Embed Size (px)
Citation preview
1
VIReC Cyber Seminar Series 2006
VA Databases and MethodsVA Databases and Methods
Using VA Pharmacy Data
Presented byTodd A. Lee, PharmD, PhD
Senior Investigator, MCHSPR COEVIReC, Senior Scientific Expert Pharmacy Data
Research Assistant Professor, Northwestern University Feinberg School of Medicine
2
Session Objectives
Measurement Issues with Pharmacy Data
Key Data Source Review: PBM Data & DSS Pharmacy Data
Measurement Issues and Use of Pharmacy Data
Where To Go For More Help
3
Pharmacy Data Measurement Issues
Comparability of data sources– Do PBM and DSS contain the same data?
Medication utilization– Recent year? Longer historical view? Does policy change impact
medication use?Exposure to specific medications or medication classes– Are specific drugs associated with better/worse outcomes?
Medication adherence– How much of a prescribed medication are patients using?
Combining outpatient and pharmacy data to identify events– Can we identify acute exacerbations of COPD with outpatient and
prescription data?Assessing comorbidity or case-mix with medication data– Diagnoses-based measures vs. pharmacy-based measures
4
Session Objectives
Measurement Issues with Pharmacy Data
Key Data Source Review: PBM Data & DSS Pharmacy Data
Measurement Issues and Use of Pharmacy Data
Where To Go For More Help
5
Pharmacy Data Sources Local Databases– VistA– VISN Warehouses
