Embed Size (px)
Citation preview

1
Understanding Healthcare –Associated Pneumonia
Antonio Anzueto, MD
Professor of Medicine
University of Texas Health Science Center at San Antonio

Defining VAP, HAP, and HCAP
• HAP (hospital-acquired pneumonia)– Pneumonia that occurs ≥48 hours from time of admission
• VAP (ventilator-associated pneumonia)– Pneumonia 48 to 72 hours after endotracheal intubation
• HCAP (healthcare-associated pneumonia)– Prior hospitalization (within 90 days)– Resided in nursing home or long-term care facility– Received recent IV antibiotics (within 30 days)
ATS. Am J Respir Crit Care Med. 2005;171:388-416.AJRCCM. 2005; 171:388-416

3
Kollef M, et al. Chest. 2005;128:3854-3862.
Epidemiology and Outcomes of HCAP: Results From a Large US Database of Culture-positive Pneumonia
• DESIGN– Retrospective cohort analysis
(the Atlas database) – 4,543 pneumonias identified via ICD-9
(2002-2003)
• PRIMARY OBJECTIVE– Characterize microbiology and outcome for
culture-positive CAP, HCAP, HAP, and VAP

4
• OUTCOMES
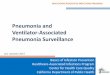
– 49% CAP, 22% HCAP, 18% HAP, and 11% VAP
– MRSA =most common cause of HCAP
– MRSA as percentage of all S. aureas HCAP>HAP>CAP>VAP
– Mortality for HCAP and HAP were similar; both were significantly higher than CAP and lower than VAP
– HCAP differed from HAP and VAP to a lesser degree than CAP relative to:
• Pt characteristics
• Pathogen distribution patterns
• Outcomes
Epidemiology and Outcomes of HCAP: Results From a Large US Database of Culture-positive Pneumonia
Kollef M, et al. Chest. 2005;128:3854-3862.

5
Kollef M, et al. Chest. 2005;128:3854-3862.
Epidemiology and Outcomes of HCAP: Results From a Large US Database of Culture-positive Pneumonia
0
10
20
30
MSSA
MRSA
Strep p
neum
o
Pseudom
onas
Haem
ophilus
Acinet
obacte
r
CAP HCAP HAP VAP
Fre
qu
ency
of
Bac
teri
al P
ath
og
ens

Risk Factors for MDR Pathogens in HCAP
• Antimicrobial therapy in preceding 90 days
• Recent hospitalization of ≥5 days
• High frequency of antibiotic resistance in the community or in the specific hospital unit
• Presence of risk factors for HCAP
• Immunosuppressive disease and/or therapy
ATS. Am J Respir Crit Care Med. 2005;171:388-416.

7
Are HCAP Patients Bringing MDR Pathogens To The Hospital?
Pop-Vicas AE, D’Agata EMC. Clin Infect Dis 2005; 40: 1792-8

8
Are HCAP Patients Bringing MDR Pathogens To The Hospital?
• 1998-2003 with 464 MDR GNB (12%,35%, 53% resistant to 5,4,3 antibiotic groups)
• Case-control study of MDR (at least 3 antibiotic classes) GNB isolated w/I 24 hours admit from clinical infection (not pneumonia)
• Risk factors for MDR on admit: age > 65 (OR 2.8), prior antibiotics for > 14 d (OR 8.7), residence in LTCF (OR3.5). Univariate risks: > 2 hospitalizations in last yr., prior ICU stay.
Pop-Vicas AE, D’Agata EMC. Clin Infect Dis 2005; 40: 1792-8

Factors associated with Resistant Pathogen
9
Shore et al Arch Inter Med 2008; 168:2205

10
Shore et al Arch Inter Med 2008; 168:2205

Point Score and risk stratification for pneumonia due to resistant pathogens
11
Score: Recent hospitalization – 4Nursing home – 3Hemodyalysis – 2ICU admission – 1Total 10
Shore et al Arch Inter Med 2008; 168:2205

