Embed Size (px)
Citation preview

1
Using Structural Funds to reduce health inequalities: lessons from EUREGIO III
Prof Jonathan Watson
HE2020 Workshop (WP4)Brussels 17 October 2012
HCN Executive Director; EUREGIO III Project Director; HealthEquity-2020 Project Director,; Special Professor of Health & Public Policy, University of Nottingham; External Partner to European Masters degree in Sustainable Regional Health Systems (Deusto, Vilnius, Corvinus, Verona)
disadvantaged groupslimited evidence that SF have reduced inequities for disadvantaged groups
short-lived projects have undertaken innovative actions but these have rarely been mainstreamed and sustained (Degryse, 2010)
EUREGIO III evidence
EUREGIO III (2009-2011)
WHO/EU Equity Project Policy briefing (2010)
EU Council Conclusions ‘Towards modern, responsive and sustainable health systems’ (2011)
Guide for DG REGIO desk officers (2011)
High Level Reflection sub group 2 (2012+)
3

Tackling trends: demographics and chronic illness
Poverty Housing
Diet Smoking
Cardiovascular disease
Treatment
Death
Current bias towards curative investment
Transformational investment
Patient centred interventional support

Rethinking healthcare care – an alternative model
The ‘wellness park’ model,
Kymenlaasko,Finland
• Rethinking the acute hospital
• Repositioning services, from illness to wellness
support• Healthy ageing

Remote community strategies

critical success factors
Strategic vision
Accountability
Financial realism
Integration
Measurable ROI
Technology diffusion
Social cohesion
3 integrated elements of health care delivery:• service delivery
models• Workforce• Capital
(infrastructure; technology; ICT
Population health statusHealth outcomesEconomic outcomes

“Objectives are European, funds are national and needs are local”National Reform
ProgrammePartnership
Contract
Operational Programme
s
Joint Action Plans
Individual projects
STRUCTURAL FUNDSProject instrument or strategic development?ConditionalitiesAd hoc stakeholder engagement?Spend or added valueCOMMUNITY EXPERIENCEClay Cross 1984: do not listen to us Drumchapel 1996: isolation & frustrationSouth Lanarkshire CP 2000: no pooling of fundsSkelmersdale 2004: community cliques

