Embed Size (px)
Citation preview

1
Treatment of Fungal infections in Hematologic Malignancies
George Samonis M.D. PhD
Professor of Medicine
The University of Crete

22
Challenges of Diagnosing Opportunistic Infections at the Bedside

3
Challenges of Diagnosing Opportunistic Infections at the Bedside
3
Challenges of Diagnosing Opportunistic Infections at the Bedside

4
Usual fungal infections in immunocompromised patients
Candidiasis
Aspergillosis
Mucormycosis
Fusariosis
Cryptococcosis
Candidiasis
Aspergillosis
Mucormycosis
Fusariosis
Cryptococcosis

5
Risk factors for development of IFIs
Neutropenia
Lymphopenia
Corticosteroids
Immunosuppressives
Chemotherapy
Bone Marrow Transplantation
Broad-spectrum antibiotics
Mucositis
Parenteral alimentation
Central venous catheters (CVCs)
Hospital construction
Neutropenia
Lymphopenia
Corticosteroids
Immunosuppressives
Chemotherapy
Bone Marrow Transplantation
Broad-spectrum antibiotics
Mucositis
Parenteral alimentation
Central venous catheters (CVCs)
Hospital construction

6

7

8

9

10

11

12

13

14

15

16

17

18

19

20

21

22

23

24

25

26

27

28

29

30

31

32
Wingard1987
Wingard1987
O’Donnell1994
O’Donnell1994
Morrison1994
Morrison1994
Baddley2001
Baddley2001
Martino2002
Martino2002
Increased Incidence of Mould Infection
Martino R, Subira M. Ann Hematol. 2002;81:233-243. Martino R, Subira M. Ann Hematol. 2002;81:233-243.
Aspergillus sppAspergillus spp
1996-20001996-2000
1997-19981997-1998
1974-19891974-1989
1983-19891983-1989
1976-19851976-1985
4.0%4.0%
6.0%6.0%
11.4%11.4%13.0%13.0%
11.0%11.0%

33
Distribution of IA in the Post-Engraftment Phase of HSCT
Marr KA et al. Blood. 2002;100:4358-4366.Marr KA et al. Blood. 2002;100:4358-4366.
0%
10%
20%
30%
40%
50%
60%
30%30%
40-180(n=99)40-180(n=99)
>180(n=31)>180
(n=31)
Number of Days Post HSCTNumber of Days Post HSCT
Inci
den
ce o
f IA
in
HS
CT
Inci
den
ce o
f IA
in
HS
CT
53%53%
17%17%
<40(n=57)
<40(n=57)

34
Incidence of Aspergillosis in HSCT Recipients Is Growing
1-Year Cumulative Incidence of Aspergillosis at FHCRC* (%)1-Year Cumulative Incidence of Aspergillosis at FHCRC* (%)
Allograft recipientsAllograft recipients Autograft recipientsAutograft recipients
Data from 1990 through 1992 were obtained from another study.*FHCRC, Fred Hutchinson Cancer Research CenterAdapted from Marr KA et al. Clin Infect Dis. 2002;34:909-917.
Data from 1990 through 1992 were obtained from another study.*FHCRC, Fred Hutchinson Cancer Research CenterAdapted from Marr KA et al. Clin Infect Dis. 2002;34:909-917.
00
22
44
66
88
1010
1212
1414
19901990 19911991 19921992 19931993 19941994 19951995 19961996 19971997 19981998
Inci
den
ce (
%)
Inci
den
ce (
%)
YearYear

35
IA Risk
NeutropeniaNeutropenia
Invasive Aspergillosis Risk Increases During the Post-Engraftment Period
1. Marr KA. Oncology. 2001;15:15-19. 2. Hagen EA et al. Clin Infect Dis. 2003;36:9-15.1. Marr KA. Oncology. 2001;15:15-19. 2. Hagen EA et al. Clin Infect Dis. 2003;36:9-15.
Pre-engraftmentPre-engraftment
Immunosuppression:GVHD
CorticosteroidsDiminished T-cell function
Immunosuppression:GVHD
CorticosteroidsDiminished T-cell function
Post-engraftmentPost-engraftment
IA Risk

