Embed Size (px)
Citation preview
1
Validation of Bone Allograft Processing:
Reducing Risk of Disease Transmission via Conventional Agents While Maintaining Graft Performance
Validation of Bone Allograft Processing:
Reducing Risk of Disease Transmission via Conventional Agents While Maintaining Graft Performance
TSE Advisory Committee Meeting
June 26, 2002
Gaithersburg, MD
TSE Advisory Committee Meeting
June 26, 2002
Gaithersburg, MD
Richard Russo
Osteotech, Inc.
2
Validation of Bone Allograft ProcessingValidation of Bone Allograft Processing
Risk reduction is a multi-functional process, built on several factors:
Donor testing and screening Donor deferral and tissue discard policies Appropriate segregation and quarantine procedures Adequate cleaning and disinfection between batches Processing to inactivate and/or remove pathogens
Risk reduction is a multi-functional process, built on several factors:
Donor testing and screening Donor deferral and tissue discard policies Appropriate segregation and quarantine procedures Adequate cleaning and disinfection between batches Processing to inactivate and/or remove pathogens
3
Validation of Bone Allograft ProcessingValidation of Bone Allograft Processing
Potential pathogens in tissue: Bacteria, yeasts, mold and fungi Viruses TSE
Presentation focus: Viruses in standard non-demineralized grafts
Principal viruses of concern: HIV 1 + 2, HTLV 1+2, HBV, HCV
Potential pathogens in tissue: Bacteria, yeasts, mold and fungi Viruses TSE
Presentation focus: Viruses in standard non-demineralized grafts
