Embed Size (px)
Citation preview
1 TITLE PAGE
TITLE OF STUDY: Clinical Efficacy of a Sonic Power Toothbrush in Adults with Plaque and Gingivitis in a Thirty-Day Model
INVESTIGATIONAL MATERIALS:
Manual toothbrush: ADA reference manual soft-bristled toothbrush (Colgate® Classic [Pokey], Colgate-Palmolive Co., New York, NY) and ADA Accepted 0.243% sodium fluoride CREST® Cavity Protection toothpaste (Procter & Gamble, Cincinnati, OH, USA) Sonic toothbrush: BURST sonic power toothbrush (BURST.USA inc, Walnut, CA; brushing mode: whitening) and ADA Accepted 0.243% sodium fluoride CREST® Cavity Protection toothpaste (Procter & Gamble, Cincinnati, OH, USA)
Sponsor: BURST.USA.inc 340 S. Lemon Avenue #4658 Walnut, CA 91789
Protocol No.: PTB-001-2019
Investigator: Jeffrey L. Milleman, DDS, MPA Salus Research, Inc. 1220 Medical Park Drive, Building #4 Fort Wayne, Indiana 46825
Study period: First Subject First Visit: 06 August 2019 Last Subject Last Visit: 06 September 2019
GCP Statement: This study was performed in compliance with ICH Good Clinical Practice (GCP) including the archiving of essential documents.
Date of report: 24 October 2019
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 1 of 177
Signature Page for Clinical Study Report
I have read this report and confirm that to the best of my knowledge it accurately describes the conduct and results of the study.
Principal Investigator:
Signed: Date:
Jeffrey L. Milleman, DDS, MPA Salus Research, Inc. 1220 Medical Park Drive, Building #4 Fort Wayne, Indiana 46825
Sponsor Representative:
Signed: Date:
Brittany Stewart Chief Operating Officer BURST.USA.inc 340 S. Lemon Avenue #4658 Walnut, CA 91789
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 2 of 177
11/01/2019


1 TITLE PAGE ............................................................................................................................... 1
2 SYNOPSIS REPORT .................................................................................................................... 6
2.2 INTRODUCTION ................................................................................................................ 6
2.3 METHODOLOGY ............................................................................................................... 7
2.4 STATISTICAL METHODS .................................................................................................... 9
3 SUMMARY RESULTS AND CONCLUSIONS .............................................................................. 10
3.1 SAFETY RESULTS ............................................................................................................. 12
3.2 EFFICACY RESULTS .......................................................................................................... 12
3.3 DISCUSSION .................................................................................................................... 20
3.4 CONCLUSION .................................................................................................................. 21
3.5 REFERENCES ................................................................................................................... 22
4 APPENDICES ........................................................................................................................... 25
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 3 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 3 of 177

ABSTRACT
Clinical Efficacy of a Sonic Power Toothbrush in Adults with Plaque and Gingivitis in a Thirty-Day Model
Objective: This 30-day, randomized, controlled, single-center, examiner-blind, parallel design clinical trial evaluated the efficacy of a marketed sonic power toothbrush (BURST Sonic) on plaque and gingivitis, compared to a manual toothbrush. Methods: Upon meeting eligibility criteria, a total of 94 generally healthy subjects with mild to moderate plaque and gingivitis levels were randomly assigned to one of two treatment groups: 1) twice daily brushing in usual manner with an ADA reference flat trim manual toothbrush andstandard 0.243% sodium fluoride Crest® Cavity Protection toothpaste (control group); 2) Twicedaily brushing for a total of 2 minutes with a BURST Sonic power toothbrush and standard0.243% sodium fluoride Crest® Cavity Protection toothpaste (sonic toothbrush group). In total,92 subjects completed the study. At baseline, Day 15 (± 2 days) and Day 30 (± 2 days), subjectsrefrained from oral hygiene for approximately 8 – 12 hours prior to each exam visit, received aclinical oral examination for oral safety, and were assessed for gingivitis according to theModified Gingival Index (MGI), gingival bleeding according to the Bleeding Index (BI) andsupragingival plaque levels according to the Lobene-Soparkar Modification of the TureskyModification of the Quigley-Hein Plaque Index (PI). Following the supervised use of the assignedproducts at baseline, subjects were examined again for post-brushing plaque removal.Treatment means and between-treatment means were assessed by the ANCOVA model.Results: There were no treatment-related oral adverse events identified during the studydemonstrating that all treatment materials were well-tolerated. For the 92 evaluable subjects,there were no significant differences between groups for demographics or for the baselineefficacy variables. Statistically significant reductions in gingivitis, bleeding, and plaque wereobserved for the sonic toothbrush group compared to the manual toothbrush control at Days15 and 30 (p<0.001). Mean MGI was reduced from baseline by 35.7% and 33.4% for the sonictoothbrush and by 10.3% and -3.7% for the manual toothbrush group at Days 15 and 30,respectively. Using the sonic toothbrush resulted in an average of 35.71 (Day 15) and 32.91(Day 30) more healthy gingival sites (MGI) than at baseline. Mean BI scores were reduced frombaseline by 64.8% and 66.3% for the sonic toothbrush as compared with 16.2% and 20.3% forthe manual toothbrush control. The baseline Pre- to post-brushing whole mouth, gumline, andinterproximal plaque reductions for the sonic toothbrush group were 20.9%, 37.5% and 14.0%,respectively. Compared to the manual toothbrush, improvements in baseline post-brushingwhole mouth and gumline plaque scores for the sonic toothbrush were significantly better(p<0.05) with 33% greater improvement in plaque removal. At Days 15 and 30, mean wholemouth PI reductions from baseline were 8.9% and 11.4% for the sonic toothbrush and 0.8% and1.1% for the manual toothbrush.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 4 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 4 of 177

Conclusion: The sonic toothbrush was superior in reducing gingivitis, bleeding and plaque at Days 15 and 30 when compared to the control manual toothbrush, and with respect to baseline Pre- to Post-brush plaque removal.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 5 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 5 of 177

2 SYNOPSIS REPORT
2.1 OBJECTIVE The objective of this 30-day, randomized, controlled, examiner-blind, parallel design clinical trial was to evaluate the efficacy of a marketed sonic power toothbrush (BURST sonic) on plaque and gingivitis compared to a manual toothbrush and standard fluoride dentifrice. Safety was assessed through oral clinical examinations and interviews to determine soft tissue or oral irritation symptoms, and monitoring of adverse events (AEs) / serious AEs.
2.2 INTRODUCTION
The effective management of dental plaque and gingivitis continues to be a high priority for the dental health of the public. Dental professionals recommend brushing at least twice a day to remove plaque and reduce the risk of tooth decay and gum disease.1 A recent study by Ebel and co-workers2 assessed the impact of brushing time, brushing techniques, and brushing systematics of young adults (18 years old) on efficiency of plaque removal with a standard manual toothbrush. Subjects were asked to clean their teeth to the best of their abilities. They found that participants distributed their brushing time across surfaces unevenly which explained the variance of plaque and bleeding. Brushing technique appeared to be of minor importance. The researchers concluded that the results indicated that establishing systematic interventions or prophylactic programs should emphasize the importance of brushing all surfaces and not neglecting any teeth. However, the high prevalence of oral diseases worldwide suggests that consumers do not achieve sufficient plaque removal with their manual toothbrushing routine. Although dental professionals emphasize the importance of improving brushing habits with patients, research indicates behavior modification is challenging.
Clinical studies have shown that improvement in mechanical oral hygiene can be achieved through the use of power toothbrushes.2-8 Power toothbrush innovations are intended not only to optimize plaque removal and improve gingival health but also to encourage better brushing behavior. This single-center, randomized, controlled, examiner-blind, 30-day, parallel study was designed to evaluate the safety and efficacy of a sonic power toothbrush with charcoal infused toothbrush bristles compared to an ADA reference manual soft toothbrush on plaque and gingivitis.
Standard plaque and gingivitis clinical trials test for differences between treatment groups evaluating changes in mean plaque and gingivitis index scores. For this study, post-treatment efficacy endpoints included mean change in MGI scores (whole mouth and interproximal) change in mean number of healthy sites (MGI=0, 1) at Days 15 and 30; mean change in BI scores (whole mouth and interproximal) and mean change in number of bleedings sites (BI=1 or
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 6 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 6 of 177

2 from baseline to “0” bleeding sites) at Days 15 and 30; and mean change in PI scores at baseline (Pre – Post-brushing), Day 15 and Day 30 (whole mouth, gumline, and interproximal PI scores).
2.3 METHODOLOGY
Prior to the initiation of this study, the study protocol, informed consent document and subject instructions received ethical review and approval from U.S Investigational Review Board. The study was conducted in accordance with the International Conference on Harmonization Good Clinical Practice guidelines (ICH GCP) and all subjects signed an informed consent prior to entering the study. The study was a single-center, randomized, controlled, examiner-blind, 30-day parallel study. Based on the assumption that the sonic power toothbrush group improvement would exceed that of the control group by at least 25% at Days 15 and 30, the calculated total sample size of 90 completed subjects (45 per group) provided 90% power to detect a difference of 0.24 with respect to MGI, and 0.4 with respect to PI when compared to the control group, with an effect size (mean/standard deviation) of 0.7, at the Day 30 assessment. These calculations were based on two-sided tests at the 0.05 significance level.
This study was designed according to the American Dental Association Council on Scientific Affairs Acceptance Program Requirements for Toothbrushes. Generally healthy adult subjects (≥ 18 years of age) were eligible and enrolled in this study if they presented with a least 18 natural teeth with scorable facial and lingual surfaces, a mean gingival index of 1.75–2.3, according to the Modified Gingival Index (MGI),9 a minimum of 20 bleeding sites based on the Bleeding Index of Saxton and van der Ouderaa,10 and a mean plaque index ≥ 1.95 according to the Lobene-Soparkar Modification of the Turesky Modification of the Quigley-Hein Plaque Index (PI).11,12 Subjects were excluded if they had significant oral soft tissue pathology; severe periodontal disease or concurrent periodontal treatment; grossly carious, fully crowned, or extensively restored teeth; orthodontic appliances; peri/oral piercings or removable partial dentures; self-reported serious medical conditions; under treatment for a heart condition requiring use of a pacemaker; required antibiotic premedication prior to dental procedures; having had antibiotic, anti-inflammatory, anti-coagulant medication or chemotherapeutic antiplaque/antigingivitis therapy within 30 days of screening; or participated in any study involving oral care products concurrently or within 30 days of screening.
All subjects who enrolled in the study signed an informed consent document and agreed to refrain from dental treatment during the course of the study, except on an emergency basis, and were willing to discontinue use of other oral hygiene products for the duration of the
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 7 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 7 of 177
study. This study consisted of a Screening/baseline visit during which subjects read and signed an informed consent form, completed health and dental questionnaires and received a clinical oral examination. At Screening/baseline, Day 15 and Day 30, subjects received an oral examination that included assessments in the following order:
• Oral safety (soft and hard tissue examination for evidence of irritation or otherabnormalities);
• Gingivitis according to the Modified Gingival Index (MGI);• Gingival bleeding according to the Bleeding Index described by Saxton and van der
Ouderaa (BI);• Supragingival plaque levels, determined according to the Lobene-Soparkar Modification
of the Turesky Modification of the Quigley-Hein Plaque Index (PI).o At the baseline visit only, a Post-Brush PI assessment was performed.o Plaque was disclosed by rinsing with an erythrosine dye solution prior to each
assessment of supragingival plaque.
Prior to each exam visit, subjects refrained from oral hygiene for 8 to 12 hours and did not eat, drink or smoke for at least 30 minutes prior to the visit. All clinical exams were conducted by two, experienced and validated dental examiners.
Subjects meeting study entrance criteria were randomly assigned to one of two treatment groups:
1) Manual Toothbrush (Control): Twice daily brushing with ADA reference manual soft-bristled toothbrush (Colgate® Classic [Pokey], Colgate-Palmolive Co., New York, NY) andADA Accepted 0.243% sodium fluoride CREST® Cavity Protection toothpaste (Procter &Gamble, Cincinnati, OH, USA)
2) Sonic Toothbrush: Twice daily brushing with BURST sonic power toothbrush (BURST.USAinc, Walnut, CA; brushing mode: whitening) and ADA Accepted 0.243% sodium fluorideCREST® Cavity Protection toothpaste (Procter & Gamble, Cincinnati, OH, USA)
Subjects were provided verbal and written instructions on the use of their assigned toothbrush. All subjects brushed with their assigned toothbrush under the supervision of study personnel for the first use, and unsupervised thereafter. Subjects assigned to the sonic toothbrush were instructed to brush for two minutes according the manufacturer’s instruction. Those assigned to the manual toothbrush were instructed to brush in their usual manner. Immediately following the first use of their assigned toothbrush at baseline, subjects were redisclosed with erythrosine dye and examined again to assess the immediate effect of each toothbrush in removing supragingival plaque. All subjects maintained a daily diary to document compliance.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 8 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 8 of 177
Both the assignment process and subsequent product distribution were conducted in a protected area that ensured blinding of the clinical examiner and the data recorders to subjects’ assignments to their toothbrush. Following the baseline exams, subjects returned at Days 15 and 30 for the same assessments for oral safety, gingival health (MGI and BI) and plaque. A single experienced examiner conducted the oral tissue safety examination and the Modified Gingival Index exams, and a second examiner assessed plaque and bleeding levels. During the study, subjects refrained from using any oral care products other than the assigned toothbrush and toothpaste provided to them and they also avoided the use of other toothbrushes, toothpaste, mouthwashes, chewing gums, breath films, mints, flow or interdental cleaning aids, or other oral care cleaning aids. Subjects were instructed to only use dental floss to remove food impaction.
The efficacy endpoints were:
• Mean change in MGI scores at Days 15 and 30: Whole mouth Interproximal (mesial & distal)
• Change in mean number of healthy sites (MGI=0, 1) at Days 15 and 30• Mean change in BI scores at Day 15 and 30:
Whole mouth Interproximal (mesial & distal)
• Mean change in number of bleeding sites (BI=1 or 2) from baseline to “0” bleeding sitesat Days 15 and 30. Whole mouth Interproximal (mesial & distal)
• Mean change in PI scores at baseline Pre – Post-brushing, Days 15 and 30 for: Whole mouth PI scores; Gumline PI scores (marginal); Interproximal PI scores (mesial and distal).
2.4 STATISTICAL METHODS Data analysis sets included evaluable subjects, defined as subjects without major protocol violations. Data for safety analysis included all subjects who received treatment. Demographic and baseline characteristics were summarized for age, gender, race, tobacco use, mean MGI, BI and PI, and mean number of healthy gingival sites (MGI=0, 1; BI=0). Analysis of the number of healthy sites were performed to assess the performance of the toothbrushes in achieving healthy gingival status. Summary statistics were provided by treatment group for plaque and gingivitis (MGI and BI) scores before brushing at baseline, for plaque scores post-brushing at baseline, and for plaque and gingivitis (MGI and BI) scores before brushing at Days 15 and 30.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 9 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 9 of 177
Categorical demographic and baseline data were evaluated using Fisher’s Exactness Test and continuous demographic and baseline data were evaluated using ANOVA. All tests were two-sided and conducted at the 0.05 significance level. No adjustments were made for multiple comparisons or multiple testing.
Full details of the study protocol are provided in Appendix 4.1.1
3 SUMMARY RESULTS AND CONCLUSIONS
A total of 94 subjects met the study entrance criteria and were randomized to one of the two treatment groups; Two subjects withdrew from the study due to schedule conflicts, hence, 92 subjects completed all study visits.
Demographics characteristics for the 94 randomized subjects are provided in Table 1 and Appendix 4.2.4 Appendix Table 1 of the Statistical Report. Randomized subjects’ ages ranged from 20 to 70 years with an overall mean of 45.8 years. There were 68 females and 26 males, and the majority of the population was white (83.0%), non-Hispanic (98.9%) and not tobacco users (97.9%). There were no significant differences between groups for baseline demographics or for the baseline efficacy variables (MGI, p>0.391; BI, p>0.448; PI, p>0.678).
Compliance: Subject compliance with their assigned toothbrush was assessed at the Day 15 and 30 visits through review of the subjects’ daily diaries. Subjects were required to maintain their daily diary and to record the time of completion of their assigned morning and evening toothbrushing. Based on review of completed diaries and interviews with subjects, all were deemed compliant with their twice daily use of their assigned toothbrush. All 92 subjects who completed the study attended visits as scheduled, with the exception of three subjects who had schedule conflicts. The three subjects were seen for their Day 30 visit one day outside of the ± 2-day window. The deviation was considered minor and subject data for the three subjectswere included in the data set. Details of the deviations are provided in Appendix 4.2.1.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 10 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 10 of 177

Table 1: Demographic Data for Evaluable Subjects Parameters Manual Brush
(n=47) Sonic Brush
(n=47) Total
(N=94) Age, mean (SD), years 47.0 (12.73) 44.6 (12.21) 45.8 (12.46) Range 20.0–70.0 22.0–67.0 20.0–70.0
p=0.365* Gender
Female, n (%) 35 (74.5%) 33 (70.2%) 68 (72.3%) Male, n (%) 12 (25.5%) 14 (29.8%) 26 (27.7%)
p=0.818† Race, n (%)
Black or African American 6 (12.8%) 6 (12.8%) 12 (12.8%) White 38 (80.9%) 40 (85.1%) 78 (83.0%) Asian 1 (2.1%) 1 (2.1%) 2 (2.1%) American Indian/Alaska Native 2 (4.3%) — 2 (2.1%) Native Hawaiian or other Pacific Islander — — —
Other‡ — — — p=0.835†
Ethnicity, n (%) Hispanic, Latino 1 (2.1%) — 1 (1.1%) Non-Hispanic or Non-Latino 46 (97.9%) 47 (100.0%) 93 (98.9%)
p=1.000† Tobacco use, n (%)
Yes, Smoker — 2 (4.3%) 2 (2.1%) Yes, Smokeless tobacco — — — No 47 (100.0%) 45 (95.7%) 92 (97.9%)
p=0.495† baseline whole mouth MGI, mean (SD) 2.06 (0.19) 2.06 (0.20) p=0.924* baseline interproximal MGI, mean (SD) 2.27 (0.23) 2.32 (0.23) p=0.391* baseline whole mouth BI, mean (SD) 0.46 (0.20) 0.43 (0.14) p=0.469* baseline interproximal BI, mean (SD) 0.53 (0.22) 0.50 (0.16) p=0.448* baseline Pre-Brush whole mouth PI, mean (SD) 2.93 (0.28) 2.90 (0.35) p=0.680*
baseline Pre-Brush gumline PI, mean (SD) 2.58 (0.36) 2.55 (0.46) p=0.714* baseline Pre-Brush interproximal PI, mean (SD) 3.11 (0.26) 3.08 (0.31) p=0.678*
*p-value from ANOVA; †p-value from Fisher’s Exactness Test; ‡a randomized subject indicated their raceas white but also wrote biracial in the Other category.ANOVA, Analysis of Variance; BI, Bleeding Index; MGI, Modified Gingival Index; PI, Plaque Index; SD,Standard Deviation.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 11 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 11 of 177
3.1 SAFETY RESULTS
There were no oral adverse events related to the study treatment observed or reported during the study demonstrating that all treatment materials were well tolerated in this study. Only two adverse events, unrelated to the treatments, were reported during this 30-day study. One subject had a food burn on the left side of the hard palate, and one subject had an ulcer on the left mandibular mucosa. Both adverse events were not serious and resolved without sequelae. See Appendix 4.2.5 for additional details.
3.2 EFFICACY RESULTS
Gingivitis: Compared to baseline, both toothbrushes had significantly reduced whole mouth MGI scores at Day 15. At Day 30, only the sonic power toothbrush group demonstrated a significant reduction in whole mouth MGI scores compared to baseline (p<0.001) whereas the manual toothbrush MGI scores actually worsened (p=0.232). The best results were provided by the sonic toothbrush with reductions in whole mouth mean gingivitis scores from baseline of 35.7% and 33.4% at Days 15 and 30, respectively, vs 10.3% (Day 15) and -3.7% (Day 30) in the manual toothbrush group. The adjusted mean difference between the two groups in whole mouth MGI scores was 0.52 and 0.76 at Days 15 and 30 (p<0.001 for both), respectively (Figure 1, Table 2). Similarly, the difference between the adjusted means was statistically significant for the interproximal MGI scores at Day 15 (0.45) and 30 (0.71). The BURST sonic toothbrush was 3.5x and 10x more effective than the manual toothbrush in improving MGI scores at Days 15 and 30, respectively.
Site-specific gingivitis: A site-based analysis of the MGI scores evaluated the change in number of healthy gingival sites from baseline to Days 15 and 30. Essentially, the analysis represents a transition of inflamed sites (MGI = 2, 3, or 4) to healthier gingival tissue (MGI = 0, 1). Out of an average of 98 scorable sites for MGI and BI assessments, the mean number of whole mouth healthy gingival sites for both groups at baseline were small, 16.5 for the manual group, 17.7 for the sonic group; the mean number of interproximal healthy sites were 2.5 and 2.4 (Table 3, Appendix 4.2.4 Appendix Table 1). The analysis of MGI mean change in healthy sites from baseline demonstrated that there were 35.71 and 32.91 more healthy sites (MGI score=0, 1) in the sonic toothbrush group at Days 15 and 30, respectively; brushing with the manual toothbrush (control) resulted in 11.62 (Day 15) and 3.15 (Day 30) more healthy sites compared to baseline (Figure 2, Table 3). The sonic toothbrush provided significantly greater improvement in the mean number of healthy gingival sites compared to the manual toothbrush at Days 15 and 30 for both whole mouth and interproximal sites (p<0.001 at both time points). The sonic toothbrush group experienced 10.4x greater healthy gingival sites after 30 days.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 12 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 12 of 177

Figure 1. Gingivitis Reduction From baseline
MGI, Modified Gingival Index.
Table 2: Adjusted MGI Means and Percent Reductions
VISITS EFFICACY VARIABLES Manual Toothbrush (n=47)
Sonic Toothbrush (n=45)
Mean ± SE Mean ± SE
BASELINE Whole Mouth MGI¥ 2.06 ± 0.03 2.06 ± 0.03
Interproximal MGI¥ 2.27 ± 0.03 2.32 ± 0.03 DAY 15 Whole Mouth MGI 1.84 ± 0.06 1.32 ± 0.06
Difference between adj. means 0.52* ± 0.08 % Reduction from baseline 10.3% 35.7%
Interproximal MGI 2.19 ± 0.05 1.74 ± 0.05 Difference between adj. means 0.45* ± 0.07 % Reduction from baseline 3.9% 24.5%
DAY 30 Whole Mouth MGI 2.13 ± 0.07 1.37 ± 0.08 Difference between adj. means 0.76* ± 0.105 % Reduction form baseline -3.7% 33.4%
Interproximal MGI 2.50 ± 0.07 1.79* ± 0.07 Difference between adj. means 0.71* ± 0.095 % Reduction from baseline -9.5% 22.1%
*p<0.001 vs MB. ¥ baseline Unadjusted Means ; MB, manual brushing (control); SB, sonic brush; MGI,Modified Gingival Index.
10.30%
-3.70%
3.90%
-9.50%
35.70%33.40%
24.50%22.10%
-15%
-10%
-5%
0%
5%
10%
15%
20%
25%
30%
35%
40%
Day 15Whole Mouth
Day 30Whole Mouth
Day 15Interproximal
Day 30Interproximal
MGI Percent Reduction From baseline
Manual Toothbrush (Control) Sonic Toothbrush
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 13 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 13 of 177

Figure 2. Mean Change in Healthy Sites for MGI
MGI, Modified Gingival Index.
Table 3: Mean Change From baseline in Number of Healthy Sites (MGI=0, 1)
VISITS SITE-SPECIFIC VARIABLES Manual Toothbrush (n=47)
Sonic Toothbrush (n=45)
Mean ± SE Mean ± SE BASELINE Whole Mouth Healthy Sites¥ 16.45 ± 1.41 17.67 ± 1.65
Interproximal Healthy Sites¥ 2.45 ± 0.35 2.38 ± 0.45 DAY 15 Whole Mouth Healthy Sites 11.62 ± 2.78 35.71 ± 2.84
Difference between adj. means 24.09*± 3.97 Interproximal Healthy Sites 1.27 ± 1.27 13.22* ± 1.30 Difference between adj. means 11.95*± 1.82
DAY 30 Whole Mouth Healthy Sites 3.15 ± 3.22 32.91 ± 3.30 Difference between adj. means 29.76*± 4.62 Interproximal Healthy Sites 0.40 ± 1.41 13.09 ± 1.44 Difference between adj. means 12.68* ± 2.02
*p<0.001 vs MB. ¥baseline Unadjusted Means; MB, manual brushing (control); SB, sonic brush; MGI,Modified Gingival Index.
Bleeding: At baseline, there were no significant between-group differences in mean whole mouth bleeding scores (p=0.469), with baseline mean scores of 0.46 for the manual toothbrush and 0.43 for the BURST sonic toothbrush. Baseline interproximal mean bleeding scores were not significantly different (p=0.448) with means of 0.53 and 0.50 for the manual
11.62
3.151.28 0.40
35.7132.91
13.22 13.09
0
5
10
15
20
25
30
35
40
Day 15Whole Mouth
Day 30Whole Mouth
Day 15Interproximal
Day 30Interproximal
Mean Change in Number of Gingivitis Sites to Healthy Sites (MGI=0,1)
Manual Toothbrush (Control) Sonic Toothbrush
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 14 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 14 of 177
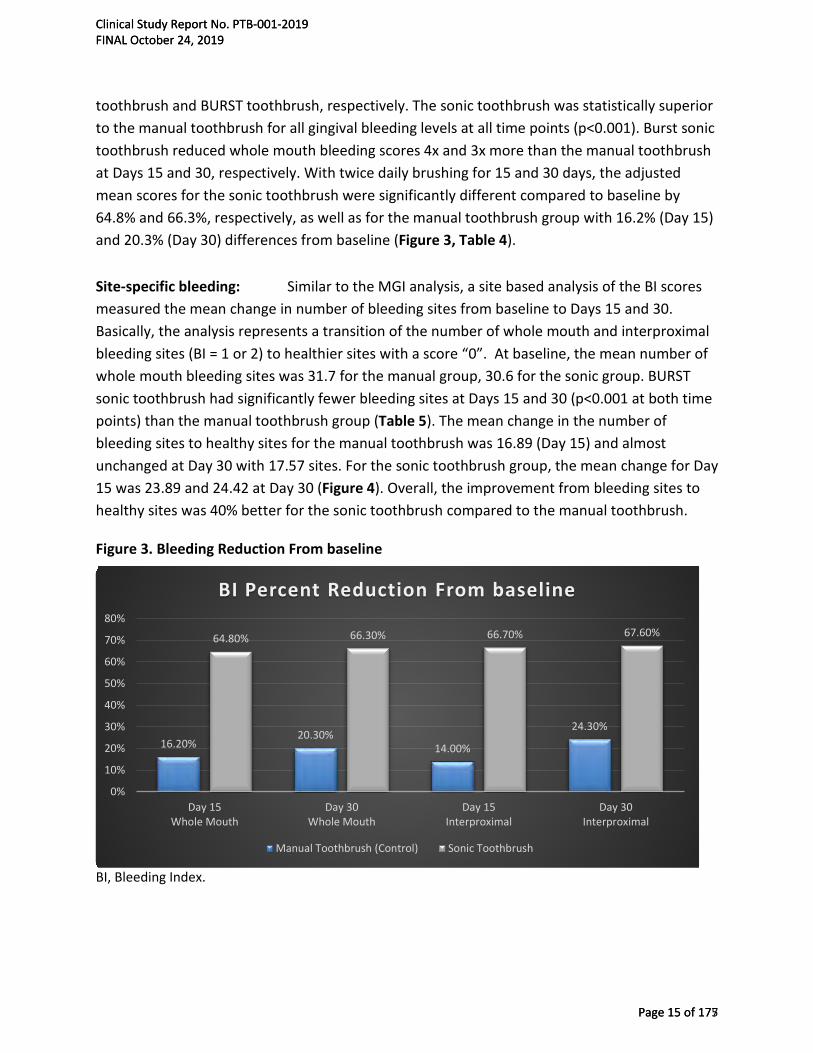
toothbrush and BURST toothbrush, respectively. The sonic toothbrush was statistically superior to the manual toothbrush for all gingival bleeding levels at all time points (p<0.001). Burst sonic toothbrush reduced whole mouth bleeding scores 4x and 3x more than the manual toothbrush at Days 15 and 30, respectively. With twice daily brushing for 15 and 30 days, the adjusted mean scores for the sonic toothbrush were significantly different compared to baseline by 64.8% and 66.3%, respectively, as well as for the manual toothbrush group with 16.2% (Day 15) and 20.3% (Day 30) differences from baseline (Figure 3, Table 4).
Site-specific bleeding: Similar to the MGI analysis, a site based analysis of the BI scores measured the mean change in number of bleeding sites from baseline to Days 15 and 30. Basically, the analysis represents a transition of the number of whole mouth and interproximal bleeding sites (BI = 1 or 2) to healthier sites with a score “0”. At baseline, the mean number of whole mouth bleeding sites was 31.7 for the manual group, 30.6 for the sonic group. BURST sonic toothbrush had significantly fewer bleeding sites at Days 15 and 30 (p<0.001 at both time points) than the manual toothbrush group (Table 5). The mean change in the number of bleeding sites to healthy sites for the manual toothbrush was 16.89 (Day 15) and almost unchanged at Day 30 with 17.57 sites. For the sonic toothbrush group, the mean change for Day 15 was 23.89 and 24.42 at Day 30 (Figure 4). Overall, the improvement from bleeding sites to healthy sites was 40% better for the sonic toothbrush compared to the manual toothbrush.
Figure 3. Bleeding Reduction From baseline
BI, Bleeding Index.
16.20%20.30%
14.00%
24.30%
64.80% 66.30% 66.70% 67.60%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Day 15Whole Mouth
Day 30Whole Mouth
Day 15Interproximal
Day 30Interproximal
BI Percent Reduction From baseline
Manual Toothbrush (Control) Sonic Toothbrush
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 15 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 15 of 177

Table 4: Adjusted BI Means and Percent Reductions
VISITS EFFICACY VARIABLES Manual Toothbrush (n=47)
Sonic Toothbrush (n=45)
Mean ± SE Mean ± SE
BASELINE Whole Mouth BI¥ 0.46 ± 0.03 0.43 ± 0.02 Interproximal BI¥ 0.53 ± 0.03 0.50 ± 0.02
DAY 15
Whole Mouth BI 0.38 ± 0.02 0.16 ± 0.02 Difference between adj. means 0.22* ± 0.02
% Reduction from baseline 16.2% 64.8% Interproximal BI 0.45 ± 0.02 0.17* ± 0.02
Difference between adj. means 0.27* ± 0.03 % Reduction from baseline 14.0% 66.7%
DAY 30
Whole Mouth BI 0.36 ± 0.02 0.15 ± 0.02 Difference between adj. means 0.21* ± 0.02
% Reduction from baseline 20.3% 66.3% Interproximal BI 0.39 ± 0.02 0.17* ± 0.02
Difference between adj. means 0.23* ± 0.03 % Reduction from baseline 24.3% 67.6%
*p<0.001 vs MB; ¥baseline Unadjusted Means; BI, Bleeding Index; MB, manual brushing (control); SB,sonic brush.
Table 5: Mean Change in Number of Healthy Sites (BI=0) From baseline
VISITS SITE-SPECIFIC VARIABLES Manual Toothbrush (n=47)
Sonic Toothbrush (n=45)
Mean ± SE Mean ± SE BASELINE Whole Mouth Bleeding Sites (BI=1,2)¥ 31.68 ± 1.39 30.58 ± 0.99
Interproximal Bleeding Sites (BI=1,2) ¥ 17.19 ± 0.476 16.76 ± 0.59 DAY 15 Whole Mouth BI 16.89 ± 0.79 23.89± 0.80
Difference between adj. means 7.00* ± 1.12 Interproximal BI 9.04 ± 0.52 13.33 ± 0.53
Difference between adj. means 4.29* ± 0.75 DAY 30 Whole Mouth BI 17.57 ± 0.81 24.42 ± 0.83
Difference between adj. means 6.85* ± 1.16 Interproximal BI 9.83 ± 0.55 13.42 ± 0.56
Difference between adj. means 3.59* ± 0.78
*p<0.001 vs MB; ¥baseline Unadjusted Means; BI, Bleeding Index; MB, manual brushing (control); SB,sonic brush.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 16 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 16 of 177

Figure 4. Mean Change in Healthy Sites for BI
BI, Bleeding Index.
Supragingival Plaque: For comparison of the single use brushing at the baseline visit (Pre- to Post-Brush assessment), both toothbrushing showed statistically significant whole mouth plaque reductions from the pre-brushing plaque levels for whole mouth, gumline and interproximal areas, p<0.001 (Appendix 4.2.4 App. Tables 10–11). The sonic toothbrush demonstrated greater plaque removal compared to the manual toothbrush (Table 6). Specifically, the sonic toothbrush removed 33% more whole mouth and gumline plaque than the manual toothbrush which was statistically significantly (p=0.035 for whole mouth) and (p=0.020 for gumline), with a similar trend for interproximal plaque removal, although not statistically significant (p=0.082). See Figure 5 for a summary representation of plaque removal performance of the sonic toothbrush compared to the manual toothbrush control at the baseline visit.
At Days 15 and 30, the sonic toothbrush was significantly superior to the manual toothbrush for plaque reduction (p<0.001; Table 6). The sonic toothbrush reductions of 8.9% (Day 15 Pre-Brush), and 11.4% (Day 30 Pre-Brush) vs 0.8% (Day 15 Pre-Brush), and 1.1% (Day 30 Pre-Brush) when using the manual toothbrush control (Figure 6; Table 6, Appendix 4.2.4 Tables 5–7).
16.89 17.57
23.89 24.42
0
5
10
15
20
25
30
Day 15 Day 30
Mean Change in Number of Whole Mouth Bleeding Sites to Healthy Sites (BI=0)
Manual Toothbrush (Control) Sonic Toothbrush
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 17 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 17 of 177

Whole mouth plaque reductions for the BURST toothbrush were 10x greater than the manual toothbrush at Days 15 and 30.
Table 6: Adjusted PI Means and Percent Reductions
VISITS EFFICACY VARIABLES Manual Toothbrush (n=47)
Sonic Toothbrush (n=45)
Mean ± SE Mean ± SE BASELINE Whole Mouth PI¥ 2.93 ± 0.04 2.90 ± 0.05
Gumline PI¥ 2.58 ± 0.05 2.55 ± 0.07 Interproximal PI¥ 3.11 ± 0.04 3.08 ± 0.05
BASELINE Post-Brush Whole Mouth PI 2.46 ± 0.05 2.31 ± 0.05 Difference between adj. means 0.15* ± 0.07 % Reduction from baseline 15.7% 20.9%
Gumline PI 1.84 ± 0.07 1.61 ± 0.07 Difference between adj. means 0.23† ± 0.099 % Reduction from baseline 28.1% 37.5%
Interproximal PI 2.77 ± 0.04 2.66 ± 0.04 Difference between adj. means 0.11‡± 0.06 % Reduction from baseline 10.5% 14.0%
DAY 15 Whole Mouth PI 2.89 ± 0.03 2.65§ ± 0.03 Difference between adj. means 0.24 ± 0.042 % Reduction from baseline 0.8% 8.9%
Gumline PI 2.56 ± 0.05 2.16 ± 0.05 Difference between adj. means 0.40§ ± 0.07 % Reduction from baseline 0.3% 15.5%
Interproximal PI 3.07 ± 0.03 2.90 ± 0.03 Difference between adj. means 0.17§ ± 0.04 % Reduction from baseline 1.0% 6.1%
DAY 30 Whole Mouth PI 2.89 ± 0.03 2.58 ± 0.03 Difference between adj. means 0.31§ ± 0.05 % Reduction from baseline 1.1% 11.4%
Gumline PI 2.56 ± 0.05 2.04 ± 0.05 Difference between adj. means 0.52§± 0.07 % Reduction from baseline 0.4% 20.4%
Interproximal PI 3.06 ± 0.03 2.85§ ± 0.03 Difference between adj. means 0 .21§ ± 0.04 % Reduction from baseline 1.3% 7.7%
¥baseline Unadjusted Means; *p=0.035 vs MB; †p=0.020 vs MB; ‡p=0.082 vs MB; §p<0.001 vs MB.MB, manual brushing (control); PI, Plaque Index; SB, sonic brush.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 18 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 18 of 177

Figure 5. baseline Post-Brush Plaque Removal: Whole Mouth and Hard-to-Reach Areas (e.g., Gumline, Interproximal)
Figure 6. Plaque Reductions From Baseline
15.70%
28.10%
10.50%
20.90%
37.50%
14.00%
0%
5%
10%
15%
20%
25%
30%
35%
40%
Whole Mouth Gumline Interproximal
baseline Post-Brush Plaque Index Percent Reduction
Manual Toothbrush (Control) Sonic Toothbrush
15.70%
0.80% 1.10%
20.90%
8.90%
11.40%
0%
5%
10%
15%
20%
25%
Baseline Post-Brush Day 15 Day 30
Plaque Index Whole Mouth Percent Reduction From baseline Pre-Brush
Manual Toothbrush (Control) Sonic Toothbrush
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 19 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 19 of 177

3.3 DISCUSSION
Adequate and consistent oral hygiene is necessary for maintaining oral health and prevention of caries and periodontal diseases.13 One of the most efficient approaches for controlling dental disease is the mechanical removal of plaque,14 and the manual toothbrush is a frequently used oral hygiene aid for plaque removal. Unfortunately, a manual toothbrush only partially removes plaque,14 and this mechanical routine does not appear to be sufficient since it is has been estimated that 63% of the population in the United States and up to 80% in other regions of the world have some form of gingivitis.15-17 In an effort to improve plaque removal, powered toothbrushes were introduced to consumers as early as the 1940s18 with several studies demonstrating superior plaque removal with use of a powered brush as compared to a standard manual toothbrush.14,19,20
Since its introduction, power toothbrushes have had improvements in advanced designs and offer different modes of action, including rotating-oscillating, side-to-side and sonic brushes. A review conducted by the Cochrane collaboration revealed that power toothbrushes provide superior plaque and gingivitis reduction after short-term use as compared to manual brushing8; however, another Cochrane review by Deacon et al. (2010) demonstrated that rotating-oscillating brushes had better efficacy than side-to-side bristles.21 Unfortunately, sonic and side-to-side brushes were not identified as a separate mode of action by Deacon et al (2010), instead studies evaluating sonic brushes were grouped with side-to-side toothbrush trials.21 In a recent meta-analysis by de Jager et al (2017), sonic brushes demonstrated a favorable plaque removal effect and comparable gingivitis reduction vs oscillating-rotating toothbrushes; thus, both modes of action (e.g., oscillating-rotating and sonic) demonstrate comparable efficacy and deliver a clinical benefit over manual brushing.22
The BURST sonic toothbrush features 33,000 sonic vibrations per minute, 30 second quadrant paced brushing and three modes: whitening, sensitive and massage. In this 30-day trial, the effectiveness of BURST sonic power toothbrush with charcoal-infused bristles (whitening mode) on plaque removal and reduction in gingivitis was compared to brushing with an ADA reference standard manual toothbrush. Assessments of gingival health and plaque levels at Days 15 and 30 occurred approximately 8–12 hours after the assigned toothbrush use, which represents the approximate period of time between usual home care procedures. The efficacy of the mechanical plaque removal portion of the sonic toothbrush is highlighted by the difference in plaque levels vs the manual toothbrush. Specifically, the sonic power toothbrush had superior whole mouth) and gumline plaque removal after a single use at the baseline Pre- to Post-brush assessment. A similar trend in plaque removal was also observed for interproximal sites. The
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 20 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 20 of 177

results of the single use plaque assessments demonstrate the superior plaque removal performance of the BURST sonic power toothbrush compared with manual brushing and are consistent with previous single-use sonic power toothbrush studies using a similar plaque index.14,18,23
A revealing measure of the efficacy of a toothbrush is the improvement in plaque-induced gingivitis. Results observed in this study reflect the ability of the BURST sonic power toothbrush on removing more plaque vs manual brushing and thereby improved gingival health. After just 15 days, the BURST sonic toothbrush reduced bleeding gums up to 4x more than a manual toothbrush. After 30 days of use, the sonic toothbrush provided 10x greater improvement in plaque removal and up to 10.4x greater healthy gingival sites vs the manual toothbrush control and 10x more improvement in whole mouth mean gingivitis scores. The cumulative benefit in plaque reduction that was observed in the sonic power toothbrush group suggests that the brushing routine effectively disrupted dental plaque colonies, helping to minimize further accumulation of plaque bacteria. Similarly, sonic power toothbrushes have been shown to disrupt viable bacteria in plaque, even in areas beyond the reach of toothbrush bristles.24–26 Furthermore, the superiority in plaque removal and gingivitis reduction vs a manual toothbrush are consistent with findings from previous sonic toothbrush studies conducted over 4-weeks,6,23, 27-34 including results from a recent meta-analysis of 18 clinical studies (N=1,870)22 demonstrating greater plaque and gingivitis reductions by a sonic power toothbrush vs a manual toothbrush.
3.4 CONCLUSION
Within the limits and controls of this single center, randomized, controlled clinical trial, the BURST sonic toothbrush was superior in reducing plaque and improving gingival health vs an ADA reference manual toothbrush.
• The sonic toothbrush was superior in reducing whole mouth and gumline plaque atbaseline Pre- to Post-Brush, and before brushing at Day 15 and Day 30, when comparedto the manual brushing control.
• Compared to the manual toothbrush control, the sonic toothbrush was superior inreducing gingivitis and bleeding at Days 15 and 30, as well as providing a greaternumber of healthy gingival sites.
• The results of this study demonstrate the safety of the BURST sonic toothbrush andbenefits in providing clinically measurable improvement in plaque removal and gingivalhealth.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 21 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 21 of 177

In this 30-day study, the sonic toothbrush provided the best results at both Day 15 and the final Day 30 visits for all endpoints measured. The results of this study highlight the benefits of incorporating a power toothbrush into a home care routine in reducing plaque and improving gingival health compared to brushing with a standard manual toothbrush.
3.5 REFERENCES
1. American Dental Association Mouth Healthy™ A-Z Topics.http://www.mouthhealthy.org/en/az-topics/p/plaque. Accessed July 12, 2019.
2. Ebel S, Blättermann H, Weik U, Margraf-Stiksrud J, Deinzer R. High plaque levels afterthorough toothbrushing: What impedes efficacy? J Dent Res. 2018;4(2):135-142.
3. Davidovich E, Ccahuana-Vasquez RA, Timm H, Grender J, Cunningham P, Zini A.Randomised clinical study of plaque removal efficacy of a power toothbrush in apaediatric population. International Journal of Paediatric Dentistry. 2017;Nov;27(6):558-567. doi: 10.1111/ipd.12298. Epub 2017 May 11.
4. Klukowska M, Grender JM, Timm H. A single-brushing study to compare plaque removalefficacy of a new power brush to an ADA reference manual toothbrush. Am J Dent.2012;25:10A–13A.
5. Starke EM, Mwatha A, Ward M, Argosino K, Jenkins W, Milleman JL, Milleman KR. AComparison of the Effects of a Powered and Manual Toothbrush on Gingivitis andPlaque: A Randomized Parallel Clinical Trial. J Clin Dent. 2019;30(Spec Iss A)A24–29.
6. Delaurenti M, Ward M, Souza S, Jenkins W, Putt MS, Milleman KR, Milleman JL. TheEffect of Use of a Sonic Power Toothbrush and a Manual Toothbrush Control on Plaqueand Gingivitis. J Clin Dent. 2017 Mar;28(1 Spec No A):A1-6.
7. Sharma NC, Klukowska M, Mielczarek A, Grender JM, Qaqish J. A 4-week clinicalcomparison of a novel multi-directional power brush to a manual toothbrush in thereduction of gingivitis and plaque. Am J Dent. 2012 Sep;25 Spec No A(A):14A-20A.
8. Yaacob M, Worthington HV, Deacon SA, et al. Powered versus manual toothbrushing fororal health. Cochrane Database Syst Rev. 2014;6:CD002281.
9. Lobene RR, Weatherford T, Ross NM, Lamm RA, Menaker L. A modified gingival indexfor use in clinical trials. Clin Prev Dent. 1986;8(1):3-6.
10. Saxton CA, van der Ouderaa FJ. The effect of a dentifrice containing zinc citrate andtriclosan on developing gingivitis. J Periodontol. 1989;24:75-80.
11. Turesky S, Gilmore ND, Glickman I. Reduced plaque formation by the chloromethylanalogue of victamine C. J Periodontol. 1970;41(1):41-43.
12. Lobene RR, Soparkar PM, Newman MB. Use of dental floss. Effect on plaque andgingivitis. Clin Prev Dent. 1982;4(1):5-8.
13. Kaur A, Singh RA, Bhola K, Khilji I, Dhawan S, Kochar D. Comparative assessment of theefficacy of two commercially available manual toothbrushes for removal of dentalplaque. J Adv Med Dent Scie Res. 2018;6(9):62-65.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 22 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 22 of 177
14. Re D, Augusti G, Battaglia D, Gianni AB, Augsti D. Is a new sonic toothbrush moreeffective in plaque removal than a manual toothbrush? Eur J Paediatr Dent. 2015.16(1):13-18.
15. Albandar JM, Rams TE. Global epidemiology of periodontal diseases: an overview.Periodontol 2000. 2002;29:7-10.
16. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden oforal diseases and risks to oral health. Bull World Health Organ. 2005;83(9):661-669.
17. Brown LJ, Brunelle JA, Kingman A. Periodontal status in the United States, 1988-91:prevalence, extent, and demographic variation. J Dent Res. 1996;75:672-683.
18. Elkerbout TA, Slot DE, Rosema NAM, Van der Weijden GA. How effective is a poweredtoothbrush as compared to a manual toothbrush? A systematic review and meta-analysis of single brushing exercises. Int J Dent Hygiene. 2019;00:1-10.
19. Terezhalmy GT, Bartizek RD, Biesbrock AR. Relative plaque removal of threetoothbrushes in a nine-period crossover study. J Periodontology. 2005;76:2230-2235.
20. Lazarescu D, Boccaneala S, Illiescu A, De Boever JA. Efficacy of plaque removal andlearning effect of a powered and a manual toothbrush. J Clinical Periodontology.2003;30:726-731.
21. Deacon SA, Glenny A-M, Deery C, Robinson PG, Heanue M, Walmsley AD, Shaw WC.Different powered toothbrushes for plaque control and gingival health. CochraneDatabase Syst Rev. 2010;12:CD004971.
22. De Jager M, Rmaile A, Darch O, Bikker JW. The effectiveness of manual versus high-frequency, high-amplitude sonic powered toothbrushes for oral health: a meta-analysis.J Clin Dent. 2017;28(Spec Iss A):A13-28.
23. Moritis K, Delaurenti M, Johnson MR, Berg J, Boghosian AA. Comparison of the SonicareElite and a manual toothbrush in the evaluation of plaque reduction. Am J Dent.2002;15(Spec Iss)23B-25.
24. Klonowicz D, Czerwinska M, Sirvent A, Gatignol J-P. A new tooth brushing approachsupported by an innovative hybrid toothbrush-compared reduction of dental plaqueafter a single use versus an oscillating-rotating powered toothbrush. BMC Oral Health.2018;18:185.
25. Schmidt JC, Zaugg C, Weiger R, Walter C. Brushing without brushing? A review of theefficacy of powered toothbrushes in noncontact biofilm removal. Clin Oral Investig.2013;17:682–709.
26. Hope CK, Wilson M. Effects of dynamic fluid activity from an electric toothbrush on invitro oral biofilms. J Clin Periodontol. 2003;30:624–629.
27. Johnson BD, McInnes C. Clinical evaluation of the efficacy and safety of a new sonictoothbrush. J Periodontol. 1994;65:692-697.
28. Nunn ME, Ruhlman CD, Mallatt PR, Rodriguez SM, Ortbald KM. Plaque reduction overtime of an integrated oral hygiene system. Compend Contin Educ Dent. 2004;25:8-14.
29. Holt J. Sturm D, Master A, Jenkins W, Schmitt P, Hefti A. A randomized, parallel-designstudy to compare the effects of the Sonicare Flexcare and the Oral-B P40 manualtoothbrush on plaque and gingivitis. Compend Contin Educ Dent. 2007;28:35-41.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 23 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 23 of 177

30. DeLaurenti M, Putt MS, Milleman JL, Jenkins W, Wei J, Strate J. Plaque removal bySonicare and manual toothbrushes in orthodontic subjects. J Dent Res. 2008;87(Spec IssB):2044 (www.iadr.org).
31. DeLaurenti M, Putt MS, Milleman JL, Milleman K, Ward M, Jenkins W, Souza S, NelsonM. An evaluation of two toothbrushes on plaque and gingivitis. J Dent Res. 2012;91(SpecIss B):0552 (www.iadr.org).
32. DeLaurenti M, Sourza S, Nelson M, Jenkins W, Argosino K, Ward M, Milleman J,Milleman KR. Investigation of a novel sonic toothbrush on plaque and gingivitis. J DentRes. 2013;92(Spec Iss A):3748 (www.iadr.org).
33. Ward M, Jenkins W, Argosino K, Souza S, Nelson M, Milleman J, Milleman KR.Assessment of a sonic toothbrush on plaque and gingivitis. J Dent Res. 2013;92(Spec IssA):3753 (www.iadr.org).
34. Argosino K, Milleman J, Milleman K, Mwatha A, Ward M, Jenkins W, Souza S. Anevaluation of power toothbrushing on gingivitis and plaque biofilm. J Dent Res.2015;94(Spec Iss A):3075 (www.iadr.org).
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 24 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 24 of 177
4 APPENDICES
List of Appendices
4.1 Study Information
4.1.1 Protocol and Protocol Amendments
4.1.2 Case Report Forms
4.1.3 Ethics Committees and Subject Information
4.1.4 Investigators and Study Personnel
4.1.5 Sponsor and Investigator Signatures
4.1.6 Randomization Scheme and Codes
4.1.7 Publication Referenced in the Report
4.2 Subject Data Listings
4.2.1 Protocol Deviations
4.2.2 Demographic Data
4.2.3 Individual Efficacy Response Data
4.2.4 Statistical Report
4.2.5 Adverse Event Listings (Each Subject)
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 25 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 25 of 177
4.1 Study Information
4.1.1 Protocol and Protocol Amendments
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 26 of 177
BURST.USA.inc
Clinical Efficacy of a Sonic Power Toothbrush in Adults with Plaque and Gingivitis in a Thirty-Day Model
Clinical Protocol
Protocol No. PTB-001-2019
FINAL
26 July 2019
CONFIDENTIALITY STATEMENT
The information in this document contains trade secrets and commercial information that are privileged or confidential and may not be disclosed unless such disclosure is required by federal or state law or regulations. In any event, persons to whom the information is disclosed must be informed that the information is privileged or confidential and may not be disclosed by them. These restrictions on disclosure will apply equally to all future information supplied, which is indicated as privileged or confidential.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 27 of 177
STATEMENT OF COMPLIANCE
This trial will be conducted in compliance with the protocol and in accordance with Good Clinical Practice (GCP) as required by the following:
• United States (US) Code of Federal Regulations (CFR) applicable to clinical studies (45 CFRPart 46, 21 CFR Part 50, 21 CFR Part 56, 21 CFR Part 312, and/or 21 CFR Part 812)
• International Conference on Harmonisation Good Clinical Practice E6 R2 (ICH-GCP); U.S. Foodand Drug Administration (FDA) March 2018. International E6(R2) Good Clinical Practice:Integrated Addendum to ICH E6(R1) Guidance for Industry, Accessed July 13, 2019
All study personnel will be trained on study procedures and will be knowledgeable in GCP guidelines on protection of subject interests, health and confidentiality.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 28 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 28 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 29 of 177
CONTENTS Statement of Compliance ................................................................................................................ 2
SIGNATURE PAGE ............................................................................................................................ 3
List of Abbreviations ....................................................................................................................... 7
1 Key Roles ............................................................................................................................... 11
2 Background Information and Scientific Rationale ................................................................ 12
3 Objective ............................................................................................................................... 12
3.1 Endpoints ........................................................................................................................ 12
3.1.1 Safety ...................................................................................................................... 12
3.1.2 Efficacy .................................................................................................................... 13
4 Study Design.......................................................................................................................... 13
5 Study Population ................................................................................................................... 14
5.1 Inclusion Criteria ............................................................................................................ 14
5.2 Exclusion Criteria ............................................................................................................ 15
5.3 Subject Identification, Screening and Enrollment ......................................................... 16
5.4 Treatment Assignment Procedures ............................................................................... 16
5.4.1 Withdrawal ............................................................................................................. 16
5.4.2 Termination of Study .............................................................................................. 17
6 Investigational Product ......................................................................................................... 17
6.1 Study Material Description ............................................................................................ 17
6.2 Packaging, Labeling and Storage .................................................................................... 18
6.3 Dosage, Preparation and Administration of Investigational Product ............................ 19
6.4 Accountability Procedures for the Investigational Product(s) ....................................... 19
6.5 Assessment of Subject Compliance with Investigational Product ................................. 19
6.6 Concomitant Medications/Treatments .......................................................................... 19
7 Study Procedures, Evaluation and Schedule ........................................................................ 20
7.1 Screening/Baseline Exam (Visit 1) ............................................................................... 20
7.2 Day 15 (± 2 days) – Midpoint Exams (Visit 2) ................................................................ 20
7.3 Day 30 (± 2 days) – Final Exams (Visit 3) ....................................................................... 21
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 30 of 177
7.4 Early Termination Visit ................................................................................................... 21
8 Study Procedures/Evaluations .............................................................................................. 21
8.1 Demographics................................................................................................................. 21
8.2 Safety Assessments ........................................................................................................ 22
8.2.1 Oral Examinations.................................................................................................. 22
8.3 Efficacy Assessments .................................................................................................... 22
8.3.1 Gingival Inflammation ........................................................................................... 22
8.3.2 Gingival Bleeding ..................................................................................................... 22
8.3.3 Plaque Index ............................................................................................................ 23
8.4 Examiner Repeatability Exercises ................................................................................... 23
9 Adverse Event Reporting and Documentation ..................................................................... 24
9.1 Adverse Events ............................................................................................................... 24
9.2 Definition of a Serious Adverse Event (SAE) .................................................................. 24
9.3 Unanticipated adverse device effect (UADE) ................................................................. 25
9.4 Recording an Adverse Event .......................................................................................... 25
9.5 Follow-up ........................................................................................................................ 26
9.6 Reporting Adverse Events .............................................................................................. 26
9.7 Reporting Unanticipated Adverse Device Effects .......................................................... 27
10 Statistical Considerations ...................................................................................................... 27
10.1 Sample Size Considerations ........................................................................................ 27
10.2 Safety Review ............................................................................................................. 27
10.3 Demographic and Baseline Characteristics ................................................................ 27
10.4 Efficacy Review ........................................................................................................... 28
10.5 Data Sets to be Analyzed ............................................................................................ 28
11 Data Handling and Record Keeping ...................................................................................... 29
11.1 Study Records Retention ............................................................................................ 29
11.2 Protocol Deviations .................................................................................................... 30
12 Ethics ..................................................................................................................................... 30
12.1 Institutional Review Board ......................................................................................... 30
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 31 of 177
12.2 Ethical Conduct of the Study ...................................................................................... 30
12.3 Subject Information and Consent ............................................................................... 30
12.4 Authorization to Disclose Protected Health Information ........................................... 31
13 MONITORING ........................................................................................................................ 31
14 AMENDMENTS/MODIFICATION OF THIS PROTOCOL ........................................................... 32
15 Table 1. Study Flow Chart ..................................................................................................... 33
16 References ............................................................................................................................ 34
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 32 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 32 of 177
LIST OF ABBREVIATIONS
AE Adverse Event/Adverse Experience
ANOVA Analysis of Variance
ANCOVA Analysis of Covariance
BI Gingival Bleeding Index of Saxton and van der Ouderaa
CFR Code of Federal Regulations
CRF Case Report Form
DCF Data Clarification Form
FDA Food and Drug Administration
GCP Good Clinical Practice
ICF Informed Consent Form
ICH International Conference on Harmonisation
IRB Institutional Review Board
MGI Modified Gingival Index
PI Lobene-Soparkar Modification of the Turesky Modification of the Quigley-Hein Plaque Index (PI)
QA Quality Assurance
QC Quality Control
SAE Serious Adverse Event/Serious Adverse Experience
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 33 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 33 of 177
PROTOCOL SUMMARY
TITLE:
Clinical Efficacy of a Sonic Power Toothbrush in Adults with Plaque and Gingivitis in a Thirty-Day Model
Protocol Number: Protocol # PTB-001-2019
Population:
Approximately 100 generally healthy male and female subjects will be screened and randomized so that 90 (45 per group) subjects complete this trial.
Number of Sites:
1, this is a single center study
Study Duration:
Each subject will participate in a 30-day clinical trial.
Description of Test Agents:
1) Control group: ADA Standard manual toothbrush with fluoride toothpaste2) Sonic power toothbrush with fluoride toothpaste
Objective:
The objective of this 30-day, randomized, examiner-blind clinical trial is to assess the efficacy of a sonic power toothbrush on plaque and gingivitis, compared to a manual toothbrush.
Key Inclusion Criteria:
1. Generally healthy males and females at least 18 years of age or older.2. Volunteers must read, sign and receive a copy of the signed informed consent form.3. A minimum of 18 natural teeth with scorable facial and lingual surfaces. Teeth that
are grossly carious, orthodontically banded, exhibiting general cervical abrasionand/or enamel abrasion, or third molars will not be include in the tooth count.
4. A gingival index score of ≥ 1.75 and ≤ 2.3 according to the Modified Gingival Index.5. A plaque index score ≥ 1.95 according to the Lobene-Soparkar Modification of the
Turesky Modification of the Quigley-Hein Plaque Index, following 8 to 12 hours plaqueaccumulation period.
6. A minimum of 20 bleeding sites based on the Gingival Bleeding Index of Saxton andvan der Ouderaa.
Study Design:
This single-center, randomized, controlled, double-blind, 30-day parallel study will include an oral screening examination consisting of assessments in the following order:
• Oral safety will be assessed through soft and hard tissue examination for irritations orother abnormalities;
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 34 of 177

• Gingivitis according to the Modified Gingival Index (MGI);• Gingival bleeding according to the Gingival Bleeding Index of Saxton and van der
Ouderaa (BI);• Supragingival plaque levels, determined according to the Lobene-Soparkar
Modification of the Turesky Modification of the Quigley-Hein Plaque Index (PI).Plaque will be disclosed using a red disclosing solution and each tooth will be scoredin six areas (distobuccal, midbuccal and mesiobuccal, distolingual, midlingual andmesiolingual).
Prior to each exam visit, subjects will refrain from oral hygiene for 8 to 12 hours and will not have eaten 30 minutes prior to the visit. Following informed consent procedures and collection of baseline demographics, qualified subjects will receive an oral examination and assessment for MGI, BI and PI per sequence. Subjects will be enrolled into the study with existing mild to moderate gingivitis and there will be no dental prophylaxis performed during the study.
Subjects meeting study entrance criteria will be stratified based on typical toothbrush used (power or manual), and baseline whole mouth mean PI score and randomly assigned to one of two treatment groups:
1) Twice daily brushing with flat trim manual toothbrush and standard anticavity fluoridetoothpaste;
2) Twice daily brushing with sonic power toothbrush and standard anticavity toothpaste
Subjects will be provided verbal and written instructions on the use of their assigned oral care brushing. The first product use will be performed at the clinical site under the supervision of study personnel. Subjects assigned to the sonic power brush will brush their teeth for two minutes using the Whitening mode, while those using the manual toothbrush will be instructed to brush in their usual manner. Following the first use of their assigned product, subjects will be examined again for plaque removal. All subjects will maintain a daily diary to document compliance with the use of their assigned products.
Following the Baseline exams, subjects will return at Days 15 and 30 for the same assessments for oral safety, gingival health and plaque. At Day 30, subjects will brush with their assigned product and will be re-examined again for plaque removal.
During the study, subjects will refrain from using any oral care products other than the toothbrush and toothpaste products provided to them and will avoid the use of chewing gums and mints..
Safety:
Safety will be assessed through oral clinical examinations and interviews to determine soft tissue or oral irritation symptoms. Oral soft tissue findings will be tabulated and summarized by treatment group for each exam visit. The number and percentage of subjects
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 35 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 35 of 177
experiencing adverse events will be tabulated by treatment. Adverse events will be summarized according to relationship to study material and according to severity.
Efficacy Endpoints:
• Mean change in MGI scores at Day 15 and Day 30: Whole mouth Interproximal (mesial & distal)
• Change in mean number of healthy sites (MGI=0, 1) at Day 15 and Day 30• Mean change in BI scores at Day 15 and Day 30:
Whole mouth Interproximal (mesial & distal)
• Mean change in number of bleeding sites (BI=1 or2) from Baseline to “0” bleedingsites at Days 15 and 30. Whole mouth Interproximal (mesial & distal)
• Mean change in PI scores at Baseline Pre - Post-brushing, Days 15 and 30 for: Whole mouth PI scores; Gumline PI scores (marginal); Interproximal PI scores (mesial and distal).
Statistical Analyses:
A sample size of 90 completed and 45 per group evaluable subjects achieves a 90% power to detect treatment differences at Day 30. This assumes improvements by 0.24 with respect to MGI, and 0.4 with respect to PI, when compared to the negative control, with an effect size (mean/standard deviation) of 0.7. These calculations are based on two-sided tests at the 0.05 significance level.
For each efficacy variable summary statistics using appropriate descriptive statistics (mean, median, minimum, maximum) by treatment group and overall will be provided at each visit.
Post-brushing plaque analysis will be performed for Baseline visit. Analyses will be performed for Day 15 and Day 30 for each efficacy variable, analyses will be performed using the ANCOVA model with treatment as a factor and the corresponding baseline value as a covariate. The comparisons will be made at the 0.05 level, 2-sided. Differences between the means, simultaneous 95% confidence intervals and test results will be presented.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 36 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 36 of 177

1 KEY ROLES
Principle Investigator: Jeffrey Milleman, DDS, MPA Salus Research 1220 Medical Park Drive, Building #4 Fort Wayne, IN 46825 Tel: (260) 755-1099 [email protected]
Others (study coordinator): Abigale Yoder Salus Research Phone: (260) 755-1099 Fax: (260) 755-1128 [email protected]
Sponsor: Brittany Stewart Chief Operating Officer BURST.USA.inc 340 S. Lemon Avenue #4658 Walnut, CA 91789 mobile: 310-310-1223 [email protected]
Monitor: Sylvia L. Santos, RDH, MS SLS Clinical Research Consulting, LLC Phone: 201-572-9223 [email protected]
Study sites: Salus Research 1220 Medical Park Drive, Building #4 Fort Wayne, IN 46825 Tel: (260) 755-1099
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 37 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 37 of 177
2 BACKGROUND INFORMATION AND SCIENTIFIC RATIONALE
The effective management of dental plaque and gingivitis continues to be a high priority for the dental health of the public. Dental professionals recommend brushing at least twice a day to remove plaque and reduce the risk of tooth decay and gum disease.1 A recent study by Ebel and co-workers2 assessed the impact of brushing time, brushing techniques, and brushing systematics of young adults (18 years old) on efficiency of plaque removal with a standard manual toothbrush. Subjects were asked to clean their teeth to the best of their abilities. They found that participants distributed their brushing time across surfaces unevenly which explained the variance of plaque and bleeding. Brushing technique appeared to be of minor importance. The researchers concluded that the results indicated that establishing systematic interventions or prophylactic programs should emphasize the importance of brushing all surfaces and not neglecting any teeth. However, the high prevalence of oral diseases worldwide suggests that consumers do not achieve sufficient plaque removal with their manual toothbrushing routine. Although dental professionals emphasize the importance of improving brushing habits with patients, research indicates behavior modification is challenging.
Clinical studies have shown that improvement in mechanical oral hygiene can be achieved through the use of power toothbrushes.2-8 Power toothbrush innovations are intended not only to optimize plaque removal and improve gingival health but also to encourage better brushing behavior. This single-center, randomized, controlled, examiner-blind, 30-day, parallel study is designed to evaluate the safety and efficacy of a sonic power toothbrush with charcoal infused toothbrush bristles compared to an ADA reference manual soft toothbrush on plaque and gingivitis.
3 OBJECTIVE
The objective of this 30-day, randomized, controlled, examiner-blind, parallel design clinical trial is to assess the safety and efficacy of twice daily use of a marketed sonic power toothbrush (BURST Sonic) on plaque and gingivitis, compared to a manual toothbrush when brushing with a standard fluoride dentifrice.
3.1 Endpoints
3.1.1 Safety Safety will be assessed through oral clinical examinations and interviews to determine soft tissue or oral irritation symptoms.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 38 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 38 of 177
3.1.2 Efficacy Efficacy endpoints will be:
• Mean change in Modified Gingival Index (MGI) scores at Day 15 and Day 30: Whole mouth Interproximal (mesial & distal)
• Change in mean number of healthy sites (MGI=0, 1) at Day 15 and Day 30• Mean change in Bleeding Index (BI) scores at Day 15 and Day 30:
Whole mouth Interproximal (mesial & distal)
• Mean change in number of bleeding sites (BI=1 or2) from Baseline to “0” bleeding sites at Days15 and 30. Whole mouth Interproximal (mesial & distal)
• Mean change in Plaque Index (PI) scores at Baseline Pre - Post-brushing, Days 15 and 30 for: Whole mouth PI scores; Gumline PI scores (marginal) Interproximal PI scores (mesial and distal).
4 STUDY DESIGN
This single-center, randomized, controlled, examiner-blind, 30-day parallel study will consist of a Screening/Baseline visit during which potential subjects will read and sign an informed consent form, complete health and dental questionnaires and a receive a clinical oral examination. The oral examination will include assessments in the following order:
• Oral safety will be assessed through soft and hard tissue examination for evidence ofirritation or other abnormalities;
• Gingivitis according to the Modified Gingival Index (MGI);9
• Gingival bleeding according to the Gingival Bleeding Index described by Saxton and vander Ouderaa (BI);10
• Supragingival plaque levels, determined according to the Lobene-Soparkar Modificationof the Turesky Modification of the Quigley-Hein Plaque Index (PI).11, 12
Prior to each exam visit, subjects will refrain from oral hygiene for 8 to 12 hours and will not have eaten 30 minutes prior to the visit. Following informed consent procedures and collection of Baseline demographics, qualified subjects will receive an oral examination and assessment for MGI, BI and PI per sequence.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 39 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 39 of 177

Subjects meeting study entrance criteria will be randomly assigned to one of four treatment groups:
1) Control Group: Twice daily brushing with ADA reference manual soft toothbrush andADA Accepted, 0.243% sodium fluoride Crest® Cavity Protection dentifrice (Procter &Gamble, Cincinnati, OH, USA);
2) Sonic Toothbrush Group: Twice daily brushing with Burst Sonic power toothbrush andADA Accepted, 0.243% sodium fluoride Crest® Cavity Protection dentifrice (Procter &Gamble, Cincinnati, OH, USA)
Subjects will be provided verbal and written instructions on the use of their assigned toothbrush. The first assigned brushing will be performed at the clinical site under the supervision of study personnel. Following the first use of assigned toothbrush products, subjects will be examined again for plaque. All subjects will maintain a daily diary to document compliance with the use of their assigned products.
Following the Baseline exams, subjects will return at Days 15 and 30 for the same assessments for oral safety, gingival health and plaque.
During the study, subjects will refrain from using any oral care products other than the toothbrush or toothpaste provided to them and will avoid the use of other toothbrushes, toothpaste, mouthwashes, chewing gum, breath film, mints, floss or interdental cleaning aids, or other oral care cleaning aids for the duration of this research study.
5 STUDY POPULATION
Up to 100 generally healthy male and female subjects will be screened so that approximately 90 (45 per group) complete this trial. To participate in this study, all subjects will fulfill the inclusion and exclusion criteria as outlined in sections 5.1 and 5.2.
5.1 Inclusion Criteria To be eligible for study participation, subjects must meet the following criteria:
1) Be generally healthy males and females at least 18 years of age.2) Be able to read, sign and receive a copy of the signed informed consent form.3) Be regular manual toothbrush users.4) Be willing to refrain from all oral hygiene 8-12 hours prior to each study visit, and
discontinue eating, drinking and smoking 30 minutes prior to each study visit.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 40 of 177
5) Have a minimum of 18 natural teeth with scorable facial and lingual surfaces. Teeth thatare grossly carious, orthodontically banded, exhibiting general cervical abrasion and/orenamel abrasion, or third molars will not be include in the tooth count.
6) Present with a gingival index score ≥ 1.75 ≤ 2.3 according to the Modified Gingival Index.7) Present with a plaque index score > 1.95 according to the Lobene-Soparkar Modification
of the Turesky Modification of the Quigley-Hein Plaque Index, following an 8 to 12-hourplaque accumulation period.
8) Have a minimum of 20 bleeding sites based on the Gingival Bleeding Index of Saxton andvan der Ouderaa.
9) Be willing and able to refrain from dental treatment during the course of the study,except on an emergency basis.
5.2 Exclusion Criteria Subjects presenting with any of the following will not be included in the study:
1) Having a history of adverse effects, oral soft or hard tissue sensitivity, to any ingredientin the test materials.
2) Having self-reported serious medical conditions.3) Being self-reported as pregnant or nursing.4) Being under treatment for a heart condition requiring use of pacemaker.5) Having anything that, in the opinion of the investigator, would place the subject at
increased risk or preclude the subject’s full compliance with or completion of the study.6) Require antibiotic premedication prior to dental procedures.7) Having had antibiotic, anti-inflammatory, anti-coagulant medication or
chemotherapeutic antiplaque/antigingivitis therapy within 30 days of screening exams.8) Having participated in any study involving oral care products, concurrently or within the
30 days of screening exams.9) Unwilling to discontinue use of other oral hygiene products for the duration of the
study.10) Presence of severe periodontal disease or being actively treated for periodontal disease.11) Having grossly carious, fully crowned, or extensively restored teeth.12) Having orthodontic appliances, peri/oral piercings, or removable partial dentures.13) Having significant oral soft tissue pathology based on a visual examination.
If the subject reports taking medication, a history of allergy, and/or a chronic disease which in the opinion of investigator will not affect the clinical parameter(s) being assessed or the
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 41 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 41 of 177

safety of the subject, the subject may be enrolled in the study and the conditions will be noted on the Subject’s source document.
5.3 Subject Identification, Screening and Enrollment Subjects will be recruited from the local population utilizing the recruitment materials approved by the IRB. Subject screening, enrollment, product assignments, and dental assessments will be conducted at the clinic site. The investigator will maintain a screening and enrollment log of all subjects who sign an ICF for this study. The log will include unique subject identification numbers/screening numbers (1001-1100) and dates of subject screening, enrollment and completion (or early termination). Once a number has been assigned to a subject, it cannot be reassigned to another subject. For subjects who fail screening, the reason(s) for non-participation will be recorded on the log. The Investigator will also maintain a confidential identification list containing each enrolled subject’s name and corresponding unique subject number, to enable records to be identified.
5.4 Treatment Assignment Procedures A minimum of 100 qualified subjects will be randomly assigned to one of two treatment groups. Upon qualification, each enrolled subject will be sequentially issued a unique subject randomization number (001-100), which determines the treatment assignments according to a randomization scheme prepared by the Sponsor. Subjects will be randomized to one of two treatment groups:
1) Control Group: Twice daily brushing with ADA reference manual soft toothbrush andCrest® Cavity Protection dentifrice;
2) Sonic Toothbrush Group: Twice daily brushing with Burst Sonic power toothbrush andCrest® Cavity Protection dentifrice.
The Investigator or designee will maintain randomization worksheets documenting the subject assignment to treatment groups.
5.4.1 Withdrawal Every effort will be made within the bounds of safety and subject choice to have each subject complete the study. A discontinuation occurs when an enrolled subject ceases participation in the study, regardless of the circumstances, prior to completion of the protocol. The reason for a subject discontinuation from the study will be reported in the case report form. The investigators must attempt to determine the primary reason for discontinuation. A study subject will be discontinued from participation in the study if:
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 42 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 42 of 177
• Any clinical adverse event (AE), intercurrent illness, or other medical condition or situationoccurs such that continued participation in the study would not be in the best interest ofthe subject;
• The subject meets any exclusion criteria (either newly developed or not previouslyrecognized).
Subjects are free to withdraw from participation in the study at any time upon request. A discontinuation must be immediately reported to the sponsor’s clinical monitor or his/her designated representative if it is due to a serious adverse event. The final evaluation required by the protocol will be performed at the time of study discontinuation.
5.4.2 Termination of Study This study may be prematurely terminated if, in the opinion of the investigator or the sponsor, there is sufficient reasonable cause. Written notification, documenting the reason for study termination, will be provided to the investigator or sponsor by the terminating party.
Circumstances that may warrant termination include, but are not limited to:
• Determination of unexpected, significant, or unacceptable risk to subjects;• Insufficient adherence to protocol requirements;• Data that are not sufficiently complete and/or evaluable;• Plans to modify, suspend or discontinue the development of the experimental test
article.
If the study is prematurely terminated or suspended, the sponsor will promptly inform the investigators/institutions, of the termination or suspension and the reason(s) for the termination or suspension. The IRB will also be informed promptly and provided the reason(s) for the termination or suspension by the investigator/institution.
6 INVESTIGATIONAL PRODUCT
6.1 Study Material Description
Manual Toothbrush Control: Manual toothbrush Trade name 47 Tuft Soft Flat Trim Manual Toothbrush Dosage form Brush twice daily Packaging Single packaging
Power Toothbrush: Sonic Rechargeable Power Toothbrush
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 43 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 43 of 177