36
Aspergillus-Related Mortality in Allogeneic HSCT Remains Relatively High
31.6%*31.6%*
Lin 20011Lin 20011 Cornet 20022Cornet 20022 Thursky 20043Thursky 20043 Cordonnier 20064Cordonnier 20064 Upton 20075Upton 20075
87.0%87.0%
71.0%71.0% 68.0%68.0%
56.0%56.0%
1. Lin SJ et al. Clin Infect Dis. 2001;32:358-366. 2. Cornet M et al. J Hosp Infect. 2002;51:288-296. 3. Thursky K et al. Bone Marrow Transplant. 2004;34:115-121. 4. Cordonnier C et al. Clin Infect Dis. 2006;42:955-963. 5. Upton A et al. Clin Infect Dis. 2007;44:531-540.
1. Lin SJ et al. Clin Infect Dis. 2001;32:358-366. 2. Cornet M et al. J Hosp Infect. 2002;51:288-296. 3. Thursky K et al. Bone Marrow Transplant. 2004;34:115-121. 4. Cordonnier C et al. Clin Infect Dis. 2006;42:955-963. 5. Upton A et al. Clin Infect Dis. 2007;44:531-540.
Studies used crude mortality rate or attributable mortality rates. *Crude mortality rate at 4 months post IA diagnosis.Studies used crude mortality rate or attributable mortality rates. *Crude mortality rate at 4 months post IA diagnosis.

37
Pre-mortem
Chamilos 20062Chamilos 20062
The Majority of IFIs Are Identified Post-mortem
*Incidence of moulds and yeasts in AML patients (7.9% due to moulds). †Prevalence of invasive moulds and Candida (22% due to moulds).1. Pagano L et al. Haematologica. 2006;91:1068-1075. 2. Chamilos G et al. Haematologica. 2006;91:986-989.
*Incidence of moulds and yeasts in AML patients (7.9% due to moulds). †Prevalence of invasive moulds and Candida (22% due to moulds).1. Pagano L et al. Haematologica. 2006;91:1068-1075. 2. Chamilos G et al. Haematologica. 2006;91:986-989.
Post-mortem
33%†33%†
12.3%*12.3%*
Pagano 20061Pagano 20061
Only 1/4 Diagnosed Pre-mortem
Only 1/4 Diagnosed Pre-mortem
How Can We Better Identify Patients With
IFI During Life?

38
Invasive Aspergillosis Role of Early Diagnosis & Therapy
Have We Made Progress??

39
Non-Culture Based Diagnosis ofInvasive Aspergillosis
Galactomannan
– Sandwich ELISA (Platelia)
PCR
– 18s ribosomal DNA
– Multi-copy or single target genes
b-D-glucan
– Amebocyte Limulus lysate
– Chromogenic (Glucatell, FungiTec G)
– Kinetic (Wako)
Galactomannan
– Sandwich ELISA (Platelia)
PCR
– 18s ribosomal DNA
– Multi-copy or single target genes
b-D-glucan
– Amebocyte Limulus lysate
– Chromogenic (Glucatell, FungiTec G)
– Kinetic (Wako)

40
Early diagnosis and treatment of invasive aspergillosis
Impact of early diagnosis of IA in patients with acute leukemia:– 90% mortality when
treatment instigated ≥ 10 days after first clinical or radiological sign of disease
– 40% mortality when treatment is instigated early
Serial HR CT scanning:– early and systematic high
resolution CT scan in high-risk patients improves outcome
(von Eiff M, et al. Ann Hematol. 1995) (Reprinted with permission from Caillot D, et al. J Clin Oncol. 1997)
100
75
50
25
00 50 100 150 200
Days After IPA
Survival (%) IA: CT Scanning
Systematic CT
Non-Systematic CT
P = 0.006 (Logrank Test)

41
Relationship between hospital mortality and the timing of antifungal treatment
Ho
spit
al m
ort
alit
y (%
)
0
35
30
25
20
15
10
5
< 12
Delay in start of antifungal treatment (hours)
12–24 24–48 > 48
Morrell M, et al. Antimicrob Agents Chemother 2005; 49:3640–5

42
Patients with Satisfactory Treatment Response categorized by Baseline CT Findings
0%
10%
20%
30%
40%
50%
60%
70%
Satisfa
cto
ry R
esp
on
se (C
R/P
R)
Nodular lesion with Halo Nodular lesion without Halo*
ALL Treated
Vori Arm
Ampho Arm
42%
52%
41%
29%
16%
62%
*Note: Required positive mycologyGreene R et al. ECCMID 2003

