Embed Size (px)
Citation preview
V BERAXIOMEDICAL I N C O R P O R A T E D
1
Verax BiomedicalPlatelet PGD® Test
V BERAXIOMEDICAL I N C O R P O R A T E D
2
Verax Biomedical Platelet PGD® Test
• Results in approximately 30 minutes
• Designed for use with LR or non-LR: RDPs, Pooled RDPs & SDPs
• 2 to 3 minutes attended labor per test
• Analytical sensitivity ~ 103 – 104 CFU/mL
• 510(k) lots produced, prepared to enter clinical trials

V BERAXIOMEDICAL I N C O R P O R A T E D
3
Medical Advisory Board
James AuBuchon, M.D.Dartmouth-Hitchcock Medical Center
Leslie Silberstein, M.D.Harvard School of Medicine
Ira Shulman, M.D.University of Southern California
Roslyn Yomtovian, M.D.Case Western Reserve University
Mark Brecher, M.D.University of North Carolina
V BERAXIOMEDICAL I N C O R P O R A T E D
4
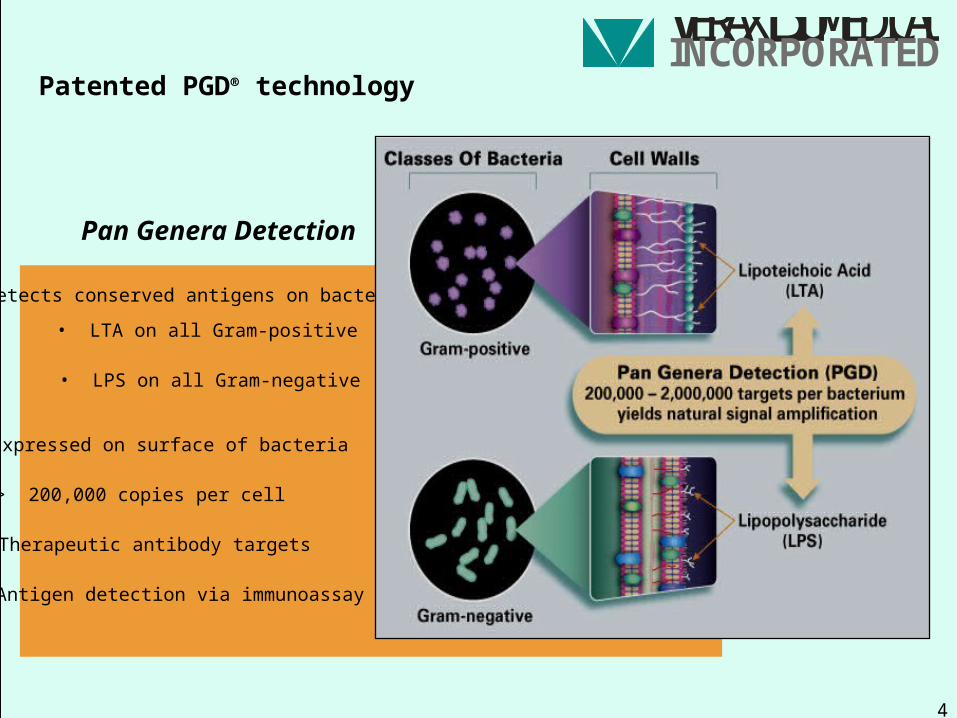
Patented PGD® technology
Detects conserved antigens on bacteria
Expressed on surface of bacteria
> 200,000 copies per cell
Therapeutic antibody targets
Antigen detection via immunoassay
• LPS on all Gram-negative
• LTA on all Gram-positive
Pan Genera Detection
V BERAXIOMEDICAL I N C O R P O R A T E D
5
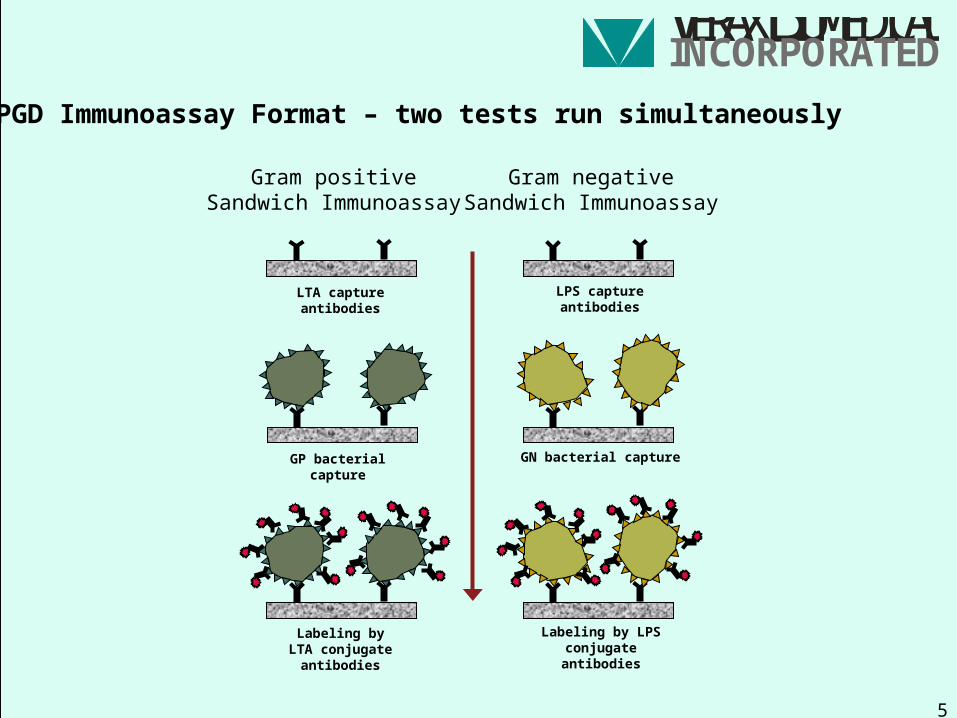
Labeling by LTA conjugateantibodies
Gram positiveSandwich Immunoassay
LTA captureantibodies
GP bacterial capture
Labeling by LPSconjugateantibodies
Gram negativeSandwich Immunoassay
LPS captureantibodies
GN bacterial capture
PGD Immunoassay Format – two tests run simultaneously
V BERAXIOMEDICAL I N C O R P O R A T E D
6
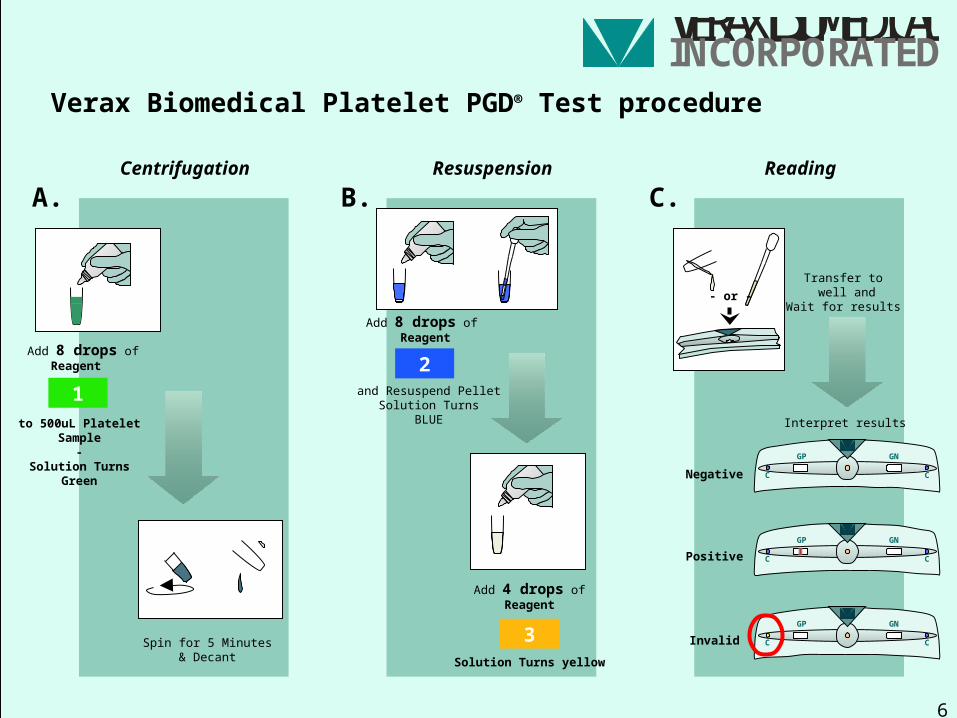
1
Add 8 drops ofReagent
to 500uL Platelet Sample
-Solution Turns
Green
A.