Principal viruses of concern: HIV 1 + 2, HTLV 1+2, HBV, HCV
4
Validation of Bone Allograft ProcessingValidation of Bone Allograft Processing
Performance
Primary purpose of bone graft is to support bone formation across a defect due to disease, trauma, or reconstructive surgery
Not all processing has same effect on bone graft performance
Failure of graft procedure typically leads to revision surgery
Limitation of capacity of graft to support bone formation leads to increased morbidity and risk to patient
Performance
Primary purpose of bone graft is to support bone formation across a defect due to disease, trauma, or reconstructive surgery
Not all processing has same effect on bone graft performance
Failure of graft procedure typically leads to revision surgery
Limitation of capacity of graft to support bone formation leads to increased morbidity and risk to patient
5
Validation of Bone Allograft Processing:Treatments Affecting Performance
Validation of Bone Allograft Processing:Treatments Affecting Performance
Preprocessing Storage Temperature Multiple Freeze-Thaw Cycles Sterilization Procedures
UV Radiation Gamma E-beam Ethylene Oxide
Solvents (GnHC1, Acid-Alcohol, EDTA) Sonication (> 20,000 cycles/sec.) Peracetic Acid Hydrogen Peroxide
Concentration and time dependent Strong base, e.g, NaOH
Reviewed by Russell & Block, Orthopedics Vol. 22 (5); 524, 1999
Preprocessing Storage Temperature Multiple Freeze-Thaw Cycles Sterilization Procedures
UV Radiation Gamma E-beam Ethylene Oxide