43
Utility of Galactomannan Detection in BAL Samples
# pt
160
Sens
(%)
Spec
(%)
PPV
(%)
NPV
(%)
Serum 47 93 73 82
BAL 85 100 100 88
GM detection in CT-based BAL fluid has a high PPV for diagnosing IPA early in untreated patients
Becker et al. Br J Haematol 2003; 121: 448

44
Treatment definitions
Prophylactic therapy: Use of antifungals from chemotherapy until prolonged febrile neutropenia
Chance of infection: remote
Empirical therapy: Use of antifungals from febrile neutropenia to culture and/or tissue evidence of fungal infection
Chance of infection: possible
Preemptive therapy: Use of antifungals based on early clinical and/or laboratory markers of invasive disease
Chance of infection: probable
Prophylactic therapy: Use of antifungals from chemotherapy until prolonged febrile neutropenia
Chance of infection: remote
Empirical therapy: Use of antifungals from febrile neutropenia to culture and/or tissue evidence of fungal infection
Chance of infection: possible
Preemptive therapy: Use of antifungals based on early clinical and/or laboratory markers of invasive disease
Chance of infection: probable

45
Lack of Consensus on the Use of Empirical Antifungal Therapy
ProsPros
Development of resistance
ToxicityCost
Development of resistance
ToxicityCost
ConsCons
Reduces mortalityAddresses
diagnostic concerns
Reduces mortalityAddresses
diagnostic concerns
Broad-Spectrum antibiotics
>96 h
Broad-Spectrum antibiotics
>96 h
Persistent or recurring fever of unknown origin
>38C
Persistent or recurring fever of unknown origin
>38C
Persistent neutropenia Absolute neutrophil
count <500 cells/mm3
Persistent neutropenia Absolute neutrophil
count <500 cells/mm3
Wingard JR. N Engl J Med. 2002;346:225-234.Wingard JR. N Engl J Med. 2002;346:225-234.

46
Antifungal treatment evolution
AMB deoxycholate
5-fluocytosine
1st generation azoles (ketoconazole, miconazole)
2nd generation triazoles (fluconazole, itraconazole)
Lipid and liposomal formulations of AMB
Extended spectrum triazoles (voriconazole, posaconazole)
Echinocandins (caspofungin, micafungin, anidulafungin)
AMB deoxycholate
5-fluocytosine
1st generation azoles (ketoconazole, miconazole)
2nd generation triazoles (fluconazole, itraconazole)
Lipid and liposomal formulations of AMB
Extended spectrum triazoles (voriconazole, posaconazole)
Echinocandins (caspofungin, micafungin, anidulafungin)

47
Cellular Targets of Antifungal Therapy
Polyenes:Target membrane function
Echinocandins:Target cell wall synthesis
Azoles: Target ergosterol synthesis

48
Pts on azole prophylaxis
Pts with sinusitis or pneumonia
Pts with prolonged neutropenia (e.g. leukemia)
Pts with history of invasive aspergillosis (IA) or positive
surveillance cultures for Aspergillus spp.
Pts at institutions undergoing construction
Fluconazole: Not a good choice for empirical therapy in certain patients

49
L-AMB vs. AMB for empirical therapy of febrile neutropenia
Ambisome AMB
Patients 343 344
Acute Leukemia 168 165
Success 50 49
BFI (%) * 3.2 7.8
Infusion Fever (%) † 17 44
Nephrotoxicity (%) 19 34
* p=0.009 † p<0.001 Walsh NEJM 1999; 340:764

50
Polyene Therapy for Invasive Aspergillosis
Hiemenz JW et al. Blood 1995;86(suppl 1):849a; Leenders ACAP et al. Br J Haem 1998;103:205; Bowden RA et al. Clin Infect Dis 2002;35:359-66.
0
10
20
30
40
50
60
70
80
90
100
Hiemenz Salvage Leenders IncludesSuspected IA
Bowden Primary Tx
Lipid Formulation of AmB DAMB
Re
sp
on
se
%
HistoricalControl
23%
DAMB29% DAMB
23%ABCD18%
L-AMB52%ABLC
42%
Note: ABLC=amphotericin B lipid complex; L-AmB=liposomal amphotericin B; ABCD=amphotericin B colloidal dispersion; D-AMB=amphotericin B deoxycholate

