician in my care as part of the University's medical education programs. Some UCSF Medical Center faculty are identified by their name badge as "Visiting Professors". These faculty members do not have a California license, but are licensed in another state or country. These physicians are permitted to practice medicine in California under a special program developed by the Medical Board of California.
I also understand that a University institutional review board approves projects conducted by University researchers in accordance with state and federal law. As a result, I understand that I may be contacted and asked to participate in research studies but I am under no obligation to do so. My decision whether to participate or not will not affect my ability to obtain medical care.
4. USE OF MEDICAL INFORMATION AND SPECIMENS: I understand that my medical information, photographs, and/or video in any form may be used for other UCSF Medical Center purposes, such as quality improvement, patient safety and education. I also understand that my medical information and tissue, fluids, cells and other specimens (collectively, "Specimens") that UCSF Medical Center may collect during the course of my treatment and care may be used and shared with researchers. I understand that under California law, I do not have any rights to any commercially useful products that may be developed from such research. I further understand that any use of my medical information or Specimens by UCSF Medical Center or other research institutions will be in accor-dance with state and federal law, including all laws and regulations governing patient confidentiality, in the manner outlined in the UCSF Medic~ Center Notice of Privacy Practices.
t
\.._~ 5. PERSONAL VALUABLES: UCSF Medical Center maintains fireproof safes for the safekeeping of money and
valuables. UCSF Medical Center shall not be liable for the loss of or damage to any money, documents, jewelry, glasses, dentures, furs or other articles of unusual value and shall not be liable for loss or damage to any personal property, unless deposited in a safe or locked storeroom. The liability for loss of any personal property deposited
$: g _J
UJ >-
>"-0 ()
0 a: 0 () UJ a: _J
<! ()
i5 UJ ::;; _J
<! z C3 0: 0
with UCSF Medical Center shall be no more than $500.
6. RELEASE OF MEDICAL INFORMATION: The State of California Information Practices Act requires UCSF Medical Center to provide the following information to individuals who supply information about themselves. As a patient of UCSF Medical Center, I will be asked to submit certain personal information, such as my address and phone number, Social Security number, insurance information, medical history and treatment. The principal purpose for requesting this information is to ensure accurate identification, continuity of medical care, and payment for such care. Under the authority of The Federal Privacy Act of 1974, Article IX, Section 9 of the California Constitution, the California Information Practices Act (Civil Code 1798 et seq.), California Code of Regulations, Title 22, Section 70749, UCSF Medical Center is authorized to maintain this information. As required by UCSF Medical Center, furnishing all information requested is mandatory unless otherwise noted. I understand that failure to provide such
., information may affect my medical care and/or insurance benefits and coverage. c: 0 ~ UCSF Medical Center will obtain my written authorization to release information about my medical treatment, J except in those circumstances when UCSF Medical Center is permitted or required by law to release information ;::- (see UCSF Medical Center's Notice of Privacy Practices for a description of the specific circumstances under which
·\....,_ ~ UCSF Medical Center may release this information). For example, UCSF Medical Center may release a copy of 0
~ my patient record to health care providers, health plans, governmental agencies and workers' compensation carri-[S ers. Additionally, I understand that if I am diagnosed with cancer, a reportable disease in California, UCSF Medical ~ Center is required by law to report my diagnosis to the State Department of Health Services.
~ ~-----------------------------------------------------------------------------------Page 1 of 2 TERMS AND CONDITIONS OF SERVICE: ADMISSION,
MEDICAL SERVICES AND FINANCIAL AGREEMENT

>-0.. 0 ()
1-z w
'-· ~ 0..
~ 0 --' --' w >-
>-0.. 0 ()
0 a: 0 () w a: --' <( ()
Ci w ::;; _:. <( z (3 ii' 0 Q)
" 0 ;: 0
~ ~
·"-· ,:::-Q <D 0
:> <I> ~ m ,._ "' :1: ,._ <D
lJQ;f: Medical Center
TERMS AND CONDITIONS OF SERVICE: ADMISSION, MEDICAL SERVICES AND FINANCIAL AGREEMENT
UNIT NUMBER
PT. NAME
BIRTHDATE
LOCATION DATE
7. FINANCIAL AGREEMENT: I understand that even if I have insurance, I may be financially responsible for some or all of my medical services. For instance, if I have a co-pay or deductible, I agree to pay the amounts I owe. If I do not have insurance that covers the service I receive, I agree to pay The Regents of the University of California for professional, hospital and clinic services, including UCSF Medical Center physician services, in accordance with the regular rates and terms of UCSF Medical Center. I also agree to pay for other professional services provided at UCSF Medical Center by other health care providers. If I am unable to pay, I understand I may qualify for public assistance, special payment arrangements and/or charity care. I also understand that when this agreement is signed by my spouse, parent or a financial guarantor, my spouse, parent or financial guarantor shall be jointly and individually liable with me for payment, including all collection fees (attorneys' fees, costs and collection expenses), in addition to any other amounts due. Unpaid accounts referred to outside agencies for collection bear interest at the current legal rate.
8. ASSIGNMENT OF BENEFITS (INCLUDING MEDICARE BENEFITS): I authorize and direct payment to UCSF Medical Center of any insurance benefits including hospital insurance and unemployment compensation disability benefits otherwise payable to or on my behalf for UCSF Medical Center services, including emergency services, at a rate not to exceed UCSF Medical Center actual charges. I understand that I am financially responsible for charges not paid pursuant to this agreement. I further agree that any credit balance resulting from payment of insurance or other sources may be applied to any other account owed to UCSF Medical Center by me.
I have read, agreed to and received a copy of this Terms and Conditions of Service.
Signature of Patient or Signature of Patient Representative
Signature of Witness (required if patient unable to sign) Relationship of Representative to Patient
Signature of Interpreter Language used i.
Date of Signing
Financial Responsibility Agreement by Person Other than the Patient or the Patient's Legal Representative I agree to accept financial responsibility for services rendered to the patient and to accept the terms of the Financial Agreement (Paragraph 7) and Assignment Of Benefits (Including Medicare Benefits) (Paragraph 8) set forth above.
Date Financially Responsible Party Witness
Elective Section:
PATIENT RIGHTS NOTICE: (applies to inpatient admissions only) Would you like your agent under a durable power of attorney for health care or your next of kin to receive a copy of the Patient Rights and Responsibilities Notice? If so, please contact the Patient Relations Department at (415) 353-1936.
Page 2 of 2 TERMS AND CONDITIONS OF SERVICE: ADMISSION, MEDICAL SERVICES AND FINANCIAL AGREEMENT