12
What Do We Know About HCAP Therapy?
• ATS/IDSA guidelines (2005) recommend therapy be the same as HAP targeted at drug resistant gram-negatives and MRSA– Am J Respir Crit Care Med 2005; 171:388-416
• Literature Search (PubMed 11/12/08)– Textword: healthcare associated pneumonia (399 articles),
antibiotic therapy (201,780 articles)• Combined with “AND” for a total of 19 articles
– Textword: nursing home pneumonia (452 articles)• Combined with “AND ANTIBIOTIC THERAPY” for a total of
47 articles

13
What Do We Know About HCAP Therapy?
–Textword: chronic hemodialysis (35,454 articles)•Combined with “AND PNEUMONIA” for a total of 107 articles
–Textword: prior hospitalization (5084 articles)•Combined with “AND PNEUMONIA THERAPY” for a total of 205 articles

14
Defining Empiric Therapy Issues: Should HCAP Be Treated The Same As HAP??
• Site of care– All HAP, by definition, occurs in the hospital– HCAP can be inpatient or outpatient therapy
• Route of therapy– IV vs oral (many nursing home patients get only oral therapy)
• Bacteriology and Antibiotic choice : Direct at likely pathogens, including– CAP pathogens for some patients
• Pneumococcus and DRSP• Atypicals/Legionella/Viruses: EPIDEMICS in nursing home
– MDR gram negatives and MRSA for other patients

15
Site of Care And Route of Therapy
• HAP, by definition, is ALWAYS treated in the hospital
• NOT ALL HCAP is treated in the hospital with IV therapy– Hemodialysis– Nursing home
• Out of hospital therapy of elderly and nursing home patients is common– Loeb M, et al. JAMA. 2006;295:2503-2510. Oral therapy in Nursing
Home– Hospital at home for the elderly can include IV meds, oxygen. Leff B,
et al. J Am Geriatr Soc. 2006;54:1355-1363.– Many nursing home pneumonia patients prefer therapy in the nursing
home if possible. Carusone SC, et al. BMC Geriatr. 2006;6:2.

16
Asp.=aspirations. *Expectorated sputum with >25 white blood cells per low-power field and <10 squamous epithelial cells per low-power field.Hutt E, Kramer AM. J Fam Pract. 2002;51:709-716.
Bacteriology of NHAP: One form of HCAP
Nursing home pneumonia etiology according to studies using verified sputum* or blood culture
Study N Year
S. Pneumoniae (%)
S. Aurus (%)
Gram-negative rods (%)
H. Influenzae (%)
Anerobes (%) Multiple Organisms (%)
Alvarez 414 1988 32 — 29 — — 22
Peterson 123 1988 10 3 21 9 — —
Marrie 131 1989 16 13 13 — 4 —
Hirata-Davis 50 1991 12 4 15 10 — —
Drinka 17 1994 30 6 — 25 — (Atypicals=0)
Marrie and Blanchard
71 1997 2/5 — 2/5 — — —
Pick 257(98 asp.)
1996 3 38 6 3 — Group B streptococci 43%

17
Bacteriology of NHAP: Can Include Virus and Atypical Pathogens
• Legionella and viruses are important causes of pneumonia in nursing homes and are NOT covered by empiric therapies for HAP– Epidemics of Legionella have occurred in nursing homes,
often related to colonization of drinking water. Each facility may need to test annually. • Seenivasan MH, et al. J Am Geriatr Soc. 2005;53:875-
880.– Rhinovirus outbreaks reported in 2 nursing homes in
Pennsylvania, with up to 40% of hospitalized pneumonia patients infected by this organism. • Hicks LA, et al. J Am Geriatr Soc. 2006;54:284-289.