Solvents (GnHC1, Acid-Alcohol, EDTA) Sonication (> 20,000 cycles/sec.) Peracetic Acid Hydrogen Peroxide
Concentration and time dependent Strong base, e.g, NaOH
Reviewed by Russell & Block, Orthopedics Vol. 22 (5); 524, 1999
6
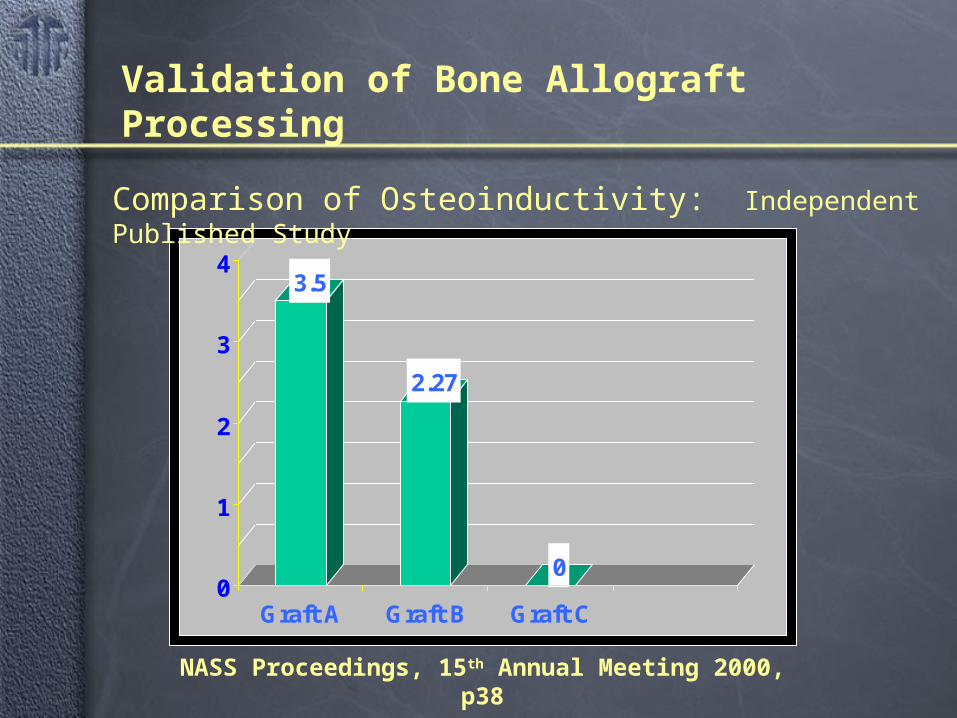
3.5
2.27
00
1
2
3
4
Graft A Graft B Graft C
NASS Proceedings, 15th Annual Meeting 2000, p38
Validation of Bone Allograft Processing
Comparison of Osteoinductivity: Independent Published Study
7
Validation of Bone Allograft ProcessingValidation of Bone Allograft Processing
Risk reduction via processing begins with characterization of tissues and assessment of risk
Each type of tissue presents its own profile
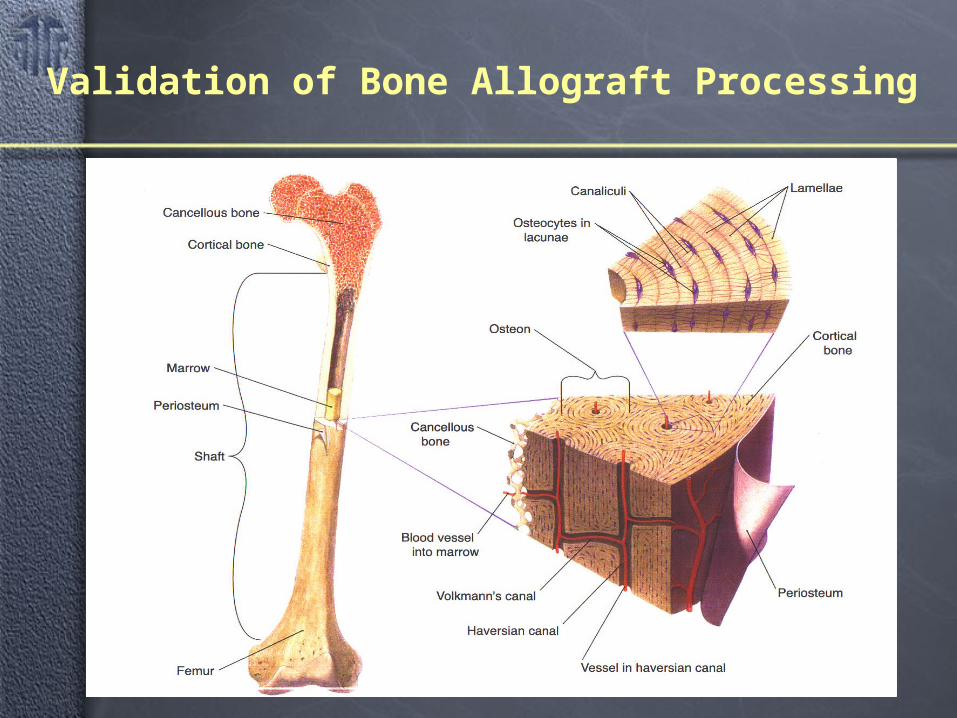
Musculoskeletal tissues can be characterized as soft or hard
Soft: ligaments, tendons, fascia, cartilage Hard: bone
• Cancellous• Cortical
Risk reduction via processing begins with characterization of tissues and assessment of risk
Each type of tissue presents its own profile
Musculoskeletal tissues can be characterized as soft or hard
Soft: ligaments, tendons, fascia, cartilage Hard: bone
• Cancellous• Cortical
8
Validation of Bone Allograft ProcessingValidation of Bone Allograft Processing
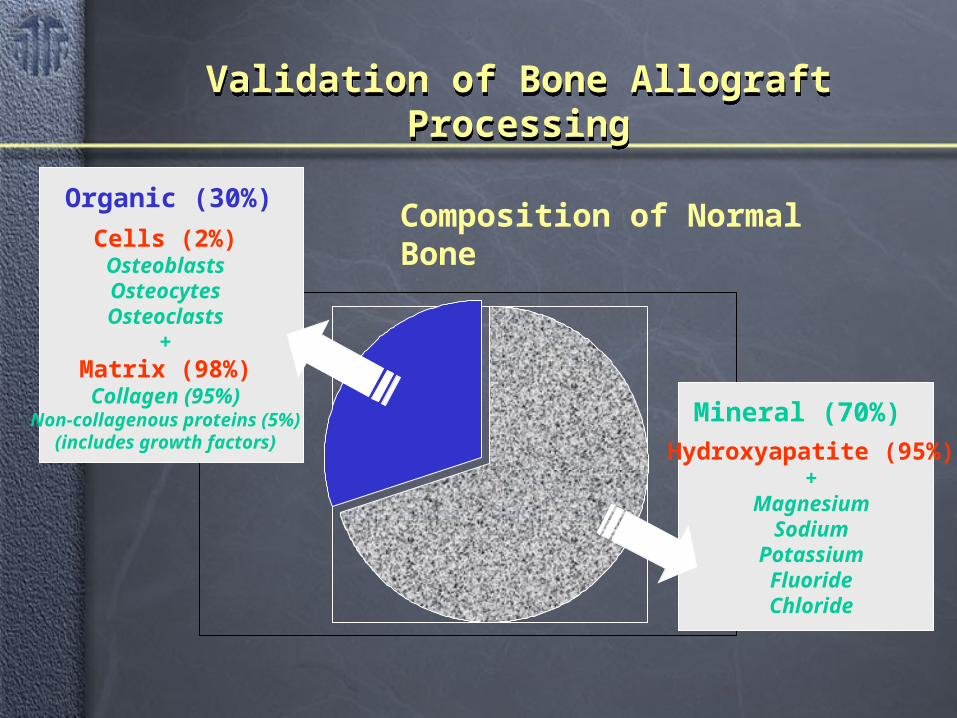
In terms of mass, bone tissue can be described as having two phases:
Inorganic
Organic
In terms of mass, bone tissue can be described as having two phases:
Inorganic
Organic
9
Validation of Bone Allograft ProcessingValidation of Bone Allograft Processing
Mineral (70%)
Hydroxyapatite (95%)+
MagnesiumSodium
PotassiumFluorideChloride