Trade name BURST Sonic Toothbrush Manufacturer BURST.USA.inc Dosage form Brush twice daily Packaging Single packaging
Ancillary supplies include a single tube of Crest® Cavity Protection dentifrice (0.243% sodium fluoride, Procter & Gamble, Cincinnati, OH, USA), at least 4.6 oz. tube.
6.2 Packaging, Labeling and Storage All products must be stored by the clinical site at room temperature. Manual toothbrushes, Burst Sonic Toothbrush and Crest® Cavity Protection toothpaste will be supplied in the original marketed packages with no overwrap.
Each subject will receive a carrying bag that will contain the label noting the relevant randomization number.
The manual toothbrush control group carrying bag will have the following label:
Protocol: PTB-001-2019 Subject Randomization#:
INSTRUCTIONS FOR USE:
1) Wet your toothbrush and dispense a full ribbon of toothpaste (Crest®Regular) onto the brush head.
2) Brush in your usual manner with your assigned toothbrush.3) Rinse with tap water.
Warnings: Keep all test materials out of reach of children under 12 years of age. For Investigational Use Only – Not for Sale If you have questions, contact the Salus Research Emergency number: 260-413-7777
The Sonic Toothbrush group carrying bag will have the following label:
Protocol: PTB-001-2019 Subject Randomization#: 1) Wet the toothbrush bristles and apply the provided toothpaste.2) Place the brush head in your mouth before turning on your power brush and keep
your mouth closed during brushing, otherwise toothpaste may splatter.3) Press the power button once to turn brush on in the first cleaning mode4) Follow the detailed directions provided with your daily diary5) BRUSH A TOTAL OF 2 MINUTES!6) Thoroughly rinse your mouth out with water. Do not swallow toothpaste while
brushing.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 44 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 44 of 177
7) Rinse brush head after use.Warnings: Keep all test materials out of reach of children under 12 years of age. For Investigational Use Only – Not for Sale If you have questions, contact the Salus Research Emergency number: 260-413-7777
6.3 Dosage, Preparation and Administration of Investigational Product At Screening/Baseline visit, all subjects will receive regular fluoride toothpaste and their assigned toothbrush. Subjects will be instructed to dispense toothpaste onto their assigned toothbrush and brush their teeth twice daily as detailed in their instructions attached to their daily diary.
6.4 Accountability Procedures for the Investigational Product(s) Burst Oral Care will provide the investigator with sufficient amounts of the study test materials. The investigator must ensure that deliveries of investigational product from the sponsor are received by a responsible person, that all receipts are recorded in writing and that the product is stored in a secure area under recommended storage conditions. It is also the responsibility of the investigator to ensure that the integrity of packaged study product not be jeopardized prior to dispensing. The investigator will dispense the test material only to subjects included in this study following the procedures specified in the study protocol. Each subject will be administered only the test material carrying his/her randomization number.
All dispensing will be documented. The investigator is responsible for ensuring all full, partially full, and empty test material containers are returned to Burst Oral Care. The investigator must maintain accurate and adequate records including dates of receipt and return of test material shipments, and quantities received/returned from/to Burst Oral Care as well as, dates and amounts dispensed to the study subjects.
6.5 Assessment of Subject Compliance with Investigational Product Compliance will be assessed at the Days 15 and 30 visits through review of the subjects’ daily diaries. Subjects will be required to maintain a daily diary and to record the time of completion of their assigned morning and evening toothbrushing.
6.6 Concomitant Medications/Treatments Any medication the subject takes during the study is considered concomitant medication. All concomitant medications and non-drug therapy (e.g. tooth extraction, endodontic treatment, etc.) must be recorded in the subject’s medical source document.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 45 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 45 of 177

7 STUDY PROCEDURES, EVALUATION AND SCHEDULE
The schedule of observations and assessments is provided in Sec. 15, Table 1, Study Flow Chart.
7.1 Screening/Baseline Exam (Visit 1) Prior to randomization to treatment groups, the following procedures will be performed:
• Informed consent form, medical and dental history.• Inclusion/Exclusion Criteria checklist.• Clinical exams:
Oral soft and hard tissue evaluation for safety assessment; Modified Gingival Index (MGI); Bleeding Index (BI); Lobene-Soparkar Modification of the Turesky Modification of the Quigley-Hein
Plaque Index (PI); Identify subjects with qualifying levels of gingivitis and plaque: MGI ≥ 1.75 and ≤
2.3, PI ≥ 1.95.
If subject meets entry criteria, the following procedures will be performed:
• Randomization to test groups.• Supervise initial use of assigned test products.• Dispense assigned test materials.• Study staff review and dispense daily diary and home use written instructions.• Post-Treatment Plaque Assessment (PI.)• Appoint subjects for next visit.
7.2 Day 15 (± 2 days) – Midpoint Exams (Visit 2) • Query to update medical and oral health and record adverse events and
concomitant medications.• Assess compliance with study instructions and use of test materials.• Oral soft and hard tissue examination for safety.• Clinical exams:
Oral soft and hard tissue evaluation for safety assessment; Modified Gingival Index (MGI); Bleeding Index (BI); Lobene-Soparkar Modification of the Turesky Modification of the Quigley-Hein
Plaque Index (PI);
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 46 of 177
• Appoint subjects for next visit.
7.3 Day 30 (± 2 days) – Final Exams (Visit 3) • Query to update medical and oral health and record adverse events and
concomitant medications.• Assess compliance with study instructions and use of test materials.• Oral soft and hard tissue examination for safety.• Clinical exams:
Oral soft and hard tissue evaluation for safety assessment; Modified Gingival Index (MGI); Bleeding Index (BI); Lobene-Soparkar Modification of the Turesky Modification of the Quigley-Hein
Plaque Index (PI).• Discharge subject and provide final instructions for follow-up of ongoing adverse
events, as applicable.
During the study, subjects will follow their usual dietary habits, but will be instructed to refrain from using any oral care products other than the test materials provided to them.
7.4 Early Termination Visit If a subject discontinues from the study for any reason prior to the final visit, the following procedures should be conducted:
• Record adverse events and concomitant medications;• Oral soft and hard tissue examination;• Schedule follow-up visit for any ongoing adverse events.
8 STUDY PROCEDURES/EVALUATIONS
8.1 Demographics Demographic information will be collected at the Screening/Baseline Visit and will include the subject’s race, gender, age and tobacco use.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 47 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 47 of 177
8.2 Safety Assessments
8.2.1 Oral Examinations An oral examination will be conducted at all visits to monitor the effect of the test articles on the soft and hard tissues. Lips, buccal, labial and sublingual mucosae, tongue, hard and soft palate, uvula and oropharynx, and teeth will be examined for signs of reddening/inflammation, ulceration, white patches and desquamation/ sloughing of mucosal tissues and findings will be recorded on the Oral Exam CRF. Changes from Baseline will be recorded and deviations from normal will be recorded.
Clinically significant findings will be recorded as adverse events and an assessment will be made regarding relationship to test materials.
8.3 Efficacy Assessments Clinical efficacy assessments will be performed by a single examiner at Baseline, Days 15 and 30 in the following sequence: MGI, BI and PI.
8.3.1 Gingival Inflammation Gingival inflammation will be assessed at Baseline, Days 15 and 30, according to the Modified Gingival Index (MGI),9 and will be scored on buccal and lingual marginal gingivae and interdental papillae (four gingival areas: buccal, mesiobuccal, lingual and mesiolingual) of all scorable teeth using a scale of 0 – 4 as noted below:
0 = Normal (absence of inflammation). 1 = Mild inflammation (slight change in color, little change in texture) of any portion of
the entire gingival unit. 2 = Mild inflammation of the entire gingival unit. 3 = Moderate inflammation (moderate glazing, redness, edema, and/or hypertrophy) of
the gingival unit. 4 = Severe inflammation (marked redness and edema/hypertrophy, spontaneous
bleeding, or ulceration) of the gingival unit.
Whole mouth MGI scores will be calculated by summing all scores and dividing by the number of scorable sites examined.
8.3.2 Gingival Bleeding Gingival bleeding tendency will be assessed according to the Bleeding Index (BI) described by Saxton and van der Ouderaa.10 The gingiva will be lightly air-dried and a periodontal probe with a 0.5 mm diameter tip will be inserted into the gingival crevice to a depth of approximately 1 mm. The probe will be moved gently around the tooth at an angle of approximately 60 degreesto the long axis of the tooth, stroking the inner surface of the sulcular epithelium. Each of four
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 48 of 177

gingival areas (distobuccal, midbuccal, mesiolingual, and midlingual) of the scorable teeth will be probed in a likewise manner, waiting approximately 30 seconds before recording the number of gingival units which bleed, according to the following scale:
0 = absence of bleeding after 30 seconds; 1 = bleeding observed after 30 seconds; and 2 = immediate bleeding observed.
8.3.3 Plaque Index Supragingival dental plaque will be assessed according to the Turesky Modification of the Quigley-Hein Plaque Index as further modified by Lobene and Soparkar (PI).11,12 Plaque will be disclosed using a red disclosing solution and each tooth will be scored in six areas (distobuccal, midbuccal and mesiobuccal, distolingual, midlingual and mesiolingual), according to the criteria noted below:
0 = No plaque. 1 = Separate flecks or discontinuous band of plaque at the gingival (cervical) margin. 2 = Thin (up to 1 mm), continuous band of plaque at the gingival margin. 3 = Band of plaque wider than 1 mm but less than 1/3 of tooth surface area. 4 = Plaque covering 1/3 or more, but less than 2/3 of tooth surface area. 5 = Plaque covering 2/3 or more of tooth surface area.
At the Baseline visit only, subjects will brush with their assigned toothbrush at the clinical test site and will be re-disclosed for a second plaque assessment (post-treatment).
A whole mouth plaque index will be calculated for each subject by adding all the individual scores and dividing this sum by the number of measurements. To understand the plaque removal efficacy of each toothbrush in hard to reach areas, separate subsets of the plaque index will be calculated for gingival margin (gumline) and the interproximal surfaces. Gumline PI scores will calculated by summing the number of gingival margin (buccal and lingual) scores and dividing by the number of measurements. Interproximal PI scores (mesial and distal) will be calculated by summing the number of interproximal site scores (distobuccal, mesiobuccal, distolingual and mesiolingual) and dividing by the number of measurements.
8.4 Examiner Repeatability Exercises
A single trained dental examiner will perform the oral examinations and MGI assessments. A second examiner will assess the BI and PI. Prior to Baseline exams, at least 10 subjects will be assessed for gingival inflammation and plaque levels, according to the MGI and PI with at least 10 minutes between repeat examinations. Repeatability will be evaluated through the
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 49 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 49 of 177
demonstration of at least 80% frequency of agreement of assessments. Re-training and/or recalibration (followed by a repeat of the exercise) will be performed if the evaluated level of reliability is judged to be low.
NOTE: Repeatability exercises will not be needed if the examiner has used MGI and PI in a clinical trial within two months prior to the start of this study.
9 ADVERSE EVENT REPORTING AND DOCUMENTATION
Adverse events will be determined by visual examination of the oral cavity by the dental examiner. In addition, clinical research center personnel will ask subjects about the occurrence of any adverse events during their participation in this study. All observed or volunteered adverse events, regardless of treatment group or suspected causal relationship to study product, will be recorded on the adverse event page(s) of the case report form.
9.1 Adverse Events
An adverse event (AE) is any untoward medical occurrence in a clinical investigation of a patient administered an investigational product and that does not necessarily have a causal relationship with the treatment. An AE is therefore any unfavorable and unintended sign (including an abnormal laboratory finding), symptom or disease temporally associated with the administration of an investigational product, whether or not related to that investigational product. An unexpected AE is one of a type not identified in nature, severity, or frequency in the investigational product safety summary or of greater severity or frequency than expected based on the information in the investigational product safety summary.
The Investigator will probe, via discussion with the subject, for the occurrence of AEs during each subject visit and record the information in the site’s source documents. Adverse events will be recorded in the patient CRF. Adverse events will be described by duration (start and stop dates and times), severity, outcome, treatment and relation to study drug, or if unrelated, the cause.
Pre-existing conditions will not be regarded as AEs if the condition follows a normal course Of recovery, unless it worsens after exposure to the investigational product.
9.2 Definition of a Serious Adverse Event (SAE) The Investigator or other study personnel must immediately (within 24 hours) inform the Sponsor of all Serious Adverse Events (SAEs) that occur in study subjects.
An SAE is any untoward medical occurrence that at any dose:
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 50 of 177
• Results in death.• Is life-threatening.• Requires hospitalization, or prolongation of existing hospitalization.• Results in persistent or significant disability/incapacity.• Is a congenital anomaly or birth defect.
Important medical event/experience that may not result in death, be life-threatening, or require hospitalization may be considered a serious adverse event when, based upon appropriate medical judgment, may jeopardize the subject and may require medical or surgical intervention to prevent one of the outcomes listed above.
9.3 Unanticipated adverse device effect (UADE) An unanticipated adverse device effect is any serious adverse effect on health or safety or any life-threatening problem or death caused by, or associated with, a device, if that effect problem, or death was not previously identified in nature, severity, or degree of incidence in the investigational plan, or any other unanticipated serious problem associated with a device that relates to the rights, safety, or welfare of subjects.
9.4 Recording an Adverse Event All serious adverse events will be recorded and reported immediately to the Study Sponsor. An AE shall be documented when a subject reports an untoward event or when subjects are asked directly about concurrent illnesses and concomitant medication or from answers on subject-completed diary forms. When an AE is discovered or reported, the PI or designee shall complete the AE/SAE Case Report Form. The Principal Investigator shall review all AEs/SAEs and determine the severity, relationship (of the AE/SAE to the test article/investigational product), and outcome. The PI also will determine whether the subject will remain in the study.
Severity, relationship and outcome will be defined as follows:
Severity Description
Mild Awareness of signs or symptoms, but easily tolerated.
Moderate Discomfort to a degree that the AE/SAE causes interference with normal daily life activities and/or requires medication.
Severe Incapacity with regard to work or usual daily life activities. Requires medical attention/intervention.
Relationship Description
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 51 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 51 of 177
Unrelated Clearly evident relationship to other etiologies such as concomitant medications or conditions or subject’s known clinical state.
Possible Uncertain association. Other etiologies are also possible.
Probable Causal relationship cannot be ruled out.
Definite AE/SAE with a clear-cut temporal association
Outcome Description
Not recovered/Not resolved
AE/SAE had not resolved by end of study. (Does not mean AE/SAE was not followed until resolution.)
Resolved without sequelae
AE/SAE completely resolved by end of study (or ongoing yet unrelated to study, therefore resolved for purposes of study).
Resolved with sequelae
AE/SAE resolved by end of study, but aftereffect or disease or injury is present. e.g. a stroke that resulted in partial paralysis; the stroke resolved,but residual paralysis.
Death
9.5 Follow-up Study-related adverse events will be monitored to resolution by the Investigator for at least 30 days following study completion or discontinuing use of the investigational product.
Serious Adverse Events/Experiences will be followed to resolution to the extent possible (e.g., medical attention by subject’s primary care physician).
9.6 Reporting Adverse Events The Investigator will report all serious adverse events immediately to the Sponsor monitor, Sylvia L. Santos, RDH, MS at 201-572-9223, and will complete a Serious Adverse Event Form within the following timelines:
• All deaths and immediately life-threatening events, whether related or unrelated, will berecorded on the Serious Adverse Event Form and sent by email within 24 hours of siteawareness to the attention of Sylvia L. Santos at [email protected].
• Serious adverse events other than death and immediately life-threatening events,regardless of relationship, will be reported by email within 72 hours of site awareness to theattention of Sylvia L. Santos at [email protected].
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 52 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 52 of 177
The Sponsor’s representative or monitor will be notified within the time frame specified above, after any adverse event has been reported to the Investigator or Investigator’s staff.
9.7 Reporting Unanticipated Adverse Device Effects Investigators are required to submit a report of a UADE to the Sponsor and the reviewing IRB as soon as possible, but in no event later than 10 working days after the Investigator first learns of the event.
Sponsors must immediately conduct an evaluation of a UADE and must report the results of the evaluation to FDA, all reviewing IRBs, and participating Investigators within 10 working days after the Sponsor first receives notice of the effect.
10 STATISTICAL CONSIDERATIONS
Data will be manually recorded on Case Report Forms (CRFs). Salus Research will be responsible for data entry and statistical analysis of the data will be performed by Reinhard Schuller Consulting.
10.1 Sample Size Considerations It is expected that the active treatments improvement will exceed that of the negative control by at least 25% at Days 15 and 30. This translates into active treatments being superior by 0.24 with respect to MGI, and 0.4 with respect to PI when compared to the negative control at each post baseline assessment. A sample size of 90 completed and 45 per group evaluable subjects achieves a 90% power to detect treatment differences at Day 30. This assumes improvements by 0.24 with respect to MGI, and 0.4 with respect to PI, when compared to the negative control, with an effect size (mean/standard deviation) of 0.7. These calculations are based on two-sided tests at the 0.05 significance level.
10.2 Safety Review Oral soft tissue findings will be tabulated and summarized by treatment group for each exam visit. The number and percentage of subjects experiencing adverse events will be tabulated by treatment. Adverse events will be summarized according to relationship to study material and according to severity.
10.3 Demographic and Baseline Characteristics Demographic and Baseline characteristics will be summarized for age, gender, race, tobacco use, mean MGI, BI and PI, and mean number of healthy gingival sites (MGI = 0, 1). Data will be summarized using appropriate descriptive statistics (mean, median, minimum, maximum) by treatment group and overall. Categorical demographic and baseline data will be evaluated
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 53 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 53 of 177
using Fisher’s Exactness Test and continuous demographic and baseline data will be evaluated using ANOVA. All tests will be two-sided and conducted at the 0.05 significance level. No adjustments for multiple comparisons or multiple testing will be made.
10.4 Efficacy Review Post-treatment efficacy endpoints will be:
• Mean change in MGI scores at Days 15 and 30: Whole mouth Interproximal (mesial & distal)
• Change in mean number of healthy sites (MGI=0, 1) at Days 15 and 30• Mean change in BI scores at Day 15 and 30:
Whole mouth Interproximal (mesial & distal)
• Mean change in number of bleeding sites (BI=1 or2) from Baseline to “0” bleeding sitesat Days 15 and 30. Whole mouth Interproximal (mesial & distal)
• Mean change in PI scores at Baseline Pre - Post-brushing, Days 15 and 30 for: Whole mouth PI scores; Gumline PI scores (marginal);
Interproximal PI scores (mesial and distal).
For each efficacy variable summary statistics using appropriate descriptive statistics (mean, median, minimum, maximum) by treatment group and overall will be provided at each visit.
Analyses will be performed at Days 15 and 30 for each efficacy variable, analyses will be performed using the ANCOVA model with treatment as a factor and the corresponding baseline value as a covariate. The comparisons will be made at the 0.05 level, 2-sided. Tables comparing treatment groups will provide differences in the least squares mean, the standard error of the differences, the confidence interval for the difference, and the p-value. At Days 15 and 30 post ANCOVA pairwise comparisons between each of the three active treatments and the negative control will be made using a two-sided Dunnett’s test, which controls the error rate for the simultaneous comparisons.13 Differences between the means, simultaneous 95% confidence intervals and test results will be presented.
10.5 Data Sets to be Analyzed Data analysis sets will include evaluable subjects, defined as subjects who do not have major protocol violations. Data for safety analysis will include all subjects who received treatment.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 54 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 54 of 177

11 DATA HANDLING AND RECORD KEEPING
The investigator is responsible to ensure the accuracy, completeness, legibility, and timeliness of the data reported. All source documents should be completed in a neat, legible manner to ensure accurate interpretation of data. Dark ink is required to ensure clarity of reproduced copies. When making changes or corrections, cross out the original entry with a single line, and initial and date the change. DO NOT ERASE, OVERWRITE, OR USE CORRECTION FLUID OR TAPE ON THE ORIGINAL.
The investigator will prepare and maintain adequate and accurate source documents designed to record all observations and other pertinent data for each subject participating in the study. Data captured in source documents includes subject information, original records of clinical findings, observations, medical histories, prior and concomitant medication records, inclusion/exclusion eligibility checklist, records of subject visits and phone calls, progress notes, subjects’ diaries or evaluation checklists, test product dispensing and accountability records
A Case Report Form (CRF) will be completed for each subject enrolled in the study and will include documenting subject demographics and subject’s study completion status. All information recorded on the CRFs for this study must be consistent with the subject’s source documentation records. The Investigator or designee must review all entries for completeness and correctness.
The Investigator or designee agrees to make all CRFs and source documents available to the Sponsor’s Study Monitor for full inspection. After resolution of the monitor’s queries, a copy of the final CRF will be placed in the investigator’s study file and the original will be taken by the site monitor and provided to the Sponsor.
The sponsor will review the CRFs and additional source documents for completeness and adherence to the protocol.
11.1 Study Records Retention Study documents should be retained for a minimum of 2 years after the last approval of a marketing application in an ICH region and until there are no pending or contemplated marketing applications in an ICH region or until at least 2 years have elapsed since the formal discontinuation of clinical development of the investigational product. These documents should be retained for a longer period, however, if required by local regulations. No records will be destroyed without the written consent of the Sponsor, if applicable. It is the responsibility of the sponsor to inform the investigator when these documents no longer need to be retained.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 55 of 177
11.2 Protocol Deviations A protocol deviation is any noncompliance with the clinical trial protocol, Good Clinical Practice (GCP) requirements. The noncompliance may be either on the part of the subject, the investigator, or the study site staff. As a result of deviations, corrective actions are to be developed by the site and implemented promptly.
It is the responsibility of the site to use continuous vigilance to identify and report deviations within 5 working days of identification of the protocol deviation, or within 5 working days of the scheduled protocol-required activity. All deviations must be promptly reported to the Sponsor and must be addressed in study subject source documents. In addition, protocol deviations must be sent to the local IRB per their guidelines. The site PI/study staff are responsible for knowing and adhering to their IRB requirements.
12 ETHICS
12.1 Institutional Review Board This study will be reviewed by U.S. Investigational Review Board which is an appropriately constituted Institutional Review Board (IRB) as outlined in 21 CFR Part 56. The IRB will review the protocol, any amendments, the informed consent form (ICF), subject instructions, safety information, Investigator’s curriculum vitae (CV) and advertisements.
Approval by the Board must be obtained prior to the initiation of the study.
12.2 Ethical Conduct of the Study
This study will be conducted in accordance with 21 Code of Federal Regulations (CFR) Parts 50 and 56. The study will be conducted in accordance with the Principles of Good Clinical Practice.
Burst Oral Care is responsible for the ongoing safety evaluation of the investigational products and will promptly notify participating Investigators and regulatory authorities of findings that could adversely affect the safety of subjects, impact the conduct of the study, or alter the IRB’s approval to continue the study. Burst Oral Care will promptly report all adverse reactions related to the test articles that are both serious and unexpected to the appropriate regulatory authorities and to all Investigators and IRBs currently involved in studies of this test article.
12.3 Subject Information and Consent
Subject consent will be obtained prior to participation in the study as required by the regulatory guidelines (21 CFR Part 50). Subjects will be given ample opportunity to read the consent form and have all questions regarding study participation answered prior to signing the consent
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 56 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 56 of 177

form. Each subject will be provided with a signed copy of the ICF to retain for his or her records. The original signed ICF will be retained on file at the study center.
12.4 Authorization to Disclose Protected Health Information Subjects will be informed of the following information: The purpose of the protected health information (PHI) being collected, the possibility the PHI may be re-disclosed, the duration of the authorization, the right to revoke the authorization, and the right to refuse signature and limit access to PHI during and following the conduct of the trial. As applicable, written authorization to disclose PHI will be incorporated into the informed consent process and will be obtained prior to the subject entering the study. Each subject will be provided with a signed copy of the authorization and the original will be retained on file at the study center.
Subject confidentiality is strictly held in trust by the participating investigators, their staff, and the sponsor(s) and their agents. This confidentiality is extended to cover testing of biological samples and genetic tests in addition to the clinical information relating to participating subjects.
The study protocol, documentation, data, and all other information generated will be held in strict confidence. No information concerning the study or the data will be released to any unauthorized third party without prior written approval of the sponsor.
The study monitor or other authorized representatives of the sponsor may inspect all documents and records required to be maintained by the investigator, including but not limited to, medical records (office, clinic, or hospital) and pharmacy records for the subjects in this study. The clinical study site will permit access to such records.
13 MONITORING
A Sponsor representative may meet with the Investigator and his/her staff prior to the entrance of the first subject to review the procedures to be followed in conducting the study. After the enrollment of the first subject, the Investigator will permit the Sponsor to monitor the progress of the trial on site periodically. The Investigator will make available the source documents as well as the subjects’ records and signed consent forms.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 57 of 177

14 AMENDMENTS/MODIFICATION OF THIS PROTOCOL
No amendment to the protocol will be permitted without approval from the study Sponsor, Investigator, and IRB. Such changes will be documented in writing. Approval by the IRB must be obtained prior to initiation of the amendment.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 58 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 58 of 177
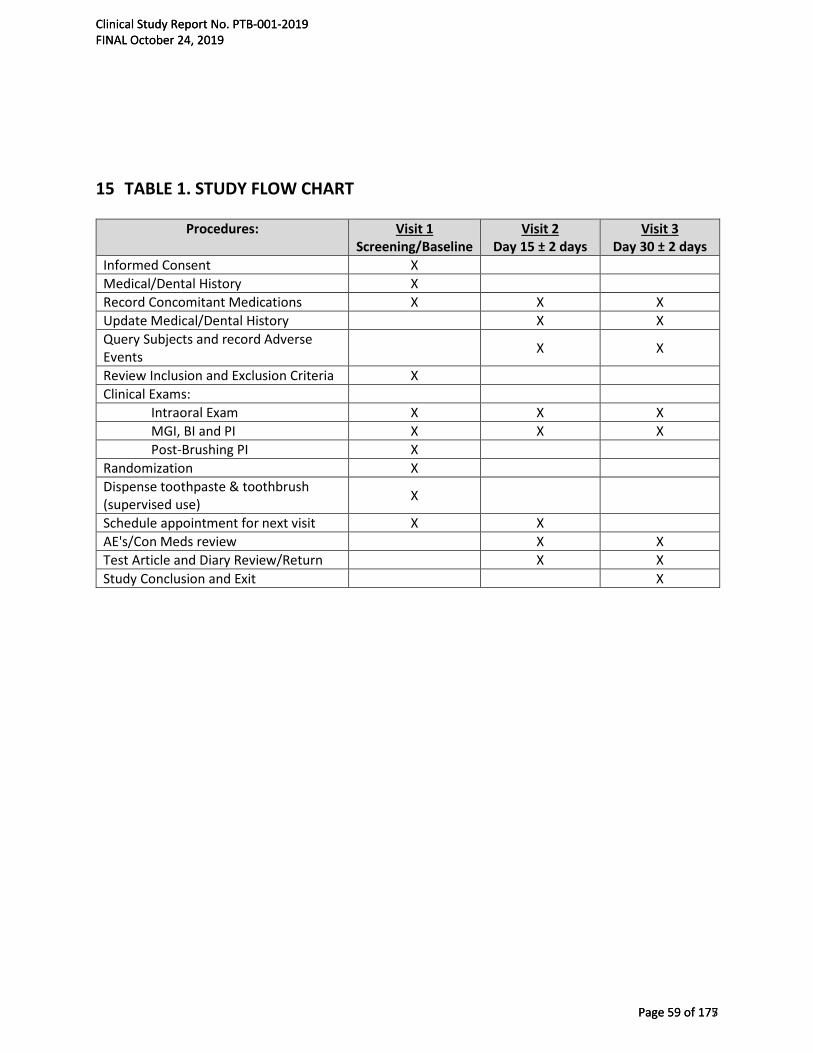
15 TABLE 1. STUDY FLOW CHART
Procedures: Visit 1 Screening/Baseline
Visit 2 Day 15 ± 2 days
Visit 3 Day 30 ± 2 days
Informed Consent X Medical/Dental History X Record Concomitant Medications X X X Update Medical/Dental History X X Query Subjects and record Adverse Events X X
Review Inclusion and Exclusion Criteria X Clinical Exams:
Intraoral Exam X X X MGI, BI and PI X X X Post-Brushing PI X
Randomization X Dispense toothpaste & toothbrush (supervised use) X
Schedule appointment for next visit X X AE's/Con Meds review X X Test Article and Diary Review/Return X X Study Conclusion and Exit X
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 59 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 59 of 177

16 REFERENCES
1. American Dental Association Mouth Healthy™ A-Z Topics.http://www.mouthhealthy.org/en/az-topics/p/plaque. Accessed July 12, 2019
2. Ebel S, Blättermann H, Weik U, Margraf-Stiksrud J and Deinzer R. High plaque levelsafter thorough toothbrushing: What impedes efficacy? J Dent Res. 2018;4(2):135-142.
3. Davidovich E, Ccahuana-Vasquez RA, Timm H, Grender J, Cunningham P, Zini A.Randomised clinical study of plaque removal efficacy of a power toothbrush in apaediatric population. International Journal of Paediatric Dentistry. 2017;Nov;27(6):558-567. doi: 10.1111/ipd.12298. Epub 2017 May 11.
4. Klukowska M, Grender JM, Timm H. A single-brushing study to compare plaque removalefficacy of a new power brush to an ADA reference manual toothbrush. Am J Dent 2012;25: 10A– 13A.
5. Starke EM, Mwatha A, Ward M, Argosino K, Jenkins W, Milleman JL, Milleman KR. AComparison of the Effects of a Powered and Manual Toothbrush on Gingivitis andPlaque: A Randomized Parallel Clinical Trial. J Clin Dent 2019;30(Spec Iss A)A24–29.
6. Delaurenti M, Ward M, Souza S, Jenkins W, Putt MS, Milleman KR, Milleman JL. TheEffect of Use of a Sonic Power Toothbrush and a Manual Toothbrush Control on Plaqueand Gingivitis. J Clin Dent. 2017 Mar;28(1 Spec No A):A1-6.
7. Sharma NC, Klukowska M, Mielczarek A, Grender JM, Qaqish J. A 4-week clinicalcomparison of a novel multi-directional power brush to a manual toothbrush in thereduction of gingivitis and plaque. Am J Dent. 2012 Sep;25 Spec No A(A):14A-20A
8. Yaacob M, Worthington HV, Deacon SA, et al. Powered versus manual toothbrushing fororal health. Cochrane Database Syst Rev 2014; 6: CD002281.
9. Lobene RR, Weatherford T, Ross NM, Lamm RA, Menaker L. A modified gingival indexfor use in clinical trials. Clin Prev Dent. 1986;8(1):3-6.
10. Saxton CA, van der Ouderaa FJ. The effect of a dentifrice containing zinc citrate andtriclosan on developing gingivitis. J Periodontol 1989;24:75-80.
11. Turesky S, Gilmore ND, Glickman I. Reduced plaque formation by the chloromethylanalogue of victamine C. J Periodontol. 1970;41(1):41-43.
12. Lobene RR, Soparkar PM, Newman MB. Use of dental floss. Effect on plaque andgingivitis. Clin Prev Dent. 1982;4(1):5-8.
13. Westfall PH, Tobias RD, Rom D, Wolfinger RD, Hochberg Y. Multiple Comparisons andMultiple Testing Using the SAS System. SAS Institute Inc. Cary NC, 1999.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 60 of 177

4.1.2 Case Report Forms
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 61 of 177
CASE REPORT FORMS
Study No.
PTB-001-2019
Screening Number 1
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 62 of 177

SUBJECT DEMOGRAPHICS
Date of Birth / /
dd mmm yyyy
Gender ☐ Male ☐ Female
RACE (Select One):
☐ American Indian/Alaskan Native ☐Native Hawaiian or other Pacific Islander
☐ Black or African American ☐ Asian
☐ White ☐
Other, please specify:
Ethnicity (Select One):
☐ Hispanic or Latino ☐ Non-Hispanic or Latino
Tobacco Use: Smoker: yes ☐ no ☐
Smokeless Tobacco: yes ☐ no ☐
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 63 of 177

ORAL EXAM
LOCATION Normal Abnormal Describe Abnormality
Mucosa (including lips) ☐ ☐
Gingival Mucosa ☐ ☐
Hard Palate ☐ ☐
Soft Palate ☐ ☐
Mucogingival Folds ☐ ☐
Tongue ☐ ☐
Sublingual Area ☐ ☐
Submandibular Area ☐ ☐
Salivary Glands ☐ ☐
Tonsilar Area ☐ ☐
Pharyngeal Area ☐ ☐
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 64 of 177

MODIFIED GINGIVAL INDEX
MAXILLARY
Tooth 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Palatal
MANDIBULAR
Tooth 31 30 29 28 27 26 25 24 23 22 21 20 19 18
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Lingual
Area Total # Sites Mean Maxilla
Mandible Total
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 65 of 177
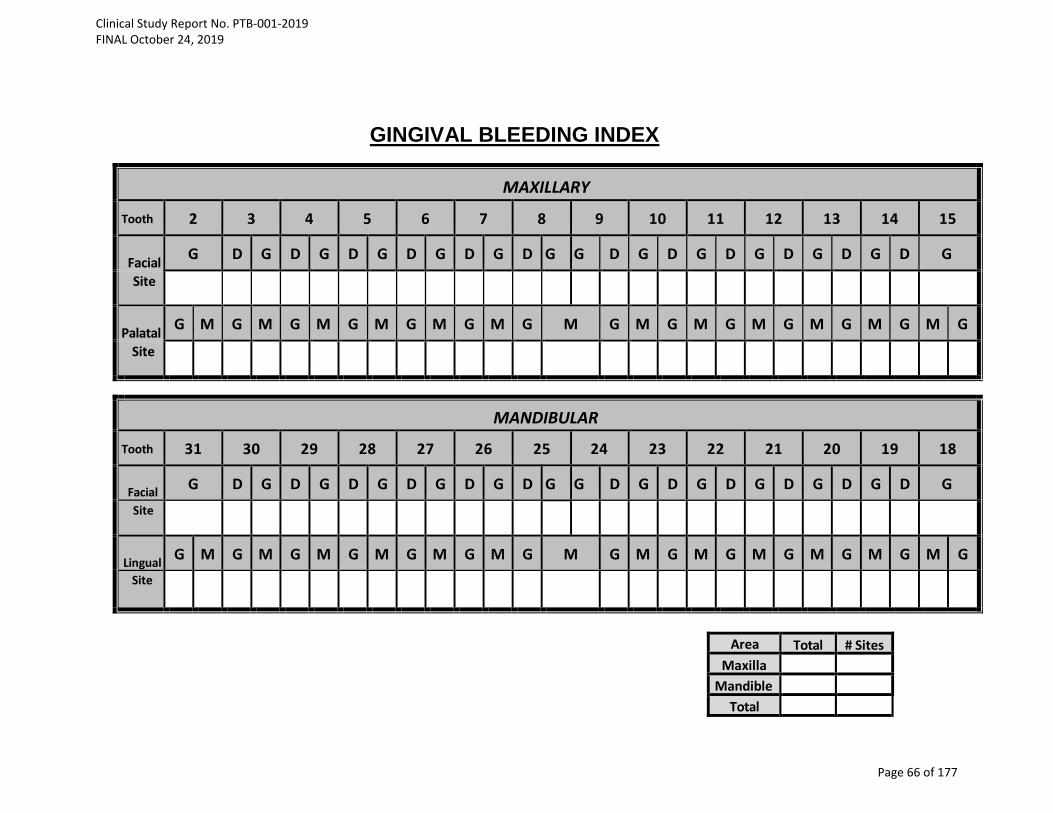
GINGIVAL BLEEDING INDEX
MAXILLARY
Tooth 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Facial G D G D G D G D G D G D G G D G D G D G D G D G D G
Site
Palatal G M G M G M G M G M G M G M G M G M G M G M G M G M G
Site
MANDIBULAR
Tooth 31 30 29 28 27 26 25 24 23 22 21 20 19 18
Facial G D G D G D G D G D G D G G D G D G D G D G D G D G Site
Lingual G M G M G M G M G M G M G M G M G M G M G M G M G M G Site
Area Total # Sites Maxilla
Mandible Total
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 66 of 177
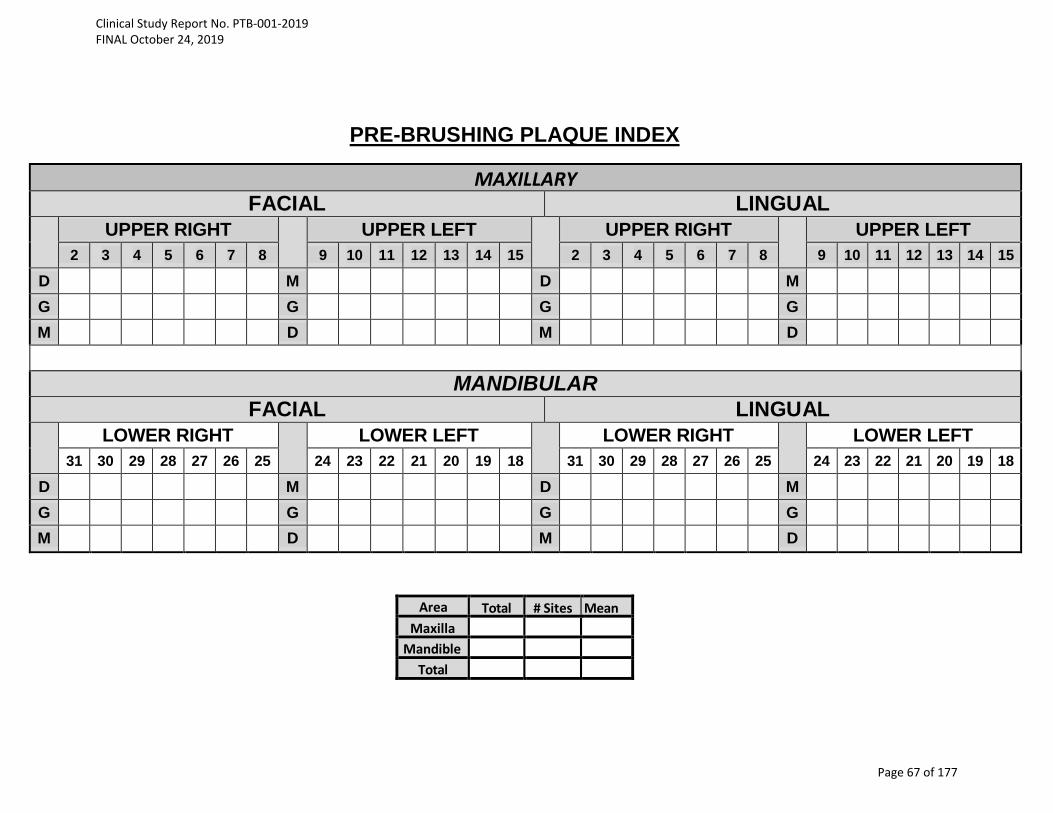
PRE-BRUSHING PLAQUE INDEX
MAXILLARY FACIAL LINGUAL
UPPER RIGHT UPPER LEFT UPPER RIGHT UPPER LEFT 2 3 4 5 6 7 8 9 10 11 12 13 14 15 2 3 4 5 6 7 8 9 10 11 12 13 14 15
D M D M G G G G
M D M D
MANDIBULAR FACIAL LINGUAL
LOWER RIGHT LOWER LEFT LOWER RIGHT LOWER LEFT 31 30 29 28 27 26 25 24 23 22 21 20 19 18 31 30 29 28 27 26 25 24 23 22 21 20 19 18
D M D M G G G G
M D M D
Area Total # Sites Mean Maxilla
Mandible Total
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 67 of 177
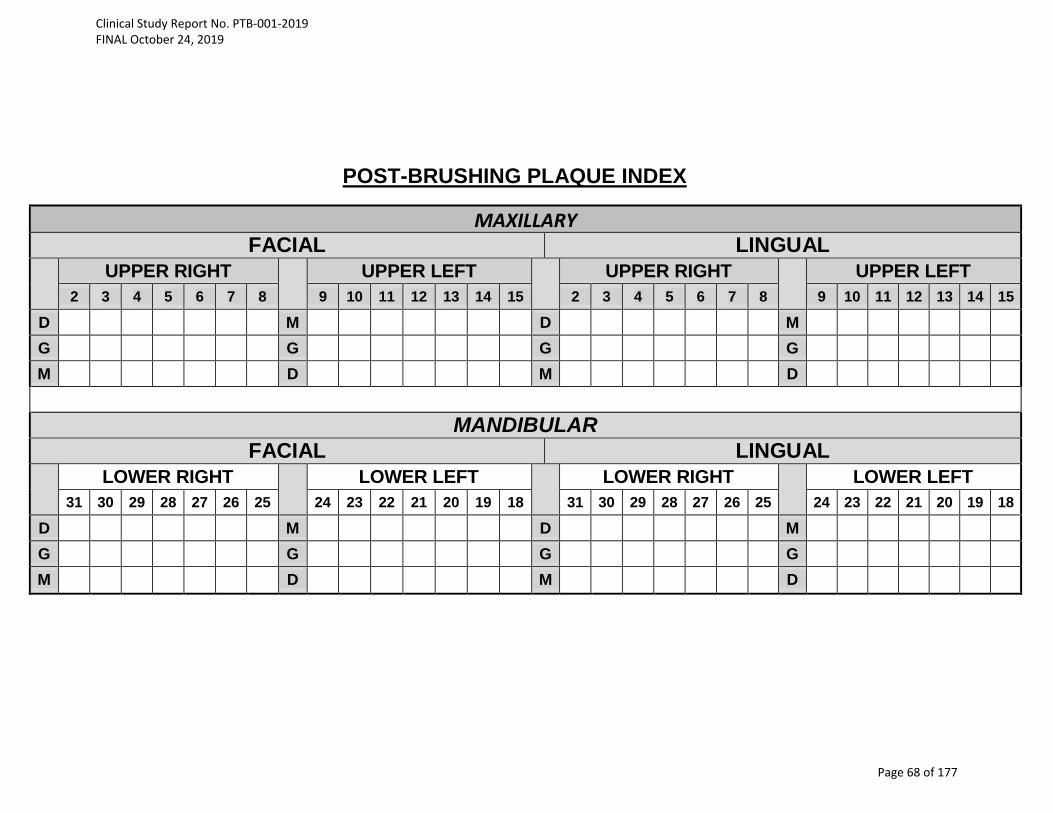
POST-BRUSHING PLAQUE INDEX
MAXILLARY FACIAL LINGUAL
UPPER RIGHT UPPER LEFT UPPER RIGHT UPPER LEFT 2 3 4 5 6 7 8 9 10 11 12 13 14 15 2 3 4 5 6 7 8 9 10 11 12 13 14 15
D M D M G G G G
M D M D
MANDIBULAR FACIAL LINGUAL
LOWER RIGHT LOWER LEFT LOWER RIGHT LOWER LEFT 31 30 29 28 27 26 25 24 23 22 21 20 19 18 31 30 29 28 27 26 25 24 23 22 21 20 19 18
D M D M G G G G
M D M D
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 68 of 177

SCREENING ELIGIBILITY DETERMINATION
Subject meets eligibility entry criteria:
All criteria must have positive response
• MGI score of 1.75-2.3 YES ☐1 NO ☐2
• BI score ≥ 20 YES ☐1 NO ☐2
• PI score ≥1.95 YES ☐1 NO ☐2
Randomization Number
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 69 of 177

ORAL EXAM
LOCATION Normal Abnormal Describe Abnormality
Mucosa (including lips) ☐ ☐
Gingival Mucosa ☐ ☐
Hard Palate ☐ ☐
Soft Palate ☐ ☐
Mucogingival Folds ☐ ☐
Tongue ☐ ☐
Sublingual Area ☐ ☐
Submandibular Area ☐ ☐
Salivary Glands ☐ ☐
Tonsilar Area ☐ ☐
Pharyngeal Area ☐ ☐
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 70 of 177

MODIFIED GINGIVAL INDEX
MAXILLARY
Tooth 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Palatal
MANDIBULAR
Tooth 31 30 29 28 27 26 25 24 23 22 21 20 19 18
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Lingual
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 71 of 177
GINGIVAL BLEEDING INDEX
MAXILLARY
Tooth 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Facial G D G D G D G D G D G D G G D G D G D G D G D G D G
Site
Palatal G M G M G M G M G M G M G M G M G M G M G M G M G M G
Site
MANDIBULAR
Tooth 31 30 29 28 27 26 25 24 23 22 21 20 19 18
Facial G D G D G D G D G D G D G G D G D G D G D G D G D G Site
Lingual G M G M G M G M G M G M G M G M G M G M G M G M G M G Site
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 72 of 177
PLAQUE INDEX
MAXILLARY FACIAL LINGUAL
UPPER RIGHT UPPER LEFT UPPER RIGHT UPPER LEFT 2 3 4 5 6 7 8 9 10 11 12 13 14 15 2 3 4 5 6 7 8 9 10 11 12 13 14 15
D M D M G G G G
M D M D
MANDIBULAR FACIAL LINGUAL
LOWER RIGHT LOWER LEFT LOWER RIGHT LOWER LEFT 31 30 29 28 27 26 25 24 23 22 21 20 19 18 31 30 29 28 27 26 25 24 23 22 21 20 19 18
D M D M G G G G
M D M D
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 73 of 177
ORAL EXAM
LOCATION Normal Abnormal Describe Abnormality
Mucosa (including lips) ☐ ☐
Gingival Mucosa ☐ ☐
Hard Palate ☐ ☐
Soft Palate ☐ ☐
Mucogingival Folds ☐ ☐
Tongue ☐ ☐
Sublingual Area ☐ ☐
Submandibular Area ☐ ☐
Salivary Glands ☐ ☐
Tonsilar Area ☐ ☐
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 74 of 177
MODIFIED GINGIVAL INDEX
MAXILLARY
Tooth 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Palatal
MANDIBULAR
Tooth 31 30 29 28 27 26 25 24 23 22 21 20 19 18
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Lingual
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 75 of 177
GINGIVAL BLEEDING INDEX
MAXILLARY
Tooth 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Facial G D G D G D G D G D G D G G D G D G D G D G D G D G
Site
Palatal G M G M G M G M G M G M G M G M G M G M G M G M G M G
Site
MANDIBULAR
Tooth 31 30 29 28 27 26 25 24 23 22 21 20 19 18
Facial G D G D G D G D G D G D G G D G D G D G D G D G D G Site
Lingual G M G M G M G M G M G M G M G M G M G M G M G M G M G Site
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 76 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 76 of 177

PLAQUE INDEX
MAXILLARY FACIAL LINGUAL
UPPER RIGHT UPPER LEFT UPPER RIGHT UPPER LEFT 2 3 4 5 6 7 8 9 10 11 12 13 14 15 2 3 4 5 6 7 8 9 10 11 12 13 14 15
D M D M G G G G
M D M D
MANDIBULAR FACIAL LINGUAL
LOWER RIGHT LOWER LEFT LOWER RIGHT LOWER LEFT 31 30 29 28 27 26 25 24 23 22 21 20 19 18 31 30 29 28 27 26 25 24 23 22 21 20 19 18
D M D M G G G G
M D M D
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 77 of 177
SUBJECT SUMMARY
1. Did subject experience an AdverseEvent?
Yes ☐ No ☐
2. Date Subject first used test article: - -
dd/mmm/yyyy
3. Date Subject last used test article: - -
dd/mmm/yyyy
4. Did the Subject complete the studyas planned? Yes ☐ No ☐
If 'No', indicate ONE reason:
Withdrawal of consent ☐
Deviation from protocol (including non-compliance)
☐
Lost to follow-up ☐
Adverse Event ☐
Other (give details)_______________________
☐
5. Date of Last Visit: - -
dd/mmm/yyyy
Date: - -
Investigator Signature dd/mmm/yyyy
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 78 of 177
Adverse Event Form Complete this form only if subject experienced any Adverse Events during this study
Page ___ of ___
Severity Study Intervention Relationship
Action Taken Regarding Study Intervention
Outcome of AE Serious
1 = Mild 2 = Moderate 3 = Severe
1 = Unrelated 2 = Possible 3 = Probable 4 = Definite
1 = None 2 = Rx Therapy 3 = Discontinued Study 4 = Other (specify)
1= Resolved w/o sequelae 2 = Resolved w/sequelae 3 = Not recovered/resolved 4 = Death
1 = Yes 2 = No (If yes, complete SAE form)
Adverse Event Start Date (dd/mmm/yyyy)
Stop Date (dd/mmm/yyyy)
Severity Relationship to
Study Treatment
Action Taken
Outcome of AE
Serious Adverse Event?
1.
2.
3.
4.
5.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 79 of 177
1. SAE Onset Date: _____/______/________ (dd/mmm/yyyy)
2. SAE Stop Date: ____/______/________(dd/mmm/yyyy)
3. Was this an unexpected adverse event? Yes No
4. Brief description of participant(s) with no personal identifiers:
Sex: F M Date of Birth: _____/______/________ (dd/mmm/yyyy)
5. Brief description of the nature of the serious adverse event (attach descriptionif more space needed):___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
6. Category of the serious adverse event:
death – date ____/_______/________ (dd/mmm/yyyy) congenital anomaly / birth defect
life-threatening required intervention to prevent
hospitalization-initial or prolonged permanent impairment
disability / incapacity
other:__________________
7. Relationship of event to study test material:
Unrelated (clearly not related to the intervention)
Possible (may be related to intervention)
Definite (clearly related to intervention)
Serious Adverse Event
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 80 of 177

8. Was study test material/participation discontinued due to event? Yes No
9. What medications or other steps were taken to treat serious adverse event?
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
10. List any relevant tests, laboratory data, history, including preexisting medicalconditions
_____________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
11. Type of report:
Initial
Follow-up
Final
Signature of Principal Investigator: _____________________________Date: _____/______/________
(dd/mmm/yyyy)
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 81 of 177

4.1.3 Ethics Committees and Subject Information
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 82 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 83 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 84 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 85 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 86 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 87 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 88 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 89 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 90 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 91 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 92 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 93 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 94 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 95 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 96 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 97 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 98 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 99 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 100 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 101 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 102 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 103 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 104 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 105 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 106 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 107 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 108 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 109 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 110 of 177
4.1.4 Investigators and Study Personnel
Curriculum Vitae and License copies are attached for the following study personnel:
Investigator: Jeffery L. Milleman, DDS, MPA
Sub Investigator: Kimberly R. Milleman, RDH, BS, MS
Study Coordinator: Abigale Yoder, AS, BS
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 111 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 112 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 113 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 114 of 177

4.1.5 Sponsor and Investigator Signatures
Sponsor and Investigator Signatures appear on page 2 of this report.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 115 of 177

4.1.6 Randomization Scheme and Codes
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 116 of 177

block identifier
Random No
sequence within block
Treatment
1 001 1 Group A1 002 2 Group A1 003 3 Group B1 004 4 Group B2 005 1 Group A2 006 2 Group B2 007 3 Group A2 008 4 Group B3 009 1 Group A3 010 2 Group B3 011 3 Group A3 012 4 Group B4 013 1 Group A4 014 2 Group B4 015 3 Group A4 016 4 Group B5 017 1 Group A5 018 2 Group B5 019 3 Group A5 020 4 Group B6 021 1 Group B6 022 2 Group A6 023 3 Group A6 024 4 Group B7 025 1 Group A7 026 2 Group B7 027 3 Group A7 028 4 Group B8 029 1 Group B8 030 2 Group A8 031 3 Group B8 032 4 Group A9 033 1 Group A9 034 2 Group B9 035 3 Group B9 036 4 Group A
10 037 1 Group A10 038 2 Group A10 039 3 Group B10 040 4 Group B11 041 1 Group B11 042 2 Group B11 043 3 Group A11 044 4 Group A
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 117 of 177

12 045 1 Group A12 046 2 Group B12 047 3 Group B12 048 4 Group A13 049 1 Group A13 050 2 Group A13 051 3 Group B13 052 4 Group B14 053 1 Group A14 054 2 Group B14 055 3 Group B14 056 4 Group A15 057 1 Group A15 058 2 Group A15 059 3 Group B15 060 4 Group B16 061 1 Group B16 062 2 Group B16 063 3 Group A16 064 4 Group A17 065 1 Group A17 066 2 Group B17 067 3 Group B17 068 4 Group A18 069 1 Group B18 070 2 Group B18 071 3 Group A18 072 4 Group A19 073 1 Group A19 074 2 Group A19 075 3 Group B19 076 4 Group B20 077 1 Group A20 078 2 Group B20 079 3 Group B20 080 4 Group A21 081 1 Group B21 082 2 Group B21 083 3 Group A21 084 4 Group A22 085 1 Group B22 086 2 Group A22 087 3 Group A22 088 4 Group B23 089 1 Group A23 090 2 Group B23 091 3 Group A
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 118 of 177

23 092 4 Group B24 093 1 Group A24 094 2 Group B24 095 3 Group A24 096 4 Group B25 097 1 Group A25 098 2 Group B25 099 3 Group B25 100 4 Group A
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 119 of 177
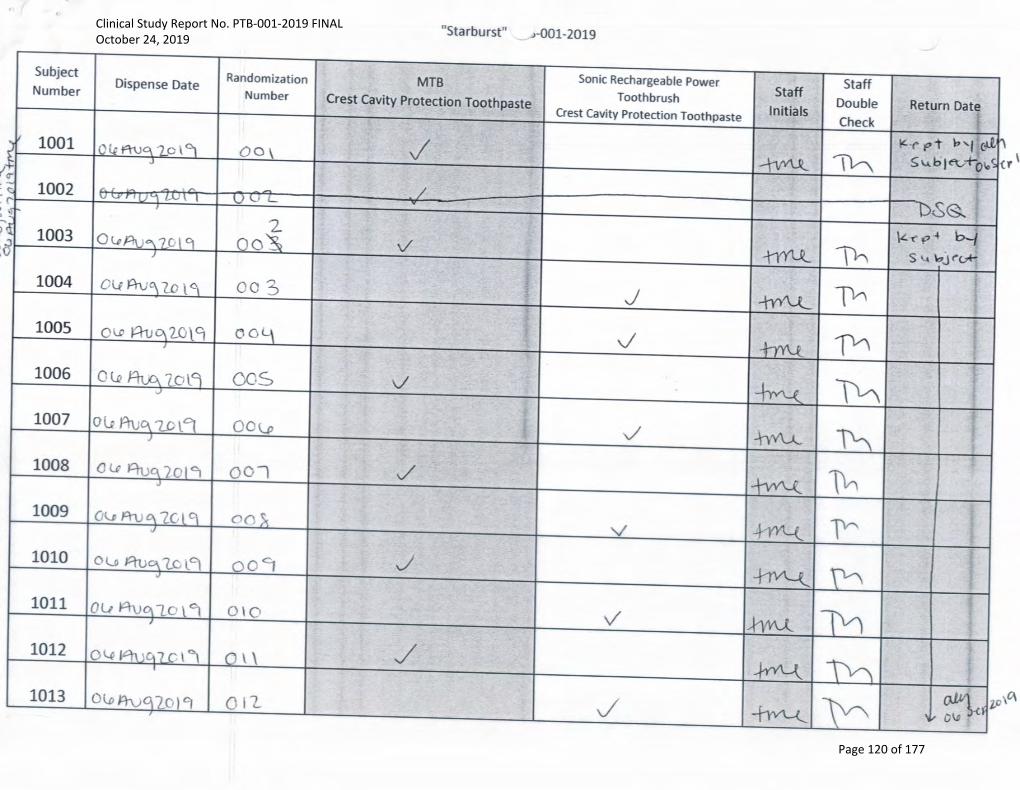
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 120 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 121 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 122 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 123 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 124 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 125 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 126 of 177
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 127 of 177
From: Abbie YoderTo: ANGELA MORRIS; Reinhard SchullerCc: Sylvia Santos; [email protected]: Re: Randomization codes for Salus BURST studyDate: September 27, 2019 4:14:45 PM
Hello,
Here is the randomization code for the BURST study:A=Manual BrushB=Burst Brush
Let me know if you need anything else!
Thanks,
Abbie
Get Outlook for iOS
On Fri, Sep 27, 2019 at 3:51 PM -0400, "ANGELA MORRIS" <[email protected]>wrote:
Hi Reinhard: Attached please find the master randomization list. I've also copied Abbie on this email
because she'll be able to release the treatment / randomization assignment codes to you.
Hi Abbie: will you please send the treatment code assignment for study PTB-001-2019 to Reinhard
today? I really appreciate your help with this urgent request!
Many thanks and best regards,
Angie
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 128 of 177

4.1.7 Publications Referenced in the Report
Copies of publications are maintained in section 9.2 (References) of the TMF
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 129 of 177

4.2 Subject Data Listings
4.2.1 Protocol Deviations
A summary of protocol deviations is provided in the attached log.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 130 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 131 of 177

Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 132 of 177

4.2.2 Demographic Data
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 133 of 177
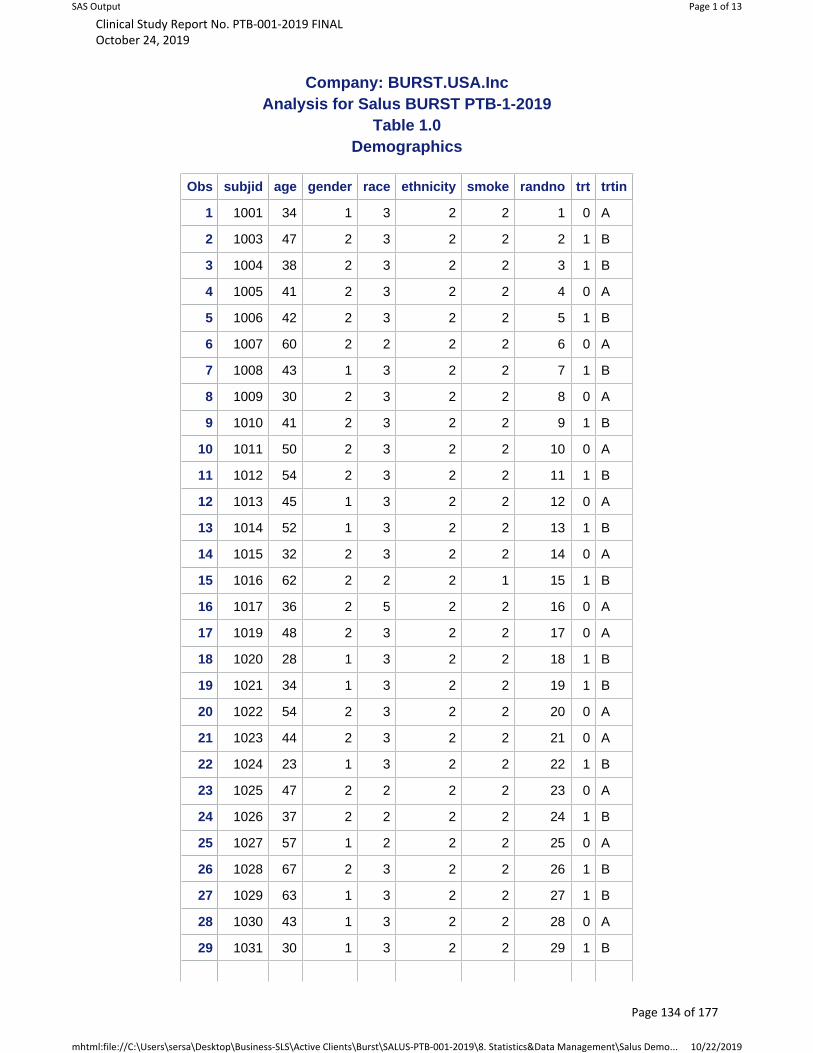
Company: BURST.USA.Inc Analysis for Salus BURST PTB-1-2019
Table 1.0Demographics
Obs subjid age gender race ethnicity smoke randno trt trtin
1 1001 34 1 3 2 2 1 0 A
2 1003 47 2 3 2 2 2 1 B
3 1004 38 2 3 2 2 3 1 B
4 1005 41 2 3 2 2 4 0 A
5 1006 42 2 3 2 2 5 1 B
6 1007 60 2 2 2 2 6 0 A
7 1008 43 1 3 2 2 7 1 B
8 1009 30 2 3 2 2 8 0 A
9 1010 41 2 3 2 2 9 1 B
10 1011 50 2 3 2 2 10 0 A
11 1012 54 2 3 2 2 11 1 B
12 1013 45 1 3 2 2 12 0 A
13 1014 52 1 3 2 2 13 1 B
14 1015 32 2 3 2 2 14 0 A
15 1016 62 2 2 2 1 15 1 B
16 1017 36 2 5 2 2 16 0 A
17 1019 48 2 3 2 2 17 0 A
18 1020 28 1 3 2 2 18 1 B
19 1021 34 1 3 2 2 19 1 B
20 1022 54 2 3 2 2 20 0 A
21 1023 44 2 3 2 2 21 0 A
22 1024 23 1 3 2 2 22 1 B
23 1025 47 2 2 2 2 23 0 A
24 1026 37 2 2 2 2 24 1 B
25 1027 57 1 2 2 2 25 0 A
26 1028 67 2 3 2 2 26 1 B
27 1029 63 1 3 2 2 27 1 B
28 1030 43 1 3 2 2 28 0 A
29 1031 30 1 3 2 2 29 1 B
Page 1 of 13SAS Output
10/22/2019mhtml:file://C:\Users\sersa\Desktop\Business-SLS\Active Clients\Burst\SALUS-PTB-001-2019\8. Statistics&Data Management\Salus Demo...
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 134 of 177

30 1032 65 2 3 2 2 30 0 A
31 1033 48 2 3 2 2 31 0 A
32 1034 59 2 3 2 2 32 1 B
33 1035 55 2 2 2 2 33 1 B
34 1036 46 1 3 2 2 34 0 A
35 1037 67 2 3 2 2 35 0 A
36 1038 26 2 2 2 2 36 0 A
37 1039 60 1 3 2 2 37 1 B
38 1040 53 2 3 2 2 38 1 B
39 1041 24 2 3 2 2 39 1 B
40 1042 48 2 3 2 2 40 1 B
41 1043 51 1 1 2 2 41 0 A
42 1044 40 1 3 2 2 42 0 A
43 1045 37 2 3 2 2 43 0 A
44 1046 31 2 3 2 2 44 1 B
45 1047 38 2 3 2 2 45 1 B
46 1048 47 2 3 2 2 46 0 A
47 1049 32 2 2 2 2 47 0 A
48 1050 24 2 3 2 2 48 0 A
49 1051 36 1 3 2 2 49 1 B
50 1052 52 2 3 2 2 50 1 B
51 1053 68 2 3 2 2 51 0 A
52 1054 23 2 3 2 2 52 1 B
53 1055 56 2 2 2 2 53 1 B
54 1056 54 2 2 2 2 54 0 A
55 1057 51 2 3 2 2 55 0 A
56 1058 40 1 3 2 2 56 0 A
57 1059 66 2 3 2 2 57 1 B
58 1060 39 2 3 2 1 58 1 B
59 1061 37 2 3 2 2 59 1 B
60 1062 57 2 3 2 2 60 1 B
61 1063 49 2 3 2 2 61 0 A
62 1064 20 2 3 2 2 62 0 A
63 1065 70 1 1 1 2 63 0 A
64
Page 2 of 13SAS Output
10/22/2019mhtml:file://C:\Users\sersa\Desktop\Business-SLS\Active Clients\Burst\SALUS-PTB-001-2019\8. Statistics&Data Management\Salus Demo...
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 135 of 177
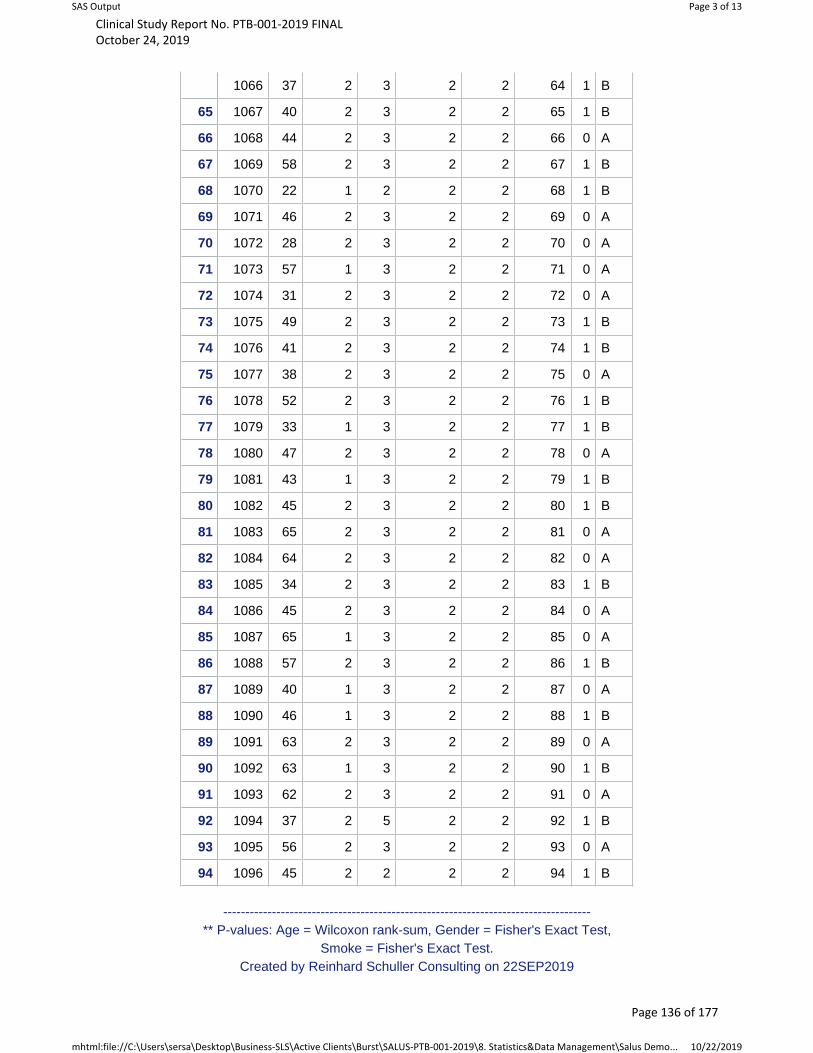
1066 37 2 3 2 2 64 1 B
65 1067 40 2 3 2 2 65 1 B
66 1068 44 2 3 2 2 66 0 A
67 1069 58 2 3 2 2 67 1 B
68 1070 22 1 2 2 2 68 1 B
69 1071 46 2 3 2 2 69 0 A
70 1072 28 2 3 2 2 70 0 A
71 1073 57 1 3 2 2 71 0 A
72 1074 31 2 3 2 2 72 0 A
73 1075 49 2 3 2 2 73 1 B
74 1076 41 2 3 2 2 74 1 B
75 1077 38 2 3 2 2 75 0 A
76 1078 52 2 3 2 2 76 1 B
77 1079 33 1 3 2 2 77 1 B
78 1080 47 2 3 2 2 78 0 A
79 1081 43 1 3 2 2 79 1 B
80 1082 45 2 3 2 2 80 1 B
81 1083 65 2 3 2 2 81 0 A
82 1084 64 2 3 2 2 82 0 A
83 1085 34 2 3 2 2 83 1 B
84 1086 45 2 3 2 2 84 0 A
85 1087 65 1 3 2 2 85 0 A
86 1088 57 2 3 2 2 86 1 B
87 1089 40 1 3 2 2 87 0 A
88 1090 46 1 3 2 2 88 1 B
89 1091 63 2 3 2 2 89 0 A
90 1092 63 1 3 2 2 90 1 B
91 1093 62 2 3 2 2 91 0 A
92 1094 37 2 5 2 2 92 1 B
93 1095 56 2 3 2 2 93 0 A
94 1096 45 2 2 2 2 94 1 B
-----------------------------------------------------------------------------------** P-values: Age = Wilcoxon rank-sum, Gender = Fisher's Exact Test,
Smoke = Fisher's Exact Test. Created by Reinhard Schuller Consulting on 22SEP2019
Page 3 of 13SAS Output
10/22/2019mhtml:file://C:\Users\sersa\Desktop\Business-SLS\Active Clients\Burst\SALUS-PTB-001-2019\8. Statistics&Data Management\Salus Demo...
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 136 of 177