Spin for 5 Minutes& Decant
Verax Biomedical Platelet PGD® Test procedure
Add 8 drops of Reagent
2
B. C.
Add 4 drops ofReagent
Solution Turns yellow
3
GP GN
CC
GP GN
CC
GP GN
CC
Transfer to well and
Wait for results
Negative
Positive
Invalid
Interpret results
Centrifugation Resuspension Reading
- or -
and Resuspend PelletSolution Turns
BLUE
V BERAXIOMEDICAL I N C O R P O R A T E D
7
Unused test cartridge
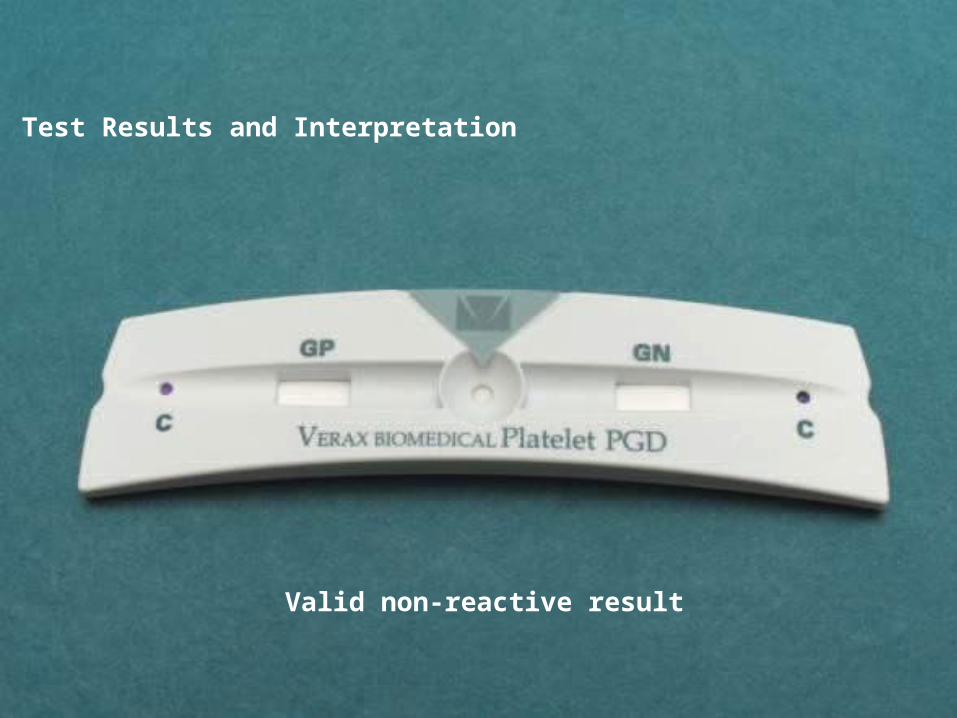
Test Results and Interpretation
V BERAXIOMEDICAL I N C O R P O R A T E D
8
Valid non-reactive result
Test Results and Interpretation
V BERAXIOMEDICAL I N C O R P O R A T E D
9
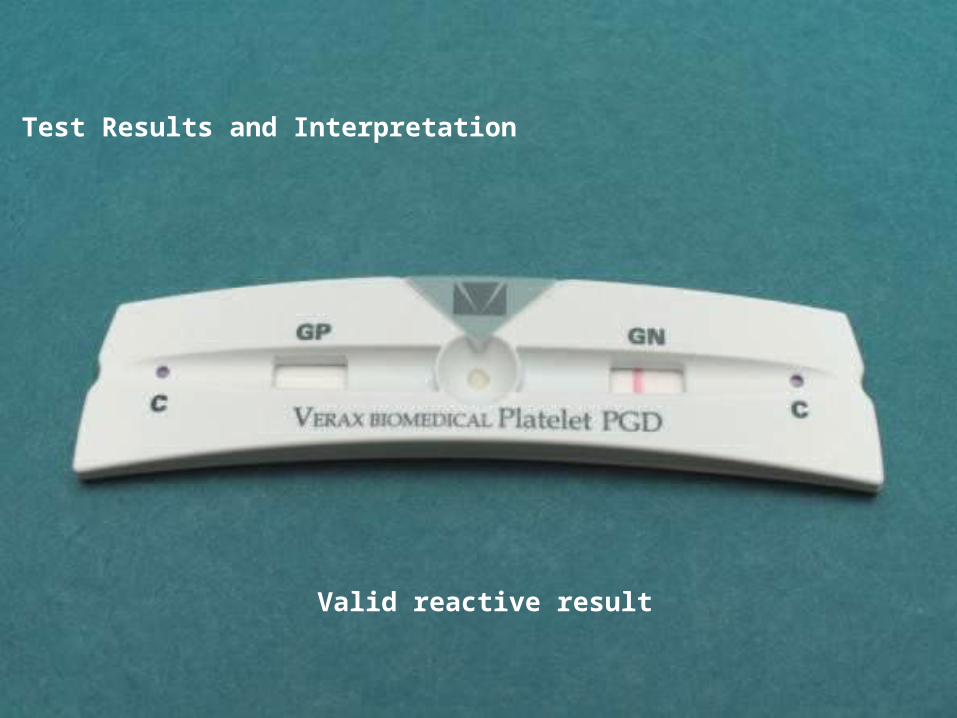
Valid reactive result
Test Results and Interpretation
V BERAXIOMEDICAL I N C O R P O R A T E D