51
Comparative Aspergillosis Study: Better Outcomes & Survival of Voriconazole
0 14 28 42 56 70 840.0
0.2
0.4
0.6
0.8
1.0
Number of days of Therapy
Pro
bab
ilit
y o
f S
urv
ival
Amphotericin B arm
Voriconazole arm
Hazard ratio = 0.6095% CI (0.40, 0.89)
• Outcomes at wk 12 Vori AmB
■ Survival 70.8% 57.9%■ Response 56.8% 31.6%
Poor efficacy of AmB prior “gold standard”
Vori recommended for primary therapy
• Questions?■ Role of Other Licensed
Antifungal therapy■ Lipid for primary therapy■ Efficacy in high risk■ Combinations
Herbrecht R et al NEJM 2002;347:408-15

52
Voriconazole vs. Ambisome in febrile neutropenia
Vorico
(N=415)
LAMB (N=422)
P
Composite success 26% 31% NS
Breakthrough fungal
infections 1.9% 5% 0.002
Survival rate 87% 90% NS
Toxicity-related withdrawal
13% 10% NS
Nephrotoxicity (SCr>1.5) 11% 19% <0.001
Visual changes 4.3% 0.5% <0.001
Walsh et al. N Engl J Med. 2002; 346: 225-34

53
Voriconazole: need for monitoring
ΒορικοναζόληΠότε χρειάζεται «monitoring»;
• Υποψία δυσαπορρόφησης (βλεννογονίτιδα, GvHD)
• Επιδείνωση νόσου
• Συγχορήγηση φαρμάκων που επάγουν το P-450
• Παχυσαρκία
• Παιδιατρικό πληθυσμό
• Rx > 30 μέρες
• Μετάβαση σε μονοθεραπεία από του στόματος
• Σε υποψία μη συμμόρφωσης στη θεραπεία
• Ανεξήγητη ηπατοτοξικότητα

54
Voriconazole Treatment
Cyclodextrin Toxicity
• Unmodified cyclodextrins, namely a- and b-cyclodextrins, are typically reabsorbed and concentrated in the renal tubule, interacting with and extracting cholesterol and other lipid membrane components from cellular structures.
• >300 mg/kg/d in rats produced reversible renal tubular vacuolation
• Human dose = 48 mg/kg/d (toxicity?)

55
Subtherapeutic Voriconazole - Omeprazole
Omeprazole = competitive inhibitor of CYP2C19
40 mg omeprazole daily Voriconazole AUC 141%

56
Posaconazole
Posaconazole: broad spectrum of activity
only oral formulation
variable absorption
variable bioavailability
Established for prophylaxis in acute leukemia and HSCT
Posaconazole: broad spectrum of activity
only oral formulation
variable absorption
variable bioavailability
Established for prophylaxis in acute leukemia and HSCT

57

58
Posaconazole
Παράγοντες που επηρεάζουν την απορρόφηση της ποσακοναζόλης
Posaconazole NDA. www.accessdata.fda.gov/
H2 ή PPI θεραπεία
Πτωχή απορρόφηση PO
Καταστροφή φραγμού
βλεννογόνων
GvHD (γαστρεντερικό σύστημα)
Σοβαρή διάρροιαΥποθεραπευτικέ
ς ή μη ανιχνεύσιμες συγκεντρώσειςποσακοναζόλης
Συμμόρφωση!

59
Echinocandins
· Latest class of antifungal drugs
First discovered in 1970s in screening
programs for new antibiotics
Cell-wall active agents:
nhibition of (1, 3)-β-D glucan synthetase cell wall glucan depletion
osmotic instability cell lysis
· Latest class of antifungal drugs
First discovered in 1970s in screening
programs for new antibiotics
Cell-wall active agents:
nhibition of (1, 3)-β-D glucan synthetase cell wall glucan depletion
osmotic instability cell lysis

60
Echinocandins
· Formerly known as Pneumocandins due to activity
against Pneumocystis carinii
· Rapidly fungicidal against most Candidae including azole-resistant strains
· Fungistatic against most Aspergillus spp
· Limited or no activity against Fusarium spp and Zygomycetes.
· No activity against Cryptococcus neoformans
· Formerly known as Pneumocandins due to activity
against Pneumocystis carinii
· Rapidly fungicidal against most Candidae including azole-resistant strains
· Fungistatic against most Aspergillus spp
· Limited or no activity against Fusarium spp and Zygomycetes.
· No activity against Cryptococcus neoformans

