Embed Size (px)
Citation preview
1
Using GroupSystems with Simulation to Validate Concepts for Municipal Response to
Terrorist Attacks with Biological Weapons
John Walther, Edgewood CB Center
Freeman Marvin, Decision Advantage
Susan Hayes, Litton-TASC
March 28, 2000
2
Agenda
• First hour– BW Improved Response Program
– BW Response Template Validation
– Introduction to the Simulation Exercise
– NEHC Simulation Exercise
• Second hour– Use of GroupSystems in the NEHC Validation
– Introduction to the Simulation Exercise
– NEHC Simulation Exercise
– Questions and Answers
3
Background
• PL 104-201 (National Defense Authorization Act for Fiscal Year 1997) initiated BW Improved Response Program
• Title XIV - Defense Against Weapons of Mass Destruction– “The Secretary of Defense shall develop and carry out a
program for testing and improving the responses of Federal, State and local agencies to emergencies involving biological weapons and related materials and emergencies involving chemical weapons and related materials.”
4
Background
• BW IRP is a multi-year, multi-agency effort begun in April 1998
• BW IRP objectives:– complete an assessment of the BW response
problem– formulate an integrated approach to BW
emergency response – identify gaps and improvements in response
capabilities
5
Template Development
• Series of five 3-day workshops during 1998– Day 1: tutorials / pre-selected topics– Day 2: presentation of a selected BW terrorist
attack scenario / develop response activities designed to mitigate the emerging consequences of the scenario
– Day 3: review and integrate the response template
6
Attack Scenarios
• 5 potential BW scenarios were analyzed (covert release of BW agent)– Scenario #1: Francisella tularensis producing
1,100 casualties of which 380 were fatalities– Scenario #2: Staphylococcus Enterotoxin B in
combination with Fracisella tularensis producing 22,500 casualties, of which 10,000 were fatalities
7
Attack Scenarios
– Scenario #3: Bacillus anthracis spores producing 126,000 casualties, of which 120,000 were fatalities
– Scenario #4: Venezuelan Equine Encephalitis (VEE) producing 1,300,000 casualties, of which 13,000 were fatalities
– Scenario #5: Rift Valley Fever on a cattle feed lot infecting 700,000 cattle and producing 48,000 human casualties, of which 250 were fatalities
8
Typical Effects of Bio Agents
Biological agents can be disseminated as odorless, colorless aerosols that are highly lethal. Aerosolized agents are easily absorbed both through the respiratory system and mucous membranes (e.g., eyes). The onset of clinical symptoms may be rapid (within several minutes for toxins) or gradual (within a day to weeks) depending on the amount of exposure and constitution of the individual exposed. For example, typical symptoms for tularemia usually present within 3 to 6 days and include headache, fever, chest pain, stiff neck, and pneumonia. For higher concentration exposure or less resistant individuals, the symptoms may present earlier and be more acute. Individuals who eventually die typically suffer from cardiopulmonary failure. First-aid and treatment techniques include artificial respiration plus oxygen and administering fluids and antibiotics.
9
Summary
• A BW terrorist event would primarily represent a public health catastrophic medical emergency.
• An organized, effective emergency response to a large BW attack involving a million or more people appears possible.
• The BW Response Template represents a flexible, integrated response system.
• Effective response to a major BW incident requires pre-planning before the event , and rapid implementation of the plan following an incident.