4.2.3 Individual Efficacy Response Data
Individual efficacy data listing are provided in the TMF, section 8.1
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 137 of 177
4.2.4 Statistical Report
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 138 of 177
Statistical Report
Protocol Title:
Clinical Efficacy of a Sonic Power Toothbrush in Adults
with Plaque and Gingivitis in a Thirty-Day Model
Protocol:
BURST.USA Inc. Study Number: PTB-001-2019
FINAL
October 21, 2019
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 137 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 139 of 177
Table of Contents
Executive Summary .......................................................................................................... 3 Demographic and Baseline Data .................................................................................................. 3
Modified Gingival Index Summary ............................................................................................. 4
Bleeding Index Summary ............................................................................................................ 5
Plaque Index Summary ................................................................................................................ 7
Overall Summary ......................................................................................................................... 9
Study Synopsis and Objectives ...................................................................................... 10 Inclusion and Exclusion Criteria ................................................................................................ 10
Analysis Endpoints .................................................................................................................... 10
Sample Size and Statistical Analysis ......................................................................................... 11
Results .............................................................................................................................. 12 Demographic and Baseline ........................................................................................................ 12
Modified Gingival Index ........................................................................................................... 12
Bleeding Index ........................................................................................................................... 15
Plaque Index .............................................................................................................................. 18
Conclusion ....................................................................................................................... 20 Appendix .......................................................................................................................... 21
Tables ......................................................................................................................................... 21
Data Displays ............................................................................................................................. 37
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 140 of 177
Executive Summary
The objective of this 30-day, randomized, controlled, examiner-blind, parallel design
clinical trial is to assess the safety and efficacy of twice daily use of a marketed sonic
power toothbrush (BURST Sonic) on plaque and gingivitis, compared to a manual
toothbrush when brushing with a standard fluoride dentifrice.
The two treatment groups are:
• Group 1: Twice daily brushing with ADA standard manual toothbrush and fluoridetoothpaste (MB)
• Group 2: Twice daily brushing with BURST sonic toothbrush and fluoride toothpaste(SB)
This Executive Summary provides summary results of the following assessments:
Modified Gingival Index (MGI), Bleeding Index (BI), Plaque Index (PI) and changes in
healthy sites; along with efficacy comparisons of the two toothbrushes following 30 days
of use. The body of the report and the Appendix Tables provide more information.
Demographic and Baseline Data
Ninety-four (94) subjects were randomized and all but two completed the study. The
gender breakdown was 68 females and 26 males. The mean age was 45.8 with the
minimum age being 20 years and the maximum being 70 years. Two of the study
participants were smokers. All baseline, gingival and plaque endpoints were comparable
between toothbrushes. The number of scorable teeth was also comparable between
treatments. Full demographic summary data are given in Appendix Table 1.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 139 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 141 of 177
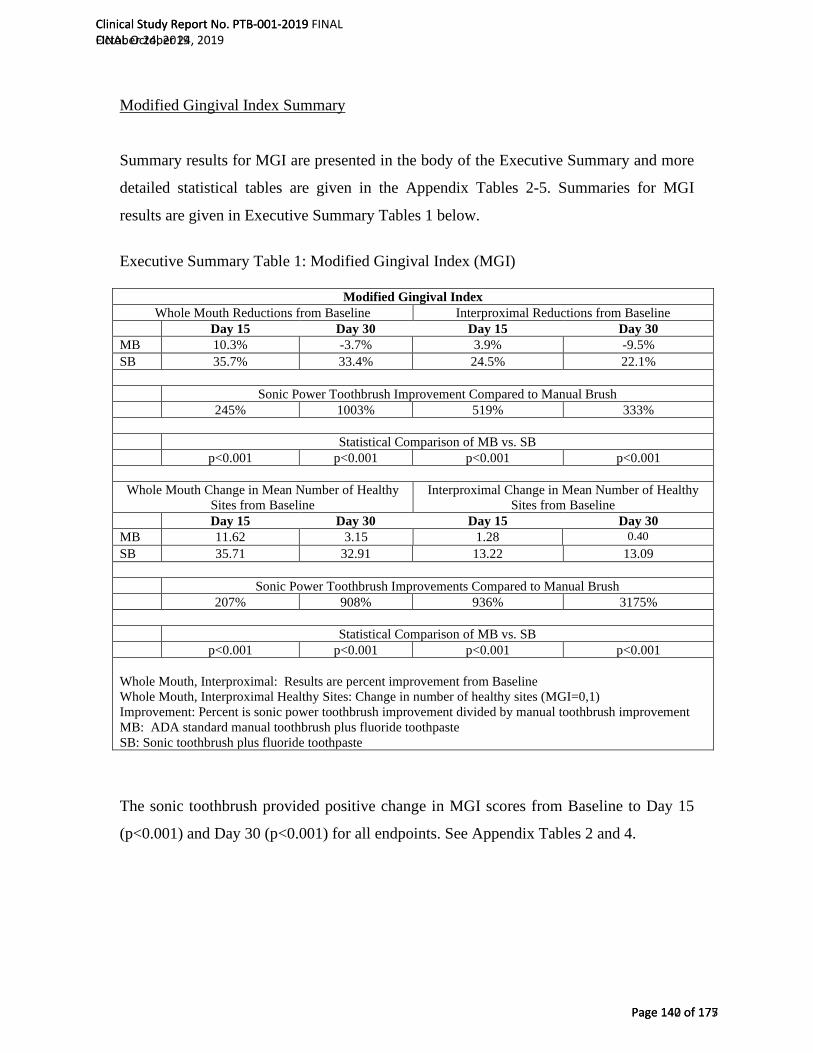
Modified Gingival Index Summary
Summary results for MGI are presented in the body of the Executive Summary and more
detailed statistical tables are given in the Appendix Tables 2-5. Summaries for MGI
results are given in Executive Summary Tables 1 below.
Executive Summary Table 1: Modified Gingival Index (MGI)
Modified Gingival Index Whole Mouth Reductions from Baseline Interproximal Reductions from Baseline
Day 15 Day 30 Day 15 Day 30 MB 10.3% -3.7% 3.9% -9.5%SB 35.7% 33.4% 24.5% 22.1%
Sonic Power Toothbrush Improvement Compared to Manual Brush 245% 1003% 519% 333%
Statistical Comparison of MB vs. SB p<0.001 p<0.001 p<0.001 p<0.001
Whole Mouth Change in Mean Number of Healthy Sites from Baseline
Interproximal Change in Mean Number of Healthy Sites from Baseline
Day 15 Day 30 Day 15 Day 30 MB 11.62 3.15 1.28 0.40 SB 35.71 32.91 13.22 13.09
Sonic Power Toothbrush Improvements Compared to Manual Brush 207% 908% 936% 3175%
Statistical Comparison of MB vs. SB p<0.001 p<0.001 p<0.001 p<0.001
Whole Mouth, Interproximal: Results are percent improvement from Baseline Whole Mouth, Interproximal Healthy Sites: Change in number of healthy sites (MGI=0,1) Improvement: Percent is sonic power toothbrush improvement divided by manual toothbrush improvement MB: ADA standard manual toothbrush plus fluoride toothpaste SB: Sonic toothbrush plus fluoride toothpaste
The sonic toothbrush provided positive change in MGI scores from Baseline to Day 15
(p<0.001) and Day 30 (p<0.001) for all endpoints. See Appendix Tables 2 and 4.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 140 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 142 of 177
The sonic toothbrush reduced whole mouth MGI by an average of 34.6% at both Day 15
and Day 30. The sonic toothbrush provided superior gains compared to the manual
toothbrush for all MGI endpoints evaluated at Day 15 and Day 30. Improvements in
whole mouth and interproximal scores were statistically significantly better when
compared to the manual toothbrush (p<0.001).
The sonic toothbrush produced changes in mean number of whole mouth healthy sites at
both Day 15 and Day 30 that were statistically significantly superior to the manual
toothbrush (p<0.001).
Bleeding Index Summary
Both toothbrushes provided positive change from Baseline to Day 15 (p<0.005) and Day
30 (p<0.001) for all BI endpoints (see Appendix Tables 6 to Table 9).
The sonic toothbrush provided gains over the manual toothbrush for all gingival bleeding
endpoints evaluated at Day 15 and Day 30. Whole mouth and interproximal
improvements were statistically significant from the manual toothbrush (p<0.001).
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 141 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 143 of 177

Summary results for gingival bleeding endpoints are given in Executive Summary Table 2 below.
Executive Summary Table 2: Bleeding Index (BI)
Bleeding Index Whole Mouth Reductions from Baseline Interproximal Reductions from Baseline
Day 15 Day 30 Day 15 Day 30 MB 16.2% 20.3% 14.0% 24.3% SB 64.8% 66.3% 66.7% 67.6%
Sonic Power Toothbrush Improvement Compared to Manual Brush 301% 227% 376% 179%
Statistical Comparison of MB vs. SB p<0.001 p<0.001 p<0.001 p<0.001
Whole Mouth Change in Mean Number of Healthy Sites from Baseline
Interproximal Change in Mean Number of Healthy Sites from Baseline
Day 15 Day 30 Day 15 Day 30 MB 16.89 17.57 9.04 9.83 SB 23.89 24.42 13.33 13.42
Sonic Power Toothbrush Improvements Compared to Manual Brush 41% 39% 47% 37%
Statistical Comparison of MB vs. SB p<0.001 p<0.001 p<0.001 p<0.001
Whole Mouth, Interproximal: Results are percent improvement from Baseline Whole Mouth, Interproximal Change to Healthy Sites: Change in number of bleeding sites (BI=1,2) from Baseline to “0” bleeding sites Improvement: Percent is sonic power toothbrush improvement divided by manual toothbrush improvement MB: ADA standard manual toothbrush plus fluoride toothpaste SB: Sonic toothbrush plus fluoride toothpaste
Changes to healthy whole mouth bleeding scores were superior for the sonic toothbrush
both at Day 15 and Day 30 (p<0.001). At Day 15 and Day 30 the sonic toothbrush
outperformed the manual toothbrush by an average of 7 sites in the change in the number
of whole mouth bleeding sites to healthy sites (BI=0).
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 142 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 144 of 177

Plaque Index Summary
Summary results for Baseline plaque pre- to post-brushing endpoints are given in
Executive Summary Table 3 below. The sonic powered toothbrush provided statistically
significant reductions in plaque for Baseline Pre-brushing to Post-brushing (p<0.001).
See Appendix Table 10.
The sonic toothbrush plaque improvements for whole mouth and gumline were
statistically significantly (p=0.035, or less) better than the manual brush at Baseline pre -
post-brushing. The Baseline Pre-Brushing to Post-Brushing plaque reductions for the
sonic toothbrush ranged from 37.5% for gumline sites to 14.0% for interproximal sites.
The reductions for the sonic toothbrush were greater than the reductions seen with the
manual toothbrush; for whole mouth the sonic toothbrush plaque reductions exceeded the
manual toothbrush reductions by 33%.
The sonic toothbrush provided statistically significant reductions from Baseline to Day
15 (p<0.001) and Day 30 (p<0.001) for all endpoints (Appendix Tables 12, 14). Table 3
below provides summary results.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 143 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 145 of 177
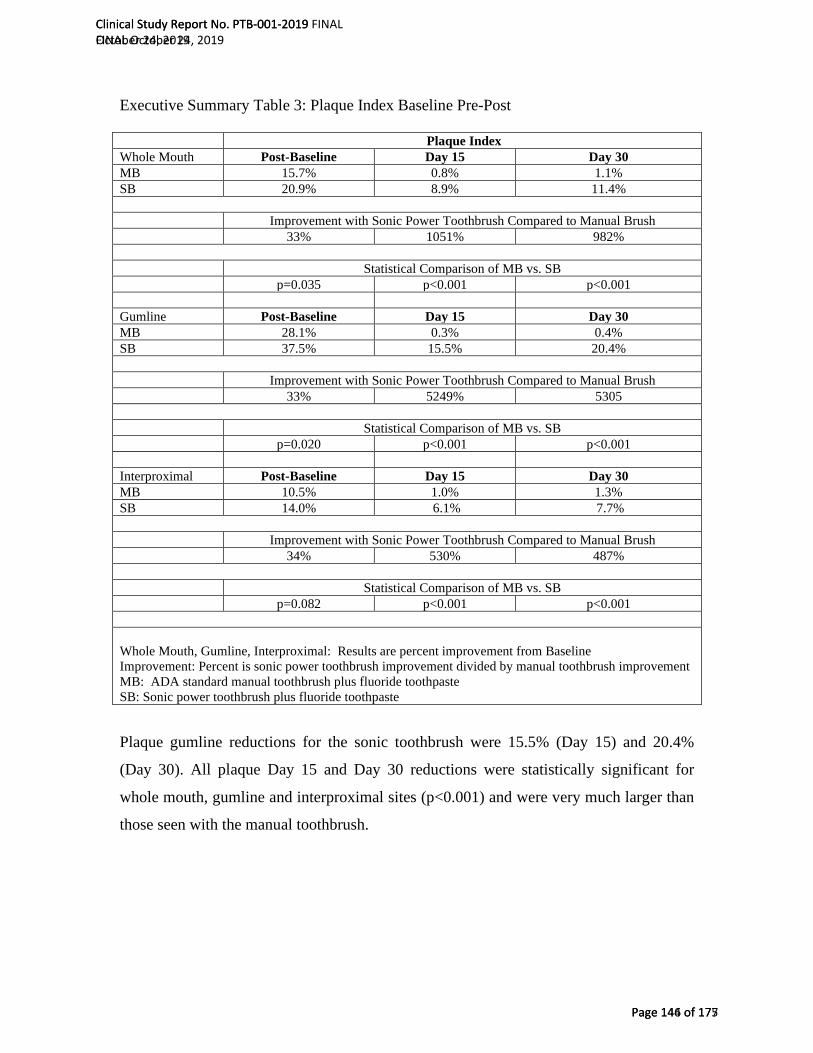
Executive Summary Table 3: Plaque Index Baseline Pre-Post
Plaque Index Whole Mouth Post-Baseline Day 15 Day 30 MB 15.7% 0.8% 1.1% SB 20.9% 8.9% 11.4%
Improvement with Sonic Power Toothbrush Compared to Manual Brush 33% 1051% 982%
Statistical Comparison of MB vs. SB p=0.035 p<0.001 p<0.001
Gumline Post-Baseline Day 15 Day 30 MB 28.1% 0.3% 0.4% SB 37.5% 15.5% 20.4%
Improvement with Sonic Power Toothbrush Compared to Manual Brush 33% 5249% 5305
Statistical Comparison of MB vs. SB p=0.020 p<0.001 p<0.001
Interproximal Post-Baseline Day 15 Day 30 MB 10.5% 1.0% 1.3% SB 14.0% 6.1% 7.7%
Improvement with Sonic Power Toothbrush Compared to Manual Brush 34% 530% 487%
Statistical Comparison of MB vs. SB p=0.082 p<0.001 p<0.001
Whole Mouth, Gumline, Interproximal: Results are percent improvement from Baseline Improvement: Percent is sonic power toothbrush improvement divided by manual toothbrush improvement MB: ADA standard manual toothbrush plus fluoride toothpaste SB: Sonic power toothbrush plus fluoride toothpaste
Plaque gumline reductions for the sonic toothbrush were 15.5% (Day 15) and 20.4%
(Day 30). All plaque Day 15 and Day 30 reductions were statistically significant for
whole mouth, gumline and interproximal sites (p<0.001) and were very much larger than
those seen with the manual toothbrush.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 144 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 146 of 177

Overall Summary
The BURST sonic toothbrush achieved clinical improvements in oral health, in particular
reductions in plaque and gingivitis. The improvements were statistically significantly
better than those of a manual toothbrush.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 147 of 177
Introduction
Study Synopsis and Objectives
This single-center, randomized, controlled, examiner-blind, 30-day, parallel study is
designed to evaluate the safety and efficacy of a sonic power toothbrush with charcoal
infused toothbrush bristles compared to an ADA reference manual soft toothbrush on
plaque and gingivitis.
Inclusion and Exclusion Criteria
See the protocol.
Analysis Endpoints
Post treatment efficacy endpoints are:
• Mean change in MGI scores at Day 15 and Day 30 for
o Whole mouth
o Interproximal (mesial & distal)
• Change in mean number of healthy sites (MGI=0,1) at Days 15 and 30
• Mean change in BI scores at Day 15 and Day 30 for
o Whole mouth
o Interproximal (mesial & distal)
• Mean change in number of bleeding sites (BI=1,2) from Baseline to “0” bleeding
sites at Day 15 and 30 for
o Whole mouth
o Interproximal (mesial & distal)
Mean change in plaque index score at Baseline Pre - Post-brushing, Day 15 and 30 for
o Whole mouth
o Gumline (marginal)
o Interproximal (mesial & distal)
Analyses were performed for Day 15 and Day 30 for each efficacy variable and Baseline
for pre - post-brushing plaque. Analyses used the ANCOVA model with treatment as a
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 146 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 148 of 177

factor and the corresponding baseline value as a covariate. For change in mean number of
healthy MGI sites the ANOVA model was used since the baseline value was typically
zero. The comparisons were made at the 0.05 level, 2-sided. Differences between the
means, 95% confidence intervals and test results will be presented.
For each efficacy variable summary statistics using appropriate descriptive statistics
(mean, median, minimum, maximum) by treatment group and overall will be provided at
each visit.
Sample Size and Statistical Analysis
In addition to what is stated in the protocol no statistical adjusts were made for multiple testing.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 147 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 149 of 177

Results
Demographic and Baseline
Full results are given in Appendix Table 1.
Age, gender, race, ethnicity, and smoking status were comparable among the treatments
at Baseline (see Appendix Table 1). Appendix Table 1 contains summary data for all
randomized subjects. For all randomized subjects the mean age was 45.8 years with a
standard deviation of 12.5. The gender breakdown was 68 females and 26 males. Overall,
92 subjects did not use tobacco or smokeless tobacco and 2 subjects were smokers.
Baseline comparability was conducted for all endpoints. The two (2) toothbrushes were
comparable at Baseline for gingival indices (BI: whole mouth, interproximal, p>0.448;
MGI: whole mouth, interproximal p>0.391; see Appendix Table 1). All plaque endpoints
were similar at Baseline (whole mouth, gumline, interproximal, p>0.678; see Appendix
Table 1). Also, the number of scorable sites was comparable between the two
toothbrushes (gingival sites, plaque sites, p>0.100; see Appendix Table 1).
Modified Gingival Index
Appendix Table 2 and Appendix Table 3 provide more summary data for Day 15, and
Appendix Table 4 and Appendix Table 5 provide Day 30 results. The sonic toothbrush
provided positive change from Baseline to Day 15 (p<0.001, see Appendix Tables 2) and
Day 30 (p<0.001; see Appendix Tables 4).
At Day 30, the use of the sonic toothbrush resulted in about 33 more whole mouth
healthy sites than at Baseline. The sonic toothbrush also reduced whole mouth MGI by an
average of 34.6% at both Day 15 and Day 30.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 148 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 150 of 177

Table 1 below provides summary data for the MGI results.
Table 1: Summary Data for Modified Gingival Index (MGI)
Modified Gingival Index Whole Mouth Reductions from Baseline Interproximal Reductions from Baseline
Day 15 Day 30 Day 15 Day 30 MB 10.3% -3.7% 3.9% -9.5%SB 35.7% 33.4% 24.5% 22.1%
Sonic Power Toothbrush Improvement Compared to Manual Brush 245% 1003% 519% 333%
Statistical Comparison of MB vs. SB p<0.001 p<0.001 p<0.001 p<0.001
Whole Mouth Change in Mean Number of Healthy Sites from Baseline
Interproximal Change in Mean Number of Healthy Sites from Baseline
Day 15 Day 30 Day 15 Day 30 MB 11.62 3.15 1.28 0.40 SB 35.71 32.91 13.22 13.09
Sonic Power Toothbrush Improvements Compared to Manual Brush 207% 908% 936% 3137%
Statistical Comparison of MB vs. SB p<0.001 p<0.001 p<0.001 p<0.001
Whole Mouth, Interproximal: Results are percent improvement from Baseline Whole Mouth, Interproximal Healthy Sites: Change in number of healthy sites (MGI=0,1) Improvement: Percent is sonic power toothbrush improvement divided by manual toothbrush improvement MB: ADA standard manual toothbrush plus fluoride toothpaste SB: Sonic toothbrush plus fluoride toothpaste
The sonic toothbrush provided statistically significantly superior gains compared to the
manual toothbrush for all MGI endpoints evaluated at Day 15, and Day 30 (p<0.001).
Table 2 below provides results for comparisons between toothbrushes.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 149 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 151 of 177
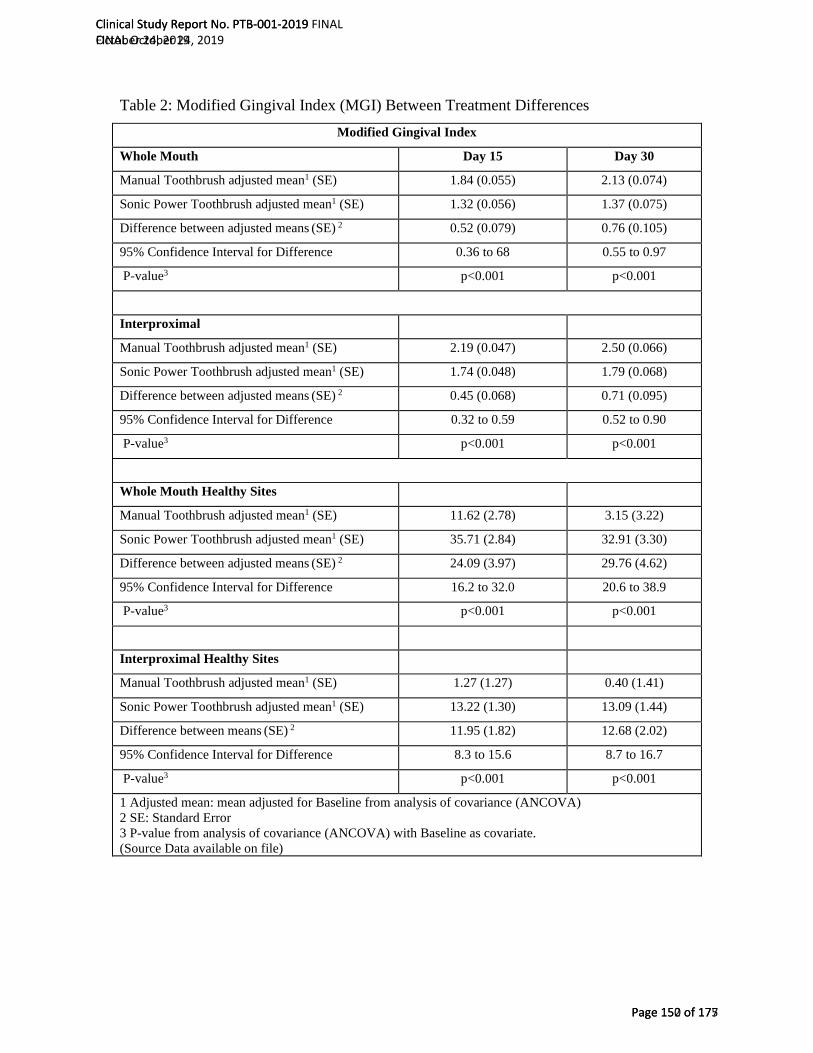
Table 2: Modified Gingival Index (MGI) Between Treatment Differences Modified Gingival Index
Whole Mouth Day 15 Day 30
Manual Toothbrush adjusted mean1 (SE) 1.84 (0.055) 2.13 (0.074)
Sonic Power Toothbrush adjusted mean1 (SE) 1.32 (0.056) 1.37 (0.075)
Difference between adjusted means (SE) 2 0.52 (0.079) 0.76 (0.105)
95% Confidence Interval for Difference 0.36 to 68 0.55 to 0.97
P-value3 p<0.001 p<0.001
Interproximal
Manual Toothbrush adjusted mean1 (SE) 2.19 (0.047) 2.50 (0.066)
Sonic Power Toothbrush adjusted mean1 (SE) 1.74 (0.048) 1.79 (0.068)
Difference between adjusted means (SE) 2 0.45 (0.068) 0.71 (0.095)
95% Confidence Interval for Difference 0.32 to 0.59 0.52 to 0.90
P-value3 p<0.001 p<0.001
Whole Mouth Healthy Sites
Manual Toothbrush adjusted mean1 (SE) 11.62 (2.78) 3.15 (3.22)
Sonic Power Toothbrush adjusted mean1 (SE) 35.71 (2.84) 32.91 (3.30)
Difference between adjusted means (SE) 2 24.09 (3.97) 29.76 (4.62)
95% Confidence Interval for Difference 16.2 to 32.0 20.6 to 38.9
P-value3 p<0.001 p<0.001
Interproximal Healthy Sites
Manual Toothbrush adjusted mean1 (SE) 1.27 (1.27) 0.40 (1.41)
Sonic Power Toothbrush adjusted mean1 (SE) 13.22 (1.30) 13.09 (1.44)
Difference between means (SE) 2 11.95 (1.82) 12.68 (2.02)
95% Confidence Interval for Difference 8.3 to 15.6 8.7 to 16.7
P-value3 p<0.001 p<0.001
1 Adjusted mean: mean adjusted for Baseline from analysis of covariance (ANCOVA) 2 SE: Standard Error 3 P-value from analysis of covariance (ANCOVA) with Baseline as covariate. (Source Data available on file)
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 150 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 152 of 177

Bleeding Index
Appendix Table 6 and Appendix Table 7 provide more summary data for Day 15, and
Appendix Table 8 and Appendix Table 9 provide Day 30 results. Both toothbrushes
provided positive change from Baseline to Day 15 (p<0.001, except manual brush
interproximal p=0.005; see Appendix Tables 6, 7) and Day 30 (p<0.001; see Appendix
Tables 8, 9).
Summaries for the bleeding index results are given in Table 3 below.
Table 3: Summary Data for l Bleeding Index (BI)
Bleeding Index Whole Mouth Reductions from Baseline Interproximal Reductions from Baseline
Day 15 Day 30 Day 15 Day 30 MB 16.2% 20.3% 14.0% 24.3% SB 64.8% 66.3% 66.7% 67.6%
Sonic Power Toothbrush Improvement Compared to Manual Brush 301% 227% 376% 179%
Statistical Comparison of MB vs. SB p<0.001 p<0.001 p<0.001 p<0.001
Whole Mouth Change in Mean Number of Healthy Sites from Baseline
Interproximal Change in Mean Number of Healthy Sites from Baseline
Day 15 Day 30 Day 15 Day 30 MB 16.89 17.57 9.04 9.83 SB 23.89 24.42 13.33 13.42
Sonic Power Toothbrush Improvements Compared to Manual Brush 41% 39% 47% 37%
Statistical Comparison of MB vs. SB p<0.001 p<0.001 p<0.001 p<0.001
Whole Mouth, Interproximal: Results are percent improvement from Baseline Whole Mouth, Interproximal Change to Healthy: Change in number of bleeding sites (BI=1,2) from Baseline to “0” bleeding sites Improvement: Percent is sonic power toothbrush improvement divided by manual toothbrush improvement MB: ADA standard manual toothbrush plus fluoride toothpaste SB: Sonic toothbrush plus fluoride toothpaste
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 151 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 153 of 177

The sonic toothbrush achieved improvements in BI for whole mouth of 64.8% (Day 15)
and 66.3% (Day 30). Changes in gingival bleeding for both Day 15 and Day 30 averaged
about a 65% improvement for both whole mouth and interproximal sites. Change in the
number of bleeding sites to healthy sites for the sonic toothbrush averaged about 40%
more healthier sites at both Day 15 and Day 30.
Tables 4 below provides results from the between treatment analyses. The sonic
toothbrush provided superior gains compared to the manual toothbrush for all BI
endpoints evaluated at Day 15 (p<0.001) and Day 30 (p<0.001).
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 152 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 154 of 177
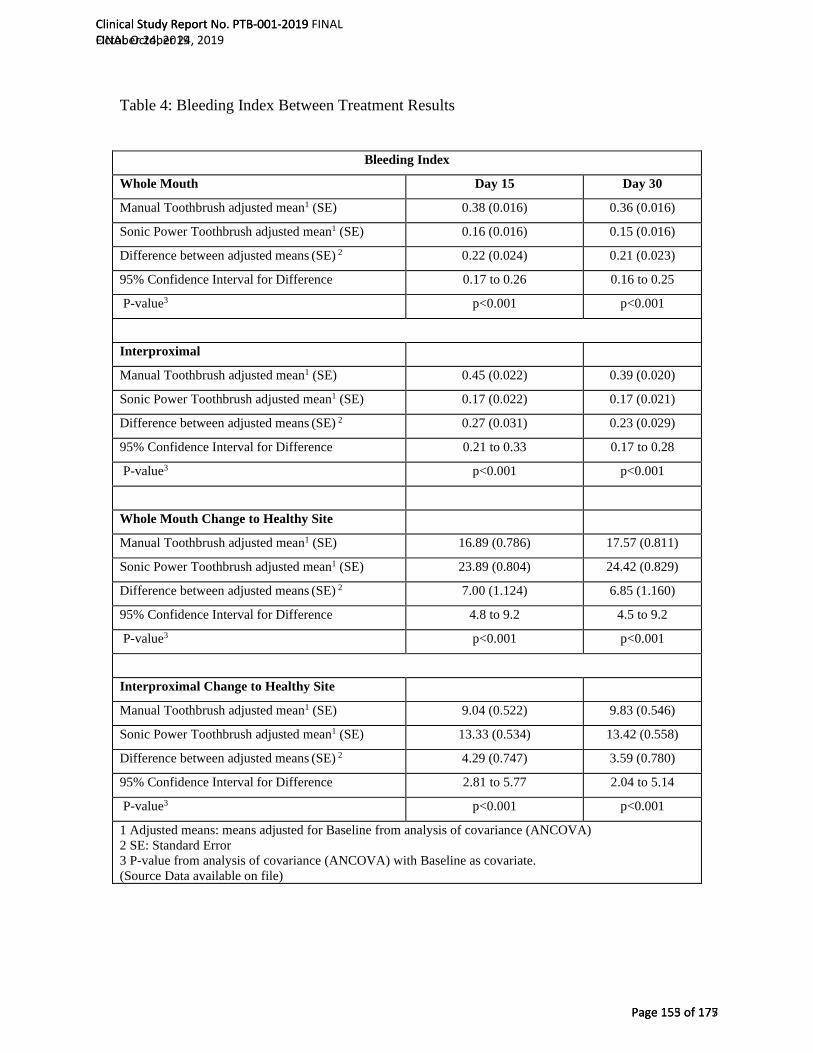
Table 4: Bleeding Index Between Treatment Results
Bleeding Index
Whole Mouth Day 15 Day 30
Manual Toothbrush adjusted mean1 (SE) 0.38 (0.016) 0.36 (0.016)
Sonic Power Toothbrush adjusted mean1 (SE) 0.16 (0.016) 0.15 (0.016)
Difference between adjusted means (SE) 2 0.22 (0.024) 0.21 (0.023)
95% Confidence Interval for Difference 0.17 to 0.26 0.16 to 0.25
P-value3 p<0.001 p<0.001
Interproximal
Manual Toothbrush adjusted mean1 (SE) 0.45 (0.022) 0.39 (0.020)
Sonic Power Toothbrush adjusted mean1 (SE) 0.17 (0.022) 0.17 (0.021)
Difference between adjusted means (SE) 2 0.27 (0.031) 0.23 (0.029)
95% Confidence Interval for Difference 0.21 to 0.33 0.17 to 0.28
P-value3 p<0.001 p<0.001
Whole Mouth Change to Healthy Site
Manual Toothbrush adjusted mean1 (SE) 16.89 (0.786) 17.57 (0.811)
Sonic Power Toothbrush adjusted mean1 (SE) 23.89 (0.804) 24.42 (0.829)
Difference between adjusted means (SE) 2 7.00 (1.124) 6.85 (1.160)
95% Confidence Interval for Difference 4.8 to 9.2 4.5 to 9.2
P-value3 p<0.001 p<0.001
Interproximal Change to Healthy Site
Manual Toothbrush adjusted mean1 (SE) 9.04 (0.522) 9.83 (0.546)
Sonic Power Toothbrush adjusted mean1 (SE) 13.33 (0.534) 13.42 (0.558)
Difference between adjusted means (SE) 2 4.29 (0.747) 3.59 (0.780)
95% Confidence Interval for Difference 2.81 to 5.77 2.04 to 5.14
P-value3 p<0.001 p<0.001
1 Adjusted means: means adjusted for Baseline from analysis of covariance (ANCOVA) 2 SE: Standard Error 3 P-value from analysis of covariance (ANCOVA) with Baseline as covariate. (Source Data available on file)
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 153 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 155 of 177

Plaque Index
The sonic toothbrush provided positive changes at Baseline post-brushing (p<0.001),
from Baseline to Day 15 (p<0.001) and Day 30 (p<0.001) for all plaque endpoints
(Appendix Tables 10, 12, 14). Table 5 below gives plaque summary results.
Table 5: Plaque Index Results Plaque Index
Whole Mouth Post-Baseline Day 15 Day 30 MB 15.7% 0.8% 1.1% SB 20.9% 8.9% 11.4%
Improvement with Sonic Power Toothbrush Compared to Manual Brush 33% 1051% 982%
Statistical Comparison of MB vs. SB p=0.035 p<0.001 p<0.001
Gumline Post-Baseline Day 15 Day 30 MB 28.1% 0.3% 0.4% SB 37.5% 15.5% 20.4%
Improvement with Sonic Power Toothbrush Compared to Manual Brush 33% 5249% 5305%
Statistical Comparison of MB vs. SB p=0.020 p<0.001 p<0.001
Interproximal Post-Baseline Day 15 Day 30 MB 10.5% 1.0% 1.3% SB 14.0% 6.1% 7.7%
Improvement with Sonic Power Toothbrush Compared to Manual Brush 34% 530% 487%
Statistical Comparison of MB vs. SB p=0.082 p<0.001 p<0.001
Whole Mouth, Gumline, Interproximal: Results are percent improvement from Baseline Improvement: Percent is sonic power toothbrush improvement divided by manual toothbrush improvement MB: ADA standard manual toothbrush plus fluoride toothpaste SB: Sonic power toothbrush plus fluoride toothpaste
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 154 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 156 of 177
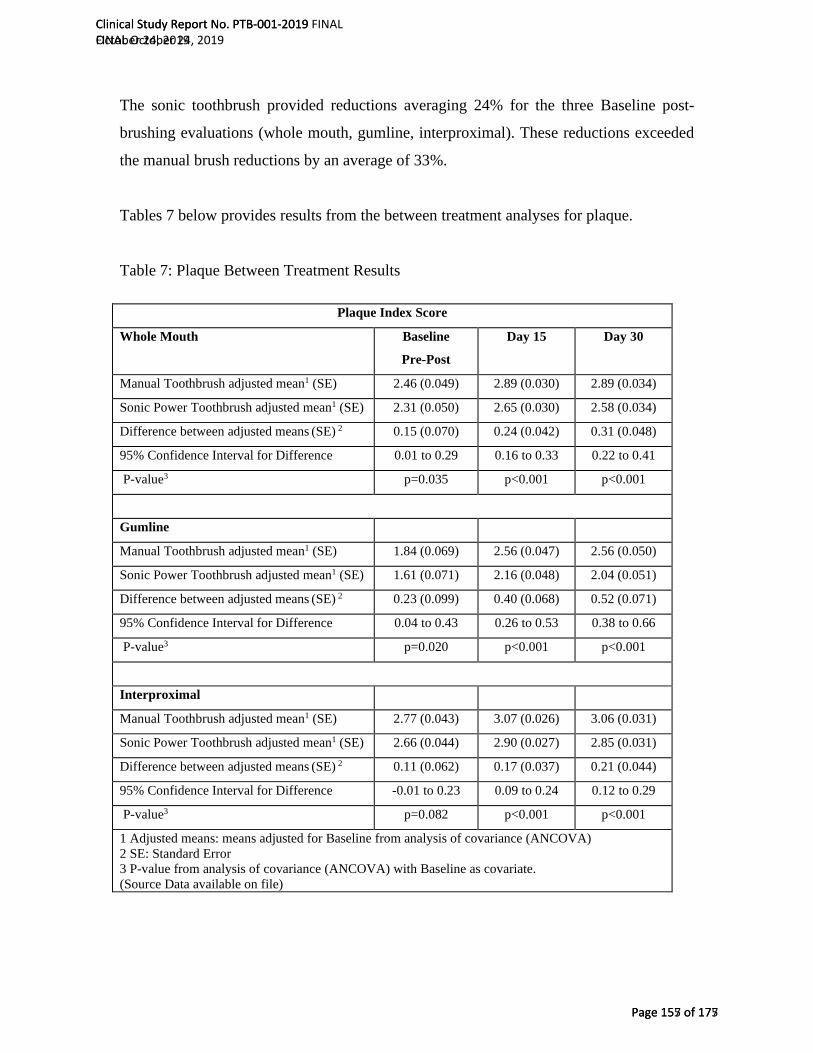
The sonic toothbrush provided reductions averaging 24% for the three Baseline post-
brushing evaluations (whole mouth, gumline, interproximal). These reductions exceeded
the manual brush reductions by an average of 33%.
Tables 7 below provides results from the between treatment analyses for plaque.
Table 7: Plaque Between Treatment Results
Plaque Index Score
Whole Mouth Baseline
Pre-Post
Day 15 Day 30
Manual Toothbrush adjusted mean1 (SE) 2.46 (0.049) 2.89 (0.030) 2.89 (0.034)
Sonic Power Toothbrush adjusted mean1 (SE) 2.31 (0.050) 2.65 (0.030) 2.58 (0.034)
Difference between adjusted means (SE) 2 0.15 (0.070) 0.24 (0.042) 0.31 (0.048)
95% Confidence Interval for Difference 0.01 to 0.29 0.16 to 0.33 0.22 to 0.41
P-value3 p=0.035 p<0.001 p<0.001
Gumline
Manual Toothbrush adjusted mean1 (SE) 1.84 (0.069) 2.56 (0.047) 2.56 (0.050)
Sonic Power Toothbrush adjusted mean1 (SE) 1.61 (0.071) 2.16 (0.048) 2.04 (0.051)
Difference between adjusted means (SE) 2 0.23 (0.099) 0.40 (0.068) 0.52 (0.071)
95% Confidence Interval for Difference 0.04 to 0.43 0.26 to 0.53 0.38 to 0.66
P-value3 p=0.020 p<0.001 p<0.001
Interproximal
Manual Toothbrush adjusted mean1 (SE) 2.77 (0.043) 3.07 (0.026) 3.06 (0.031)
Sonic Power Toothbrush adjusted mean1 (SE) 2.66 (0.044) 2.90 (0.027) 2.85 (0.031)
Difference between adjusted means (SE) 2 0.11 (0.062) 0.17 (0.037) 0.21 (0.044)
95% Confidence Interval for Difference -0.01 to 0.23 0.09 to 0.24 0.12 to 0.29
P-value3 p=0.082 p<0.001 p<0.001
1 Adjusted means: means adjusted for Baseline from analysis of covariance (ANCOVA) 2 SE: Standard Error 3 P-value from analysis of covariance (ANCOVA) with Baseline as covariate. (Source Data available on file)
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 155 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 157 of 177

The sonic brush whole mouth and gumline plaque improvements at Baseline post-
brushing were better than the manual brush for whole mouth and gumline (p=0.035, or
less). The change in interproximal sites at Baseline post-brushing did not differ for the
two treatments (p=0.082).
Day 15 and Day 30 plaque improvements were statistically significantly better for the
sonic brush than the manual brush for all endpoints evaluated (p<0.001).
Conclusion
The BURST sonic toothbrush achieved clinical improvements in oral health, in particular
reductions in plaque and gingivitis. The improvements were statistically significantly
better than those of a standard ADA manual toothbrush.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 156 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 158 of 177
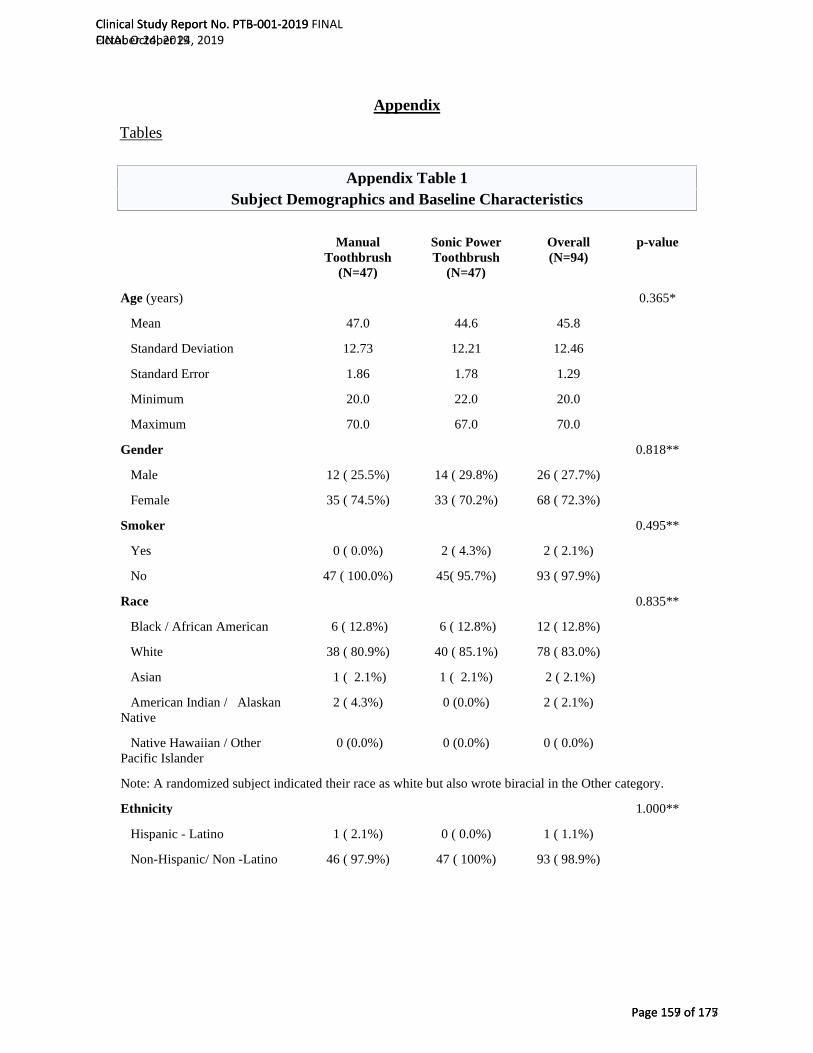
Appendix
Tables
Appendix Table 1 Subject Demographics and Baseline Characteristics
Manual Toothbrush
(N=47)
Sonic Power Toothbrush
(N=47)
Overall (N=94)
p-value
Age (years) 0.365*
Mean 47.0 44.6 45.8
Standard Deviation 12.73 12.21 12.46
Standard Error 1.86 1.78 1.29
Minimum 20.0 22.0 20.0
Maximum 70.0 67.0 70.0
Gender 0.818**
Male 12 ( 25.5%) 14 ( 29.8%) 26 ( 27.7%)
Female 35 ( 74.5%) 33 ( 70.2%) 68 ( 72.3%)
Smoker 0.495**
Yes 0 ( 0.0%) 2 ( 4.3%) 2 ( 2.1%)
No 47 ( 100.0%) 45( 95.7%) 93 ( 97.9%)
Race 0.835**
Black / African American 6 ( 12.8%) 6 ( 12.8%) 12 ( 12.8%)
White 38 ( 80.9%) 40 ( 85.1%) 78 ( 83.0%)
Asian 1 ( 2.1%) 1 ( 2.1%) 2 ( 2.1%)
American Indian / Alaskan Native
2 ( 4.3%) 0 (0.0%) 2 ( 2.1%)
Native Hawaiian / Other Pacific Islander
0 (0.0%) 0 (0.0%) 0 ( 0.0%)
Note: A randomized subject indicated their race as white but also wrote biracial in the Other category.
Ethnicity 1.000**
Hispanic - Latino 1 ( 2.1%) 0 ( 0.0%) 1 ( 1.1%)
Non-Hispanic/ Non -Latino 46 ( 97.9%) 47 ( 100%) 93 ( 98.9%)
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 157 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 159 of 177

Manual Toothbrush
(N=47)
Sonic Power Toothbrush
(N=47)
Overall (N=94)
p-value
Whole Mouth Baseline MGI 0.924*
Mean 2.06 2.06
Standard Deviation 0.19 0.20
Interproximal Baseline MGI 0.391*
Mean 2.27 2.32
Standard Deviation 0.23 0.23
Whole Mouth Baseline BI 0.469*
Mean 0.46 0.43
Standard Deviation 0.20 0.14
Interproximal Baseline BI 0.448*
Mean 0.53 0.50
Standard Deviation 0.22 0.16
Whole Mouth Baseline PI 0.680*
Mean 2.93 2.90
Standard Deviation 0.28 0.35
Gumline Baseline PI 0.714*
Mean 2.58 2.55
Standard Deviation 0.36 0.46
Interproximal Baseline PI 0.678*
Mean 3.11 3.08
Standard Deviation 0.26 0.31
Scorable (MGI, BI) Sites 0.100*
Mean 97.91 101.20
Standard Deviation 10.54 8.17
Scorable (Plaque) Sites
Mean 156.00 159.73 0.125*
Standard Deviation 13.12 9.68
* p value from ANOVA
** p value from Fisher’s Exact test
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 158 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 160 of 177
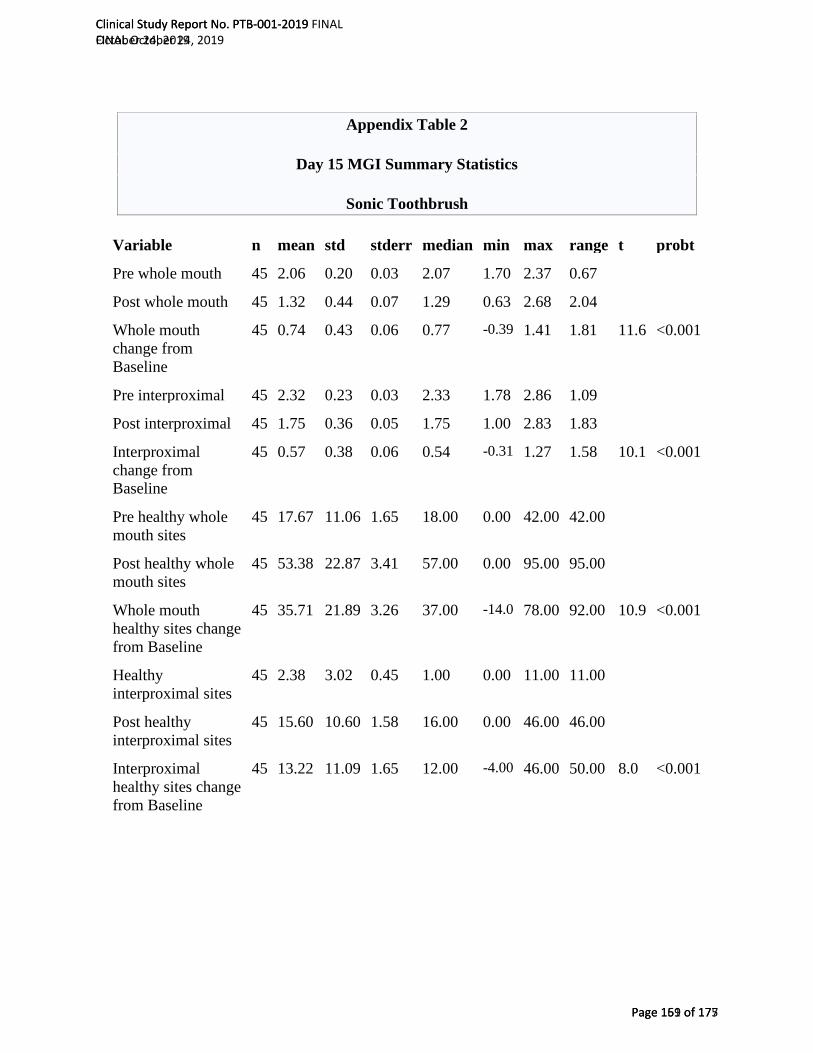
Appendix Table 2
Day 15 MGI Summary Statistics
Sonic Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 45 2.06 0.20 0.03 2.07 1.70 2.37 0.67
Post whole mouth 45 1.32 0.44 0.07 1.29 0.63 2.68 2.04
Whole mouth change from Baseline
45 0.74 0.43 0.06 0.77 -0.39 1.41 1.81 11.6 <0.001
Pre interproximal 45 2.32 0.23 0.03 2.33 1.78 2.86 1.09
Post interproximal 45 1.75 0.36 0.05 1.75 1.00 2.83 1.83
Interproximal change from Baseline
45 0.57 0.38 0.06 0.54 -0.31 1.27 1.58 10.1 <0.001
Pre healthy whole mouth sites
45 17.67 11.06 1.65 18.00 0.00 42.00 42.00
Post healthy whole mouth sites
45 53.38 22.87 3.41 57.00 0.00 95.00 95.00
Whole mouth healthy sites change from Baseline
45 35.71 21.89 3.26 37.00 -14.0 78.00 92.00 10.9 <0.001
Healthy interproximal sites
45 2.38 3.02 0.45 1.00 0.00 11.00 11.00
Post healthy interproximal sites
45 15.60 10.60 1.58 16.00 0.00 46.00 46.00
Interproximal healthy sites change from Baseline
45 13.22 11.09 1.65 12.00 -4.00 46.00 50.00 8.0 <0.001
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 159 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 161 of 177

Appendix Table 3 Day 15 MGI Summary Statistics
Manual Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 47 2.06 0.19 0.03 2.07 1.74 2.33 0.60
Post whole mouth 47 1.84 0.36 0.05 1.83 0.91 2.65 1.73
Whole mouth change from Baseline
47 0.21 0.33 0.05 0.25 -0.42 1.13 1.55 4.4 <0.001
Pre interproximal 47 2.27 0.23 0.03 2.25 1.94 2.88 0.93
Post interproximal 47 2.18 0.32 0.05 2.16 1.58 2.96 1.38
Interproximal change from Baseline
47 0.09 0.31 0.05 0.09 -0.52 0.86 1.38 2.0 0.054
Pre healthy whole mouth sites
47 16.45 9.65 1.41 17.00 0.00 37.00 37.00
Post healthy whole mouth sites
47 28.06 17.12 2.50 27.00 0.00 69.00 69.00
Whole mouth healthy sites change from Baseline
47 11.62 15.82 2.31 14.00 -25.0 50.00 75.00 5.0 <0.001
Healthy interproximal sites
47 2.45 2.42 0.35 2.00 0.00 10.00 10.00
Post healthy interproximal sites
47 3.72 5.46 0.80 1.00 0.00 22.00 22.00
Interproximal healthy sites change from Baseline
47 1.28 5.64 0.82 0.00 -6.00 20.00 26.00 1.6 0.127
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 160 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 162 of 177
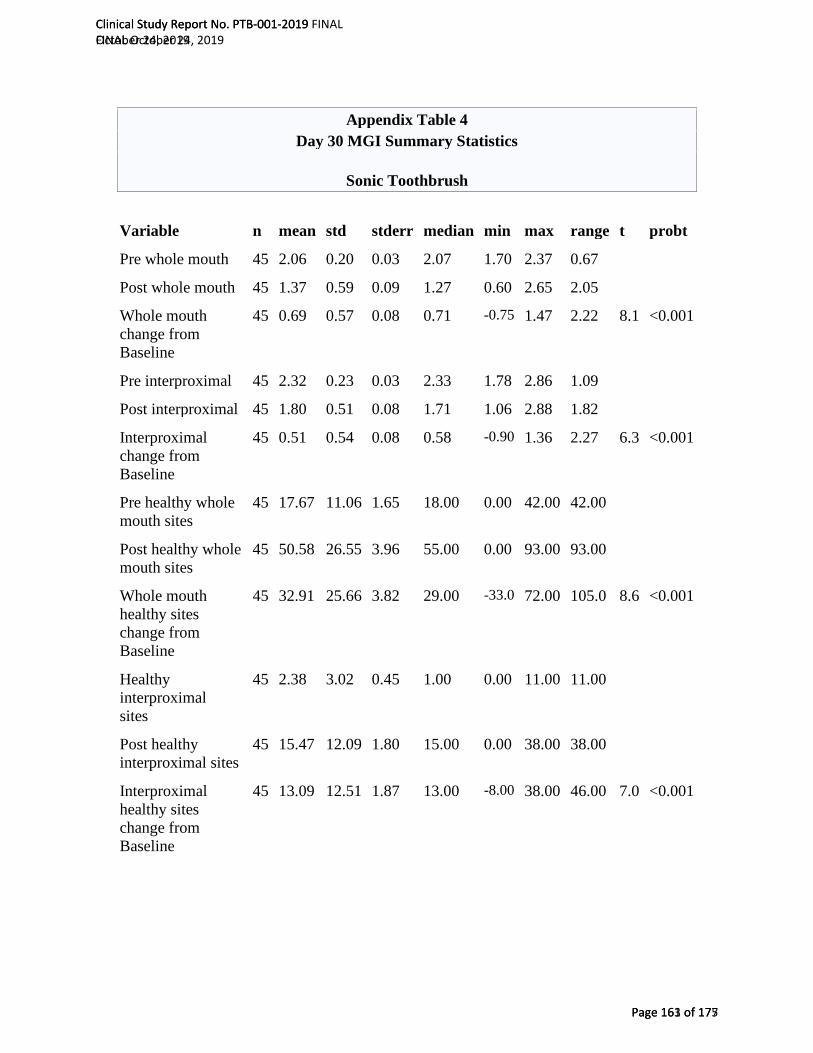
Appendix Table 4 Day 30 MGI Summary Statistics
Sonic Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 45 2.06 0.20 0.03 2.07 1.70 2.37 0.67
Post whole mouth 45 1.37 0.59 0.09 1.27 0.60 2.65 2.05
Whole mouth change from Baseline
45 0.69 0.57 0.08 0.71 -0.75 1.47 2.22 8.1 <0.001
Pre interproximal 45 2.32 0.23 0.03 2.33 1.78 2.86 1.09
Post interproximal 45 1.80 0.51 0.08 1.71 1.06 2.88 1.82
Interproximal change from Baseline
45 0.51 0.54 0.08 0.58 -0.90 1.36 2.27 6.3 <0.001
Pre healthy whole mouth sites
45 17.67 11.06 1.65 18.00 0.00 42.00 42.00
Post healthy whole mouth sites
45 50.58 26.55 3.96 55.00 0.00 93.00 93.00
Whole mouth healthy sites change from Baseline
45 32.91 25.66 3.82 29.00 -33.0 72.00 105.0 8.6 <0.001
Healthy interproximal sites
45 2.38 3.02 0.45 1.00 0.00 11.00 11.00
Post healthy interproximal sites
45 15.47 12.09 1.80 15.00 0.00 38.00 38.00
Interproximal healthy sites change from Baseline
45 13.09 12.51 1.87 13.00 -8.00 38.00 46.00 7.0 <0.001
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 161 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 163 of 177

Appendix Table 5 Day 30 MGI Summary Statistics
Manual Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 47 2.06 0.19 0.03 2.07 1.74 2.33 0.60
Post whole mouth 47 2.13 0.50 0.07 2.22 1.11 2.94 1.84
Whole mouth change from Baseline
47 -0.08 0.43 0.06 -0.19 -0.66 0.96 1.62 1.2 0.232
Pre interproximal 47 2.27 0.23 0.03 2.25 1.94 2.88 0.93
Post interproximal 47 2.49 0.42 0.06 2.60 1.65 3.00 1.35
Interproximal change from Baseline
47 -0.22 0.38 0.06 -0.26 -0.80 0.67 1.46 3.9 <0.001
Pre healthy whole mouth sites
47 16.45 9.65 1.41 17.00 0.00 37.00 37.00
Post healthy whole mouth sites
47 19.60 19.88 2.90 14.00 0.00 66.00 66.00
Whole mouth healthy sites change from Baseline
47 3.15 18.15 2.65 0.00 -25.0 51.00 76.00 1.2 0.240
Healthy interproximal sites
47 2.45 2.42 0.35 2.00 0.00 10.00 10.00
Post healthy interproximal sites
47 2.85 5.14 0.75 0.00 0.00 22.00 22.00
Interproximal healthy sites change from Baseline
47 0.40 5.76 0.84 -1.00 -10.0 21.00 31.00 0.5 0.633
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 162 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 164 of 177
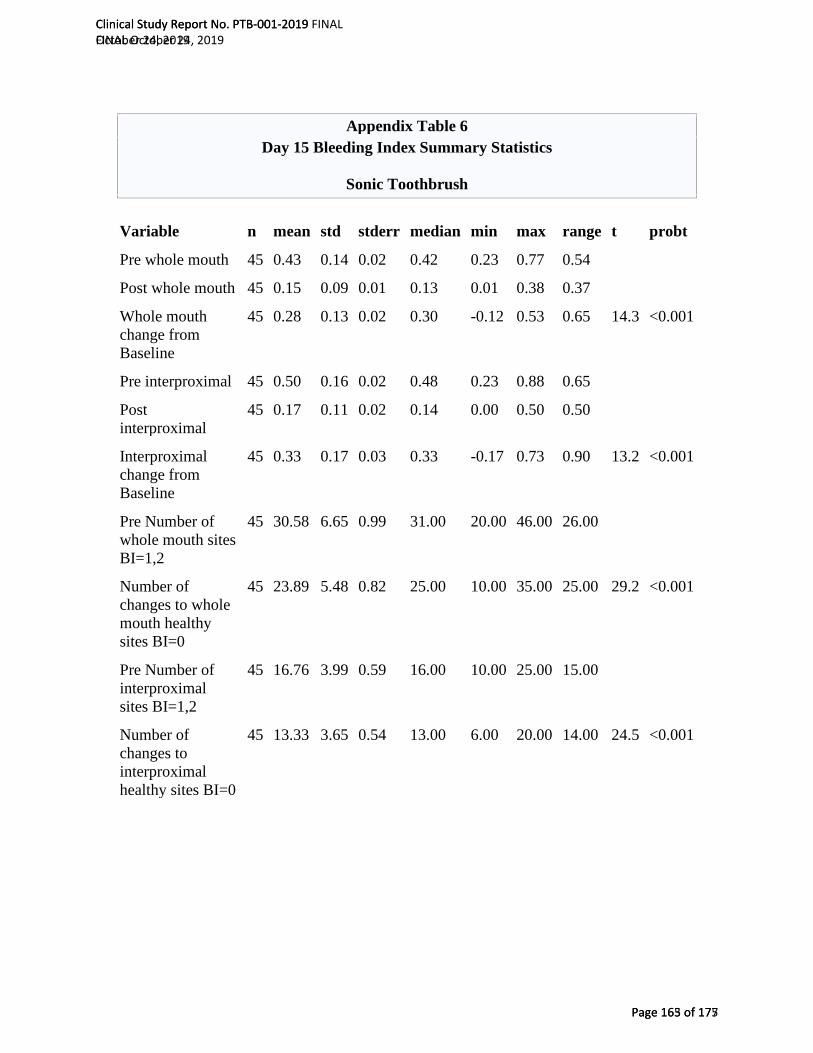
Appendix Table 6 Day 15 Bleeding Index Summary Statistics
Sonic Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 45 0.43 0.14 0.02 0.42 0.23 0.77 0.54
Post whole mouth 45 0.15 0.09 0.01 0.13 0.01 0.38 0.37
Whole mouth change from Baseline
45 0.28 0.13 0.02 0.30 -0.12 0.53 0.65 14.3 <0.001
Pre interproximal 45 0.50 0.16 0.02 0.48 0.23 0.88 0.65
Post interproximal
45 0.17 0.11 0.02 0.14 0.00 0.50 0.50
Interproximal change from Baseline
45 0.33 0.17 0.03 0.33 -0.17 0.73 0.90 13.2 <0.001
Pre Number of whole mouth sites BI=1,2
45 30.58 6.65 0.99 31.00 20.00 46.00 26.00
Number of changes to whole mouth healthy sites BI=0
45 23.89 5.48 0.82 25.00 10.00 35.00 25.00 29.2 <0.001
Pre Number of interproximal sites BI=1,2
45 16.76 3.99 0.59 16.00 10.00 25.00 15.00
Number of changes to interproximal healthy sites BI=0
45 13.33 3.65 0.54 13.00 6.00 20.00 14.00 24.5 <0.001
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 163 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 165 of 177
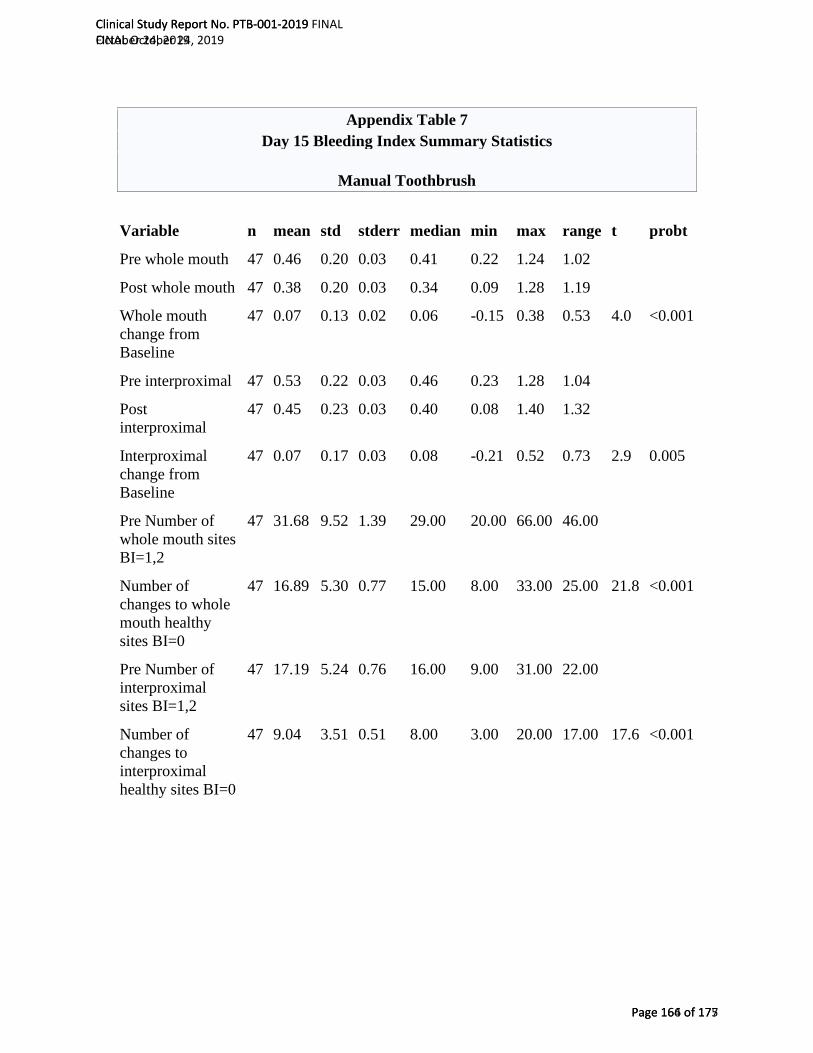
Appendix Table 7 Day 15 Bleeding Index Summary Statistics
Manual Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 47 0.46 0.20 0.03 0.41 0.22 1.24 1.02
Post whole mouth 47 0.38 0.20 0.03 0.34 0.09 1.28 1.19
Whole mouth change from Baseline
47 0.07 0.13 0.02 0.06 -0.15 0.38 0.53 4.0 <0.001
Pre interproximal 47 0.53 0.22 0.03 0.46 0.23 1.28 1.04
Post interproximal
47 0.45 0.23 0.03 0.40 0.08 1.40 1.32
Interproximal change from Baseline
47 0.07 0.17 0.03 0.08 -0.21 0.52 0.73 2.9 0.005
Pre Number of whole mouth sites BI=1,2
47 31.68 9.52 1.39 29.00 20.00 66.00 46.00
Number of changes to whole mouth healthy sites BI=0
47 16.89 5.30 0.77 15.00 8.00 33.00 25.00 21.8 <0.001
Pre Number of interproximal sites BI=1,2
47 17.19 5.24 0.76 16.00 9.00 31.00 22.00
Number of changes to interproximal healthy sites BI=0
47 9.04 3.51 0.51 8.00 3.00 20.00 17.00 17.6 <0.001
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 164 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 166 of 177

Appendix Table 8 Day 30 Bleeding Index Summary Statistics
Sonic Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 45 0.43 0.14 0.02 0.42 0.23 0.77 0.54
Post whole mouth 45 0.15 0.10 0.02 0.12 0.02 0.50 0.48
Whole mouth change from Baseline
45 0.29 0.13 0.02 0.27 0.08 0.63 0.55 14.7 <0.001
Pre interproximal 45 0.50 0.16 0.02 0.48 0.23 0.88 0.65
Post interproximal
45 0.16 0.14 0.02 0.13 0.00 0.48 0.48
Interproximal change from Baseline
45 0.34 0.19 0.03 0.29 0.00 0.88 0.88 12.1 <0.001
Pre Number of whole mouth sites BI=1,2
45 30.58 6.65 0.99 31.00 20.00 46.00 26.00
Number of changes to whole mouth healthy sites BI=0
45 24.42 5.59 0.83 23.00 15.00 40.00 25.00 29.3 <0.001
Pre Number of interproximal sites BI=1,2
45 16.76 3.99 0.59 16.00 10.00 25.00 15.00
Number of changes to interproximal healthy sites BI=0
45 13.42 4.11 0.61 13.00 5.00 24.00 19.00 21.9 <0.001
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 165 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 167 of 177
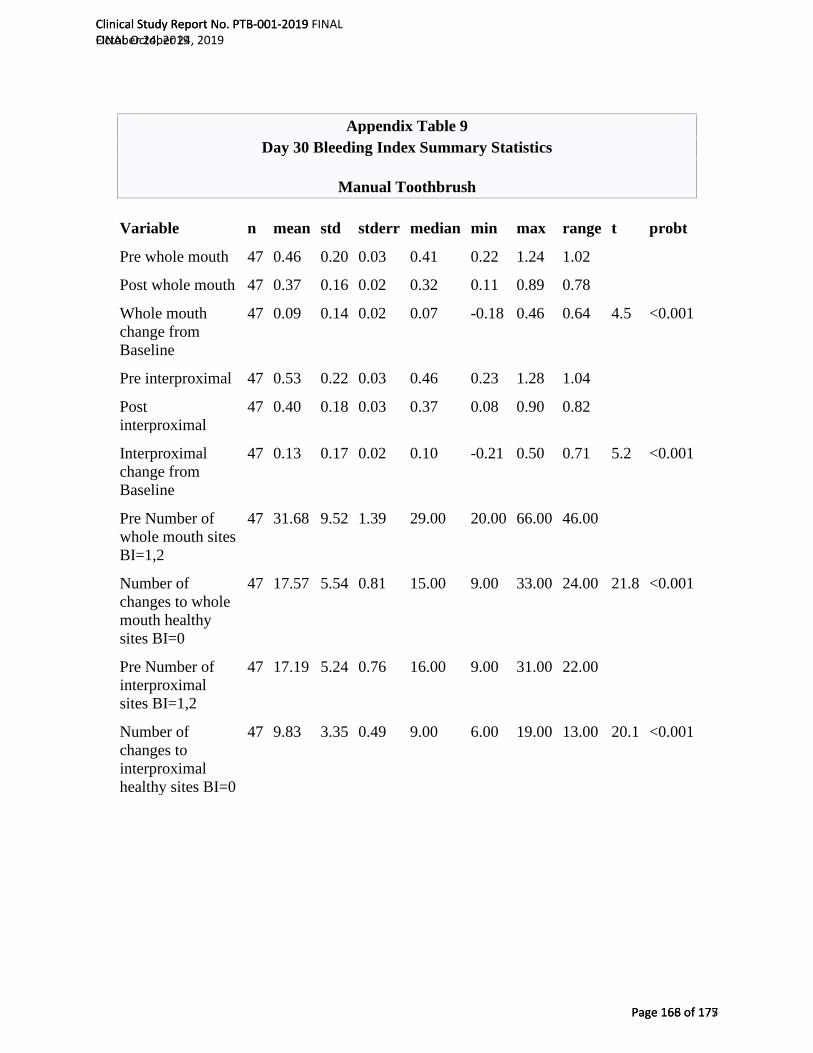
Appendix Table 9 Day 30 Bleeding Index Summary Statistics
Manual Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 47 0.46 0.20 0.03 0.41 0.22 1.24 1.02
Post whole mouth 47 0.37 0.16 0.02 0.32 0.11 0.89 0.78
Whole mouth change from Baseline
47 0.09 0.14 0.02 0.07 -0.18 0.46 0.64 4.5 <0.001
Pre interproximal 47 0.53 0.22 0.03 0.46 0.23 1.28 1.04
Post interproximal
47 0.40 0.18 0.03 0.37 0.08 0.90 0.82
Interproximal change from Baseline
47 0.13 0.17 0.02 0.10 -0.21 0.50 0.71 5.2 <0.001
Pre Number of whole mouth sites BI=1,2
47 31.68 9.52 1.39 29.00 20.00 66.00 46.00
Number of changes to whole mouth healthy sites BI=0
47 17.57 5.54 0.81 15.00 9.00 33.00 24.00 21.8 <0.001
Pre Number of interproximal sites BI=1,2
47 17.19 5.24 0.76 16.00 9.00 31.00 22.00
Number of changes to interproximal healthy sites BI=0
47 9.83 3.35 0.49 9.00 6.00 19.00 13.00 20.1 <0.001
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 166 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 168 of 177

