Embed Size (px)
Citation preview

1
Tonsillectomy, and Tonsillectomy, and AdenoidectomyAdenoidectomy

04/18/23 [email protected] 2
HistoryHistory
• Celsus 50 A.D.
• Caque of Rheims
• Philip Syng
• Wilhelm Meyer 1867
• Samuel Crowe

04/18/23 [email protected] 3
EmbryologyEmbryology
• 8 weeks: Tonsillar fossa and palatine tonsils develop from the dorsal wing of the 1st pharyngeal pouch and the ventral wing of the 2nd pouch; tonsillar pillars originate from 2nd/3rd arches
• Crypts 3-6 months; capsule 5th month; germinal centers after birth
• 16 weeks: Adenoids develop as a subepithelial infiltration of lymphocytes

04/18/23 [email protected] 4
AnatomyAnatomy
TonsilsTonsils• Plica triangularis• Gerlach’s tonsil
AdenoidsAdenoids• Fossa of Rosenmüller• Passavant’s ridge
04/18/23 [email protected] 5
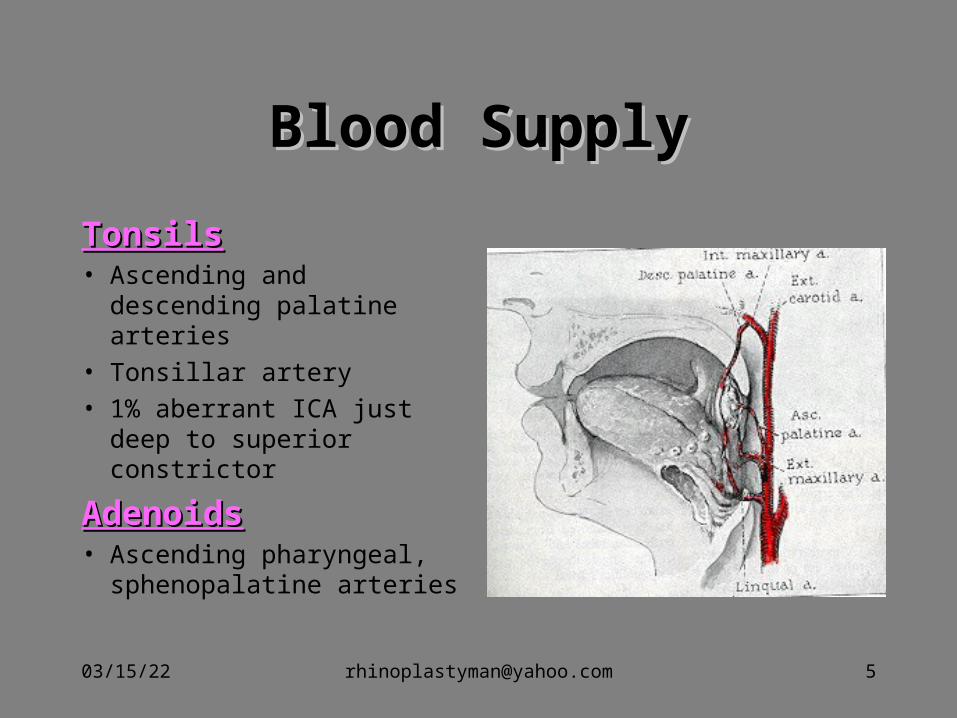
Blood SupplyBlood Supply
TonsilsTonsils• Ascending and descending
palatine arteries
• Tonsillar artery
• 1% aberrant ICA just deep to superior constrictor
AdenoidsAdenoids• Ascending pharyngeal,
sphenopalatine arteries

04/18/23 [email protected] 6
Common Diseases of the Common Diseases of the Tonsils and AdenoidsTonsils and Adenoids
• Acute adenoiditis/tonsillitis
• Recurrent/chronic adenoiditis/tonsillitis
• Obstructive hyperplasia
• Malignancy

04/18/23 [email protected] 7
Acute AdenotonsillitisAcute Adenotonsillitis
Etiology
• 5-30% bacterial; of these 39% are beta-lactamase-producing (BLPO)
• Anaerobic BLPO
GABHS most important pathogen because of potential sequelae
• Throat culture
• Treatment

04/18/23 [email protected] 8
Microbiology of Microbiology of AdenotonsillitisAdenotonsillitis
Most common organisms cultured from patients with chronic tonsillar disease (recurrent/chronic infection, hyperplasia):
• Streptococcus pyogenes (Group A beta-hemolytic streptococcus)
• H.influenza
• S. aureus
• Streptococcus pneumoniae
Tonsil weight is directly proportional to bacterial load.