18
El Solh AA, et al. Clin Infect Dis. 2004;39:474-480.
Suggest therapy for NHAP: Avoid broad-spectrum rx and use 1 drug if functionally active, no recent antibiotics, even if severely ill. Triple therapy (incl. MRSA) if poor ADL or prior antibiotics, with severe illness. MDR= Multi- Drug resistant pathogen
BAL Confirmed Bacteriology of Severe NHAP: Not all at risk for MDR Pathogens
N=88DRP=17
19%N=71
DRP=57%
N=17DRP=12
71%
N=42MDR=0
0%
N=29MDR=5
17%
N=7MDR=3
42%
N=10MDR=9
90%
No prior antibiotics Prior antibiotics (at least 3days in last 6 months)
ADL<12.5
ADL≥12.5
ADL<12.5
ADL≥12.5

19
Need for anaerobic coverage
• Aspiration pleuro-pulmonary syndrome:–History of loss of consciousness due to
alcohol/and or drug overdose–s/p seizures–Gingival disease–Esophageal motility disorder

Role of Anaerobes in Patients With VAP and
Aspiration Pneumonia (AP)
• 185 episodes of suspected VAP and 25 AP patients requiring mechanical ventilation support
• Bacterial pneumonia diagnosed in 63 of 185 episodes (34%) of suspected VAP and 12 of 25 cases (48%) of suspected AP
• More than 1 organism was found in 11 VAP and 4 AP patients• Only 1 anaerobic organism (Veillonella paravula) was isolated from entire
group of patients. It was not considered to be a true pathogen
Marik and Careau. Chest. 1999;115:178-183.
Marik and Careau. Chest. 1999;115:178-183.

Absence of Anaerobes in HAP
VAP Isolates AP Isolates(n = 74) (n = 17)
P aeruginosa 16 -Methicillin-sensitive S aureus 15 2Enterobacter spp 8 3S pneumoniae 5 2Methicillin-resistant S aureus 4 -S agalactiae 4 -S maltophilia 3 -H influenzae 3 2A baumannii 3 -K pneumoniae 3 2E coli 1 2Flavobacterium spp - 2Serratia sp 1 1V paravula - 1Other 8 -
Marik and Careau. Chest. 1999;115:178–183.
Marik and Careau. Chest. 1999;115:178-183.

Aspiration Pneumonia
22
NEJM 2008

23
Slinin Y, et al. Kidney Int. 2006;70:1135-1141.
Pneumonia in Hemodialysis Patients
• DESIGN– Retrospective analysis of Medicare data set on 10,635
dialysis patients
• PRIMARY OBJECTIVE– Define incidence, mortality risk, and bacteriology of
pneumonia
• OUTCOMES– Cumulative probability of pneumonia 0.09 at 1 year,
0.36 at 5 years. – One-year mortality 45%, 83% at 5 years

24
Pneumonia in Hemodialysis Patients
Slinin Y, et al. Kidney Int. 2006;70:1135-1141.
Organism %No organism identified 81.8Gram-positive bacteria 4.8 Streptococcus pneumoniae 3.4 Other Streptococcus species 1.0 Staphylococcus species 0.4Gram-negative bacteria 11.1 Pseudomonas aeruginosa 2.8 Hemophilus influenzae 1.5 Klebsiella pneumoniae 1.6 Escherichia coli 0.7 Other gram-neg organisms 4.5Anaerobic bacteria 0.03 Atypical bacterium: Mycoplasma pneumoniae
0.3
Viral 1.0 Fungal 1.0
Microbiologic spectrum among index pneumonia hospitalizations (n=3101)
Adjusted mortality hazards ratios(with 95% CIs) from Poisson regression analysis, in 6-month intervals
6
5
4
3
2
1
0A
dju
ste
d P
os
t-p
ne
um
on
ia
Ha
zard
s R
ati
o f
or
De
ath
6 24 42 60 78 96
Follow up Intervals (Months)