National Data Sources– PBM– DSS NDE Pharmacy SASⓇ Datasets– FCDM
6
VistA Pharmacy Data
Veterans Health Information Systems and Technologies Architecture
All Prescription Orders and Fills– Inpatient and Outpatient– CMOP (Consolidated Mail Outpatient Pharmacy)
• in VistA system for site where fill was requested
Local Files– At each VistA installation
7
VistA Pharmacy Data
Prescription Orders Dispensed– Prescription File (FILE 52) - Outpatient– Pharmacy Patient File (FILE 55) - Inpatient
• IV Orders (FILE 55.01)• Unit Dose Orders (FILE 55.06)
– Local Drug File (FILE 50)
Years covered– 1997 forward – Varies by site
8
VistA Pharmacy Data
Accessing– FileMan – hierarchical database management
system– MUMPS– SQL
VISN Warehouses– Some contain prescription data– Relational databases
9
PBM Database
Pharmacy Benefits Management Database
FY1999 forward (October 1, 1998)
Maintained by PBM/SHG at Hines VA Hospital
Researchers must request extract
10
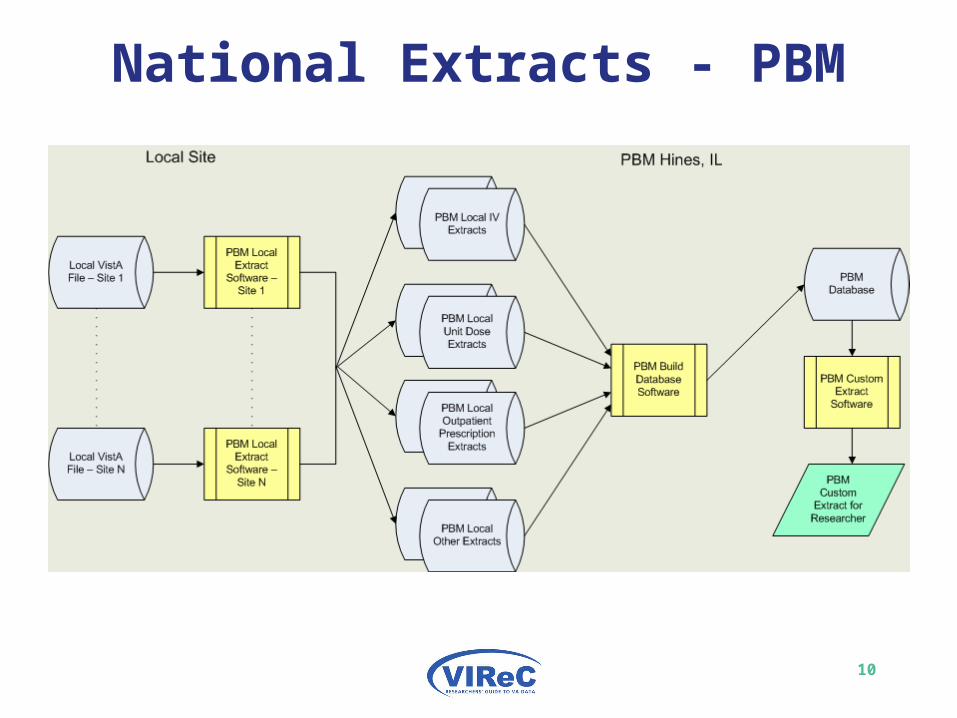
National Extracts - PBM
11
PBM Database
Information in the Database– Outpatient Prescriptions Dispensed– Inpatient Prescriptions Dispensed (IV & Unit Dose)– Selected Labs– Controlled Substance Use– Automatic Replenishment/Ward Stock– Procurement and Accounting– Provider Information– Patient Information
12
PBM Database Variables
Outpatient Prescription
Dispensing Details– Fill Date– Drug Name– Station Name– Quantity– NDC – National Drug Code– Dosing Instructions– VA Drug Class– Dispense Unit and Price per Dispense Unit