61
Mechanism of action1-4
1- ECALTA® SPC. 2- Odds F.C., Brown A.J.P., Gow N.A.R. Antifungal agents: mechanism of action. Trends Microbiol. 2003;11:272-279. 3- Debono M., Turner W.W., LaGrandeur L. et al. Semisynthetic chemical modification of the antifungal lipopeptide echinocandin B (ECB): structure-activity studies of the lipophilic and geometric parameters of polyarylated acyl analogs of ECB. J Med Chem. 1995;38(17):3271-3281. 4- Raasch R.H. Anidulafungin: review of a new echinocandin antifungal agent. Expert Rev Anti Infect Ther. 2004;2:499-508.
Mechanism of action involves a target specific for fungus4
inhibitor of 1,3--D-glucan synthase1
Enzyme is present in fungal, but not mammalian, cells1
Glucan is essential to fungal cell wall integrity2-4
Without it, fungal cells are osmotically fragile and easily lysed4

62
Echinocandins
· IV administration
· Long half life
CNS penetration: poor
Dose: once daily
Little infusion related toxicity
Little or no renal and hepatic toxicity
Drug-drug interaction limited (cyclosporin)
Potential combination with other antifungals (AMB or azoles)
· Animal data suggest synergistic effect
· Echinocandins: Caspofungin Anidulafungin Micafungin
· IV administration
· Long half life
CNS penetration: poor
Dose: once daily
Little infusion related toxicity
Little or no renal and hepatic toxicity
Drug-drug interaction limited (cyclosporin)
Potential combination with other antifungals (AMB or azoles)
· Animal data suggest synergistic effect
· Echinocandins: Caspofungin Anidulafungin Micafungin

63
Echinocandins : In vitro activity1
1- Cappelletty D. et al. Reviews of therapeutics : the echinocandins Pharmacotherapy 2007, 27(3):369-388.
Anidulafungin Micafungin* Caspofungin
Candida species MIC50(µg/ml)
MIC90(µg/ml)
MIC50(µg/ml)
MIC90(µg/ml)
MIC50(µg/ml)
MIC90(µg/ml)
albicans 0.03 0.03 0.015-0.03 0.03 0.03-0.5 0.06-1
glabrata 0.03 0.13 0.015-0.03 0.015-0.06 0.03-1 0.06-2
tropicalis 0.03 0.13 0.03 0.06 0.12-0.5 0.25-1
dubliniensis 0.03 0.06 0.03 0.033 0.25-0.5 0.5
krusei 0.06 0.13 0.06-0.13 0.06-0.25 0.12-2 0.25-2
lusitaniae 0.06 0.25 0.06 2 0.5-1 1-2
parapsilosis 2 2 1 2 1-2 1-4
guilliermondii ND 1 ND 0.5 2 -> 8 2 -> 8
Minimum inhibitory concentrations of the echinocandins against Candida species
MIC50 or MIC90 = minimum inhibitory concentration for 50% or 90%, respectively, of tested strains; ND = not done.

64
Caspofungin in Invasive Aspergillosis
• Well-documented disease• Efficacy
– High risk pts
– Progressive infection
– Multiple prior antifungals
•Excellent tolerability
•Clinical utility
– No data for primary therapy
– Combination therapy
– Optimal dose not known
• Well-documented disease• Efficacy
– High risk pts
– Progressive infection
– Multiple prior antifungals
•Excellent tolerability
•Clinical utility
– No data for primary therapy
– Combination therapy
– Optimal dose not known
Maertens J, et al. Clin Infect Dis 2004;39:1563-71
Proven/Probable IA
41
17
0
20
40
60
80
100
Caspofungin(n=56)
HistoricalControls (n=206)
CR
/PR
(%
)
%
%

65
Caspo (556) L-AmB (539)
Composite Success 33.9% 33.7%
Success Baseline Infections 14/27 (52%) 7/27 (26%)
Breakthrough Infections 29 (5.2%) 24 (4.5%)
Etiological Agents*
Aspergillus 10 9
Candida 16 15
Fusarium 1 0
Zygomycetes 2 0
Other 1 1
Caspo (556) L-AmB (539)
Composite Success 33.9% 33.7%
Success Baseline Infections 14/27 (52%) 7/27 (26%)
Breakthrough Infections 29 (5.2%) 24 (4.5%)
Etiological Agents*
Aspergillus 10 9
Candida 16 15
Fusarium 1 0
Zygomycetes 2 0
Other 1 1
Efficacy of Caspofungin vs Empirical L-AmB in Neutropenic Patients*
Walsh TJ et al, New Eng J Med, 2004;351:1391-1402
*Patients may have had more than one organism

66
Anidulafungin
Clinical data
Anidulafungin vs Fluconazole
Reboli A.C. et al.
Anidulafungin versus Fluconazole for Invasive Candidiasis.
N Engl J Med 2007;356:2472-82.