25
Data On Therapy of HCAP
Proven Efficacy of Therapies That May Not Be Expected To Be
Effective

26
Peterson PK, et al. Am J Med. 1988;85:164-171.
Prospective Study of LRTI in an Extended-care Nursing Home: Oral Cipro vs IM Cefamandole
• DESIGN– 40 patients with pneumonia, 20 with acute bronchitis– Prospective, randomized study in nursing home
• PRIMARY OBJECTIVE– Compare efficacy of oral quinolone vs IM cephalosporin
• OUTCOMES– Both therapies effective, with low in-hospital mortality
(6.5%)– Pneumococcus most common but 81% with gram
negatives in sputum

27
Trenholme GM, et al. Am J Med. 1989;87:116S-118S.
Prospective Study of Hospital or Nursing Home-acquired Pneumonia: IV Ciprofloxacin vs IV Ceftazidime
• DESIGN– 45 patients – Prospective, randomized study in hospitalized adults with nursing
home or hospital-acquired pneumonia
• PRIMARY OBJECTIVES– Compare efficacy of IV quinolone vs IV cephalosporin– Switch to oral therapy when able
• OUTCOMES– More favorable response with cipro (100% vs 70%, P=0.025)– More severely ill with ceftazidime by APACHE II score– One relapse on oral therapy after ceftazidime

28
Oral Quinolone Therapy of Nursing Home-acquired Pneumonia
Loeb M, et al. JAMA. 2006;295:2503-2510.
• DESIGN
– Cluster-randomized trial of 680 patients age >65 at 20 nursing homes in Canada with radiographic pneumonia
– 10 with usual care, 10 with clinical pathway
• PRIMARY OBJECTIVE
– To determine the efficacy of a clinical pathway for oral therapy of pneumonia in the nursing home
• OUTCOMES
– Clinical pathway: oral rx with levofloxacin 500 mg qD, oxygen saturuation monitor, rehydration, close nursing observation
– Fewer hospitalizations (10% vs 22%, P=0.001), fewer hospital days (0.79 vs 1.74, P=0.004), similar mortality and functional status. NO BACTERIOLOGY.
• Cost saving of $1,016 per resident

29
Oral Quinolone Therapy of Nursing Home-acquired Pneumonia
Loeb M, et al. JAMA. 2006;295:2503-2510.
Resident of nursing home with ≥2 of the followingSymptoms or signs of lower respiratory tract infection:
– New or increased cough –– New or increased sputum production –
– Temperature >38° C –– Pleuritic chest pain –
– New or increased abnormal findings on chest examination –
Obtain mobile chest radiograph
Does the resident meet the following criteria?– Ability to eat and drink –
– Pulse ≤100/min –– Respiratory rate <30/min –– Systolic BP ≥90 mm Hg –– Oxygen saturation ≥92% –
Treatment on-site in the nursing homeQuinolone orally for 10 days
Hypodermodysis to treat dehydration if neededTransfer to hospital if no longer meets criteria
for nursing home treatment
Transfer to hospitalQuinilone orally or IV for 10 days
Transfer back to nursing home whencriteria for nursing home treatment met
Yes No

30
Yakovlev SV, et al. Eur J Clin Microbiol Infect Dis. 2006;10:633-641.
TOC Response by Bacteriology
Prospective Randomized Trial of Ertapenem vs Cefepime for HCAP and Nonintubated HAP
• DESIGN– Prospective, double-blind, randomized trial – 303 enrolled, 195 clin eval– HCAP: 23 ertapenem, 28 cefepime.
Minimum 3 days IV– Exclude if Pseudomonal risks or severe
illness• PRIMARY OBJECTIVES:
– Comparative efficacy, bacteriology• OUTCOMES
– At TOC, both equivalent, with 86%-87% efficacy
– Favorable response NHAP: 75% ertapenem vs 90% cefepime
– Of 103 with bacteriology: 81 gram negatives, 41 gram positives. Equivalent responses in all groups