10
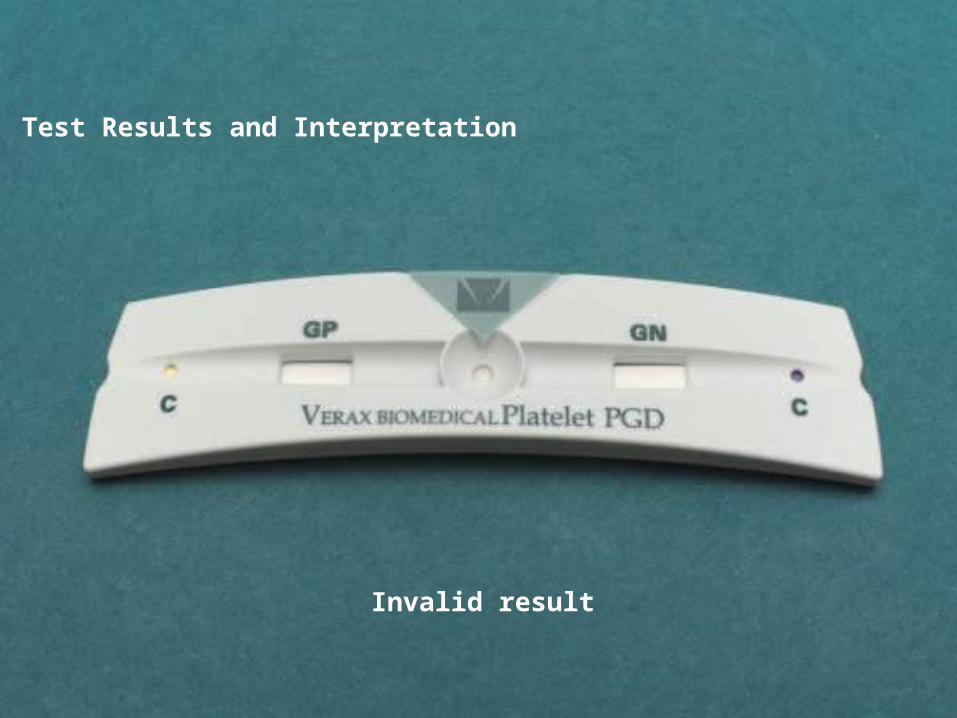
Invalid result
Test Results and Interpretation
V BERAXIOMEDICAL I N C O R P O R A T E D
11
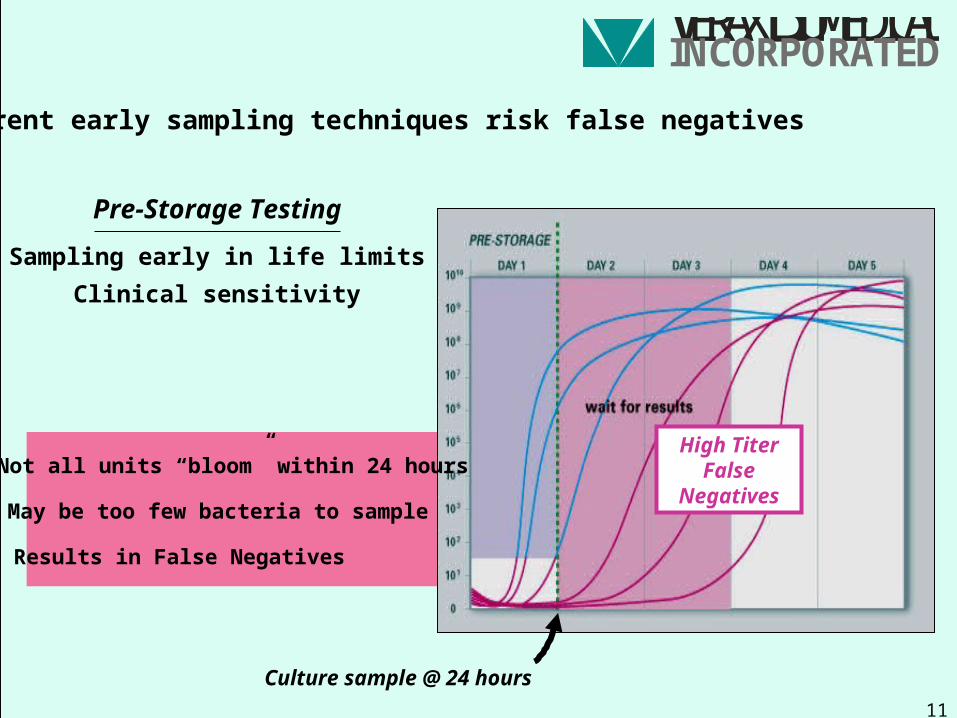
May be too few bacteria to sample
Results in False Negatives
Clinical sensitivity
Sampling early in life limits
Pre-Storage Testing
Not all units “bloom” within 24 hours
Culture sample @ 24 hours
High TiterFalse
Negatives
Current early sampling techniques risk false negatives
V BERAXIOMEDICAL I N C O R P O R A T E D
12
Breakthrough cases – False Negatives associated with current testing
Reported by CDC at January 2005 DHHS Blood Safety & Availability Meeting:
• FATALITY - Culture false negative
• FATALITY - Culture false negative
• FATALITY - pH false negative 74 year old patient with leukemia receiving a routine platelet transfusion. Received a 5 unitirradiated platelet pool tested normal by pH (>6.4). Pool contaminated with Staph aureus. Patient died after a 21 day hospital stay.
79 year old coronary-artery bypass patient transfused apheresis unit that tested negativefor bacteria by BacT Alert on a 24 hour sample. Unit contaminated with Staphylococcus lugdunensis. Patient died 27 hours later. Original BacT culture still negative after 10 days.
Premature newborn received two doses from an apheresis platelet unit. Unit tested negativeby 24 hour sample plate culture and normal pH (7.3). Unit contaminated with Serratia marcescens. Child died 27 hours later. Second culture on original sample also negative.