Appendix Table 10 Baseline Pre-Post Plaque Index Summary Statistics
Sonic Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 45 2.90 0.35 0.05 2.87 2.33 3.71 1.38
Post whole mouth 45 2.30 0.45 0.07 2.30 1.50 3.18 1.68
Whole mouth change from Baseline
45 0.61 0.32 0.05 0.63 0.06 1.37 1.32 12.6 <0.001
Pre gumline 45 2.55 0.46 0.07 2.54 1.64 3.50 1.86
Post gumline 45 1.59 0.64 0.10 1.59 0.35 3.00 2.65
Gumline change from Baseline
45 0.95 0.49 0.07 0.93 0.13 1.91 1.78 13.1 <0.001
Pre interproximal 45 3.08 0.31 0.05 3.04 2.51 3.81 1.30
Post interproximal 45 2.65 0.39 0.06 2.71 1.80 3.33 1.54
Interproximal change from Baseline
45 0.43 0.27 0.04 0.42 0.02 1.20 1.18 10.7 <0.001
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 167 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 169 of 177

Appendix Table 11 Baseline Pre-Post Plaque Index Summary Statistics
Manual Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 47 2.93 0.28 0.04 2.91 2.34 3.38 1.04
Post whole mouth 47 2.47 0.43 0.06 2.54 1.40 3.23 1.82
Whole mouth change from Baseline
47 0.46 0.35 0.05 0.41 0.02 1.38 1.36 9.0 <0.001
Pre gumline 47 2.58 0.36 0.05 2.56 1.80 3.14 1.34
Post gumline 47 1.85 0.55 0.08 1.91 0.75 2.94 2.19
Gumline change from Baseline
47 0.72 0.46 0.07 0.60 0.00 1.93 1.93 10.8 <0.001
Pre interproximal 47 3.11 0.26 0.04 3.12 2.49 3.61 1.12
Post interproximal 47 2.78 0.39 0.06 2.80 1.73 3.46 1.73
Interproximal change from Baseline
47 0.33 0.32 0.05 0.25 -0.08 1.19 1.27 7.0 <0.001
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 168 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 170 of 177
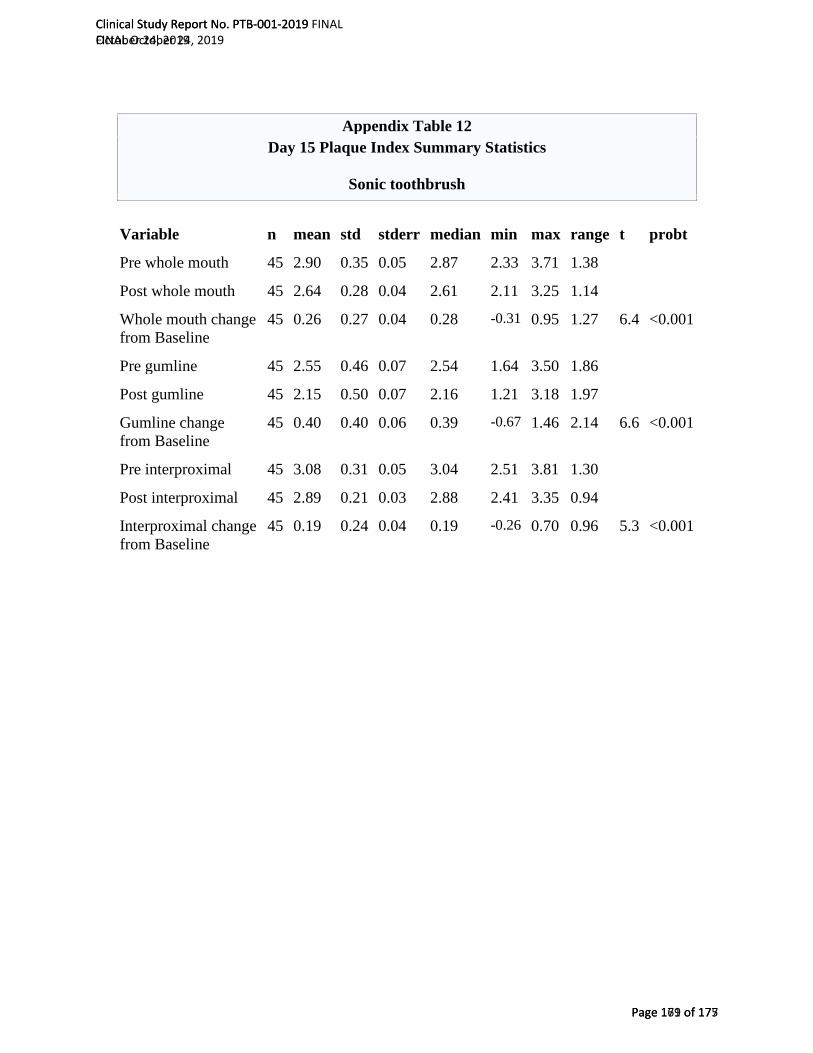
Appendix Table 12 Day 15 Plaque Index Summary Statistics
Sonic toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 45 2.90 0.35 0.05 2.87 2.33 3.71 1.38
Post whole mouth 45 2.64 0.28 0.04 2.61 2.11 3.25 1.14
Whole mouth change from Baseline
45 0.26 0.27 0.04 0.28 -0.31 0.95 1.27 6.4 <0.001
Pre gumline 45 2.55 0.46 0.07 2.54 1.64 3.50 1.86
Post gumline 45 2.15 0.50 0.07 2.16 1.21 3.18 1.97
Gumline change from Baseline
45 0.40 0.40 0.06 0.39 -0.67 1.46 2.14 6.6 <0.001
Pre interproximal 45 3.08 0.31 0.05 3.04 2.51 3.81 1.30
Post interproximal 45 2.89 0.21 0.03 2.88 2.41 3.35 0.94
Interproximal change from Baseline
45 0.19 0.24 0.04 0.19 -0.26 0.70 0.96 5.3 <0.001
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 169 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 171 of 177

Appendix Table 13 Day 15 Plaque Index Summary Statistics
Manual Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 47 2.93 0.28 0.04 2.91 2.34 3.38 1.04
Post whole mouth 47 2.91 0.29 0.04 2.89 2.25 3.52 1.27
Whole mouth change from Baseline
47 0.02 0.19 0.03 0.02 -0.39 0.46 0.86 0.8 0.413
Pre gumline 47 2.58 0.36 0.05 2.56 1.80 3.14 1.34
Post gumline 47 2.57 0.35 0.05 2.59 1.71 3.50 1.79
Gumline change from Baseline
47 0.01 0.28 0.04 -0.04 -0.66 0.77 1.43 0.2 0.856
Pre interproximal 47 3.11 0.26 0.04 3.12 2.49 3.61 1.12
Post interproximal 47 3.07 0.28 0.04 3.07 2.35 3.54 1.20
Interproximal change from Baseline
47 0.03 0.17 0.03 0.04 -0.36 0.42 0.78 1.2 0.242
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 170 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 172 of 177
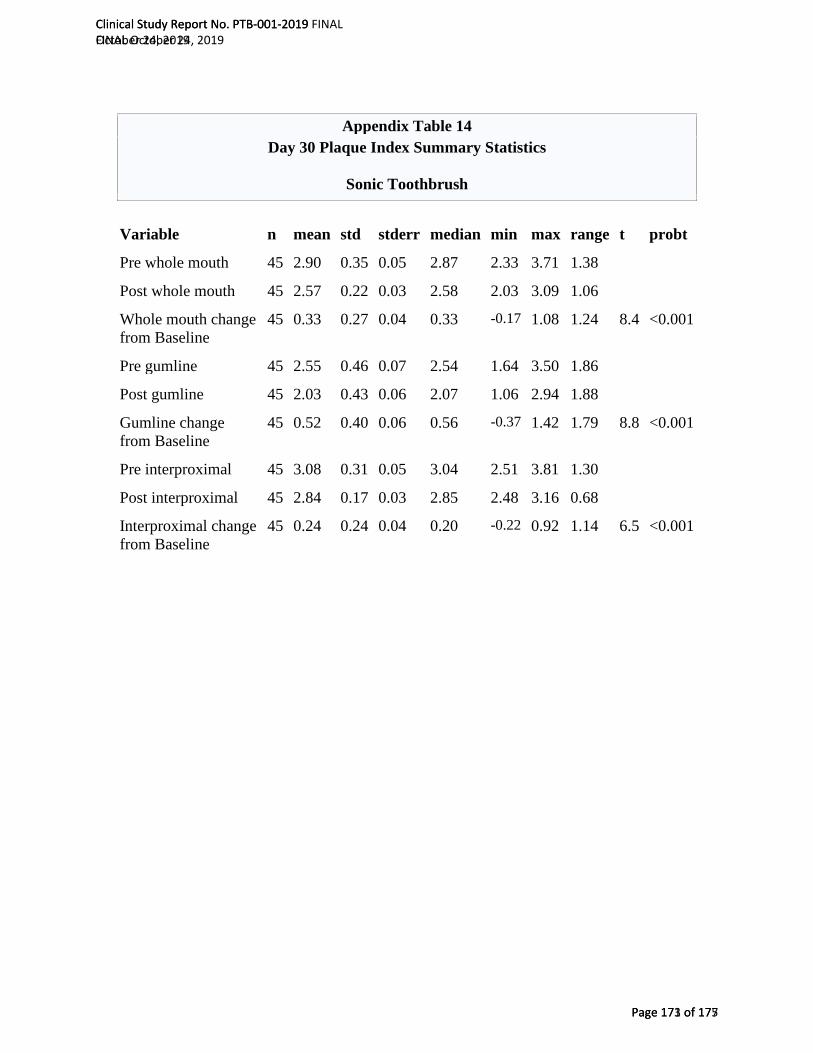
Appendix Table 14 Day 30 Plaque Index Summary Statistics
Sonic Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 45 2.90 0.35 0.05 2.87 2.33 3.71 1.38
Post whole mouth 45 2.57 0.22 0.03 2.58 2.03 3.09 1.06
Whole mouth change from Baseline
45 0.33 0.27 0.04 0.33 -0.17 1.08 1.24 8.4 <0.001
Pre gumline 45 2.55 0.46 0.07 2.54 1.64 3.50 1.86
Post gumline 45 2.03 0.43 0.06 2.07 1.06 2.94 1.88
Gumline change from Baseline
45 0.52 0.40 0.06 0.56 -0.37 1.42 1.79 8.8 <0.001
Pre interproximal 45 3.08 0.31 0.05 3.04 2.51 3.81 1.30
Post interproximal 45 2.84 0.17 0.03 2.85 2.48 3.16 0.68
Interproximal change from Baseline
45 0.24 0.24 0.04 0.20 -0.22 0.92 1.14 6.5 <0.001
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 171 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 173 of 177

Appendix Table 15 Day 30 Plaque Index Summary Statistics
Manual Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 47 2.93 0.28 0.04 2.91 2.34 3.38 1.04
Post whole mouth 47 2.90 0.34 0.05 2.92 2.27 3.59 1.32
Whole mouth change from Baseline
47 0.03 0.27 0.04 0.01 -0.74 0.58 1.32 0.8 0.443
Pre gumline 47 2.58 0.36 0.05 2.56 1.80 3.14 1.34
Post gumline 47 2.57 0.40 0.06 2.57 1.86 3.42 1.57
Gumline change from Baseline
47 0.01 0.36 0.05 0.02 -0.87 0.83 1.69 0.2 0.830
Pre interproximal 47 3.11 0.26 0.04 3.12 2.49 3.61 1.12
Post interproximal 47 3.06 0.32 0.05 3.09 2.40 3.67 1.27
Interproximal change from Baseline
47 0.04 0.25 0.04 0.01 -0.75 0.51 1.26 1.1 0.270
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 172 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 174 of 177
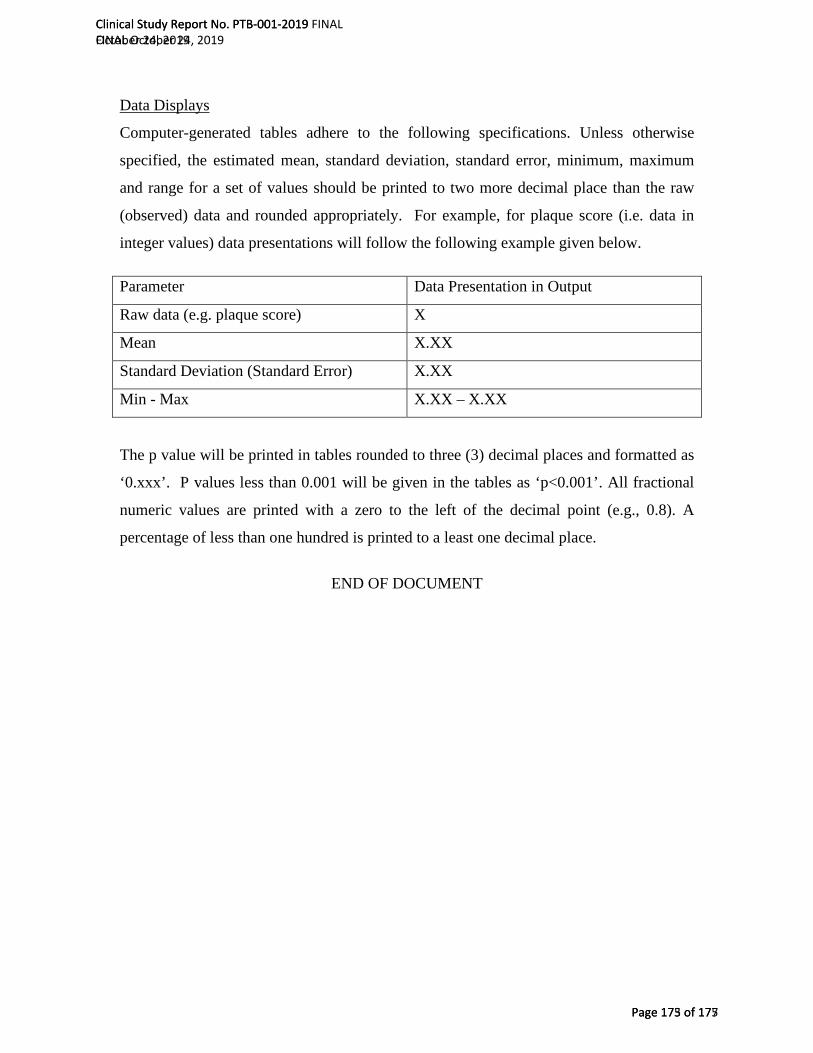
Data Displays
Computer-generated tables adhere to the following specifications. Unless otherwise
specified, the estimated mean, standard deviation, standard error, minimum, maximum
and range for a set of values should be printed to two more decimal place than the raw
(observed) data and rounded appropriately. For example, for plaque score (i.e. data in
integer values) data presentations will follow the following example given below.
Parameter Data Presentation in Output
Raw data (e.g. plaque score) X
Mean X.XX
Standard Deviation (Standard Error) X.XX
Min - Max X.XX – X.XX
The p value will be printed in tables rounded to three (3) decimal places and formatted as
‘0.xxx’. P values less than 0.001 will be given in the tables as ‘p<0.001’. All fractional
numeric values are printed with a zero to the left of the decimal point (e.g., 0.8). A
percentage of less than one hundred is printed to a least one decimal place.
END OF DOCUMENT
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 173 of 175
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 175 of 177

4.2.5 Adverse Event Listings (Each Subject)
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 176 of 177
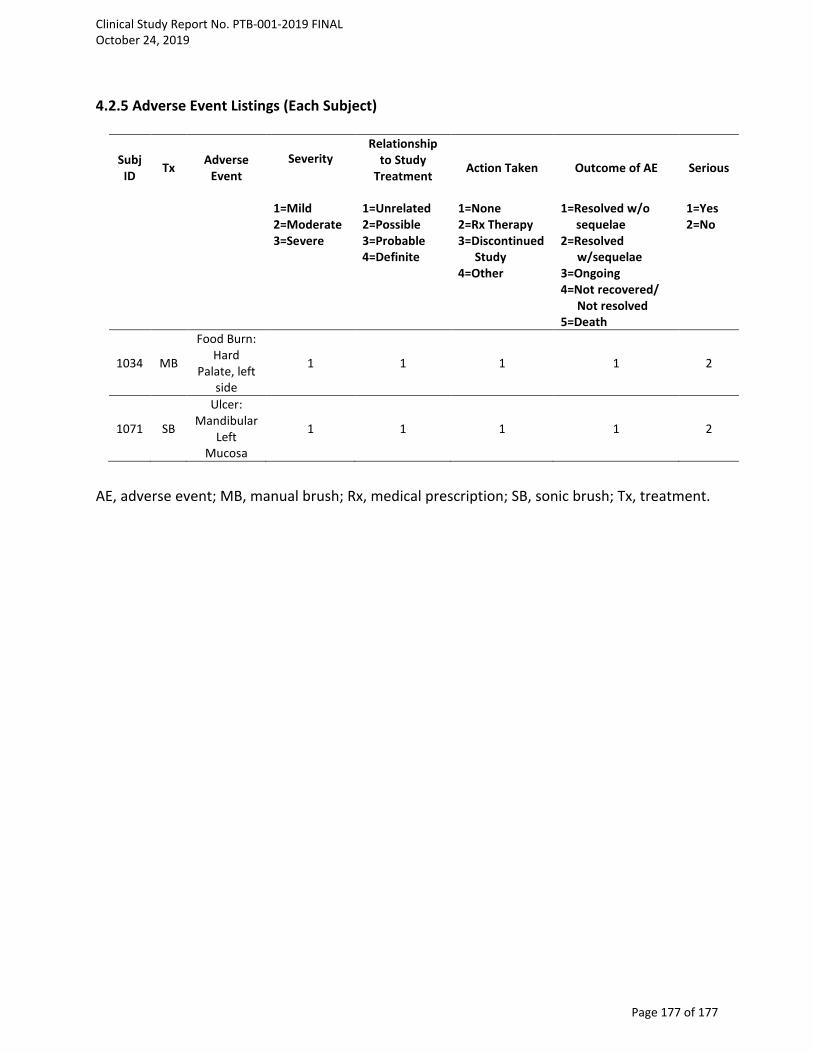
4.2.5 Adverse Event Listings (Each Subject)
Subj ID Tx Adverse
Event Severity
Relationship to Study
Treatment Action Taken Outcome of AE Serious
1=Mild 2=Moderate 3=Severe
1=Unrelated 2=Possible 3=Probable 4=Definite
1=None 2=Rx Therapy 3=Discontinued
Study 4=Other
1=Resolved w/o sequelae
2=Resolved w/sequelae
3=Ongoing 4=Not recovered/
Not resolved 5=Death
1=Yes 2=No
1034 MB
Food Burn: Hard
Palate, left side
1 1 1 1 2
1071 SB
Ulcer: Mandibular
Left Mucosa
1 1 1 1 2
AE, adverse event; MB, manual brush; Rx, medical prescription; SB, sonic brush; Tx, treatment.
Clinical Study Report No. PTB-001-2019 FINAL October 24, 2019
Page 177 of 177
1 TITLE PAGE
TITLE OF STUDY: Thirty-Day Evaluation of a Sonic Power Toothbrush Versus a Manual Toothbrush on Plaque and Gingivitis Efficacy
INVESTIGATIONAL MATERIALS:
Manual toothbrush: ADA reference manual soft-bristled toothbrush (Colgate® Classic [Pokey], Colgate-Palmolive Co., New York, NY) and ADA Accepted 0.243% sodium fluoride CREST® Cavity Protection toothpaste (Procter & Gamble, Cincinnati, OH, USA) Sonic toothbrush: BURST sonic power toothbrush (BURST.USA inc, Walnut, CA; brushing mode: whitening) and ADA Accepted 0.243% sodium fluoride CREST® Cavity Protection toothpaste (Procter & Gamble, Cincinnati, OH, USA)
Sponsor: BURST.USA.inc 340 S. Lemon Avenue #4658 Walnut, CA 91789
Protocol No.: PTB-002-2019
Investigator: Chhaju Ram Goyal, BDS All Sum Research Center Ltd. 1065 Canadian Place, Unit 102 Mississauga, ON, L4W 0C2
Study period: First Subject First Visit: 13 August 2019 Last Subject Last Visit: 13 September 2019
GCP Statement: This study was performed in compliance with ICH Good Clinical Practice (GCP) including the archiving of essential documents.
Date of report: 24 October 2019
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 1 of 179
11/01/2019
1 TITLE PAGE ............................................................................................................................... 1
2 SYNOPSIS REPORT .................................................................................................................... 6
2.2 INTRODUCTION ................................................................................................................ 6
2.3 METHODOLOGY ............................................................................................................... 7
2.4 STATISTICAL METHODS .................................................................................................... 9
3 SUMMARY RESULTS AND CONCLUSIONS .............................................................................. 10
3.1 SAFETY RESULTS ............................................................................................................. 12
3.2 EFFICACY RESULTS .......................................................................................................... 12
3.3 DISCUSSION .................................................................................................................... 20
3.4 CONCLUSION .................................................................................................................. 21
3.5 REFERENCES ................................................................................................................... 22
4 APPENDICES ........................................................................................................................... 25
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 3 of 179

ABSTRACT
Thirty-Day Evaluation of a Sonic Power Toothbrush Versus a Manual Toothbrush on Plaque and Gingivitis Efficacy
Objective: This single-center, randomized, controlled, examiner-blind, 30-day parallel clinical trial evaluated the efficacy of a sonic power toothbrush on plaque and gingivitis, compared to a manual toothbrush. Methods: Upon meeting eligibility criteria, a total of 97 generally healthy subjects with mild to moderate plaque and gingivitis levels were randomly assigned to one of two treatment groups: 1) twice daily brushing in usual manner with an ADA reference flat trim manual toothbrush and standard 0.243% sodium fluoride Crest® Cavity Protection toothpaste (control group); 2) Twice daily brushing for a total of 2 minutes with a BURST Sonic power toothbrush and standard 0.243% sodium fluoride Crest® Cavity Protection toothpaste (sonic toothbrush group). At baseline, Day 15 (± 2 days) and Day 30 (± 2 days), subjects refrained from oral hygiene for approximately 8 – 12 hours prior to each exam visit, received a clinical oral examination for oral safety, and were assessed for gingivitis according to the Modified Gingival Index (MGI), gingival bleeding according to the Bleeding Index (BI) and supragingival plaque levels according to the Lobene-Soparkar Modification of the Turesky Modification of the Quigley-Hein Plaque Index (PI). Following the supervised use of the assigned products at baseline, subjects were examined again for post-brushing plaque removal. Treatment means and between-treatment means were assessed by the ANCOVA model. Results: There were no treatment-related oral adverse events identified during the study demonstrating that all treatment materials were well-tolerated. For the 97 evaluable subjects, there were no significant differences between groups for demographics or for the baseline efficacy variables. Statistically significant reductions in gingivitis, bleeding, and plaque were observed for the sonic toothbrush group compared to the manual toothbrush control at Days 15 and 30 (p<0.05). Mean MGI was reduced from baseline by 6.3% and 9.5% for the sonic toothbrush and by 3.2% and 5.4% for the manual toothbrush group at Days 15 and 30, respectively. Using the sonic toothbrush resulted in 6.0 (Day 15) and 14.0 (Day 30) more healthy gingival sites (MGI) than at baseline. Mean whole mouth BI scores were reduced from baseline by 21.2% and 35.0% for the sonic toothbrush as compared with 11.1% and 17.6% for the manual toothbrush control. Improvement in Baseline Pre- to Post-brushing plaque scores for the sonic toothbrush were significantly better (p<0.001) than the manual toothbrush control for whole mouth, gumline, and interproximal sites at 33%, 27% and 37%, respectively. At Days 15 and 30, mean whole mouth PI reductions from baseline were 11.0% and 15.7% for the sonic toothbrush and 5.8% and 9.0% for the manual toothbrush at Days 15 and 30.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 4 of 179
Conclusion: The sonic toothbrush was superior in reducing gingivitis, bleeding and plaque at Days 15 and 30 when compared to the control manual toothbrush, and with respect to baseline Pre- to Post-brush plaque removal.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 5 of 179

2 SYNOPSIS REPORT 2.1 OBJECTIVE The objective of this 30-day, randomized, controlled, examiner-blind, parallel design clinical trial was to evaluate the efficacy of a marketed sonic power toothbrush (BURST sonic) on plaque and gingivitis compared to a manual toothbrush and standard fluoride dentifrice. Safety was assessed through oral clinical examinations and interviews to determine soft tissue or oral irritation symptoms, and monitoring of adverse events (AEs) / serious AEs.
2.2 INTRODUCTION The effective management of dental plaque and gingivitis continues to be a high priority for the dental health of the public. Dental professionals recommend brushing at least twice a day to remove plaque and reduce the risk of tooth decay and gum disease.1 A recent study by Ebel and co-workers2 assessed the impact of brushing time, brushing techniques, and brushing systematics of young adults (18 years old) on efficiency of plaque removal with a standard manual toothbrush. Subjects were asked to clean their teeth to the best of their abilities. They found that participants distributed their brushing time across surfaces unevenly which explained the variance of plaque and bleeding. Brushing technique appeared to be of minor importance. The researchers concluded that the results indicated that establishing systematic interventions or prophylactic programs should emphasize the importance of brushing all surfaces and not neglecting any teeth. However, the high prevalence of oral diseases worldwide suggests that consumers do not achieve sufficient plaque removal with their manual toothbrushing routine. Although dental professionals emphasize the importance of improving brushing habits with patients, research indicates behavior modification is challenging. Clinical studies have shown that improvement in mechanical oral hygiene can be achieved using power toothbrushes.2-8 Power toothbrush innovations are intended not only to optimize plaque removal and improve gingival health but also to encourage better brushing behavior. This single-center, randomized, controlled, examiner-blind, 30-day, parallel study was designed to evaluate the safety and efficacy of a sonic power toothbrush with charcoal infused toothbrush bristles compared to an ADA reference manual soft toothbrush on plaque and gingivitis. Standard plaque and gingivitis clinical trials test for differences between treatment groups evaluating changes in mean plaque and gingivitis index scores. For this study, post-treatment efficacy endpoints included mean change in MGI scores (whole mouth and interproximal) change in mean number of healthy sites (MGI=0, 1) at Days 15 and 30; mean change in BI scores (whole mouth and interproximal) and mean change in number of bleedings sites (BI=1 or
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 6 of 179
2 from baseline to “0” bleeding sites) at Days 15 and 30; and mean change in PI scores at baseline (Pre – Post-brushing), Day 15 and Day 30 (whole mouth, gumline, and interproximal PI scores).
2.3 METHODOLOGY
Prior to the initiation of this study, the study protocol, informed consent document and subject instructions received ethical review and approval from Veritas IRB, Inc. The study was conducted in accordance with the International Conference on Harmonization Good Clinical Practice guidelines (ICH GCP) and all subjects signed an informed consent prior to entering the study. The study was a single-center, randomized, controlled, examiner-blind, 30-day parallel study. Based on the assumption that the sonic power toothbrush group improvement would exceed that of the control group by at least 25% at Days 15 and 30, the calculated total sample size of 90 completed subjects (45 per group) provided 90% power to detect a difference of 0.24 with respect to MGI, and 0.4 with respect to PI when compared to the control group, with an effect size (mean/standard deviation) of 0.7, at the Day 30 assessment. These calculations were based on two-sided tests at the 0.05 significance level.
This study was designed according to the American Dental Association Council on Scientific Affairs Acceptance Program Requirements for Toothbrushes. Generally healthy adult subjects (≥ 18 years of age) were eligible and enrolled in this study if they presented with a least 18 natural teeth with scorable facial and lingual surfaces, a mean gingival index of 1.75–2.3, according to the Modified Gingival Index (MGI),9 a minimum of 20 bleeding sites based on the Bleeding Index of Saxton and van der Ouderaa,10 and a mean plaque index ≥ 1.95 according to the Lobene-Soparkar Modification of the Turesky Modification of the Quigley-Hein Plaque Index (PI).11,12 Subjects were excluded if they had significant oral soft tissue pathology; severe periodontal disease or concurrent periodontal treatment; grossly carious, fully crowned, or extensively restored teeth; orthodontic appliances; peri/oral piercings or removable partial dentures; self-reported serious medical conditions; under treatment for a heart condition requiring use of a pacemaker; required antibiotic premedication prior to dental procedures; having had antibiotic, anti-inflammatory, anti-coagulant medication or chemotherapeutic antiplaque/antigingivitis therapy within 30 days of screening; or participated in any study involving oral care products concurrently or within 30 days of screening.
All subjects who enrolled in the study signed an informed consent document and agreed to refrain from dental treatment during the course of the study, except on an emergency basis, and were willing to discontinue use of other oral hygiene products for the duration of the
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 7 of 179
study. This study consisted of a Screening/Baseline visit during which subjects read and signed an informed consent form, completed health and dental questionnaires and received a clinical oral examination. At Screening/Baseline, Day 15 and Day 30, subjects received an oral examination that included assessments in the following order:
• Oral safety (soft and hard tissue examination for evidence of irritation or other abnormalities);
• Gingivitis according to the Modified Gingival Index (MGI); • Gingival bleeding according to the Bleeding Index described by Saxton and van der
Ouderaa (BI); • Supragingival plaque levels, determined according to the Lobene-Soparkar Modification
of the Turesky Modification of the Quigley-Hein Plaque Index (PI). o At the baseline visit only, a Post-Brush PI assessment was performed. o Plaque was disclosed by rinsing with an erythrosine dye solution prior to each
assessment of supragingival plaque.
Prior to each exam visit, subjects refrained from oral hygiene for 8 to 12 hours and did not eat, drink or smoke for at least 30 minutes prior to the visit. All clinical exams were conducted by a single, experienced and validated dental examiner.
Subjects meeting study entrance criteria were randomly assigned to one of two treatment groups:
1) Manual Toothbrush (Control): Twice daily brushing with ADA reference manual soft-bristled toothbrush (Colgate® Classic [Pokey], Colgate-Palmolive Co., New York, NY) and ADA Accepted 0.243% sodium fluoride CREST® Cavity Protection toothpaste (Procter & Gamble, Cincinnati, OH, USA)
2) Sonic Toothbrush: Twice daily brushing with BURST sonic power toothbrush (BURST.USA inc, Walnut, CA; brushing mode: whitening) and ADA Accepted 0.243% sodium fluoride CREST® Cavity Protection toothpaste (Procter & Gamble, Cincinnati, OH, USA)
Subjects were provided verbal and written instructions on the use of their assigned toothbrush. All subjects brushed with their assigned toothbrush under the supervision of study personnel for the first use, and unsupervised thereafter. Subjects assigned to the sonic toothbrush were instructed to brush for two minutes according the manufacturer’s instruction. Those assigned to the manual toothbrush were instructed to brush in their usual manner. Immediately following the first use of their assigned toothbrush at baseline, subjects were redisclosed with the erythrosine dye examined again to assess the immediate effect of each toothbrush in removing supragingival plaque. All subjects maintained a daily diary to document compliance.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 8 of 179
Assignment process, subsequent product distribution and supervised brushing were conducted in a protected area that ensured blinding of the clinical examiner and the data recorders to subjects’ assignments to their toothbrush. Following the baseline exams, subjects returned at Days 15 and 30 for the same assessments for oral safety, gingival health (MGI and BI) and plaque. A single experienced examiner conducted the oral tissue safety examination and the plaque and gingivitis/bleeding assessments. During the study, subjects refrained from using any oral care products other than the assigned toothbrush and toothpaste provided to them and they also avoided the use of other toothbrushes, toothpaste, mouthwashes, chewing gums, breath films, mints, flow or interdental cleaning aids, or other oral care cleaning aids. Subjects were instructed to only use dental floss to remove food impaction.
The efficacy endpoints were:
• Mean change in MGI scores at Days 15 and 30: Whole mouth Interproximal (mesial & distal)
• Change in mean number of healthy sites (MGI=0, 1) at Days 15 and 30 • Mean change in BI scores at Day 15 and 30:
Whole mouth Interproximal (mesial & distal)
• Mean change in number of bleeding sites (BI=1 or 2) from baseline to “0” bleeding sites at Days 15 and 30. Whole mouth Interproximal (mesial & distal)
• Mean change in PI scores at Baseline Pre - Post-brushing, Days 15 and 30 for: Whole mouth PI scores; Gumline PI scores (marginal); Interproximal PI scores (mesial and distal).
2.4 STATISTICAL METHODS Data analysis sets included evaluable subjects, defined as subjects without major protocol violations. Data for safety analysis included all subjects who received treatment. Demographic and baseline characteristics were summarized for age, gender, race, tobacco use, mean MGI, BI and PI, and mean number of healthy gingival sites (MGI=0, 1; BI=0). Analysis of the number of healthy sites were performed to evaluate the performance of the toothbrushes in achieving healthy gingival status. Summary statistics were provided by treatment group for plaque and gingivitis (MGI and BI) scores before brushing at baseline, for plaque scores post-brushing at baseline, and for plaque and gingivitis (MGI and BI) scores before brushing at Days 15 and 30.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 9 of 179

Categorical demographic and baseline data were evaluated using Fisher’s Exactness Test and continuous demographic and baseline data were evaluated using ANOVA. All tests were two-sided and conducted at the 0.05 significance level. No adjustments were made for multiple comparisons or multiple testing.
Full details of the study protocol are provided in Appendix 4.1.1
3 SUMMARY RESULTS AND CONCLUSIONS A total of 97 subjects met the study entrance criteria and were randomized to one of the two treatment groups. All 97 subjects completed all study visits. Demographics characteristics for the 97 evaluable subjects are provided in Table 1 and Appendix 4.2.4 Appendix Table 1 of the Statistical Report. Randomized subjects’ ages ranged from 18 to 72 years with an overall mean of 48 years. There were 66 females and 31 males, and the majority of the population was white (53.6%), non-Hispanic (99.0%) and not tobacco users (93.8%). There were no significant differences between groups for baseline demographics or for the baseline efficacy variables (MGI, p>0.259; BI, p>0.575; PI, p>0.615).
Compliance: Subject compliance with their assigned home care routine was assessed at the Day 15 and 30 visits through review of the subjects’ daily diaries. Subjects were required to maintain their daily diary and to record the time of completion of their assigned morning and evening toothbrushing. Based on review of completed diaries and interviews with subjects, all 97 subjects were in compliant with their twice daily use of their assigned toothbrush. All subjects attended study visits as scheduled and there were no protocol deviations.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 10 of 179
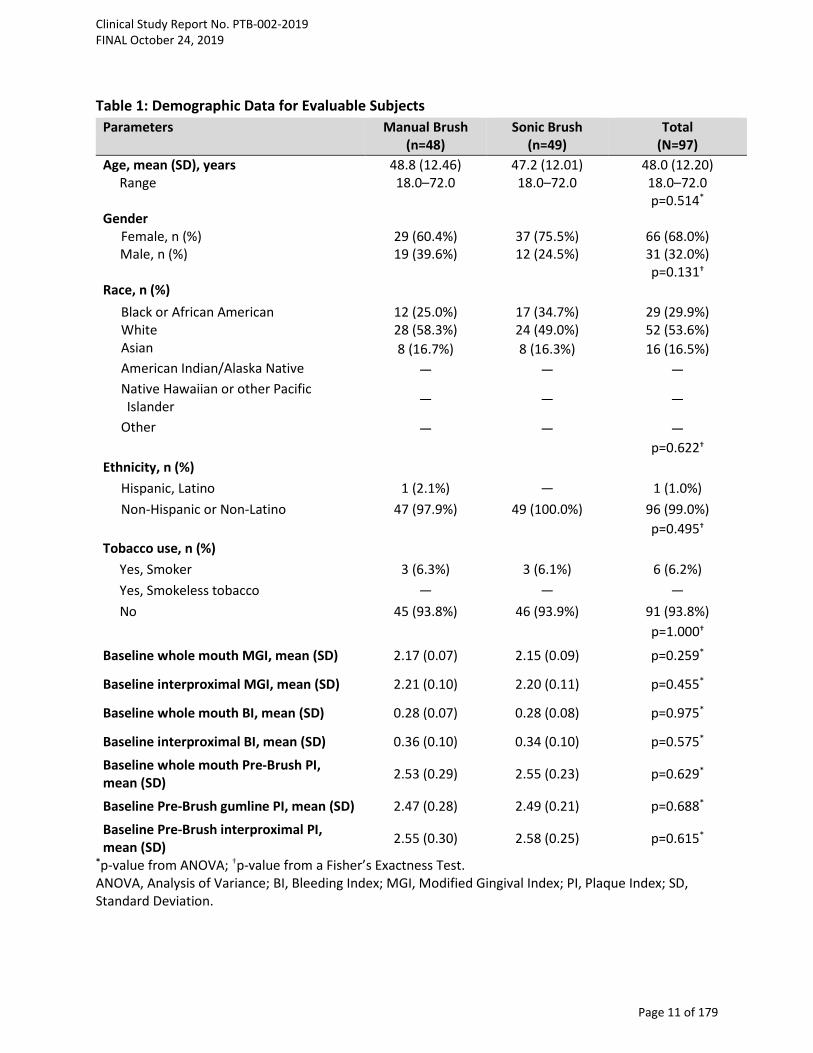
Table 1: Demographic Data for Evaluable Subjects Parameters Manual Brush
(n=48) Sonic Brush
(n=49) Total
(N=97) Age, mean (SD), years 48.8 (12.46) 47.2 (12.01) 48.0 (12.20) Range 18.0–72.0 18.0–72.0 18.0–72.0 p=0.514* Gender
Female, n (%) 29 (60.4%) 37 (75.5%) 66 (68.0%) Male, n (%) 19 (39.6%) 12 (24.5%) 31 (32.0%)
p=0.131† Race, n (%)
Black or African American 12 (25.0%) 17 (34.7%) 29 (29.9%) White 28 (58.3%) 24 (49.0%) 52 (53.6%) Asian 8 (16.7%) 8 (16.3%) 16 (16.5%) American Indian/Alaska Native — — — Native Hawaiian or other Pacific Islander — — —
Other — — — p=0.622†
Ethnicity, n (%) Hispanic, Latino 1 (2.1%) — 1 (1.0%) Non-Hispanic or Non-Latino 47 (97.9%) 49 (100.0%) 96 (99.0%)
p=0.495† Tobacco use, n (%) Yes, Smoker 3 (6.3%) 3 (6.1%) 6 (6.2%) Yes, Smokeless tobacco — — — No 45 (93.8%) 46 (93.9%) 91 (93.8%) p=1.000†
Baseline whole mouth MGI, mean (SD) 2.17 (0.07) 2.15 (0.09) p=0.259*
Baseline interproximal MGI, mean (SD) 2.21 (0.10) 2.20 (0.11) p=0.455*
Baseline whole mouth BI, mean (SD) 0.28 (0.07) 0.28 (0.08) p=0.975*
Baseline interproximal BI, mean (SD) 0.36 (0.10) 0.34 (0.10) p=0.575*
Baseline whole mouth Pre-Brush PI, mean (SD) 2.53 (0.29) 2.55 (0.23) p=0.629*
Baseline Pre-Brush gumline PI, mean (SD) 2.47 (0.28) 2.49 (0.21) p=0.688*
Baseline Pre-Brush interproximal PI, mean (SD) 2.55 (0.30) 2.58 (0.25) p=0.615*
*p-value from ANOVA; †p-value from a Fisher’s Exactness Test. ANOVA, Analysis of Variance; BI, Bleeding Index; MGI, Modified Gingival Index; PI, Plaque Index; SD, Standard Deviation.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 11 of 179
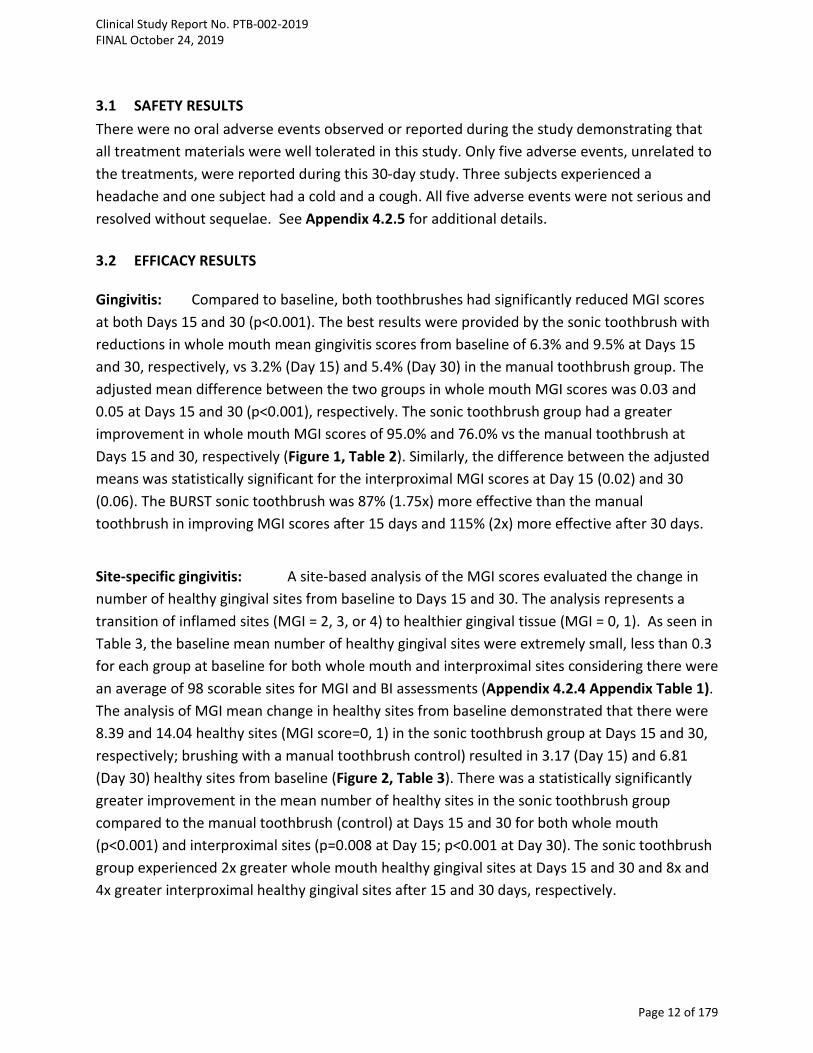
3.1 SAFETY RESULTS There were no oral adverse events observed or reported during the study demonstrating that all treatment materials were well tolerated in this study. Only five adverse events, unrelated to the treatments, were reported during this 30-day study. Three subjects experienced a headache and one subject had a cold and a cough. All five adverse events were not serious and resolved without sequelae. See Appendix 4.2.5 for additional details. 3.2 EFFICACY RESULTS Gingivitis: Compared to baseline, both toothbrushes had significantly reduced MGI scores at both Days 15 and 30 (p<0.001). The best results were provided by the sonic toothbrush with reductions in whole mouth mean gingivitis scores from baseline of 6.3% and 9.5% at Days 15 and 30, respectively, vs 3.2% (Day 15) and 5.4% (Day 30) in the manual toothbrush group. The adjusted mean difference between the two groups in whole mouth MGI scores was 0.03 and 0.05 at Days 15 and 30 (p<0.001), respectively. The sonic toothbrush group had a greater improvement in whole mouth MGI scores of 95.0% and 76.0% vs the manual toothbrush at Days 15 and 30, respectively (Figure 1, Table 2). Similarly, the difference between the adjusted means was statistically significant for the interproximal MGI scores at Day 15 (0.02) and 30 (0.06). The BURST sonic toothbrush was 87% (1.75x) more effective than the manual toothbrush in improving MGI scores after 15 days and 115% (2x) more effective after 30 days.
Site-specific gingivitis: A site-based analysis of the MGI scores evaluated the change in number of healthy gingival sites from baseline to Days 15 and 30. The analysis represents a transition of inflamed sites (MGI = 2, 3, or 4) to healthier gingival tissue (MGI = 0, 1). As seen in Table 3, the baseline mean number of healthy gingival sites were extremely small, less than 0.3 for each group at baseline for both whole mouth and interproximal sites considering there were an average of 98 scorable sites for MGI and BI assessments (Appendix 4.2.4 Appendix Table 1). The analysis of MGI mean change in healthy sites from baseline demonstrated that there were 8.39 and 14.04 healthy sites (MGI score=0, 1) in the sonic toothbrush group at Days 15 and 30, respectively; brushing with a manual toothbrush control) resulted in 3.17 (Day 15) and 6.81 (Day 30) healthy sites from baseline (Figure 2, Table 3). There was a statistically significantly greater improvement in the mean number of healthy sites in the sonic toothbrush group compared to the manual toothbrush (control) at Days 15 and 30 for both whole mouth (p<0.001) and interproximal sites (p=0.008 at Day 15; p<0.001 at Day 30). The sonic toothbrush group experienced 2x greater whole mouth healthy gingival sites at Days 15 and 30 and 8x and 4x greater interproximal healthy gingival sites after 15 and 30 days, respectively.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 12 of 179

Figure 1. Gingivitis Reduction from Baseline
MGI, Modified Gingival Index.
Table 2: Adjusted MGI Means and Percent Reductions
VISITS EFFICACY VARIABLES Manual
Toothbrush (n=48)
Sonic Toothbrush (n=49)
Mean ± SE Mean ± SE
BASELINE Whole Mouth MGI¥ 2.17 ± 0.01 2.15 ± 0.01 Interproximal MGI¥ 2.21 ± 0.01 2.2 ± 0.02
DAY 15
Whole Mouth MGI¥ 2.09 ± 0.01 2.03 ± 0.01 Difference between adj. means 0.07* ± 0.016
% Reduction from baseline 3.2% 6.3% Interproximal MGI 2.16 ± 0.01 2.11 ± 0.01
Difference between adj. means 0.05† ± 0.01 % Reduction from baseline 2.3% 4.3%
DAY 30
Whole Mouth MGI 2.04 ± 0.01 1.96 ± 0.01 Difference between adj. means 0.08* ± 0.015
% Reduction from baseline 5.4% 9.5% Interproximal MGI 2.14 ± 0.01 2.05* ± 0.01
Difference between adj. means 0.08* ± 0.016 % Reduction from baseline 3.2% 6.8%
¥Baseline Unadjusted Means; *p<0.0001 vs MB; †p=0.002 vs MB. MB, manual brush; SB, sonic brush; MGI, Modified Gingival Index.
3.20%
5.40%
2.30%
3.20%
6.30%
9.50%
4.30%
6.80%
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
Day 15Whole Mouth
Day 30Whole Mouth
Day 15Interproximal
Day 30Interproximal
MGI Percent Reduction From Baseline
Manual Toothbrush (Control) Sonic Toothbrush
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 13 of 179
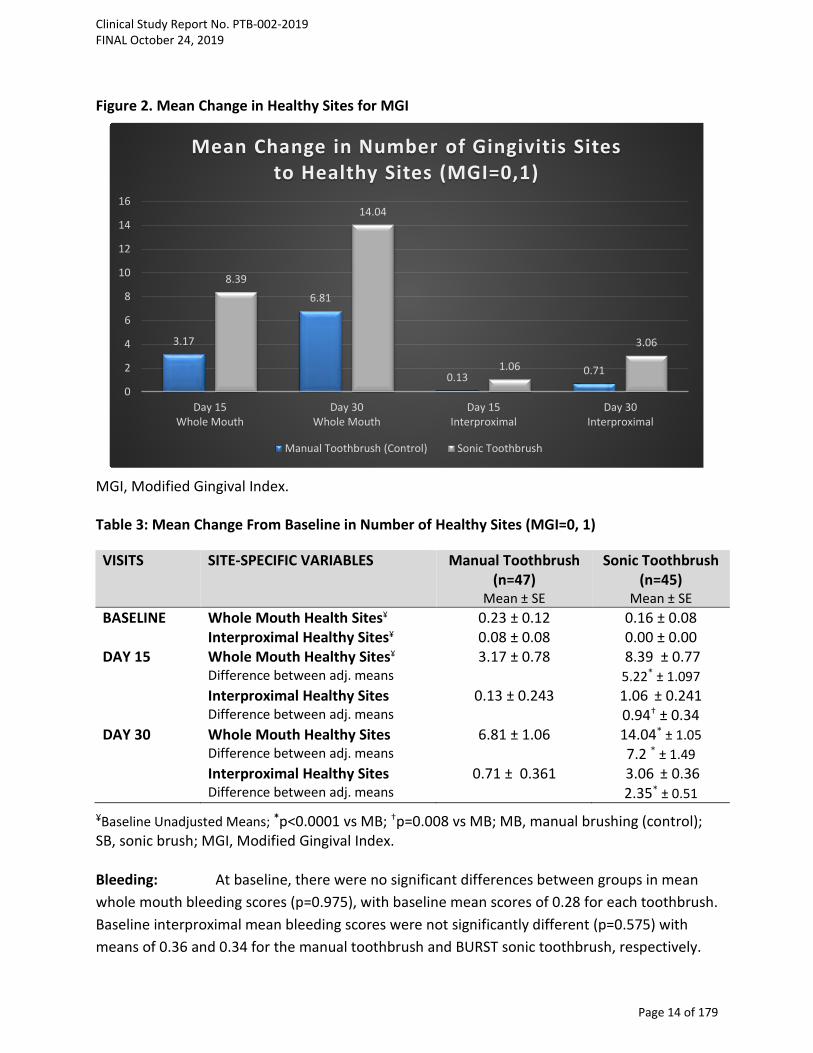
Figure 2. Mean Change in Healthy Sites for MGI
MGI, Modified Gingival Index.
Table 3: Mean Change From Baseline in Number of Healthy Sites (MGI=0, 1)
VISITS SITE-SPECIFIC VARIABLES Manual Toothbrush (n=47)
Sonic Toothbrush (n=45)
Mean ± SE Mean ± SE BASELINE Whole Mouth Health Sites¥ 0.23 ± 0.12 0.16 ± 0.08 Interproximal Healthy Sites¥ 0.08 ± 0.08 0.00 ± 0.00 DAY 15 Whole Mouth Healthy Sites¥ 3.17 ± 0.78 8.39 ± 0.77 Difference between adj. means 5.22* ± 1.097 Interproximal Healthy Sites 0.13 ± 0.243 1.06 ± 0.241 Difference between adj. means 0.94† ± 0.34 DAY 30 Whole Mouth Healthy Sites 6.81 ± 1.06 14.04* ± 1.05 Difference between adj. means 7.2 * ± 1.49 Interproximal Healthy Sites 0.71 ± 0.361 3.06 ± 0.36 Difference between adj. means 2.35* ± 0.51
¥Baseline Unadjusted Means; *p<0.0001 vs MB; †p=0.008 vs MB; MB, manual brushing (control); SB, sonic brush; MGI, Modified Gingival Index.
Bleeding: At baseline, there were no significant differences between groups in mean whole mouth bleeding scores (p=0.975), with baseline mean scores of 0.28 for each toothbrush. Baseline interproximal mean bleeding scores were not significantly different (p=0.575) with means of 0.36 and 0.34 for the manual toothbrush and BURST sonic toothbrush, respectively.
3.17
6.81
0.13 0.71
8.39
14.04
1.06
3.06
0
2
4
6
8
10
12
14
16
Day 15Whole Mouth
Day 30Whole Mouth
Day 15Interproximal
Day 30Interproximal
Mean Change in Number of Gingivitis Sites to Healthy Sites (MGI=0,1)
Manual Toothbrush (Control) Sonic Toothbrush
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 14 of 179

BURST sonic toothbrush was statistically superior to the manual toothbrush control at all time points (p=0.031, or less). As shown in Table 4 and Figure 3, whole mouth and interproximal bleeding for both groups was significantly reduced from baseline (p<0.001). The sonic toothbrush had the greatest reduction in whole mouth bleeding with percent reductions from baseline of 21.2% and 35.0% at Days 15 and 30 as compared with 11.1% (Day 15) and 17.6% (Day 30) in the manual toothbrush group. By Day 15 and Day 30, the sonic toothbrush provided 2x (92% and 99%, respectively) greater improvement in gingival bleeding compared to the ADA reference brush (Figure 3, Table 4).
Site-specific bleeding: Similar to the MGI analysis, a site based analysis of the BI scores measured the mean change in number of bleeding sites from baseline to Days 15 and 30. The analysis represents a transition of the number of whole mouth and interproximal bleeding sites (BI = 1 or 2) to healthier sites with a score “0”. At baseline, the mean number of whole mouth bleeding sites was 25.81 for the manual toothbrush group, 25.9 for the sonic toothbrush group. BURST sonic toothbrush had significantly fewer bleeding sites at Days 15 (p=0.002) and 30 (p<0.001) than the manual toothbrush group (Table 5). The mean change in the number of bleeding sites (BI=1 or 2) to non-bleeding, healthy sites (BI=0) for the manual toothbrush (control) was 4.06 (Day 15) and 6.77 (Day 30) vs 6.04 (Day 15) and 9.96 (Day 30) for the sonic toothbrush group (Figure 4). The sonic toothbrush provided 49% (1.5x) and 47% (1.5x) greater improvement of mean change in whole mouth bleeding sites, compared to the manual toothbrush.
Figure 3. Bleeding Reduction from Baseline
BI, Bleeding Index.
11.10%
17.60%13.80%
20.50%21.20%
35.00%
19.90%
36.00%
0%
5%
10%
15%
20%
25%
30%
35%
40%
Day 15Whole Mouth
Day 30Whole Mouth
Day 15Interproximal
Day 30Interproximal
BI Percent Reduction From Baseline
Manual Toothbrush (Control) Sonic Toothbrush
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 15 of 179
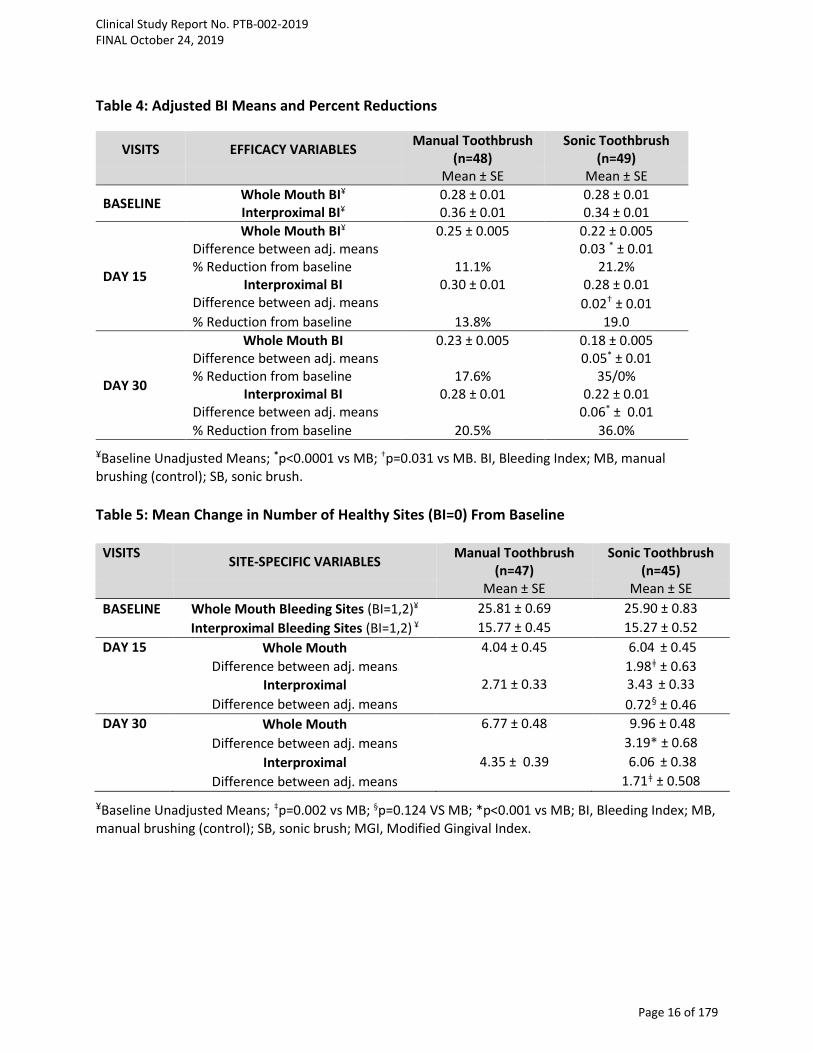
Table 4: Adjusted BI Means and Percent Reductions
VISITS EFFICACY VARIABLES Manual Toothbrush (n=48)
Sonic Toothbrush (n=49)
Mean ± SE Mean ± SE
BASELINE Whole Mouth BI¥ 0.28 ± 0.01 0.28 ± 0.01 Interproximal BI¥ 0.36 ± 0.01 0.34 ± 0.01
DAY 15
Whole Mouth BI¥ 0.25 ± 0.005 0.22 ± 0.005 Difference between adj. means 0.03 * ± 0.01 % Reduction from baseline 11.1% 21.2%
Interproximal BI 0.30 ± 0.01 0.28 ± 0.01 Difference between adj. means 0.02† ± 0.01 % Reduction from baseline 13.8% 19.0
DAY 30
Whole Mouth BI 0.23 ± 0.005 0.18 ± 0.005 Difference between adj. means 0.05* ± 0.01 % Reduction from baseline 17.6% 35/0%
Interproximal BI 0.28 ± 0.01 0.22 ± 0.01 Difference between adj. means 0.06* ± 0.01 % Reduction from baseline 20.5% 36.0%
¥Baseline Unadjusted Means; *p<0.0001 vs MB; †p=0.031 vs MB. BI, Bleeding Index; MB, manual brushing (control); SB, sonic brush. Table 5: Mean Change in Number of Healthy Sites (BI=0) From Baseline
VISITS SITE-SPECIFIC VARIABLES Manual Toothbrush (n=47)
Sonic Toothbrush (n=45)
Mean ± SE Mean ± SE BASELINE Whole Mouth Bleeding Sites (BI=1,2)¥ 25.81 ± 0.69 25.90 ± 0.83 Interproximal Bleeding Sites (BI=1,2) ¥ 15.77 ± 0.45 15.27 ± 0.52 DAY 15 Whole Mouth 4.04 ± 0.45 6.04 ± 0.45 Difference between adj. means 1.98ǂ ± 0.63 Interproximal 2.71 ± 0.33 3.43 ± 0.33 Difference between adj. means 0.72§ ± 0.46 DAY 30 Whole Mouth 6.77 ± 0.48 9.96 ± 0.48 Difference between adj. means 3.19* ± 0.68 Interproximal 4.35 ± 0.39 6.06 ± 0.38 Difference between adj. means 1.71ǂ ± 0.508
¥Baseline Unadjusted Means; ‡p=0.002 vs MB; §p=0.124 VS MB; *p<0.001 vs MB; BI, Bleeding Index; MB, manual brushing (control); SB, sonic brush; MGI, Modified Gingival Index.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 16 of 179
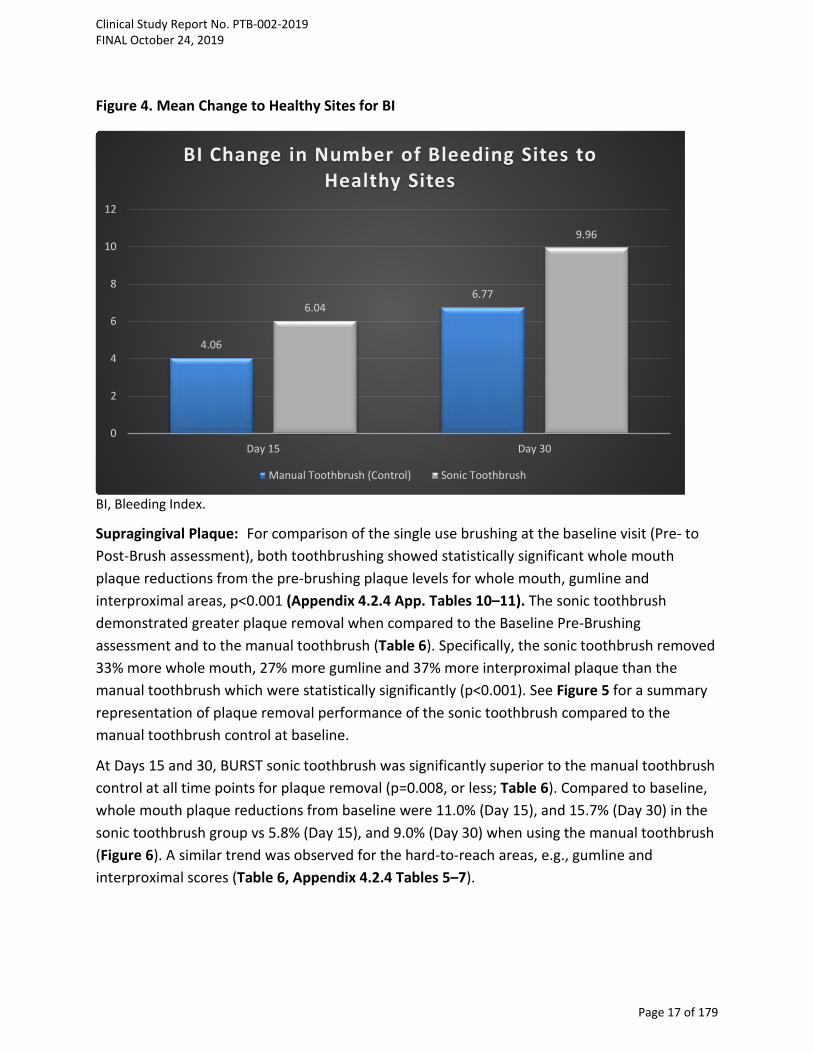
Figure 4. Mean Change to Healthy Sites for BI
BI, Bleeding Index.
Supragingival Plaque: For comparison of the single use brushing at the baseline visit (Pre- to Post-Brush assessment), both toothbrushing showed statistically significant whole mouth plaque reductions from the pre-brushing plaque levels for whole mouth, gumline and interproximal areas, p<0.001 (Appendix 4.2.4 App. Tables 10–11). The sonic toothbrush demonstrated greater plaque removal when compared to the Baseline Pre-Brushing assessment and to the manual toothbrush (Table 6). Specifically, the sonic toothbrush removed 33% more whole mouth, 27% more gumline and 37% more interproximal plaque than the manual toothbrush which were statistically significantly (p<0.001). See Figure 5 for a summary representation of plaque removal performance of the sonic toothbrush compared to the manual toothbrush control at baseline.
At Days 15 and 30, BURST sonic toothbrush was significantly superior to the manual toothbrush control at all time points for plaque removal (p=0.008, or less; Table 6). Compared to baseline, whole mouth plaque reductions from baseline were 11.0% (Day 15), and 15.7% (Day 30) in the sonic toothbrush group vs 5.8% (Day 15), and 9.0% (Day 30) when using the manual toothbrush (Figure 6). A similar trend was observed for the hard-to-reach areas, e.g., gumline and interproximal scores (Table 6, Appendix 4.2.4 Tables 5–7).
4.06
6.776.04
9.96
0
2
4
6
8
10
12
Day 15 Day 30
BI Change in Number of Bleeding Sites to Healthy Sites
Manual Toothbrush (Control) Sonic Toothbrush
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 17 of 179
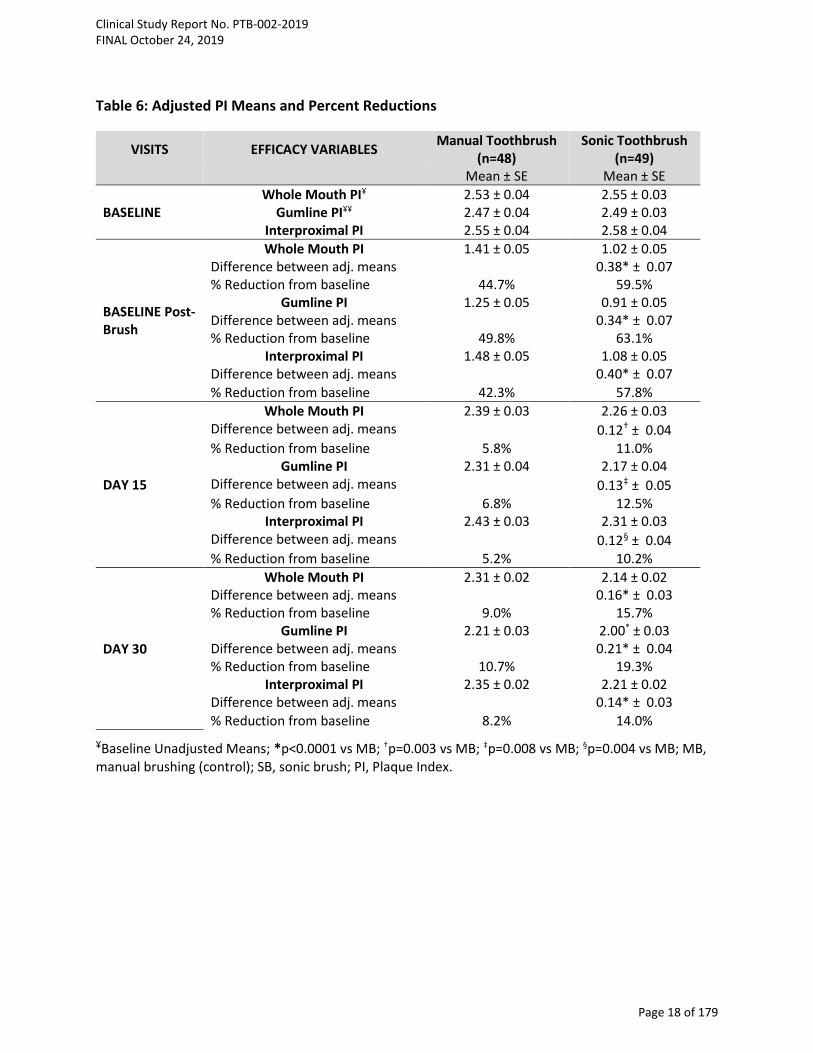
Table 6: Adjusted PI Means and Percent Reductions
VISITS EFFICACY VARIABLES Manual Toothbrush (n=48)
Sonic Toothbrush (n=49)
Mean ± SE Mean ± SE
BASELINE Whole Mouth PI¥ 2.53 ± 0.04 2.55 ± 0.03
Gumline PI¥¥ 2.47 ± 0.04 2.49 ± 0.03 Interproximal PI 2.55 ± 0.04 2.58 ± 0.04
BASELINE Post-Brush
Whole Mouth PI 1.41 ± 0.05 1.02 ± 0.05 Difference between adj. means 0.38* ± 0.07 % Reduction from baseline 44.7% 59.5%
Gumline PI 1.25 ± 0.05 0.91 ± 0.05 Difference between adj. means 0.34* ± 0.07 % Reduction from baseline 49.8% 63.1%
Interproximal PI 1.48 ± 0.05 1.08 ± 0.05 Difference between adj. means 0.40* ± 0.07 % Reduction from baseline 42.3% 57.8%
DAY 15
Whole Mouth PI 2.39 ± 0.03 2.26 ± 0.03 Difference between adj. means 0.12† ± 0.04 % Reduction from baseline 5.8% 11.0%
Gumline PI 2.31 ± 0.04 2.17 ± 0.04 Difference between adj. means 0.13‡ ± 0.05 % Reduction from baseline 6.8% 12.5%
Interproximal PI 2.43 ± 0.03 2.31 ± 0.03 Difference between adj. means 0.12§ ± 0.04 % Reduction from baseline 5.2% 10.2%
DAY 30
Whole Mouth PI 2.31 ± 0.02 2.14 ± 0.02 Difference between adj. means 0.16* ± 0.03 % Reduction from baseline 9.0% 15.7%
Gumline PI 2.21 ± 0.03 2.00* ± 0.03 Difference between adj. means 0.21* ± 0.04 % Reduction from baseline 10.7% 19.3%
Interproximal PI 2.35 ± 0.02 2.21 ± 0.02 Difference between adj. means 0.14* ± 0.03 % Reduction from baseline 8.2% 14.0%
¥Baseline Unadjusted Means; *p<0.0001 vs MB; †p=0.003 vs MB; ‡p=0.008 vs MB; §p=0.004 vs MB; MB, manual brushing (control); SB, sonic brush; PI, Plaque Index.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 18 of 179
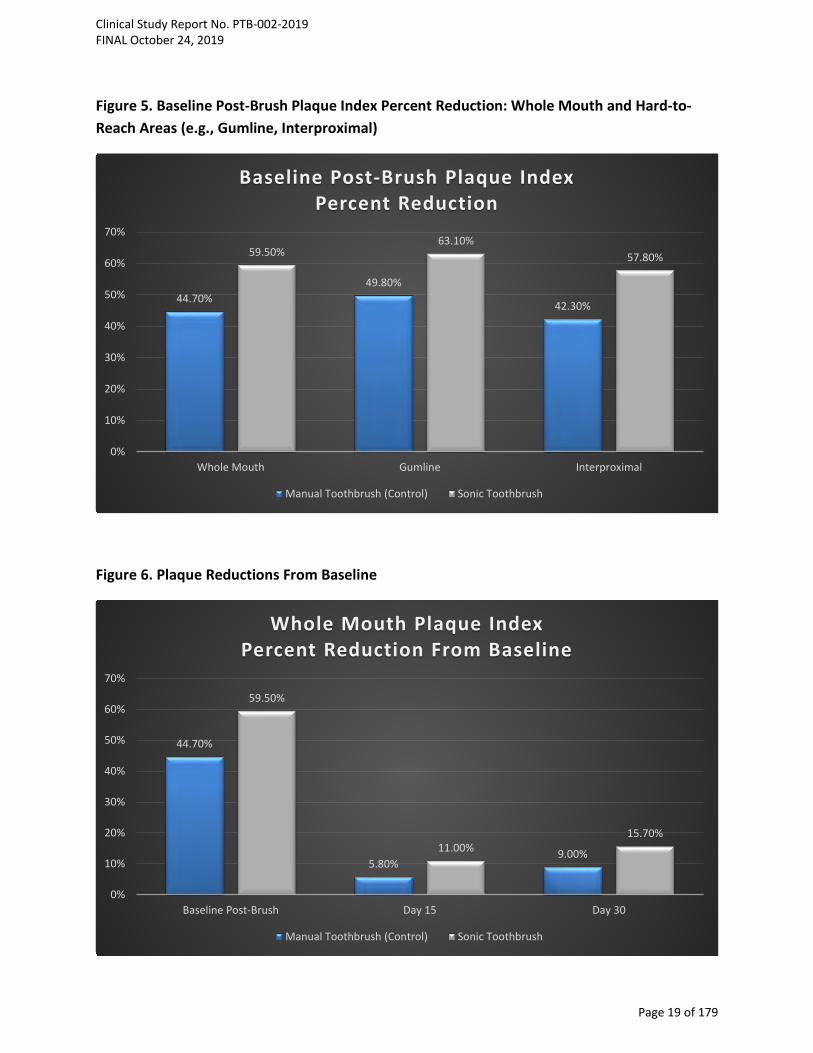
Figure 5. Baseline Post-Brush Plaque Index Percent Reduction: Whole Mouth and Hard-to-Reach Areas (e.g., Gumline, Interproximal)
Figure 6. Plaque Reductions From Baseline
44.70%49.80%
42.30%
59.50%63.10%
57.80%
0%
10%
20%
30%
40%
50%
60%
70%
Whole Mouth Gumline Interproximal
Baseline Post-Brush Plaque Index Percent Reduction
Manual Toothbrush (Control) Sonic Toothbrush
44.70%
5.80%9.00%
59.50%
11.00%15.70%
0%
10%
20%
30%
40%
50%
60%
70%
Baseline Post-Brush Day 15 Day 30
Whole Mouth Plaque Index Percent Reduction From Baseline
Manual Toothbrush (Control) Sonic Toothbrush
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 19 of 179