Thematic objectives for Cohesion Policy 2014-2020
Thematic objective Pathways to health equity
1. strengthening research, technological development and innovation;
Access to health care, living and working conditions
2. enhancing access to, and use and quality of, information and communication technologies;
Access to health care, living and working conditions
3. enhancing the competitiveness of small and medium-sized enterprises, the agricultural sector (for the EAFRD) and the fisheries and aquaculture sector (for the EMFF);
Working conditions
4. supporting the shift towards a low-carbon economy in all sectors;
Living and working conditions
5. promoting climate change adaptation, risk prevention and management;
Living and working conditions
6. protecting the environment and promoting resource efficiency;
Living and working conditions
7. promoting sustainable transport and removing bottlenecks in key networkinfrastructures
Access to health care, living and working conditions
8. promoting employment and supporting labour mobility; Living and working conditions
9. promoting social inclusion and combating poverty; Access to health care,, living and working conditions
10. investing in education, skills and lifelong learning; Access to health care, working conditions
11. enhancing institutional capacity and an efficient public administration.
Access to health care
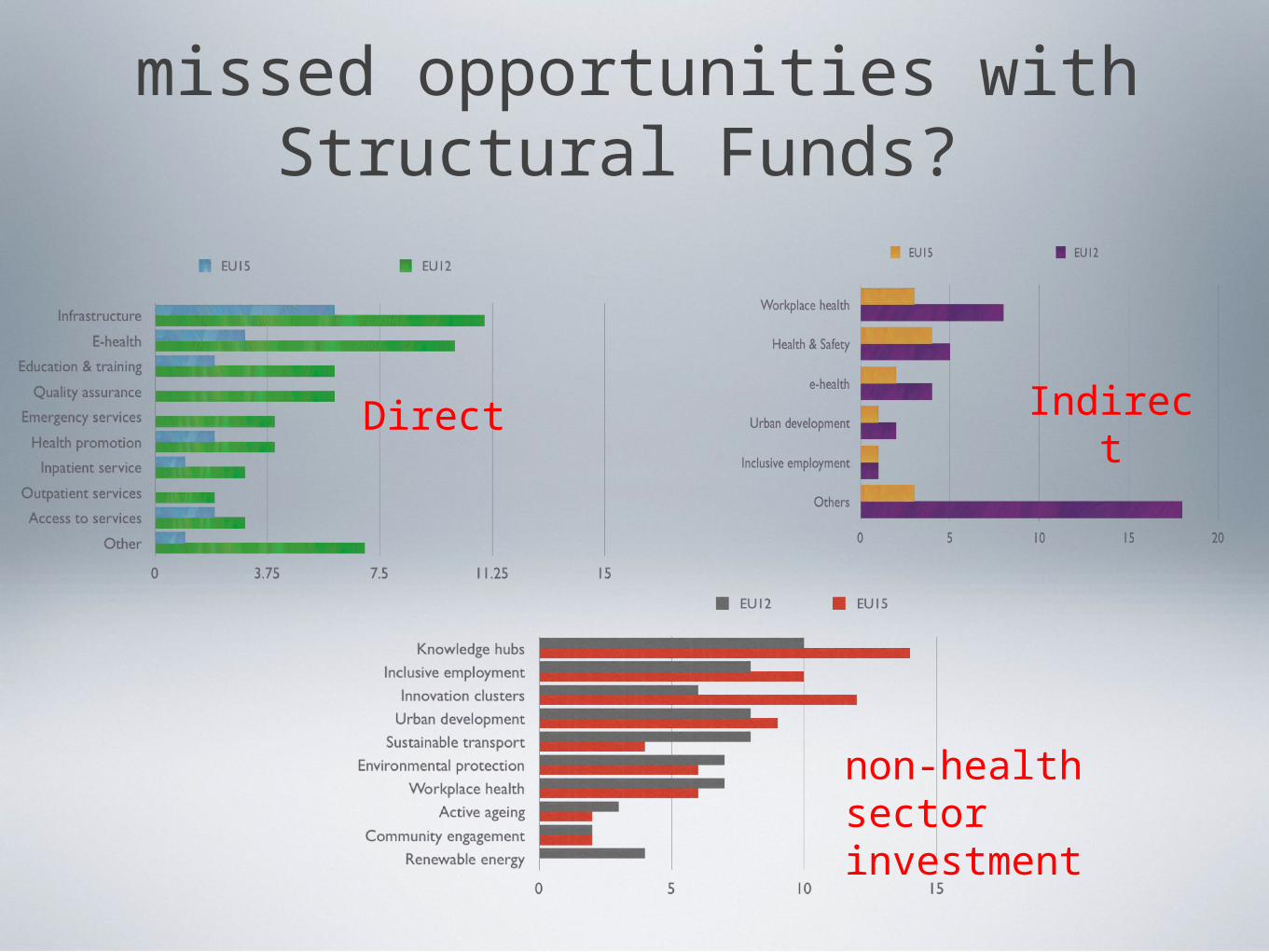
missed opportunities with Structural Funds?
Direct Indirect
non-health sector investment

11
organisational response
12
What MS and Regions need to think about
Realistic starting points - taking into consideration the peculiarities of socialised, non-reformed health systems especially in the EU10
Commitment to transformational change – prioritising the shift away from a hospital-centric model of care to more pluralistic community-based and integrated models of care contributing to sustainable health systems
Affordable investment priorities – how ERDF/ESF spending can contribute to changes in structure and delivery of health services. This is likely to include e-health, infrastructure and equipment
Address health inequalities - this will include access to basic health services (GP, outpatient clinic, polyclinic, community based care) by poor and marginalised communities
Multiple roles for regional health systems – economic growth, renewable energy, environmental quality, social cohesion

REGIO checklist

principles for action
Engage stakeholders – it’s a long conversation
Plan – map the intervention logic
Innovate – create and do the right thing
Be transparent - accountable decision-making
Disinvest to reinvest – financial realism
Build capacity – processes, procedures, people
Return on investment – deliver added value

15
thank you
www.euregio3.eu
www.healthclusternet.eu