V BERAXIOMEDICAL I N C O R P O R A T E D
13
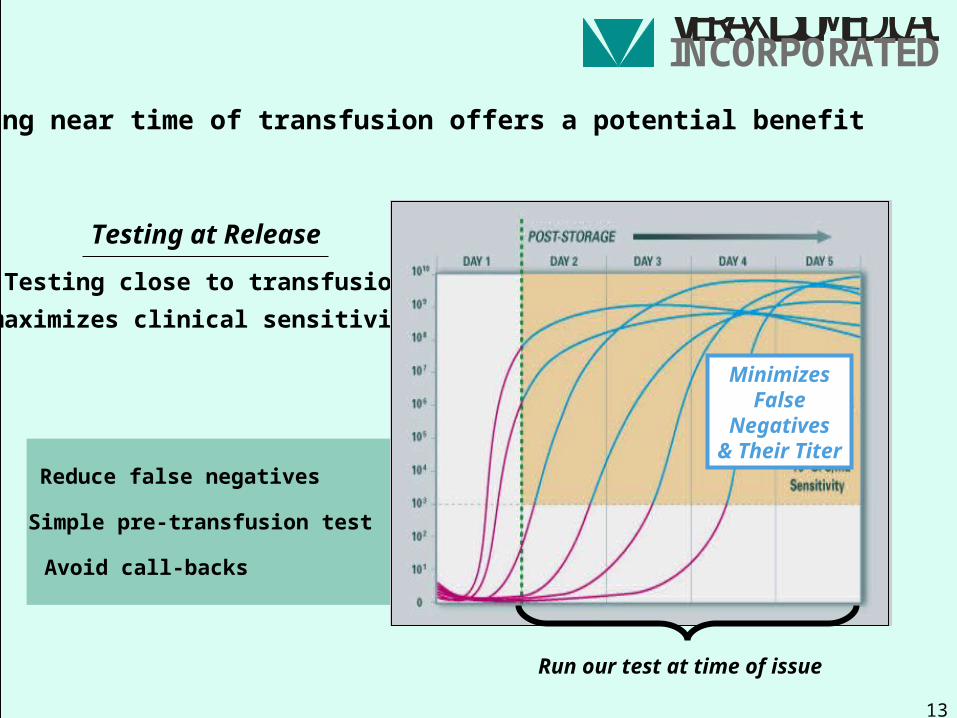
Testing near time of transfusion offers a potential benefit
maximizes clinical sensitivity
Testing close to transfusion
Testing at Release
Simple pre-transfusion test
Avoid call-backs
Reduce false negatives
Run our test at time of issue
MinimizesFalse
Negatives& Their Titer
V BERAXIOMEDICAL I N C O R P O R A T E D
14
This approach is the one most likely to demonstrate equivalence for QC purposes:
Considerations for the establishment of a regulatory pathway for rapid tests for bacterial contamination….
- Allows for the differing analytical sensitivities of the two methods
Kinetic studies for QC claim equivalence
- Allows for the widely differing time of sampling for culture methods and rapid tests intended to be used near the time of release
V BERAXIOMEDICAL I N C O R P O R A T E D
15
We must be careful in establishing a priori analytical sensitivity targets now for tests intended for use near the time of transfusion:
Considerations for the establishment of a regulatory pathway for rapid tests for bacterial contamination….