3.3 DISCUSSION
Adequate and consistent oral hygiene is necessary for maintaining oral health and prevention of caries and periodontal diseases.13 One of the most efficient approaches for controlling dental disease is the mechanical removal of plaque,14 and the manual toothbrush is a frequently used oral hygiene aid for plaque removal. Unfortunately, a manual toothbrush only partially removes plaque,14 and this mechanical routine does not appear to be sufficient since it is has been estimated that 63% of the population in the United States and up to 80% in other regions of the world have some form of gingivitis.15-17 In an effort to improve plaque removal, powered toothbrushes were introduced to consumers as early as the 1940s18 with several studies demonstrating superior plaque removal with use of a powered brush as compared to a standard manual toothbrush.14,19,20
Since its introduction, power toothbrushes have had improvements in advanced designs and offer different modes of action, including rotating-oscillating, side-to-side and sonic brushes. A review conducted by the Cochrane collaboration revealed that power toothbrushes provide superior plaque and gingivitis reduction after short-term use as compared to manual brushing 8; however, another Cochrane review by Deacon et al. (2010) demonstrated that rotating-oscillating brushes had better efficacy than side-to-side bristles.21 Unfortunately, sonic and side-to-side brushes were not identified as a separate mode of action by Deacon et al (2010), instead studies evaluating sonic brushes were grouped with side-to-side toothbrush trials.21 In a recent meta-analysis by de Jager et al (2017), sonic brushes demonstrated a favorable plaque removal effect and comparable gingivitis reduction vs oscillating-rotating toothbrushes; thus, both modes of action (e.g., oscillating-rotating and sonic) demonstrate comparable efficacy and deliver a clinical benefit over manual brushing.22
The BURST sonic toothbrush features 33,000 sonic vibrations per minute, 30 second quadrant paced brushing and three modes: whitening, sensitive and massage. In this 30-day trial, the effectiveness BURST sonic power toothbrush with charcoal-infused bristles on plaque removal and reduction in gingivitis was compared to brushing with an ADA reference standard manual toothbrush. Assessments of gingival health and plaque levels at Days 15 and 30 occurred approximately 8–12 hours after the assigned toothbrush use, which represents the approximate period of time between usual home care procedures. The efficacy of the mechanical plaque removal portion of the sonic toothbrush is highlighted by the difference in plaque levels after a single use at the baseline post-brush assessment. Specifically, the sonic toothbrush provided 33% greater whole mouth plaque removal than the manual brush control after a single use. The same trend in plaque removal was observed in the hard-to-reach areas,
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 20 of 179

gumline and interproximal sites. The results of the single use plaque assessments demonstrate the superior plaque removal performance of the BURST sonic power toothbrush compared with manual brushing and are consistent with previous single-use sonic power toothbrush studies using a similar plaque index.14,18,23 A revealing measure of the efficacy of a toothbrush is the improvement in plaque-induced gingivitis. Results observed in this study reflect the ability of the BURST sonic power toothbrush on removing more plaque vs manual brushing and thereby improved gingival health. After 15 days, the sonic toothbrush surpassed the manual toothbrush by 91% in reduction of whole mouth plaque. For areas of the mouth that consumers have difficulty cleaning (gumline and interproximal), BURST users experienced up to 95% greater improvement in plaque reductions compared to the manual toothbrush. In addition, Day 30 plaque results trended similarly to Day 15 results (75% greater improvement vs manual brushing), The sonic toothbrush group had >1.5x greater plaque removal and 2x more healthy gingival sites compared to control. Further, there was a 95% greater improvement in whole mouth gingivitis mean scores for the sonic toothbrush compared to the manual toothbrush group. The cumulative benefit in plaque reduction that was observed in the sonic power toothbrush group suggests the brushing routine effectively disrupted dental plaque colonies, helping to minimize further accumulation of plaque bacteria and reducing and inhibiting gingival inflammation and bleeding. Similarly, sonic power toothbrushes have been shown to disrupt viable bacteria in plaque, even in areas beyond the reach of toothbrush bristles.24–26 The superiority in plaque removal and gingivitis reduction vs a manual toothbrush are consistent with findings from previous sonic toothbrush studies conducted over 4-weeks,6,23,27-34 including results from a recent a meta-analysis of 18 clinical studies (N=1,870)22 demonstrating greater plaque and gingivitis reductions by a sonic power toothbrush vs a manual toothbrush.
3.4 CONCLUSION In conclusion, the BURST sonic toothbrush demonstrated a superior reduction in plaque as early as the Baseline Post-Brush assessment vs manual brushing. The sonic toothbrush also showed a beneficial improvement in gingival health compared with the manual toothbrush.
• The sonic toothbrush was superior in reducing whole mouth, gumline, and interproximal plaque at Baseline Pre- to Post-Brush, and before brushing at Day 15 and Day 30, when compared to the manual brushing control.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 21 of 179
• Compared to the manual toothbrush control, the sonic toothbrush was superior in reducing gingivitis and bleeding at Days 15 and 30, as well as providing a greater number of healthy gingival sites.
• The results of this study demonstrate the safety of the BURST sonic toothbrush and benefits in providing clinically measurable improvement in plaque removal and gingival health.
In this 30-day study, the sonic toothbrush provided the best results at both Day 15 and the final Day 30 visits for all endpoints measured. The results of this study highlight the benefits of incorporating a power toothbrush into a home care routine in reducing plaque and improving gingival health compared to brushing with a standard manual toothbrush.
3.5 REFERENCES
1. American Dental Association Mouth Healthy™ A-Z Topics. http://www.mouthhealthy.org/en/az-topics/p/plaque. Accessed July 12, 2019.
2. Ebel S, Blättermann H, Weik U, Margraf-Stiksrud J, Deinzer R. High plaque levels after thorough toothbrushing: What impedes efficacy? J Dent Res. 2018;4(2):135-142.
3. Davidovich E, Ccahuana-Vasquez RA, Timm H, Grender J, Cunningham P, Zini A. Randomised clinical study of plaque removal efficacy of a power toothbrush in a paediatric population. International Journal of Paediatric Dentistry. 2017; Nov;27(6):558-567. doi: 10.1111/ipd.12298. Epub 2017 May 11.
4. Klukowska M, Grender JM, Timm H. A single-brushing study to compare plaque removal efficacy of a new power brush to an ADA reference manual toothbrush. Am J Dent. 2012;25:10A–13A.
5. Starke EM, Mwatha A, Ward M, Argosino K, Jenkins W, Milleman JL, Milleman KR. A Comparison of the Effects of a Powered and Manual Toothbrush on Gingivitis and Plaque: A Randomized Parallel Clinical Trial. J Clin Dent. 2019;30(Spec Iss A)A24–29.
6. Delaurenti M, Ward M, Souza S, Jenkins W, Putt MS, Milleman KR, Milleman JL. The Effect of Use of a Sonic Power Toothbrush and a Manual Toothbrush Control on Plaque and Gingivitis. J Clin Dent. 2017 Mar;28(1 Spec No A):A1-6.
7. Sharma NC, Klukowska M, Mielczarek A, Grender JM, Qaqish J. A 4-week clinical comparison of a novel multi-directional power brush to a manual toothbrush in the reduction of gingivitis and plaque. Am J Dent. 2012 Sep;25 Spec No A(A):14A-20A.
8. Yaacob M, Worthington HV, Deacon SA, et al. Powered versus manual toothbrushing for oral health. Cochrane Database Syst Rev. 2014;6:CD002281.
9. Lobene RR, Weatherford T, Ross NM, Lamm RA, Menaker L. A modified gingival index for use in clinical trials. Clin Prev Dent. 1986;8(1):3-6.
10. Saxton CA, van der Ouderaa FJ. The effect of a dentifrice containing zinc citrate and triclosan on developing gingivitis. J Periodontol. 1989;24:75-80.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 22 of 179

11. Turesky S, Gilmore ND, Glickman I. Reduced plaque formation by the chloromethyl analogue of victamine C. J Periodontol. 1970;41(1):41-43.
12. Lobene RR, Soparkar PM, Newman MB. Use of dental floss. Effect on plaque and gingivitis. Clin Prev Dent. 1982;4(1):5-8.
13. Kaur A, Singh RA, Bhola K, Khilji I, Dhawan S, Kochar D. Comparative assessment of the efficacy of two commercially available manual toothbrushes for removal of dental plaque. J Adv Med Dent Scie Res. 2018;6(9):62-65.
14. Re D, Augusti G, Battaglia D, Gianni AB, Augsti D. Is a new sonic toothbrush more effective in plaque removal than a manual toothbrush? Eur J Paediatr Dent. 2015. 16(1):13-18.
15. Albandar JM, Rams TE. Global epidemiology of periodontal diseases: an overview. Periodontol 2000. 2002;29:7-10.
16. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005;83(9):661-669.
17. Brown LJ, Brunelle JA, Kingman A. Periodontal status in the United States, 1988-91: prevalence, extent, and demographic variation. J Dent Res. 1996;75:672-683.
18. Elkerbout TA, Slot DE, Rosema NAM, Van der Weijden GA. How effective is a powered toothbrush as compared to a manual toothbrush? A systematic review and meta-analysis of single brushing exercises. Int J Dent Hygiene. 2019;00:1-10.
19. Terezhalmy GT, Bartizek RD, Biesbrock AR. Relative plaque removal of three toothbrushes in a nine-period crossover study. J Periodontology. 2005;76:2230-2235.
20. Lazarescu D, Boccaneala S, Illiescu A, De Boever JA. Efficacy of plaque removal and learning effect of a powered and a manual toothbrush. J Clinical Periodontology. 2003;30:726-731.
21. Deacon SA, Glenny A-M, Deery C, Robinson PG, Heanue M, Walmsley AD, Shaw WC. Different powered toothbrushes for plaque control and gingival health. Cochrane Database Syst Rev. 2010;12:CD004971.
22. De Jager M, Rmaile A, Darch O, Bikker JW. The effectiveness of manual versus high-frequency, high-amplitude sonic powered toothbrushes for oral health: a meta-analysis. J Clin Dent. 2017;28(Spec Iss A):A13-28.
23. Moritis K, Delaurenti M, Johnson MR, Berg J, Boghosian AA. Comparison of the Sonicare Elite and a manual toothbrush in the evaluation of plaque reduction. Am J Dent. 2002;15(Spec Iss)23B-25.
24. Klonowicz D, Czerwinska M, Sirvent A, Gatignol J-P. A new tooth brushing approach supported by an innovative hybrid toothbrush-compared reduction of dental plaque after a single use versus an oscillating-rotating powered toothbrush. BMC Oral Health. 2018;18:185.
25. Schmidt JC, Zaugg C, Weiger R, Walter C. Brushing without brushing? A review of the efficacy of powered toothbrushes in noncontact biofilm removal. Clin Oral Investig. 2013;17:682–709.
26. Hope CK, Wilson M. Effects of dynamic fluid activity from an electric toothbrush on in vitro oral biofilms. J Clin Periodontol. 2003;30:624–629.
27. Johnson BD, McInnes C. Clinical evaluation of the efficacy and safety of a new sonic toothbrush. J Periodontol. 1994;65:692-697.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 23 of 179
28. Nunn ME, Ruhlman CD, Mallatt PR, Rodriguez SM, Ortbald KM. Plaque reduction over time of an integrated oral hygiene system. Compend Contin Educ Dent. 2004;25:8-14.
29. Holt J. Sturm D, Master A, Jenkins W, Schmitt P, Hefti A. A randomized, parallel-design study to compare the effects of the Sonicare Flexcare and the Oral-B P40 manual toothbrush on plaque and gingivitis. Compend Contin Educ Dent. 2007;28:35-41.
30. DeLaurenti M, Putt MS, Milleman JL, Jenkins W, Wei J, Strate J. Plaque removal by Sonicare and manual toothbrushes in orthodontic subjects. J Dent Res. 2008;87(Spec Iss B):2044 (www.iadr.org).
31. DeLaurenti M, Putt MS, Milleman JL, Milleman K, Ward M, Jenkins W, Souza S, Nelson M. An evaluation of two toothbrushes on plaque and gingivitis. J Dent Res. 2012;91(Spec Iss B):0552 (www.iadr.org).
32. DeLaurenti M, Sourza S, Nelson M, Jenkins W, Argosino K, Ward M, Milleman J, Milleman KR. Investigation of a novel sonic toothbrush on plaque and gingivitis. J Dent Res. 2013;92(Spec Iss A):3748 (www.iadr.org).
33. Ward M, Jenkins W, Argosino K, Souza S, Nelson M, Milleman J, Milleman KR. Assessment of a sonic toothbrush on plaque and gingivitis. J Dent Res. 2013;92(Spec Iss A):3753 (www.iadr.org).
34. Argosino K, Milleman J, Milleman K, Mwatha A, Ward M, Jenkins W, Souza S. An evaluation of power toothbrushing on gingivitis and plaque biofilm. J Dent Res. 2015;94(Spec Iss A):3075 (www.iadr.org).
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 24 of 179
4 APPENDICES
List of Appendices
4.1 Study Information
4.1.1 Protocol and Protocol Amendments
4.1.2 Case Report Forms
4.1.3 Ethics Committees and Subject Information
4.1.4 Investigators and Study Personnel
4.1.5 Sponsor and Investigator Signatures
4.1.6 Randomization Scheme and Codes
4.1.7 Publication Referenced in the Report
4.2 Subject Data Listings
4.2.1 Protocol Deviations
4.2.2 Demographic Data
4.2.3 Individual Efficacy Response Data
4.2.4 Statistical Report
4.2.5 Adverse Event Listings (Each Subject)
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 25 of 179
4.1 Study Information
4.1.1 Protocol and Protocol Amendments
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 26 of 179

Page 1
BURST.USA.inc
Thirty-Day Evaluation of a Sonic Power Toothbrush Versus a Manual Toothbrush on Plaque and Gingivitis Efficacy
Clinical Protocol
Protocol No. PTB-002-2019
FINAL
26 July 2019
CONFIDENTIALITY STATEMENT
The information in this document contains trade secrets and commercial information that are privileged or confidential and may not be disclosed unless such disclosure is required by federal or state law or regulations. In any event, persons to whom the information is disclosed must be informed that the information is privileged or confidential and may not be disclosed by them. These restrictions on disclosure will apply equally to all future information supplied, which is indicated as privileged or confidential.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 27 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
2
STATEMENT OF COMPLIANCE
This trial will be conducted in compliance with the protocol and in accordance with Good Clinical Practice (GCP) as required by the following:
• United States (US) Code of Federal Regulations (CFR) applicable to clinical studies (45 CFR Part 46, 21 CFR Part 50, 21 CFR Part 56, 21 CFR Part 312, and/or 21 CFR Part 812)
• International Conference on Harmonisation Good Clinical Practice E6 R2 (ICH-GCP); U.S. Food and Drug Administration (FDA) March 2018. International E6(R2) Good Clinical Practice: Integrated Addendum to ICH E6(R1) Guidance for Industry, Accessed July 13, 2019
All study personnel will be trained on study procedures and will be knowledgeable in GCP guidelines on protection of subject interests, health and confidentiality.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 28 of 179

Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 29 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
4
CONTENTS Statement of Compliance ................................................................................................................ 2
SIGNATURE PAGE ............................................................................................................................ 3
List of Abbreviations ....................................................................................................................... 7
1 Key Roles ............................................................................................................................... 11
2 Background Information and Scientific Rationale ................................................................ 12
3 Objective ............................................................................................................................... 12
3.1 Endpoints ........................................................................................................................ 12
3.1.1 Safety ...................................................................................................................... 12
3.1.2 Efficacy .................................................................................................................... 13
4 Study Design.......................................................................................................................... 13
5 Study Population ................................................................................................................... 14
5.1 Inclusion Criteria ............................................................................................................ 14
5.2 Exclusion Criteria ............................................................................................................ 15
5.3 Subject Identification, Screening and Enrollment ......................................................... 16
5.4 Treatment Assignment Procedures ............................................................................... 16
5.4.1 Withdrawal ............................................................................................................. 16
5.4.2 Termination of Study .............................................................................................. 17
6 Investigational Product ......................................................................................................... 17
6.1 Study Material Description ............................................................................................ 17
6.2 Packaging, Labeling and Storage .................................................................................... 18
6.3 Dosage, Preparation and Administration of Investigational Product ............................ 19
6.4 Accountability Procedures for the Investigational Product(s) ....................................... 19
6.5 Assessment of Subject Compliance with Investigational Product ................................. 19
6.6 Concomitant Medications/Treatments .......................................................................... 19
7 Study Procedures, Evaluation and Schedule ........................................................................ 20
7.1 Screening/Baseline Exam (Visit 1) ............................................................................... 20
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 30 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
5
7.2 Day 15 (± 2 days) – Midpoint Exams (Visit 2) ................................................................ 20
7.3 Day 30 (± 2 days) – Final Exams (Visit 3) ....................................................................... 21
7.4 Early Termination Visit ................................................................................................... 21
8 Study Procedures/Evaluations .............................................................................................. 21
8.1 Demographics................................................................................................................. 21
8.2 Safety Assessments ........................................................................................................ 21
8.2.1 Oral Examinations.................................................................................................. 21
8.3 Efficacy Assessments .................................................................................................... 22
8.3.1 Gingival Inflammation ........................................................................................... 22
8.3.2 Gingival Bleeding ..................................................................................................... 22
8.3.3 Plaque Index ............................................................................................................ 23
8.4 Examiner Repeatability Exercises ................................................................................... 23
9 Adverse Event Reporting and Documentation ..................................................................... 24
9.1 Adverse Events ............................................................................................................... 24
9.2 Definition of a Serious Adverse Event (SAE) .................................................................. 24
9.3 Unanticipated adverse device effect (UADE) ................................................................. 25
9.4 Recording an Adverse Event .......................................................................................... 25
9.5 Follow-up ........................................................................................................................ 26
9.6 Reporting Adverse Events .............................................................................................. 26
9.7 Reporting Unanticipated Adverse Device Effects .......................................................... 27
10 Statistical Considerations ...................................................................................................... 27
10.1 Sample Size Considerations ........................................................................................ 27
10.2 Safety Review ............................................................................................................. 27
10.3 Demographic and Baseline Characteristics ................................................................ 27
10.4 Efficacy Review ........................................................................................................... 28
10.5 Data Sets to be Analyzed ............................................................................................ 28
11 Data Handling and Record Keeping ...................................................................................... 29
11.1 Study Records Retention ............................................................................................ 29
11.2 Protocol Deviations .................................................................................................... 30
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 31 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
6
12 Ethics ..................................................................................................................................... 30
12.1 Institutional Review Board ......................................................................................... 30
12.2 Ethical Conduct of the Study ...................................................................................... 30
12.3 Subject Information and Consent ............................................................................... 30
12.4 Authorization to Disclose Protected Health Information ........................................... 31
13 MONITORING ........................................................................................................................ 31
14 AMENDMENTS/MODIFICATION OF THIS PROTOCOL ........................................................... 32
15 Table 1. Study Flow Chart ..................................................................................................... 33
16 References ............................................................................................................................ 34
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 32 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
7
LIST OF ABBREVIATIONS
AE Adverse Event/Adverse Experience
ANOVA Analysis of Variance
ANCOVA Analysis of Covariance
BI Gingival Bleeding Index of Saxton and van der Ouderaa
CFR Code of Federal Regulations
CRF Case Report Form
DCF Data Clarification Form
FDA Food and Drug Administration
GCP Good Clinical Practice
ICF Informed Consent Form
ICH International Conference on Harmonisation
IRB Institutional Review Board
MGI Modified Gingival Index
PI Lobene-Soparkar Modification of the Turesky Modification of the Quigley-Hein Plaque Index (PI)
QA Quality Assurance
QC Quality Control
SAE Serious Adverse Event/Serious Adverse Experience
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 33 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
8
PROTOCOL SUMMARY
TITLE:
Thirty-Day Evaluation of a Sonic Power Toothbrush Versus a Manual Toothbrush on Plaque and Gingivitis Efficacy
Protocol Number: Protocol # PTB-002-2019
Population:
Approximately 100 generally healthy male and female subjects will be screened and randomized so that 90 (45 per group) subjects complete this trial.
Number of Sites:
1, this is a single center study
Study Duration:
Each subject will participate in a 30-day clinical trial.
Description of Test Agents:
1) Control group: ADA Standard manual toothbrush with fluoride toothpaste 2) Sonic power toothbrush with fluoride toothpaste
Objective:
The objective of this 30-day, randomized, examiner-blind clinical trial is to assess the efficacy of a sonic power toothbrush on plaque and gingivitis, compared to a manual toothbrush.
Key Inclusion Criteria:
1. Generally healthy males and females at least 18 years of age or older. 2. Volunteers must read, sign and receive a copy of the signed informed consent form. 3. A minimum of 18 natural teeth with scorable facial and lingual surfaces. Teeth that
are grossly carious, orthodontically banded, exhibiting general cervical abrasion and/or enamel abrasion, or third molars will not be include in the tooth count.
4. A gingival index score of ≥ 1.75 and ≤ 2.3 according to the Modified Gingival Index. 5. A plaque index score ≥ 1.95 according to the Lobene-Soparkar Modification of the
Turesky Modification of the Quigley-Hein Plaque Index, following 8 to 12 hours plaque accumulation period.
6. A minimum of 20 bleeding sites based on the Gingival Bleeding Index of Saxton and van der Ouderaa.
Study Design:
This single-center, randomized, controlled, double-blind, 30-day parallel study will include an oral screening examination consisting of assessments in the following order:
• Oral safety will be assessed through soft and hard tissue examination for irritations or other abnormalities;
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 34 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
9
• Gingivitis according to the Modified Gingival Index (MGI); • Gingival bleeding according to the Gingival Bleeding Index of Saxton and van der
Ouderaa (BI); • Supragingival plaque levels, determined according to the Lobene-Soparkar
Modification of the Turesky Modification of the Quigley-Hein Plaque Index (PI). Plaque will be disclosed using a red disclosing solution and each tooth will be scored in six areas (distobuccal, midbuccal and mesiobuccal, distolingual, midlingual and mesiolingual).
Prior to each exam visit, subjects will refrain from oral hygiene for 8 to 12 hours and will not have eaten 30 minutes prior to the visit. Following informed consent procedures and collection of baseline demographics, qualified subjects will receive an oral examination and assessment for MGI, BI and PI per sequence. Subjects will be enrolled into the study with existing mild to moderate gingivitis and there will be no dental prophylaxis performed during the study.
Subjects meeting study entrance criteria will be stratified based on typical toothbrush used (power or manual), and baseline whole mouth mean PI score and randomly assigned to one of two treatment groups:
1) Twice daily brushing with flat trim manual toothbrush and standard anticavity fluoride toothpaste;
2) Twice daily brushing with sonic power toothbrush and standard anticavity toothpaste
Subjects will be provided verbal and written instructions on the use of their assigned oral care brushing. The first product use will be performed at the clinical site under the supervision of study personnel. Subjects assigned to the sonic power brush will brush their teeth for two minutes using the Whitening mode, while those using the manual toothbrush will be instructed to brush in their usual manner. Following the first use of their assigned product, subjects will be examined again for plaque removal. All subjects will maintain a daily diary to document compliance with the use of their assigned products.
Following the Baseline exams, subjects will return at Days 15 and 30 for the same assessments for oral safety, gingival health and plaque. At Day 30, subjects will brush with their assigned product and will be re-examined again for plaque removal.
During the study, subjects will refrain from using any oral care products other than the toothbrush and toothpaste products provided to them and will avoid the use of chewing gums and mints..
Safety:
Safety will be assessed through oral clinical examinations and interviews to determine soft tissue or oral irritation symptoms. Oral soft tissue findings will be tabulated and summarized by treatment group for each exam visit. The number and percentage of subjects
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 35 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
10
experiencing adverse events will be tabulated by treatment. Adverse events will be summarized according to relationship to study material and according to severity.
Efficacy Endpoints:
• Mean change in MGI scores at Day 15 and Day 30: ▪ Whole mouth ▪ Interproximal (mesial & distal)
• Change in mean number of healthy sites (MGI=0, 1) at Day 15 and Day 30 • Mean change in BI scores at Day 15 and Day 30:
▪ Whole mouth ▪ Interproximal (mesial & distal)
• Mean change in number of bleeding sites (BI=1 or2) from Baseline to “0” bleeding sites at Days 15 and 30.
▪ Whole mouth ▪ Interproximal (mesial & distal)
• Mean change in PI scores at Baseline Pre - Post-brushing, Days 15 and 30 for: ▪ Whole mouth PI scores; ▪ Gumline PI scores (marginal); ▪ Interproximal PI scores (mesial and distal).
Statistical Analyses:
A sample size of 90 completed and 45 per group evaluable subjects achieves a 90% power to detect treatment differences at Day 30. This assumes improvements by 0.24 with respect to MGI, and 0.4 with respect to PI, when compared to the negative control, with an effect size (mean/standard deviation) of 0.7. These calculations are based on two-sided tests at the 0.05 significance level.
For each efficacy variable summary statistics using appropriate descriptive statistics (mean, median, minimum, maximum) by treatment group and overall will be provided at each visit.
Post-brushing plaque analysis will be performed for Baseline visit. Analyses will be performed for Day 15 and Day 30 for each efficacy variable, analyses will be performed using the ANCOVA model with treatment as a factor and the corresponding baseline value as a covariate. The comparisons will be made at the 0.05 level, 2-sided. Differences between the means, simultaneous 95% confidence intervals and test results will be presented.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 36 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
11
1 KEY ROLES
Principle Investigator:
Chhaju Ram Goyal, BDS All Sum Research, Ltd. 6635 Kitimat Road, Units 36 & 37 Mississauga, Ontario L5N 6J2 Canada Tel: (905) 812-1099 [email protected]
Others (study coordinator):
Jimmy G. Qaqish, Vice President All Sum Research Center Ltd. 6635 Kitimat Road, Units 36 & 37 Mississauga, Ontario L5N 6J2 Canada Tel: (905) 812-1099 [email protected]
Sponsor: Brittany Stewart Chief Operating Officer BURST.USA.inc 340 S. Lemon Avenue #4658 Walnut, CA 91789 mobile: 310-310-1223 [email protected]
Monitor: Sylvia L. Santos, RDH, MS or Designee SLS Clinical Research Consulting, LLC Phone: 201-572-9223 [email protected]
Study sites: All Sum Research Center Ltd. 6635 Kitimat Road, Units 36 & 37 Mississauga, Ontario L5N 6J2 Canada Tel: (905) 812-1099
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 37 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
12
2 BACKGROUND INFORMATION AND SCIENTIFIC RATIONALE The effective management of dental plaque and gingivitis continues to be a high priority for the dental health of the public. Dental professionals recommend brushing at least twice a day to remove plaque and reduce the risk of tooth decay and gum disease.1 A recent study by Ebel and co-workers2 assessed the impact of brushing time, brushing techniques, and brushing systematics of young adults (18 years old) on efficiency of plaque removal with a standard manual toothbrush. Subjects were asked to clean their teeth to the best of their abilities. They found that participants distributed their brushing time across surfaces unevenly which explained the variance of plaque and bleeding. Brushing technique appeared to be of minor importance. The researchers concluded that the results indicated that establishing systematic interventions or prophylactic programs should emphasize the importance of brushing all surfaces and not neglecting any teeth. However, the high prevalence of oral diseases worldwide suggests that consumers do not achieve sufficient plaque removal with their manual toothbrushing routine. Although dental professionals emphasize the importance of improving brushing habits with patients, research indicates behavior modification is challenging. Clinical studies have shown that improvement in mechanical oral hygiene can be achieved through the use of power toothbrushes.2-8 Power toothbrush innovations are intended not only to optimize plaque removal and improve gingival health but also to encourage better brushing behavior. This single-center, randomized, controlled, examiner-blind, 30-day, parallel study is designed to evaluate the safety and efficacy of a sonic power toothbrush with charcoal infused toothbrush bristles compared to an ADA reference manual soft toothbrush on plaque and gingivitis.
3 OBJECTIVE
The objective of this 30-day, randomized, controlled, examiner-blind, parallel design clinical trial is to assess the safety and efficacy of twice daily use of a marketed sonic power toothbrush (BURST Sonic) on plaque and gingivitis, compared to a manual toothbrush when brushing with a standard fluoride dentifrice.
3.1 Endpoints
3.1.1 Safety
Safety will be assessed through oral clinical examinations and interviews to determine soft tissue or oral irritation symptoms.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 38 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
13
3.1.2 Efficacy
Efficacy endpoints will be:
• Mean change in Modified Gingival Index (MGI) scores at Day 15 and Day 30: ▪ Whole mouth ▪ Interproximal (mesial & distal)
• Change in mean number of healthy sites (MGI=0, 1) at Day 15 and Day 30 • Mean change in Bleeding Index (BI) scores at Day 15 and Day 30:
▪ Whole mouth ▪ Interproximal (mesial & distal)
• Mean change in number of bleeding sites (BI=1 or2) from Baseline to “0” bleeding sites at Days 15 and 30.
▪ Whole mouth ▪ Interproximal (mesial & distal)
• Mean change in Plaque Index (PI) scores at Baseline Pre - Post-brushing, Days 15 and 30 for: ▪ Whole mouth PI scores; ▪ Gumline PI scores (marginal) ▪ Interproximal PI scores (mesial and distal).
4 STUDY DESIGN
This single-center, randomized, controlled, examiner-blind, 30-day parallel study will consist of a Screening/Baseline visit during which potential subjects will read and sign an informed consent form, complete health and dental questionnaires and a receive a clinical oral examination. The oral examination will include assessments in the following order:
• Oral safety will be assessed through soft and hard tissue examination for evidence of irritation or other abnormalities;
• Gingivitis according to the Modified Gingival Index (MGI);9 • Gingival bleeding according to the Gingival Bleeding Index described by Saxton and van
der Ouderaa (BI);10 • Supragingival plaque levels, determined according to the Lobene-Soparkar Modification
of the Turesky Modification of the Quigley-Hein Plaque Index (PI).11, 12
Prior to each exam visit, subjects will refrain from oral hygiene for 8 to 12 hours and will not have eaten 30 minutes prior to the visit. Following informed consent procedures and collection of Baseline demographics, qualified subjects will receive an oral examination and assessment for MGI, BI and PI per sequence.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 39 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
14
Subjects meeting study entrance criteria will be randomly assigned to one of four treatment groups:
1) Control Group: Twice daily brushing with ADA reference manual soft toothbrush and ADA Accepted, 0.243% sodium fluoride Crest® Cavity Protection dentifrice (Procter & Gamble, Cincinnati, OH, USA);
2) Sonic Toothbrush Group: Twice daily brushing with Burst Sonic power toothbrush and ADA Accepted, 0.243% sodium fluoride Crest® Cavity Protection dentifrice (Procter & Gamble, Cincinnati, OH, USA)
Subjects will be provided verbal and written instructions on the use of their assigned toothbrush. The first assigned brushing will be performed at the clinical site under the supervision of study personnel. Following the first use of assigned toothbrush products, subjects will be examined again for plaque. All subjects will maintain a daily diary to document compliance with the use of their assigned products.
Following the Baseline exams, subjects will return at Days 15 and 30 for the same assessments for oral safety, gingival health and plaque.
During the study, subjects will refrain from using any oral care products other than the toothbrush or toothpaste provided to them and will avoid the use of other toothbrushes, toothpaste, mouthwashes, chewing gum, breath film, mints, floss or interdental cleaning aids, or other oral care cleaning aids for the duration of this research study.
5 STUDY POPULATION
Up to 100 generally healthy male and female subjects will be screened so that approximately 90 (45 per group) complete this trial. To participate in this study, all subjects will fulfill the inclusion and exclusion criteria as outlined in sections 5.1 and 5.2.
5.1 Inclusion Criteria
To be eligible for study participation, subjects must meet the following criteria:
1) Be generally healthy males and females at least 18 years of age. 2) Be able to read, sign and receive a copy of the signed informed consent form. 3) Be regular manual toothbrush users. 4) Be willing to refrain from all oral hygiene 8-12 hours prior to each study visit, and
discontinue eating, drinking and smoking 30 minutes prior to each study visit.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 40 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
15
5) Have a minimum of 18 natural teeth with scorable facial and lingual surfaces. Teeth that are grossly carious, orthodontically banded, exhibiting general cervical abrasion and/or enamel abrasion, or third molars will not be include in the tooth count.
6) Present with a gingival index score ≥ 1.75 ≤ 2.3 according to the Modified Gingival Index. 7) Present with a plaque index score > 1.95 according to the Lobene-Soparkar Modification
of the Turesky Modification of the Quigley-Hein Plaque Index, following an 8 to 12-hour plaque accumulation period.
8) Have a minimum of 20 bleeding sites based on the Gingival Bleeding Index of Saxton and van der Ouderaa.
9) Be willing and able to refrain from dental treatment during the course of the study, except on an emergency basis.
5.2 Exclusion Criteria
Subjects presenting with any of the following will not be included in the study:
1) Having a history of adverse effects, oral soft or hard tissue sensitivity, to any ingredient in the test materials.
2) Having self-reported serious medical conditions. 3) Being under treatment for a heart condition requiring use of pacemaker. 4) Having anything that, in the opinion of the investigator, would place the subject at
increased risk or preclude the subject’s full compliance with or completion of the study. 5) Require antibiotic premedication prior to dental procedures. 6) Having had antibiotic, anti-inflammatory, anti-coagulant medication or
chemotherapeutic antiplaque/antigingivitis therapy within 30 days of screening exams. 7) Having participated in any study involving oral care products, concurrently or within the
30 days of screening exams. 8) Unwilling to discontinue use of other oral hygiene products for the duration of the
study. 9) Presence of severe periodontal disease or being actively treated for periodontal disease. 10) Having grossly carious, fully crowned, or extensively restored teeth. 11) Having orthodontic appliances, peri/oral piercings, or removable partial dentures. 12) Having significant oral soft tissue pathology based on a visual examination.
If the subject reports taking medication, a history of allergy, and/or a chronic disease which in the opinion of investigator will not affect the clinical parameter(s) being assessed or the safety of the subject, the subject may be enrolled in the study and the conditions will be noted on the Subject’s source document.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 41 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
16
5.3 Subject Identification, Screening and Enrollment
Subjects will be recruited from the local population utilizing the recruitment materials approved by the IRB. Subject screening, enrollment, product assignments, and dental assessments will be conducted at the clinic site. The investigator will maintain a screening and enrollment log of all subjects who sign an ICF for this study. The log will include unique subject identification numbers/screening numbers (1001-1100) and dates of subject screening, enrollment and completion (or early termination). Once a number has been assigned to a subject, it cannot be reassigned to another subject. For subjects who fail screening, the reason(s) for non-participation will be recorded on the log. The Investigator will also maintain a confidential identification list containing each enrolled subject’s name and corresponding unique subject number, to enable records to be identified.
5.4 Treatment Assignment Procedures
A minimum of 100 qualified subjects will be randomly assigned to one of two treatment groups. Upon qualification, each enrolled subject will be sequentially issued a unique subject randomization number (001-100), which determines the treatment assignments according to a randomization scheme prepared by the Sponsor. Subjects will be randomized to one of two treatment groups:
1) Control Group: Twice daily brushing with ADA reference manual soft toothbrush and Crest® Cavity Protection dentifrice;
2) Sonic Toothbrush Group: Twice daily brushing with Burst Sonic power toothbrush and Crest® Cavity Protection dentifrice.
The Investigator or designee will maintain randomization worksheets documenting the subject assignment to treatment groups.
5.4.1 Withdrawal
Every effort will be made within the bounds of safety and subject choice to have each subject complete the study. A discontinuation occurs when an enrolled subject ceases participation in the study, regardless of the circumstances, prior to completion of the protocol. The reason for a subject discontinuation from the study will be reported in the case report form. The investigators must attempt to determine the primary reason for discontinuation. A study subject will be discontinued from participation in the study if:
• Any clinical adverse event (AE), intercurrent illness, or other medical condition or situation occurs such that continued participation in the study would not be in the best interest of the subject;
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 42 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
17
• The subject meets any exclusion criteria (either newly developed or not previously recognized).
Subjects are free to withdraw from participation in the study at any time upon request. A discontinuation must be immediately reported to the sponsor’s clinical monitor or his/her designated representative if it is due to a serious adverse event. The final evaluation required by the protocol will be performed at the time of study discontinuation.
5.4.2 Termination of Study
This study may be prematurely terminated if, in the opinion of the investigator or the sponsor, there is sufficient reasonable cause. Written notification, documenting the reason for study termination, will be provided to the investigator or sponsor by the terminating party.
Circumstances that may warrant termination include, but are not limited to:
• Determination of unexpected, significant, or unacceptable risk to subjects; • Insufficient adherence to protocol requirements; • Data that are not sufficiently complete and/or evaluable; • Plans to modify, suspend or discontinue the development of the experimental test
article.
If the study is prematurely terminated or suspended, the sponsor will promptly inform the investigators/institutions, of the termination or suspension and the reason(s) for the termination or suspension. The IRB will also be informed promptly and provided the reason(s) for the termination or suspension by the investigator/institution.
6 INVESTIGATIONAL PRODUCT
6.1 Study Material Description
Manual Toothbrush Control: Manual toothbrush
Trade name 47 Tuft Soft Flat Trim Manual Toothbrush Dosage form Brush twice daily Packaging Single packaging
Power Toothbrush: Sonic Rechargeable Power Toothbrush
Trade name BURST Sonic Toothbrush Manufacturer BURST.USA.inc Dosage form Brush twice daily
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 43 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
18
Packaging Single packaging
Ancillary supplies include a single tube of Crest® Cavity Protection dentifrice (0.243% sodium fluoride, Procter & Gamble, Cincinnati, OH, USA), at least 4.6 oz. tube.
6.2 Packaging, Labeling and Storage
All products must be stored by the clinical site at room temperature. Manual toothbrushes, Burst Sonic Toothbrush and Crest® Cavity Protection toothpaste will be supplied in the original marketed packages with no overwrap.
Each subject will receive a carrying bag that will contain the label noting the relevant randomization number.
The manual toothbrush control group carrying bag will have the following label:
Protocol: PTB-001-2019 Subject Randomization#:
INSTRUCTIONS FOR USE:
1) Wet your toothbrush and dispense a full ribbon of toothpaste (Crest® Regular) onto the brush head.
2) Brush in your usual manner with your assigned toothbrush. 3) Rinse with tap water.
Warnings: Keep all test materials out of reach of children under 12 years of age. For Investigational Use Only – Not for Sale If you have questions, contact the AllSum Research Emergency number: 416-735-2480
The Sonic Toothbrush group carrying bag will have the following label:
Protocol: PTB-001-2019 Subject Randomization#: 1) Wet the toothbrush bristles and apply the provided toothpaste. 2) Place the brush head in your mouth before turning on your power brush and keep
your mouth closed during brushing, otherwise toothpaste may splatter. 3) Press the power button once to turn brush on in the first cleaning mode 4) Follow the detailed directions provided with your daily diary 5) BRUSH A TOTAL OF 2 MINUTES! 6) Thoroughly rinse your mouth out with water. Do not swallow toothpaste while
brushing. 7) Rinse brush head after use.
Warnings: Keep all test materials out of reach of children under 12 years of age. For Investigational Use Only – Not for Sale
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 44 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
19
If you have questions, contact the AllSum Research Emergency number: 416-735-2480
6.3 Dosage, Preparation and Administration of Investigational Product
At Screening/Baseline visit, all subjects will receive regular fluoride toothpaste and their assigned toothbrush. Subjects will be instructed to dispense toothpaste onto their assigned toothbrush and brush their teeth twice daily as detailed in their instructions attached to their daily diary.
6.4 Accountability Procedures for the Investigational Product(s)
Burst Oral Care will provide the investigator with sufficient amounts of the study test materials. The investigator must ensure that deliveries of investigational product from the sponsor are received by a responsible person, that all receipts are recorded in writing and that the product is stored in a secure area under recommended storage conditions. It is also the responsibility of the investigator to ensure that the integrity of packaged study product not be jeopardized prior to dispensing. The investigator will dispense the test material only to subjects included in this study following the procedures specified in the study protocol. Each subject will be administered only the test material carrying his/her randomization number.
All dispensing will be documented. The investigator is responsible for ensuring all full, partially full, and empty test material containers are returned to Burst Oral Care. The investigator must maintain accurate and adequate records including dates of receipt and return of test material shipments, and quantities received/returned from/to Burst Oral Care as well as, dates and amounts dispensed to the study subjects.
6.5 Assessment of Subject Compliance with Investigational Product
Compliance will be assessed at the Days 15 and 30 visits through review of the subjects’ daily diaries. Subjects will be required to maintain a daily diary and to record the time of completion of their assigned morning and evening toothbrushing.
6.6 Concomitant Medications/Treatments
Any medication the subject takes during the study is considered concomitant medication. All concomitant medications and non-drug therapy (e.g. tooth extraction, endodontic treatment, etc.) must be recorded in the subject’s medical source document.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 45 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
20
7 STUDY PROCEDURES, EVALUATION AND SCHEDULE
The schedule of observations and assessments is provided in Sec. 15, Table 1, Study Flow Chart.
7.1 Screening/Baseline Exam (Visit 1)
Prior to randomization to treatment groups, the following procedures will be performed:
• Informed consent form, medical and dental history. • Inclusion/Exclusion Criteria checklist. • Clinical exams:
▪ Oral soft and hard tissue evaluation for safety assessment; ▪ Modified Gingival Index (MGI); ▪ Bleeding Index (BI); ▪ Lobene-Soparkar Modification of the Turesky Modification of the Quigley-Hein
Plaque Index (PI); ▪ Identify subjects with qualifying levels of gingivitis and plaque: MGI ≥ 1.75 and ≤
2.3, PI ≥ 1.95.
If subject meets entry criteria, the following procedures will be performed:
• Randomization to test groups. • Supervise initial use of assigned test products. • Dispense assigned test materials. • Study staff review and dispense daily diary and home use written instructions. • Post-Treatment Plaque Assessment (PI.) • Appoint subjects for next visit.
7.2 Day 15 (± 2 days) – Midpoint Exams (Visit 2)
• Query to update medical and oral health and record adverse events and concomitant medications.
• Assess compliance with study instructions and use of test materials. • Oral soft and hard tissue examination for safety. • Clinical exams:
▪ Oral soft and hard tissue evaluation for safety assessment; ▪ Modified Gingival Index (MGI); ▪ Bleeding Index (BI); ▪ Lobene-Soparkar Modification of the Turesky Modification of the Quigley-Hein
Plaque Index (PI);
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 46 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
21
• Appoint subjects for next visit.
7.3 Day 30 (± 2 days) – Final Exams (Visit 3)
• Query to update medical and oral health and record adverse events and concomitant medications.
• Assess compliance with study instructions and use of test materials. • Oral soft and hard tissue examination for safety. • Clinical exams:
▪ Oral soft and hard tissue evaluation for safety assessment; ▪ Modified Gingival Index (MGI); ▪ Bleeding Index (BI); ▪ Lobene-Soparkar Modification of the Turesky Modification of the Quigley-Hein
Plaque Index (PI). • Discharge subject and provide final instructions for follow-up of ongoing adverse
events, as applicable.
During the study, subjects will follow their usual dietary habits, but will be instructed to refrain from using any oral care products other than the test materials provided to them.
7.4 Early Termination Visit
If a subject discontinues from the study for any reason prior to the final visit, the following procedures should be conducted:
• Record adverse events and concomitant medications; • Oral soft and hard tissue examination; • Schedule follow-up visit for any ongoing adverse events.
8 STUDY PROCEDURES/EVALUATIONS 8.1 Demographics
Demographic information will be collected at the Screening/Baseline Visit and will include the subject’s race, gender, age and tobacco use.
8.2 Safety Assessments
8.2.1 Oral Examinations
An oral examination will be conducted at all visits to monitor the effect of the test articles on the soft and hard tissues. Lips, buccal, labial and sublingual mucosae, tongue, hard and soft
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 47 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
22
palate, uvula and oropharynx, and teeth will be examined for signs of reddening/inflammation, ulceration, white patches and desquamation/ sloughing of mucosal tissues and findings will be recorded on the Oral Exam CRF. Changes from Baseline will be recorded and deviations from normal will be recorded.
Clinically significant findings will be recorded as adverse events and an assessment will be made regarding relationship to test materials.
8.3 Efficacy Assessments
Clinical efficacy assessments will be performed by a single examiner at Baseline, Days 15 and 30 in the following sequence: MGI, BI and PI.
8.3.1 Gingival Inflammation
Gingival inflammation will be assessed at Baseline, Days 15 and 30, according to the Modified Gingival Index (MGI),9 and will be scored on buccal and lingual marginal gingivae and interdental papillae (four gingival areas: buccal, mesiobuccal, lingual and mesiolingual) of all scorable teeth using a scale of 0 – 4 as noted below:
0 = Normal (absence of inflammation). 1 = Mild inflammation (slight change in color, little change in texture) of any portion of
the entire gingival unit. 2 = Mild inflammation of the entire gingival unit. 3 = Moderate inflammation (moderate glazing, redness, edema, and/or hypertrophy) of
the gingival unit. 4 = Severe inflammation (marked redness and edema/hypertrophy, spontaneous
bleeding, or ulceration) of the gingival unit.
Whole mouth MGI scores will be calculated by summing all scores and dividing by the number of scorable sites examined.
8.3.2 Gingival Bleeding
Gingival bleeding tendency will be assessed according to the Bleeding Index (BI) described by Saxton and van der Ouderaa.10 The gingiva will be lightly air-dried and a periodontal probe with a 0.5 mm diameter tip will be inserted into the gingival crevice to a depth of approximately 1 mm. The probe will be moved gently around the tooth at an angle of approximately 60 degrees to the long axis of the tooth, stroking the inner surface of the sulcular epithelium. Each of four gingival areas (distobuccal, midbuccal, mesiolingual, and midlingual) of the scorable teeth will be probed in a likewise manner, waiting approximately 30 seconds before recording the number of gingival units which bleed, according to the following scale:
0 = absence of bleeding after 30 seconds;
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 48 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
23
1 = bleeding observed after 30 seconds; and 2 = immediate bleeding observed.
8.3.3 Plaque Index
Supragingival dental plaque will be assessed according to the Turesky Modification of the Quigley-Hein Plaque Index as further modified by Lobene and Soparkar (PI).11,12 Plaque will be disclosed using a red disclosing solution and each tooth will be scored in six areas (distobuccal, midbuccal and mesiobuccal, distolingual, midlingual and mesiolingual), according to the criteria noted below:
0 = No plaque. 1 = Separate flecks or discontinuous band of plaque at the gingival (cervical) margin. 2 = Thin (up to 1 mm), continuous band of plaque at the gingival margin. 3 = Band of plaque wider than 1 mm but less than 1/3 of tooth surface area. 4 = Plaque covering 1/3 or more, but less than 2/3 of tooth surface area. 5 = Plaque covering 2/3 or more of tooth surface area.
At the Baseline visit only, subjects will brush with their assigned toothbrush at the clinical test site and will be re-disclosed for a second plaque assessment (post-treatment).
A whole mouth plaque index will be calculated for each subject by adding all the individual scores and dividing this sum by the number of measurements. To understand the plaque removal efficacy of each toothbrush in hard to reach areas, separate subsets of the plaque index will be calculated for gingival margin (gumline) and the interproximal surfaces. Gumline PI scores will calculated by summing the number of gingival margin (buccal and lingual) scores and dividing by the number of measurements. Interproximal PI scores (mesial and distal) will be calculated by summing the number of interproximal site scores (distobuccal, mesiobuccal, distolingual and mesiolingual) and dividing by the number of measurements.
8.4 Examiner Repeatability Exercises
A single trained dental examiner will perform the oral examinations and MGI assessments. A second examiner will assess the BI and PI. Prior to Baseline exams, at least 10 subjects will be assessed for gingival inflammation and plaque levels, according to the MGI and PI with at least 10 minutes between repeat examinations. Repeatability will be evaluated through the demonstration of at least 80% frequency of agreement of assessments. Re-training and/or recalibration (followed by a repeat of the exercise) will be performed if the evaluated level of reliability is judged to be low.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 49 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
24
NOTE: Repeatability exercises will not be needed if the examiner has used MGI and PI in a clinical trial within two months prior to the start of this study.
9 ADVERSE EVENT REPORTING AND DOCUMENTATION
Adverse events will be determined by visual examination of the oral cavity by the dental examiner. In addition, clinical research center personnel will ask subjects about the occurrence of any adverse events during their participation in this study. All observed or volunteered adverse events, regardless of treatment group or suspected causal relationship to study product, will be recorded on the adverse event page(s) of the case report form.
9.1 Adverse Events
An adverse event (AE) is any untoward medical occurrence in a clinical investigation of a patient administered an investigational product and that does not necessarily have a causal relationship with the treatment. An AE is therefore any unfavorable and unintended sign (including an abnormal laboratory finding), symptom or disease temporally associated with the administration of an investigational product, whether or not related to that investigational product. An unexpected AE is one of a type not identified in nature, severity, or frequency in the investigational product safety summary or of greater severity or frequency than expected based on the information in the investigational product safety summary.
The Investigator will probe, via discussion with the subject, for the occurrence of AEs during each subject visit and record the information in the site’s source documents. Adverse events will be recorded in the patient CRF. Adverse events will be described by duration (start and stop dates and times), severity, outcome, treatment and relation to study drug, or if unrelated, the cause.
Pre-existing conditions will not be regarded as AEs if the condition follows a normal course Of recovery, unless it worsens after exposure to the investigational product.
9.2 Definition of a Serious Adverse Event (SAE)
The Investigator or other study personnel must immediately (within 24 hours) inform the Sponsor of all Serious Adverse Events (SAEs) that occur in study subjects.
An SAE is any untoward medical occurrence that at any dose:
• Results in death. • Is life-threatening. • Requires hospitalization, or prolongation of existing hospitalization.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 50 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
25
• Results in persistent or significant disability/incapacity. • Is a congenital anomaly or birth defect.
Important medical event/experience that may not result in death, be life-threatening, or require hospitalization may be considered a serious adverse event when, based upon appropriate medical judgment, may jeopardize the subject and may require medical or surgical intervention to prevent one of the outcomes listed above.
9.3 Unanticipated adverse device effect (UADE)
An unanticipated adverse device effect is any serious adverse effect on health or safety or any life-threatening problem or death caused by, or associated with, a device, if that effect problem, or death was not previously identified in nature, severity, or degree of incidence in the investigational plan, or any other unanticipated serious problem associated with a device that relates to the rights, safety, or welfare of subjects.
9.4 Recording an Adverse Event
All serious adverse events will be recorded and reported immediately to the Study Sponsor. An AE shall be documented when a subject reports an untoward event or when subjects are asked directly about concurrent illnesses and concomitant medication or from answers on subject-completed diary forms. When an AE is discovered or reported, the PI or designee shall complete the AE/SAE Case Report Form. The Principal Investigator shall review all AEs/SAEs and determine the severity, relationship (of the AE/SAE to the test article/investigational product), and outcome. The PI also will determine whether the subject will remain in the study.
Severity, relationship and outcome will be defined as follows:
Severity Description
Mild Awareness of signs or symptoms, but easily tolerated.
Moderate Discomfort to a degree that the AE/SAE causes interference with normal daily life activities and/or requires medication.
Severe Incapacity with regard to work or usual daily life activities. Requires medical attention/intervention.
Relationship Description
Unrelated Clearly evident relationship to other etiologies such as concomitant medications or conditions or subject’s known clinical state.
Possible Uncertain association. Other etiologies are also possible.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 51 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
26
Probable Causal relationship cannot be ruled out.
Definite AE/SAE with a clear-cut temporal association
Outcome Description
Not recovered/Not resolved
AE/SAE had not resolved by end of study. (Does not mean AE/SAE was not followed until resolution.)
Resolved without sequelae
AE/SAE completely resolved by end of study (or ongoing yet unrelated to study, therefore resolved for purposes of study).
Resolved with sequelae
AE/SAE resolved by end of study, but aftereffect or disease or injury is present. e.g. a stroke that resulted in partial paralysis; the stroke resolved, but residual paralysis.
Death
9.5 Follow-up
Study-related adverse events will be monitored to resolution by the Investigator for at least 30 days following study completion or discontinuing use of the investigational product.
Serious Adverse Events/Experiences will be followed to resolution to the extent possible (e.g., medical attention by subject’s primary care physician).
9.6 Reporting Adverse Events
The Investigator will report all serious adverse events immediately to the Sponsor monitor, Sylvia L. Santos, RDH, MS at 201-572-9223, and will complete a Serious Adverse Event Form within the following timelines:
• All deaths and immediately life-threatening events, whether related or unrelated, will be recorded on the Serious Adverse Event Form and sent by email within 24 hours of site awareness to the attention of Sylvia L. Santos at [email protected].
• Serious adverse events other than death and immediately life-threatening events, regardless of relationship, will be reported by email within 72 hours of site awareness to the attention of Sylvia L. Santos at [email protected].
The Sponsor’s representative or monitor will be notified within the time frame specified above, after any adverse event has been reported to the Investigator or Investigator’s staff.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 52 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
27
9.7 Reporting Unanticipated Adverse Device Effects
Investigators are required to submit a report of a UADE to the Sponsor and the reviewing IRB as soon as possible, but in no event later than 10 working days after the Investigator first learns of the event.
Sponsors must immediately conduct an evaluation of a UADE and must report the results of the evaluation to FDA, all reviewing IRBs, and participating Investigators within 10 working days after the Sponsor first receives notice of the effect.
10 STATISTICAL CONSIDERATIONS
Data will be manually recorded on Case Report Forms (CRFs). All Sum Research will be responsible for data entry and statistical analysis of the data will be performed by Reinhard Schuller Consulting.
10.1 Sample Size Considerations
It is expected that the active treatments improvement will exceed that of the negative control by at least 25% at Days 15 and 30. This translates into active treatments being superior by 0.24 with respect to MGI, and 0.4 with respect to PI when compared to the negative control at each post baseline assessment. A sample size of 90 completed and 45 per group evaluable subjects achieves a 90% power to detect treatment differences at Day 30. This assumes improvements by 0.24 with respect to MGI, and 0.4 with respect to PI, when compared to the negative control, with an effect size (mean/standard deviation) of 0.7. These calculations are based on two-sided tests at the 0.05 significance level.
10.2 Safety Review
Oral soft tissue findings will be tabulated and summarized by treatment group for each exam visit. The number and percentage of subjects experiencing adverse events will be tabulated by treatment. Adverse events will be summarized according to relationship to study material and according to severity.
10.3 Demographic and Baseline Characteristics
Demographic and Baseline characteristics will be summarized for age, gender, race, tobacco use, mean MGI, BI and PI, and mean number of healthy gingival sites (MGI = 0, 1). Data will be summarized using appropriate descriptive statistics (mean, median, minimum, maximum) by treatment group and overall. Categorical demographic and baseline data will be evaluated using Fisher’s Exactness Test and continuous demographic and baseline data will be evaluated
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 53 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
28
using ANOVA. All tests will be two-sided and conducted at the 0.05 significance level. No adjustments for multiple comparisons or multiple testing will be made.
10.4 Efficacy Review
Post-treatment efficacy endpoints will be: • Mean change in MGI scores at Days 15 and 30:
▪ Whole mouth ▪ Interproximal (mesial & distal)
• Change in mean number of healthy sites (MGI=0, 1) at Days 15 and 30 • Mean change in BI scores at Day 15 and 30:
▪ Whole mouth ▪ Interproximal (mesial & distal)
• Mean change in number of bleeding sites (BI=1 or2) from Baseline to “0” bleeding sites at Days 15 and 30.
▪ Whole mouth ▪ Interproximal (mesial & distal)
• Mean change in PI scores at Baseline Pre - Post-brushing, Days 15 and 30 for: ▪ Whole mouth PI scores; ▪ Gumline PI scores (marginal);
Interproximal PI scores (mesial and distal). For each efficacy variable summary statistics using appropriate descriptive statistics (mean, median, minimum, maximum) by treatment group and overall will be provided at each visit.
Analyses will be performed at Days 15 and 30 for each efficacy variable, analyses will be performed using the ANCOVA model with treatment as a factor and the corresponding baseline value as a covariate. The comparisons will be made at the 0.05 level, 2-sided. Tables comparing treatment groups will provide differences in the least squares mean, the standard error of the differences, the confidence interval for the difference, and the p-value. At Days 15 and 30 post ANCOVA pairwise comparisons between each of the three active treatments and the negative control will be made using a two-sided Dunnett’s test, which controls the error rate for the simultaneous comparisons.13 Differences between the means, simultaneous 95% confidence intervals and test results will be presented.
10.5 Data Sets to be Analyzed
Data analysis sets will include evaluable subjects, defined as subjects who do not have major protocol violations. Data for safety analysis will include all subjects who received treatment.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 54 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
29
11 DATA HANDLING AND RECORD KEEPING
The investigator is responsible to ensure the accuracy, completeness, legibility, and timeliness of the data reported. All source documents should be completed in a neat, legible manner to ensure accurate interpretation of data. Dark ink is required to ensure clarity of reproduced copies. When making changes or corrections, cross out the original entry with a single line, and initial and date the change. DO NOT ERASE, OVERWRITE, OR USE CORRECTION FLUID OR TAPE ON THE ORIGINAL.
The investigator will prepare and maintain adequate and accurate source documents designed to record all observations and other pertinent data for each subject participating in the study. Data captured in source documents includes subject information, original records of clinical findings, observations, medical histories, prior and concomitant medication records, inclusion/exclusion eligibility checklist, records of subject visits and phone calls, progress notes, subjects’ diaries or evaluation checklists, test product dispensing and accountability records
A Case Report Form (CRF) will be completed for each subject enrolled in the study and will include documenting subject demographics and subject’s study completion status. All information recorded on the CRFs for this study must be consistent with the subject’s source documentation records. The Investigator or designee must review all entries for completeness and correctness.
The Investigator or designee agrees to make all CRFs and source documents available to the Sponsor’s Study Monitor for full inspection. After resolution of the monitor’s queries, a copy of the final CRF will be placed in the investigator’s study file and the original will be taken by the site monitor and provided to the Sponsor.
The sponsor will review the CRFs and additional source documents for completeness and adherence to the protocol.
11.1 Study Records Retention
Study documents should be retained for a minimum of 2 years after the last approval of a marketing application in an ICH region and until there are no pending or contemplated marketing applications in an ICH region or until at least 2 years have elapsed since the formal discontinuation of clinical development of the investigational product. These documents should be retained for a longer period, however, if required by local regulations. No records will be destroyed without the written consent of the Sponsor, if applicable. It is the responsibility of the sponsor to inform the investigator when these documents no longer need to be retained.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 55 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
30
11.2 Protocol Deviations
A protocol deviation is any noncompliance with the clinical trial protocol, Good Clinical Practice (GCP) requirements. The noncompliance may be either on the part of the subject, the investigator, or the study site staff. As a result of deviations, corrective actions are to be developed by the site and implemented promptly.
It is the responsibility of the site to use continuous vigilance to identify and report deviations within 5 working days of identification of the protocol deviation, or within 5 working days of the scheduled protocol-required activity. All deviations must be promptly reported to the Sponsor and must be addressed in study subject source documents. In addition, protocol deviations must be sent to the local IRB per their guidelines. The site PI/study staff are responsible for knowing and adhering to their IRB requirements.
12 ETHICS
12.1 Institutional Review Board
This study will be reviewed by U.S. Investigational Review Board which is an appropriately constituted Institutional Review Board (IRB) as outlined in 21 CFR Part 56. The IRB will review the protocol, any amendments, the informed consent form (ICF), subject instructions, safety information, Investigator’s curriculum vitae (CV) and advertisements.
Approval by the Board must be obtained prior to the initiation of the study.
12.2 Ethical Conduct of the Study
This study will be conducted in accordance with 21 Code of Federal Regulations (CFR) Parts 50 and 56. The study will be conducted in accordance with the Principles of Good Clinical Practice.
Burst Oral Care is responsible for the ongoing safety evaluation of the investigational products and will promptly notify participating Investigators and regulatory authorities of findings that could adversely affect the safety of subjects, impact the conduct of the study, or alter the IRB’s approval to continue the study. Burst Oral Care will promptly report all adverse reactions related to the test articles that are both serious and unexpected to the appropriate regulatory authorities and to all Investigators and IRBs currently involved in studies of this test article.
12.3 Subject Information and Consent
Subject consent will be obtained prior to participation in the study as required by the regulatory guidelines (21 CFR Part 50). Subjects will be given ample opportunity to read the consent form and have all questions regarding study participation answered prior to signing the consent
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 56 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
31
form. Each subject will be provided with a signed copy of the ICF to retain for his or her records. The original signed ICF will be retained on file at the study center.
12.4 Authorization to Disclose Protected Health Information
Subjects will be informed of the following information: The purpose of the protected health information (PHI) being collected, the possibility the PHI may be re-disclosed, the duration of the authorization, the right to revoke the authorization, and the right to refuse signature and limit access to PHI during and following the conduct of the trial. As applicable, written authorization to disclose PHI will be incorporated into the informed consent process and will be obtained prior to the subject entering the study. Each subject will be provided with a signed copy of the authorization and the original will be retained on file at the study center.
Subject confidentiality is strictly held in trust by the participating investigators, their staff, and the sponsor(s) and their agents. This confidentiality is extended to cover testing of biological samples and genetic tests in addition to the clinical information relating to participating subjects.
The study protocol, documentation, data, and all other information generated will be held in strict confidence. No information concerning the study or the data will be released to any unauthorized third party without prior written approval of the sponsor.
The study monitor or other authorized representatives of the sponsor may inspect all documents and records required to be maintained by the investigator, including but not limited to, medical records (office, clinic, or hospital) and pharmacy records for the subjects in this study. The clinical study site will permit access to such records.
13 MONITORING
A Sponsor representative may meet with the Investigator and his/her staff prior to the entrance of the first subject to review the procedures to be followed in conducting the study. After the enrollment of the first subject, the Investigator will permit the Sponsor to monitor the progress of the trial on site periodically. The Investigator will make available the source documents as well as the subjects’ records and signed consent forms.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 57 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
32
14 AMENDMENTS/MODIFICATION OF THIS PROTOCOL
No amendment to the protocol will be permitted without approval from the study Sponsor, Investigator, and IRB. Such changes will be documented in writing. Approval by the IRB must be obtained prior to initiation of the amendment.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 58 of 179

Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
33
15 TABLE 1. STUDY FLOW CHART
Procedures: Visit 1 Screening/Baseline
Visit 2 Day 15 ± 2 days
Visit 3 Day 30 ± 2 days
Informed Consent X Medical/Dental History X Record Concomitant Medications X X X Update Medical/Dental History X X Query Subjects and record Adverse Events X X
Review Inclusion and Exclusion Criteria X Clinical Exams:
Intraoral Exam X X X MGI, BI and PI X X X Post-Brushing PI X
Randomization X Dispense toothpaste & toothbrush (supervised use) X
Schedule appointment for next visit X X AE's/Con Meds review X X Test Article and Diary Review/Return X X Study Conclusion and Exit X
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 59 of 179
Protocol #: PTB-002-2019 CONFIDENTIAL FINAL 26 July 2019
34
16 REFERENCES
1. American Dental Association Mouth Healthy™ A-Z Topics. http://www.mouthhealthy.org/en/az-topics/p/plaque. Accessed July 12, 2019
2. Ebel S, Blättermann H, Weik U, Margraf-Stiksrud J and Deinzer R. High plaque levels after thorough toothbrushing: What impedes efficacy? J Dent Res. 2018;4(2):135-142.
3. Davidovich E, Ccahuana-Vasquez RA, Timm H, Grender J, Cunningham P, Zini A. Randomised clinical study of plaque removal efficacy of a power toothbrush in a paediatric population. International Journal of Paediatric Dentistry. 2017; Nov;27(6):558-567. doi: 10.1111/ipd.12298. Epub 2017 May 11.
4. Klukowska M, Grender JM, Timm H. A single‐brushing study to compare plaque removal efficacy of a new power brush to an ADA reference manual toothbrush. Am J Dent 2012; 25: 10A– 13A.
5. Starke EM, Mwatha A, Ward M, Argosino K, Jenkins W, Milleman JL, Milleman KR. A Comparison of the Effects of a Powered and Manual Toothbrush on Gingivitis and Plaque: A Randomized Parallel Clinical Trial. J Clin Dent 2019;30(Spec Iss A)A24–29.
6. Delaurenti M, Ward M, Souza S, Jenkins W, Putt MS, Milleman KR, Milleman JL. The Effect of Use of a Sonic Power Toothbrush and a Manual Toothbrush Control on Plaque and Gingivitis. J Clin Dent. 2017 Mar;28(1 Spec No A):A1-6.
7. Sharma NC, Klukowska M, Mielczarek A, Grender JM, Qaqish J. A 4-week clinical comparison of a novel multi-directional power brush to a manual toothbrush in the reduction of gingivitis and plaque. Am J Dent. 2012 Sep;25 Spec No A(A):14A-20A
8. Yaacob M, Worthington HV, Deacon SA, et al. Powered versus manual toothbrushing for oral health. Cochrane Database Syst Rev 2014; 6: CD002281.
9. Lobene RR, Weatherford T, Ross NM, Lamm RA, Menaker L. A modified gingival index for use in clinical trials. Clin Prev Dent. 1986;8(1):3-6.
10. Saxton CA, van der Ouderaa FJ. The effect of a dentifrice containing zinc citrate and triclosan on developing gingivitis. J Periodontol 1989;24:75-80.
11. Turesky S, Gilmore ND, Glickman I. Reduced plaque formation by the chloromethyl analogue of victamine C. J Periodontol. 1970;41(1):41-43.
12. Lobene RR, Soparkar PM, Newman MB. Use of dental floss. Effect on plaque and gingivitis. Clin Prev Dent. 1982;4(1):5-8.
13. Westfall PH, Tobias RD, Rom D, Wolfinger RD, Hochberg Y. Multiple Comparisons and Multiple Testing Using the SAS System. SAS Institute Inc. Cary NC, 1999.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 60 of 179

4.1.2 Case Report Forms
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 61 of 179

CASE REPORT FORMS
Study No.
PTB-002-2019
Screening Number 1
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 62 of 179

SUBJECT DEMOGRAPHICS
AGE
Gender ☐ Male ☐ Female
RACE (Select One):
☐ American Indian/Alaskan Native ☐ Native Hawaiian or other Pacific Islander
☐ Black or African American ☐ Asian
☐ White ☐ Other, please specify:
Ethnicity (Select One):
☐ Hispanic or Latino ☐ Non-Hispanic or Latino
Tobacco Use: Smoker: yes ☐ no ☐
Smokeless Tobacco: yes ☐ no ☐
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 63 of 179
ORAL EXAM
LOCATION Normal Abnormal Describe Abnormality
Mucosa (including lips) ☐ ☐
Gingival Mucosa ☐ ☐
Hard Palate ☐ ☐
Soft Palate ☐ ☐
Mucogingival Folds ☐ ☐
Tongue ☐ ☐
Sublingual Area ☐ ☐
Submandibular Area ☐ ☐
Salivary Glands ☐ ☐
Tonsilar Area ☐ ☐
Pharyngeal Area ☐ ☐
Teeth ☐ ☐
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 64 of 179

MODIFIED GINGIVAL INDEX
MAXILLARY
Tooth 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Palatal
MANDIBULAR
Tooth 31 30 29 28 27 26 25 24 23 22 21 20 19 18
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Lingual
Area Total # Sites Mean Maxilla
Mandible Total
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 65 of 179

GINGIVAL BLEEDING INDEX
MAXILLARY
Tooth 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Palatal
MANDIBULAR
Tooth 31 30 29 28 27 26 25 24 23 22 21 20 19 18
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Lingual
Area Total # Sites
Maxilla Mandible
Total
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 66 of 179
PRE-BRUSHING PLAQUE INDEX
MAXILLARY FACIAL LINGUAL
UPPER RIGHT UPPER LEFT UPPER LEFT UPPER RIGHT 2 3 4 5 6 7 8 9 10 11 12 13 14 15 15 14 13 12 11 10 9 8 7 6 5 4 3 2
D M D M
G G G G
M D M D
MANDIBULAR FACIAL LINGUAL
LOWER RIGHT LOWER LEFT LOWER LEFT LOWER RIGHT 31 30 29 28 27 26 25 24 23 22 21 20 19 18 18 19 20 21 22 23 24 25 26 27 28 29 30 31
D M D M
G G G G
M D M D
Area Total # Sites Mean Maxilla
Mandible Total
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 67 of 179
SCREENING ELIGIBILITY DETERMINATION
Subject meets eligibility entry criteria:
All criteria must have positive response
• MGI score of 1.75-2.3 YES ☐1 NO ☐2
• BI score ≥ 20 YES ☐1 NO ☐2
• PI score ≥1.95 YES ☐1 NO ☐2
Randomization Number
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 68 of 179
POST-BRUSHING ORAL EXAM
LOCATION Normal Abnormal If
Abnormal Check ☒
if AE
Describe Abnormality
Mucosa (including lips) ☐ ☐ ☐
Gingival Mucosa ☐ ☐ ☐
Hard Palate ☐ ☐ ☐
Soft Palate ☐ ☐ ☐
Mucogingival Folds ☐ ☐ ☐
Tongue ☐ ☐ ☐
Sublingual Area ☐ ☐ ☐
Submandibular Area ☐ ☐ ☐
Salivary Glands ☐ ☐ ☐
Tonsilar Area ☐ ☐ ☐
Pharyngeal Area ☐ ☐ ☐
Teeth ☐ ☐ ☐
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 69 of 179
POST-BRUSHING PLAQUE INDEX
MAXILLARY FACIAL LINGUAL
UPPER RIGHT UPPER LEFT UPPER LEFT UPPER RIGHT 2 3 4 5 6 7 8 9 10 11 12 13 14 15 15 14 13 12 11 10 9 8 7 6 5 4 3 2
D M D M
G G G G
M D M D
MANDIBULAR FACIAL LINGUAL
LOWER RIGHT LOWER LEFT LOWER LEFT LOWER RIGHT 31 30 29 28 27 26 25 24 23 22 21 20 19 18 18 19 20 21 22 23 24 25 26 27 28 29 30 31
D M D M
G G G G
M D M D
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 70 of 179