10
BW Response Template Validation
11
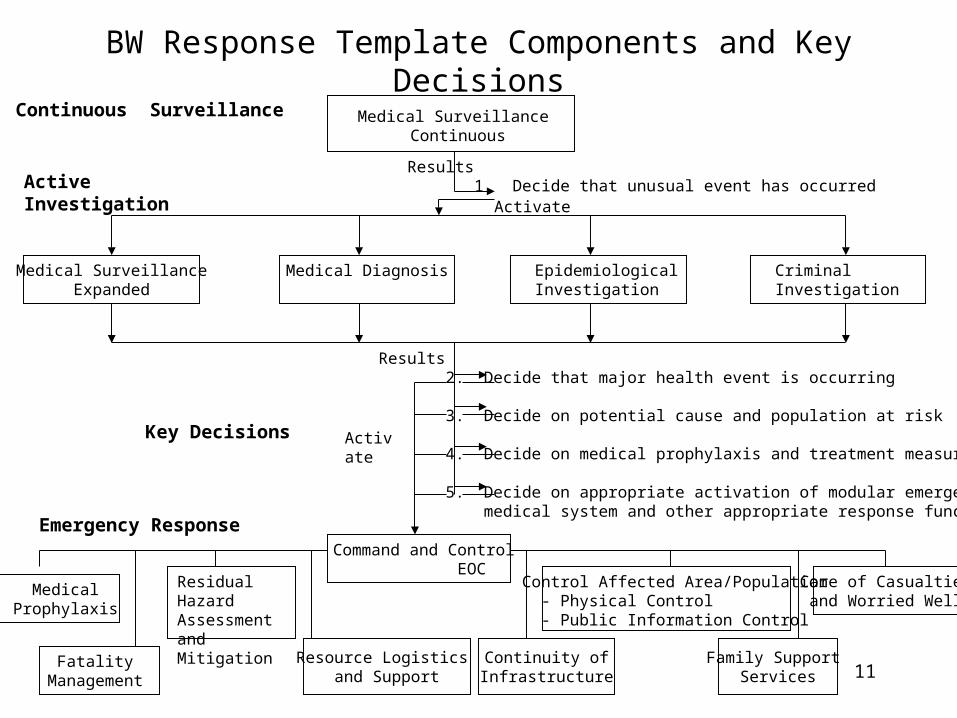
BW Response Template Components and Key Decisions
Results 1. Decide that unusual event has occurred
Continuous Surveillance
ActiveInvestigation
Medical SurveillanceExpanded
Medical Surveillance Continuous
Activate
Medical Diagnosis EpidemiologicalInvestigation
CriminalInvestigation
Results 2. Decide that major health event is occurring
3. Decide on potential cause and population at risk
4. Decide on medical prophylaxis and treatment measures
5. Decide on appropriate activation of modular emergency medical system and other appropriate response functions
Activate
Care of Casualtiesand Worried Well
Residual HazardAssessment andMitigation
Control Affected Area/Population - Physical Control - Public Information Control
FatalityManagement
Command and Control EOC
Resource Logistics and Support
Continuity ofInfrastructure
Family Support Services
Emergency Response
MedicalProphylaxis
Key Decisions
12
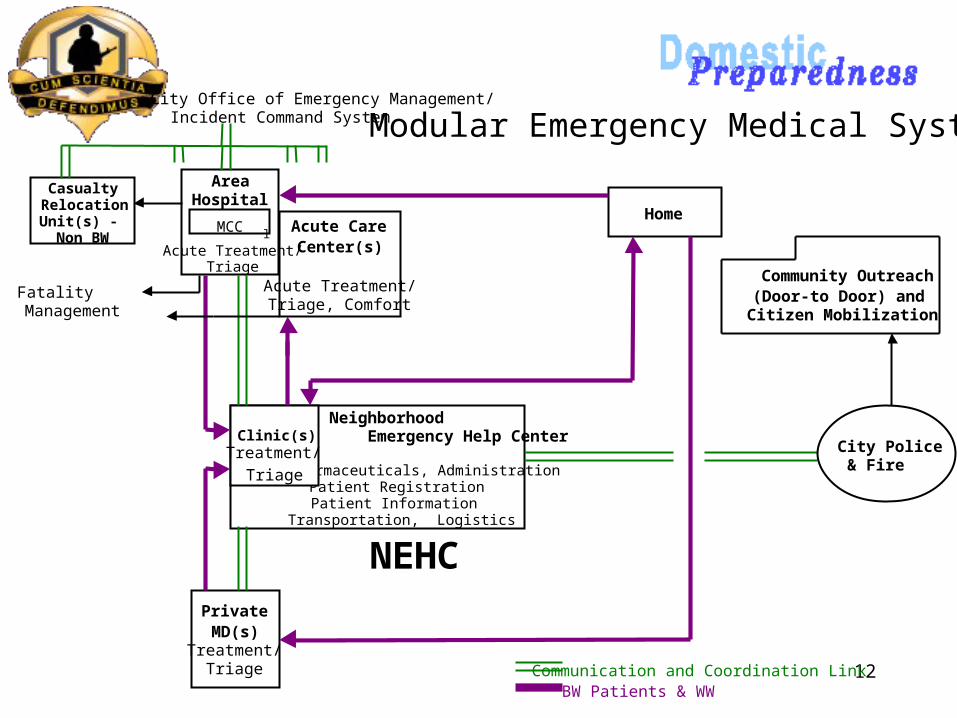
AreaHospital
Acute Treatment/Triage
PrivateMD(s)
Treatment/Triage
Home
Modular Emergency Medical System
CasualtyRelocationUnit(s) - Non BW
Neighborhood
Emergency Help Center
Pharmaceuticals, Administration Patient Registration Patient Information
Transportation, Logistics
Clinic(s)Treatment/
Triage
Acute CareCenter(s)
Acute Treatment/Triage, Comfort
FatalityManagement
City Office of Emergency Management/Incident Command System
Communication and Coordination Link
Community Outreach(Door-to Door) andCitizen Mobilization
City Police& Fire
BW Patients & WW
lMCC
NEHC
13
Key Validation Issues
• Rapid and large scale emergence of casualties
• Potential for high number of fatalities
• Effectiveness depends on ability to provide rapid response
• Standards of medical care
• Must minimize number of staff while ensuring adequate capacity
14
Validation Approach
• Establish expected performance for the template component using models
• Conduct tests (live and simulated) and measure actual performance
• Compare expected and measured performances