- Time of testing is likely to be a more significant driver of clinical performancethan analytical sensitivity
- The more important question is: how many contaminated units do we avoid transfusing? – best answered with populations studies
Analytical sensitivity targets
V BERAXIOMEDICAL I N C O R P O R A T E D
16
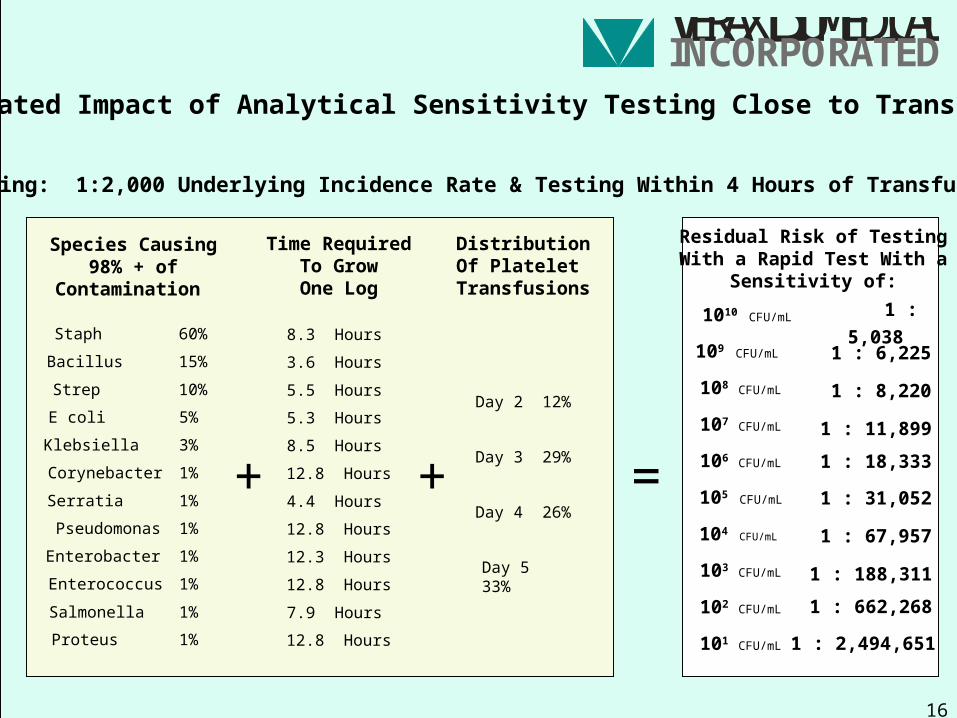
Residual Risk of Testing With a Rapid Test With a
Sensitivity of:
Species Causing98% + of
Contamination
Staph
Bacillus
Strep
E coli
Klebsiella
Salmonella
Pseudomonas
Serratia
Enterobacter
Enterococcus
Corynebacter
Proteus
60%
15%
10%
5%
3%
1%
1%
1%
1%
1%
1%
1%
+
Time RequiredTo GrowOne Log
8.3 Hours
3.6 Hours
5.5 Hours
5.3 Hours
8.5 Hours
7.9 Hours
12.8 Hours
4.4 Hours
12.3 Hours
12.8 Hours
12.8 Hours
12.8 Hours
+
DistributionOf Platelet
Transfusions
Day 2 12%
Day 3 29%
Day 4 26%
Day 5 33%
=
Assuming: 1:2,000 Underlying Incidence Rate & Testing Within 4 Hours of Transfusion
Calculated Impact of Analytical Sensitivity Testing Close to Transfusion
1 : 6,225
1 : 8,220
1 : 11,899
1 : 18,333
1 : 31,052
1 : 67,957
1 : 188,311
1 : 662,268
1 : 2,494,651
1 : 5,038
109 CFU/mL
108 CFU/mL
107 CFU/mL
106 CFU/mL
105 CFU/mL
104 CFU/mL
103 CFU/mL
102 CFU/mL
101 CFU/mL
1010 CFU/mL
V BERAXIOMEDICAL I N C O R P O R A T E D
17
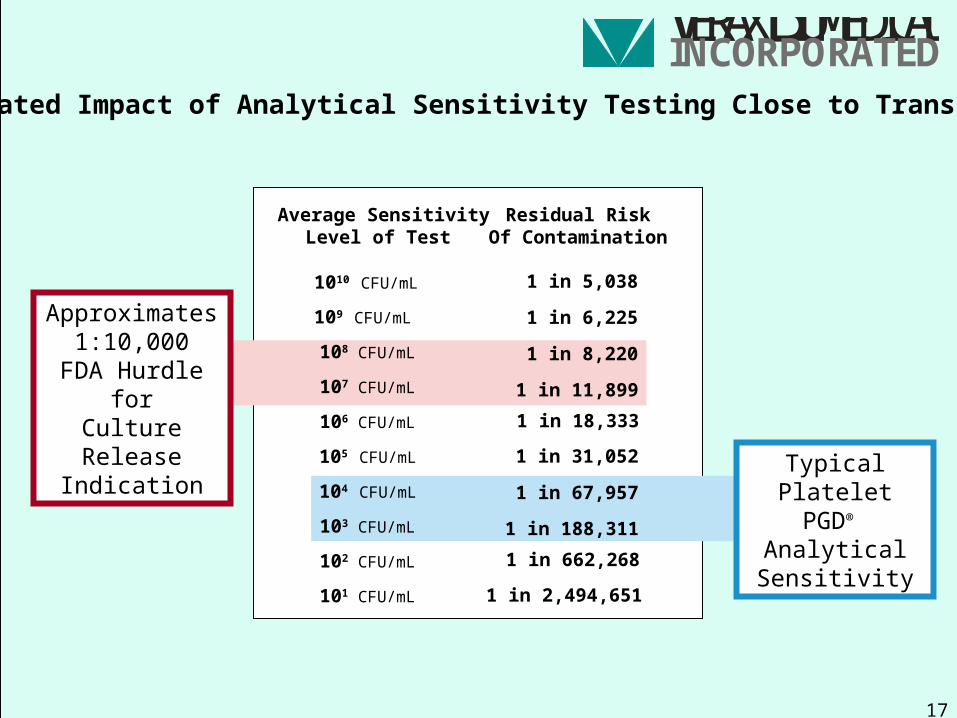
Calculated Impact of Analytical Sensitivity Testing Close to Transfusion
Approximates1:10,000
FDA Hurdle forCulture Release
Indication
Residual RiskOf Contamination
1 in 6,225
1 in 8,220
1 in 11,899 1 in 18,333
1 in 31,052
1 in 67,957
1 in 188,311 1 in 662,268
1 in 2,494,651
1 in 5,038
Average SensitivityLevel of Test
109 CFU/mL
108 CFU/mL
107 CFU/mL
106 CFU/mL
105 CFU/mL
104 CFU/mL
103 CFU/mL
102 CFU/mL
101 CFU/mL
1010 CFU/mL
TypicalPlatelet PGD®
Analytical Sensitivity
V BERAXIOMEDICAL I N C O R P O R A T E D
18