ORAL EXAM
LOCATION Normal Abnormal If Abnormal
Check ☒ if AE
Describe Abnormality
Mucosa (including lips) ☐ ☐ ☐
Gingival Mucosa ☐ ☐ ☐
Hard Palate ☐ ☐ ☐
Soft Palate ☐ ☐ ☐
Mucogingival Folds ☐ ☐ ☐
Tongue ☐ ☐ ☐
Sublingual Area ☐ ☐ ☐
Submandibular Area ☐ ☐ ☐
Salivary Glands ☐ ☐ ☐
Tonsilar Area ☐ ☐ ☐
Pharyngeal Area ☐ ☐ ☐
Teeth ☐ ☐ ☐
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 71 of 179
MODIFIED GINGIVAL INDEX
MAXILLARY
Tooth 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Palatal
MANDIBULAR
Tooth 31 30 29 28 27 26 25 24 23 22 21 20 19 18
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Lingual
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 72 of 179

GINGIVAL BLEEDING INDEX
MAXILLARY
Tooth 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Palatal
MANDIBULAR
Tooth 31 30 29 28 27 26 25 24 23 22 21 20 19 18
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Lingual
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 73 of 179
PLAQUE INDEX
MAXILLARY FACIAL LINGUAL
UPPER RIGHT UPPER LEFT UPPER LEFT UPPER RIGHT 2 3 4 5 6 7 8 9 10 11 12 13 14 15 15 14 13 12 11 10 9 8 7 6 5 4 3 2
D M D M
G G G G
M D M D
MANDIBULAR FACIAL LINGUAL
LOWER RIGHT LOWER LEFT LOWER LEFT LOWER RIGHT 31 30 29 28 27 26 25 24 23 22 21 20 19 18 18 19 20 21 22 23 24 25 26 27 28 29 30 31
D M D M
G G G G
M D M D
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 74 of 179

ORAL EXAM
LOCATION Normal Abnormal If Abnormal
Check ☒ if AE
Describe Abnormality
Mucosa (including lips) ☐ ☐ ☐
Gingival Mucosa ☐ ☐ ☐
Hard Palate ☐ ☐ ☐
Soft Palate ☐ ☐ ☐
Mucogingival Folds ☐ ☐ ☐
Tongue ☐ ☐ ☐
Sublingual Area ☐ ☐ ☐
Submandibular Area ☐ ☐ ☐
Salivary Glands ☐ ☐ ☐
Tonsilar Area ☐ ☐ ☐
Pharyngeal Area ☐ ☐ ☐
Teeth ☐ ☐ ☐
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 75 of 179

MODIFIED GINGIVAL INDEX
MAXILLARY
Tooth 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Palatal
MANDIBULAR
Tooth 31 30 29 28 27 26 25 24 23 22 21 20 19 18
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Lingual
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 76 of 179

GINGIVAL BLEEDING INDEX
MAXILLARY
Tooth 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Palatal
MANDIBULAR
Tooth 31 30 29 28 27 26 25 24 23 22 21 20 19 18
Site G P G P G P G P G P G P G P G P G P G P G P G P G P G
Facial
Lingual
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 77 of 179
PLAQUE INDEX
MAXILLARY FACIAL LINGUAL
UPPER RIGHT UPPER LEFT UPPER LEFT UPPER RIGHT 2 3 4 5 6 7 8 9 10 11 12 13 14 15 15 14 13 12 11 10 9 8 7 6 5 4 3 2
D M D M
G G G G
M D M D
MANDIBULAR FACIAL LINGUAL
LOWER RIGHT LOWER LEFT LOWER LEFT LOWER RIGHT 31 30 29 28 27 26 25 24 23 22 21 20 19 18 18 19 20 21 22 23 24 25 26 27 28 29 30 31
D M D M
G G G G
M D M D
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 78 of 179
SUBJECT SUMMARY
1. Did subject experience an Adverse Event?
Yes ☐ No ☐
2. Date Subject first used test article: - -
dd/mmm/yyyy
3. Date Subject last used test article: - -
dd/mmm/yyyy
4. Did the Subject complete the study as planned? Yes ☐ No ☐
If 'No', indicate ONE reason:
Withdrawal of consent ☐
Deviation from protocol (including non-compliance)
☐
Lost to follow-up ☐ Adverse Event ☐
Other (give details)_______________________
☐
5. Date of Last Visit: - -
dd/mmm/yyyy
Date: - -
Investigator Signature dd/mmm/yyyy
With my signature, I confirm that all information recorded in these CRFs are accurate and complete.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 79 of 179
Adverse Event Form Complete this form only if subject experienced any Adverse Events during this study
Page ___ of ___
Severity Study Intervention Relationship
Action Taken Regarding Study Intervention
Outcome of AE Serious
1 = Mild 2 = Moderate 3 = Severe
1 = Unrelated 2 = Possible 3 = Probable 4 = Definite
1 = None 2 = Rx Therapy 3 = Discontinued Study 4 = Other (specify)
1= Resolved w/o sequelae 2 = Resolved w/sequelae 3 = Not recovered/resolved 4 = Death
1 = Yes 2 = No (If yes, complete SAE form)
Adverse Event Start Date (dd/mmm/yyyy)
Stop Date (dd/mmm/yyyy) Severity
Relationship to Study
Treatment
Action Taken
Outcome of AE
Serious Adverse Event?
1.
2.
3.
4.
5.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 80 of 179

1. SAE Onset Date: _____/______/________ (dd/mmm/yyyy)
2. SAE Stop Date: ____/______/________(dd/mmm/yyyy)
3. Was this an unexpected adverse event? Yes No
4. Brief description of participant(s) with no personal identifiers:
Sex: F M Date of Birth: _____/______/________ (dd/mmm/yyyy)
5. Brief description of the nature of the serious adverse event (attach description if more space needed): ___________________________________________________________________
___________________________________________________________________
___________________________________________________________________ 6. Category of the serious adverse event:
death – date ____/_______/________ (dd/mmm/yyyy) congenital anomaly / birth defect
life-threatening required intervention to prevent
hospitalization-initial or prolonged permanent impairment
disability / incapacity
other:__________________ 7. Relationship of event to study test material: Unrelated (clearly not related to the intervention)
Possible (may be related to intervention)
Definite (clearly related to intervention)
Serious Adverse Event
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 81 of 179
8. Was study test material/participation discontinued due to event? Yes No
9. What medications or other steps were taken to treat serious adverse event?
______________________________________________________________________
______________________________________________________________________ ______________________________________________________________________
______________________________________________________________________
10. List any relevant tests, laboratory data, history, including preexisting medical conditions
_____________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________ 11. Type of report:
Initial
Follow-up
Final
Signature of Principal Investigator: _____________________________Date: _____/______/________ (dd/mmm/yyyy)
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 82 of 179

4.1.3 Ethics Committees and Subject Information
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 83 of 179
Telephone 514.337.0442 • Facsimile 514.336.1142 • www.veritasIRB.com
A member of the ethica Clinical Research Inc. group of companies.
8555 Transcanada Hwy., Suite 201, Saint-Laurent (Montreal), Quebec H4S 1Z6
Page 1 of 2
Research ethics simplified™
INDEPENDENT REVIEW BOARD COMMUNICATION
IRB Review Date: September 23, 2019
IRB Tracking Number: 16410-12:10:5923-09-2019
Sponsor: BURST.USA.inc.
Study Number: PTB-002-2019 Study Name: Thirty-Day Evaluation of a Sonic Power Toothbrush versus a
Manual Toothbrush on Plaque and Gingivitis Efficacy Principal Investigator: Dr. Chhaju Ram Goyal
Study Expiration Date: August 4, 2020
RE: Changes to Research – Study Closure – Acknowledged
The Independent Review Board has completed its review using the delegated review procedure, in compliance with normative documents governing research with humans. Please find attached a list of the members (by affiliation) who participated in this review. The following document was reviewed and acknowledged by the Independent Review Board: Ø Study Closure Report dated September 23, 2019 (Site-specific: Dr. Chhaju Ram Goyal).
NOTE Ø As the Site of Dr. Chhaju Ram Goyal is now closed, all documents pertaining to this Study will be archived
according to Veritas IRB Standard Operating Procedures.
Should you have any questions or require clarification of any issues, please do not hesitate to contact us. Thank you. Veritas IRB Inc. Verified by Kevin Emery on 25-Sep-19 @ 16:23
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 84 of 179

Page 2 of 2
Research ethics simplified™
Veritas Independent Review Board – Member List
Chair/Ethics Representative Male – B.A. (Hon), Specialist in Bioethics, University of Toronto (2005), M.A. (Distinction), Applied Ethics, Norwegian University of Science and Technology (2008) – Quality Coordinator, Eye Bank of Canada – Former Ethicist, University Health Network Research Ethics Board (Board C (Oncology Research)) – Former Clinical Quality Assurance and Human Research Protection Program Manager, Merita CQA Inc. – Former Program Coordinator, Clinical Trials Ontario – English
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 85 of 179

Name of Principal Investigator (PI):
Site / Clinic / Company Name:
Print Name
Signature
STUDY CLOSURE REPORT
1. PI/Site Administrative Information
Sponsor of the Research:
Protocol Number: (If there is no protocol number check here: )
Protocol Title:
2. Study Identification
Study Closure Date:
Veritas IRB considers that a study is closed only when all of the criteria listed below are met. Please confirm for each of the following:All participants have exited the studyAll research-related interventions, including long term follow-up, have ceasedAll queries have been resolvedPrivate identifiable information is no longer being collected/accessedThe Sponsor/CRO has formally confirmed site closure (please attach the confirmation of site closure)
*If No, please specify. Please note that Veritas IRB will only issue an acknowledgement of study closure upon receipt and review of writtenSponsor confirmation of such (to be provided to the IRB by the Site).
________ / ________ / ____________
Total number of Participants enrolled into Study at this Site:
Total number of screen failures:
Total number of Participants withdrawn from Study at this Site:
Total number of Participants who completed the Study at this Site:
3. Study Closure Information
DD MM YYYY
DD MM YYYY
How many unexpected and related Serious Adverse Events were experienced in this Study at this Site in total?
Were there any unexpected and related Serious Adverse Events or other Unanticipated Problems at your Site that have not been previously reported to the IRB?
I certify that I have submitted all the required documentation and that the above information is accurate and truthful to the best of my knowledge.
4. Safety Information
If Yes, attach a summary describing the Unanticipated Problems.
________ / ________ / ____________
Yes No
Yes No Yes No
Yes No Yes No*
Yes No
Page 1 of 1Version: May 31, 2013www.VeritasIRB.com
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 86 of 179
Telephone 514.337.0442 • Facsimile 514.336.1142 • www.veritasIRB.com
A member of the ethica Clinical Research Inc. group of companies.
8555 Transcanada Hwy., Suite 201, Saint-Laurent (Montreal), Quebec H4S 1Z6
Page 1 of 3
Research ethics simplified™
INDEPENDENT REVIEW BOARD COMMUNICATION
IRB Review Date: August 8, 2019
IRB Tracking Number: 16410-16:49:327-08-2019
Sponsor: BURST.USA.inc.
Study Number: PTB-002-2019 Study Name: Thirty-Day Evaluation of a Sonic Power Toothbrush versus a
Manual Toothbrush on Plaque and Gingivitis Efficacy Principal Investigator: Dr. Chhaju Ram Goyal
Study Expiration Date: August 4, 2020
RE: Response to Conditions – Initial Review – Principal Investigator and Site Review – Unconditionally Approved
The Independent Review Board has completed its review using the delegated review procedure, in compliance with normative documents governing research with humans. Please find attached a list of the members (by affiliation) who participated in this review. The following documents were reviewed and acknowledged by the Independent Review Board:
1. Communication from CRO dated August 7, 2019 2. Informed Consent Documentation – Main, English version, dated August 7, 2019 (Site-Specific: Dr. Chhaju
Ram Goyal).
Please find below the status of approval for the following documents:
Study Protocol n Unconditionally Approved Site-specific: Dr. Boulos Haraoui (dated July 26, 2019) r Conditionally Approved Version 1.03 r Deferred
r Disapproved
Informed Consent Documentation – Main n Unconditionally Approved Site Specific: Dr. Chhaju Ram Goyal r Conditionally Approved (English version, dated August 7, 2019) r Deferred r Disapproved Principal Investigator and Site Submission Form, Curriculum Vitae and Current Dental License: Ø Dr. Chhaju Ram Goyal is unconditionally approved as a Principal Investigator for the above-referenced
Study.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 87 of 179

Page 2 of 3
Research ethics simplified™
NOTES Ø As the Study Protocol, dated July 26, 2019, Informed Consent Documentation, Study Budget and
Investigator have been approved, the above-referenced Study may now commence at the Site of Dr. Chhaju Ram Goyal;
Ø All Unanticipated Events involving risks to Research Participants must be reported to the Independent
Review Board within 5 business days. Should these Unanticipated Events occur, please alert us by completing the appropriate form available at http://www.veritasirb.com/resources.html, and returning it to us via our website, http://www.veritasirb.com/online_submit.html, or by email at [email protected]. In the event that a more complete report may be needed, you will be notified. Any Unanticipated Events must be reported in a timely manner, in accordance with Veritas IRB Reporting Policies and Procedures;
Ø As part of our ongoing commitment to promote best practices in ethical conduct of research and the
protection of human research participants, we would like to offer you a complimentary copy of Veritas IRB’s Investigator Manual.
Should you have any questions or require clarification of any issues, please do not hesitate to contact us. Thank you. Veritas IRB Inc. Verified by Ana Amélia Simōes Lopes on 8-Aug-19 @ 12:41
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 88 of 179

Page 3 of 3
Research ethics simplified™
Veritas Independent Review Board – Member List
Chair/Ethics Representative Male – LL.B., M.Sc. (Experimental Medicine (Specialization in Biomedical Ethics)), B.Sc. with Honors (Biochemistry) – Senior Officer, Legal Affairs, TransMedTech Institute – Member, Quebec Bar Association – English and French
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 89 of 179
Subject # Subject Initials
For office use only
Sponsor #PTB-002-2019 All Sum Study #2019-BR-1
Confidential Document Version FINAL, AUG 7, 2019 Page 1 of 8
INFORMED CONSENT FORM
Title: Thirty-Day Evaluation of a Sonic Power Toothbrush Versus a Manual Toothbrush on Plaque and Gingivitis Efficacy
Sponsor: BURST.USA.inc
340 S. Lemon Avenue #4658 Walnut, CA 91789
Site: All Sum Research Center Ltd. 6635 Kitimat Road, Units 36 & 37 Mississauga, Ontario L5N 6J2 Canada
Investigator: Chhaju Ram Goyal, BDS All Sum Research Center Ltd. 6635 Kitimat Road, Units 36 & 37 Mississauga, Ontario L5N 6J2 Canada
Study related phone numbers: 905-282-1099
SUBJECT NAME (Please Print) (First Name) (Last Name) Thank you for your willingness to consider participating in our clinical research study. Before agreeing to participate in this study, it is important that you read this form. This form, called a consent form, describes the purpose, procedures, benefits, financial payment, risks and discomforts of this research study. It also describes your rights to withdraw from this research study at any time. Please ask any questions you need to help you decide whether you want to be in this study. This consent form may contain words that you do not understand. Please ask the study staff to explain any words or information that you do not clearly understand.
PURPOSE The objective of this 30-day, randomized, examiner-blind clinical trial study is to assess the oral safety and efficacy of a marketed sonic power toothbrush with charcoal-infused toothbrush bristles in reducing dental plaque and gingivitis (gum inflammation), compared to a manual toothbrush. Manual toothbrushes are effective in removing plaque but depend on the skill, technique and time commitment of the user. A sonic toothbrush is a type of electric or power toothbrush that uses ultrasound and sonic waves to vibrate the brush and remove plaque. Routine removal of plaque is important to preventing tooth decay and gum disease. Power toothbrushes provide the cleaning action and the user only needs to guide the brush along the surfaces of the teeth to disrupt and remove plaque. This sonic power toothbrush under study has a built-in two-minute timer with 30-second interval alerts to help the user move the brush to the next quadrant of the
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 90 of 179

Subject # Subject Initials
For office use only
Sponsor #PTB-002-2019 All Sum Study #2019-BR-1
Confidential Document Version FINAL, AUG 7, 2019 Page 2 of 8
mouth. This feature helps to encourage longer and more thorough teeth cleaning and with minimal pressure required.
Charcoal manual toothbrushes are found on the Canadian market and claim to help whiten teeth by removing surface stains. Although the sonic toothbrush in this study has charcoal infused bristles, it is not being evaluated for its stain removal benefits. Research has shown that electric toothbrushes are better in removing dental plaque and reducing gum inflammation than brushing with a manual toothbrush. Therefore, the manufacturer wants to learn if their sonic brush is better than a manual toothbrush in removing plaque and reducing gingivitis. As with most oral care studies, the effect of the toothbrush on the soft and hard tissues in the mouth will be monitored. There are no known risks associated with the use of the sonic power toothbrush. The toothbrush is currently marketed in Canada and is similar to other sonic power toothbrushes available for purchase in the U.S. and Canada. The possible risks of using toothbrushes may include some minor and reversible damage to oral soft tissue (gums) that can occur with improper brushing.
DESCRIPTION OF THE STUDY You have been identified as an individual who is a regular manual toothbrush user and may qualify to participate in this research study. Approximately 100 healthy adults are planned to be eligible and enroll in this research study. Your participation in this study will last 30 days. If you qualify for this research study and you are enrolled, you will be randomly assigned (by chance, like flipping a coin) to one of two treatment groups. All exams will take place at the All Sum Research Center. All toothbrushes and toothpastes are commercially marketed products. The Crest® Regular Cavity protection toothpaste is marketed in Canada. The sonic power toothbrush is sold in the U.S. and Canada. This research study will compare plaque removal of a marketed power toothbrush compared to ADA reference manual soft toothbrush. The dental exams and procedures to be performed in this research study are standard techniques; however, they are being used in an experimental setting to assess the dental plaque removal ability of different toothbrushes. SPECIFIC STUDY PROCEDURES After you read and sign this consent form, you will complete health and dental questionnaires and provide information about your age, date of birth, race, gender and tobacco use. A staff member will review the inclusion and exclusion criteria to determine if you qualify to participate in this study. The investigator will perform a screening examination to determine whether you qualify to enter this research study, and they will:
• Confirm you are a regular manual toothbrush user. • Ask you to complete a medical questionnaire and interview you about your medical and dental
history, such as any current oral conditions and medicines. • Examine tissues in your mouth to check for abnormalities, e.g. evidence of gingival abrasion,
irritations, lacerations, or ulcerations. • Complete a dental charting to record the presence of dental restorations such as crowns, veneers,
alloys, and composites. • Assess the levels of gingival inflammation (color and swelling of your gums) and gingival bleeding
following a gentle probing around the whole mouth. • Measure the amount of plaque on your teeth (a red dye that will temporarily discolor your teeth and
gums will be used to assist the examiner).
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 91 of 179

Subject # Subject Initials
For office use only
Sponsor #PTB-002-2019 All Sum Study #2019-BR-1
Confidential Document Version FINAL, AUG 7, 2019 Page 3 of 8
To qualify for this study, you must meet the following criteria:
• You must be generally healthy and at least 18 years of age. • You must be able to read, sign and receive a copy of the signed informed consent form. • Be regular manual toothbrush users. • Be willing to refrain from all oral hygiene 8-12 hours prior to each study visit, and discontinue
eating, drinking and smoking 30 minutes prior to each study visit. • You have a minimum of 18 natural teeth. • You have moderate dental plaque formation and gum inflammation, based on the investigator’s
evaluation. • You must be willing to refrain from dental treatment during the course of the study, except on an
emergency basis. • You do not have a history of adverse effects or known allergies to any ingredient in the test
materials. • You do not have any serious medical conditions. • You are not pregnant or nursing. • You are not under treatment for a heart condition requiring use of pacemaker. • You do not have any health condition that, in the opinion of the investigator, would place you at
increased risk or prevent you from completing the study. • You are not participating in any study involving oral care products, now or within the 30 days of
screening exam. • You must be willing to discontinue use of other oral hygiene products for the duration of the study. • You do not have severe periodontal (gum) disease or oral soft tissue irritations based on a visual
examination by the dentist investigator. • You do not have orthodontic appliances, oral piercings or removable partial dentures.
CLINCAL PROCEDURES During the study you will follow your usual dietary and smoking habits. You will be provided with both written and verbal instructions on how to use your study products. You will be asked to carefully read and follow the instructions. You must not participate in any other dental/oral product studies during the course of this study. You will be instructed to refrain from routine dental treatment during the study, but should an emergency arise, you should not postpone any necessary or emergency dental treatment. In the event that you seek emergency dental treatment, or any non-routine procedure or treatment which may affect the outcome of this study, please let the examining dentist know immediately. Visit 1 (Screening/Baseline): This visit will last approximately sixty (60) minutes. You will report to the clinical facility having refrained from oral hygiene 8-12 hours prior to each study visit, and discontinue eating, drinking and smoking 30 minutes prior to each study visit. If you meet all these screening requirements the investigators will enroll you in this research study and will provide you with further instruction. Once you qualify, the research study staff will:
• Randomly assign you (by chance, like flipping a coin) to one of two toothbrush groups. • Issue your research study products for the 30-day plaque and gingivitis study.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 92 of 179

Subject # Subject Initials
For office use only
Sponsor #PTB-002-2019 All Sum Study #2019-BR-1
Confidential Document Version FINAL, AUG 7, 2019 Page 4 of 8
• Distribute either a sonic power toothbrush or ADA reference manual soft toothbrush, a tube of Crest® Cavity Protection dentifrice (Procter & Gamble, Cincinnati, OH, USA) toothpaste and brushing diary to all subjects.
• Verbally instruct you about this research study’s treatment requirements and supervise your first use of your assigned toothbrush to be sure that you understand the instructions.
• Direct you to brush at home twice daily (morning and evening) for the next 14 days with your assigned toothbrush as instructed with your assigned toothbrush (two minutes with the sonic power toothbrush and your customary usage pattern with the manual brush).
• Remind you not to use other toothbrushes, toothpaste, mouthwashes, chewing gum, breath film, floss or interdental cleaning aids, or other oral care cleaning aids for the duration of this research study.
• Schedule your follow-up appointment 15 days later. Please do not to discuss your oral hygiene regimen with the study dentist or other subjects for the duration of this research study. The research study dentist is blinded (will not know which oral hygiene regimen you are assigned to use). However, this information is made available to the research study dentist in an emergency. Visit 2 (Day 15): This visit will last approximately thirty (30) minutes. You will return to the clinic for your second visit 15 (± 2) days later. You will need to bring your assigned toothbrush, toothpaste and treatment diary to the clinic, and you will be asked to refrain from brushing your teeth for 8 to 12 hours before this appointment. During Visit 2 the research study staff will:
• Inventory all your assigned research study materials (i.e. toothbrush, toothpaste and diary). • Update your medical/dental history for any changes in your health or new medicines. • Interview you to determine if you were able to follow the instructions and use the assigned test
products correctly during the treatment phase of this research study. • Ask if you encountered any problems during this research study and record any comments. • Examine the tissues inside your mouth to check for abnormalities. • Assess the levels of gingival inflammation (color and swelling of your gums) and gingival bleeding
following a gentle probing around the whole mouth. • Measure the amount of plaque on your teeth (a red dye that will temporarily discolor your teeth and
gums will be used to assist the examiner). • Direct you to brush at home twice daily (morning and evening) for the next 14 days with your
assigned toothbrush as instructed. • Remind you not to use other toothbrushes, toothpaste, mouthwashes, chewing gum, breath film, or
other oral care cleaning aids for the duration of this research study. • Schedule your follow-up appointment 15 (± 2) days later for the Day 30 visit.
Visit 3 (Day 30): This visit will last approximately thirty (30) minutes. You will return to the clinic for your third visit 30 days after Visit 1 (± 2 days). You will need to bring your assigned toothbrush, toothpaste and treatment diary with you. Also, you will be asked to refrain from brushing your teeth for 8 to 12 hours before this final appointment. During Visit 3 the research study staff will:
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 93 of 179
Subject # Subject Initials
For office use only
Sponsor #PTB-002-2019 All Sum Study #2019-BR-1
Confidential Document Version FINAL, AUG 7, 2019 Page 5 of 8
• Collect all your assigned research study materials (i.e. toothbrush and diary). • Update your medical/dental history for any changes in your health or new medicines. • Interview you to determine if you were able to follow the instructions and use the assigned test
products correctly during the treatment phase of this research study. • Ask if you encountered any problems during this research study and record any comments. • Examine the tissues inside your mouth to check for abnormalities. • Assess the levels of gingival inflammation (color and swelling of your gums) and gingival bleeding
following a gentle probing around the whole mouth. • Measure the amount of plaque on your teeth (a dye that will temporarily discolor your teeth and
gums will be used to assist the examiner). • A staff member will supervise your brushing session with the assigned toothbrush. • Ask you if you experienced any adverse changes during brushing. • Re-examine the tissues inside your mouth to check for abnormalities. • Repeat plaque measurement after again applying the dye to your teeth. • You will then be dismissed from the research study and paid a gratuity.
SUBJECT RESPONSIBILITIES You must be available to attend the research study visit and refrain from all oral hygiene procedures for 8 to 12 hours prior to the clinical examination. LENGTH OF PARTICIPATION If you qualify and you are enrolled after the screening exam (Visit 1), you will use your assigned toothbrush and toothpaste for 30 days (±2 days). All exams will take place at the All Sum Research Center dental clinic. Approximately 90 subjects will complete the research study. POTENTIAL RISKS The risk of permanent harm or injury, or disability as a result of participation in this study is minimal. The dental exams are similar to those used as part of routine oral health care. Your participation is not expected to cause any oral conditions different from those normally experienced in routine dental care. No known side effects or risks are associated with the use of the study toothbrushes or toothpaste. The toothpaste in this study is currently marketed and contains ingredients that are commonly sold in commercially available products. The power sonic toothbrush is currently marketed and is similar to other sonic power toothbrushes available for purchase in the U.S. and Canada. In addition, the manual soft bristle toothbrush is currently marketed. The possible risks of using toothbrushes may include some minor and reversible damage to oral soft tissue (gums) that can occur with improper brushing. Based on consumer data, these risks are minimal. Some people may be sensitive to the flavoring agents in the toothpaste causing allergic reactions or irritation. Based on consumer data, these risks are minimal. These events are usually mild and temporary, but if they continue, you should report them to the Study Dentist, and go immediately to a hospital if you experience a serious reaction. No other known side effects or risks are associated with the use of the research study products. There is a chance the use of the research study products may involve risks that are currently unknown.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 94 of 179
Subject # Subject Initials
For office use only
Sponsor #PTB-002-2019 All Sum Study #2019-BR-1
Confidential Document Version FINAL, AUG 7, 2019 Page 6 of 8
You will be asked to report any discomfort or irritation you experience while using your research study products and for up to 5 days after the last use of this research study products. All products provided to you as part of this research study are for your use only. Keep all assigned products out of the reach of children and persons who may not be able to read or understand the label, as well as pets.
BENEFITS This study is for research purposes only. There is no direct benefit to you from your participation in the study. ALTERNATIVE TO PARTICIPATION This research is not for the treatment of a medical condition. The only alternative is to not participate in this research. You may also see a dentist for professional treatment options.
NEW FINDINGS Any significant new findings that may relate to your willingness to continue participation will be provided to you in a timely manner. COST There will be no charge to you for your participation in this research. The study visits will be provided at no charge to you or your insurance company. You will not lose any of your legal rights by signing this consent document. COMPENSATION FOR INJURY If you are injured in the course of the study, medical treatment will be provided to you under your Provincial Health Insurance Plan. By signing this consent form, you are not giving up any of your legal rights. If there is any physical injury as a direct result of your participation in this study, the sponsoring company will be responsible for medical costs provided you seek medical attention as directed by the sponsoring company or investigator. The sponsor will not pay you or provide any other type of benefit for any adverse experience that happens while participating in this research study. QUESTIONS If any questions or problems arise, you should contact the study investigator immediately:
Dr. C.R. Goyal All Sum Research Center Ltd 905-282-1099 For after hour emergencies please call (416) 735-2480.
This study has been reviewed and approved by Veritas Independent Review Board (IRB). If you have any questions about your rights as a research participant or the Investigator’s responsibilities, you may contact the Manager of Veritas IRB 24 hours per day and 7 days per week at 514-337-0442 or toll-free at 1-866-384-4221.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 95 of 179
Subject # Subject Initials
For office use only
Sponsor #PTB-002-2019 All Sum Study #2019-BR-1
Confidential Document Version FINAL, AUG 7, 2019 Page 7 of 8
An IRB is a group of scientific and non-scientific individuals who perform the initial and ongoing ethical review of the research study with the subject’s rights and welfare in mind. If you have any study-related comments, complaints or concerns, you should first contact the study investigator. Please call the IRB if you need to speak to a person independent from the Investigator and the research staff, and/or the investigator and the research staff could not be reached. COMPENSATION You will be monetarily compensated by All Sum Research Center Ltd after you complete the study. Upon successfully completing all of the provisions and the procedures of this study, you will receive a financial remuneration in the amount of $120.00 (one hundred twenty dollars). If you withdraw from the study, the amount you will receive will be in proportion to your participation. If you do not follow the instructions given to you exactly, you can be disqualified from the study and your compensation will be prorated. There will be no charge to you for the products required by this research study. INVESTIGATOR COMPENSATION The study dentist (Clinical Investigator) has made financial arrangements with All Sum Research Center Ltd for his fees related to the study. RIGHT TO LEAVE THE STUDY If any significant new findings, directly pertinent to your interests, develop during the course of the study, you will be so advised. If you decide to discontinue participation in the study, you should feel free to do so at any time without penalty. However, it is important that you return study materials. Your participation may be terminated by the Investigator if you violate the study plan, do not comply with the instructions, or for administrative reasons, without regard to your consent. CONFIDENTIALITY OF RECORDS The records of your participation in this study are confidential and these records are available to the investigator, the sponsoring company, the IRB, and the Food and Drug Administration (U.S.A.) or Health Canada. The results of this study may be published, and your initials and age may be used but not your name. Your study information and related personal medical information will be shared with the study sponsor. Your identity will be kept confidential and all study records will be labeled only with a code such as Subject Number. Records pertaining to this study will be retained by the site for at least 2 years. Study records will be kept secure in locked filing cabinets under the Investigator’s supervision. The Investigator must receive written authorization from the Sponsor before destroying any study document. The Investigator will make the records available for inspection and copying upon the request of an authorized employee of a government authority or the Sponsor, at reasonable times. In the event the Investigator retires, relocates, or for any other reason withdraws from the responsibility for maintaining records for the period of time required, custody of the records may be transferred to another person who will accept responsibility for the records. Notice of such a transfer must be given in writing to the Sponsor. Subjects will have the right to review their Study records at any time.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 96 of 179
Subject # Subject Initials
For office use only
Sponsor #PTB-002-2019 All Sum Study #2019-BR-1
Confidential Document Version FINAL, AUG 7, 2019 Page 8 of 8
AUTHORIZATION I understand the nature, duration and purpose of the study and, if selected, hereby voluntarily consent to participate. I agree I have received a signed copy of this document. Subject's Name (Please Print) Subject’s Signature Date Person Obtaining/Administrating Consent Date
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 97 of 179

4.1.4 Investigators and Study Personnel
Curriculum Vitae are attached for the following study personnel:
Investigator: Chhaju Ram Goyal, BDS
Study Coordinator: Jimmy Qaqish
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 98 of 179
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 99 of 179
(Private Dental Practice) North York, ON Canada Dental Hygienist 1993-1999 Global Dental Laboratory
Thornhill, ON Canada Dental Technologist
1977-1992 Deluca Dental Laboratory
North York, ON Canada Dental Technologist Supervisor- Gold/Metal Department
Dental Technologist Responsibilities:
♦ Construction of appliances and prostheses. ♦ Quality control. ♦ Management. ♦ Training and upgrading of junior staff. ♦ Consultation with clients. ♦ Generating sales.
EDUCATIONAL QUALIFICATIONS
1999 License to Practice General Dentistry Royal College of Dental Surgeons Toronto, ON Canada 1999 National Dental Examination Board of Canada - Certification Ottawa, ON Canada 1993 Honours Certification in Dental Hygiene George Brown College of Applied Arts and Technology Toronto, ON Canada 1983 Registered Dental Technologist Toronto, ON Canada 1977 National Board Dental Examination-American Dental Association 1976 Bachelor of Dental Surgery Punjab Govt. Dental College & Hospital Amritsar, Punjab, India PROFESSIONAL MEMBERSHIPS and CERTIFICATIONS Ontario Dental Association
PROFESSIONAL DEVELOPMENT
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 100 of 179
Attended all Ontario Dental Association’s Annual Conventions since 1999 Attended all AADR, CADR and IADR Annual Conventions since 1999 2002 Getting the most our of Panrex film – Lyndon Smith 2002 “What you don’t know can hurt you” – TMCH Health Law Group 2001 “What’s new night” – Ash Temple 2000 Advanced Endodontic Diagnosis & Treatment – Dr. Herb Borsuk 1999 Ethic & Jurisprudence – RCDSO 1997 A Dental Practice Review – University of Toronto 1995 Certificate of Dental implant system- NOBELPHARMA CANADA. INC. 1994 “Soft tissue management” certificate of attendance -PRO-Dentec Canada. 1994 “Basic Periodontics for the 90’s” lecturer -Dr. Murray Arlin. 1991 “Ten easy steps to crowns and bridges” lecturer - Dr. M.S. Rubinoff. 1990 Certificate of Dental implant system- CORE-VENT, Arlington, TX 1983 “Roundhouse course on Dental Techniques” George Brown College of Applied Arts and Technology. Toronto, ON RECENT PUBLICATIONS 2018 C.R. Goyal1, M. Klukowska2, JG Qaqish 1, R, Eusebio, A.Wilberg, M. Gabbard,
(1Procter & Gamble Co., Mason, OH, USA; 2 All Sum Research Center Ltd., Canada) “Extrinsic Stain Removal by Non-Peroxide Sodium Hexametaphosphate Rinse” Abstract #0748 AADR/CADR, Fort Lauderdale, Florida, USA, March 22, 2018
2018 S. Santos, C.R. Goyal, J. Qaqish, J. Bowman, A. Sacarello, H. Katz, P. Rubin, (1H.
Katz, Dr Harold Katz, LLC, Los Angeles, CA, USA; 2All Sum Research Center Ltd., Canada); 3SLS Clinical Research Consulting LLC, Pine Brook, NJ, USA; 4J.Bowman, James P Bowman and Associates, Loveland, Ohio, USA “Three Week Clinical Efficacy of Chlorine Dioxide-Containing Mouthrinse on Oral Malodor” Abstract 0752, AADR/CADR, Fort Lauderdale, Florida, USA, March 22, 2018
2018 M. Klukowska2, C.R. Goyal1, T. He, JG Qaqish 1, S. Xie, C. Haught, S. Tansky, T,.
Huggins, D. Ramsey, R, Eusebio, C. Combs, D White, (1Procter & Gamble Co., Mason, OH, USA; 2 All Sum Research Center Ltd., Canada) “The Effect of SnF2
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 101 of 179
Dentifrice on Virulence of Subgingival Plaque” Abstract #0755 AADR/CADR, Fort Lauderdale, Florida, USA, March 22, 2018
2017 L. Friesen, T.He, M. Klukowska, R,Eusebio, H. Eynon, J. Qaqish, C.R. Goyal,
(1University of Missouri, Kansas City; 2Oral Health Care, Procter & Gamble Company, Mason, Ohio, USA; 3All Sum Research Center Ltd., Canada) “Comparative Anti-plaque Effect of Two Antimicrobial Dentifrices” J Clin Dent 2017;28 (Spec Iss B);B6-11)
2017 T.He, R,Eusebio, J. Qaqish, C.R. Goyal, (1Oral Health Care, Procter & Gamble
Company, Mason, Ohio, USA; 2All Sum Research Center Ltd., Canada) “Assessment of the Effects of a Novel Stabilized Stannous Fluoride Dentifrice on Gingivitis in a Two-Month Positive-Controlled Clinical Study” J Clin Dent 2017;28 (Spec Iss B);B12-16)
2017 L. Friesen, T.He, M. Klukowska, R,Eusebio, H. Eynon, J. Qaqish, C.R. Goyal,
(1University of Missouri, Kansas City; 2Oral Health Care, Procter & Gamble Company, Mason, Ohio, USA; 3All Sum Research Center Ltd., Canada) “Comparative Anti-plaque Effect of Two Antimicrobial Dentifrices” Oral Session, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 A. Gassemi, L.M. Vorwerk, W. Hooper, W. Hooper, A. Buelo, J. Qaqish, C.R. Goyal,
(1Church & Dwight Co., Inc., Princeton, NJ, USA; 2All Sum Research Center Ltd., Canada ) “Single-brushing Plaque Removal Efficacy Evaluation” Abstract 0883, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 C.R. Goyal, Deborah M. Lyle, JG Qaqish, Reinhard Schuller, (1Water Pik Inc. Fort
Collins, CO, USA; 2All Sum Research Center Ltd., Canada) “Efficacy of Two Interdental Cleaning Devices on Clinical Signs of Inflammaton: A Randomized Controlled Trial” Abstract 0883, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 S. Santos, C.R. Goyal, JG. Qaqish, J. Bruns, K. Yost, R. Schuller, (1Ranir Global LLC,
Grand Rapids, Michigen, USA; 2All Sum Research Center Ltd., Canada); 3SLS Clinical Research Consulting LLC, Pine Brook, NJ, USA “Comparison of a Water Flosser and Manual Brushing to Manual Brushing Only: A Four Week Randomized Controlled Trial” Abstract 0886, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 C.R. Goyal, Deborah M. Lyle, JG Qaqish, Reinhard Schuller, (1Water Pik Inc. Fort
Collins, CO, USA; 2All Sum Research Center Ltd., Canada) “Cost Effective Plaque and Gingivitis Reduction through Brush-Floss-Rinse Regimen” Abstract 0887, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 C.R. Goyal, J. Qaqish, T.He, M. Klukowska, JL. Winston, (1Oral Health Care, Procter
& Gamble Company, Mason, Ohio, USA; 2All Sum Research Center Ltd., Canada) “Clinical Anti-Gingivitis Efficacy of a 0.454% SnF2 Dentifrice” Abstract 0889, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 102 of 179
2017 C.R. Goyal, J. Qaqish, RA.C. Vasquez, JM. Grender, E. Conde, PA. Cunningham,
(1Oral Health Care, Procter & Gamble Company, Mason, Ohio, USA; 2All Sum Research Center Ltd., Canada) “Efficacy of a Battery Manual Toothbrush removing Dental Stain” Abstract 1532, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 J. Creeth, J. Gallob, J. Qaqish, C.R. Goyal, F. Sufi, N. Patel, (1GSK Consumer
Healthcare, Weybridge, UK; 2Silverstone Research Group, LV, USA, 3All Sum Research Center Ltd., Canada) “Short-Term Efficacy Studies of an Occluding Dentifrice on Dentinal Hypersensitivity” Abstract 1543, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 C.R. Goyal, F. Sufi, J. Qaqish, J. Creeth, (1All Sum Research Center Ltd., Canada;
2GSK Consumer Healthcare, Weybridge, UK) “Two-Week Efficacy of an Occluding Dentifrice on Dentinal Hypersensitivity” Abstract 1544, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 N. Gurich, M. Anastasia, C.R. Goyal, J. Qaqish, (1Oral Health Care, Procter &
Gamble Company, Mason, Ohio, USA; 2All Sum Research Center Ltd., Canada) “Clinical Trial to Evaluate Efficacy of Whitening Dentifrice” Oral Session, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2016 C.R. Goyal, Deborah M. Lyle, JG Qaqish, Reinhard Schuller, (1Water Pik Inc. Fort
Collins, CO, USA; 2All Sum Research Center Ltd., Canada) “Comparison of Water Flosser and Interdental Brush on Reduction of Gingival Bleeding and Plaque: A Randomized Controlled Pilot Study” Abstract J Clin Dent 2016: 27:61-65
2016 T.He, J. Qaqish, C.R. Goyal, M.K. Anastasia, R. Eusebio (Oral Health Care, Procter &
Gamble Company, Mason, Ohio, USA; 2All Sum Research Center Ltd., Canada) “Comparative Extrinsic Stain Removal Efficacy of Two Whitening Dentifrice” Abstract #0476 AADR, Los Angeles, Calif, USA, March 17, 2016
2016 L. Friesen, T.He, M.K. Anastasia, R. Eusebio, J. Qaqish, C.R. Goyal, (University of
Missouri, Kansas City; 2Oral Health Care, Procter & Gamble Company, Mason, Ohio, USA; 3All Sum Research Center Ltd., Canada) “Stain Removal Efficacy of a Whitening Dentifrice Versus Marketed Control” Abstract #0475 AADR, Los Angeles, Calif, USA, March 17, 2016
2016 T.He, J. Qaqish, C.R. Goyal, M.K. Anastasia, R. Eusebio (Oral Health Care, Procter &
Gamble Company, Mason, Ohio, USA; 2All Sum Research Center Ltd., Canada) “Superior Extrinsic Stain Removal Efficacy of a Whitening Dentifrice” Abstract #0472 AADR, Los Angeles, Calif, USA, March 17, 2016
2016 A. Gassemi, L.M. Vorwerk, W. Hooper, W. Hooper, M. Kwang, J.Qaqish, C.R. Goyal,
M. Naji (Church & Dwight Co., Inc., Princeton, NJ, USA; 2All Sum Research Center Ltd., Canada ) “Plaque Removal Efficacy Evaluation and Comparison of Three Manual Toothbrushes” Abstract 0456, AADR, Los Angeles, Calif, USA, March 17, 2016. Abstract J Clin Dent 2016: 27:71-75
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 103 of 179
2016 C.R. Goyal, Deborah M. Lyle, JG Qaqish, Reinhard Schuller, (1Water Pik Inc. Fort Collins, CO, USA; 2All Sum Research Center Ltd., Canada) “Comparison of Two Interdental Cleaning Devices: A Pilot Study” Abstract #0465 AADR, Los Angeles, Calif, USA, March 17, 2016
2015 C.R. Goyal, Deborah M. Lyle, JG Qaqish, Reinhard Schuller, (1Water Pik Inc. Fort
Collins, CO, USA; 2All Sum Research Center Ltd., Canada) “Efficacy of Two Interdental Cleaning Devices on Clinical Signs of Inflammation: A Four-Week Randomized Controlled Trial” Abstract J Clin Dent 2015: 26:55-60, 2015
2015 RA Ccahuana-Vasquez1, JM Grender2, E. Conde, P. Cunningham, C.R. Goyal, JG
Qaqish (1Procter & Gamble Co., Kronberg, Germany; 2Procter & Gamble Co.,Mason, OH, USA; All Sum Research Center Ltd., Canada) “An Eight-Week Clinical Evaluation of an Oscillating-Rotating Power Toothbrush with a Brush Head Utilizing Angled Bristles Compared with a Sonic Toothbrush in the Reduction of Gingivitis and Plaque”Abstract J Clin Dent 2015: 26:80-85, 2015
2015 M. Klukowska1, C.R. Goyal2, D. Khambe, M. Cannon, M. Miner, N. Gurich, B.
Circello, T. Huggins, M. Barker, C. Furnish, E. Conde, P. Hoke, C. Haught, S. Xie, D.J. White (1Procter & Gamble Co., Mason, OH, USA; 2 All Sum Research Center Ltd., Canada) “Response of Chronic Gingivitis to Hygiene Therapy and Experimental Gingivitis. Clinical, Microbiological and Metabonomic Changes” Abstract AM J Clin Dent 2015: 28:273-284, 2015
2014 C.A. Charles, T.A. Lisante, R. Revankar, J. R. Cortelli, S.C. Cortelli, D. Aquino,
C.R. Goyal, P. Amini; (Johnson & Johnson Consumer & Personal Products Worldwide, Morris Plains, NJ, USA) “Early Benefits with Daily Rinsing on Gingivial Health Improvements with an Essential Oil Mouthrinse – Post-Hoc Analysis of 5 Clinical Trials” Journal of Dental Hygiene Vol. 88, Supplement 2014
2013 C.R. Goyal, Deborah M. Lyle, JG Qaqish, Reinhard Schuller, (1Water Pik Inc. Fort
Collins, CO, USA; 2BioSci Research Canada Ltd., Canada) “Evaluation of the Plaque Removal Efficacy of a Water Flosser Compared to String Floss in Adults After a Single Use” Abstract J Clin Dent 2013: 24:37-42, July 21, 2013
2013 M. Klukowska1, J. Grender, E. Conde, C.R. Goyal2, (1Procter & Gamble Co., Mason,
OH, USA; 2BioSci Research America Inc., America) “A 12-Week Clinical Comparison of an Oscillating-Rotating Power Brush Versus a Marketed Sonic Brush with Self-Adjusting Technology in Reducing Plaque and Gingivitis” Abstract J Clin Dent 2013: 24:55-61, July 21, 2013
2013 M. Klukowska1, C.R. Goyal2, JG Qaqish 3, (1Procter & Gamble Co., Mason, OH, USA;
2BioSci Research Canada Ltd., Canada) “Anti-Gingivitis Effect of Combined Antimicrobial and Mechanical Oral Hygiene” Abstract #1301 IADR, Seattle, Washington, USA, March 21, 2013
2012 RA Ccahuana-Vasquez1, MA Klukowska2, A. Mielczarek3, Goyal4, JG Qaqish 4, JM
Grender2 (1Procter & Gamble Co., Kronberg, Germany; 2Procter & Gamble Co., Mason, OH, USA; 3Medical University, Warsaw, Poland; 4BioSci Research Canada Ltd., Canada) “Plaque and Gingivitis Reduction on Surfaces by Novel Toothbrush”
Abstract #209 PER/IADR Congress, Helsinki, Finland, September 12-15, 2012
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 104 of 179

2012 R. Adam*1, MA Klukowska1, Goyal2, JG Qaqish2, JM Grender1 (1Procter &
Gamble Co., Mason, OH USA, 2BioSci Research Canada Ltd., Canada) “Gingival Bleeding Reduction on Lingual and Approximal Surfaces by a Novel Toothbrush”
Abstract #214 PER/IADR Congress, Helsinki, Finland, September 12-15, 2012 2012 MA Klukowska*1, Goyal2, JM Grender1, P Cunningham1, JG Qaqish2, A Biesbrock1 (1 Procter & Gamble Co., Mason, OH, USA, 2 BioSci Research Canada Ltd., Canada) “Comparative Anti-gingivitis Efficacy of Oscillation-Rotation and Sonic Power
Toothbrush” Abs tract #524 PER/IADR Congress, Helsinki, Finland, September 12- 15, 2012
2012 Malgorzata Klukowswka, DDS, PhD, Julie M. Grender, PhD, C. Ram Goyal, DDS,
Christian Mandi, PhD & Aaron R. Biesbrock, DDS, PhD, MSc. “12-Week Clinical Evaluation of a Rotation/Oscillation Power Toothbrush Versus a New Sonic Power Toothbrush in Reducing Gingivitis and Plaque” AJD, Vol 25, No. 5, October 2012.
2012 C.R. Goyal, M Klukowska, J.M Grender, P. Cunningham & J. Qaqish “Evaluation of a
New Multi-directional Power Toothbrush Versus a Marketed Sonic Toothbrush on Plaque and Gingivitis Efficacy” AJD, Volume 25, Special Issue A, September 2012
2012 M. Klukowska, J.M. Grender, C.R. Goyal, J. Qaqish & A.R. Biesbrock “8-week
Evaluation of Anti-Plaque and Anti-Gingivitis Benefits of a Unique Multi-Directional Power Toothbrush Versus a Sonic Control Toothbrush” AJD, Volume 25, Special Issue A, September 2012
2012 Tao He, DDS, PhD, Matthew L. Barker, PhD, C. Ram Goyal, DDS & Aaron R.
Biesbrock, DMD, PhD, MS “Anti-Gingivitis Effects of a Novel 0.454% Stabilized Stannous Fluoride Dentifrice Relative to a Positive Control” AJD, Vol 25, No. 3, June 2012
2012 Tao He, DDS, PhD, Matthew L. Barker, PhD, A.R. Biesbrock, DMD, PhD, MS,
Procter & Gamble Company, Mason , OH, USA, N.C. Sharma, DDS, J. Qaqish, BSc, C.R. Goyal, DDS, BioSci Research Canada Ltd., Mississauga, Ontario, Canada “Assessment of the Effects of a Stannous Fluoride Dentifrice on Gingivitis in a Two- Month Positive Controlled Clinical Study” J. Clin Dent, Vol. 23, No. 3, 2012.
2012 N. Sharma1, J.E. Pelino2, A.M. Parikh3, Q. Du4, C. Charles3, C.R. Goyal1, M.W.
Araujo3, and J. Qaqish1, 1BioSci Research Canada, Ltd., Mississauga, ON, Canada, 2Johnson & Johnson, CPPW, Sao Paulo, Brazil, 3 Johnson & Johnson, CPPW, Morris
Plains, NJ, 4Johnson & Johnson China, Shanghai, China “Superiority of Essential-Oil vs. 0.075 CPC Rinses: Experiumental Gingivitis Model” Abstract 149 IADR, Iguaçu Falls, Brazil
2012 C. Ram Goyal , Deborah M. Lyle, Jimmy G. Qaqish, Reinhard Schuller “The
Addition of a Water Flosser to Power Tooth Brushing: Effect on Bleeding, Gingivitis, and Plaque” J. Clin. Den. Vol. XXIII, Number 2, 2012
2012 M.Barker*, T. He, A.R. Biesbrock, M.C. Miner, C.R. Goyal and J. Qaqish (Procter & Gamble Company, Mason, OH, USA) “2-Month Gingivitis Treatment Comparison of Stannous Fluoride and Triclosan/Copolymer Dentifrices”
Abstract 0742 IADR, Tampa, Florida
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 105 of 179
2012 T. He*, M. Barker, A. Biesbrock, P. Amini, C. Goyal and J. Qaqish (The Procter &
Gamble Company, Mason, OH, USA) “Superior Anti-gingivitis Benefits of Stannous Fluoride among Triclosan Dentifrice Users” Abstract 0746 IADR, Tampa Florida 2011 C.R. Goyal, J. Qaqish, S. Farrell, J.M. Grender, J.R. Rooney and P. Cunningham
“Plaque and Gingivitis Effects of Sonic Brush with New Brushhead” (BioSci Research Canada, Ltd., Mississauga, Canada) Abstract 0801 IADR, San Diego, California
2011 S. Farrell, J.M. Grender, J.R. Rooney, C.R. Goyal and J. Qaqish “Long Term Plaque
and Gingivitis Reduction Benefits of New Sonic Toothbrush” (Biosci Research America, Inc., Las Vegas, NV, USA) Abstract 0802 IADR, San Diego, California
2010 S. Santos, K. Thai, A. Morris, C. Goyal, N. Sharma, J. McGuire, S. Demissie and J.
Qaqish (Johnson & Johnson Consumer & Personal Products Worldwide, Morris Plains, NJ “Comparability of Two Marketed Toothbrushes on Dental Plaque Removal” Abstract 1710 IADR, Barcelona, Spain
2010 S. Farrell, J.M. Grender, J.E. Rooney, A.R. Biesbrock, C. Goyal and J. Qaqish (The
Procter & Gamble Company, Mason, OH, USA)”Gingivitis Reduction Following 4- Week Use of Three Sonic Rechargeable Toothbrushes” Abstrace 1717 IADR Barcelona, Spain
2010 J. Strate, C. Goyal, M. Olson, J. Wei, and W. Jenkins (Philips Oral Healthcare,
Snoqualmie, WA, USA) “Plaque Removal Efficacy of Three Sonic Power Toothbrushes” Abstract 1720 IADR, Barcelona Spain
2010 A. Morris*, S. Santos, B. Lemli, J. Edelstein, N. Sharma, C. Goyal, J.A. McGuire, J.
Qaqish, A. Hee and J. Knutzen (Johnson & Johnson Consumer & Personal Products Worldwide, Morris Plains, NJ, USA) “Comparative Evaluation of Three Manual Toothbrushes for Removing Dental Plaque” Abstract 1130 AADR, Washington, DC
2010 A. Morris, S. Santos, C. Goyal, N. Sharma, J. Qaqish, S. Demissie, J.A. McGuire, B.
Lemli, J. Edelstein and C. Charles* (Johnson & Johnson Consumer & Personal Products Worldwide, Morris Plains, NJ, USA) “Efficacy of Two New REACH® Manual Toothbrushes for Dental Plaque Removal” Abstract 1131 AADR, Washington, DC
2009 C.R. Goyal, J. Qaqish, Tao He, Julie Grender, Pat Walters, Aaron R. Biesbrock “A Randomized 12-Week Study to Compare the Gingivitis and Plaque Reduction Benefits of a Rotation-Oscillation Power Toothbrush” J. Clin. Den Vol XX Number 3,
2009. 2009 A. Morris, S. Santos*, K. Sinatra, M. Cronin, C.R. Goyal, N. Sharma, W. Dembling, K.
Qaqish, J. Qaqish, R. Perfekt, M-M. Wu, S. Demisse, J.A. McGuire, C. Gell, D. Queiroz and J. Coelho (Johnson & Johnson Consumer & Personal Healthcare Products Worldwide, Division of Johnson & Johnson Consumer Companies, Morris Plains, NJ USA) “Plaque Removal of a Revolutionary Monofilament Floss with Flexible Micro- grooves Abstract 1574 IADR Miami, Florida
2009 S. Santos, A. Morris, J. Edelstein*, B. Lemli, C.R. Goyal, N. Sharma, J. Qaqish, P.
Peng, J. McGuire and J. Coelho (Johnson & Johnson Consumer & Personal Products
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 106 of 179
Worldwide, Skillman, NJ, USA) “Comparative Effecacy of Two Manual Toothbrushes on Gingivitis and Plaque” Abstract 2590 IADR Miami, Florida
2008 “Controlling Oral Malodor Following Two-Week Use of a Fluoride Mouthrinse” A.
Morris, S. Santos, J. Coelho, J.A. McGuire, R. Perfekt, J. Qaqish and C.R.Goyal Abstract 3356 IADR Toronto
2008 Biesbrock AR, Walters PA, Bartizek RD, Goyal CR, Qaqish JG “Plaque Removal
Efficacy of an Advanced Rotation-Oscillation power Toothbrush Versus a New Sonic Toothbrush” AMJ Dent June 2008 Vol. 21 No. 3, 185-188
2008 S. Santos, J.A. McGuire, R. Perfekt, C. Beneduce, J. Qaqish, C.R. Goyal “Reducing
Oral Malodor with a Fluoride- and Zinc-containing Mouthrinse” Abstract 0147 AADR Dallas
2008 S.J. Blanchard, M. Harris, J.F. Coelho, J. Qaqish, C.R. Goyal and P. Amini “Plaque
Removal Efficacy of a Novel Toothbrush” Abstract 1162 AADR Dallas 2007 Aaron R. Biesbrock, Robert D. Bartizek, Patricia A. Walters, Paul R. Warren,
MaryAnn Cugini, C.R. Goyal, J. Qaqish “Clinical Evaluations of Plaque Removal Efficacy: An Advanced Rotating-Oscillating Power Toothbrush versus a Sonic Toothbrush” J. Clin. Den.Vol. XV111, Number 4, 2007
2007 C. Ram Goyal, Jimmy G. Qaqish, Jack Galustians, Katherine Ortblad “Efficacy and
Safety of a New Power Toothbrush in a Population with Mild to Moderate Gingivitis” J. Clin. Den. Vol XVIII, Number 3, 2007 2007 T.A. Lisante, S. Santos, J. McGuire, R. Perfekt, M.W.B. Araujo, M.C. Lynch, J.
Qaqish, C.R. Goyal “Vanilla-Mint mouthrinse Reduces and Controls Oral Malodor Using Hedonic Methodology” Abstract 2204 IADR New Orleans
2007 C. Charles, T. Lisante, Q. Zhao, J. Qaqish, M.C. Lynch, C.R. Goyal and N. Sharma
“Two Efficacy Studies of a Children’s Pre-brush Plaque Tinting Mouthrinse” Abstract 2206 IADR New Orleans
2007 C. Beneduce, S. Santos, M-M. Wu, R. Perfekt, M. Lynch, L. Bailey, J. Krawczuk, J. Qaqish and C.R. Goyal “Efficacy of an Essential-oil-containing Mouthrinse in Controlling Oral Malodor” Abstract 2207 IADR New Orleans 2006 Goyal CR1, Qaqish J, 1 Galustians J1, Ortblad K2 “Efficacy and Safety of Ultreo in a
Population with Mild to Moderate Gingivitis” ” 1BioSci Research Canada Ltd., Mississauga, Ontario; 2 Ultreo Inc., Redmond, Washington
2006 Goyal CR, 1 Qaqish J1, Galustians J1, Ortblad K2 “Assessing the Ability of Ultreo to
Remove Extrinsic Surface Stain from the Teeth” 1BioSci Research Canada Ltd., Mississauga, Ontario; 2 Ultreo Inc., Redmond, Washington
2006 C.R. Goyal, N. Sharma, J. Qaqish, M. Cugini, M.C. Thompson and P. Warren “Plaque Removal of a Power Toothbrush Compared to Manual Toothbrushing” Abstract
2045, ADEA/AADR/CADR Orlando 2006 C.R. Goyal, N. Sharma, J. Qaqish, M. Cugini, M.C. Thompson and P.R. Warren
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 107 of 179

“Comparison of Two Power Toothbrushes Versus Manual Toothbrushing” Abstract 2043 ADEA/AADR/CADR Orlando 2006 N. Sharma, C. Goyal, J. Qaqish, M. Cugini, M.C. Thompson and P.R. Warren “Plaque Removal of a Novel Manual Toothbrush” Abstract 2046 ADEA/AADR/CADR Orlando 2006 C.R. Goyal, N. Sharma, J. Qaqish, M. Cugini, M.C. Thompson and P.R. Warren “Approximal Plaque Removal of Two Toothbrushes Incorporating Novel Textured Elements” Abstract 2039 ADEA/AADR/CADR Orlando 2006 C. Goyal, N. Sharma, J. Qaqish, M. Cugini, M.C.Thompson and P.R. Warren “Evaluation of the Plaque Removal Efficacy of Two Power Toothbrushes” Abstract 2047 ADEA/AADR/CADR Orlando 2006 C. Goyal, N. Sharma, H. Galustians, J. Qaqish, M.Cugini, M.C. Thompson and P.R. Warren “Comparative Plaque Removal of a Manual and Two Battery Toothbrushes” Abstract 0572 ADEA/AADR/CADR 2005 C. Ram Goyal, Jimmy G. Qaqish, Naresh C. Sharma, Paul R. Warren, MaryAnn
Cugini, Maureen C. Thompson “Plaque Removal Efficacy of a Novel Tooth Wipe” J. Clin. Den 2005 Vol XVI, No. 2
2005 N.C. Sharma, C.R. Goyal, J.G. Qaqish, M.A. Cugini, M.C. Thompson, P.R. Warren “Single-use Plaque Removal Efficacy of Three Power Toothbrushes” Journal of Dentistry June 2005, Vol 33 Suppl. 1 2005 N.C. Sharma, J.G. Qaqish, H.J. Galustians, C.R. Goyal, M.A. Cugini, M.C. Thompson, P.R. Warren “Plaque Removal Efficacy of Two Electric Toothbrushes with Different Brush Head Designs” Journal of Dentistry June 2005, Vol 33 Suppl. 1 2005 C.R. Goyal, N.C. Sharma, J.G. Qaqish, M.A. Cugini, M.C. Thompson, P.R. Warren “Efficacy of a Novel Brush Head in the Comparison of Two Power Toothbrushes on Removal of Plaque and Naturally Occuring Extrinsic Stain” Journal of Dentistry June 2005, Vol 33 Suppl. 1 . 2005 Goyal CR, Sharma NC, Qaqish JG, Cugini MA, Thompson M, Warren, PR
“Evaluation of Plaque Removal Efficacy of Three Power Toothbrushes” J Den Res 2005; 84 (Spec Iss A) Abstract 0934
2005 Qaqish JG, Sharma NC, Goyal CR, Thompson M., Warren PR, Cugini MA, “Safety
and Efficacy of Two Whitening Strip Products” J Den Res 2005; 84 (Spec Iss A), Abstract 2121
2004 P.R. Warren, M.A. Cugini, M.C. Thompson, R.C. Goyal, J.G. Qaqish, H.G.
Galustians, N.C. Sharma “Plaque Removal Efficacy of a Novel Tooth Cleaning Device” I.A.D.R. Abstr. 0861
2004 N.C. Sharma, J.G. Qaqish, H.J. Galustians, C.R. Goyal, M.A. Cugini, M.C.
Thompson, P.R. Warren “Plaque Removal Efficacy of Two Toothbrushes with Differing Brush Head Size” I.A.D.R. Abstr. 0856
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 108 of 179
2004 C.R. Goyal, J.G. Qaqish, N.C. Sharma, M.A. Cugini, M.C. Thompson, P.R. Warren “Efficiency of Three Toothbrushes Assessed with Two Plaque Indices” I.A.D.R. Abstr. 0868
2003 Cugini MA, Warren PR, Qaqish JG, Goyal CR, Sharma NC. “Plaque Removal Efficacy of Three Power Toothbrushes” J Clin Periodontal 2003; 30 (Suppl 4) :53, I. Abstr. 198
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 109 of 179

Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 110 of 179
* Client contact. * Primary liaison for clients interested in research studies. * Co-ordinate the execution of study. * Supervise and train technicians. * Study and personnel scheduling. * Delegate clinical duties to study personnel * Conduct preliminary data analysis. * Author final project reports. * IRB liaison. * Biostatistician liaison. * Study case report development. * Oversee study subject recruitment. * Project/Study pricing. * ISO Management Team Member. * Attend research conferences.
2001-2014 BioSci Research Canada, Ltd. Mississauga, ON Canada Manager, Clinical Operations Responsibilities:
* Develop study protocol. * Oversee research studies. * Client contact. * Primary liaison for clients interested in research studies. * Co-ordinate the execution of study. * Supervise and train technicians. * Delegate clinical duties to study personnel * Conduct preliminary data analysis. * Author final project reports.
1996-2000 BioSci Research Canada, Ltd. Mississauga, ON Canada Group Leader-Dental Clinical Research Responsibilities:
* Develop study protocol. * Coordinate the execution of study. * Responsible for product dispensary. * Supervise and train technicians. * Delegate clinical duties to study personnel * Instruct subjects on study guidelines. * Conduct preliminary data analysis. * Author final project reports.
1992-1996 BioSci Research Canada, Ltd. Mississauga, ON Canada Project Leader-Dental clinical research
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 111 of 179
Responsibilities:
* Coordinate the execution of study. * Responsible for product dispensary. * Instruct subjects on study guidelines. * Conduct preliminary data analysis. * Author final project reports.
EDUCATIONAL QUALIFICATIONS 1991-Present Computer proficency in DOS and Microsoft systems and software for word
processing, spread sheets and data bases. Safety certification: C.P.R. and Standard First Aid.
GCP Training.
Bi-lingual: English, Arabic.
1991 Bachelor of Science -Biology and Physical Anthropology (double major) University of Toronto Toronto (Erindale), ON Canada 1987 Ontario Secondary School Honour Graduation Diploma Chaminade College School Toronto, ON Canada
* Ontario Scholar - Mathematics award 1987 PROFESSIONAL MEMBERSHIPS International Association of Dental Research Canadian Association of Dental Research International Society of Breath Odor Research RECENT PUBLICATIONS 2018 C.R. Goyal1, M. Klukowska2, JG Qaqish 1, R, Eusebio, A.Wilberg, M. Gabbard,
(1Procter & Gamble Co., Mason, OH, USA; 2 All Sum Research Center Ltd., Canada) “Extrinsic Stain Removal by Non-Peroxide Sodium Hexametaphosphate Rinse” Abstract #0748 AADR/CADR, Fort Lauderdale, Florida, USA, March 22, 2018
2018 S. Santos, C.R. Goyal, J. Qaqish, J. Bowman, A. Sacarello, H. Katz, P. Rubin, (1H.
Katz, Dr Harold Katz, LLC, Los Angeles, CA, USA; 2All Sum Research Center Ltd., Canada); 3SLS Clinical Research Consulting LLC, Pine Brook, NJ, USA; 4J.Bowman,
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 112 of 179
James P Bowman and Associates, Loveland, Ohio, USA “Three Week Clinical Efficacy of Chlorine Dioxide-Containing Mouthrinse on Oral Malodor” Abstract 0752, AADR/CADR, Fort Lauderdale, Florida, USA, March 22, 2018
2018 M. Klukowska2, C.R. Goyal1, T. He, JG Qaqish 1, S. Xie, C. Haught, S. Tansky, T,.
Huggins, D. Ramsey, R, Eusebio, C. Combs, D White, (1Procter & Gamble Co., Mason, OH, USA; 2 All Sum Research Center Ltd., Canada) “The Effect of SnF2 Dentifrice on Virulence of Subgingival Plaque” Abstract #0755 AADR/CADR, Fort Lauderdale, Florida, USA, March 22, 2018
2017 L. Friesen, T.He, M. Klukowska, R,Eusebio, H. Eynon, J. Qaqish, C.R. Goyal,
(1University of Missouri, Kansas City; 2Oral Health Care, Procter & Gamble Company, Mason, Ohio, USA; 3All Sum Research Center Ltd., Canada) “Comparative Anti-plaque Effect of Two Antimicrobial Dentifrices” J Clin Dent 2017;28 (Spec Iss B);B6-11)
2017 T.He, R,Eusebio, J. Qaqish, C.R. Goyal, (1Oral Health Care, Procter & Gamble
Company, Mason, Ohio, USA; 2All Sum Research Center Ltd., Canada) “Assessment of the Effects of a Novel Stabilized Stannous Fluoride Dentifrice on Gingivitis in a Two-Month Positive-Controlled Clinical Study” J Clin Dent 2017;28 (Spec Iss B);B12-16)
2017 L. Friesen, T.He, M. Klukowska, R,Eusebio, H. Eynon, J. Qaqish, C.R. Goyal,
(1University of Missouri, Kansas City; 2Oral Health Care, Procter & Gamble Company, Mason, Ohio, USA; 3All Sum Research Center Ltd., Canada) “Comparative Anti-plaque Effect of Two Antimicrobial Dentifrices” Oral Session, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 A. Gassemi, L.M. Vorwerk, W. Hooper, W. Hooper, A. Buelo, J. Qaqish, C.R. Goyal,
(1Church & Dwight Co., Inc., Princeton, NJ, USA; 2All Sum Research Center Ltd., Canada ) “Single-brushing Plaque Removal Efficacy Evaluation” Abstract 0883, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 C.R. Goyal, Deborah M. Lyle, JG Qaqish, Reinhard Schuller, (1Water Pik Inc. Fort
Collins, CO, USA; 2All Sum Research Center Ltd., Canada) “Efficacy of Two Interdental Cleaning Devices on Clinical Signs of Inflammaton: A Randomized Controlled Trial” Abstract 0883, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 S. Santos, C.R. Goyal, JG. Qaqish, J. Bruns, K. Yost, R. Schuller, (1Ranir Global LLC,
Grand Rapids, Michigen, USA; 2All Sum Research Center Ltd., Canada); 3SLS Clinical Research Consulting LLC, Pine Brook, NJ, USA “Comparison of a Water Flosser and Manual Brushing to Manual Brushing Only: A Four Week Randomized Controlled Trial” Abstract 0886, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 C.R. Goyal, Deborah M. Lyle, JG Qaqish, Reinhard Schuller, (1Water Pik Inc. Fort
Collins, CO, USA; 2All Sum Research Center Ltd., Canada) “Cost Effective Plaque and Gingivitis Reduction through Brush-Floss-Rinse Regimen” Abstract 0887, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 113 of 179