67
Global success at the end of IV therapy
ECALTA® demonstrated superiority vs fluconazole:
• Significantly greater response rate in the anidulafungin group
• Difference: 15.4% (95% CI: 3.9% to 27.0%)
Mean (median) duration of IV therapy:
fluconazole: 12.1 (11) days
anidulafungin: 13.5 (14) days
Primary endpoint1
1- Reboli A.C., Rotstein C., Pappas P.G. et al. Anidulafungin versus Fluconazole for Invasive Candidiasis. N Engl J Med 2007;356:2472-82.

68
*2.0 mg/kg/day in patients weighing ≤ 40 kg†Treatment continued until at least one week after resolution of clinical signs and symptoms and obtaining of two sequential negative blood cultures‡Maximum 8 weeks in chronic disseminated candidiasis, Candida osteomyelitis or Candida endocarditis
Micafungin 100 mg/day* L-AmB 3 mg/kg/day
Treatment period† 2–4 weeks‡
Randomisation(1:1)
12 weeksPost-treatment period
Phase III study micafungin vs. L-AmB Study design
Kuse ER, et al. Lancet 2007; 369:1519–27

69
Phase III study micafungin vs. L-AmB Overall treatment success
Kuse ER, et al. Lancet 2007; 369:1519–27 mITT = modified intent-to-treat; PP = per-protocol set
Trea
tmen
t su
cces
s ra
te (
%)
74.1
89.6
69.6
89.5
0
20
40
60
80
100
mITT PP
Micafungin L-AmB
n = 247 247 202 190

70
*70 mg loading dose on Day 1†8 weeks in chronic disseminated candidiasis or Candida endophthalmitis; switch to oral fluconazole permitted after 10 days in patients meeting protocol-specified criteria‡Time from last dose day of protocol-defined antifungal therapy to final evaluation
Micafungin 100 mg/day
CAS 50 mg/day*
Treatment period† Max 4 weeks†
Randomisation(1:1:1)
6 weeks‡Post-treatment period
Phase III study micafungin vs. caspofungin Study design
Micafungin 150 mg/day
Pappas PG, et al. Clin Infect Dis 2007; 45:883–93 CAS = caspofungin
Patients were stratified by region and APACHE II score (≤ 20 or > 20)

71
Phase III study micafungin vs. caspofungin Treatment success
Pappas PG, et al. Clin Infect Dis 2007; 45:883–93
n = 191 n = 188n = 199
Caspofungin50 mg/day*
Trea
tmen
t su
cces
s ra
te (
%) 76.4
71.4 72.3
0
20
40
60
80
n = 191 199 188
Micafungin100 mg/day
Micafungin150 mg/day
*Loading dose 70 mg; mITT population

72
Micafungin vs Caspofungin in febrile neutropenia

73
Conclusions
Micafungin as effective and safe as caspofungin in empirical treatment of fungal infections in patients with febrile neutropenia
Conclusions
Micafungin as effective and safe as caspofungin in empirical treatment of fungal infections in patients with febrile neutropenia
Micafungin vs Caspofungin in febrile neutropenia

74
Empirical micafungin treatment of IFIs in hematologic malignancies

75
Empirical micafungin treatment of IFIs in hematologic malignancies
Efficacy
Micafungin monotherapy: 66,1% (109/165)
Mica + Ampho B and / or azoles: 78,1% (25/32)
΄΄For the patients who were in grave conditions and suffered from probable to
proven IFIs, combination of micafungin and azoles or amphotericin B could be considered.΄΄
Efficacy
Micafungin monotherapy: 66,1% (109/165)
Mica + Ampho B and / or azoles: 78,1% (25/32)
΄΄For the patients who were in grave conditions and suffered from probable to
proven IFIs, combination of micafungin and azoles or amphotericin B could be considered.΄΄