31
Wenisch C, et al. Infection. 2006;34:190-195.
Pneumonia After Prior Antibiotic Therapy and Failure in CAP
• DESIGN– Prospective randomized trial of 63 patients hospitalized after
failing outpatient antibiotics for CAP – Moxifloxacin vs standard therapy
• PRIMARY OBJECTIVE– Clinical failure rates with therapy
• OUTCOMES– Clinical failure during therapy in 30% standard vs 6%
moxifloxacin (P=0.009)– 28-day failure in 21% standard vs 6% moxifloxacin (P=0.003)

32
Pneumonia After Prior Antibiotic Therapy and Failure in CAP
Wenisch C, et al. Infection. 2006;34:190-195.
Severity at the time of admission, laboratory data, outcome of treatment.
ParameterStandard Therapy (n=33)
Moxifloxacin Therapy (n=30) P Value
Leukocytes (g/L) 15.2 ± 121.5 13.2 ± 6.7 0.39
CRP (g/L) 127 ± 111 142 ± 92 0.34
PSI 118 ± 55 127 ± 36 0.23
Risk class at admission
I-III 11 (33%) 10 (30%) 0.58
IV-V 22 (67%) 20 (70%)
Admission to the ICU within 72 h 6 (18%) 8 (26%) 0.33
Failure of initial intra-hospital therapy during treatment
10 (30%) 2 (6%) 0.009

35
Bacteriology and Therapy of Severe NHAP Requiring Mechanical Ventilation
El Solh AA, et al. Am J Respir Crit Care Med. 2001;163:645-651.
• DESIGN
– Case series of 104 patients with severe pneumonia, including 47 from nursing homes
• PRIMARY OBJECTIVE
– Define natural history, bacteriology (usually bronchoscopic) and therapies
• OUTCOMES
– 57% mortality for NHAP vs 55% for CAP– Higher mortality with inadequate therapy (OR 2.6, P=0.034)– Common therapy: 2nd and 3rd gen cephs, BL/BLI, macrolide,
quinolone; 47% monotherapy and mortality the same as combination therapy

36
Bacteriology and Therapy of Severe NHAP Requiring Mechanical Ventilation
El Solh AA, et al. Am J Respir Crit Care Med. 2001;163:645-651.
Microorganisms Home, n (%) Nursing Home, n (%)
Streptococcus pneumoniae 8 (14) 4 (9)
Staphylococcus aureus 4 (7) 14 (29)
Methicillin-sensitive 4 (7) 11 (23)
Methicillin-resistant 0 3 (6)
Morexalla catarrhalis 2 (4) 1 (2)
Chlamydia pneumonaie 1 (2) 0
Enterococcus sp. 0 1 (2)
Hemophilus influenzae 4 (7) 1 (2)
Kebsiella pneumonia 2 (4) 3 (6)
The distribution of respiratory pathogens isolated from patients with severe pneumonia

40
Zilberberg et al Chest 2008; 134:963

41
Zilberberg et al Chest 2008; 134:963

HCAP mortality according to treatment
42
Zilberberg et al Chest 2008; 134:963

43
Zilberberg et al Chest 2008; 134:963

44
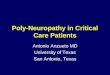
Are at least 2 present? Local Epidemics?
Severe:Treat for MDR pathogens
With HAP recommendationsNeed 3 drugs
Non-Severe:Treat for common CAP
Pathogens (consider oral rx)Quinolone,Beta-lactam/
Macrolide
Assess: Severity of Illness (ICU or Mechanical Ventilation) , Recent Antibiotic Therapy , Presence of Poor Functional Status
YESYESNONO
HCAP Is Present: From a nursing home, Home infusion Therapy,
Home wound care, Dialysis center, Hospitalized in past 90 days
Non-Severe:Treat for MDR pathogens
With HAP recommendations
Severe:Treat IV, consider hospitalBeta-lactam with Macrolide
Or Quinolone
Proposed Algorithm For HCAP Therapy

Obrigado, Muchas Gracias, Thank you
45