2017 C.R. Goyal, J. Qaqish, T.He, M. Klukowska, JL. Winston, (1Oral Health Care, Procter & Gamble Company, Mason, Ohio, USA; 2All Sum Research Center Ltd., Canada) “Clinical Anti-Gingivitis Efficacy of a 0.454% SnF2 Dentifrice” Abstract 0889, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 C.R. Goyal, J. Qaqish, RA.C. Vasquez, JM. Grender, E. Conde, PA. Cunningham,
(1Oral Health Care, Procter & Gamble Company, Mason, Ohio, USA; 2All Sum Research Center Ltd., Canada) “Efficacy of a Battery Manual Toothbrush removing Dental Stain” Abstract 1532, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 J. Creeth, J. Gallob, J. Qaqish, C.R. Goyal, F. Sufi, N. Patel, (1GSK Consumer
Healthcare, Weybridge, UK; 2Silverstone Research Group, LV, USA, 3All Sum Research Center Ltd., Canada) “Short-Term Efficacy Studies of an Occluding Dentifrice on Dentinal Hypersensitivity” Abstract 1543, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 C.R. Goyal, F. Sufi, J. Qaqish, J. Creeth, (1All Sum Research Center Ltd., Canada;
2GSK Consumer Healthcare, Weybridge, UK) “Two-Week Efficacy of an Occluding Dentifrice on Dentinal Hypersensitivity” Abstract 1544, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2017 N. Gurich, M. Anastasia, C.R. Goyal, J. Qaqish, (1Oral Health Care, Procter &
Gamble Company, Mason, Ohio, USA; 2All Sum Research Center Ltd., Canada) “Clinical Trial to Evaluate Efficacy of Whitening Dentifrice” Oral Session, IADR/AADR/CADR, San Francisco, Calif, USA, March 22-25, 2017
2016 T.He, J. Qaqish, C.R. Goyal, M.K. Anastasia, R. Eusebio (Oral Health Care, Procter &
Gamble Company, Mason, Ohio, USA; 2All Sum Research Center Ltd., Canada) “Comparative Extrinsic Stain Removal Efficacy of Two Whitening Dentifrice” Abstract #0476 AADR, Los Angeles, Calif, USA, March 17, 2016
2016 C.R. Goyal, Deborah M. Lyle, JG Qaqish, Reinhard Schuller, (1Water Pik Inc. Fort
Collins, CO, USA; 2All Sum Research Center Ltd., Canada) “Comparison of Water Flosser and Interdental Brush on Reduction of Gingival Bleeding and Plaque: A Randomized Controlled Pilot Study” Abstract J Clin Dent 2016: 27:61-65
2016 L. Friesen, T.He, M.K. Anastasia, R. Eusebio, J. Qaqish, C.R. Goyal, (University of
Missouri, Kansas City; 2Oral Health Care, Procter & Gamble Company, Mason, Ohio, USA; 3All Sum Research Center Ltd., Canada) “Stain Removal Efficacy of a Whitening Dentifrice Versus Marketed Control” Abstract #0475 AADR, Los Angeles, Calif, USA, March 17, 2016
2016 T.He, J. Qaqish, C.R. Goyal, M.K. Anastasia, R. Eusebio (Oral Health Care, Procter &
Gamble Company, Mason, Ohio, USA; 2All Sum Research Center Ltd., Canada) “Superior Extrinsic Stain Removal Efficacy of a Whitening Dentifrice” Abstract #0472 AADR, Los Angeles, Calif, USA, March 17, 2016
2016 A. Gassemi, L.M. Vorwerk, W. Hooper, W. Hooper, M. Kwang, J. Qaqish, C.R. Goyal,
M. Naji (Church & Dwight Co., Inc., Princeton, NJ, USA; 2All Sum Research Center Ltd., Canada) “Plaque Removal Efficacy Evaluation and Comparison of Three Manual
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 114 of 179
Toothbrushes” Abstract 0456, AADR, Los Angeles, Calif, USA, March 17, 2016. Abstract J Clin Dent 2016: 27:71-75
2016 C.R. Goyal, Deborah M. Lyle, JG Qaqish, Reinhard Schuller, (1Water Pik Inc. Fort
Collins, CO, USA; 2All Sum Research Center Ltd., Canada) “Comparison of Two Interdental Cleaning Devices: A Pilot Study” Abstract #0465 AADR, Los Angeles, Calif, USA, March 17, 2016
2015 C.R. Goyal, Deborah M. Lyle, JG Qaqish, Reinhard Schuller, (1Water Pik Inc. Fort
Collins, CO, USA; 2All Sum Research Center Ltd., Canada) “Efficacy of Two Interdental Cleaning Devices on Clinical Signs of Inflammation: A Four-Week Randomized Controlled Trial” Abstract J Clin Dent 2015: 26:55-60, 2015
2015 RA Ccahuana-Vasquez1, JM Grender2, E. Conde, P. Cunningham, C.R. Goyal, JG
Qaqish (1Procter & Gamble Co., Kronberg, Germany; 2Procter & Gamble Co.,Mason, OH, USA; All Sum Research Center Ltd., Canada) “An Eight-Week Clinical Evaluation of an Oscillating-Rotating Power Toothbrush with a Brush Head Utilizing Angled Bristles Compared with a Sonic Toothbrush in the Reduction of Gingivitis and Plaque”Abstract J Clin Dent 2015: 26:80-85, 2015
2013 C.R. Goyal, Deborah M. Lyle, JG Qaqish, Reinhard Schuller, (1Water Pik Inc. Fort
Collins, CO, USA; 2BioSci Research Canada Ltd., Canada) “Evaluation of the Plaque Removal Efficacy of a Water Flosser Compared to String Floss in Adults After a Single Use” Abstract J Clin Dent 2013: 24:37-42, July 21, 2013
2013 M. Klukowska1, C.R. Goyal2, JG Qaqish 3, (1Procter & Gamble Co., Mason, OH, USA;
2BioSci Research Canada Ltd., Canada) “Anti-Gingivitis Effect of Combined Antimicrobial and Mechanical Oral Hygiene” Abstract #1301 IADR, Seattle, Washington, USA, March 21, 2013
2012 RA Ccahuana-Vasquez1, MA Klukowska2, A. Mielczarek3, Goyal4, JG Qaqish 4, JM
Grender2 (1Procter & Gamble Co., Kronberg, Germany; 2Procter & Gamble Co., Mason, OH, USA; 3Medical University, Warsaw, Poland; 4BioSci Research Canada Ltd., Canada) “Plaque and Gingivitis Reduction on Surfaces by Novel Toothbrush”
Abstract #209 PER/IADR Congress, Helsinki, Finland, September 12-15, 2012 2012 R. Adam*1, MA Klukowska1, Goyal2, JG Qaqish2, JM Grender1 (1Procter &
Gamble Co., Mason, OH USA, 2BioSci Research Canada Ltd., Canada) “Gingival Bleeding Reduction on Lingual and Approximal Surfaces by a Novel Toothbrush”
Abstract #214 PER/IADR Congress, Helsinki, Finland, September 12-15, 2012 2012 MA Klukowska*1, Goyal2, JM Grender1, P Cunningham1, JG Qaqish2, A Biesbrock1 (1 Procter & Gamble Co., Mason, OH, USA, 2 BioSci Research Canada Ltd., Canada) “Comparative Anti-Gingivitis Efficacy of Oscillation-Rotation and Sonic Power
Toothbrush” Abs tract #524 PER/IADR Congress, Helsinki, Finland, September 12- 15, 2012
2012 N.C. Sharma, M. Klukowska, A. Mielczarek, J.MN. Grender & J. Qaqish “A 4-Week
Clinical Comparison of a Novel Multi-Directional Power Brush to a Manual Toothbrush in the Reduction of Gingivitis and Plaque” AJD Volume 25, Special Issue A, September 2012
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 115 of 179
2012 C.R. Goyal, M Klukowska, J.M Grender, P. Cunningham & J. Qaqish “Evaluation of a New Multi-directional Power Toothbrush Versus a Marketed Sonic Toothbrush on Plaque and Gingivitis Efficacy” AJD, Volume 25, Special Issue A, September 2012
2012 M. Klukowska, J.M. Grender, C.R. Goyal, J. Qaqish & A.R. Biesbrock “8-week
Evaluation of Anti-Plaque and Anti-Gingivitis Benefits of a Unique Multi-Directional Power Toothbrush Versus a Sonic Control Toothbrush” AJD, Volume 25, Special Issue A, September 2012
2012 Tao He, DDS, PhD, Matthew L. Barker, PhD, A.R. Biesbrock, DMD, PhD, MS,
Procter & Gamble Company, Mason , OH, USA, N.C. Sharma, DDS, J. Qaqish, BSc, C.R. Goyal, DDS, BioSci Research Canada Ltd., Mississauga, Ontario, Canada “Assessment of the Effects of a Stannous Fluoride Dentifrice on Gingivitis in a Two- Month Positive Controlled Clinical Study” J. Clin Dent, Vol. 23, No. 3, 2012.
2012 N. Sharma1, J.E. Pelino2, A.M. Parikh3, Q. Du4, C. Charles3, C.R. Goyal1, M.W.
Araujo3, and J. Qaqish1, 1BioSci Research Canada, Ltd., Mississauga, ON, Canada, 2Johnson & Johnson, CPPW, Sao Paulo, Brazil, 3 Johnson & Johnson, CPPW, Morris
Plains, NJ, 4Johnson & Johnson China, Shanghai, China “Superiority of Essential-Oil vs. 0.075 CPC Rinses: Experiumental Gingivitis Model” Abstract 149 IADR, Iguaçu Falls, Brazil
2012 C. Ram Goyal, Deborah M. Lyle, Jimmy G. Qaqish, Reinhard Schuller “The
Addition of a Water Flosser to Power Tooth Brushing: Effect on Bleeding, Gingivitis, and Plaque” J. Clin. Den. Vol. XXIII, Number 2, 2012
2012 P. Amini, R. Costa*, H. Shang, J. Qaqish, J. Gallob and M.W. Araujo (Johnson &
Johnson Consumer Companies Inc., Morris Plains, NJ, USA) “Antiplaque/Antigingivitis Efficacy of an Alcohol-Free Essential Oil Containing
Mouthrinse” Abstract 0042 IADR Tampa, Florida 2012 A. Ghassemi*, L. Vorwerk, W. Hooper, V. Patel, N. Sharma and J. Qaqish (Church &
Dwight Co., Inc. Princeton, NJ, USA) “Plaque Removal Efficacy of Children’s Powered Toothbrush Versus Manual Toothbrush” Abstract 0353 IADR, Tampa, Florida
2012 S. Farrell*, J.M. Grender, P. Cunningham, N. Sharma and J. Qaqish (Procter &
Gamble Company, Mason, OH, USA) “Effects of Manual Toothbrush with Flexing Elements on Plaque Removal” Abstract 0356 IADR, Tampa, Florida 2012 P. Amini*, J. Qaqish, S. Farrell, J.M. Grender, and P. Cunningham (BioSci Research, Las Vegas, NV, USA) “Effects of Manual Toothbrush with Flexing Elements on
Gingivitis Reduction” Abstract 0357 IADR, Tampa, Florida 2012 M.Barker*, T. He, A.R. Biesbrock, M.C. Miner, C.R. Goyal and J. Qaqish (Procter & Gamble Company, Mason, OH, USA) “2-Month Gingivitis Treatment Comparison of Stannous Fluoride and Triclosan/Copolymer Dentifrices”
Abstract 0742 IADR, Tampa, Florida 2012 T. He*, M. Barker, A. Biesbrock, P. Amini, C. Goyal and J. Qaqish (The Procter &
Gamble Company, Mason, OH, USA) “Superior Anti-gingivitis Benefits of Stannous
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 116 of 179
Fluoride among Triclosan Dentifrice Users” Abstract 0746 IADR, Tampa Florida 2012 P. Amini, M. Barker, S. Barrett, M. Gabbard, A. Walanski* and R. Gerlach (Procter &
Gamble Company, Mason,OH, USA) “6-Week Combination Oral Hygiene Effects on Plaque and Gingivitis” Abstract 0902 IADR, Tampa, Florida
2012 N. Sharma*, J. Qaqish, T. He, M. Barker, M. Miner, H. Eynon and A. Biesbrock
(BioSci Research America, Inc., Las Vegas, NV, USA) “Superior Plaque Reduction Efficacy of a Stannous Fluoride Dentifrice” Abstract 1448 IADR, Tampa, Florida
2012 Naresh C. Sharma, Deborah M. Lyle, Jimmy G. Qaqish, Reinhard Schuller
“Comparison of Two Power Interdental Cleaning Devices on Plaque Removal” J. Clin Den Vol. XXIII, No 1, 2012 2011 C.R. Goyal, J. Qaqish, S. Farrell, J.M. Grender, J.R. Rooney and P. Cunningham
“Plaque and Gingivitis Effects of Sonic Brush with New Brushhead” (BioSci Research Canada, Ltd., Mississauga, Canada) Abstract 0801 IADR, San Diego, California
2011 S. Farrell, J.M. Grender, J.R. Rooney, C.R. Goyal and J. Qaqish “Long Term Plaque
and Gingivitis Reduction Benefits of New Sonic Toothbrush” (Biosci Research America, Inc., Las Vegas, NV, USA) Abstract 0802 IADR, San Diego, California
2011 A. Gassemi, L. Vorwerk, W. Hooper, S. Thong, P. Soparkar, N. Sharma and J. Qaqish
(Church & Dwight Co., Inc., Princeton, NJ, USA) Abstract 0811, IADR, San Diego, California
2011 T.A. Lisante, C. Charles, J. Qaqish and N. Sharma “Efficacy of Brush, Floss, Rinse
Regimens vs. Mechanical Oral Hygiene” (Johnson & Johnson Consumer & Personal Products Worldwide Division of Johnson & Johnson Consumer Companies, Inc, Morris Plains, NJ, USA) Abstract 1320 IADR, San Diego, California
2011 N. Sharma, J. Qaqish, M.L. Barker and T. He “Instant Sensitivity Relief of a Stannous-
containing Sodium Fluoride Dentifrice” (BioSci Research Canada Ltd., Mississauga, Canada) Abstract 1476 IADR San Diego, California
2011 P. Amini, J. Qaqish, E. Conde, M.K. Anastasia, V. Widmeyer and S. Farrell (BioSci Research America, Inc., Las Vegas, NV, USA) “Immediate Effects and Color Degredation Profile of 2-Hour Whitening Strip” Abstract 2539 IADR, San Diego, California
2011 M.L. Barker, N. Sharma, J. Qaqish, J.R. Briesbrock and T. He (The Procter &
Gamble Company, Mason, OH, USA) “RCT Evaluating Onset of Sensitivity Relief for Stannous Fluoride Dentifrice” Abstract 2991 IADR, San Diego, Calilfornia
2011 N.C. Sharma, J. Qaqish, M. Klukowska, J. Grender, J. Rooney “The Plaque Removal
Efficacy of a Novel Power Brush Head” J. Clin. Den. Vol. XXII No. 1, 2011 2010 S. Santos, K. Thai, A. Morris, C. Goyal, N. Sharma, J. McGuire, S. Demissie and J.
Qaqish (Johnson & Johnson Consumer & Personal Products Worldwide, Morris Plains, NJ “Comparability of Two Marketed Toothbrushes on Dental Plaque Removal” Abstract 1710 IADR, Barcelona, Spain
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 117 of 179
2010 H.-C Timm, N. Sharma, J. Qaqish, M. Klukowska, J. Grender, J. Rooney, P. Hoke and P. Cunningham (Procter & Gamle, Kronburg im Taunu, Germany) “Plaque Removal from a Power Toothbrush with Novel Brush Head” Abstract 1716 IADR Barcelona, Spain
2010 S. Farrell, J.M. Grender, J.E. Rooney, A.R. Biesbrock, C. Goyal and J. Qaqish (The
Procter & Gamble Company, Mason, OH, USA)”Gingivitis Reduction Following 4- Week Use of Three Sonic Rechargeable Toothbrushes” Abstract 1717 IADR Barcelona, Spain
2010 S. Farrell, M.K. Anastasia, B.A. Ohmer, V.C. Widmeyer, P. Amini and J. Qaqish
(BioSci Research America Inc., Las Vegas, Nevada, USA) “Relative Efficiency of High-Adhesion Whitening Strips and In-Office Whitening Treatment” Abstract 2374, IADR, Barcelona, Spain
2010 P. Amini, J. Qaqish, M.K. Anastasia, E. Conde, V.C. Widmeyer and S. Farrell (BioSci
Research America Inc., Las Vegas, Nevada, USA) “Clinical Comparison of Take- Home Whitening Strips and Chairside Whitening Procedure” Abstract 2375 IADR Barcelona, Spain
2010 M. Klukowska, N. Sharma, J. Qaqish, J.M. Grender, J.E. Rooney, P.D. Hoke and P.
Cunningham (The Procter & Gamble Company, Mason, OH, USA) “Gingivitis Reduction from a Power Toothbrush with Novel Brush Head” Abstract 3695 IADR, Barcelona, Spain
2010 N.C. Sharma, J. Qaqish, P.A. Walters, J. Grender, A.R. Biesbrock “A Clinical
Evaluation of the Plaque Removal Efficacy of Five Manual Toothbrushes” J. Clin Den Vol XXI Number 1, 2010
2010 K. Simmons*, C. Charles, J. McGuire, A. Hee, J.Qaqish and P. Amini (Johnson &
Johnson Consumer & Personal Products Worldwide Division of Johnson & Johnson Consumer Companies Inc., Morris Plains, NJ, USA) “Efficacy of BRUSH, FLOSS & RINSETM Regimen vs. Mechanical Oral Hygiene” Abstract 0168 AADR, Washington, DC
2010 L. Vorwerk*, A. Ghassemi, W. Hooper, P. Amini, J. Gallob, J. Qaqish and H. Proskin
(Church & Dwight Co. Inc., Princeton, NJ, USA) “Comparative Plaque Removal Efficacy of SpinBrush-Swirl® Battery-powered and Manual Toothbrushes” Abstract 0330 AADR,Washington, DC
2010 A. Ghassemi, W. Hooper*, L. Vorwerk, S. Thong, P. Amini and J. Qaqish (Church &
Dwight Co. Inc., Princeton, NJ, USA) “Comparative Plaque Removal Efficacy of Two Toothbrush-Dentifrice Combinations” Abstract 0333 AADR, Washington, DC
2010 N. Sharma, J. Qaqish, M. Klukowska*, J. Rooney, J. Grender, P. Hoke and P.
Cunningham (The Procter & Gamble Company, Mason, OH, USA) “Plaque Removal by Oscillating-Rotating Power Toothbrush and Manual Toothbrush” Abstract 0599 AADR, Washington, DC
2010 S. Santos*, A. Morris, N. Sharma, J. Edelstein, J. McGuire, A. Hee and J. Qaqish
(Johnson & Johnson Consumer & Personal Products Worldwide, Morris Plains, NJ,
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 118 of 179

USA) “Four-week Evaluation of Toothbrush and Floss Regimen in Reducing Gingivitis” Abstract 1127 AADR, Washington, DC
2010 A. Morris*, S. Santos, B. Lemli, J. Edelstein, N. Sharma, C. Goyal, J.A. McGuire, J.
Qaqish, A. Hee and J. Knutzen (Johnson & Johnson Consumer & Personal Products Worldwide, Morris Plains, NJ, USA) “Comparative Evaluation of Three Manual Toothbrushes for Removing Dental Plaque” Abstract 1130 AADR, Washington, DC
2010 A. Morris, S. Santos, C. Goyal, N. Sharma, J. Qaqish, S. Demissie, J.A. McGuire, B.
Lemli, J. Edelstein and C. Charles* (Johnson & Johnson Consumer & Personal Products Worldwide, Morris Plains, NJ, USA) “Efficacy of Two New REACH® Manual Toothbrushes for Dental Plaque Removal” Abstract 1131 AADR, Washington, DC
2009 C.R. Goyal, J. Qaqish, Tao He, Julie Grender, Pat Walters, Aaron R. Biesbrock “A Randomized 12-Week Study to Compare the Gingivitis and Plaque Reduction Benefits of a Rotation-Oscillation Power Toothbrush” J. Clin. Den Vol XX Number 3,
2009. 2009 A. Morris, S. Santos*, K. Sinatra, M. Cronin, C.R. Goyal, N. Sharma, W. Dembling, K.
Qaqish, J. Qaqish, R. Perfekt, M-M. Wu, S. Demisse, J.A. McGuire, C. Gell, D. Queiroz and J. Coelho (Johnson & Johnson Consumer & Personal Healthcare Products Worldwide, Division of Johnson & Johnson Consumer Companies, Morris Plains, NJ, USA) “Plaque Removal of a Revolutionary Monofilament Floss with Flexible Micro-grooves Abstract 1574 IADR Miami, Florida
2009 A. Morris, J. Gallob*, P. Amini, S. Santos, J. Qaqish, P. Peng, J. McGuire, R. Parikh, M.
Martinez and J. Coelho (BioSci Research America Inc., Las Vegas, NV, USA) “Efficacy of a Potassium Nitrate Mouthrinse for Relieving Dental Hypersensitivity” Abstract 1575 IADR Miami, Florida
2009 P. Amini*, J. Qaqish, M.K. Anastasia, A.J. Hamilton, R.W. Gerlach and S. Farrell (BioSci Research America Inc., Las Vegas, NV. USA) “Clinical Responses of
Experimental Whitening Strips with 6-week Daily Use” Abstract 2277 IADR Miami, Florida
2009 N. Sharma, J. Qaqish*, T. He, P. Walters, J. Grender and A. Biesbrock (BioSci
Research Canada Ltd., Mississauga, ON Canada “Comparative Anti-gingivitis Effects of Sonic Rechargeable and Manual Toothbrushes” Abstract 2588 IADR Miami, Florida
2009 S. Santos, A. Morris, J. Edelstein*, B. Lemli, C.R. Goyal, N. Sharma, J. Qaqish, P.
Peng, J. McGuire and J. Coelho (Johnson & Johnson Consumer & Personal Products Worldwide, Skillman, NJ, USA) “Comparative Efficacy of Two Manual Toothbrushes on Gingivitis and Plaque” Abstract 2590 IADR Miami, Florida
2009 T.A. Lisante*, J. Askinazi, K. Simmons, C. Charles, J.T. McGuire, J. Qaqish and N.
Sharma (Johnson & Johnson Consumer & Personal Products Worldwide, Morris Plains, NJ, USA) “Comparative Whitening Effectiveness of Three Hydrogen-peroxide- containing Mouthrinses” Abstract 2597 IADR Miami, Florida
2009 John Gallob DDS, Pejmon Amini DDS, Jimmy Qaqish BS, Pat Chaknis BS, James A.
Kemp BA ans William DeVizio DMD “A Clinical Study to Determine the Tooth Hypersensitivity Reduction in Subjects Who Brushed with the New Colgate 360º
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 119 of 179

Sensitive Toothbrush” Compendium of Continued Education in Dentistry” July/August 2009 – Vol 30, Iss. 6
2008 Biesbrock AR, Walters PA, Bartizek RD, Goyal CR, Qaqish JG “Plaque Removal
Efficacy of an Advanced Rotation-Oscillation power Toothbrush Versus a New Sonic Toothbrush” AMJ Dent June 2008 Vol. 21 No. 3, 185-188
2008 Naresh C. Sharma, Deborah M. Lyle, Jimmy G. Qaqish, Jack Galustians and Reinhard
Schuller “Effect of a Dental Water Jet with Orthodontic Tip on Plaque and Bleeding in Adolescent Patients with Fixed Orthodontic Appliances” Am J Ortho Dentof Orthop 2008, 133(4):565-571 Vol 133 Number 4, April 2008
2008 “Controlling Oral Malodor Following Two-Week Use of a Fluoride Mouthrinse” A.
Morris, S. Santos, J. Coelho, J.A. McGuire, R. Perfekt, J. Qaqish and C.R.Goyal Abstract 3356 IADR Toronto
2008 S. Santos, J.A. McGuire, R. Perfekt, C. Beneduce, J. Qaqish, C.R. Goyal “Reducing
Oral Malodor with a Fluoride- and Zinc-containing Mouthrinse” Abstract 0147 AADR Dallas
2008 S.J. Blanchard, M. Harris, J.F. Coelho, J. Qaqish, C.R. Goyal and P. Amini “Plaque
Removal Efficacy of a Novel Toothbrush” Abstract 1162 AADR Dallas 2007 Aaron R. Biesbrock, Robert D. Bartizek, Patricia A. Walters, Paul R. Warren,
MaryAnn Cugini, C.R. Goyal, J. Qaqish “Clinical Evaluations of Plaque Removal Efficacy: An Advanced Rotating-Oscillating Power Toothbrush versus a Sonic Toothbrush” J. Clin. Den.Vol.XV111, Number 4, 2007
2007 C. Ram Goyal, Jimmy G. Qaqish, Jack Galustians, Katherine Ortblad “Efficacy and
Safety of a New Power Toothbrush in a Population with Mild to Moderate Gingivitis” J. Clin. Den. Vol XVIII, Number 3, 2007 2007 S. Santos, C. Beneduce, J. McGuire, R. Perfekt, M.W.B. Araujo, J. Qaqish, M.C.
Lynch and N. Sharma “Antiplaque/Antigingivitis Efficacy of Vanilla Mint Listerine Antiseptic” Abstract 2483 IADR New Orleans
2007 C. Charles, T. Lisante, Q. Zhao, J. Qaqish, M.C. Lynch, C.R. Goyal and N. Sharma
“Two Efficacy Studies of a Children’s Pre-brush Plaque Tinting Mouthrinse” Abstract 2206 IADR New Orleans
2007 T.A. Lisante, S. Santos, J. McGuire, R. Perfekt, M.W.B. Araujo, M.C. Lynch, J.
Qaqish, C.R. Goyal “Vanilla-Mint mouthrinse Reduces and Controls Oral Malodor Using Hedonic Methodology” Abstract 2204 IADR New Orleans
2007 C. Beneduce, S. Santos, M-M. Wu, R. Perfekt, M. Lynch, L. Bailey, J. Krawczuk, J. Qaqish and C.R. Goyal “Efficacy of an Essential-oil-containing Mouthrinse in Controlling Oral Malodor” Abstract 2207 IADR New Orleans 2006 Sharma NC, 1 Qaqish J, 1 Galustians J1, Ortblad K2 “Efficacy of Ultreo in Dental
Plaque Removal” 1BioSci Research Canada Ltd., Mississauga, Ontario; 2 Ultreo Inc., Redmond, Washington
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 120 of 179

2006 Goyal CR1, Qaqish J, 1 Galustians J1, Ortblad K2 “Efficacy and Safety of Ultreo in a Population with Mild to Moderate Gingivitis” ” 1BioSci Research Canada Ltd., Mississauga, Ontario; 2 Ultreo Inc., Redmond, Washington
2006 Goyal CR, 1 Qaqish J1, Galustians J1, Ortblad K2 “Assessing the Ability of Ultreo to
Remove Extrinsic Surface Stain from the Teeth” ” 1BioSci Research Canada Ltd., Mississauga, Ontario; 2 Ultreo Inc., Redmond, Washington
2006 C.R. Goyal, N. Sharma, J. Qaqish, M. Cugini, M.C. Thompson and P. Warren “Plaque Removal of a Power Toothbrush Compared to Manual Toothbrushing” Abstract
2045, ADEA/AADR/CADR Orlando 2006 N. Sharma, J. Qaqish, M. Cugini, M.C. Thompson and P.R. Warren “”Plaque Removal of Three Power Toothbrushes” Abstract 2054 ADEA/AADR/CADR Orlando 2006 C.R. Goyal, N. Sharma, J. Qaqish, M. Cugini, M.C. Thompson and P.R. Warren “Comparison of Two Power Toothbrushes Versus Manual Toothbrushing” Abstract 2043 ADEA/AADR/CADR Orlando 2006 N. Sharma, C. Goyal, J. Qaqish, M. Cugini, M.C. Thompson and P.R. Warren “Plaque Removal of a Novel Manual Toothbrush” Abstract 2046 ADEA/AADR/CADR Orlando 2006 C.R. Goyal, N. Sharma, J. Qaqish, M. Cugini, M.C. Thompson and P.R. Warren “Approximal Plaque Removal of Two Toothbrushes Incorporating Novel Textured Elements” Abstract 2039 ADEA/AADR/CADR Orlando 2006 C. Goyal, N. Sharma, J. Qaqish, M. Cugini, M.C.Thompson and P.R. Warren “Evaluation of the Plaque Removal Efficacy of Two Power Toothbrushes” Abstract 2047 ADEA/AADR/CADR Orlando 2006 C. Goyal, N. Sharma, H. Galustians, J. Qaqish, M.Cugini, M.C. Thompson and P.R. Warren “Comparative Plaque Removal of a Manual and Two Battery Toothbrushes” Abstract 0572 ADEA/AADR/CADR 2006 M.A. Cugini, M.C. Thompson, P.R. Warren, N.C. Sharma, J.G. Qaqish “Clinical Evaluation of the Plaque Removal Efficacy of Three Toothbrushes” Abstract 1297 2005 C. Ram Goyal, Jimmy G. Qaqish, Naresh C. Sharma, Paul R. Warren, MaryAnn Cugini,
Maureen C. Thompson “Plaque Removal Efficacy of a Novel Tooth Wipe” J. Clin. Den 2005 Vol XVI, No. 2
2005 N.C. Sharma, C.R. Goyal, J.G. Qaqish, M.A. Cugini, M.C. Thompson, P.R. Warren “Single-use Plaque Removal Efficacy of Three Power Toothbrushes” Journal of Dentistry June 2005, Vol 33 Suppl. 1 2005 N.C. Sharma, J.G. Qaqish, H.J. Galustians, C.R. Goyal, M.A. Cugini, M.C. Thompson, P.R. Warren “Plaque Removal Efficacy of Two Electric Toothbrushes with Different Brush Head Designs” Journal of Dentistry June 2005, Vol 33 Suppl. 1 2005 C.R. Goyal, N.C. Sharma, J.G. Qaqish, M.A. Cugini, M.C. Thompson, P.R. Warren “Efficacy of a Novel Brush Head in the Comparison of Two Power Toothbrushes on Removal of Plaque and Naturally Occuring Extrinsic Stain” Journal of Dentistry June
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 121 of 179

2005, Vol 33 Suppl. 1 2005 Goyal CR, Sharma NC, Qaqish JG, Cugini MA, Thompson M, Warren, PR “Evaluation
of Plaque Removal Efficacy of Three Power Toothbrushes” J Den Res 2005; 84 (Spec Iss A) Abstract 0934.
2005 Sharma NC, Qaqish JG, Cugini MA, Warren PR, Thompson M. “Clinical Comparison
of Extrinsic Stain Removal by Two Power Toothbrushes” J Den Res 2005 84 (Spec Iss A) Abstract 0935.
2005 Sharma NC, Qaqish JG, Cugini MA, Thompson M, Warren PR. “Evaluation of Plaque
Removal Efficacy of Two Power Toothbrushes” J Den Res 2005; 84 (Spec Iss A) Abstract 9036.
2005 Qaqish JG, Sharma NC, Goyal CR, Thompson M., Warren PR, Cugini MA, “Safety and
Efficacy of Two Whitening Strip Products” J Den Res 2005; 84 (Spec Iss A), Abstract 2121
2005 Naresh C. Sharma, DDS, Jimmy G. Qaqish, BSc, H. Jack Galustians, BSc, MaryAnn
Cugini, RDH, MHP, Maureen C. Thompson, RDH, BS & Paul R.Warren, LDS “Plaque Removal Efficacy and Safety of the Next Generation of Manual Toothbrush with Angled Bristle Technology: Results from Three Compatative Clinical Studies” AJD Vol. 18, No. 1 3-7, Feb 2005
2004 Naresh Sharma, DMD, H. Jack Galustians, BS, Jimmy Qaqish, BS, BioSci Research
Canada Ltd., Mississauga, Ontario, Canada; Kedar Rustogi DDS, Yun Po Zhang, PhD, Margaret E. Petrone, JD, William DeVizio, DMD, Colgate-Palmolive Technology Center, Piscataway, NJ, USA; Howard Proskin, PhD, H.M. Proskin & Associates, Inc., Rochester, NY, USA “Comparative Tooth Whitening and Extrinsic Tooth Stain Preventation Efficacy of a New Dentifrice and a Commercially Available Tooth Whitening Dentifrice: Six-Week Clinical Trial” J. Clin Den. Vol. 15, 52-57, 2004
2004 N. Sharma, D.D.S., B.D.S.; C.H. Charles, B.S., R.D.H.; M.C. Lynch, D.M.D., Ph.D.; J. Qaqish, B.S.; J.A. McGuire, M.S.; J.G. Galustians; L.D. Kumar, PhD “Adjunctive Benefit of an Essential-oil Containing Mouthrinse in Reducing Plaque and Gingivitis in Patients who Brush and Floss Regularly” JADA Vol. 135, 496-504, April 2004. 2004 P.R. Warren, M.A. Cugini, M.C. Thompson, R.C. Goyal, J.G. Qaqish, H.G. Galustians,
N.C. Sharma “Plaque Removal Efficacy of a Novel Tooth Cleaning Device” I.A.D.R. Abstr. 0861
2004 J. Strate, M.A. Cugini, P.R. Warren, J.G. Qaqish, H.J. Galustians, N.C. Sharma “Plaque
Removal Efficacy of Two Power Toothbrushes” I.A.D.R. Abstr. 0863 2004 N.C. Sharma, J.G. Qaqish, H.J. Galustians, C.R. Goyal, M.A. Cugini, M.C. Thompson,
P.R. Warren “Plaque Removal Efficacy of Two Toothbrushes with Differing Brush Head Size” I. A.D.R. Abstr. 0865
2004 C.R. Goyal, J.G. Qaqish, N.C. Sharma, M.A. Cugini, M.C. Thompson, P.R. Warren
“Efficiency of Three Toothbrushes Assessed with Two Plaque Indices” I.A.D.R. Abstr. 0868
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 122 of 179

2003 M. Harris*1, B,J, MacKay1, N.C. Sharma2, J.G. Qaqish2, and J. Galustians2, 1 Johnson & Johnson Consumer Companies, Inc., Skillman, NJ, USA, 2 BioSci Research Canada Ltd., Mississauga, Canada “Effectiveness of a Novel Dental Floss Product in Reducing Plaque” J. Den Res 82 Special Issue [I.A.D.R. Abstract 2773] B357, June 2003.
2003 Cugini MA, Warren PR, Qaqish JG, Goyal CR, Sharma NC. “Plaque Removal
Efficacy of Power Toothbrushes” J. Clin Periodontal 2003; 30 (Suppl 4) :53, Abstr. 198
2002 N.C. Sharma, H.J. Galustians, J. Qaqish, M.A. Cugini & P.R. Warren “The Effect of
Two Power Toothbrushes on Calculus and Stain Formation” AJD Vol. 15, No. 2, 71- 76, April 2002
2002 J.G. Qaqish, N.C. Sharma, H.J. Galustians, M.A. Cugini, P.R. Warren “A
Comparison of Two Power Toothbrushes with Respect to Plaque Removal and Safety” J. Den Res.Special Issue [I.A.D.R. Abstract 2861] A-357, 2002
2002 C.H. Charles1*, N.C. Sharma2, J.G. Qaqish2, H.J. Galustians2, and Q. Zhao1
Pfizer Inc, Morris Plains, NJ, 2BioSci Research Canada, Ltd., Mississauga, Ontario “Comparative Antiplaque/Antigingivitis Efficacy Essential Oil Mouthrinse vs. Flossing” J. Dent. Res. 81 Special Issue A. [I.A.D.R. Abstract 2866] A358, March 2002.
2002 Naresh C. Sharma, DDS, H. Jack Galustians, BS, Jimmy Qaqish, BS, Ana
Galustians, BS, BioSci Research Canada Ltd., Mississauga, Ontario, Canada, Margaret E. Petrone, JD, Kedar N. Rustogi, DDS, Yun Po Zhang, PhD, William DiVizio, DMD, Anthony R. Volpe, DDS, MS, Colgate-Palmolive Technology Center, Piscataway, New Jersey, USA “The Clinical Efficacy of Colgate Total Plus Whitening Toothpaste Containing a Special Grade of Silica and Colgate Total Toothpaste for Controlling Breath Odor Twelve Hours After Toothbrushing: A Single-Use Clinical Study” J. Clin Dent. Vol X111 Special 2002.
2001 N.C. Sharma, H.J. Galustians, J. Qaqish & M.A. Cugini “Safety and Plaque Removal
Efficacy of a Battery-operated Power Toothbrush and a Manual Toothbrush” AJD Vol. 14 Special 9B-12B Nov. 2001
2001 Christof E. Dörfer, Eric R. von Bethlenfalvy, Thomas Pioch, H. Jack Galustians,
Jimmy Qaqish, Naresh C. Sharma “Clinical Evaluation of the Efficacy of a Battery- powered Toothbrush. Results from two Independent Studies” AJD Vol. 14 273-277 Oct. 2001.
2001 Naresh C. Sharma, DDS: Jack H. Galustians, BSc, Jimmy G. Qaqish, BSc “An
Evaluation of a Commercial Ghewing Gum in Combination with Normal Toothbrushing for Reducing Dental Plaque and Gingivitis” Compendium Special Vol 22, No. 7A, 2001
2001 Christine H. Charles, R.D.H.; Naresh C. Sharma, B.D.S., D.D.S., F.D.S.R.C.S.; H. Jack Galustians, B.Sc.; Jimmy Qaqish, B.Sc.; J. Anthony McGuire, M.S.; Jack W. Vincent, D.D.S., Ph.D. “Comparative Efficacy of an Antiseptic Mouthrinse and an Antiplaque/Antigingivitis Dentifrice – A Six Month Trial” JADA Vol. 132, May 2001.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 123 of 179
2001 N.C. Sharma1, J.G. Qaqish1, M.A. Cugini2, P.R. Warren2 (1BioSci Research Canada Ltd.,
Mississauga, Ontario, 2Oral-B Laboratories, Boston, MA) “The Effect of Two Power Toothbrushes on Calculus and Stain” J Den Res Vol 80, Special 548, 2001.
2000 Arnold M. Olshan, MS, Bruce E. Kohut, DMD, Jack W. Vincent, PhD, Loretta
C. Borden, MS, Nelly Delgado, BS, Jimmy Qaqish, BS, Naresh C. Sharma, DDS, & James A. McGuire, MS “Clinical effectiveness of essential oil-containing dentifrices in controlling oral malodor” A.J Dent Vol 13, Special 18C-22C, 2000.
2000 Christine H. Charles, RDH, BS, Jack W. Vincent, DDS, PHD, Linda Borycheski, Yuri Amatnieks, BSc (Hons), MLT, Marilyn Sarina, BMLSc, ART, MT (ASCP),
James Qaqish, BS & Howard Proskin, PhD “Effect of an essential oil-containing dentifrice on dental plaque microbial composition” A.J Dent Vol 13, Special 26C-30C, 2000.
2000 Naresh C. Sharma, DDS, Jimmy G. Qaqish, BSc, H. Jack Galustians, BSc, Dennis W.
King, PhD, Mari-Anne L. Low, RDH, MSc, Diane M. Jacobs, DDS MSc & David A. Weber PhD “An Advanced Toothbrush with Improved Plaque Removal Efficacy “ A.J. Den Vol 13, Special 15A-19A, 2000.
2000 Naresh C. Sharma, DDS, H. Jack Galustians, BSc, Jimmy Qaqish BSc, MaryAnn
Cugini RDH, MHP & Paul Warren LDS “A comparison of the Braun Oral-B 3D Plaque Remover and the Sonicare Plus Electric Toothbrush in Removing Naturally Occurring Extrinsic Staining”. A.J. Den Vol 13, No. 1: 17-20, 2000.
2000 H.J. Galustians, D.M. Jacobs*, G. Lim, J.G. Qaqish, N.C. Sharma and D.A. Weber
(BioSci Research Canada, Ltd., Mississauga, Ontario, Canada; and Oral-B Laboratories, Belmont, California, USA) J. Den. Res. 2250 Vol. 79: 425, 2000.
1999 Sharma N., Galustians J., Qaqish J., Galustians A., Rustogi K.N., Petrone M.E.,
Chaknis P., Garcia L., Volpe A.R. & Proskin H.M. “The Clinical Effectiveness of a Dentifrice Containing Triclosan and a Copolymer for Controlling Breath Odor Measured Organoleptically Twelve Hours After Toothbrushing” J. Clin. Dent. Vol. X No.4: 131-134, 1999.
1999 Sharma N., Galustians J., Qaqish J., Cugini M. “Comparison of 2 Electric Toothbrushes in Removing Extrinsic Stain” J. Den. Res. 249[I.A.D.R. Abstracts]:2467, 1999 1999 Sharma N., Galustians J., Qaqish J., Charles C., Vincent J., McGuire J.
Comparative Antiplaque/Antigingivitis Efficacy: Listerine Antiseptic Mouthrinse and Colgate Total Dentifrice” J. Den. Res. 312[I.A.D.R. Abstracts]:3138, 1999
1998 Sharma N., Qaqish J., Maykar S., Rustogi K., Preneipe M., Volpe T.
“The Clinical Efficacy of a Dentifrice containing Xylitol & Triclosan for the Reduction of Supra Gingival Plaque and Gingivitis” J.Den. Res. 77[I.A.D.R. Abstracts]: 140, 1998
1998 Sharma N., Galustians J., Qaqish J., Cugini M.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 124 of 179

“A Comparison of two electric toothbrushes with respect to plaque removal and subject preference” A. J. Den. Vol. 11, Special Issue, September 1998 - pS29-S33
1997 Sharma N., Galustians J., Qaqish J., Nathoo S.A., Viscio D.B., Rustogi K. & Gaffar
A.“Tooth Whitening with a Tartar Control Toothpaste Containing Baking Soda and Peroxide” J. Den. Res. 76[I.A.D.R. Abstracts]:95, 1997
1996 Sharma N., Galustians J., Qaqish J., Nathoo S.A., Viscio D.B., Rustogi K. & Gaffar
A."Improved cleaning with a baking soda/Peroxide/tarter control Dentifrice" J. Den. Res. 75[I.A.D.R. Abstracts]:430, 1996
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 125 of 179
4.1.5 Sponsor and Investigator Signatures
Sponsor and Investigator Signatures appear on page 2 of this report.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 126 of 179

4.1.6 Randomization Scheme and Codes
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 127 of 179
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 128 of 179

Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 129 of 179
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 130 of 179
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 131 of 179

4.1.7 Publications Referenced in the Report
Copies of publications are maintained in section 9.2 (References) of the TMF
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 132 of 179
4.2 Subject Data Listings
4.2.1 Protocol Deviations
There were no protocol deviations in this study.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 133 of 179

4.2.2 Demographic Data
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 134 of 179

Company: BURST.USA.Inc Analysis for Salus BURST PTB-1-2019
Table 1.0Demographics
Obs subjid age gender race ethnicity smoke sex trt trtin
1 1001 56 2 2 2 2 F 0 A
2 1002 43 1 2 2 2 M 1 B
3 1003 38 1 3 2 2 M 0 A
4 1004 57 2 2 2 2 F 1 B
5 1005 51 1 5 2 2 M 1 B
6 1006 45 2 2 2 2 F 1 B
7 1007 45 1 5 2 2 M 0 A
8 1008 58 2 2 2 2 F 0 A
9 1009 36 2 2 2 2 F 1 B
10 1010 44 2 2 2 2 F 0 A
11 1011 53 2 3 2 2 F 1 B
12 1012 60 1 2 2 2 M 0 A
13 1013 47 1 2 2 2 M 1 B
14 1014 40 2 3 2 2 F 1 B
15 1015 61 1 3 2 2 M 0 A
16 1017 62 2 5 2 2 F 0 A
17 1018 59 1 3 2 2 M 0 A
18 1019 59 2 3 2 2 F 0 A
19 1020 52 2 3 2 2 F 1 B
20 1021 48 2 3 2 2 F 1 B
21 1022 30 1 2 2 2 M 1 B
22 1023 20 2 3 2 2 F 0 A
23 1024 23 1 3 2 2 M 0 A
24 1025 52 2 2 2 2 F 1 B
25 1026 54 2 3 2 2 F 0 A
26 1027 43 1 3 2 2 M 1 B
27 1028 56 2 2 2 2 F 0 A
28 1029 46 2 2 2 2 F 1 B
29 1030 48 2 3 2 2 F 1 B
Page 1 of 13SAS Output
10/29/2019mhtml:file://C:\Users\sersa\Desktop\Business-SLS\Active Clients\Burst\ALL SUM-PTB-002-2019\8. Statistics&Data Management\All Sum D...
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 135 of 179

30 1031 18 1 3 2 2 M 0 A
31 1032 56 2 3 2 2 F 0 A
32 1033 54 2 5 2 2 F 1 B
33 1034 56 2 3 2 2 F 0 A
34 1035 18 2 3 2 2 F 1 B
35 1036 58 2 3 2 2 F 1 B
36 1037 46 2 3 2 2 F 0 A
37 1038 72 1 3 2 2 M 1 B
38 1039 20 1 3 2 2 M 1 B
39 1040 18 1 3 2 2 M 0 A
40 1041 34 1 3 1 2 M 0 A
41 1042 57 2 3 2 2 F 1 B
42 1043 60 2 3 2 2 F 0 A
43 1044 36 2 2 2 2 F 1 B
44 1045 54 2 2 2 2 F 0 A
45 1046 42 2 2 2 2 F 1 B
46 1047 48 2 3 2 2 F 1 B
47 1048 44 1 3 2 2 M 0 A
48 1049 46 2 3 2 2 F 0 A
49 1050 72 2 3 2 2 F 0 A
50 1051 38 2 3 2 1 F 0 A
51 1052 66 2 2 2 2 F 1 B
52 1053 61 2 3 2 2 F 1 B
53 1054 53 2 2 2 2 F 0 A
54 1055 70 1 3 2 2 M 0 A
55 1056 65 2 3 2 2 F 1 B
56 1057 56 2 2 2 2 F 1 B
57 1058 46 2 2 2 2 F 0 A
58 1059 48 2 3 2 1 F 0 A
59 1060 46 2 3 2 2 F 1 B
60 1061 36 1 5 2 2 M 1 B
61 1062 36 2 5 2 2 F 1 B
62 1063 57 1 5 2 2 M 0 A
63 1064 51 2 2 2 2 F 1 B
64
Page 2 of 13SAS Output
10/29/2019mhtml:file://C:\Users\sersa\Desktop\Business-SLS\Active Clients\Burst\ALL SUM-PTB-002-2019\8. Statistics&Data Management\All Sum D...
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 136 of 179

1065 49 2 3 2 2 F 0 A
65 1066 55 2 2 2 2 F 0 A
66 1067 51 1 2 2 2 M 0 A
67 1068 42 2 3 2 1 F 1 B
68 1069 44 1 3 2 1 M 1 B
69 1070 58 2 3 2 2 F 0 A
70 1071 55 2 3 2 2 F 0 A
71 1072 19 2 2 2 2 F 1 B
72 1073 56 2 2 2 2 F 1 B
73 1074 37 1 3 2 1 M 0 A
74 1075 51 2 3 2 2 F 1 B
75 1076 21 2 3 2 2 F 1 B
76 1077 47 1 2 2 2 M 0 A
77 1078 32 1 2 2 2 M 0 A
78 1079 53 1 5 2 2 M 0 A
79 1080 43 2 5 2 2 F 1 B
80 1081 41 2 3 2 1 F 1 B
81 1082 59 2 3 2 2 F 0 A
82 1083 42 2 2 2 2 F 1 B
83 1084 57 2 3 2 2 F 0 A
84 1085 54 1 3 2 2 M 1 B
85 1086 47 2 3 2 2 F 0 A
86 1087 36 1 5 2 2 M 0 A
87 1088 55 2 3 2 2 F 1 B
88 1089 59 2 3 2 2 F 1 B
89 1090 38 2 3 2 2 F 0 A
90 1091 48 2 5 2 2 F 1 B
91 1092 59 1 5 2 2 M 1 B
92 1093 55 2 5 2 2 F 0 A
93 1094 63 2 3 2 2 F 1 B
94 1095 46 2 2 2 2 F 1 B
95 1096 46 1 5 2 2 M 0 A
96 1097 56 2 5 2 2 F 0 A
97 1098 55 1 5 2 2 M 1 B
Page 3 of 13SAS Output
10/29/2019mhtml:file://C:\Users\sersa\Desktop\Business-SLS\Active Clients\Burst\ALL SUM-PTB-002-2019\8. Statistics&Data Management\All Sum D...
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 137 of 179

4.2.3 Individual Efficacy Response Data
Individual efficacy data listing are provided in the TMF, section 8.1
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 138 of 179

4.2.4 Statistical Report
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 139 of 179

Statistical Report
Protocol Title:
Thirty-Day Evaluation of a Sonic Power Toothbrush versus
a Manual Toothbrush on Plaque and Gingivitis Efficacy
Protocol:
BURST.USA Inc. Study Number: PTB-002-2019 All Sum Research Study Number: 2019-BR-1
FINAL
October 21, 2019
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 140 of 179

Table of Contents
Executive Summary .......................................................................................................... 3 Demographic and Baseline Data .................................................................................................. 3
Modified Gingival Index Summary ............................................................................................. 4
Bleeding Index Summary ............................................................................................................ 5
Plaque Index Summary ................................................................................................................ 7
Overall Summary ......................................................................................................................... 9
Study Synopsis and Objectives ...................................................................................... 10 Inclusion and Exclusion Criteria ................................................................................................ 10
Analysis Endpoints .................................................................................................................... 10
Sample Size and Statistical Analysis ......................................................................................... 11
Results .............................................................................................................................. 12 Demographics and Baseline....................................................................................................... 12
Modified Gingival Index ........................................................................................................... 13
Bleeding Index ........................................................................................................................... 15
Plaque Index .............................................................................................................................. 18
Conclusion ....................................................................................................................... 20 Appendix .......................................................................................................................... 21
Tables ......................................................................................................................................... 21
Data Displays ............................................................................................................................. 38
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 141 of 179
Executive Summary
The objective of this 30-day, randomized, controlled, examiner-blind, parallel design
clinical trial is to assess the safety and efficacy of twice daily use of a marketed sonic
power toothbrush (BURST Sonic) on plaque and gingivitis, compared to a manual
toothbrush when brushing with a standard fluoride dentifrice.
The two treatment groups are:
• Group 1: Twice daily brushing with ADA standard manual toothbrush and fluoride toothpaste (MB)
• Group 2: Twice daily brushing with BURST sonic toothbrush and fluoride toothpaste (SB)
This Executive Summary provides summary results of the following assessments:
Modified Gingival Index (MGI), Bleeding Index (BI), Plaque Index (PI) and changes in
healthy sites; along with efficacy comparisons of the two toothbrushes following 30 days
of use. The body of the report and the Appendix Tables provide more information.
Demographic and Baseline Data
Demographic data are given in Appendix Table 1. Ninety-seven (97) subjects were
randomized and all completed the study. The gender breakdown was 66 females and 31
males. The mean age was 48.0 with the minimum age being 18 years and the maximum
being 72 years. Six of the study participants were smokers. All baseline gingival and
plaque endpoints were comparable between toothbrushes (see Appendix Table 1). The
number of scorable sites was also comparable between treatments (see Appendix Table
1).
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 142 of 179
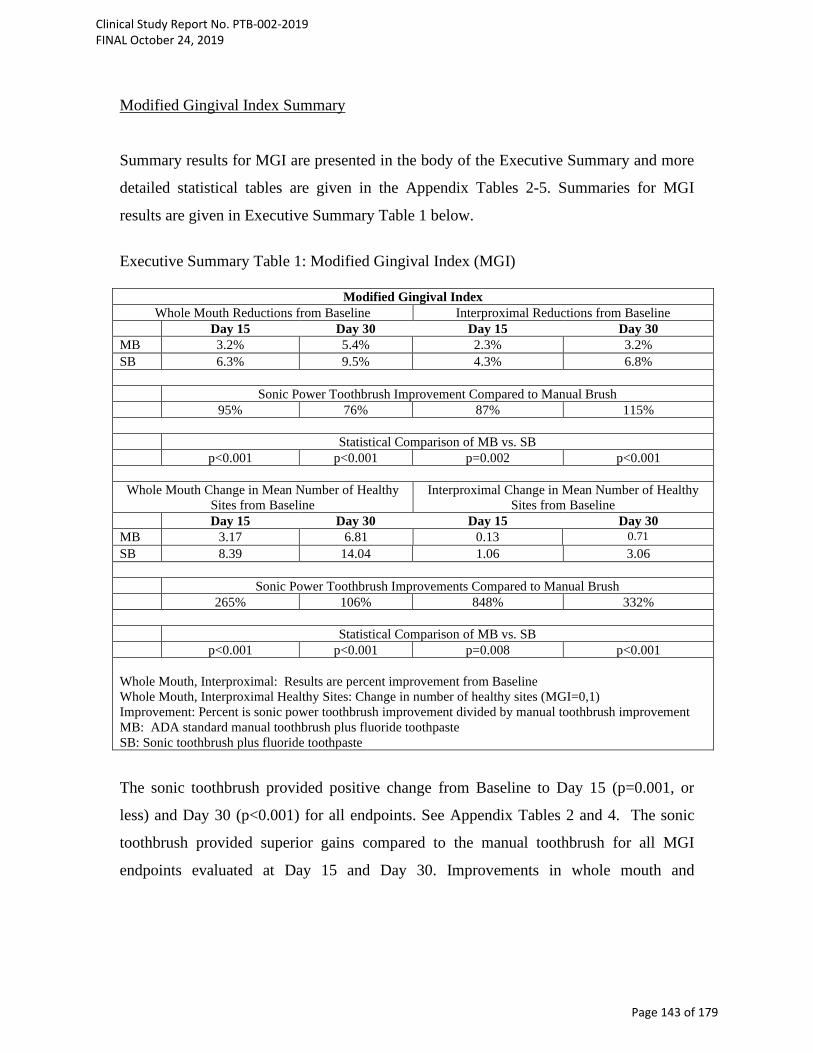
Modified Gingival Index Summary
Summary results for MGI are presented in the body of the Executive Summary and more
detailed statistical tables are given in the Appendix Tables 2-5. Summaries for MGI
results are given in Executive Summary Table 1 below.
Executive Summary Table 1: Modified Gingival Index (MGI)
Modified Gingival Index Whole Mouth Reductions from Baseline Interproximal Reductions from Baseline
Day 15 Day 30 Day 15 Day 30 MB 3.2% 5.4% 2.3% 3.2% SB 6.3% 9.5% 4.3% 6.8%
Sonic Power Toothbrush Improvement Compared to Manual Brush 95% 76% 87% 115%
Statistical Comparison of MB vs. SB
p<0.001 p<0.001 p=0.002 p<0.001
Whole Mouth Change in Mean Number of Healthy Sites from Baseline
Interproximal Change in Mean Number of Healthy Sites from Baseline
Day 15 Day 30 Day 15 Day 30 MB 3.17 6.81 0.13 0.71 SB 8.39 14.04 1.06 3.06
Sonic Power Toothbrush Improvements Compared to Manual Brush 265% 106% 848% 332%
Statistical Comparison of MB vs. SB
p<0.001 p<0.001 p=0.008 p<0.001 Whole Mouth, Interproximal: Results are percent improvement from Baseline Whole Mouth, Interproximal Healthy Sites: Change in number of healthy sites (MGI=0,1) Improvement: Percent is sonic power toothbrush improvement divided by manual toothbrush improvement MB: ADA standard manual toothbrush plus fluoride toothpaste SB: Sonic toothbrush plus fluoride toothpaste
The sonic toothbrush provided positive change from Baseline to Day 15 (p=0.001, or
less) and Day 30 (p<0.001) for all endpoints. See Appendix Tables 2 and 4. The sonic
toothbrush provided superior gains compared to the manual toothbrush for all MGI
endpoints evaluated at Day 15 and Day 30. Improvements in whole mouth and
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 143 of 179

interproximal scores were statistically significantly better when compared to the manual
toothbrush (p<0.001, for all endpoints, except p=0.002 for Day 15 interproximal sites).
The sonic toothbrush produced changes in mean number of whole mouth healthy sites at
both Day 15 and Day 30, that were statistically significantly superior to the manual
toothbrush (p<0.001, for all endpoints).
Bleeding Index Summary
Both toothbrushes provided positive change from Baseline to Day 15 (p<0.001) and Day
30 (p<0.001) for all endpoints (see Appendix Tables 6, 7, 8 and 9).
Changes to whole mouth bleeding scores were superior for the sonic toothbrush both at
Day 15 and Day 30. At Day 15 the sonic toothbrush outperformed the manual toothbrush
by 92%, and by 99% at Day 30 in reductions in the bleeding score.
The sonic toothbrush provided gains over the manual toothbrush for all gingival bleeding
endpoints evaluated at Day 15, and Day 30. Whole mouth and interproximal scores, as
well as whole mouth mean change to number of healthy bleeding sites were statistically
significant (p=0.031, or less).
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 144 of 179
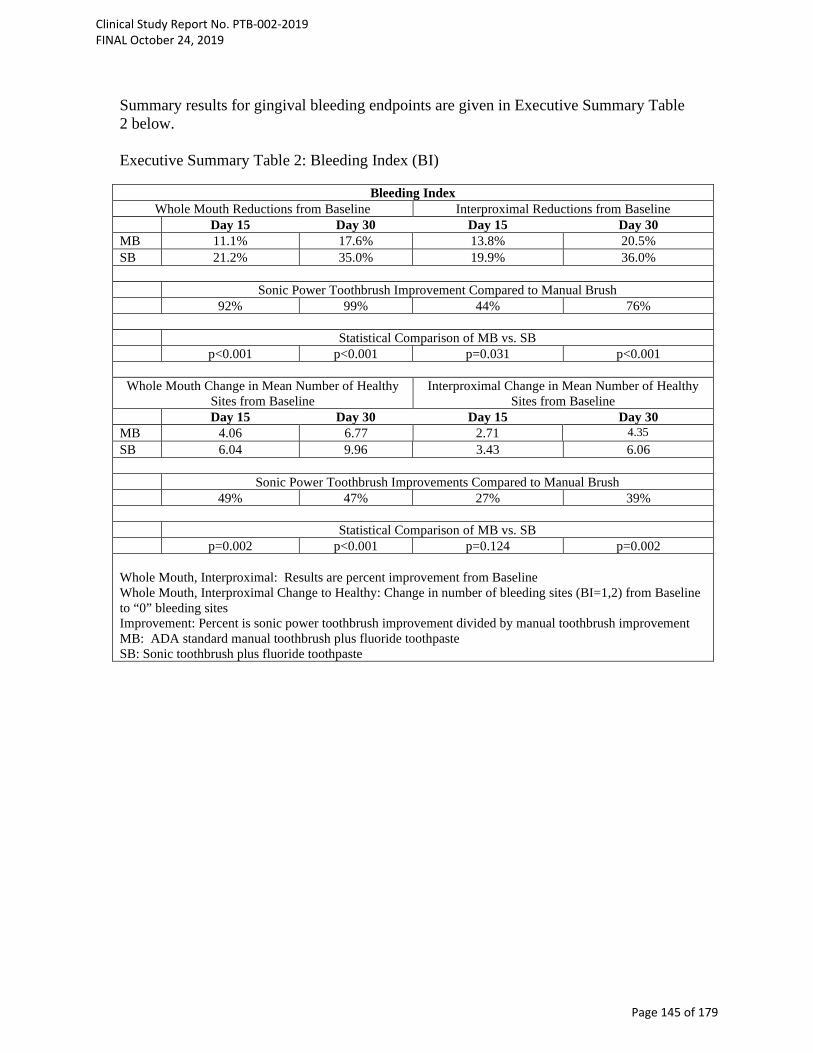
Summary results for gingival bleeding endpoints are given in Executive Summary Table 2 below. Executive Summary Table 2: Bleeding Index (BI)
Bleeding Index Whole Mouth Reductions from Baseline Interproximal Reductions from Baseline
Day 15 Day 30 Day 15 Day 30 MB 11.1% 17.6% 13.8% 20.5% SB 21.2% 35.0% 19.9% 36.0%
Sonic Power Toothbrush Improvement Compared to Manual Brush 92% 99% 44% 76%
Statistical Comparison of MB vs. SB
p<0.001 p<0.001 p=0.031 p<0.001
Whole Mouth Change in Mean Number of Healthy Sites from Baseline
Interproximal Change in Mean Number of Healthy Sites from Baseline
Day 15 Day 30 Day 15 Day 30 MB 4.06 6.77 2.71 4.35 SB 6.04 9.96 3.43 6.06
Sonic Power Toothbrush Improvements Compared to Manual Brush 49% 47% 27% 39%
Statistical Comparison of MB vs. SB
p=0.002 p<0.001 p=0.124 p=0.002 Whole Mouth, Interproximal: Results are percent improvement from Baseline Whole Mouth, Interproximal Change to Healthy: Change in number of bleeding sites (BI=1,2) from Baseline to “0” bleeding sites Improvement: Percent is sonic power toothbrush improvement divided by manual toothbrush improvement MB: ADA standard manual toothbrush plus fluoride toothpaste SB: Sonic toothbrush plus fluoride toothpaste
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 145 of 179

Plaque Index Summary
Summary results for Baseline plaque pre- to post-brushing endpoints are given in
Executive Summary Table 3 below. Both toothbrushes provided statistically significant
reductions in plaque for Baseline Pre-brushing to Post-brushing (p<0.001). The sonic
toothbrush plaque improvements for whole mouth, gumline and interproximal were
statistically significantly (p<0.001) better than the manual brush at Baseline pre - post-
brushing. The Baseline Pre-Brushing to Post-Brushing plaque reductions for the sonic
toothbrush ranged from 63.1% for gumline sites to 57.8% for interproximal sites. The
reductions for the sonic toothbrush were greater than the reductions seen with the manual
toothbrush; for whole mouth the sonic toothbrush plaque reductions exceeded the manual
toothbrush reductions by 33%.
The sonic toothbrush provided statistically significant reductions from Baseline to Day
15 (p<0.001) and Day 30 (p<0.001) for all endpoints (Whole mouth, Gumline and
Interproximal sites). See Appendix Tables 12 and 14.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 146 of 179
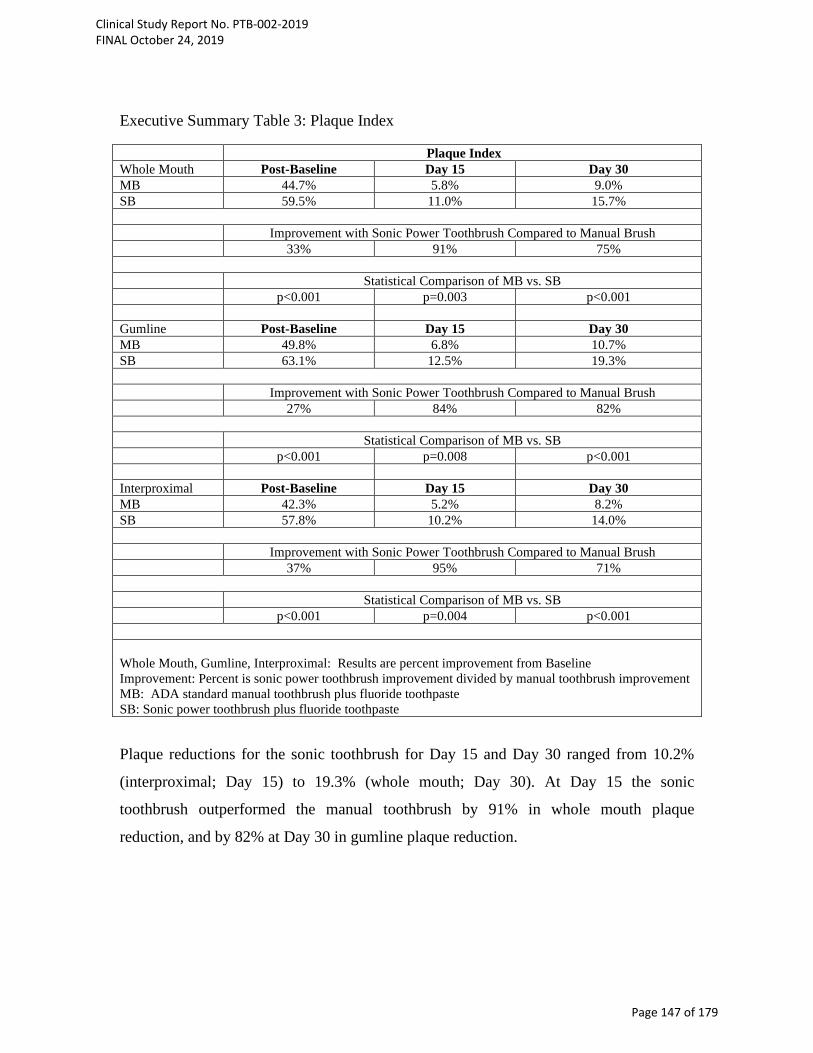
Executive Summary Table 3: Plaque Index Plaque Index Whole Mouth Post-Baseline Day 15 Day 30 MB 44.7% 5.8% 9.0% SB 59.5% 11.0% 15.7%
Improvement with Sonic Power Toothbrush Compared to Manual Brush 33% 91% 75%
Statistical Comparison of MB vs. SB p<0.001 p=0.003 p<0.001 Gumline Post-Baseline Day 15 Day 30 MB 49.8% 6.8% 10.7% SB 63.1% 12.5% 19.3%
Improvement with Sonic Power Toothbrush Compared to Manual Brush 27% 84% 82%
Statistical Comparison of MB vs. SB p<0.001 p=0.008 p<0.001 Interproximal Post-Baseline Day 15 Day 30 MB 42.3% 5.2% 8.2% SB 57.8% 10.2% 14.0%
Improvement with Sonic Power Toothbrush Compared to Manual Brush 37% 95% 71%
Statistical Comparison of MB vs. SB p<0.001 p=0.004 p<0.001 Whole Mouth, Gumline, Interproximal: Results are percent improvement from Baseline Improvement: Percent is sonic power toothbrush improvement divided by manual toothbrush improvement MB: ADA standard manual toothbrush plus fluoride toothpaste SB: Sonic power toothbrush plus fluoride toothpaste
Plaque reductions for the sonic toothbrush for Day 15 and Day 30 ranged from 10.2%
(interproximal; Day 15) to 19.3% (whole mouth; Day 30). At Day 15 the sonic
toothbrush outperformed the manual toothbrush by 91% in whole mouth plaque
reduction, and by 82% at Day 30 in gumline plaque reduction.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 147 of 179
The sonic brush whole mouth, gumline and interproximal plaque improvements at Day
15 and Day 30 were statistically significantly better than the manual brush (p=0.008, or
less).
Overall Summary
The BURST sonic toothbrush achieved clinical improvements in oral health, in particular
reductions in plaque and gingivitis. The improvements were statistically significantly
better than those of a manual toothbrush.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 148 of 179
Introduction
Study Synopsis and Objectives
This single-center, randomized, controlled, examiner-blind, 30-day, parallel study is
designed to evaluate the safety and efficacy of a sonic power toothbrush with charcoal
infused toothbrush bristles compared to an ADA reference manual soft toothbrush on
plaque and gingivitis.
Inclusion and Exclusion Criteria
See the protocol.
Analysis Endpoints
Post treatment efficacy endpoints are:
• Mean change in MGI scores at Day 15 and Day 30 for
o Whole mouth
o Interproximal (mesial & distal)
• Change in mean number of healthy sites (MGI=0,1) at Days 15 and 30
• Mean change in BI scores at Day 15 and Day 30 for
o Whole mouth
o Interproximal (mesial & distal)
• Mean change in number of bleeding sites (BI=1,2) from Baseline to “0” bleeding
sites at Day 15 and 30 for
o Whole mouth
o Interproximal (mesial & distal)
Mean change in plaque index score at Baseline Pre - Post-brushing, Day 15 and 30 for
o Whole mouth
o Gumline (marginal)
o Interproximal (mesial & distal)
Analyses were performed for Day 15 and Day 30 for each efficacy variable and Baseline
for pre - post-brushing plaque. Analyses used the ANCOVA model with treatment as a
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 149 of 179

factor and the corresponding baseline value as a covariate. For change in mean number of
healthy MGI sites the ANOVA model was used since the baseline value was typically
zero. The comparisons were made at the 0.05 level, 2-sided. Differences between the
means, 95% confidence intervals and test results will be presented.
For each efficacy variable summary statistics using appropriate descriptive statistics
(mean, median, minimum, maximum) by treatment group and overall will be provided at
each visit.
Sample Size and Statistical Analysis
In addition to what is stated in the protocol no statistical adjustments were made for multiple testing.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 150 of 179