Organic (30%)
Cells (2%)OsteoblastsOsteocytesOsteoclasts
+Matrix (98%)Collagen (95%)
Non-collagenous proteins (5%)(includes growth factors)
Composition of Normal Bone
10
Validation of Bone Allograft Processing
11
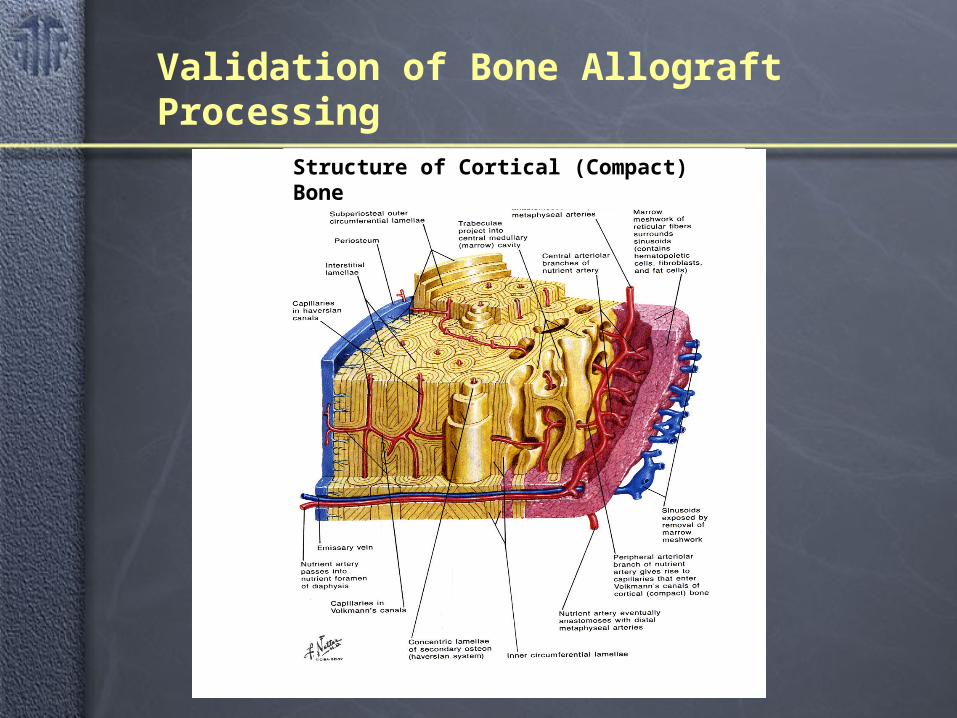
Validation of Bone Allograft Processing
Structure of Cortical (Compact) Bone
12
13
Validation of Bone Allograft ProcessingValidation of Bone Allograft Processing
No published reports that quantitative viral burden in bone
Extrapolate viral burden from values reported for blood: data exist for HIV, HTLV, HBV, and HCV
Bone is divided into discrete compartments
Conservative bone allografts “dose” 90cc mineralized tissue
Calculation of blood volumes
Calculation of theoretical maximum viral burden
No published reports that quantitative viral burden in bone
Extrapolate viral burden from values reported for blood: data exist for HIV, HTLV, HBV, and HCV
Bone is divided into discrete compartments
Conservative bone allografts “dose” 90cc mineralized tissue
Calculation of blood volumes
Calculation of theoretical maximum viral burden
Maximum Viral Burden in Bone: General Considerations
14
Validation of Bone Allograft ProcessingValidation of Bone Allograft Processing
Spike bone with known amount of virus
Relevant panel
Demonstrate quantitative recovery
Proceed through process step
Quantitatively assay viral inactivation
Calculate difference between theoretical maximum viral burden and log reduction value of process
Viral clearance must be at least 3 logs greater than maximum viral burden to provide acceptable level of safety