Given the need for tests with release indications, we are concerned that FDA’s proposal may not be the least burdensome route to a release test:
Considerations for the establishment of a regulatory pathway for rapid tests for bacterial contamination….
- a 450,000 unit post market surveillance data set, plus
- an additional 100,000 unit post market study comparing with culture @ outdate (how is this possible when units have been transfused?)
Three tiers of data required fora release test indication
- a post market study of unknown size testing culture positives, plus
- the requirement for a QC equivalence claim, plus
V BERAXIOMEDICAL I N C O R P O R A T E D
19
For example:
Considerations for the establishment of a regulatory pathway for rapid tests for bacterial contamination….
- this pathway would likely delay a release indication by 3 to 4 years
Three tiers of data required fora release test indication
- this pathway would take longer to answer the question of the actual clinical sensitivity of the method than simply performing a classic virus screening trial
- the 3 post market data sets would appear to gather overlapping data
- some data (culture confirmation at outdate for rapid test-negatives) could not be obtained as the platelets would have been transfused
V BERAXIOMEDICAL I N C O R P O R A T E D
20
We recommend that FDA consider a streamlined, two-step regulatory strategy for a release claim:
- Step 1: 510(k) for Quality Control
- Step 2: Screening for release (well-controlled, structured trial comparing to culture at time of transfusion on 50,000 to 100,000 units)
Three tiers of data required fora release test indication
Considerations for the establishment of a regulatory pathway for rapid tests for bacterial contamination….
- Supplemented by ongoing post market surveillance of observed incidence data from end-users