13
PBM Database Variables
Outpatient PrescriptionProvider Information– Provider ID– Provider Service
• Cardiology, Dental, Nursing, Surgery, etc.
– Provider Specialty & Subspecialty– Provider Type
• Staff, Fee, or Non-VA (TPB)
Patient Information– Patient Prescription Status
14
DSS NDE Pharmacy SASⓇ Datasets
Decision Support System National Data Extract Pharmacy SASⓇ Datasets.
FY2002 forward
Located on the host at the Austin Automation Center
Directly accessible by Researchers
15
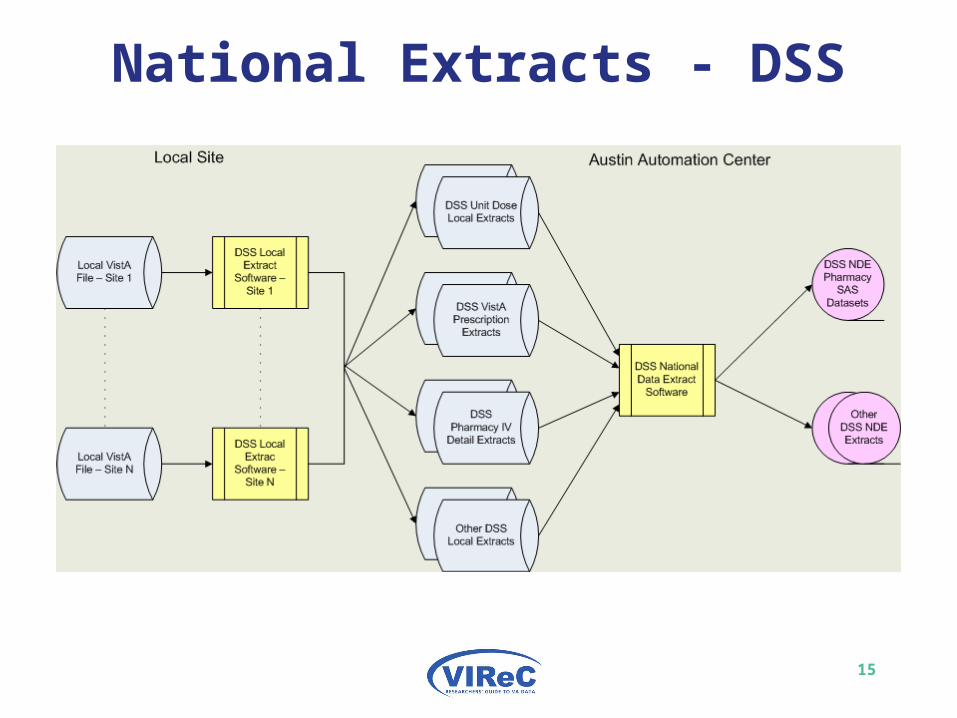
National Extracts - DSS
16
DSS NDE Pharmacy SASⓇDatasets
Information in the Datasets– Outpatient Prescriptions Dispensed– Inpatient Prescriptions Dispensed
• IV• Unit Dose
17
DSS NDE Pharmacy SASⓇ Datasets
Files– RMTPRD.MED.DSS.SAS.FYYY.VISNX.PHA
• YY – year• VISN – V1TO5, V6TO10, V11TO16, V17TO22• X – I for inpatient, O for outpatient
– Based on patient status for encounter not type of prescription
– Safest to always use both files
– Inpatient• RMTPRD.MED.DSS.SAS.FY03.V1TO5I.PHA
– Outpatient• RMTPRD.MED.DSS.SAS.FY03.V1TO5O.PHA
18
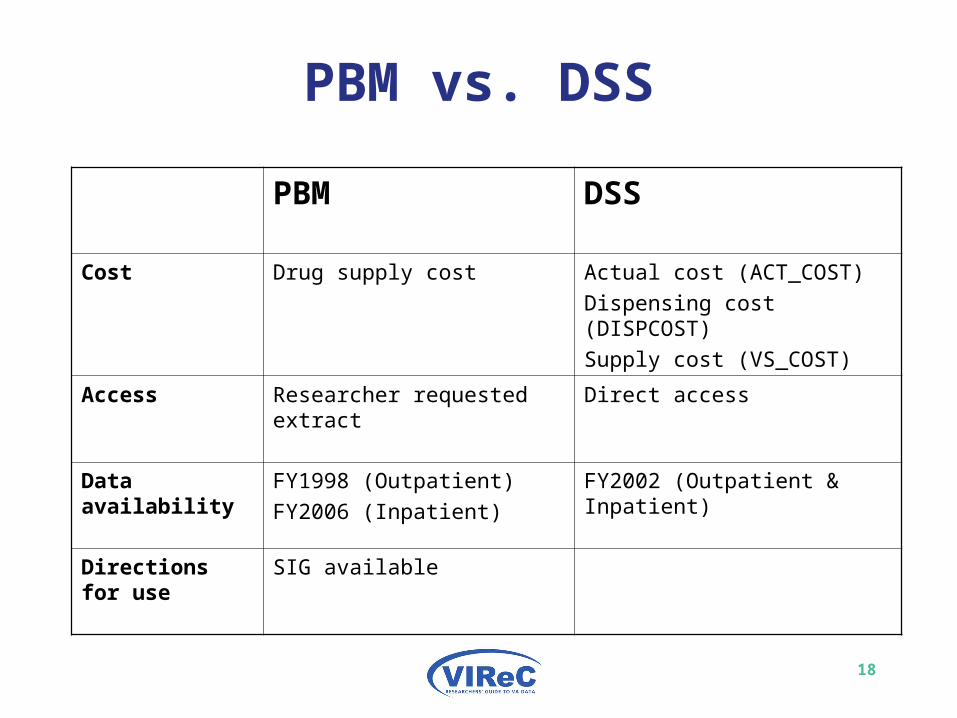
PBM vs. DSS
PBM DSS
Cost Drug supply cost Actual cost (ACT_COST)
Dispensing cost (DISPCOST)
Supply cost (VS_COST)
Access Researcher requested extract Direct access
Data availability FY1998 (Outpatient)
FY2006 (Inpatient)
FY2002 (Outpatient & Inpatient)
Directions for use
SIG available