Spike bone with known amount of virus
Relevant panel
Demonstrate quantitative recovery
Proceed through process step
Quantitatively assay viral inactivation
Calculate difference between theoretical maximum viral burden and log reduction value of process
Viral clearance must be at least 3 logs greater than maximum viral burden to provide acceptable level of safety
Viral Clearance Process Validation: General Approach
15
Validation of Bone Allograft ProcessingValidation of Bone Allograft Processing
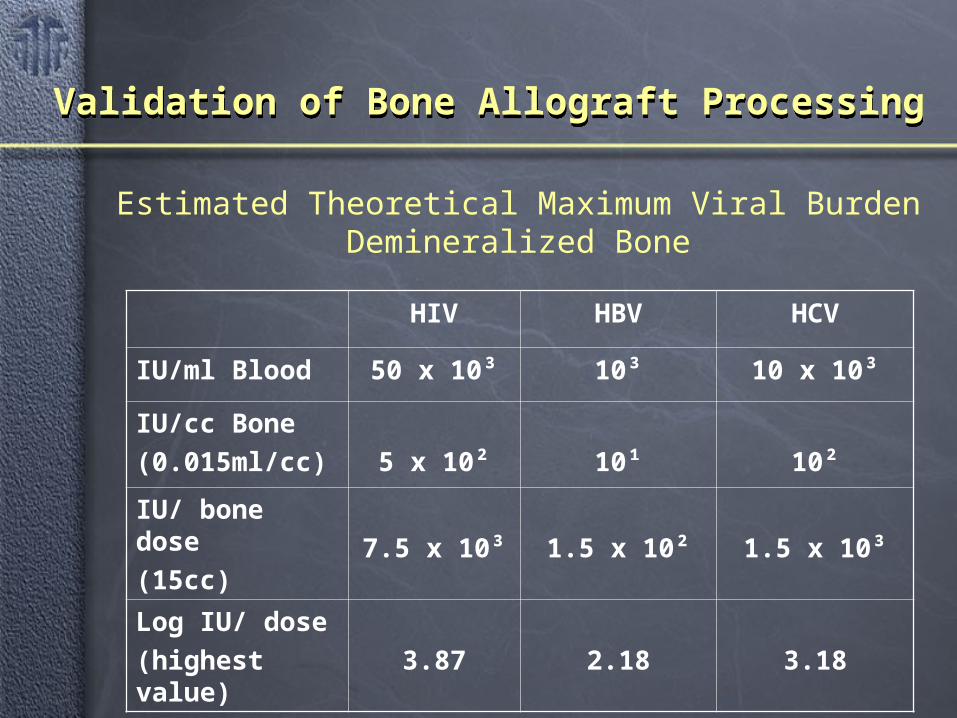
HIV HBV HCV
IU/ml Blood 50 x 10³ 10³ 10 x 10³
IU/cc Bone
(0.015ml/cc) 5 x 10² 10¹ 10²
IU/ bone dose
(15cc) 7.5 x 10³ 1.5 x 10² 1.5 x 10³
Log IU/ dose
(highest value) 3.87 2.18 3.18
Estimated Theoretical Maximum Viral BurdenDemineralized Bone
16
Validation of Bone Allograft ProcessingValidation of Bone Allograft Processing
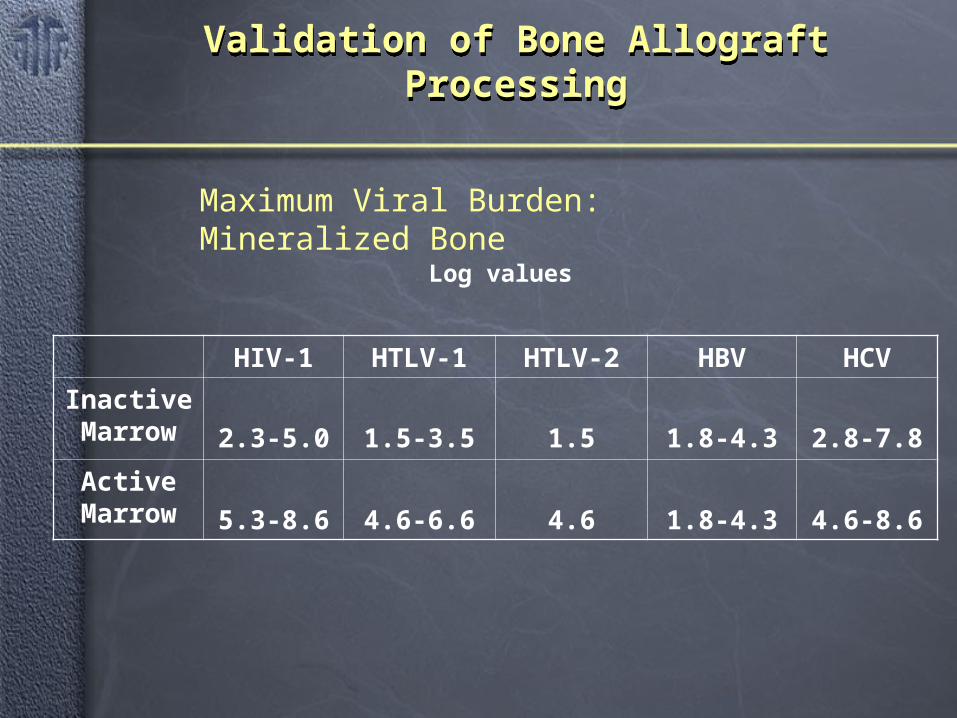
HIV-1 HTLV-1 HTLV-2 HBV HCV
Inactive Marrow 2.3-5.0 1.5-3.5 1.5 1.8-4.3 2.8-7.8
Active Marrow 5.3-8.6 4.6-6.6 4.6 1.8-4.3 4.6-8.6
Log values
Maximum Viral Burden: Mineralized Bone
17
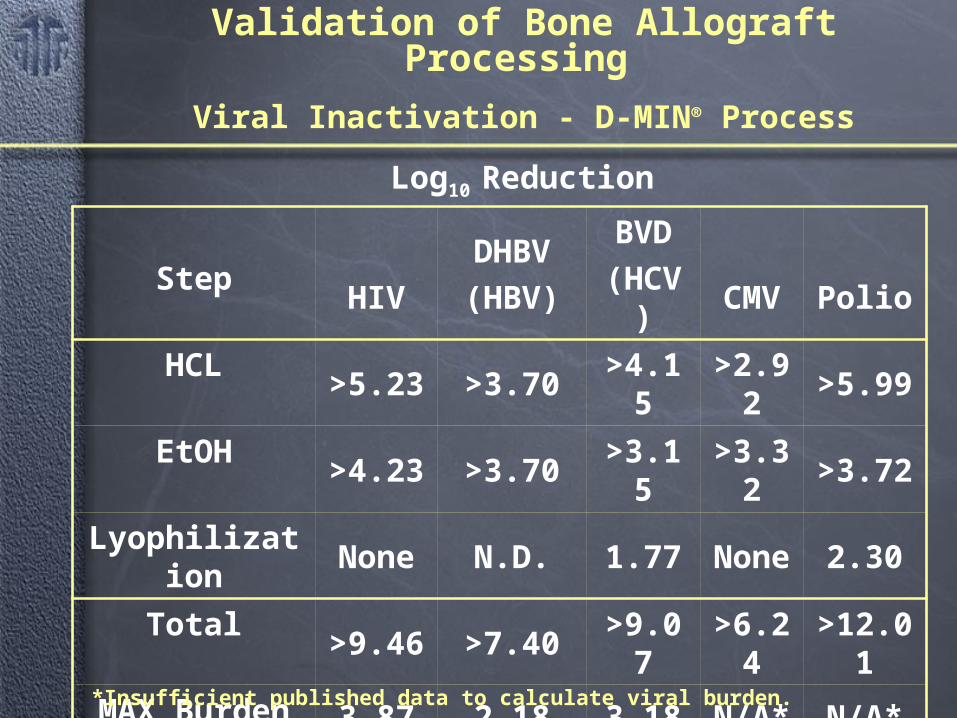
Validation of Bone Allograft Processing
Viral Inactivation - D-MIN® Process
Step HIV
DHBV
(HBV)
BVD
(HCV) CMV Polio
HCL >5.23 >3.70 >4.15 >2.92 >5.99
EtOH >4.23 >3.70 >3.15 >3.32 >3.72
Lyophilization None N.D. 1.77 None 2.30
Total >9.46 >7.40 >9.07 >6.24 >12.01
MAX Burden 3.87 2.18 3.18 N/A* N/A*
Safety Factor 5.59 5.22 5.89
Log10 Reduction
*Insufficient published data to calculate viral burden.