04/18/23 [email protected] 9
Acute AdenotonsillitisAcute Adenotonsillitis
Differential diagnosisInfectious mononucleosisMalignancy: lymphoma, leukemia, carcinomaDiptheriaScarlet feverAgranulocytosis

04/18/23 [email protected] 10
Medical ManagementMedical Management• PCN is first line, even if throat culture is negative for
GABHS• For acute UAO: NP airway, steroids, IV abx, and immediate
tonsillectomy for poor response• Recurrent tonsillitis: PCN injection if concerned about
noncompliance or antibiotics aimed against BLPO and anaerobes
• For chronic tonsillitis or obstruction, antibiotics directed against BLPO and anaerobes for 3-6 weeks will eliminate need for surgery in 17%
• Co-amoxiclav or clindamycin or PCN+Rifampin

04/18/23 [email protected] 11
Obstructive HyperplasiaObstructive Hyperplasia
• Adenotonsillar hypertrophy most common cause of SDB in children
• Diagnosis:snoring, restless sleep, FTT, daytime symptoms… poor mentation, decreased attn span, poor scholastic performance, dysphagia, nocturnal enuresis, chronic mouth breathing
• Indications for polysomnography• Interpretation of polysomnography• Perioperative considerations

• Interpretation of polysomnography:
Indications for surgical intervention
>1 apnea in 1 hour
Central apnea + o2sat<90%
O2sat<92%
CO2>53
CO2>45 in more than 60% of test time
04/18/23 [email protected] 12

04/18/23 [email protected] 13
Unilateral Tonsillar Unilateral Tonsillar EnlargementEnlargement
Apparent enlargement vs true enlargement
Non-neoplastic: • Acute infective• Chronic infective • Hypertrophy• Congenital
Neoplastic

04/18/23 [email protected] 17
Other Tonsillar PathologyOther Tonsillar Pathology
• Hyperkeratosis, mycosis leptothrica
• Tonsilloliths
04/18/23 [email protected] 21
Indications for Tonsillectomy; Indications for Tonsillectomy; Historical EvolutionHistorical Evolution

04/18/23 [email protected] 22
Indications for TonsillectomyIndications for Tonsillectomy
Paradise study • Frequency criteria: 7 episodes in 1 year or 5
episodes/year for 2 years or 3 episodes/year for 3 years
• Clinical features (one or more): T 38.3, cervical LAD (>2cm) or tender LAD; tonsillar/pharyngeal exudate; positive culture for GABHS; antibiotic treatment
04/18/23 [email protected] 23
Indications for TonsillectomyIndications for Tonsillectomy
AAO-HNS:• 3 or more episodes/year• Hypertrophy causing malocclusion, UAO• PTA unresponsive to nonsurgical mgmt• Halitosis, not responsive to medical therapy• UTE, suspicious for malignancy• Individual considerations

04/18/23 [email protected] 24
Also:1.Recurrent tonsillitis in patient with heart valve dis2.In patient with febrile convulsion3.Unresponsive carrier 4.Obstructive IMN unresponsive to medical therapy5.Carrier of diphtheria6.Chronic tonsillitis with never-ending sore throat7.OSAS8.FTT9.Disphagia10.phonation disorders11.Malocclusion12.Craniofacial growth abnormalities13.Corpulmonale14.Suspicious malignancy

04/18/23 [email protected] 25
Pathophysiology of corpulmonale in OSA:
1.URT obstruction2.Alveolar hypovantilation3.Chronic hypoxia and hypercapnea4.Respiratory acidosis5.Vasoconstriction of alveolar capillaries6.Right atrial dilatation7.Pulmonary hypertension 8.Corpulmonale and CHF
04/18/23 [email protected] 26
Pathophysiology of enuresis:1.SDB 2.REM abnormalities3.Irregularities in ADH secretion
Pathophysiology of FTT:1.SDB2.REM abnormalities3.Irregularities in GH secretion, may sometimes stop totally
Both return to normal following A&T

04/18/23 [email protected] 27
ADHD (Attention Deficit Hyperactivity Disorder) is the mostCommon psychiatric diagnosis in children.
In direct correlation with Sleep Disordered Breathing(SDB)
Pathophysiology uncertain, Maybe due to abnormal sleep pattern
Neurocognitive development delays:Healthy sleeping pattern: important component of brain growthFrontal cortex growth continues up to pubertyMost critical age: 3-7

04/18/23 [email protected] 28
Indications for AdenoidectomyIndications for Adenoidectomy
Paradise study • 28-35% fewer acute episodes of OM with adenoidectomy in
kids with previous tube placement
• Adenoidectomy or T & A not indicated in children with recurrent OM who had not undergone previous tube placement
Gates et al • Recommend adenoidectomy with M & T as the initial
surgical treatment for children with MEE > 90 days and CHL > 20 dB