76
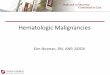
Micafungin vs fluconazole for prophylaxis of invasive fungal infections during neutropenia in hematopoietic stem cell transplantation patients Study endpoints
Primary endpoint: treatment success (absence of proven, probable, or suspected systemic fungal infection until the end of prophylaxis therapy and the absence of a proven or probable systemic fungal infection until the end of the 42-day post-treatment period)
Secondary endpoints included: use of systemic antifungal agents for treatment of suspected fungal infections; frequency of proven or probable fungal infections throughout the post-treatment period; pathogen-based frequency of proven infections
Primary endpoint: treatment success (absence of proven, probable, or suspected systemic fungal infection until the end of prophylaxis therapy and the absence of a proven or probable systemic fungal infection until the end of the 42-day post-treatment period)
Secondary endpoints included: use of systemic antifungal agents for treatment of suspected fungal infections; frequency of proven or probable fungal infections throughout the post-treatment period; pathogen-based frequency of proven infections
van Burik JA, et al. Clin Infect Dis 2004; 39:1407–16

77
Phase III study micafungin vs. fluconazole Overall treatment success
Trea
tmen
t su
cces
s (%
)
van Burik JA, et al. Clin Infect Dis 2004; 39:1407–16
p = 0.03
Micafungin Fluconazole
80.073.5
0
10
20
30
40
50
60
70
80
90
Micafungin Fluconazole
n = 425 457

78
Is combination of antifungals indicated?

79
Randomized blinded trial of high-dose fluconazole plus placebo vs fluconazole plus AMB as therapy for candidemia in non-neutropenic patients.
The combination of fluconazole and AMB was evaluated versus monotherapy with high-dose fluconazole in 219 non-neutropenic patients
No difference in survival between the two groups; however, candidemia cleared more rapidly with combination therapy, suggesting potential use in persistent Candida infections
Rex JH, et al. Clin Infect Dis 2003; 36:1221-8
The combination of fluconazole and AMB was evaluated versus monotherapy with high-dose fluconazole in 219 non-neutropenic patients
No difference in survival between the two groups; however, candidemia cleared more rapidly with combination therapy, suggesting potential use in persistent Candida infections
Rex JH, et al. Clin Infect Dis 2003; 36:1221-8

80
. Efficacy and Toxicity of Caspofungin in Combination with L-AMB as Primary or Salvage treatment of Invasive Aspergillosis in Patients with Hematologic Malignancies. Kontoyiannis DP, et al Cancer 2003; 98: 292-9
48 patients with documented or possible IA
The majority (65%) received CAS/L-AMB as salvage therapy for progressive IA despite 7 days of previous L-AMB monotherapy
Overall response rate 42%
No significant toxicity
Factors associated with failure: documented IA, significant steroid use, duration of combination therapy < 14 days
Response rate in patients with progressive documented IA 18%
Conclusions: The CAS/L-AMB combination is a promising preemptive therapy
48 patients with documented or possible IA
The majority (65%) received CAS/L-AMB as salvage therapy for progressive IA despite 7 days of previous L-AMB monotherapy
Overall response rate 42%
No significant toxicity
Factors associated with failure: documented IA, significant steroid use, duration of combination therapy < 14 days
Response rate in patients with progressive documented IA 18%
Conclusions: The CAS/L-AMB combination is a promising preemptive therapy

81
Combination antifungal therapy for invasive aspergillosis. Marr KA, et al. Clin Infect Dis. 2004; 39: 797-802
Salvage therapy with the combination of voriconazole and caspofungin was associated with reduced mortality, compared with voriconazole monotherapy
Salvage therapy with the combination of voriconazole and caspofungin was associated with reduced mortality, compared with voriconazole monotherapy

82

83

84
Br J Haematol. 2004; 126: 165-75

85
Conclusions
Patients at high risk may benefit from empirical therapy
Patients under close surveillance may receive preemptive treatment after early prodromal clues of infection
No clear drug of choice, decisions should be individualized
Lipid AMB, voriconazole and echinocangins: high risk pts
Fluconazole, itraconazole: lower risk pts
Limited data point out to combination treatments for selected high risk pts
Patients at high risk may benefit from empirical therapy
Patients under close surveillance may receive preemptive treatment after early prodromal clues of infection
No clear drug of choice, decisions should be individualized
Lipid AMB, voriconazole and echinocangins: high risk pts
Fluconazole, itraconazole: lower risk pts
Limited data point out to combination treatments for selected high risk pts

86
Future issues
Should we move from empirical to preemptive therapy based on surrogate markers of early diagnosis of IFIs?
Is sequence of antifungals important?
Which combinations are more effective?

87