18
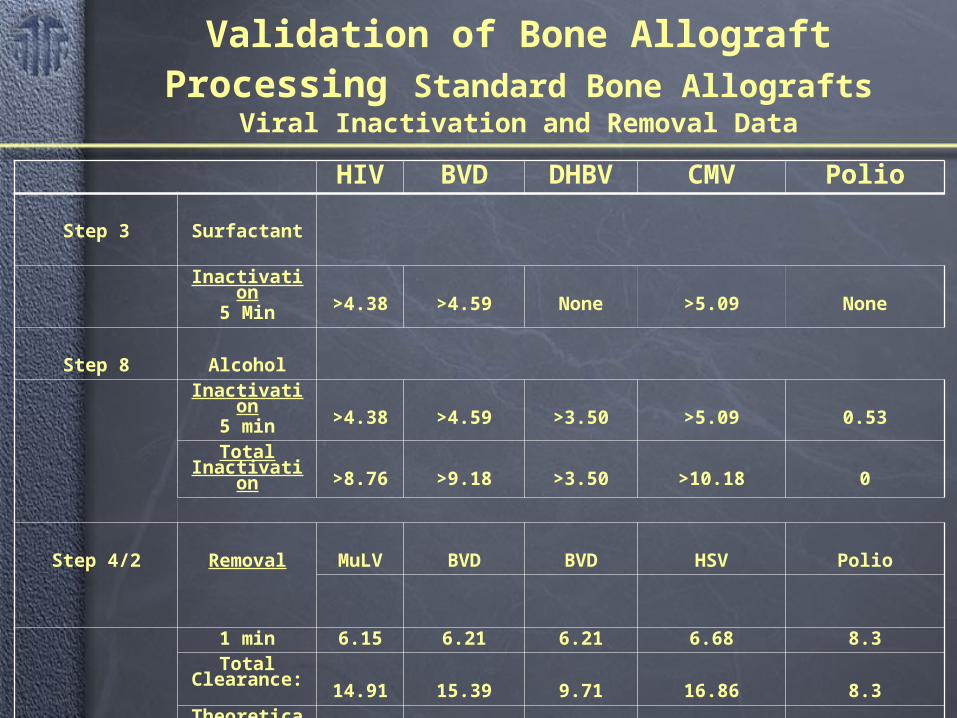
Validation of Bone Allograft Processing Standard Bone Allografts
Viral Inactivation and Removal Data
HIV BVD DHBV CMV Polio
Step 3 Surfactant
Inactivation5 Min >4.38 >4.59 None >5.09 None
Step 8 AlcoholInactivation
5 min >4.38 >4.59 >3.50 >5.09 0.53Total
Inactivation>8.76 >9.18 >3.50 >10.18 0
Step 4/2 Removal MuLV BVD BVD HSV Polio
1 min 6.15 6.21 6.21 6.68 8.3Total
Clearance:14.91 15.39 9.71 16.86 8.3
Theoretical Max. Viral
Burden 5.3-8.6 4.6-8.4 1.8-4.3 ND ND
Safety Factor 6.31 6.99 5.41 - -
19
Current process validation guidance documents and virology perspectives can be successfully adapted to viral clearance process validation for bone allografts
Bone allograft performance can be maintained while producing a significant SAL using a conservatively calculated theoretical maximum viral burden
Current process validation guidance documents and virology perspectives can be successfully adapted to viral clearance process validation for bone allografts
Bone allograft performance can be maintained while producing a significant SAL using a conservatively calculated theoretical maximum viral burden
Validation of Bone Allograft Processing
20
Validation of Bone Allograft ProcessingValidation of Bone Allograft Processing
Center for Biologics Evaluation and Research. “Points to Consider in the Characterization of Cell Lines Used to Produce Biologicals” (Food and Drug Administration) 1993
Center for Biologics Evaluation and Research. “Points to Consider in Manufacture and Testing of Monoclonal Antibody Products for Human Use” (Food and Drug Administration) 1997