Results Demographics and Baseline Full results are given in Appendix Table 1.
Age, gender, race, ethnicity, and smoking status were comparable among the treatments
at Baseline (see Appendix Table 1). Appendix Table 1 contains summary data for all
randomized subjects. For all randomized subjects the mean age was 48.0 years with a
standard deviation of 12.2. The gender breakdown was 66 females and 31 males. Overall,
91 subjects did not use tobacco or smokeless tobacco and 6 subjects were smokers.
Baseline comparability was conducted for all endpoints. The two (2) toothbrushes were
comparable at Baseline for gingival indices (BI: whole mouth, interproximal, p>0.575;
MGI: whole mouth, interproximal p>0.259; see Appendix Table 1). All plaque endpoints
were similar at Baseline (whole mouth, gumline, interproximal, p>0.615; see Appendix
Table 1). Also, the number of scorable sites was comparable between the two
toothbrushes (gingival sites, plaque sites, p>0.520; see Appendix Table 1).
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 151 of 179
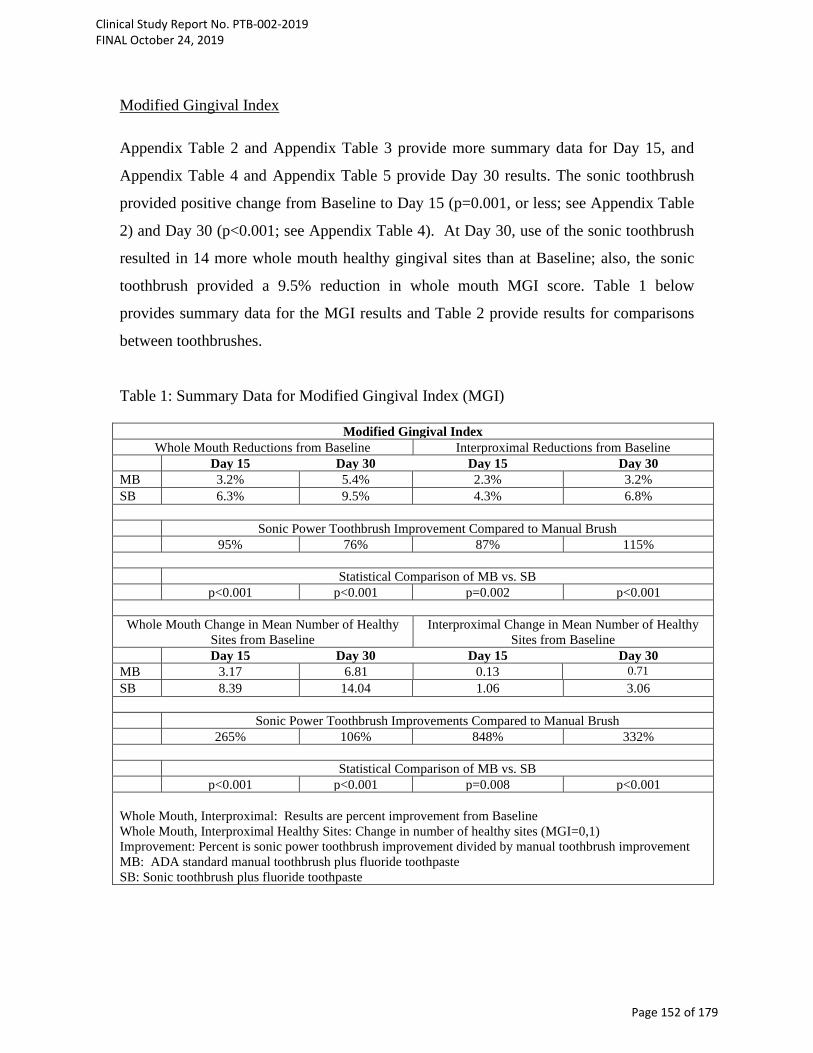
Modified Gingival Index Appendix Table 2 and Appendix Table 3 provide more summary data for Day 15, and
Appendix Table 4 and Appendix Table 5 provide Day 30 results. The sonic toothbrush
provided positive change from Baseline to Day 15 (p=0.001, or less; see Appendix Table
2) and Day 30 (p<0.001; see Appendix Table 4). At Day 30, use of the sonic toothbrush
resulted in 14 more whole mouth healthy gingival sites than at Baseline; also, the sonic
toothbrush provided a 9.5% reduction in whole mouth MGI score. Table 1 below
provides summary data for the MGI results and Table 2 provide results for comparisons
between toothbrushes.
Table 1: Summary Data for Modified Gingival Index (MGI)
Modified Gingival Index Whole Mouth Reductions from Baseline Interproximal Reductions from Baseline
Day 15 Day 30 Day 15 Day 30 MB 3.2% 5.4% 2.3% 3.2% SB 6.3% 9.5% 4.3% 6.8%
Sonic Power Toothbrush Improvement Compared to Manual Brush 95% 76% 87% 115%
Statistical Comparison of MB vs. SB
p<0.001 p<0.001 p=0.002 p<0.001
Whole Mouth Change in Mean Number of Healthy Sites from Baseline
Interproximal Change in Mean Number of Healthy Sites from Baseline
Day 15 Day 30 Day 15 Day 30 MB 3.17 6.81 0.13 0.71 SB 8.39 14.04 1.06 3.06
Sonic Power Toothbrush Improvements Compared to Manual Brush 265% 106% 848% 332%
Statistical Comparison of MB vs. SB
p<0.001 p<0.001 p=0.008 p<0.001 Whole Mouth, Interproximal: Results are percent improvement from Baseline Whole Mouth, Interproximal Healthy Sites: Change in number of healthy sites (MGI=0,1) Improvement: Percent is sonic power toothbrush improvement divided by manual toothbrush improvement MB: ADA standard manual toothbrush plus fluoride toothpaste SB: Sonic toothbrush plus fluoride toothpaste
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 152 of 179
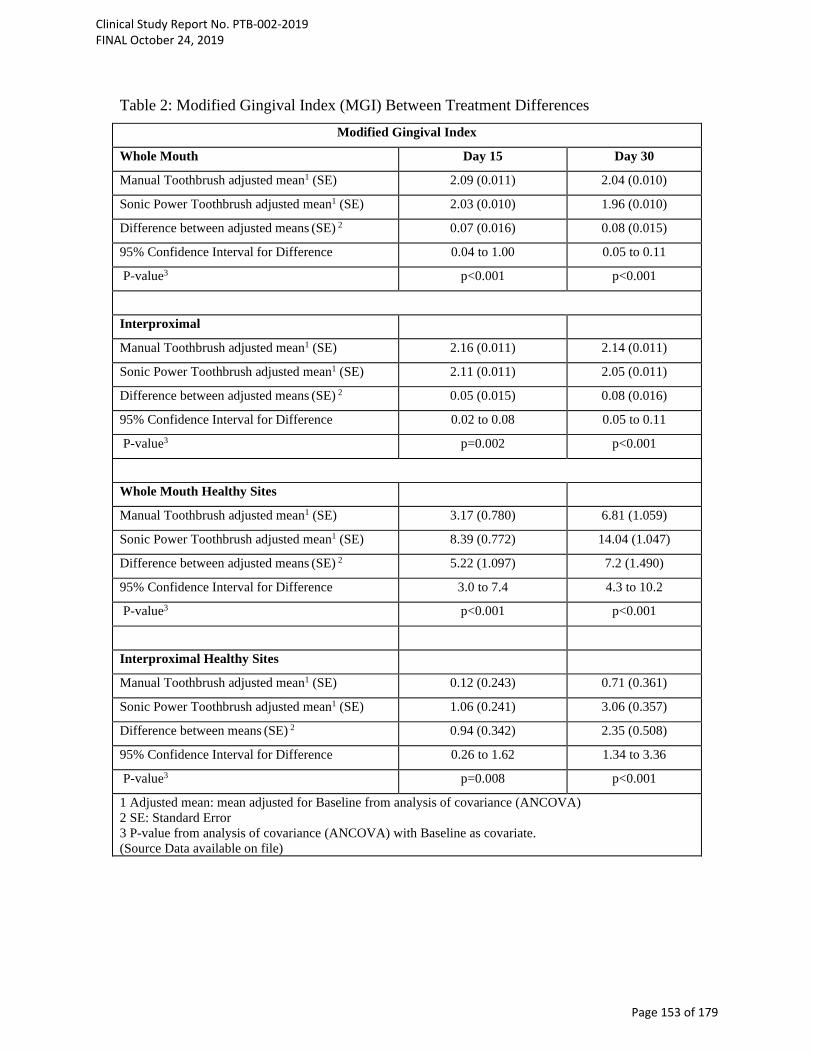
Table 2: Modified Gingival Index (MGI) Between Treatment Differences Modified Gingival Index
Whole Mouth Day 15 Day 30
Manual Toothbrush adjusted mean1 (SE) 2.09 (0.011) 2.04 (0.010)
Sonic Power Toothbrush adjusted mean1 (SE) 2.03 (0.010) 1.96 (0.010)
Difference between adjusted means (SE) 2 0.07 (0.016) 0.08 (0.015)
95% Confidence Interval for Difference 0.04 to 1.00 0.05 to 0.11
P-value3 p<0.001 p<0.001
Interproximal
Manual Toothbrush adjusted mean1 (SE) 2.16 (0.011) 2.14 (0.011)
Sonic Power Toothbrush adjusted mean1 (SE) 2.11 (0.011) 2.05 (0.011)
Difference between adjusted means (SE) 2 0.05 (0.015) 0.08 (0.016)
95% Confidence Interval for Difference 0.02 to 0.08 0.05 to 0.11
P-value3 p=0.002 p<0.001
Whole Mouth Healthy Sites
Manual Toothbrush adjusted mean1 (SE) 3.17 (0.780) 6.81 (1.059)
Sonic Power Toothbrush adjusted mean1 (SE) 8.39 (0.772) 14.04 (1.047)
Difference between adjusted means (SE) 2 5.22 (1.097) 7.2 (1.490)
95% Confidence Interval for Difference 3.0 to 7.4 4.3 to 10.2
P-value3 p<0.001 p<0.001
Interproximal Healthy Sites
Manual Toothbrush adjusted mean1 (SE) 0.12 (0.243) 0.71 (0.361)
Sonic Power Toothbrush adjusted mean1 (SE) 1.06 (0.241) 3.06 (0.357)
Difference between means (SE) 2 0.94 (0.342) 2.35 (0.508)
95% Confidence Interval for Difference 0.26 to 1.62 1.34 to 3.36
P-value3 p=0.008 p<0.001
1 Adjusted mean: mean adjusted for Baseline from analysis of covariance (ANCOVA) 2 SE: Standard Error 3 P-value from analysis of covariance (ANCOVA) with Baseline as covariate. (Source Data available on file)
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 153 of 179

The sonic toothbrush provided statistically significantly superior gains compared to the
manual toothbrush for all MGI endpoints evaluated at Day 15, and Day 30 (p=0.008, or
less).
Bleeding Index
Appendix Table 6 and Appendix Table 7 provide more summary data for Day 15, and
Appendix Table 8 and Appendix Table 9 provide Day 30 results. Both toothbrushes
provided positive change from Baseline to Day 15 (p<0.001; see Appendix Tables 6, 7)
and Day 30 (p<0.001; see Appendix Tables 8, 9).
Summaries for bleeding index results are given in Table 3 below.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 154 of 179
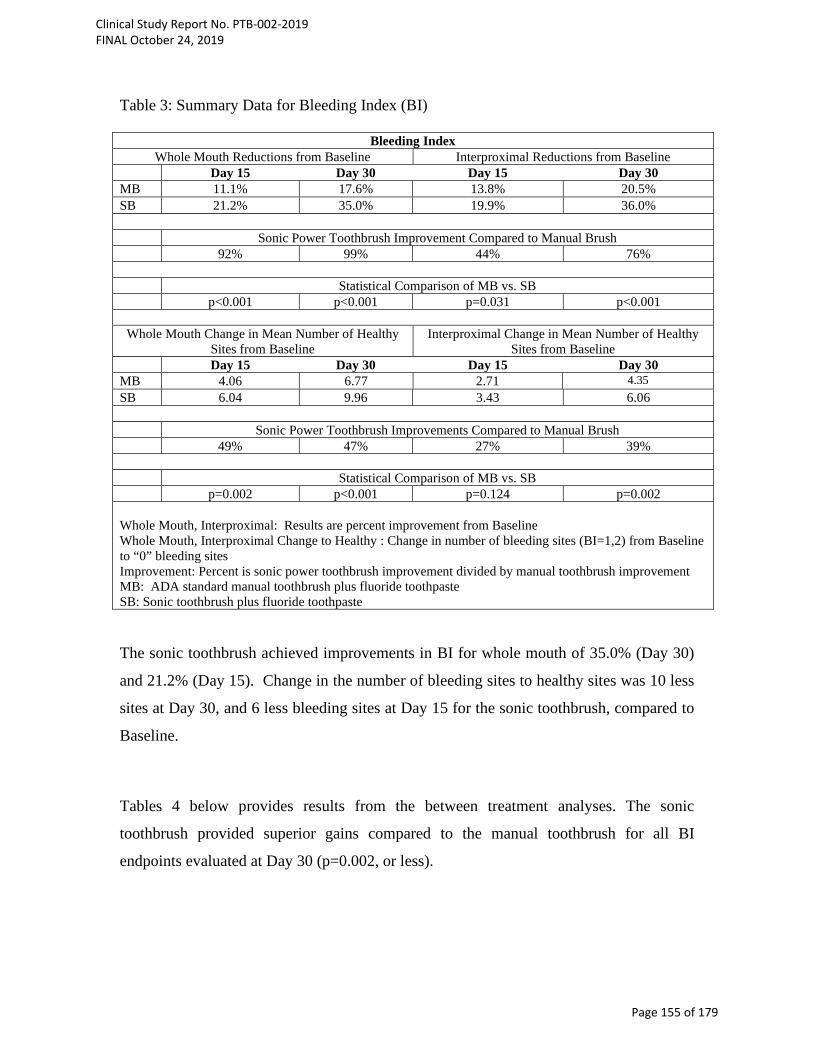
Table 3: Summary Data for Bleeding Index (BI)
Bleeding Index Whole Mouth Reductions from Baseline Interproximal Reductions from Baseline
Day 15 Day 30 Day 15 Day 30 MB 11.1% 17.6% 13.8% 20.5% SB 21.2% 35.0% 19.9% 36.0%
Sonic Power Toothbrush Improvement Compared to Manual Brush 92% 99% 44% 76%
Statistical Comparison of MB vs. SB
p<0.001 p<0.001 p=0.031 p<0.001
Whole Mouth Change in Mean Number of Healthy Sites from Baseline
Interproximal Change in Mean Number of Healthy Sites from Baseline
Day 15 Day 30 Day 15 Day 30 MB 4.06 6.77 2.71 4.35 SB 6.04 9.96 3.43 6.06
Sonic Power Toothbrush Improvements Compared to Manual Brush 49% 47% 27% 39%
Statistical Comparison of MB vs. SB
p=0.002 p<0.001 p=0.124 p=0.002 Whole Mouth, Interproximal: Results are percent improvement from Baseline Whole Mouth, Interproximal Change to Healthy : Change in number of bleeding sites (BI=1,2) from Baseline to “0” bleeding sites Improvement: Percent is sonic power toothbrush improvement divided by manual toothbrush improvement MB: ADA standard manual toothbrush plus fluoride toothpaste SB: Sonic toothbrush plus fluoride toothpaste The sonic toothbrush achieved improvements in BI for whole mouth of 35.0% (Day 30)
and 21.2% (Day 15). Change in the number of bleeding sites to healthy sites was 10 less
sites at Day 30, and 6 less bleeding sites at Day 15 for the sonic toothbrush, compared to
Baseline.
Tables 4 below provides results from the between treatment analyses. The sonic
toothbrush provided superior gains compared to the manual toothbrush for all BI
endpoints evaluated at Day 30 (p=0.002, or less).
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 155 of 179
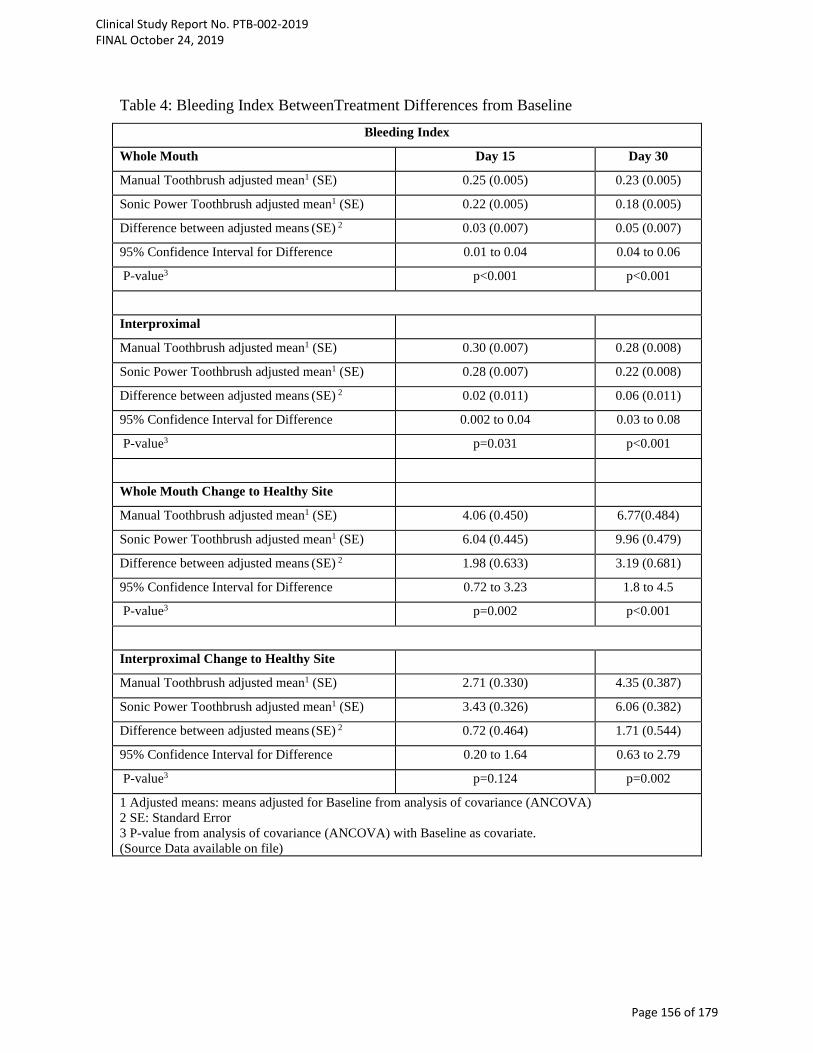
Table 4: Bleeding Index BetweenTreatment Differences from Baseline Bleeding Index
Whole Mouth Day 15 Day 30
Manual Toothbrush adjusted mean1 (SE) 0.25 (0.005) 0.23 (0.005)
Sonic Power Toothbrush adjusted mean1 (SE) 0.22 (0.005) 0.18 (0.005)
Difference between adjusted means (SE) 2 0.03 (0.007) 0.05 (0.007)
95% Confidence Interval for Difference 0.01 to 0.04 0.04 to 0.06
P-value3 p<0.001 p<0.001
Interproximal
Manual Toothbrush adjusted mean1 (SE) 0.30 (0.007) 0.28 (0.008)
Sonic Power Toothbrush adjusted mean1 (SE) 0.28 (0.007) 0.22 (0.008)
Difference between adjusted means (SE) 2 0.02 (0.011) 0.06 (0.011)
95% Confidence Interval for Difference 0.002 to 0.04 0.03 to 0.08
P-value3 p=0.031 p<0.001
Whole Mouth Change to Healthy Site
Manual Toothbrush adjusted mean1 (SE) 4.06 (0.450) 6.77(0.484)
Sonic Power Toothbrush adjusted mean1 (SE) 6.04 (0.445) 9.96 (0.479)
Difference between adjusted means (SE) 2 1.98 (0.633) 3.19 (0.681)
95% Confidence Interval for Difference 0.72 to 3.23 1.8 to 4.5
P-value3 p=0.002 p<0.001
Interproximal Change to Healthy Site
Manual Toothbrush adjusted mean1 (SE) 2.71 (0.330) 4.35 (0.387)
Sonic Power Toothbrush adjusted mean1 (SE) 3.43 (0.326) 6.06 (0.382)
Difference between adjusted means (SE) 2 0.72 (0.464) 1.71 (0.544)
95% Confidence Interval for Difference 0.20 to 1.64 0.63 to 2.79
P-value3 p=0.124 p=0.002
1 Adjusted means: means adjusted for Baseline from analysis of covariance (ANCOVA) 2 SE: Standard Error 3 P-value from analysis of covariance (ANCOVA) with Baseline as covariate. (Source Data available on file)
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 156 of 179

Plaque Index
The sonic toothbrush provided positive change from Baseline pre-post brushing
(p<0.001), from Baseline to Day 15 (p<0.001) and Day 30 (p<0.001) for all plaque
endpoints (Appendix Tables 10, 12, 14). Table 5 below gives plaque summary results. Table 5: Plaque Index Results Plaque Index Whole Mouth Post-Baseline Day 15 Day 30 MB 44.7% 5.8% 9.0% SB 59.5% 11.0% 15.7%
Improvement with Sonic Power Toothbrush Compared to Manual Brush 33% 91% 75%
Statistical Comparison of MB vs. SB p<0.001 p=0.003 p<0.001 Gumline Post-Baseline Day 15 Day 30 MB 49.8% 6.8% 10.7% SB 63.1% 12.5% 19.3%
Improvement with Sonic Power Toothbrush Compared to Manual Brush 27% 84% 82%
Statistical Comparison of MB vs. SB p<0.001 p=0.008 p<0.001 Interproximal Post-Baseline Day 15 Day 30 MB 42.3% 5.2% 8.2% SB 57.8% 10.2% 14.0%
Improvement with Sonic Power Toothbrush Compared to Manual Brush 37% 95% 71%
Statistical Comparison of MB vs. SB p<0.001 p=0.004 p<0.001 Whole Mouth, Gumline, Interproximal: Results are percent improvement from Baseline Improvement: Percent is sonic power toothbrush improvement divided by manual toothbrush improvement MB: ADA standard manual toothbrush plus fluoride toothpaste SB: Sonic power toothbrush plus fluoride toothpaste
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 157 of 179
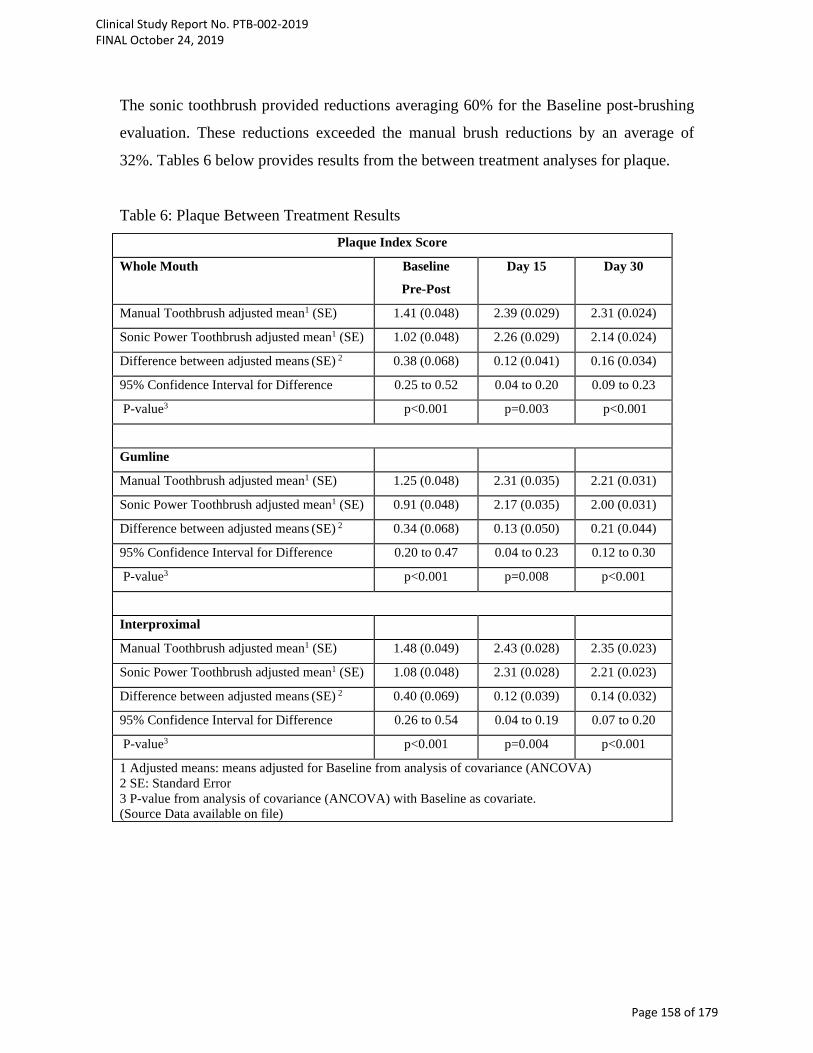
The sonic toothbrush provided reductions averaging 60% for the Baseline post-brushing
evaluation. These reductions exceeded the manual brush reductions by an average of
32%. Tables 6 below provides results from the between treatment analyses for plaque.
Table 6: Plaque Between Treatment Results Plaque Index Score
Whole Mouth Baseline
Pre-Post
Day 15 Day 30
Manual Toothbrush adjusted mean1 (SE) 1.41 (0.048) 2.39 (0.029) 2.31 (0.024)
Sonic Power Toothbrush adjusted mean1 (SE) 1.02 (0.048) 2.26 (0.029) 2.14 (0.024)
Difference between adjusted means (SE) 2 0.38 (0.068) 0.12 (0.041) 0.16 (0.034)
95% Confidence Interval for Difference 0.25 to 0.52 0.04 to 0.20 0.09 to 0.23
P-value3 p<0.001 p=0.003 p<0.001
Gumline
Manual Toothbrush adjusted mean1 (SE) 1.25 (0.048) 2.31 (0.035) 2.21 (0.031)
Sonic Power Toothbrush adjusted mean1 (SE) 0.91 (0.048) 2.17 (0.035) 2.00 (0.031)
Difference between adjusted means (SE) 2 0.34 (0.068) 0.13 (0.050) 0.21 (0.044)
95% Confidence Interval for Difference 0.20 to 0.47 0.04 to 0.23 0.12 to 0.30
P-value3 p<0.001 p=0.008 p<0.001
Interproximal
Manual Toothbrush adjusted mean1 (SE) 1.48 (0.049) 2.43 (0.028) 2.35 (0.023)
Sonic Power Toothbrush adjusted mean1 (SE) 1.08 (0.048) 2.31 (0.028) 2.21 (0.023)
Difference between adjusted means (SE) 2 0.40 (0.069) 0.12 (0.039) 0.14 (0.032)
95% Confidence Interval for Difference 0.26 to 0.54 0.04 to 0.19 0.07 to 0.20
P-value3 p<0.001 p=0.004 p<0.001
1 Adjusted means: means adjusted for Baseline from analysis of covariance (ANCOVA) 2 SE: Standard Error 3 P-value from analysis of covariance (ANCOVA) with Baseline as covariate. (Source Data available on file)
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 158 of 179

The sonic brush whole mouth, gumline and interproximal improvements at Day 15 and
Day 30 were statistically significantly better than the manual brush for all endpoints
(p=0.008, or less).
Conclusion
The BURST sonic toothbrush achieved clinical improvements in oral health, in particular
reductions in plaque and gingivitis. The improvements were statistically significantly
better than those of a standard ADA manual toothbrush.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 159 of 179
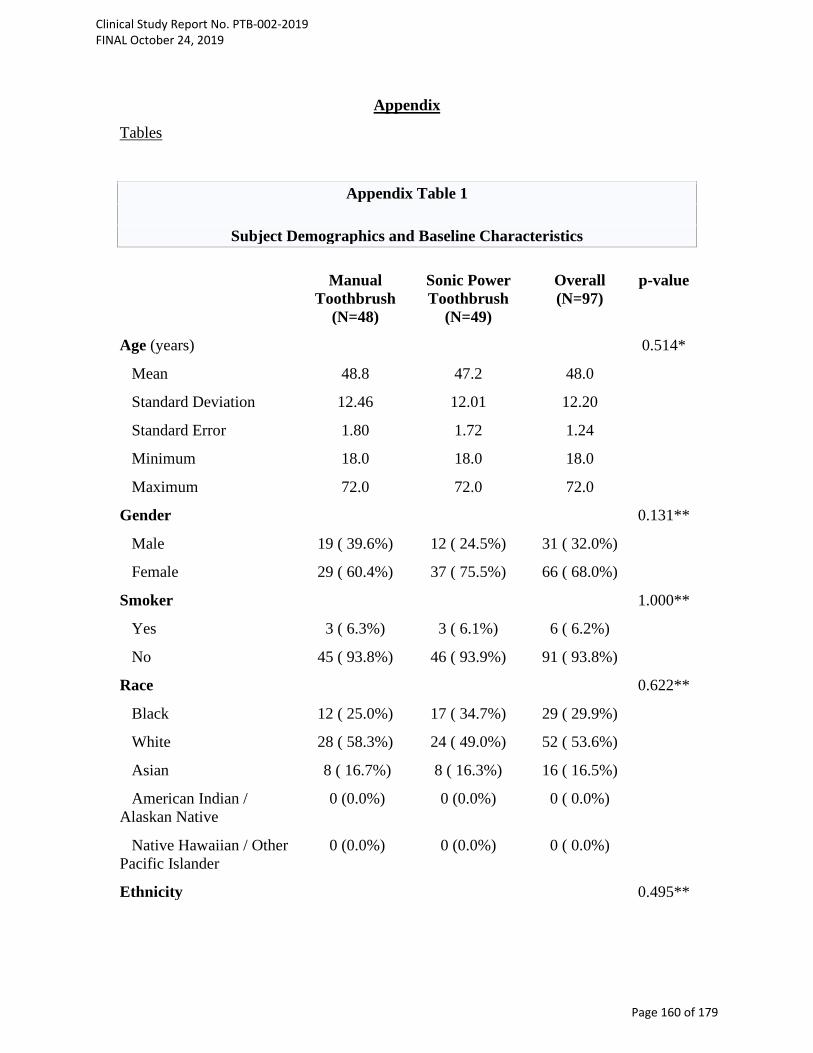
Appendix
Tables
Appendix Table 1
Subject Demographics and Baseline Characteristics
Manual Toothbrush
(N=48)
Sonic Power Toothbrush
(N=49)
Overall (N=97)
p-value
Age (years) 0.514*
Mean 48.8 47.2 48.0
Standard Deviation 12.46 12.01 12.20
Standard Error 1.80 1.72 1.24
Minimum 18.0 18.0 18.0
Maximum 72.0 72.0 72.0
Gender 0.131**
Male 19 ( 39.6%) 12 ( 24.5%) 31 ( 32.0%)
Female 29 ( 60.4%) 37 ( 75.5%) 66 ( 68.0%)
Smoker 1.000**
Yes 3 ( 6.3%) 3 ( 6.1%) 6 ( 6.2%)
No 45 ( 93.8%) 46 ( 93.9%) 91 ( 93.8%)
Race 0.622**
Black 12 ( 25.0%) 17 ( 34.7%) 29 ( 29.9%)
White 28 ( 58.3%) 24 ( 49.0%) 52 ( 53.6%)
Asian 8 ( 16.7%) 8 ( 16.3%) 16 ( 16.5%)
American Indian / Alaskan Native
0 (0.0%) 0 (0.0%) 0 ( 0.0%)
Native Hawaiian / Other Pacific Islander
0 (0.0%) 0 (0.0%) 0 ( 0.0%)
Ethnicity 0.495**
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 160 of 179
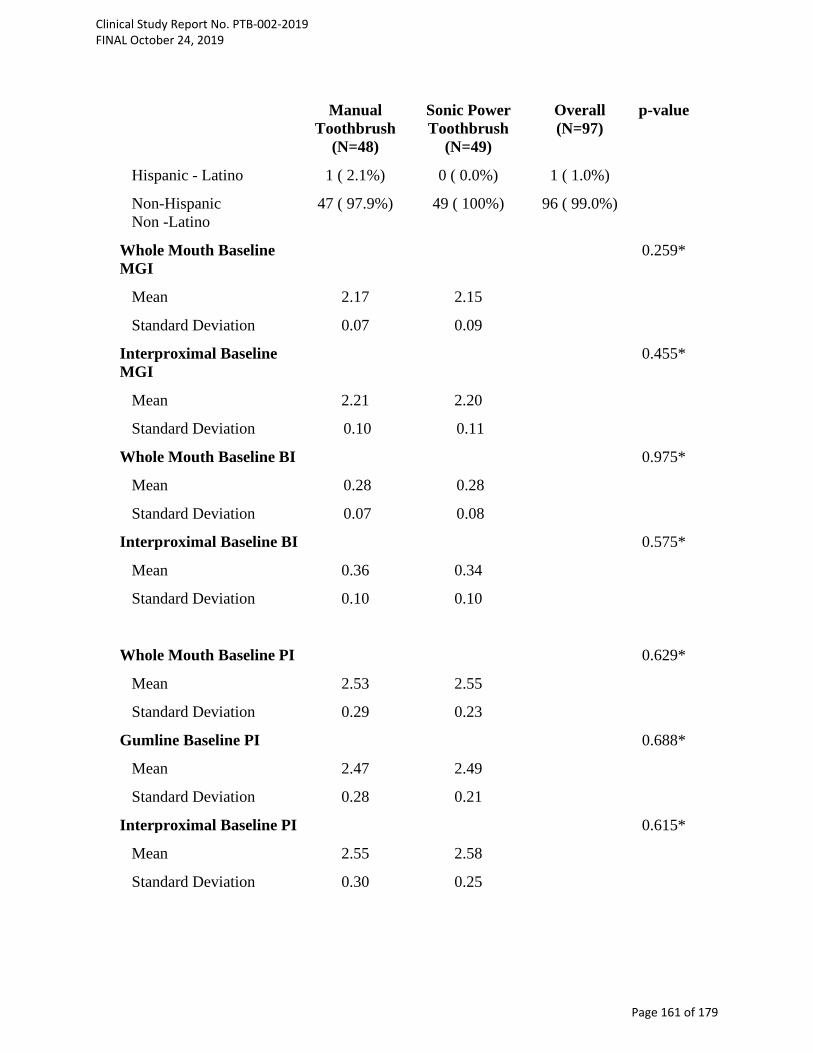
Manual
Toothbrush (N=48)
Sonic Power Toothbrush
(N=49)
Overall (N=97)
p-value
Hispanic - Latino 1 ( 2.1%) 0 ( 0.0%) 1 ( 1.0%)
Non-Hispanic Non -Latino
47 ( 97.9%) 49 ( 100%) 96 ( 99.0%)
Whole Mouth Baseline MGI
0.259*
Mean 2.17 2.15
Standard Deviation 0.07 0.09
Interproximal Baseline MGI
0.455*
Mean 2.21 2.20
Standard Deviation 0.10 0.11
Whole Mouth Baseline BI
0.975*
Mean 0.28 0.28
Standard Deviation 0.07 0.08
Interproximal Baseline BI 0.575*
Mean 0.36 0.34
Standard Deviation 0.10 0.10
Whole Mouth Baseline PI
0.629*
Mean 2.53 2.55
Standard Deviation 0.29 0.23
Gumline Baseline PI 0.688*
Mean 2.47 2.49
Standard Deviation 0.28 0.21
Interproximal Baseline PI 0.615*
Mean 2.55 2.58
Standard Deviation 0.30 0.25
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 161 of 179

Manual
Toothbrush (N=48)
Sonic Power Toothbrush
(N=49)
Overall (N=97)
p-value
Scorable (MGI, BI) Sites 0.522*
Mean 99.83 98.53
Standard Deviation 9.22 10.66
Scorable (Plaque) Sites
Mean 155.75 153.80 0.520*
Standard Deviation 13.84 15.91
* p value from ANOVA
** p value from Fisher’s Exact test
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 162 of 179
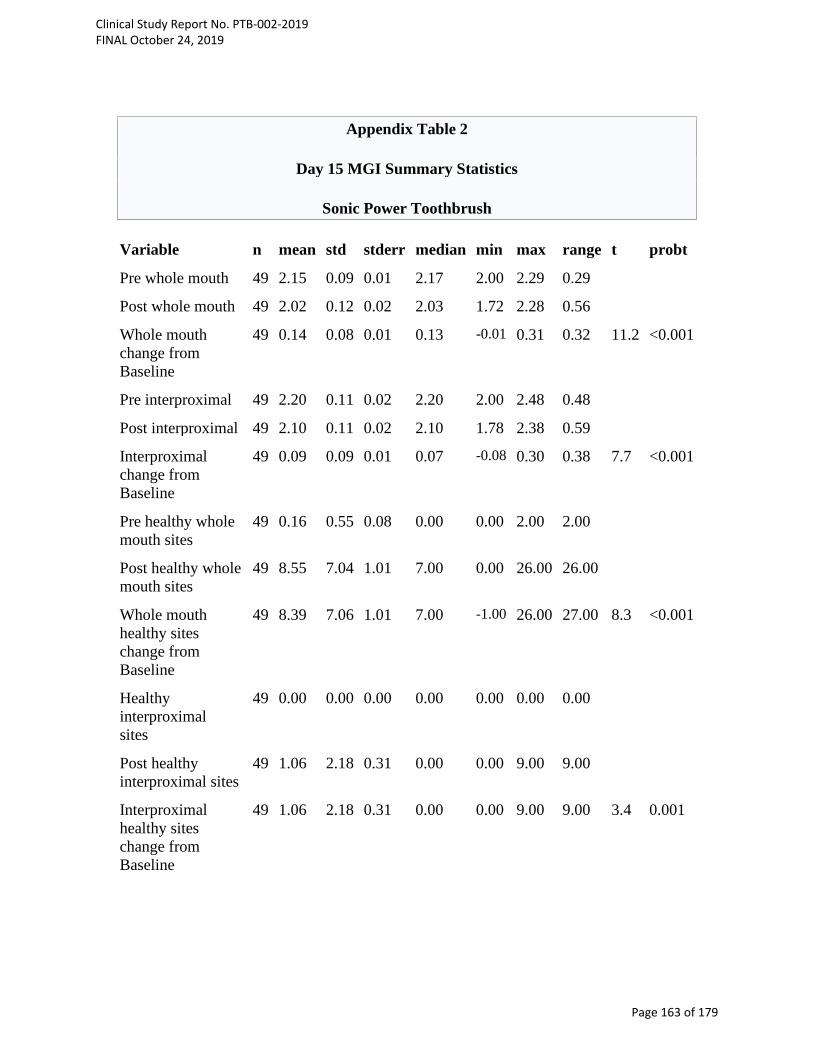
Appendix Table 2
Day 15 MGI Summary Statistics
Sonic Power Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 49 2.15 0.09 0.01 2.17 2.00 2.29 0.29
Post whole mouth 49 2.02 0.12 0.02 2.03 1.72 2.28 0.56
Whole mouth change from Baseline
49 0.14 0.08 0.01 0.13 -0.01 0.31 0.32 11.2 <0.001
Pre interproximal 49 2.20 0.11 0.02 2.20 2.00 2.48 0.48
Post interproximal 49 2.10 0.11 0.02 2.10 1.78 2.38 0.59
Interproximal change from Baseline
49 0.09 0.09 0.01 0.07 -0.08 0.30 0.38 7.7 <0.001
Pre healthy whole mouth sites
49 0.16 0.55 0.08 0.00 0.00 2.00 2.00
Post healthy whole mouth sites
49 8.55 7.04 1.01 7.00 0.00 26.00 26.00
Whole mouth healthy sites change from Baseline
49 8.39 7.06 1.01 7.00 -1.00 26.00 27.00 8.3 <0.001
Healthy interproximal sites
49 0.00 0.00 0.00 0.00 0.00 0.00 0.00
Post healthy interproximal sites
49 1.06 2.18 0.31 0.00 0.00 9.00 9.00
Interproximal healthy sites change from Baseline
49 1.06 2.18 0.31 0.00 0.00 9.00 9.00 3.4 0.001
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 163 of 179

Appendix Table 3 Day 15 MGI Summary Statistics
Manual Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 48 2.17 0.07 0.01 2.17 2.04 2.29 0.25
Post whole mouth 48 2.10 0.09 0.01 2.09 1.93 2.34 0.40
Whole mouth change from Baseline
48 0.07 0.07 0.01 0.07 -0.09 0.25 0.34 7.3 <0.001
Pre interproximal 48 2.21 0.10 0.01 2.22 2.00 2.41 0.41
Post interproximal 48 2.16 0.09 0.01 2.15 2.00 2.50 0.50
Interproximal change from Baseline
48 0.05 0.07 0.01 0.06 -0.16 0.22 0.38 4.9 <0.001
Pre healthy whole mouth sites
48 0.23 0.86 0.12 0.00 0.00 4.00 4.00
Post healthy whole mouth sites
48 3.40 3.02 0.44 3.50 0.00 9.00 9.00
Whole mouth healthy sites change from Baseline
48 3.17 2.86 0.41 3.00 0.00 9.00 9.00 7.7 <0.001
Pre healthy interproximal sites
48 0.08 0.58 0.08 0.00 0.00 4.00 4.00
Post healthy interproximal sites
48 0.21 0.71 0.10 0.00 0.00 4.00 4.00
Interproximal healthy sites change from Baseline
48 0.13 0.94 0.14 0.00 -4.00 4.00 8.00 0.9 0.360
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 164 of 179

Appendix Table 4 Day 30 MGI Summary Statistics
Sonic Power Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 49 2.15 0.09 0.01 2.17 2.00 2.29 0.29
Post whole mouth 49 1.95 0.14 0.02 1.96 1.65 2.31 0.67
Whole mouth change from Baseline
49 0.20 0.09 0.01 0.22 -0.04 0.38 0.41 16.6 <0.001
Pre interproximal 49 2.20 0.11 0.02 2.20 2.00 2.48 0.48
Post interproximal 49 2.05 0.13 0.02 2.04 1.78 2.33 0.55
Interproximal change from Baseline
49 0.15 0.09 0.01 0.15 -0.02 0.45 0.47 11.2 <0.001
Pre healthy whole mouth sites
49 0.16 0.55 0.08 0.00 0.00 2.00 2.00
Post healthy whole mouth sites
49 14.20 9.16 1.31 13.00 0.00 34.00 34.00
Whole mouth healthy sites change from Baseline
49 14.04 9.06 1.29 13.00 0.00 34.00 34.00 10.8 <0.001
Pre healthy interproximal sites
49 0.00 0.00 0.00 0.00 0.00 0.00 0.00
Post healthy interproximal sites
49 3.06 3.12 0.45 3.00 0.00 11.00 11.00
Interproximal healthy sites change from Baseline
49 3.06 3.12 0.45 3.00 0.00 11.00 11.00 6.9 <0.001
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 165 of 179

Appendix Table 5
Day 30 MGI Summary Statistics
Manual Toothbrush Variable n mean std stderr median min max range t probt
Pre whole mouth 48 2.17 0.07 0.01 2.17 2.04 2.29 0.25
Post whole mouth 48 2.05 0.10 0.01 2.05 1.84 2.26 0.42
Whole mouth change from Baseline
48 0.12 0.06 0.01 0.11 0.01 0.23 0.22 14.4 <0.001
Pre interproximal 48 2.21 0.10 0.01 2.22 2.00 2.41 0.41
Post interproximal 48 2.14 0.09 0.01 2.14 1.92 2.36 0.44
Interproximal change from Baseline
48 0.07 0.06 0.01 0.06 -0.07 0.22 0.28 8.2 <0.001
Pre healthy whole mouth sites
48 0.23 0.86 0.12 0.00 0.00 4.00 4.00
Post healthy whole mouth sites
48 7.04 5.16 0.74 8.00 0.00 22.00 22.00
Whole mouth healthy sites change from Baseline
48 6.81 5.00 0.72 7.50 0.00 22.00 22.00 9.4 <0.001
Pre healthy interproximal sites
48 0.08 0.58 0.08 0.00 0.00 4.00 4.00 1.0
Post healthy interproximal sites
48 0.79 1.50 0.22 0.00 0.00 7.00 7.00 3.7
Interproximal healthy sites change from Baseline
48 0.71 1.65 0.24 0.00 -4.00 7.00 11.00 3.0 0.005
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 166 of 179

Appendix Table 6
Day 15 Bleeding Index Summary Statistics
Sonic Power Toothbrush Variable n mean std stderr median min max range t probt
Pre whole mouth 49 0.28 0.08 0.01 0.26 0.20 0.54 0.33
Post whole mouth 49 0.22 0.07 0.01 0.21 0.09 0.43 0.34
Whole mouth change from Baseline
49 0.06 0.05 0.01 0.06 -0.03 0.23 0.26 8.5 <0.001
Pre interproximal 49 0.34 0.10 0.01 0.33 0.19 0.80 0.61
Post interproximal
49 0.28 0.09 0.01 0.27 0.10 0.52 0.42
Interproximal change from Baseline
49 0.07 0.07 0.01 0.06 -0.06 0.40 0.46 6.5 <0.001
Pre Number of whole mouth sites BI=1,2
49 25.90 5.80 0.83 24.00 21.00 53.00 32.00
Number of changes to whole mouth healthy sites BI=0
49 6.04 3.21 0.46 6.00 0.00 16.00 16.00 13.2 <0.001
Pre Number of interproximal sites BI=1,2
49 15.27 3.67 0.52 14.00 10.00 28.00 18.00
Number of changes to interproximal healthy sites BI=0
49 3.43 2.42 0.35 3.00 0.00 12.00 12.00 9.9 <0.001
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 167 of 179
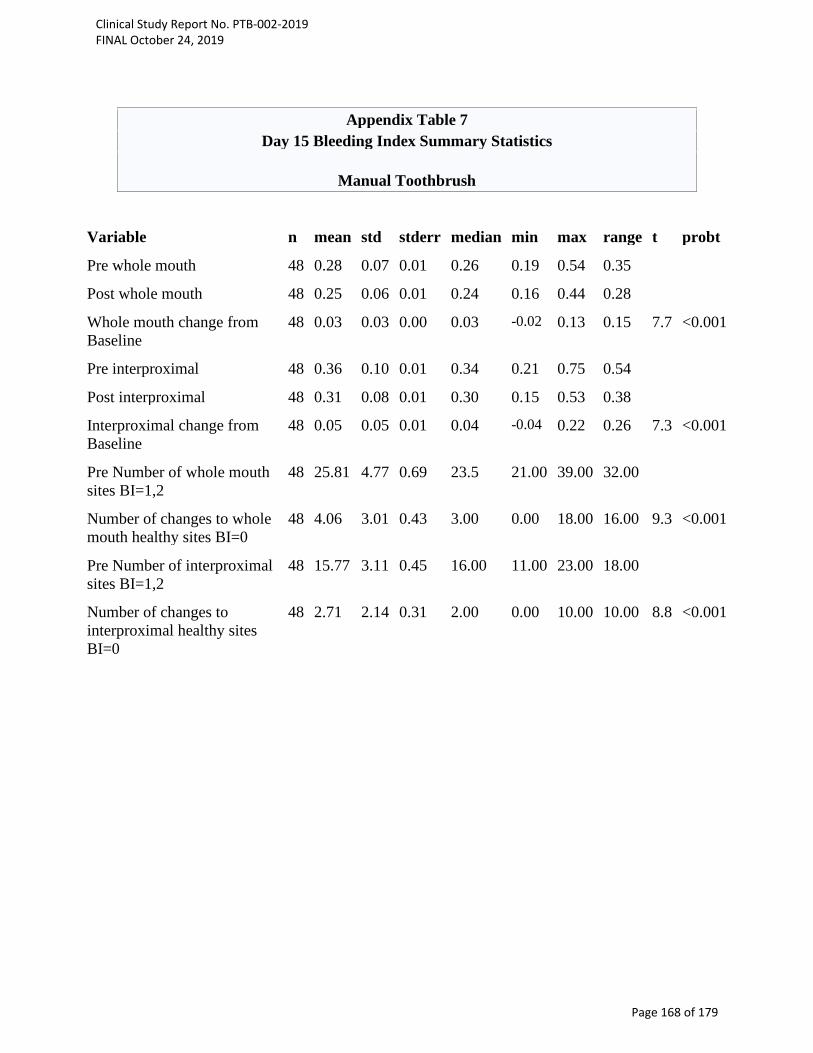
Appendix Table 7 Day 15 Bleeding Index Summary Statistics
Manual Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 48 0.28 0.07 0.01 0.26 0.19 0.54 0.35
Post whole mouth 48 0.25 0.06 0.01 0.24 0.16 0.44 0.28
Whole mouth change from Baseline
48 0.03 0.03 0.00 0.03 -0.02 0.13 0.15 7.7 <0.001
Pre interproximal 48 0.36 0.10 0.01 0.34 0.21 0.75 0.54
Post interproximal 48 0.31 0.08 0.01 0.30 0.15 0.53 0.38
Interproximal change from Baseline
48 0.05 0.05 0.01 0.04 -0.04 0.22 0.26 7.3 <0.001
Pre Number of whole mouth sites BI=1,2
48 25.81 4.77 0.69 23.5 21.00 39.00 32.00
Number of changes to whole mouth healthy sites BI=0
48 4.06 3.01 0.43 3.00 0.00 18.00 16.00 9.3 <0.001
Pre Number of interproximal sites BI=1,2
48 15.77 3.11 0.45 16.00 11.00 23.00 18.00
Number of changes to interproximal healthy sites BI=0
48 2.71 2.14 0.31 2.00 0.00 10.00 10.00 8.8 <0.001
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 168 of 179

Appendix Table 8
Day 30 Bleeding Index Summary Statistics
Sonic Power Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 49 0.28 0.08 0.01 0.26 0.20 0.54 0.33
Post whole mouth 49 0.18 0.06 0.01 0.17 0.06 0.41 0.34
Whole mouth change from Baseline
49 0.10 0.05 0.01 0.09 0.03 0.28 0.25 14.2 <0.001
Pre interproximal 49 0.34 0.10 0.01 0.33 0.19 0.80 0.61
Post interproximal 49 0.22 0.09 0.01 0.21 0.10 0.54 0.44
Interproximal change from Baseline
49 0.12 0.08 0.01 0.12 0.00 0.46 0.46 11.2 <0.001
Pre Number of whole mouth sites BI=1,2
49 25.91 5.80 0.83 24.00 21.00 53.00 32.00
Number of changes to whole mouth healthy sites BI=0
49 9.96 3.20 0.46 10.00 5.00 18.00 13.00 21.8 <0.001
Pre Number of interproximal sites BI=1,2
49 15.27 3.67 0.52 14.00 10.00 28.00 18.00
Number of changes to interproximal healthy sites BI=0
49 6.06 2.88 0.41 6.00 2.00 16.00 14.00 14.8 <0.001
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 169 of 179
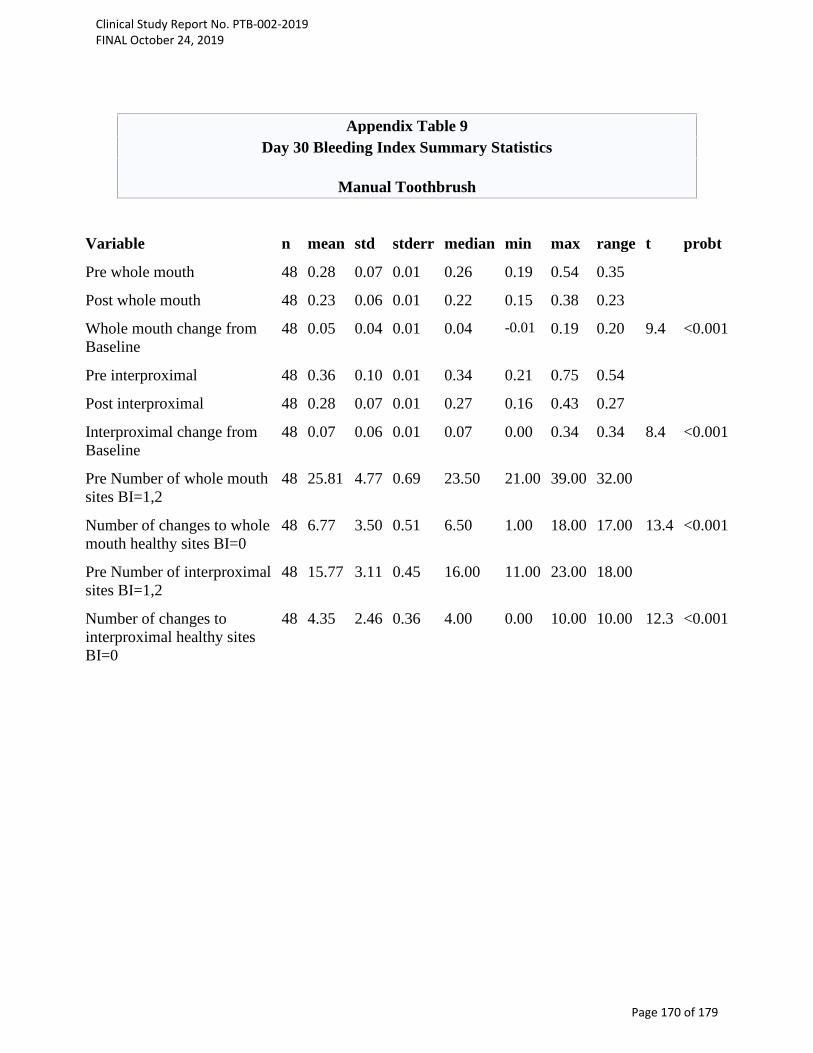
Appendix Table 9
Day 30 Bleeding Index Summary Statistics
Manual Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 48 0.28 0.07 0.01 0.26 0.19 0.54 0.35
Post whole mouth 48 0.23 0.06 0.01 0.22 0.15 0.38 0.23
Whole mouth change from Baseline
48 0.05 0.04 0.01 0.04 -0.01 0.19 0.20 9.4 <0.001
Pre interproximal 48 0.36 0.10 0.01 0.34 0.21 0.75 0.54
Post interproximal 48 0.28 0.07 0.01 0.27 0.16 0.43 0.27
Interproximal change from Baseline
48 0.07 0.06 0.01 0.07 0.00 0.34 0.34 8.4 <0.001
Pre Number of whole mouth sites BI=1,2
48 25.81 4.77 0.69 23.50 21.00 39.00 32.00
Number of changes to whole mouth healthy sites BI=0
48 6.77 3.50 0.51 6.50 1.00 18.00 17.00 13.4 <0.001
Pre Number of interproximal sites BI=1,2
48 15.77 3.11 0.45 16.00 11.00 23.00 18.00
Number of changes to interproximal healthy sites BI=0
48 4.35 2.46 0.36 4.00 0.00 10.00 10.00 12.3 <0.001
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 170 of 179
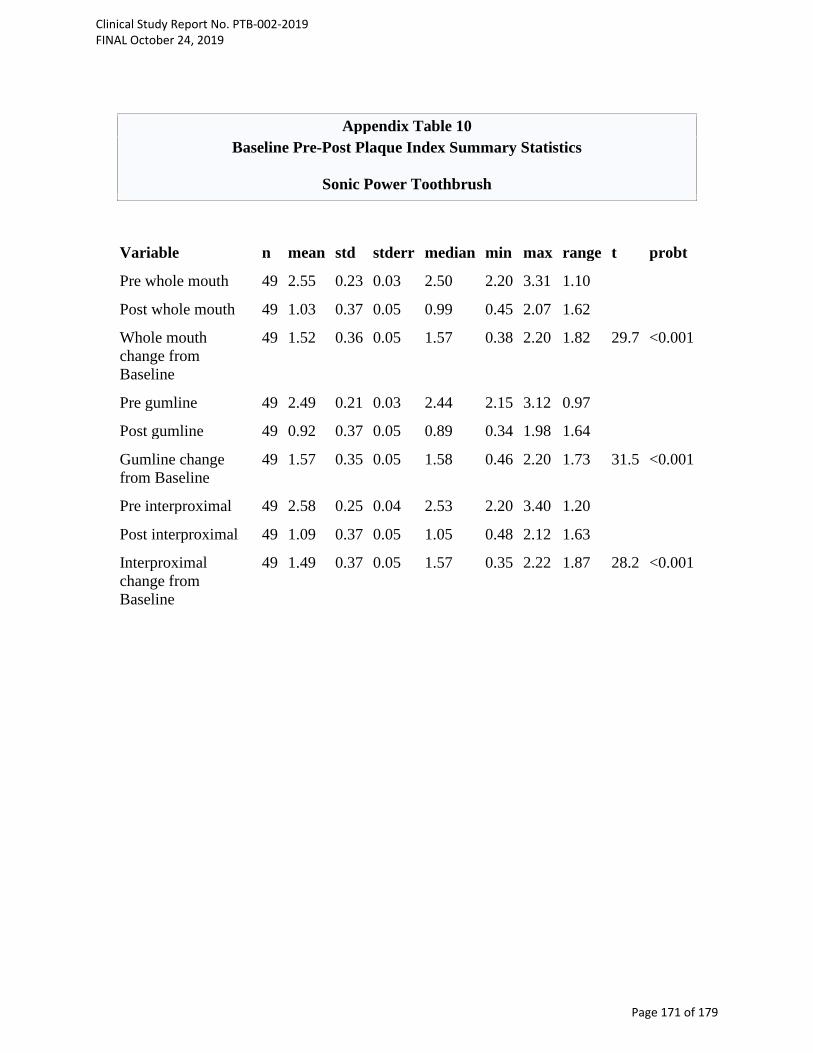
Appendix Table 10
Baseline Pre-Post Plaque Index Summary Statistics
Sonic Power Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 49 2.55 0.23 0.03 2.50 2.20 3.31 1.10
Post whole mouth 49 1.03 0.37 0.05 0.99 0.45 2.07 1.62
Whole mouth change from Baseline
49 1.52 0.36 0.05 1.57 0.38 2.20 1.82 29.7 <0.001
Pre gumline 49 2.49 0.21 0.03 2.44 2.15 3.12 0.97
Post gumline 49 0.92 0.37 0.05 0.89 0.34 1.98 1.64
Gumline change from Baseline
49 1.57 0.35 0.05 1.58 0.46 2.20 1.73 31.5 <0.001
Pre interproximal 49 2.58 0.25 0.04 2.53 2.20 3.40 1.20
Post interproximal 49 1.09 0.37 0.05 1.05 0.48 2.12 1.63
Interproximal change from Baseline
49 1.49 0.37 0.05 1.57 0.35 2.22 1.87 28.2 <0.001
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 171 of 179
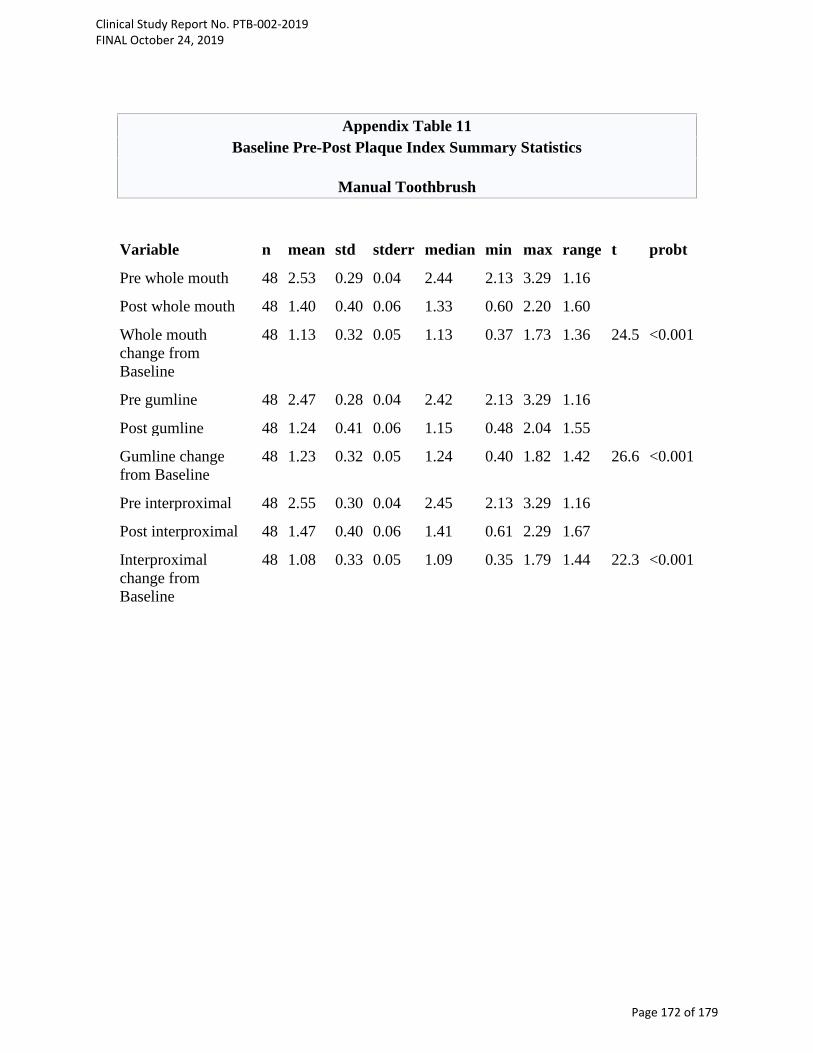
Appendix Table 11
Baseline Pre-Post Plaque Index Summary Statistics
Manual Toothbrush Variable n mean std stderr median min max range t probt
Pre whole mouth 48 2.53 0.29 0.04 2.44 2.13 3.29 1.16
Post whole mouth 48 1.40 0.40 0.06 1.33 0.60 2.20 1.60
Whole mouth change from Baseline
48 1.13 0.32 0.05 1.13 0.37 1.73 1.36 24.5 <0.001
Pre gumline 48 2.47 0.28 0.04 2.42 2.13 3.29 1.16
Post gumline 48 1.24 0.41 0.06 1.15 0.48 2.04 1.55
Gumline change from Baseline
48 1.23 0.32 0.05 1.24 0.40 1.82 1.42 26.6 <0.001
Pre interproximal 48 2.55 0.30 0.04 2.45 2.13 3.29 1.16
Post interproximal 48 1.47 0.40 0.06 1.41 0.61 2.29 1.67
Interproximal change from Baseline
48 1.08 0.33 0.05 1.09 0.35 1.79 1.44 22.3 <0.001
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 172 of 179
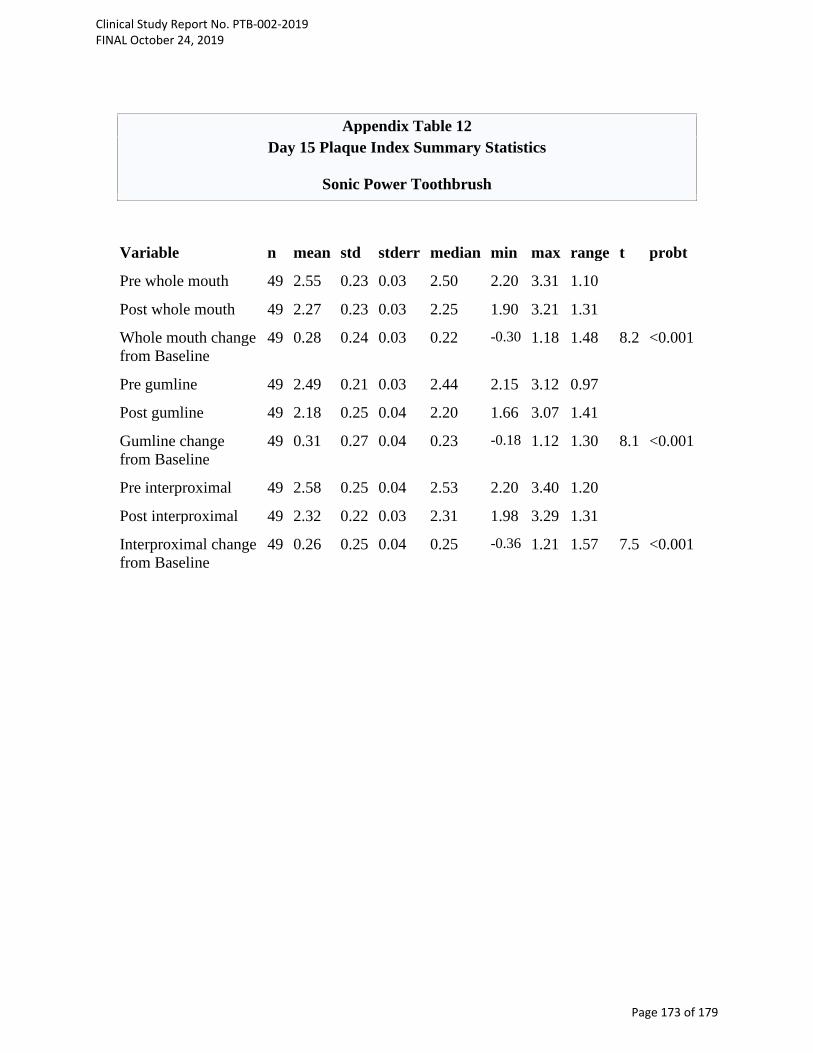
Appendix Table 12
Day 15 Plaque Index Summary Statistics
Sonic Power Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 49 2.55 0.23 0.03 2.50 2.20 3.31 1.10
Post whole mouth 49 2.27 0.23 0.03 2.25 1.90 3.21 1.31
Whole mouth change from Baseline
49 0.28 0.24 0.03 0.22 -0.30 1.18 1.48 8.2 <0.001
Pre gumline 49 2.49 0.21 0.03 2.44 2.15 3.12 0.97
Post gumline 49 2.18 0.25 0.04 2.20 1.66 3.07 1.41
Gumline change from Baseline
49 0.31 0.27 0.04 0.23 -0.18 1.12 1.30 8.1 <0.001
Pre interproximal 49 2.58 0.25 0.04 2.53 2.20 3.40 1.20
Post interproximal 49 2.32 0.22 0.03 2.31 1.98 3.29 1.31
Interproximal change from Baseline
49 0.26 0.25 0.04 0.25 -0.36 1.21 1.57 7.5 <0.001
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 173 of 179
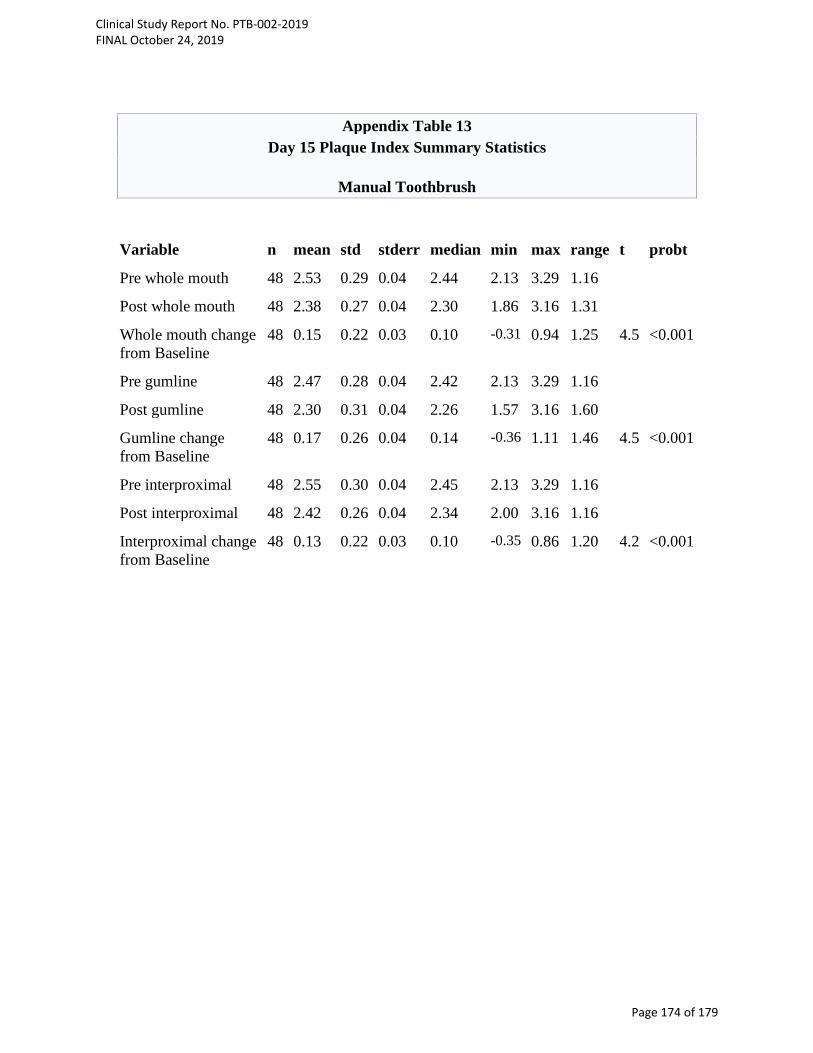
Appendix Table 13
Day 15 Plaque Index Summary Statistics
Manual Toothbrush Variable n mean std stderr median min max range t probt
Pre whole mouth 48 2.53 0.29 0.04 2.44 2.13 3.29 1.16
Post whole mouth 48 2.38 0.27 0.04 2.30 1.86 3.16 1.31
Whole mouth change from Baseline
48 0.15 0.22 0.03 0.10 -0.31 0.94 1.25 4.5 <0.001
Pre gumline 48 2.47 0.28 0.04 2.42 2.13 3.29 1.16
Post gumline 48 2.30 0.31 0.04 2.26 1.57 3.16 1.60
Gumline change from Baseline
48 0.17 0.26 0.04 0.14 -0.36 1.11 1.46 4.5 <0.001
Pre interproximal 48 2.55 0.30 0.04 2.45 2.13 3.29 1.16
Post interproximal 48 2.42 0.26 0.04 2.34 2.00 3.16 1.16
Interproximal change from Baseline
48 0.13 0.22 0.03 0.10 -0.35 0.86 1.20 4.2 <0.001
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 174 of 179

Appendix Table 14
Day 30 Plaque Index Summary Statistics
Sonic Power Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 49 2.55 0.23 0.03 2.50 2.20 3.31 1.10 77.4 <0.001
Post whole mouth 49 2.15 0.19 0.03 2.15 1.72 2.67 0.95 78.7 <0.001
Whole mouth change from Baseline
49 0.40 0.22 0.03 0.34 -0.05 0.90 0.94 12.5 <0.001
Pre gumline 49 2.49 0.21 0.03 2.44 2.15 3.12 0.97 83.1 <0.001
Post gumline 49 2.01 0.24 0.03 1.98 1.59 2.67 1.08 57.5 <0.001
Gumline change from Baseline
49 0.48 0.24 0.03 0.48 -0.05 1.06 1.11 13.8 <0.001
Pre interproximal 49 2.58 0.25 0.04 2.53 2.20 3.40 1.20 71.6 <0.001
Post interproximal 49 2.22 0.18 0.03 2.24 1.79 2.67 0.88 87.7 <0.001
Interproximal change from Baseline
49 0.36 0.24 0.03 0.29 -0.05 0.86 0.91 10.6 <0.001
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 175 of 179

Appendix Table 15
Day 30 Plaque Index Summary Statistics
Manual Toothbrush
Variable n mean std stderr median min max range t probt
Pre whole mouth 48 2.53 0.29 0.04 2.44 2.13 3.29 1.16
Post whole mouth 48 2.30 0.26 0.04 2.21 1.89 2.93 1.04
Whole mouth change from Baseline
48 0.23 0.16 0.02 0.22 -0.11 0.70 0.81 9.7 <0.001
Pre gumline 48 2.47 0.28 0.04 2.42 2.13 3.29 1.16
Post gumline 48 2.21 0.31 0.04 2.17 1.68 2.93 1.25
Gumline change from Baseline
48 0.26 0.21 0.03 0.26 -0.16 0.80 0.96 8.8 <0.001
Pre interproximal 48 2.55 0.30 0.04 2.45 2.13 3.29 1.16
Post interproximal 48 2.34 0.25 0.04 2.26 2.00 2.93 0.93
Interproximal change from Baseline
48 0.21 0.17 0.02 0.20 -0.17 0.70 0.87 8.4 <0.001
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 176 of 179
Data Displays
Computer-generated tables adhere to the following specifications. Unless otherwise
specified, the estimated mean, standard deviation, standard error, minimum, maximum
and range for a set of values should be printed to two more decimal place than the raw
(observed) data and rounded appropriately. For example, for plaque score (i.e. data in
integer values) data presentations will follow the following example given below. Parameter Data Presentation in Output
Raw data (e.g. plaque score) X
Mean X.XX
Standard Deviation (Standard Error) X.XX
Min - Max X.XX – X.XX
The p value will be printed in tables rounded to three (3) decimal places and formatted as
‘0.xxx’. P values less than 0.001 will be given in the tables as ‘p<0.001’. All fractional
numeric values are printed with a zero to the left of the decimal point (e.g., 0.8). A
percentage of less than one hundred is printed to a least one decimal place.
END OF DOCUMENT
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 177 of 179

4.2.5 Adverse Event Listings (Each Subject)
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 178 of 179

4.2.5 Adverse Event Listings (Each Subject)
Subj ID Tx Adverse Event
Severity Relationship
to Study Treatment Action Taken Outcome of AE Serious
1=Mild 2=Moderate 3=Severe
1=Unrelated 2=Possible 3=Probable 4=Definite
1=None 2=Rx Therapy 3=Discontinued
Study 4=Other
1=Resolved w/o sequelae
2=Resolved w/sequelae
3=Ongoing 4=Not recovered/
Not resolved 5=Death
1=Yes 2=No
1007 MB Headache 1 1 1 1 2
1023 MB Headache 1 1 1 1 2
1054 MB Headache 1 1 1 1 2
1057 SB Cold 1 1 1 1 2
1057 SB Cough 1 1 1 1 2
AE, adverse event; MB, manual brush; Rx, medical prescription; SB, sonic brush; Tx, treatment.
Clinical Study Report No. PTB-002-2019 FINAL October 24, 2019
Page 179 of 179







![Wits Oral History Interviews[Type the document title]€¦ · Wits Oral History Interviews[Type the document title] 10 October 2011: Kimberley Page 4 me. So when I was still with](https://img.pdfslide.us/doc/110x75/608464ae0390162c86176899/wits-oral-history-interviewstype-the-document-title-wits-oral-history-interviewstype.jpg)





