19
Session Objectives
Measurement Issues with Pharmacy Data
Key Data Source Review: PBM Data & DSS Pharmacy Data
Measurement Issues and Use of Pharmacy Data
Where To Go For More Help
20
Measurement Issues: Pharmacy Data Comparison
CSP 456 Hernia Study
Population– 1,591 Patients in the CSP 456 Study
Prescriptions– Outpatient– FY2002– Fills and refills– 42,469 prescriptions
Report Available at: Report Available at: http://www.virec.research.va.gov/References/TechnicalReports/VIReCTechnicalReport1.pdfhttp://www.virec.research.va.gov/References/TechnicalReports/VIReCTechnicalReport1.pdf
21
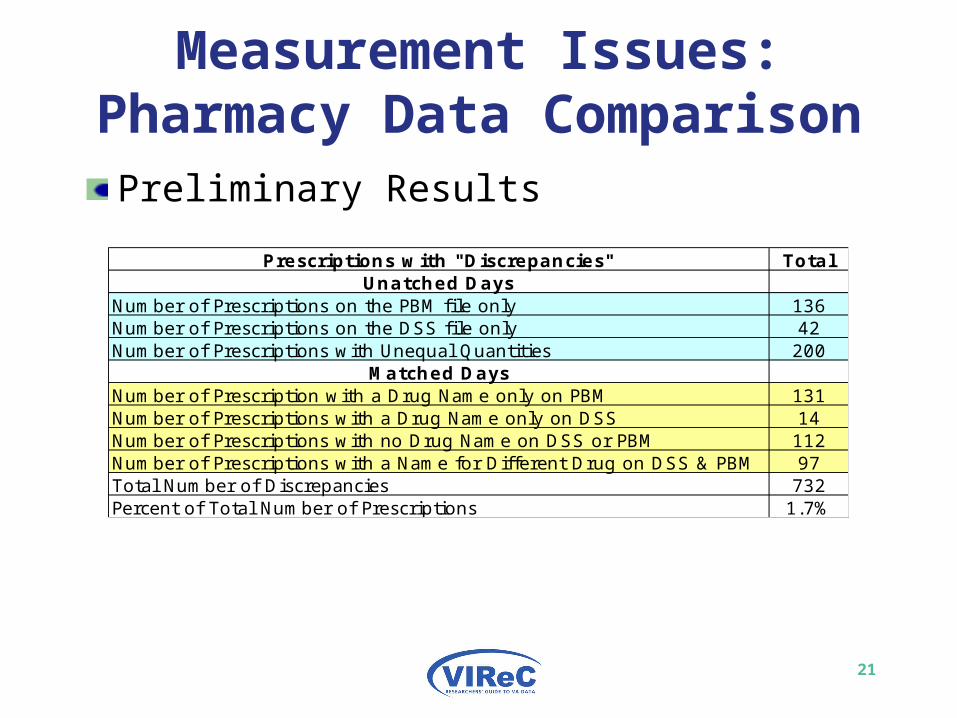
Measurement Issues: Pharmacy Data ComparisonPreliminary Results
Prescriptions with "Discrepancies" TotalUnatched Days
Number of Prescriptions on the PBM file only 136Number of Prescriptions on the DSS file only 42Number of Prescriptions with Unequal Quantities 200
Matched DaysNumber of Prescription with a Drug Name only on PBM 131Number of Prescriptions with a Drug Name only on DSS 14Number of Prescriptions with no Drug Name on DSS or PBM 112Number of Prescriptions with a Name for Different Drug on DSS & PBM 97Total Number of Discrepancies 732Percent of Total Number of Prescriptions 1.7%
22
Measurement Issues: Pharmacy Data ComparisonLimitations– Outpatient only– Cohort not representative of whole population
Conclusions– DSS and PBM Pharmacy extracts capture same
prescriptions– DSS or PBM?