Committee for Proprietary Medicinal Products Ad Hoc Working Party on Biotechnology/Pharmacy and Working Party on Safety Medicines, Note for Guidance. “Validation of Virus Removal and Inactivation Procedures”, Biologicals 1991: 19-247-251
Committee for Proprietary Medicinal Products: EEC Council Directive 89/381: “Medicinal Products Derived from Human Plasma” (Revised Draft 1995)
Center for Biologics Evaluation and Research. “Points to Consider in the Characterization of Cell Lines Used to Produce Biologicals” (Food and Drug Administration) 1993
Center for Biologics Evaluation and Research. “Points to Consider in Manufacture and Testing of Monoclonal Antibody Products for Human Use” (Food and Drug Administration) 1997
Committee for Proprietary Medicinal Products Ad Hoc Working Party on Biotechnology/Pharmacy and Working Party on Safety Medicines, Note for Guidance. “Validation of Virus Removal and Inactivation Procedures”, Biologicals 1991: 19-247-251
Committee for Proprietary Medicinal Products: EEC Council Directive 89/381: “Medicinal Products Derived from Human Plasma” (Revised Draft 1995)
21
Validation of Bone Allograft ProcessingValidation of Bone Allograft Processing
Committee for Proprietary Medicinal Products: 1995 Revised CPMP Guidelines. Virus Validation Studies: The design, contribution and interpretation of studies validating the inactivation and removal of viruses (revised)