04/18/23 [email protected] 29
Indications for AdenoidectomyIndications for Adenoidectomy
Obstruction:• Chronic nasal obstruction or obligate mouth breathing
• SDB with FTT, cor pulmonale
• Dysphagia
• Speech problems
• Severe orofacial/dental abnormalities
Infection:• Recurrent/chronic adenoiditis (3 or more episodes/year)
• Recurrent/chronic OME (+/- previous BMT)

Also:
• Chronic sinusitis: first step
biofilm in 95% adenoid specimen vs. 2% in SDB
• Chronic recurrent AOM
• COM
• Chronic otorrhea
• VT and persistent discharge
• Suspecious malignancy
04/18/23 [email protected] 30

04/18/23 [email protected] 31
PreOp Evaluation ofPreOp Evaluation of Adenoid Adenoid DiseaseDisease
• Triad of hyponasality, snoring, and mouth breathing
• Rhinorrhea, nocturnal cough, post nasal drip
• “Adenoid facies”• “Milkman” & “Micky
Mouse”• Overbite, long face,
crowded incisors

04/18/23 [email protected] 32
PreOp Evaluation of Adenoid PreOp Evaluation of Adenoid DiseaseDisease
Differential diagnoses• Allergic rhinitis
• Sinusitis
• GERD
• For concomitant sinus disease, treat adenoids first

04/18/23 [email protected] 33
PreOp Evaluation of Adenoid PreOp Evaluation of Adenoid DiseaseDisease
Evaluate palate• Symptoms/FH of CP or
VPI• Midline diastasis of
muscles, bifid uvula• CNS or neuromuscular
disease
• Preexisting speech disorder?

04/18/23 [email protected] 34
PreOp Evaluation of Adenoid PreOp Evaluation of Adenoid DiseaseDisease
Lateral neck films are useful only when history and physical exam are not in agreement.
Accuracy of lateral neck films is dependent on proper positioning and patient cooperation.
04/18/23 [email protected] 35
PreOp Evaluation of Adenoid PreOp Evaluation of Adenoid DiseaseDisease

04/18/23 [email protected] 36
PreOp Evaluation of Tonsillar PreOp Evaluation of Tonsillar DiseaseDisease
History• Documentation of episodes by physician
• FTT
• Cor pulmonale
• Poststreptococcal GN
• Rheumatic fever
04/18/23 [email protected] 37
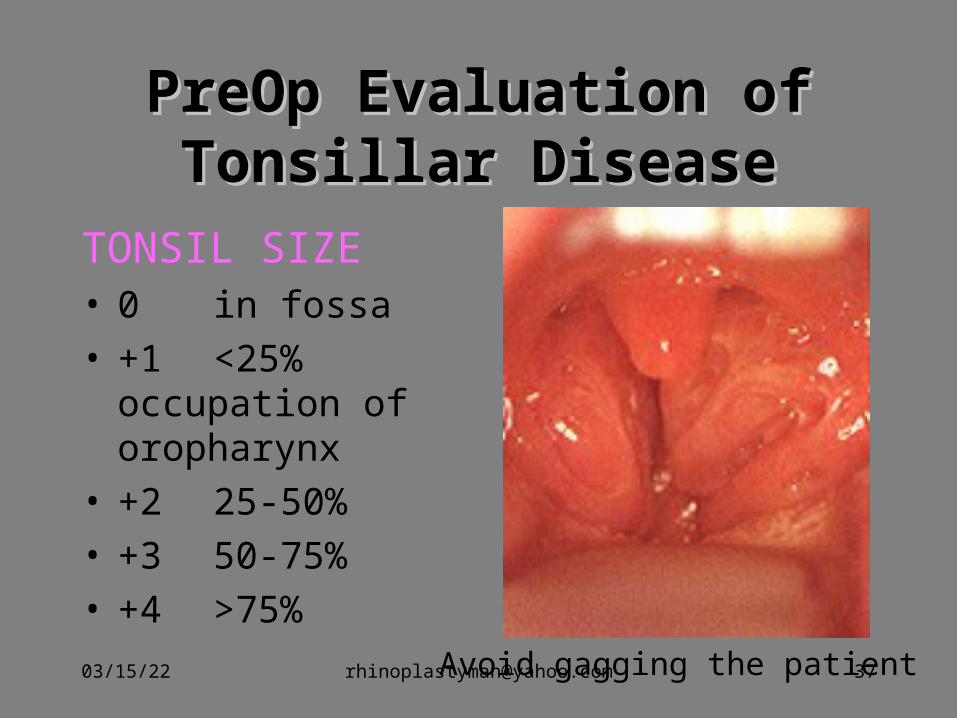
PreOp Evaluation of Tonsillar PreOp Evaluation of Tonsillar DiseaseDisease
TONSIL SIZE• 0 in fossa• +1 <25%
occupation of oropharynx
• +2 25-50%• +3 50-75%• +4 >75%
Avoid gagging the patient