Future Comparisons– Inpatient data?– Representative Cohort
Anecdotal evidence of other examples where match is not as good
23
Measurement Issues: Medication Utilization
Did change in prescription drug copayment impact medication utilization? (HSR&D ECI 02-220, PI: Kevin T. Stroupe, PhD)Examined 30-day equivalents of use of chronic medications in 3 groups of patients before and after copayment changeIdentified utilization in several categories: essential vs. non-essential; OTC vs. prescription; high cost vs. low cost; brand vs. genericNumber of medications obtained from the VA decreased among those subject to copayments and biggest effects were in low cost and OTC medications
24
Measurement Issues: Exposure to specific medications
Determine if the use of ICS is associated with an increased risk of non-vertebral fractures in patients with COPD in the VAConducted a nested case-control study in a cohort of VA patients with COPDFound increased risk of fractures in COPD patients using high dose ICSNeeded to quantify amount of use of inhaled medicationsPharmacy data not always easy to work with – particularly true with regard to inhaled products– More straightforward to calculate cumulative exposure when
dealing with tablets/capsules than with inhalers
25
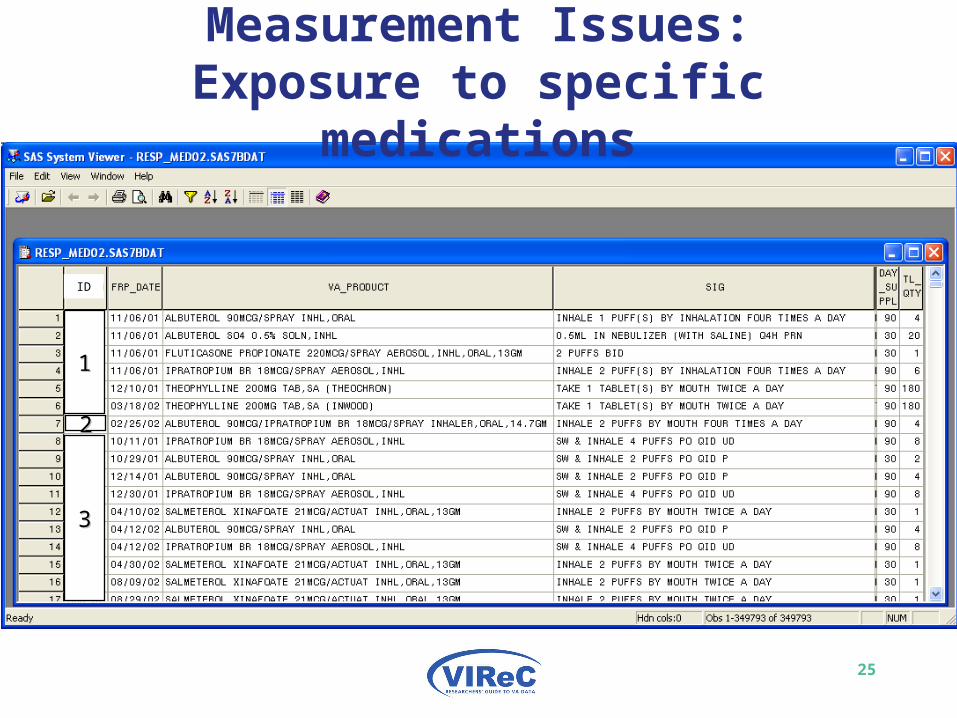
Measurement Issues: Exposure to specific medications
ID
11
33
22
26
Measurement Issues: Exposure to specific medications
VA_PRODUCT– Used to determine specific product– Used to determine dose strength– Used to determine number of actuations
SIG– Used to determine dosing frequency– Used to determine number of doses per day
27
Measurement Issues: Exposure to specific medications
Calculation of cumulative ICS exposure– Determine strength for each prescription
• Fluticasone 220g
– Convert strength to beclomethasone equivalents• BDP_Equiv => 220*0.5 = 110g per dose
– Determine number of doses per prescription• quantity dispensed * doses per product• 1 canister * 120 actuations/canister = 120 doses
– Calculate beclomethasone equivalents for each prescription and sum for cumulative exposure
28
Measurement Issues: Medication Adherence
Examine factors associated with non-adherence in patients with COPD
Measured adherence to respiratory medications using Medication Possession Ratio (MPR)
MPRi =
Found use of CMOP and hospitalizations in prior period associated with higher adherence
Cautions: day supply variable accuracy (oral meds vs. inhaled meds); accounting for medications and days supply at beginning and end of period of interest
)2003,1)((2004,312003,1
AugDaySupplyLastRxDate
DaySupply toJulyAug
29
Measurement Issues: Combining Outpatient and Pharmacy Data
Identify acute exacerbations of COPD in the outpatient settingUse a combination of outpatient ICD-9 codes and Rx dataFound many outpatient ICD-9 codes non-specific for identifying COPD exacerbationMost Rx for oral steroids or antibiotics dispensed within ±5 days of ICD-9 codeUsed algorithm to disqualify ICD-9 codes and medication prescriptions– SIGS with cellulitis, pharyngitis, sinusitis, etc.