ICH Viral Safety Document: QSA Viral Safety Evaluation of Biotechnology Products Derived from Cell Lines of Human or Animal Origin: 1998
Committee for Proprietary Medicinal Products: 1995 Revised CPMP Guidelines. Virus Validation Studies: The design, contribution and interpretation of studies validating the inactivation and removal of viruses (revised)
ICH Viral Safety Document: QSA Viral Safety Evaluation of Biotechnology Products Derived from Cell Lines of Human or Animal Origin: 1998
22
Validation of Allograft Bone ProcessingValidation of Allograft Bone Processing
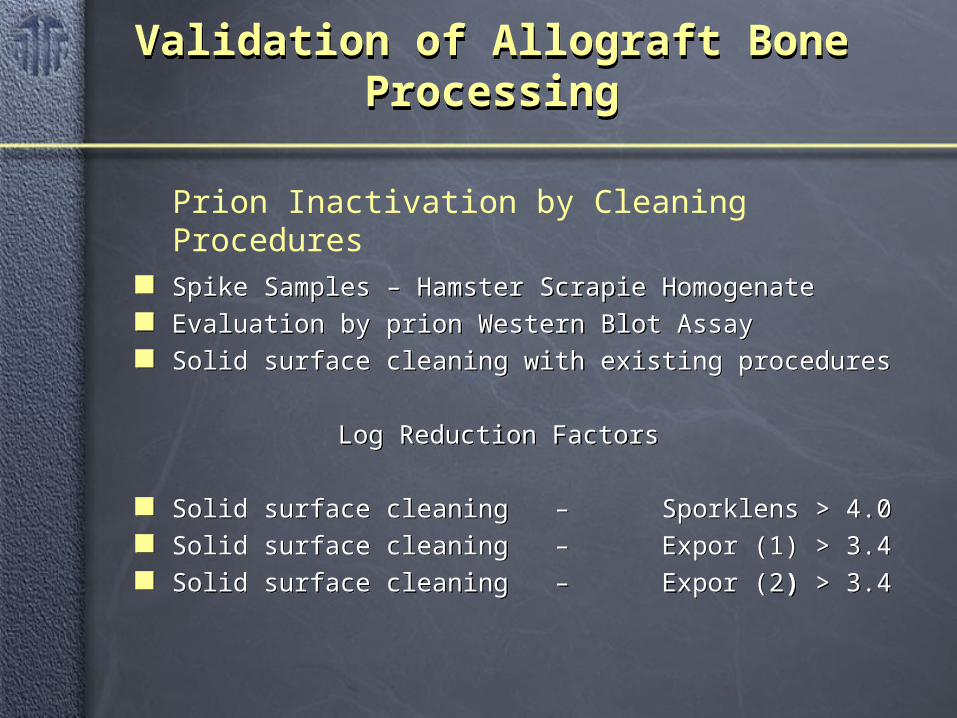
Spike Samples – Hamster Scrapie Homogenate Evaluation by prion Western Blot Assay Solid surface cleaning with existing procedures
Log Reduction Factors
Solid surface cleaning – Sporklens > 4.0 Solid surface cleaning – Expor (1) > 3.4 Solid surface cleaning – Expor (2) > 3.4
Spike Samples – Hamster Scrapie Homogenate Evaluation by prion Western Blot Assay Solid surface cleaning with existing procedures
Log Reduction Factors
Solid surface cleaning – Sporklens > 4.0 Solid surface cleaning – Expor (1) > 3.4 Solid surface cleaning – Expor (2) > 3.4
Prion Inactivation by Cleaning Procedures
23
Validation of Allograft Bone ProcessingValidation of Allograft Bone Processing
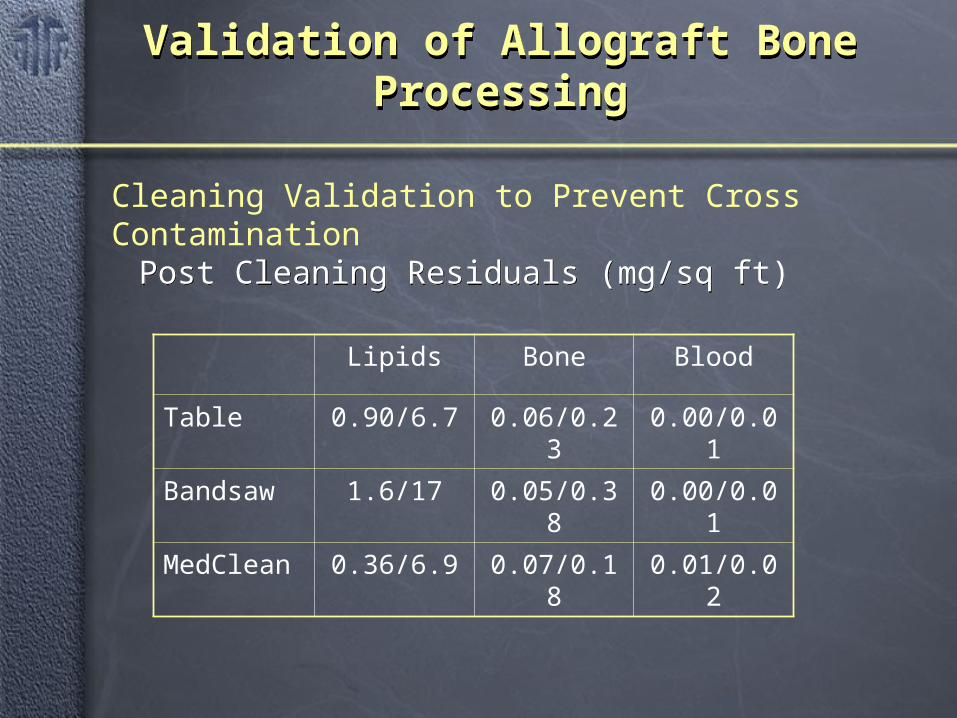
Post Cleaning Residuals (mg/sq ft) Post Cleaning Residuals (mg/sq ft)
Lipids Bone Blood
Table 0.90/6.7 0.06/0.23 0.00/0.01
Bandsaw 1.6/17 0.05/0.38 0.00/0.01
MedClean 0.36/6.9 0.07/0.18 0.01/0.02
Cleaning Validation to Prevent Cross Contamination





