• Recommend improvements to the template component
15
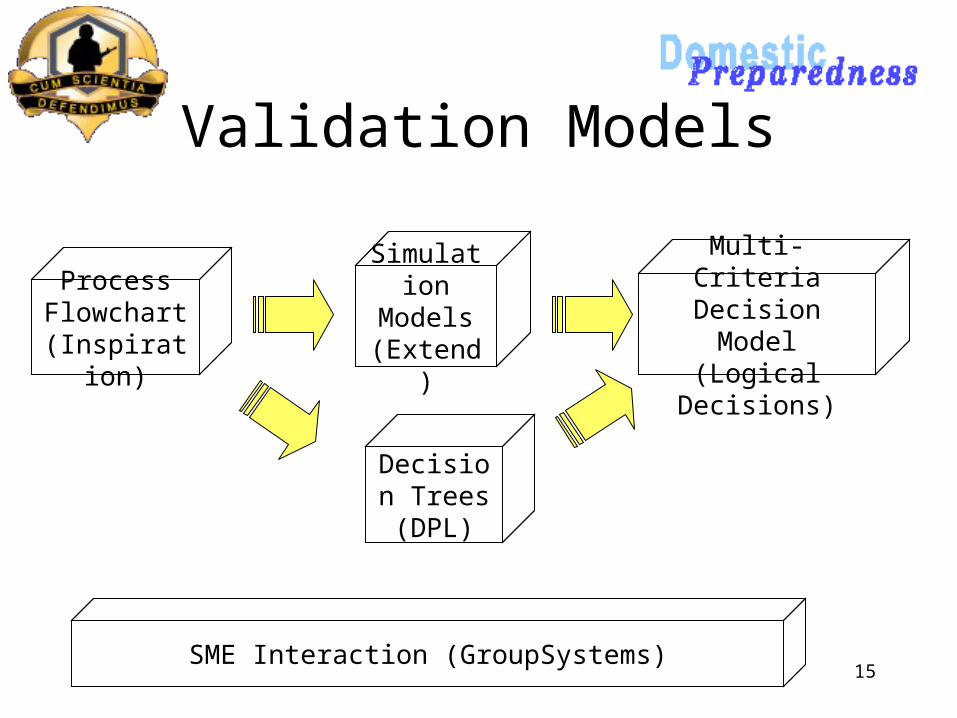
Validation Models
Process Flowchart(Inspiratio
n)
Simulation
Models(Extend)
Multi-Criteria Decision Model
(Logical Decisions)
Decision Trees(DPL)
SME Interaction (GroupSystems)
16
Desktop Exercise - Step-by-step critical review by subject matter expert panel
Simulation Exercise - Small group of responders simulating scenarios using networked computers
Live Exercise - Field exercise with actual responders and actors as casualties
Validation Protocols

17
Introduction to the Simulation Exercise
18
NEHC Simulation Exercise
• The goal of the exercise is to maximize MOE scores in a simulated BW attack
• Players represent the Medical Director and staff in each NEHC area
• Rules:1. Staff can be shifted between areas
2. Secondary triage policy can be changed
19
Measures of Effectiveness
• Throughput
• Cycle time to ACC
• Cycle time to home
• Percent infected sent to ACC
• Percent non-infected sent home
• Reneging
20
NEHC Players
• Medical Director (MD)
• Initial Triage
• Registration
• Secondary Triage
• Treatment and Stabilization
• Observation and Holding
• Discharge
21
Rule 1: NEHC Staff Shifting• Initial Triage - EMT/Nurse
• Registration - Clerks and Volunteers
• Secondary Triage - EMT/Nurse and Volunteers
• Treatment and Stabilization - EMT/Nurse and Volunteers
• Observation and Holding - EMT/Nurse and Volunteers
• Discharge - Clerks and Volunteers
22
Rule 2: Triage Policy Options
• Conservative– Send casualties showing any symptoms to the ACC
• Prudent– Send casualties showing multiple symptoms to the
ACC
• Efficient– Send only critical casualties to the ACC
23
Scenario
• Day 0: Agent released
• Day 1 and 2: Local medical facilities overwhelmed
• Day 3: Public Health officials determine that an outbreak is in progress
• Day 4: NEHC opened
24
Exercise Procedures
• Run simulation• Pause in 6-hour intervals• Review Status Board• Recommend staff changes to the MD• MD decides which changes to make to staff
and/or triage policy• Continue simulation