30
Measurement Issues: Identifying Comorbidities with Pharmacy Data
Development of a VA-based version of RxRisk (Chronic Disease Score)– Sloan KL, et al. Construction and characteristics of RxRisk-
V: a VA-adapted pharmacy-based case-mix instrument. Med Care 2003; 41(6): 761-74
Potential value in using pharmacy-based measures versus ICD-based measuresRxRisk-V performed similarly to HCC and ADG case-mix adjusters when predicting costs prospectively– Sales AE, et al. Predicting costs of care using a pharmacy-
based measure risk adjustment in a veteran population. Med Care 2003; 41(6): 753-60
31
Session Objectives
Measurement Issues with Pharmacy Data
Key Data Source Review: PBM Data & DSS Pharmacy Data
Measurement Issues and Use of Pharmacy Data
Where To Go For More Help
32
VIReC Help
VIReC Webpage http://www.virec.research.va.gov
– Information on VA data sources and how to access data
– Documentation on some VA datasets, i.e., Medical SAS datasets:
• http://www.virec.research.va.gov/DataSourcesName/Medical-SAS-Datasets/SASdocumentation.htm
• Includes lists of variables and their dataset locations• Descriptions of each of the variables• Values for selected variables
33
VIReC Help (cont’d)
HSRData Listserv– Join at VIReC Web site– Discussion among > 200 data stewards, managers,
and users– Past messages in archive (on intranet)
VIReC Help Desk– VIReC staff will answer your question and/or direct
you to available resources on topics– [email protected] – (708) 202-2413
34
References
Arnold N, Hynes DM, Stroupe KT. VIReC Technical Report 1: Comparison of VA Outpatient Prescriptions in the DSS Datasets and the PBM Database. Edward Hines, Jr. VA Hospital, Hines, IL: VA Information Resource Center, January 15, 2006. Lee TA, Weiss KB. Risk of non-vertebral fractures associated with inhaled corticosteroid use in obstructive lung disease. Am J Respir Crit Care Med. 2004; 169(7): 855-859.Charbonneau A, Rosen AK, Ash AS, Owen RR, Kader B, Spiro A, III, et al. Measuring the quality of depression care in a large integrated health system. Med Care 2003; 41(5):669-680.Sloan KL, et al. Construction and characteristics of RxRisk-V: a VA-adapted pharmacy-based case-mix instrument. Med Care 2003; 41(6): 761-74Sales AE, et al. Predicting costs of care using a pharmacy-based measure risk adjustment in a veteran population. Med Care 2003; 41(6): 753-60
35
VIReC CyberSeminar Series 2006
VA Databases and MethodsVA Databases and MethodsSponsored by VA Information Resource Center (VIReC)
Every first Tuesday of the month from 1 – 2 pm ET
Next Cyber Seminar:
November 7, 2006
“VA-Medicare Data”
Presented by: Kathy Mallin, PhD and Kristin Koelling, MPH (VIReC)This session focuses on assessing non-VA health care use using VA-Medicare data. The following is the session agenda:
* Why use VA-Medicare Data?
* Learn about the VA-Medicare Data Merge Initiative and available data
* Understand how to request VA-Medicare data
* Learn where to go for help
Schedule available at: http://www.hsrd.research.va.gov/for_researchers/cyber_seminars/