04/18/23 [email protected] 38
PreOp Evaluation of Tonsillar PreOp Evaluation of Tonsillar DiseaseDisease
Down syndrome• 10% have AtlantoAxial laxity
• Obtain lateral cervical films (flexion/extension) when positive findings on history, PE
• If unstable, need neurosurgical evaluation preoperatively
• Large tongue and small mandible… difficult intubation
• Prone to cardiac arrhythmias/hypotension during induction

04/18/23 [email protected] 39
PreOp Evaluation for PreOp Evaluation for Adenotonsillar DiseaseAdenotonsillar Disease
Coagulation disorders• Historical screening
• CBC, PT/PTT, BT, vWF activity
• Hematology consult
• von Willebrand’s disease
• ITP
• Sickle cell anemia
04/18/23 [email protected] 40
Principles of Surgical Principles of Surgical ManagementManagement
Numerous techniques:
• Guillotine
• Tonsillotome
• Beck’s snare
• Dissection with snare (Scissor dissection, Fisher’s knife dissection, Finger dissection
• Electrodissection
• Laser dissection (CO2, KTP)
• Coblation
• RadioFrequency
… Surgeon’s preference
04/18/23 [email protected] 41
Post Operative ManagmentPost Operative Managment
Criteria for Overnight Observation• Poor oral intake, vomiting, hemorrhage• Age < 3• Home > 45 minutes away• Poor socioeconomic condition• Comorbid medical problems• Surgery for OSA or PTA• Abnormal coagulation values (+/- identified disorder)
in patient or family member
04/18/23 [email protected] 42
ComplicationsComplications
#1 Postoperative bleeding
Other:• Sore throat, otalgia, uvular swelling
• Respiratory compromise
• Dehydration
• Burns and iatrogenic trauma
• Dental problems and trauma

04/18/23 [email protected] 43
Rare ComplicationsRare Complications
• Velopharyngeal Insufficiency• Nasopharyngeal stenosis• Atlantoaxial subluxation/ Grisel’s syndrome• Regrowth• Eustachian tube injury• Depression• Laceration of ICA/ pseudoaneursym of ICA

04/18/23 [email protected] 44
Management of HemorrhageManagement of Hemorrhage
• Ice water gargle, afrin
• Overnight observation and IV fluids
• Dangerous induction
• ECA ligation
• Arteriography

04/18/23 [email protected] 45

04/18/23 [email protected] 46

04/18/23 [email protected] 47
Case study
• 13 year old female referred by PCP for frequent throat infections
• “She’s always sick. She’s been on four different antibiotics this year.”
• You call her pediatrician… he is out of town and his nurse can’t find the chart

04/18/23 [email protected] 48
Case study
• No known medical problems, no prior surgical procedures
• Takes motrin for menustrual cramps
• No personal history of bleeding other than occasional nose bleeds and extremely heavy periods.
• Family history unknown. Patient is adopted.
04/18/23 [email protected] 49
Case study• Physical exam is unremarkable. • Mom breaks down in tears when you tell her you
do not have enough documentation of illness to warrant T & A. “I had to go on welfare because I’ve missed so much work from her being out sick.”
• You hesitate. She adds, “Her grades have dropped from all A’s to all F’s. If she misses any more school, she’ll be held back.”
04/18/23 [email protected] 50
Case study• You confirm with her pediatrician that she has had
4 episodes of tonsillitis this year and agree to T & A.
• Because of her history of epistaxis and menorrhagia, you order a PT, PTT, CBC, BT.
• She has a mild microcytic anemia and prolonged bleeding time.
• You order vWF activity level and consult hematology

04/18/23 [email protected] 51
Case study
• She has a subnormal level of vWF, which responds to a DDAVP challenge (rise in vWF and Factor VII greater than 100%).
• You advise her to stop taking motrin.
• Before surgery, she receives desmopressin 0.3 microg/kg IV over 30 min and amicar 200mg/kg.

04/18/23 [email protected] 52
Case study
• She receives the same dose of DDVAP 12 hours postoperatively and every morning.
• Amicar is given 100mg/kg PO q 6 hr.
• Before each dose of DDAVP, serum sodium is drawn. Sodium levels drop to 130.
• Desmopressin is discontinued and substituted with cryoprecipitate.
04/18/23 [email protected] 53
Case study
• Patient presents to the ER on POD # 7 complaining of intermittent bleeding from her mouth.
• You order cryoprecipitate, draw a Factor VII level and CBC, and call her hematologist.
• Hemoglobin has dropped from 11.9 to 9.6.

04/18/23 [email protected] 54
Case study
• PE reveals no active bleeding; an old clot is present
• You establish IV access, admit the patient for overnight observation, have her gargle with ice water, and administer crypoprecipitate
• No further bleeding occurs, patient is discharged the next day